Embed Size (px)
Citation preview

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
CHAPTER 1
Water, Acids, Bases, and Buffers
1.1 Properties of Water
Acid and base concentrations in living systems are care-fully regulated to maintain conditions compatible withnormal life. Biochemical reactions involving acids andbases occur in the body water, whereas buffer systems pro-tect the body from significant variations in the concentra-tions of acids and bases. This chapter introduces basic con-cepts of the properties of water, acids, bases, and buffers,and Chapter 39 presents a detailed discussion of both nor-mal and pathological aspects of acid–base metabolism.
Life cannot be sustained without water. Water consti-tutes 45–73% of total human body weight. It is distributedin intracellular (55%) and extracellular (45%) compart-ments and provides a continuous solvent phase betweenbody compartments. As the biological solvent, water playsa major role in all aspects of metabolism: absorption, trans-port, digestion, and excretion of inorganic and organic sub-stances as well as maintenance of body temperature. Theunique properties of water are due to its structure.
Hydrogen Bonding
Water (H2O) is a hydride of oxygen in which the highlyelectronegative oxygen atom attracts the bonding elec-trons from two hydrogen atoms. This leads to polar H–Obonds in which the hydrogen atoms have a slightly positive
charge(δ+)
and the oxygen atom has a slightly negativecharge
(δ−)
(Figure 1-1). Water molecules have a rela-tively high dipole moment because of the angle (104.5◦)of the H–O–H bond and the polarity of the bonds. Neigh-boring liquid water molecules interact with one another toform an extensive lattice-like structure similar to the struc-ture of ice. The intermolecular bonding between watermolecules arises from the attraction between the partialnegative charge on the oxygen atom and the partial positivecharge on the hydrogen atom of adjacent water molecules.This type of attraction involving a hydrogen atom is knownas a hydrogen bond (Figure 1-2).
Hydrogen bonds contain a hydrogen atom between twoelectronegative atoms (e.g., O and N). One is the formalhydrogen donor; the other is the hydrogen acceptor. Theamount of energy required to break a hydrogen bond (bondenergy) is estimated to be 2–5 kcal/mol (8.4–20.9 kJ/mol)in the gas phase. Covalent bonds have bond energies of50–100 kcal/mol (209–418 kJ/mol). The cumulative effectof many hydrogen bonds is equivalent to the stabilizingeffect of covalent bonds. In proteins, nucleic acids, andwater, hydrogen bonds are essential to stabilize overallstructure. In ice, each water molecule forms a hydrogenbond with four other water molecules, giving rise to a rigidtetrahedral arrangement (Figure 1-2). In the liquid state,water maintains a tetrahedrally coordinated structure overshort ranges and for short time periods.
MEDICAL BIOCHEMISTRY, Second EditionCopyright ©C 2002 by Academic Press. All rights of reproduction in any form reserved. 1

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
2 CHAPTER 1 Water, Acids, Bases, and Buffers
FIGURE 1-1Structure of the water molecule.
Physical Properties
Other properties of water uniquely suited to biologicalsystems include melting point, boiling point, heat of va-porization (quantity of heat energy required to transform1 g of liquid to vapor at the boiling point), heat of fusion(quantity of heat energy required to convert 1 g of solidto liquid at the melting point), specific heat (the amountof heat required to raise the temperature of 1 g of sub-stance by 1◦C, and surface tension (Table 1-1). All thesevalues for water are much higher than those for other low-molecular-weight substances because of the strong inter-molecular hydrogen bonding of water. These propertiescontribute to maintenance of temperature and to dissipa-tion of heat in living systems. Thus, water plays a majorrole in thermoregulation in living systems. The optimalbody temperature is a balance between heat production andheat dissipation. Impaired thermoregulation causes eitherhypothermia or hyperthermia and has serious metabolicconsequences; if uncorrected, impaired thermoregulationmay lead to death (Chapter 39). Water freezes to formice at 0◦C, but its maximum density is at 4◦C. Aquatic
FIGURE 1-2Tetrahedral hydrogen-bonded structure of water molecules in ice. Thetetrahedral arrangement is due to the fact that each water molecule has fourfractional charges: two negative charges due to the presence of a lone pairof electrons on the oxygen atom and two positive charges, one on each ofthe two hydrogen atoms. In the liquid phase this tetrahedral array occurstransiently.
TABLE 1-1Physical Properties of Water*
Density (at 4°C) 1.0 g/mLMolecular weight 18Liquid range 0°–100°C
Melting point 0°CBoiling point 100°C
Heat of fusion 80 cal /gHeat of vaporization 540 cal /gDipole moment 1.86 Debye unitDielectric constant (E) 78.4Solid/ liquid density ratio 0.92
*Some of these properties are measured at 1 atm pressure.
organisms survive cold winters because ice floats over andinsulates liquid water from sub-zero-degree temperature.If ice were denser than liquid water—which is the casefor most liquid-to-solid transformations—the solid formwould sink and the entire amount of fluid would solid-ify rapidly in freezing weather. During hot weather, deeplakes and oceans remain cool because heat generated bysunlight can be dissipated by evaporation of surface water.
Water is transported across cell membranes in one oftwo ways:
1. by simple diffusion through the phospholipid bilayerand
2. by the action of membrane-spanning transportproteins known as aquaporins.
Thus, the concentration of water is in thermodynamicequilibrium across the cell membrane. In the renal collect-ing duct, water is reabsorbed through a specific aquaporinchannel protein (aquaporin 2). This reabsorption of wateris regulated by the antidiuretic hormone (also known as va-sopressin). A defect or lack of functional aquaporin 2, va-sopressin, or its receptor leads to enormous loss of water inthe urine, causing the disease known as diabetes insipidus(Chapter 39). Water plays a significant role in enzymefunctions, molecular assembly of macromolecules, andallosteric regulation of proteins. For example, the effectof protein solvation in allosteric regulation is implicatedin the transition of deoxyhemoglobin to oxyhemoglobin.During this process about 60 extra water molecules bindto oxyhemoglobin (Chapter 28).
Solutes, Micelles, and Hydrophobic Interactions
Water is an excellent solvent for both ionic compounds(e.g., NaCl) and low-molecular-weight nonionic polar

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
SECTION 1.1 Properties of Water 3
compounds (e.g., sugars and alcohols). Ionic compoundsare soluble because water can overcome the electrostaticattraction between ions through solvation of the ions.Nonionic polar compounds are soluble because watermolecules can form hydrogen bonds to polar groups (e.g.,–OH).
Amphipathic compounds, which contain both largenonpolar hydrocarbon chains (hydrophobic groups) andpolar or ionic groups (hydrophilic groups) may associatewith each other in submicroscopic aggregations calledmicelles. Micelles have hydrophilic (water-liking) groupson their exterior (bonding with solvent water), and hy-drophobic (water-disliking) groups clustered in their in-terior (Figure 1-3). They occur in spherical, cylindrical,or ellipsoidal shapes. Micelle structures are stabilizedby hydrogen bonding with water, by van der Waals at-tractive forces between hydrocarbon groups in the inte-rior, and by energy of hydrophobic reactions. The lastis the stabilization energy that would be lost if each hy-drocarbon group were transferred from the hydrophobicmedium to the polar aqueous solvent. As with hydrogenbonds, each hydrophobic interaction is very weak, butmany such interactions result in formation of large, stablestructures.
A micelle may contain many hundreds of thousands ofamphipathic molecules. The interior molecular organiza-tion of micelles has been likened to a “liquid hydrocar-bon droplet.” However, a recent model departs from thisconventional concept and suggests that because of severeconstraints in the space-filling requirements of hydrocar-bon chains in the interior as well as because of micellar
FIGURE 1-3A geometrical representation of a cylindrical micelle showing thehydrocarbon chains in the micelle. The hydrophilic groups are attracted towater, and the hydrophobic chains are within the micelle. The ends of thehydrocarbon chains are nonuniformly distributed, and many are located inthe middle. The degree of disorder is much higher in the periphery than inthe center of the micelle.
geometry, the chain ends are not uniformly distributedthroughout the micelle but tend to be clustered between thecenter of the micelle and the outer surface, implying thatmany of the hydrocarbon side chains are bent back uponthemselves (Figure 1-3). In this model, there appears to bea progression from ordered (as in crystals) to disordered(as in liquids) structures proceeding from the center of themicelle to the periphery.
Hydrophobic interaction plays a major role in main-taining the structure and function of cell membranes,the activity of proteins, the anesthetic action of nonpo-lar compounds such as chloroform and nitrous oxide, theabsorption of digested fats, and the circulation of hy-drophobic molecules in the interior of micelles in bloodplasma.
Colligative Properties
The colligative properties of a solvent depend upon theconcentration of solute particles. These properties includefreezing point depression, vapor pressure depression, os-motic pressure, and boiling point elevation. The freezingpoint of water is depressed by 1.86◦C when 1 mol of non-volatile solute, which neither dissociates nor associatesin solution, is dissolved in 1 kg of water. The same con-centration of solute elevates the boiling point by 0.543◦C.Osmotic pressure is a measure of the tendency of watermolecules to migrate from a dilute to a concentrated solu-tion through a semipermeable membrane. This migrationof water molecules is termed osmosis. A solution contain-ing 1 mol of solute particles in 1 kg of water is a 1-osmolalsolution. When 1 mol of a solute (such as NaCl) that dis-sociates into two ions (Na+ and Cl−) is dissolved in 1 kgof water, the solution is 2-osmolal.
Measurement of colligative properties is useful in esti-mating solute concentrations in biological fluids. For ex-ample, in blood plasma, the normal total concentrationof solutes is remarkably constant (275–295 milliosmolal).Pathological conditions (e.g., dehydration, renal failure)involving abnormal plasma osmolality are discussed inChapter 39.
Dissociation of Water and the pH Scale
Water dissociates to yield a hydrogen ion (H+) and a hy-droxyl ion (OH−).
H2O � H+ + OH− (1.1)
The H+ bonds to the oxygen atom of an undissociatedH2O molecule to form a hydronium ion (H3O+).
H2O + H2O � H3O+ + OH−

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
4 CHAPTER 1 Water, Acids, Bases, and Buffers
Thus, water functions both as an acid (donor of H+ orproton) and as a base (acceptor of H+ or proton). This de-scription of an acid and a base follows from the Bronsted–Lowry theory. According to the Lewis theory, acids areelectron pair acceptors and bases are electron pair donors.The equilibrium constant, K , for the dissociation reactionin Equation (1.1) is
K = [H+][OH−]
[H2O](1.2)
where the square brackets refer to the molar concentrationsof the ions involved. K can be determined by measurementof the electrical conductivity of pure water, which has thevalue of 1.8 × 10−16 M at 25◦C, indicative of a very smallion concentration, where M (molar) is the units of molesper liter. Therefore, the concentration of undissociated wa-ter is essentially unchanged by the dissociation reaction.
Since 1 L of water weighs 1000 g and 1 mol of waterweighs 18 g, the molar concentration of pure water is55.5 M. Substitution for K and [H2O] in Equation (1.2)yields
[H+][OH−] = (55.5 M) × (1.8 × 10−16 M)
[H+][OH−] = 1.0 × 10−14 M2 = Kw
Kw is known as the ion product of water. In pure water,[H+] and [OH−] are equal, so that
[OH−] = [H+] = 1.0 × 10−7 M.
pH is employed to express these ion concentrations in aconvenient form, where the “p” of pH symbolizes “neg-ative logarithm (to the base 10)” of the concentration inquestion. Thus,
pH = − log10[H+] = log1
[H+]
Similarly,
pOH = − log10[OH−] = log1
[OH−]
Therefore, for water,
log[H+] + log[OH−] = log 10−14
or
pH + pOH = 14.
The pH value of 7 for pure water at 25◦C is considered tobe neutral, and values below 7 are considered acidic andabove 7 basic. Table 1-2 illustrates the pH scale extend-ing from −1 to +15. It is important to recognize that asthe pH decreases, [H+] increases. A decrease in one pHunit reflects a 10-fold increase in H+ concentration. In
TABLE 1-2The pH Scale
[H+], M pH [OH–], M
10.0 –1 10–15
1.0 0 10–14
0.1 1 10–13
0.01(10–2) 2 10–12
10–3 3 10–11
10–4 4 10–10
10–5 5 10–9
10–6 6 10–8
10–7 7 Neutral 10–7
10–8 8 10–6
10–9 9 10–5
10–10 10 10–4
10–11 11 10–3
10–12 12 0.0110–13 13 0.110–14 14 110–15 15 10
Acidic
Basic
discussions of acid–base problems in human biochem-istry, it is often preferable to express H+ concentrationas nanomoles per liter (nmol/L).
1.2 Buffers
Buffers resist change in pH in solutions when acids orbases are added. They are either a mixture of a weak acid(HA) and its conjugate base (A−) or a mixture of a weakbase (B) and its conjugate acid (HB+).
EXAMPLE 1 Acetic acid (CH3COOH) and car-bonic acid (H2CO3) are weak acids. Ammonia(NH3) is a weak base. CH3COOH/CH3COO−,H2CO3/HCO−
3 , and NH3/NH+4 constitute buffer
systems.
A buffer solution functions in the following mannerto resist changes in acidity or alkalinity. In an aceticacid/sodium acetate buffer system, the species presentin solution are CH3COOH, CH3COO−, Na+, and H2O.Amounts of H+ and OH− are initially assumed to be small.
When acid is added to the buffer, almost all of theH+ ions react with acetate ions to produce weakly ion-ized acetic acid (H+ + CH3COO− � CH3COOH). TheH+ ions are thereby prevented from appreciably changingthe pH.

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
SECTION 1.2 Buffers 5
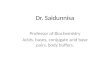
FIGURE 1-4Titration profile of acetic acid (CH3COOH) with sodium hydroxide(NaOH). Maximum buffering capacity is at pH = pK′, at which pointminimal change in pH occurs upon addition of acid or base.
When OH− is added, almost all of the hydroxyl radicalsreact with acetic acid molecules to produce more acetateions and water (OH−+ CH3COOH � CH3COO−+ H2O).The additional OH− is thus consumed with little increasein pH.
Adding H+ or OH− to a buffer causes only slight pHchanges provided there is excess salt (CH3COO−) or acid(CH3COOH). If all of the acid is converted to the salt formby the addition of a large amount of OH−, the solution canno longer behave as a buffer. Adding more OH− will causethe pH to rise rapidly, as if the solution contained no bufferor only salt. The maximum buffering capacity exists whenthe molarities of the salt and acid are equal, i.e., when pH =pK′ (or − log K′). The pK′ is at an inflection point on thetitration curve and hence is the point of minimum slope orminimum change in pH for a given addition of acid or base(Figure 1-4). In a generalized weak acid buffer reaction,
H2O + HA � H3O+ + A−
a hydronium ion, H3O+, is formed by the association of ahydrogen ion with a water molecule. In dilute solutions,the concentration of water changes very little when HA isadded; therefore, by convention, the dissociation reactionequation is usually written as
HA � H+ + A− (1.3)
A weak acid, HA, does not readily dissociate, owingto the high affinity of the conjugate base, A−, for thehydrogen ion. Similarly in the hydrolysis reaction of a
weak base (B) and water, the ions OH− and HB+ (theconjugate acid) are produced.
B + H2O � HB+ + OH−
The concentration of the conjugate base (or acid)generated from a weak acid (or base) is small, since,by definition, weak acids and bases are only slightlydissociated in aqueous solution. Examples of weak acidsare organic acids (e.g., acetic) and of strong acids aremineral acids (e.g., hydrochloric and sulfuric).
Henderson–Hasselbalch Equation
The Henderson–Hasselbalch equation was developed inthe early part of this century independently by the Amer-ican biological chemist L.J. Henderson and the Swedishphysiologist K.A. Hasselbalch, for relating the pH to thebicarbonate buffer system of the blood (see below). In itsgeneral form, the Henderson–Hasselbalch equation is auseful expression for buffer calculations. It can be derivedfrom the equilibrium constant expression for a dissociationreaction of the general weak acid (HA) in Equation (1.3):
K = [H+][A−]
[HA](1.4)
where K is the equilibrium constant at a given temper-ature. For a defined set of experimental conditions, thisequilibrium constant is designated as K ′ (K prime) and re-ferred to as an apparent dissociation constant. The higherthe value of K ′, the greater the number of H+ ions liber-ated per mole of acid in solution and hence the strongerthe acid. K ′ is thus a measure of the strength of an acid.Rearrangement of Equation (1.4) yields
[H+] = K ′[HA]
[A−](1.5)
Taking logarithms of both sides of Equation (1.5) and mul-tiplying throughout by −1 gives
− log[H+] = − log K ′ − log[HA] + log[A−] (1.6)
Substituting pH for − log[H+] and pK′ for − log K ′ yields
pH = pK′ + log[A−]
[HA](1.7)
or
pH = pK′ + log[conjugate base]
[acid](1.8)
This relationship is represented by the Henderson–Hasselbalch equation.
Since a buffer is intended to give only a small changein pH with added H+ or OH−, the best buffer for a givenpH is the one that gives the smallest change. As may be

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
6 CHAPTER 1 Water, Acids, Bases, and Buffers
TABLE 1-3Percent Unprotonated Species and Ratio of UnprotonatedForms Relative to the Difference between the pH and pK′*
Log [A–] / [HA]%A– [A–] / [HA] (pH – pK′)
“100” 999/1 3.0099 99/1 2.0098 98/2 1.6996 96/4 1.3894 94/6 1.2092 92/8 1.0691 91/9 1.0090 90/10 0.9580 80/20 0.6070 70/30 0.3760 60/40 0.1850 50/50 0.0040 40/60 – 0.1830 30/70 – 0.3720 20/80 – 0.6010 10/90 – 0.958 8/92 –1.066 6/94 –1.204 4/96 –1.382 2/98 –1.691 1/99 –2.00
“0” 1/999 –3.00
*Reproduced, with permission, from J. N. Aronson: The Henderson-Hasselbalch equation revisited. Biochemical Education 11(2), 68(1981).
seen from the Henderson–Hasselbalch equation, when thepH of the solution equals the pK′ of the buffer, [conju-gate base] = [acid], and the buffer can therefore respondequally to both added acid and added base. It also followsfrom Equation (1.7) that when the pH of the solution is onepH unit above or below the pK′ value, the solution containsapproximately 9% unprotonated or protonated species, re-spectively. Similarly, if the pH of the solution is two unitsabove or below the pK′ value, the solution contains almostentirely (99%) unprotonated or protonated species, respec-tively. Table 1-3 provides percent unprotonated speciesand the corresponding unprotonated/protonated ratios forselected (pH–pK′) values.
Buffer Systems of Blood and Exchangeof O2 and CO2
If the H+ concentration departs significantly from its nor-mal value in blood, the health and survival of the human
TABLE 1-4pH Values of Human Body Fluids and Secretions
Body Fluid or Secretion pH
Blood 7.4Milk 6.6–6.9Hepatic bile 7.4–8.5Gall bladder bile 5.4–6.9Urine (normal) 6.0Gastric juice (parietal secretion) 0.87Pancreatic juice 8.0Intestinal juice 7.7Cerebrospinal fluid 7.4Saliva 7.2Aqueous humor of eye 7.2Tears 7.4Urine (range in various disease 4.8–7.5
states)Feces 7.0–7.5
Muscle cell, resting 6.94–7.06(at 37°C; extracellular pH = 7.4) (intracellular)
body are in jeopardy. H+ is the smallest ion, and it com-bines with many negatively charged and neutral functionalgroups. Changes of [H+], therefore, affect the chargedregions of many molecular structures, such as enzymes,cell membranes, and nucleic acids, and dramatically al-ter physiological activity. If the plasma pH reaches either6.8 or 7.8, death may be unavoidable. Despite the fact thatlarge amounts of acidic and basic metabolites are producedand eliminated from the body, buffer systems maintain afairly constant pH in body fluids (Table 1-4).
The major metabolic product from oxidation of ingestedcarbon compounds is CO2. Hydration of CO2 dissolvedin water yields the weak acid H2CO3 (carbonic acid).Depending on the type of food ingested and oxidized,0.7–1.0 mol of CO2 is produced per mole of O2 consumed.This results in the metabolic production of about 13 molof hydrated CO2 each day in a normal person.
For efficient transport of relatively insoluble CO2 fromthe tissues where it is formed to the lungs where it mustbe exhaled, the buffers of the blood convert CO2 to thevery soluble anionic form HCO−
3 (bicarbonate ion). Theprincipal buffers in blood are bicarbonate-carbonic acid inplasma, hemoglobin in red blood cells, and protein func-tional groups in both. The normal balance between ratesof elimination and production of CO2 yields a steady-stateconcentration CO2 in the body fluids and a relatively con-stant pH.

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
SECTION 1.2 Buffers 7
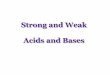
FIGURE 1-5Schematic representation of the transport of CO2 from the tissues to the blood. Note that the majority of CO2 istransported as HCO−
3 in the plasma and that the principal buffer in the red blood cell is hemoglobin. Solid lines refer tomajor pathways, and broken lines refer to minor pathways. Hb = hemoglobin.
Other acids that are products of metabolism are lacticacid, acetoacetic acid, β-hydroxybutyric acid, phospho-ric acid, sulfuric acid, and hydrochloric acid. The organicacids (e.g., lactate, acetoacetate, and β-hydroxybutyrate)are normally oxidized further to CO2 and H2O. Thehydrogen ions and anions contributed by mineral acidsand any unmetabolized organic acids are eliminated viathe excretory system of the kidneys. Thus, although bodymetabolism produces a large amount of acid, a constant pHis maintained by transport of H+ ions and other acid an-ions in buffer systems and by elimination of CO2 throughalveolar ventilation in the lungs and through excretion ofaqueous acids in the urine.
Metabolic activities continuously release CO2 to theblood (Figure 1-5), and the lungs continuously elimi-nate CO2 (Figure 1-6). As oxygen is consumed in pe-ripheral tissues, CO2 is formed and its pressure (PCO2 )builds to about 50 mm Hg, whereas the blood enteringthe tissue capillaries has a PCO2 of about 40 mm Hg.Because of this difference in PCO2 values, CO2 diffusesthrough the cell membranes of the capillary endotheliumand the blood PCO2 rises to 45–46 mm Hg. Despite thisincrease in PCO2 , the blood pH value drops by only about0.03 during the flow from the arterial capillary (pH 7.41)to the venous capillary (pH 7.38) as a consequence ofbuffering.
About 95% of the CO2 entering the blood diffuses intothe red blood cells. Within the red blood cells, the enzymecarbonic anhydrase catalyzes conversion of most of the
CO2 to H2CO3:
CO2 + H2O � H2CO3
H2CO3 dissociates to H+ and HCO−3 . Although H2CO3
is a weak acid, its dissociation is essentially 100% be-cause of removal of H+ ions by the buffering action ofhemoglobin. The presence of CO2 and the production ofH+ cause a reduction in the affinity of hemoglobin foroxygen. Oxyhemoglobin (HbO2) consequently dissoci-ates into oxygen and deoxyhemoglobin (Hb). This effectof pH on the binding of O2 to hemoglobin is known as theBohr effect (Chapter 28).
Oxygen diffuses into the tissues because the PO2 inblood is greater than the PO2 in tissue cells and be-cause protonated deoxyhemoglobin (HHb) is a weakeracid than HbO2 and thereby binds H+ more stronglythan HbO2. When purified HbO2 dissociates at pH 7.4to yield oxygen and Hb, the Hb binds 0.7 mol of H+ permole of oxygen released. However, under physiologicalconditions in whole blood, the Hb combines 0.31 molof H+ per mole of oxygen released. This process is re-versible. The remainder of the H+ is buffered by phos-phate and proteins other than hemoglobin. The majorbuffering group involved in the transport of H+ is an im-idazolium group of a histidine residue in hemoglobin.The imidazolium group has a pK′ value of about 6.5(Figure 1-7 depicts the reactions). The difference in acid–base properties between the two forms of hemoglobinmolecules is explained by the conformational change that

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
8 CHAPTER 1 Water, Acids, Bases, and Buffers
FIGURE 1-6Schematic representation of the transfer of CO2 from the alveolus (and its loss in the expired air in the lungs) andoxygenation of hemoglobin. Note that the sequence of events occurring in the pulmonary capillaries is the opposite ofthe process taking place in the tissue capillaries (Figure 1-5). Solid lines indicate major pathways and broken linesindicate minor pathways. Hb = hemoglobin.
accompanies conversion from HbO2 to HHb+ (Chapters7 and 28).
As the concentration of HCO−3 (i.e., of metabolic CO2)
in red blood cells increases, an imbalance occurs betweenthe bicarbonate ion concentrations in the red blood cell andplasma. This osmotic imbalance causes a marked effluxof HCO−
3 to plasma and consequent influx of Cl− fromplasma in order to maintain the balance of electrostaticcharges. The latter osmotic influx, known as the chlorideshift, is accompanied by migration of water to red bloodcells. Thus, transport of metabolic CO2 in the blood occursprimarily in the form of plasma bicarbonate formed afterCO2 diffuses into red blood cells.
FIGURE 1-7Buffer function of the imidazole/imidazolium functional groups ofhistidine residues in protein.
A small percentage of CO2 entering the red bloodcells combines reversibly with an un-ionized amino group(–NH2) of hemoglobin:
hemoglobin–NH2 + CO2 � hemoglobin–NH–COO−+ H+
Hemoglobin–NH–COO−, commonly known as car-baminohemoglobin, is more correctly named hemoglobincarbamate. Formation of this compound causes a low-ering of the affinity of hemoglobin for oxygen. Thus,an elevated concentration of CO2 favors dissociation ofoxyhemoglobin to oxygen and deoxyhemoglobin. Con-versely, CO2 binds more tightly to deoxyhemoglobin thanto oxyhemoglobin. All of these processes occurring inthe red blood cells of peripheral capillaries are function-ally reversed in the lungs (Figure 1-6). Since alveolar PO2
is higher than that of the incoming deoxygenated blood,oxygenation of hemoglobin and release of H+ occur. TheH+ release takes place because HbO2 is a stronger acid(i.e., has a lower pK′) than deoxyhemoglobin. The releasedbicarbonate, which is transported to the red blood cellswith the corresponding efflux of Cl−, combines with thereleased H+ to form H2CO3. Cellular carbonic anhydrasecatalyzes dehydration of H2CO3 and release of CO2 fromthe red blood cells.
Thus, red blood cell carbonic anhydrase which catalyzesthe reversible hydration of CO2, plays a vital role in carbondioxide transport and elimination. Carbonic anhydrase isa monomeric (M.W. 29,000) zinc metalloenzyme and is

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
SECTION 1.2 Buffers 9
present in several different isoenzyme forms. The mostprevalent red blood cell isoenzyme of carbonic anhydraseis type I (CAI). Zinc ion, held by coordinate covalent link-age by three imidazole groups of three histidine residues,is involved in the catalytic mechanism of carbonic anhy-drase. Water bound to zinc ion reacts with CO2 bound tothe nearby catalytic site of carbonic anhydrase to produceH2CO3. The action of carbonic anhydrase is essential fora number of metabolic functions. Some include the for-mation of H+ ion in stomach parietal cells (Chapter 12),in bone resorption by the osteoclasts (Chapter 37) andreclamation of HCO−
3 in renal tubule cells (Chapter 39).In osteoclasts and in the renal tubule cells, the isoenzymeCAII catalyzes the hydration reaction of CO2. A deficiencyof CAII caused by an autosomal recessive disorder con-sists of osteoporosis (marble bone disease), renal tubularacidosis, and cerebral calcification.
The diffusion of CO2 from venous blood into the alveoliis facilitated by a pressure gradient of CO2 between the ve-nous blood (45 mm Hg) and the alveoli (40 mm Hg) and bythe high permeability of the pulmonary membrane to CO2.Blood leaving the lungs has a PCO2 of about 40 mm Hg;thus, essentially complete equilibration occurs betweenalveolar CO2 and blood CO2.
Blood Buffer Calculations
Carbonic acid has the following pK′ values:
H2CO3 � H+ + HCO−3 pK′
1 = 3.8 (1.9)
HCO−3 � CO2−
3 + H+ pK′2 = 10.2 (1.10)
It is apparent from the pK′ values that neither equilib-rium can serve as a buffer system at the physiological pHof 7.4. However, carbonic acid (the proton donor) is inequilibrium with dissolved CO2, which in turn is in equi-librium with gaseous CO2:
H2O + CO2(aqueous) � H2CO3 (1.11)
The hydration reaction (1.11), coupled with the firstdissociation of carbonic acid (1.9), produces an apparentpK′ of 6.1 for bicarbonate formation. Thus, the summationof Equations (1.9) and (1.11) yields
H2O + CO2 � H+ + HCO−3 (1.12)
pK′ (apparent) =[HCO−
3
][H+]
[H2CO3]= 6.1 (1.13)
The ratio of HCO−3 to H2CO3 at a physiological pH of 7.4
can be calculated by using the Henderson–Hasselbalchrelationship:
7.4 = 6.1 + log
[HCO−
3
][H2CO3]
(1.14)
log
[HCO−
3
][H2CO3]
= 1.3
Taking antilogarithms,[HCO−
3
][H2CO3]
= 20
1= proton acceptor
proton donor
This ratio is large because the pH is greater than the pK′
(see Table 1-3). At pH 7.4, the bicarbonate system is a goodbuffer toward acid (i.e., it can neutralize large amounts ofacid) but a poor buffer for alkali. However, blood H2CO3
is in rapid equilibrium with a relatively large (about 1000times as much) reservoir of cellular CO2 and can functionas an effective buffer against increases in alkalinity. TheHCO−
3 /H2CO3 ratio in blood is coupled to the partial pres-sure of CO2, i.e., to the metabolic production of CO2 andto the loss of CO2 during respiration. In the equilibriumexpression for the bicarbonate-carbonic acid buffer sys-tem at pH 7.4, the carbonic acid term can be replaced by apressure term because the carbonic acid concentration isproportional to PCO2 in the blood.
pH = 6.1 + log
[HCO−
3
]a PCO2
(1.15)
where a, a proportionality constant, is defined by the equa-tion
[H2CO3] = a PCO2 (1.16)
The numerical value of a depends on the solventand the temperature. For normal plasma at 37◦C, a =0.0301 mmol of dissolved CO2 per liter of plasma permm Hg of CO2 pressure. Assuming that 37◦C (310 K)is approximately the same as standard temperature, 25◦C(298 K), and that [H2CO3] in Equation (1.16) includesboth carbonic acid and dissolved CO2, the value of a canbe derived from two facts:
1. At 37◦C and 760 mm Hg of CO2 pressure, 521 mL ofCO2 will dissolve per liter of normal plasma;
2. At standard temperature and pressure, 1 mol of dryCO2 occupies a volume of 22.26 L (not 22.4 L sinceCO2 is not an ideal gas).
a = 521 mL CO2/L of plasma
760 mm Hg × 22.26 mL/mmol of CO2
= 0.0301mmol CO2/L of plasma
mm Hg of CO2 pressure
The equation form of the Henderson–Hasselbalch ex-pression [Equation (1.15)] can be further modified bysubstituting another expression for the bicarbonate term.When excess strong acid is added to plasma, CO2 is sto-ichiometrically released from dissolved CO2, carbonic

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
10 CHAPTER 1 Water, Acids, Bases, and Buffers
acid, bicarbonate ions, and carbonate. Carbonate concen-tration is negligible; thus,
Total [CO2] = [HCO−
3
] + dissolved[CO2] + [H2CO3]
But
Dissolved[CO2] + [H2CO3] = 0.0301PCO2
so that [HCO−
3
] = total[CO2] − 0.0301PCO2
Finally,
pH = 6.1 + log
(total [CO2] − 0.0301PCO2
[0.0301PCO2 ]
)
(1.17)
Equation (1.17) is useful for calculating the pH from thetotal [CO2] and PCO2 .
The HCO−3 /H2CO3 buffer system effectively maintains
a constant blood pH of 7.4 if bicarbonate and H2CO3 con-centrations are maintained at a ratio of 20:1. The concen-tration of HCO−
3 is regulated by its selective excretion andreclamation by the membranes of the renal tubular epithe-lial cell. PCO2 and [H2CO3] in the blood can be alteredby changes in the rate and depth of respiration. For ex-amples, hypoventilation (slow, shallow breathing) leadsto increased blood PCO2 , whereas hyperventilation (rapid,deep breathing) has the opposite effect. PCO2 changes me-diated by the lungs are more rapid than [HCO−
3 ] changesaffected through the kidneys (Chapter 39).
Nonbicarbonate Buffers in Blood
Other important nonbicarbonate blood buffers are proteinand phosphate. The predominant buffer system in the redblood cells is hemoglobin. Protein amino acid side chains(R-groups) that act as buffers are carboxylate groups ofglutamate and aspartate and the weakly basic groups oflysine, arginine, and histidine. To be effective, the pK′
value of a buffer should be close to the pH of the system tobe buffered. Except for the R-group of histidine, which isan imidazolium group (Figure 1-7), the pK′ values of theother amino acids mentioned above are not close enough tothe physiological pH of blood to be effective buffers. Theimidazolium group has a pK′ value of 6.5 but it can varyfrom 5.3 to 8.3 depending on differences in electrostaticenvironment either within the same protein molecule orin different proteins. Another potential buffering group inprotein is the α-amino group of the amino acid residues atthe amino terminus of the protein. This group has a pK′
value ranging from 7.8 to 10.6, with a typical value ofabout 8 (acid–base properties of amino acids and proteinsare discussed in detail in Chapters 2 and 3). In plasma,
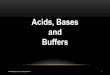
FIGURE 1-8Titration profile of phosphoric acid (H3PO4) with sodium hydroxide(NaOH). The three pK′ values correspond to three buffer regions. Thephysiological buffering occurs at the pK′ region with H2PO−
4 (acid) andHPO2−
4 (conjugate base) ionic species.
the protein buffer system has a limited role; the principalplasma buffer is the bicarbonate-carbonic acid system.
Compared with hemoglobin in the red blood cells andHCO−
3 /H2CO3 in plasma, phosphates (both organic and in-organic) play minor roles in physiological buffering. Phos-phoric acid (H3PO4) has three dissociable protons:
H3PO4 � H2PO−4 + H+ pK′
1 = 1.9 (1.18)
H2PO−4 � HPO2−
4 + H+ pK′2 = 6.8 (1.19)
HPO2−4 � PO3−
4 + H+ pK′3 = 12.4 (1.20)
The titration profile of phosphoric acid with NaOH isshown in Figure 1-8. The principal dissociation expres-sion functioning at a given pH depends on which pK′
is closest to the pH. At a plasma pH of 7.4, the impor-tant conjugate pair is HPO2−
4 /H2PO−4 . The Henderson–
Hasselbalch equation can be used to obtain the value ofthe ratio HPO2−
4 /H2PO−4 at pH 7.4:
7.4 = 6.8 + log
[HPO2−
4
][H2PO−
4
] (1.21)
log
[HPO2−
4
][H2PO−
4
] = 0.6 and
[HPO2−
4
][H2PO−
4
] = 4
As was the case for the bicarbonate-carbonic acid sys-tem, the conjugate base form (HPO2−
4 ) of the phosphatebuffer is present in large (fourfold) excess compared tothe acid form (H2PO−
4 ) and provides acid buffering capac-ity. Since the body metabolism produces more acid than

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
SECTION 1.3 Measurement of pH 11
base, this ratio assists in neutralizing acid and in maintain-ing a constant pH. The HPO2−
4 /H2PO−4 buffering system
plays a minor role in plasma because of the low concen-trations of these ions, but it is important in raising theplasma pH through the excretion of H2PO−
4 via the kidney(Chapter 39). In summary, hemoglobin absorbs a majorportion of the hydrogen ions produced by the dissocia-tion of H2CO3 generated by the hydration of CO2—themost important buffer system in the blood. However, sincehemoglobin and carbonic anhydrase are present only in redblood cells, the HCO−
3 /H2CO3 system in the plasma is anindispensable intermediary in transporting the acid. Thus,the principal method of CO2 transport is in the form ofHCO−
3 in blood plasma.
1.3 Measurement of pH
Blood and urine pH can be measured easily by meansof a calibrated glass electrode, whereas pH measurementinside the metabolizing cells is not easily accomplished.Techniques for estimating intracellular pH include glasselectrode measurements on homogenates, calorimetric orfluorometric analysis of intracellular distribution of indi-cator dyes, and microelectrode methods.
Nuclear Magnetic Resonance andMagnetic Resonance Imaging
The noninvasive technique of nuclear magnetic resonance(NMR) spectrometry has been used to measure the con-centration of H+ and other selected ions in isolated cellsand tissues. NMR analysis is based on the principle thatsome atomic nuclei behave like tiny bar magnets becausethe spinning of charged nuclei generates a magnetic mo-ment along the axis of the spin. If a nucleus with a magneticdipole (spin) is placed in an external magnetic field, it willacquire an orientation aligned either with the applied field(low-energy state) or against the applied field (high-energystate). The former state is analogous to the way in whicha compass needle aligns itself with the earth’s magneticfield. Thus, the nuclei, in the presence of an external mag-netic field, can remain in either of two unequal energystates. If the aligned nuclei are excited with electromag-netic energy of the proper frequency, some of the nucleiin the low-energy state (ground state) will be excited tothe high-energy state. Subsequent release of energy byexcited nuclei leads to relaxation back to the ground stateand completes the resonance cycle between the two energystates.
The NMR spectrum is essentially a measure of theemission of electromagnetic radiation associated with the
FIGURE 1-9Pathway of creatine biosynthesis. In GMT deficiency, precursorguanidinoacetate accumulates and the synthesis of creatine andphosphocreatine is severely reduced. Creatinine, a nonmetabolizable endproduct that is excreted by the renal system, is also diminished.
return of the nuclei from the high-energy state to thelow-energy state. Each atomic nucleus has a character-istic spectrum of resonance absorption frequencies thatare influenced by the chemical environment surroundingthat nucleus and that appear as shifts in the resonance fre-quency (known as chemical shifts). Thus, the chemicalshifts (expressed numerically in parts per million [ppm]relative to a standard NMR signal or frequency) can beused to distinguish different chemical compounds contain-ing the same nuclei. NMR spectral features are correlatedwith spectra of known structures to provide structural in-formation that may permit identification of the molecule

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
12 CHAPTER 1 Water, Acids, Bases, and Buffers
FIGURE 1-10The 1H-NMR pattern (in vitro, 600 MHz) of cerebrospinal fluid (CSF) of a patient with creatine deficiency syndrome(A) compared with normal CSF (B). Note the near absence of creatine and creatinine in the patient’s CSF. Theethosuximide observed in the patient’s CSF is a drug used in antiepileptic therapy. [Reproduced with permission fromA. Schulze et. al., Creatine deficiency syndrome caused by guanidinoacetate methyltransferase deficiency: diagnostictools for a new inborn error of metabolism. J. Pediatr., 131, 626 (1997).]
under investigation. Determining the area under the NMRspectrum for a given compound provides a measure of thenumber of nuclei that are polarized by the magnetic field,and the relative abundance of different nuclei in tissuescan be measured.
Atomic nuclei suitable for biological studies include1H, 13C, 15N, 19F, 23Na, 31P, and 39K. Determination ofintracellular pH utilizes 31P-NMR because the resonancefrequency of inorganic phosphate (Pi) varies predictablywith changes in pH. The exact location of the Pi sig-nal depends on the relative concentrations of H2PO−
4 andHPO2−
4 , which in turn depend on the intracellular pH andpK′ of inorganic phosphate under physiological condi-tions. Thus, the position of the Pi signal in the NMRspectrum provides a measure of intracellular pH. Apartfrom measurements of H+ concentrations in several tis-sues under varying physiological conditions, NMR anal-ysis of muscle tissues in a patient’s forearm has beenused to diagnose a hereditary defect in the breakdown ofmuscle glycogen (McArdle’s syndrome). In normal indi-viduals during exercise, glycogen in the muscle breaksdown to lactic acid, thus decreasing the pH. However,in patients with McArdle’s syndrome, the pH does not
change with exercise because glycogen is not catabo-lized to lactic acid (Chapter 15). 1H- and 31P-NMR spec-troscopy has been used to measure metabolically signifi-cant components in tissues and fluids, including brain andcerebrospinal fluid. In a 4-year-old female patient with adefect in creatine formation due to a deficiency of guani-dinoacetate methyltransferase, phosphocreatine synthesisis severely diminished in many tissues including the brain(Figure 1-9). Determination of creatine and creatinine incerebrospinal fluid by NMR can be used to diagnose cre-atine deficiency syndrome (Figure 1-10). Creatinine is anend product of creatine and phosphocreatine (Chapter 17).The phosphocreatine pool is essential for the storage andtransfer of energy via high-energy phosphate compounds(ATP). In this patient who exhibited dystonic-dyskineticsyndrome, seizures, and psychomotor retardation, NMRspectroscopy revealed a depletion of creatine, phosphocre-atine, and accumulation of guanidinoacetate (Figure 1-10).Oral administration of creatine resulted in clinicalimprovement.
High-quality anatomical cross-sectional images can beproduced by the use of tomographic methods with NMRinstead of x-rays as a probe. Magnetic resonance images

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
SECTION 1.3 Measurement of pH 13
are generated by measuring the relaxation time of returnto equilibrium for hydrogen nuclei in a constant magneticfield following excitation by a radiofrequency pulse. Thetime taken by the hydrogen nuclei to return to their originalposition when the radiofrequency pulse is terminated isknown as the T1-relaxation time. The time taken for thehydrogen nuclei to lose the energy that they acquire duringthe radiofrequency pulse sequence is known as the T2relaxation time. T2 is always less than T1 and the qualityof the MRI depends upon the concentration of hydrogennuclei (known as proton density or spin density) and theweight given to the T1 and T2 components. In T1-weightedimages, lipids have a characteristic short T1 relaxationtime and are hyperintense (bright), whereas water has along T1 relaxation time and is hypointense (dark). Thus,tissues rich in fat appear bright and tissues rich in freewater appear dark. In T2 weighted images the opposite istrue; lipids appear dark and water bright.
The resolution of anatomical structures is achieved byvirtue of different relaxation times of hydrogen nucleiin different tissues. Differences in relaxation time re-flect gross chemical characteristics, including fat content,degree of hydration, and presence of paramagnetic sub-stances. Proton density is also an important parameter indetermining the intensity of an image, so that soft tissuesas well as bone can readily be visualized, making the tech-nique superior to x-ray and other methods of imaging thebrain and other soft tissues.
Use of the intravascular contrast agent gadolinium-diethylamine pentaacetic acid (GdDPTA) during the MRIprocedure enhances the T1 relaxation time of hydrogennuclei. This alters the magnetic susceptibility of adjacenttissue and provides information on the integrity of theblood-brain barrier. MRI is the diagnostic procedure ofchoice in several neurologic diseases. In one autoimmuneinflammatory demyelinating disorder of the central ner-vous system, multiple sclerosis (MS), MRI is the preferredimaging procedure both in diagnosis and as a prognos-tic tool (Figure 1-11). MS is a progressive degenerativedisease and exhibits scattered focal lesions of the myelinsheath of the axons. MS usually manifests during the thirdor fourth decade of life and affects more women (60%)than men (40%). No known risks are associated with MRI,which is another advantage of the procedure.
Gibbs–Donnan Equilibrium
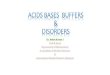
The bicarbonate-carbonic acid buffer system plays a majorrole in regulating the pH of fluids in tissue spaces outsideblood vessels. This fluid, commonly referred to as inter-stitial fluid and separated from plasma by the membranebarrier known as the capillary endothelium, primarily
FIGURE 1-11Magnetic resonance image (T1 weighted) of brain from a patient withmultiple sclerosis. The image obtained is a horizontal section at the level ofthe head of the caudate nucleus showing characteristic marked increase ofsignal as indicated by arrows. (Courtesy of Robert M. DiMauro and JohnH. Hardman.)
contains the diffusible ions, Na+, K+, Cl−, and HCO−3 .
Plasma contains proteins in addition to diffusible ions.Membranes (Chapter 10) have a lipid-protein fluid mosaicstructure and the membrane proteins may occupy surfacepositions or extend through the lipid bilayer (Figure 1-12).
Plasma proteins are polyionic at pH 7.4 and cannot dif-fuse across membranes. The normal difference in concen-trations of diffusible ions between the plasma and intersti-tial compartments is due to the presence of nondiffusibleprotein in plasma, shown in Table 1-5.
The difference is explained by Gibbs’ theory of equilib-ria and was studied experimentally by Donnan; the overallprocess is known as the Gibbs–Donnan equilibrium.
Gibbs–Donnan equilibria can best be understood in atwo-compartment system. Compartment 1 contains thesodium salt of an anionic protein (Na+
n Pn−) at an ini-tial concentration C1, with n representing the numberof charges; compartment 2 contains NaCl at an initial

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
14 CHAPTER 1 Water, Acids, Bases, and Buffers
TABLE 1-5Concentration of Cations and Anions in Plasma Water and Interstitial Fluid*
Plasma Water† Interstitial Fluid‡
Ion mEq/L mmol/L mEq/L mmol/L
CationsNa+ 153.2 153.2 145.1 145.1K+ 4.3 4.3 4.1 4.1Ca2+ 3.8 1.9§ 3.4 1.7Mg2+ 1.4 0.7k 1.3 0.65
Total 162.7 160.1 153.9 151.6Anions
Cl– 111.5 111.5 118 118HCO3
– 25.7 25.7 27 27H2PO4
––HPO42– 2.2 0.66 2.3 0.7
Other 6.3 5.9 6.6 6.2Protein 17.0 1.5 0 0
Total 162.7 145.3 153.9 151.9
Total mOsm per liter 305.4 303.5
*Reproduced, with permission, from D. M. Woodbury in Physiology and Biophysics. T. Ruch, H. Patton, and A. Scher, Eds. (Saunders, 1974).†Plasma water content assumed to be 93%.‡Gibbs-Donnan factors used as multipliers are 0.95 for monovalent cations, 0.9 for divalent cations, 1.05 for monovalent anions, and 1.10 for divalent anions.§Total Ca is 2.7 mmol/L; ionized Ca is about 70% of total Ca.kTotal Mg is 1 mmol/L; ionized Mg is about 65% of total Mg.
FIGURE 1-12Fluid mosaic model of a membrane consists of lipids and proteins. Globular proteins are interspersed within the lipidmatrix: Protein A traverses the entire bilayer; protein B is embedded in one leaflet; proteins C and D are on the periphery.

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
SECTION 1.4 H+ Concentration and pH 15
FIGURE 1-13Gibbs–Donnan equilibrium exists in systems consisting of two fluidcompartments separated by a semipermeable membrane, which permitsdiffusion of some ions (e.g., Na+, Cl−) but is impermeable to proteinanions. Note that the concentration of diffusible cation in compartment 1 isgreater than in compartment 2 and that osmotic differences exist betweencompartments 1 and 2.
concentration of C2 (Figure 1-13). For simplicity, assumen = 1. The initial concentration of Cl− is higher in com-partment 2 than in compartment 1 so that Cl− will diffuseinto compartment 2. Na+ also migrates into compartment2 to maintain electrical neutrality. This net migration oc-curs until an equilibrium is reached, i.e., when the rate ofion diffusion from 2 into 1 equals that from 1 into 2. Ifx represents the net concentration of Na+ or Cl− trans-ferred to compartment 1, the final equilibrium concentra-tions differ from the initial values by ±x (Figure 1-13).The rate of diffusion of NaCl from 2 into 1 is proportionalto the product of the concentrations of Na+ and Cl− in2, which is (C2 − x)2. Similarly, the rate of diffusion ofNaCl from 1 into 2 is proportional to the product of theconcentrations of Na+ and Cl− in 1, which is (C1 + x)x .At equilibrium, the diffusion rates from 2 into 1 and 1 into2 are equal:
(C1 + x)x = (C2 − x)2
From which,
x = C22
C1 + 2C2
This unequal equilibrium distribution of solutes dependsupon the concentration of both the nondiffusible proteinanion C1 and the value of C2. This disparity in ion con-centrations also causes differences in osmotic pressure.
In the above example, if H+ replaced Na+ as the dif-fusible cation, the Gibbs–Donnan effect would lead toa pH change; compartment 1 would have a decrease inpH, while compartment 2 would have an increase in pH.Consistent with this, relatively protein-rich plasma has ahigher [H+] (i.e., lower pH) than that of protein-poor in-terstitial fluid. Although Gibbs–Donnan equilibria affectionic concentrations between many compartments (e.g.,blood/interstitial fluid or plasma/red blood cells), majorionic gradients between various compartments are main-tained at the expense of energy-requiring transport sys-tems (e.g., ATP-dependent Na+ and K+ transport at cellmembranes).
1.4 H+ Concentration and pH
The use of pH to designate [H+] is due to the fact that abroad range of [H+] can be compressed within the manage-able numerical scale of 0–14. However, in clinical acid–base problems, use of the pH scale has some disadvan-tages. Since the pH is the logarithm of the reciprocal of[H+], significant variations of [H+] in a patient may not befully appreciated. For example, if the blood pH decreasesfrom 7.4 to 7.1, [H+] is doubled; or if the pH increasesfrom 7.4 to 7.7, [H+] is halved (Figure 1-14). In addition,the use of the pH scale masks the relationship between[H+] and the concentrations of other cations, e.g., Na+ andK+. Thus, in clinical situations it is preferable to express
FIGURE 1-14The relationship of pH to hydrogen ion concentration (in nanomoles perliter). The normal blood pH of 7.40 corresponds to 40 nmol/L of H+. Thesolid straight line is drawn to show the linear relationship between theconcentration of H+ and pH, over the pH range of 7.20–7.50. A 0.01-unitchange in pH is equivalent to about 1.0 nmol/L change in the oppositedirection.

P1: GKW/SPH P2: GKW/UKS QC: GKW/UKS T1: GKW
PB065-01 APxxx-Bhagavan April 16, 2001 18:45 Char Count= 0
16 CHAPTER 1 Water, Acids, Bases, and Buffers
[H+] directly as nanomoles per liter in order to better eval-uate acid–base changes and interpret laboratory tests. Ablood pH of 7.40 corresponds to 40 nM [H+], which isthe mean of the normal range (Figure 1-14). The normalrange is 7.36–7.44 on the pH scale, or 44–36 nM [H+]. Ifthe pH of blood falls below pH 7.36 ([H+] > 44 nM), thecondition is called acidemia. Conversely, if the pH risesabove pH 7.44 ([H+] < 36 nM), the condition is calledalkalemia. The suffix -emia refers to blood and usually toan abnormal concentration in blood. Over the pH rangeof 7.20–7.50, for every change of 0.01 pH unit, there isa change of approximately 1 nM [H+] in the oppositedirection.
Since the Henderson–Hasselbalch expression uses pHterms, its utility in clinical situations is less than optimal.Kassirer and Bleich have derived a modified Henderson–Hasselbalch expression that relates [H+], instead of pH,to PCO2 and HCO−
3 , as follows:
H2CO3 � H+ + HCO−3
for which
K ′ =[HCO−
3
][H+]
[H2CO3]
Substituting a × PCO2 for [H2CO3], as in Equation (1.16),yields
K ′ =[HCO−
3
][H+]
a × PCO2
and
H+ = K ′a × PCO2[HCO−
3
] (1.22)
In Equation (1.22), K ′ and a are constants, and the numer-ical value of K ′a is 24 when PCO2 is expressed in mm Hg,[HCO−
3
]in mM, and [H+] in nM. Therefore,
H+ = 24 × PCO2[HCO−
3
] (1.23)
The above formulation expresses the interdependence ofthree factors; if two of them are known, the third canbe readily calculated. For example, at a blood [HCO−
3 ]of 24 nM and a PCO2 of 40 mmHg, [H+] is 40 mM.
Clinical applications of Equation (1.23) are discussed inChapter 39.
Supplemental Readings and References
Properties of Water
M.F. Colombo, D.C. Rau, and V.A. Parsegian: Protein solvation in allostericregulation: A water effect on hemoglobin. Science 256, 655 (1992).
M.A. Knepper: Molecular physiology of urinary concentrating mechanism:Regulation of aquaporin water channels by vasopressin. American Journalof Physiology 272 (Renal Physiology 41), F3 (1997).
M.A. Knepper, J.G. Verbalis, and S. Nielsen: Role of aquaporins in waterbalance disorders. Current Opinion in Nephrology and Hypertension 6,367 (1997).
M.D. Lee, L.S. King, and P. Agre: The aquaporin family of water channelproteins in clinical medicine. Medicine 76, 141 (1997).
R.P. Rand: Raising water to new heights. Science 256, 618 (1992).P.M. Wiggins: Role of water in some biological processes. Microbiological
Reviews 54, 432 (1990).
Acid–Base Chemistry and Respiratory Functionof Hemoglobin
H.J. Androgue and N.E. Madias: Management of life-threatening acid–basedisorders. New England Journal of Medicine; First of two parts 338, 26(1998); Second of two parts 338, 107 (1998).
C.C.W. Hsia: Respiratory function of hemoglobin. New England Journal ofMedicine 338, 239 (1998).
Nuclear Magnetic Resonance and MagneticResonance Imaging
R.R. Edeman and S. Warach: Medical progress: Magnetic resonance imag-ing. New England Journal of Medicine; First of two parts 328, 708 (1993);Second of two parts 328, 785 (1993).
S. Gilman: Medical progress: Imaging of the brain. New England Journalof Medicine; First of two parts 338, 812 (1998); Second of two parts 338,889 (1998).
S.J. Knoury and H.L. Weiner: Multiple sclerosis. Archives of InternalMedicine 158, 565 (1998).
L.A. Moulopoulos and M.A. Dimopoulos: Magnetic resonance imaging ofthe bone marrow in the hematologic malignancies. Blood 90, 2127 (1997).
A. Schulze, T. Hess, R. Wevers, et. al.: Creatine deficiency syndrome causedby guanidinoacetate methyltransferase deficiency: Diagnostic tools for anew inborn error of metabolism. Journal of Pediatrics 131, 626 (1997).
S. Stockler-Ipsiroglu: Creatine deficiency syndromes: A new perspective onmetabolic disorders and a diagnostic challenge. Journal of Pediatrics 131,510 (1997).