Embed Size (px)
Citation preview
1
Shu-Hua Wang, MD, MPH &TMAssistant Professor of Medicine
The Ohio State University
For anti-tuberculosis medications: Describe clinical monitoring for adverse drug reactions Case Reviews Nursing interventions and medical management
Review specific drug side effects Review adverse drug reactions
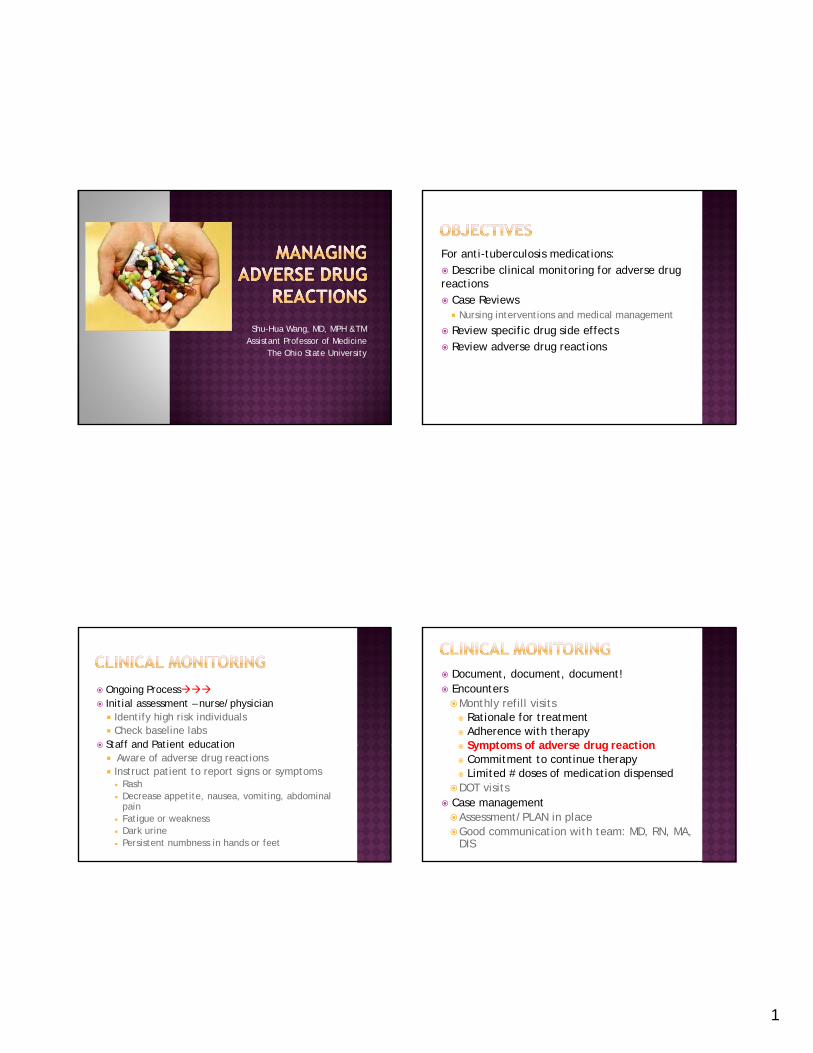
Ongoing Process Initial assessment – nurse/physician Identify high risk individuals Check baseline labs
Staff and Patient education Staff and Patient education Aware of adverse drug reactions Instruct patient to report signs or symptoms
Rash Decrease appetite, nausea, vomiting, abdominal
pain Fatigue or weakness Dark urine Persistent numbness in hands or feet
Document, document, document! EncountersMonthly refill visits Rationale for treatment Adherence with therapy Symptoms of adverse drug reaction Symptoms of adverse drug reaction Commitment to continue therapy Limited # doses of medication dispensed
DOT visits Case management Assessment/PLAN in placeGood communication with team: MD, RN, MA,
DIS
2
Mild reactions
No lasting effect
Usually do not require change in TB meds
Discoloration of body fluid
Gas, bloating, mild nausea
Itching, mild rash
Photosensitivity
Sleep disturbances
Headache
Serious
May be life threatening
Require change in
Significant nausea, vomiting, diarrhea
Hepatotoxiciy Toxic skin / systemic
reactionsmedication
May require hospitalization
Hearing loss Kidney failure Vision loss Hematologic reactions Electrolyte
abnormalities Neurologic damage Death
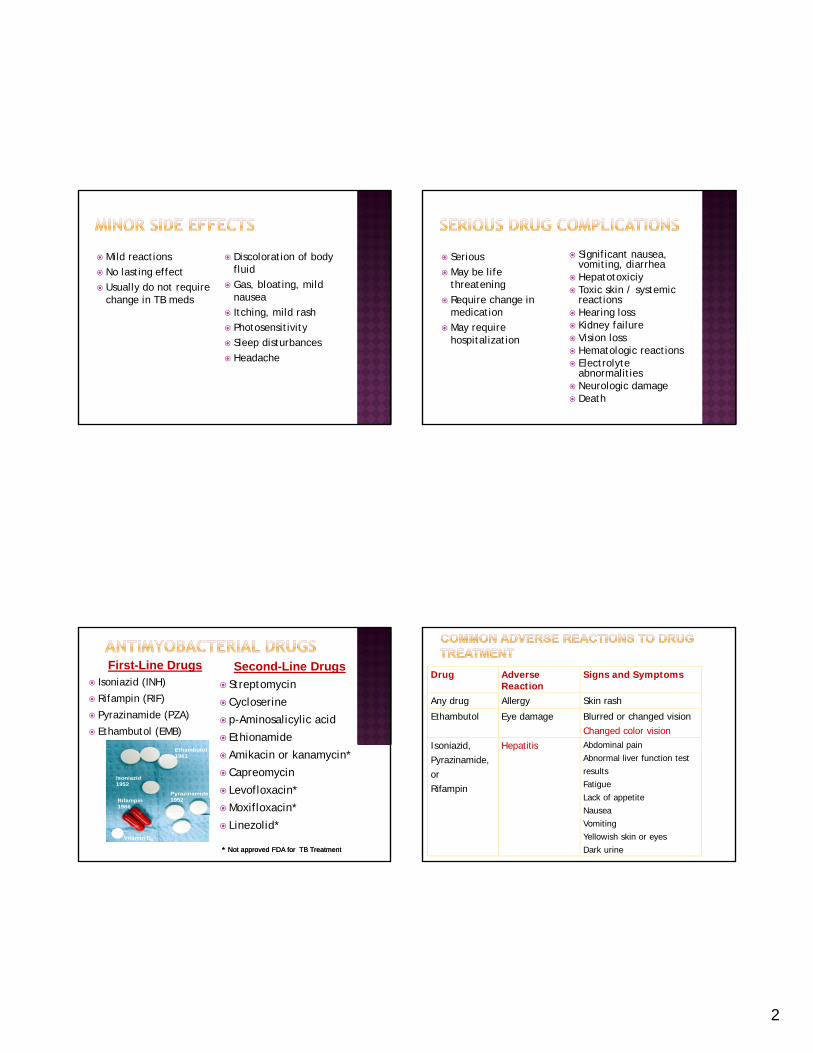
Isoniazid (INH)
Rifampin (RIF)
Pyrazinamide (PZA)
Ethambutol (EMB)
First-Line Drugs Second-Line Drugs
Streptomycin
Cycloserine
p-Aminosalicylic acid
Ethionamide
Amikacin or kanamycin*
Capreomycin
Levofloxacin*
Moxifloxacin*
Linezolid*
** Not approved FDA for TB TreatmentNot approved FDA for TB Treatment
Rifampin1966
Isoniazid1952
Ethambutol1961
Pyrazinamide1952
Vitamin B6
Drug Adverse Reaction
Signs and Symptoms
Any drug Allergy Skin rash
Ethambutol Eye damage Blurred or changed visionChanged color vision
Isoniazid Hepatitis Abdominal painIsoniazid,Pyrazinamide,orRifampin
Hepatitis Abdominal painAbnormal liver function test resultsFatigueLack of appetiteNauseaVomitingYellowish skin or eyesDark urine
3
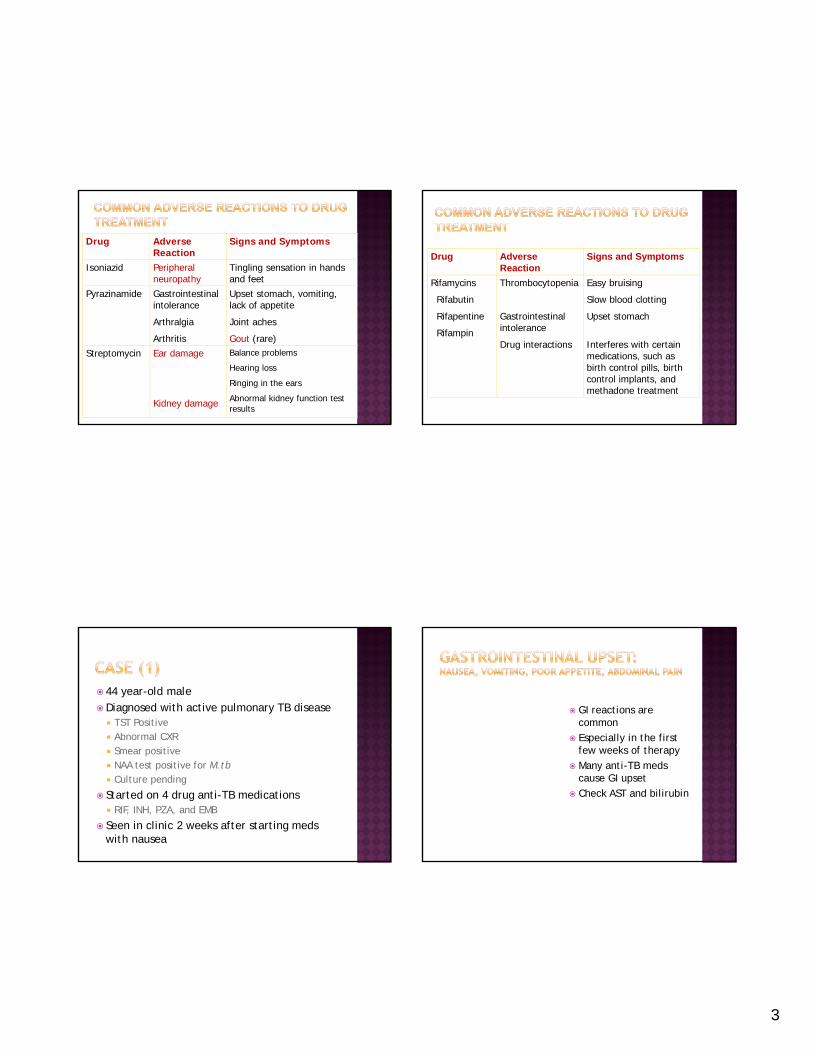
Drug Adverse Reaction
Signs and Symptoms
Isoniazid Peripheral neuropathy
Tingling sensation in hands and feet
Pyrazinamide Gastrointestinalintolerance
Upset stomach, vomiting, lack of appetiteintolerance
Arthralgia
Arthritis
lack of appetite
Joint aches
Gout (rare)Streptomycin Ear damage
Kidney damage
Balance problems
Hearing loss
Ringing in the ears
Abnormal kidney function test results
Drug Adverse Reaction
Signs and Symptoms
Rifamycins
Rifabutin
Thrombocytopenia Easy bruising
Slow blood clotting
Rifapentine
Rifampin
Gastrointestinal intolerance
Drug interactions
Upset stomach
Interferes with certain medications, such as birth control pills, birth control implants, and methadone treatment
44 year-old maleDiagnosed with active pulmonary TB disease TST Positive Abnormal CXR Smear positive NAA test positive for M.tb Culture pending
Started on 4 drug anti-TB medications RIF, INH, PZA, and EMB
Seen in clinic 2 weeks after starting meds with nausea
GI reactions are common
Especially in the first few weeks of therapy
Many anti-TB meds cause GI upset
Check AST and bilirubin
4
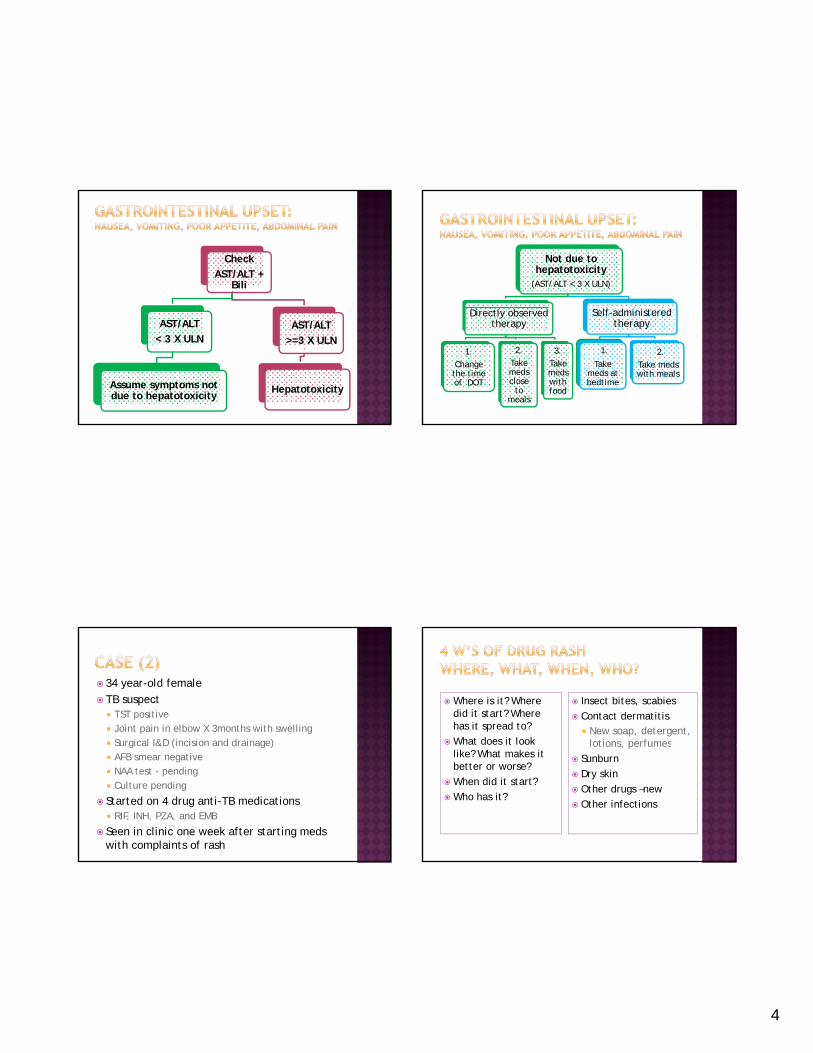
Check
AST/ALT + Bili
AST/ALT
< 3 X ULN
Assume symptoms not due to hepatotoxicity
AST/ALT
>=3 X ULN
Hepatotoxicity
Not due to hepatotoxicity
(AST/ALT < 3 X ULN)
Directly observed therapy
1.
Change the time of DOT
2.
Take meds close
to meals
3.
Take meds with food
Self-administeredtherapy
1.
Take meds at bedtime
2.
Take meds with meals
34 year-old female TB suspect TST positive Joint pain in elbow X 3months with swelling Surgical I&D (incision and drainage)Surgical I&D (incision and drainage) AFB smear negative NAA test - pending Culture pending
Started on 4 drug anti-TB medications RIF, INH, PZA, and EMB
Seen in clinic one week after starting meds with complaints of rash
Insect bites, scabies
Contact dermatitis New soap, detergent,
lotions perfumes
Where is it? Where did it start? Where has it spread to?
What does it look lotions, perfumes
Sunburn
Dry skin
Other drugs –new
Other infections
like? What makes it better or worse?
When did it start?
Who has it?
5
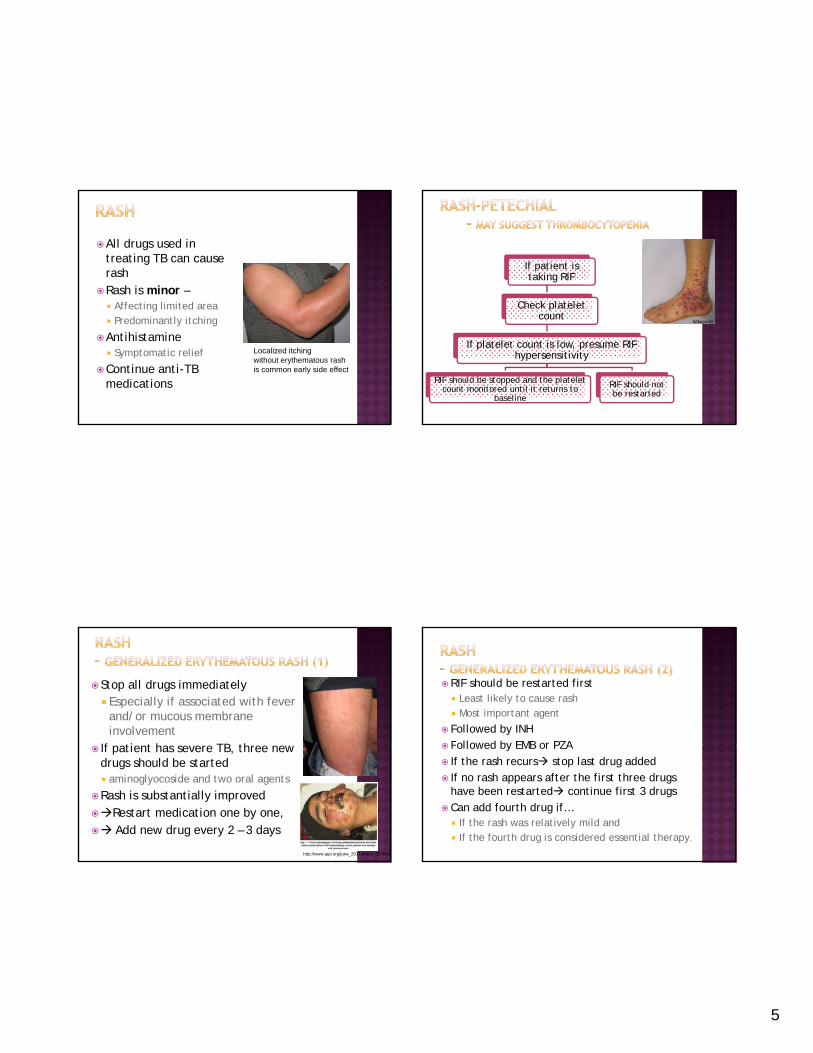
All drugs used in treating TB can cause rash
Rash is minor – Affecting limited area Affecting limited area Predominantly itching
Antihistamine Symptomatic relief
Continue anti-TB medications
Localized itching without erythematous rashis common early side effect
If patient is taking RIF
Check platelet Check platelet count
If platelet count is low, presume RIF hypersensitivity
RIF should be stopped and the platelet count monitored until it returns to
baseline
RIF should not be restarted
Wikepedia
Stop all drugs immediately Especially if associated with fever
and/or mucous membrane involvement
If ti t h TB th If patient has severe TB, three new drugs should be started aminoglyocoside and two oral agents
Rash is substantially improved Restart medication one by one, Add new drug every 2 – 3 days
http://www.japi.org/june_2011/article_15.html
RIF should be restarted first Least likely to cause rash Most important agent
Followed by INH Followed by EMB or PZA Followed by EMB or PZA If the rash recurs stop last drug added If no rash appears after the first three drugs
have been restarted continue first 3 drugsCan add fourth drug if… If the rash was relatively mild and If the fourth drug is considered essential therapy.
6
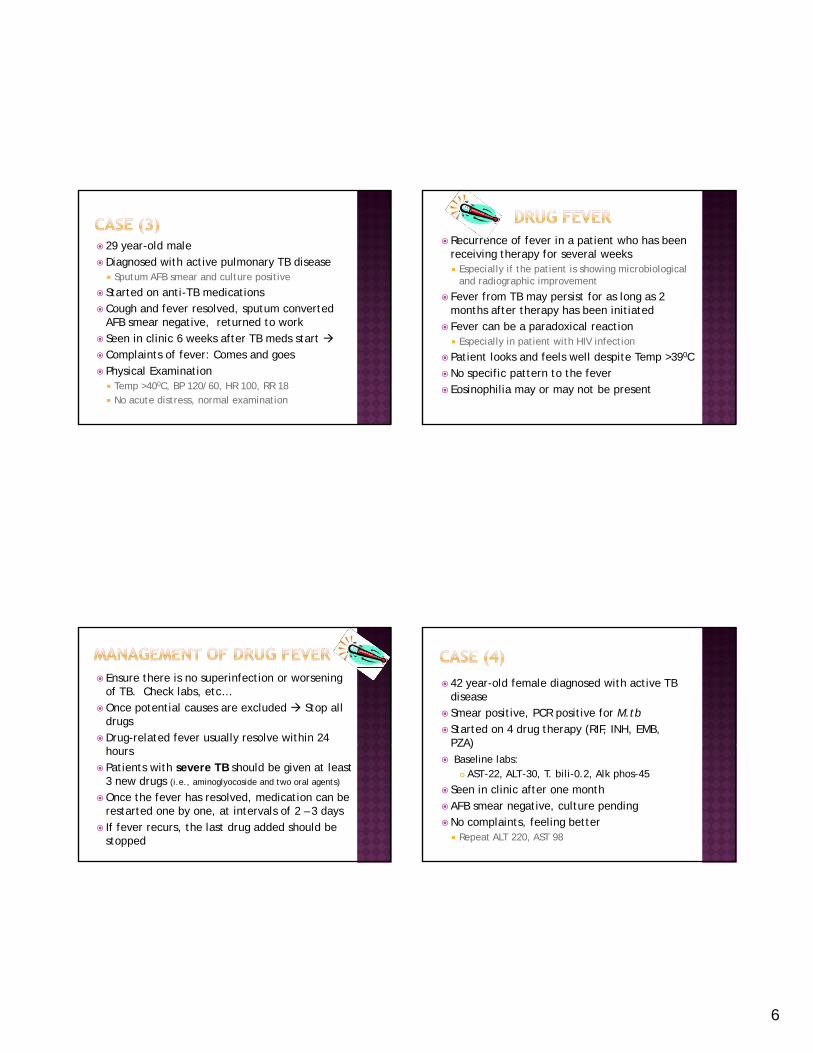
29 year-old maleDiagnosed with active pulmonary TB disease Sputum AFB smear and culture positive
Started on anti-TB medications Cough and fever resolved sputum converted Cough and fever resolved, sputum converted
AFB smear negative, returned to work Seen in clinic 6 weeks after TB meds start Complaints of fever: Comes and goes Physical Examination Temp >400C, BP 120/60, HR 100, RR 18 No acute distress, normal examination
Recurrence of fever in a patient who has been receiving therapy for several weeks Especially if the patient is showing microbiological
and radiographic improvement
Fever from TB may persist for as long as 2 th ft th h b i iti t dmonths after therapy has been initiated
Fever can be a paradoxical reaction Especially in patient with HIV infection
Patient looks and feels well despite Temp >390CNo specific pattern to the fever Eosinophilia may or may not be present
Ensure there is no superinfection or worsening of TB. Check labs, etc…
Once potential causes are excluded Stop all drugs
Drug-related fever usually resolve within 24 hours
Patients with severe TB should be given at least 3 new drugs (i.e., aminoglyocoside and two oral agents)
Once the fever has resolved, medication can be restarted one by one, at intervals of 2 – 3 days
If fever recurs, the last drug added should be stopped
42 year-old female diagnosed with active TB disease
Smear positive, PCR positive for M.tb Started on 4 drug therapy (RIF, INH, EMB,
PZA)PZA) Baseline labs:
AST-22, ALT-30, T. bili-0.2, Alk phos-45
Seen in clinic after one month AFB smear negative, culture pendingNo complaints, feeling better Repeat ALT 220, AST 98
7
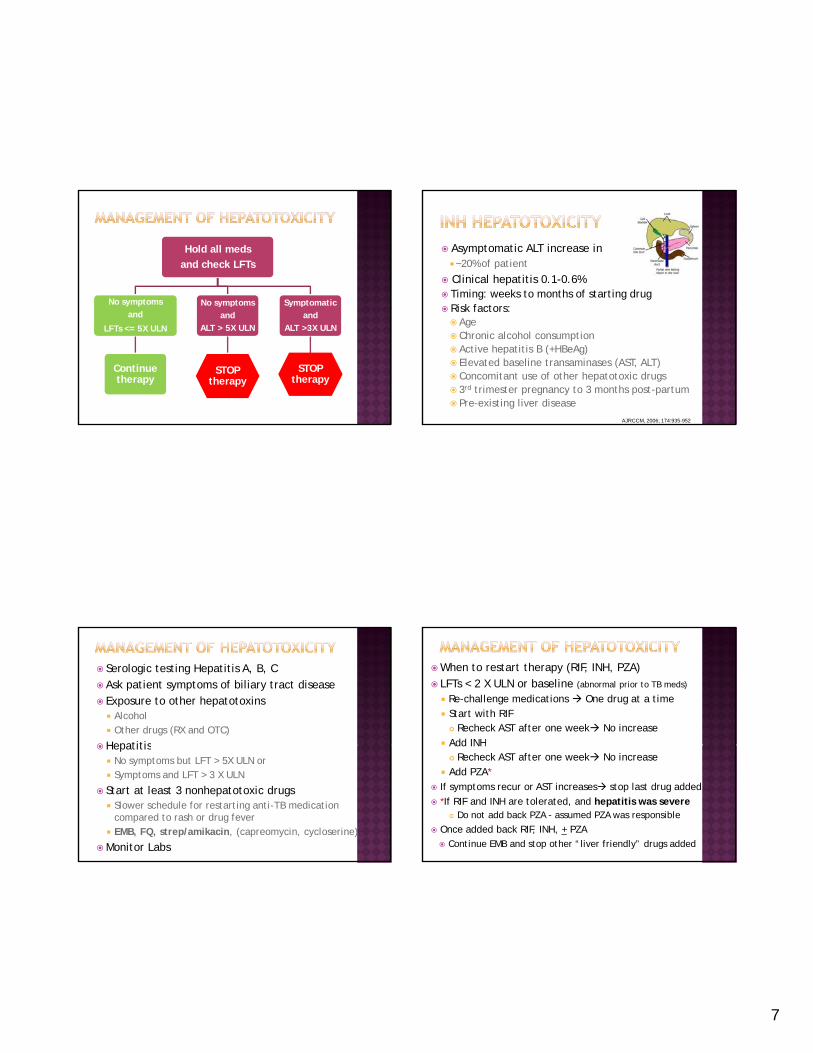
Hold all meds
and check LFTs
No symptoms No symptoms Symptomatic and
LFTs <= 5X ULN
Continue therapy
and
ALT > 5X ULN
STOP therapy
and
ALT >3X ULN
STOP therapy
Asymptomatic ALT increase in ~20% of patient
Clinical hepatitis 0.1-0.6% Timing: weeks to months of starting drug Risk factors: Risk factors: Age Chronic alcohol consumption Active hepatitis B (+HBeAg) Elevated baseline transaminases (AST, ALT) Concomitant use of other hepatotoxic drugs 3rd trimester pregnancy to 3 months post-partum Pre-existing liver disease
AJRCCM, 2006; 174:935-952
Serologic testing Hepatitis A, B, C Ask patient symptoms of biliary tract disease Exposure to other hepatotoxins Alcohol Other drugs (RX and OTC)
HepatitisHepatitis No symptoms but LFT > 5X ULN or Symptoms and LFT > 3 X ULN
Start at least 3 nonhepatotoxic drugs Slower schedule for restarting anti-TB medication
compared to rash or drug fever EMB, FQ, strep/amikacin, (capreomycin, cycloserine)
Monitor Labs
When to restart therapy (RIF, INH, PZA) LFTs < 2 X ULN or baseline (abnormal prior to TB meds)
Re-challenge medications One drug at a time Start with RIF Recheck AST after one week No increase
Add INHAdd INH Recheck AST after one week No increase
Add PZA* If symptoms recur or AST increases stop last drug added
*If RIF and INH are tolerated, and hepatitis was severe Do not add back PZA - assumed PZA was responsible
Once added back RIF, INH, + PZA Continue EMB and stop other “liver friendly” drugs added
8
Dose related, uncommon
Risk factors Other conditions with neuropathy: Malnutrition, diabetes, HIV, renal failure, alcohol,
pregnant femalep g
Mild peripheral neuritis - Stocking glove syndrome ~2%
Retrobulbar (optic) neurititis
CNS toxicity: Slurred speech, ataxia, seizure, memory
Pyridoxine INH
http://en.wikipedia.org/wiki/Isoniazidhttp://en.wikipedia.org/wiki/Pyridoxine
Orange discoloration of body fluid
Cutaneous reactions: Mild Generally self-limited Treat symptomatically - antihistamine
Gastrointestinal symptoms: Nausea, anorexia, abdominal pain
Hepatocellular injury less common Insidious cholestasis Anorexia, nausea, vomiting, fever, jaundice
RIF is much less likely to cause hepatoxicity than INH or PZA
http://connect.in.com/thrombocytopenia/photo-gallery-more.html
Flu-like syndrome with fever, chills, headache, & bone pain◦ Can begin 1-2 hrs after medication dose and resolve
spontaneously after 6-8 hrs◦ More common in intermittent dosing higher doseMore common in intermittent dosing, higher dose◦ Can try daily therapy if mild
Severe immunologic reactions – rare, each < 0.1% patients◦ Low platelet count / petechiae◦ Kidney dysfunction◦ Hemolytic anemia◦ Thrombotic thrombocytopenic purpura
9
Rifampin induces cytochrome P450 class of enzymes Involved in drug metabolism
Rifampin interacts with Narcotics (methadone) Narcotics (methadone) - Corticosteroids – Warfarin (coumadin) – Phenytoin (dilantin) – Contraceptives (estrogens) - HIV protease inhibitors & non-nucleoside reverse
transcriptase inhibitors – complex interactions
Hepatotoxicity: Both dose-dependent & idiosyncratic
Causes hepatotoxicity less often than INH but Can be more prolonged Can continue after drug discontinued Can be most severe
Can cause granulomatous hepatitis Fever, rash, lymphadenopathy, elevated ALT
Gastrointestinal symptoms: nausea, vomiting Arthralgias common – Rx symptomatically Elevated uric acid◦ PZA is a pro-drug active compound Pyrazinoic acid Blocks renal tubular excretion of uric acid Increase uric acid
◦ Allopurinol does not reverse this◦ Routine measurement of uric acid is not
recommended◦ Gout is rare◦ Hyperuricemia without gout is not a reason for
discontinuing drug
Retrobulbar neuritis: decrease visual acuity or red-green color discrimination
Increase risk with renal insufficiency Peripheral neuritisCutaneous reactions: <1% Joint pain

10
Baseline and monthly Visual acuity test
(Snellen chart)
Color discrimination test (Ishihara tests)
Patient education
Monthly symptom check blurred vision etc
Opthalmologyevaluaion
Hold medication – for any symptoms
Arthralgias, tendonitis, tendon rupture –very rare All ages Greater risk age >60
P i ki i id Patients taking corticosteroids Transplant patients
EKG abnormalities: QT prolongationNausea & diarrhea: 0.5-2% Rash/Pruritis/Photosensitivity: 0.2-0.4% Avoid in pregnancy
OtotoxicityVestibular toxicityNephrotoxicity Electrolyte disturbancesy Potassium, calcium, and magnesium depletion Cardiac dysrhythmias
Local pain at IM injection site Avoid in pregnancy
11
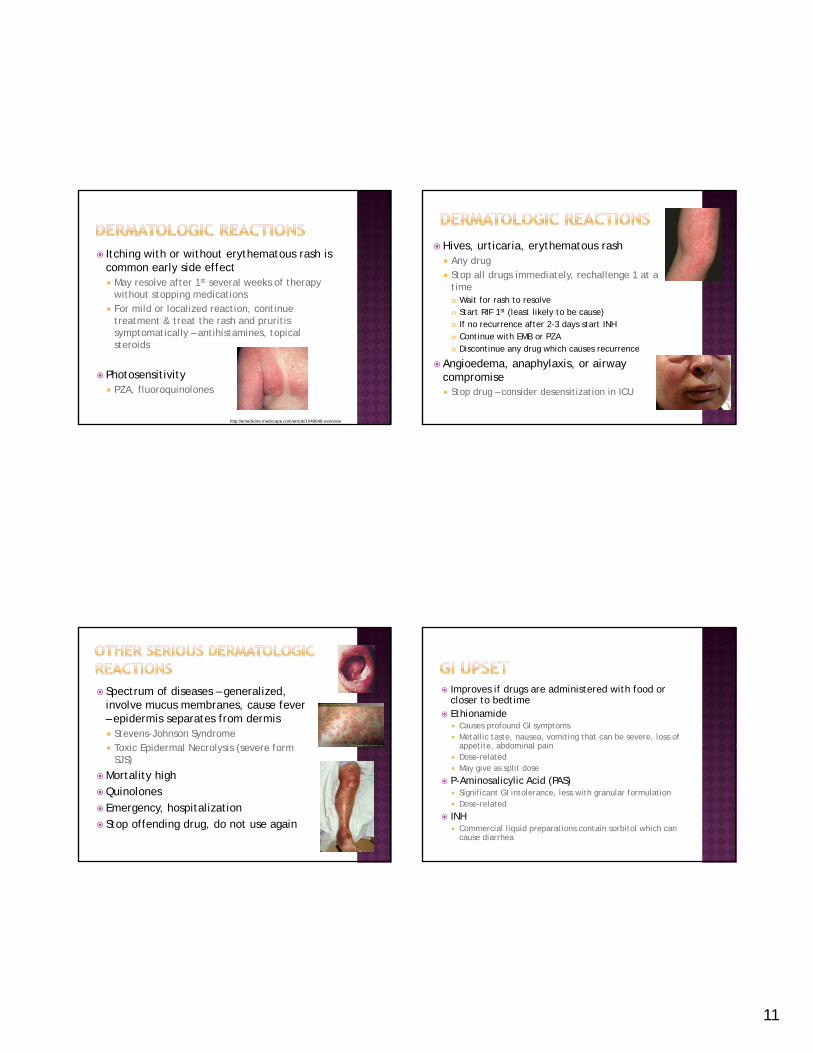
Itching with or without erythematous rash is common early side effect May resolve after 1st several weeks of therapy
without stopping medicationsFor mild or localized reaction continue For mild or localized reaction, continue treatment & treat the rash and pruritis symptomatically – antihistamines, topical steroids
Photosensitivity PZA, fluoroquinolones
http://emedicine.medscape.com/article/1049648-overview
Hives, urticaria, erythematous rash Any drug Stop all drugs immediately, rechallenge 1 at a
time Wait for rash to resolve Start RIF 1st (least likely to be cause) If no recurrence after 2-3 days start INH Continue with EMB or PZA Discontinue any drug which causes recurrence
Angioedema, anaphylaxis, or airway compromise Stop drug – consider desensitization in ICU
Spectrum of diseases – generalized, involve mucus membranes, cause fever – epidermis separates from dermis Stevens-Johnson Syndrome
T i E id l N l i ( f Toxic Epidermal Necrolysis (severe form SJS)
Mortality highQuinolones Emergency, hospitalization Stop offending drug, do not use again
Improves if drugs are administered with food or closer to bedtime
Ethionamide Causes profound GI symptoms Metallic taste, nausea, vomiting that can be severe, loss of
appetite abdominal painappetite, abdominal pain Dose-related May give as split dose
P-Aminosalicylic Acid (PAS) Significant GI intolerance, less with granular formulation Dose-related
INH Commercial liquid preparations contain sorbitol which can
cause diarrhea
12
Numbness, tingling hands & feet in stocking-glove pattern
Risk factors: diabetes, alcoholism, HIV, hypothyroidism, pregnancy, poor nutrition, inadequate dietary intake of pyridoxine
Pyridoxine supplements 10-50 mg daily (should this be routine?) for INH 100-200 for cycloserine &/or ethionamide
INH Dose-related Interferes with biologic function of vitamin B6
Ethionamide Increased incidence with prolonged use
Linezolid Increased incidence with prolonged use 600 mg daily instead of twice daily is used to
prevent this
Ethambutol, cycloserine Rare
INH Inability to concentrate, irritability, dysarthria,
seizures, dysphoria
Cycloserine (Dr K’s mnemonic – cyclo, psycho) Headache, restlessness, psychosis, seizures (dose-Headache, restlessness, psychosis, seizures (dose
related) Pyridoxine 100-200 mg daily to prevent / treat
Ethionamide Anxiety, depression, psychosis Increased incidence with prolonged treatment
Fluoroquinolones Dizziness, insomnia, tremulousness, headache
Ethambutol Retrobulbar neuritis Dose related – very rare (if at all) with currently
recommended doses Decreased red green color discrimination (1 or Decreased red-green color discrimination (1 or both eyes), decreased visual acuity
With renal disease
Ethionamide Optic neuritis Dose related
13
Streptomycin Vestibular (balance) and hearing disturbance Related to single dose size and cumulative dose
(>100-200 g)Increased with incidence if diuretics are used Increased with incidence if diuretics are used
Monitor with audiogram, Romberg Hearing loss can be permanent – consider
stopping
Amikacin & Kanamycin Less vestibular toxicity than SM
Capreomycin These drugs also cause nephrotoxicity & require monitoring
Injectable agents – 15mg/kg daily or 25 mg/kg TIW Ototoxicity often permanent *Hearing loss > 20 db occurred in 32/87 (37%)
patients, 88% had persistent loss at end of follow upfollow-up
Associated with older age, duration of treatment, & total dose, not to vestibular or renal toxicity
Amikacin>Kanamycin >Streptomycin TIW = daily Rx
*Peloquin, et al. Aminoglycoside toxicity…Clin Inf Dis 2004;38:1538-44
Acknowledgement: Special thanks to Dr. Dana Kissner , Wayne State University
44 year old female diagnosed with latent TB infection
8/3 seen by physician and nurse Started INH Baseline labs:
AST 19 ALT 19 T bili 0 3 Alk h 68 AST-19, ALT-19, T. bili-0.3, Alk phos-68
9/1 - Nurse Refill Visit #2 Repeat AST on 09/01 was 27
10/6 - Nurse Refill Visit #3 11/10 – Nurse Refill Visit #4 11/30 admitted for “jaundice”
14
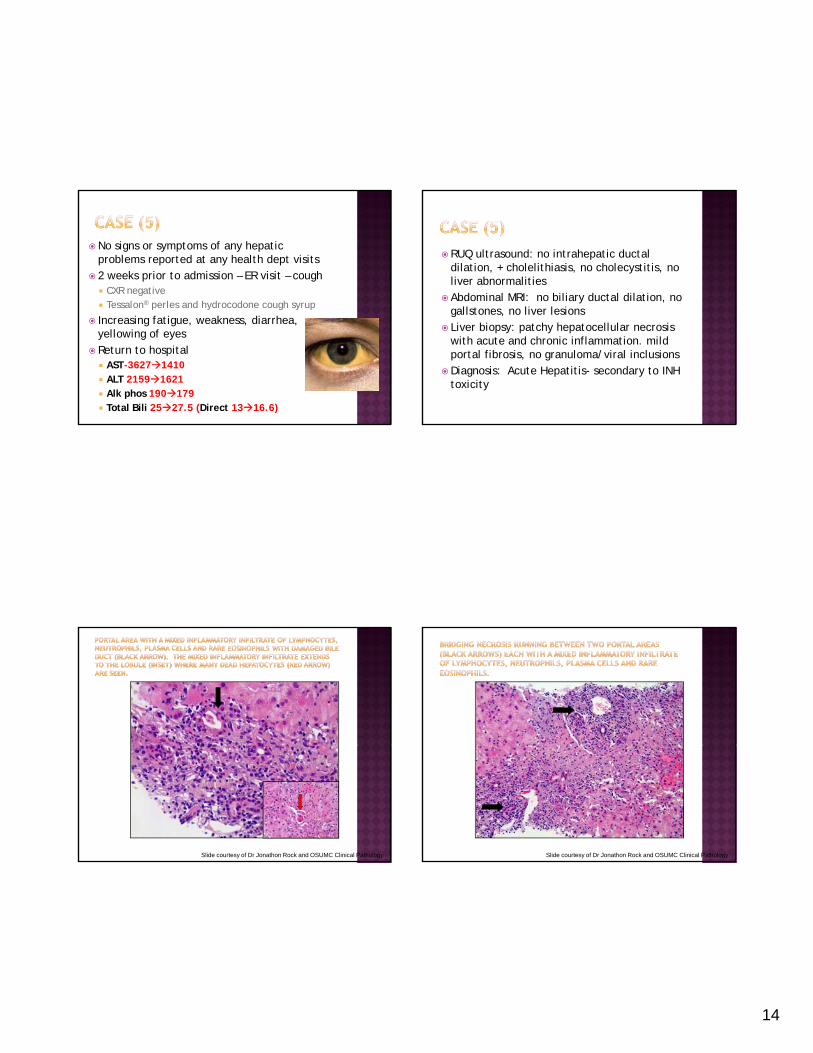
No signs or symptoms of any hepatic problems reported at any health dept visits
2 weeks prior to admission – ER visit – cough CXR negative Tessalon® perles and hydrocodone cough syrupTessalon perles and hydrocodone cough syrup
Increasing fatigue, weakness, diarrhea, yellowing of eyes
Return to hospital AST-36271410 ALT 21591621 Alk phos 190179 Total Bili 2527.5 (Direct 1316.6)
RUQ ultrasound: no intrahepatic ductal dilation, + cholelithiasis, no cholecystitis, no liver abnormalities
Abdominal MRI: no biliary ductal dilation, no ll t li l igallstones, no liver lesions
Liver biopsy: patchy hepatocellular necrosis with acute and chronic inflammation. mild portal fibrosis, no granuloma/viral inclusions
Diagnosis: Acute Hepatitis- secondary to INH toxicity
Slide courtesy of Dr Jonathon Rock and OSUMC Clinical Pathology Slide courtesy of Dr Jonathon Rock and OSUMC Clinical Pathology
15
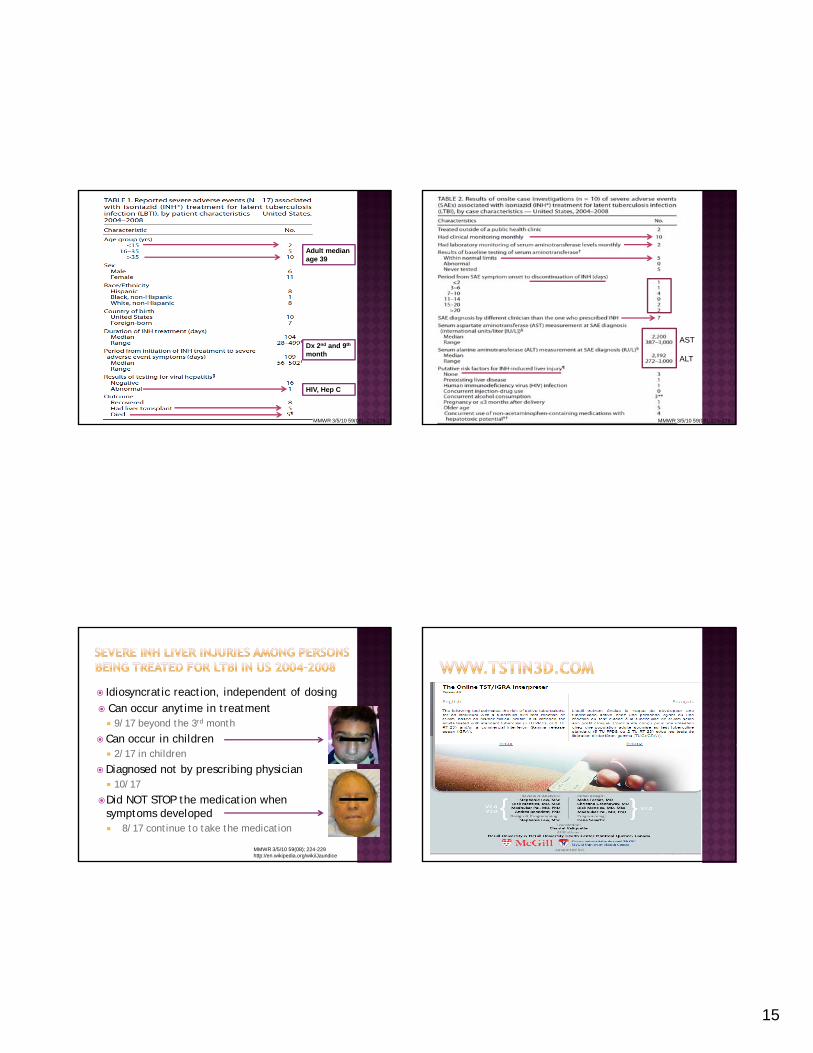
Adult median age 39
MMWR 3/5/10 59(08); 224-229
Dx 2nd and 9th
month
HIV, Hep C
AST
ALT
MMWR 3/5/10 59(08); 224-229
Idiosyncratic reaction, independent of dosing Can occur anytime in treatment 9/17 beyond the 3rd month
Can occur in children 2/17 in children
Diagnosed not by prescribing physician 10/17
Did NOT STOP the medication when symptoms developed 8/17 continue to take the medication
MMWR 3/5/10 59(08); 224-229http://en.wikipedia.org/wiki/Jaundice
16
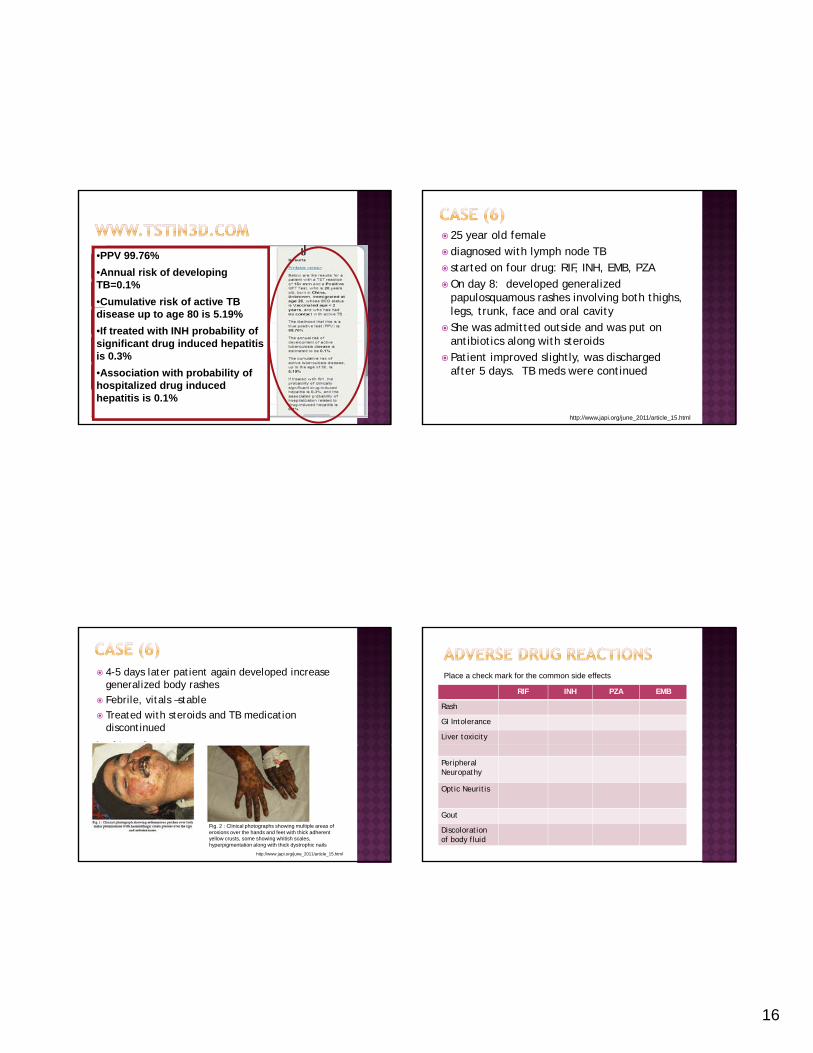
•PPV 99.76%
•Annual risk of developing TB=0.1%
•Cumulative risk of active TB disease up to age 80 is 5.19%
•If treated with INH probability of significant drug induced hepatitis is 0.3%
•Association with probability of hospitalized drug induced hepatitis is 0.1%
25 year old female diagnosed with lymph node TB started on four drug: RIF, INH, EMB, PZA On day 8: developed generalized
papulosquamous rashes involving both thighs, l t k f d l it legs, trunk, face and oral cavity
She was admitted outside and was put on antibiotics along with steroids
Patient improved slightly, was discharged after 5 days. TB meds were continued
http://www.japi.org/june_2011/article_15.html
4-5 days later patient again developed increase generalized body rashes
Febrile, vitals –stable
Treated with steroids and TB medication discontinued
Fig. 2 : Clinical photographs showing multiple areas of erosions over the hands and feet with thick adherent yellow crusts, some showing whitish scales, hyperpigmentation along with thick dystrophic nails
http://www.japi.org/june_2011/article_15.html
RIF INH PZA EMB
Rash
GI Intolerance
Liver toxicity
Place a check mark for the common side effects
Peripheral Neuropathy
Optic Neuritis
Gout
Discolorationof body fluid
17
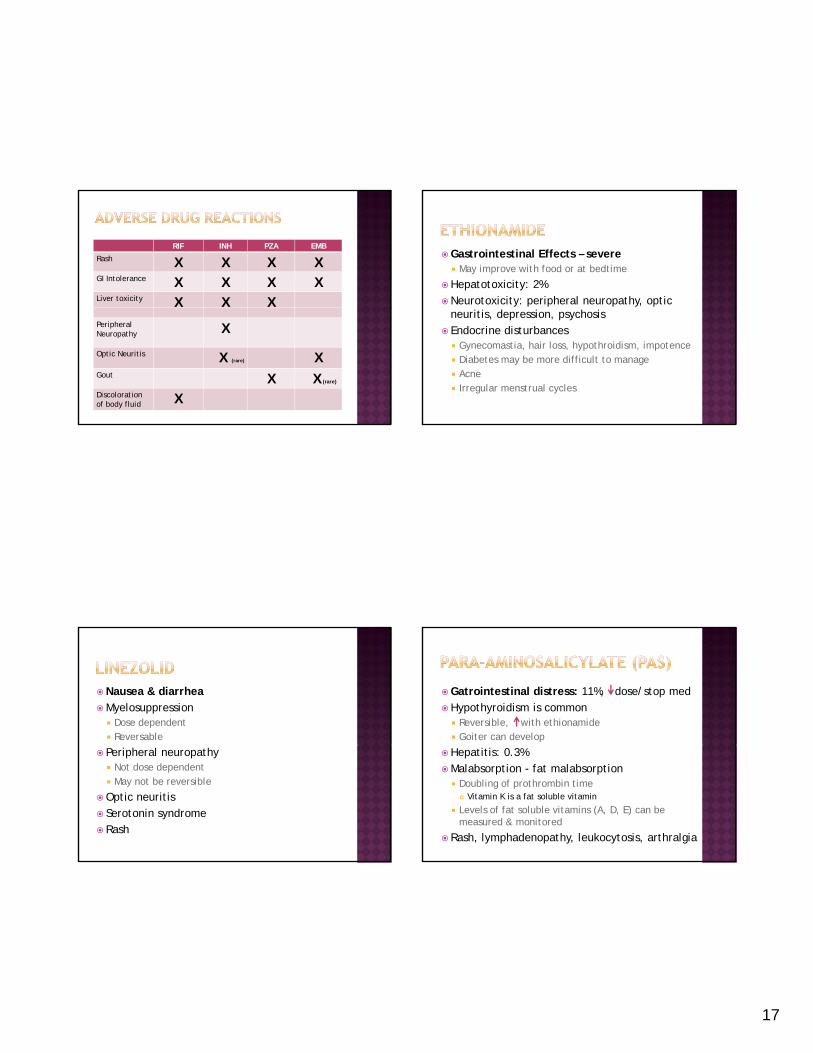
RIF INH PZA EMB
Rash X X X XGI Intolerance X X X XLiver toxicity X X XPeripheral Neuropathy X
Optic Neuritis X (rare) XGout X X (rare)
Discolorationof body fluid X
Gastrointestinal Effects – severe May improve with food or at bedtime
Hepatotoxicity: 2%Neurotoxicity: peripheral neuropathy, optic
neuritis, depression, psychosis Endocrine disturbances Gynecomastia, hair loss, hypothroidism, impotence Diabetes may be more difficult to manage Acne Irregular menstrual cycles
Nausea & diarrheaMyelosuppression Dose dependent Reversable
Peripheral neuropathy Not dose dependent May not be reversible
Optic neuritis Serotonin syndrome Rash
Gatrointestinal distress: 11%, dose/stop medHypothyroidism is common Reversible, with ethionamide Goiter can develop
Hepatitis: 0.3%Malabsorption - fat malabsorption Doubling of prothrombin time Vitamin K is a fat soluble vitamin
Levels of fat soluble vitamins (A, D, E) can be measured & monitored
Rash, lymphadenopathy, leukocytosis, arthralgia

18
Central nervous system effects: headaches, restlessness, suicidal ideation, psychosis, seizures (3% 500mg/day)
Caution in patients with underlying seizure di d t l illdisorders or mental illness
Pyridoxine 100-200mg/day may decrease neurotoxic side effect
Peripheral neuropathy Rash – skin changes (lichenoid eruptions,
Stevens-Johnson Syndrome)

![Treatment of Pediatric TB€¦ · 1/5/2011 6 TB DRUGS IN CHILDREN Aminoglycosides: Mostly CNS, drug-resistant TB Amikacin preferred for CNS [more resistance to streptomycin] OtoOto--](https://img.pdfslide.us/doc/110x75/5e94e78ad0de0f234a03c22a/treatment-of-pediatric-tb-152011-6-tb-drugs-in-children-aminoglycosides-mostly.jpg)