Embed Size (px)
Citation preview
In thIs Issue
p. 3 I’m sorryCheck out this sample apology letter one organization uses to apologize for ED waits.
p. 6 It’s time for dischargeRead how a collaborative—and organized—approach can improve patient flow.
p. 8 You’re totally in denialSee how patient access and case management can team up to reduce denials.
p. 10 that’s a good questionOur expert provides answers to some of your toughest observation questions.
For years, Domino’s Pizza had a 30-minute guarantee:
Order a pizza to be delivered, and if it’s not at your door-
step in 30 minutes or less, the pizza’s on Domino’s.
No questions asked.
Sister hospitals St. Mary’s in Blue Springs, MO, and St.
Joseph in Kansas City, MO, have their own 30-minute
guarantee: If you’re a patient in the ED, and you’re not
seen by a doctor or nurse practitioner within 30 minutes
of the time you walk in, you get two free movie passes.
No questions asked.
The facilities one-up the national pizza chain when it
comes to customer service—if they fail, they send a letter
of apology to patients. The 143-bed St. Mary’s and 300-
bed St. Joseph offer acute care, outpatient, and extended
Waiting for more than 30 minutes? We’ll send you to the moviesKansas City, MO, medical center guarantees a short wait in ER, or it’s tickets on the house
care services. They implemented the 30-minute rule in
June with an aim to trim wait times for ED patients and
improve their satisfaction.
Wait times for patients have not only improved—in
some cases by 40 minutes on overall stay in the depart-
ment—but the program also boosts staff morale, from
the person who registers the patients to the doctor who
treats them.
“We started this program with the idea of increas-
ing patient satisfaction and improving the quality with
patients coming
into the ER,” says
Deborah White,
coordinator of
public relations for
Carondelet Health, a
Catholic-sponsored
healthcare system
that includes five
facilities, including
St. Mary’s and St. Joseph, in the Kansas City metropoli-
tan area. “Overall, the staff has responded very positively.
They’re seeing how it affects patient quality and how
patients are pleased. A lot of the patients say we don’t need
to give them movie tickets, but we say we want to recog-
nize [their] time, and that we know we made [them] wait.
I think the fact that we’re acknowledging their time and
acknowledging the fact that we made them wait helps.”
Identifying the problem
White says St. Mary’s modeled its program after
a similar one in the Emergency & Trauma Center at
Borgess Health System and the Borgess-Pipp ED in
Kalamazoo, MI. They are all members of Ascension
Health, the largest national Catholic healthcare facility
in the nation.
> continued on p. 2
november 2007 Vol. 4, no. 11
“A lot of the patients say
we don’t need to give
them movie tickets,
but we say we want to
recognize [their] time,
and that we know we
made [them] wait.”
—Deborah White

Patient Access AdvisorPage 2
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
In its Emergency & Trauma Center, Borgess, accord-
ing to its Web site, makes the 30-minute guarantee work
with the following:
Bedside registration for all patients
Addition of a second triage bay
Streamlined triage process
Reorganization and reduction of paperwork
That is the model St. Mary’s adapted when it began
rethinking its ED response to patients in August 2006.
“We started looking at ED performance because we
knew there were things we needed to do better,” says
➤
➤
➤
➤
Debbie Gengler, RN, director of emergency services
for St. Mary’s. “Our initial plan was to get to the point
where patients would have a length of stay in the ER of
90 minutes. We started doing things to see if we could
get there.”
the process
St. Mary’s began in August with committee meetings
involving radiology, patient access representatives, and
staff nurses and doctors. They recorded times for patient
visits to the ED. They broke down the problems step by
step, from the time a patient parks to the time he or she
checks out and leaves the hospital.
➤ Parking. The first problem the team identified did
not begin with the registration process. It actually began
outside the hospital—in the parking lot.
“We did a patient-mapping process and went to the
parking lot,” says Gengler. “What are the obstacles?
One of them was we didn’t have designated emergency
patient parking areas. We had handicap spots and that
sort of thing, but we didn’t have a first-level tier for ER
patients. You would have visitors parking there, and it’s
sort of inconvenient for a person with an injured ankle
to have to hobble in to the emergency room.”
➤ Registration. When a patient comes in the door at
St. Mary’s, he or she is immediately greeted at the front
desk. Before, Gengler says, the center had the front desk
covered only 12 hours; now, it’s 24.
At St. Joseph, patient access representatives are
usually the first to see the patients. The representative
creates what the center calls a “short form” registra-
tion, just enough to create an account—name, birth
date, and reason why the patient is there. From there,
the information is logged in the ED’s FirstNet Tracking
system, a computerized monitoring program that uses
icons to track patient status. It informs the triage nurse
that someone needs to be seen. “It’s not even a minute
to do the short form,” says Denise Ashby-Cohen,
Wait time < continued from p. 1
> continued on p. 5
editorial Advisory Board Patient Access Advisor
Group Publisher: Lauren McLeod
Executive Editor: Lori Levans
Senior Managing Editor: Dom nicastro
Rose t. Dunn, RhIA, CPA, FAChe, FhFMA Chief operating officer, First Class Solutions, Inc., St. Louis, MO
Donna K. GilleyDirector of revenue cycle and regulatory compliance, LBMC Healthcare Group, Brentwood, TN
Amy harttVice president, VHA Southwest, Plano, TX
Diane Jepsky Healthcare consultant, Seattle, WA
steven OrvisSenior consultant, Sinaiko Healthcare Consulting, Los Angeles, CA
Joyce sourbeck, Ms, RnAssistant vice president for patient financial services, Washington Hospital Center, Washington, DC
David s. szabo Nutter, McClennen & Fish, LLP, Boston, MA
sandra J. Wolfskill, FhFMA President, Wolfskill & Associates, Inc., Chardon, OH
Joe Zebrowitz, MDExecutive vice president/senior medical director, Executive Health Resources, Newtown Square, PA
Patient Access Advisor (ISSN 1933-3307) is published monthly by HCPro, Inc., 200 Hoods Lane, Marblehead, MA 01945. Subscription rate: $399/year; back issues are available at $25 each. • Postmaster: Send address changes to Patient Access Advisor, P.O. Box 1168, Marblehead, MA 01945. • Copyright 2007 HCPro, Inc. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro, Inc., or the Copyright Clearance Center at 978/750-8400. Please notify us immediately if you have received an unauthorized copy. • For editorial comments or questions, call 781/639-1872 or fax 781/639-2982. For new subscriptions, renewals, change of address, back issues. billing questions, or permission to reproduce any part of PAA, call customer service at 800/650-6787, fax 800/639-8511, or e-mail: [email protected]. • Visit our Web site at www.hcpro.com. • Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to be included on this mailing list, please write to the Marketing Department at the address above. • Opinions expressed are not necessarily those of PAA. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions.
Patient Access Advisor is one of the resources from the Patient Access Resource Center from HCPro, Inc. For information, call 800/650-6787 or go to www.accessresourcecenter.com.

Patient Access Advisor Page 3
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
FormThis Month’s
➤ Download this entire form in the Patient Access Advisor section of www.accessresourcecenter.com.
sample customer service apology letter
The following is a sample apology letter St. Joseph Medical Center sends to patients if it does not keep its promise of a
30-minute wait time in the ED.
Dear Patient:
Thank you for choosing St. Joseph Medical Center’s emergency department. We hope your recent experience was positive, and
that you are well on the road to recovery.
At St. Joseph, our objective is to provide the highest level of quality care and treatment as quickly as possible. At the same time,
we must provide care based on the needs of all patients who are present. Patients in critical or serious condition must be seen
and stabilized first. For that reason, there are circumstances in which providing care to these patients makes it necessary for
other patients to wait longer than normal.
We regret that your visit to the emergency department coincided with one of these rare situations and that we were unable to
meet our promise of having you seen by a physician within 30 minutes. As a token of our understanding of the fact that you
were inconvenienced, enclosed are two movie tickets. We will continue to provide our 30-minute guarantee and expect to be
able to meet it nearly all of the time.
While you continue to recover, please remember that you are always welcome to contact us with any questions or concerns;
just call 816/943-2713 at any time.
Thank you once again for choosing St. Joseph. We look forward to providing you high-quality, timely care whenever you might
need it in the future.
Sincerely,
Karen Lee, MSN, RN, CNAA
Vice President, Nursing
Carondelet Health
Source: St. Joseph Medical Center, Kansas City, MO. Reprinted with permission.
Patient Access AdvisorPage 4
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
FormThis Month’s
➤ Download this entire form in the Patient Access Advisor section of www.accessresourcecenter.com.
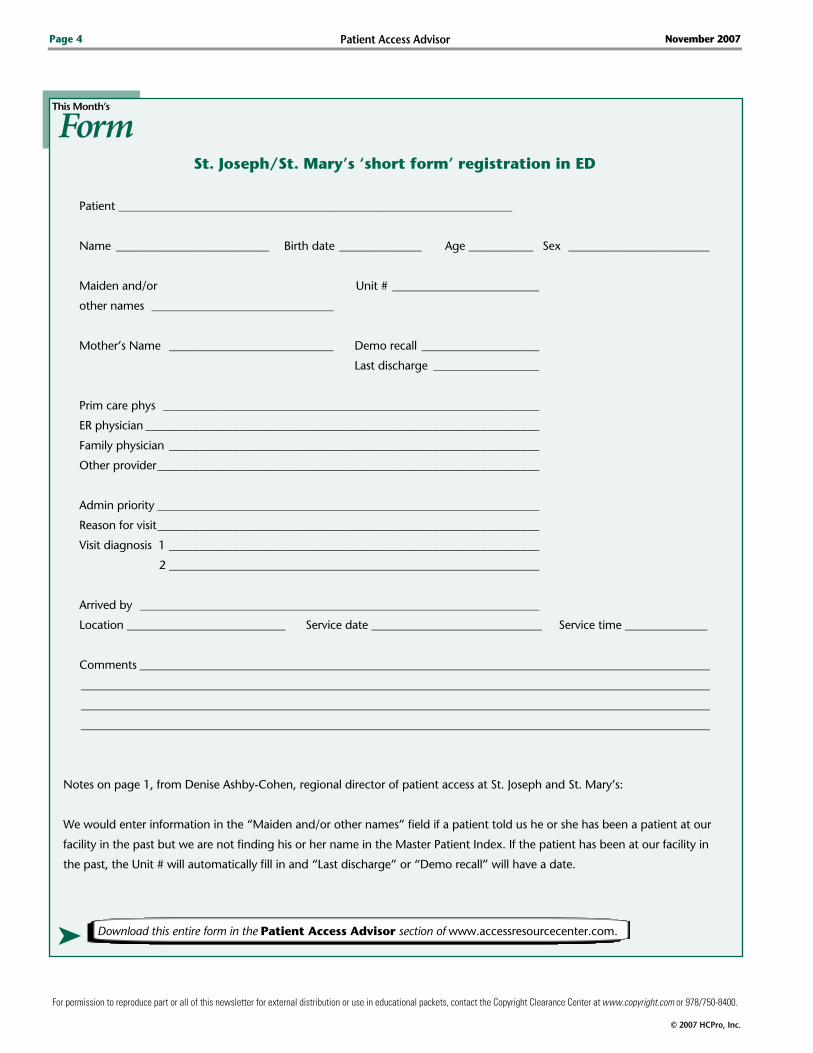
st. Joseph/st. Mary’s ‘short form’ registration in eD
Patient ___________________________________________________________________
Name __________________________ Birth date ______________ Age ___________ Sex ________________________
Maiden and/or Unit # _________________________
other names _______________________________
Mother’s Name ____________________________ Demo recall ____________________
Last discharge __________________
Prim care phys ________________________________________________________________
ER physician ___________________________________________________________________
Family physician _______________________________________________________________
Other provider _________________________________________________________________
Admin priority _________________________________________________________________
Reason for visit _________________________________________________________________
Visit diagnosis 1 _______________________________________________________________
2 _______________________________________________________________
Arrived by ____________________________________________________________________
Location ___________________________ Service date _____________________________ Service time ______________
Comments _________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
___________________________________________________________________________________________________________
Notes on page 1, from Denise Ashby-Cohen, regional director of patient access at St. Joseph and St. Mary’s:
We would enter information in the “Maiden and/or other names” field if a patient told us he or she has been a patient at our
facility in the past but we are not finding his or her name in the Master Patient Index. If the patient has been at our facility in
the past, the Unit # will automatically fill in and “Last discharge” or “Demo recall” will have a date.

FormThis Month’s
Patient Access Advisor Page �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
regional director of patient access at St. Joseph and St.
Mary’s, who manages a staff of 55. “It could be saving
five minutes of time or it could be saving 15 minutes of
time. If a patient has never been in the system, we have
to type in a lot of information.”
Once the short form is done, a patient access repre-
sentative marks a little key icon on the tracking board so
a triage nurse knows it’s that patient’s turn. The entire
registration is completed after the patient is treated—usu-
ally at bedside. “If we’ve completed registration but need
to get an ER copay, we’ll put a stop sign icon on there,”
says Ashby-Cohen, “so nurses can see that and stop [the
patient] before [he or she] leave[s].”
Gengler says the 30-minute program helps patient
access representatives strive for a goal and not forget
about the current patient. “Being aware and having a
goal to work toward has helped, whereas before if you
were working on something else, you would finish that
and then go to the current patient,” she says.
➤ On-site radiologist. St. Mary’s has a radiologist
technician dedicated to the ER who tracks patient flow
and anticipates the need for imaging. “If [he] see[s] a
patient come in with a broken arm, [he] say[s], ‘I’m
going to get an x-ray ready,’ instead of waiting for them
to come to radiology,” says White. “He’s keeping tabs on
what’s going on and anticipating any need for imaging
services.”
➤ Quick cleaning. Rooms are getting cleaned faster
now, ensuring a smooth transition for new patients.
Employees are also clearing out rooms on the inpatient
side faster for a quicker transition from the ER.
➤ Staff incentives. The facilities recognize staff work
on the 30-minute initiative. They give coupons for free
meals and other perks. “So if you have a day when you
hit 99 or 100%, we say, ‘Thanks for all your hard work,’ ”
says Gengler.
In all, the changes have helped decrease overall wait
times in the ER by 40 minutes in some cases, Gengler
says. As for ensuring the program works, White says the
center is always revisiting response times and tracking
patient response through telephone surveys.
Three months into the program, officials say it’s a win-
win for the ED—and for its patients, whose preference is
most likely quality, efficient care rather than a free pass
to the movies. “The concept is we understand their time
is valuable,” says Gengler. n
Wait time < continued from p. 2
st. Joseph/st. Mary’s ‘short form’ registration in eD (cont.)
The main fields we fill in are:
Name
Birth date
Age and sex
Family physician (if the patient has one)
“E” for emergency for the “Admin priority”
Reason for visit
Arrived by (car, ambulance, air ambulance)
Source: St. Joseph’s Medical Center, Kansas City, MO. Reprinted with permission.
➤
➤
➤
➤
➤
➤
➤

Patient Access AdvisorPage �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
Discharge appointments: Remedies for poor patient flowMost new front-end directors spend their first
couple of days on the job introducing themselves
to staff members and patients, touring the hospital,
and organizing their desks. This was not the case for
Jackie Connor, RN, MS, CCS, director of case man-
agement at St. Joseph’s Medical Center (SJMC) in
Townsend, MD.
Before she could even set up her office, Connor was
immediately assigned the duty of revamping SJMC’s
discharge system. “Literally the day I started, the exec-
utive team wanted me to assemble a task force to study
and explore new ways to improve hospital discharges,”
says Connor.
Like many hospitals, SJMC had a universal discharge
time system in place with a goal of getting all patients
discharged by 11 a.m.
After collecting and tracking data, Connor and the
new discharge task force—a team consisting of nurses,
physicians, social workers, and ancillary staff mem-
bers—decided that overall patient flow could be bet-
ter leveraged by pushing the discharge time back an
hour—to noon.
But midway through crafting her first policy change
and making the case for a later universal discharge
time, Connor had an epiphany: A noontime discharge
goal would only slightly improve patient flow and not
bring about the type of change the executive team
wanted to see.
“After looking at our ED visits, surgeries, OR sched-
ule, and population, we realized that a universal dis-
charge time—whether at 11 a.m. or noon—would still
create bolus discharges and bolus admissions later in
the day,” says Connor. “There would still be an uneven
workload throughout the day.”
After further dissecting the policy of universal dis-
charge times at SJMC, Connor and her team identified
the following flaws in its system:
The reality of discharging 70–80 patients at a desig-
nated time always created a chaotic scramble of ser-
vices and demands on the entire staff
No matter how hard case managers tried, it was
always an uphill battle to get all physicians to round
at certain times in the morning
Certain patients require more tests or special instruc-
tions, and addressing all of these issues within a few
hours in the morning was not realistic
After identifying the major roadblocks of the univer-
sal discharge time system, the discharge task force at
SJMC decided it was necessary to move in a completely
different direction and try something new. In an effort
to even patient flow and create balanced scheduling
throughout the day, Connor and her team abolished
universal discharge times and switched to a discharge-
by-appointment system.
how it works
SJMC case managers, along with members of the
discharge task force, now make daily rounds to identify
patients who are almost ready to be discharged. Once
a patient has been identified, a case manager or nurse
contacts the physician to get his or her approval, and a
scheduled discharge is made 24–48 hours in advance.
Discharge appointments are made throughout the
day—mornings, afternoons, and early evenings—based
on patient, family, and physician needs.
“After an appointment has been made, it goes into
the computer system, and the physician is reminded,
and the ancillary departments are notified so they can
prepare necessary labs and tests ahead of time instead
of having to scramble at the end,” says Connor. “This
structure allows doctors and ancillary staff time to pre-
pare and eliminates some of the surprise factors that
come along with patient discharges.”
➤
➤
➤
Patient Access Advisor Page 7
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
Under a scheduled system, if a physician wants to
see a final chest x-ray or a blood test, the ancillary staff
is alerted ahead of time and can prepare to have these
exams ready, adds Connor. The ancillary department’s
goal is to have all requested tests three hours before
a patient’s scheduled discharge time. This way, says
Connor, if anything unexpected arises, the department
has time to review and preplan.
“I’ve never done [discharge by appointment] at any
of the other facilities I’ve worked for, but it immediately
made sense,” says Connor. “The more predictable we can
make our work, the more we can manage our patient’s
expectations and, ultimately, their overall satisfaction.”
Implementation
Discharge by appointment at SJMC began on the
surgical unit and with interventional cardiology patients
and has recently expanded to include all hospitalists.
“We started piloting discharge by appointment on
the cardiac floor because it’s our largest practice and we
have more of a captive audience with these patients,”
says Connor. “And we expanded to our hospitalists first
because they’re generally more flexible and open to
ideas than the private physicians.”
After deciding where to pilot the new program and
who would be involved, the task force next had to
decide how to identify patients for discharge. “At first,
our goal was to attempt to predict a patient’s discharge
time and plan upon admission,” says Connor. “But
what we found was there were too many unknowns
during a patient’s first 24–48 hours. For example, a
cardiac patient would not even have a clear diagnosis
or course of treatment, which makes it very difficult to
schedule a discharge ahead of time.”
In light of this, the decision was made to schedule
discharges the day before they occur, says Connor.
“Every day, the case managers and nurses do rounds
to identify patients we believe are most likely to be dis-
charged the next day.”
“Some of the processes are automated,” Connor
adds. “In order for the scheduled discharge appoint-
ment to be recognized by the physician and the ancil-
lary departments, we have to communicate that time.
Before the date and time can be put into the system to
alert the physicians and the ancillaries, there has to be
an agreement between the case manager or nurse and
the physician.”
time saved, satisfaction gained
Discharging by appointment has drastically im-
proved communication between case managers and
physicians and also saves case managers a lot of time,
says Andrea Cottrell, MS, RN, case manager on the
cardiology floor at SJMC.
“Discharge times are now on a physician’s roster in
the morning, which helps them prioritize what patients
they need to see first,” says Cottrell. “So as a case man-
ager, I’m spending a lot less time on the phone tracking
down doctors and asking them for dictation, instruc-
tions, and what time they may or may not be able to
discharge a patient.”
Cottrell admits there are a few challenges to sched-
uling discharges by appointment, such as knowing
each physician’s rounding preferences and making sure
patients don’t slow down the process on their end by
not being prepared, but she says the benefits far out-
weigh these challenges.
“Case managers and nurses love this new system
because it helps us plan our day and we know exactly
what we have to do to get a patient discharged,” says
Cottrell. “Since getting rid of universal discharge times,
I’ve never felt more organized.” n
Contact senior Managing editor Dom nicastro
E-mail [email protected]
Questions? Comments? Ideas?
Patient Access AdvisorPage �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
Like many hospitals, West Virginia University Hospital
(WVUH) in Morgantown had a way of tracking and man-
aging details that resembled a game of scavenger hunt.
A denial would come in from an insurance company or
Medicare and often sit on someone’s desk or in-box for
days or weeks. The denial notice would then get passed
around and sometimes make it to the proper person or
department, and sometimes not. Once the notice found
its proper home, a mad scramble would ensue to reverse
the denial, but without a formal plan intact, WVUH was
successful only about half the time.
“Our denials were falling through the cracks,” says
Christy Whetsell, BSB, RN, MBA, director of care
management at WVUH. “Nobody really knew what to do
because we lacked a protocol and didn’t have a solid sys-
tem in place.”
To help streamline denials and organize an official
policy, a multidisciplinary team consisting of directors
from case management, patient access, finance, and the
executive suite got together and mapped out an entirely
new denial management protocol. The first plan of action
was to designate centralized headquarters for all denials
coming through the system, says Whetsell.
Because case management already worked as a liaison
between so many departments and followed patients
across the continuum of care, the team voted unani-
mously to make it the gatekeeper of denials.
However, being the gatekeeper didn’t mean that case
management would take responsibility for all denials, just
help direct them, says Whetsell.
“The next crucial step we took was to help define all
the different types of denials and assign who would be
responsible for each type,” says Whetsell.
For example, case management would oversee inpa-
tient denials while patient access would handle all preop-
eration denials.
“Assigning responsibility was huge, because before
everybody was essentially responsible, which meant
nobody was responsible,” says Whetsell.
Once WVUH’s denial infrastructure was in place, the
multidisciplinary team focused on the communications
component—getting the word out to payers. Whetsell
sent out letters to all the different insurance companies
explaining that all denial notices should be sent to the
case management department.
“We had to get everyone on the same page, both inter-
nally and externally,” says Whetsell. “Insurance compa-
nies would send notices to physician’s offices, to different
departments, and they would get lost in the maze. We
spent a lot of time reaching out to payers to get them to
understand our new system.”
To help get the word out, Whetsell began her public
relations campaign by:
Developing individualized relationships with pay-
ers through phone calls, e-mail, and scheduled
teleconferences
Using associations with patient access and patient
financial services to communicate to payers using
template language about how denials were to be
delivered to the hospital
Attending regularly scheduled payer update meetings
After establishing key contacts with each of the payers
and adequately getting the message out about how and
where to send denial notices, the next step for Whetsell
and the interdisciplinary team was to focus on the inter-
nal steps of denial management.
enter technology
Even though case management was elected headquar-
ters of denials, a centralized electronic database was creat-
ed, allowing anyone involved in the denials process access
➤
➤
➤
Case study
Denial management: Collaboration between front-end departments can result in significant improvement
Your source code: N0001
Name
Title
Organization
Address
City State ZIP
Phone Fax
E-mail address(Required for electronic subscriptions)
❏ Payment enclosed. ❏ Please bill me.❏ Please bill my organization using PO # ❏ Charge my: ❏ AmEx ❏ MasterCard ❏ VISA
Signature(Required for authorization)
Card # Expires(Your credit card bill will reflect a charge to HCPro, the publisher of PARC.)
❏ Start my subscription to Patient Access Resource Center immediately.
Options No. of issues Cost Shipping Total
❏ 1 yr membership 12 issues $399 (PARC) $24.00
Sales tax (see tax information below)*
Grand total
Order online at www.hcmarketplace.com.
Be sure to enter source code N0001 at checkout!
*Tax Information Please include applicable sales tax. Electronic subscriptions are exempt. States that tax products and shipping and handling: CA, CO, CT, FL, GA, IL, IN, KY, LA, MA, MD, ME, MI, MN, MO, NC, NJ, NM, NY, OH, OK, PA, RI, SC, TN, TX, VA, VT, WA, WI, WV. State that taxes products only: AZ. Please include $27.00 for shipping to AK, HI, or PR.
Mail to: HCPro, P.O. Box 1168, Marblehead, MA 01945 Tel: 800/650-6787 Fax: 800/639-8511 E-mail: [email protected] Web: www.hcmarketplace.com
For discount bulk rates, call toll-free at 888/209-6554.
PARC Subscriber Services Coupon
Patient Access Advisor Page �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
to information about any denial, any time. “Anyone can
access the database and submit information about a deni-
al, and the program will automatically send the denial to
the appropriate person or department responsible,” says
Whetsell. “This way, everybody knows we have a denial
out there and knows who’s handling it.”
Case management checks the database daily, moni-
tors start and end dates, and tracks the response activity
between the hospital and payers.
“Centralizing our denials has improved the speed in
which we submit and track denials and has enhanced
everybody’s awareness about their part in denial man-
agement,” says Whetsell.
tag-team effort
The final and perhaps most important step in WVUH’s
new denial management program is the ongoing dia-
logue and collaboration among case management, patient
access, and physicians, says Whetsell.
The three departments now have monthly meetings
to discuss denials, and directors at every level are more
involved.
Whetsell says her new role at these meetings is that
of translator because she’s able to talk numbers with the
finance people and clinical-speak with the physicians and
anyone else involved in medicine.
“I translate what the other person needs to hear,
because finance does not understand the clinical
complications that may be preventing a patient from
going home, and the clinicians don’t understand lan-
guage such as ‘your LOS is up,’ ” says Whetsell. “I help
bridge the perspectives, and this helps with fighting
denials.”
A strong new foundation combined with contin-
ued collaboration has paid off in a big way for WVUH.
Since overhauling its entire denials management pro-
gram two years ago, the hospital has seen the following
improvements:
Physicians now seeking information related to their
denials and actively participating in the appeal process,
which leads to stronger appeal letters
A decreased turnaround time with appeal submissions
and financial resolutions
Overall denial awareness from every healthcare pro-
fessional involved in patient care
The biggest mark of success, however, is in the hospi-
tal’s bottom line.
In 2005, before revamping its denials management
program, WVUH had a denial reversal rate of 50%, com-
pared to 2007 when 80% of all denials were reversed in
the hospital’s favor.
“We’ve improved because of our tracking methods,
interdisciplinary collaboration, and relationships with
payers,” says Whetsell. “If we didn’t make these changes,
we’d be in the same boat.” n
➤
➤
➤

Patient Access AdvisorPage 10
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
Editor’s note: Check out some of the questions your peers
asked during HCPro’s September audioconference “Inpatient
vs. Observation Status: Managing levels of care to ensure com-
pliance and reimbursement.”
The following responses are informational only and should
not be taken as official answers to the services described in the
clinical scenarios below. Our audioconference speaker Deborah
K. Hale, CCS, has provided her guidance in an attempt to help
hospitals sort through a number of observation status issues,
but each hospital should determine how to overcome its own
individual challenges. If you should need further clarification
or if you disagree with a response, we urge you to request guid-
ance from the appropriate healthcare professionals or regula-
tory agencies.
If a patient is in observation status for three days and
then converts to inpatient on day four, can the hospital
bill for observation status and the inpatient hospitalization?
For a Medicare patient, all diagnostic services pro-
vided within 72 hours (three calendar days) of the
inpatient admission order are rolled into the inpatient
account paid by DRG. The time in observation is not
separately paid, and the days don’t count toward the
acute care length of stay. This becomes a problem when
the patient requires skilled nursing facility care and does
not have enough inpatient days to achieve the three-day
qualifying stay. The observation days don’t count.
We are a small critical access hospital in rural
Wisconsin that does not have a 24-hour, seven-
day-a-week pharmacy in our town. We have analyzed
the numbers, and it’s just not cost-effective to have a
drug-dispensing machine at our facility. I’ve heard that
some hospitals just do not bill for drugs given out dur-
ing certain off-peak times, but I thought we had to bill
all Medicare patients the same. Could you clarify this?
Would you treat self-administered drugs and take-home
drugs the same?
Take-home drugs are to be billed with revenue code
253 (take-home drugs) and should be billed to the
patient, or the payment may be collected at the time of
service. Medicare does not cover these drugs for home
use, and the hospital must implement a process to iden-
tify take-home drugs. Self-administered drugs are those
drugs that can usually be self-administered by the patient
and are not integral to the treatment or procedure in the
outpatient setting. CMS clarified this in the 2003 OPPS
final rule and gave examples. This is also stated in CMS
Transmittal A-02-129.
If a patient is admitted to observation for chest
pain with negative enzymes, no EKG changes, and
has been in the hospital for 24 hours, and the physi-
cian decides to do a heart cath prior to discharge on the
second day, should this patient be changed to inpatient
after 24 hours? Additionally, if an outpatient cath patient
is kept in the hospital overnight for monitoring, should
he or she be changed to inpatient? Are there any specific
references/guidelines in the CMS manuals to cover these
types of situations, or anything related to chest pain
observation, heart caths, stents, etc.?
It is difficult to determine the appropriate steps
without reviewing the medical record. If all markers
continue to be negative and the patient is pain free and
has no other indicators for admission, most likely the
patient should remain as an observation patient. Please
understand that my response is not medical advice, and
only a physician should make a determination regard-
ing medical necessity of admission. See Medicare Benefit
Policy Manual, Chapter 1. In a PPS hospital (not critical
access), hospitals do not receive a separate observation
payment for chest pain if a status T procedure is provided
during the visit. Cardiac cath is a status T procedure. The
patient would continue to be considered an outpatient
if the continued stay and scheduling of the cath was for
the convenience of the physician, patient, or patient’s
Answers to your toughest observation inquiries

Patient Access Advisor Page 11
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
family. If there are risk factors that would make it unsafe
to send the patient home without performance of the
cath, and those factors are well documented in the medi-
cal record along with a timely inpatient admission order,
a physician reviewer might be convinced to approve the
inpatient stay.
We are a hospital that has a hemodialysis unit within
our organization. The certification of need for this
unit states that it is an inpatient facility and we cannot bill
for outpatient hemodialysis. We run into the following
scenario frequently: A patient comes to the facility with a
malfunctioning graft of some sort, and it is repaired as an
outpatient procedure. However, before the patient is dis-
charged, the physician would like to use the site to ensure
that there are no complications, or it is the patient’s
dialysis day and the physician wants the patient to receive
services before he or she leaves the hospital. If a patient
has been placed in observation status, is it appropriate to
change the status to inpatient because we are not allowed
to bill outpatient dialysis? Does this billing rule supercede
the observation status rule?
Several concerns come to mind. If the patient is an
outpatient surgery patient, observation would not be
appropriate for the routine recovery associated with this
procedure. If the patient develops a complication that
requires more than 4–6 hours of additional care, obser-
vation could be ordered for this additional time with
good documentation of the physician’s rationale. During
this recovery time, the patient’s need for dialysis may be
covered by billing HCPCS code G0257.
If an order to admit a patient is written by the attend-
ing physician and a locum tenens writes the discharge
orders to include “discharge patient and change patient
status to observation,” how should we bill the claim and
would additional documentation be required?
The initial order to admit as inpatient stands, and
the case is billed as an inpatient admission unless the
hospital’s utilization review committee has deemed the
admission unnecessary, and the appropriate procedure
is followed for billing as Condition Code 44 (if reviewed
and decided before discharge) or 121 (if determination is
made after discharge).
Education for locum tenentes, hospitalists, etc., is criti-
cal to comply with Medicare regulations.
We are having a hard time getting stop times docu-
mented. With IV fluid infusion—both intravenous
piggyback and longer maintenance fluids—if the volume,
start time, and infusion rate are clearly documented, is this
sufficient to calculate infusion time? Keep in mind we have
a policy of charting by exception if there is a problem.
Adequate documentation would include the begin-
ning and ending times of all infusion therapy, includ-
ing infusion hydration.
There are Medicare fiscal intermediaries that are per-
forming probe reviews on drug administration services,
such as Trailblazers, and they are stating that if the start
and end times are not documented for an infusion thera-
py, then it is not billable.
We recommend that facilities use a drug administra-
tion documentation form, which will prompt nursing
staff for all required documentation for injections and
infusion therapy. This form should be used in all out-
patient settings where drug administration is performed
(e.g., ED, observation, treatment room, chemotherapy,
and wound clinic).
If an on-call doctor admits a patient from the ER to
observation, and the attending doc comes in the
next day and changes the status to inpatient, should the
bill be separate for observation and inpatient, or will the
ER and observation be included in the inpatient bill?
All diagnostic services provided within 72 hours
(three calendar days) are rolled into the inpatient
admission and paid by DRG. (Exception: critical access
hospitals.) n

Patient Access AdvisorPage 12
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
november 2007
The following are FAQs CMS posted on its Web site
in regard to its July implementation of the “Important
Message from Medicare” requirement. You can read the
FAQs in their entirety at www.cms.hhs.gov/BNI/Downloads/
WeichardtFrequentlyAskedQuestionsJuly2007.pdf.
Representatives
When a patient is not competent, the representa-
tive cannot be located, and/or there is no current
phone number or address, what process meets CMS
requirements?
We recognize that any type of notice delivery
requirement, particularly in the acute care set-
ting, raises questions about authorized representatives.
However, the need to identify appropriate individuals
to deal with in these situations is not new or limited to
these notices.
Thus, hospitals should have processes in place for
identifying an individual who can act on behalf of an
incompetent patient. In some cases, state law addresses
cases where hospitals, nursing home administrators, or
the like can act as representatives or guardians for pur-
poses of making these decisions.
A representative cannot be reached by phone,
e-mail, or fax. For contact by certified letter, must
a hospital keep the patient until it gets the signed card
back by U.S. mail?
Providers have the flexibility to select a means of
delivery that is most appropriate for their opera-
tions (e.g., U.S. mail, FedEx, UPS, or a phone/faxed
response). If a representative is to be contacted using
certified U.S. mail, hospitals should initiate the process in
a timely fashion that will allow return of the card before
discharge. If the card indicates a refusal to sign or that
the notice is undeliverable, the hospital may proceed
accordingly. (Please refer to the Manual Instructions in
Chapter 30, Section 200.3.1, “Delivery of the Important
Message from Medicare,” subsection “Notice Delivery to
Representatives,” of the Medicare Claims Processing Manual.)
Documentation of the IM follow-up copy
If hospitals use a new blank IM for the follow-up copy
and obtain a signature on the form, do they keep
that form in the medical record (permanent) or do they
just give it to the patient?
You may either make a copy of the new signed IM
and put the copy in the patient record, or keep the
signed page 1 for the medical record and give page 2 to
the patient.
Inpatient to inpatient transfers
Two hospitals have different Medicare ID (provider)
numbers. Patients are transferred from one facility
to the other for other inpatient care. Sometimes patients
are returned to the initiating facility, whereas other times
they remain at the second facility to later be discharged
or moved to a lower level of care. Does the sending hos-
pital need to issue a follow-up copy of the IM? Does the
receiving facility need to issue a new IM?
Regardless of the hospital affiliation, the receiv-
ing hospital would provide a new IM if the transfer
involves different Medicare ID (provider) numbers.
However, no follow-up copy is needed prior to leaving
the sending hospital/unit if the transfer is an inpatient to
inpatient hospital level of care. The hospital ultimately
responsible for discharging the patient (i.e., releasing or
lowering the level of care) would provide the follow-up
copy if more than two days have passed since the last IM
was delivered.
Whenever the sending and receiving units have the
same provider number, no follow-up copy and no new
IM is required. The hospitals would operate as if it is
continual inpatient care from the same facility. n
CMs: ‘Important Message from Medicare’ FAQs
Emergency department scripting
A supplement to Patient Access Advisor November 2007
CP—Care personnel (i.e., nurse, nurse’s aide, licensed practical nurse)
PT—Patient
PSR—Patient service representative
CP (escorting): “Please let me escort you to our checkout area.”
PT: “Okay, thank you.”
CP (directing): “Please let me give you directions to our checkout area. They are printed here (handing the
patient written directions), but I will also review them with you before sending you on your way.”
PT: “Okay, thank you.”
If patient/guarantor asks what will happen at the checkout area . . .
CP: “Our checkout area is where we will verify all of the information we have recorded. We want to be sure that
we file your insurance claim quickly and correctly.”
If the patient/guarantor states that there is no insurance coverage . . .
CP: “Thank you. I understand. However, our checkout area will still need to verify the information you have pro-
vided for our billing records.”
If the patient/guarantor expresses concern about proceeding to the checkout area . . .
CP: “I’m sure when we/you arrive at the checkout area, they will be able to answer any questions you have.”
CP has successfully escorted/directed the patient/guarantor to the checkout area . . .
PSR : “Good morning/afternoon [applicable title and name[. Thank you, ______________ [name of CP if escorted
to PSR]. My name is ______________ and I am a patient service representative here at [name of hospital].
I’m sorry an emergency brought you here today, and I hope things are better now. Let me explain quickly
what we will be doing. Is that okay?”
PT: “Yes” or “no.”
PSR (if “no”): “What may I help you with before we go on?”
Note: Based on the response, it may be necessary to reconnect with the CP or allow the PT time to take care of
some immediate need (i.e., going to the restroom, getting a beverage, handing off a child, etc.).
Training ToolTraining Tool

Emergency department scripting (cont.)
PSR (if “yes”): “I just need to review some of the information you have provided. We want to be sure we have
complete and accurate information to file a claim with your insurance company. Let’s go over this quickly,
and please feel free to interrupt me if you don’t understand something or if we have recorded something
incorrectly. Does that sound alright to you?”
PT: “Yes” or “no.”
Source: Scripting developed by The Cleveland Clinic Health System and provided by Southwest General Healthcare Patient Access; 2004. Reprinted with permission from Wolfskill & Associates, Chardon, OH, www.wolfskill.com.
November 2007 A supplement to Patient Access Advisor









![One Republic- Apologize [Piano Sheet]](https://img.pdfslide.us/doc/110x75/55cf8e6e550346703b9211fc/one-republic-apologize-piano-sheet.jpg)