Embed Size (px)
Citation preview
© Sudan JMS Vol. 7, No.4. December 2012 43
VVttááxx eexxÑÑÉÉÜÜààGiant orbitofacial basidiobolomycosis: diagnostic and management
challenges in a resource limited environment.Akhiwu B. Idemudia1*, Adebola R. Adetokumbo1, Atanda T.Akinfenwa2,
Kolo E. Sara3
AbstractBasidiobolomycosis, a rare disease caused by the fungus Basidiobolusranarum, an environmentalsaprophyte, member of the class Zygomycetes; order Entomophthorales, found worldwide is anopportunistic infection that can be life-threatening in immune compromised patients. This reportpresents an unusual case of a giant orbito-facial basidiobolomycosis in a 30-year-old, otherwisehealthy Nigerian farmer. The diagnostic and treatment challenges peculiar in our environment werealso discussed.
Key words: orbitofacial lesions, fungal infections, basidiobolomycosis, Splendore-Hoeppliphenomenon.
asidiobolomycosis is a rare fungaldisease caused by the saprophyticfungus Basidiobolusranarum, an
environmental saprophyte that is usuallytransmitted by inoculation and largelyrestricted to tropical areas of Africa, Asia, andSouth America1. Except for theiropportunistic character, little is known aboutits pathogenesis; hence the use of broad-spectrum and highly nephrotoxic antifungalagents like amphotericin B2. Also, it ischaracterized by the formation of firm andnon-tender swellings, generally on theextremities, trunk, and rarely other parts ofthe body. Thotanet al3 have described theselesions as mimicking a soft tissue tumor. Tothe authors� knowledge,no report ofgiganticorbitofacialbasidiobolomycosisoccurringbilaterally was found in the English literature.We, therefore, share our experience ondiagnostic and management challenges of arare.________________________________________________________1. Consultant Oral & Maxillofacial surgeon, AminuKano Teaching Hospital/Bayero University, KanoNigeria.2. Consultant Pathologist. Department of Pathology,Aminu Kano Teaching Hospital.3. ConsultantOtorhinolaryngologist.Department ofOtorhinolaryngology, Aminu Kano Teaching Hospital.* correspondence:Dr.Akhiwu Benjamin Idemudia.
E-mail: [email protected]
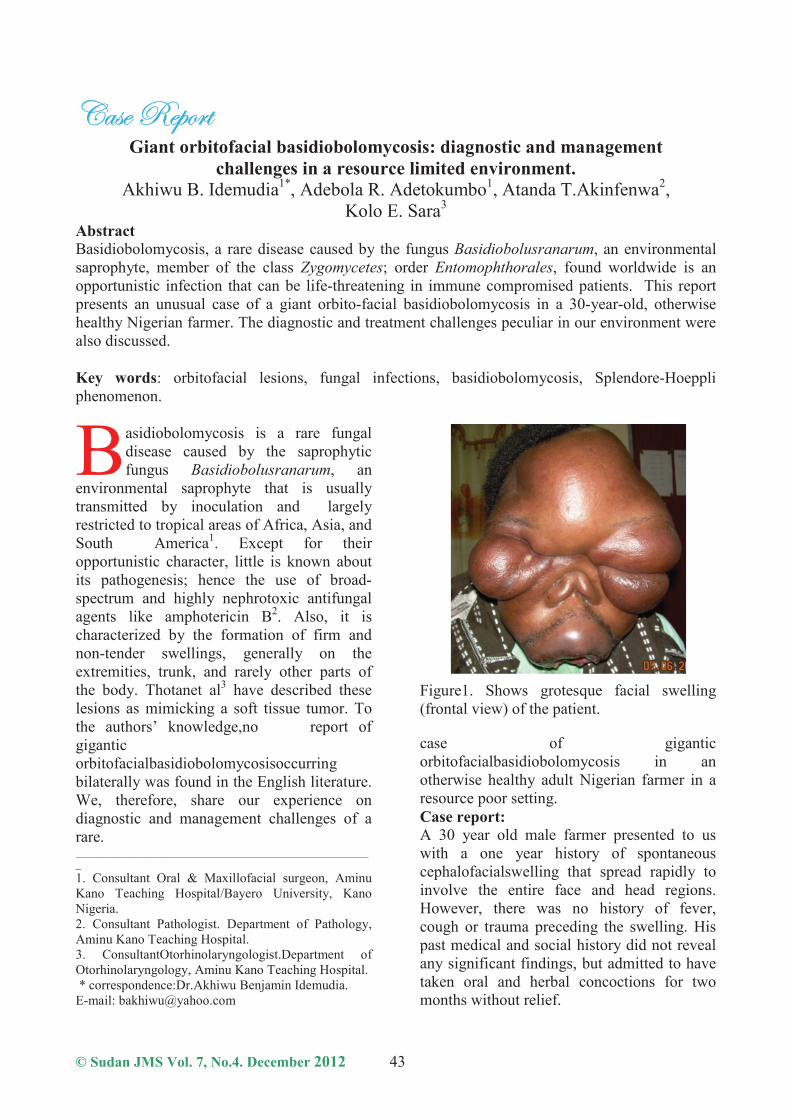
Figure1. Shows grotesque facial swelling(frontal view) of the patient.
case of giganticorbitofacialbasidiobolomycosis in anotherwise healthy adult Nigerian farmer in aresource poor setting.Case report:A 30 year old male farmer presented to uswith a one year history of spontaneouscephalofacialswelling that spread rapidly toinvolve the entire face and head regions.However, there was no history of fever,cough or trauma preceding the swelling. Hispast medical and social history did not revealany significant findings, but admitted to havetaken oral and herbal concoctions for twomonths without relief.
B

Akhiwu B. Idemudia et al Giant orbitofacial basidiobolomycosis
© Sudan JMS Vol. 8, No.1. Mar 2013 44
On admission, he was weak, mildly pale,anicteric, acyanosed and vital signs werestable. Maxillofacial examination showedbilateral gross cephalofacialdysmorphism(Fig. 1), with affectation of the fronto-parietal, ocular (with inability to part open theeyelids), nasal and orofacial regions.Swellings were smooth and rounded mostlysubcutaneous, non-tender, mobile, with mixedconsistency (firm and nodular); but baggy andsoft around the eyes, with inability to partopen the eyelids. The overlying skin wasnormal. Except for the presence of trismus,the intra-oral, neck and other systemicexaminations were essentially normal.All the blood investigations were normal.Plain radiograph revealed only soft tissueswellings. A CT scan was not done becauseof financial constraints by the patient.A wedge shaped intraoral incisional tissuebiopsy under local anaesthesia was taken andsent for microbiological and histopathologicalexaminations.Microbiological examination of tissue wettedwith 10% potassium hydroxide revealedbroad, irregular hyphae. Culture withSabouraud�s dextrose agar could not be donedue to non-availability of the reagent in ourcentre at the time the patient was seen.Histopathological examination withHematoxylin and Eosin stains showed severalfungal spores and hyphae surrounded bymixed inflammatory cell infiltrates containinghistiocytes, multinucleated giant cells andnumerous eosinophils within the stromaclassical of Splendore-Hoeppli phenomenon(fig.2). There was, however, no evidence ofmalignancy.GrocottGomoriMethenamineSilver was usedto stain the tissue specimen which revealedelongated structure with irregular diameter,thin- walled, broad-based ribbon-like, non-septate fungal hyphae within the tissue (Fig.3). As a result, a presumptive diagnosis ofbasidiobolomycosis infection was made asdefinitive diagnosis would require culture ofthe organism, serological testing via animmunodiffusion method as well as DNA
Fig. 2.shows several fungal spores andhyphae (A) surrounded by multinucleatedgiant cells (B) engulfing them andsurrounding stroma showing numerouseosinophils (C). H and E X20.
Fig. 3.shows broad-based ribbon-like, non-septate fungal hyphae (arrow) within thetissue. Grocott Gomori Methenamine SilverX100.
sequence analysis (facilities not available inour center). Consequently, the patient wascommenced on long term oral antifungaltherapy (fluconazole 400mg/day) withsuccessful outcome resulting in a remarkablereduction of facial swelling after four months.Other medication given was ocular genticinfor one week. Patient was followed up for aperiod of one year at monthly interval but waslost thereafter. Patient was located by one ofthe authors two years later with a residualbaggy swelling and ectropion of the rightlower eyelid that would require surgicalexcision (Figure 4).

Akhiwu B. Idemudia et al Giant orbitofacial basidiobolomycosis
© Sudan JMS Vol. 8, No.1. Mar 2013 45
Figure 4. Residual upper lip swelling withbaggy tissues and ectropion of the right lowereyelid.
Discussion:Basidiobolomycosis is a rare fungal infectionoccurring almost exclusively inimmunocompromised individuals4. To theauthors� knowledge (Medline Englishliterature search), only unilateral cases havebeen reported in the orbitofacial region andnone in the northern part of Nigeria.Although our patient lacked any of the knownpredisposing factors the fact that he is afarmer might suggest a possible aetiologicalfactor.As a results, traumatic implantation couldprobably be the route of entry in this patientas highlighted in the literature5, 6 . Hence, theneed for physicians, microbiologists andpathologists to consider basidiobolomycosisas a differential for swellings involving theorofacial region as this could increase theprobability of an early and accurate diagnosis.Otherwise, these pathogens can disseminateperhaps, with significant morbidity andmortality as seen with the marked trismusresulting in limitation of mouth opening. Themanagement of this patient has not beenwithout its challenges, especially in aresource limited setting like ours. Forinstance, this patient could not afford the costof a CT scan. Therefore, the extent of thislesion and its relationship with vital structuresin this region could not be ascertained. Again,the response to treatment could not be
adequately monitored since the patient wasplaced on long term antifungal therapy.The diagnosis of basidiobolomycosis is basedon clinical and pathologic features.Confirmation is done by culturing themicroorganism on Sabouraud's dextrose agarand lactophenol cotton blue wet mount.6 Thediagnostic dilemma we had was due tononavailability of the culture medium. Hence,our reliance on presumptive diagnosis usingGrocott-gomorimethenamine silver staintechnique.Basidiobolomycosis is a potentially curabledisease that mimics a tumor. Cases have beenreported in the literature wherebasidiobolomycosis was misdiagnosed as softtissue tumor, sarcomas and even as Burkitt�slymphoma5, 9. The medical treatmentadvocated for basidiobolomycosis is with oralsaturated potassium iodide therapy, as well asazoles especially intravenous itraconazole.8Treatment with terbinafine and itraconazolecombination has been used with successfuloutcome10. In the present case, our patientwas placed on high dose oral fluconazole. Ithas the advantage of being safe, cost effectiveand has few drug interactions11. Interestinglyin spite of the severity and the presence ofpoor prognosticators (orbital involvement andtrismus with limitation of mouth opening),this patient made a remarkable clinicalimprovement with oral fluconazole.Regrettably, this patient defaulted on hisfollow up appointments; although, this is acommon phenomenon in our practice.Perhaps, this could possibly be attributed toignorance and poverty. As a result, thechances of recurrence and even death fromthis disease remain high.In conclusion, we have presented an unusualcase of orbitofacialbasidiobolomycosishighlighting some peculiar challenges in itsmanagement in our practice.
Acknowledgement:We wish to thank the entire staff of the dentaland maxillofacial department of Aminu KanoTeaching Hospital for their cooperationduring

Akhiwu B. Idemudia et al Giant orbitofacial basidiobolomycosis
© Sudan JMS Vol. 8, No.1. Mar 2013 46
the course of this work. Also, we are gratefulto Profs Ajike and Ladeinde for theirencouragement.
References :1. Taha SM, Masaad AM, Hassan LA et al.
Gastrointestinal Basidiobolomycosis mimickingcolon cancer in a Sudanese patient. Sudan Journalof Medical Sciences 2011; 6(1): 51 � 54.
2. Auxiliadora-Martins M, Alkmim-Teixeira GC,Machado-Viana J et al. Meningoencephalitiscaused by a zygomycete fungus (Basidiobolus)associated with septic shock in animmunocompetent patient: 1-year follow-up aftertreatment. Braz J Med Biol Res 2010; 43(8): 794-798.
3. Thotan SP, Kumar V, Gupta A et al. Subcutaneousphycomycosis-fungal infection mimicking a softtissue tumor: a case report and review of literature.Journal of Tropical Pediatrics 2010; 56(1): 65�66.
4. Iatta R, Napoli C, Borghi E et al. Rare mycoses ofthe oral cavity: a literature epidemiologic review.Oral Surg, Oral Med, Oral Pathol, OralRadiolEndod. 2009; 108(5): 647 � 54.
5. Khan ZU, Khoursheed M, Makar R.Basidiobolusranarum as an etiological agent ofgastrointestinal zygomycosis. J ClinMicrobiol2001; 39(6):2360 � 3.
6. Naniwadekar MR, Jagtap SV, NikamBP et al.Subcutaneous phycomycosis in a child. Online JHealth Allied Scs. 2009; 8(3): 14.
7. Gugnani HC. A review of Zygomatosis due toBasidiobolusranarum. Eur J Epidemiol, 1999;15(10): 923 � 9.
8. Sujatha S, Sheeladevi C, KhyriemA et al.Subcutaneous zygomatosis caused byBasidiobolusranarum � a case report. Indian J MedMicrobiol 2003; 21(3): 205 � 6.
9. Mani A, Sanjay D, Dilip P et al. Subcutaneouszygomycosis due to Basidiobolusranarum: A casereport from Maharastra, India. J Tropical Med2010; vol 2010: Article ID 950390. doi:1155/2010/950390.
10. Goyal A, Gupta N, Das S et al.Basidiobolomycosis of the nose and face: a casereport and a mini-review of unusual cases ofbasidiobolomycosis. Mycopathologia 2010;170(3): 165 � 8.
11. Zonios DI, Bennett JE. Update on azoleantifungals. SeminRespirCrit Care Med. 2008;29(2):198 � 210.






