Embed Size (px)
Citation preview

VTE PreventionVTE Prevention
Roxie M. Albrecht, MD, FACSRoxie M. Albrecht, MD, FACS
Associate Professor of SurgeryAssociate Professor of Surgery
University of OklahomaUniversity of Oklahoma

Rationale for Rationale for ThromboprophylasisThromboprophylasis
• High Prevalence of VTEHigh Prevalence of VTE
• Adverse Consequences of VTEAdverse Consequences of VTE
• Efficacy and effectiveness of Efficacy and effectiveness of thromboprophylaxisthromboprophylaxis– Highly efficacious in prevention of DVTHighly efficacious in prevention of DVT– Highly efficacious in prevention of symptomatic Highly efficacious in prevention of symptomatic
VTE and fatal PEVTE and fatal PE– DVT prevention prevents PEDVT prevention prevents PE– Cost effectiveness has been demonstratedCost effectiveness has been demonstrated

IncidenceIncidence
• 10-40% in medical or general surgery 10-40% in medical or general surgery patientspatients
• 40-60% following major orthopaedic 40-60% following major orthopaedic surgerysurgery
• 10% hospital deaths attributed to PE10% hospital deaths attributed to PE

Absolute Risk of DVT in Absolute Risk of DVT in Hospitalized PatientsHospitalized Patients
Patient GroupPatient Group DVT Prevalence, %DVT Prevalence, %Medical patientsMedical patients 10-2010-20
General surgeryGeneral surgery 15-4015-40
Major GYN surgeryMajor GYN surgery 15-4015-40
Major GU surgeryMajor GU surgery 15-4015-40
NeurosurgeryNeurosurgery 15-4015-40
StrokeStroke 20-5020-50
Hip or Knee surgeryHip or Knee surgery 40-6040-60
Major TraumaMajor Trauma 40-8040-80
Spinal Cord InjurySpinal Cord Injury 60-8060-80
Critical Care patientsCritical Care patients 10-8010-80

Consequences of Unprevented VTEConsequences of Unprevented VTE
• Symptomatic DVT and PESymptomatic DVT and PE• Fatal PEFatal PE• Costs of investigating symptomatic patientsCosts of investigating symptomatic patients• Risks and costs of treating unprevented VTERisks and costs of treating unprevented VTE• Increased future risk of recurrent VTEIncreased future risk of recurrent VTE• Chronic post-thrombotic syndromeChronic post-thrombotic syndrome

Thromboprophylaxis reduces Thromboprophylaxis reduces VTE eventsVTE events
• PE is the most common preventable PE is the most common preventable cause of hospital deathcause of hospital death
• Highest ranked safety practice -Highest ranked safety practice -– Appropriate use of VTE prophylaxisAppropriate use of VTE prophylaxis

Risk Factors for VTERisk Factors for VTE
• SurgerySurgery• TraumaTrauma• Immobility, paresisImmobility, paresis• MalignancyMalignancy• Cancer therapyCancer therapy• Previous VTEPrevious VTE• Increasing ageIncreasing age• Pregnancy and postpartumPregnancy and postpartum• Estrogen-containing oral Estrogen-containing oral
contraception or HRTcontraception or HRT• Selective estrogen receptor Selective estrogen receptor
modulatorsmodulators• Acute medical illnessAcute medical illness
• Heart or respiratory failureHeart or respiratory failure• Inflammatory bowel diseaseInflammatory bowel disease• Nephrotic syndromeNephrotic syndrome• Myeloproliferative disordersMyeloproliferative disorders• Paroxysmal nocturnal Paroxysmal nocturnal
hemoglobinuriahemoglobinuria• ObesityObesity• Smoking Varicose veinsSmoking Varicose veins• Central venous Central venous
catheterizationcatheterization• Inherited or acquired Inherited or acquired
thrombophiliathrombophilia

Risk Factor StratificationRisk Factor Stratification
• Individual ApproachIndividual Approach– Individual predisposing factors and risk Individual predisposing factors and risk
associated with current illness or associated with current illness or procedureprocedure
• Group-specific prophylaxisGroup-specific prophylaxis

Guidelines for ProphylaxisGuidelines for Prophylaxis
• American College of Chest PhysiciansAmerican College of Chest Physicians– Chest 2004Chest 2004
• Grade I – Recommendations are strong and indicate that Grade I – Recommendations are strong and indicate that the benefits do or do not out weigh risks, burden and the benefits do or do not out weigh risks, burden and costscosts
• Grade 2 – Recommendations are less certain. Suggest Grade 2 – Recommendations are less certain. Suggest feasibility, acceptability and cost related to feasibility, acceptability and cost related to implementation strategies. implementation strategies.
• Grade A – RCT’s with consistent resultsGrade A – RCT’s with consistent results• Grade B – RCT’s with inconsistent results or method Grade B – RCT’s with inconsistent results or method
weaknessesweaknesses• Grade C – Observational studies or generalizations from Grade C – Observational studies or generalizations from
one group of patients in a RCT. A one group of patients in a RCT. A ++ is given if the is given if the generalizations are secure or overwhelming.generalizations are secure or overwhelming.

Methods of ProphylaxisMethods of Prophylaxis
• Mechanical MethodsMechanical Methods– Graduated Compression StockingsGraduated Compression Stockings– Intermittent pneumatic compression deviceIntermittent pneumatic compression device– Venous foot pumpVenous foot pump
• StudiesStudies– Not blindedNot blinded– High rate of false negative scansHigh rate of false negative scans– Compliance in true practice – poorCompliance in true practice – poor
• Acceptable optionAcceptable option– High risk for bleeding (Grade 1C+)High risk for bleeding (Grade 1C+)– Adjunct to anticoagulant prophylaxis (Grade 2A)Adjunct to anticoagulant prophylaxis (Grade 2A)
• Improves efficacy when used in combination with anticoagulant Improves efficacy when used in combination with anticoagulant prophylaxisprophylaxis

Methods of ProphylaxisMethods of Prophylaxis
• AspirinAspirin– Poor study methodsPoor study methods
• Acceptable DVT screening – 38%Acceptable DVT screening – 38%• ASA alone in only 1/3 of trialsASA alone in only 1/3 of trials
– No significant benefitNo significant benefit– Small increased risk of major bleedingSmall increased risk of major bleeding– Poor results v. LMWHPoor results v. LMWH– Not recommended alone for VTE in any Not recommended alone for VTE in any
patient group (Group 1A)patient group (Group 1A)

Unfractionated Heparin &Unfractionated Heparin &Low Molecular Weight HeparinLow Molecular Weight Heparin
• Most widely used and studied prophylaxisMost widely used and studied prophylaxis• Low molecular weight heparin have more Low molecular weight heparin have more
predictable pharmacokinetic and predictable pharmacokinetic and pharmacodynamic properties due to consistent pharmacodynamic properties due to consistent binding sitesbinding sites
• Dosing LMWH more cumbersome – Anti – Xa Dosing LMWH more cumbersome – Anti – Xa monitoringmonitoring
• UFH – needs site specific validation of aPTT UFH – needs site specific validation of aPTT therapeutic range due to variability of reagentstherapeutic range due to variability of reagents
• LMWH – ? Limited uses in renal failure and LMWH – ? Limited uses in renal failure and obesity – dose adjustments possibleobesity – dose adjustments possible

Low Molecular Weight HeparinLow Molecular Weight Heparin
• Reduced anti-factor IIa relative to anti-factor Xa Reduced anti-factor IIa relative to anti-factor Xa activityactivity
• More favorable benefit/risk ratio in animal More favorable benefit/risk ratio in animal studiesstudies
• Superior pharmacokinetic propertiesSuperior pharmacokinetic properties– SC bioavailability near 100%SC bioavailability near 100%– More predicable dose response peak at 3-5 hrMore predicable dose response peak at 3-5 hr
• MonitoringMonitoring– Renal failure (CrCl < 30mL/Kg) & obesityRenal failure (CrCl < 30mL/Kg) & obesity
• Four hours post dose - anti-factor Xa levelFour hours post dose - anti-factor Xa level– Enoxaparin 1.0 IU/mL, Tinzaparin 0.85 IU/mL, Nadroparin 1.3 Enoxaparin 1.0 IU/mL, Tinzaparin 0.85 IU/mL, Nadroparin 1.3
IU/mL, Dalteparin 1.05 IU/mLIU/mL, Dalteparin 1.05 IU/mL

Reversal LMWHReversal LMWH
Protamine Neutralizes approx. 60%Protamine Neutralizes approx. 60%– 1mg per 100 anti-factor Xa units LMWH1mg per 100 anti-factor Xa units LMWH
• 1 mg enoxaparin = 100 anti-factor Xa units1 mg enoxaparin = 100 anti-factor Xa units
• ? Activated factor VIIa ? Activated factor VIIa

General SurgeryGeneral Surgery
• 46 RTC Low Dose Unfractionated 46 RTC Low Dose Unfractionated Heparin v. placebo or no proph.Heparin v. placebo or no proph.– Reduced Reduced
• DVT 22 to 9%DVT 22 to 9%• Symptomatic PE 2 to 1.3%Symptomatic PE 2 to 1.3%• Fatal PE .8 to 3%Fatal PE .8 to 3%
• Meta-analysis Meta-analysis – 5000 Units TID more efficacious than BID5000 Units TID more efficacious than BID– No increase in wound hematoma or No increase in wound hematoma or
bleedingbleeding

General SurgeryGeneral Surgery
• LMWHLMWH– Meta-analysis Meta-analysis (Douketis Arch Intern Med 2002)(Douketis Arch Intern Med 2002)
• 70 % reduction DVT v. no prophylaxis70 % reduction DVT v. no prophylaxis
– Nine meta-analysis and systematic reviewsNine meta-analysis and systematic reviews• No difference in DVT LMWH and UFHNo difference in DVT LMWH and UFH• Some trial fewer hematomas and bleeding Some trial fewer hematomas and bleeding
complications with LMWHcomplications with LMWH• No difference in total mortality, fatal PE between LDUH No difference in total mortality, fatal PE between LDUH
5000 units TID and LMWH5000 units TID and LMWH

General SurgeryGeneral Surgery
• Low RiskLow Risk– Minor SurgeryMinor Surgery– < 40 years of age< 40 years of age– No additional risk factorsNo additional risk factors
• RiskRisk– DVT DVT Calf – 2%Calf – 2% Proximal – 0.4%Proximal – 0.4%– PEPE Clinical – 0.2%Clinical – 0.2% Fatal - <0.01%Fatal - <0.01%
• Prevention StrategiesPrevention Strategies– No specific prophylaxis; early mobilizationNo specific prophylaxis; early mobilization– Grade 1C+Grade 1C+

General SurgeryGeneral Surgery• Moderate RiskModerate Risk
– Minor Surgery with additional risk factorsMinor Surgery with additional risk factors– Age 40-60 with no risk factorsAge 40-60 with no risk factors– Major surgery, < 40 with no risk factorsMajor surgery, < 40 with no risk factors
• RiskRisk– DVTDVT Calf - 10-20%Calf - 10-20% Proximal - 2-4%Proximal - 2-4%– PEPE Clinical - 1-2%Clinical - 1-2% Fatal - 0.1-0.4 %Fatal - 0.1-0.4 %
• Prevention StrategiesPrevention Strategies– LDUH (5,000 units q 12 hours, start 1-2 hrs pre-op)LDUH (5,000 units q 12 hours, start 1-2 hrs pre-op)**– LMWH ( LMWH ( << 3,400 U daily) 3,400 U daily)**– (Grade 1A)(Grade 1A)
– Graduated compression stockingsGraduated compression stockings– Intermittent Pneumatic Compression devicesIntermittent Pneumatic Compression devices

General SurgeryGeneral Surgery
• High RiskHigh Risk– Non-major surgery in age > 60 yr. or have additional Non-major surgery in age > 60 yr. or have additional
risk factorsrisk factors– Major Surgery > 40 or have additional risk factorsMajor Surgery > 40 or have additional risk factors
• RisksRisks– DVTDVT Calf – 20-40%Calf – 20-40% Proximal – 4-8%Proximal – 4-8%– PEPE Clinical – 2-4 %Clinical – 2-4 % Fatal – 0.4-1.0%Fatal – 0.4-1.0%
• Prevention StrategiesPrevention Strategies– LDUH (5,000 U q LDUH (5,000 U q 8 hours8 hours))– LMWH ( > 3,400 U daily)LMWH ( > 3,400 U daily)– Grade 1AGrade 1A

General SurgeryGeneral Surgery• Highest RiskHighest Risk
– Surgery in patients with multiple risk factorsSurgery in patients with multiple risk factors
• RiskRisk– DVT Calf – 40-80%DVT Calf – 40-80% Proximal – 10-20%Proximal – 10-20%– PE Clinical – 4-10%PE Clinical – 4-10% Fatal - 0.2 - 5%Fatal - 0.2 - 5%
• Prevention StrategiesPrevention Strategies– LDUH ( 5,000 q 8 hours)LDUH ( 5,000 q 8 hours)
oror– LMWH ( > 3,400 U daily)LMWH ( > 3,400 U daily)
withwith– GCS and/or IPCGCS and/or IPC
Grade 1C+Grade 1C+

General SurgeryGeneral Surgery
• Special ConsiderationsSpecial Considerations– High Risk of bleedingHigh Risk of bleeding
• Properly fitted GCS and/or IPC Properly fitted GCS and/or IPC (Grade 1A)(Grade 1A)
– Major Cancer SurgeryMajor Cancer Surgery• Post hospital discharge prophylaxis with Post hospital discharge prophylaxis with
LMWH for 2-3 weeks LMWH for 2-3 weeks (Grade 2A)(Grade 2A)
Prolonged prophylaxis in abdominal and pelvic cancer Prolonged prophylaxis in abdominal and pelvic cancer reduced DVT 12 to 5%reduced DVT 12 to 5%
Bergqvist NEJM 2002Bergqvist NEJM 2002

Vascular SurgeryVascular Surgery• RiskRisk
– Aortic Surgery - DVT – 0.9 - 12 %Aortic Surgery - DVT – 0.9 - 12 % No prophylaxis – 41%No prophylaxis – 41%– Femorodistal – DVT – 0.7 – 9%Femorodistal – DVT – 0.7 – 9% No prophylaxis – No prophylaxis –
18%18%• RPCT – 4 – Heparin during the procedure in allRPCT – 4 – Heparin during the procedure in all
– 1 - 49 patients – ABF – Belch Thromb Haemost 19791 - 49 patients – ABF – Belch Thromb Haemost 1979• LDUH 5000 U BID 4% DVT v placebo 24% DVTLDUH 5000 U BID 4% DVT v placebo 24% DVT• Stopped early due to significantly greater clinical bleedingStopped early due to significantly greater clinical bleeding
– 2 – 43 patients – Spebar Am J Surg 19812 – 43 patients – Spebar Am J Surg 1981• No Benefit LDUH v no prophylaxisNo Benefit LDUH v no prophylaxis
– 3 - 100 patients – Aortic Surgery –Killewich Arch Surg 19973 - 100 patients – Aortic Surgery –Killewich Arch Surg 1997• LDUH plus GCS v no prophylaxis - No difference in DVTLDUH plus GCS v no prophylaxis - No difference in DVT
– 4 – 233 patients – Aorta/Infraing. – Farkas Eur J Vas Surg 19934 – 233 patients – Aorta/Infraing. – Farkas Eur J Vas Surg 1993• LDUH 7500 Units BID v enoxaparin 40 mg daily for < 2 daysLDUH 7500 Units BID v enoxaparin 40 mg daily for < 2 days• No difference in DVT, major bleeding 2% in both groupsNo difference in DVT, major bleeding 2% in both groups
• Prevention StrategiesPrevention Strategies– No routine prophylaxis in patients without risk factors No routine prophylaxis in patients without risk factors (Grade 2B)(Grade 2B)– LDUH or LMWH in patients with risk factors LDUH or LMWH in patients with risk factors (Grade 1C+)(Grade 1C+)

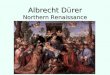
Laparoscopic SurgeryLaparoscopic Surgery• Laparoscopic CholecystectomyLaparoscopic Cholecystectomy
– J Soc Laparosc Surg 2001J Soc Laparosc Surg 2001• 587 patients587 patients• 3% received thromboprophylaxis3% received thromboprophylaxis• No DVT or PENo DVT or PE
– Surg Laparosc Endosc 1997Surg Laparosc Endosc 1997• 153,832 patients153,832 patients• Various thromboprophylaxis techniquesVarious thromboprophylaxis techniques• Clinical DVT – 0.03%Clinical DVT – 0.03% PE - 0.06% PE - 0.06% Fatal PE – 0.02%Fatal PE – 0.02%
• GI laparoscopy GI laparoscopy Surg Laparosc Endosc Precutan Tech 1999Surg Laparosc Endosc Precutan Tech 1999 – 2,384 patients2,384 patients– LMWHLMWH– DVT – 0.3%DVT – 0.3% PE - NonePE - None

Prospective Trials DVT following LaparoscopyProspective Trials DVT following Laparoscopy

Recommendations in LaparoscopyRecommendations in Laparoscopy
• European Association for Endoscopic SurgeryEuropean Association for Endoscopic Surgery– Intraoperative IPC for all prolonged laparoscopic Intraoperative IPC for all prolonged laparoscopic
proceduresprocedures
• SAGESSAGES– Same thromboprophylaxis options with laparoscopic Same thromboprophylaxis options with laparoscopic
procedures as for the equivalent open surgical procedures as for the equivalent open surgical proceduresprocedures
• ACCPACCP– No risk factors – aggressive early mobilization No risk factors – aggressive early mobilization (G1A)(G1A)– With risk factors – LDUH, LMWH, IPC or GCS With risk factors – LDUH, LMWH, IPC or GCS (G1C+)(G1C+)

Major TraumaMajor Trauma• Highest Risk of all Hospitalized PatientsHighest Risk of all Hospitalized Patients• Risk – without Rx exceeds 50%Risk – without Rx exceeds 50%
– DVT Calf – 40-80%DVT Calf – 40-80% Proximal – 10-20%Proximal – 10-20%– PE Clinical – 4-10%PE Clinical – 4-10% Fatal - 0.2 - 5%Fatal - 0.2 - 5%
• Risk with routine thromboprophylaxisRisk with routine thromboprophylaxis– DVT Calf – 27%DVT Calf – 27% Proximal – 7%Proximal – 7%
• Increased Risk FactorsIncreased Risk Factors– Spinal Cord injury, lower extremity or pelvic Fx, need Spinal Cord injury, lower extremity or pelvic Fx, need
for surgery, increasing age, for surgery, increasing age, femoral venous linefemoral venous line insertion or major venous repair, prolonged insertion or major venous repair, prolonged immobility, prolonged ventilatory support and longer immobility, prolonged ventilatory support and longer duration of hospital stay, +/- ISSduration of hospital stay, +/- ISS

Trauma Prophylaxis Trials

Compression DevicesCompression Devicesin Trauma Patientsin Trauma Patients
• Meta-analysis IPCMeta-analysis IPC– No RRR with IPC v. no prophylaxisNo RRR with IPC v. no prophylaxis– Problems with useProblems with use
• 1/3 unable to use1/3 unable to use– Fractures, casts, dressing, poor complianceFractures, casts, dressing, poor compliance
• Foot PumpsFoot Pumps– RCT – DVT was 3x higher that with IPCRCT – DVT was 3x higher that with IPC– Cohort Study – DVT rate 57%Cohort Study – DVT rate 57%

LDUH v. LWMH in Trauma PatientsLDUH v. LWMH in Trauma Patients
• Double blind, RCT Double blind, RCT (Geerts NEJM 1996)(Geerts NEJM 1996)
– 344 major trauma without ICH344 major trauma without ICH– 11stst dose within 36 hours of injury dose within 36 hours of injury – No mechanical prophylaxisNo mechanical prophylaxis– 5000 U LDUH v. 30 mg enoxaparin BID5000 U LDUH v. 30 mg enoxaparin BID– RRR DVT 30% and pDVT 58% for LMWHRRR DVT 30% and pDVT 58% for LMWH– No significant difference in bleeding, No significant difference in bleeding,
transfusions or hematocrit changestransfusions or hematocrit changes
• Cost effective analyses favors LMWH Cost effective analyses favors LMWH (Shorr, CCM 2001)(Shorr, CCM 2001)

Trauma RecommendationsTrauma Recommendations
• All patients with at least one risk factor receive All patients with at least one risk factor receive thromboprophylaxis (G1A)thromboprophylaxis (G1A)
• LMWH as soon as considered ‘safe’ (G1A)LMWH as soon as considered ‘safe’ (G1A)• If LMWH delayed – IPC (G1B)If LMWH delayed – IPC (G1B)• Continued thromboprophylaxis until mobility Continued thromboprophylaxis until mobility
adequate with LMSH or VKA (G2C)adequate with LMSH or VKA (G2C)• Duplex ultrasound screening – high risk and Duplex ultrasound screening – high risk and
suboptimal prophylaxis or no prophylaxis (G1C)suboptimal prophylaxis or no prophylaxis (G1C)

OUMC Trauma Protocol• Trauma DVT Prophylaxix – Trauma DVT Prophylaxix –
Enoxaparin CriteriaEnoxaparin Criteria• Enoxaparin 30 mg sq q12hEnoxaparin 30 mg sq q12h• - start between 24-36 hours after - start between 24-36 hours after
admissionadmission• after HCT stableafter HCT stable• for patients requiring DVT for patients requiring DVT
prophylaxisprophylaxis• if pt. Is immobile or projected to be if pt. Is immobile or projected to be
immobile for > 24 hrsimmobile for > 24 hrs• - femur, tibia, fibula fractures- femur, tibia, fibula fractures• - any pelvic fracture- any pelvic fracture• - facial or abdominal or chest - facial or abdominal or chest
trauma on a ventilatortrauma on a ventilator• - vascular repair- vascular repair• - spinal cord injuries- spinal cord injuries
• Hold drug for:Hold drug for:• - subdural hematoma- subdural hematoma• - epidural hematoma- epidural hematoma• - focal intracranial hemorrhage- focal intracranial hemorrhage• - intraventricular hemorrhage- intraventricular hemorrhage• - subarachnoid hemorrhage- subarachnoid hemorrhage• - ocular hemorrhage- ocular hemorrhage• - systemic coagulopathy- systemic coagulopathy• - PTT > 40 sec or INR > 1.5- PTT > 40 sec or INR > 1.5• - Platelets < 70,000- Platelets < 70,000• - or a platelet decrease by 50% - or a platelet decrease by 50%
or platelets < 70,000or platelets < 70,000• after enoxaparin startedafter enoxaparin started• - unexplained drop in HCT > 5%- unexplained drop in HCT > 5%• - signs of active hemorrhage- signs of active hemorrhage• - hypersensitivity reaction to - hypersensitivity reaction to
medicationmedication• - serum creatinine of > 3- serum creatinine of > 3• - if pt is going to OR hold morning - if pt is going to OR hold morning
dosedose• - resume 12 hrs post operative- resume 12 hrs post operative• Discontinue enoxaparin:Discontinue enoxaparin:• - If pt is fully ambulatory- If pt is fully ambulatory

Spinal Cord InjurySpinal Cord Injury• Highest RiskHighest Risk• RiskRisk
– DVT Calf – 40-80%DVT Calf – 40-80% Proximal – 10-20%Proximal – 10-20%– PE Clinical – 4-10%PE Clinical – 4-10% Fatal - 0.2 - 5%Fatal - 0.2 - 5%
• Prevention StrategiesPrevention Strategies– Small RCT’s – LDUH and IPC – ineffectiveSmall RCT’s – LDUH and IPC – ineffective– Multicenter trial Multicenter trial (Spinal Cord Injury Thromboprophylaxis (Spinal Cord Injury Thromboprophylaxis
Investigators J Trauma 2003)Investigators J Trauma 2003)• 107 patients acute phase, 72 hours of injury, no diff UFH v. LMWH107 patients acute phase, 72 hours of injury, no diff UFH v. LMWH• 476 patients in rehab, C2- T12476 patients in rehab, C2- T12• LDUH 5000 U TID/IPC v. enoxaparin 30mg BIDLDUH 5000 U TID/IPC v. enoxaparin 30mg BID• Major VTE 16% v. 12%, no fatal PE and equal bleeding ratesMajor VTE 16% v. 12%, no fatal PE and equal bleeding rates
– Uncontrolled studiesUncontrolled studies• Oral VKA – reduces symptomatic VTEOral VKA – reduces symptomatic VTE
– IVC Filter placementIVC Filter placement• Use has not been proven to decrease VTE/PEUse has not been proven to decrease VTE/PE

DVT after Spinal Cord InjuryDVT after Spinal Cord Injury

Acute Spinal Cord Injury VTE Acute Spinal Cord Injury VTE prophylaxis recommendationsprophylaxis recommendations
• Recommend Recommend againstagainst the use of LDUH, GCS or the use of LDUH, GCS or IPC as single agents IPC as single agents (G1A)(G1A)
• GCS and/or IPC when anticoagulation is GCS and/or IPC when anticoagulation is contraindicated early after injury contraindicated early after injury (G1C+)(G1C+)
• Prophylaxis with LMWH once primary Prophylaxis with LMWH once primary hemostasis is evident hemostasis is evident (G1B)(G1B)
• Combined use of IPC and LDUH Combined use of IPC and LDUH (G2B)(G2B) or or LMWH LMWH (G2C)(G2C) as alternative to above as alternative to above
• Continuation of LMWH or oral VKA during Continuation of LMWH or oral VKA during rehabilitation phase rehabilitation phase (G1C)(G1C)

NeurosurgeryNeurosurgery
• Risk FactorsRisk Factors– Intracranial surgery, active malignancy, length of Intracranial surgery, active malignancy, length of
procedure, presence of leg weakness and advance age.procedure, presence of leg weakness and advance age.– Highest risk - Malignant Brain TumorsHighest risk - Malignant Brain Tumors
• 31% symptomatic DVT31% symptomatic DVT
• IPC with or without GCS - Most commonIPC with or without GCS - Most common• Concern for intracranial/spinal bleedingConcern for intracranial/spinal bleeding• 68% relative risk reduction – lowering DVT from 22 to 7%68% relative risk reduction – lowering DVT from 22 to 7%
• HeparinHeparin– One RCT - LDUH v. no Rx – RRR of 82%One RCT - LDUH v. no Rx – RRR of 82%– 2 Studies – GCS v. GCS/LMWH postop2 Studies – GCS v. GCS/LMWH postop
• Control DVT/pDVT – 26/12%Control DVT/pDVT – 26/12% Rx 19/7%Rx 19/7%• Control DVT/pDVT – 33/13%Control DVT/pDVT – 33/13% Rx 17/5%Rx 17/5%

CraniotomyCraniotomy
• RCT – 100 patients - preopRCT – 100 patients - preop– IPC + LDUH 5000 BID or IPC + dalteparin 2500 dailyIPC + LDUH 5000 BID or IPC + dalteparin 2500 daily– Intracranial bleed equal 1/49 v 2/51Intracranial bleed equal 1/49 v 2/51– DVT rate equal – 0/49 v. 2 asymptomatic/51DVT rate equal – 0/49 v. 2 asymptomatic/51
• Pooled DataPooled Data– Intracranial hemorrhage in RCT’s Intracranial hemorrhage in RCT’s
• 2.1% for postoperative LMWH2.1% for postoperative LMWH• 1.1% for mechanical or no prophylaxis1.1% for mechanical or no prophylaxis
– Intracranial hemorrhage in meta-analysisIntracranial hemorrhage in meta-analysis• Bleeding with post operative LMWH – 6.1%Bleeding with post operative LMWH – 6.1%• Bleeding with mechanical prophylaxis – 3.0%Bleeding with mechanical prophylaxis – 3.0%

Traumatic Brain InjuryTraumatic Brain Injury
• Norwood Arch Surg 2002Norwood Arch Surg 2002– 150 patients with Blunt TBI150 patients with Blunt TBI– LMWH 24 hours after admissionLMWH 24 hours after admission– Marshall CT grade progression of ICHMarshall CT grade progression of ICH– 23% had CT progression – 19% before 23% had CT progression – 19% before
LMWH and 6% afterLMWH and 6% after– All with progression survived, none to ORAll with progression survived, none to OR– DVT rate 2%DVT rate 2%

Neurosurgery RecommendationsNeurosurgery Recommendations
• Major Elective Neurosurgery/Intracranial Major Elective Neurosurgery/Intracranial SurgerySurgery– IPC, with or without GCS (Grade 1A)IPC, with or without GCS (Grade 1A)– IPC, w or w/o GCS + LDUH (Grade 2B)IPC, w or w/o GCS + LDUH (Grade 2B)– IPC, w or w/o GCS + postoperative LMWH IPC, w or w/o GCS + postoperative LMWH
(G2A)(G2A)
• High Risk Neurosurgery PatientsHigh Risk Neurosurgery Patients– Mechanical + LDUH or LMWH (G2B)Mechanical + LDUH or LMWH (G2B)

Critical CareCritical Care
• Critical Ill patients have multiple risk Critical Ill patients have multiple risk factors for VTE, some predate factors for VTE, some predate admissionadmission
• ICU entry ICU entry – 990 patients with DUS at admit990 patients with DUS at admit– DVT rate 5.5%DVT rate 5.5%

DVT in Critical CareDVT in Critical Care
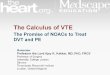
**
** Abstract onlyAbstract only

DVT in Critical Care PatientsDVT in Critical Care PatientsOnly 4 published RCT’s of Thromboprophylaxis in Critical CareOnly 4 published RCT’s of Thromboprophylaxis in Critical Care
**
**
* Abstract only* Abstract only
119 pt119 pt
223 pt223 pt
324 pt in 28 ICU’s324 pt in 28 ICU’s

Recommendations: Critical CareRecommendations: Critical Care
• Assess all patients risk for VTE at admit Assess all patients risk for VTE at admit (G1A)(G1A)– Moderate VTE risk – LDUH or LMWH Moderate VTE risk – LDUH or LMWH (G1A)(G1A)
• Medically ill or postoperativeMedically ill or postoperative
– High VTE risk – LMWH High VTE risk – LMWH (G1A)(G1A)• Major trauma, orthopaedic surgeryMajor trauma, orthopaedic surgery
• High bleeding risk patientsHigh bleeding risk patients– Mechanical Prophylaxis Mechanical Prophylaxis (G1C+)(G1C+)

New Antithrombotic AgentsNew Antithrombotic Agents• XimelagatranXimelagatran
– Oral direct thrombin inhibitorOral direct thrombin inhibitor– Rapid absorption and conversion to melagatranRapid absorption and conversion to melagatran– predictable pharmacokinetics, no food interactionspredictable pharmacokinetics, no food interactions
• Hip and knee replacement (Lancet 2002, phase II trial)Hip and knee replacement (Lancet 2002, phase II trial)• Melagatran 3mg BID/ximelagatran 24mg/d v dalteparin 5000 Melagatran 3mg BID/ximelagatran 24mg/d v dalteparin 5000
IU BIDIU BID• DVT 15.1 v 28.2%DVT 15.1 v 28.2%
• FondaparinuxFondaparinux– syntheticsynthetic pentasaccharides with selective inhibitor of pentasaccharides with selective inhibitor of
activated factor Xactivated factor X (NEJM 2001, Lancet 2002)(NEJM 2001, Lancet 2002)• RRR 56.4%/59.5% v. enoxaparin q day hip surgeryRRR 56.4%/59.5% v. enoxaparin q day hip surgery• RRR 22.6% v enoxaparin BIDRRR 22.6% v enoxaparin BID• RRR 12.5% in Knee sugery higher bleedingRRR 12.5% in Knee sugery higher bleeding
Both have better efficacy that LMWH for prophylaxis Both have better efficacy that LMWH for prophylaxis however cost effectiveness has not yet been provenhowever cost effectiveness has not yet been proven

ConclusionConclusion
• Most strategies include LMWHMost strategies include LMWH• Exception – Exception –
– high bleeding risk – GCS and IPS best optionhigh bleeding risk – GCS and IPS best option– Renal failure – monitorRenal failure – monitor– Obesity - monitorObesity - monitor
• Further researchFurther research– LaparoscopyLaparoscopy– VascularVascular– DurationDuration– Safety of LMWHSafety of LMWH
• NeurosurgeryNeurosurgery
– New antithrombotic agents in nonorthopedic groupsNew antithrombotic agents in nonorthopedic groups


Weight Based Heparin DosingWeight Based Heparin Dosing
• Unfractionated Heparin Unfractionated Heparin TreatmentTreatment of Venous of Venous ThromboembolismThromboembolism– Bolus – 80 Units/KgBolus – 80 Units/Kg– Infusion – 18 Units/Kg/hourInfusion – 18 Units/Kg/hour– MonitoringMonitoring
• Measure 6 hours after bolusMeasure 6 hours after bolus• Goal – Plasma heparin concentration of 0.3 IU/mL (by Goal – Plasma heparin concentration of 0.3 IU/mL (by
factor Xa inhibition – anti factor-Xa units)factor Xa inhibition – anti factor-Xa units)• aPTT levels vary due to reagents and methods of clot aPTT levels vary due to reagents and methods of clot
detection and are inaccurate measures of heparin levelsdetection and are inaccurate measures of heparin levels
– CAP and ACCP recommendationCAP and ACCP recommendation• Therapeutic aPTT range calibrated with heparin levels Therapeutic aPTT range calibrated with heparin levels
equivalent to 0.3 – 0.7 IU/mL by factor Xa inhibitionequivalent to 0.3 – 0.7 IU/mL by factor Xa inhibition

Vitamin K antagonistsVitamin K antagonists• Initiation of Oral DoseInitiation of Oral Dose
– 5-10 mg for first 1-2 days – most patients5-10 mg for first 1-2 days – most patients– < 5 mg for first days – elderly/elevated bleeding risk/liver < 5 mg for first days – elderly/elevated bleeding risk/liver
disease/CHF/malnutritiondisease/CHF/malnutrition
• GoalGoal– INR 2.0-3.0INR 2.0-3.0
• MonitoringMonitoring– Initiation – daily, 2-3 X/wk for 1-2 weeks, when stable 1X/4 weeksInitiation – daily, 2-3 X/wk for 1-2 weeks, when stable 1X/4 weeks
• ReversalReversal– Elevated INRElevated INR
• Hold dose v. Oral Vitamin K (1 – 2.5 mg)Hold dose v. Oral Vitamin K (1 – 2.5 mg)
– Elective SurgeryElective Surgery• Hold for 4 daysHold for 4 days• Hold for 4 days and initiate UFH or LMWHHold for 4 days and initiate UFH or LMWH
– Serious/Life threatening BleedingSerious/Life threatening Bleeding• Vitamin K – IV, FFP, protamine, recombinant Factor VIIaVitamin K – IV, FFP, protamine, recombinant Factor VIIa

Hip or Knee ArthroplastyHip or Knee Arthroplasty
• Highest RiskHighest Risk• RiskRisk
– DVT Calf – 40-80%DVT Calf – 40-80% Proximal – 10-20%Proximal – 10-20%– PE Clinical – 4-10%PE Clinical – 4-10% Fatal - 0.2 - 5%Fatal - 0.2 - 5%
• Prevention StrategiesPrevention Strategies– LMWH ( >3,400 U daily) start before or LMWH ( >3,400 U daily) start before or
within 24 hours of surgerywithin 24 hours of surgery– Oral VKA (INR 2-3) preoperative or evening Oral VKA (INR 2-3) preoperative or evening
after surgeryafter surgery