Embed Size (px)
Citation preview
CLINICAL CASE REPORTNeil E. Strickman, MD and Federico E. Azpurua-Gil, MD Texas Heart Institute / St. Luke’s Hospital, Houston Texas
VascuTrak® PTA Dilatation Catheter and Crosser® CTO Recanalization Catheter Successfully Relieved CTO of the Anterior Tibial Artery
V����T���®
PTA Dilatation Catheter
OverviewThis patient is a 47-year-old Hispanic male with a medical history including end-stage renal disease on dialysis, diabetes mellitus, hypertension, coronary artery disease, peripheral arterial disease and a below the knee amputation (BKA) years earlier. Previously, he had undergone PTA/stenting of the left popliteal artery with a self-expanding nitinol stent but the exact date remains unclear. He was admitted to the hospital with left leg critical limb ischemia (CLI), osteomyelitis and a non-healing ulcer of that foot.
On physical examination, he had palpable left femoral and popliteal pulses but no palpable pedal pulses. A large ischemic ulcer was present in the lateral plantar surface of the foot with necrotic tissue.
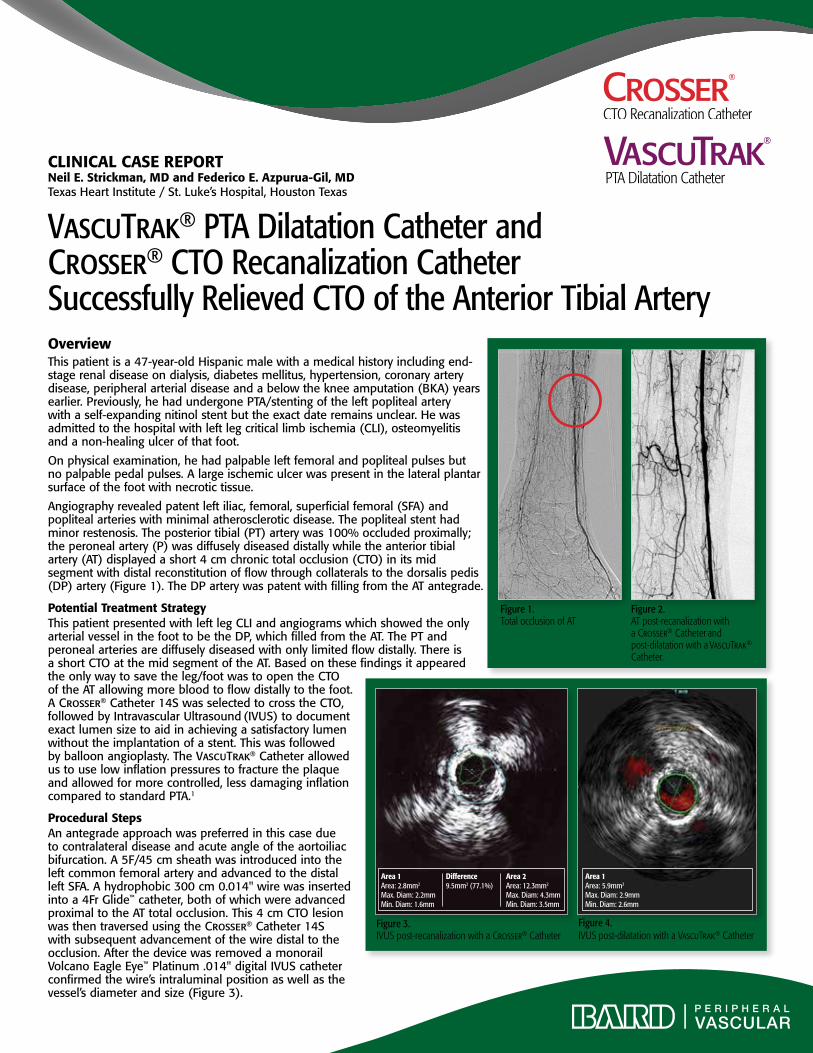
Angiography revealed patent left iliac, femoral, superficial femoral (SFA) and popliteal arteries with minimal atherosclerotic disease. The popliteal stent had minor restenosis. The posterior tibial (PT) artery was 100% occluded proximally; the peroneal artery (P) was diffusely diseased distally while the anterior tibial artery (AT) displayed a short 4 cm chronic total occlusion (CTO) in its mid segment with distal reconstitution of flow through collaterals to the dorsalis pedis (DP) artery (Figure 1). The DP artery was patent with filling from the AT antegrade.
Potential Treatment StrategyThis patient presented with left leg CLI and angiograms which showed the only arterial vessel in the foot to be the DP, which filled from the AT. The PT and peroneal arteries are diffusely diseased with only limited flow distally. There is a short CTO at the mid segment of the AT. Based on these findings it appeared the only way to save the leg/foot was to open the CTO of the AT allowing more blood to flow distally to the foot. A Crosser® Catheter 14S was selected to cross the CTO, followed by Intravascular Ultrasound (IVUS) to document exact lumen size to aid in achieving a satisfactory lumen without the implantation of a stent. This was followed by balloon angioplasty. The VascuTrak® Catheter allowed us to use low inflation pressures to fracture the plaque and allowed for more controlled, less damaging inflation compared to standard PTA.1
Procedural StepsAn antegrade approach was preferred in this case due to contralateral disease and acute angle of the aortoiliac bifurcation. A 5F/45 cm sheath was introduced into the left common femoral artery and advanced to the distal left SFA. A hydrophobic 300 cm 0.014" wire was inserted into a 4Fr Glide™ catheter, both of which were advanced proximal to the AT total occlusion. This 4 cm CTO lesion was then traversed using the Crosser® Catheter 14S with subsequent advancement of the wire distal to the occlusion. After the device was removed a monorail Volcano Eagle Eye™ Platinum .014" digital IVUS catheter confirmed the wire’s intraluminal position as well as the vessel’s diameter and size (Figure 3).
Figure 2. AT post-recanalization with a Crosser® Catheter and post-dilatation with a VascuTrak® Catheter.
Figure 1. Total occlusion of AT
Area 1Area: 2.8mm2
Max. Diam: 2.2mmMin. Diam: 1.6mm
Difference9.5mm2 (77.1%)
Area 2Area: 12.3mm2
Max. Diam: 4.3mmMin. Diam: 3.5mm
Area 1Area: 5.9mm2
Max. Diam: 2.9mmMin. Diam: 2.6mm
Figure 3. IVUS post-recanalization with a Crosser® Catheter
Figure 4. IVUS post-dilatation with a VascuTrak® Catheter

VascuTrak® PTA Dilatation Catheter
Indications for Use: The VascuTrak® PTA Dilatation Catheter is intended to dilate stenoses in the iliac, femoral, ilio-femoral, popliteal, infra-popliteal and renal arteries and for the treatment of obstructive lesions of native or synthetic arterioveneous dialysis fistulae. This device is also recommended for post dilatation of balloon expandable stents, self-expanding stents, and stent grafts in the peripheral vasculature.
Contraindications: The VascuTrak® PTA Dilatation Catheter is contraindicated: 1) where there is the inability to cross the target lesion with a guidewire; 2) for use in the coronary or neuro vasculature.
Warnings: 1) Contents supplied sterile using ethylene oxide (EO). Non-pyrogenic. Do not use if sterile barrier is opened or damaged. Do not reuse, reprocess or re-sterilize. Use the catheter prior to the “Use By” date specified on the package label. 2) This device has been designed for single use only. Reusing this medical device bears the risk of cross-patient contamination as medical devices – particularly those with long and small lumina, joints and/or crevices between components – are difficult or impossible to clean once body fluids or tissues with potential pyrogenic or microbial contamination have had contact with the medical device for an indeterminable period of time. The residue of biological material can promote the contamination of the device with pyrogens or microorganisms, which may lead to infectious complications. 3) Do not resterilize. After resterilization, the sterility of the product is not guaranteed because of an indeterminable degree of potential pyrogenic or microbial contamination, which may lead to infectious complications. Cleaning, reprocessing and/or resterilization of the present medical device increases the probability that the device will malfunction due to potential adverse effects on components that are influenced by thermal and/or mechanical changes. 4) To reduce the potential for vessel damage, the inflated diameter and length of the balloon should approximate the diameter and length of the vessel just proximal and distal to the stenosis. 5) When the catheter is exposed to the vascular system, it should be manipulated while under high-quality fluoroscopic observation. Do not advance or retract the catheter unless the balloon is fully deflated. If resistance is met during manipulation, determine the cause of the resistance before proceeding. Applying excessive force to the catheter can result in tip breakage or balloon
separation. 6) Do not exceed the RBP recommended for this device. Balloon rupture may occur if the RBP rating is exceeded. To prevent over-pressurization, use of a pressure monitoring device is recommended. 7) After use, this product may be a potential biohazard. Handle and dispose of in accordance with acceptable medical practices and applicable local, state and federal laws and regulations.
Precautions: 1) Carefully inspect the catheter prior to use to verify that catheter has not been damaged during shipment and that its size, shape and condition are suitable for the procedure for which it is to be used. Do not use if product damage is evident. 2) The VascuTrak® PTA Dilatation Catheter should only be used by physicians trained in the performance of percutaneous transluminal angioplasty. 3) In order to activate the hydrophilic coating, wet the VascuTrak® balloon and catheter with sterile saline or wipe the balloon catheter with sterile saline saturated gauze immediately prior to its insertion in the body. Do not wipe the balloon catheter with dry gauze. 4) When backloading the catheter onto the guidewire, support the catheter and ensure that the guidewire tip does not snag or come into contact with the balloon. 5) The minimal acceptable sheath French size is printed on the package label. Do not attempt to pass the PTA catheter through a smaller size introducer sheath than indicated on the label. 6) Use the recommended balloon inflation medium (50% contrast medium/50% sterile saline solution). It has been shown that a 25/75% contrast/saline ratio has yielded faster balloon inflation/deflation times. Never use air or other gaseous medium to inflate the balloon. 7) VascuTrak® PTA Dilatation Catheters should be used with caution for procedures involving calcified lesions or synthetic vascular grafts due to the abrasive nature of these lesions. 8) Never attempt to move the guidewire when the balloon is inflated. 9) Fully evacuate the balloon prior to withdrawing the system. Larger sizes of VascuTrak® balloons may exhibit slower deflation times. If the balloon does not deflate, advance a sheath or catheter over the proximal portion of the balloon to straighten out the transition from connection of the balloon to the inflation lumen. 10) If resistance is felt during post-procedure withdrawal of the catheter through the introducer sheath, determine if contrast medium is trapped in the balloon with fluoroscopy. If contrast is present, push the balloon out of the sheath and then completely evacuate the contrast before proceeding to withdraw the balloon. 11) If resistance is still felt during post-procedure withdrawal of the catheter, it is recommended to remove the balloon catheter and guidewire/ introducer sheath as
a single unit. 12) Do not continue to use the balloon catheter if the shaft has been bent or kinked. 13) Prior to re-insertion through the introducer sheath, re-activate the hydrophilic coating and clean the balloon catheter by wiping the balloon catheter with sterile saline saturated gauze and rinsing with sterile saline. Do not wipe the balloon catheter with dry gauze.
Potential Adverse Reactions: The complications that may result from a peripheral balloon dilatation procedure include: • Additional intervention • Allergic reaction to drugs or contrast medium • Aneurysm or pseudoaneurysm • Arrhythmias • Embolization • Hematoma • Hemorrhage, including bleeding at the puncture site • Hypotension/hypertension • Inflammation • Occlusion • Pain or tenderness • Pneumothorax or hemothorax • Sepsis/infection • Shock • Short-term hemodynamic deterioration • Stroke • Thrombosis • Vessel dissection, perforation, rupture or spasm.
Please consult product labels and package inserts for indications, contraindications, hazards, warnings, cautions, and information for use. The opinions and clinical experiences presented herein are for informational purposes only. The results from this case study may not be predictive for all patients. Individual results may vary depending on a variety of patient specific attributes. The physician has been compensated by Bard Peripheral Vascular, Inc. for the time and effort in preparing the above case study for Bard’s further use and distribution.
Bard, Crosser and VascuTrak are trademarks and/or registered trademarks of C. R. Bard, Inc. All other trademakes are the property of their respective owners. Copyright ® 2012, C. R. Bard, Inc. All Rights Reserved.
S120201 Rev 0
Bard Peripheral Vascular, Inc.1625 W. 3rd Street Tempe, AZ 85281 USA
Tel: 1 480 894 9515 / 1 800 321 4254Fax: 1 480 966 7062 / 1 800 440 5376
www.bardpv.com
After removal of the IVUS catheter, a 3.5 mm x 40 mm VascuTrak® Catheter was advanced into the AT and inflated gradually over 2 minutes to 6 atmospheres at the site of occlusion. The balloon was held at 6 atmospheres for 4 minutes and then deflated and removed. Post interventional IVUS and angiographic results showed no significant residual stenosis or dissection (Figures 2 and 4).
Keys to Success• TheuseoftheCrosser® Catheter and VascuTrak® Catheter in
this location provides an alternate approach to stenting, which has not been shown to have long-term benefits regarding continued patency.
• GradualinflationoftheVascuTrak® Catheter has continued to yield excellent results with respect to flow-limiting dissection occurrence.
• TheVascuTrak® Catheter minimized the expansion of the vessel. This can reduce elastic recoil and injury to the vessel and result in greater luminal gain.1
Discussion of Interventional ReportThis patient had a CTO of the AT in the setting of CLI with the AT being the only remaining vessel supplying the viable foot. With use of the Crosser® CTO Catheter, the anterior tibial arterial CTO was crossed without any significant difficulties of remaining intraluminal. Subsequently, a single, slow and prolonged inflation with an appropriately sized VascuTrak® Catheter created a wide lumen without dissection or perforations, improving distal perfusion without the need for stenting. IVUS imaging was useful in selecting size and length of the balloon, which is paramount to avoid dissections or perforations.
ConclusionWhen faced with opening the only vessel remaining to an actively ischemic leg/foot, one needs to use the tools and equipment readily available. Appropriate usage of the Crosser®
CTO Catheter and VascuTrak® Catheter can help address difficult revascularization needs.
References1. Based on Finite Element Analysis. Data on file.
The crosser® CTO Recanalization CatheterIndications: The Crosser® Recanalization System is indicated to facilitate the intra-luminal placement of conventional guidewires beyond peripheral artery chronic total occlusions via atherectomy. The Crosser® Catheter is only intended for use with the Crosser® Generator. Refer to the Crosser® Generator Manual of Operations for proper use.
Contraindications: The device is contraindicated for use in carotid arteries.
Warnings and Precautions• The Crosser® Recanalization System should only be used by individuals trained
in percutaneous transluminal angioplasty (PTA or PTCA).
• Prior to use, the packaging and product should be inspected for signs of damage. Never use damaged product or product from a damaged package.
• DO NOT activate the Crosser® Recanalization System without proper irrigation. Make sure to establish proper irrigation prior to introduction into guide catheter. Always use REFRIGERATED SALINE.
• The Crosser® Recanalization System should be used in conjunction with proper anticoagulation agents.
• Never advance or withdraw the Crosser® Catheter without proper fluoroscopic guidance.
• It is not recommended to use the Crosser® Catheter over wires which have polymer-jacketed distal ends.
• Do not exceed 5 minutes of activation time as Crosser® Catheter malfunction may occur. If 5 minutes of activation time is achieved exchange for a second Crosser® Catheter before resetting the Crosser® Generator.
• When using the Crosser® Catheter 14S or 14P with the MicroSheath® XL Support Catheter Tapered, the Crosser® Catheter can be advanced approximately 15 cm from the tip before resistance is encountered due to the taper on the Crosser® Catheter aligning with the taper on the support catheter. A femoral marker is located 120cm from the distal tip of the Crosser® Catheter. The femoral marker can be used as an indicator that the tapers on the catheters are nearing alignment; advance the Crosser® Catheter slowly. Do not continue to advance the Crosser® Catheter if resistance is encountered. Refer to the table below for each specific support catheter, the Crosser® Catheter that it is used with, and how far the Crosser® Catheter can be advanced before resistance occurs.
• When manipulating the Crosser® Catheter, the Catheter shaft may become warm to the touch. A warm feeling is normal, however, if the Catheter shaft becomes hot discontinue use immediately and withdraw from patient. Once removed from the patient confirm that irrigation is flowing.
• When using the Crosser® Catheter in tortuous anatomy, the use of a support catheter is recommended to prevent kinking or prolapse of the Crosser® Catheter tip. Kinking or prolapse of the tip could cause catheter breakage and/or malfunction.
• Position Foot Switch and cable to minimize potential tripping hazard.
• Ensure Crosser® Generator is securely mounted to IV pole to reduce risk of falling.
• Should high frequency vibration fail to stop when foot switch is released, power off Crosser® Generator or unplug from power receptacle.
• Never activate the Crosser® Generator without a Crosser® Catheter attached to the Transducer.
• The Crosser® Catheter is designed and intended for single patient use only. DO NOT resterilize and/or reuse it.
Adverse Effects: As with most percutaneous interventions, potential adverse effects include: Bleeding which may require transfusion or surgical intervention • Hematoma • Perforation • Dissection • Guidewire entrapment and/or fracture • Hypertension / Hypotension • Infection or fever • Allergic reaction • Pseudoaneurysm or fistula Aneurysm • Acute reclosure • Thrombosis • Ischemic events • Distal embolization • Excessive contrast load resulting in renal insufficiency or failure • Excessive exposure to radiation • Stroke/CVA • Restenosis • Repeat catheterization / angioplasty • Peripheral artery bypass • Amputation • Death or other bleeding complications at access site.
Please consult product labels and package inserts for indications, contraindications, hazards, warnings, cautions and instructions for use.
V����T���®
PTA Dilatation Catheter
V����T���®
PTA Dilatation Catheter
Scan with a Smart Phone and your local Bard Rep will contact you.









![, VT[5] LIVE! and VT[5] LIVE SDI! VT[5] VT[5]LIVE] VT[5 ... · Virtual Studios SDI switcher HD/SD Editing VT[5] ... FEATURES Live video mixer ... Dual-channel upstream Effects bus](https://img.pdfslide.us/doc/110x75/5b0b5ac27f8b9ae61b8da9b2/-vt5-live-and-vt5-live-sdi-vt5-vt5live-vt5-studios-sdi-switcher.jpg)



















