Embed Size (px)
Citation preview

VOYAGER PAD trial
RCT investigating efficacy and safety of rivaroxaban to reduce the risk of
major thrombotic vascular events in patients with symptomatic PAOD
undergoing revascularization – the concept of an event driven trial
Rupert M. Bauersachs Dept. of Vascular Medicine
CTH – Professorship for
Vulnerable Individuals and
Populations (VIP)
Disclosures
Rupert M. Bauersachs
• Research Support / Principal Investigator:
– Bayer, BMS, Boehringer Ingelheim, Daiichi-Sankyo, Leo, Pfizer, Portola
• Consultant & Speakers Bureau:
– Bayer, BMS, Boehringer Ingelheim, Daiichi-Sankyo, Pfizer
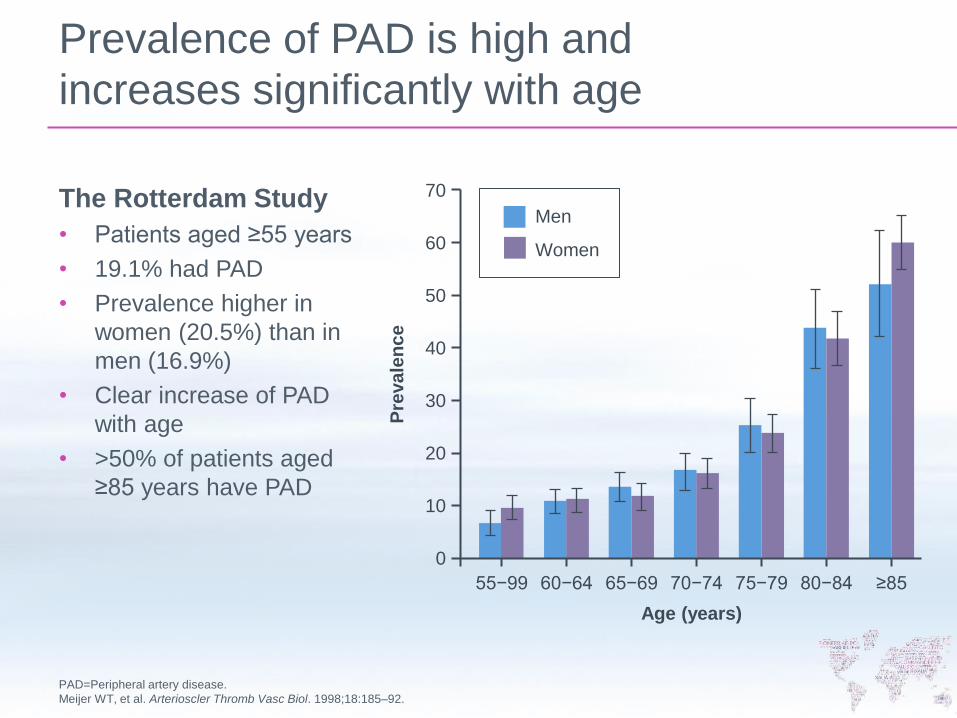
Prevalence of PAD is high and
increases significantly with age
The Rotterdam Study
• Patients aged ≥55 years
• 19.1% had PAD
• Prevalence higher in
women (20.5%) than in
men (16.9%)
• Clear increase of PAD
with age
• >50% of patients aged
≥85 years have PAD
PAD=Peripheral artery disease.
Meijer WT, et al. Arterioscler Thromb Vasc Biol. 1998;18:185–92.
55−99 60−64 65−69 70−74 75−79 80−84 ≥85
Age (years)
Pre
va
len
ce
70
60
50
40
30
20
10
0
Men
Women
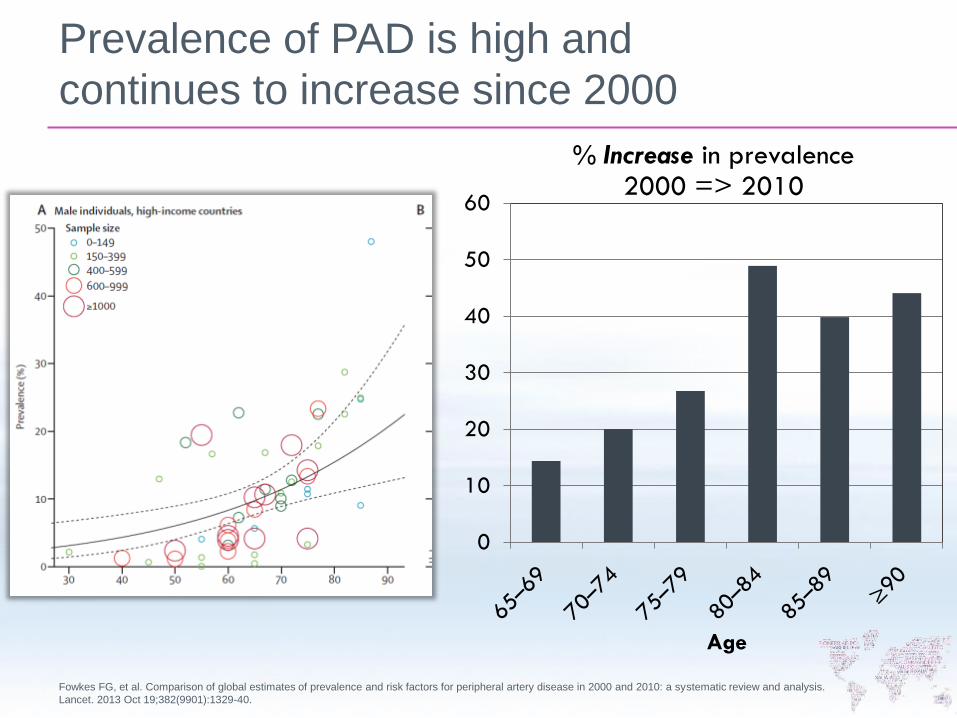
Prevalence of PAD is high and
continues to increase since 2000
Fowkes FG, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis.
Lancet. 2013 Oct 19;382(9901):1329-40.
0
10
20
30
40
50
60
Age
% Increase in prevalence 2000 => 2010
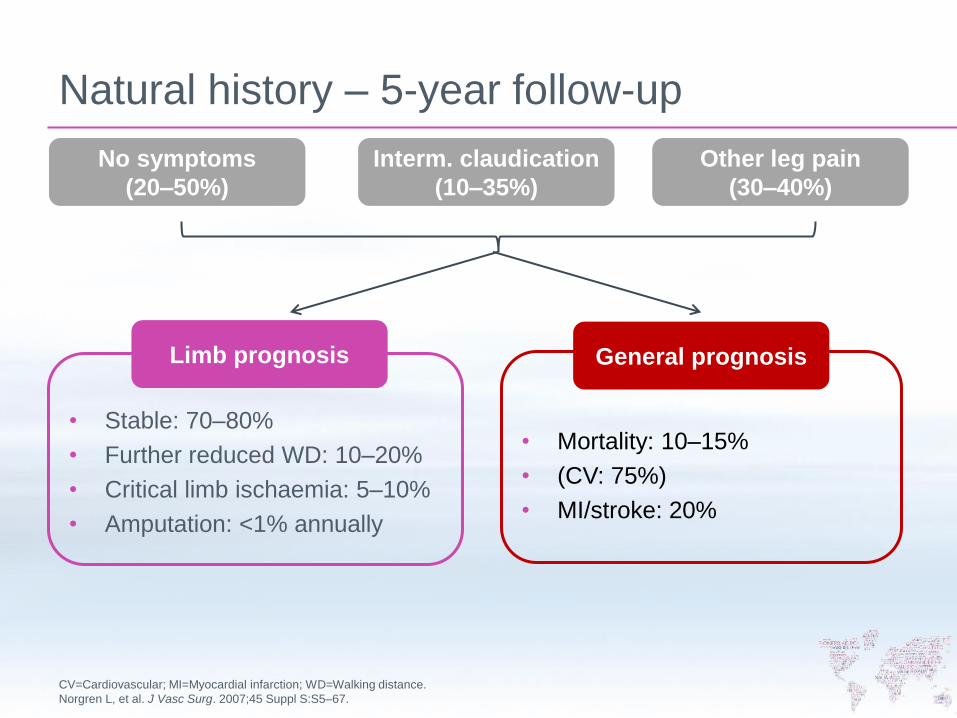
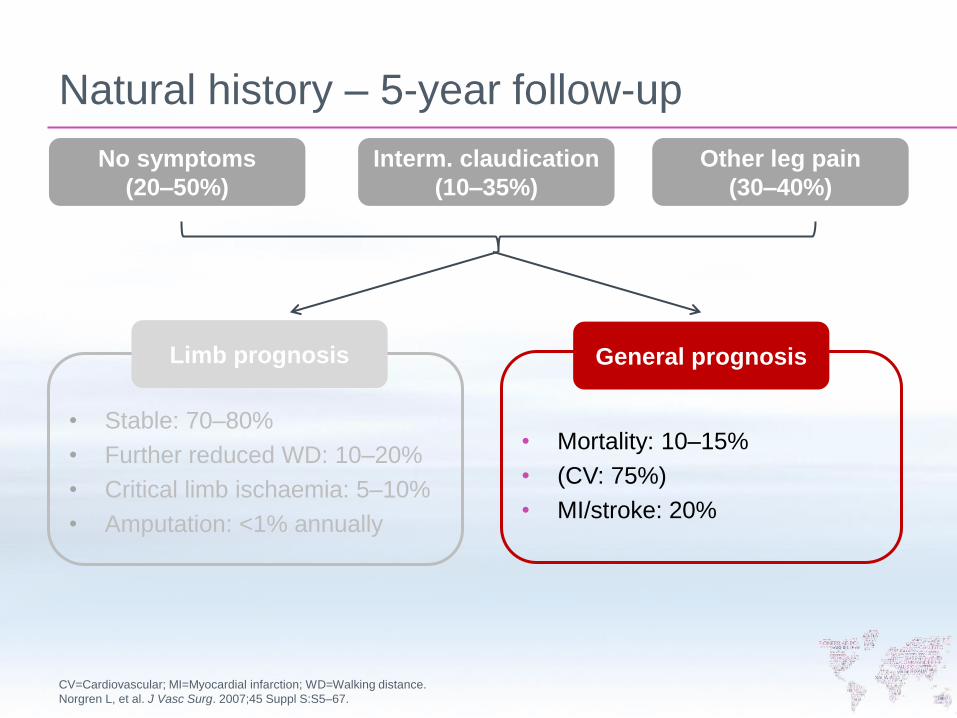
Natural history – 5-year follow-up
CV=Cardiovascular; MI=Myocardial infarction; WD=Walking distance.
Norgren L, et al. J Vasc Surg. 2007;45 Suppl S:S5–67.
No symptoms
(20–50%)
Interm. claudication
(10–35%)
Other leg pain
(30–40%)
• Stable: 70–80%
• Further reduced WD: 10–20%
• Critical limb ischaemia: 5–10%
• Amputation: <1% annually
Limb prognosis
• Mortality: 10–15%
• (CV: 75%)
• MI/stroke: 20%
General prognosis

CAD and PAD: Overlapping conditions
The REACH registry showed
3 out of 5 patients with PAD
also have CAD and/or CVD
8322 patients had PAD
• ~39% had PAD only
• ~38% had PAD and CAD
• ~10% had PAD and CVD
• ~13% PAD, CAD and CVD
CAD=Coronary artery disease; CVD=Cerebrovascular disease; PAD=Peripheral artery disease.
Cacoub PP, et al. Atherosclerosis. 2009;204:e86–92.
Patients
with
CAD
Patients
with CVD
2 to 3- fold
risk of
stroke
4-fold risk
of fatal MI Patients
with PAD
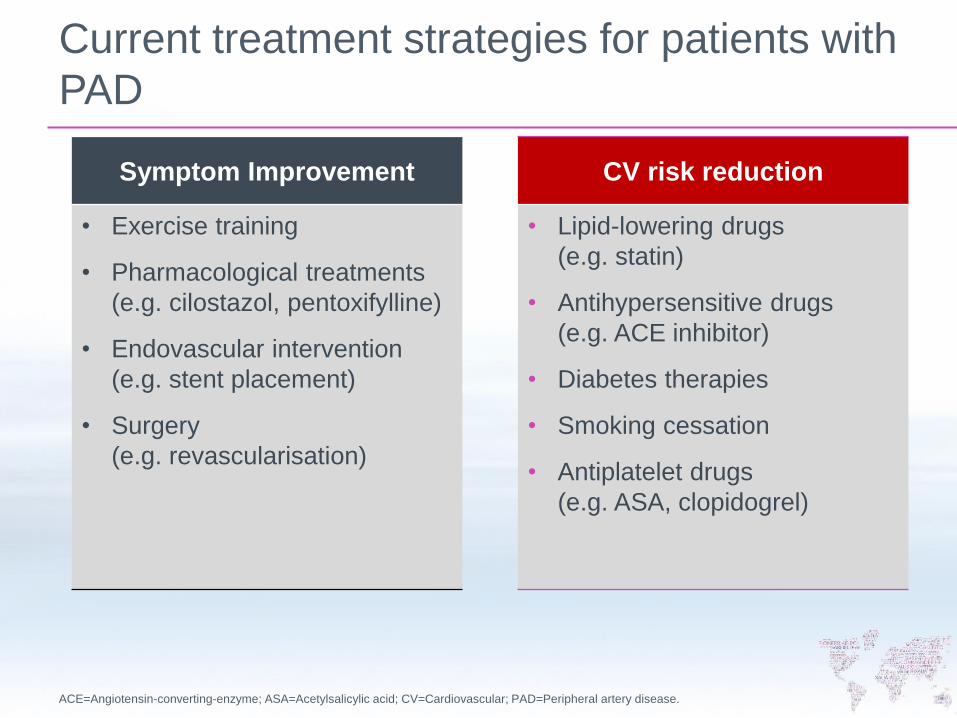
Current treatment strategies for patients with
PAD
ACE=Angiotensin-converting-enzyme; ASA=Acetylsalicylic acid; CV=Cardiovascular; PAD=Peripheral artery disease.
Symptom Improvement
• Exercise training
• Pharmacological treatments
(e.g. cilostazol, pentoxifylline)
• Endovascular intervention
(e.g. stent placement)
• Surgery
(e.g. revascularisation)
CV risk reduction
• Lipid-lowering drugs
(e.g. statin)
• Antihypersensitive drugs
(e.g. ACE inhibitor)
• Diabetes therapies
• Smoking cessation
• Antiplatelet drugs
(e.g. ASA, clopidogrel)
• Cochrane Review conclusions
• Limited evidence suggesting that restenosis/reocclusion
is reduced by antiplatelet drugs;
• information on bleeding and side effects is lacking.
• Trials are small and of variable quality and side effects
are not addressed.
• Further good quality, large-scale RCTs are required.
Robertson L, Ghouri MA, Kovacs F. Antiplatelet and anticoagulant drugs for prevention of restenosis/reocclusion following
peripheral endovascular treatment. Cochrane Database of Systematic Reviews 2012, Issue 8. Art. No.: CD002071. DOI:
10.1002/14651858.CD002071.pub3.
Antithrombotic treatment after intervention
Antithrombotic treatment after intervention
Guidelines
• ACC/AHA and ESC are divergent
• Recommendations often extrapolated from CAD,
or expert opinions
• ACCP recommend single antiplatelet over DAPT
post angioplasty/ and stent in PAD (2C)
• ESC: DAPT with aspirin / thienopyridine for ≥ 1 month after
infrainguinal BMS (IC)
• Anticoagulation after infrainguinal PTA / stenting was assessed
in 3 RCTs: None showed significant improvement in patency
=> anticoagulation cannot be recommended
ACCF/AHA [Anderson et al. 2013] and ESC [Tendera et al. 2011] ACCP [Alonso-Coello et al. 2012].
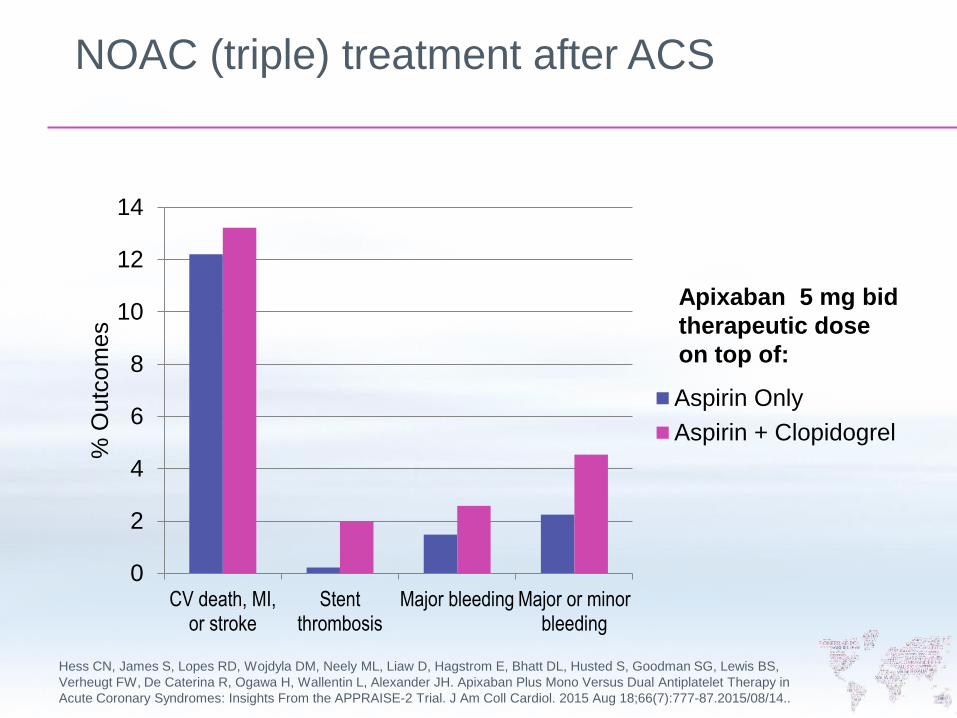
NOAC (triple) treatment after ACS
Hess CN, James S, Lopes RD, Wojdyla DM, Neely ML, Liaw D, Hagstrom E, Bhatt DL, Husted S, Goodman SG, Lewis BS,
Verheugt FW, De Caterina R, Ogawa H, Wallentin L, Alexander JH. Apixaban Plus Mono Versus Dual Antiplatelet Therapy in
Acute Coronary Syndromes: Insights From the APPRAISE-2 Trial. J Am Coll Cardiol. 2015 Aug 18;66(7):777-87.2015/08/14..
0
2
4
6
8
10
12
14
CV death, MI,or stroke
Stentthrombosis
Major bleeding Major or minorbleeding
% O
utc
om
es
Aspirin Only
Aspirin + Clopidogrel
Apixaban 5 mg bid
therapeutic dose
on top of:
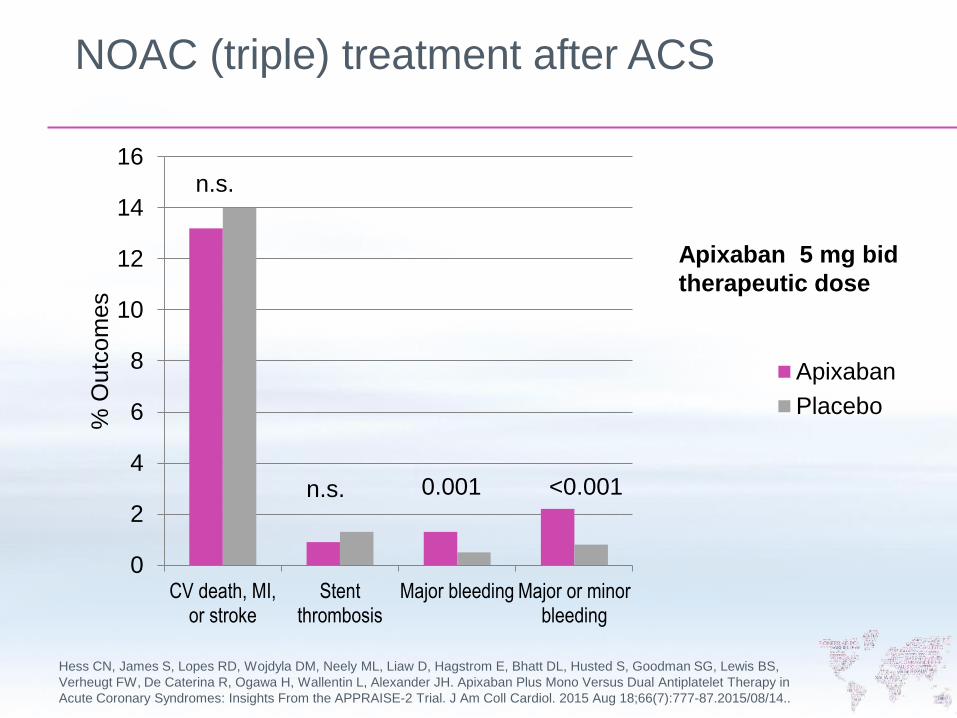
NOAC (triple) treatment after ACS
Hess CN, James S, Lopes RD, Wojdyla DM, Neely ML, Liaw D, Hagstrom E, Bhatt DL, Husted S, Goodman SG, Lewis BS,
Verheugt FW, De Caterina R, Ogawa H, Wallentin L, Alexander JH. Apixaban Plus Mono Versus Dual Antiplatelet Therapy in
Acute Coronary Syndromes: Insights From the APPRAISE-2 Trial. J Am Coll Cardiol. 2015 Aug 18;66(7):777-87.2015/08/14..
0
2
4
6
8
10
12
14
16
CV death, MI,or stroke
Stentthrombosis
Major bleeding Major or minorbleeding
% O
utc
om
es
Apixaban
Placebo
Apixaban 5 mg bid
therapeutic dose
<0.001 0.001 n.s.
n.s.
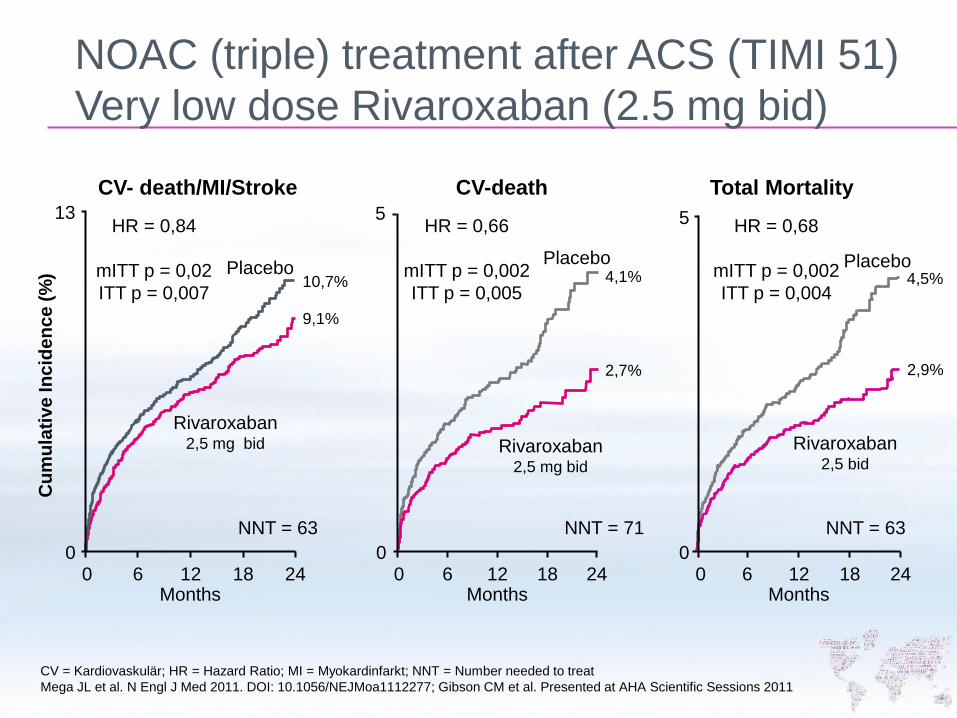
0
Months
CV-death
NNT = 71
5
0 24
4,1%
2,7%
Placebo
Rivaroxaban 2,5 mg bid
HR = 0,66
mITT p = 0,002
ITT p = 0,005
18 12 6 0
5
Total Mortality
Months
4,5%
2,9%
24 0
Placebo
Rivaroxaban 2,5 bid
HR = 0,68
mITT p = 0,002
ITT p = 0,004
18 12 6
NNT = 63
Months
CV- death/MI/Stroke
Cu
mu
lati
ve
In
cid
en
ce
(%
)
HR = 0,84
mITT p = 0,02
ITT p = 0,007 10,7%
9,1%
Rivaroxaban 2,5 mg bid
Placebo
13
0 24 0 18 12 6
NNT = 63
CV = Kardiovaskulär; HR = Hazard Ratio; MI = Myokardinfarkt; NNT = Number needed to treat
Mega JL et al. N Engl J Med 2011. DOI: 10.1056/NEJMoa1112277; Gibson CM et al. Presented at AHA Scientific Sessions 2011
NOAC (triple) treatment after ACS (TIMI 51)
Very low dose Rivaroxaban (2.5 mg bid)
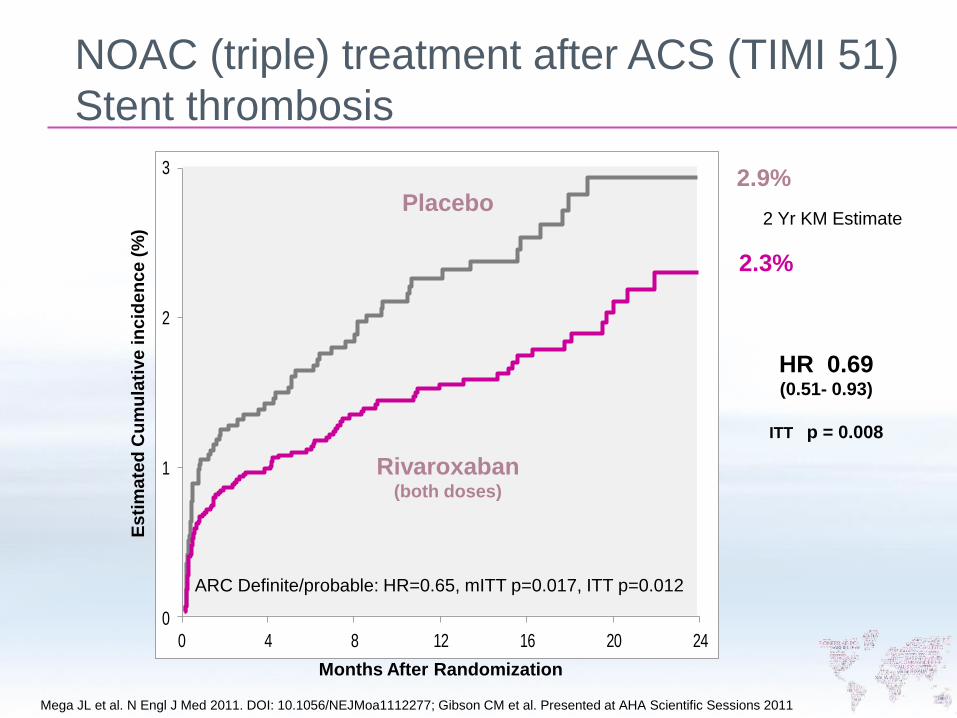
0
1
2
3
0 4 8 12 16 20 24
Months After Randomization
Rivaroxaban (both doses)
HR 0.69
(0.51- 0.93)
ITT p = 0.008
2.9%
2.3%
Es
tim
ate
d C
um
ula
tive
in
cid
en
ce
(%
)
Placebo 2 Yr KM Estimate
ARC Definite/probable: HR=0.65, mITT p=0.017, ITT p=0.012
Mega JL et al. N Engl J Med 2011. DOI: 10.1056/NEJMoa1112277; Gibson CM et al. Presented at AHA Scientific Sessions 2011
NOAC (triple) treatment after ACS (TIMI 51)
Stent thrombosis
Natural history – 5-year follow-up
CV=Cardiovascular; MI=Myocardial infarction; WD=Walking distance.
Norgren L, et al. J Vasc Surg. 2007;45 Suppl S:S5–67.
No symptoms
(20–50%)
Interm. claudication
(10–35%)
Other leg pain
(30–40%)
• Stable: 70–80%
• Further reduced WD: 10–20%
• Critical limb ischaemia: 5–10%
• Amputation: <1% annually
Limb prognosis
• Mortality: 10–15%
• (CV: 75%)
• MI/stroke: 20%
General prognosis
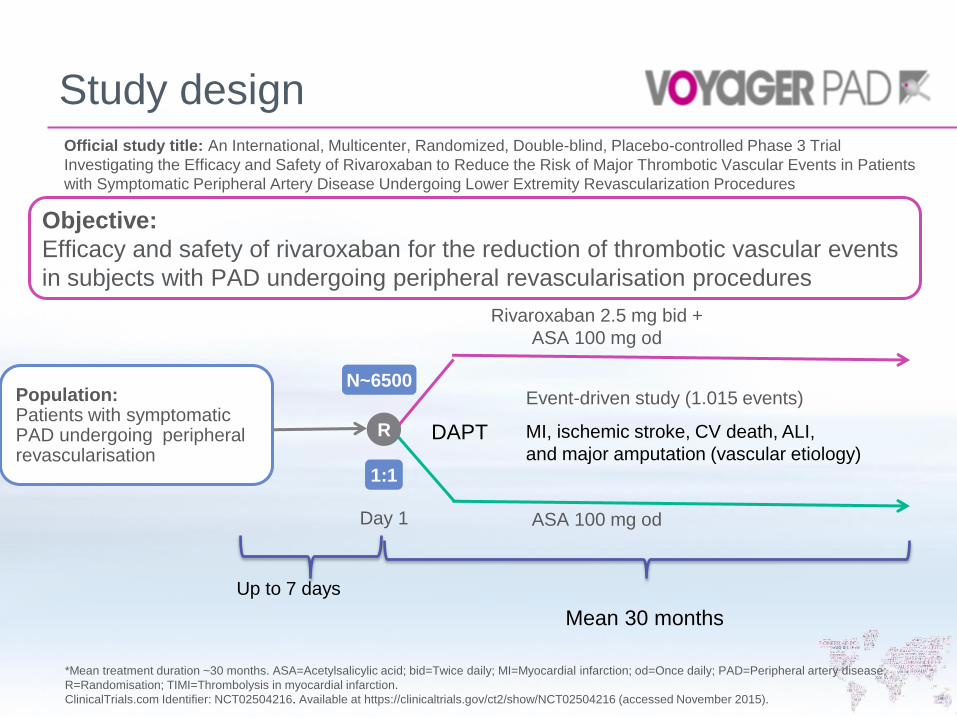
Objective:
Efficacy and safety of rivaroxaban for the reduction of thrombotic vascular events
in subjects with PAD undergoing peripheral revascularisation procedures
Rivaroxaban 2.5 mg bid +
ASA 100 mg od
ASA 100 mg od
R
N~6500
1:1
Day 1
Population: Patients with symptomatic PAD undergoing peripheral revascularisation
Event-driven study (1.015 events)
MI, ischemic stroke, CV death, ALI,
and major amputation (vascular etiology)
Study design Official study title: An International, Multicenter, Randomized, Double-blind, Placebo-controlled Phase 3 Trial
Investigating the Efficacy and Safety of Rivaroxaban to Reduce the Risk of Major Thrombotic Vascular Events in Patients
with Symptomatic Peripheral Artery Disease Undergoing Lower Extremity Revascularization Procedures
*Mean treatment duration ~30 months. ASA=Acetylsalicylic acid; bid=Twice daily; MI=Myocardial infarction; od=Once daily; PAD=Peripheral artery disease;
R=Randomisation; TIMI=Thrombolysis in myocardial infarction.
ClinicalTrials.com Identifier: NCT02504216. Available at https://clinicaltrials.gov/ct2/show/NCT02504216 (accessed November 2015).
Up to 7 days
DAPT
Mean 30 months
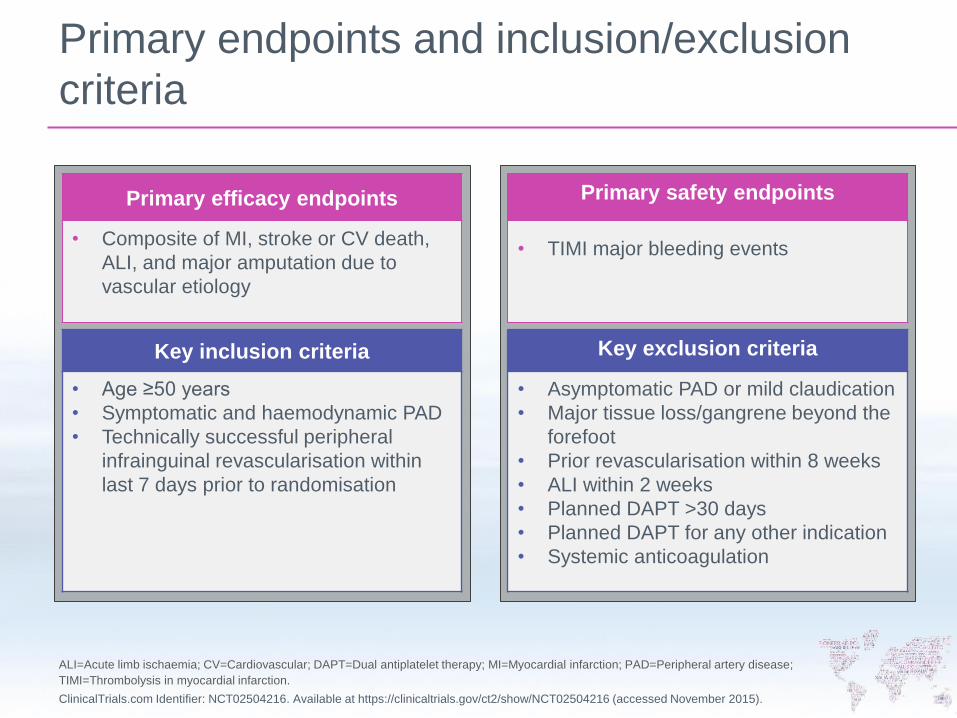
Primary endpoints and inclusion/exclusion
criteria
ALI=Acute limb ischaemia; CV=Cardiovascular; DAPT=Dual antiplatelet therapy; MI=Myocardial infarction; PAD=Peripheral artery disease;
TIMI=Thrombolysis in myocardial infarction.
ClinicalTrials.com Identifier: NCT02504216. Available at https://clinicaltrials.gov/ct2/show/NCT02504216 (accessed November 2015).
Primary efficacy endpoints
• Composite of MI, stroke or CV death,
ALI, and major amputation due to
vascular etiology
Primary safety endpoints
• TIMI major bleeding events
Key inclusion criteria
• Age ≥50 years
• Symptomatic and haemodynamic PAD
• Technically successful peripheral
infrainguinal revascularisation within
last 7 days prior to randomisation
Key exclusion criteria
• Asymptomatic PAD or mild claudication
• Major tissue loss/gangrene beyond the
forefoot
• Prior revascularisation within 8 weeks
• ALI within 2 weeks
• Planned DAPT >30 days
• Planned DAPT for any other indication
• Systemic anticoagulation
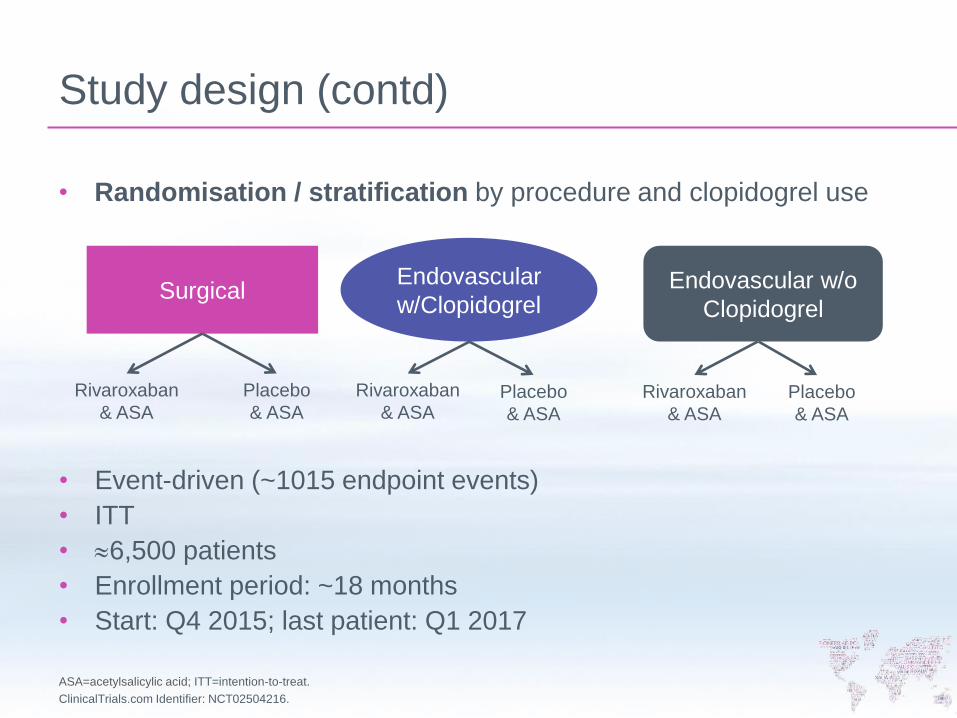
Study design (contd)
• Event-driven (~1015 endpoint events)
• ITT
• 6,500 patients
• Enrollment period: ~18 months
• Start: Q4 2015; last patient: Q1 2017
ASA=acetylsalicylic acid; ITT=intention-to-treat.
ClinicalTrials.com Identifier: NCT02504216.
• Randomisation / stratification by procedure and clopidogrel use
Surgical
Endovascular
w/Clopidogrel Endovascular w/o
Clopidogrel
Rivaroxaban
& ASA Rivaroxaban
& ASA
Rivaroxaban
& ASA
Placebo
& ASA Placebo
& ASA
Placebo
& ASA

Committee chairs
Executive Committee
William R. Hiatt, MD – Chair University of Colorado and CPC
Rupert M. Bauersachs, MD – Co-Chair Klinikum Darmstadt GmbH
Independent Data Monitoring
John Dormandy, MD – Chair St. George’s Hospital Medical School
Independent Clinical Adjudication
Warren Capell, MD – Chair CPC Clinical Research
International Steering Committee
Richard Powell, MD – Co--Chair Dartmouth-Hitchcock Medical Center
Dierk Scheinert, MD – Co--Chair University Hospital Leipzig

National lead investigators
Argentina A. Alarcon
Austria M. Brodmann
Belgium F. Vermassen
Brazil D. Brasil
Bulgaria V. Chervenkoff
Canada D. Szalay
China TBD
Czech Republic K. Roztocil
Denmark H. Sillesen
France J. B. Ricco
Germany D. Scheinert
Hungary L. Matyas
Japan H. Shigematsu & Y. Yonemitsu
Italy C. Rabbia
Netherlands F. Moll
Poland A. Jawien
Portugal A. Mansilha
Romania I. Coman
South Korea D. Choi
Spain V. Riambau
Sweden L. Norgren
Switzerland I. Baumgartner
Taiwan S. Wang
Thailand P. Mutirangura
United Kingdom G. Hamilton
United States R. Powell, A. Hirsch,
J. Mustapha & J. Mills
Conclusion
Unmet needs in PAD
PAD remains a frequent and serious disorder with a high rate
of severe thrombotic complications,
including AMI, stroke, CV death, ALI and amputation
The risk is particularly high in incident patients, i.e. patients
undergoing revascularisation
VOYAGER PAD is the largest antithrombotic trial ever
performed in PAOD patients undergoing revascularization
VOYAGER PAD will also provide important long-term and
large-scale outcome data in patients undergoing
revascularisation procedures for PAD
VOYAGER PAD is
the first trial to
examine the effect
of a very low dose
anticoagulant (2.5
mg Rivaroxaban
bid) on top of
standard treatment
to improve limb and
systemic outcomes
after intervention or
surgery
Thank you very much for your attention!

Thank you very much for your attention!










![Voyager price proposal · Web viewDear [Greeting] Voyager price proposal Thank you for your interest in Voyager as your future navigation management solution. Voyager is widely recognised](https://img.pdfslide.us/doc/110x75/612245d99494a012852d3f53/voyager-price-proposal-web-view-dear-greeting-voyager-price-proposal-thank-you.jpg)