Embed Size (px)
DESCRIPTION
University of Western Ontario Medical Journal Schulich School of Medicine & Dentistry
Citation preview

The UNIVERSITY of WESTERN ONTARIO
~
I ~ -An interdi ciplinary medical cience publication; establi hed 1930 -
Volume 70 umber 1 Spring 2000
CARDIOVASCULAR MEDICINE
TAY periodical W1.ME344D Medical journal. Received on : 2000-05-31 70:1
An excellent ute to reach your patients' lipid targets
r f _)..!JD2Ja
_0_;-J_r_r:_u_; _f -_fj_r::;-~ j
In achie\in effecti,·e lipid control, many deJa, rna' pre,·ent ,·ou from reachin \OUf £an!e .
-E: J:/ .=JJn].=.;J} ~.;J -.r.;J
. ·ew dara- ho,,·ed LIPITOR actually e patien to er ,,;th fe,,·er titration and fewer repeat ,; i than Zocor , :\le,-aco . or Le co l .
j, } ur new rarin patien th benefi ofUPIT R:
Exceptional LDL reduction - 39-6 % \er the full do e rano-e·
i~ificanuy beuer LDL and T , HDL ratio reductio . compared to Zo or or Pra,-achol at t:art.ino- do
The added benefit of excellent T reducti - I 3/% \ r the full d ran
Priced to be competiti\·e - LIPITOR co le than Zocor or PraYachol at
ual
Avai lable on all provincial formularies
An excellent #'i rst choice vvhen you choose rtatin therapy
ATDRVASWIN CALCIUM

EDITORIAL STAFF Editor-in-Chief Dan Hackam ... ..... ... Meds 2000
Senior Associate Editor Mason Ross .. ...... ..... Meds 2001
Junior Associate Editor Eric Wong .. ... .... .... ... Med 2002
Departmental Editors
Advertising View-An-Ad
Printer Willow Printing Group Limited
Ethics .. .. ...... .. .. ......... ... ..... ... ....... .... .David Satin .. ...... ....... .. ... .. ..... Meds 2001 yan arine ........ ..... ...... ...... Meds 2002
Michael Lee-Poy ......... .... ..... Meds 2003 Kim Gilmour ....... ...... ...... ..... Meds 2003
Humour .... ...... .. .... ... ..... .. ... ............ Ben Barankin ..... ....... ............ Meds 2001 Keir Peterson ... ......... ...... ...... Med 2003
Medical Myths .... ....... .... ...... ......... Matt Crystal ... ........... ........ .... Meds 2001 Heather Cox ... ... ... ....... .... ..... Meds 2003
Medicine On The Internet .. ....... .. Munsif Bhimani .................. . Meds 2002 Mark Baumgartner .. .. .... ...... Meds 2003
Profiles ................ .... ....... .... ...... .... .. Helen Lewandowski ....... .... Meds 2001 aji Touma .. .. .. ........ ..... ... ..... Meds 2003
Promotion and Prevention .... ... .. .Daniel Mendonca ...... ..... ..... Meds 2001 Albina Veltman ...... .. .... .. ...... Meds 2003
Thinking on Your Feet ............... .. Allan Vescan .................... ..... Meds 2001 John Lee .......... ..... ... ..... ... ...... Meds 2003
History of Medicine ..... .... .. ......... . Vadim Sherman .... ...... ... ...... Meds 2000 Alli on Suk ...... .............. ... .... Meds 2003
Medicine and the Law ....... .... ... ... Mahmoud Sharaf .... .......... ... Meds 2001 Najib Safieddine ...... ...... ...... Meds 2001 Azadeh Moaveni ..... ........ .... Meds 2003
Cover Art ............ ... ....... ............ .. .. .Scott Kish, Human Interactive co .
••••••••••••••••••••••••••••••• UWO MEDICAL JOURNAL ADVISORY COUNCIL Dr. Colby, Microbiology Dr. Nisker, Obstetrics/Gynecology Dr. Silcox, Obstetrics I Gynecology Dr. Rieder, Pediatrics Dr. Wexler, Anaesthesia
••••••••••••••••••••••••••••••• ALL CORRESPO DE CE regarding Journal content MUST be sent to the Editor of the Journal (NOT to members of the Advisory Council). Letters to the Editor will be pub/is/zed and edited at the discretion of tlze Editor. Tlze Advisory Council wa created to assist managerial & business aspects of UWO Medical Journal operations. THE A DVISO RY COU ClL HAS 0 ROLE REGARD! G CO TE T. All material pub/is/zed in tlze Journal reflects solely tlze views and opinions of the au thors of tlze material printed and not necessarily tlze editorial staff or the Advisory Council of tire Journal .
THE NEXT ISSUE
FAMILY MEDICINE
www.med.uwo.ca/ medirnl/
COVER ART: Scott Kish
A native of London, Ontario, Scott obtained his degree in Kinesiology from the University of Waterloo, where he specializes in anatomy, and visual information processing. As a self taught illustrator, Scott delivers a unique style of conceptualizing complex information pertaining to the human body in order to attract attention and increase comprehension. His work appears both locally and internationally with clients including doctors, lawyers, advertising agencies, etc.
HUMAN iNTERACTIVE INC. Medical Illustration & Graphics
Phone: (519) 850-8050 FaJc (519) eso.«l51 142 Fulanon ~(Ground Floor) l.orGxl. ON N6ASP2
Canada Post - Publication Mail Agreement Number 1720198 POSTMASTER: Undeliverable copies, please return to: UWO Medical Journal Faculty of Medicine & Dentistry University of Western Ontario London Ontario N6A 588
••••••••••••••••••••••••••••••••••••••••••••• U. W.O. Medical Journal 70 (1} 2000-------------------------
GUIDELINES FOR AUTHORS The UWO Medical Journal is an interdisciplinary medical publication, established in 1930. The Journal is
published twice each academic year: Fall and Spring. . © All material published by the UWO Medical Journal is copyright_ protected-:-- '!0 section of ~he UWO Medzcal
journal may be reproduced without the expressed wntten permzsswn of the Edztor.
SUBMISSIONS WHICH DO NOT FOLLOW THESE GWDELINES WILL NOT BE ACCEPTED FOR PUBLTCATTO
All inquiries should be directed to the Editorial Board. Please do not contact the editorial staff at home.
Office: MS-175, Health Sciences Building e-mail: [email protected]
Phone & Fax: (519) 661-4238 WebSite: www.med.uwo.ca / medjml /
Nature of The Journal The purpose of the UWO Medical Journa l is to
provide a single forum for original articles based on research or clinical medicine of topical or historical interest . Since readership of the Journa l is interdisciplinary, articles published will attempt to reflect a wide range of medical interests . In this regard , submissions should be directed towards the general medical reader. Articles which do not pertain to the feature topic will be given lower priority as will those with excessive technical jargon. Please restrict submi sions to under 2,000 words.
Informal peer review is required, i.e., non-specialist authors are encouraged to collaborate with, or at minimum, have their work reviewed for content by a specialist in the field. This individual, if not a co-author, is to be acknowledged at the end of the paper. In addition, it is recommended that all submissions be proof read for significant stylistic or grammatical errors. The editor will not assume responsibility for corrections of this nature and articles requiring such revisions will be returned to the author.
Submissions and disks become the property of the Journal. The Journal reserves the right to correct errors of punctuation or spelling. Affiliation with UWO is no t a prerequisite for authorship.
References are indicated numerically in the text1 and listed as endnotes in order of appearance.2 Do not use the 'endnote' feature of your word processing program; list references as part of the text on a separate page immediately following the body of the document. Punctuation comes before reference number and sentences are separated by one space only. Examples of Journal reference format follow below:
1. Douglas NJ, Thomas S, Jan MA. Clinical va lue of polysomnography. Lancet 1992; 339(2):347-50.
2. Dement WC, Carskadon MA, Richardson G. Excessive daytime sleepiness in the sleep apnea syndrome. In: Guilleminault C, Dement WC, eds . Sleep A pnea Syndromes. New York: Alan R Liss, 1978:23-46.
SUBMISSIONS
Please direct submissions, including return address, phone and fax numbers, to: UWO Medical Journal, Health Science Building, Room MS-175, University of Western Ontario, London, Ontario, 6A SCI.
Submissions are to include a cover letter, two doublespaced paper copies, and the full text on a 3.5" IBM compatible flopp y diskette in Microsoft Word o r WordPerfect format. The cover letter should be signed by all authors and indicate that the manuscript has not been published previously.
Short biographical notes on the authors are to be included at the beginning of each paper, on a separate page.
Figures should be profess ionall y dra w n; photocopying of illustrations from texts, without the permission of the publisher, is copyright infringement. Each figure, table, or illustration should be submitted on a separate page. Any illustration with a grey-scale should be in the form of a photograph. Two copies of each figure, table, or illustration should be included; each should have its number written on the back, as well as the name of the first author. Legends, which are to be included at the end of the text, should start on a separate page with Arabic numerals corresponding to the figures and tables.
Electronic Submission
Articles and letter to the Editor may be submitted via our e-mail link on our site on the world wide web at our URL: w ww.med.uwo.ca / medjrnl /. Any documents intended for publication should be sent as attached files, and not as e-mail messages. Acceptable formats for attached files are document fil es of any version of Microsoft Word, or WordPerfect; other file formats will not be accepted. All elements of the submission, including biographical notes on the authors, body of the article, captions for tables and figures, and references should be included as described above. A statement indicating that the manuscript is original and has not been published previously should be included as a separate page at the beginning of the document file . Illustrations a nd photographs cannot be submitted electronically at present, and must be delivered or mailed to the Journal office.
Submit To Us!!
2 ------------------------- U. W .O. Medical Journal 70 (1) 2000
CONTENTS
EDITORIAL PROGRESS CARDIOVASCULAR MEDIONE By Dan Hackarn .............................................................. ........................ ...... ............... 6
DEPARTMENTS Profiles
PROFILES 1. AN TERVIEW WITH DR. DOUGLAS BOYD
By aji Touma and Helen Lewandowski .............. .......... ............... .. ...... .. ............... ?
THINKING 0 YOUR FEET 1. A U USUAL CASE OF CHEST PAl
By Dan Hackam ...... .. ....... .... .... ... ...... ... .. .............................. ... .. ................................. lO
MEDICINE A D THE LAW 1. DEFECTIVE PACEMAKERS A D LEGAL LIABILITY
By Mahmoud Sharaf ... ..................................................................... ......................... 12
ZEBRA FILES 1. A BRIEF REVIEW OF TRUNCUS ARTERIOSUS
By John D. Stein and Jason Ashley .... .. ............................................. .... .... ............... 14
HISTORY OF MEDICINE 1. TAOISM AND THE ADVENT OF ANOE CHINESE MEDICINE
By Vadirn Sherman .. .. ... ... ........ ........ ..... ....... .. ... .. ..... ............ ......... ... ........... ... ............ I
PROMOTIO AND PREVENTIO 1. PSYCHOSOCIAL RECUPERA TTO FOLLOWING CARDIAC SURGERY
By Dan Mendonca .. ............................. ..... .................... ...... .............................. .... ... .. 20
Tire Zebra Files
U. W.O. Medical Journal 70 (1) 2000------------------------- 3
Content
FEATURE ARTICLES
1. A REVIEW OF CARDIAC MARKERS By orman Mah ....... .. .. ... ...... ....... .. ... ..... ....................... ..... ............. ...... ..... .............. 22
2. HYPERTENSION IN PREGNANCY: AN UNUSUAL ETIOLOGYA CASE REPORT By Andrea Lau man ............... ... .. .......................................... ... .. ... ... .... ................... 25
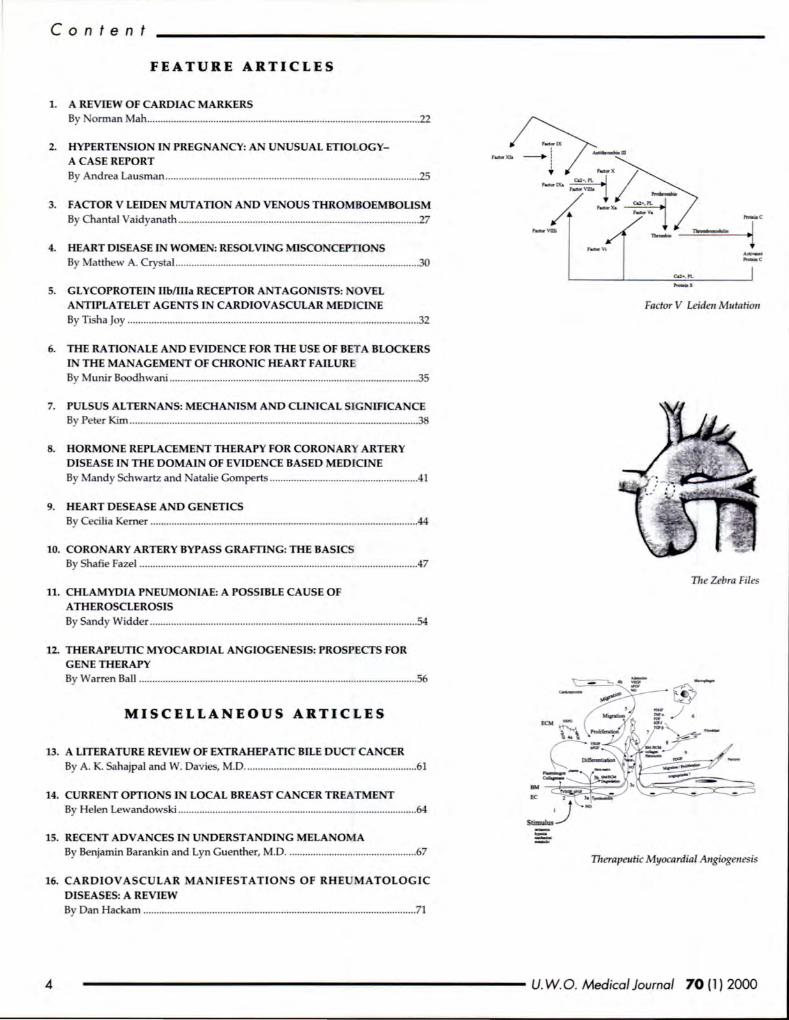
3. FACTOR V LEIDEN MUTATION AND VENOUS THROMBOEMBOLISM By Chantal Vaidyanath ... .. .................................... .. ........... .... .. ...... .. ....................... 27
4. HEART DISEASE IN WOMEN: RESOLVING MISCONCEPTIONS By Matthew A. Cry tal ............................................................ ......... ....................... 30
5. GLYCOPROTEIN llbffila RECEPTOR ANTAGONISTS: OVEL ANTIPLA TELET AGENTS IN CARDIOVASCULAR MEDICINE By Ti ha joy ........................ ........................ ...... .......... ........ ..... ........... .. ... ................. 32
6. THERA TJONALE AND EVIDENCE FOR THE USE OF BET A BLOCKERS IN THE MAN AGEMENT OF CHRONIC HEART FAILURE By Munir Boodhwani ... .... .... .. ... ... .. ................................... .. .. .......... ........................ 35
7. PULSUS ALTERNANS: MECHANISM AND CLINICAL SIGNIFICANCE By Peter Kim .. .... ... ........................ ... .. .. ..... ................. .... .. ... .. ........... .. ....................... 38
8. HORMONE REPLACEMENT THERAPY FOR CORONARY ARTERY DISEASE IN THE DOMAIN OF EVIDENCE BASED MEDICINE By Mandy Schwartz and atalie Gompert ........ .. ........ ............. .. ...................... .41
9. HEART DESEASE AND GENETICS By Cecilia Kerner ...... .. ............................................................. .. ..... ....... .................. 44
10. CORONARY ARTERY BYPASS GRAFTING: THE BASICS By Shafie Fazel .................. .... ....... ...... ................. ........... ............ .. ... .. .... .. ... .............. 47
11. CHLAMYDIA PNEUMONIAE: A POSSIBLE CAUSE OF ATHEROSCLEROSIS By Sandy Widder ......... .............. .... ... ....... .. ............. ...... .. ..... .... .... .... .... .... ..... ........... 54
12. THERAPEUTIC MYOCARDIAL ANGIOGENESIS: PROSPECTS FOR GENE THERAPY By Warren Ball ...................................................... .. .. ....... .... ........... .. ...... ................. 56
MISCELLANEOUS ARTICLES
13. A LITERATURE REVIEW OF EXTRAHEPATIC BILE DUCT CANCER By A. K. Sahajpal and W. Davies, M.D ........................................ ... ....... ............... 61
14. CURRENT OPTIONS IN LOCAL BREAST CANCER TREATMENT By Helen Lewandowski ... ...... ... ... ... ... ........................................ ... ... ....................... 64
15. RECENT ADVANCES IN UNDERSTANDING MELANOMA By Benjamin Barankin and Lyn Guenther, M.D .. .......... ............. .. ...................... 67
16. CARDIOVASCULAR MANIFESTATIO N S OF RHE MATOLOGIC DISEASES: A REVIEW By Dan Hackam ........................... ...... .... ...... .... .............. ...... ............ .. ............... ..... .. 71
Fador V Leiden Mutation
I11e Zebra Files
-= Therapeutic Myocardial Angiogenesis
------------------------ U. W.O. Medical Journal 70 (1) 2000
ABOUT THE EDITORIAL BOARD
EDITOR-IN-CHIEF
Dan Hackam is a fourth-year medical student at UWO. He will begin hi internal medicine re idency on July 1, 2000. Dan has a strong interest in cardiovascular medicine and the determinants of atherosclerosis. He plans to pursue training as a clinician scientist.
SENIOR ASSOCIATE EDITOR
Ma on Ross i a third-year medical student at UWO. He completed an HBSc in Physiology at UWO, and is currently interested in pursuing a career in a surgical discipline. Mason will be Editor-in-Chief of the UWO Medical Journal next year.
JU lOR ASSOCIATE EDITOR
Eric Wong is a second-year medical student at UWO. He will be Senior Associate Editor of the UWO Medical Journal next year.
U. W. O. Medico/ Journal 70 (1) 2000------------------------- 5
EDITORIAL
PROGRESS IN CARDIOVASCULAR MEDICINE
D e pi te recent declines in mortality, the toll of cardiova cular disea e (CVD) in pre ent ociety is
till taggering. CVD accounted for 38% of all death in Canada in 1994, more than any other cau e of death, including cancer (28%). Twenty-three thou and individuals die each year as a result of a myocardial infarction. Cardiovascular disea e cost the Canadian economy approximately 19 billion every year in medical ervice , hospitalization expen e , lo s of income and lo s
of productivity. With the increa e in the proportion of the population that is elderly, the total burden of CVD is expected to rise, at least for the next 15 year .1
The term "cardiovascular di ea e" is a broad one and refers to many different entities, depending on the speciali t you peak to, the organ sy tern affected, the age of the patient, whether the di ea e wa acquired or congenital, and o forth. To many, CVD refer to atherosclerosis, which is a spectrum encompa sing ischemic heart di ea e (angina, myocardial infarction, ischemic cardiomyopathy, udden cardiac death), cerebrovascular di ea e (stroke, transient cerebral i chemia, va cular dementia), peripheral va cular di ea e, and arterial aneury mal di ea e. Mo t, but not all, article in this issue of the journal deal with athero dero i .
Medical cience has made va t trides in the past halfcentury toward understanding the underlying mechani ms of cardiova cular di ease and innovating new treatment . Epidemiologi ts, including tho e invol ed in the cia ic Framingham study, have given us an appreciation of the inherent risk factors that contribute to CVD: moking, hypertension, hyperlipidemia, diabetes mellitu , and age. With the exception of age, the e ri k factor are largely modifiable: it i likely that public health efforts, focu ing on improvement in diet and exercise, are re pon ible for the dramatic declines in CVD incidence and mortality een in the pa t everaJ decade .
In term of the secondary prevention of va cular disea e (that is, the prevention of event occuring in patient with pre-existing disea e), clinical inve tigator have hown us that a multitude of effective pharmacological therapeutics are available, and thi has led to much excitement in recent year . Example include beta-blocker and ace inhibitor for the prevention of death in heart failure patients, tatins for the prevention of heart attack and troke , warfarin for the prevention of troke in atrial fibrillation, ju t to name a few.
Unfortunately, this body of evidence i va tly underutilized in much of clinical practice in orth America: for instance, one recent tudy howed that only
By Dan Hackam, BSc., Editor-in-Chief
27% of hypertensive patients are adequately treated. Here too, then, there is room for improvement.
Diagno is and therapy of acute cardiovascular event ( troke, myocardial infarction, unstable angina) have also made great leap in the modern era, giving further credence to the u e of the term "progress" in the title of this editorial. The u e of radionuclide imaging tudie a well as more accurate cardiac enzyme have revolutionized the detection of coronary artery di ea e and myocardial infarction, re pectively. Thrombolytic agents, such as recombinant tis ue-type pla minogen activator and treptokina e, have roughly halved the mortality of heart attack patients presenting to hospital. And more revolutionary treatment are on the way: neuroprotective agents for acute troke, angiogene i promoter in coronary artery disease, as well as a multitude of other experimental approaches to the problem of myocardial revasculariza tion, technique which may one day replace coronary artery bypas grafting and angiopla ty.
The epidemic of cardiova cular disease in the western world i a real one, with staggering economic and human consequences. One can only hope that scientific advance in the coming century, in combination wi th better implementation of measures devi ed in the pa t century, will u her in the beginning of the end of this modem-day courge.
REFER£ CES
1. lAboratory Centre for Disease Control, 1996. Q
6 ------------------------- U. W.O. Medical Journal 70 (1} 2000
PROFILES EDITORS: NAJI TOUMA AND HELEN L EWANDOWSKI
AN DR.
INTERVIEW DOUGLAS
WITH BOYD
D r. Dougla Boyd is a cardiac urgeon at the London Health Science Centre- University Campus (LHSC-UC) who ha a pecial intere t in robotics
a i ted urgery. On September 24 1999, Dr. Boyd and hi team performed the fir t ucce ful clo ed-che t, robotic a i ted beating heart ingle bypa on John Penner, 60, of Seaforth. Thi new procedure could revolutionize the world ?f cardiac urgery and i propelling London' reputation as a world class facility for cardiac re earch and innovation.
. I?r. Boyd re~eived hi MD and cardiac surgery trauung at the Uruver ity of Ottawa and the Ottawa Heart In titute, respectively. His primary po t-cardiac training wa in_ ~~art tran plant urgery and the development of the artlfioal heart. He_wa later attracted to London by it world cia reputation as a transplant centre . He is currently a i tant profe or of urgery at the Univer ity
By Naji Touma and Helen Lewandowski
of We tern Ontario and director of the Minimally Inva ive Cardiac Surgery Program at LHSC-UC.
Do you consider yourself a researcher or a clinical surgeon?
Honestly, I really don't think of myself as a re earcher per e. I am are earcher but a clinical re earcher. My be t work i really done in the operating room. My kill and experti e are in urgery and urgical techniques. Some of the e technique have to be innovated and in order for that to happen, work has to be done in the lab; but the lab work alway involve practical model uch a tudie on ~al . I gue s I am a re earcher but most of my work is clinical. In fact, ince I have been here, I would spend four days in the operating room and one day on re earch. ~tely, with _this new technology, it is more like two days m the operating room and three days in the lab.
Could you discuss the technology behind the robotics assisted heart bypass that you recently performed at LHSC-UC?
. w_e have been concentrating our efforts in minimally mva 1ve urgery lately on beating heart techniques. We know that the mailer the incision is, the more difficult it is to maneuver conventional endo copic instruments to be able to do the job. B fore we knew we were going to be a~le to use a robot, I went to the lab and u ed about fifty ptg heart in a training model in order to learn the dexter~ty . r~quired to perform coronary bypass with very mall rna 10n . We learned very quickly that there are a
number of problems that have to be overcome before that job can be done. One problem i visualization. The two dime~sional c~era available at the time did not give us the kmd of visual dexterity required. That is when we tarted experimenting with three dimensional
vi ualization sy terns. Three dimensional cameras gave us a better perception of depth and improved the vi ual dexterity. Another problem wa tabilization. To operate on the beating heart, one ha to be able to locally tabilize the area so that ana tomosi could be performed afterward . Yet another problem wa in trumentation. Conventional endo copic in truments did not allow sufficient degrees of freedom to operate freely wi thin mall ~ci ions a in the open heart ituation. For example, th~ ability to _move one's hands left and right and look at thing fre~Iy_ 1~ reduced greatly. One i also limited by the angle of mc1 ton and the di tance from the heart to the ~h~ ~ wal_I. We found that the operation through small mci JOn IS doable but not practical. For example, to do
U. W.O. Medical Journal 70 (l) 2000------------------------ 7
P r o fil es
one single graft, it took u 90 minutes while in the open heart situation, it took us only 10-12 minute . In addition to the time, the accuracy left something to be desired in that we were not able to obtain the same kind of quality grafts as in the open heart procedure. So there were a number of factors that made us realize it is not qui te so easy to perform heart surgeries through small incisions.
All of a sudden, this new robotic technology comes along that would allow the surgeon the arne dexterity enjoyed outside the chest with absolute preci ion . Movements of the surgeon outside are digitiz d by computer control and translated to a robotic manipulator attached through pin sized holes within the chest wall. The surgeon sits down in front of a control console and manipulates surgical instruments by looking at a magnified TV screen. This view comes from a little 3D camera that is attached to a robotic arm that is in turn hooked up to a computer controller and a head et. The robot supporting the camera is activated by a sophisticated voice activation software that only recognizes the surgeon's voice. The robot only responds to the commands of the surgeon and allows for different camera movements. Hence, the visualization inside the chest is controlled by voice command . The surgeon is sitting at the console, holding instruments very similar to the ones used in open heart surgery. The movemen ts of these instruments are digitized by computer control and transmitted to the instruments inserted within the chest. A surgeon could scale very gross movements on the console to very fine movements in the chest. For example a 6 em movement outside can be translated to a 6mm movement inside. A surgeon could also move his / her hand from a certain position to a more comfortable position by stepping off a clutch. The computer control also has builtin filters so that very fine tremors are screened out. Another feature is the ability to scale a 180° rota tion outside to a 360° rotation inside. Hence, the robot has the effect of increasing a surgeon's dexterity. This is a very interactive system or a robot in the loop that enhances the urgeon's skills but doe not take over the operation.
Could you discuss the benefits of minimally invasive surgery as opposed to open heart surgery?
There are two factors that make a heart u rgery invasive and in turn force patients to stay an average of one week in the hospital after the operation. The first is the incision which is large enough to strip the breast bone and necessitate time for healing. The second is the use of the heart-lung machine. When one takes a patient's blood supply, reroute it into the heart-lung machine (which takes over the functions of both the heart and the lung) and recirculates his blood volume about 20,000 to 30,000 times in this artificial surface, something has got to happen. You never get something for nothing. Thing that happen, and they have been very well documented years ago, include: a total body inflammatory response: blood coagulation due to exposure to an artificial surfac . The incidence of strokes after heart surgery increases dramatically with age. Our studies have shown that this is largely due to the use of the heart-lung machine; manipulating the blood vessels or having to insert tubes into the aorta. Any manipulation of the aorta causes
microemboli that could go to the brain. Microemboli from the pump itself could also go to the brain. Dr. Merken, a professor of anesthesiology, has demonstrated that the use of the heart-lung machine causes a 20-30% increa e in neuro-cognitive dysfunction. That being said, there is merit in avoiding the heart-lung machine and invasive surgery.
In minimally invasive surgery, we have not only avoided the use of the heart-lung machine, we have also done small incisions so we don ' t need to spread an incision about eight inche as in open heart surgery. In fact, one small working port of 2-3 em long is enough to get the heart stabilized. This enable us to not break any bone and have only a small amount of tissue trauma and ultimately make the surgery a lot more comfortable. This is likely to reduce the need for transfusions and the overall morbidity and complication of the surgery.
When do you think this new technology will move from the experimental or research s tage to become m ore routine surgery?
In my own practice now, it is almost routine because I am doing a robotic surgery every week. However, before it is widely adopted, I think it is very important that this new procedure undergoe rigorou scientific evaluation and we have to be very careful before we proceed any further. For example, we do not yet know if these devices are safe. We have been using simple robotics for years and have had no complications associated with the robot whatsoever. We anticipate that this will be the same but until we have an appropriate number of cases, we can't cientifically say it is safe. Once safety is shown, we will be
able to demonstrate very clearly the benefits of this technology. After that, we will adopt the robot in routine urgery. I believe that within the next two years, the u e of
robotics will become mainstream.
What do you think the limitations of this technology are?
I think cost is a major i ue. This is a very expensive technology. Although, ultimately I believe this technology will pay for it elf. We compared low risk patients who underwent robotic beating heart urgery and conventional surgery. Of tho e 30 patients we looked at, we saved $45,000 by adopting the robotics technology. At this rate, we fore ee that our robot will pay for itself within one year. We anticipate that if we can get 24-48 hour stays and patients up and out of the hospital and back to work quickly, this technology will pay for itself; but right now, the cost is the greatest limiting factor. This technology is in a rapid state of evolution. I don' t think the unit we have now will be the same unit used two years from now. We currently have contracts with a pri ate company that we will be involved in helping them develop their instruments. In return, we will get upgrades in the equipment in order to stay up to date.
Other than th e b ypass, do you fo re see u s ing th is technology for other types of surgery?
Absolutely, there is no question about that. I believe very strongly that in the next two years, we will be doing beating heart robotic valve replacements, robotic
8 ------------------------- U. W .O . M edical Journal 70 (1) 2000
arrhythmia operations and even pediatric surgery.
Could you discuss the genesis of this technology and how it developed?
Robotic research really started in the early 90's. There were two major groups in California working on it independently. One was the S military with the Stanford Re earch Institute and the other was ASA and the Jet Propul ion Lab . The e two groups had different objectives.
The goal of the military group that contracted out to the Stanford Research Group was to have a robotic manipulator on a bunker like tractor trailer. The idea was to have the ability to move wounded oldiers quickly into this portable hospital with robot and have surgeons on their command console performing urgery from mile away. With the advent of fiber optics technology, data transmi sion could be done almo t at the speed of light.
The objective of the group at the Jet Propulsion Lab of ASA was to have a robot on a mission to Mars where
astronauts could go for two years without a hospital. The idea was to have a technician deploying the robot on board of the spacecraft and have a surgeon on earth perform any potential surgeries. This idea is not o far fetched and there is no question in my mind that this will be something available within seven years.
Could you talk about how important private funding such as the Ivey Foundation gift is for maintaining and developing this research technology?
Right now, I think we have established our elve as a major robotic surgery centre in the world. One of the obligations we have is to further robotic surgery and if we are going to do that in a scientific way, we have to have the foundations. The additional money from Ivey will not only support our research effort but also our clinical efforts. Just having a robot will not make us a world class facility; we need research, teaching and clinical applications. This generous Ivey gift will help in laying down the e foundations. It will not only fund the robotic program but also the imagery program. It will enhance our ability to link robotic urgery and interventional cardiology. This will make London a leader in the world in this minimally invasive approach to heart disease.
Could you discuss other important current issues in cardiology and cardiac surgery?
There is no question that angiogene is and the whole i ue of genetic research plays an important role. Also, stem transfer technology or the ability to transfer heart muscle cells into dead areas and regrowing it. Other important research areas include: myocardial revascularization, cardio-la er reva cularization in a ociation with genetic manipulation, robotics, catheterba ed interventions, and endocardioly or ethocardioly.
What would you tell medical students who may be interested in pursuing cardiac surgery as a career?
Cardiac surgery is an extremely demanding but al o an extremely rewarding career. This is really an exciting time to be a cardiac surgeon. Heart surgery has been
Prof il es
practiced the same way for almost 30 years. In the last few years, even while I was undergoing my cardiac surgery training, it is being completely changed. Right now, we are about to redefine the way cardiac surgery is practiced and that is really incredible. The advent of things like computers, genetics and robotics have greatly impacted on cardiac surgery and that i very exciting. Q
't
BEAlEX CANADA INC. }i!e concentrate our act.illities on tM three Ou$lnes:t areas of Diagrrostic fm~A&in:§, Tbe.rnpeuti·~ and Women~ Health.
Our portfolio of~um includes: O mtro t media/or X-ray$ computed tomogriJphy, magnetic ' resonance inurging -and altrasollnd; products for leukaemia. p1'0$tate ciJ.Tic r <tmJ multipl:e $clel'()!fi ; a:nd products for hormonal and nonhormonal oeontrareption.
JSearching for better solutions
a research-based pharmaceutical company, Berlex Canada $t.nv#$for innovation and is dedicated to providing products that make a igni.ficant contnou:tion to medi~l
progre and improve the quality of life of Canadians.
- , '
U. W .O. Medical Journal 70 (1) 2000------------------------- 9
THINKING ON YouR FEE T EDITORS: ALLAN VESCAN AND ]OHN L EE
AN UNUSUAL CASE OF CHEST PAIN
A 45-year old gentleman (A.B.) pre ent to hi family phy ician with a 24-hour hi tory of evere chest pain. The pain is localized to his left anterior che t,
i harp and tabbing in quality, and wa fairly sudden in on et and has not remitted ince yesterday. The pain i worse with recumbency, cough, and deep inspiration, and better with itting up and taking hallow breath . A.B. took a pirin with only moderate relief.
PLEASE STOP A 0 A SWER THE FOLLOW! G QUESTIO S:
1) What is your differential diagno i for che t pain in thi gentleman?
2) What other que tions on hi tory would clarify the differential diagnosis?
3) Given the mo t likely diagnosi , what particular finding on phy ical examination would you be diligent to eek out?
Examination of the head and neck, abdominal, re piratory and mu culo keletal sy tern i unremarkable. Turning your attention to the cardiova cular ystem, you obtain the following parameter : HR 100 and regular, BP 140 /70, JVP 3 em above the ternal angle. Carotid are bri k bilaterally with no evidence of bruit. On insp cting the precordium, you note no abnormal lift , heave , or pul ations. On palpation, there i no parasternal lift and the apex beat i located in the fifth inter pace, midclavicular line (i t is normal in timing, duration and intensity). On au cultation, you note normal h art ounds, a Grade IT / VI y tolic ejection murmur at the base with no radiation to the carotid , no extra heart ounds, and no rub.
PLEASE STOP A 0 A SWER THE FOLLOW! G QUESTIO S:
4) If a carotid bruit were pre ent, what would thi indica te, and what clinical entity on the differential diagnosi would thi make more likely?
5) What is the significance of a para ternallift? What would a di placed apex beat tell you?
6) What is the ignificance (if any) of the murmur?
7) What initial investigations would you order?
By Dan Hackam, BSc., Editor-in-Chief
CBC reveals a left- hift with mild leukocytosi (WBC 11.3) and a neutrophilic predominance. Cardiac enzyme (myoglobin, troponin-1, CK-MB) and ESR are mildly elevated. A re ting electrocardiogram (ECG) reveals the following: normal sinus rhythm, rate 98, ST elevation in multiple contiguous leads. Che t X-ray reveal a normal heart ize with no evidence of pleural effusion or pulmonary infiltrate .
PLEASE STOP A 0 A SWER THE FOLLOW! G QUESTIO S:
8) Given the abnormality on ECG, what diagno i mo t likely?
The patient i referred to a cardiologi t for further a e ment. Echocardiography (ECHO) reveals evidence of a mild pericardia! effu ion, with no evidence of pericardia! thickening, valvular abnormality, or dyskinetic myocardial segment . Ejection fraction is 55%.
PLEASE STOP A 0 A SWER THE FOLLOW! G QUESTIO S:
9) What are the etiologie of thi condition?
10) What i the progno i of thi condition?
11) Outline, in general and p cific term , the management of thi condition?
ANSWERS:
1) One can never be faulted for placing at the top of the differential tho e entitie that might endanger the life of the patient, and therefore mu t be ruled out. Given the udden on et of evere che t pain, myocardial infarction or i chemia, aortic di ection, or pulmonary embolus are all po ible. However, pericarditis is more likely, given that the pain of acute pericarditi i often pleuritic, relieved by sitting up and aggravated by recumbency and deep breathing.
2) The four cardinal cardiac ymptom are: che t pain, dy pnea, palpitations and y ncope. In addition to the e, one would a k about symptom of heart failure: orthopnea, paroxy mal nocturnal dy pnea, and ankle welling. Che t pain related to exertion, emotion, cold weather or meal , or in the pre ence of diaphore is, nau ea, or vomiting, or against a background of coronary risk factors ( making, hyperten ion, diabetes, family hi tory,
10 ------------------------- U. W.O. Medical Journal 70 (1) 2000
----------------------- T h i n k i n g o n Yo u r F e e t
and hyperlipidemia) make infarction / ischemia more likely. One would al o a k about habits such a tobacco and ethanol con umption, as well as medications, and other medical conditions (for in tance, lupus [SLE] and other connective tissue disorder are associated with pericarditis).
3) The sine qua non finding of pericarditis is the pericardia! friction rub. It may have up to three components per cardiac cycle and i high-pitched, scratching, and grating; it can ometime be elicited only when firm pre ure with the diaphragm of the tetho cope is applied to the che t wall at the left lower ternal border. It is heard mo t frequently during e piration with the patient in the sitting po ition. The rub i often incon tant and the loud to-and-fro leathery ound may disappear within a few hours, possibly to reappear the following day.
4) A carotid bruit indicate turbulent flow in the carotid artery and i diagnostic of cerebral va cular disease. Becau e athero clerosi is a generalized disease, the finding of a carotid bruit would make coronary i chemia or infarction omewhat more likely.
5) A para temal lift is palpated in right ventricular hypertrophy. A di placed apex can be found in left ventricular dilatation.
6) The murmur de cribed has all the characteristics of a benign ("functional") flow murmur, which i often een in healthy, young adult and in highflow sta tes uch pregnancy, exerd e, and anemia. The e characteri tic are : mid y tolic timing, Grade II or le , non-radiating, be t heard in the pulmonic area, non-mu ical in character.
7) The following investigation are appropriate : complete blood count (CBC), erythrocy te edimentation rate (ESR; a non- pedfic marker of
inflammation), cardiac enzymes, electrocardiogram, and che t x-ray.
8) Pericarditis.
9) Differential : infectiou (viral, bacterial, tuberculous, fungal, protozoal), a ociated with myocardial infarction (actuely, or days to weeks later; the latter is known a Ore ler's syndrome), collagen vasc u lar di ea e (SLE, periarteritis nodo a, rheumatoid arthriti ), uremia, neoplasm (brea t, lung, renal, melanoma), infiltrative di ea e, drug , trauma, radiation, and idiopathic.
10) The progno i i dependant on the underlying etiology. Acute idiopathic (or viral) pericarditis i u ually elf-limited and abate wi thin 1 month. One or more episodes of recurrent pericarditis occur in up to one-fourth of patients. Constrictive pericarditis is a rare complication.
11) The treatment of pericarditi is virtually always ymptomatic and directed toward optimizing the
comfort of the patient . Bed res t and antiinflammatory treatment with a pirin, if nece ary up to 900 mg qid, may be given . If thi s i ineffecti ve, one of the nonsteroidal anti inflammatory agents, such as indomethacin (25 to 75 mg qid) or a glucocorticoid (e.g., predni one, 20 to 80 mg daily ) u ually suppresses the clinical manifestation of the acute illness and may be u eful in p atient in whom the purulent and tuberculou form of pericarditi have been excluded. Anticoagulant hould be avoided. After the patient ha been a ymptomatic and afebrile for about a week, the do e of the anti-inflammatory agent is gradually tapered. When recurrences are multiple, frequent, disabling, and continue beyond 2 year , pericardiectomy may be effective in terminating the illness. Q
You Want It All. We have it right here.
Cbatlwn-Kcnt H ealth Alliance is a partncrshlp of three hospitals operating 235 beds. We provide state-of-the-art diagnostic and support services, including CT Scan, a laparoscopic suite, progressive medical staff, dynamic administration and strong links to surrounding academic centres.
You will work in a beautiful southwest Ontario city that is safe and affordable, with golf, beaches, lakes and easy access to centres of reaeation, culture and education. We are currently seeking:
ER and Family Practice Physicians
" Group or solo practice available " On site physician office complex being explored " APP program at Sydenham campus " CME courses funded " Reasonable call schedule " Relocation grants
To H ave It All, Call
*CHATHAM-Ir:ENT Health Alliance www.ph sicianswanted.com
Td: (519) 628-4100 E-mail: [email protected]
or C2ll toll free 1-877-<D-SWORM
U. W.O. Medical Journa l 70 (1} 2000------------------------- 11
MEDICINE AND THE LAW EDITORS: MAHMOUD SHARAF, NAJIB SAFIEDDINE, AzADEH MOAVENI
DEFECTIVE PACEMAKERS LEGAL LIABILITY
AND
W ith the development of pacemakers and implanted defibrillators, patients pron e to cardiac arrhythmia by reason of ischemic di ease
or congenital abnormality have seen dra m atic improvement in quality of life and life expectancy. The pacemaker consists of an external unit, either single or dual-chambered, with a lead embedded in the right atrium, or two leads implanted in atrium and ventricle1
•
The pacemaker sets the heart rate and can ad just dynamically to suit systemic activity levels1
•
The combination of intense patient reliance on these devices to sustain an active lifestyle and the inevitable tendency of mechanical parts to malfunction can result in cardiac events, and even death. The courts are a frequent recourse for settlement of claims of manufacturer liability for the complications of pacemaker malfunction. There are several actual and potential claims that plaintiffs can use. This paper will serve to discuss a few of them using illustrative examples.
In the case of Tracy v. Telectronics Pacing Systems, Inc., Ronald Tracy of St. Clair County, Michigan brought forth a lawsuit against the manufacturer after his pacemaker failed, forcing him to replace it at the Cleveland Clinic at substantial personal risk and expense •. The J-lead pacemaker has a thin, flat intracardiac lead that is abnormally prone to metal fatigue, thereby incapacitating the pacemaker. The proceedings in the U.S. District Court indicated the manufacturer was aware of the fault as early as 1992, but did not recall the unit until1994, a year before this trial 1
• The court decided in favour of the plaintiffl. The Food and Drug Administration ascertained from Telectronics, Inc. that 22 000 persons have received the Jlead model which the company estimates has a 17% failure rate1
• It is estimated that 2 individuals have died as a result of this malfunction•. There are currently 60 pending cases against Telectronics Pacing Systems, Inc. in U.S. courts1
.
In Ontario there are 2 cases pending aga inst Medtronics, Inc.'s Canadian subsidiary, out of Mississauga1
. In 1998, Sudbury residents brought a class action suit against the company because of fa ulty polyurethane insulation on the leads. Any of the thou and Ontarians having received the 4004 model (between 1989-1995) is eligible to participate in the suit1
•
Susan and Jeff Blanchard of London, Ontario brought forth a suit in ovember, 1998 in the Ontario Court of Justice against the same manufacturer of the 4004 model alleging negligence in the design, development, testing, manufacture, licensing and distribution of their product. They seek $275 000 in assorted damages•.
By Mahmoud Sharaf, MEDS 2002
The risk of serious atrial thrombus formation pursuant to pacemaker lead implantation is rare (only about 2%t However, the possibility of claims being drafted based on thrombogenic lead configuration can not be discounted.
Another interesting potential cause for future claims is the proposed link between cellular phone use and interference in pacemaker signaling. The ew England Journal of Medicine study (May 29, 1997) indicated that if cellular phones were operated directly over the precordium, interference could be noted in 20% of individuals. Serious interference wa noted in one third of this twenty percent. Normal operation of cellular phones at ear level had no role in producing interference•. There have been no cases to date brought to general attention that have been argued along these lines, but this may not dissuade enterprising lawyers from trying.
The last, and perhaps most interesting, potential cause of lawsuits in the future is the Y2K non-compliance issue. This cause celebre of Ann Couffou, Managing Director of the Giga Year 2000 Relevance Service, was serious enough to warrant her testimony before the House Subcommittee on Science and Technology in 19971
•
The Veterans Adminis tration asked 5 pacemaker companies about Y2K readiness. One company refused outright to cooperate while the other four indicated readiness would be achieved before the end of 19991
•
In actuality, most pacemakers (including those made by Medtronic, Inc. and PaceArt, Inc.) have no datecomputing chips, and are thus Y2K-proofl . Some pacemakers contain chips that serve to record cardiac traces for physicians to study. These date-computing chips would cease to record information on New Year's Day, and thus will sacrifice the close monitoring required in some patients•. Implanted defibrillators, which assess arrhythmia and rectify it, do use date-computing chips. If these monitors have recorded no event in 6 months time, then the defibrillators will not subsequently function, assuming the long inactivity means that the device should be replaced because it may be defective. If no event has been recorded since 1900 (which is the case on 01.01.2000), then th e defibrillators will s top, not in line with replacement schedules•.
Some manufacturers of date-computing chips have switched to an 8-digit date format to avoid Y2K problems, like the British manufacturer of CriSPR. Others are still considering the problem 1•
In conclusion, the grounds for successful liability suits for pacemaker malfunction will primarily rest on demonstration of mechanical defect present at production or abnormal tendency to wear out. It is important to show
12 ------------------------ U. W.O. Medical Journal 70 (1) 2000
multiple cases of malfunction for the model in question. The technology of pacemakers ha greatly improved over the decades and lawsuits, despite their unsavoury conno tations, ha ve played an integral part in the con tinuous dri ve towards product quality and standardization.
REFERE CES
1. Harrison 's Principles of Internal Medicine, 14th ed. McGraw-Hill . ew York: ew York. 1998, p.1258-1260.
2. Ibid. 3. ]osar, David. Man Sues over Defective Pacemaker. Detroit ews.
ovember 15, 1995. 4. http://VJWW. uscourts.gov!news.html. 5. Ibid. 6. ]osar, David. Man Sues over Defective Pacemaker . Detroit News .
ovember 15, 1995. 7. Ibid. 8. Ibid. 9. Carmichael , Harold . Sudburians Part of Lawsrlit. Toronto Star,
May 20, 1998. 10. Ibid 11 . http://VJWW.siskind.com/cases 12. http://VJWW.perfline.comllinkslpacemaker 13. http://medisVJWW.cwru.edu/DrTed/medmomentslmm052197/mm052197T 14. Couffou, Anne. Testimony before the House Subcommittee on Science and
Technology. United States House of Representatives. ovember 14, 1997. 15. http:IIVJWW.house.gov/science/couffou 3-20.html 16. http:IIVJWW.perfline.com/limks/pacemakers 17. Ibid. 18. http://facm-kdrent.unl.eduly2klgarynorth/736 .htm 19. http://VJWW.pacemaker.co.uk Q
Medic ne and The Law
ICN CANADA L TO
1956, rue Bourdon St ., Montrbl, (Qu6becl H4M 1 V1
tel : (51 41744-6792, 1·800-361· 1448, fax : (514)744-6272,
lli1iiJI • ~. ( •S" C onjugated E suogens
~ \.: from S ovo
A unique combination of innovative
5:1 L and generic products are
r manufactured at ICN Canada for the Canadian market and
Gly Oe<m
KIN ERA •
Through quality management resources, sales & marketing support, and product development, ICN Canada is poised for expansion in the new millennium.
w ww .icncanada .com
selected markets around the world .
dltfie>r &moderm
A Centre of Diagnostic Excellence.
.. St. Thomas-Elgin ~ General Hospital
Located in the beautiful heartland of Southwestern Ontario .....
The St. Thomas-Elgin General Hospital cooperatively serves a community of75,000. We are dedicated to the finest health care for our community. On-site facilities include Emergency Room, /CU. a
Cardiac Care Unit, 6 operating theatres, a sleep lab as well as the latest CIT
Scanner. All this is minutes from London and a world class teaching hospital.
189 Elm Street, P.O. Box 2007, St. Thomas, ON NSP 3W2
(519) 631-2020
U. W .O. Medical Journal 70 (1 ) 2000------------------------- 13
THE ZEBRA FILES EDITORS: ]OHN D. STEIN AND ]ASO ASHLEY
A BRIEF REVIEW OF TRUNCUS ARTERIOSUS
INTRODUCTION
Truncu Arteriosu , fir t de cribed in detail in 179 , i a congenital defect of the great ve el invol v ing incomplete eparation of the pulmonary artery and the aorta during embryogene is. The condition affect 1 in 12,500 births 1 and patient pre ent with cyan i , tachypnea (very rapid ventilation), murmur , sweatinp during feeding, a failure to thrive and hepatomegaly . Other anomalie a ociated with TA include ventricular eptal defect , truncal valve regurgitation and incr a ed
pulmonary va cular re i tance1• Untreated, thi condition
has a 65% mortality rate in the fir t 6 months of life increasing to 75% within the fir t year 1
• Cau e of mortality include excessive pulmonary blood flow, conge tive heart failure and progre ive cyanosis due to accelerated pulmonary va cular ob tructi e di a e . Palliative urgical intervention performed before the e conditions appear ha lowered the two-year mortality to approximately 20%.1
Embryology and Etiology In the normal development of the great ve e ls,
truncal ridge form in the truncus during the fifth and ixth week of embryogenesis. The left anterior ridge
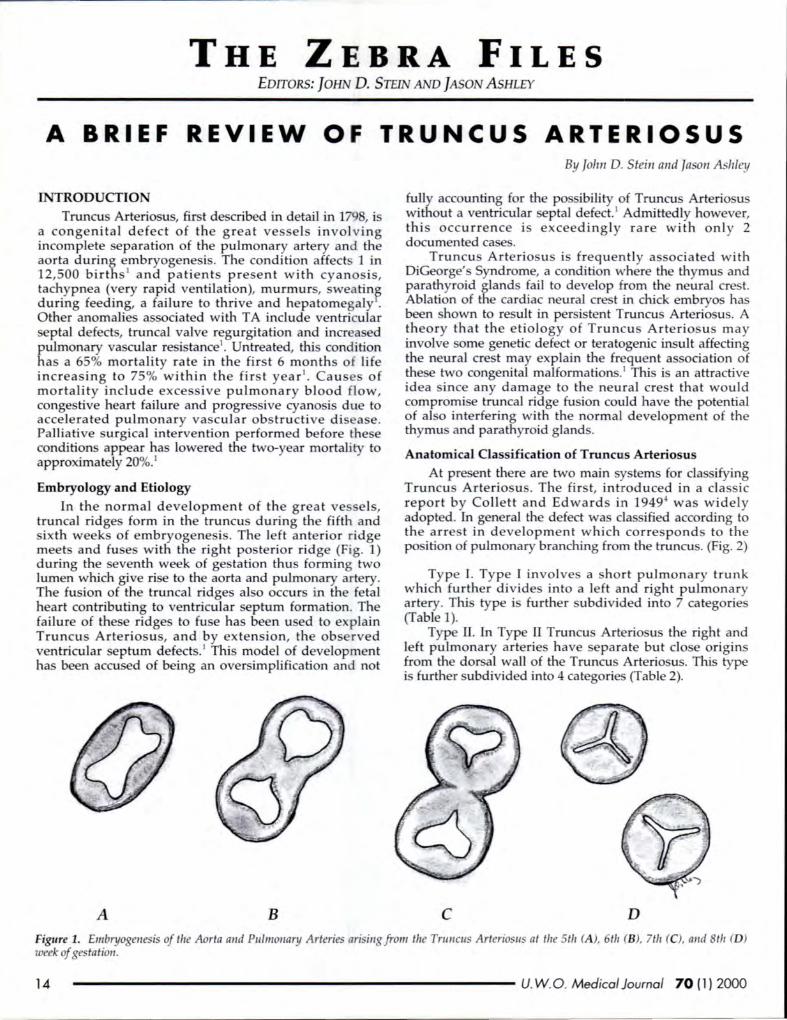
meet and fuse with the right po terior ridge (Fig. 1) during the eventh week of ge tation thu forming two lumen which give rise to the aorta and pulmonary artery. The fusion of the truncal ridges al o occur in the fetal heart contributing to ventricular eptum formation . The failure of the e ridge to fu e ha been u ed to explain Truncu Arteria u , and by exten ion, the ob rved ventricular eptum defect .1 Thi model of development ha been accu ed of being an oversimplification and not
A B
By John D. Stein and Jason Ashley
fully accounting for the po ibility of Truncus Arteria u without a ventricular eptaJ defect. 1 Admittedly however, thi occurrence i exceedingly rare with only 2 documented case .
Truncu Arteria u i frequent ly as ociated with DiGeorge' Syndrome, a condition where the thymus and parathyroid gland fail to develop from the neural ere t. Ablation of the cardiac neural cr t in chick embryo has b en hown to re ult in per i tent Truncu Arteria u . A theory that the etio logy of Truncu Arteria u s may involve orne genetic defect or teratogenic insult affecting the neural ere t may explain the frequent a ociation of the e two congenital malformation .1 This i an attractive idea ince any damage to the neural ere t that would comprorni e truncal ridge fu ion could have the potential of al o interfering with the normal development of the thymu and parathyroid glands.
Anatomical Classification of Truncus Arteriosus At pre ent there are two main y tern for cla sifying
Truncu Arteria u . The first, introduced in a classic report by Collett and Edward in 19494 wa widely adopted. In general the defect wa cla ified according to the arre t in development which corre pond to the po ition of pulmonary branching from the truncu . (Fig. 2)
Type I. Type I involve a hort pulmonary trunk which further divide into a left and right pulmonary artery. Thi type i further subdivided into 7 categories (Table 1).
Type II. In Type II Truncu Arteria u the right and left pulmonary arterie have separa te but do e origins from th dor al wall of the Truncu Arteria u . This type is further subdivided into 4 categorie (Table 2).
c D
Figure 1. Embryogenesis of the Aorta and Pulmonary A rteries ari ing from the Tru ncus Arteriosus at the 5th (A ), 6th (B), 7th (C), and 8th (D) week of gestation.
14 ------------------------- U. W.O. Medical Journal 70 (1) 2000

------------------------- T h e Z e b r a F I e s
Collett and Edwards I II
Van Praagh Al A2 A3 A4
Figure 2. A comparison of the Collett & Edwards and Van Praagh & Van Praagh Clas ifications ofTnmcus Arteriosus.
Type ill. In type ill Truncus Arteria us the right and left pulmonary arterie have eparate origins from the right and left lateral walls of the truncu . This type is further subdivided into 4 categorie (Table 3).
Type IV. Type IV Truncu Arteria us is characterized b an ab ence of pulmonary arterie a well as a lack of any 6th aortic arch derivatives. Perfu ion of the lungs occurs by way of the bronchial arteries. Type IV i further ubdivided into 4 categories (Table 4).
Table 1
Type I
Subtype 1 Subtype 2 Subtype 3 Subtype 4 Subtype 5 Subtype 6 Subtype 7
Table 2
Type II
Subtype 1 Subtype 2 Subtype 3
Subtype 4
Single pulmonary trunk arising from the Truncus Arteriosus (from the left side unless otherwise noted) Pulmonary trunk from left side. Pulmonary trunk from right side. Patent ductus arteriosus. Patent ductus arteriosus and coarctation of the aortic arch. Complete atresia of part of the aortic arch. Right aortic arch. Double aortic arch.
Separate but close origins of the right and left pulmonary arteries Ductus arteriosus is absent. Patent ductus arteriosus. Patent ductus arteriosus with coarctation and atresia of the aortic arch. Right aortic arch
An alternative cia ification sy tern was offered by Van Praagh and Van Praagh7 to include in tance of Truncus Arteria us without ventricular eptal defects (VSD) and further, to exclude Collett and Edward' Type IV category . It wa argued that Type IV hould be con idered a ca e of failed pulmonary artery formation rather than a failure of the aorta and pulmonary artery to eparate.
Table 3
Type Ill
Subtype 1 Subtype 2
Subtype 3 Subtype 4
Table 4
Type IV Subtype 1 Subtype 2 Subtype 3 Subtype 4
Separate origins of the right and left pulmonary arteries from the right and left lateral wall of the truncus. Ductus arteriosus is absent and both 6th aortic arches present. Patent ductus arteriosus with only one 6th aortic arch present and supplying one lung. The other lung perfused by the ductus arteriosus or bronchial arteries. Right aortic arch and both 6th aortic arches present. Right aortic arch with only one 6th aortic arch present and supplying one lung. The other lung perfused by the ductus arteriosus or bronchial arteries.
Pulmonary arteries are absent Bronchial supply to lungs via descending aorta. Bronchial supply to lungs via descending aorta and aortic arch. Bronchial supply to lungs via aortic arch. Right aortic arch and bronchial supply to the lungs via descending aorta.
U. W.O. Medical Journal 70 (1) 2000------------------------- 15
T h e Z e b r a F I e s --------------------------
Table 5
Type A Subtype 1 Subtype 2
Subtype 3
Subtype 4
Truncus Arteriosus with VSD Partial separation of a main pulmonary artery from the truncus. No main pulmonary artery, right and left branch off from the truncus separately. Absence of single pulmonary artery (left or right). Ipsilateral lung receives collateral perfusion. Atretic or absent aortic arch with large patent ductus arteriosus. A main pulmonary artery arises from the ascending aorta.
Table 6
Type B Subtype 1 Subtype 2
Subtype 3
Subtype 4
Truncus Arteriosus without VSD Partial separation of a main pulmonary artery from the truncus. No main pulmonary artery, right and left branch off from the truncus separately. Absence of single pulmonary artery (left or right). Ipsilateral lung receives collateral perfusion. Atretic or absent aortic arch with large patent ductus arteriosus.
c
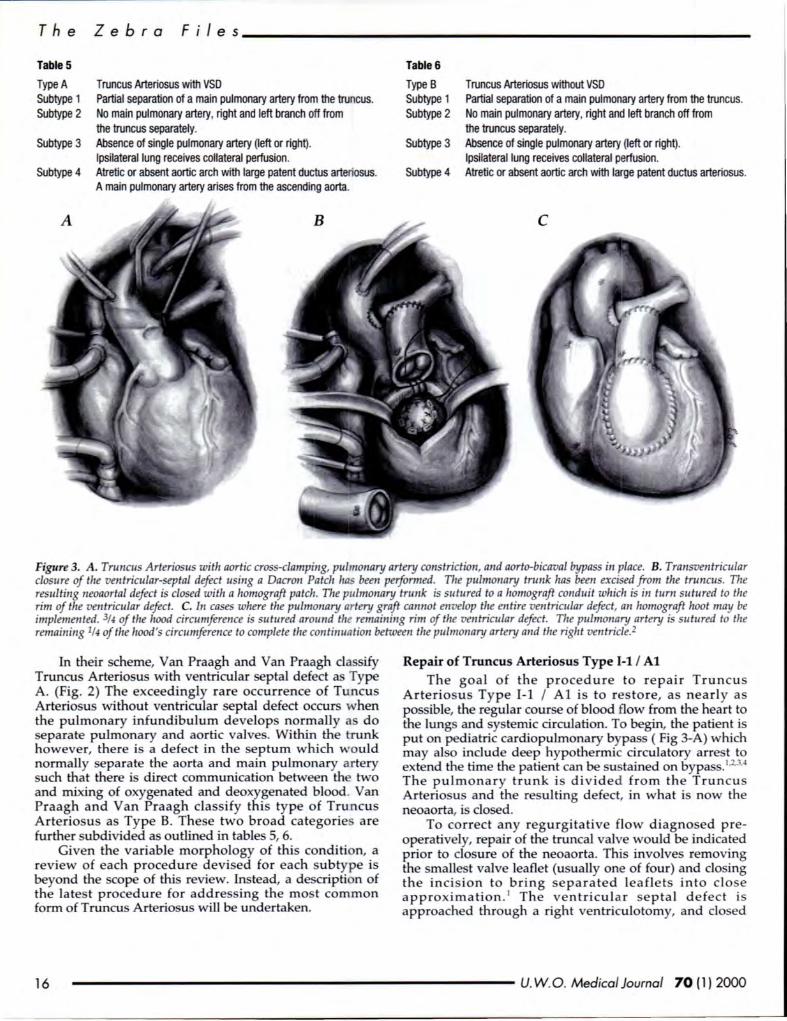
Figure 3. A. Truncus Arteriosus with aortic cross-clamping, pulmonary artery constriction, and aorto-bicaval bypass in place. B. Transventricular closure of the ventricular-septal defect using a Dacron Patch has been performed. The pulmonary trunk has been excised from the truncus. The resulting neoaortal defect is closed with a homograft patch. The pulmonary trunk is sutured to a homograft conduit which is in turn sutured to the rim of the ventricular defect. C. In cases where the pulmonary artery graft cannot envelop the entire ventricular defect, an homograft hoot may be implemented. 3f4 of the hood circumference is sutured around the remaining rim of the ven tricular defect. The pulmonary artery is su tured to the remaining 1f4 of the hood's circumference to complete the continuation between the pulmonary artery and the right ven tricle.2
In their scheme, Van Praagh and Van Praagh cla sify Truncus Arteriosus with ventricular septal defect as Type A. (Fig. 2) The exceedingly rare occurrence of Tuncus Arteriosus without ventricular septal defect occurs when the pulmonary infundibulum develops normally as do separate pulmonary and aortic valves. Within the trunk however, there is a defect in the septum which would normally separate the aorta and main pulmonary artery such that there is direct communication between th two and mixing of oxygenated and deoxygenated blood. Van Praagh and Van Praagh classify this type of Trun cus Arteriosus as Type B. These two broad categorie are further ubdivided as outlined in tables 5, 6.
Given the variable morphology of this condition, a review of each procedure devised for each subtype is beyond the scope of this review. Instead, a de cription of the latest procedure for addressing the mo t common form of Truncus Arteriosus will be undertaken.
Repair of Truncus Arteriosus Type 1-1 I Al The goal o f the procedure to repair Truncus
Arteriosu s Ty pe 1-1 I A l is to restore, as nearly as possible, the regular course of blood flow from the heart to the lung and systemic circulation. To begin, the patient is put on pediatric cardiopulmonary bypass ( Fig 3-A) which may also include deep hypothermic circulatory arrest to extend the time the patient can be su tained on bypass. 1
·2.3·4
The pu lmona ry trunk is d ivide d fro m th e Truncu s Arteriosus and the resulting defect, in what i now the neoaorta, is closed.
To co rrect any regurgitative flow diagnosed preoperatively, repair of the truncal valve would be indicated prior to closure of the neoaorta. This involves removing the smalle t valve lea£let (u ually one of four) and do ing th e inci ion to br ing se p a ra te d lea fl e ts into clo e a pproximation . 1 The ve ntricul ar septal d e fec t is approached through a right ventriculotomy, and do ed
16 ------------------------- U. W.O. Medical Journal 70 (1) 2000
-------------------------- T h e Z e b r a F i I e s
with an albuminized Dacron or Gortex patch (Fig 3-B).5
The exci ed pulmonary artery is fashioned into a tube with the aid of an allograft patch if nece ary (Fig 3-B). The pulmonary trunk is then sutured to the right ventricle at the site of the ventriculotomy (Fig 3-B). This final communication may implement a non-valved Dacron conduit1 or a valved homograft. If the graft is unable to completely surround the ventricular defect a homograftpericardia! hood may be implemented to channel blood flow from the ventricle and into the pulmonary artery (Fig 3-C).
Post-Operative Mortality The morbidity associated with the repair of Truncus
A rteriosus has certainly been reduced with recent technological innovations that improve the surgeon's ability to maintain an infant on cardiopulmonary bypass. However, one of the most significant factor contributing to a reduction in mortality for repair of this condition is the indication that such repair be performed before the patient reaches ix months of age. 5
•11
•1 In this way, a
s ignificant contributor to early death, pulmonary morbidity due to protracted pulmonary hypertension, can be preempted with early repair of the defect.
While a patient age of le s than six months of age is de irable for reducing mortality, more stringent requirements may be necessary for minimizing morbidity. Hanley et al. reported that morbidity, a indicated by pulmonary hypertension, was increased by postponing surgery beyond 1 month of age.11 While not an immediate contributor to death, Hanley et al. sugge t that " ... an inten ive care unit team with less experience managing pulmonary va cular problems could theoreticallY. increa e the significance of this factor as a ri k for death." 1
The age of the patient has been demon trated to greatl y improve intermediate urvival. For repairs performed on infants less than 30 days old, survival at 1 month ha been reported at 87% and 81% at 3 months and beyond5
. Hanley et al. reported 83% of patients urviving to 4 months post-operatively and a many as 76% urviving to a late as 22 months po t-operatively.
Conclusion Truncus Arteriosus is a rare cardiac congenital defect.
While the mortality rate of the condition is very high in the untreated infant there are procedures to repair ve sel architecture which have promi ing rate of succe . The opportunity for a favourable outcome is maximized with earl y intervention as the equelae of pulmonary hypertension and the associated pulmonary morbidity can be mitigated or eliminated.
REFER£ CES
1. Sadler, T.W. Langman's Medical Embryology( 6th ed). Baltimore: Williams and Wilkins, 1990
2. Mavroudis, C., Backer, C.L. Truncus arterioszts. In: Mavroudis, C., Backer, C.L. eds. Pediatric Cardiac Surgery (2nd ed). St Louis: Mosby, 1994: 237-246.
3. De Leva/, M ., Persistent trt1ncus arteriosus. In: Stark, f. , De Leva/, M ., eds. Surgery for Congenital Heart Defects (2nd ed). Phiiidelphia: W. B. Saunders Co., 1994: 539-548.
4. Collett, R. W., Edwards, j.E., Persistent truncus arteriosus: a classification according to anatomic types, Surg Ciin orth Am 1949; August: 1245~5.
5. Bove, E. L. , Lupinetti, F.M., Pridjian, A.K., Beekman Ill, R.H., Co/law, L.B., Snider, A .R., Rosenthal, A ., Results of a Policy of Primary Repair of Truncus Arteriosus in the eonate, J Thorac Cardiovasc S urg 1993; 105:1057-66.
6. de Ia Cruz, M.B., da Rocha, J.P., An ontogenetic theory for the explanation of congenital malformations involving the truncus and conus, Am Heart J 1956; 51 : 782-805.
7. Van Praag, R., Van Praag, S., The anatomy of common aorticapz1lmonary trunk (truncus arteriosus communis) and its embryologic implications, Am J Cardiol1965; 16:406-425.
8. Kirby, M.L., odose placode provides ectomesenchyme to the developing chick heart in the absence of cardiac neural cres t, Cell Ti ue Res, 1988; 252:17-22.
9. Conte, S., fensen ,T., Jacobsen, J.R. , Larsen, B., Helvind, M., Lauridsen, P., Pettersson, G., Double homograft repair of truncus arteriosus witlz severe truncal valve dysfunction, Scand Cardiovasc J 1997; 31 : 245-247
10. Conte, S., Jensen, T., Jacobsen, J.R. , Joyce, F.S., Lauridsen, P., Pettersson, G., One stage repair of truncus arteriosus, CA VC, and T APVC, Ann Tlzorac Surg 1997; 63: 1781-3.
11 . Ha1zley, F.L. , Heinemann, M .K. , Jonas, R. A., Mayer Jr., j.E., Cook, N .R., Wessel, D.L., Castaneda, A.R., Repair of tnmcu arteriosus in the neonate, J Tltorac Cardiovasc Surg 1993; 105: 1047-56.
12. Sharma, A.K., Brawn, W.J., M ee, R.B.B., Truncus arteriosus, J Thorac Cardiovasc Surg 1985; 90: 45-9.
13. Imamura, M ., Drummond-Webb, f.J., Sarria, G.E., M ee, R.B.B., Improving early and intennediate results of truncus arteriosus repair: a new technique of truncal valve repair, Ann Tltorac Surg, 1999; 67: 1142-6.
14. Kirklin , f. W., Barratt-Boyse, B.G., Truncus arteriosus, In: Kirklin, f. W., Barratt-Boyse, B.G., eds. Cardiac Surgery (2nd ed). New York: Churchill Livingstone, 1993.
15. Ebert , P.A ., Turly, K. , Stanger, P., Hoffman, f.l .E., Heymann , M .A ., Rudolph, A.M., Surgical treatmen t of truncus arteriosus in the first six month of life, Ann Surg 1984; 200:451-55 Q
U. W.O. Medical Journal 70 (1) 2000------------------------- 17
HISTORY OF MEDICINE EDITORS: V ADIM SHERMAN & ALuso SUI<
TAOISM AND THE CHINESE ANCIENT
ADVENT OF MEDICINE
A retro pective view of civilization has shown that cientific advancement of a ociety can only take
place if the social infra tructure allows for it. Ancient China was no exception in that the tructure of ociety and the conditions of the time were uch a to
allow for advancement in medicine. More specifically, ancient Chine e society fostered the Taoist religion, thereby allowing Taoist follower to pur ue their ultimate goal of immortality, thus indirectly advancing medical knowledge, mainly in the field of pharmaceutic .
Society wa capable of fo tering the ideas of Taoism ince the underlying belief that Chinese society
pre cribed to paralleled the paradigms of Taoism. The e beliefs were centred around the doctrine of Yin and Yang, in which ature was a ingle, unified y tern with polar and complementary aspect . When they are in balance, life i harmonious. However, when the delicate balance i up et, di a ter looms 1
• The fir t follower of Tsou Yen' philo ophy merged with the Taoi ts, who then adopted T ou Yen' ideas. Furthermore, the a pect of Taoism that dealt with the earch for immortality had originated from folk medicine3
. Thus, since the Taoi t religion conformed to prevailing ideas held in the culture, uch as that of Yin and Yang, and was born of the magico-religiou part of ociety, Taoi m wa able to progre within the ociety
generally unabated. Another parallel between social attitudes and Taoi m
that allowed it to flourish wa that both were cone rned with the idea of prevention. In ancient times, China wa a bureaucratic feudalism where great importance wa attached to the prevention of trouble both in politics and in p r onal health3
. As the term bur aucracy irnplie , th re would be little imagination on the part of government emplo ee to olve problems ince they would all be dealt with in a preordained mechani tic fashion. This then nece itated a need to prevent potential problems from ever ari ing. Prominent member of ociety, uch a Emp ror H ia Tzu-Liang, e tabli hed the first permanent ho pital in 491AD. Before uch time, ho pices had been formed only in time of locu t plague, evere drought or other type of epidemic 3
. Thi action, on the part of the Emp ror was most probably due to the prevailing attitude
ABOUT THE AUTHOR Vadim Shennan is a fourth-year medical student with
an interest in the history of medicine. He is also the recipient of 1996-1997 Rowntree Prize in Medical History.
ByVadimShennan
of prevention pre ent in ancient China. Taoism mirrored thi ba ic principle in their philo ophies of immortality4
•
By earching for immortality, the Taoi ts were concerned with keeping the health of the individual so as to prevent the occurrence of any di ease which could potentially lead to death.
By being devout Taoist , many monks were able to advance their social standing by ri ing to positions in the Emperor' s court. Since their philo ophie were favored by the ruling class, the religion wa free to develop. Their e calation through the ocial hierarchy was facilitated by the de ire of Emporer to drink the formula of life. To fulfill this desire, they enli ted the knowledge and cientific kills of the Taoi t , and with it came the open upport of the religion. The fa cination Emperor had with
Taoi t beliefs of immortality i reflected in a preface to one recipe for the elixir. It de cribe the Yellow Emporer' journey to the Taoist Chung Huang-chih to tell him that he i giving up his place on the throne to pursue Tao (the order of things) . The Taoi t philosophy was a trong current under a great number of rulers, especially from the Fir t Emperor onward through the Han dynasty. The Taoi t were favored by ruler to the point that their religion wa actively furthered.
One uch ruler, Thopa Kuei, instituted a profe or hip of Taoi m and alchem with facilities for the tudy and preparation of elixir . The Mongol , like Thopa Kuei, were al o very receptive to various Taoist practice 6
• For instance, in 1276, Khubilai i ued an edict in which he ummoned the head of the South Taoi t clergy to Shang-tu
from whence they had a formal pokesman in the capital. From this point on and until the end of Mongol rule, Taoism held a major po ition in the religious Jive of the ruler and the Taoist influence wa there in the court and government. The influence Taoi m exerted upon the court was evidenced strongly between the years 1307 and 1322, when on many occa ion there were edict i ued that demanded the protection of the Taoist religion6
. The Taoist were very capable of attaining influence in the ruling ection of society and with thi influence the Taoi t philo ophy was further fo tered .
With this fo tering by th court and their political influence a een in Mongol time , it is obviou that the religion was anything but per ecuted. A long a the religion i not per ecuted by the ruler, it is allowed to flouri h and thereby attempt to achieve its goals. Alchemy was the main occupation of the Taoi ts and it flouri hed during the Mongol rule6
• It was through these alchemical practices that the pharmaceutical knowledge of ancient China developed.
18 ------------------------- U.W.O. Medica/Journal 70 (1) 2000
------------------------- H i s t o r y o f M e d i c i n e
A con equence of the Taoi t earch for immortality wa that many recipe for the elixir of life were created, which amounted to a wealth of knowledge about "lifeprolonging drug ". Although many of the e elixir proved to be impotent, thi doe not detract from the fact that due to Taoist work in alchemy, the amount of experimentation increa ed, leading to the increa ed knowledge of drug in general. One of the thing that Taoists living in olitude occupied them elve with wa the writing of compendium of pharmaceutics. Thee b came known a the Pen-t ' ao 7
. The de criptions of elixir were followed with Taoi t monk ' to in ight and experience on how to achieve long life without aging . The Taoi t Ma Chih compiled a collection of drug by adding another 133 type to the repertory of the Pen-t ' ao, which were u ed then and now a ucce ful pre cription 7
. In another of the Pen t ' ao , one of the many recip for immortality include ulfur, which found u later in civilization a an antidote to ar enic poi oning7
.
The u e of ulfur wa one of many ucce sful drug a nd recipe that came into u e through the e perimentation of Taoi t alchemist . There were many more, one of which wa ammonium chloride. Medically, it wa u ed to timulate exp ctoration. It wa introduced by Arab , who had picked it up from their Chine e alchemical colleague . Moreover, T'ao Hung-ching, another Taoi t alchemi t, wa quick to ob erve through hi alchemical experiment that mercury wa able to change gold and ilver into a pa te . It turned out that he had di covered the principle of amalgam and this wa to have an effect on health care ince the e amalgam were then u ed for filling teeth7
.
Taoists also dabbled in iatro-chemi try, leading to further advancement in m dicine. By preparing mixtures of androgens and e trogen in a relatively purified form, they were able to treat many hypo-gonadic condition . Thi advent of medicine had come about ince exual endocrinology and pecial e ual practice had always b en one Taoi t method of attaining immortality3
.
Ev idently , Taoi m ha made a distinctive mark on medicine through con tant experimentation and development of new therapie .
Mo t of Taoist ucce in medicine wa een in pharmacopoeias, where the Taoi t philo ophy led to more work and expan ion of work on drug literature. One author of the pharmaceutical , Tang Shen-wei, combined the Chia-yu pu-chu Shen-mung pen-t ' ao and the T' uching pen-t 'ao into a ingle work that wa more practical for the practitioner. He al o in erted an additional 662 treati e of drugs and e panded the complete work by approximately 29,000 instructions for drug application . He did not write into the books any of hi own view , but in tead quoted from other author and referenced other material. ine of tho e reference pertained to other Pent 'ao , 9 were from other medical literature, one from a Buddhi t work, and 35 were from Taoi t work 7
•
The way in which the ancient Chine e ociety can be viewed then, i a a cyclical arrangement. One can tart by aying that Taoi t experiment in alchemy led to advances
in drug knowledge and other general field of medicine. However, thi would not have been pos ible, were it not
for the fact that ociety, on all levels, fostered the development of Taoism, thu allowing it to p ur ue its goal with the utmo t freedom. With this freedom, then, the Taoists were able to influence odety into ub cribing to their philo ophie , in piring them to make medical advancement with Taoi tic tendencie in mind . Therefore, just as the Taoi t believed that everything was circular and interconnected in their odety, o they proved it with their progre in medicine.
REFER£ CES
1. Beinfield H. and Komgold E., Between Heaven and Earth, Ballantine Books, ew York, 1991 .
2. Breuer H., Columbus was Chinese, trans. Sa/valor Attanasio, Herder and Herder, ew York, 1970.
3. eedham f. , Clerks and Craft men in China and the West , Cambridge Univer ity Press, Cambridge, 1970.
4. Yoke H. P. , Li, Qi and S/111, University ofWa lrington Press, Seattle, 1985. 5. Tamba Y. , The Essentials of Medicine in A ncient China and japan ,
Iran . E. Hsia, I. Veith, and R. Geert ma, Leiden, etherlands, 1986. 6. Langlois ]. D., China Under Mongol Rule, Princeton University Press,
Princeton, 1981 . 7. Unsclruld P., Medicine in China, University of Califomia Pre , Los
Angeles, 1986. 8. Ronarr C. and eedham ]., Tire horter Science and Civilization in China,
v. 2, Cambridge University Press, Cambridge, 1981 . Q
WILLIAM Etobicoke Hospital Campus
OSLER Brampton Memorial Hospital Campus
HEALTH Georgetown Hospital Campus
CENTRE www.williamoslerhc.on.ca
CO GRATULATIONS! UNIVERSITY OF WESTERN ONTARIO GRADUATING MEDICAL STUDE TS
2000
Our promi eat William 0 ler Health entre is that we will ne er
forget why we' re here ...
To care for people and to care about people.
We' re proud of our hi tory, our kill and our expeni e.
We' re proud to be pan of our community; and
We ' re proud to be building the tronge t health centre in the Province.
We believe that there i only one way of doing thing - the be t way;
and we will be a leader in hea lth care by committing to that attitude.
FOR ORE INFORMATIO ABOUT MEDICAL OPPORT ITI E AT WILL LAM 0 LER HEL TH CENTRE PLEA E CONTACT:
DR. TOM DICKSO CHIEF OF T AFF
(90 -) 796-446 I tom_dickson oslerhc.org
U. W.O. Medical Journal 70 (1) 2000-------------------------- 19
PROMOTION AND PREVENTION EDITOR: DAN MENoo c;A & ALBINA VELTMAN
PSYCHOSOCIAL RECUPERATION FOLLOWING CARDIAC SURGERY
Cardiac surgery and angioplasty have advanced to the point where fatality rates for these procedures, performed electively in patients under 70 years of
age, are less than 2% in many medical centers 1•
Unfortunately, there are patients who do not benefit to the extent that would be expected from successful surgery. For these patients, a poor social outcome is associated with lingering somatic complaints and a lack of confidence concerning physical exertion. These patients do not engage in activities of the type that their improved cardiac tatus might allow. Poor psychosocial adaptation is also linked with social isolation and low compliance with medical and exercise regimens 2•
It is well known that psychological distress figures prominently in a patient's rehabilitation following surgery for cardiac disease. Timberlake et al (1997) provide the following benchmarks regarding the pattern of depre sian after such surgeri: Eight days following surgery, SO % are depressed due to discomfort, pain, and estrangement from the home setting. At eight weeks, 24 % and at twelve months, 22% are still depressed. Given, for example, that most coronary bypass patients at London Health Sciences Centre (LHSC) will be discharged post-operatively after five days or less, this means that many will have to cope with depressive symptoms at home. Depre sive symptoms increase the probability of visits to the emergency department and frantic calls to h ealth professionals on account of a cognitive state of helplessness and other symptoms involved in depre sian. Similarly, a sub-clinical level of pessimism involving negative self-perception has been found to be associated with a reluctance to return to work and a reduction in leisure activities4
•
Using a prospective sample of patients admitted for coronary angioplasty and coronary artery bypass, Levine et al (1996) found that both psychological depression and disease severity predicted the number of days of rehospitalization when patients were followed fo r six months after discharge5
. Statistical analysis revealed the independent contribution of psychosocial variables (in particular, in predicting frequency of patient symptoms) after indicators of left ventricular function (e.g. angina, dyspnea and fatigue) had been controlled fo~. With this in mind, it should be possible to improve our abili ty to predict which patients will recover well and which will recover incompletely after heart surgery.
A recent study has found that patients with less severe disease pre-operatively may be more prone to depre sion following surgerr. It is possible that those patients who were most incapacitated prior to surgery received the greatest relief from their operation. Alternatively, patients
By Dan Mendonca
who were under the impression that their disease severity was not very serious may have been ill-prepared for the subsequent incapacitation. Langosch et al (1992) reported that patients who perceived their operation as a purely technical event (avoiding emotional involvement) were more depressed post-operatively6
. It is important, therefore, to take into account patients' expectations and their understanding of the extent of their disease.
During the early phase of recovery, there is heightened somatic concern and anxiety. Anxiety, in this case, results in activation of the sympathetic nervous system, a key modulator of cardiovascular function. Strategies aimed at inducing a relaxation response might be useful during this initial phase. Unfortunately, a h igh level of anxiety provides the motivation for relatively swift learning of maladaptive conduct. A perceived reduction in fear reinforce negative behaviours such as phobic responses, superstitious acts, and avoidance behaviour 7•
With reference to social disability, it has been found that 50 % of marriages may deteriorate after a myocardial infarction . This might be due, in part, to changes in role imposed during the recovery process which often affect self-esteem. Patients and family could benefit from the opportunity to interact with well-adjusted former patients to develop positive expectations regarding the future.
Patients report experiencing pecific problems of emotional adjustment following cardiac surgery. In a study involving focus groups of former patients, Border et al (1985) report the following 9
: i) going through a "downer" (e.g. crying for no reason, memory problems, crying because one cannot return home), ii) feeling fearful on leaving the security of the hospital, iii) fearing they will appear less attractive to their partners on account of their scar. Patients may go through different phases in terms of accepting emotional support. Some patients may prefer to "crawl into a hole" and wait while they either "die or get better" . Others opt to have family milling about them, talking and doing all kinds of things.
Chest pain is perhaps the major symptom that concerns patients, spouses, and personnel. Patients should be encouraged to mentally review the experience of chest pain and its implications6
• Medical staff can clarify misconceptions and provide new information to aid patients in appraising their physical condition. Patients can be taught to notice whether they change their rate of breathing, tense up specific muscles, change their posture, or focus on specific thoughts during the experience of chest pain. Techniques which can be used to counteract the anxiety associated with chest pain include breathing exercises, deep muscle relaxation techniques, imagery, and diversion (e.g. focusing on the idea that the pain will
20 ------------------------- U. W.O. Medical Journal 70 (1) 2000
quickly pass t One of the key ingredient of depre ion following
urgery is " learned helplessne s"-ie, a belief that the patient cannot meaningfully alter their own recovery. With respect to counteracting this effect, two major foci have been identified: symptom reporting and activity progression6
• Both strategies are directed at helping patients regain a sense of personal control. In the fir t case, patients can be taught specific vocabulary which allows them to accurately describe bothersome symptoms (eg, chest pain). Positive reinforcement is given to patients when de criptors give clear information about the pain experience. Pain in the chest wall, for instance, can be readily differentiated from anginal pain. In the second instance, patients can be taught to assess the body's respon e to exercise and thu participate in planning activity progression. This might involve taking the pulse before and after specific activitie . In this context, fatigue, shortness of breath and chest pain might be viewed as indicators of the body' s slowly improving response to exercise (rather than imminent threats) . The patient experiences a sense of control in helping to determine when their heart can successfully manage a particular load.
In addition to monitoring physical symptom and activity progression, patients can be taught ways to better manage recurring worries regarding their future . These thoughts lead to changes in mood which can impact on a patient's ability to improve. The cognitive technique of " thought stoppinf is one which can be used to arrest such ruminations 0
. Patients may also be disturbed by fluctuations in affect which are commonly experienced following heart attack. Counselor might be used to help patients articulate their troubling feelings and place them into perspective.
Interventions designed to promote patients' perception of control are one approach to improving psycho ocial recovery following a cardiac event. Patients' perception of control (relating specifically to their cardiac disease) appears to be adaptable (amenable to change) and, indeed, predictive of later psychosocial recovery. In studies where patients were involved in planning a pects of their own rehabilitation programme, psychological distre s was found to decrease a perceived control among patients increased2
•
Artinian et al (1995) sought to determine whether phy icaJ, psychological or social recovery differ for men and women during the first six weeks following coronary artery by pass 11
. Women in the study reported a significantly higher number of physical symptoms. This wa especially true for activities involving ambulation. Women al o had more ymptom of depre sion than men. (It is worth noting that female patients were more likely to be without a spou e.) Importantly, female patients experienced lengthier recoverie and were less likely to have adequate spou al support (e.g . with home management activitie ).
In recent year , controversy has ari en over the i sue of long-term psychological maladjustment in patients following open-heart surgery. While Timberlake et al (1997) confirm an increase in the prevalence of depre ion following surgery, they report an eventual decrease in
Promotion & Prevention
prevalence to a level below that een prior to surgery 3. Perhaps patients' improved cardiovascular function following surgery can account for the long-term decline in depressive symptoms.
Beck et al (1995) report that the crucial component of depression may be the cognitive dimension 1 · Further investigation is needed to elucidate the course of depression and artXiety, particularly the cognitive core, following cardiac surgery. (The cognitive core refers to perceptions of diminished self-worth, helplessness and pe sirnism regarding the future). Providing interventional therapy for all patients receiving open-heart surgery would be both expensive and time-consuming. It may be possible, however, to identify those patients who may be at risk of showing poor postoperative psychological adjustment.
SUMMARY Although most patients experience a successful
psychosocial recovery following cardiac surgery, a significant proportion experience persistent distress which impacts negatively on physical well-being and reintegration into ordinary work, leisure, and domestic activities. The potential economic benefit of assisting the psychosocial recuperation of such patients is substantial. Fundamental information regarding the mechanisms of emotional maladjustment could prove indispensable to the cardiac care team. This should continue to be an area of focus for cardiac rehabilitation re earch.
REFERE CES
1. Jenkins CD, Stanton BA, Jono RT. (1994) Quantifying and predicting recovery after heart surgery. Psychosomatic Medicine. 56: 203-212.
2. Moser DK. Dracup, K. (1995) Psychosocial recovery from a cardiac event: The influence of perceived control. Heart and Lung. 24(4): 273-279.
3. Timberlake , Klinger L, Smith P. (1997) Incidence and patterns of depression following coronary artery bypass graft surgery. Journal of Psychosomatic Research. 43: 197-207.
4. Pimm J, Feist J. Psychological risks of coronary bypass surgery. ew York: Plenum Press, 1984.
5. Levine JB , Cov ino A , Slack WD. (1996) Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. Journal of Cardiopulmonary Rehabilitation. 16: 109-116.
6. Langosch W, Sc/mroli-Fiockerzier H. Psyclwlogical reactions to open heart surgery: Results of a quantitative and qualitative analysis of the recavery process . In : Walter PJ (ed), Quality of life after open heart surgery. Dordrec/rt: Kluwer,1992.
7. Runions, J. (1985) A program for psychological and social enhancement during rehabilitation after myocardial infarction . Heart and Lung. 14(2): 117-125.
8. Wishnie HA, Hackett TP, Cassem . (1971) Psychological hazards of convalescence following myocardial infarction . Jou rnal of the American Medical Association. 215: 1292.
9. Border, C. (1985) "By God, I made it": When the bypas patient return home. Patient Care. 7: 47-93.
10. Rimm DC, Masters JC. Behavior Tlrerapy. ew York: Academic Press, 1979. Chapter 9.
11 . Artinian T, Duggan CH. (1995) Sex differeences in patient recovery patterns after coronary artery bypass surgery . Heart and Lung. 24(6): 483-494.
Beck AT, Rush A. Cognitive therapy. In H.I. Kapla n &B.J Sadock (Eds ), Comprelrensive textbook of psychiatry. Baltimore: Williams & Wilkins, 1995. fl
U. W .O. Medical Journal 70 (l) 2000------------------------- 21
FEATURE ARTICLES
A REVIEW OF NEW MARKERS
CARDIAC
INTRODUCTIO
I n the emergency room etting, early diagno i i important in the initial treatment and management of patient presenting with acute on et of che t pain .
Early monitoring in the coronary care unit and the u e of thrombolytic therapy greatly decrea e morbidity and mortality1
• Diagno i ha traditionally been ba ed on clinical history, physical examination, and electrocardiographic (ECG) findings. When World H alth Organization (WHO) criteria (pre entation of che t pain over 20 minute , evolutionary chan§e on the ECG, and abnormal level of cardiac enzyme ) are used to da ify patients with uspected myocardial infarction, only 50% of all che t pain ufferer admitted to the CCU are confirmed a having thi condition. Although the ECG can be performed ea ily and rapidly, pecific change may be ab ent or inconclusive in the early hour in about half of the patient arriving at ho pita] with acute myocardial infarction (AMI)3
. Furthermore, approximately 2% of patient with AMI are inadvertently ent home4
• It i for this rea on that mea urement of biochemical marker of myocardial mu de cell damage play an important role in the diagno i of AMI.
In the pa t, te t for lactate dehydrogena e, aspartate transaminase, and creatine kina e were developed and widely u ed . The e te ts were later replaced by newer technology uch a minicolumn and electrophoretic eparation methods for mea uring the erum CK-MB
i oenzyme, a more cardiac- pecific marker5. But the e
traditional cardiac marker (total CK and CK-MB activity) do not aid in the early diagno i of AMI becau e they peak too late and are not pecific for cardiac injury. In r cent years, the earch for more en itive and pecific marker of myocardial infarction ha brought about a new generation of biochemical cardiac markers such a the rna concentration assay of CK-MB, CK i oforms of the i oenzyme CK-MB (MB2 / MB1 ratio), myoglobin, and troponin I and T. In the following review article, the e new biochemical markers will be examined.
MYOGLOBI Myoglobin, an oxygen-binding cyto olic protein of
low molecular weight, is normally found in cardiac and keletal mu de. When necro i of the e mu des occur ,
myoglobin is relea ed into the erum and can be detected by radioimmunoa ay as early as 1-4 h after cell death with a peak between 4-12 hour and a return to norma118-24 h later6
•7
• Woo concluded that becau e myoglobin i an early and en itive marker of necro is, it i valuabl for early detection and exclusion of AMr. However, becau e myoglobin i al o found in keletal mu cle, it ha poor
By orman Mah
pecificity, and can lead to many fal positive in patients pre enting with keletal mu de trauma. Some re earcher have sugge ted simultaneous mea urement of a keletal mu de pecific marker, carbonic anhydra e Ill to re olve thi limitation10
.
Myoglobin ha been compared with CK-MB (activity and rna ) in a number of tudies with inconsistent finding . One tudy howed that the te t for CK-MB mass was superior to that of myoglobin ''. However, Brogan reported that myoglobin wa a more ensitive marker of myocardial necro i than CK-MB (mass) during the first 3h of pre entation in the emergency department12
• Thi wa upported by Tucker, who howed that the en itivity within 4 h of the on et of ymptoms was 78% for myoglobin ver us 63% for CK-MB mass13
• Finally, another study howed no significant difference in the performance of myoglobin compared to CK-MB rna 15
• Bakker concluded that the be t predictor of AMI within 4 h after on et of che t pain u ing WHO criteria were the combination of ECG and myoglobin14
•
Although myoglobin lacks p cificity, it early relea e sugg~ t that it may ? co~e an ~portant dia~o tic tool for triage of che t pam patients m the future 11
• 3•16
• This is support d by the fact that orne ho pita! emergency department have already in tituted the rou tine u e myoglobin to aid in triaging patients presen ting wi th chest pain (Ed. Note - LHSC-UC routinely measures myoglobin in the emergency department).
CREATINE KINASE Creatine kina e i a cardiac enzyme that is relea ed
into the blood when myocardial necro i occur . It con i ts of three i oenzyme - CK-MM, CK-MB, and CK-BB, but it i the CK-MB i oenzyme which i most widely u ed a a biochemical marker for the diagno i of AMI 16
•17
•
Specifically, erial mea urement of CK and CK-MB are u ed to diagnose myocardial cell damage and its characteri tic ri e and fail in serial measurement i nearly pathognomic for AMI. The a ay of CK-MB i oenzyme and the calculation of it percentage relative to total CK i the tandard of reference for the diagno i of AMI 1
•
Although the en itivity of CK-MB activity for AMI diagnosis is very high, cardiac pecificity is comprorni ed in patient with keletal mu cle tra um a, myocarditis, chronic renal failure, cardiac urgery, a well a rare ectopic production in patient with tumor 19
•
Thi problem ha led to effort to find more specific marker for AMI. In earlier studie , electrophoretic or chromatographic procedure were u ed to mea ure levels of CK-MB. Thi led the way for the production of CK-MB monoclonal antibodie , which were e sential in the
22 ------------------------- U. W.O. Medical Journal 70 (1 ) 2000
development of rapid and co t-effective a ay procedure using fully automated analyzer 5
. The development of automated rna a ay for CK-MB also led to improvement in clinical en itivity and specificity and turnaround time when com~ared to catalytical determinations done in the pa t11
• 7
• However, CK-MB i not a perfect biochemical marker becau e -12 h may be required after the on t of ymptoms for the test to be elevated above normal and yield a high en itivity and specificity 19 (although CK-MB has been noted to rise earlier in orne patient with large infarcts). Another major drawback is that CK-MB mas concentration ha been hown to increase in the first 48-72 h with a return to
normal within 72 h after the on et of chest pain in patient with known AMI. This leaves a relatively short diagnostic window of only 2-3 day 22.23
.
CK ISOFORMS OR SUBFORM In addition to the three i oenzymes of CK, both CK
MM and CK-MB can be metabolized by enzymatic cleavage of the terminal ly ine amino acid from the "M" ubunit. High-voltage electrophoresis technique can be
u ed to eparate and measure CK-MB and it two i oforms - CK-MB 2 and CK-MB 1 in an attempt to improve CK-MB ensitivity in the early tages of AMI. Bhayana found that
time to po itivity of both the rna s monoclonal a ay of CK-MB and the i oform as ay were comparable, but noted greater difficulty in performing and interpreting the i oform assaf~. Hetland and Dickstein reported that the i oform ratio was the mo t en itive test in the early 0-3 h after the onset of chest pain and at adrnis ion to ho pital15
•
In the following 3-5 h, no ignificant difference among the ensitivitie of myoglobin, CK-MB i oform ratio and CK
MB mass concentration wa found 15• Puleo performed a
tudy comparing CK-MB activity with CK-MB i oform in diagno ing AMI and ha recommended widespread CKMB i oform testing after finding reliable detection of AMI within the first 6 hour after the onset of symptoms25
.
However, no study comparing CK-MB rna with CK-MB i oform has been done at the pre ent time.
There are some disadvantages to u ing CK-MB i oform te ting. The time to perform isoform quantitation, difficulty of the procedure, lack of a practical 24-hour tat a ay, difficulty in interpretation, a well a high co t will restrict the wide- pread implementation of this te t until further development are made.
TROPONIN
The troponin complex play an important regulatory role in the contraction of triated muscle. Thi complex con i t of three protein ubunit -troponin C, which bind to calcium and regulate contraction, troponin I, which inhibits actomyo in A TPa e, and troponin T, which bind the troponin complex to the tropomyo in strand22
•
Troponin T and troponin I have amino acid sequences that differ in skeletal and cardiac muscle at various location 22
• Antibodie have been developed which recognize the e cardiac- pecific equence , and it i the e antibodies which form the ba i for cardiac troponin T (cTnT) and cardiac troponin I (cTnl) immunoa ays22
•
Troponin C cannot be utilized a a cardiac-specific marker
Feature Articles
b ecau e it amino acid es uence i identical in both keletal and cardiac mu cle . CTnT differ from cTnl in
that the former i found in great amounts in the cyto olic pool and has a longer life pan in the bloodstream. Cardiac troponin T al o ha a lower ab olute cardiac pecificity than cardiac troponin I19
•
Quantitative as ay for both cTnT and cTni te t have been hown to be more en itive and pecific than CK-MB for the diagno i of AMI 19
• The enhanced pecificity allow for more accurate diagno i of cardiac injury, especially when keletal mu cle trauma is pre ent. As well, troponin level remain elevated up to 7-14 days after an AMI 1
•
Thu , troponins can be mea ured long after myoglobin and CK-MB have returned to normal levels. This broader diagno tic window i advantageous in the minority of p a tient who delay eeking medical care becau e of equivocal ymptoms or other rea ons. However, the fact that troponin can detect cardiac damage days after infarction limit it ability to detect reinfarction.
A recent pro pecti ve tudy examined the use of a rapid, qualitative troponin T and troponin I te t in patients arriving to the emergency department with acute che t pain . The result indicated that no patient was inappropriately di charged when the troponin T bed ide te twas routinely u ed3
. Furthermore, when patient were te ted 6 h after the on et of pain, 94% of patient with MI and without ST-segment elevation had a po itive troponin T te t, and 100% had a po itive troponin I te . Although the diagno tic pecificity of the e tests were omewhat low, the e figures are nonetheless significant.
Cardiac troponin T has been recognized as a highly en itive and pecific a ay for AMI in a number of tudie 23
.26. Wu demonstrated in their tudy that cTnT wa a ensitive marker of myocardial damage during the fir t 6 h, and wa comparable with the "gold standard" CK-MB mas a ay. After thi time, the clinical sensitivity of cTnT urpa ed that of CK-MB because of the prolonged relea e
of cTnT into the blood 23. The same study, however
reported a diagno tic pecificity for cTnT of only 46%, a lower pecificity than in earlier papers. Another tudy found that cTnT to be more efficient than CK-MB in determining and excluding AMI17
• Bakker found that the diagno tic ensitivity of troponin T wa much better than that of myoglobin, CK, and CK-MB activity14
.
Cardiac troponin I, unlike CK-MB, is highly specific for myocardial ti ue, and i not found in the blood of healthy individuals19
• Troponin I ha been shown to have great progno tic value. Antman examined the prognostic value of cardiac troponin I in patients with either unstable angina or non-Q-wave myocardial infarction. He found that cTni i an independent ri k factor identifying patients with un table angina or non-Q wave MI who are at increa ed ri k of death27
• The progno tic value of cTni wa found to be greater in tho patients presenting more than 6 h after the onset of che t pain27
. Antman a! o reported that there wa a direct relationship between the amount of cTni and mortality. That i , the hi:9her the level of cTni, the greater the ri k of mortality-. The e findings are ignificant in that cTni allow for the early identification of
patient at increa ed risk of death. A di advantage for troponin use is that the assay for
U. W.O. Medica/Journal 70 (1) 2000------------------------- 23
F e atur e Articl e s
troponin requires a dedicated instrument that i not widely available, as well as 90 minute for completion. Furthermore, the cost of the reagents is much higher than tho e for CK-MB. A relatively new rapid troponin test a ay, which allows the determination of troponin levels in whole blood at the patient's bedside shows some promise. It can be performed conveniently in the emergency room or in laboratories, and can potentially be used to aid in the triage of chest pain patients.
CONCLUSIONS
Early diagnosis of myocardial infarction is of great importance in decreasing morbidity and mortality, especially with recent advances in thrombolytic therapy. Although the ECG remains the standard test for diagnosing AMI and initiating thrombolytic therapy, often it is unable to guide the clinician to definitive management. Therefore, alternative diagnostic methods must be used, especially in those patients without ECG changes or with unstable angina3
. ew biochemical markers have been shown to facilitate successful intervention by identifying individuals at risk of sudden death from an ischemic cardiac event. These markers are not only useful in aiding in the diagnosis of AMI, but they ma y also have valuable prognostic utility as w ell. Specifically, cardiac troponin I is an important prognostic marker of acute coronary syndromes or unstable angina. This allows some patients to be discharged home rather than being admitted to hospital resulting in enormous savings to the health care system.
Myoglobin, CK-MB, and troponin have all been shown to be valuable diagnostic tools for reliable and rapid detection of patients with AMI Early recognition of myocardial cell death will allow appropriate triage of patients with chest pain and the selection of therapeutic strategie .
ACKNOWLEDGMENTS The author would like to thank Dr. Karl D. Theakston,
MD, for his input in preparing this paper. Dr. Theakston is an emergency physician and Chair of the Qua lity Improvement Committee at the London Health Sciences Centre, University Campus.
REFERE CES
1. GUSTO Angiographic lnve tigator . The effects of tissue plasminogen activator, streptokinase, or botlr on coronary artery patency, ventricular function , and survival after acute myocardial infarction . New England jounral of Medicine, 1993;329:1615-1622.
2. Report of the joint International Society and Federation of Cardiology/World Health Organization Task Force and Standardization of Clinical omenclah~re. omenclature and criteria for diagnosi of ischemic heart
disease. Circulation 1979; 59:607-8. 3. Gibler WB, Young GP, Hedges JR, et a/. Acute myocardial illfarction in
chest pain patients witlr non-diagnostic ECGs: serial CK-MB sampling in the emergency department. Annals of Emergency Medicine, 1992;21:504-12.
4. McCarthy BD, Beshansky JR, D'Agostino RB, Selker HP. Missed diagnoses of acute myocardial infarction in the emergency department: results from a multicenter study. Annals of Emergency Medicine, 1993;22:579-82.
5. Mercer, DW. Role of cardiac markers in evaluation of u peeled myocardial infarction. Postgraduate Medicine, 1997;102(5);113-7.
6. Cairns ]A, Missirlis E, Walker WHC. Usefulness of serial determinations of myoglobin and creatine kinase in serum compared for assessment of acute myocardial infarction. Clinical Oremistry, 1983;29(3):469-472.
7. Bhayana V, Co/10e S, Pellar TG, Jablon ky G, Henderson AR, Combination (multiple) testing for myocardial infarction using myoglobin, creatine kinase-2 (mass), and troponin T. Clinical Biochemistry, 1994;27(5):395-406.
8. Gibler WB, Runyon ]P, Levy RC, et a/. A rapid diagnostic and treatment center for patients with drest pain in the emergency department . Annals of Emergency Medicine, 1995;25:1-8.
9. Woo ], Lacbawan FL, Sunheimer R et a/. Is myoglobin useful in the diagnosis of acute myocardial infarction in the emergency department etti1rg? American journal of Clinical Pathology, 1995;103(6): 725-9.
10. Vuori ], Rasi S, Taka/a T, Vaananen K. Dual-label time resolved fluroimmunoossay for simultaneou detection of myoglobin and carbonic anhydrase 111 in serum. Clinical Clremistry 1991;37:2087-2092.
11 . Mair ], Artner-Dworzak E, Diensti A , et a/. Early detection of acute myocardial infarction by measurement of rna s concentration of creatinekinase-MB. American journal of Cardiology, 1991;68:1545-50.
12. Brogan GX, Friedman S, McCuskey C, et a/. Evaluation of a new rapid quantitative immunoassay for serum myoglobin versus CK-MB for ruling out acute myocardial infarction in the emergency department . Annals of Emergency Medicine, 1994;24:665-71.
13. Tucker ]F, Collins RA, Anderson A], et a/. Value of serial myoglobin levels in the early diagnosis of patients admitted for acute myocardial infarction. Annals of Emergency Medicine, 1994;24(4):704-708.
14. Bakker A], Koelemay M]W, Gorgels JPMC, eta/. Troponin T and myoglobin at admission: value of early diagnosis of acute myocardial infarction . European Heart Journal, 1994;15:45-53.
15. Hetland 0, Dickstein K. Cardiac markers in the early hours of acute myocardial infarction: clinical perfomrance of creatine kinase, creatine kinase MB isoenzyme (activity and moss concentration), creatine kinase MM and MB subform ratios, myoglobin and cardiac troponin T. Scand J Clin Lab Invest, 1996;56:701-13.
16. Adams JE Ul, Schedrtman KB, Landt Y, Ladenson JH, Jaffe AS. Comparable detection of acute myocardial infarction by creatine kinase MB isoenzyme and cardiac troponin I. Clinical Chemistry, 1994;40(7):1291-1295.
17. Apple FS. Acute myocardial infarction and coronary reperfusion: serum cardiac markers for the 1990s. American Journal of Clinical Pathology, 1992;97:217-26.
18. Wu AHB, Gomet TG, Bretaudiere JP, Panfili PR. Comparison of enzyme immunoassay and immru10inhibition for creati11e kinase MB in diagnosis of acute myocardial infarction. Clinical Chemistry, 1985;31:470-74.
19. Chan KM, Ladenson ]H, Pierce GF, Jaffe AS. Increased creatine kinase in tire absence of acute myocardial infarction. Clinical Chemistry, 1986;32:2044-51 .
20. Adams JE, Bodo GS, Davilla-Roman VG et a/. Cardiac troponin 1: a marker witlr lrigh specificity for cardiac injury. CirClllation, 1993;88:101-106.
21 . Alonsozana GL, Christenson RH. The case for cardiac troponin T: marker for effective risk stratification of patients with acute cardiac ischemia. Clinical Chemistry, 1996;42(5):803-808.
22. Mair J, Artner-Dworzak E, Leclrleitner P, et a/ . Cardiac troponin T in diagnosis of awte myocardial infarction . Clinical Chemistry, 1991;37(6):845-852.
23. Wu AHB, Valdes R, Apple FS, et a/. Cardiac troponin T immunoas say for diagnosis of acute myocardial infarction . Clinical Chemis try, 1994;40(6):900-7.
24. Blrayana V, Cohoe S, Leung FY, Jablonsky G, Henderson AR Diagnostic evaluation of creatine kinase-2 ma s and creatine kinase-3 and -2 isoform ratios in early diagnosi of acute myocardial infarction. Clinical Chemistry, 1993;39:488-495.
25. Puleo PR, Meyer D, Wathen C, et a/. Use of rapid assay of subforms of creatine kinase MB to diagnose or rule out acute myocardial infarction. ew England Journal of Medicine, 1994;331:561-566.
26. Kallrs HA, Sclreffold T, Noe A , et a/. Diagnostic efficiency of troponin T measurements in acute myocardial infarction. Circulation, 1991;83(3):1107-9.
27. Antman EM, Tanasijevic Mj, Tlrompson B, eta/. Cardiac-specific troponin I levels to predict tire risk of mortality in patients witlr acute coronary syndrome. New England journal of Medicine, 1996;335(18):1342-1349. Q
24 ------------------------ U. W.O. Medical Journal 70 (1) 2000
Featur e A rti c les
PREGNANCY: HYPERTENSION IN AN UNUSUAL ETIOLOGY
REPORT A CASE
Hypertension pre enting in, or being aggravated by pregnancy i a common occurrence. It is e timated that 6-10% of nulliparous women 1 will have a
pregnancy complicated by hyperten ion. If a woman develop hypertension during her pregnancy, most clinicians initially a ume the diagno i of preclampsia or pregnancy induced hypertension . It is important to remember, however, that occasionally, the etiology of a condition characteri tic or pecific to pregnancy may be the re ult of some other pathology. A ca e is presented below in which the etiology of hypertension occurring in pregnancy was an aldo terone- ecreting adrenal adenoma.
Primary hyperaldosteronism is a rare, but welldocumented disea e occurring during pregnancy. There have been less than twenty ca e reported, the majority of which were due to an adrenal adenoma. Since surgery is the treatment of choice for active adrenal tumour , it i important to document the presence of a neopla m o that it can be treated appropriately.
CASE REPORT
A 33 year old nulliparou woman pre ented to the emergency department at 17+4 weeks gestation complaining of acute onset of proximal leg weakness. This came on quite uddenly after a three week hi tory of migraine headache , vomiting, and migratory myalgias involving her lower limb bilaterally including her right hip, calf, left foot and calf. Significant past medical history includes a two year hi tory of hyperten ion and headache , for which she wa taking atenolol.
On phy ical examination, abnormal finding included a blood pressure of 190 / 110, decreased power in the hip flexor and dor iflexor at the ankles bilaterally, and pitting edema bilaterally to the knees. The only abnormal laboratory value wa a erum potas ium of 1.8 mmol / L (ref. 3.3 -3.5 mmol / L}, and U wave present on the ECG. There wa no proteinuria.
At this point, a tentative diagnosis of hyperaldosteronism was made, and the patient was admitted to ho pital. Her pota sium level was tabilized using pota ium boluses and supplements. Inve tigations in hospital included a renal ultrasound and serum aldo terone level . o adrenal masse were een, but the aldo terone level was found to be elevated at 2041pmol / L. The blood pres ure was stabilized using atenolol, and the patient was placed on potassium supplements.
At 29 week ge tation the patient had an abdominal MR1 which demonstrated a 2.5 em adenoma on the left ide. This confirmed the diagno is of an adrenal tumour; it
was concluded that the tumour was most likely secreting aldo terone.
As she continued with her prenatal care, her blood
By Andrea Lausman
pre ure was found to be high, but stable at 170/100. Her urine was normal until 33+{; weeks ge tation when she had 1 + protein on the urine dip tick. A 24 hour urine collection for protein wa done, and wa found to be within the normal range at 400mg / day. Subsequent urine dips were normal, until her antenatal vi it at 36+5 weeks, when he again had 1 + protein in her urine. Her blood pre sure was becoming more volatile at this time as well. Since the patient was non-compliant and refu ed admi sion to ho pital for fetal-maternal monitoring, she was induced at 37 weeks gestation. She had a normal labour and vaginal delivery which produced a healthy infant.
She has been sub equently referred to a surgeon for the removal of her tumour.
DISCUSSION Primary hyperaldosteronism, due mo t commonly to
adrenal adenoma or bilateral adrenal hyperplasia, is the cau e for approximately 1-2% of hypertension found in non-pregnant adult 2
• It i more common in women (2:1}, and usually occurs between the age of 30 and 50 years. However, there are les than twenty case report of aldo terone ecreting adrenal adenoma presenting during pregnancy.
The mo t common pre entation, in pregnancy as well a non-pregnancy is ymptoms of fatigue, muscle weakness, nocturia, lassitude and headaches. Blood pressure i mildly to severely elevated. In pregnancy, however, a complicating factor may be uperimpo ed preclamp ia; it may present quite a challenge to appropriately interpret all of the clinical findings.
The laboratory value which are abnormal include a low erum pota ium, high serum aldo terone, low erum renin, and often a metabolic alkalosis . A definitive diagnosis can be made using CT scanning or MRI. Since CT scanning during pregnancy is not desirable, and MR1 is an imaging modality which is becoming more acce ible, these tumour may be identified using MRI. A renal ultra ound i often the first radiologic procedure done; however, as this ca e demonstrated, renal / adrenal ultrasound may not be helpful in making the diagnosi .
In a non-pregnant adult, the treatment of an aldo terone secreting adenoma is surgical re ection3
.
However, medical treatment, in the form of pironolactone, an aldosterone antagonist, can be used to
stabilize blood pressure and treat hypokalemia4• Other
anti-hypertensives, such a calcium channel blockers and ACE inhibitors have been tried with some success5•
Problems specific to the pregnant state ari e in the treatment of hyperaldosteronism during pregnancy. Spironolactone i known to have antiandrogenic effects in humans; as well it can cause feminization of male rat
U. W.O. Medical Journal 70 (1) 2000------------------------- 25

Feature Articles
fetu e when adrnini tered to pregnant rats, it i therefore not recommended for u e during pregnancy6
. Since urgery i the definitive treatment, it i po ible that if the
di ea e wa medically unmanageable, using antih y perten ive and pota ium upplement , then adrenalectom could be performed during pregnancf.
In conclu ion, hyperten ion during pregnancy i not an uncommon clinical finding. Although the va t majority of hypertensive, pregnant women will be diagno ed with preclamp ia, it i important to remind one elf that the differential diagno i of hyperten ion in pregnan y i quite diver e, and the ca e that one i dealing with may have a more unu ual etiology that expected.
ACKNO~EDGENrnNTS
The author would like to acknowledge Dr. A . D. Backing, M.D., FRCSC, for hi input in preparing thi paper. Dr Backing i an Obstetrician / Gynaecologi t; Dept. of Ob / Gyn and Phy iology, Division of Maternal Fetal Medicine, at the Univer ity of We tern Ontario.
REFER£ CES
1. Crmuiuglram, F. Eta/. Williams Obstetrics. Appleton & lAnge. Stamford, Comreticut. 1997: p1234.
2. Andreoli, T. Cecil Essentials of Medicine. W.B. Sauuder Company. Harcourt Brace & Company. Plriladelplria. 1997: 228-229.
3. Hsuelr, W. ew Insights into the Medical Management of Prrmary Aldosteronism. Hyperteu ion. 1986; 8: 76-82.
4. Ganguly, A . Primary A/do terorrism . The ew Errgland journal of Medicirre. 1998. 339(25): 1828-34.
5. eerlrof M ., Slrlossmau, P. Poll, D., et a/. Idiopathic A/do terorri m in Pregnancy. Tire Americmr joumal ofOb tetrics and Gynecology. 1988. 160: 1225-1226.
6. Me ina, M., Biffignandi P. , Glriga E. et a/. Pos ible Coutrairrdicatrou of Spirouolactorre during Pregnarrcy. jouma/ of Eudocrirrologic luvestigatiorr. 1979; 2:222-223.
7. Barorr, F., praue, M., Huddlestorr, f., Fisher, A. Diagrrosis arrd Surgical Treatment of Primary Aldoslerorrism in Preguarrcy: A Case Report . Obstetrics & Gynecology. 1995. 86(4Pt 2): 644-5.
8. Mile , S., Moult, P., Hoffbrarrd, B. Co111r 's Syndrome due to a ReuirrResporrsive Adrenal Aderroma. J R Soc Med. 1993. 86(5): 294.
9. Webb, J., Bayli P. Preguarrcy Complicated by Primary Aldosteronism. Soul/rem Medical jouma/.1997; 90(2) 243-5. Q
0 MERCK FROSST
Discovering today
for o better tomorrow.
Merck Frosst Canada & Co. , Kirkland, Quebec Telephone: (514) 428-7920 www.merckfrosst.com
sanofi-synthelabo
Sanofi- Synthelabo, a global
healthcare company built on the successes
of an innovative worldw ide R&D
organization, congratulates the 2000 graduates
for all their passion and commitment.
* f'\a~~ers ·-. Because H eal~h
L'esse n tie/ c ' est I
a sa '"'te
Sanofi-Synthelabo, un groupe
pharmaceutique global, construit grace aux
succes d'une Recherche mondiale
innovante, tient a fEdiciter Jes diplomes 2000
pour leur passion et leur engagement.
26 ------------------------- U. W.O. Medical Journal 70 (1) 2000

Feature A rticles
FACTOR V VENOUS
LEIDEN MUTATION AND THROMBOEMBOLISM
Venou thrombo i i a multicau a] di ea e in which genetic and acquired ri k factor interact in an individual to determine whether or not a
thrombotic event will occur at a pecific point in time. 1
Recently, the Heart and E trogen Replacement Study (HERS), the fir t major placebo-controlled clinical trial of hormone replacement therapy (HRT) in the econdary prevention of coronary heart di ea wa published. Over an average of 4.1 years of follow-up, HRT failed to reduce the overall rate of coronary heart di ea e event , but increa ed thromboembolic events (a econdary outcome mea ure) by 2. 9 time .2 In the pa t five year , advance in the genetic of thrombo i have re ulted in the elucidation of novel coagulation abnormalitie that predi po e to venou thrombosi . In particular, a defect in the hemo tatic pathway, called activated protein C (APC) re i tance, and it underlying mutation, factor V Leiden, were found to be common in the population (3% to 7%) .3. 1 0. 1 ~ . 15, 1 6
They are a ociated with ubstantially higher ri k of venou thromboemboli m among patient with a coexi tent predi po ition for thrombo i , uch a advanced age, u e of oral contraceptive , hyperhomocy teinemia, and deficiencie of protein C and protein S.3 To date, the thromboembolic ri k in po tmenopausal women with the factor V Leiden mutation ha not been tudied. The intent of thi review is to e tabli h a rationale for research into the po ible a ociation of venou thromboemboli m in po tmenopau al e trogen u r and the APC re i tance phenotype, or the factor V Leiden mutation.
Risk Factors for Venous Thrombosis Ri k factor for venou thrombo i are different from
those for arterial thrombosi , and are cla ified into genetic and acquired ri k factor . Many acquired ri k factors for venous thrombosi have been identified, uch a pregnancy, the puerperium, immobilization, urgery, trauma, lupu anticoagulant, malignant di ea e, and female hormone .1 For example, oral contraceptive u e i a ociated with a four-fold ri k for venou thrombo i above ba eline.6 The ri k of venou thromboemboli m with hormone replacement therapy are also welle tabli hed. Prior to the HERS trial, re earcher in Britain and in the United State found relative ri k estimate for venou thromboemboli m in current u er of hormone replacement therapy of 3.5 and 3.6, re pectively, compared with non-u er or pa t-u ers.~.s
ABOUT THE AUTHOR Chantal Vaidyanath is a third-year medical student at
the University of Western Ontario. Before entering medical school, she completed a BS c. in Biochemistry at the University of Ottawa.
By Chantal Vaidyanath, BSc.
The genetic ri k factor for venous thrombo is include di order of the clotting y tern, uch a protein C and protein S deficiencies, antithrombin III deficiency, prothrombin 20210A, hyperhomocysteinemia and re i tance to activated protein C.1 Re i tance to APC wa fir t de cribed in 1993 by Dahlback et al, and it ha been ub equently hown that in the majority of ca e , it i
caused b what is now known a the factor V Leiden mutation.
Activated Protein C Resistance and the Factor V Leiden Mutation
In the protein C / protein S pathway of coagulation inhibition, protein C i activa ted (ie becomes an active protea e) when it bind to thrombomodulin, an endothelial membrane protein.9 On a pho pholipid urface, activated protein C, in the pre ence it cofactor,
protein S, and calcium ion , inhibits coagulation by proteolytic cleavage of activated factor V and VIII, thu mainly acting on the feed-back activation of the intrin ic pathway of coagulation.10·11 (Fig. I). The factor V Leiden mutation involve a single adenine-for-guanine point mutation in the gene encoding for coagulation factor V which lead to the replacement of arginine by glutamine at po ition 506. This po ition i one of the three cleavage ite on factor V for APC, and thu the mutation cau e the activated form of factor V (Va) to be degraded at a slower rate than normal factor Va.3 Thi results in the APC re i tance phenotype, which cau e increa ed thrombin forma tion and a lifelong hypercoagulable tate.12 The factor V Leiden mutation is inherited in an auto omal dominant fa hion. 10 In 1997, the pre ence of a factor V genetic component other than factor, the HR2 haplotype, was de cribed in patient who did not have the VRSOOQ mutation. This genetic component, i also able to contribute to the APC re i tance phenotype in patient with venous thromboemboli m. 13 The original factor V R506Q
mutation will be the focu of thi review, however, becau e it has been tudied exten ively, and henceforth, u e of the term " factor V Leiden mutation" will refer to the VRSOOQ mutation.
Unlike other inherited defect of hemo tasis, such as protein C and S deficiencie , and antithrombin III deficiency, factor V Leiden mutation is common. The carrier frequency of factor V Leiden mutation in healthy control populations ranges from 3% to 7% in Europe and the United States and may be as high a 15% in orne elected group . 1 0· 1 ~ · 1 5· 16 It is mo t prevalent in white
per ons (5.27%) and i notably uncommon in Asian and African populations, a fact that may explain the decrea ed ri k for venou thromboembolism in these groups. 17·1
Factor V Leiden Mutation and Risk of Venous Thromboembolism
In referral populations of patient with venou
U. W.O. Medical Journal 70 (1) 2000------------------------- 27
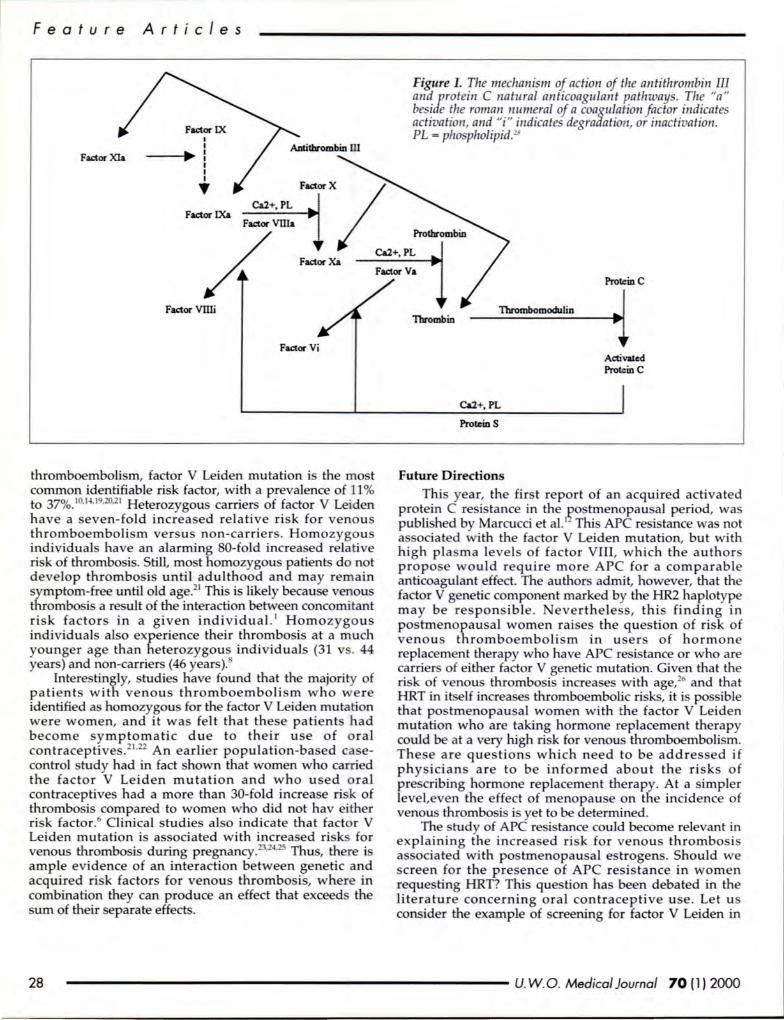
Fea tur e
Fac:tor Xla
A rti c l es
I I
---t ... P: I I I • Ca2+, PL
Fac:tor IXa
Fac:tor X
Figure I. The mechanism of action of the antithrombin III and protein C natural anticoagulant pathways. The "a" beside the roman numeral of a coagulation factor indicates activation, and " i " indicates degradation, or inactivation. PL = phospholipid.28
71Ca2+, PL I
Fac:tor Xa a
Fac:tor Vllli Thrombomodulin
Protein c
1 Fac:tor Vi
thromboemboli m, factor V Leiden mutation is the mo t common identifiable risk factor, with a prevalence of 11% to 37%. 10
•14
•19.20.21 Heterozygous carrier of factor V Lei den
have a even-fold increa ed relative risk for venous thromboembolism versu non-carriers. Homozygous individuals have an alarming 80-fold increased relative risk of thrombo is. Still, mo t homozygou patient do not develop thrombosis until adulthood and may remain symptom-free until old age.21 Thi is likely becau e venous thrombo i a result of the interaction between concomitant risk factors in a given individual. ' Homozygous individuals al o experience their thrombo i at a much younger age than heterozygous individuals (31 v . 44 year ) and non-carriers ( 46 year ).
lntere tingly, studies have found that the majority of patient with venous thromboembolism who were identified as homozygous for the factor V Leiden mutation were women, and it was felt that these patients had become ymptomatic due to their u e of oral contraceptive .2
1.22 An earlier population-based ca e
control tudy had in fact shown that women who carried the factor V Leiden mutation and who used oral contraceptive had a more than 30-fold increase risk of thrombo is compared to women who did not hav either ri k factor. 6 Clinical studies al o indicate that factor V Leiden mutation is associated with increased risk for venous thrombosis during pregnancy.23.24
.25 Thus, there i ample evidence of an interaction between genetic and acquired risk factors for venous thrombosis, where in combination they can produce an effect that exceeds the sum of their separate effects.
Thrombin
Ca2+, PL
Proteins
Future Directions
Activaled Protein c
This year, the fir t report of an acquired activated protein C resistance ~ the ~o ~enopaus_al period, wa publi hed by MarcucCI et al. 1 Thi APC resistance wa not a ociated with the factor V Leiden mutation, but with high pia rna levels of factor VIII, which the author propo e would require more APC for a comparable anticoagulant effect. The author admit, however, that the factor V genetic component marked by the HR2 haplotype may be responsible . everthele s, thi finding in postmenopausal women rai es the question of risk of venou thromboembolism in users of hormone replacement therapy who have APC resi tance or who are carriers of either factor V genetic mutation. Given that the ri k of venous thrombosis increa e with age,26 and that HRT in it elf increases thromboembolic risks, it i po ible that po tmenopau al women with the factor V Leiden mutation who are taking hormone replacement therapy could be at a very high risk for venous thromboembolism. The e are question which need to be addressed if phy icians are to be informed abo ut the risks of pre cribing hormone replacement therapy. At a simpler level,even the effect of menopause on the incidence of venous thrombosis is yet to be determined.
The study of APC resistance could become relevant in explaining the increa ed ri k for venous thrombosi associated with postmenopausal estrogens. Should we screen for the presence of APC resistance in women reque ting HRT? This que tion has been debated in the literature concerning oral contraceptive use. Let us consider the example of creening for factor V Leiden in
28 ------------------------ U. W.O. Medical Journal 70 (1 ) 2000
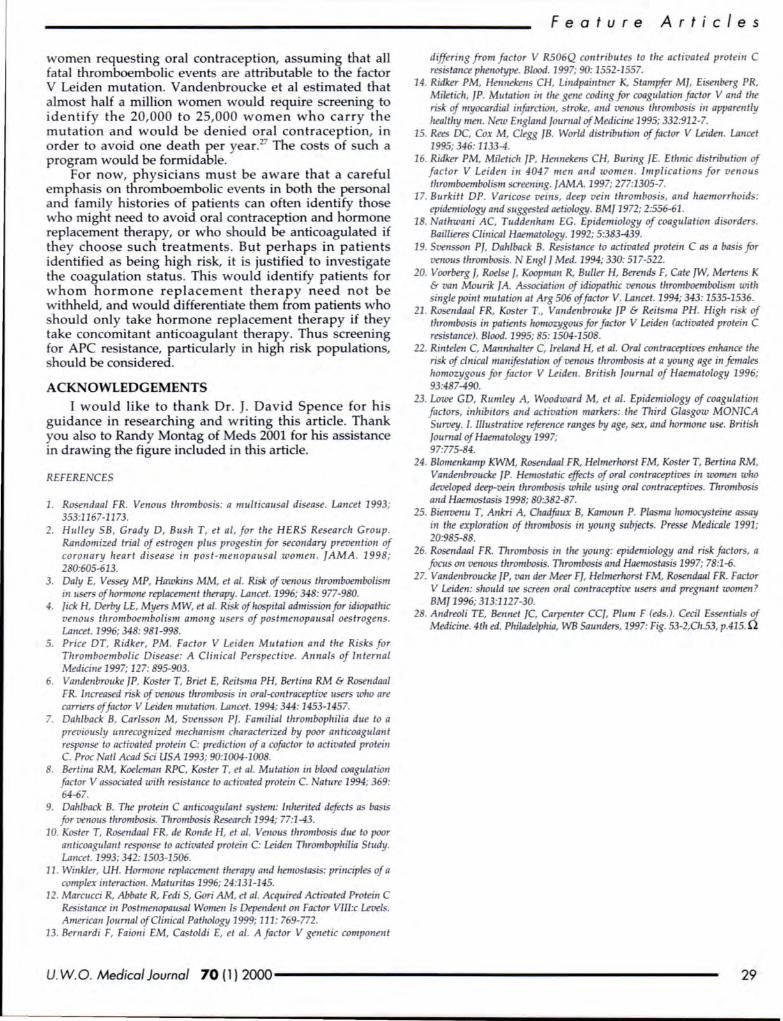
women requesting oral contraception, assuming that all fatal thromboembolic event are attributable to the factor V Leiden mutation. Vandenbroucke et al estimated that almo t half a million women would require screening to identify the 20,000 to 25,000 women who carry the mutation and would be denied oral contraception, in order to avoid one death per year.27 The costs of such a program would be formidable.
For now, physicians must be aware that a careful empha is on thromboembolic events in both the per onal and family histories of patient can often identify those who might need to avoid oral contraception and hormone replacement therapy, or who hould be anticoagulated if they choose such treatments. But perhaps in patients identified as being high risk, it is justified to investigate the coagulation statu . Thi would identify patients for w hom hormone replacement therapy need not be withheld, and would differentiate them from patients who hould only take hormone replacement therapy if they
take concomitant anticoagulant therapy. Thus screening for APC re istance, particularly in high risk populations, should be considered.
ACKNO~EDGEMlliNTS
I would like to thank Dr. J. David Spence for his guidance in researching and writing this article. Thank you also to Randy Montag of Meds 2001 for his assistance in drawing the figure included in this article.
REFER£ CES
1. Rosendaa/ FR. Venous thrombosis: a multicausal disease. Lancet 1993; 353:1167-1173.
2. Hulley SB, Grady D, Bush T, et a/, for the HERS Research Group. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in post-menopausal women. JAMA . 1998; 280:605-613.
3. Daly E, Vessey MP, Hawkins MM, et a/. Risk of venous thromboembolism in users ofhomJOne replacement therapy. Lancet. 1996; 348: 977-980.
4. Jick H, Derby LE, Myers MW, eta/. Ri k of hospital admission for idiopathic venous thromboembolism among users of postmenopausal oestrogens. Lancet. 1996; 348: 981-998.
5. Price DT, Ridker, PM. Factor V Leiden Mutation and the Risks for Thromboembolic Disease: A Clinical Perspective. Annals of Internal Medicine 1997; 127: 895-903.
6. Vandenbrouke JP, Koster T, Briel E, Reit ma PH, Bertina RM & Rosendaa/ FR. Increased risk of venous thrombosis in ora/-contraceptioe users who are carriers of factor V l..eiden mutation. Lancet. 1994; 344: 1453-1457.
7. Dahlback B, Carlsson M, Sven on Pf. Familial thrombophilia due to a previously unrecognized mechani m characterized by poor anticoagulant response to activated protein C: prediction of a cofactor to activated protein C. Proc at/ Acad Sci USA 1993; 90:1004-1008.
8. Bertina RM, Koeleman RPC, Koster T, et a/. Mutation in blood coagulation factor V associated with resistance to activated protein C. Nature 1994; 369: 64-67.
9. Dahlback B. The proteiu C anticoagulant system: luherited defects as basis for venous thrombosis. Thrombosis Research 1994; 77:1-43.
10. Koster T, Rosendaal FR, de Roude H, et a/. VenoiiS thrombosis due to poor anticoagulaut response to activated protein C: l..eiden Thrombophilia Shtdy. Ltmcet. 1993; 342: 1503-1506.
11 . Wiukler, UH. Hormone replacement therapy aud henzostasis: principles of a complex interaction. Maturitas 1996; 24:131-145.
12. Marcucci R, Abbate R, Fedi S, Gori AM, eta/. Acquired Activated Protein C Resistance iu Poshnenopausal Women I Dependent on Factor Vll/:c Levels. American journal of Clinical Pathology 1999; 111:769-772.
13. Bernardi F, Faioui EM, Castaldi E, et a/. A factor V genetic component
F ea tur e A rti c les
differing from factor V R506Q contributes to the activated protein C resistance phenotype. Blood. 1997; 90: 1552-1557.
14. Ridker PM, Hennekens CH, Liudpaintner K, Stampfer MJ, Eisenberg PR, Miletich, jP. Mutation in the gene codirzg for coagulation factor V and the risk of myocardial infarction, stroke, and venou thrombosis in apparently healthy men. New England journal of Medicine 1995; 332:912-7.
15. Rees DC, Cox M, Clegg JB. World distribution of factor V l..eiden. Lancet 1995; 346: 1133-4.
16. Ridker PM, Miletich JP, Hennekens CH, Buring JE. Ethnic distribution of factor V Leiden in 4047 men and women . Implications for venous thromboembolism screening. JAMA. 1997; 277:1305-7.
17. Burkitt DP. Varicose veins, deep vein thrombosis, and haemorrhoids: epidemiology and suggested aetiology. BMJ 1972; 2:556-61.
18. athwani AC, Tuddenham EG. Epidemiology of coagulation disorders. Baillieres Clinical Haematology. 1992; 5:383-439.
19. Svensson PJ, Dahlback B. Resistance to activated protein C as a basis for venous thrombosis. N Eng/ J Med. 1994; 330:517-522.
20. Voorberg J, Roelse J, Koopman R, Buller H, Berends F, Cate ]W, Mertens K & van Mourik fA. Association of idiopathic venous thromboembolism with single point mutation at Arg 506 of factor V. Lancet. 1994; 343: 1535-1536.
21 . Rosendaa/ FR, Koster T., Vandenbrouke JP & Reitsma PH. High ri k of thrombosis in patients homozygous for factor V l..eiden (activated protein C resistance). Blood. 1995; 85: 1504-1508.
22. Rintelen C, Mannhalter C, Ireland H, et a/. Oral contraceptives enhance the risk of clnical manifestation of venous thrombosis at a young age in females homozygous for factor V l..eiden . British Journal of Haematology 1996; 93:487-490.
23. Lowe GO, Rumley A, Woodward M, et a/. Epidemiology of coagulation factors, inhibitors and activation markers: the Third Glasgow MO ICA Survey. 1. Illu trative reference ranges by age, sex, and hormone use. British Journal of Haematology 1997; 97:775-84.
24. Blomenkamp KWM, Rosendaal FR, Helmerhorst FM, Koster T, Bertina RM, Vandenbroucke JP. Hemostatic effects of oral contraceptives in women who developed deep-vein thrombosis while using oral contraceptives. Thrombosis and Haemostasis 1998; 80:382-87.
25. Bienvenu T, Ankri A, Chadfaux B, Kamoun P. Plasma homocy teine assay in the exploration of thrombosis in young subjects. Presse Medicate 1991; 20:985-88.
26. Rosendaal FR. Thrombosis in the yo1mg: epidemiology and risk factors, a focus on venous thrombosis. Thrombosis and Haemostasis 1997; 78:1-6.
27. Vandenbro1tcke JP, van der Meer FJ, He/merltorst FM, Rosendaal FR. Factor V l..eiden: should we screen oral contraceptive users and pregnant women? BMJ 1996; 313:1127-30.
28. Andreoli TE, Bennet JC, Carpenter CCJ, Plum F (eds.). Cecil Essentials of Medicine. 4th ed. Phi/adelpltia, WB Saunders, 1997: Fig. 53-2,Ch.53, p.415. Q
U. W.O. Medical Journal 70 (l) 2000------------------------ 29

Fea tur e A rticl es
HEART DISEASE IN WOMEN: RESOLVING MISCONCEPTIONS
I n the past decade there has been a strong drive to discover the sex differences regarding heart disea e. 1
Many misconceptions have been corrected in the literature; however, men, women and their physicians alike are still not keeping abreast of new discoveries. From a physician's standpoint, educating one's patients can be one of the most effective means of preventive medicine. Unfortunately, misconceptions still prevail, allowing symptom recognition and lifestyle changes to become less effective as time passe .
What are these misconceptions and what are the facts? Heart di ease is now the number one killer of both men and women in the United States and Canada.1
•2.3 It had been believed for a long time that heart disea e only affects older women who are post-menopau al. While it is true that the effects of e trogen have a cardia-protective function, this only delays the on et of di ea e. Studies have shown that a woman's first pre entation to the health care sy tern is between three and ten years later than men on average, but the outcome for women are wor e after having a myocardial infarction.4 The e patterns reinforce the notion that women should be better educated about their risks of heart disease.
Life tyle improvements and risk factor modifications have been implemented aggressively with men, in order to reduce their prevalence of heart di ea e. This same aggressive preventive medicine should be used in affecting the outcomes that women face. Although 41% of all deaths in women are related to heart di ease, women continue to believe that their major health ri k is breast cancer. In the 1990 Ontario Health Survey, 81% of women stated their most serious health concern to be br a t cancer,5 when in reality the number of women who die from heart disea e each year is almost a great as the number of deaths in women from all cancer combined.2
These misconceptions not only give women fa ! e impressions about their general health, but their abili to modify their risk factors is severely hindered a well .
As a member of the health care system, the phy ician's role is to diagnose, treat and educate patients. Education is an incredibly important factor in successfully implementing preventive medicine protocols. When people are empowered with knowledge they are more likely to respond to ri k factor modification . Wher do mo t women receive pertinent health information? Their physicians. Herein lies another problem. A 1997 study in
ABOUT THE AUTHOR Matthew A. Crystal is in his third year of medical
school at UWO. He previously completed three years of undergraduate science at York University.
By Matthew A. Crystal
the Journal of Women's Health report that 59% of the subjects who responded believed that their primary care phy ician had inadequately coun eled them about heart di ease. Ma ny women also felt that they were never properly assessed for heart di ease risk factor .2
The e bia es have been propagated, hi torically, by the exclusion and under-representation of women in cardiova cular clinical trials.6 As national regulations have changed in the pa t decade, study populations ha ve become more repre entative of the pa tient population that are een each day. The e change have led to many large scale re earch projects that will report their finding on women's health in the early part of the 21st century.7
The goal of such projects is to correctly asse s the health ri ks of women, while correctly documenting the sign and ymptom with which they will pre ent.
What is known already? Gender difference have been de cribed in clinical presentation and in ri k factor profile . For example, re earch has shown that women uffer from heart di ea e, with an average age of onset ten
years greater than that of men. Women are more likely, however, to face a worse prognosi after a myocardial infarction than men, and their prognosi following urgical therapy for coronary artery di ease i al o wor e
than that for men. In terms of clinical pre entation, che t pain in women is not as specific an indicator for heart di ea e a is the ca e with men. This does not allow one to di rni the po sibility of heart di ease. On the contrary, a very careful history hould be elicited to ensure that the number one killer of women i not overlooked, especially becau e 50% of women with heart di ea e first pre ent with angina.
Men and women do share a lot of symptoms and risk factors, but in different ways and wi th a different emphasi . Smoking i a strong predictor of heart disease in both men and women, to the point that women who moke lo e their protective e trogen advantage and are
ju t as likely to develop heart di ea e men of the same age.1 Diabete is a prominent ri k factor for men and ha been hown to be more o in women. In term of cholesterol status, hypertriglyceridemia and low level of HDL are more predictive than total chole terol status and elevated LDL level ; the oppo ite i true for men. Another modifiable risk factor which has been ignored to a large extent in women i edentary lifestyle. Men tend to lead more active lives than women, with an a tounding 83% of women in a elf-reporting database being rated a inactive. The e difference do exi t, but many of the strategie for modifying ri k are not different.
Re earch protocols have come a long way in the Ia t ten year to actively report on women's health issue . With re pect to heart di ea e, women have been shown to have similar risk to men that should not only be recognized, but monitored and treated with pecial
30 ------------------------- U. W.O. Medical Journal 70 (1) 2000
F ea tur e A rt c l e s
empha is on the gender differences that do exist. Women have different needs than men, but the important thing to remember is that every patient who visits a doctor has their own pecial story, needs and risk factors. The most important tool that we have still remains a good, detailed hi tory. ever underestimate its usefulness.
REFERE CES
1. Thomas JL, Braus PA. Coronary Artery Disease in Women: A Historical Perspective. Archives of lntemal Medicine 1998; 158: 333-337.
2. Legato MJ, Pad us E, Slaughter E. Women 's Perceptions of Their General Healtlt , witlt Special Reference to Their Risk of Coronary Artery Disease: Results of a ational Telephone Survey. joumal of Women's Health 1997; 6(2): 189-198.
3. jadin RL, Margolis K. Coronary artery disease in women: How customary expectation can inteifere with interpretation of test results. Postgraduate Medicine 1998; 103 (3): 71-84.
4. jong P, Mohammed S, Sternberg L. Sex differences in the features of coronary artery disease of patients undergoing coronary angiography. Canadian joumal of Cardiology 1996; 12 (7): 671-677.
5. Hodgson C, jamieson E. Self-reported cardiovascular disease and risk factors: Prevalence in Ontario among women 50 and older. Canadian Family Physician 1997; 43: 1747-1753.
6. Steingart RM, Forman S, Coglianese M, Bittner V, Mueller H, Frishman W, Handberg E, Gambino A, Knatterud G, Conti CR. Factors Limiting the Enrollment of Women in a Randomized Coronary Artery Disease Trial . Glinical Cardiology 1996; 19:614-618.
7. Moser OK. Correcting Miscanceptions About Women and Heart Disease. American joumal of ursing 1997; 97 (4): 26-34. Q
Wyeth-Ayerst Canada Inc. wishes you a successful outcome in preparing for your medical career.
Venlafax in e HCI Exte nd ed Release Capsules
ANTIDEPRESSANT I ANXIOLYTIC
0 2000 Wyeth·Ayerst Canada tnc.
U. W.O. Medical Journal 70 (l) 2000------------------------ 31
F e ature Articl e s
GLYCOPROTEIN lib/lila RECEPTOR ANTAGONISTS: NOVEL ANTIPLATELET
IN CARDIOVASCULAR AGENTS MEDICINE
Coronary artery disease (CAD) is one of the leading causes of death in developed countries . The atherosclerotic plaques in CAD consist of two main
components: a fibrous cap and a lipid core. Disruption of the fibrous cap leads to exposure of the underly ing components such as lipid, foam cells, and tissue factor, resulting in platelet aggregation and ultimately, thrombus formation . This process of atherosclerotic plaque disruption leading to platelet aggregation and formation of associated thrombus defines the acute coronary syndrome (ACS), a continuum of clinical manifestations ranging from unstable angina to non Q-wave myocardial infarction or Q-wave myocardial infarction.1 Platelets are, thus, key players in the triggering of the acute manifestations of CAD.
Antiplatelet therapy, such as aspirin, has become mainstay in both the primary and secondary prevention of cardiovascular events. However, aspirin is a relatively weak antiplatelet agent since it is only able to prevent thromboxane A2-dependent platelet aggregation without any inhibition of thromboxane A2-independent aggregation. Circulating mediators for thromboxane A2-independent platelet aggregation include adenos ine diphosphate (ADP), thrombin, serotonin, and shear rate.2
In fact, more than a hundred different mechanism can result in platelet activation. Yet, regardless of the pathway chosen, all mechanisms lead eventually to a final common pathway involving the platelet surface glycoprotein llb l illa receptor.
The glycoprotein llb I ma receptor, a member of the integrin family, is the most abundant receptor on the platelet surface. For platelet aggregation to occur, a conform a tiona! change in the glycoprotein lib /I lia receptor from the inactive to the active state must occur before the receptor will bind to its primary liga nd, fibrinogen . Fibrinogen causes platelet crosslinking necessary for aggregation by simultaneously binding to the glycoprotein lib I lila receptors of two adjacent platelets.3 Thus, since glycoprotein lib I Ilia receptors comprise the final common pathway leading to platelet aggregation, blocking these receptors via antagonists
ABOUT THE AUI'IIOR Tisha Joy is a third-year medical student at the
University of Western Ontario. Prior to entering medical school, she completed a Bachelor of Science (Honours) degree in the Microbiology Specia list program at the University of Toronto.
By Tisha Joy, Meds 2001
would be an effective means of preventing platelet aggregat ion, thrombus formation, and ultimately, cardiovascular ischemic events.
Abciximab is one such glycoprotein llb I ma receptor antagonist that is currently being investigated for clinical use. It is a chimeric monoclonal an tibody Fab fragment (c7E3) tha t binds w ith high avidity to the glycoprotein lib /lila receptor as well as to the " v$3 vi tronectin receptor, which is involved in smooth muscle cell migration and proliferation.4 The fir t large-scale double blind randomized control trial to investigate the potential benefits of using abciximab to prevent cardiovascular events was EPIC (Evaluation of 7E3 for the Prevention of Ischemic Complications). This trial involved 2099 patients undergoing high-risk atheroplasty or atherectomy. All patients received a pirin as well as heparin. The patients were then randomly assigned to one of three treatment arms: 1). abciximab bolus + abciximab infusion; 2). abciximab bolus + placebo infusion; or 3). placebo bolus + placebo infusion. The treatment arm of abciximab bolus + abciximab infusion demonstrated a significant 35% reduction in the composite primary end point of death, nonfatal myocardial infarction, refractory ischemia, or urgent revascularization within 30 days, when compared to the placebo group. Only a 10% reduction was noted in the abciximab bolus group compar d to placebo. There was, however, a two-fold increase in the risk of bleeding complications and need for transfusions in the abciximab bolus + abciximab infusion group compared to control. Yet, the reduction in ischemic events noted in the abciximab bolus + abciximab infu ion treatment arm persisted at both 6 months and 3 years followup.s-7
The EPILOG (Evaluation in PTCA to Improve LongTerm Outcome with Abciximab Glycoprotein lib I Ilia Blockage) trial was conducted next to determine whether low-risk patients could also benefit from abciximab. The trial wa prematurely terminated ince the abciximab treatment group had a 57% reduction in the composite 30 day endpoint of death, myocardial infarction, or urgent revascularization as compared to control (standard heparin therapy). Interestingly, unlike the EPIC trial, there was no increased risk of bleeding in the abciximab treatment group. It was determined that the highe r bleeding rate in the EPIC trial were due to the use of high do e adjuvant heparin therapy. Thus, the EPILOG tri al demon trated two critical points: 1). The benefits o f reductions in ischemic complication from abciximab treatment could be extended to low-risk patients; and 2). The risk of bleeding complications could be decreased by using only low do es of adjuvant heparin therapy.
32 ------------------------- U. W.O. Medical Journal 70 (1 J 2000
The ability of platelet glycoprotein Ilb I rna receptor antagonists to not only prevent progre sion to myocardial infarction in patients with unstable angina but al o avoid myocardial infarction at the time of coronary intervention wa fir t demonstrated in the CAPTURE (Chimeric 7E3 Antiplatelet Therapy in Unstable Angina Refractory to Standard Therapy) trial. Patient were randomly assigned to receive either abcixirnab or placebo infu ion prior to angioplasty and continuing until 1 hour after the procedure. The trial was terminated prematurely ince there wa not only a 29% decrease in the compo ite 30 day e ndpoint of death, m yocardial infarction, or reva cularization but al o a ubstantial 71% reduction in the progression to myocardial infarction prior to percutaneous transluminal coronary angioplasty (PTCA). The re ult of this trial, thu , showed that abiciximab could a! o provide benefit for patients with unstable angina not undergoing angioplasty.9
Ba ed on the results of the above trial , it eems rea onable to con ider the po ible application of abciximab to the management of acute myocardial infarction. Animal studie have demonstrated increa ed thromboly tic activity a well a prevention of early reocclusion after reperfu ion with the admini tration of glycoprotein Ilb / illa receptor antagoni ts.10
•11 Pilot studie
w ith humans have indeed reported improved patency rate of infarct-related artery v ia increa ed peed of reperfusion, although only a small number of patients were involved.12 Based on the e encouraging re ult , the potential for using glycoprotein lib I Ilia receptor antagoni t in the management of acute myocardial infarction does certainly exist.
Abciximab i just one o f the many glycoprotein Ilb I Ilia receptor antagonists being currently studied. The ynthetic agents under inve tigation include lamifiban,
eptifibatide (Integrilin), and tirofiban which, unlike abciximab, are all specific for the glycoprotein Ilb / llla receptor alone . All four agent can only be u ed parenterally.~ Oral glycoprotein lib/lila receptor antagoni t al o exi t, including ibrafiban, xemilofiban, and lefradafiban. Trial with oral agents are currently underway to determine efficacy and afety . Thu far, tudie have reported consistent blockade of receptors
ranging from 50- 0% depending on the agent. However, the e studies have noted an increa e in mucocutaneous bleeding with the oral agent _1 3- ts Yet, the importance of the oral agent lies in their potential use in both acute ituations a well as in econdary prevention. Table 1 lists orne of the po sible indications for the oral glycoprotein
Ilb I Ilia receptor antagonists. Since the glycoprotein lib / Ilia receptor antagoni t act
a t the final common pathway required for platelet aggregation, the e antagoni t offer everal important advantages: 1) their effect on platelet aggregation will be considerably more potent than any of the other available antiplatelet agent ; 2) their efficacy can not be bypassed by redundant pathways of platelet activation; and 3) the on et of action of parenteral agent is nearly in tantaneous .16 These advantages together with the clinical trials supporting the u e of glycoprotein Ilb / illa receptor antagonist to reduce i chemic complications
F eatu r e A rt c les
Table 1 Potential Indications of Oral Inhibitors of Platelet GPIIb/llla Membrane Receptor
Acute Indications Percutaneous coronary interventions Acute coronary syndromes Unstable angina Non Q-wave Ml Ml with ST elevation
Secondary Prevention Percutaneous coronary interventions Acute coronary syndromes Stroke
Prevention of acute events in patients with stable disease
Primary prevention in high-risk individuals
Control of atherothrombosis and progression of coronary artery disease
explain the huge intere t currently in these antagonists as a novel means for combatting the acute manifestations of cardiova cular di ease, and in particular, as a possible addition to the current therapy for the acute coronary yndromes, including Q-wave myocardial infarction, non
Q-wave myocardial infarction, and unstable angina.
ACKNOWLEDGEMENTS The author gratefully acknowledge Dr. J. G .
Pickering MD PhD of the Departments of Medicine (Cardiology), Biochemi try, and Medical Biophysics for his helpful suggestions and generous contributions to this article.
REFERE CES
1. jesse RL. The platelet in acute coronary yndromes: defining the pivotal role of platelet glycoprotein Ilblllla receptor blockade. Journal of Emergency Medicine 1999; 17(3):575-580.
2. Theroux P. Oral inhibitors of platelet membrane receptor glycoprotein Ilbi/ Ila in clinical cardiology: issues and opporllmities. American Heart Journa/1998; 135 (5Pt2Su):S107-S112.
3. Lejlrovits J, Plow EF, Topol EJ. Platelet glycoprotein Ilb/llla receptors in cardiovascular medicine. ew England journal of Medicine 1995; 332:1553-9.
4. Adgey AA]. An overview of the results of clinical trials with glycoprotein llbll/Ia inhibitors. European Heart ]ouma/1998; 19(Suppl 0 ):0 10-0 21 .
5. The EPIC I vestigators. Use of a monoclonal antibody directed against the platelet glycoprotein Ilb/111a receptor in ltigh-risk coronary angioplasty. New England journal of Medicine 1994; 330:956-961 .
6. Topol E], Califf RM, Weisman HF, Ellis SG, Tcheng ]E, Worley S, Ivanhoe R, George BS, Finlel 0 , Weston M, Sigmon K. Anderson KM, Lee KL, Willerson JT. Randomised trial of coronary intervention w ith antibody against platelet llblllia integrin for reduction of clinical restenosis: results at six months. Lancet 1994; 343:881-886.
7. Topol E], Ferguson Jl, Weisman HF, Tcheng JE, Ellis SG, Kleiman NS, Ivanhoe RJ, Wang AL, Miller OP, Anderson KM, Califf RM. Long-tem1 protection from myocardial ischemic events in a randomized trial of brief integrin 3 blockade with percutaneotiS coronary intervention. ]AMA 1997; 278:479-484.
8. Tite EPILOG Investigators. Platelet glycoprotein Ilblllla receptor blockade and low-dose heparin during percutaneo11s coronary revascularization. ew England Joumal of Medicine 1997; 336:1689-96.
U. W.O. Medical Journal 70 (1) 2000------------------------- 33

F e atur e Articles
9. The CAPTURE Inve tigator . Randomised placebo-controlled trial of abciximab before and during coronary intervention in refractory un table angina: the CAPTUR E study. Lancet1997; 349:1429-35.
10. Gold HK, Garabedian HD, Din more RE, Guerrero Lf, Cigarroa ]E, Palacios IF, Leinbach RC. Restoration of coronary fluw in myocardial infarction by IV chimeric 7E3 antibody wit/rout erogenous plasminogen activators: observation in animals and humans. Circu/ation1997;95:1755-9.
11 . Raux SP, Tsclrapp TP, Kuhn H, Steiner B, Hadvary P. Effects of heparin, aspirin, and a synthetic platelet glycoprotein Ub-llla receptor antagonist (Ro 43-5054) on coronary artery reperfusion and reocc/usion after thrombolysis with tissue-type plasminogen activators in lite dog. ]. of Plrannacol Exp Tirer 1993; 264:501-8.
12. Tite IMPACT-AMI Investigators. Combined accelerated tissue-plasminogen activator and platelet glycoprotein lib/lila integrin receptor blockade with integrilin in acute MI. Results of a randomized, placebo-controlled doseranging trial. Circulation 1997; 95:846-54.
13. Camton CP, McCabe CH, Borzak S, Henry TO, Tiscltler MD, Mueller HS, Feldman R, Palmeri ST, Ault K, Hamilton SA, Rothman TM, ovotny WF, Braunweld E. Randomized trial of an oral platelet glycoprotein lib/Ilia antagonist, sibrafiban, in patients after an acute coronary syndrome. Result of the TIM112 Trial. Circulation 1998; 97:340-349.
14. Simpenforder C, Kottke-Marclrant K, Lowrie M, Ander RJ, Bums OM, Miller DP, Cove CS, DeFranco AC, Ellis SG, Molitemo OJ, Raymond RE, Sutton JM, Topol Ej. A randomized,placebo-control/ed pilot study of xemilofiban in uns table angina with percutaneous coronary interventions. Circulation 1997; 96:76-81.
15. Muller TH, Weisenberger H, Brick/ R, arjes H, Himmelsbach F, Krause f. Profound and sustairted inhibition of platelet aggregation by Jradafiban, a nonpeptide platelet glycaprotein lib/Ilia antagonist, and its orally active prodrug, lefradafiban, in men. Circulation 1997; 96:1130-8.
16. Kleiman S, Lincoff AM, Ohman EM, Harrington RA. Glycoprotein llb!Wa inhibitors in acute coronary syndromes: patlroplrysiologic foundatio n and clinical findings . American Hearl jouma/1998; 136(4Pt2Su): S32-S42. Q
Alcon® CANADA
The Vision Leader «~
Leading the Field of Ophthalmology with Therapeutic Equipment and Surgical Products.
Continually supporting the pursuit of Academic Excellence.
For firther information, please visit our website at: www.alconlabs.com
Neal, Pallett & Townsend LLP
C HARTERED ACCOUNTANTS
289 DUFFERIN A VENUE, LoNDON, 01\'T ARlO 68 I Z I (5 19) 432-5534 Fu (519) 432-6544
ADVISORS TO HEALTH CARE PRO FE SIONALS
Barrie eat Glenn Hardman
iNTEGRATED PLANNI G
FINANCIAL L"WEPENDE CE
PART ERS
David Pallett John Prueter
Jonathan Townsend L J. Sandy Wetstein
34 ------------------------ U. W.O. Medical Journal 70 (1) 2000
F e atur e A rticles
RATIONALE AND EVIDENCE BLOCKERS
THE FOR THE USE OF BETA
THE MANAGEMENT OF HEART FAILURE
IN CHRONIC
Introduction
H eart Failure i a major cau e of morbidity and mortality in orth America. The incidence of heart failure in the general population varies from 1 to 5
per 1000 per annum and can be as high as 40 per IOOO per annum for people over the age of 75 year . The prevalence ranges from 3 to 20 per 1000 for the general population and can be a high a 130 p r 1000 in people over the age of 65 year . 1 De pite the heavy burden of di ease, there i no univer ally agreed upon definition of heart failure. The diagno i is made clinically and therefore, there i no one 'gold standard' te t to confirm the diagno i .1 The primary igns and symptom include hortne of breath,
orthopnea, paroxy mal nocturnal dy pnea, fatigue, peripheral edema and elevated jugular venous pressure. Thi article will briefly discus the medical management of chronic heart failure focu ing on the role of beta blocker .
Medical Management of CHF The medical management of chronic heart failure
(CHF) i a complex undertaking and typically involves the use of multiple da e of drugs. The goals of treatment are to reduce symptoms, decrea e the number of recurrent ho pitalizations, and to improve urvival.2
Diuretic are often the firs t line treatment for acute exacerbations of heart failure . They work by reducing excessive salt and water ret ntion and therefore, decreas the preload which, in turn, re ults in a decrease in ymptom from pulmonary and ystemic conge tion.
Although the impact of long-term diuretic u e on urvival is difficult to evaluate, their ability to reduce symptom ha made them one of the mainstays of heart failure !re~t~ent. 2 Angioten in Converting Enzyme (ACE) inhibttor have made a igrlificant impact on heart failure treatment and numerous Randomized Controlled Trial (RCTs) have been conducted to evaluate their impact on urvival. It ha been found that ACE inhibitor reduce
mortality by about 23% when compared to placebo. This effect was hown to be con i tent aero all ew York Heart A ociation (NYHA) cla e and all ACE inhibitor .4
Digoxin, a cardiac glyco ide which is commonly pre cribed in heart failure, has been shown to have no
ABOUT THE AUTHOR Munir Boodhwani is currently a third-year medical
student at UWO. He previously received a BSc in human biology from the University of Toronto. He has a strong interest in cardiovascular medicine.
By Munir Boodhwani
impact on mortality but doe decrease the risk of hospitalization by approximately 30%.5 Additional drugs u ed to treat heart failure include organic nitrates, calcium channel blocker (e.g. Amlodipine), antiarrhythmics (e.g. Amiodarone), Angiotensin II receptor blockers (e .g. Lo artan), Spironolactone a well as Beta Blockers which will be di cus ed below.
Rationale for Beta Blocker Use The sympathetic nervou system has long been known
to play a sigrlificant role in the pathophy iology of heart failure. When ventricular dy function lead to a decrea e in cardiac output, there is a baroreceptor-mediated increa e in sympathetic tone, which has several con equence . ln the short term, it results in increa ed m yocardial contractility, tachycardia, arterial va ocon triction with a con equent increa e in afterload, and venoconstriction with a consequent increase in preload. Long-term activation of these compensatory mechanisms re ult in remodeling and hypertrophy of the myocardium and al o leads to myocyte toxicity, apopto is, and altered gene expression? orepinephrirle is known to be directly toxic to myocardial cell , an effect mediated through calcium overload and induction of apoptosis.6
Since the failing heart is dependent on this constant ympathetic drive, beta blockade wa thought to be
contraindicated in patients with heart failure.6•7 However,
if beta blockers can be tolerated in the hort-term, then they have been shown to have beneficial effects on ventricular function likely due to reduced myocardial toxicity. An up-regulation of P-receptor expre sion, which occur in response to treatment with a beta blocker, is al o as ociated with improved ventricular function?
Important Properties of Beta Blockers Beta Blocker have certain important characteri tics
which can affect their efficacy and u efulness. They are briefly described below:
• Cardioselec tive vs. nonselec tive-PI receptors are responsible for mo t of the cardiac effects of beta blocker wherea P2 receptor are prevalent in pulmonary ti sue. Therefore, cardioselectivity of beta blockers is imply a mea ure of the ability of the drug to more potently antagonize the PI receptor as opposed to the P2 receptor. This is al o thought to be the reason why cardioselective beta blockers are better tolerated in a thmatic patients . Bucindolol, propranolol, and carvedilol are examples of nonselective beta blockers whereas bi oprolol and metoprolol are example of cardioselective ones.
U. W.O. Medical Journal 70 {l) 2000------------------------ 35
Feat u re Art i c l es
• Lipophilicity vs. hydrophilicity-The lipophilicity o f a beta blocker allows it to penetrate the central nervous system and therefore, potentially alter the vagal tone which is already altered in heart failure.
• In ver e Agonism-Thi is a property by which an antagonist may inactivate an unoccupied active state receptor. An agent with a high degree of inv rse agonism may have a greater degree of negative inotropic and chronotropic effect.
• !SA/Partial Agon ism-A beta blocker with this property partially timulates the receptor while blocking the effects of the ympathetic nervous sy tern on the receptor.
• Ancillary properties-Carvedilol has a very prominent non-hemodynamic property i.e . antioxidant eff cts which may play a role in heart failure possibly by reducing apoptosi in myocardial tissue.9
Evidence for Beta Blocker Use Although numerous RCTs have been conducted on
heart failure patients to evaluate the effects of beta blockers on hemodynamic , exercise, and quality of life, relatively few RCTs have measured the impact of beta blockers on morbidity and mortality. The re ults of three of the major trials, which involved a large number of patients and used mortality as their primary endpoint, are discu sed below.
In May 1996, The U.S. Carvedilol Heart Failure Study Group published the results of a trial that involved 1094 patients and compared the effects of Carvedilol to plac bo. This trial was discontinued early due to the obvio us survival benefit in the Carvedilol group. The conclusions were that the relative ri k reduction (RRR) in mortality due to Carvedilol was 65% and there was also a relative risk reduction of ho pitalization due to cardiovascular cause of 27%. 10
The Cardiac Insufficiency Bi oprolol Study II (CIBIS-11), published in January 1999, studied the effect of bisoprolol (a cardioselective beta blocker) on patient wi th
YHA cla s ill or class IV heart failure. This trial was also stopped early and demonstrated a reduction in risk of mortality of 32% as well as a significant decrease in the number of sudden deaths (RRR- 44%) in patient on bisoprolol vs. placebo. Although, the effect wa consi tent across both NYHA classes, the greatest effect was een in patients with NYHA class ill heart failure at ba eline.11
The third major trial i the most recent and w as published in June 1999. Metoprolol CR / XL Randomized Intervention Trial in Congestive Heart Failure (MERITHF) tudied 3991 patients with NYHA class II - IV heart failure and was also stopped early due to a 34% reduction in all-cause mortality. It also demonstrated a significant decrease in sudden deaths (RRR- 41%) as well as deaths from worsening heart failure (RRR - 49%), which w as consistent across all NYHA classes. 12
In addition, a meta-analysis of double-blinded, placebo-controlled, randomized trials published in May 1998 combined the results of 18 trials with a total of 3023 patients . The authors concluded that beta-blockade increased ejection fraction by an average of 29% and reduced the risk of all-cause mortality by 32%. Another
important finding wa that there was no difference in mortali ty risk reduction between cardioselective and nonselective agent .13
Some Considerations
It i important to note a few characteristics pertaining to the above trials, which help determine the criteria for beta blocker use.
• In all three major trials above, beta blocker were added to standard optimal therapy, which included ACE inhibitor and diuretics. 1 0- 1~ In the Carvedilol trial, the patients were also on digoxin.10
• All p atients included in these trials were s table in terms of heart failure symptoms, regardless of the NYHA class that they belonged to.1
0-12
• The mean age of the patients included in these trials was between 58 and 63 with very few patients over the age of 75 years. 1a-12 A significant portion of patients in the general population presenting with symptoms of heart failure are over the age of 75 years.
• Since ventricular fibrillation has been documented a the m ajor cause of sudden d eath in heart failure patient , the ignificant decrease in sudden death in th e beta-blocker group u ?zges ts a po s ibl e antiarrhythmic effect of the drug.
Conclusion Beta blocker have been known for many year to
have beneficial effects in patients with coronary artery disea e . Their role in the treatment of heart failure, however, has been unclear and they have traditionally been avo ided for fear of exacerbation of the di sea e process. Recent s tudies have clearly demons trated a survival benefit of long-term beta blocker u e in addition to treatm nt with ACE inhibitors and diuretics in patient with table symptoms of congestive heart failure . Thus, beta blockers should be given to all patients with mild to moderate heart fa ilure in the absence of a n y contraindications ( evere asthma, etc). The role of beta blockers in treating YHA class IV i till unclear, and caution should be exercised when treating elderly patient (age > 75) due to lack of clear evidence. Ongoing trials are currently underway to determine the effects in these high risk group a well a in patients with asymptomatic left ventricular dysfunction.
REFERENCES
1. Cowie MR, Mosterd A, Wood DA eta/. The epidemiology of heart failure. European Hearl Jouma/1997;18:208-25.
2. john lone DE, Abdulla A , O'Amold JM eta/. D10gnosis and management of heart failure. Canadian journal of Cardiology 1994;10(6):613-31 .
3. The Task Force on Hearl Failure of the European Society of Cardiology. Guideline for the diagnosis of heart failure. European Hearl joumal 1995;16:741-51.
4. Guyatt G. A 75-Year-Old Man With Congestive Hearl Failure. JAMA june 1999;281(24):2321-8
5. The Digitalis Investigation Group. Tire effect of digoxin on mortality aud morbidity in patients with heart failure . Tire ew England Journal of Medicine Feb. 1997;336(8):525-33
6. Schrier RW, Abraham WT. Honnones aud Hemodynamics in Hearl Failure. The New England journal of Medicine Aug. 1999;341(8):577-85
36 ------------------------- U. W. O. Medical Journal 70 (l ) 2000
Feature Art cles
7. Bri tow MR. Why does the myocardium fail? Insights from basic science. Lancet1998;352(suppl 1):8-14
8. Carson PE. Beta Blocker Treatm ent in Heart Failure. Progress in Cardiavascular Diseases 1999;41(4):301-22
9. Frishman WH. Carvedilol. The ew England Journal of Medicine 1998;339(24):1759-65
10. Packer M, Bristow MR, Colm fN eta/. Tire effect ofCarvedilol 01r morbidity and mortality in patients with chronic heart failure. The ew England Jor1mal of Medicine 1996;334:1349-55
11. CJBJS-11/nvesligators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CJBIS-ll): a randomized trial. Tire Lancet 1999;353:9-13
12 . MERJT-HF Study Group. Effect of metoprolol CRIXL in chronic heart failure: Metoprolol CRIXL Randomized Intervention Trial in Congestive Heart Failr1re (MERJT-HF). Tire Lance/1999;353:2001-7.
13. Lechat P, Packer M, Chalon S, Cucheral M, Arab T, Boissel f. Clinical Effects of b-Adrenergic Blockade in Chronic Hearl Failure. Circulation 1998;98:1184-91 Q
MAKE YOUR PRACTICE PERECT AT
HOTEL-DIEU GRACE HOSPITAL- WINDSOR/ESSEX COUNTY
www.hdgh.org
Advantages: • Tertiary level programs and services in a large community hospital • $68.3M redevelopment and expansion now halfway complete which includes brand new OR's, Emergency,
Diagnostic Imaging, Renal Dialysis and I.C.U. • Southern, pre-eminent underserviced community, surrounded by world class waterfront with a rapid growing
vibrant economy • Key programs include: Trauma/Neurosciences
Contact
Cardiology including Cardiac Catheterization Renal Dialysis Vascular!rhoracic Surgery Mental Health Paediatrics Long Term Care at Villa Maria
• To find out more about our community and our team approach based on "centres of excellence" please contact: Dr. John Greenaway, Chief of Staff (519) 973-4430 Fax: (519) 973-0803 Email: [email protected]
U. W .O . Medical Journal 70 (1) 2000------------------------- 37

Feat ur e A rti c l es
PULSUS ALTERNANS: MECHANISM SIGNIFICANCE AND CLINICAL
Definition and History
Put us alternan (mechanical alternans) i the phenomenon of alternating trong and weak beat in the pre ence of regular interval . It i not
ynonymou with electrical alternans which indicate a beat to b at alternation in one or more component of the electrocardiogram. Pul us alternan wa fir t described under e perimental condition in a frog' heart over a century ago by Ga kell. 1 The clinical de cription of pul u alteman by Traube was made even earlier in 1872. Since then, alternan ha been tudied both in human and experim ntal animals and there ha been continuou debate about its underl ying mechani m and clinical igni£icance.
Proposed Mechanisms The cia ic debate about the m echanism which
precipitate put u s alternan i taged between the hemodynamic argument and the contractility argument. The former employ the concept of alternating ventricular filling and the latter, an intrin ic defect in the myocardium a a po ible factor contributing to the alternating b at . Recently, a cellular mechani m hypothe i ha emerged.
The Hemodynamic Argument
Thi argument i ba ed on the Frank-Starling mechani m that involve the alternation of ventricular filling (preload).3 A ventricular premature contraction (VPC) i one of the event that ha been ob erved to r ult in pul u altemans. It has been propo ed that although the VPC would have a relatively low ventricular filling, the beat following it would have an enhanc d troke volume and it y tole would la t longer. On the next beat, the dia tole would be horter and a a con equence, the re ulting lower ventricular end dia tolic volume would re ult in lower troke volume and aortic pre ure. This equence would continue, manife ting a alternating trong and weak pul e . Thi h y pothe is wa fi r t ugge ted by Wenckebach~ in 1902. Although there have
been orne tudie in animals and humans that support thi hypothe i ,5 recent studie again t the hypothe i have ugge ted that the hemodynamic abnormality i not the primary mechani m underlying pul u altemans.6
The Contractility Argument
Thi argument is based on the h y pothesis of an intrin ic myocardial defect that inevitably re ult in an aberrant contractility of the heart. Although it is till not clear what the ba ic mechani m of the contractile disturbance due to the myocardial defect is, a few studie on pre ure-volume relationship in an intact hea rt demon trated alternation of contractility a the primary mechani m underlying alternans.7 In a tudy on i olated
By Peter Kim
canine heart preparation , the lope of the end- ystolic pre ure-volume relation hip wa ignificantly greater than tho e of weak beat , ugge ting that alternating contractile tate i the ource of alternans.9 Alternation of ventricular filling was ob erved in the e studies, but it wa econdary to the changes in contractility.
The Cellular Argument
Alternation of the action potential duration and alternation in intracellular Ca2
+ cycling to and from the sarcoplasmic reticulum have been the ba i of thi argument. It was been uggested that alternation of action potential duration would re ult in mechanical alternans by altering sarcopla mic reticular Ca 2
+ release. There are everal line of evidence against this theory 10 and
mechanical alternan ha been a sociated with both prolonged and hortened action potentials.5 Although action potential duration doe not eem to play a major role in mechanical alternans, there i mounting evidence for the role of calcium in alteman . Recent studie have shown the phenomenon of " calcium alternans" ~alternating large and mall calcium currents in regular mterval ) a odated with mechanical alternan in i olated animal ventricular mu cle.10
•11 Thi ob ervation upport
the role of Ca 2+ as the principal factor in mechanical
alternan , and the favored view at present is that mechanical alternan repre ent a Ca2+ cycling phenomenon involving the arcopla mic reticulum.
Clinical Relevance of Pulsus Altemans
Phy ica/ Examination
Pulsus alternan i more readily recognized by phygmomanometry than by palpa tion . As the blood
pre sure cuff i lowly deflated, only alternate beats are heard for a number of millimetr of mercury below the sy tolic level and then all beat are heard. When the y tolic pre ure alternate by more than 20 mm Hg, it can
b detected by palpation of peripheral pulse (e pedally the femoral) rather than the central pulse.12 To avoid the uperimpo ition of re piratory variation of the pul e,
palpation hould be carried out while the patient hold hi / her breath in mid-expiration. Total alternan occurs when the left ventricular ystolic pre sure is less than the aortic pressure o that the aortic valve fai ls to open, re ulting in apparent halving of the pul e rate. Decrea e in venous return by maneuvers uch as tilting the patient in upright position and nitroglycerin administration may e aggerate pulsu altemans and a i tin it detection.12
In the cour e of it detection, pulsus altemans should be differentiated from conditions with similar examination characteri tics. Pulsu bigeminu occurs when the cardiac rhythm i bigeminal with the premature beats decrea ing stroke volume and sy tolic peak pre sure. Put u
38 ------------------------ U. W.O. Medical Journal 70 (1) 2000
paradoxu i a decrease in pulse amplitude of greater than 10 mm Hg during in piration and i cia ically een in pericardia! tamponade, po ibly in con tricti ve pericarditis (although le s commonly), and in obstructive airway di ea e13
•15
• In this condition, when the patient has a rapid re piratory rate which i equal to the heart rate, the phy ical findings may re emble pulsu alteman .13
•14
Clinical Significance of Pulsus Altemans
Pul u alternan occurs mo t commonly in heart failure and implies left ventricular systolic dysfunction. It is also found in patient with evere myocardial di ea e due to aortic steno i , sy temic arterial hyperten ion, coronary athero clero i , and dilated cardiomyopathy. 12
Thi i mo t likely due to the contribution of these conditions to ventricular dy function. Pul u alteman i often a ociated with the third heart ound (53) and disappears with treatment of heart failure .12 It has however, been de cribed in patient with normal hearts for brief periods during or after an epi ode of upraventricular tachycardia . Therefore, it should be
emphasized that the ab ence of pulsus alternans doe not exclude left ventricular sys tolic d y function 3 and conver ely, its pre ence is not nece sarily indicative of di ea e. 12 everthele , pul u alternan i a helpful finding in diagno ing and confirming the left ventricular ys tolic dy function. Presence of pulsus alternans
indicate a poor progno is.13
Conclusion The mechanism underlying the pul u alternans i yet
to be elucidated. However, it i generally accepted that pul u alternans reflects event occurring at the cellular level rather than the hemodynamic . The favored view at pre ent is that pulsus alternan is associated with Ca2
+
cycling phenomenon involv ing the arcoplasmic reticulum. It i po sible that the initiation of the alternans is at the cellular level, but it i further augmented and perpetuated by al teration in the hemodynamic . In the clinical etting, pulsus altemans i as ociated with heart failure and severe myocardial di ea e. It may be helpful in diagnosis of left ventricular dy function.
ACKNO~EDGEMENTS
Author would like to thank Dr. Patrick Teefy for his valuable sugges tions. Dr. Teefy is an interventional cardiologist at the London Health Science Centre.
REFERENCES
1. Gaskell W. On the rhythm of the heart of tire frog and 011 tire nature of the action of the vagus nerve. Phil Tra1rs B 1882; 173:993-1034.
2. Traube L. Ein Fall von pulsus begemi1111s nebst Bermerkungen uber die Leberschwelltmgen bei Klappenfehlem und uber acute Leberatrophie. Berl klin Wschr 1872; 9:185, 221 .
3. Compreherrsive Cardiovoscular Medicine. Volume 1. Edited by Eric f. Topol. 1998. Lippincott-Raven. Philadelphia. pp.326-327.
4. Wenckebaclr KF. Zrtr Analyze des unregelmassigen Pulses: IV. Uber den Pulsus Altemans. Z K/in Med 1902; 44:218-25.
5. Lab MJ, Seed WA. Pulsus Alternans. Cardiovascular Research 1993; 27:1407-1412.
6. Lendrum B, Feinberg H, Boyd E., Katz L . Rhythm effects on contractility of tire beating isovolumic left ventricle. Am J Physio/1960; 199:1115-20.
Feature Articles
7. oble RJ, utter DO. Tire demonstration of a/temating contractile tate in pulsus altemarrs. J Clinlrrvest 1970; 49:1166-77.
8. Gilbert JL, Janse MJ, Lu HH, Pinkston JO, Brooks C McC. Production and abolition of altemation irr mechanical action of the verrtric/e. Am J Physiol 1965; 209: 945-50.
9. McGaughey MD, Maughan L, Sunagawa K, Sagawa K. Alternating contractility in pulsus alternans studied in the isolated canine heart . Circulation1985; 71 :357-62.
10. Lab MJ, Lee fA . Changes in intracellular calcium during mechanical alleman in isolated ferret ventricular muscle. Circ Res 1990; 66:585-95.
11 . Kotsanas G, Holroyd SM, Young R, Gibbs CL. Mec/rarri m contributing to pulsus alternans in pressure-overload cardiac hypertrophy. Am I Physiol 1996; H2490-H2500.
12. Heart Disease: A Textbook of Cardiovascular Medicine. 5tlr edition., val 1. Edited by E. Brarmwald. 1997. W.B. Saunders Company, Plriladephia. pp. 20-23, 455.
13. History Taking and Phy ica/ Examination. Essentials and Clinical Correlates by J Greenberger and DR Hint/rom. 1993. Mosby Year Book. 1993 p. 168.
14. Schoen WJ, Talley JD, Morton JK. Interpretation of cardiac pathophysiology fro m pressure waveform analysis: pulsus alternans. Catlrerization and cardiovascular diagnosi 1991; 24:315-319.
15. A Guide to Physical Examination and History Taking. 6tlr edition. Bates, B, Bickley, LS, Hoekelman, RA. 1995. J.B. Lippincott Company. pp. 299, 302. Q
SOME GOALS SEEM DISTANT AND REMOTE.
SOMEONE HAS TO BELIEVE THEY CAN BE REACH ED.
We do.
Effective treatments and cures are needed. We're working as hard as we can to find them
Our motivation is simple -improving and even saving peoples' lives.
Remember. the smallest step today can lead to a giant leap tomorrow.
lii .JANSSEN-oRTHO Inc~
Good health above all.
C 1999 Janssen-Ortho Inc. JAJOI991001A
U. W.O. Medical Journal 70 (1) 2000------------------------- 39
,--------- --- - ---
PUTTING EVERYTHING YOU'VE LEARNED INTO
PRACTICE. As a medical practitioner and a business person, your time and money are
important to you. At TD Bank, we have created the financial tools tailored to small business to ensure that you will save time and money in the management of your practice.
TO Businessline• Low-cost credit with maximum flexibility available to meet all your business requirements - putting you in control of your business finances.
TO Business Provides you immediate acce s to amounts1 from $1,000 to $10,000 to cover your Overdraft Protection business needs.
TO Mortgages TO Bank can help first time buyers move wiftly and surely toward their goal.
TO Student Line• A convenient line of credit designed to meet your ongoing credit needs for further study programs.1
TO Select Line· A personal line of credit that permits you to withdraw only what you need, when you need it, up to your credit limit ... pay interest only on the amount you u e. Apply only once to set up your line of credit.1
TO Access Bank on-line and in real time via the Internet for all your busine s banking. Web Business• Pay bills, check account balance, or transfer funds.
1m BANK FINANCIAL GROUP
Visit your local TD branch, or, for 24 .. hour convenience, contact TD Access:
t .. soo .. 9TD .. BANK www. tdbank.ca
WE ' RE HERE
TO HELP MAKE IT
EAS IER:
ml
Featur e A rticl e s
HORMONE REPLACEMENT FOR CORONARY ARTERY
THERAPY DISEASE
IN THE DOMAIN OF EVIDENCE BASED MEDICINE
INTRODUCTION
The field of medicine is evolving such that clinical practice is being guided by the findings of Evidence Based Medicine. This allows physicians to provide
the best po sible treatment for their patients based on valid outcomes. The use of Hormone Replacement Therapy (HRT) for the reduction of coronary artery di ea e (CAD) in postmenopausal women is no exception. With the abundant literature on the benefits of HRT, it is surprising to note the low rate of use of HRT in po tmenopausal women who are at high risk for CAD or have existing disea e. This article postulates reasons for current prescribing practices and patient compliance regarding HRT by examining the current information available to patients and their doctors.
CORONARY ARTERY DISEASE IN WOMEN In Canada, coronary artery disease (CAD) is cited as
being the leading cause of mortality. In women, deaths due to coronary artery disea e outweigh the number of deaths due to cancer and is econd only to bone and joint disea e in limiting daily activities and decreasing the autonomy of affected women.1 Overall CAD incidence is higher in men than in pre-menopausal women. However, after the menopause, the incidence in women increases to rate equivalent to men, sugge ting the protective role of e trogen in women. A SO year old woman has a 46% lifetime probability of developing CAD and a 31% chance of dying from heart disease.2
THE BENE FIT S O F HORM O NE REPLA CEM ENT THERAPY
Over the past 20 year more than 30 epidemiological tudie on hormone supplement and CAD have been
carried out. The e studie provide evidence of the lower morbidity and mortality from coronary artery d i ea e amo ng u ers of HRT than among non-users. 3
Observational studies comprise the majority of this
ABOUT THE AUTHORS Mandy Schwartz and Natalie Gomperts are both
second-year medical students at the University of Western Ontario. Mandy Schwartz completed a BSc at York University and is interested in Women's Health. Natalie Gomperts obtained an HBSc in Applied Health Sciences at the University of W aterloo.
By Mandy Schwartz and Natalie Gomperts
literature. These studies demonstrate the risk of coronary artery disease in HRT u ers as being 30-50% that of nonusers.4 The relative risk among users compared with nonu ers of HRT is 0.55-0.65 from meta-analyses.4 In terms of secondary prevention of CAD, HRT users have been shown to have had 84% fewer cardiac events than nonusers of HRT.4 Mechanisms of action proposed by these studies include the improvement of endothelial function, alteration of lipid profiles with a reduction in LDL cholesterol and increase in HDL cholesterol, and reduced insulin resistance .1
•5 Guidelines referring to the
cardioprotective effects of HRT have been published by the American College of Physicians and the Society of Obstetricians and Gynaecologists of Canada . These guidelines recommend that "women who have coronary artery disease or who are at risk of coronary artery disease are likely to benefit from hormone therapy" .1•
2
USE OF HORMONE REPLACEMENT THERAPY Regardless of the biological and epidemiological
evidence, as well as published guidelines supporting the benefits of prescribing HRT to those at risk for or who already have CAD, HRT use remains low.4 An American longitudinal study of 2,500 women, showed that the overall rate of use was only 12.3%.6 Further, a recent study by Wise et al proposed that HRT u e would be higher in a population of postmenopausal women who presented wi th CAD to an academic cardiology clinic in Toronto between January 1996 and August 1997. These authors based their hypothesis on the current guidelines and literature that supported HRT use for CAD. It was further thought that women at higher risk for CAD would be more likely to use HRT if informed about its potential benefits.6 The results of thi tudy revealed that only 13% of women who had CAD were currently using HRT, while only 22% of those at high ri k for CAD were current users.6
REAS O N S FOR LO W RATE OF HORMO E REPLACEMENT THERAPY USE
In light of the evident cardioprotective benefit of HRT, why does use remain low? Firstly, the perceived threat of brea t cancer plays a significant role in determining whether a woman feels confident about starting therapy, regardle s of literature finding .2
Secondly, women may al o worry about the side effects of HRT such as irregular bleeding, weight gain and symptoms of premenstrual syndrome? These factor not only deter the start of HRT but may also contribute to early ce ation of therapy.
U. W .O . M edical Journal 70 (1) 2000------------------------ 41

Fea tur e A rticl e s
Thirdly, due to the nature of CAD and its modifiable ri k factor , phy icians may not con ider the role of HRT in patient management. The main mechani m of HRT a a cardioprotective agent i it effect on erum lipid level . Phy ician may bias their treatment of abnormal lipid level towards the u e of lipid lowering af ents, proven effective by randomized control trials . A well the recommended guidelines are unclear as to do ing regimen , pretreatment inve tigations, follow up and duration of therapy. Thi may lead to phy ician confu ion regarding when to pre cribe, how long to pre cribe for, and whom to pre cribe HRT therapy to. La tly, in thi era of evidence based medicine, the greate t po ible reason for low pre cribing practice of HRT i that the evidence upporting the use of therapy i not robust.9 Tho e tudies
advocating a reduction in mortality and morbidity of CAD in u er are ba ed on ob ervational data with inherent methodological flaws.9
LIM ITATIONS OF OBSERVATIONAL STUDIES
With the limitations of ob ervational tudies, the cardioprotective finding of HRT may be mi leading. Many participants taking part in the e tudie initiated hormone therapy to reduce menopausal ymptoms, and prevent o teoporotic fracture , rather than to reduce their ri k of CAD.7 The e participant tended to be leaner, more health conscious and from higher socio-economic backgrounds than non u er of HRT, thus indicating a election bia in these tudie .7 Due to the e factors,
occurrence of CAD would be le s likely within the tudied population. 10 As such, the healthy u er effect may have bia ed the re ults in favour of a cardioprotective effect of HRT? Furthermore, women who were prone to adver e outcome , uch as a cardiac event de pite u e of HRT, were more likely to have di continued therapy. This could lead to an increa ed prevalence of urvivors participating in the ob ervational tudie 10
• Due to the controver ial nature of the protective finding of HRT, and in the r aim of evidence-ba ed medicine, mo t phy ician may only feel confident in prescribing therapy in light of the outcome of Randomized Control Trials (RCT).
HRT AND RANDOMIZED CONTROL TRIALS Currently, two orth American randomized trial are
available for consideration. It is hoped that these e perimental tudie will help to re olve quest ions regarding the effect of HRT on cardiova cular ri k. The fir t, the Heart and Estrogen I Proge tin Replacement Study (HERS) examined econdary prevention of heart di ea e in postmenopau al women. 10 The HERS t rial randomized 2,763 po tmenopausal women with exi ting heart di ease to either an e trogen and proge tin intervention or to a placebo group. The e women were followed for an average of 4.1 year with main outcome mea ure including the occurrence of non-fatal MI or CHD death . Secondary outcome of un table angina, coronary revascularization, conge tive heart failure, re u citated cardiac arre t, troke or tran ient i chemic attack and peripheral arterial di ea e were a! o included. Re ult of the tudy were worrisome in that they howed no overall significant difference between the treatment and placebo groups for primary or econdary
cardio a cular outcome .1° Further, the trial found a pattern of early increase in the risk of CAD event, although a slight improvement wa noted at the four year follow-up .10 This improvement uggests that follow-up over a longer period of time might reveal a more ignificant outcome. 10 Unfortunately the trial did not
extend it follow-up period o evidence of this effect i not available. Based on the e finding , the trial doe not recommend HRT for the econdary prevention of CAD, although, it recommend that women already receiving treatment should continue on HRT, due to the potentially favorable long term effect .1° Finally, the trial did not evaluate the effects of unoppo ed estrogen therapy for women having undergone hy terectomies, nor did HERS evaluat the cardioprotective b nefit of hormone therapy for women at high ri k for CAD .10 Thus, the recommendations made by HERS cannot be extrapolated to the cohorts and should be u ed with caution. The econd tudy, the Women' Health Initiative (WHI)
enrolled 27,500 women in March of 1993 and will not be completed until 2005.'-7 The tudy will evaluate the effect of HRT on women without exi ting CAD. The trial will include both women who have undergone a hysterectomy and are receiving unoppo ed estrogen therapy and women with an intact uteru receiving combined estrogen and proge tin therapy. 10 Re ult of this study will hopefully re olve some of the i ues rai ed by the HERS trial .
CONCLUSIONS
With the advent of evidence-based medicine, phy icians must wade through conflicting da ta regarding the prevention of CAD when considering prescribing hormone therapy for their patient . Although the gold tandard i the Randomized Control Trial, HERS remain
elu ive in providing coherent prescribing practice for women at high ri k of CAD. Due to the limitation of HERS, publication of comprehen ive guideline will have to wait for the new millennium, when results of further RCTs are available.
ACKNOWLEDGMENTS The authors would like to thank Dr. James A. Silcox,
MD, MEd, FRCSC for his help in reviewing our article and provid ing valuable feedback . Dr. Silcox is an Ob tetrician / Gynaecologi t and the Associate Dean of Admi ion / Student and Equity Affairs, Undergraduate Medical Education at the Univer ity of We tern Ontario.
REFER£ CES
1. Society of Obstetricians and Gynaecologists of Canada. Carzadianmenopause consen us conference. ] Society Ob tel Gynaecol Can 1994; 15:1647-96.
2. Grady 0 , Petit ti 0 , Rubin SM, Audet A. Guidelines for counseling postmenopausal women about preventative hormone therapy. Amz lntem Med 1992; 117:1038-41 .
3. Grady 0 , Rubin SM, Petitti DB, Fox CS, Black 0 , et a/. Hormone therapy to prevent disense and prolong life in postmenopausal women. Ann lntem Med 1992; 117:1016-1037.
4. Grover SA. Estrogen replacement therapy for women with cardiovascular disea e: Why don 't physicians and patients follow the guidelines? CMA] 1999; 161(1):42-43.
5. Sourander L, Raja la, T, Rai/w, I, Makinen ], Erkkola R, Helenius H. Cardiovascular and cancer morbidity and mortality and sudden cardiac
42 ------------------------- U. W.O. Medical Journal 70 {1} 2000
Feature A r t cles
death in postmenopausal women Oil oestrogell replacement therapy (ERT). Lancet 1998; 352:1965-69.
6. Wise MR, Stewart DE, Lirt P, Abramson BL. Use of lromrone replacemellt therapy among cardiac patients at a Calladiall academic celltre. CMAJ 1999; 161(1): 33-36.
7. Moermall Cj, Wittemall JCM, Collette HJA, et a/. Hormone replacement therapy: A useful tool in the preventioll of corollary artery disease ill postmellopausal womell? European Menopause J 1996;17:658-66.
8. Elinson L, Col1en MM, Elmslie, T. Homrone replacement therapy: a survey of Ontario physicians' prescribing practices. CMAJ 1999;161(6):695-698.
9. Clranner KS , English KM. Hormone replacement therapy in postmenopausal women and cardiovascular risk. l..allcet 1999; 353:1528.
10. Hulley 5, Grady 0 , Bush TL, Furberg CO, Herrington OM, Riggs B, et a/. Randomized trial of estrogen plus progestin for secondary prevention of coronary artery disease in postmellopausal women. JAMA 1998;280:605-13 Q
Scotia Professional Plan
Because you need to know that your bank is as
committed toyour success asyouare.
The desire to work with a financial partner that supports your changing needs and goa ls should never be a challenge. It's important to have access to a range of products and services that can evolve as you do.
Scotia Professional" Plan is designed to do just that. To grow as your practice grows and to evo lve as your li fe ambit ions evolve.
Stop by your loca l Scotiabank branch. Ask how Scot ia Professional" Plan can provide you with the fi nancia l support and security you need throughout your professional life .
.. • ~ Colkp- ol Lr ~de. • + Fam.dy P'tl ' N:&allt ~ rk r.nulk : : ol Canada du C.n.Ma .. .,
§ Scotiabank GroupN www.scotiabank.ca
e Reg•sterrd Tr.cternarit of 'The B•nk of Nov<~ Scoua no Trac:kot'Nrlt of The B.ank of Nov<~ Scot~ '" The Bri of Nova ScotiA i$ an authorized user of marie
Health Care of the
"Pleased to continue to be
a centre for care, teaching and
From Our r-ami!)' to Yours
• St. Joseph's Hospital * Parkwood Hospital • Mount Hope Cent~ for Long Term Care • St. Joseph 's Fami!Y Medical and Dental Centre • St. Joseph 's Detoxification Centre • The HIV Care Programme • Lawson Diabetes Centre • Centre for Act ivi!)t and Ageing • The Lawson Research Institute • Parkwood Hospital Foundation • St. Joseph's Health Centre Foundation
U. W .O. Medica/Journal 70 (1) 2000------------------------ 43

F e atur e Articl e s
HEART DISEASE
Introduction
H eart disease is the most common cause of mortality and morbidity in orth America. Due to the large numbers of people affected, there have b een
substantial resources directed in finding the causes and possible cures for various heart conditions. Through out this research, many risk factors such as h ypertension, smoking, obesity and diabetes have been elucida ted . Family history of cardiac disease is also a very important factor used to identify patients who may be at r isk . However, until molecular techniques became available, the genetics of how heart disease is passed down within families has been poorly understood. Current technology has now allowed for a search of common varian ces (polymorphisms) and mutations of genes related to heart disease. So far, several mutations of candidate genes for different cardiac problems have been identified within certain families. More research is still needed to determine how these mutations may cause disease and how to determine the prognosis of severity for a specific mutation. Heart disease is a complex illness and it must be understood that there will never be one responsible gene. The purpose then is to have a bank of responsible genes that can be used to screen individuals early in life in order to implement good lifestyle habits and to monitor those with the genes carefully . The discovery of these genes along with the identification of other risk factors will help in gauging an individual's risk and play an important role in preventive medicine.
Familial Hypertrophic Cardiomyopathy (FHC) FHC is an autosomal dominant disease that affects
two out of one thousand individuals1• It causes an increase
in myocardial mass and myofibrillar disarray resulting in fibrosis , abnormally small coronary vessels and arrhythrnias1
• Those who suffer are at a higher risk for sudden and premature cardiac death . There have been several mutations found in contractile proteins, a tropomyosin, troponin T and cardiac myosin binding protein C within families who have FHC1
• Over fifty mutations have already been identified most of which exhibited a defect in their organization within cells1
• An example would be a mutation found in a tropomyosin, which is a component of muscle thin filaments and is encoded on chromosome15
. The mutation involves a substitution of a negatively charged glutamic acid by a neutral glycine near the calcium binding domain2
• The resulting protein is believed to disrupt assembly and function of the sarcomere structure2
. Heterozygotes of
ABOUT THE AUTHOR Cecilia Kerner is a second-year medical student at the
University of Western who previously completed a BSc. Honours in Biology/Biotechnology at the University of Ottawa.
AND GENETICS By Cecilia Kerner
m y osin mutations are not protected because when mixtures of normal and mutant myosins were created an overall decrease in motility and activity occurred1
• It is believed that the severity of FHC among families depends on the type of mutation. Mutations that alter the amino acid and occur at actin-myosin junctions or at the essential light chain binding domain have a poorer prognosis 1
•
Those with mutations where the charge of the amino acid remains the same have been shown to have a higher life expectan~. In studies of large unrelated families sharing the same mutation an association between a specific genotype and survival rate have been shown3
. However, there is still a range on severity observed within related individuals which confirms that this disease has other factors involved.
Coronary Heart Disease (CHD)
Coronary heart disease is usually due to atheros clerosis in the ep icardial coronary arteries occluding the arterial lumen and limiting blood flow feeding the heart. When the supply of oxygen cannot meet the myocardial demand due to stenosis, ischemia occurs leading to angina pectoris or myocardial infarction. Family history is a serious risk factor for CHD and many genes are believed to be involved. Since CHD can be combated with drugs or lifestyle changes, screening may become important in both prevention and treatment. It is believed that the genotype may influence CHD risk by interacting with other risk factors such as cholesterol levels and blood pressure4
• There are several candidate genes that encode proteins related to known risk factors; not all of these genes are mutations but instead are a common variant of a gene. Apolipoprotein E for example has three common polymorphisms, E2, E3 and E4, which influence plasma lipid concentrations4
• It is a structural component of circulating chylomicrons, VLDL and HDL and affects the fasting plasma lipid levels5
• E4 produces cholesterol levels higher than average while E2 produced lower levels and may in fact protect individuals from coronary heart disease.
Angiotensin converting enzyme (ACE) converts angiotensin I into the angiotensin IT, a vasoconstrictor that may promote vascular smooth muscle growth. It also degrades bradykinin, a vasodilator and inducer of endothelial factors5
. This implies that concentration itself may contribute to vascular tone, which is critical for healthy coronary arteries. ACE concentrations are stable within an individual and appears to be unaffected by environmental factors suggesting that it must be genetically determined6
• There are two known alleles: ACE I (insertion) and ACED (deletion). As Table 1 shows ACED has the highest ACE concentration; its frequen~ is found to be higher for patients with angina and MI . A meta-analysis of fifteen studies has also correlated ACED with an increased risk of MI4
•
Gene products involved in endothelial functions such as fibrinogen, coagulation factors and PAl Bl have been
44 ------------------------- U. W .O. Medical Journal 70 (1) 2000
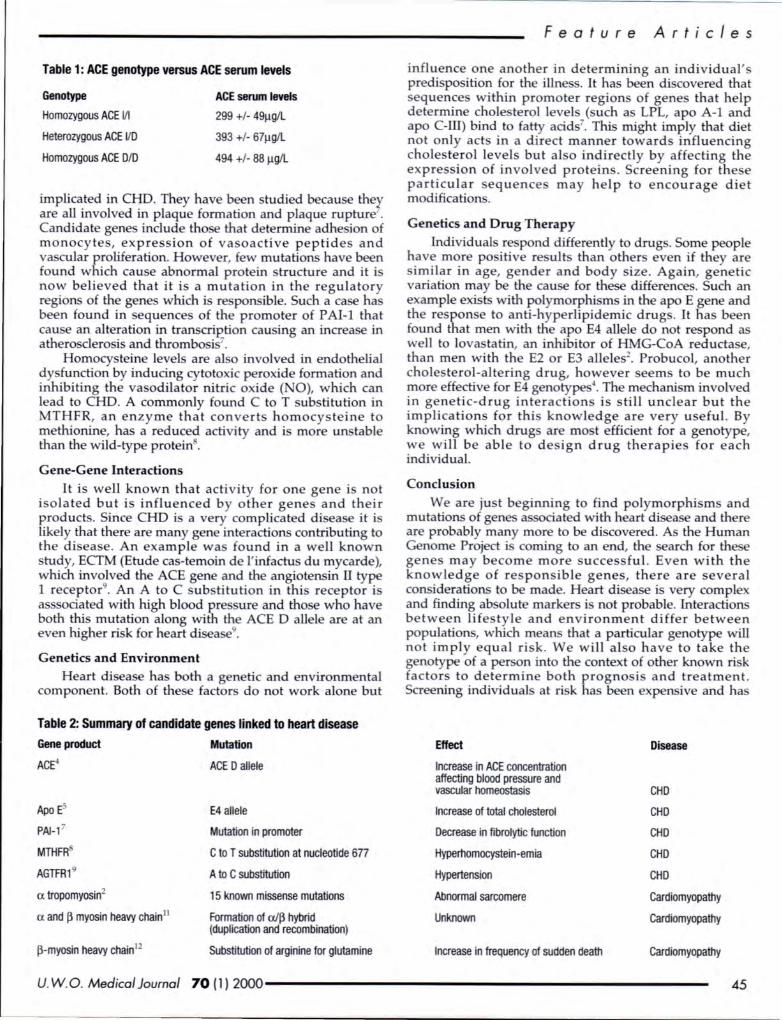
Table 1: ACE genotype versus ACE serum levels
Genotype
Homozygous ACE Ill
Heterozygous ACE VD
Homozygous ACE DID
ACE serum levels
299 +1- 49Jlg/L
393 +1- 67Jlg/L
494 +1- 88 Jlg/L
implicated in CHD. They have been studied becau ether are all involved in plaque formation and plaque rupture . Candidate gene include tho e that determine adhe ion of monocytes, expression of va oactive peptide and va cular proliferation. However, few mutations have been found which cau e abnormal protein tructure and it i now believed that it i a mutation in the regulatory regions of the genes which i re ponsible. Such a case has been found in equence of the promoter of PAI-l that cau e an alteration in transcrirtion cau ing an increa e in athero clero i and thrombo is7
.
Homocysteine levels are al o involved in endothelial dy function by inducing cytotoxic peroxide formation and inhibiting the va odilator nitric oxide ( 0), which can lead to CHD. A commonly found C to T substitution in MTHFR, an enzyme that convert homocysteine to methionine, has a reduced activity and is more un table than the wild-type protein .
Gene-Gene Interactions
It is well known that activity for one gene i not isolated but is influenced by other genes and their products. Since CHD is a very complicated di ea e it i likely that there are many gene interactions contributing to the di ea e . An example wa found in a well known study, ECTM (Etude ca -temoin de l' infactus du mycarde), which involved the ACE gene and the angiotensin II type 1 receptor9
• An A to C ub titution in thi receptor i as ociated with high blood pre ure and tho e who have both this mutation along with the ACE D allele are at an even higher risk for heart di ea e9
•
Genetics and Environment
Heart di ea e has both a genetic and environmental component. Both of these factor do not work alone but
Table 2: Summary of candidate genes linked to heart disease
Gene product Mutation
AC~ ACED allele
Apo Es E4 allele
PAl-1 7 Mutation in promoter
MTHFFf C to T substitution at nucleotide 677
AGTFR1 9 A to C substitution
a tropomyosin2 15 known missense mutations
a and~ myosin heavy chain 11 Formation of a/~ hybrid (duplication and recombination)
~-myosin heavy chain 12 Substitution of arginine for glutamine
U. W . 0. Medical Journal 70 (1} 2000
Feature Articles
influence one another in determining an individual' predispo ition for the illne s. It has been di covered that equence within promoter region of genes that help
determine chole terol levels ( uch a LPL, apo A-1 and apo C-ill) bind to fatty acids7
. This might imply that diet not only acts in a d irect manner toward influencing cholesterol level but also indirectly by affecting the expre sion of involved protein . Screening for the e particular sequences may help to encourage diet modifications.
Genetics and Drug Therapy
Individuals re pond differently to drugs. Some people have more positive re ults than other even if they are imilar in age, gender and body ize. Again, genetic
variation may be the cau e for these differences. Such an example exi t with polymorphi ms in the apo E gene and the respon e to anti -hyperlipidemic drug . It ha been found that men with the apo E4 allele do not respond as well to lovastatin, an inhibitor of HMG-CoA reductase, than men with the E2 or E3 allele 2
• Probucol, another chole terol-altering drug, however eem to be much more effective for E4 genotype 4
• The mechani m involved in genetic-drug interaction is still unclear but the implication for this knowledge are very useful. By knowing which drug are mo t efficient for a genotype, we will be able to de ign drug therapie for each individual.
Conclusion
We are just beginning to find polymorphism and mutations of gene associated with heart disea e and there are probably many more to be discovered. As the Human Genome Project i coming to an end, the earch for these gene may become more successful. Even with the knowledge of re pon ible genes, there are everal considerations to be made. Heart di ea e is very complex and finding ab olute markers is not probable. Interactions between lifestyle and environment differ between population, which means that a particular genotype will not imply equal risk. We will al o have to take the genotype of a per on into the context of other known risk factors to determine both progno i and treatment . Screening individuals at risk ha been expensive and has
Effect Disease
Increase in ACE concentration affecting blood pressure and vascular homeostasis CHD
Increase of total cholesterol CHD
Decrease in fibrolytic function CHD
Hyperhomocystein-emia CHD
Hypertension CHD
Abnormal sarcomere Cardiomyopathy
Unknown Cardiomyopathy
Increase in frequency of sudden death Cardiomyopathy
45
Fea tur e A rti c l es
had limited accessibility but now automated assay kits which can identify mutations have been created. They have shown to be sensitive, specific, reproducible and fast with only a few drops of blood or saliva needed10
. A the expense drops, it will allow both the patient and doctor to treat or change poor habits early in life to improve health and to reduce illness. Aside from lifestyle and drug treatments, gene therapy, which is only at an experimental stage may turn into reality. For example, a transfer of vascular endothelial growth factors to sites of aiterial damage, is being delivered during angioplasty to encourage collateral development4
• Although w ide screening raises both ethical and legal issues such as insurance policies, the overall benefit of identifying p ople at risk for diseases where treatments exist to prevent a premature death is very significant.
ACKNO~EDGEMrnNTS
The author would like to thank Dr. R. Yee fo r his suggestions and review of this paper.
REFERENCES
1. Vikstram KL and Leinwand LL: Contractile protein mutations and heart disease. Current Opinion in Cell Biology 1996, 8: 97-105.
2) Thierfelder L, Wathins H, MacRae C et a/: o: - Tropomyosin and cardiac troponin T : Mutations cause familial hypertrophic cardiomyopatlry: a disease of the sarcomere. Cell1994, 77:701-712
3) Anan R, Greve G, Tirierfe/der L, Wathins H, McKemron Wet a/: Prognostic implications of novel _ cardiac myosin heavy chain gene mutations that cause familial hypertroplric cardiomyopathy. Journal of Clinical lnvestications 1993, 92: 2807-2813.
4) Ellsworth DL, Sholensky P, Jaqush C and Fa/sits RR: Coronary heart disease: At the interface of molecular genetics and preventive medicine. American journal of Preventive Medicine 1999, 16(2): 122-133.
5) Andrade M, Tirrondi I, Brown S et a/: Relationship of the apolipoprotein E polymorphism with carotid artery atherosclerosis. American Journal of Human Genetics 1995, 56: 1379-1390.
6) Camilian F and Evans A : Angiotensin 1 converting enzyme gene polymorphism and coronary heart disease. European Heart Jouma/1995, 16: 13-22.
7) Hanzsten A : Molecular genetics as the rate to understanding, prevention and treatment: Tire Lancet 1992, 393: 693-696.
8) Frosst P, Blom HJ, Milos R eta/: A candidate genetic risk factor for vascular disease: A common mutation in methylenetetrahydrofolate reducatase.
ature Genetics 1995, 10: 111-114. 9) Cambien F, Poirier 0 , Mallet C and Tiret L: Coronary heart disease and
genetics: and epidemiologist's view. Molecular Medicine 1997, 197-203. 10) Baron H., Fwrg S et a/: Oligonucleotide Igation assay for the diagnosis of
familial hypercholesteremia. Nature Biotechnology 1996, 14: 1279-1282. 11) Tanigawa G, Jaricho fA , Kass S et a/: A molecular Basis for familiar
hypertrophic cardiomyopathy. Cell1990, 62:991-998. 12) Dausse E, Komajola M, Felter L et a/. Familial hypertrophic
cardiomyopathy. Joumal of Clinical investications 1994, 93: 280-285. Q
46
"We believe our first responsibility is to the
dodors, nurses and patients, to mothers and
fathers and all others who use our products
and services."
·From the first tenet of the JohJISon & Johnson Credo.
MEDICAL PRODUCTS
U. W . 0. Medical Journal 70 ( 1) 2000

Featur e Articles
CORONARY ARTERY BYPASS BASICS GRAFTING:
Introduction
Coronary artery disea e (CAD) continue to be the leading cau e of morbidity and mortality in the western world. Every year, 1.5 million people suffer
a myocardial infarction in the United State . Over onethird of these patients will die . A the baby-boom generation ages, the prevalence, incidence, total mortality, and economic co t of CAD will increa e ignificantly_l
Anatomy, physiology and pathophysiology The right and left coronary arteries arise from the
inu e of va l alva in the ascending aorta. The right coronary artery (RCA) pa e in the right atrioventricular groove, gives ri e to several acute marginal (AM) branches, and in 90% of patient , ends as the po terior de cending artery (PDA) in the posterior interventricular groove (right coronary dominance). Thu , the main upply of the right ide of the heart, including the SA and the A V nodes, and the posterior fa cicle of the left bundle branch, i the RCA. The left main coronary artery gives rise to the left anterior descending artery (LAD) and the left circumflex artery. LAD and it diagonal branche upply the anterior and apical aspect of the left ventricle. The perforating branches supply the interventricular eptum including the right bundle branch and the anterior fascicle of the left bundle branch. The LAD is a crucial coronary artery in that it supplies the major portion of the left ventricle. The circumflex artery proceeds laterally and po teriorly around the left atrioventricular groove, giving ri e to everal obtu e marginal (OM) branche . It supplies the po tero-lateral and po terior aspect of the left ventricle. In 10% of people, the circumflex artery provides the posterior de cending coronary arte:1 (left coronary dominance) and thus the AV node a well.
Coronary blood flow normally approximates 1 mL per gram of myocardium per minute and delivers 0.1 mL of oxygen per gram per minute to the heart. The extraction of oxygen in the average coronary bed is 75% and may increase to 100% in periods of stress. Coronary flow occurs primarily during dia tole, and i a function of the difference between sy temic diastolic pressure (in the proximal aorta) and left ventricular end diastolic pre ure. Coronary arterie po es ignificant va odilatory reserve, allowing a three to six-fold drop in the coronary artery re istance in periods of need.3
Athero clerotic di ea e of the coronary arteries will eventually lead to an imbalance of oxygen supply and demand that prevents adequate perfusion of the myocardial tissue. The re ulting i chemia may progre to infarction of the cardiac muscle in the distribution of the respective coronary artery. Chronic arterial insufficiency re ults in progressive dilatation of the left ventricle ub equent to accumulation of minor infarctions leading
THE By Shafie Fazel
to conge tive heart failure (CHF) econdary to y tolic dy function. The equelae of acute myocardial infarction fall into two categorie : i) CHF due to pump failure or a mechanical complication, uch a ventricular epta1 defect, mitral regurgitation due to papillary muscle dysfunction, left ventricular rupture, and cardiac tamponade; and ii) life-threatening ventricular dy rhythmias or heart-blocks.~
Management The management of coronary artery di ease (CAD)
may be divided into three progressive stages: i) life-style modifications, ii) medical management, and iii) invasive management. Life- tyle modifications include exerci e, diet, and environmental modifications. Medical management of CAD includes anti-angina medications uch a beta-blocker , calcium channel blockers, ACE
inhibitors, and anti-platelet agents particularly aspirin. Risk factor management uch as blood pre sure control in hyperten ive patient , cholesterol control in hyperlipidemic patients, and gluco e control in diabetic patients are an integral part of the medical therapy for CAD patient . The inva ive management of CAD, in patients refractory to medical management, includes two different approaches: i) percutaneou transluminal coronary angioplasty (PTCA) and I or stenting, and ii) direct reva cularization of the coronary arteries using venous and arterial conduit : coronary artery bypass grafting (CABG)Y
Patient for whom an invasive intervention is indicated fall into three categories. Fir t category includes patients in whom angina refractory to medical management is pre ent. Second category includes patients in whom the extent of CAD, the ventricular function, and the degree of inducible ischemia on stress testing are such that surgery may improve survival. In this category, CABG is indicated for patients with left main stenosis greater than 50%, three vessel di ease with ejection fraction of le than 50%, three ve el disea e with ejection fraction greater than 50% and significant i chemia, and one and two ve sel di ea e with extensive myocardial involvement with le ions not amenable to PTCA. Third category include patients in whom CAD is pre ent concomitantly with other conditions for which open-heart urgery i indicated, such as evere aortic stenosi . In
general, PTCA and I or stenting is re erved for patients with imple ingle-vessel di ease, or uncomplicated multives el di ea e, providing that the lesions are distinct, and not diffuse. 5
Surgical technique of CABG Conventional surgical revascularization of the heart
involves five step : i) median temotomy and appropriate di section through pericardium, ii) administration of heparin, e tablishment of cardiopulmonary bypass (CPB},
U. W .O . Medical Journal 70 (1) 2000------------------------- 47
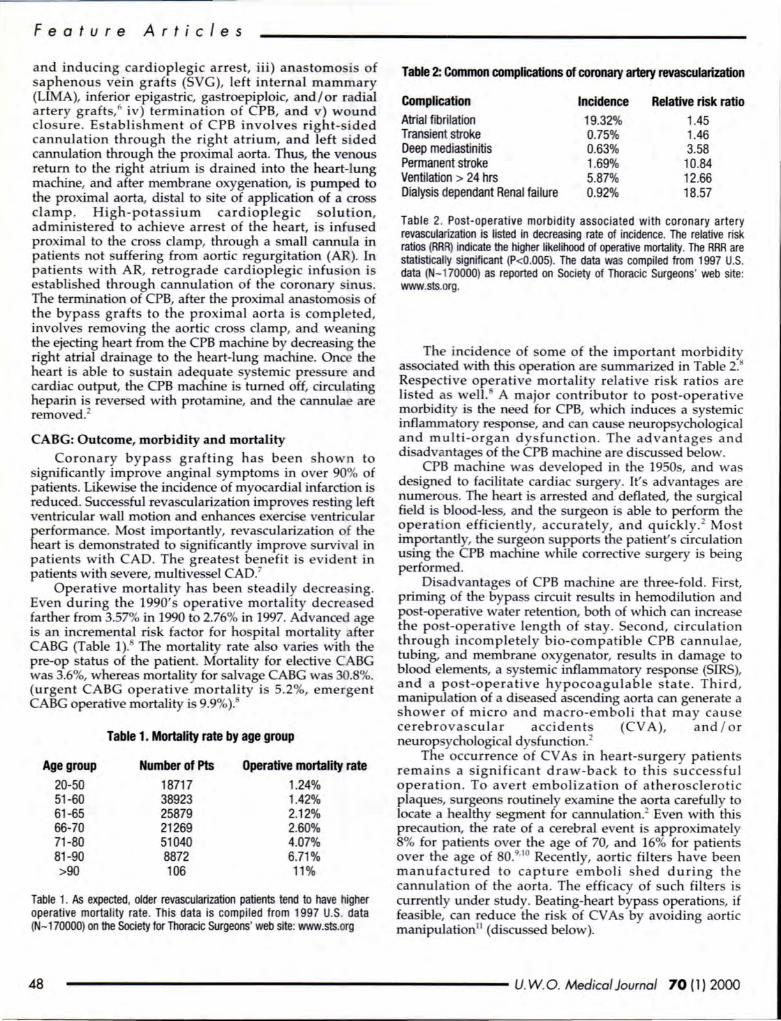
Feat ur e Art icl es
and inducing cardioplegic arrest, iii) anastomosis of aphenous vein grafts (SVG), left internal mammary
(LIMA), inferior epigastric, gastroepiploic, and/ or radial artery graft ,6 iv) termination of CPB, and v) wound closure . Establishment of CPB involves right-s ided cannulation through the right atrium, and left sided cannulation through the proximal aorta. Thus, the venous retun:'- to the right atrium is drained into the heart-lung machine,_ and after membrane oxygenation, is pumped to the proxrmal aorta, distal to ite of application of a cro s clamp . High-potassium cardioplegic solution, administered to achieve arrest of the heart, is infused proximal to the cross damp, through a small cannula in pa~ents no~ suffering from aortic regurgitation (AR). In patients with AR, retrograde cardioplegic infusion is establish~d ~hrough cannulation of the coronary sinus. The temunation of CPB, after the proximal ana tomo is of !he bypass grafts to the proximal aorta is comple ted, mvo~ve~ removing the aortic cross clamp, and weaning ~e eJec~g hea:t from the CPB machine by decreasing the nght atrial dramage to the heart-lung machine. Once the heart is able to sustain adequate systemic pre sure and cardi~c ~utput, the C~B machine is turned off, circulating heparm IS reversed W1th protamine, and the cannulae are removed.2
CABG: Outcome, morbidity and mortality
Coronary by pass grafting has been hown to significantly improve anginal symptoms in over 90% of patients. Likewise the incidence of myocardial infarction is redu~ed . Succe ful ~evascularization improves resting left ventricular wall motion and enhances exerd e ventricular performance. Most importantly, revascularization of the heart is demonstrated to significantly improve survi al in patients with CAD. The greatest benefit is evident in patients with severe, multivessel CAD?
Oper~tive mortality ha been steadily decrea ing. Even dunng the 1990's operative mortality decrea ed ~arthe~ from 3.57% ~ 1990 to 2.76% in 1997. Advanced age 1s an mcremental nsk factor for hospital mortality after CABG (Table 1). The mortality rate al o varies with the pre-op status of the patient. Mortality for elective CABG was 3.6%, whereas mortality for alvage CABG was 30. %. (urgent CABG operative mortality i 5.2%, emergent CABG operative mortality i 9.9%).
Age group 20-50 51 -60 61-65 66-70 71-80 81-90 >90
Table 1. Mortality rate by age group
Number of Pts 18717 38923 25879 21269 51040 8872 106
Operative mortality rate 1.24% 1.42% 2.12% 2.60% 4.07% 6.71% 11%
Table 1. As expected, older revascularization patients tend to have higher operative mortality rate . This data is compiled from 1997 U.S. data (N-170000) on the Society for Thoracic Surgeons' web site: www.sts.org
Table 2: Common complications of coronary artery revascularization
Complication Atrial fibrilation Transient stroke Deep mediastinitis Permanent stroke Ventilation > 24 hrs Dialysis dependant Renal failure
Incidence 19.32% 0.75% 0.63% 1.69% 5.87% 0.92%
Relative risk ratio 1.45 1.46 3.58
10.84 12.66 18.57
Table 2. Post-operative morbidity associated with coronary artery revascularization is listed in decreasing rate of incidence. The relative risk ratios (RRR) indicate the higher likelihood of operative mortality. The RRR are statistically significant (P<0.005). The data was compiled from 1997 U.S. data (N-1 70000) as reported on Society of Thoracic Surgeons' web site: www.sts.org.
T_he inci~enc~ of orne of the important morbidi ty a soaated W1th thi operation are ummarized in Table 2. ~espective operative mortality relative risk ratios are hste~ ~s ~ell . A major contributor to post-operative ~orbidity 1s the need for CPB, which induces a systemic inflammatory response, and can cau e neurop ychological a~d multi-organ d ys function . The advantage a nd disadvantages of the CPB machine are discussed below.
CPB machine wa developed in the 1950 , and was design d to facilitate cardiac surgery. It's advantage are ~um~rou . The heart i arrested and deflated, the urgical field 1 blood-less, and the surgeon i able to perform the ?peration efficie ntly, accurately, and quickly. 2 Mos t rmportantly, the surgeon upports the patient' circulation usmg the CPB machine while corrective surgery is being performed.
Di advantage of CPB machine are three-fold . First, priming of the bypas circuit result in hemodilution and po t-operative water retention, both of which can increase the pos t-operative length of tay. Second, circulation thr?ugh incompletely bio-compatible CPB cannulae, tubmg, and membrane oxygenator, results in damage to blood elements, a systemic inflammatory response (SIRS), and a po t-operati ve hy pocoagulable state . Th ird, manipulation ~fa di eased ascending aorta can generate a shower of micro and macro-embol i that ma y cause cerebrovascular accidents (CV A), and I or neurop ychological dy function.2
The occurrence of CV As in heart-surgery patients remain a significant draw-back to this s ucces ful operation. To avert embolization of athero clerotic plaque , urgeons routinely examine the aorta carefully to locate a healthy segment for cannulation.2 Even with this p~ecaution~ the rate of a cerebral e ent i approximately 8 Yo for patients over the age of 70, and 16% for patients over the age of 80.9'
10 Recently, aortic filters have been manufa~tured to ca pture e mboli shed during the cannulation of the aorta. The efficacy of such filters is curr~ntly under study. Beating-heart bypass operations, if feas1ble, can reduce the risk of CV As by avoiding aortic manipulation11 (discus ed below).
48 ------------------------ U. W.O. Medical Journal 70 (1) 2000
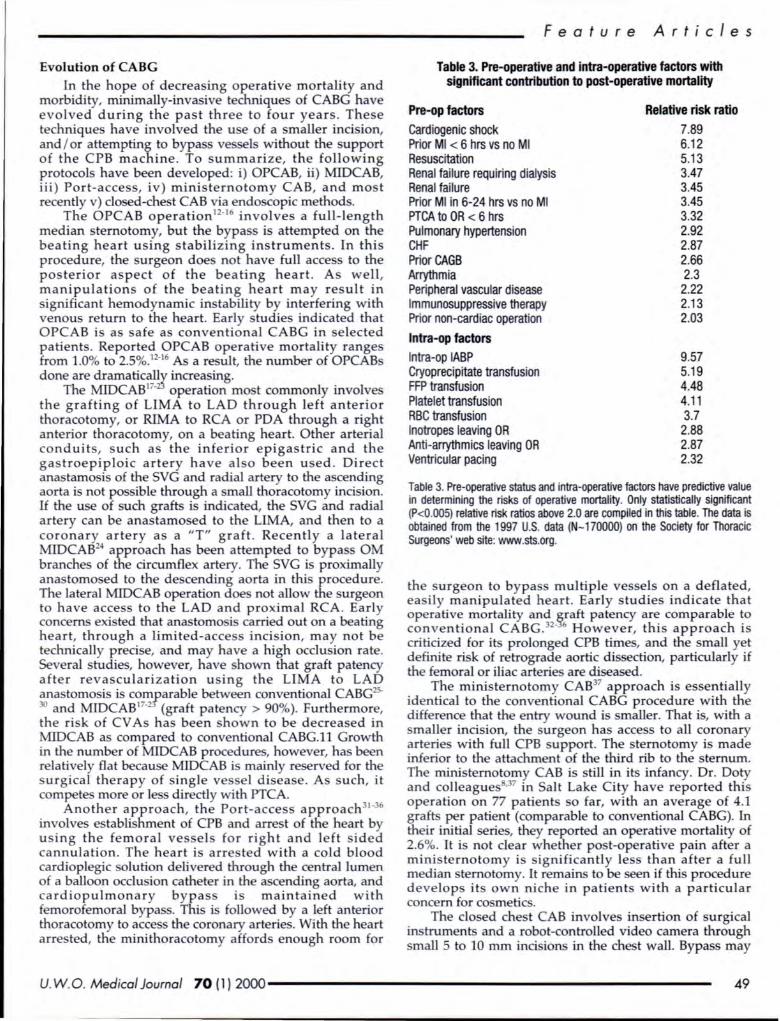
Evolution of CABG
I~ ~he h~p~ of decreasing operative mortality and morbidity, muumally-invasive techniques of CABG have evol~ed during _the past three to four years. These techniques have mvolved the use of a smaller incision, and / or attempting to bypass ve sels without the support of the CPB machine. To summarize, the following p~otocols have been developed: i) OPCAB, ii) MIDCAB, m) Port-access, iv) ministernotomy CAB, and most recently v) closed-chest CAB via endo copic methods.
~he OPCAB operation12-16 involves a full-length
med~an sternotomy, but the bypass is attempted on the beating heart using stabilizing instruments. In this procedure, the surgeon does not have full access to the posterior aspect of the beating heart. As well, n:ta~ipulations of the beating heart may result in significant hemodynamic instability by interfering with venous return to the heart. Early studies indicated that OPCAB is as safe as conventional CABG in selected patients. Reported OPCAB operative mortality ranges from 1.0% to 2.5%.12
-16 As a result, the number of OPCABs
done are dramaticallJ increasing. The ~CAB17- operation most commonly involves
the graftmg of LIMA to LAD through left anterior thora~otomy, or RIMA to RCA or PDA through a right antenor thoracotomy, on a beating heart. Other arterial conduits, such as the inferior epigastric and the gastroepiploic artery have also been used. Direct anast~osis of ~e SVG and radial artery to the ascending aorta IS not possible through a small thoracotomy incision. If the use of such grafts is indicated, the SVG and radial artery can be anastamosed to the LIMA, and then to a coronaqr artery as a "T" graft . Recently a lateral MIDCAB24 approach has been attempted to bypass OM branches of the circumflex artery. The SVG is proximally anastomosed to the de cending aorta in this procedure. The lateral MIDCAB operation does not allow the surgeon to have ac~ess to the LAD and proximal RCA. Early concerns eXIsted that anastomo is carried out on a beating heart~ through. a limited-access incision, may not be technically preCI e, and may have a high occlusion rate. Several studies, however, have shown that graft patency after revascularization using the LIMA to LAD anastomosis is con;]'arable between conventional CABG25-30 and MIDCAB17
• (graft patency > 90%). Furthermore, the risk of CV As has been shown to be decreased in MIDCAB as compared to conventional CABG.ll Growth in the number of MIDCAB procedures, however, ha been relatively flat becau e MIDCAB is mainly re erved for the surgical therapy of single ve el disea e. As such, it compete more or les directly with PTCA.
Another approach, the Port-access approach31·36
in~olve establi hment of CPB and arrest of the heart by u mg the femoral ve sel for right and left sided cannulation . The heart is arre ted with a cold blood cardioplegic solution delivered through the central lumen of a ~alloon occlu ion catheter in the a cending aorta, and cardiOpulmonary by pass is maintained with femorofemoral bypass. This is followed by a left anterior thoracotomy to access the coronary arteries. With the heart arrested, the minithoracotomy affords enough room for
Featur e A rticl e s
Table 3. Pre-operative and intra-operative factors with significant contribution to post-operative mortality
Pre-op factors Cardiogenic shock Prior Ml < 6 hrs vs no Ml Resuscitation Renal failure requiring dialysis Renal failure Prior Ml in 6-24 hrs vs no Ml PTCA to OR < 6 hrs Pulmonary hypertension CHF Prior CAGB Arrythmia Peripheral vascular disease Immunosuppressive therapy Prior non-cardiac operation
lntra-op factors lntra-op IABP Cryoprecipitate transfusion FFP transfusion Platelet transfusion RBC transfusion lnotropes leaving OR Anti-arrythmics leaving OR Ventricular pacing
Relative risk ratio 7.89 6.12 5.13 3.47 3.45 3.45 3.32 2.92 2.87 2.66 2.3 2.22 2.13 2.03
9.57 5.19 4.48 4.11 3.7 2.88 2.87 2.32
Table 3. Pre-operative status and intra-operative factors have predictive value in determining the risks of operative mortality. Only statistically significant (P<O.OOS) relative risk ratios above 2.0 are compiled in this table. The data is obtained from the 1997 U.S. data (N-170000) on the Society for Thoracic Surgeons' web site: www.sts.org.
the surgeon to bypa s multiple vessels on a deflated ea ily manipulated heart. Early studies indicate that operative mortality and §,raft patency are comparable to c~~v_entiona~ CABG .32
· 6 However, this approach is
cn~c~ed . for Its prolonged CPB times, and the small yet definite nsk of retrograde aortic dissection, particularly if the femoral or iliac arteries are diseased. . T~e ministernotomy CAB37 approach is essentially I~entical to the conventional CABG procedure with the difference that the entry wound is smaller. That is, with a smal~er in~ision, the surgeon has access to all coronary ?rte~es with full CPB upport. The ternotomy is made infenor to the attachment of the third rib to the sternum. The rninisternotomy CAB is still in its infancy. Dr. Doty and c~lleague ·37 in Salt Lake City have reported thi operation on_77 patients so far, with an average of 4.1 gr~s- ~~ pati~nt (comparable to conventional CABG). In theu uu~al senes, they reported an operative mortality of 2 .~~- It IS not clear whether post-operative pain after a mm~sternotomy is significantly les than after a full median ste~otomy. It remains to be seen if this procedure develop Its own niche in patient with a particular concern for co metics. . The clo ed chest CAB involves in ertion of urgica1 UIStrument and a robot-controlled video camera through small 5 to 10 rnm inci ions in the che t wall. Bypass may
U. W.O. Medical Journal 70 (1) 2000------------------------ 49
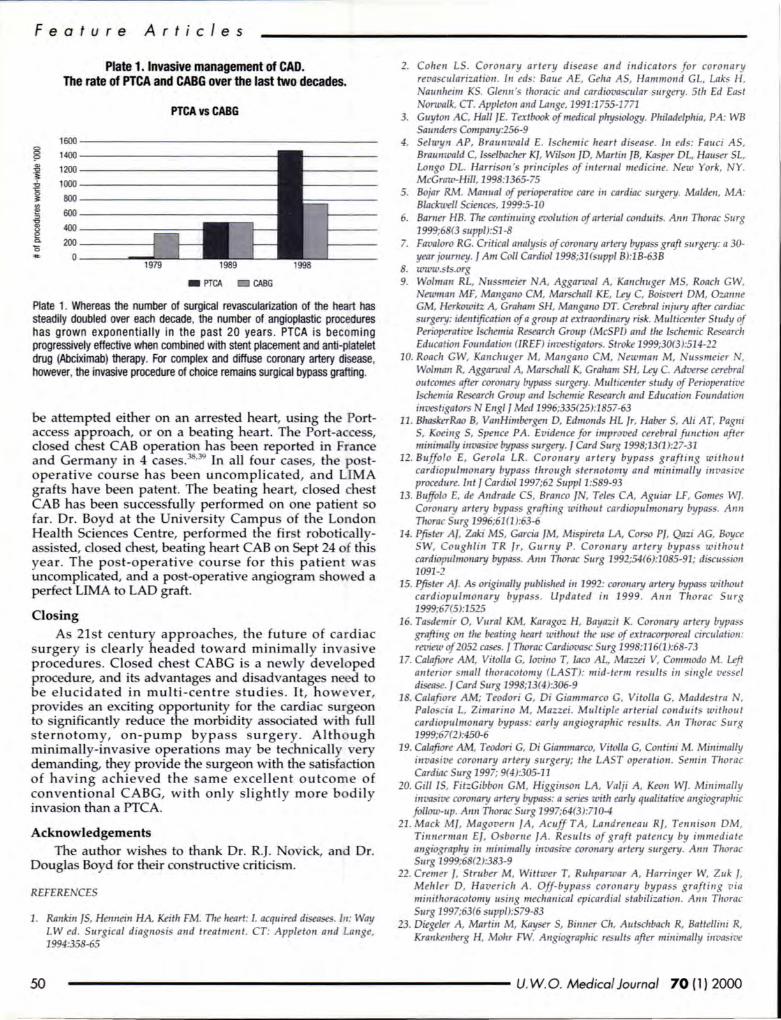
Fea tur e A rticl es
Plate 1. Invasive management of CAD. The rate of PTCA and CABG over the last two decades.
PTCA vs CABG
1600
§ 1400
"' 1200 "' "i ...;, 1000 -.:: 0
800 ~ ., e 600 , "' "' 400 e c. 200 0
0
- PTCA - CABG
Plate 1. Whereas the number of surgical revascularization of the heart has steadily doubled over each decade, the number of angioplastic procedures has grown exponentially in the past 20 years . PTCA is becoming progressively effective when combined with stent placement and anti-platelet drug (Abciximab) therapy. For complex and diffuse coronary artery disease. however, the invasive procedure of choice remains surgical bypass grafting.
be attempted either on an arrested heart, u ing the Portaccess approach, or on a beating heart. The Port-acce s, do ed che t CAB operation ha been reported in France and Germany in 4 case . ·39 In all four ca es, the postoperative cour e has been uncomplicated, and LIMA graft have been patent. The beating heart, closed che t CAB has been successfully performed on one patient o far . Dr. Boyd at the University Campu of the London Health Sciences Centre, performed the fir t roboticallyassi ted, do ed chest, beating heart CAB on Sept 24 of thi year. The post-operative course for thi patient wa uncomplicated, and a post-operative angiogram showed a perfect LIMA to LAD graft.
Closing As 21st century approache , the future of ca rdiac
surgery is clearly headed toward minimally inva ive procedures. Closed che t CABG is a newly developed procedure, and its advantages and disadvantages need to be elucidated in multi-centre studie . It, howe ver, provide an exciting opportunity for the cardiac urgeon to ignificantly reduce the morbidity a sociated with full sternotomy, on-pump bypass surgery. Altho ugh rninimally-inva ive operations may be technically very demanding, they provide the surgeon with the atisfaction of having achieved the arne excellent outcome of conventional CABG, with onl y lightly more bodil y invasion than a PTCA.
Acknowledgements The author wishes to thank Dr. R.J. ovick, and Dr.
Douglas Boyd for their con tructive critici m.
REFERE CES
1. Rankin JS, Hennein HA, Keith FM. Tire heart: I. acquired diseases. In: Way LW ed. Surgical diagnosi and treatment. CT: Appleton and Lange, 1994:358-65
2. Colreu LS . Coronary artery disease and indicators for coronary reva cularizatiou. /11 eds: Baue AE, Gelra AS, Hammond GL, Laks H,
aunlreim KS. G/erm 's thoracic and cardiova cu/ar surgery. 51/r Ed East orwalk, CT. Appleton and Lange, 1991:1755-1771
3. Guyton AC, Hall JE. Textbook of medical plrysrology. Plriladelplria, PA: WB Saunders Company:256-9
4. Selwyn AP, Braunwald E. I chemic heart disease. In eds: Fauci AS, Brarmwald C, lsselbaclrer K], Wilson JO, Martin JB, Kasper OL, Hauser SL, Longo OL. Harrison 's principle of in lema/ medicine. ew York, Y. McGraw-Hill, 1998:1365-75
5. Bojar RM. Manual of perioperative care in cardiac surgery. Malde11, MA: Blackwell Scie11ces, 1999:5-10
6. Bamer HB. Tire continuing evolution of arterial conduits. Ann Tlrorac Surg 1999;68(3 uppi):S1-8
7. Favaloro RG. Critical analysis of coronary artery bypass graft surgery: a 30-year joumey. JAm Col/ Cardiol1998;31(suppl 8):18-638
8. www. t .org 9. Wolman RL, ussmeier A, Aggarwal A, Kanclruger MS, Roac/1 GW,
ewman MF, Mangano CM, Marschall KE, Ley C, Boisvert OM, Ozanne GM, Herkowitz A, Graham SH, Mangano OT. Cerebral injury after cardiac surgery: idell tificatiou of a group at extraordinary risk. Multicenter Study of Perioperative Ischemia Research Group (McSPI) and the Ischemic Research Education Foundation (IREF) investigators. Stroke 1999;30(3):514-22
10. Roach GW, Kanclwger M, Mangano CM, ewman M, ussmeier , Wolman R, Aggarwal A, Marschall K, Graham SH, Ley C. Adverse cerebral outcomes after coronary bypas surgery. Mulllcenter study of Perioperative Ischemia Research Group and lschemie Research and Education Foundation iuvesllgator N Eng/ I Med 1996;335(25):1857-63
11. BhaskerRao 8, Van Himbergen 0, Edmonds HL Jr, Haber S, Ali AT, Pagni S, Koeing S, Spence PA. Evidence for improved cerebral function after minimally invasive bypass surgery. J Card Surg 1998;13(1):27-31
12. Buffolo E, Gerola LR. Coronary artery bypass grafting wit/rout cardiopulmonary bypass through sternotomy and minimally inva ive procedure. Jut J Cardio/1997;62 Supp11:S89-93
13. Buffolo E, de Andrade CS, Branco JN, Teles CA, Aguiar LF, Gomes W]. Coronary artery bypas grafting without cardiopulmonary bypass. Ann Tirorac Surg 1996;61(1 ):63-6
14. Pfi ter Aj, Zaki MS, Garcia JM, Mispireta LA, Corso PJ, Qazi AG, Boyce SW, Couglrlin TR Jr, Gurny P. Coronary artery bypas without cardiopulmonary bypa s. Ann Tirorac Surg 1992;54(6):1085-91; diswssion 1091-2
15. Pfister Af. As originally published in 1992: coronary artery bypass without cardiopulmonary bypa s. Upda ted in 1999. Ann Tlrorac Surg 1999;67(5):1525
16. Ta demir 0, Vural KM, Karagoz H, Bayazit K. Coronary artery bypa s grafting on tire beati11g heart wit/rout the use of extracorporeal circulation: review of 2052 cases. J Tlrorac Cardiovasc Surg 1998;116(1):68-73
17. Calafiore AM, Vitolla G, Iovino T, laco AL, Mazzei V, Commodo M. Left an/error small thoracotomy (LAST): mid-term results in single vessel disease. J Card Surg 1998;13(4):306-9
18. Calafiore AM; Teodori G, Oi Giammarco G, Vitolla G, Maddestra , Paloscia L, Zimarino M, Mazzei . Multiple arterial conduits wit/rout cardiopulmonary bypa : early angiograplric results. All Thorac Surg 1999;67(2):450-6
19. Calafiore AM, Teodori G, Oi Giammarco, Vitolla G, Contini M. Minimally invasive coronary artery surgery; the LAST operatio11 . Semi11 Tlrorac Cardiac Surg 1997; 9(4):305-11
20. Gill IS, FitzGibbon GM, Higginson LA, Valji A, Keon W]. Minimally invasive coro11ary artery bypass: a series with early qualitative angiograplric follow-up. Amr Tlrorac Surg 1997;64(3):710-4
21 . Mack M], Magovem fA , Acuff TA, Landreneau RJ, Tennison OM, Ti11nerma11 EJ, 0 borne fA. Result of graft pa tency by im mediate a11gio raplry in mi11imally i11vasive coro11ary artery surgery. An11 Tlrorac Surg 1999;68(2):383-9
22. Cremer J, Struber M, Wittwer T, Rulrpanoar A, Harringer W, Zuk f, Mehler 0, Havericlr A. Off-bypass coronary bypass graftillg via mi11itlroracotomy using meclra11ical epicardial stabilization. A1111 Tlrorac Surg 1997;63(6 suppi):S79-83
23. Oiegeler A, Martin M, Kayser S, Bimrer Clr, Autsclrbach R, Battellini R, Krankenberg H, Mohr FW. Angiograplric results after minimally invasive
50 ------------------------- U. W.O. Medical Journal 70 (1) 2000
coronary bypass grafting using the minimally invasive direct coronary bypas grafting (M IDCAB) approach. Eur I Cardiothorac Surg 1999;15(5):680-4
24. Fonger ]D, Doty JR , Su sman MS, Saolomon W. Lateral MIDCAB grafting via limited posterior thoracotomy. Eur] Cardiothorac Surg 1997;12(3):399-404
25. Barner HB, Mudd IG, Mark AL, Alrmad N, Dickens ]F. Patency of internal mammary-coronary graft . Circulation 1976;56(6 supp/):ll/70-3
26. Gelra AS, Krone Rl, MaCormick JR, Baue AE. Selection of coronary bypass. Anatomic, physiologic, and angiographic considerations of vein and mammary artery grafts I Thorac Cardiovasc Surg 1975;70(3):414-31
27. Barner HB, Swartz MT, Mudd JG, Tyras DH. Late patency of the internal mammary artery a a coronary bypass conduit. Ann Thorac Surg 1982;34(4):408-12
28. Tyras DH, Barner HB, Kaiser GC, Codd, Pennington DG, Willman VL. Bypass grafts to the left anterior descending coronary artery: saphenous vein versus internal mammary artery. I Thorac Cardiovasc Surg 1980;80(3):327-33
29. Bourassa MG, Campeau L, Lesperance J, Grondin CM. Changes in graft and coronary arteries after saphenous vein aortocoronary bypass surgery: results at repeat angiograplry. Circulation 1982;65(7 pt 2):90-7
30. /vert T, Huttmen K, Landou C, Bjork VO. Angiographic studies of internal mammary artery grafts 11 year after coronary artery bypas grafting. / Thorac Cardiovasc Surg 1988;96(1):1-12
31 . Stevens ]H, Burdon TA, Peter WS, Siegel LC, Pompili MF, Vierra MA, 51 Goar FG, Ribakove GH, Mitchell RS, Reitz BA. Port-access coronary artery bypass grafting: a proposed surgical met/rod. I Tlwrac Cardiovasc Surg 1996;111(3):567-73
32. Reichenspunrer H, Boehm DH, Welz A, Sclrmitz C, Wildlrirt 5, Schulze C, Meiser B, Schutz A, Reiclrart B. Minimally invasive coronary artery bypass grafting: port-access approaclr versrt off-pump techniques. Ann Thorac Surg 1998;66(3):1036-40
33. Ribakove GH, Miller JS, Andersan RV, Grossi EA, Applebaum RM, Cutler WM, Buttenheim PM, Baumann FG, Galloway AC, Calvin SB. Minimally invasive port-access coronary artery bypass grafting with early angiographic follow-up : initial clinical experien ce. I Thorac Cardiovasc Surg 1998;115(5):1101-10
34. Reiclrenspumer H, Gulie/mos V, Wwtderliclr I, Dangel M, Wagner FM, Pompili MF, Stevens IH, Ludwig J, Daniel WG, Schuler 5. Port-Access coronary artery bypass grafting with the use of cardiopulmonary bypass and cardioplegic arrest. Arrrr Tirorac Surg 1998;65(2):413-9
35. Grolr MA, Fallen OM. Alteration of tire traditional extracorporeal bypas circuit to accommodate port-access minimally invasive cardiac procedures using endovascular-based cardiopulmonary bypass . Artif Organs 1998;22(9):775-80
36. Schwartz OS, Ribakove GH, Grossi EA, Schwartz ]D, Buttenlreim PM, Baumann FG, Colvin SB, Galloway ACj. Single and multivessel port-access coronary artery bypas grafting witlr cardioplegic arre t: technique and reproducibility. Tirorac Cardiovasc Surg 1997;114(1):46-52
37. Doty DB, DiRusso GB, Doty JR. Full-spectrum cardiac surgery tlrrouglr a minimal incision: mini-sternotomy (/ower halj) teclrrrique. Arm Tlrorac Surg 1998;65(2):573-7
38. Lou/met D, Carpentier A, d'Attel/is , Berrebi A, Cardon C, Ponzio 0 , Aupecle B, Reiland JY. Endoscopic coronary artery bypass grafting witlr tire aid of robotic assisted instruments. I Tlrorac Cardiovasc Surg 1999;118(1):4-10
39. Reiclrenspurner H, Damiano RJ, Mack M, Boelrm DH, GulbiiiS H, Detter C, Meiser B, Ellgass R, Reichart B. Use of tire voice-controlled and computerassisted surgical system ZEUS for endoscopic coronary artery bypass grafting. ] Tlrorac Cardiovasc Surg 1999 lu/;118(1):11-6 Q
Feature Art cles
U.S.A Immigration Law
William Newell Siebert Attorney at Law
307 North Michigan Avenue Suite 924
Chicago, lllinoi 6060 l
Voice: 312-329-0646 Fax: 312-553~19
PRACTICE CONCENTRATED IN U.S. IMMIGRATIO LAW SINCE 1969
U. W .O. Medical Journal 70 {1)2000 51
Zl~ lOR* A7VR~SP117N CALCIUM
EFFICACY TO REACH TARGET THE FIRST nME
UPITOR' ~Cak:unj 10 mg. 20 mg ;nj 40 mg raiEis
TlfiW'EU!JC ClASSf!CAlXlN: ~ Me1abollsm flegla1Dr ACTIONS AJIO CUMCAI.. PHARMACOLOGY LI'ITOR (abvasla1l1 cab.ml IS a S)fllheOc ~ agert. k IS a seleciM!, ~ rl1biJr r:l3-11y011cy-3-~A~ raiJclase. ThiS enzyme cataiyles lhe CIJ1'o'ln01 r:l tt.1G-CM '> - · wl1ch IS <11 arty ;nj rare-lmlrlg Slllp 11 lhe bos)1'llhesiS r:l d'deslerti LI'ITOR bM!B J*l!rna- ;nj 1iJqmen lew!lsl]ll rllbll1g tt.1G-CM ra1Jclase ;nj-~ 11 lhe Ml' arll Ill' lncreasl1g lhe ruroer r:l hepaiJc Low Density l..ipoJrolel1 Ul) ret11!*JS on lhe cei-Slllacelor eria1ced ~ ;nj calabolism r:l Low Densl1y lWllll!f1 il.lll l.FITCJIIBIU:es I.Jl_ -Odeslircl fJl_ .q ;nj lhe ruOOer fii.Jl_ ~ LI'ITOR also IBI1D!s Very Low Density ~ ('vtll.-Q. senrn ~ (T~ arll nlinnella1e Densly~ Jll, as wet as lle ruroerr:l ~ B la!Xl~ IXI'IIaiW1I ~ tu i'aeases 1111 0ens11y ~ fO--Q EleYa!i!d senrn c:llJi!sla1j rue'> elevalllll..ll_.C IS a ll'QP nsk facU b-lhe ~ r:l ~ clsease. EleYa!i!d J*1!rna TG IS also a nsk facU lor~ c1sease. pr11o..0ty W rue'> ira8asal n. a asmaled wi1ll decreased tO. .C a iraaasafi.Jl_ -c. AIDMslallliS I3IJdY aDsorbed at1er aa1 aarnsta~m; maxrrun J*1!rna txn:e'1llmms oau Wllhll 1 '> 2 tn.rs. AlllMistatl1 raiEis a-e 95" m 99'11. boa'lailallle IXJT'!)al8d '> sciJIO'S. Mean distrbJoon r:latavasta1111s ~ 381 Alorvaslalrlls 0!98'llo IJoonj '> pasma IJOII!I1S AIDMslallliS e>aensM!Iy mecald2ed 1]11 C)1DCirune P-450 3A4 '> CJ1ho. arll ~ dellvalNes arll m VlrlOUS bela~ IJlXi,icls.~ 70'!1. r:l crtUalr1g rtibllay acawy lor tMl Co-A ra1Jclase IS alll'baed m aaJYe metiiJalilss. AloMslalrl arll liS metaboites a-e eirmaled 1]11 bky l!liCII!1ion.less lta1 ~ ct a lbse r:l - II racxwered in liTe ldlowr1g aal a:tMslralm Mean pasma e61wliiJOI1 tall r:l - 11 tunn Is _...:ely 14 tn.rs. but lhe talf-ife r:llrilbby aciM!y lor tt.1G-CM ra1Jclase Is 20 m 30 hotJS rue m lhe CXll1ll'iltAia1 r:1 Joroer.fved aaM!-INDICATIONS AIKJ CUNICAL USE l.FITCJI (ala'laslatl1 cab.ml Is i'dcaled as .., ~ m diet. at 1eas1 eopvaieni1D lhe Arllesic3l Him AssoCiaDon INIAl Step 1 diet, b-Ile reQ.aon ct elevated m dUeslerol. ~. l..ll_ .C. TG ;nj ~ 8 {IIJo ~ 11 ~ arll dyslipdernc ani!ms, when respc:nse m diel arll Olher 1 o pan~ measlfl!S atre has been mdecJ,iale, rrui1g. • Prmary h)peictDeseoleiilia (T)lle laj, • CciTtw1ed ~ (T)lle lq, ill:t.dr9 fanlaj a:mnd hJpeilpden1a. ~fl ........
d1llesllra a ri!tJanjes a-e lle lip<l abrmnalily r:l an:em. · ~lAl!ileioa (T)lle . · ~(T)lli!IV);
• Flrnlal hJIBddS8ce •oa ~ ;m ~· Fa IDTlilz)9Ws f<mial hJIBddS8ce•oa. l.FITCJI stcU!II! U98d as.., ~ '> natmenes SLd1 as I.Jl_ aP1eres15. a as ~ I SLd1 natmenes .., ra -1'1 dhcalllials, l.FITCJI (1 o mIll ~ sqili:anltt I1'IJlMld lip<l JJo1ies in palienls Wl1h a Wide vniY r:l ~ ;nj dyslipdernc ardilms. 1'12 OOSiHeslmSe Slides 11 --~ ~ palienls (FteODson Types 1a ;m ti l.FITCJI i1!0ad te 1ew1s r:1 m clr:ilesll!m (2!}-45'Aol. I.Jl_ .c P9-fiO"l. ape 8 132-5011. TG (1 9-3~ arll i'creased lwj1 dersti 1iJqmen clr:ilesll!m JQ-Q 1ew!ls 15-!W.l ~ i8IIXJISI!S wee actoENed 11 pal8llS..., heleroz)9lus trTilial hJIBddS8ce•oa. oon-trTilial lams r:1 hJIBd"*"*-ce•oa. CXI1'Ill1ed hjpeifpOma, ill:t.dr9 fanlaj a:mnd ~ ;nj palienls IDl-i1st.tn di!pinlerl clabeles melilus. i'1 pa!lei1IS Willl ~del IW (T)lle IV). l.FITCJI (10 tl Ill mg daillj i1!0ad TG (25 - 56'4) nll..ll_ .C 1e1ie1s (23 -~· 01)tmaoos. wl1ch ctaacleri2l! Types I arll V. teYe ra been measond 11 dhcal Slides 11 pate1S
Wlf111{11TG1ew!ls l>11 ~· 1'1 <11 ~lallel Sl1ltf 11 pallei1IS Wl1h ~.....,..,oa (T)lle 1). l.FITCJI (10m Ill mg dal)l i1!0ad m.c (40-~. TG (40-56'4) arll lll.C + \til. .C 1ew!ls (34·58'11.) 1'1 <11 qli!O lallel Sl1ltf 11 pate1S ..., hoinoz)gcliS tm11a1 hJIBctDesece •oa fHl LI'ITOR (10 m Ill mg dallll i1!0ad iliiBi l..ll_.C 1ew!ls !22"j. 1'1 a pb S11Jtt, l.FITCJI!ll"'!VdaY !1-.-l a iliiBi I.Jl_ .C ~ r:l ~lor pal8llS ra on plasiilal)heii!SIS arll ct 31" lor patients wile iXI1IIlJed plasrni\lei!SIS. A iliiBi I.Jl_ .C ~ ct 35'11. was <tJserved 11 receptt def8CIM! pa!lei1IS arll r:l19llo 11 receptt negatNe pa!lei1IS (see PHAAMA<Xl.OGY, CJncalsndes) Fa more delals on elllca:y resUis 1]11 ~ classdlcalm arll pooled data Ill' Frah:lcson types, see PHAAMA<Xl.OG'(, CJncal Sldes. Pnor '> ilballlQ lherapy l.FITCJI. searo.y auses stcU!II! eDJied lor eleYato1s 11 pasma lip<lliM!Is (e.g JXDIY aJ1Iroled clabeles melilus, hjpoCt1)<odsm, l1l!ltiOOC syrOome, ~ obsliu:IMl Mr dsease, ;nj
<*:dlolsm). ;m a lip<l proQe perforned m nmue m dDesli!ra. I.Jl_ .C. tO. -c. arll TG. Fa pate1S TG <4.52 illlD\. (<400 IT1!Ytl).l..ll_.C calli! esll1l2!ed l.iSI1g lhe folowr1g I!CJJ3IIon:
I.Jl_ .c (!!rndA) ; m.c -(~ 37 l (TG) + tO. -QJ I.Jl_ .c (in!Yd) ; m.c -(102 l (TG) + tO. -QJ
Fa paDei'IIS Wl1h TG 1ew!ls >452 illlD\. (>400 ~Ills I!IJ.'IIOi IS less acruale ;nj l..ll_ .C an:8"8aaD1S stoJd ll!measond ii'ecllya 1]11 ~ COifTRAJNOICATIONS
~ '> ~ CXI!'!l0'8t dills medca1m fJcM Ml' ilseese a ..-...plan!d perSIS1I!nl eleYations r:l senrn ll1mr1WlaseS l!lll8edi1g 3 limes lhe l«B' inll ct ramal (see l\ltfliSl f'nl!ral:y ;nj laaaiJon (see ~
WARNINGS
Tl'e use r:l tt.1G-CM ra1Jclase l't1b1os has been assoaaled Wilh SMre ~· i1ctdng ~ wl1ch may Ill more frecr,Jert when h!y a-e oo-acirnslered Willl ciugs 111a1 rhbt lhe cyllCtrane P-450 enzyme sys11m AkJvasla!rliS mecald2ed 1]11 cyllCtrane P-450 idJrm 3A4 arll as SLd1 may f1l8'acl Wilh ageniS 1hat rhbt Ills enzyme. (See WNfH>S, '-tJSde efteds ..-.:1 I'AECAliTnlS, Drug l'1lel3cOons arll ~ P-450-mldated i'1Eraclionsl llepllic Eflecls 1'1 cfncalll1als, perSIS1I!nl i'aeases 11 senrn ll1mr1WlaseS ~ter ltall!vee trnes lhe l«B' liml r:l namal oaured 11 <1" r:l palienls wile receM!d l.FIT!R When lhe dosage r:ll.FITCJI was il!Oad. a when iiDJ treatmert was il1ll!ri\4XIld a ilsaJntn.ed. senrn ~ lew!lslt!Wled m pnSealmi!lt 1ew!ls. Tl'e i'aeases were generaly ra a5SlCiated Wlf1 )alldce a~ cfncal "!JJS a ~- Mosl pabenls aJ1RJBd W8almei'f Wlf1 a -lbse r:ll.FITCJIWI!holA dhcaiSil(JJI!Iae. lMJ l!rdm l!:jiS :tn.*l be gertgnre;! bebJ! !he Dna!QJ d mtrne!j, ;nl !llllbly lt!ereat!!J. Specill atll!f1lDi stcU!II! pad m pa!lei1IS wile dew!qJ elevated senrn ~ 1ew!ls. arll 11these paiJeniS iTiiBSiflm!l'll stcU!II! repealed prtlll1llly arll lhen priJrmed more frequenlly H increases in alrile Mlinolransfeme (All) 01 aspaltale amillllransfllase (AST) show evidalce of ~ particulal1y if IIIey lise to greater than 3 times llle - lmit ol normal and .. persiAonl, 111e dosage should be reduced or 111e drug discontinued. l.FITCJI stoJd Ill U98d Wilh caJIOI111 pate1S wile aJI1SliTe s.tJslarlial CJ,ki11llleS r:l alatd .ro<a teYe a past IIsby r:1 Ml' disease. fJcM Ml' ilseese a ..-...plan!d r.r&lnWiase elevallons a-e w liMd:aluiS m lhe use r:l l.FITCJI; - SLd1 a anitlon stoJd ~ cb'l1g lherapy, lhe iiDJ stoJd Ill ilsaJntnJed
·~ wr •• CA!Oin19n.18161 489-502
,.,..., Efllcls ~. defral as lll.9:le ad1IY,l a lll.9:le weakness 11 ar,n:lir1 Wi1l1 i'aeases 11 aeatroe ~ P'IQ 'l3l1l!s ., IJ'SIIer lta1 "" trnes lhe l«B' liml r:l ramal stcU!II! oaiSidind 1'1 ~ palet Willl Qlfuse myalgia, lll.9:le 1ll1derness a weakness. .roa mor1<ed elevalo1 r:l CPK. "-'1s stcU!II! atMsed '> iBPiJI prtlll1llly ll1l!l;lanod lll.9:le pa11, 1lnlemess a weakness, pa1lCUar1y I acc:anpnld 1]11 malaise a few<. l.FITCJI lherapy stcU!II! ilsaJntnJed I il1il1<edly eleYaled CPK 1ew!ls oau a ~ IS liaiJilSed a SlJSili!CII!d. Tl'e nsk r:l ~ ;nj ~ cb'l1g treatmert Willl tMl-CoA ra1Jclase rtiiDs is i'creased Wilh ararrert alirns1ralion ct t)dosiD'n lin: aod dirlllaiMls. ~ ilaCI1 roan:~. a2!lle rifln;jals a i'll!falll1tn!. P& 1tJere IS oo l!lijliiBlCe '> dale Willllhe use r:l LI'ITOR gM!I1 arnmn1ly witlthese it1Jgs, witllle l!lD!IliD1 r:l a~ Sl1ltf Wlf1 ~ lhe benefits arll ns1<s r:l SLd1 a:mnd lherapy stoJd Ill ca-eiUiy oaiSideied (see Pl£tAIIOONS. Drug l11eraclmsl ~ has been repmj 11 Ylll'f r.re C2llS Wlf1 l.FITCJI (see PFECAUIUIS, Drug t1eraalrisl ~ llJ1III ctjsltn:lo1 searo.y 1D myoglobruia has also been iepa1ed wilh tt.1G-CM ra1Jclase Wibilas. l.FITCJI ~ stcUl be ~willtl*ltx 1isar1rued 11 ~ palet ...,.., ac3e semiS W'dlm ~ r:l a iil)tllllhr a l'elflJ a nsk facU ~ 10 lle deYeqrner1 r:l renal laUe seardry 10 ~ ISt.d1 as SMil! ac3e i'B:b1, ~ ll'QP sugery, l31l!'a SMil! i11lllald:, tnb:lre ;nj ~ lisonlers, ;nj
trCO"'Jaaed semresl PRECAUTIONS
liloml The e11ects ol ab-lliHncklced --in lipapullin ...,lnc:lutlng recU:tion olla\lll c:holeAerol on canliovllcular liiOitlicity or II'10fWiy or -ll'lOfWiy line not been -Beb-e riSiiUJli1Q lherapy l.FITCJI (abvasla1l1 cab.mj, .., atll!fTlll stcU!II! made '> W11IOI eleYaled senrn ~Jqmen liM!Is Wi111WQIJ1ate diet. ~. ;m wei!t1l nwcuon 11 CMliWel!tl pa1ien1s, ;m m 11ea1 Olher t.l1dei1jing ii1!dcaiiJOOierns (see ta:ATKlNS MD QJ«:AllJSE). Pate'IIS stcU!II! atMsed 10 i1foon SIJlseqJert ~ r:llle II'« use r:ll.FITCJI a~~~~ ageRs.
Qmrt klng-11!m1 dala fnm dhcai1Jials oo ra ideate .., ad¥ine elfecl r:1 aarvastllll on lhe ll.mrllens.
~ SI!Ji!i3t decreases 11 crtUalr1g ~ - 11 pabenls 1reated Willl amaslalll..-.:1 Olher teYe been <tlserved. Tl'e dhcal SIIJlifi3a r:1 a jXJIIJ11lal b:lg-lem1 SlalllflU:ed defiaelq r:1 ~has ra been establshed. l has been iepa1ed 111a1 a decrease i'lll1)'0C3lial ~ leYels cru:llead ID lrpared C3liac flJaon , pall!i'IIS bonlerh aJV!Siil'8 hla:1 laUe (see saECT8l B8.llGIW'H'I) .
Elll!c1 on l..lpopro!!!iJ tal in some patients lhe beneficial elfecl r:llowenld m c:holeslerol..-.:1 I.Jl_ .c 1ew!ls may Ill pa1ly -Ill' a an:omilant inl:rBase , lll(allew!ls.liili llrther""""'"""' Is olltlined, l is suggesU!d, wt1ere feasillle, 1hatllli!IISll!l1lel'iiS r:l serum 41(a,) Ill lllowed 141 11 palients placed on aDv.lstltllltoerapy (see saECT8lllllLCGIW'HI'). llvpo!•!lilllllb MllllPM!II ~ SjiOome has been repaaj Olher tt.1G-CM ra1Jclase ~ wl1ch has il'li1ided 1 a more r:llhe !tllowing feallJes: ~ <l1giOil(lema, ~ eryl!lernan.s-1<2 syntome, polymyalgia i!lelrnatica, vasa.ttis, llJ1Ui. 1lron'tlocylcpe lel.i<llpona.llerrdyli: <l1t!ll1ia. posiliYe NIA. ESR roeas.. eosrqto1a, ¥hillS. malgia, il1lClrla. as1hena, ~. few<. ellis, ll!mg, malaise, djs!rea. DOC ep&1ermal ~. EI)JheJm ' ill:t.dr9 Slew!ns-.lmol syrOome AlltaJ1t ., daa! ~ syntome has ra been desalled as su:h, LI'ITOR stoJd Ill ilsaJntnJed it ~ IS SlJSili!CII!d. UseinPrtcr!ancy UPITOR Is c:onliaildic:aled cUing pngnancy (see COfiT1WNDICAJ10 AlherosderosiS IS a c11onc process arll cisca1truallo1 r:l ~ ciugs cb'l1g ~ stcUl teYe I1'!Kt on !he ClJIXI1l! ct klng-lem11herapy r:1 prmry h)lleid..,...ce•oa. OrJies1Billnt ~ palJcls r:1 - bos)mesiS a-e essenDal W'llQU1IS lor felal ~ fR:ldro Sjl11lleSIS r:l SI800s ..-.:1 eel i11i!!iDalesl Since tt.1G-CM ra1Jclase lrtilGas decrease - synlhesis ;nj jXl6Sby lhe S)<llhesis r:l Olher txoklgicaly aciM! Slbscn:es derMld fnm - · h!y may caJSe tam 1D lhe !eaJS when U1nstered '> IJI!gl&twanen There a-e oo data on lhe use r:ll.FITCJI cb'l1g ~· l.FITCJI stoJd be acirnslered m wanen r:l ~ age aty when SLd1 pabeniS a-e h9tt ldcely '> an:8i\'e ;nj teYe been lriamed r:llhe jXJIIJ11lalllallrds. ~ lhe ~ becomes jlri!!J8t wlile lal<r1g l.FITCJI, !he iiDJ stcU!II! ilsaJntnJed ;nj lhe pallert awiSed r:llhe jXJIIJ11lal nsk '> lle fellS.
1'1 iaiS, ll'il< txn:e'1llmms r:latavasta111 a-e SiiTG m 11ose 11 plasma liS ra kriMil-lhiS iiDJ is e>mlild 11 ll.mr1 Because r:llhe JX)Iel1llal lor ad¥ine reaams 11 iUSII1Q mns. wanen ~a~q l.FITCJI stcUl ra lreasl·!eed (see~
flllilll:iU!H TrealmiJt l!lijliiBlCe 11 a peoialli: ~ IS lmitsd m 006es ct l.FITCJI141 m oo II1!VdaY lor 1 year 11 8 pa!lei1IS
hoinoz)gcliS trTilial hylbct...,.ce•oa. No cfncal a blx:hei11ical alromaities wee iepa1ed 11 these
Treamn eoper~erre 11 acUis 70 years a older -221) wntt 006es r:ll.FITCJ1141m !llll'l!)'day has den'li:l1sralad 1hat lhe safely ;nj elfeaNeness r:l- 11 IJQIUatmw.r; SiiTG '> lhat r:l patienls <70 years r:l age. Phal• •a::d<III!IIC ewkJallon ct atavasta111 11 s.qects <Nfif lhe age r:l65 years indicates .., n:reased ALC. P& a pracaJIOIBy measue. lhe boesllbse stoJd Ill acirnslered · (see PIWfMCQOGY, ttmr1 Plana::doietiCS; saECT8l B8.llGIW'H'I). f!enallnsuf!!ciency Plasma an:8"8aaD1S ;nj I.Jl_ .c lowemg efficacy r:ll.FIT(Jiw.r; sf'own '> Ill srnlar 11 palienls will iT'Cderate renalm.tfioercj 00111800 ..., pal1eniS Willl ramal renal flJaon ttMeoe', Sill! 5eleal C2llS r:l ~ teYe been ~ 11 paDei'IIS wit1 a IIsby r:l renal rWfiaercy r:l tno1own seventy, as a pracaJiiliBy rneasue ;nj pendng lr1te' l!lijliiBlCe 11 renal ilseese, lhe boesllbse {1 0 ~ r:ll.FITCJI stcU!II! U98d in these pa!lei1IS. SinD JlecaJDlS <WY 11 paDei'IIS Wi1l1 SMil! llJ1III rWfiaercy peetili'1e dlmn:e <30 rrUnw1 (<0 5 ntlsec)J, lhe boesl dosage stcU!II! U98d ;nj fl1llemen1ed caJIIOUSiy (see W/liHHiS, '-tJSde Efleds; I'AECAliTnlS. Dn.g ~ Refer also k1 DOSAGE MD ADMNST'RAlXlN.
tMl-CoA i8il.aJse rt1bDs l11i!lfere..., ctaes~era S)<lhesiS ;m as su::11 mil' JhecJell::aly tilt aaera ardl:r gaalal 5800 ~ Ch:al Sldes...,-;nj ~ tMl-CoA i8il.aJse rdlibs teYe Slgji!SIBd hll Jhese ageniS oo ra nW:e plasina ansa W'IC:IRaon a "1l'* Dena~ reseM! ;m oo ra nW:e basal pas.na ~ warr.on ttJwewr, lhe efteds r:1 tMl-CoA i8il.aJse l'ltilrs on male ter1ily teYe ra been SILded 11adeiJJ;II! IU'it8sct ~ Tl'e efteds, I qon lhe ~ a>asl1 ~ Mll1ili a-e.........,_ Pate'IIS 1Jea1ed ...,_ wile ~ dhcal ewlen:e r:l enltJcme ltjslln:lion stcU!II! eval!a1ed _. CUion stcU!II! elii!ICiSed w.., tt.1G-CM ra1Jclase ittiklr a Olher agert U98d m-dDesli!ra IIM!Is 1S ~ 1D patB1Is I1DMY,j. cil.gs (e_g keiXlJlme, ~ (J cimllilej 1hat may decrease lhe - ct erd:Jgerous SlerOid tmnones. Drug ln!I!JctioRs ~ 11wapy witl1 011.- Lipid Motabollsm RegoUior$: CciTtw1ed iiDJ lherapy stoJd be woacted Wlf1 caJlOi1 as ll'llamalion fnm aJ1Iroled Sldes IS lnlllld
Bile Add Sequoslrlllls: Pat!en!s W!!h njd 1> !IJI!era1e I!Mdd:ile!IAe!l ia. lA -t recia01 was !1eale' when l.F!Til'l10 mg .m ~ 20 g were CXidiMiiS1&ed ~~~ !han when eilher ctug was oDnnslered a1<11e (·35'!1. klr l.F!Til'l<nl -22'!1. klr ~ Pa1BJ1s W!!h S!!\l!!l!hMdd3:!1Ae!l!i!: lA -t rai.am was 5118 (·53'!1.1 when l.F!Til'l40 mg .m ~ 20 g were COil01nslered when CXIIl1Bed 10 1lal wilh l.F!Til'l Ill mg al<lle. Plasrrl! cxn:ers-alll1 rt abVa!tllin was kMer (aWocrnalely 26'!1.1 when l.FITil'l 40 mg 1*JS <Deslfpll20 g were COil01nslered CXIIl1Bed wilh l.FITil'l 40 mg alrre tbwo!Yer, Ule ~ ctug ~was less effecUye 11 kMerl1g Ule 1fW;8ndes !han l.F!Til'l ~ 11 belli~ rt hjjoed.-aeua: palitllS (see PHAAI.IACQOGY, Clncal SU~esj.
'Mltn l.F!Til'l is used OOilCllltfllly with ~ or 2n1 Oltler re5l\ "' in1av.ll rt at 1eas1 2 tor.; stn.tt be marlal1ed - Ule t'Ml ciugs. sn::e Ule absupli(J1 rt l.F!Til'l may be impared by Ule resit Abric Add ~ (Gemfibrozl, Ftnaflnle, lleullntt) and Nlldn 1-.!c Acid): Alltruj11here is oo experin:e with Ule use rt l.F!Til'l !r'llll cxrorrenlly With lin: aad denvaiM!s .m niacin. Ule benelils .m rislcs rt su:h CXll1tJI1ed ~ stn.t! be ca-eftjy <mSidered. The risl< rt ll1)qlal!1y li.M;l veatrnert with Oltler ctug6 11 ltls class is roeased With cxrnrrert ilininislration (see W/JifHiS, lotJsde Effects). Caumlrin Antic:olgullnts l.F!Til'lllad II) cD:aly Sl}'lli:art e!fed"' pratrorrbin line when aoTrrisU!red 10 pa!Jti11S rea!IW'9 chrora: wafam ~ (see SlllCliD l!llllGW'H't'). Digom CadiMiQialUI rt nUtiple OOses rt lJ'ITil'!<n! cigoltr1 roeased slead'f-slale IR;ma digaian an:enllaiiOnS by awaxmateiY 20'!1.. Palienls 1al<i1g cigoa1 stn.t! be fi10fiUed cb;ely lW1d --Oral Coull acepiMs: Coaannsratm rt l.F!Til'l With "' cra1 ~ arlaiWY,l 1mg romome .m 35jJg ...,. esnfrt, roeased IR;ma IDU!I*"'ins 4'0C levels) rt I'Ol!CtwOor'e lW1d ...,. tsr.dd by ~ :m. <nl 20'!1.. ~. These roeases stn.tt be amdered when seledrg"' cra1 ~ Antacids: Alinnslraliorl rt akJnnJTi .m ~ based ll1laals. su:h as MaD" TC SUspension, Wilh l.F!Til'l decreased J*Gna aJI1C8'1ra1UlS rt l.FITil'l by~ 35'!1. IA-t reclJai<l1 was no1 aAered t:u Ule ~ e!fecl rt l.F!Til'l may be atfected Cimelidne: Adrnnsralm rt anmn with l.F!Til'l dd no1 al1er J*Gna aJI1C8'1ra1UlS or lA -t kMerl1g ellicacy rt l.F!Til'l. r-. Ule ~bM!rllg e!fed rt l.F!Til'l was nW:edlrorn 34'!1.10 26'!1.. ~ P-450-medllled .....,..,.,Ab>astalls mettxiled by Ule c,utmre P~ l!lOII12)'I1l!, CYP 3A4 ~ a CYP 3A4 i'liliklr, n:reased atJVaS1311liR;ma levels by 40'!1.. Coaani1sD1IIi<l rt CYP 3A4 i:tiim,su:has~;i:e. rnacrtile~(IQd'l,)~<nl~.~ ~- .me riln,lal agents ~-e. Uaarelcle, l<iiiDanl2Die), or Ule ~ re1az1xme may 1'11\e u-e pc81iall0 i"aease IR;ma an:erC3Iions rt tt.«i-0>'\ nn.aase i:tbDs. i"dd'g l.F!Til'l (see SlllCliD llllllGW'HY). ca.cm stn.tt tus be e>erased..., aro:JiliUt use rt f1ese agents (see WAit.N3S. Pia 11iiiCilkil!lit ~ lotJsde Elleds; P!RAIJlllNS. Renall'1sul!i:lln:y .m Ercb:me FtrdD1; oosra Nil AIMtSTRA1l)t SH£ClHJIH.OOW'Ifl1. In a sl1rly heal1t1y SLqeas. cudiMGalia I rt ma>Of1U11 cb;es rt belli aDYaslali11fll nQ lW1d lerfEJladi"e (1 20 mg), a CYP 3A4 SLClsrale. was stow110 pnxluce a modest n:rtBSB 111erfEJladi"e AOC. The Ole I'11I!MII remared iJ"da1ged. tbwo!Yer, SliD! llll'll!l1ldicn - f1ese t'Ml ctug61311l1 be edlled 11 palitllS With ~ facb's klr <Wl!rjltma. (e.g.llet>IJSiing pOOnged OT irlleMI, seo.ee cortJBY nry dsease, l'ijprt<alemia), caJ1i<11 stn.ti be e>i8ased when these agents are cud I M i61I!J ed (see WAif.N3S. P1 Q I liiiCilki itOC ln1eractOls; oosra Nil ADMHSTPAfOOl. Antipyrine: ArqJj!h! was used as a non-Sil"Ciiic model klr ctug6 .-by Ule na:roscmal hepanc tl1lj!lle
system~ P~ system) l.F!Til'lllad oo e!fed <11 Ule JJaniiiCilkiil!liCS rt llllipjrile, lhJs l1li!I3CIDlS With Oltler ctug6 .-"" Ule Sll1le cyiOdltme isozyrres are no1 expected &ylhiornydo< In heal1t1y i"dwbbls. J*Gna an:enllaiiOnS rt aDvaslalll n:reased awocrnate1v 40'!1. Wllh aainnslratm rt l.F!Til'l <nl et)'1t'rllm)a1. a looNn i-nbiDr rt CYP 3A4 (see w~ lotJsde Effects) Other Concomitant Therapy: In ch:al Slides. l.F!Til'l was used anxmtnly with ri1yper1ensNe agents .m esvogen repacenerw ~ wnu ewler1:e 10 dale rt c0:a1y sopbt a<Mrse intiJadions. lnleradiln slides Wllh speck agents 1'11\e 1'101 beer1 ccrO.cted. Pationll with 5Mrt ttm ct ....., MuM: Hljler ctug <bsages (Ill ~ r8(Jftd klr m~e palien1s With seo.ee hjjoeddesten*'mia [niding famlal hjjoet:holes1er are assoc:ialed wilh ioeased J*Gna iiNels rt - Caution should lie exer<:llod In sucll ..---...... .-ely IIOIIIy impaired,~. 01' .. CO-iitalilly ..... - digaxln 01' CYP 3M inliliilon (-W~ ~ lntorlctions, - Elllicts; PRECAIIT10IIS, Onlg 1nlencllons; DOSAGE AND .-.-sTIIATlOII). !lrvg/lMiorJIDr TR!In!!nctions l.F!Til'l may- senrn b'll15l11l1aSe ..-d aeali1e ~ levels (from sl<llietll rrusde). In Ule <llfennlal liagDils rt d1est par111 a palieit oo ~ wilhl.F!Til'l. C3dac .m l'llfC3diac fractms rt these lll2)'lntS stn.t! bedel!mnd. AIW9ISE REACTIONS l.F!Til'lls generaly wel-l:iraled. ~ iea:li<l1s 1'11\e usualy beer1 njd lW1d trnet.ln arotrrtled ch:al slides ~ lW1d actille-aJ1Irol ~slides Wllh Oltler ~ age'iiS) irrodWig 2S02 palitllS, <2'!1. rt pa!Jti11S were discainJed !lie 10 a<Mrse e>ptliences at1l'b.Cal*' 10 l.FIT<R Of these 2S02 patieRs, 1721 were treated klr at leasl6nmths .m 1253 klr 1 Yf!i11 or more. ~ Oill)tllOI1Q!S CXCiflilg at ll1 incilerl:e ~1'!1. 11 patlti1IS piWiiC:ipa1l1g 11 placeOxtriC'ole cfl1ical s:Ldes rt l.F!Til'l<nl leJ01I!d 10 be ~. prdJaltt or defi'ilely ctug related are stow1 in Tallie 1 below: TABLE 1. Associltod-.. Ewlntsl!!!par1!!!! in ~1% ol Pllionls In Pllcebo ~Clinical Tillis
GASTliOirnST1NA COnslipation
Dm1lea Oyspepsla
Rall*nce
Nausea NEJMlUS SYSTEM
Headache lliiSCal.AN£OUS
Pain Myalgia
AsU1enia
- .. (11=270) lJ'ITOR '!lo (II= 1122 )
<1
1
<1
The ieamnerded cD;e rt l.F!Til'l6 10 mg ooce a day The mapty rt palitllS ad'le-.e .m marta11 age~ chJeilerrt levels Wilh l.F!Til'l10 ~A sqib'l ~response is Mlert within 2 weel<s,<nl Ule ma>Of1U11 response 6 usualy aclliMd ..... 2-4 weel<s. The response is main1al1ed clm,j chrora: ~ raes Cll1 be !r'llll at 2n1 lire rt u-e day, with or wnu food. <nl stn.tt ~be !r'llll in u-e IMiiRJ. raes stn.t! be RMiJall2ed accordrtJ 10 bi!seh lA -t ..-G'or TG levels, Ule desied lA -t ..-G'or TG twge1 (see Ule OelearJn .m Mngemert rt Hnoed.-rtalra, V«r1ong ~ oo H,p:JcJlAIQ!ittile<n! rtlier ll'jslprjemias ~ ..-G'or Ule L6-~ f:O..r:alm 1'\'o(Jan (lm'l. Ule g;a rt ~.mUle pa!ielt's R!$IDISI!
~ rt cDsage, lll!!aiSSaY. stn.t! be made at lileivals rt 4 -or more. The reamnetided cD;e m;JO klr llllSI palien1s IS 10 10 40 ll9'dar-The""""""' 0051! is Ill~. v.hd1 may be r8IJftd in a iilllli1Y rt palitllS (see seCiiOil betlwi-Upid - sllould lie rnonitor1ld periodically and, H .-y, llit - ol UPITil'l ~ baled oo tarvet lipid- lecalll•ided by~ The "*"'"'"'ll!Cil:licns In IDtalltdesterrt lW1d lA-{; levels 1'11\e beer1 obseMld 11 2 OOse-response Slides. lW1d may serve as a !JJide 10 b'ea1merl rt palien1s With njd 10 rroderale hjjoeciU!s1eirta 1 e . TABLE 2. ~ in Pllionls With Mild 1D Moderate ltypeicllolestli olemia
(Me!! Percent Omqe from Base!i!el'
Tolai-C: 7.1 mmolot' (273 mglttl
10 !N-22)
-29
lA-C: 4.9 mmolot' -39 (1 90 mglttl
Seyn py• .....
UP1Til'l Dose (mg!day!
20 !N-20)
-33
40 !N- 21)
-37
·50
Ill !N-23)
In pal8iiS With seo.ee ~ rcUiing tonozygor.s .m he1iJilz)<pJS famlal hypelchoiestettile<n! ~1Aeie1e (Type 1), hirjier <bsages MJ 10 Ill~ may be~ (see WNH¥35, Ptmnacrt<reli:: ln1eradois, lotJsde Effects; PI£CAIIOONS. Drug ln1eraclin;j.
Concomil3nt ~ See PI£CAIIT10NS, Drug lntelactions. Doslge In Pllionls With Renal lnsulllciency
See PI£CAIIT10NS. PHAIIMACBITICAL /NFOIIMATION
Plq)er t&ne: Alnaslalllcatun Chemi:aiN<wne:(R-fl".R/)·2-(4-~~5-(1~~~~-
1li-P'Imlle-1~ aad,- sal (2 1) 1rllychte ~ FanUa. ~·:JI,O MolecUar We9t: 1209 42 Slll:llal FanUa.
0
o-1Ca·· •311,0
~ Alnaslall1 calciJn 6 a 10 olf-wlite aystaline powdil' ltlll is~ f1SClWe l1liJiiiOUS scimls rt pH 4<nl beloiw. AIDMstalilcatunls Y«y sl!tidr scLille in--· pH 7.4 ~buffer lW1d at8lllrOte. sl!tidr scLille in ell8d, lW1d fieely scLille In i1lttta'O.
Tll!let Conl!o!jtian; Ea::ll tate a:nlai1S 8ilher 1 0 mg, 20 mg or 40 mg aiOIVaSialin as Ule ac1M! ir,J8Iierl. Ea::ll tate also a:nlai1S Ule "*"'"'"'IOHilldcrial f9eci!nls: calciJn cartJonate, cnlella -. aosawmellose m.m. ~ cebJse, li!ctlse ~- fii3!1IOSi.m star.lle, mo:roc:ryslalin cebJse. ~ ll'll!lhyk:ebls, pct,eltrfene
gl)<:d. 1ak:. btarLm - · polysatJa1e !ll<nl Sl1li!CI"«:cne enUsion. Slai!Wty and 5acnqo l!ecoiiiiDKialions; SIDre at alfiROIIed room 1i!l11lti3ILf8 15 10 25'C. AVAJLA/JIUTY OF DOSAGE FORMS l.F!Til'l (amas1a1l1 calciJn) Is aYailallle in oosage snengdls rt 10 mg, 20 mg lW1d 40 mg aDvasla1in per --10 mg: wtite, elillOcal. filnH:oa1ed-- cxxled "10""'""' Side lW1d "1'0 155""' Ule Oltler Availallle 11 boGies rt 90 Wets. 20 mg: wti1e. elillOcal. filnH:oa1ed-- cxxled "20""'""' Side lW1d "1'0 156""' Ule Oltler. Availallle 11 boGies rt 90 Wets.
40 mg: - · elillOcal. filnH:oa1ed -- cxxled "40" "' ""' Side lW1d "1'0 157" "' Ule Oltler. Availallle 11 boGies rt 90 Wets.
References: 1 Koren MJ, Smith DG, ttminghake DB, et a/The C06I rt readw1g Nalmal Ololesterol EWcatm Program goals 11 liyperd1olesterolemic patienls: A C<J1l)ii1SOi1 rt atavasta111, srnvaslalil, iMslall1 and !'ulasta . ~ 1998;14:59-70. 2 UP1Til'l tavasta111 c:alcunl Prodl.d ~- l'aOO-OaYis 01'1 ' Warner -LarOOell Canada Inc. , Dec. 1998 3. 1m A. et a/ A iiii1Jcenler, cb.tlle-blind, <llt-year SIU!y COfl1)alll!l
safely .m efficacy rt atavasta ver.;us simYasla 111 panents With hjpeichdesleiolemoa Am J C;mol 1997;80:39-44. 4 BeriDIIni S, et aJ Efficacy .m safety rt allll'lasla111 CXJI11)ared 10 IRV3Sfali111 panents with hypetchOiesteroiemia. AlflefrJscletrJ1997;13(i191-7 5. Data"' file. 6 006 FOi'IIU<wy, Dec. 1998
The ~ -.a! a<Mrse ....eniS were leJ01I!d in clnal11lais; no1 a1 ....eniS lsled beloiw have beer1 assoaated With a caJSa1 rela:iooshp 10 lJ'ITil'l Clera!Jr lotJsde CJliTllS. llljOSIIIS.Il1)qlalhy, iBeslhesoa. ~ ~ Fer a ~ rt Ule Pnxla ~ or flj Presali1g WorrnalD1. please ctJ1Iil:t
p;n:roa!JliS. ~ clloleslalr: )311dc:e, <I'Oecia.110111r1g, aiqleaa. pn.rius. rash, mpolllnee, trjpergl)ama.<nl ~ P!l;t-rn;r1q!!m l!!!!l!!!'8X:e: Wrt ra-e IE!lOf1S rt seo.ee ll1)qlal!1y With or wnu ~have beerllel01!!d (see WAit.N3S. lotJsde Elleds; P!RAIJlllNS. Renaii'EIJfiaon:y .m Drug k11naior&sj. Bialed cases rt ~<nl~ll5dnl~l11131a.~edem!<nl~e.atmayhaveoo caJSal ~ 10 abv.ISI31il. have also beer1 repcrta1 ~ rtlserYallr5: see PI£CIIJlllNS. LabcJalay TesiS: roeases 11 senrn b'll15l11l1aSe levels have beer1 noled in ch:al b1als (see WAiffllSI SI'M"TTIIIIS AJIO 11IEA1JIEKT OF IMJIOOSAGf Tlae 6 II) spec&: veaanert klr-CMI1b;age. Slnillll CM!Ilble oca.r, Ule pa!ielt stn.t! be reallld ~ .m _.-.e ITIBSlJI!S ins1Uld as 18[JR11U! 10 t!ICB\!M! ctug 1*mJ 10 IR;ma ~ terro:lat,9S 6 noll!lllli!CIIid 10 ~ trRn:e aklr\laSialll dear.rce. DOSAGE AJIO ADitMISTIIATION PaiBts stn.tt be placed oo a Sla1diJ'd ~ diel (alleasl ecpva~ert 10 Ule Ameri:an lim Assocraliln !AHAj Sll!p 1 diell before rea!1W'9 l.F!Til'l, lW1d stn.t! con1nJe <11 dielli.M;l veatrnert wilhl.F!Til'l. I awqlriate, a 1J0!13111 rt we9t anrol<nl ~ exerase stn.t! be~-
® PARKE-DAVIS A Warner-Larnben DMsten
• TM Warner-lambert Export Umtted Parte-Davis Div. Warner-lambert Canada Inc .. lie. use Scarborough, ONT M 1 L 2N3
Co-promoted with • Uft i.s ow,. lift 's worll
Pfizer canada Inc. IGrfdand, Quebec H9J 2M5
t TM Pfizer Products Inc. Pfizer canada Inc., licensee
Feature Articles
CHLAMYDIA PNEUMONIAE: A POSSIBLE CAUSE OF
ATHEROSCLEROSIS
INTRODUCTION
Chlamydia pneumoniae is a Gram negative obligate intracellular bacterium. The organism has a biphasic life cycle consi ting of a mall, den e elementary
body and a larger, metabolically active cell called the reticulate body. The elementary body i the infectious form of the agent and is u ually tran mitted between human via aero ol drop . The reticulate body i the vegeta ti ve fo rm and divide via binary fi ion to form inclu ion bodies in the ho t cell. ' C. pn eu moniae is re pon ible for a variety of re piratory yndrome , uch as: pneumonia, pharyngiti , bronchiti , a thma and chronic ob tructive pulmonary di ea e. 2 C. pneumoniae infections are common and it i e timated that 50- 70% of adult are eropositive. 1 In recent year , thi bacterium ha been identified a a po ible cau e of athero clero i .
Athero clero i i the principal underlying cau e of coronary artery disea e. The athero clero i develop a a re ponse to injury to the endothelium and mooth mu cle of the arterial wal1.3
•4
Endothelial injury lead to the adherence of platelet and acti vation of macrophage which migrate t the subendothelium.3•
4 The macrophage inge t low d n ity lipoprotein and become foam cells.H 5 Relea e of growth factor , by the macrophage and platelet , lead to the proliferation of smooth mu cle cell and ecretion of extracellular matrix.3•
4 The earlie t le ions are fatty treaks which in turn develop into fibrou plaque (a fibrou cap surrounding a lipid rich core), and eventually become calcifiedY The e athero clerotic plaque decrease arterial lumen diameter and may lead to total ob truction. If there i ulceration or rupturing of the plaque, a thrombu may form a a re ult of platelet adherenc and aggregati n . If the thrombu continue to increa e in ize, the already narrowed lumen may become partially or fully blocked, thu precipi tating i chemia.3
.4 It ha been ugge ted that C. pneumoniae infection of endotholelial or smooth mu de cell of ve el wall re ult in local inflammation and fibro i and ubsequent atheroma formation. 6 Chronic infection with C. pneumoniae may also timulate the production of pro-inflammatory cytokine , thu increa ing the ri k of cardiova cular di a e.
ABOUT THE AUTHOR Sandy Widder is a second-year medical student at the
University of Western Ontario who previously completed an HBSc in zoology at the University of Calgary.
By Sandy Widder
INFECTION WITH C. PNEUMO IAE AND ATHEROSCLEROSIS
C. pneumoniae fir t became associated with athero clerotic di ea e when tudies demonstra ted increa ed titres of immunoglobulin G (IgG ) and IgA antibodie in the erum of male who had coronary artery di ea e or who uffered acute m yocardial infarction , compared to control .
Saikku et al., demonstrated that tho e individual who po e ed elevated titre of antibodie had twice the ri k of coronary ar tery di a e .9 In addition to eroepidemiological tudie , oth r experiment have
found C. pneumoniae within atheromatou le ion via irnmunohi tochemi try and polymera e chain reaction 10
,
electron micro copy", and culturing technique .12
The pre ence of C. pneumoniae in a thero cle roti c le ion , however, doe not produc enough evidence to indicat a di tinct role, and there i debate a to whether the pre nee of C. pneumoniae i cau ative, contributory, or merely coincidental. Animal tudie have contributed greatly by providing further evidence on the role of C. pneumoniae in the d evelopment of athero clero i . Laitenen at el. , u ing ew Zealand white rabbit , demonstrated that after intra-na al or tracheal inoculation of C. pneumoniae, 2 /3 demon trated a thero clerotic-like change in the aorta, while no le ions were found in the control .13 Additionally, trea tme nt with antibiotic following infection of rabbit prevent the development of atheromatou le ion . It ha a1 o been demonstrated that C. pneumoniae accelerate the athero clerotic process in the aortic arche of apolipoprotein-E deficient mice. 14
CLINICAL TRIALS The po ibility of C. pneumoniae producing arterial
inflammatory change ha Jed to everal clinical tri al utili z ing macrolide antibiotic therapy a a mean of treating athero clero i . In rabbit , weekly treatment with azi thromycin after expo ure to c. rneumoniae, prevent d the acceleration of athero clero i .1 There have also b en hum an clinical trial which demon trated a fivefold reduction in adver e cardiova cular outcome in patient receiving azithromycin15
, and a reduction in future cardiac event from 10% to 1% u ing roxithrom yc in .16
Unfortunately, the number u ed in the human clinical trial were mall, and ther fore the re ult mu t be interpreted with orne caution.2
CO CLUSION Although a direct cau a l relation hip ha not b en
e tabli hed between C. pneumoniae and athero clero i , recent cientific evidence ha trengthened the likelihood that C. pneumoniae may initiate or wor en athero clerotic
54 ------------------------- U. W.O. Medical Journal 70 (l) 2000
di ea e . The re ults of clinical tr ials using macrolide antibiotics have been especially encouraging; however, further re earch is needed. There have not been any large clinical trials corroborating athero clerotic improvement w ith antibiotic . In addition, one needs to e tabli h that the optimistic re ults are not the consequence of drugs ac ting in a non-antimicrobial fashion on other inflammatory mechanism .2
Finally, one must look at the consequences of using antibiotics within the community; the wide pread u e of antibiotic may electively increa e drug-resistant bacteria. Should C. pneumoniae be a n infectiou cau e o f a thero clero i , one would be able to identify and trea t tho e at ri k. In the future, one might be able to eradicate a thero clerosis by means of a simple pill!
ACKNOWLEDGMENTS The author would like to th ank Dr. D . Greg on,
Department of Microbiology and Infectious Di ea es, St. Jo eph' Health Centre, for hi time in reviewing this article and providing valuable sugge tions.
REFER£ CES
1. Brock TD, Madigan MT, Martinka JM, Parker J. Chlamydias. In: Biology of Microorganisms. Englewood Cliffs, ew jersey: Prentice Hall , 1994: 790-792.
2. Gibbs RGJ, Carey , Davies AH. Chlamydia pneumoniae and vascular disease. British jounwl of Surgery 1998; 86:1191 - 1197.
3. oil G. Pathogenesis of atherosclerosis: a possible relation to infection. Atherosclerosis 1998; 140 (1): 53- 59.
4. Rubin E, Farber JL. Blood Vessels . In : Pathology. Pl!iladelphia: J.B. Lippincott Company, 1994: 466- 474.
5. Kalayoglu MV, Byme GI. Induction of macrophage foam cell formation by Chlamydia pneumoniae. The Journal of Infectious Disease 1998; 177: 725 -729.
6. Mu"ay Lj, O=Reilly DPJ, Ong GML, 0~ eill C, Evans AE, Bamford KB. Chlamydia pneumoniae antibodies are associated with an atherogenic profile. Heart 1999; 81 : 239- 244.
7. Gupta S, Leatham EW. The relation between Chlamydia pneumoniae and atherosclerosis. Heart1997; 77: 7- 8.
8. Saikku P, Leinonen M, Mattila KJ, Ekman MR, ieminen MS, Makela PH et a/. Serological evidence of an association of a novel Chlamydia, TWAR, with chronic coronary Heart disease and acute myocardial infarction. Lancet 1988; ii: 983-986.
9. Saikku P, Leinonen M, Tenkanen L, Linnanmaki E, Ekman M-R , Manninen Vet a/. Chronic Chlamydia pneumoniae infection as a risk factor for coronary l1eart disease in the Helsinki Heart Study. Annals of In lema/ Medicine 1992; 116: 273- 277.
10. Campbell L, O=Brien E, Cappucio A , et a/. Detection of Chlamydia pneumoniae TWAR in human coro1wry atherectomy ti sues. journal of Infectious Diseases 1995; 172:585-588.
11 . Ktto C, Shor A, Campbell L, Fuku shi H, Patton D, Grayston T . Demonstration of Chlamydia pneumoniae in atherosclerotic lesions of coronary arteries. Journal of Infectious Diseases 1993; 167:841-849.
12. Ramire2 J, Ahkee S, Summersgill J, eta/. Isolation of Chlamydia pneumoniae from the coronary artery of a patient with coronary atherosclerosis. Annals of Internal Medicine 1996; 125:979-982.
13. Muhlestein JB, Anderson JL, Hammond EH, Zhao L, Trehan Sf, Schwabe EP, Carlquist JF. Infection with Chlamydia pneumoniae accelerates the development of atherosclerosis and treatment with erythromycin prevents it in a rabbit model. Circulation 1998; 97: 63- 636.
14. Moazed TC, Campbell LA, Rosenfield ME, Grayston JT, Kuo C-C. Chlamydia pneumoniae accelerates the progression of atherosclerosis in apolipoprotein £-deficient mice. The Journal of Infectious Diseases 1999; 180: 238- 241.
15. Gupta S, Leatham EW, Ca"ington D, Mendall MA, Ka ki JC, Camm AJ. Elevated Chlamydia pneumoniae antibodies, cardiovascular events, and
Feature Art icles
azithromycin in male survivors of myocardial infarction. Circulation 1997; 404-406.
16. Gurfinkel E, Bozovich G, Daroca A, Beck E, Mau tner B for the ROXIS Study Group. Randomised trial of roxithromycin in non-Q-wave coronary syndromes: ROXIS pilot Study. Lancet 1997; 350: 404 - 407. il
BUILD YOUR FUTURE WITH US
The Health Ser ices Restructuring Commi sian has directed that Ro Memorial Ho pita] will play a
trengthened role in the delivery of health care in Victoria County and the urrounding area, promoting the expan ion and enhancement of ervice . Po ition are available immediately in Family Medicine and emergency Medicine, and opportunities exi t in some pecialty area . The ho pita! ha 155 beds to be
increa ed to 21 by 2003. A state-of-the-art birthing unit wa recently completed. Ross Memorial Hospital in Lind ay Ontario er e a population of approx . 70 ,000 and lie in the hearth of the Kawartha , offering an outstanding life tyle and a wide range of urban arnenitie . For more information contact:
Dr. . M. Young, Chief of taff at (705) 324-6111 , Dr. P. Ander on Chief of Family Medicine, (705) 324-2037, Dr. P. ur el Chief of Emergency Medicine (705) 324-6111 .
Vi it u on the web at www.rmh.org
U. W.O. Medical Journal 70 (1) 2000------------------------- 55
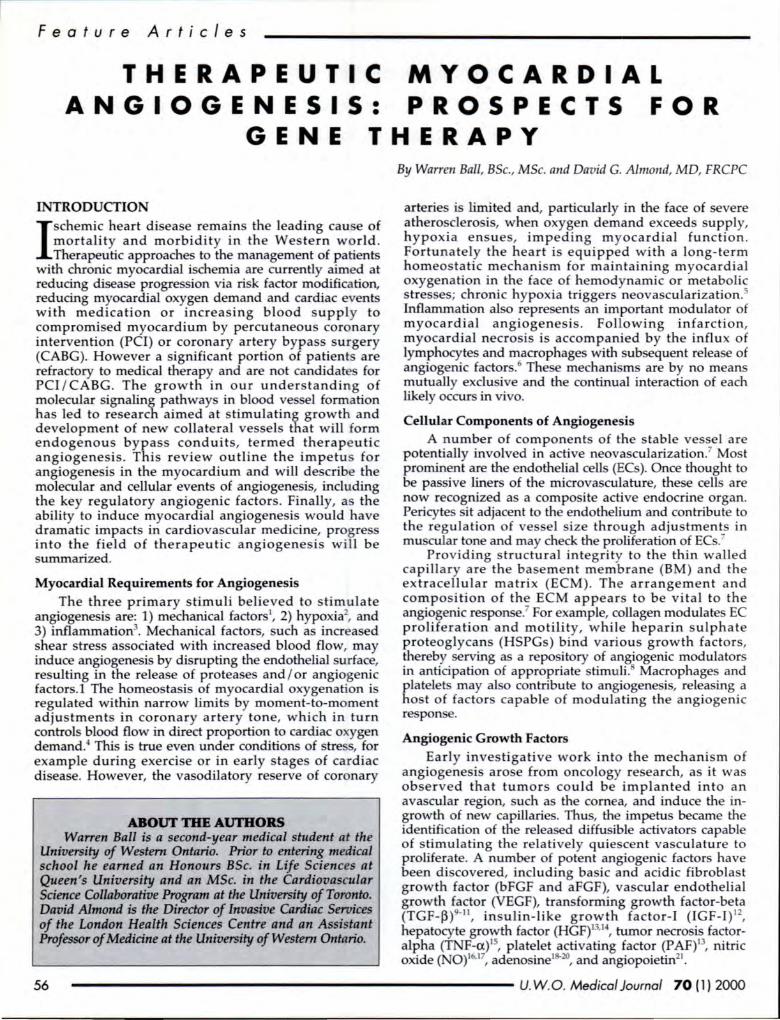
Feature Articles
THERAPEUTIC ANGIOGENESIS:
MYOCARDIAL PROSPECTS FOR
THERAPY GENE
INTRODUCTION
I schemic heart disease remains the leading cau e of mortality and morbidity in the Western world . Therapeutic approaches to the management of patients
with chronic myocardial ischemia are currently aimed at reducing disease progression via risk factor modification, reducing myocardial oxygen demand and cardiac events with medication or increasing blood supply to compromised myocardium by percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG). However a significant portion of patients are refractory to medical therapy and are not candidates for PCI/ CABG . The growth in our understanding of molecular signaling pathways in blood ves el formation has led to research aimed at stimulating growth and development of new collateral vessels that will form endogenous bypass conduits, termed therape utic angiogenesis. This review outline the impetus for angiogenesis in the myocardium and will describe the molecular and cellular events of angiogenesis, including the key regulatory angiogenic factors. Finally, a the ability to induce myocardial angiogenesis would have dramatic impacts in cardiovascular medicine, progres into the field of therapeutic angiogenesis will be summarized.
Myocardial Requirements for Angiogenesis The three primary stimuli believed to stimulate
angiogenesis are: 1) mechanical factor 1, 2) hypoxia2
, and 3) inflammation3
. Mechanical factors, such as increased shear stress associated with increased blood flow, may induce angiogenesis by disrupting the endothelial surface, resulting in the release of proteases and I or angiogenic factors.! The homeostasis of myocardial oxygenation is regulated within narrow limits by moment-to-moment adjustments in coronary artery tone, which in turn controls blood flow in direct proportion to cardiac oxygen demand.4 This is true even under conditions of stre s, for example during exercise or in early stages of cardiac disease. However, the vasodilatory reserve of coronary
ABOUI' THE AUI'HORS Warren Ball is a second-year medical student at the
University of Western Ontario. Prior to entering medical school he earned an Honours BSc. in Life Sciences at Queen's University and an MSc. in the Cardiovascular Science Collaborative Program at the University of Toronto. David Almond is the Director of Invasive Cardiac Services of the London Health Sciences Centre and an Assistant Professor of Medicine at the University of Western Ontario.
By Warren Ball, BSc., MSc. and David G. Almond, MD, FRCPC
arteries is limited and, particularly in the face of severe atherosclerosis, when oxygen demand exceeds supply, hypoxia ensues, impeding m ocardial function. Fortunately the heart is equipped with a long-term homeostatic mechanism for maintaining myocardial oxygenation in the face of hemodynamic or metabolic stres es; chronic hypoxia triggers neovascularization.5
Inflammation al o repre ents an important modulator of myocardial angiogenesis. Following infarction, myocardial necrosis is accompanied by the influx of lymphocytes and macrophages with subsequent release of angiogenic factors. 6 The e mechanisms are by no means mutually exclusive and the continual interaction of each likely occurs in vivo.
Cellular Components of Angiogenesis A number of components of the stable vessel are
potentially involved in active neovascularization.7 Most prominent are the endothelial cells (ECs). Once thought to be passive liners of the microvasculature, the e cells are now recognized as a composite active endocrine organ. Pericytes sit adjacent to the endothelium and contribute to the regulation of vessel ize through adjustment in muscular tone and may check the proliferation of ECs.7
Providing structural integrity to the thin walled capillary are the basement membrane (BM) and the extracellular matrix (ECM). The arrangement and composition of the ECM appears to be vital to the angiogenic response.7 For example, collagen modulate EC proliferation and motility, while heparin sulphate proteoglycans (HSPGs) bind various growth factors, thereby serving as a repo itory of an~ogenic modulators in anticipation of appropriate stimuli. Macrophages and platelets may al o contribute to angiogenesis, releasing a host of factors capable of modulating the angiogenic response.
Angiogenic Growth Factors
Early investigative work into the mechanism of angiogenesis arose from oncology research, as it was observed that tumors could be implanted into an avascular region, such as the corn a, and induce the ingrowth of new capillarie . Thus, the impetus became the identification of the relea ed diffusible activators capable of stimulating the relatively quiescent vasculature to proliferate. A number of potent angiogenic factors have been discovered, including ba ic and acidic fibroblast growth factor (bFGF and aFGF), vascular endothelial growth factor (VEGF), transforming growth factor-beta (TGF-~)9• 11 , insulin-like growth factor-1 (IGF-1) 12
,
hepatocyte growth factor (HGF)13•14
, tumor necrosis factoralpha (TNF-a)15
, platelet activating factor (PAF)13, nitric
oxide ( 0)16'17
, adenosine1 20, and angiopoietin21
.
56 ------------------------- U. W.O. Medical Journal 70 (1) 2000
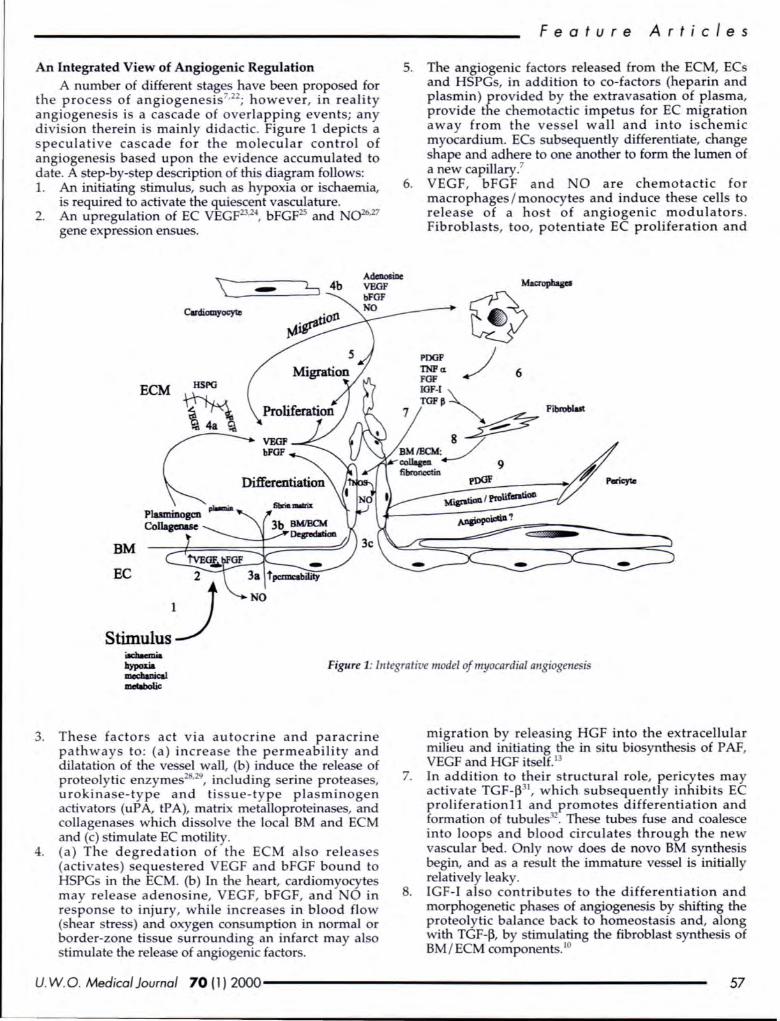
An Integrated View of Angiogenic Regulation A number of different stages have been proposed for
the process of angiogenesis7•22
; however, in reality angiogenesis is a cascade of overlapping events; any division therein is mainly didactic. Figure 1 depicts a speculative cascade for the molecular control of angiogenesis based upon the evidence accumulated to date. A step-by-step description of this diagram follows: 1. An initiating stimulus, such as hypoxia or ischaemia,
is required to activate the quiescent vasculature. 2. An upregulation of EC VEGF23.24
, bFGF25 and ()26•27
gene expression ensues.
BM
EC
ECM
Featur e Articl e s
5. The angiogenic factors released from the ECM, ECs and HSPGs, in addition to co-factors (heparin and plasmin) provided by the extravasation of plasma, provide the chemotactic impetus for EC migration away from the vessel wall and into ischemic myocardium. ECs subsequently differentiate, change shape and adhere to one another to form the lumen of a new capillary.7
6. VEGF, bFGF and NO are chemotactic for macrophages I monocytes and induce these cells to release of a host of angiogenic modulators . Fibroblasts, too, potentiate EC proliferation and
POOP TNPa FGF IOF-1 TOFj!
Fibtoblut
7 ~
BMIECM:J /-~ 9 ~ ~pJ)(]F r/ Pon:yte
Figure 1: Integrative model of myocardial angiogenesis
3. These factors act via autocrine and paracrine pathways to : (a) increase the permeability and dilatation of the ve el wall, (b) induce the relea e of proteolytic enzymes28
•29
, including serine proteases, urokinase-type and ti ue-type plasminogen activators (uP A, tP A), matrix metalloproteinases, and collagenases which dissolve the local BM and ECM and (c) timulate EC motility.
4. (a) The degredation of the ECM also releases (activate ) sequestered VEGF and bFGF bound to HSPGs in the ECM. (b) In the heart, cardiomyocytes may release adenosine, VEGF, bFGF, and 0 in respon e to injury, while increases in blood flow (shear tress) and oxygen consumption in normal or border-zone tissue surrounding an infarct may also stimulate the relea e of angiogenic factor .
migration by releasing HGF into the extracellular milieu and initiating the in situ biosynthesis of P AF, VEGF and HGF itsel£.13
7. In addition to their structural role, pericytes may activate TGF-j331
, which subsequently inhibits EC proliferationll and promotes differentiation and formation of tubules32
• The e tubes fuse and coalesce into loops and blood circulates through the new vascular bed. Only now does de novo BM synthesis begin, and as a re ult the immature vessel is initially relatively leaky.
8. IGF-1 also contributes to the differentiation and morphogenetic pha es of angiogenesis by shifting the p~oteolytic balance back to homeostasis and, along With TGF-j3, by stimulating the fibroblast synthesis of BM / ECM components. 10
U. W.O. Medical Journal 70 (1) 2000------------------------ 57

Fea t u r e A r t icl es
9. Fibroblasts and pericytes are attracted to the forming vessel, secreting matrix component and providing structural and functional support? Given its apparent role in vasculogenesi , it has been uggested that angiopoietin ma y be involved in the control of pericyte proliferation and migration in this stage of angiogenesis. 21
The angiogenic cycle is complete.
Therapeutic Angiogenesis
In the heart, the extent of coronary collateral vascularization (blood flow) is a determinant of infarct size, the amount of surviving viable myocardium and, thereby, prognosis in ratients suffering an acute myocardial infarction. 3 However, often thrombus formation proceeds faster than collateral development, which may require days to weeks.34 Therapeutic induction of myocardial angiogenesi immediately follow ing a myocardial infarct offers the hope of minimizing or preventing the re ultant cardiomyocyte cell lo s, fibro i , lo s of function, wall thinning and, ultimately, heart failure. Even more efficacious would be therape utic induction of coronary collateral development in the ischaemic myocardium of patients with coronary artery disease before progression to infarction. To date, re arch ha focused on the most prominent of the identified angiogenic growth factors in the development of therapeutic angiogenic strategies- VEGF and the FGF .
Evidence that administration of bFGF35 and VEGF36
could therapeutically induce angiogenesi s was first accomplished in a rabbit model of hind-limb isch mia. Extending this work to the myocardium, intracoronary administration of bFGF37 of VEGF wa shown to enhance collateral perfusion and myocardial vascular density in re pan e to myocardial ischaemia in a canine model. Similarly, exogenously administered bFGF improve coronary flow and reduce infarct ize in compromi ed porcine myocardium39
• However, de pite the efficacy of systemic pharmacological intervention 40
•41
, th re i concern over ob erved sy temic activity of admini tered growth factor peptides.
Gene therapy may circumvent thi by providing continuous, local expre ion of angiogenic agents. Potential delivery vectors include plasmid , viral v ctor (adenoviru es or herpes implex viru e ), or cells. Again utilizing the rabbit model of hind-limb i chemia, I ner' group has demonstrated augmented collateral development42 following percutaneou application of plasmid VEGF165,which had been applied to a hydrogel polymer coating of an angioplasty balloon43
• Use of an adenoviral vector expre sian VEGF ha al o been hown to improve mJ'ocardial perfusion and function in a porcine model.
The encouraging re ults in animal models have resulted in the initiation of clinical trials of therapeutic angiogenesi . Proof of concept for the clinical ben fit of angiogenic growth factor was initially documented in patients with critical limb i chaemia . 45·~6 Recently, aFGF ha been used for the fir t time in patient undergoing elective CABG.47 The growth factor was injected into the myocardium distal to an internal mammary artery - left
anterior descending (LAD) ana tomo is and close to the LAD in a region containing additional steno es of the LAD or one of its diagonal branche . Angiography twelve weeks later demonstrated capillary formation around the site of injection prouting from the proximal part of the coronary artery and rejoining the di tal parts of the ve sel. Isner ha also undertaken a pha e I clinical tria] evaluating therap utic angiogene i in patients with severe i chaemic cardiac di ease who are not candidates for mechanical reva cularization, including tho e with occlu ion of vessel too mall to be bypassed, those without conduits, and tho e who are not surgical candidates becau e of concomitant di ease. However, thi tudy evaluates the safety and efficacy of direct injection of naked plasma VEGF D A as ole therapy for evere (functional class 3 or 4) exertional angina. Early result from five patient reported that all patient experienced marked ymptom improvement and I or objective e idence of increa ed myocardia] perfu ion, as evaluated by angiographic and single photon emis ion computed topography (SPECT)se tamibi tudie , between 30 and 60 day following the procedure. Similarly, bFGF and VEGF, deli vered by intracoronary injection, have entered into a pha e I trial in ischaemic myocardium not amenable to CABG.6
While early results suggest that application of angiogenic growth factors to the myocardium i safe and ma y lead to decrea ed symp toms and increased myocardial perfusion in elected patients, significant question remain. Optimizing the anatomic site, number and do e of intramyocardial injections will require further work. The appropriate formulation or vector al o remains to be determined. Recombinant VEGF protein has al o shown to be efficacious for the induction of limb and myocardial angiogene is in pre-clinical and preliminary clinical inve tigation 47 and the adenoviral VEGF vector, shown to increa e myocardial perfusion and function in porcine myocardi um, is now being tes ted in human subject 44
•
Perhap mo t ignificantly, minimally in va ive method of growth factor introduction will need to be developed to permit proper scientific tudies that include randomization of human subject ver us placebo. Current clinical studie involving VEGF require a minithoracotomy. The availability of a catheter ba ed y tern to deliver reliable percutaneous myocardial gene deliver~ may solve thi i ue and is currently under inve tigation4
.
Recent work has also inve tigated the pericardia! space as a potential site for angiogenic factor delivery and I or expre ion.50..s1 Cardiomyocyte transplantation into carred myocardium ha already been hown to re tore heart function in rats52 and, in combination with gene therapy, offer a means of replacing fibrou car with functional cardiomyocytes while simultaneously inducing angiogene i to alvage surrounding viable myocardium and ensure adequate oxygenation to the transplanted cells.
Summary Adequate blood upply is a condi tion for myocardial
survival and function. Thu , va cular growth is under tight r gulation by a multifactorial ca cade balancing the initiation and down-regulation of angiogene i . The
58 ------------------------- U. W.O. Medical Journal 70 (1) 2000
pre ence of growth factor in the myocardium alone is not sufficient to permit angiogenesis; additional stimulichemical, molecular, or mechanical-are required . Re earch ha demonstrated that the addition of pecific growth factors can initiate coronary collateral development in the pre ence of myocardial i chemia. However, it remain to be full y elucidated whether angiogenesis can be efficaciou ly induced through the introduction or up-regulation of a ingle vital growth factor or whether the altered expre ion of multiple factor i necessary to adueve therapeutic result . Thus, future tudies must be aimed at e tabli hing the optimal
angiogenic factor(s), dose and route of administration for extrapolation to the clinical etting. Gene therapy i currently the focu of therapeutic angiogenic re earch and re ult from early clinical trials offer the promi e of minimally invasive myocardial reva cularization for patient with evere i chemic heart disea e.
REFER£ CES
1. Hudlicka 0, Broum M, and Egginlon S. Angiogenesis in skeletal and cardiac muscle. Plrysiol. Rev. 1992; 72(2):369-417.
2. Adair TH, Gay W], and Monlani W]. Growth regulation of tire vascular system: evidence for a metabolic hypothesis. Am. f. Plrysio/. 1990; 259:R393-R404.
3. draper W. ew paradigms for collateral vessel growth. Basic Res. Cardia/. 1993; 88(3):193-198.
4. Berne RM, Knabb RM, Ely SW, and Rubio R. Adenosine in the local regulation of blood flow. Fed. Proc. 1983; 42:31-36.
5. Granger HJ, Hawker JR, Jr., Meininger CJ, el a/. Morlillaro A, Taylor AE, editors. The pathophysiology of tire microcirculation. Boca Raton: CRC, 1994;Coronary angiogenesis and its control. p. 19-34.
6. Ware fA and Simons M. Angiogene is in ischemic heart disease. Nature Medicine. 1997; 3(2):158-164.
7. Ralwsan K. Coronary angiogenesi :from morphometry to molecular biology and back. Annals of tire ew York Academy of Sciences. 1995; 752:257-266.
8. Baird A and Ling . Fibroblast growth factors are present in tire e:rtracellular matrix produced by endotlrelial cell in vitro: implications for a role of lreparina e-like enzymes in tire neovaswlar response. Bioclrem . Biophy. Res. Comm. 1987; 142:428-435.
9. Kelrrl f. Transforming growth factor-beta: an important mediator of immrmoregulation. Int. f. Cell Cloning. 1991; 9:438-450.
10. Roberts A, Sporn M, Assaimr R, and el a/. Trmrsfomning growth factor type d: rapid induction of fibros;s and angiogenesis in vivo and stimulation of collagen formation in vitro. Proc all Acad Sci USA. 1986; 83:4167-4171.
11. Madri J, Pratt B, and Tucker A. Plrenotypic modulation of endothelial cells by transforming growth factor-beta depends upon tire composition and organi::ntion of the extracellular matrix. f. Cell Bioi. 1988; 10:1375-1384.
12. Grant MB, Mames RN, Fitzgerald C, Ellis EA, Aboufridklra M, and Guy f. Insulin-like growth factor-/ act a an angiogenelic agent in rabbit cornea and retina -comparative studies with basic fibroblast growtlr factor . Diabetologia. 1993; 36:282-291 .
13. Camussi G, Montrucclrio G, Lupia E, Soldi R, Comoglio PM, and Bussolino F. Angiogenesis induced in vivo by hepatocyte growth factor is mediated by platelet-activating factor syntlresis from macroplrages. I lmmrm . 1997; 158:1302-1309.
14. Silvagno F, Follenzi A, Arese M et a/. In vivo activation of mel tyrosine kinase by lreterodimeric hepatocyte growth factor molecule promote angiogenesis. Arleroscler Tirromb Vase Bioi. 1995; 15:1857-1865.
14. Montrucchio G, Lupia E, Battaglia E eta/. Tumor-necrosis factor a-induced angiogenesis depends on in situ platelet activating factor biosynthesis. I Exp. Med. 1994; 180:377.
16. Uvelius B, Persson L, and malliasson A. Smooth muscle cell hypertrophy and lryperpla ia in tire rat detrusor after hort-time infrnvesica/ outflow ob truclion. f. of Urology. 1984; 131 . 1:173-176.
17. Bret:el R, Hering B, and Federlin K. /solei cell transplanlationin diabetes
Feature Art i cles
mellitus -from benclr to bed ide. Experimental& Clinical Endocrinology & Diabetes. 1995; 103(Suppl 2):143-159.
18. Dusseau JW, Hitclrin PM, and Malbasa DS. Stimulation of angiogenesis by adenosine on the chick chorioallantoic membrane. Circ Res. 1986; 59:163-170.
19. Meininger CJ, Sclrelling ME, and Granger HJ. Adenosine and hypoxia timulation proliferation and migraticm of endothelial cells. Am. f. Physiol.
1988; 255:H554-H562. 20. Vinores SA, Seu J, and Campoclriaro PA . An adenosine agonist and
prostaglandin E1 cause breakdown of tire blood-retinal barrier by opening tight junctions between va cular endothelial cells. Ophtlralmol. Vis. Sci. 1992; 33:1870.
21. Folkman J and D'Amore PA. Blood vessel formation: what is it molecular basis? Cell. 1996; 87:1153-1155.
22. Granger HJ, Ziclre M, Hawker JR, Jr., Meininger CJ, Czisny LE, and Zawieja DC. Molecular and cellular basis of myocardial angiogenesis. Cell. Mol. Bioi. Res. 1994; 2:81-85.
23. Slrweiki D, /tin A, offer D, and Ke !ret E. Va cular endothelial growth factor induced by hypoxia may mediate hypoxia-initiated angiogene is.
alure. 1992; 359:843-845. 24. Banai S, Shweiki D, Pinson A, CHandra M , Lazarovici G, and Keshet E.
Upregulation of va cular endothelial growth factor expres ion induced by myocardial ischaemia: implications for coronary angiogenesis. Cardiovasc Res. 1994; 28:1176-1179.
25. Stavri GT, Zachary IC, Baskerville PA, Martin JF, and Erusalim Icy JD. Basic fibroblast growth factor upregulates the expre sion of vascular endothelial growth factor in vescular smooth muscle cells. Synergistic interaction with hypoxia. Circulation. 1995; 92(1):11-14.
26. Babaei S, Teichert-Kuliszew ka K, Monge JC, Bendeck MP, Stewart DJ. Obligatory role for 0 in endothelial cell differentiation in an in vitro model of angiogenesis. Tire Canadian journal of Cardiology 1997;13(Suppl C):83C[Abstract]
27. Morbidel/i L, Chang C, Douglas JG, Granger HJ, Ledda F, and Ziclre M. itric oxide mediates mitogenic effect of VEGF on coronary venular
endothelium. Am. f. Plry iol. 1995; 270:H411-H415. 28. Pepper MS, Ferrara , Orci L, and Montesano R. Va cular endothelial
growth factor (VEGF) induces plasminogen activator and plasminogen inlribitor-1 in microva cular endothelial cells. Bioclrem Biophys Res Commun. 1991; 181:902-906.
29. Saksela 0, Moscatelli D, and Rifkin D. Tire opposing effects of basic fibroblast growth factor and transforming growth factor beta on the regulation of plasminogen activator activity in capillary endothelial cells. f. Cell. Bioi. 1987; 105:957-963.
30. Kluge A, Zimmermann R, Moonkel B el a/. Insulin-like growth factor I is involved in inflammation linked angiogenic processes after microembolisation in procine heart. Cardiovasc Res. 1995; 29:407-415.
31. Anlonelli-Orldge A, Saunder KB, Smith SR, and D 'A more PA. An activated form of Iran ifomring growth factor beta is produced by coculture of endothelial cells and pericytes. Proc all Acad Sci USA. 1989; 86:4544-4548.
32. Lynch S, Colvin R, and Anloniades H. Growth factors in wowrd healing. f. C/in. Invest . 1989; 84:640-646.
33. abia PJ, Powers ER, Ragosta M, Sarembock If, Burwell LR, and Kaul S. As association between collateral blood flow and myocardial viability in patients with recent myocardial infarction. . Engl. f. Med. 1992; 327:1825-1831.
34. Schaper W, DeBrabander M, and Lewi P. D A-synthesis and mitoses in coronary collateral vessels of tire dog. Circ Re . 1971; 28:671-679.
35. Baffour R, Berman J, Garb JL, Ree SW, Kaufman J, and Fridmann P. Enhanced angiogenesis and growth of collateral by in vivo adminstralion of recombinmrl basic fibroblast growth factor in a rabbit model of acute lower limb ischemia: dose resporrse effect of basic fibroblast growth factor. Journal of Vascular Surgery. 1992; 16:181-191.
36. Takeshita S, Zheng LP, Brogi E, and et.al. Tirerapeutic angiogenesis: a ingle intra-arterial bolus of vascular endothelial growth factor augments reva cularization in a rabbit ischemic hindlimb model. f. Clirr. Invest . 1994; 93:662-670.
37. Unger EF, Banai S, Slrou M el a/. Basic fibroblast growth factor en/ranees myocardial colla teral flow in a canine model. Am. f . Plrysiol . 1994; 266:H1588-H1595.
38. Banai S, Jaklitsclr MT, Slrou M el a/. Angiogenic-induced enhancement of
U. W.O. Medical Journal 70 (1) 2000------------------------- 59
Feat u re Art i cles
collateral blood flcnu to ischemic myocardium by vascular endothelial growth factor in dog . Circulation. 1994; 89:2183-2189.
39. Harada K, Grossman WF, M., Edelman ER et a/. Basic fibroblast growth factor improves myocardial function in clzronically ischemic porcine hearts. f. Clin . Invest. 1994; 94:.623-630.
40. Sho11 M, Hodge E, Rajanayagam MAS et a/. Effects of chronic systemic adminstration of basic fibroblast growth factor on collateral development in the canine heart. Circulation. 1995; 91 :145-153.
41 . Lazarous DF, Shou M, Sclzeinowitz M et a/. Comparative effects of basic fibroblast growth factor and vascular endothelial growth factor on coronary collateral development and the arterial response to injury. Circulation. 1996; 94:1074-1082.
42. Takeshita S, Zheng LP, Asahara T, Riessen R, Brogi E, Ferrara N, Symes JF, Isner JM. In vivo evidence of enhanced angiogenesis following direct arterial gene transfer of the plasmid encoding vascular endothelial growth factor . Circulation 1993;88(suppll):I-476[Abstract]
43. Riessen R, Rahimizadeh H, Blessing E, Takeshita S, Barry n, and Isner JM. Arterial gene transfer using pure DNA applied directly to a hydrogel-coated angioplasty balloon. Human Gene Therapy. 1993; 4:749-758.
44. Mack CA, Patel SR, Schwarz EA et a/. Biologic bypass with the use of adenovirus-mediated gene transfer of the complementary deoxyribom1cleic acid for vascular endothelial growth factor 121 improves myocardial perfusion and function in the ischemicporcine heart. Journal of Thoracic & Cardiovascular Surgery. 1998; 115:168-176.
45. Isner JM, Pieczek A, Schainfeld R et a/. Clinical evidence of angiogenesis after arterial gene transfer of phVEGF165 in patient with ischaemic limb. The Lancet. 1996; 348:370-374.
46. Baumgartner I, Pieczek A, Manor 0 et a/. Constitutive expression of phVEGF165 following intramuscular gene transfer promotes collateral vessel development in patients with critical limb ischemia. Circulation. 1998; 97:1114-1123.
47. Schumadter B, Pecher P, von Specht BU, and Stegmann T. Induction of neoangiogenesis in ischemic myocardium by human grcnuth factors . First clinical results of a new treatment of coronary heart disease. Circulation. 1998; 97:645-650.
48. Losordo DW, Vale PR, Symes ]F et a/. Gene therapy for myocardial angiogenesis. Initial clinical results with direct myocardial injection of phVEGF165 as sole therapy for myocardial ischemia. Circulation . 1998; 98:2800-2804.
49. Vale PR, Losordo DW, Symes ]F, Isner ]M. Gene therapy for myocardial angiogenesis. Circulation 1998;98(suppll):I-322[Abstract]
50. Marclz KL, Woody M, Mehdi K, Zipes DP, Brantly M, and Trapnell BC. Efficient in vivo catheter-based pericardia/ gene transfer mediated by adenoviral vectors. Clin. Cardiol. 1999; 22(Suppl. I):I23-I29.
51 . Macris MP and Igo SR . Minimally invasive access of the normal pericardium: initial clinical experience with a novel device. Clin . Cardiol. 1999; 22(Suppl. I):I36-I39.
52. Li R-K, Jia Z-Q, Weisel RD et al. Cardiomyocyte transplarttation improves heart function . Annals of Thoracic Surgery. 1996; 62:654-661 . Q
Southwestern Ontario's Leading Centre for Patient Care, Teaching and Innovation
60
LONDON Hea lth Sciences Centre
Congratulates the UWO Faculty of Medicine Graduates.
------------------------- U. W .O. Medical Journal 70 (1) 2000

Miscellaneous Articles
A LITERATURE REVIEW BILE DUCT
OF CANCER EXTRAHEPATIC
Introduction
Extrahepatic bile duct (EHBD) carcinoma is an uncommon malignancy with overall five year survival rates less than 5%1
• Le ions are frequently mall, making diagnosis difficult, and they are often
locally invasive at the time of presentation making re ection irnpo sible2
• Tumour usually spread within the bile ducts and, locally, they may invade the hepatic artery, portal vein and liver parenchyma3
. Surgical resection offers the only chance for long-term survival1
•11
• Surgical cure and prognosis are based primarily on the stage of the tumour at the time of diagno is. Anatomical location of the lesion, morphological type, and grade of the tumour al o affect prognosis4
• Overall, the five year survival with urgical re ection is less than 30%.
These tumours arise from epithelial cells lining the major extrahepatic bile ducts. The majority of tumours appear histologically and microscopically similar5
.
Generall y, tumours are mucin-producing adenocarcinoma . Three anatomic divisions are recognized for tumour cia ification: (1) Upper third, involving the hilar region and confluence of right and left hepatic ducts -this type of EHBD tumour is also known as a Klat kin tumour; (2) distal to the junction of cystic duct and the uperior border of the pancrea (middle third); and (3) the
lower third at the distal end of common bile duc:f-11•
Location of the tumour i responsible for differing survival rate 4 11
• Lesions of the distal third are most often curable with re ection, whereas Klat kin tumours (upper third lesion) are often invasive and uruesectable at the time of g_resentation, and have low survival rates with re ection 11
• Unfortunately, the confluence of the hepatic ducts c_onstitut~ the location of argroximately one-half of all malignant bile duct cancer 6-
10•1
• •
Morphologic subtypes include papillary I polypoid, a nd clerosing tumours . These lesions can be well, moderately, or poorly differetiated2
• Papillary lesions have a significant long-term survival advantage compared to clerosing lesions 11
• In EHBD cancers, local invasion, lymph node metastases and the status of the surgical margins are primary factors affecting prognosis28
•
The etiology of EHBD cancers is not well defined29.30.
A link between gallstones, gallbladder di ease and bile duct cancers has been observed29
• In addition, biliary
ABOUf THE AurHORS Ajay Sahajpal is a third-year medical student at the
University of Western Ontario. He did his undergraduate degree in biology at the University of Prince Edward Island. Dr. Ward Davies is a hepatobiliary and general surgeon at uwo.
By A.K Sahajpal and W. Davies MD
enteric anastomosi , inflammatory bowel disease, choledocal cysts, and smoking have also been shown to increa e the risk of bile duct cancers in both men and women. Other factors uch as unsaturated fat intake, bod weight, and alcohol show only a weak correlation . Associations between cancer of the bile duct and ulcerative colitis (UC) have been observed35
• A tudy by A~"':' ari et a/35 reviewed thirteen patients at the Mayo Clinic between 1935-1973 with documented association of UC and bile duct cancer. Onset of bile duct cancer was insidious in each ca e. Common presentation for these patient wa fatigue, anorexia, and weight loss followed by dark urine, pruritus, jaundice and acholic stools35
. The incidence of bile duct cancer in patients with UC been reported as between 0.4% -1.4%35
. At onset of cancer, mo t patients had mild to moderate periodic exacerbations of UC with one having no symptoms35
•
Presentation and Diagnosis Patient typically pre ent with painless jaundice and
weight loss. Clinically the e patients present with cleral icteru , jaundice, dark, tea-coloured urine, and claycoloured stools. As ductal obstruction worsens patients develop pruritu , hepatomegaly and are at risk for developing a cending cholangitis. If the tumor is confined to right or left branche and occluding the lumen, jaundice may not be present, delaying symptoms and pre entation longer5
•31
• Early diagnosis is crucial to survival13• Initial
inve tigations after a complete history and physical examination include appropriate blood work which should include liver function tests.
Once a pattern of obstructive jaundice ha been identified, abdominal ultrasound is the most effective initial radiologic investigation. Ultrasound will demonstrate a dilated intrahepatic biliary tree and, depending on where the primary tumour is located, dilation of the extrahepatic bile ducts to the level of the ~umour. At this stage, the differential diagnosis may mclude: choledocholithiasis, benign bile duct stricture , sclerosing cholangitis, and pancreatic neoplasms. Imaging of the EHBD can be achieved by perfoming either endo copic retrograde cholangiopancreatography (ERCP) or by percutaneous tran hepatic cholangiography (PTC). At the time of ERCP or PTC, the obstructed bile duct can be tented or drained to allow for decompression of the obstructed biliary sy tern. A sub equent CT scan should be done to help stage the tumour (rule out distant metastases, and evaluate the extent of local invasion). In some centres, hepatic arterial angiography is used to assess local vascular invasion which may preclude surgical intervention. If the EHBD cancer is not re ectable, palliation can be obtained with a PTC drain or an ERCP placed drainage stent?2
·34
U. W.O. Medical Journal 70 (1) 2000------------------------ 61
M i scellan e ous A rticl e s
Management The mean survival for patient for untreated EHBD
cancer i 3-6 months ·36• Chemotherapy alone has had
little role in the treatment of EHBD tumours for curative or palliative management!. These tumours unfortunately do not respond to any great degree to currently available chemotherapeutic agents. Radiotherapy can increase length of survival, quality of life, and shows benefit in patients with previous curative or palliative surgery 1. It may al o benefit patients with local recurrences 1. The use of high dose radiotherapy is a feasible therapeutic option for the management of EHBD cancer. Radiation therapy can be delivered by external beam or intraca itary radiotherapy via a PTC drain37.51
_
Indications for use of radiation treatment include: (1) adjuvant therapy following complete resection; (2) palliative radiotherapy for patient with positive margins or local recurrence following surgery; and (3) palliative treatment of nonresectable advanced tumours 1
•
eoadjuvant chemoradiation for EHBD cancer can be used preoperatively36
•38
• Proponents of this approach believe some tumours may be decreased in ize to allow for re ection and theorize that the neoadjuvant approach may improve survival. Few data exist to support this approach at present.
The ide effect of radiation treatment for EHBD cancers are variable and most complaints are related to irradiation of inte tinal epithelium1
• Diarrhea, nau ea and vomiting are commonl.
The principles of su rgical management of HBD cancers in~olve~ comp~ete en bloc re ectio~ of the prim~ tumour With histologtcally proven negative margins · . Management based on anatomical location is as follows: (1) upper 1/3 (Klatskin tumour), resection of bifurcation of bile duct +I- as ociated hepatic resection; (2) middle 1 I 3, may be amenable to local resection or pancreaticoduodenectomy (Whipple procedure); (3) distal 1/3 of biled duct, pancreaticoduodenectomy. The aim of surgical palliation is to relieve biliary obstruction, thereby decompre ing the biliary tree39
• This i accompli hed by performing a biliary enteric bypass.
Surgically placed U-tubes have been used in the pa t to palliate patients, but are used much le s frequently than PTC drain or ERCP-placed stents3
•39
. Percutaneou techniques have associated problems. Mortali~ may reach up to 25-31% and infection is also a concern 1
• External catheters lead to the loss of fluid and electrolyte a well a bile constituents3
• They also provide a portal of entry for bacteria leading to cholangitis, epticaemia, and liver ab ces e 3
. Catheters require daily care, dressing and irrigation. If obstructed they can be changed with ea e and may be u ed as a portal for intracavitary radiotherap . Mortality rates for percutaneous and endoscopic palliative procedure have been estimated at 15-33% for 30 day po t procedure6
•22
•23
• 42
• This is imilar to the perioperative mortality rate for surgical palliative bypa s.
Palliative surgical decompre ion of biliary ob truction in patients with unre ectable EHBD cancer involve Roux-en-Y biliary-enteric ana tomose . The location of the bypa depend upon the origin of the primary tumour. The bypass can be performed both intra-
and extra-hepatically. The intra-hepatic approach commonly employed i the "round ligament" approach (segment ill approach) to the ducts of the left lobe lateral to the ligamentum teres39
•
Guidelines for the choice of a decompression procedure include: (1) general condition or health of the patient; (2) effectiveness of the procedure with re pect to quality I duration of survival; (3) associated complications17
. Regardle s of the procedure employed, the goal of palliation i the relief of ;ymptom of ob truction -jaundice, pruritu , malai e, etc1
.
Surgical re ection can be accompli hed with acceptable operative mortality and morbidity with respect to length and quality of life6
•12
-17
• The key to ucce ful surgical management of EHBD cancers is early and accurate preoperative diagno i 13
• Invasion of the hepatic artery, portal vein and di tal metasta e are the u ual reasons makin§ the e tumous nonresectable at diagno i 3
'13
'1731.38.3 • Contraindications to re ection include:
(1) regional/ distant meta ta e ; (2) bilateral intrahepatic spread beyond econd order ducts; (3) inva ion of the main trunk of the hepatic artery; (4) inva ion of the main trunk of the portal vein9
•13
•17
•43
•44
•45.
A tumour is considered re ectable if it is localized to the bile duct. Procedure for radical urgery are individualized and preoperative mapping with PTC and ERCP are crucial to plannirlg. If resection is performed a margin of 1.5 em from the edge of the tumour e pecially on the hepatic side i recommended46
.
Postoperative complication include ana tomotic leaks, wound infection, bleeding, intra-abdominal ab ce s formation, sep is, pancreatitis, and portal vein thrombo is13
• As a result of improved surgical technique and po toperative management of patients, the po toperative mortality rate has decrea ed . The perioperative mortality rate depends upon the extent of the surgical resection, but range from 2-5%47
.
Liver transplantation as a form of management i not an effective treatment for the management of EHBD cancer. It has been e timated that up to 0% of transplant patient died or manife t di ea e recurrence within one ye~·2+27 • In the literature, there have been a few report of curative surgery with liver transplantation for hilar carcioma with adequate long-term urvival, if margins are clear and lymph node are negative .4
9. At pre ent, thi
i still not an accepted therapeutic option and is considered experimental.
Conclusion Extrahepatic bile duct cancer are rare neopla m with
overall five year urvival rate less than 5%. En bloc surgical re ection with negative hi tologic margins offer the only chance for cure. Even with surgical re ection, 70-7~% of patient~ develop tumour recurrence and ultimately die from the di ease. onre ectable patients can be treated palliatively with PTC drainage of the obstructed bile duct or via ERCP placed tent . Adjuvant radiotherapy via external beam or intracavitary radiotherapy may improve urvival. Palliative radiotherapy may slow progre ion of
the tumour and minimize a ociated ymptom . Although extra-hepatic bile duct carcinoma are rare, they should be
62 ------------------------ U. W.O. Medical Journal 70 (1) 2000
con idered in the differential diagno is of patient who pre ent with ob tructive jaunctice.
REFERE CES
1. Kopelson , G., L. Harisiadis, P. Tretter, and C.H. Chong. The Role of Radiation Therapy in Cancer of the Extra Hepatic Biliary System: an analysis of thirteen patients and a review of the Iiterah~re of the effectivenes of urgery, chemotherapy, and radiotherapy. Int . f Radiation Oncology. Bioi. Phys. 1977; 2:883-894.
2. Tompkins, R.K. , D. Thomas, A. Wile, and W.P. Longmine. Prognostic fa ctors in bile duct carcinoma. American Surgical Association 1981 ; 194(4):448-455.
3. Ottow, R.T., D.A. August, and P.H. Sugarbaker. Treatment of Proximal Biliary Tract Carcinoma: An overview of techniques and results. Surgery 1985; 97(3): 251-262.
4). idwls, D.A., R.L. MacCarty, T.A. Coffey. Cholangiographic Evaluation of Bile Duct Carcinoma. AJR 1983; 141:1291-1294.
5. Zimmerman, A. Tumours of the bile duct - pathological a peel . Biliary Tumours. 925- 940.
6. Hadjis, .S., f./. Blenkharn, . Alexander, l.S. Benjamin, L.H. Blumgart. Outcome of radical surgery in hilar cholangiocarcinoma. Surgery 1990; 107(6):597-603.
7. Alexander, F., R.L. Rossi, M. O=Bryan. U. Klrettrey, and f. W. Watkins . Biliary carcinoma: a review of109 cases. Ann. f. Surg. 1984; 147:503-09.
8. Blumgart, L.H., I.S., Benjamin, .S. Hadjis, and R. Beazley. Surgical approaches to cholangiocarcinoma at confluence of hepatic duct . Lancet 1984; 66-69.
9. Voyles, C.R., .f ., Bowley, D.j. Allison, 1 . . Benjamin, L.H. Blumgart. Carcinoma of the Proximal Extrahepatic Biliary Tree: Radiologic asses ment and therapeutic alternatives. Ann. Surg. 1983; 197:188-94.
10. Terblanclre, J.K.D., P.C. Bornman, D. Warner. The role of U tube palliative treatment in high bile duct carcinoma. Surgery 1988; 103:624-32.
11 . Chung, C., . Bautista, T.X. O=Comrell. Prognosis and treatment of bile duct carcinoma. Am. Surg. 1998; 64(10):921-25.
12. Lanois, B. J.P. Campion, P. Bri sot, M . Gosselin. Carcinoma of tire Hepatic Hilus: urgical management and the case for resection. Ann. Surg. 1979; 191:23-29.
13. Evander, A., P. Fredlund., f. Hoevels, 1. lnse, S. Bengmark. Evaluation of aggressive surgery for carcinoma of the extrahepatic bile ducts. Ann. Surg. 1979; 191(1 ):23-29.
14. lwaski, Y ., T. Okamura, A. Ozaki. Surgical treatment for carcinoma at the confluence of the major hepatic ducts. Surg. Gyencol. Obstet. 1986; 162:457-64 .15)Mi zumoto, R.K. Y ., and H . Suz uki. Surgical treatment of lrilar carcinoma of tire bile duct. Surg. Gynecol. Obstet. 1986; 162:153-58.
16. Pinson, C. W. and R.L. Rossi. Extended right Jrepatic lobectomy, left hepatic lobectomy, and keletonization resection for proximal bile duct cancer. World f . Surg. 1988; 12:52-59.
17. Bismuth, H., D. Castaing, and 0 . Tragnor. Resection or Palliation: priority of surgery in tire treatment of lrilar cancer. World f. Surg. 1988; 12(1):39-47.
18. Fortner, f.G . C. E. Vitelli, and B.j. MacLean . Proximal extrahepatic bile duct tumours. Arch. Surg. 1989; 124:1275-79.
19. Bruggen, f. T. M.S. McPhee, P.S., Bhatia, and J.M . Richter. Primary Adenocarcinoma of the bile ducts: clinical characteristic and natural his tory. Dig. Dis. Sci. 1986; 31 :840-46.
20. Malangoni, M.A., D.M . McCoy, J.D. Ridrardson, and L.M. Flint. Effective palliation of malignant biliary duct obslntction. Ann. Surg. 1985; 201:554-9.
21 . arr. M.G., and ].L. Cameron. Surgical palliation of rmresectable carcinoma of tire pancreas. World f. Surg. 1984; 8:906-18.
22. Dooley, j.S., R. Dick, P. George, R.M. Kirk, K.E.F. Hubbs, S. Sherlock. Percutaneous Transhepatic Endoprosthesi for Bile Duct Obstruction: complication and results. Gastroenterology. 1984; 86: 905-09.
23 . Deviere, f. , M. Baize, f. deToeuf, and M . Cremer. Longterm follow-up of patients with hilar malignant strichtre treated by endoscopic internal biliary drainage. Gastrointest. Endosc. 1988; 34:95-101 .
24. lwatsuki, S., S .D., Gordon, B. W. Slraw, and T.E . Starzl. Role of liver transplantation in cancer therapy. Ann. Surg. 1985; 202:401-7.
25. O=Grady, f. G., R.f . Polson, K.Rolles, R . Y . Caine, R. Williams . Liver transplantation for malignant disease. Ann. Surg. 1988; 207:373-9.
26. Rossi, R.L., F. W. Hei , C. F. Beckmmm, and]. W. Braasch. Management of cancer of the bile duct . Srtrg. Clin. orth Am. 1985; 65:59-78.
Miscellaneous Articles
27. Caine, R. Y., R. Williams, and K. RoUes. Liver transplantation in the adult. World f. Surg. 1986; 10:422-31 .
28. Kurosaki, 1., K. Tsukada, H. Watanabe, K. Hatakeyama. Prognostic determinant in extrahepatic bile duct cancer. Hepatoga troenterology 1998; 45(22):905-09.
29. Rabeneck, L.Gallstones and bile duct cancer. Gastroenterology 1994; 107(4):1205-06.30)Chow, W.H., J.K. McLaughlin, H.R. Menck, T.M . Mack. Risk factors for extralrepatic bile duct cancers. 1994; 5(3):267-272.
31 . Klatskin, G. Adenocarcinoma of the Hepatic Duct at Its Bifurcation wit/tin the Porta Hepati : an 111111 ual tumour with distinctive clinical and pathological features . American formral of Medicine 1965; 38:241-256.
32. Kuroiwa, M. , H. Goto, Y. Hiruouka, T. Furukawa, T. Hoyakawa, Y. aitolt. Intraductal ultrasonography for the diagnosis of proximal invasion in extrahepatic bile duct cancer. ]. Gastroentorl Hepatol. 1998; 13(7):715-19.
33. Tamada, K., K. Ido, . Veno, M . Iclriyama, T. Tomiyama, T. ishizmo, S. Wada, T . oda, S. Tanu , T . Aizawa et a/. Assessment of pancreatic parenchymal in v a ion by bile duct cancer using intraductal ultrasonography. Endoscopy 1996; 28(6):492-6.
34. Tamada, K. K. ldo, . Veno, M . lclriyanra, T. Tomiyama, T. ishizmo, S. Wada, T. oda, S. Tanu, T . Aizawa et a/. As essnrent of hepatic artery invasion by bile duct cancer using intraductal ultrasonography. Endoscopy 1995; 27(8):579-83.
35. Akwari, O.E., f.A. VanHeerden, W. T. Foulk, A. H. Baggenstos . Cancer of the Bile Ducts . Associated with Ulcerative Colitis. Ann. Surg . 1975; 181(3):303-309.
36. McMaster , K. M ., T .M .. Tuttle, S.D. Leach, T. Rich, K.R. Cleary, D.B. Evans, S .A . Curley . eoadjrtVant chemoradiation for extrahepatic clrolangiocarcinonra. Am J Surg. 1997; 174(6):605-08.
37. Kamada, T., H. Saitou , A. Takamura, T. ojima, S.l. Okushiba. The role of radiotherapy in management of extralrepatic bile duct cancer: an analysis of 145 consecutive patients treated with intraluminal and/or external beam radiotlrerapy. Int. f. Radial. Onco/. Bioi. Phys. 1996; 34(4):767-74.
38. Tsuzuki, T . Y . Ogata, S. !ida, L. akanishi, Y . Takenaka, H. Yoshii . Carcinoma of the Bifurcation of tire Hepatic Ducts. Arch. Surg. 1983; 118:1147-1151 .
39. Blumgart, L.H., and C.f . Kelly. Hepaticojejunostomy in benign and malignant high bile duct stricture: approaches to the left lrepatic ducts. Br.]. Surg. 1984; 71(4):257-261 .
40. Dooley, S., D.R. Irving, D. Olney, and f . Sherlock. Relief of bile duct ob truction by the percutaneorts transhepatic insertion of an endoprosthesis. Clin . Radio/. 1981; 32:163.41)Harbin, W.P., P.R. Mueller, J.T. Ferrucci Jr. Transhepatic Cholangiograplry: complications and use patterns of the fine needle technique. Radiology 1980; 135:15.
42. Liu , C.L. , C.M . Lo, E.C. Lai, S.T. Fan . Endoscopic retrograde cholangiopancreatography and endoscopic endoprosthesis insertion in patient with klatskin htmours. Arclr. Surg. 1998; 133(3):293-6.43)Akwari, O.E. and K.A. Kelly . Surgical Treatment of Adenocarcinoma. Location: junction of the right, left, and common hepatic biliary ducts. Amr. Surg. 1979; 191:23.
44. Todoroki, T., T. Okamura, K. Fukao.Gros appearance of carcinoma of the mainlrepatic duct and its prognosis. Surg. Gynecol. Obstet. 1980; 150:33.
45. Yoshii, H. Carcinoma of the bifurcation of the hepatic duct . Arch. Surg. 1983; 1118:1147.
46. Yamaguchi , K., K. Chijiwa, S. Saiki, S. Shimizu, M . Takas/rima, M . Tanaka.Carcinonra of the extrahepatic bile duct : mode of spread and its prognostic implications. Hepatogastroenterology 1997; 44(17):1256-61 .
47. Zerbi, A. G. Balzano, B. E. Leone, E. Angel, P. Veronesi, V. Di Carlo. Clinical presentation, diagnosis, and survival of resected distal bile duct cancers. Dig. Srtrgery 1998; 15(5):410-16.
48. Iwatsuki, S., S. Todo, f. W. Marsh, J.R. Madariaga, R.G. Lee, I. Dvarcltik, J.f. Fung, T.F . Starzl. Treatment of hilar clrolangiocarcinoma ( Klatskin tumours) witlr hepatic resection or transplantation. f. Am. Col/. Surg. 1998; 187(4):358-64.
49. Casovilla, F.A. , f. W. Marsh, S. Iwat uki, S. Todo, R.G. Lee, j.R. Madariaga, A . Pinna, 1. Dvorclrik, f.J . Fung, T .E. Starzl. Hepatic resection and transplantation fro peripheral clwlangiocarcinoma. ]. Am. Coli. Surg. 1997; 185(5):429-36.
50. Partensky, C. Treatment oflrilar cancer . f. Chir. 1998; 135(4):162-67. 51 . Alden, M.E. , F.M. Waterman, A.K. Top/ram, D.]. Barbot, M .]. Sharpiro,
M .Mohiuddin . Cholangiocarcinoma: clinical significance of tumour location along the extrahepatic bile duct. Radiology 1995; 197(2):511-16. n
U. W.O. Medical Journal 70 (1) 2000------------------------ 63
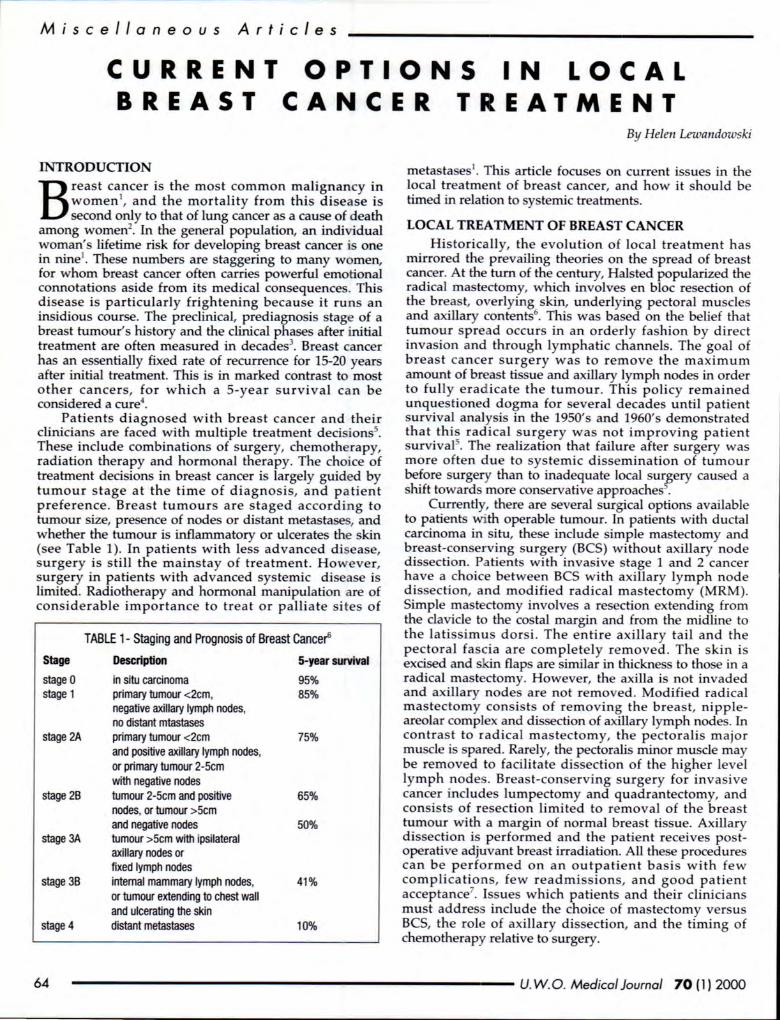
Miscellaneous Articles
CURRENT OPTIONS IN LOCAL TREATMENT BREAST CANCER
INTRODUCTION
Breast cancer is the most common malignancy in women1
, and the mortality from this disease is second only to that of lung cancer as a cause of death
among women2• In the general population, an individual
woman's lifetime risk for developing breast cancer is one in nine1
• These numbers are staggering to many women, for whom breast cancer often carries powerful emotional connotations aside from its medical consequences. This disease is particularly frightening because it runs an insidious course. The preclinical, prediagnosis stage of a breast tumour's history and the clinical phases after initial treatment are often measured in decades3
. Breast cancer has an essentially fixed rate of recurrence for 15-20 years after initial treatment. This is in marked contrast to most other cancers, for which a 5-year survival can be considered a cure4
•
Patients diagnosed with breast cancer and their clinicians are faced with multiple treatment decisions5.
These include combinations of surgery, chemotherapy, radiation therapy and hormonal therapy. The choice of treatment decisions in breast cancer is largely guided by tumour stage at the time of diagnosis, and patient preference. Breast tumours are staged according to tumour size, presence of nodes or distant metastases, and whether the tumour is inflammatory or ulcerates the skin (see Table 1). In patients with less advanced disease, surgery is still the mainstay of treatment. However, surgery in patients with advanced systemic disease is limited. Radiotherapy and hormonal manipulation are of considerable importance to treat or palliate si tes of
Stage
stage 0 stage 1
stage 2A
stage 28
stage 3A
stage 38
stage4
TABLE 1- Staging and Prognosis of Breast Cance~
Description
in situ carcinoma primary tumour <2cm, negative axillary lymph nodes, no distant mtastases primary tumour <2cm and positive axillary lymph nodes, or primary tumour 2-5cm with negative nodes tumour 2-5cm and positive nodes, or tumour >5cm and negative nodes tumour >5cm with ipsilateral axillary nodes or fixed lymph nodes internal mammary lymph nodes, or tumour extending to chest wall and ulcerating the skin distant metastases
5-year survival
95% 85%
75%
65%
50%
41%
10%
By Helen Lewandowski
metastases 1• This article focuses on current issues in the
local treatment of breast cancer, and how it should be timed in relation to systemic treatments.
LOCAL TREATMENT OF BREAST CANCER Historically, the evolution of local treatment has
mirrored the prevailing theories on the spread of breast cancer. At the turn of the century, Halsted popularized the radical mastectomy, which involves en bloc resection of the breast, overlying skin, underlying pectoral muscles and axillary contents6
. This was based on the belief that tumour spread occurs in an orderly fashion by direct invasion and through lymphatic channels. The goal of breast cancer surgery was to remove the maximum amount of breast tissue and axillary lymph nodes in order to fully eradicate the tumour. This policy remained unquestioned dogma for several decades until patient survival analysis in the 1950's and 1960's demonstrated that this radical surgery was not improving patient survival5
. The realization that failure after surgery was more often due to systemic dissemination of tumour before surgery than to inadequate local sur?ery cau ed a shift towards more conservative approaches .
Currently, there are several surgical options available to patients with operable tumour. In patients with ductal carcinoma in situ, these include simple mastectomy and breast-conserving surgery (BCS) without axillary node dissection. Patients with invasive stage 1 and 2 cancer have a choice between BCS with axillary lymph node dissection, and modified radical mastectomy (MRM). Simple mast ctomy involves a resection extending from the clavicle to the costal margin and from the midline to the latissimus dorsi . The entire axillary tail and the pectoral fascia are completely removed . The skin is excised and skin flaps are similar in thickness to those in a radical mastectomy. However, the axilla is not invaded and axillary nodes are not remo ed. Modified radical mastectomy consists of removing the breast, nippleareolar complex and dissection of axillary lymph nodes. In contrast to radical mastectomy, the pectoralis major muscle is spared. Rarely, the pectoralis minor muscle may be removed to facilitate dissection of the higher level lymph nodes. Breast-conserving surgery for invasive cancer includes lumpectomy and quadrantectomy, and consists of resection limited to removal of the breast tumour with a margin of normal breast tissue. Axillary dissection is performed and the patient receives postoperative adjuvant breast irradiation. All these procedures can be performed on an outpatient basis with few complications, few readmissions, and good patient acceptance7
• Issues which patients and their clinicians must address include the choice of mastectomy versus BCS, the role of axillary dissection, and the timing of chemotherapy relative to surgery.
64 ------------------------- U. W.O. Medical Journal 70 (1) 2000
MASTECT O M Y VERSU S BREAST-CONSERVIN G SURGERY
Initial treatment for women with stage 1 or 2 breast cancer is surgery. The option available are modified radical mastectomy and breast-conserving surgery. Evidence from six prospective randomized controlled trials has shown that removal of the tumour followed bl radiotherapy results in similar survival as mastectomy . Without particular reasons for electing mastectomy, the choice between BCS and MRM is made according to patient preference. The goal of BCS is to provide atisfactory cosmetic results without compromising local
tumour control or survival compared to l'vfRM'l. However, there are conditions in which mastectomy is favored. It is indicated for diffuse-appearing microcalcifications on mammography, multiple tumours in different breast quadrants, failure to obtain tumour-free margins, and if radiotherapy is contraindicated. Contraindications to radiotherapy include physical disabilities preventing its u e, a history of therapeutic irradiation of the breast or chest, treatment during the first or econd trimester of pregnancy, scleroderma and SLE . BCS is also not recommended in the presence of a large tumour / breast ize ratio or a large breast size5
• In addition, there are risk factors for local recurrence following BCS. These include extensive ductal carcinoma in situ, young age, multiple tumours and high nuclear grade of tumour. Local recu~rence may lead to hi~h patient anxiety and may reqwre salvage mastectomy . In the e patient , the risks and benefits of mastectomy versus BCS should be carefully weighed on an individual basis.
In addition, the option of breast reconstruction after mastectomy should be di cus ed with the patient before any definitive surgery. Breast reconstruction techniques include silicone gel implantation beneath the pectoralis major muscle, and the use of m yocutaneous flaps to transfer skin, fat and muscle from distinct parts of the body. Currently, the most commonly used flaps are the latissimus dorsi and transverse rectus abdominis (TRAM) myocutaneous flaps3
. Regardless of the technique u ed, the goal of breast reconstruction is re-creation of the breast mound. The main indication for this procedure is the patient's desire to have it performed. The only true contraindications to breast reconstruction are significant comorbid conditions that would interfere with the patient's ability to tolerate a longer operative procedure in the ca e of immediate reconstruction, or additional procedures in the case of delayed reconstruction3
.
AXILLARY DISSECTION The appropriate treatment for the axilla remains
controversial. Although Halsted' s principles promoted extensive axillary dissection, more recent evidence has questioned the impact of axillary dissection on survival. A trial by the ational Surgical Adjuvant Breast Project howed that radical axillary dis ection did not positively
affect survival in patients with stage 1 and 2 breast cancer 10
. Axillary dissection is also as ociated with ignificant surgical morbidity . Possible complications
include post-operative infection, pare thesias, alterations in houlder mobility and lymphedema. However, the
M i sce llan eous A rti cle s
presence o r absence of metastatic involvement of the axillary lymph nodes is the strongest prognostic factor for patients with primary invasive breast cancer. In addition, extensive axillary dis ection is associated with greater reduction of recurrence risk in the axilla than sampling only a few nodes 11
• Thus, the decision on whether to remove axillary nodes and how extensively to do so requires balancing expected health benefits versus side effects.
Currently, there exist clinical guidelines for axillary dissection 11
• These are that removal and pathological examination of axillary lymph nodes should be standard procedure for patients with early invasive breast cancer. For accurate staging and to reduce the risk of recurrence in the axilla, level 1 and level 2 nodes should be removed. Level 1 nodes are tho e situated lateral to or below the lateral border of the pectoralis minor muscle. These nodes receive most of the lymphatic drainage from the breast. Level 2 nodes are situated deep to the pectoralis minor muscle and receive lymph from Ievell nodes and and also some drainage directly from the breast.
After axillary dissection, irradiation of the axilla should be carried out with caution. Omission of axillary dissection may be con idered when the risk of axillary metastases is very low or when knowledge of nodal status will have no influence on therapy. Recently, attention has been focused on the technique of sentinel lymphadenectomy to identify node positive patients5
•
The e involve the use of markers such as vital blue dye and techneti u m-labelled sulfur colloid to identify a sentinel node that drains lymph from the tumour area. If the entinel node has no evidence of metastatic breast cancer, complete axillary dissection can be avoided. If the node is positive for metasta es, axillary dissection should be performed. In a study of 62 patients, the sentinel node was identified successfully in 92% of cases and was positive in all patient found to have metastatic disease. There were no skip metastase 11
• As this technique is refined, a significant amount of axillary dissection and surgical morbidity may be avoided in the future.
TIMING OF SURGERY AND CHEMOTHERAPY Traditionally, chemotherapy has been used as an
adjuvant therapy following surgical resection in breast cancer . However, neoadjuvant or preoperative chemotherapy has been commonly used in treating variou cancers, including breast cancer12
• The rationale underlying this is that treating metastases at the earliest possible time may avoid rapid growth of metastases after treatment of the primary site and may prevent emergence of resistant clones. Decreasing the size of the primary tumour may make unre ectable tumours resectable, may make organ /?reservation more likely and may improve local control . This approach is mainly used in women diagnosed with stage 3 breast cancer. This includes patients diagnosed with stage 3A disease, which is generally considered operable, and stage 3B disease which is inoperable. Patients with inflammatory breast cancer are als~ included in stage 3B disease. This subgroup of patients has a particularly poor prognosis, and is characterized by tumours with a rapid onset of erythema,
U. W.O. Medical Journal 70 (1) 2000------------------------- 65

M i sce ll a n eo u s A rt cl e s
edema and ridging13•
Women with stage 3 breast cancer are a complex group in terms of treatment. Currently, multidi ciplinary therapy is the treatment of choice for the e patients. The accepted strategy is primary or neoadjuvant chemotherapy followed by either surgery, radiotherapy or both. Most patients achieve a respon e to chemotherapy that results in downstaging of the tumour. With the multidisciplinary approach, 5-year survival rates are 30-60%, compared to 10-20% for local therapy alone13
• In one study, patients with stage 3 breast cancer including inflammatory disea e were treated with chemotherapy followed by surgery and additional chemotherapy. Patients with inflammatory brea t cancer or supraclavicular nodes also received adjuvant radiotherapy. Overall 5-year survival was 56%, and wa affected by stage (3A or 3B), presence of inflammator:f breast cancer and the number of positive nodes 1
•
However, it i not clear that the apparent improvement in outcomes resulted from the use of neoadjuvant chemotherapy as much as the use of chemotherapy itself. In another report, the addition of chemotherapy after radiotherapy and surgery in patients with stage 3 breast cancer improved 3-year survival from 57% to 90%, and this difference remained highly significant at 5 years12
•
Therefore, neoadjuvant chemotherapy has not been shown to improve survival when compared to adjuvant chemotherapy for stage 3 breast cancer. However, the u e of neoadjuvant chemotherapy may decrease the tumour size and thereby reduce the scope and difficu l ty of surgery. In one study, patients with locally advanced brea t cancer deemed unre ectable with primary wound do ure underwent 8 weeks of infusional 5-fluorouracil and radiation therapy. 73% of patient had an objective clinical response and all were able to undergo MRM with primary wound closure 14
. Additionally, the use of neoadjuvant chemotherapy reduces the likelihood that skin grafts or complex reconstruction will be required, and may decrea e the inten ity and morbidity of irradiation needed to treat the brea tor che t wall 12
•
The use of neoadjuvant chemotherapy in stage 3 breast cancer gave rise to the idea of applying this approach to patients with earlier stage, operable brea t cancer. This was based on tudies showing "micrometa tases" in the blood and bone marrow of a significant number of patients undergoing surgery for early tage breast cancer15
• It was felt that if the e are treated earlier, there is the potential for higher cure rate . However, the use of neoadjuvant chemotherapy for patients with operable breast cancer i controver ial. It may achieve significant tumour regression but the primary goal of improving survival has not yet been clearly demonstrated 15
• At this stage, neoadjuvant chemotherapy for operable brea t cancer i still considered investigational.
CONCLUSION The current management of brea t cancer require a
multidi ciplinary approach involving surgical, medical and radiation oncologists. This field is constantly evolving. Local and systemic treatment mod a lities
constitute es ential aspect of treatment. Several urgical option are available to patients and their clinicians. The choice between mastectomy and BCS should be based on tumour factors and and patient preference following a thourough di cussion of the e options. Following surgical treatment, the need for adjuvant chemotherapy and I or radiation therapy must be determined based on tumour characteristics such as stage, grade, hormonal status and patient characteri tics uch as menopausal status and previous m dical hi tory. By weighing these factors carefully, breast cancer treatment may be optimized for patients on an individual basi .
ACKNO~EDGEMENTS
The author would like to thank Dr. J. Engel, surgical oncologist at London Health Sciences Centre (South Street Campus) for his constructive uggestions and contributions to thi article.
REFERE CES
1. Gordon A. Tile Increasing Efficacy of Breast Cancer Treatment. Clinical Oncology 1997; 9:338-42.
2. Bartow SA. TI1e Breast. In: Rubin E, Farber JL, ed . Patlwlogy. Plliladelpllia: j.B Lippincott, 1994:972-93.
3. Hellman S, Harris JR , Cane/los GP, Fisller B. Cancer of tile Breast. In:DeVita VT, Hellman S, Rosenberg SA, ed . Cancer: Principles and Practice of Oncology. Pili/adelphia: j.B Lippincott, 1993:1264-332.
4. Ferguson DJ, Meier P, Karrison MS,Dawson PJ, Straus FH, Lowenstein FE. Staging of Breast Cancer and Survival Rates. JAMA 1982; 248(11): 1337-41 .
5. ixon A], Troyan SL, Harris JR. Option in the Local Managament of Invasive Breast Cancer. Seminars in Oncology 1996; 23(4):453-63.
6. Andreoli TE, Carpenter CJC, Bennett JC, Plum F, eds. Cecil's Essentials of Medici11e. Plli/adelpllia: W.B Saunders Company, 1997:519-20.
7. Tan LR, Guen ther ]M. Outpatient Definitit>e Breast Cancer Surgery. Tile American Surgeon 1997; 63:865-7.
8. Tile Steering Committee on Clinical Practice Guidelines for tl1e Care and Treatment of Breast Cancer. Mastectomy or Lumpectomy? Tile Choice of Operation for Clinical Stages 1 and 2 Breast Cancer. CMAJ 1998; 158(3 Suppl):S15-19
9. oguchi M , Kinne DW, Miyazaki I. Breast-Conserving Treatment:Controversies and Consensus. Journal of Surgical Oncology 1996; 62:228-34.
10. Smith T. TI1e Role and Extent of Surgery in Early Invasive Breast Cancer. Seminars in Oncology 1996; 23(1) Suppl 3:12-18.
11 . Tile Steering Committee on Clinical Practice Guidelines for tl1e Care and Treatment of Breast Cancer. Axillary Di section. CMAJ 1998; 153(3 Suppl):S22-25.
12. Bear, HD. Indications for Neoadjuvant Chemotherapy for Breast Cancer. Seminars in Oncology 1998; 25(2) Supp/3:3-12.
13. Honkoop AH, Wagstaff], Pinedo HM . Managament of Stage 3 Breast Cancer. Oncology 1998; 55: 218-27.
14. Skinner KA, Dunnington G, Silberman H, Florentine B, Spicer D, Formenti SC. Preoperatrve 5-F/urouraci/ and Radiation Tllerapy for Locally advanced Breast Cancer. Tile American ]oumal of Surgery 1997; 174:705-7.
15. Brenin DR, Morrow M. Breast-Conserving Surgery in tile eoadjuvan t Setting. Seminars in Oncology 1998;25(3 Supp/):13-18. Q
66 ------------------------- U. W.O. Medical Journal 70 (1) 2000

Miscellaneous Article s
RECENT ADVANCES IN MELANOMA UNDERSTANDING
Reducing melanoma mortality i an important public health goal for dermatology, and as a result, has been intensively tudied from an epidemiological
point of view. 1 The recent literature on melanoma will be di cus ed.
Melanoma i a malignant di ease ansmg from melanocytes. Melanocytes produce melanin, which generate a brown skin color. Skin cancer is the most commonly diagnosed cancer in the United State and Canada (more than 63,000 Canadian will develop kin cancer each year); anyone born today has a 1 in 7 risk of developing skin cancer during his/her lifetime. 17
Although the incidence of melanoma is lower than other type of skin cancer, it i the mo t erious form of skin cancer and has the highest death rate. 3 In 1996 in the U.S.A, there were an e timated one million ca es of kin cancer; 5 percent of tho e were melanoma and caused 75% of kin-cancer death _3 In 1999, a 6% increa e in melanoma incidence is expected which will mean that 44,200 American will be diagno ed this year (3200 in Canada), with approximately 7,300 deaths attributed to melanoma.3
In Ontario, there are approximately 1400 people diagnosed with melanoma (men > women) each year with approximately 300 deaths per year. 16 A disturbing trend is that the incidence of melanoma in Canada ha doubled during the past 20 year .17 Clearly, more need to be done in terms of education and prevention. According to Dr. Ja on Rivers from the University of British Columbia, the increase in the age-specific incidence for melanoma has tabilized for women, especially for more recent birth
cohorts, but in men the rate i till increasing.26 Table 1 provides skin cancer statistics and trends in Canada.
Melanoma occur among all racial and ethnic group . It i more frequent in re ident of areas of high ambient solar irradiance, more frequent in un ensitive people and occur with highe t density on body site expo ed to the un. In addition, melanoma ha been hown to be more
frequent in people with intermittent high sun expo ure.2
The u eful acronym for identifying a possible melanoma is de cribed in Table 2. The incidence among dark skinned ethnic groups i 1 per 100,000 per year or les , but among light- kinned people has been measured as high as 50 per 100,000. 1 In common with most cancers, melanoma incidence increases with age. However, in Cauca ians, it i relatively more common in young adult than most other
ABOUT THE AUTHORS Ben Barankin is presently a third-year medical student
at UWO. Before medical school, he studied life sciences & psychology, completing a psychology degree at Queen's University. Dr. Lyn Guenther is professor and chair of the division of dermatology at the University of Western Ontario.
By Benjamin Barankin and Lyn Guenther MD
Canadian Skin Cancer Statistics & Trends
• Half of all new cancers are skin cancers • Approximately 63 ,000 new cases of skin cancer will be
diagnosed this year in Canada • Approximately 3,200 new cases of melanoma will be diagnosed
this year in Canada • In 1998, 7 40 deaths were attributed to malignant melanoma • The incidence of melanoma doubled among the white population
between 1973 and 1991 Table 1: Skin Cancer in Canadians
cancers. In fact, in the U.S.A, melanoma is more common than any noncutaneous malignancy in the 25 to 29 year age group, and it accounts for more years of life lost per case among adults than any major site other than testicular cancer. 3 As well, a gender difference in melanoma location exi ts; that is, women have an exces of melanoma on the legs, and men have an exces of melanoma on their ear , calp and especially the posterior trunk .U5 In 1996, a study in the Journal of Cutaneous Medicine and Surgery found that men and women had a similar anatomic distribution of painful sunburns, and since the anatomic distribution of melanoma differ , "it would appear that factors in addition to sunburns in adults account for the differences in the anatomic distributions of melanomas in men and women." 15
Unawareness of Melanoma A high proportion of U.S. residents are unaware of the
dangers of melanoma . Forty-two percent of those surveyed had no knowledge of the disease, with the level of awareness lowest among people ages 18 to 24 year .
The survey also found the level of melanoma awarene s to be directly related to levels of education and income. Of those with annual incomes of less than $20,000, 60 percent reported they did not recognize the term
The ABCD's of Melanoma
Asymmetry-<>ne half doesn't match the other half. Border irregularity-edges are ragged, notched or blurred (not well circumscribed). ~lor-color is not uniform. Shades of tan, brown and black are present; red, white or blue may also be present. Diameter-more than six millimeters.
Other Warning Signs of Melanoma: • change in the size, shape, or color of a mole • oozing or bleeding from a mole • a mole that feels itchy, hard, or tender to the touch
Table 2: Principles in detecting skin cancer ' Source: American Academy of Dermatology
U. W.O. Medical Journal 70 (1} 2000------------------------ 67

Misc e ll aneo us Articl e s
melanoma. Only 31 percent of tho e with annual incomes of $75,000 or more reported no knowledge of the disea e.3 It is likely that many Canadians would be similarly unaware of melanoma.
UV and Melanoma The two types of ultraviolet radiation that reach the
earth from the sun are ultraviolet A (UV A) and ultraviolet B (UVB). UVB has long been a sociated with sunburn, while UV A has been recognized as a deeper penetrating radiation. Scientists have long suggested that there may be an association between UVA radiation and malignant melanoma.3 The wavelen?th of tanning parlors is UV A. Both tanning parlors22
•23
•2 and PUV A (Psoralen & UV A
rays) 25 increa e the ri k of melanoma. It is only r cently that UVB rays have achieved similar tatu in causing melanoma. In the recent study in the May 1998 issue of the American Journal of Pathology, 158 human newborn foreskin grafts on immunodeficient mice were treated with a chemical accelerant 7,12-dimethyl[a]benzanthracene (DMBA) alone or UVB alone, or UVB combined with DMBA, or nothing. The grafts had had no prior sun exposure. Twenty-three percent of the grafts treated with only UVB, and 38% of grafts treated with the combination of DMBA and UVB, developed abnormal pigmented lesions including one human malignant melanoma within 5-10 months of exposure. Untreated human skin xenografts were unchanged, and those receiving only DMBA had very minor changes in a few grafts.
Sun Awareness
Efforts to educate people about sun protection have resulted in an increased awarene s that sun expo ure is dangerous. In a study released in 1997 by the American Academy of Dermatology, a decline in the attitude that having a tan was healthy and an increa e in the reported u e of unscreen by adult (35% in 19 6 to 53% in 1996) was noted.3 Unfortunately, during the arne decade, the UV exposure of adults, as measured by sunburning (30% in 1986 to 36% in 1996) also increased, a did the regular use of tanning beds (2% in 1986 to 6% in 1996).3 The risk factors for developing skin cancer are listed in Table 3.
Sunscreens Increase Cancer?
• blond or red hair
• blue eyes
• Caucasian
• changed/changing mole
• congenital mole
• fair complexion
• freckles
• immunosupression
• inability to tan
• melanoma in first-degree
relative
• one or more large or
irregularly pigmented lesions
• personal history of melanoma
• severe sunburns in childhood
Table 3: Risk factors for skin cancet Source: Centers for Disease Control
Recent controversy over the role of sunscreens in preventing melanoma has raised que tions about the u e of the e agents. There is concern among some dermatologist that unscreens alone do not protect against melanoma. Sunscreen might unfortunately lull you into a fal e ense of security, making you feel that you can stay out much longer than you should. Unfortunately, some individuals with the belief that sunscreen provides sufficient protection, may ignore other sun safety behaviors that could provide additional protection. Sub equently, these same individuals may ignore suspiciou marks or lesions as potentially dangerous becau e the feel that sunscreen alone provide all the protection they need.3 Historically, the sunscreens used in the pa t offered poor longer wavelength UV A protection which may have also played a role in melanoma rate not falling with increased sunscreen use . Use of these sunscreens may have increased the long UV A exposure if sun exposure increased since the suncreen decreased burning. There is actually little evidence that protection again t the sun protects against melanoma, but this issue is difficult to study epidemiologically.2 Clearly more research into thi matter is nece ary.
Self-Examination According to a study published in the May, 1998
Journal of the A merican Academy of Dermatology, people are more motivated to examine their kin for skin cancer if they have had di cu ions with doctors and if they think they are at hi~h risk for developing melanomas and other skin cancers. It is estimated that skin self-examination (SSE) may reduce mortality from melanoma by 63%. Eighty-one percent of tho e surveyed who talked to a health care orker were doing SSE compared to 35% who were practicing SSE but had not talked about sunning with a doctor or nur e. SSE was reportedly performed 1.5 time more often by women than men, with white persons performing SSE 1.7 times more often than other races. Some education beyond high school also increa ed the practice of regular SSE. Thus, there is clear evidence for the n ed for prevention through skin self-examination in melanoma. Thi will both ease its economic burden, and more importantly save live .
Relating Melanoma Risk to Nevi Recent r search has found that the risk for melanoma
wa trongl related to the number of small nevi, large non-dysplastic nevi, and clinically dysplastic nevi. In the absence of d splastic nevi, increased numbers of small nevi were a sociated with an approximately 2-fold increased risk, and increased numbers of both small and large nondysplastic nevi were associated ith a 4-fold increa ed risk. One clinically dy plastic nevu was associated with a 2-fold increased ri k, while 10 or more conferred a 12-fold increa ed risk. As well, there is an estimated 81.6%21 to 100%19 lifetime risk of melanoma in a person with familial dysplastic nevi who ha two relatives with melanoma. 19 In regard to congenital nevi, they appear to significantly increa the risk of malignant melanoma if they are large (= 20cm).3.2° The reported risk in patient with large congenital nevi varies from 3.8% -18%.20
68 ------------------------- U. W.O. Medical Journal 70 (l) 2000
Genetic Testing for Melanoma? It has been hown that approximately 8 to 12% of
melanomas appear to be inherited in an autosomal dominant fashion. A French tudy published in the October 1995 issue of the Archives of Dermatology concluded "a familial investigation should be performed for each pat~ent with cutaneous malignant melanoma (CMM), particularly when he or he exhibits phenotypic ri k factors for CMM such a red hair and atypical moles." 13
Furthermore, th ere is now trong evidence that germline mutation of the CDKN2A gene on chromo orne 9p21 predispo e to melanoma in a sub et of melanomaprone familie . A tudy published recently in the Journal of Cutaneou Medicine and Surgery concluded "the identification and subsequent surveillance of unaffected individual who have a genetic predi position to melanoma may lead to the detection of early (curable) melanomas and to a reduction in mortality." 10
Cost of Treating Melanoma A recent tudy in the U.S. found that the annual direct
co t of treating newly diagno ed melanoma in 1997 was e timated to be $563 million. Dr. Ja on River from the University of British Columbia noted tha t the Canadian figure i unknown, but estimated it to be 5-10% of the American co t.26 The American study broke down the cost of treating each stage of the disea e and found that Stage I and II disea e each comprised about 5% of the total cost; stage Ill and stage IV disease consumed 34% and 55% of the total co t, respectively. About 90% of the total annual direct cost of treating melanoma in 1997 was attributable to less than 20% of patients (those patients with advanced di ease, that is, stage III and stage IV). The study concluded that "in addition to the potential urvival advantages, aggre sive primary prevention through sun protection and intensive screening to enhance earlier detection shou ld reduce the economic burden of melanoma care." 5
Laboratory Tests And Imaging for Melanoma There i an ongoing controversy abo u t the use of
laboratory and imaging studie for baseline and for follow-up evaluation to detect malignant melanoma (MM) metastases. Some argue that no laboratory te ts or imaging studies hould be routinely ordered for patients who exhibit no evidence of metastases on history or physical examination. However, CXR screening may be sugge ted since it detects about 5% of metastase which would have been classified clinically as AJCC (the American Joint Committee on Cancer) stage I or II MM. LDH levels, which are inexpensive, are routinely ordered by orne physicians because metastases have been infrequently detected in asymptomatic patients. Some physicians also consid er computed tomography (CT) scans for patients who have thicker primary MM; CT of the c:hest sho~d be considered e recially if the patient has cerVIcal or axillary adenopathy.1 The final position from the Guidelines for the Management of Cu taneous Melanoma i that "extensive investigation for systemic metas tases in patien ts with primary melanoma is not
M i sce ll a n eous Artic l e s
recommended" and that " inve tigation su ch as CT, ma~_etic resonance imaging (MRI) cans, and positron enusswn tomography (PET) scans should be utilised only where specific symptom suggest the pre ence of meta ta es.9
Advances in Melanoma Therapy
The improvement of treatment options and urvival rates for melanoma patient is an important health care concern as melanoma is the tenth mo t common type of cancer in Canada.1
Several advance in the evaluation of regional lymph node , adjuvant therapy and genetic immunotherapy for the treatment of malignant melanoma have improved the treatment options for patients, as well as the five year survival rate for many patients according to a study in the May 1998 issue of the Journal of the American Academy of Dermatology.
The evaluation of regional lymph nodes has proved to be an important predictor of the long-term ou tcome. In patients with nodal metastase , the actual number of di ea ed node i the mo t important factor for the prognosis and overall urvival. Selective node dissection (which focu es on the main, or entinel, node) may be u ed to determine the condition of the entire group of nodes.9 Another evaluation of the regional lymph nodes, intraoperative radiolymphatic mapf,ing, increase entinel node identification to 99 percent. Both of these options are still controver ial, and confirmation is needed.
The most significant prognostic factor for melanoma is di ea e stage at presentation. While AJCC stage I and II melanomas (localised disease) have five year survival rate of ~ 85%, the rate for tage IV (metastatic) disea e is less than 5%, with median survival time of 6-10 months.n Becau e of the poor progno i of tage IV disease, clinical trials of adjuvant therapy are underway. A promising but controversial adjuvant therapy involves interferon alpha 2b ~hich may improve the long-term survival rates of patient . A study publi hed in the January 1996 issue of the Journal of Clinical Oncology hawed that "IF alpha 2b wa the first agent to show a significant benefit in relap e-free and overall survival of high-ri k melanoma patients in a randomized controlled trial." 14 However, at a recent conference addressing the issue, it was noted that only high dose interferon therapy (as opposed to low do e) may have potential benefit, but that at present, since clearly more re earch is needed, there is no standard therapy for high-risk melanoma patients. n
Genetic immunotherapy focuse on application of gene therapy as it applies to immunotherapy ba ed upon the understanding that melanoma appears to be an immunoresponsive di ease. One approach to gene therapy involves genetically modifying tumor cells to make them more immunogenic. Another approach involve the injection of foreign genes directly into the tumor in an attempt to impact the immune response to the tumor.
Due to the inconclusive evid ence tha t adj u vant therapy is beneficial for persons with melanoma, the Guidelines for the Management of Cutaneous Melanoma recommend referral to a melanoma centre for adjuvant therapy such as immunotherapy, chemotherapy or gene
U. W .O. Medical Journal 70 (1 ) 2000------------------------ 69
M i scellaneous A rticl es
therapy in patients with melanoma > 4mm in thickne and / or wi th involved node , whose progno is is poor.9
Melanoma is certainly one of the mo t s tu died condition in Dermatology, and with reason. Wi th the promising research into it treatment and prevention, we hope to ee declines in the incidence and improved urvival in the near future .
REFERENCES
1. Williams HC, Strachan DP (Eds.). (1997). The Challenge of DermatoEpidemiology. ew York: CRC Press.
2. Leig/1 IM, ewton Bishop fA , Kripke ML (Eds.). (1996). Skin Cancer: Cancer Surveys Vo/.26. New York: Cold Spring Harbor Laboratory Press.
3. http://www.aad.org (American Academy of Dermatology) 4. http://www.wvhealth.wvu.edu/Skinlstat .him (West Virginia Umversity)
T ao H, Rogers GS, Sober AJ. An estimate of the annual direct cost of treating culnneous melanoma. JAm Acad Dermato/1998; 38: 669-6 0.
5. Atillasoy ES, Seykora JT, Soballe PW, Elenit as R, Nesbit M, Elder DE, Montone KT, Sauter E, Herlyn M . UVB induces atypical melanocytic lesions and melanoma in human skin. Am J Pathol. 1998 May; 152(5):1179-1186.
6. Robinson JK, Rigel OS, Amonette RA . What promotes sk111 selfexamination? JAm Acad Dennato/1998; 38:5.
7. johnson TM, Yahanda AM, Chang AE, Fader OJ, Sondak VK. Advances in melanoma therapy. JAm Acad Dermato/1998; 38:5.
B. Australian Cancer etwork. (1997). Guidelines for the management of cutaneous melanoma. Sydney, Australia.
9. Hogg D, Brill H, Liu L, Monzon J, Summers A, From L, Lassam ]. Role of the eye/in-dependent kinase inhibitor CDKN2A in familial mela noma. journal ofCutaneoi/S Medicine and Surgery 1998; 2(3): 172-176.
10. Kirkwood J, Eggermont A (1998, ovember). Is high-dose interferon the standard adjuvant treatment in melanoma. Express Report from data Presented at the 23rd European Society for Medical Oncology Congress (EMSO), Athens, Greece.
11. Huan g CL, Provost , Marghoob AA, Kopf AW, Levin L, Bart RS. Laboratory tests and imaging studies in patients with cutaneous malignant melanoma. JAm Acad Dermato/1998; 39 (3): 451-461 .
12. Grange F, 01ompret A, Guilloud-Bataille M , Guillaume JC, Margulis A , Prade M , Demenais F, Avrilm MF. Comparison Between Familial and
onfamilial Melanoma in France. Arch Dermato/1995; 131 : 1154-1159. 13. Kirkwood ]M, Strawderman MH, Emstoff MS, Smith T], Borden EC, Blum
RH. Interferon alfa-2b adjuvant therapy for l1igh-risk resected cutaneou melanoma: the eastern cooperative oncology group trial EST 1684. journal ofCiinical Oncology 1996; 14 (1): 7-17.
14. Wasti QH, Kopf AW, Marghoob AA, Stefanato CM, Romero ]B, Roo BK, Bart RS. Anatomic distribution of cutaneous melanoma and painful sunburns in adults. Journal of Cutaneous Medicine and Surgery 1996; 1(2): 81-85.
16. http://www.cancercare.on.ca/ocr/ m1e Ontario Cancer Registry) 17. http://wuno.dermatology.orgldivision!cmf!cmfl .htm (Canadian M elanoma
Fo1mdation) 18. http://www.hc-sc.gc.ca/ (Health Canada Online) 19. Bergman W, van Voorst Vader PC, Ruiter OJ. Dy plastic nevi and the risk
of melanoma: a guideline for patient care. ed Tijdschr Geneeskd 1997;141 (42):2010-4.
20. Marghoob AA, Sclwenbach SP, Kopf AW, Or/ow Sf, ossa R, Bart RS. Large congenital melanocytic nevi and the risk for the developmeut of malignant melanoma. Arcl1 Dermatol. 1996; 132:170-175.
21. Tucker MA, Fraser MC, Gold tein Am, et a/. Risk of melanoma ar1d other cancers in melanoma-prone families. J Invet. Derma to/. 1993;100:350S-5S.
22. Westerdah/, ], Olsson H, Masback A, Ingvar C, Jonsson , Brandt L, et a/. Use of sun beds or sunlamps and malignant melanoma in southern weden. Am J Epidemio/1994;140:691-9.
23. Walter SO, Marrett LD, From L, Hertzman C, Sharwon HS, Roy P. The association of cutaneous malignant melanoma with the use of sunbeds and sunlamps. Am f Epidemio/1990;131:232-43.
24. Cascinelli , Krutmann ], MacKie R, Pierotti M , Prota G, Rosso , et a/. European School of Oncology advisory report: 1111 exposure, UVA lamps and risk of skin cancer. Eur J Cancer 1994;30A:548-60.
25. Stern RS, icl1ols KT, Vakeva LH. Malignant melanoma in patients treated for psoriasis with methoxsalen (p ora/en) and ultraviolet A radiation (PUVA): The PUVA Follow-Up Study. N Eng/ J Med 1997;336:1041-5.
26. Rivers ]. The Un iversity of British Columbia. Personal Communication, February 11, 1999. Q
FAMILY MEDICINE
W hy 200 Ontario Physicians have discovered the benefits of
MCI's management expertise
Flexible arrangements • Full or part time positions •
Short or long term •
Busy walk-in shifts •
Family practice •
We have 24 locations in the Toronto area.
To explore your options with MCI in complete confidence, please contact Margaret Gill ies at
MCI Medical Clinics Inc.
160 Eglinton Ave. East, Suite 200 Toronto, Ontario M4P 385
(416) 440-4040 ext. 433 [email protected] www.mcimed.com
70 ------------------------- U. W.O. Medical Journal 70 (1) 2000

Miscellaneou s Articl e s
CARDIOVASCULAR MANIFESTATIONS OF RHEUMATOLOGIC DISEASES:
A REVIEW
Agreat variety of sy temic di ea e and yndrome di play cardiova cular manife tations, and among these, the rheumatologic di eases figure
prominently. Such effect range from the trivial and the benign, such as most pericardia! effusion occurring in the context of collagen vascular diseases, to the severe and life-threatening, eg myocardial fibrosis occurring in cleroderma. 1 This review erves to briefly highlight the
cardiac con equences of orne of the more common rheumatoid conditions.
Sy temic lupu erythemato us (SLE) is a multisy tern di order in which tis ue are damaged by autoantibodie and immune complexes2 The va t majority of case occur in women in their child-bearing years. The disorder has a prevalence of 20-50 cases per 100,000, and is more frequent in blacks than in white .
Pericarditi i the mo t common cardiac manife tation of SLE, and occur in two thirds of patient . It is generally benign, sometime associated with pericardia} effusion , and rarely lead to tamponade or constrictive pericarditis. If not evident from the clinical background of SLE, the diagnosis can be made by the pre ence of lupu erythematosu cells or a titre of antinuclear antibodie . Valvular insufficiency is a rare consequence of SLE and i a result of Libman Sachs endocarditis, which may lead to sy temic emboli. Myocarditis may result in conduction abnormalitie , heart failure, or udden death.
The antipho pholipid yndrome is a well-known ub t of lupus and is associated with valvular dysfunction, a tendency towards thrombo i , myocardial infarction (MI), pulmonary hypertension. and cardiomyopathy. MI occurring in a lupus patient may be due to this prothrombotic tendency, or may be the result of lupu vasculiti , chronic steroid treatment, or coronary athero clerosis. Anticoagulation i recommended with high dose coumadin treatment, aiming for an INR between 2.5 and 3.0.
Rheumatoid arthriti (RA) i another multisy tern di ea e with diverse multiorgan effect , the sine qua non being an inflammatory synoviti that chiefly affect the peripheral joints.3 The prevalence of thi disorder is approximately 0.8%, with a female:male preponderance of 3:1. RA may affect any part of the heart, with pericarditi again being the mo t common cardiac complication (10-50% of RA patients); it is particularly prevalent in tho e patient with ubcutaneous nodules. Coronary arteriti , occurring in up to 20% of patients (ba ed on autop y
ABOUf THE AUTHOR Dan Hackam is the editor-in-chief of the University of
Western Ontario Medical journal. He has an interest in academic medicine and cardiology.
By Dan Hackam BSc, Editor-in-Chief
tudie ), may infrequently result in the occurrence of MI or angina pectori . Myocarditi and valvular insufficiency are further, rare complications.
Raynaud's phenomenon can be defined as episodic ischemia of the finger or toes occurring in the context of expo ure to cold weather or objects.~ It may be primary and idiopathic, in which ca e it is known as Raynaud's disea e, or may be econdary to an underlying disease, medication, or other process. Raynaud's disease has a female :male preponderance of 5:1, with a peak onset between the age of 20 and 40. The disorder is associated with primary pulmonary hyperten ion and coronary va o pasm (also known as variant angina).
Scleroderma is a multiorgan disease typified by fibrosis of the kin, blood ve els, and viscera. 5 Cardiovascular complications are frequent in the diffuse cutaneous systemic dero i ubset, and rare in the more limited form of scleroderma. The e manife tations include pericarditis, heart failure secondary to hypertension or cor pulmonale, and arrhythmias. Left- ided heart failure occurs in up to 30% of patients with diffuse cutaneous scleroderma.
Ankylosing spondyliti (AS) is an inflammatory di order that characteristically affects the axial skeleton, starting in the 2nd or 3rd decade of life.6 The male:female preponderance is 3:1. The two cardiovascular effects of AS are aortic regurgitation and conduction defects. In a small percentage of patient , all three layers of the aortic valve and proximal thoracic aorta are thickened and scarred, re ult:ing in aortic insufficiency. The frequency of both the valvular abnormality and the conduction defect increase with the duration of the di ease.
In do ing, the e cardiovascular manifestations are by no means the commonest effects of rheumatological disorder , but when they occur, they may be devastating to the patient. It is therefore important that the noncardiologi t have a good grasp of these complications, in term of natural history, diagno i , and management.
REFERE CES
1. Eugene Braunwald. Approach to the patient with heart disease. In : Fauci AS, Braunwald E, lsselbacher K], WilsonJD, MartinJB, Kasper DL, Hauser SL, Longo DL, ed . Harrison=s Principles of lntemal Medicine. 14th ed.
ew York: McGraw-Hill, 1998: 1229-1231. 2. Boumpas DT et a/. Systemic lupus erytlzematosus: emerging concepts. Part
1: Renal, neuropsychiatric, cardiovascular, pulmonary, and hematologic disease. Ann lntem Med 1995; 123:42.
3. Harris ED, Jr. Rheumatoid arthritis: pathophysiology and implications for therapy. Eng/ I Med 1990; 322:1277.
4. Coffman JD. Raynaud' phenomenon. ew York: Oxford University Press, 1989.
5. l.egerton CW ill et al. Systemic sclerosis (scleroderma). Oiniad management of its majoramzplimtions. Rheum Dis Gin North Am1995; 21:2Q3.
6. Calin A and Taurog JD, eds. The Spondyloartlzritides. Oxford: Oxford University Press, 1997. Q
U. W.O. Medical Journal 70 (1} 2000------------------------- 71
mN~rvasc ··· Brief Prescribillf 1o1..-.. NORVASC famlodipine besylate) Tablets 2.5, 5 and 10 mg Antihypertensive-Antianginal Agent ACTION AND CUNICAl PHARMACOLOGY
' , .. ·.
NORVASC (amlodipine besylate) is a calcium ion influx inhibitor (calcium entry blocker or calcium ion anugonist). Amtodipine is a member of the dihydropyridine class of calcium antagonists. INDICATIONS AND CUNICAl USE llyporteosioa NORVASC (amlodipine besylate) is indicated in lht treatment of mikt-to-moderate essential hypen.ension NORVASC should normalty be used in those patients in whom treatmem with diuretics or beta-blockers was found ineffective or has been associated with unacceptable adverse effects. NORVASC can be tried as an initial agent in those patients in whom the use of diuretics and/or beta·bktckers is contraindicated or in patients with medical conditions in which these drugs frequently causa serious adverse effects. Combination of NORVASC with a diuretic. a beta·IOOcking agent. or an angiotensin converting enzyme inhibR:or has been found to be compatible and showed additive antihypertensive effect. Cluooic Slo~le AllfiN NORVASC is indicated for the managemem of chronic stable angina (effort-associated angina) in patients who remain symptomatic desp e adequate doses of beta-blockers and/or organic nitrates or who caMot tolerate those agents. NORVASC may be tried in combination with beta-blockers in chronic stable angina in patients With normal ventricular function. 'Nhen such concomitant therapy is introduced, care must be taken to monitor blood pressure ~~~~'.:~=~";ion con occur from the combined effects of the drugs.
NORVASC famlodipine besylatel is contraindicated in patients with hypersensitivity to the drug or other dihydropyridine• and in patients with severe hypotension floss than 90 mmHg systo~c) . WARNINGS lncrouo4 Allfino ertd/a< MyGcenliellllfon:tioa ~arety. pa ·enu, particularty those with severe obstructive coronary artery disease. have devetoped documented mcreased frequency, duratiOn end/or severity of angtna or acute myocardial infarction on starting calcium channel blocker therapy or at the time of dosage increase. The mechanism of this effect has not been etucidated Olllllow OhtrtoctiH (Aomc SIHosis) NORVASC should be used with caution in a presence of fixed left ventricular outflow obstruction (aortic stenosisl. Uso in Potients widllmpoirocl Hepotic Ftonction There are no adequate studies in patients with liver dysfunction and dosage recommendations have not been established. ln a sman number of patients with mild· to-moderate hepatic impairment given single dose of 5 mg, amlodipine hd-f~e has been prolonged. ORVASC should. therefore, be administered with caution in those patients and careful monitoring should bo performed. A lower starting dose may bo required (see DOSAGE AND AOMINISTRAnON). B ... · blockor Wttlldrowol NORVASC gives no protection against the dangers of abrupt beta-blocker withdrawal and such withdrawal should be done by the gradual reduction of the dose of be •-blocker. PRECAUTIONS Use: ia PMints willl Cotttestiw H .. rt Fail•re Although generllty caldum channel blockers should onty be used with caution in patients with heart failure, it has been observed that NORVASC had no overall deleterious effect on survival and cardiovascular morbidRy tn both short-term and long-term clinical trials in these patients. While a significant proportion of the patients in these studies had a history of ischemic hean disease, ang•na or hypenension. the studies were not designed to evaluate e treatment of angina or hypenension in patients with concomitant hean faiure. HypototosiH NORVASC famlodipine besylate) may occasionally precipitate symptomatic hypotension. Careful monitormg of blood pressure 1s recommended, especiatty in patients with a history of cerebrovascular insufficiency, .,,d those taking medications known to lower blood pressure. Peripllorol Edot111 Mild·to·moderate peripheral edema was the most common adverse evant in the clinical trials (see ADVERSE REACTIONS). The incidence of peripheral edema was dose-dependent and ranged in frequency from 3.0 to 10.11% in 5 to 10 mg dose range. Care shoutd be taken to dffferentiate this peripheral edema from the effects of Jncrusing left ventricular dysfunction. Uso io f'rotNocy Although arNod1pine was not teratogenic in the rat and rabbn. some dihydropyridine compounds have been found to be teratogenic in animals. In rats, amlodipine has been shown to prolong both the gestation period and the duration of labor. There is no clinical experience with NORVASC in pregnant women. NORVASC should be used during pregnancy ontv if the potential benefit outweighs the potential risk to the mother and fetus. N•rsi .. Modters It is not known whether amlodipine is excreted in human m;lk. Since amlodipine safety in newborns has not been established, NORVASC should not be given to nursing mothers. Use: in Ctlildqn The use ol NORVASC is not reconwnended in children since safety ond efficacy have not been established in that popula1ion. Usoio EJclorty In elderty patients (265 years) clearance of amlodipine is decreased with a resulting increase in AUC. In dnical trials the incidence of adverse reactions in elderly patients was approxunatety 6" higher than that of younger population 1<65 years). Adverse reactions include edema, muscle cramps and dizziness. NORVASC should bo used cautiously in elderly patients. Dosage adjustment is advisable I see DOSAGE AND AOMINISTRAnON). lnlorlctioo wid! Gropofno~ Juice Published data indicate that through inhibition of the cytDchrome P450 system, gropefru~ juice can increase plasma levels and augmem pharmacodynamic effects of some dihydropyridine calcium channel blockers. followmg oral ad · ·stration of 10 mg amlodipine to 20 male volunteers, pharmacokinetics of amlodipine were sirrular when amlodipine was admirvstered with and without grapefruit juice. D ... lotoroc:ti-As 'Nith al drugs, care shoukl be exercised when treating patients wRh rootbple medications. Dihydropyridine calcium channel bk)ckers undergo biotransformation by the cytochrome P450 system, mainty via CYP 3A4 isoenzyme. Coad· ministration of amlodipine with other drugs which follow the same route of biotransformation may resutt 1n altered btoavailabiiRy of amlodipine or these drugs. Dosages of similarly metabolized drugs, particularty those of low therapeutic ratio, and especia in patients with renal and/or hepatic impairment. may raquire adjustment whan starting or stopping concomitlntty administered amlodipina to maintain optimum therapeutic blood levels. Drugs known to be inhibitors of tho cytochrome P450 system include: azote antifungals. cimetidine, cyclosporine, arythromycin. quinidine, terfenadine. warfarin. Drugs known to be inducers of the cytochrome P450 system include: phenobarbital, phenytOin, rifampin. Drugs known to be l>iotansformed via P450 include: bonzodiazepines. ftecainide, imipramine, propofenone, theophylline. Amlodipine has a low Irate of first-pass) hepatic clearonce and consequent high bioava~ability, and thus. may be expected to have a low potential for clinicalty relevant effects associated with elevation of amlodipine plasma levels when used concomitantly with drugs that compete for or inhibit the cytochrome P450 system. Ci..tidiH, Warfarin. C,Ciosporia. Digoxia; Pharmacokinetic interaction studies with amlodipine in heatthy volunteers haw indicated: • ciiMtidina did not alter the pharmacokinetics of amlodipine. • amlodipine did not change warfari•·induced prothrombin response time. • amlodipine does not significandy alter the pharmacokinetics of ~losporiL • amlodipine did not change serum digoxi• levels or digoxi• renal clearance. Alotacids Concomitant administration of Maatox- (magnesium hydroxide and aluminum hydroxide I had no effect on the dis· position of a single 5 mg dose of amlodip10e in 24 subjects. Bota-bloekers: When beta-adrenergic receptor blocking drugs are administered concomitantly with NORVASC, patients should be carefully monitored since blood pressure lowering effect of beta-blockers may be augmented by amlodipine's reduction in peripheral vascular resistance. ADVERSE REACTIONS
ORVASC famlodipine bosylatel has been administered to 1,714 patients (1105 hypertensive and 909 angona patients) in controled clinical trials fvs placebo alone and with active cornparatiivo agents). Most adverso
reactions reponed during therapy were of mild·to·moderate severity. ltyportoosioa In the 805 hypertensive patients treated with NDRVASC in comoled clinic II trials, adverse effects were reported in 29.9ll ol patients and requirod discontinuation ol therapy due to side effects in I A ol patients. The most common adverse rwac:tions in comoled clinicll trials were: edema f8.9'Jf.land headache fti.J'JI~ The folowing adverse reactJOns wore reported With an incidence of~" in the comoled clinical trials program fn=Ui~ Conliovosuler. edema I8.9'Jf.), palp~ations l2.0ll), tachycardia 10.7"1. poSilJral dizziness 10.5"1-Skio and ~pruritus fD.n.). Mncolosltel ... l: muscle cramps (0.5"1-Cootraleod Poripllorol Nervoa SystoM: headache (8.3"1. diuiness IJ.Oll), paresthesia (0.5"1--ic N.,.... SysteM: flushing (3.1"1. increased sweating f0.9'Jf.), dry mouth fo.7"1-Psyc~iotric: somnolence (1.4"1-Gomoiotntioal: nausea 12.4"1. abdominal pein 11.1"1. dys>epsia ID.6"1. constipation IO.S"I- GOMrlll: fa ·gue (4.1"1. pain 10.5"1-AIIfioa In the cootroled clinical trials in 909 angina patients treated with NORVASC. adverso effects were reported in :ns" of patients and required discontinuation of therapy due to side effects in 0.6" of patients. The most common adverse reactions reported in controlled clinical trials were: edema f9.9'Jf.land headache 0 .11%). The following adve,.e reactions occurred at an incidence of~" in tho cootrolled cirical trials program fn=909): Conliowasc:uler. edema I9.9'Jf.), palpitations I2.Dll). postural diuiness 10.6"1- Skio 1od Appoodegos: rash fi.Oll), pruritus 10.11%~ Mncolosltelotat muscle cramps (l .!Jll). Cootralood Poripllofal No.- S,.U. headache 0 .11%), dizziness 14.5"1. partsthesll(l.Oll). hypoestheSio IDA~- Nonooo SystoK ftushing (1.9'Jf.). Psyc~iotric: somnolanco(1.3 , insomrna I0.9'Jf.), nervousness ID.7"1-Gomoiotntioat nausea 14.3), obdominal pein 12.2"1. dys:>epsi1 fU"I. diarrhea 11.1"1. flatulence II .alii, constipation I0.9'Jf.). Rospirotory Syst- dyspnea 11 . 1"~ Spoc:iel Senses: abnormal vision 11~1. tinnitus (0.6"1-G-rot fatigue (4.11%). poin (l.Oll), asthenia fl .!Jll). NORVASC has been evalueted for safety in about 11,000 patients with hypertension and angina. The follow;ng events occurred in <1% but >0.1% of panents in comparative clinical trials (double· blind comparative vs placebo or active agents; n = 2.,615) or under conditions of open trials or marketing experience where a causal relationshi:l is uncertain. Conliowasc:olar. arrhythmia (including ventricular tachycardia and atrial fibrilation), bradycardia, hypotansion, peripheral ischemia, sync ape, tachycardia, poSilJral dizziness, poSilJral hypotension. Cootralood Poripllofal NOfVOft Systotn: hypoesthesia, tremor, vertigo. Gulroiotntioal: anorexia, constipation, dysphagia, vomiting, gingival hyperplasia. Gnenl: asthenia'. back pain. hot flushes, malaise, rigors, weight gain. Mac•loskei.UI Syst:eta: arthnlgia. arthros s. myalgiL Psycli•imic: sexual dysfunction (male' and fematat insomnia, nervous· ness, depression. abnormal dreams. anxiety. depersoMiilltion. Respir-.tory Systeta: epistaxis. Skin aH Appondogos: pruritus', rash erythematous, rash maculopapular, erythema mulliforme. Spoc:ial Sotosos: canjunctivilis. diplopia, eye pa10. tinnitus. Urinary System: micturition frequency, micturition disorder, nocturia. Autnomic Ner, .... Systonl: dry mouth, increased sweating. M ... bolic ond Nutritioo 1: thirst. H-iotic: purpura. These events occurred in less than 1" in placebo-controlled trials, but the incidence of these side effects was
between 1" and 2% in aU muttiple dose studies. The foUowing events occurred in sO. I" of patients: cardiac failure, skin discoloration. urticaria, skin dryness, Stevens,.Johnson S'(Odrome,afopecie, twitching. ataxia, hypertonia, m.graina, apathy, amnesia. gastritis, pancreatitis, increased appetite, coughing. rhinitis, parosmia, taste perversion, and xerophthalmia. Isolated cases of angioedema have been reported. Angioedema may be accompanied by breathing difficulty. In postrnarketing experience, jaundice and hepatic enzyme elevations (mostJy consistent with cholestasisl in some cases severe enough to require hospitalization have been reported in association with use of amlodipine. SYMPTOMS AND TREATMENT OF OVERDOSAGE s,..,._ Overdosage can cause ucessive peripheral vasodilabOn with marted and probably prolonged hypotension end possibly a reflex tachycardia. In humans. experience with overdosage ol NORVASC famlodipine bosylate) is · ed. When amlod1pine was ing sted at doses of 1()5..250 mg some patients remained normotensive with or without gastric lavage while anothor patient experienced hypotansion 190150 mmHg) which normalized following plasma expansion. A patiem who took 10 mg of amlodipine with banzodiazepine developed shock which was refractory to treatment and died. In a 19 month-old child who ingested 3D mg of amlodipine Ia boot 2 mglkg) there was no evtdance of hypotension but tachycerdia (180 bpm) was observed. Ipecac was administered 3.5 hrs after ingestJon 1nd on subsequent observation (overnight} no sequelae were noted. TreltMIIt Clinicalty significant hypotension due to overdosage requires active cardiovascular suppon including frequent monn.oring of cardiac and respiratory function, elevation of extremities, and attention to circulating nuid volume and urine output A vasoconstrictor (such as norepinephrine) may be elpful in restoring vascular tone and bfood pressure. provided that there is no contraindica on to its use. As NORVASC is highty protein bound, hemodialysis is not likety to be of benefit. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channeJ blockade. Clearance of amlodipine is prolonged in eklerty patients and in pa ents with impaired liver function. Sinceamlodipine absorption is stow. gastric lavage may be worthwhile in some cases. DOSAGE AND ADMINISTRAnON Dosage should be individu>fized depending on patien(s tolerance and responsiveness. For both hypertension and angina, the recommended initial dose of NORVASC famlodipine besylate) is 5 mg once daily. ~necessary, dose can be increased ah.er 1·2 weeks to a maximum dose of 10 mg once daity. Uso iotloo Elclortya<io PotiHCswido hlopairociRooalfwctiH The recommended initial dose in patients over 65 years of age or patie1'1tS with impaired renal function is 5 mg once daily. ~ required, increasing in the dose should bo done gradually and with caution (see PRECAUTIONS). Uso io Potieots widlhlopairocl Hepotic Ftooction Dosage requirements have not been established in patients with impaired hepatic function. When NORVASC is used in these patients, the dosage should be carefuttv and gradualty adjusted depending on patient's tolerance and response. A lower starting dose of 2.5 mg once deity should be considered (see WARNINGSI. DOSAGE FORMS Availability NORVASC is available as Ylhhe octagonal tablets contavnng amlodipine besytate equivalent to 2.5, Sand 10 mg amlodipine per tablet The respective tablet strengths are debossed on one tablet face as ·NRV z.s·. ·NRV 5'" and "NRV 10" with "Pfaer· on the opposita face. The 5 mg tablet is scored. Supplied in wh~e plastic (high density ~'7:ne) bottles of I DO tablets for each strength. Also the 5 mg and 10 mg are supplied in bottles of250tablets.
Store at 15-JO"C. Protect from 6ght REf£RENCES: ANGINA I. NORVASC" Product Monogreph, Pfizer Conada Inc.. Dec. 1!1, 1!197. 2. PureeD H, Waller DG, Fox K. Therapeutic focus: calcium antagonists in cardiovascular disease. Br J Clin Pract
1989;43110):369-79. 3. Salerno SM and Zugibe FT. Calcium channel antagonists. What do the second generation agents have to
offer? Postgrad Med 19!!4;9511 ):181-90. 4. Oeanfield JE at al Amlodipine reduces transient myocardial ischem a in patients wilh coronary artery dtsease:
double-blind circadian anti-ischemia program in Europe (CAPE triaij JAm Col Canlioll!l94;2416):1460-7. 5. Ezekowitz MD et al Amlodipine in chronic stable angina: resutts of a multicenter double· blind crossover trial.
Am Heart J 1996;129131:527-35. 6. van Kest:eren HAM. A double-blind, comparative study of amlodipine vs dilt:iazem CR i1 the treatmem of stable
angina. Poster presonta ·on. XVIIth Coogress of the European Society of Cardiology, Amsterdam. August 23. 1995. RER:RENCES: HYPERTINSION 1. NORVASC" Product Monogroph, Pfizer Canada Inc. Dec. 19, 1997. 2. Hernandez-Hernandez R et al The effects of missing 1 dose of enalapril versus amlodipine on ambulatory
blood pressure. Blood Pcessure Monitoring 1996;1:121-6. 3. Uischer TF and Cosentiro F. The classification of calcium antagonists and their selection in the treatment of
hypertens on - a reappraisal. Drugs 1998;5514~50!!-17. 4. leenen FHH, Fourney A. Tanner J. Persistence of anti-hypenensive effect ah.er interruption of therapy with
long-acting famlodipine) vs short-acting fdiltiazem) calcium-antagonist. Clin and Investigative Medicine 1!194;17(4) Suppl. B 70.
5. Hoegholm A et al. Compuative effects of amlodipine and felodipine ER on office and ambulatory blood pressure in patients with mild to moderate hypertension. J Human lfypertens 1995;91SuppiiO):S25-S28.
6. Ostergren Jet al. Effect of amlodipine versus felodipine extended release on 24·hour ambulatory blood pressure in hypertension. Am J Hypertens 1998;11~.
7. Neaton JD et al Treatment of mild hypertension SllJdy. JAMA 1993".27016):713-24. 8. Perna GP et al. Tolerabilty of omlodipine - A meta-onalysis. Clin Drug Invest 1997;131Suppll ): l63-68.
• ()1999 Pfizer Canada Inc • Kirtland, Quebec H9J2M5
rev.CHF.I:II99
I PAAB I
"TM Pfaer Products Inc. Pfizer Canada lnc .. licensee Product Monograph Avaaable Upon Request.
AlanD. EII!I'Oted blood pressure
Quit smoking
for listening. with careful li tening.
That wh~ for over 25 years, more health care
pro iders have counted on the reliability
and uperior acou tics of 3M"' Littmann'"
C 3M 1998 9804MS07717
tetho cope than any other brand. To hear
more, call 3M Health are at 1- 00-3M
HELP (364-3577), or vi it our web ite at
http://www.3M.com/ Littmann.
3M Health Care
Long-acting BP control for mild-tomoderate h pertensi es
• effecti el control BP a ar e le el for a full 24 hour and bevond --
• intrin icall lon hal'-li'e maintain plasma le el to reduce BP up to 2 hours a· era mi sed dose
• hm n to be more effecti e han felodipine a arne dose· •
C.1 999 Pizer Canada Inc.
i land. Quebec H9J 2\.\5
e
lmpressi e tolerability after 4 years
• compared \\ith antih perten i e from four different cia ses, more OR C patients remained on therap after 4 ear -,
• onl 3°o \ i dra\ al rate among 12,831 pa ien in 16 clinical udies
and headache 83'11.1.
in"oona ion ior lmportan saret) infoonation interactiCW!s
"T\.~ Piizer Products Inc. Piizer Canada Inc .. licensee PAAB
H E R E TODAY. H E R E TOMORROW.