Embed Size (px)
Citation preview

Table of Contents
In-House CounselorA Publication of the American Health Lawyers Association In-House Counsel Practice Group
Editor’s CornerTizgel High Amanda Brown Jody Joiner ...........................................1
A Practical Guide to Planning and Executing a Hospital TransactionKatherine Lofft Colin McCulloch ..................................3
Marching Forward with HIPAA Omnibus: Three Priorities for 2014Jan McDavid ........................................6
Clinically Integrated Networks and Contracts with Commercial Payers: The New FrontierGary Herschman Diana Fratto John Harris ..........................................8
Chair’s ColumnCharlesWhipple ..................................12
The Sunshine Act: Shining Light on Impending ImplementationKatherine Kraschel Brendan Abel .....................................13
Unique Factors Impact Fair Market Value Determinations for Children’s Hospitals and Pediatric ProvidersTom Schnack Cori Casey Turner .............................16
VOLUME
20 ISSUE1 March
2014
In-House Counselor © 2014 is published by the American Health Lawyers Association. All rights reserved. No part of this publication may be reproduced in any form except by prior written permission from the publisher. Printed in the United States of America.“This publication is designed to provide accurate and authoritative information in regard to the subject matter covered. It is provided with the understanding that the publisher is not engaged in rendering legal or other professional services. If legal advice or other expert assistance is required, the services of a competent professional person should be sought.”
—from a declaration of the American Bar Association
Editor’s CornerTizgel K.S. HighLifePoint Hospitals Brentwood, TN
Editorial BoardAmanda BrownWaller Lansden Dortch & Davis LLP Nashville, TN
Jody JoinerINTEGRIS Health Oklahoma City, OK
We are pleased to offer you a very informative and timely array of articles for this Spring issue of the In-House Counselor. I hope that every member of the In-House Counsel Practice Group
(In-House PG) can find a nugget that adds value to your practice and the companies that you serve. As the health care landscape continues to evolve, we strive to bring you information that keeps you in the know.
In A Practical Guide to Planning and Executing a Hospital Transaction, Katherine Lofft and Colin McCulloch provide a “top ten” list of the most-common failures of transaction planning and execution to help you avoid potential landmines as you work your way through a sale, merger, acquisition, or other change of control of a health care entity.
In-House Counselor
2
Jan McDavid, in Marching Forward with HIPAA Omnibus: Three Priorities for 2014, points out areas of focus for health care covered entities and business associates to ensure continued compliance with the requirements of the Health Insurance Portability and Accountability Act Omnibus Rule.
In Clinically Integrated Networks and Contracts with Commercial Payers: The New Frontier, Gary Herschman, Diana Fratto, and John Harris give a thorough overview of clinically integrated networks (CINs) and provide practical recommendations regarding the structure and implementation of CINs as the health care industry moves towards these arrangements with increasing frequency.
Katherine Kraschel and Brendan Abel focus on the Physi-cian Payments Sunshine Act provision of the Afford-able Care Act in The Sunshine Act: Shining Light on Impending Implementation, discussing the potential impact of the Act as we near the first annual reporting deadline for manufacturers on March 31, 2014.
In Unique Factors Impact Fair Market Value Determina-tions for Children’s Hospitals and Pediatric Providers, Tom Schnack highlights the unique challenges of deter-mining fair market value for services provided in a pedi-atric patient setting.
I would like to thank our authors for submitting these informative articles on matters that are of timely impor-tance. I would also like to thank the Editorial Board for their generous time spent preparing this newsletter. The In-House PG is always looking for authors. If you have an interest in publishing your work, please contact me (see page 2 for contact information). We are currently interested in newsletter articles for publication in the next issue of the In-House Counselor.
Sincerely,
Tizgel In-House PG Vice Chair of Publications
Charles R. Whipple, Chair Executive Vice President & Chief Legal Officer Hallmark Health System Melrose, MA (781) 979-3050 [email protected]
Robert A. Gerberry, Vice Chair– Educational Programs Summa Health System Avon, OH (330) 375-7515 [email protected]
Susan Feigin Harris, Vice Chair– Membership Baker & Hostetler LLP Houston, TX (713) 646-1307 [email protected]
Tizgel K.S. High, Vice Chair– Publications Assistant General Counsel LifePoint Hospitals Brentwood, TN (615) 920-7634 [email protected]
Davis W. Turner, Vice Chair– Research and Website Frost Brown Todd LLC Nashville, TN (615) 251-5566 [email protected]
In-House Counsel Practice Group Leadership
3
A Practical Guide to Planning and Executing a Hospital TransactionKatherine R. Lofft*Colin G. McCulloch Epstein Becker & Green PC Washington, DC
The sale, merger, acquisition, or other disposition or any change of control of a public or private hospital raises a number of legal and regulatory, as well as financial,
operational, administrative, and other issues. The failure to identify and proactively manage these issues can help derail or needlessly complicate an already-complex deal. Below, we share our experience with the most-common failures of transaction planning and execution in the form of a “top ten” list, together with our recommendations to address each of them.
1. Not Having a Game Plan (“Ready, Go, Set”).We have seen transactions fail because the seller identified a “deal-breaker” late in the process, or the buyer realized the “opportunistic” transaction it was pursuing didn’t have a place in its strategy.
A hospital transaction is time and resource intensive, for both the buyer and seller. We recommend identifying your objectives, timing, and deal breakers early. Try also to antici-pate the other side’s own objectives, timing, and options. This allows all parties to be in a position to communicate their positions, needs, and desires clearly, which may help avoid a later catastrophe.
2. Using Inexperienced/Unmanaged Resources (“He’s Not an Expert, but He Plays One on Television”).
We have seen transactions run off the rails when an organi-zation engages so-called expert advisors who lack sufficient industry or transaction experience, or the ability to under-stand the client’s business or to communicate effectively. We also have seen transactions that have been complicated or delayed by the client’s use of internal resources, only to find later that they lack the time, background, experience, or oversight to effectively or efficiently complete the job.
We advise weighing the tradeoffs involved in using internal resources versus external and experienced vendors. If utilizing internal resources, ensure that those resources have the time and experience to perform the tasks assigned to them. Carefully vet any potential outside advisors in advance. If multiple advisors are engaged, identify a single project manager and carefully delineate roles and responsi-bilities, which will help minimize duplication of effort and
contradictory approaches or advice, and help avoid missed issues and poor communication.
3. Inability to Manage Key Stakeholders (“You Bought the House, but Someone Else Holds the Keys”).
Although it is easy to identify who owns or controls a hospital, others may have an important stake in that hospital’s continued existence and/or future operations. These “other” stakeholders may include members of the hospital’s medical staff, the local community, and/or local and state govern-ment agencies, and they can materially delay or even prevent a transaction. We’ve seen public meetings devolve into ugly protests simply because the interests and perspective of the local community were not anticipated and addressed.
We recommend anticipating critical path areas and potential opportunities for other stakeholders to undermine the transac-tion. Identify and cultivate people who can help promote or champion the transaction with affected stakeholders and assist with messaging and managing stakeholder expectations.
4. Inconsistent Messaging (“The Neighbors May Be Watching”).Although confidentiality in the early stages may be critical for negotiating the key terms of a hospital transaction, it is a rare transaction that can or will be kept secret until closing. A community hospital may be one of the largest and/or oldest employers in a given area. Between the medical staff and hundreds or thousands of employees, and the efforts of professional journalists and bloggers looking for stories of keen local interest, it can be difficult to keep the lid on a potential transaction. It is not uncommon to read inaccurate news articles and editorials regarding a transaction, which is often a consequence of un- or ill-informed sources, reporters, or public officials.
Consider developing a media and/or public relations strategy for the transaction. Designate individuals who are autho-rized to speak to the media and public about the transac-tion. Devise scripts and have each spokesperson rehearse in advance of key hearings, interviews, and public appear-ances. Once a potential transaction is announced, consider providing regular updates to the community and/or sharing milestone events.
5. Neglect of Regulatory Oversight (“Big Brother Is Watching”).We have seen hospital transactions fall apart when challenged by state or federal authorities. Even if a challenged transaction ultimately proceeds to closing, it is likely to take longer and/or be more costly to close. Anticipating and preparing for key issues, challenges, and questions that are likely to arise in the context of a regulatory review can help facilitate the process and may help ensure a favorable outcome.

In-House Counselor
4
The average hospital transaction is likely to require the approval of one or more federal and/or state regulatory authorities. We recommend identifying these authori-ties and any associated review process or requirements as early as possible. Identify and cultivate contacts with these authorities. Review prior decisions or opinions of the authority regarding similar transactions and anticipate and proactively address issues or questions that are likely to arise in the course of review.
6. Failure to Appreciate the Devil in the Details (“What Do You Mean I Can’t Get Out of Your Bad Contract?”).
All too often we have seen due diligence fall casualty to the need to quickly close a transaction for strategic, competitive, or financial reasons. Inadequate due dili-gence, however, can lead to a laundry list of problems. It can complicate efforts to integrate and realize key opera-tional or economic efficiencies from an acquired business or assets, or can increase (sometimes dramatically) the acquiring party’s estimated transaction costs. Similarly, the parties may fail to carefully identify what assets and/or liabilities are intended to be transferred, versus retained, in the transaction.
We recommend treating due diligence as a critical part of the transaction process. Devote due attention and resources to this effort. Carefully review, among other things, the assignability and termination clauses in the target’s material contracts, any title and lien issues involving the target’s real or personal property, and any donor restrictions that may apply to land or other capital assets to be transferred. Thor-ough diligence prior to closing can help reveal these issues and allow the acquiring party to minimize or mitigate any problems they may create, or to plan for adverse impacts.
7. Loss of Focus on Business Operations (“Keep Your Eyes on the Road”).
We have seen hospitals lose value during the negotia-tion, documentation, and closing of a transaction because management was so focused on the transaction that it lost sight of running the hospital. This can apply to both targets and acquirers. Leaving off the day-to-day opera-tional requirements and details may lead to issues that could constitute grounds for terminating the deal, or that may reduce the anticipated benefits of the transaction and/or undermine public support for the deal.
Operating a hospital is like running a train—it is not easily started or stopped and if left to run on its own, it will quickly derail. No transaction is completed until it is closed, and even then, effective integration is important. Ensure that senior management and key officers and employees who may need to be involved in the transaction planning or negotia-
tions have adequate time and attention to devote to their day-to-day activities. Delegate authority and responsibility for transaction-related matters, including integration efforts, where appropriate. Make strategic use of outside advisors or resources to help ensure the availability of internal resources to continue to run the business.
8. Not Appreciating the Value of Early Courtship (“Don’t Wait Until the Marriage to Start Dating”).
We have seen transactions become unnecessarily compli-cated or expensive, or that have failed, simply as a result of the parties’ and their advisors’ poor interactions with one another. A party’s perception or expectations of how it will or should be treated by the other can underlie its interest or enthusiasm, or its very rationale, for the transaction. Regard-less of whether the seller will have continuing involvement in the future operations of the hospital, other stakeholders such as the medical staff, employees, and community may make judgments about the new owner based on what they heard (whether true or not) about the transaction process.
The “world” is small and we recommend that both buyers and sellers conduct themselves accordingly. Ensure the principals on each side of the transaction have ample time to meet and to get to know one another. Do not necessarily discount the value of reputation. No matter the nature and extent of any direct interactions, an organization or indi-vidual that has separately developed a reputation for indeci-sion, imperiousness, or irascibility—of not “playing nicely

5
in the sandbox”—may well exhibit those same qualities during the transaction process or after closing.
9. Understand Your Options in the Event the Transaction Fails (“What’s Our Back-Up Plan?”).
It is not uncommon for a party to enter into a potential transaction, particularly a once-in-a-lifetime “opportu-nistic” play, without a back-up plan. However, a party that starts negotiating a deal without having a “Plan B” often finds itself at the whim of the other party(ies). It usually does not take the other side long to figure out that its counterparty has or believes it has no choice but to do the deal, and to use this against them. In this scenario, the negotiation generally devolves to one intended less to maximize advantage, than to merely soften the terms of surrender.
Every organization should understand why it is entering into a potential transaction. Not every hospital transac-tion will be successful, and there is often more than one way for a party to execute its mission and to realize its strategic goals and objectives. Understanding your orga-nization’s goals, and its options to achieve those goals, can keep you focused on the important elements of the transaction and ensure you don’t chase a “great” deal into undesirable territory.
10. Not Identifying Who Is Empowered to Negotiate for the Parties (“Too Many Cooks Spoil the Broth”).
We have seen transactions compromised because the terms the parties thought they had negotiated required approval of a previously unknown or unidentified party. Sometimes, a deal flounders because a party empowers several advisors or entities (whether attorneys, financial or other advisors, directors, or management) to negotiate on its behalf, which can cause uncertainty and confusion.
A hospital is generally run by a single individual—we believe a similar principle should hold true for a hospital transaction as well. We recommend you designate a single individual or small group of individuals who are empowered to negotiate all terms on your behalf. That individual or group should meet or communicate regularly with the project team responsible for diligence, drafting and negotiation of the definitive agreements, and integration issues, to ensure everyone is reading from the same playlist. If you are faced with a counter-party that presents multiple decision makers, insist that the party clarify each individual’s role and authority.
*Katherine R. Lofft is a member of the firm and Colin G. McCulloch is an associate in the Washington, DC, office of Epstein Becker & Green PC, a national law firm.
A similar version of this article was published in AHLA’s Business Law & Governance newsletter, with the permis-sion of the AHLA staff.
Practice Groups StaffTrinita Robinson
Vice President of Practice Groups (202) 833-6943
Magdalena Wencel Senior Manager of Practice Groups
(202) 833-0769 [email protected]
K. J. Forest Practice Groups Distance Learning Manager
(202) 833-0782 [email protected]
Brian Davis Practice Groups Communications and
Publications Manager (202) 833-6951
Crystal Taylor Practice Groups Activities Coordinator
(202) 833-0763 [email protected]
Arnaud Gelb Practice Groups Distance Learning Coordinator
(202) 833-0761 [email protected]
Tazeen Dhanani Practice Groups Communications and
Publications Coordinator (202) 833-6940
Dominique Sawyer Practice Groups Distance Learning Assistant
(202) 833-0765 [email protected]
Matthew Ausloos Practice Groups Distance Learning Web Assistant
(202) 833-6952 [email protected]
Jasmine Santana Practice Groups Editorial Assistant
(202) 833-6955 [email protected]
Graphic Design StaffMary Boutsikaris Creative Director (202) 833-0764
Ana Tobin Graphic Designer/Coordinator
(202) 833-0781 [email protected]

In-House Counselor
6
Marching Forward with HIPAA Omnibus: Three Priorities for 2014Jan McDavid*HealthPort Technologies Alpharetta, GA
The Health Insurance Portability and Accountability Act (HIPAA) Omnibus Rule (Final Omnibus Rule), the long-awaited update to HIPAA, arrived to great fanfare in
early 2013.1 It is now in effect, and health care compliance teams worked to accommodate its stipulations.
Health care covered entities (CEs) and business associates (BAs) now await the initial waves of audits. The question you must ask is if 2013 preparations have effectively insu-lated organizations from fault and financial penalty; the
answer may be “no.” Legal counselors and compliance teams for all CEs and BAs must continue to manage and monitor several key issues as introduced by the Final Omnibus Rule. Counselors, in particular, must stay abreast of the following issues and avoid the complacency that may occur following successful compliance. Continued vigilance will save time, avoid unnecessary expense, and help your organization avoid financial penalty.
Adjusting Your Electronic Health RecordThe option for patients to withhold specific information from their electronic health record (EHR)2 is part of the Final Omnibus Rule and has been an area of great concern. Patients who pay for their care out of pocket can request that the information surrounding that visit not be shared with health plans or insurance carriers. It is imperative that providers prevent that data, regardless of the medical encounter, from flowing through the usual EHR, revenue cycle, and reporting channels.
It is the responsibility of the information technology (IT) departments, with the guidance of HIPAA specialists and legal oversight, to program the hospital’s EHRs to review all requests for restriction to identify, isolate, and flag the data in question. For example, if a patient undergoes a cardiac catheterization and pays for the procedure, that individual has the right to restrict that information from their health plan. Your EHR cannot allow that data to flow through unabated, including to physician practices and health information exchanges. According to new HIPAA rules, that would be considered a breach.
In certain situations one group might identify the data requested for restriction, but another group allows the information to flow through. Providers must design a system capable of flagging the data that are requested for restriction and prevent it from flowing to a payer. In the eyes of the U.S. Department of Health & Human Services (HHS), this is not a gray area.
Redefining “Breach”—New Factors to ConsiderSecondly, as we ease into 2014 it is imperative that providers firmly grasp the Omnibus Final Rule’s new definition of “harm” and all of its legal implications. That definition is the basis for how to analyze potential breaches of protected health information (PHI) and also is stated within the Final Omnibus Rule.
The new rule assesses harm that may or may not result from unauthorized use, access, or disclosure of PHI. The following four factors will help determine if a breach occurred. Moving forward, all workflows, policies, and procedures should include these factors in determining whether there is a “low probability of compromise” of the PHI:

7
• The nature and extent of the PHI involved, including the types of identifiers and the likelihood of re-identification;
• The unauthorized person who used the PHI or to whom the disclosure was made;
• Determination of whether the PHI was actually acquired or viewed, or whether there was an opportunity for the PHI to be acquired or viewed; and
• The extent to which the risk to the PHI has been mitigated.
Additionally, audit logs and other records of IT security measures should be reviewed to make certain they comply with HIPAA’s 18 items considered to be PHI.3 These records should document all acquired data and what was viewed. As an example, if a provider mails a patient’s lab results to an incor-rect address and the envelope is returned unopened, there is a presumption of no harm/compromise of the data. However, if the document is returned and has been opened, a higher level of risk must be assigned. Health information managers, IT, HIPAA specialists, and legal staff must cooperate to seamlessly review and assess facts, logs, and security records.
Another best practice to consider is to simply notify patients of every potential breach of their PHI. If there is any doubt about the occurrence of a breach, notify patients.
Document Compliance EffortsMake certain to carefully document Omnibus Final Rule compliance efforts. In the event of a breach, HHS has proven to be more lenient in situations where there was no evidence of willful neglect. Thorough documentation of your organi-zation’s mitigation efforts, from every level of your organiza-tion, shows respect for the security of PHI and that a breach was not due to neglect.
Legal departments can take a lead role in painting a vivid picture of HIPAA expectations for their organizations—as well as the ramifications of failing to address them.
*Jan McDavid is a seasoned attorney with more than 20 years of experience in corporate law. Jan has served as the Chief Compliance Officer and General Counsel for Health-Port since 1998, handling the company’s corporate litigation obligations and managing the regulatory compliance of the company’s business.
1. U.s. Dep’t Of Health & Human Servs., Press Release, “New rule pro-tects patient privacy, secures health information,” Jan. 17, 2013, available at www.hhs.gov/news/press/2013pres/01/20130117b.html.
2. 78 Fed. Reg. 5565 (Jan. 25, 2013), available at www.gpo.gov/fdsys/pkg/FR-2013-01-25/pdf/2013-01073.pdf.
3. U.s. Dep’t Of Health & Human Servs., Nat’l Insts. Of Health, “How can covered entities use and disclose protected health information for research and comply with the privacy rule?” available at http://priva-cyruleandresearch.nih.gov/pr_08.asp.
In-House Counselor
8
Clinically Integrated Networks and Contracts with Commercial Payers: The New FrontierGary W. Herschman*Diana M. FrattoSills Cummis & Gross PC Newark, NJ
John HarrisDGA Partners Bala Cynwyd, PA
National health care reform and intense competition are pressuring hospitals and health systems to improve quality while reducing the overall cost of care. These
improvements often require more-effective coordination with physicians and better arrangements with payers. Clinically integrated networks (CINs) can be a very effective vehicle for achieving these results.
This article provides insight into, and practical recommen-dations concerning, the structure and implementation of CINs, and includes an overview of legal, regulatory, and business issues. Importantly, CINs doing business strictly in the commercial arena do not have the same protections and waivers afforded to accountable care organizations (ACOs) participating in the Medicare Shared Savings Program (MSSP); thus, providers should carefully structure CINs consistent with the legal and regulatory insights described in this article.
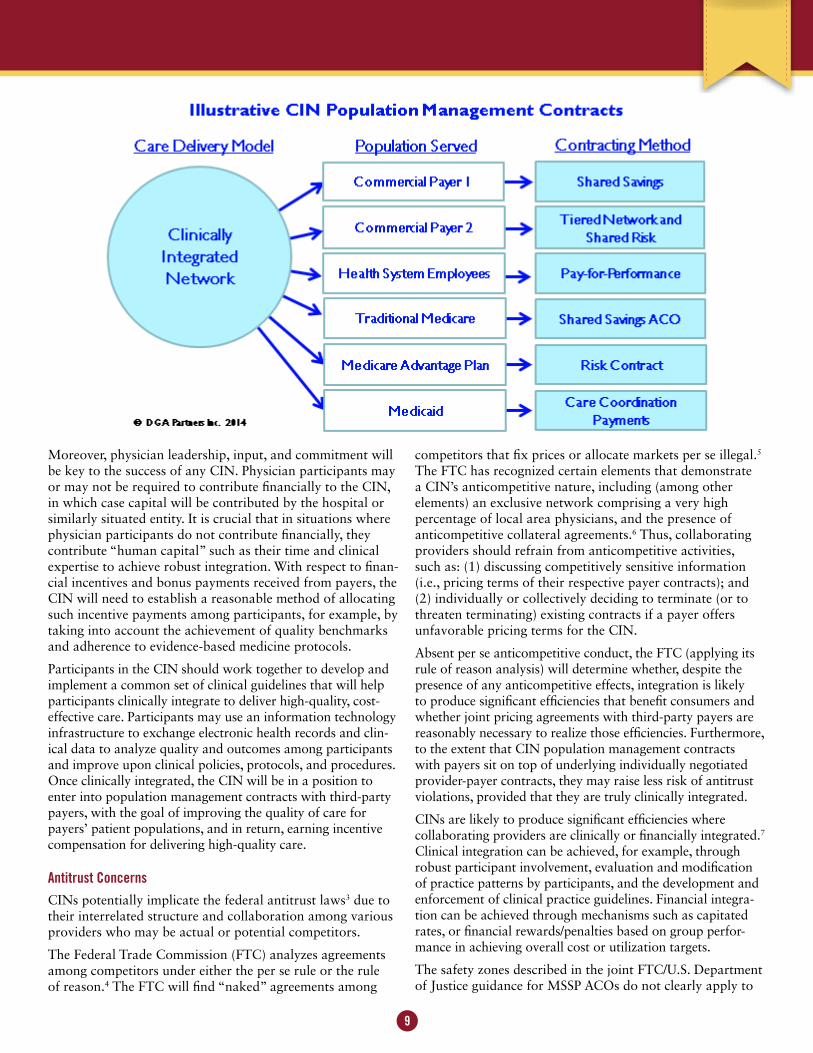
What Is a CIN?Through CINs, hospitals engage independent and hospital-employed physicians to improve the quality of patient care and reduce costs; they then contract with third-party payers to receive additional incentive compensation as a result of providing such high-quality, low-cost care.1 CINs are some-times referred to in the industry as “commercial ACOs.” The additional payments CINs receive from payers often are referred to as “value-based payments” as they reward providers for providing additional value (quality and cost savings) to health plans and consumers. CIN contracts with third-party payers are sometimes referred to as “population management contracts” and may involve value-based payments such as pay for performance, shared savings, shared risk, and tiered network arrangements. CIN contracts may be structured so that: (1) the providers’ underlying participation contracts with payers continue unaffected, and incentive-based contracts are added on top of those underlying contracts; and (2) as CINs become increasingly clinically integrated, direct contracts with payers may supersede existing provider contracts.
Since a CIN pursues both improvements in quality of care and payer arrangements that reward this success, it can be a useful vehicle to drive improvements the hospital/
health system views as strategically necessary. One of the advantages of CINs is that they seek to redesign the care delivery model on more of a “macro” basis for all patients before entering into population management contracts with payers, which simplifies physician administrative tasks. At the same time, the CIN can enter into several different types of payer arrangements, all of which will pursue quality and cost improvement (using the CIN’s policies, procedures, and protocols for care improvement), but which may have varying degrees of risk and reward. An illustration of patient populations and potential contracts is provided below.
It is worth noting that CIN population management contracts often improve results for patients who are less “tightly managed” than previous payer-provider arrange-ments. For example, shared savings or pay-for-performance arrangements with commercial preferred provider organi-zations can allow CINs to drive improvements in a much larger population, without being restricted to a health main-tenance organization population.2
CINs often focus on reducing utilization, especially of expen-sive services like avoidable hospital admissions. Though care improvements are positive for patients and typically support the hospital’s mission, decreased inpatient volume can be a concern for hospital chief financial officers. The hospital’s share of payer incentives often does not make up the differ-ence in lost short-term revenue. However, a successful CIN can be an attractive choice for patients and can provide more-coordinated care for patients, making them more likely to seek follow-up care at the same hospital rather than a competing hospital. In addition, if a CIN successfully manages overall costs of care, insurers may offer lower cost insurance to subscribers who choose a network focused on the CIN’s providers, or otherwise “steer” patients to CIN providers. This payer opportunity has become increasingly common as health plans search for cost-effective products to offer on public and private insurance exchanges or directly to employers.
Structure and Governance of CINsMost CINs are organized as separate legal entities (either limited liability companies or nonprofit organizations). While in past years physician-hospital organizations were typically set up as joint ventures, most CINs are now established as subsidiaries of hospitals or health systems.
The CIN should be governed by its participants, who may include hospitals, physicians, physician groups, and other health care entities. It is important to engage the participa-tion of a representative sample of participants in governance and leadership roles—including employed and independent physicians, primary care physicians, and specialty physi-cians, as well as members of the hospital entity and other participating entities, if any. A multi-class governing struc-ture is helpful in giving representation on the “board” to the various participants. Many important decisions will require the “buy-in” of different stakeholder types by, for example, a majority vote of each class of stakeholder.
9
Moreover, physician leadership, input, and commitment will be key to the success of any CIN. Physician participants may or may not be required to contribute financially to the CIN, in which case capital will be contributed by the hospital or similarly situated entity. It is crucial that in situations where physician participants do not contribute financially, they contribute “human capital” such as their time and clinical expertise to achieve robust integration. With respect to finan-cial incentives and bonus payments received from payers, the CIN will need to establish a reasonable method of allocating such incentive payments among participants, for example, by taking into account the achievement of quality benchmarks and adherence to evidence-based medicine protocols.
Participants in the CIN should work together to develop and implement a common set of clinical guidelines that will help participants clinically integrate to deliver high-quality, cost-effective care. Participants may use an information technology infrastructure to exchange electronic health records and clin-ical data to analyze quality and outcomes among participants and improve upon clinical policies, protocols, and procedures. Once clinically integrated, the CIN will be in a position to enter into population management contracts with third-party payers, with the goal of improving the quality of care for payers’ patient populations, and in return, earning incentive compensation for delivering high-quality care.
Antitrust ConcernsCINs potentially implicate the federal antitrust laws3 due to their interrelated structure and collaboration among various providers who may be actual or potential competitors.
The Federal Trade Commission (FTC) analyzes agreements among competitors under either the per se rule or the rule of reason.4 The FTC will find “naked” agreements among
competitors that fix prices or allocate markets per se illegal.5
The FTC has recognized certain elements that demonstrate a CIN’s anticompetitive nature, including (among other elements) an exclusive network comprising a very high percentage of local area physicians, and the presence of anticompetitive collateral agreements.6 Thus, collaborating providers should refrain from anticompetitive activities, such as: (1) discussing competitively sensitive information (i.e., pricing terms of their respective payer contracts); and (2) individually or collectively deciding to terminate (or to threaten terminating) existing contracts if a payer offers unfavorable pricing terms for the CIN.
Absent per se anticompetitive conduct, the FTC (applying its rule of reason analysis) will determine whether, despite the presence of any anticompetitive effects, integration is likely to produce significant efficiencies that benefit consumers and whether joint pricing agreements with third-party payers are reasonably necessary to realize those efficiencies. Furthermore, to the extent that CIN population management contracts with payers sit on top of underlying individually negotiated provider-payer contracts, they may raise less risk of antitrust violations, provided that they are truly clinically integrated.
CINs are likely to produce significant efficiencies where collaborating providers are clinically or financially integrated.7 Clinical integration can be achieved, for example, through robust participant involvement, evaluation and modification of practice patterns by participants, and the development and enforcement of clinical practice guidelines. Financial integra-tion can be achieved through mechanisms such as capitated rates, or financial rewards/penalties based on group perfor-mance in achieving overall cost or utilization targets.
The safety zones described in the joint FTC/U.S. Department of Justice guidance for MSSP ACOs do not clearly apply to

In-House Counselor
10
non-MSSP commercial arrangements with payers; however, CINs can be informed by such guidance. To be conservative: (1) participating providers of a “common service” should have a combined market share of less than 30% for each common service in each participant’s primary service area; (2) hospital or ambulatory surgery center participants should be non-exclusive, regardless of market share; and (3) partici-pants having greater than 50% of the market share in any primary service should be non-exclusive to the CIN, and the CIN, in its population management contracts, should not require commercial payers to be exclusive to the CIN.8
Internal Revenue Service IssuesCINs should be aware of certain Internal Revenue Service (IRS) issues regarding tax exemption. They need to deter-mine whether they should seek tax-exempt status, and if applicable, whether a participating provider’s tax-exempt status would be affected as a result of participation in a for-profit CIN. In the latter situation, federal case law and IRS guidance discussed below can help guide a participating tax-exempt entity.
First, the activities of a CIN must further the charitable purpose of a participating tax-exempt entity. If not, a tax-exempt entity’s status could be jeopardized if the CIN’s activ-ities represent more than an insubstantial part of the total activities of the tax-exempt entity. Guidance from the IRS suggests that less than 5% of revenue would be considered insubstantial, and between 5% and 15% of revenue would be riskier.9
Second, the CIN’s activities should be substantially related to the participating entity’s tax-exempt purpose. The IRS has expressed that many non-MSSP activities are not charitable activities, including negotiating with private health insurers on behalf of unrelated parties, regardless of whether the agreement negotiated involves a program aimed at achieving cost savings in health care delivery, because unlike MSSP activities, activities with commercial payers do not lessen the burden of government; however, improving the quality of health care to patients in the hospital’s service area may arguably still advance some of the participating entity’s stated tax-exempt purposes.10
Next, CINs must be certain that their revenues are not distrib-uted for the benefit of private individuals. Any benefit flowing to private parties should be incidental to an organization pursuing tax-exempt charitable purposes.11 IRS guidance for MSSP ACOs states that to protect against any impermissible private inurement or private benefit, a participating entity’s share of economic benefits (and share of losses) derived from the ACO should be proportional to the benefits or contribu-tions (including monetary and non-monetary contributions) the participating entity provides to the ACO.
Finally, a tax-exempt entity must retain control over deci-sions that could affect its tax-exempt status. “Control” may include retaining control over the governing body of the CIN, retaining the ability to exercise certain reserve powers
if the entity’s tax-exempt status is in jeopardy, or exercising control over the chief officer of the CIN.12
Health Care Regulatory ComplianceCIN participants should actively monitor and audit compli-ance with the health care laws and regulations described below.
The Anti-Kickback Statute and the Stark Law13
A CIN’s participants will be working together toward estab-lishing clinical integration, but nonetheless, they must ensure that their interdependence does not result in any payment or benefit in exchange for patient referrals. Participants should avoid threatening to cease or reduce patient referrals to physi-cians or entities that do not become members of the CIN, or otherwise conditioning referrals on participating in the CIN.
MSSP ACOs have the benefit of fraud and abuse waivers for activities that are “reasonably related to the purposes of the Shared Savings Program,” which include: (1) promoting accountability for a patient population; (2) coordinating items and services provided to Medicare Part A and Part B beneficiaries; and (3) encouraging investment in infra-structure and redesigned care processes for high-quality and efficient service delivery.14 The Centers for Medicare & Medicaid Services (CMS) has not expressly granted CINs the benefit of the MSSP waivers; however, in its Interim Final Rule regarding the MSSP ACO waivers, CMS explained that performance-based payments received from a commercial plan do not necessarily implicate the fraud and abuse laws.15
Civil Monetary Penalties Act16
The Civil Monetary Penalties Act (CMP Act) applies to Medicare and Medicaid beneficiaries. In working toward achieving cost savings, best practices suggest that partici-pating providers in CINs comply with the CMP Act, which requires, among other things, that: cost-containment measures do not result in any adverse impact on the quality of patient care; cost-savings measures are not applied in clinically inappropriate circumstances; providers do not stint on care to patients; providers do not “cherry-pick” healthier patients or patients who cost less to treat; and providers do not inappropriately accelerate patient discharges.
Health Insurance Portability and Accountability Act and Health Information Technology for Economic and Clinical Health Act17
CINs will likely aggregate and share electronic health records and data across participating providers. Thus, CINs must comply with the Health Insurance Portability and Account-ability Act and the Health Information Technology for Economic and Clinical Health Act, in addition to state privacy laws. CINs, acting as a business associate of each provider in the network, should execute business associate agreements with each provider. Furthermore, CINs should comply with the Electronic Health Records Items and Services Anti-Kick-back Statute safe harbor and Stark exception.18

11
State Law and Payer Contract IssuesCINs should be structured to comply with state fraud and abuse, insurance, and corporate practice of medicine laws and regulations, and state privacy laws, as applicable. For example, state insurance laws may require that CIN partici-pants providing certain services on behalf of a health plan obtain a license or certification from the state insurance agency. Moreover, state corporate practice of medicine laws may prohibit the CIN from controlling aspects of partici-pating physicians’ medical practices.
CINs must carefully structure their contracts with payers and ensure that such contracts clearly set forth certain key terms, such as: (1) the clinical benchmarks required to receive incen-tive payments and how such benchmarks will be measured (including sample calculations); (2) the patients covered under such contracts; (3) information technology, claims, and data-sharing requirements; (4) terms of payment; (5) audit and appeal rights; (6) communications with members; (7) any exclu-sivity provisions; and (8) termination rights and processes.
ConclusionCINs may represent the future of multi-provider collabora-tions, increasing accountability among physicians, organizing and coordinating care among providers, and developing clini-cally integrated policies, procedures, and protocols to provide high-quality services while reducing overall health care costs. In some markets CINs face competition for the participation of independent physicians. CINs of competing hospitals may be trying to attract them to a different CIN, and some physi-cian entities also may seek their allegiance. It is important that CINs are carefully structured to be attractive to physicians and functionally effective, while ensuring compliance with the legal and regulatory framework described above.
*Gary W. Herschman ([email protected]) is a member of Sills Cummis & Gross PC in Newark, NJ, and is chair of the firm’s Health Care Practice Group. He represents diverse health care clients, including hospitals, health care systems, long term care facilities, home health companies, and other health care facilities. He handles complex strategic transactions, joint ventures, acquisitions, affiliations, physician alignment strategies, and clinical integration. He advises clients on federal and state health care regulatory compliance issues, government investigations, and Stark audits of physician arrangements. Mr. Herschman also frequently writes articles and presents at seminars on health care compliance and trans-actions, serves on the Editorial Board of Compliance Today, and serves as a vice chair of the American Health Lawyers Association’s (AHLA’s) Fraud and Abuse Practice Group.
Diana M. Fratto ([email protected]) is an associate in the Health Care Practice Group at Sills Cummis & Gross PC in Newark, NJ. She actively represents a variety of health care providers in transactional and regulatory compliance matters, including hospitals, nursing homes, home care agen-cies, adult day care facilities, physician groups, and various
other health care facilities and businesses. She has been involved in strategic transactions, joint ventures, acquisi-tions, affiliations, and clinical integration. She is a member of AHLA’s Fraud and Abuse Practice Group.
John Harris ([email protected]) is a principal of DGA Partners, management consultants to the health care industry. His work on CINs includes facilitation, engaging physicians, reaching agreement on structure, launching the CIN, and supporting operations. DGA Partners also advises on a range of physician-hospital alignment strategies, provides valuations in support of these strategies, and assists with mergers and acquisitions. Mr. Harris has had articles published in major health care publications and frequently presents on new value-based payment models, health care strategy, finance, and physician alignment.
1 CINs are similar to physician hospital organizations (PHOs). In fact, some PHOs consider themselves to be CINs as well. The concept of CINs first surfaced in the 1990s, when the Federal Trade Commission (FTC) recognized “clinical integration” as a way for providers to collaborate without violating federal antitrust laws. Bearing substantial financial risk is the other way to collaborate. Most recently, in February 2013, the FTC issued a favorable advisory opinion for a Norman PHO in Oklahoma, which shows additional flexibility in the government’s approach toward health care delivery models that are consistent with health care reform.
2 Medicare Shared Savings Program ACOs are an example of one type of payer arrangement that can be pursued by a CIN and that serves a population that is not subject to typical health maintenance organization constraints.
3 The Sherman Act, 15 U.S.C. §§ 1-7 (2012); The Clayton Act, 15 U.S.C. §§ 12-27 (2012); The Federal Trade Commission Act, 15 U.S.C. §§ 41-58 (2012).
4 U.S. Dep’t of Justice & Fed. Trade Comm’n, Statements of Anti-trust Policy in Health Care, Statement 9: Enforcement Policy on Multiprovider Networks (1996).
5 Id.6 U.S. Dep’t of Justice & Fed. Trade Comm’n, Statements of Anti-
trust Policy in Health Care, Statement 8: Enforcement Policy on Physician Network Joint Ventures (1996).
7 Statement 9, supra note 4, and Statement 8, supra note 6.8 Federal Trade Commission and Antitrust Division of the U.S.
Department of Justice, Statement of Antitrust Enforcement Policy Regarding Accountable Care Organizations Participat-ing in the Medicare Shared Savings Program (Oct. 20, 2011).
9 IRS Notice 2011-20.10 Id. See also I.R.C. 501(c)(3) (2012) (Detailing a list of the different types
of tax-exempt purposes).11 Redlands Surgical Servs. v. Comm’r, 113 T.C. 47, 92-93 (1999), aff’d 242
F.3d 904 (9th Cir 2001).12 See Rev. Rul. 2004-51(Tax-exempt university retained control of the ac-
tivities of a joint venture with a for-profit entity by retaining control over its curriculum); See also St. David’s Health Care Sys. v. United States, 349 F.3d 232, 236-237 (5th Cir. 2003) (The nonprofit partner must not have “ceded control” of its activities to its for-profit joint venturer in order to retain its tax-exempt status).
13 31 U.S.C. § 3729 et seq. (2012); 42 U.S.C. § 1320a-7b(b) (2012); 42 U.S.C. § 1395nn (2012).
14 76 Fed. Reg. 68002 (Nov. 2, 2011).15 Id.16 42 U.S.C. § 1320a-7a (2012).17 Pub. L. No. 104-191; Pub. L. No. 111-5.18 42 C.F.R. § 1001.952(y); 42 C.F.R. § 411.357(w).
In-House Counselor
12
Chair’s ColumnCharles R. Whipple, JD, MHSAHallmark Health Melrose, MA
Welcome to the Spring issue of the In-House Counselor newsletter for the In-House Counsel Practice Group (In-House PG). We are excited to be able to bring you this edition and all of the other great benefits that membership in the In-House PG brings—from webinars to our popular salary survey.
We currently are in the process of implementing a leader-ship development program and hope that many of you want to get involved in the great activities of the PG. There are many ways to get involved in PG leadership, even if you only have a small amount of time to offer. You might want to consider one of the following opportunities:
• Write an article for the Fall issue of the newsletter, or help with a member briefing (ideas and deadlines can be tailored to your interests and schedule);
• Sign up to be an email alert author or editor;
• Provide an idea for a short tutorial;
• Provide an idea for webinars, or serve as a speaker or moderator on a webinar;
• Contribute documents for the MediTract database;
• Be active on the discussion list;
• Join the Children’s Hospital Affinity Group or Physician In-House Counsel Affinity Group; or
• Volunteer for one of the task forces that our Practice Group co-sponsors.
The In-House PG thanks you for being a member. We want to hear ideas from you and encourage you to serve the other members of our PG with any small contribution of time, legal information, or volunteer hours. It is through the volunteers that we identify the future leadership of the PG.
I look forward to working with many of you during the coming year and seeing you at various conferences, seminars, and colloquiums. Please feel free to contact me or any of the vice chairs if you would like to get more involved in your PG.
Sincerely,
Charles

13
The Sunshine Act: Shining Light on Impending ImplementationKatherine L. Kraschel*Foley & Lardner LLP Boston, MA
Brendan AbelOffice for Interactions with Industry Partners HealthCare Boston, MA
The Physician Payments Sunshine Act (Sunshine Act or Act) is a rarely cited component of the Affordable Care Act (ACA). The Sunshine Act increases the transparency of
payments and other transfers of value from manufacturers or group purchasing organizations (GPOs) of pharmaceuticals and medical devices to physicians and hospitals. With the first annual reporting deadline for manufacturers approaching on March 31, and the launch of a resulting public, searchable website, entitled Open Payments, listing details of payments to individual physicians slated for September, this provision of the law will attract the attention of affected parties such as manufacturers, physicians, and hospitals as well as third parties such as the media and health care consumers.
HistoryDisclosure of financial interests is not a new concept within the medical community. The Cleveland Clinic, for example, has required the posting of certain information regarding their physicians’ ties with industry on its website since 2007.1 Several states, including Massachusetts, Minne-sota, and Vermont, have passed legislation requiring public reporting of certain information about payments made to physicians.2 At least 13 pharmaceutical companies are now required to publicly post information about payments they make to physicians as conditions of corporate integrity agreements.3 Lastly, many industry and medical professional societies require disclosure of certain financial interests either publicly or in relevant situations (i.e., presentations, journal publications, advisory boards, etc.). Never before, though, have financial disclosure requirements come from the federal government to the biomedical community, and rarely have disclosure requirements, regardless of source, been as expan-sive as those contained in the Sunshine Act.
The Sunshine Act was sponsored by Senators Herb Kohl (D-WI) and Charles Grassley (R-IA). Grassley first piqued the interest of conflicts of interest in academic medicine through an inquiry into several Boston-based psychiatrists receiving large payments from industry in 2008. A previous stand-alone attempt by Kohl and Grassley to pass the Sunshine Act was blocked by Congress in 2007, but the
ACA provided the perfect avenue through which to pass the Sunshine Act—included among myriad components of the law added by individual legislators during the chaotic drafting and negotiating of the bill.
The resistance in the path towards passage was not surprising given the large number of financial relationships that poten-tially require disclosure and thus create an administrative burden for manufacturers and GPOs. In a large-scale survey in 2007 of more than 3,000 physicians across six specialties, 94% of physicians reported some type of relationship with industry, while 18% reported receiving compensation for consulting.4 A substantial portion of the biomedical commu-nity will be affected by the law, leading physicians, hospitals, and manufacturers to pay close attention to the regulations that operationalize the law as they have emerged.
The Centers for Medicare & Medicaid Services (CMS) issued proposed regulations in December 2011 and requested commentary from all interested parties.5 In February 2013 CMS issued final regulations that require reporting of payments or transfers of value from all pharmaceutical and medical device manufacturers and GPOs to physicians or teaching hospitals (covered recipients) occurring on or after August 1, 2013 for calendar year 2013.6 Reports for the shortened August-December 2013 calendar year must be submitted by manufacturers and GPOs electronically to CMS by March 31, 2014 and will be due on the 90th day of each year for the subsequent calendar year.
Types of Payments ReportedPayment or transfer of value is defined broadly with a low threshold of $10, and thus will include a vast array of funds transferred from covered recipients. However, reporting only applies to payment from entities that manufacture at least one covered product that includes any drug, device, biolog-ical, or medical supply covered under Medicare, Medicaid, or the Children’s Health Insurance Program.7
In addition to payments made directly from manufacturers, indirect payments or transfers of value must be reported. These indirect payments are defined as payments or transfers in which the manufacturer “requires, instructs, directs, or otherwise causes the third party” to pay or transfer value to a covered recipient. There is no knowledge requirement that triggers reporting of these third-party payments. If a manu-facturer is not aware of the identity of the covered recipient, a payment made by a third party will be imputed back to the manufacturer and must be reported.
Food and beverage values of $10 or more must be disclosed as well as values of less than $10 when the aggregate annual amount transferred to the covered recipient exceeds $100. In reporting food and beverage values, manufacturers must determine and report the value per person by dividing the entire cost of food and beverage by the number of indi-viduals who partake in a meal (including individuals who are

In-House Counselor
14
non-covered recipients). However, meals, snacks, soft drinks, or coffee that a manufacturer provides and are generally available to all participants at a large conference or similar events need not be reported.8
The breadth of the Sunshine Act is exemplified by the inclu-sion of “research” as a category of reportable payments. The regulations require disclosure of all transfers of value for research, from basic and applied research through product development (or, in other terms, preclinical through Phase IV research).9 Research-related payments are reportable whether made directly or indirectly to a covered recipient, and the research only needs to be subject to a written agree-ment or contract or a research protocol. Of note, the Open Payments website will treat research payments differently by listing them separately on the website, and by including additional information such as the name of the research study, the covered products subject to the study, and at the manufacturer’s option, the ClinicalTrials.gov identifier. These measures are taken to address concerns regarding the appearance of substantial payments to investigators who are performing sponsored research and to mitigate confusion that such research payments are akin to other reportable payments on the Open Payments website.
For sponsored research agreements, the entire sum of research support will be attributed as a payment to an individual physician who is the principal investigator, even though all or most of the money will be used to fund the research overhead, salaries for research staff, subcontracts to third parties, insti-tutional review board fees, etc.10 Many times, the researcher listed as receiving substantial support from a manufacturer will, in fact, receive no salary support or increase for such arrangements.11 The regulations contain a notable provision to offer market protection of certain research that is in develop-ment but has not yet reached regulatory approval: disclosure of such research payments can be delayed until the earlier of four years from the date of transfer or U.S. Food and Drug Administration (FDA) approval of the product to protect the companies’ proprietary interests.
Definition of ManufacturerUnder the Act, all pharmaceutical and device manufacturers and GPOs are required to register with CMS within 90 days of the end of the calendar year in which payments are to be reported.12 There are two categories of manufacturers as defined by the regulations. The first category includes entities engaged in the production, preparation, propaga-tion, compounding, or conversion of a covered product. It does not include distributors or wholesalers that do not hold title to any covered product or entities that produce covered product solely for use by or within the entity or by the entity’s own patients. Manufacturers that do not produce a covered product or do so only under a written agreement for another entity and do not hold FDA approval, license, or clearance are only required to report payments related to covered products. In addition, manufacturers whose total
gross revenues from covered products constitute less than 10% of its total gross revenue are not required to report payments that are related to covered products.
The second category of manufacturer includes entities under common ownership with a manufacturer as defined by the first category that provides assistance or support to the manufacturer with respect to production, preparation, prop-agation, compounding, conversion, marketing, promotion, sale, or distribution of a covered product. In issuing the Final Rule, CMS declined to increase the percentage ownership required to determine whether common ownership exists. Five percent ownership is sufficient to establish common ownership. Entities that are under common ownership may submit individual or consolidated reports.
Appeals ProcedureOnce manufacturers or GPOs report payments, a review and resolution period will begin at least 60 days before the information is made public to allow for a two-phase review and dispute resolution process to occur. Covered recipients may register with CMS to receive notification regarding the review process and are otherwise notified using an online posting and notification via CMS’ listservs. The notification will indicate when the 45-day review process begins.
Upon reviewing the information reported about the covered recipient, if the information is correct, the covered recipient may electronically certify the information reported is accurate. If the covered recipient disagrees with information reported, the covered recipient may initiate a dispute any time once the 45-day review process has begun and before the end of the calendar year. In order for any data to be corrected prior to publication on Open Payments, the applicable manufac-turer or GPO must notify CMS of any resolved dispute and changes to information submitted within 60 days of the beginning of the review period (15 days after the end of the covered recipient’s 45-day review period). Disputes that are not resolved within the allotted 60-day window may still be resolved, but data as submitted by the manufacturer or GPO will be published on Open Payments marked as disputed. If the dispute is ultimately resolved after the 60-day window, changes resulting from the dispute may not be changed until the next time the data is refreshed.
CMS plans to monitor the volume and terms of disputes and resolutions and to provide additional guidance to resolve situ-ations in which the cost of resolving a dispute may outweigh the benefits, resulting in uncontested, incorrect information.
PenaltiesA manufacturer’s or GPO’s failure to report is subject to a civil monetary penalty (CMP) of not less than $1,000 but not more than $10,000 for each payment or transfer of value not reported in a timely, accurate, or complete manner as required under the regulations. The aggregate CMP that can be imposed on each manufacturer or GPO in a given annual reporting period may not exceed $150,000. If a manu-

15
facturer or GPO knowingly fails to report, the maximum annual CMP is $1 million.13
Considerations as Reporting Deadline and Open Payments Site Launch ApproachWhile hospitals and physicians do not have an affirmative duty to report information under the Sunshine Act, one ques-tion they face is how proactive to be in accessing information reported by manufacturers and GPOs. By registering with CMS to receive notice of all their applicable payments and transfers and monitoring Open Payments regarding affiliated physi-cians, hospitals can prepare for and anticipate inquiries about reported payments to the hospital and its physicians and use the information as a cross-check for other reporting obligations.
The new source of information will give institutions with public health service funding a method to uncover possibly omitted “significant financial interests” that are required to be reported by certain researchers under the research conflict-of-interest regulations.14 General counsels’ offices also should confirm that the reportable payments do not uncover any unknown clinical trial research occurring at their institutions, as this would raise several compliance issues that should be addressed promptly. However, given the apples-and-oranges nature of the different reporting systems, comparing data may be difficult and time consuming. The cost-benefit ratio of dili-gently reviewing data will have to be determined by each insti-tution and may depend on the yet-to-be-seen interoperability of Open Payments data with established internal reporting and conflict-management data systems, particularly for large systems with many research clinicians.
From a public relations perspective, close cooperation and strategic planning with communications offices in the weeks leading up to the Open Payments launch are advis-able to prepare for responses to press and patient inquiries, particularly when there is a large amount of funding or compensation reported or a prominent researcher involved. In addition, hospitals privy to information prior to its release on Open Payments will be prepared to respond to requests for clarification about discrepancies of reported payments across disclosure sources. For example, a physi-cian in Massachusetts could have one set of disclosures listed on the Open Payments website, while only a portion of those payments are reported on a state repository because of conflicting inclusion criteria or date ranges. Meanwhile, a journal publication by the same physician could list yet other disclosures, such as expert witness compensation or equity in a basic science start-up, that are not contained on state or federal websites, or it could list substantially higher payment amounts because of aggregation over two or three years.
Finally, the food and beverage reporting requirement has created its own bevy of confusion and administra-tive burdens. Substantial ambiguity remains regarding the threshold of how many attendees it takes to constitute a “large conference” that does not require food-related reporting for buffet meals, and confusion about when there
are “identified” recipients, and to what extent manufacturers can require hospitals to track names of such recipients. At least, such issues should proactively be addressed while negotiating the written agreements, and at times, alternative sources of funding can be considered for food portions of relevant meetings or conferences.
*Katherine Kraschel is a health care associate at Foley & Lardner LLP and a Division of Medical Ethics fellow in the Department of Global Health and Social Medicine at Harvard Medical School.
Brendan Abel is a project specialist in the Office for Interac-tions with Industry at Partners HealthCare and a Division of Medical Ethics fellow in the Department of Global Health and Social Medicine at Harvard Medical School.
1 R. Steinbrook, Online Disclosure of Physician-Industry Relationships, 360 New Eng. J. Med. 325, 325 (2009).
2 American Med. Ass’n, State “Sunshine” Laws, available at www.ama-assn.org/resources/doc/washington/state-sunshine-laws-chart.pdf.
3 S. Agrawal, N. Brennan, and P. Budetti, The Sunshine Act—Effects on Physicians, 368 New Eng. J. Med. 2054, 2055 (2013).
4 Campbell EG, Gruen RL, Mountford J, Miller LG, Cleary PD, Blumen-thal D., A national survey of physician-industry relationships, New Eng. J. Med. 2007;356:1742-1750 (Of note, many of these “relation-ships” would not be subject to disclosure under the Sunshine Act: many relationships consisted of receiving food in the workplace that could be under the de minimis, and many reported receiving drugs samples, which is generally excluded in the law.).
5 76 Fed. Reg. 78742-78773 to be codified at 42 C.F.R. pts. 402 and 403.6 78 Fed. Reg. 9458 to be codified at 42 C.F.R. pts. 402, 403.7 CMS requires payments to be reported in one of 14 categories: charitable
contributions, consulting fees, compensation for non-consulting services, current or prospective ownership or investment interests, direct compen-sation for speaker or faculty for medical education programs, education, entertainment, food and beverages, gifts, grants, honoraria, research, royalty or licenses, or travel and lodging.
8 The law requires manufacturers to provide the names of the recipients of food, though CMS recently clarified that disclosure of specific recipients is not required when it would be difficult to identify who exactly con-sumed the food and beverage.
9 Research is defined as “a systematic investigation designed to develop or contribute to generalized knowledge relating to public health, includ-ing behavioral or social sciences research. This term encompasses basic and applied research and product development.” Centers for Medicare & Medicaid Services. Medicare, Medicaid, Children’s Health Insurance Programs: transparency reports and reporting of physician ownership or investment interests.
10 See Gary Shangold and Michael Koren, Impact of the Sunshine Law ‘Open Payment’ Provision on Clinical Research, 12 MRLR 828 (2013).
11 Id.12 As of the date of submission, CMS has not yet opened registration for
manufacturers and has changed the date of registration opening from January 1, 2013 to “early 2014.”
13 Factors used in determining the amount of CMP imposed include: the length of time the manufacturer or GPO failed to report, including the amount of time the manufacturer or GPO knew of the payments or transfer of value that should be reported; the amount of payment the manufacturer or GPO failed to report; the level of culpability of the manufacturer or GPO; the nature and amount of information reported in error; and the degree of diligence exercised in correcting information reported in error.
14 42 C.F.R. pt. 50, subpt. F; 42 C.F.R. pt. 94.
In-House Counselor
16
Unique Factors Impact Fair Market Value Determinations for Children’s Hospitals and Pediatric ProvidersTom SchnackSeim Johnson LLP Omaha, NE
Editor Cori Casey Turner Husch Blackwell LLP Kansas City, MO
The Children’s Hospital Affinity Group (CHAG) is designed for those members of the In-House Counsel and Teaching Hospitals and Academic Medical Centers
Practice Groups who work with or for a health care institu-tion dedicated to children’s health care needs. CHAG explores medico-legal issues that are unique to providing health care to children such as consent, Children’s Health Insurance Programs, Medicaid, and other government program funding, guardianship, and state protective services agencies. Addi-tionally, CHAG covers issues impacting children’s academic medical centers including research and graduate medical education matters.
Several factors distinguish the evaluation of fair market value (FMV) for compensation arrangements involving children’s hospitals and pediatric providers from the typical FMV value analysis. Smaller numbers of pediatric subspecialists result in fewer compensation survey responses and influence the quality and interpretation of the survey data. Additionally, smaller numbers mean a lack of pediatric subspecialists in certain markets impacting FMV in some communities.
Lack of supply also requires pediatric subspecialists to assume multiple roles within a provider or even among several providers. It is not unusual for children’s hospitals to contract with a provider for a fixed number of hours per week or for a specific element of care or patient population. Many times these arrangements also include other duties such as adminis-trative responsibilities and call. These “parts and pieces” types of arrangements tend to be more complex and evolving as the parties negotiate the services to be provided to address the changing needs of the pediatric population.
Limited Supply of Pediatric SubspecialistsThere are about 24,000 pediatric subspecialists and more than 105,000 general pediatricians1 in the United States. The U.S. Census Bureau reports about 74 million children under the age of 18.2 There is a marked connection between access to pediatric subspecialty care for children who have complex, severe, acute, or chronic conditions and better outcomes.3 When compared to care given by general (adult)
specialists, studies demonstrate care provided by pediatric subspecialists reduces the length of hospital stays, number of readmissions and complications, and decreases medical costs.4 According to the American Academy of Pediatrics,5 when a community lacks pediatric subspecialties:
• Care may be provided by adult medicine subspecialists who lack training in pediatric care;
• Care for children who have complex illnesses may be provided by general pediatricians;
• Families must travel to a distant center for care; and
• Families may need to locate to another community.
As cost and quality become even more important, demand for pediatric subspecialist services is likely to increase, and the valuation hurdles associated with establishing these relation-ships in a compliant manner may become more prevalent.
Evaluating Survey DataIn evaluating compensation survey data, it is important to consider the survey response rate and the number of enti-ties reporting. The most-recent Medical Group Manage-ment Association (MGMA) Physician and Compensation and Production Survey (MGMA Survey), one of the most frequently cited compensation surveys, reported about 1,500 responses in the pediatric subspecialties out of 60,000 overall responses.6 Pediatric response rates by specialty
17
ranged from a low of 13 respondents (pediatrics: radiology and pediatric: genetics) to a high of 156 respondents (pedi-atrics: neonatology).7 For comparison purposes, pediatric anesthesiology had 91 respondents while anesthesiology had 2,660 respondents.8 In evaluating the use of survey data to determine FMV, low response rate is one of the first items to consider. Similar to any sampling, higher sample size (responses) indicates higher confidence in the result.
Valuation consultants utilize several ways to increase the number of available responses. One way is to utilize multiple surveys in the evaluation of FMV. The Stark Phase II Interim Final Rule9 provided a list of sources for survey data, including: Sullivan Cotter and Associates Inc.—Physician Compensation and Productivity Survey; Hay Group—Physicians Compen-sation Survey; Hospital and Healthcare Compensation Services—Physician Salary Survey Report; MGMA—Physician Compensation and Productivity Survey; ECS Watson Wyatt—Hospital and Health Care Management Compensation Report; and William M. Mercer—Integrated Health Networks Compensation Survey. Unfortunately, while the list was current in 2004, some surveys listed are no longer available.
Moreover, there are other prominent surveys not listed in the Stark Phase II Interim Final Rule. The American Medical Group Association produces an annual compensation survey, which is available for purchase, with a large response rate. There also are other restricted sources of survey data available, including association surveys and proprietary
subscription databases. For example, the Association of Administrators in Academic Pediatrics (AAAP) conducts an annual survey (Faculty Salary and Productivity Survey) that is utilized by many pediatric providers. However, the survey results are only available to AAAP’s provider members and are not generally available to third parties or consultants.
While pediatric-specific restricted surveys can provide a good snapshot of market compensation, the use of restricted surveys presents challenges. Survey data that can be accessed by a variety of users is typically considered more impartial because responses for restricted sources tend to be low and the responses may be limited to a select demographic. Addi-tionally, the data can be tainted by a large provider reporting results. If a large provider both reports and uses a low response survey, they may actually be benchmarking against themselves. These factors should be considered before relying solely on data presented in a restricted survey.
To ensure an adequate number of survey responses and impartial results, some accounting and consulting firms utilize multiple surveys in each valuation, ensuring that each survey’s respondents target a different demographic; thus, providing a broader representation of reporting providers. In determining which surveys to use, it is important to align the survey with the type of services to be provided. If evaluating compensation for clinical services, FMV should be based on surveys where the respondents provide clinical services, like the MGMA Survey. If evaluating compensation for administrative duties, a survey like Sullivan Cotter, which reports compensation for administrative positions, should be considered.
Another method to increase the number of available responses is to utilize historical surveys. In business valua-tions, it is common to look back several years to evaluate past results. This same standard can be applied to compensa-tion arrangements by using several years’ survey results in the evaluation. This method not only provides additional responses, but also normalizes fluctuations between years that are more prominent when response rates are low in the pediatric subspecialties.
Once the surveys have been selected, care must be taken to ensure that the survey responses are a valid basis for supporting a FMV conclusion. Low response rates in pediatric subspecialties are typical. However, the number of respondents is not the only determinant for validity. It is important to consider the number of entities reporting as well. As the number of entities reporting increases, the validity of the survey increases because the results come from many different sources. For example, a survey with 52 responses from 23 entities will yield better data than 52 responses from six entities.
Survey responses across the various percentiles also should be tested to better understand and evaluate the survey results. One way to test the percentiles is to review the standard deviation as a percentage of the mean. A higher percentage indicates the data is spread out over a large range

In-House Counselor
18
of values meaning more variation or less reliable. A lower percentage indicates the survey results are more-closely clus-tered around the mean and less variation or more reliable. Another test is to compare mean to median. Similar amounts indicate a more-symmetric distribution that increases reli-ability, while dissimilar amounts indicate an asymmetric distribution with more outlier responses. If the mean signifi-cantly exceeds the median, there is more disparity and less reliability on the responses in the upper end of the range. This evaluation of survey results is more important among pediatric subspecialties as the adult or general subspecialties have many more physicians reporting in greater numbers, raising confidence in those results.
If a review of the available survey information results in a low number of aggregate responses for the relevant pediatric subspecialty, an alternative source of survey data is the adult or general subspecialty category. Adult subspecialists provide services to pediatric patients. Consistency in the determi-nation of survey category among surveys is important to reduce the likelihood of mixing pediatric provider data and adult provider data. However, all surveys do not necessarily examine all of the same specialties. Subjective judgment is required to determine the proper specialties for each survey. This problem is more prevalent in pediatric valuations due to the lower number of pediatric specialists. Fewer providers in each pediatric specialty or subspecialty mean fewer responses that are then aggregated and mapped to more-general special-ties. For example, the survey data for a pediatric hand surgeon may be embedded in the pediatric orthopedic surgery data that does not appropriately represent the complexity and acuity associated with hand surgery. Accordingly, care must be taken to properly match the duties performed by pediatric subspecialists to the most appropriate survey specialty and to acknowledge and account for differences between the survey specialty and a physician’s actual specialty.
Fair Market ValueDue to the low number of pediatric subspecialists, there can be variation in FMV based on an individual community and its needs. While some surveys report compensation by region, it is difficult to draw any conclusions. Also, the low number of pediatric subspecialists reporting means there are few pediatric subspecialty survey results by region.
Generally, physician salaries are driven by a national market. However, supply and demand is determined at the community level. There are communities that cannot meet their physician needs using FMV derived from survey data. Ultimately FMV is determined based on “facts and circumstances.” The appro-priate method of determining FMV will depend on the nature of the transaction, its location, and other factors.
A good place to start is to consider the following: is this a new subspecialty not previously recruited? If adding to an existing pediatric subspecialty, how does the expected compensation compare to existing compensation? What is causing the need for higher compensation? Is it specialty
specific or a general recruiting issue for all pediatric special-ties that is perhaps related to the provider or community?
Due to the shortage of pediatric subspecialties, there is often an imbalance between demand and supply. Studies have shown that patients have to travel much greater distances for access to pediatric subspecialties than for adult or general subspecialties. According to a study by Mayer,10 about 98% of adults have access to a general surgeon within 20 miles. Only 63% of children have access to a pediatric surgeon within 20 miles. More than 42% of pediatric patients would have to travel greater than 40 miles to access a pediatric neurosurgeon while only 6% of adults travel this distance for a neurosurgeon. Studies have concluded that while practice locations of pediatric subspecialists parallel the geographic distribution of children in the United States, many hospital referral regions lack pediatric subspecialists suggesting an inequitable distribution.11
General principles used in business valuations also are relevant to determining FMV in compensation arrange-ments. One such principle is called the “Principle of Alterna-tives.”12 It states that each party always has an alternative to completing the arrangement. It serves as a reminder that the arrangement does not need to be completed. The second is called the “Principle of Substitution.”13 It means that the value of something tends to be the price paid for an equally desirable substitution.

19
These principles may be used to support alternative or unique applications of survey data in certain geographic markets. For example, when applying the Principle of Substi-tution, one would evaluate whether there are other viable alternatives to the proposed pediatric subspecialist. Alterna-tives may include contracting for the services from another provider, using locum tenens physicians, securing telemedi-cine services, engaging an alternative background physi-cian like an adult subspecialist, or even referring patients to another provider outside the community. One must consider which of the alternatives would provide the necessary quality of care. The cost of each alternative also is important to consider. If under the Principle of Substitution these alterna-tives would be delivered at a higher cost, then FMV also may support a higher compensation range.
Multiple Role ArrangementsDue to a more-limited demand for pediatric subspecialty services, it is common for children’s hospitals and pediatric providers to contract for services that require less than a full-time clinical physician. Children’s hospitals or other providers may need a pediatric subspecialty but not have enough demand for a full-time clinical position.
The limited supply and demand means these arrangements require the physicians to assume multiple responsibilities requiring an evaluation of multiple compensation compo-nents. Each contract is individualized with common duties
that may include clinical services, medical directorship, administration, teaching, and on-call services. Multiple component arrangements should be carefully evaluated. A key aspect of the valuation is to develop an understanding of how each component relates to the others and how each component will be delivered.
It also is important to avoid “double dipping” when FMV compensation is determined for individual components that are delivered at the same time. For example, if an arrangement includes a half-day clinic and medical director duties, will the medical director duties be delivered outside the half-day clinic? If the arrangement provides for fixed clinic hours, what happens if the clinic is not fully scheduled for the fixed clinic hours? Will the physician be allowed to leave or provide other duties? These questions tend to be more relevant to pediatric valuations given the frequency of part-time or multiple-component service arrangements in the pediatric context.
ConclusionLack of survey information and increased demand for pedi-atric subspecialty services require a different approach to assessing FMV. It is important to review the underlying survey data and make sure it supports any FMV conclusions. Consider alternative sources of delivering comparable quality services and what impact these sources have on FMV. Addi-tionally, the nature of the part-time and multiple-component agreements typical with children’s hospitals and pediatric providers require a thorough understanding to document the arrangement and verify that the FMV assessment matches the arrangement and appropriately values the services provided.
1 The Am. Bd. of Pediatrics, Workforce Data 2012-2013, available at www.abp.org/abpwebsite/stats/wrkfrc/workforcebook.pdf.
2 U.S. Census Bureau, Age and Sex Composition in the United States: 2012, Table 1 Population by Age and Sex: 2012, (2012), available at www.census.gov/population/age/data/files/2012/2012gender_table1.xlsx.
3 Brent Snow. Does Surgical Subspecialty Care Come with a Higher Price? Current Opinion in Pediatrics (June 2005): 407-408.
4 Daphna Gans, Molly Battistelli, Mark Ramirez, Livier Cabezas, and Nadareh Pourat. Assuring Children’s Access to Pediatric Subspecialty Care in California, UCLA Center for Health Policy Research Policy Note (2013).
5 Mary Ellen Rimsza, Pediatric Workforce Shortage: Policy and Advocacy Challenges, for the Am. Academy of Pediatrics, available at www.aap.org/en-us/about-the-aap/departments-and-divisions/department-of-education/Documents/PedSubspecialtyWkfcPolicyAd.ppt.
6 Medical Grp. Mgmt. Ass’n, Physician and Compensation and Produc-tion Survey: 2013 Report Based on 2012 Data (2013).
7 Id.8 Id.9 Medicare Program; Physicians’ Referrals to Health Care Entities with
Which They Have Financial Relationships (Phase II), Interim Final Rule, 69 Fed. Reg. 16128 (Mar. 26, 2004).
10 Michelle Mayer, Heather Beil, and Daniel von Allmen. Distance to care and relative supply among pediatric surgical subspecialties, J. of Pediat-ric Surgery 483-495 (Mar. 2009).
11 Michelle Mayer, Are we there yet? Distance to care and relative supply among pediatric subspecialties, Pediatrics 2313-2321 (Dec. 2006).
12 Raymond C. Miles, Basic Business Appraisal (1984).13 Id.
Order Today! Enterprise Risk Management Handbook for Healthcare EntitiesCall toll-free 800.533.1637 Online at www.healthlawyers.org/bookstore
AHLA is pleased to announce the publication of the Second Edition of Enterprise Risk Management Handbook for Healthcare Entities, published in conjunction with ASHRM. This new edition addresses the need for and implementation of a comprehensive risk management process and plan that encompasses the entire enterprise and crosses departmental barriers. The coverage begins with an overview of enterprise risk management (ERM) and its evolution, including a discussion of the Sarbanes-Oxley Act of 2002. The authors provide guidance on structuring an ERM system, as well as insight on risk financing methods. They delineate how organiza-tions can manage risk in various settings, including contract management, claims management, environmental compliance, human research, peer review and credentialing, due diligence in business transactions, consent to treatment, and numerous others. The publication also includes insight on the impact that electronic health record systems, combined with the advent of e-discovery rules, will have on traditional documentation issues.
1620 Eye Street, NW 6th Floor Washington, DC 20006-4010
Health Care Liability & Litigation