Embed Size (px)
Citation preview

healthAnnual Conference Issue
Behavioral Health Integration Demands a Multifaceted Approach, p.28
Volume 10 • No. 2 Summer 2016
Amitabh Chandra, PhD: The Healthcare Trilemma, p.12
A Medical Group’s Managed Care Journey, p.32

Quest Diagnostics is the largest laboratory service provider in the world, which affords us the opportunity to gather large-scale health data and extract meaningful insights. Leveraging this rich collection of data, we offer you a suite of data analytics solutions designed to deliver important insights and illuminate answers to better inform your decisions and help optimize your bottom line.
Visit us at booth #XXX Learn more today at QuestForHealthSystems.com
© 2016 Quest Diagnostics Incorporated. All rights reserved.
The information you need, when you need it, to support your healthcare decisions
BOOTH #311

Driving Readmissions Down Just Got More Do-able
Include VITAS® Healthcare in your care transition model.
A referral to VITAS expands your alternatives for transitioning fragile and at-risk patients.
• Patient-centered services wherever the patient resides
• 24/7 patient support with Telecare®
• Continuous care at home and inpatient hospice care when medically necessary
• Smooth transition to alternative levels of care of hospice-appropriate patients whose DRG days have expired
Partnering with an experienced hospice and palliative care provider is critical to your success as an ACO. By relying on VITAS, you benefit from our evidence-based care protocols, transition processes and ancillary resources.
800.93.VITAS • VITAS.com

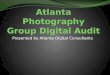
The numbers may surprise you, but the most important number of all is one. It’s our commitment to caring
for our community one patient at a time. From our top ranked hospitals to our vibrant and growing primary
care network, UCLA is world-renowned but focused right here at home. It’s a commitment we can all count on.
1-800-UCLA-MD1 (1-800-825-2631) uclahealth.org uclahealth.org/getsocial
150
1,200Over community offices
physicians
40Over primary care offices
Patients enter our community offi ces
2.5 million times each year
Over 30years of
managed care experienceThe Impact of
map notto scale
N
210
405
110710
105
605
10
10
5
5
405
2
101
170
118
101
134
90
60
91
23
Westwood
Century City
West Los Angeles
Torrance
Simi Valley
Malibu
ThousandOaks
Brentwood
PacificPalisades
PorterRanch
Northridge Panorama City
Pasadena
Arcadia
Alhambra
Santa Monica
Marina del Rey
ManhattanBeach
RedondoBeach
WestlakeVillage
Santa Clarita
IrvinePalos Verdes
Fountain Valley
Burbank

The numbers may surprise you, but the most important number of all is one. It’s our commitment to caring
for our community one patient at a time. From our top ranked hospitals to our vibrant and growing primary
care network, UCLA is world-renowned but focused right here at home. It’s a commitment we can all count on.
1-800-UCLA-MD1 (1-800-825-2631) uclahealth.org uclahealth.org/getsocial
150
1,200Over community offices
physicians
40Over primary care offices
Patients enter our community offi ces
2.5 million times each year
Over 30years of
managed care experienceThe Impact of
map notto scale
N
210
405
110710
105
605
10
10
5
5
405
2
101
170
118
101
134
90
60
91
23
Westwood
Century City
West Los Angeles
Torrance
Simi Valley
Malibu
ThousandOaks
Brentwood
PacificPalisades
PorterRanch
Northridge Panorama City
Pasadena
Arcadia
Alhambra
Santa Monica
Marina del Rey
ManhattanBeach
RedondoBeach
WestlakeVillage
Santa Clarita
IrvinePalos Verdes
Fountain Valley
Burbank

tab
le o
f c
on
ten
ts ON the COVer 12amitabh chandra, PhD the Healthcare trilemma: access, Quality, and cost
DepartmeNtS
7Notes from the president
8Names in the News
10Upcoming events
14 policy Briefing: hands-On or hands-Off:
Balancing monitoring and Oversight
at the State level
18Work-life Balance
20Federal Update: advancing risk-Based
Coordinated Care through Federal
advocacy
24CapG member list
32CapG member Spotlight:
austin regional Clinic’s
managed Care Journey
FeatUreS
26Using mobile technology to reduce
hospital readmissions
28Behavioral health Integration Demands
multifaceted approach
30Colon Cancer Screening: home testing
Increases patient activation
34pharmacists on the Interdisciplinary
Care team
36Improving medication adherence and
patient health Using the appointment–
Based model
38primary Care at a Crossroads
healthPublisherValerie Okunami
Editor-in-ChiefDon Crane
Editorial Advisory Board Lura Hawkins, MBA Amy Nguyen Howell, MD, MBA Mary Kay Payne, Arch Health Partners
Managing EditorDaryn Kobata
Editorial AssistantNelson Maldonado
Contributing WritersJanet Appel, RN, MSNKhuram Arif, MDBill BarcellonaAmitabh Chandra, PhDNorman Chenven, MDDon CraneRenee Debose, MDCorey EdwardsRussell D. Foster Amy Nguyen Howell, MD, MBADon Hufford, MDNeil Korsen, MDMara McDermottMarc MertzBellamay MontesaSheila A. Stephens
CAPG Health Magazine is published byValerie Okunami MediaPO Box 674, Sloughhouse, CA 95683Phone 916.761.1853
capghealth.comPlease send press releases and editorial inquiries to [email protected] or c/o CAPG Health, 915 Wilshire Blvd., Suite 1620, Los Angeles, CA 90017
For advertising, please send email to [email protected]
Subscription rates: $32 per year; $58 two years; $3 single copy.
Advertising rates on request. Bulk third class mail paid in Jefferson City, MOEvery precaution is taken to ensure the accuracy of the articles published inCAPG Health Magazine.
Opinions expressed or facts supplied by its authors are not the responsibility ofCAPG Health Magazine.
© 2015, CAPG Health Magazine.All rights reserved.
Reproduction in whole or in part without written permission is strictly prohibited.
6 l capg health Summer 2016

Your care is the center of all we doExcellent service. Every patient. Every time.
• Privately owned, primary care physician group
• Hospitalist program including nurse case managers for continuity and transition of care
• Behavioral Health, Cardiology, Endocrinology, Gastroenterology, and Neurology
• Diabetes and Nutrition Center
• Integrated, relationship-based approach to patient care for 22 years
Meet your care team at nwphysicians.com
17 Denver metro area locations | (303) 763-4900
Tom Jeffers, MD, Ruth Benton, CEO, Ken Cohen, MD, FACP,Nicole Dorotik, MD, Mark Pattridge, MD
At New West, we don’t just treat illnesses —
we help people.
Our coordinated and comprehensive
approach is designed
to partner with each person
to enhance physical, mental
and spiritual health.
CapG members and Friends:
Welcome to the 2016 Conference Issue of CAPG Health. this special edition highlights several of the topics to be covered at the CapG annual Conference 2016, with articles contributed by Conference speakers. I hope they’ll inspire and engage you.
providing educational opportunities, such as our annual Conference and the upcoming CapG Colloquium, September 28-30, has always been one of CapG’s priorities. But today, more than ever, I believe we’ve entered a critical new era of learning. With our healthcare system undergoing transformation at lightning speed, everyone in the sector must stay up to date on clinical and technology advances, policy and regulatory issues, payment models, and more. In particular, with implementation of the medicare access and ChIp reauthorization act (maCra) slated to begin January 2017, CapG has been hearing increasing requests for assistance and resources on how to move into alternative payment models (apms).
In light of this need, we recently launched two new initiatives. the CapG educational Series 2016 is a yearlong program on the fundamentals of risk-based payment models. the series comprises two one-day symposia and four quarterly webinars, with each session focusing on specific aspects of taking risk. to date, our first webinar and symposium have been great successes, and future events will cover topics including improving patient satisfaction, utilization resource management, performance measurement, and more. See our upcoming events at capg.org/riskessentials.
the second initiative, CapG Consulting, is a natural outgrowth of the vast wealth of knowledge represented by our membership. CapG physician groups and Ipas range from those just starting in risk to renowned organizations that have thrived in capitation for decades. We’re fortunate to know a number of highly experienced, recently retired CeOs eager to share what they’ve learned to help others succeed. You can learn more about our consultants at capg.org/consulting or by contacting Nelson maldonado (213.239.5041 or [email protected]).
as your association, it’s our responsibility to keep you ahead of the curve with knowledge and learning opportunities. I hope you’ll find these resources valuable. o
From the presidenta meSSaGe FrOm DONalD CraNe, preSIDeNt aND CeO, CapG
Donald Crane, CAPG President and CEO
Summer 2016 capg health l 7

WelCOme tO NeW CapG memBerS
CapG warmly welcomes our newest members who have joined us in 2016:
Organizational Membersel paso Integral Care, Ipa, el paso, tXGuthrie medical Group, pC, Sayre, pahorizon medical Group, pC, Goshen, NYmemorial hermann physician Network, houston, tXmercy health physicians, Cincinnati, OhSynergy healthCare, llC, Nashville, tN
Affiliate Membersable health, San Francisco, CaaSpIra laBS, austin, tXaxene health partners, murrieta, CamyWoundDoctor, Inc., Nashville, tN
Partners in Care Foundation’s June Simmons congratulates CAPG President and CEO Don Crane, recipient of the 2016 Mathies Award for Vision and Excellence in Healthcare Leadership. The award was presented at Partners’ 17th Annual Tribute Dinner on May 9 in Los Angeles.
Dr. rICharD merkIN eStaBlISheS FUND FOr CItY OF hOpe prOFeSSOrShIpS
Dr. richard merkin, president and CeO of heritage provider Network, has made a commitment to City of hope to establish two endowed professorships: the heritage provider Network professor of Immunology and the heritage provider Network professor of Gene therapy. City of hope is a National Cancer Institute–designated Comprehensive Cancer Center based in Duarte, California. “this generous gift will enable City of hope to advance promising clinical research programs in immunology and gene therapy,” said robert W. Stone, the center’s president and CeO.
Names in the Newsthe gene therapy professorship will be directed by Stephen J. Forman, mD, leader of City of hope’s hematologic malignancies and Stem Cell transplantation Institute. Yuman Fong, mD, chair and professor of the Department of Surgery and professor of the Department of experimental therapeutics, will direct the immunology professorship. Both will work in consultation with Steven t. rosen, mD, provost and chief scientific officer and director of the organization’s comprehensive cancer center and Beckman research Institute.
heNrY lOUBet NameD CeO OF palaDIN healthCare allIaNCe
los angeles–based paladin healthcare recently named henry loubet as Chief executive Officer of its new division, paladin healthcare alliance. loubet is a nationally recognized industry leader who was named as one of California’s
top 100 healthcare executives. at paladin, he will lead development of a comprehensive risk-based managed care platform, an affiliated physician alignment strategy, and a community-based integrated healthcare delivery system to expand access to quality care in underrepresented and disadvantaged communities. loubet’s experience includes serving as CeO of Unitedhealthcare’s Western region and as president of health Net/Foundation health.
HeriTage PrinciPal invesTigaTOr aT calTecH rePOrTs BreakTHrOugH Finding
a team led by andré hoelz, assistant professor of biochemistry and a heritage principal Investigator at the California Institute of technology (Caltech), reports in the april 15, 2016 issue of Science the successful mapping of the structure of the symmetric core of the nuclear pore complex (NpC). the NpC is a cellular gatekeeper that determines what molecules can enter and exit the cell’s nucleus, where genetic information is stored. the finding may lead to new classes of medicine that could treat diseases associated with NpC dysfunction. Dr. hoelz is one of nine inaugural heritage principal Investigators of the heritage medical research Institute for the advancement of medicine and Science, which supports translational sciences and health technology at Caltech through a commitment from heritage medical research Institute (hmrI). Dr. richard N. merkin, president and CeO of heritage provider Network, founded the nonprofit hmrI in 2003 and has been a Caltech trustee since 2007. o
8 l capg health Summer 2016

HEALED

up
co
mi
ng
e
ve
nt
scaPG annual conference 2016thursday to Sunday, June 16-19manchester Grand hyatt, San Diego
caPG colloQuium 2016Wednesday to Friday, September 28-30hyatt regency on Capitol hill, Washington, DC
caPG national meetinGthursday, June 16CapG annual Conference, San Diego Webinar: current state of affairs at cms: tHe neW innovation centerthursday, June 30Webex
Public Policy committee conference callthursday, July 14
meDicare alternative Payment moDel (aPm) committeetuesday, July 19Webex
contracts committeethursday, July 21CapG
coloraDo reGional meetinGthursday, august 11Denver, tBD
Public Policy committee conference callsthursday, august 11
Primary care Practice transformation collaborative Wednesday, august 17CapG
PHarmaceutical care committeeWednesday, august 24 CapG
Public relations/ marketinG committee tuesday, September 6Webex
inlanD emPire reGional meetinGs 9/6/2016tuesday, September 6riverside, mission Inn
san DieGo reGional meetinGsWednesday, September 7San Diego, tBD
Public Policy committee conference callsthursday, September 8
state Government ProGrams committeetuesday, September 13Sacramento, tBD
Webinar: HoW to imProve Patient satisfactiontuesday, September 20Webex
General membersHiP - soutHern californiaWednesday, September 21CapG
Human resources committeeWednesday, September 21CapG
General membersHiP - nortHern californiathursday, September 22Oakland, hilton Oakland airport hotel
caPG national meetinGWednesday, September 28CapG Colloquium, Washington, DC
clinical Quality leaDersHiP committeetuesday, October 11CapG
10 l capg health Summer 2016

Summer 2016 capg health l 11
nortHWest reGional meetinGsthursday, October 13Seattle, tBD
Public Policy committee conference callsthursday, October 13
nortHeast reGional meetinGstuesday, October 18philadelphia, tBD
soutHeast reGional meetinGthursday, October 20Orlando, tBD
contracts committeethursday, October 20CapG
aPm committeetuesday, October 25Webex
symPosium: HoW to tHrive in risk-baseD coorDinateD carethursday, October 27Chicago, hyatt regency O’hare
PHarmaceutical care committee Wednesday, November 2CapG
texas reGional meetinGstuesday, November 8houston, JW marriott
soutHWest reGional meetinGthursday, November 10phoenix, tBD
Public Policy committee conference callsthursday, November 10
state Government ProGrams committeetuesday, November 15CapG
Primary care Practice transformation collaborativeWednesday, November 16CapG
Webinar: HealtH Plan DeleGation oversiGHt, comPliance, anD reGulationsFriday, December 2Webex
Public Policy committee conference callsthursday, December 8
Visit capg.org/calendar or call 213.624.CapG for the most up to date information.
JUNE 22-25, 2017MANCHESTER GRAND HYATT, SAN DIEGO, CA
ANNUALCONFERENCE2017date!TH
E

12 l capg health Summer 2016
Amitabh Chandra, PhD, is the Malcolm Wiener Professor of Social Policy and Director of Health Policy Research at the Harvard Kennedy School of Government. His research centers on innovation and cost growth in healthcare, racial disparities, and medical malpractice. Dr. Chandra spoke with CAPG Health about some of the topics to be covered in his General Session address at the CAPG Annual Conference on Friday, June 17.
caPG Health: Dr. Chandra, you’ve described the situation facing our healthcare system as more than a dilemma—a “trilemma.” please explain what you mean.
Dr. chandra: If you think about the main challenges to U.S. healthcare, there are three: 1) access, or insurance for people who can’t afford it; 2) quality—we want to be sure that the newly insured receive quality healthcare, and for that matter, that all of us receive quality healthcare; and 3) cost. It is possible to have high quality but costly healthcare, or low quality but costly healthcare, which is what we have now. It’s actually possible to have two of the three as well, but quite hard to get all three. No country in the world has all three.
First, access is a financing issue—it requires taxpayers to step up and say we’re willing to do something. But expanding insurance is not going to do much if you give people access to low quality care. It is then up to physicians to meet the challenges of quality and cost, But if physicians fail in this enterprise, government will likely step in and take over. Despite being able to finance an insurance expansion, government is not particularly good at dealing with the quality and cost challenges. this is unsurprising because government isn’t a healthcare provider. But despite this, we have started to see government pushing hospitals to reduce readmissions, and periodically lowering payments.
caPG Health: What are physicians able to do in terms of quality and cost?
Dr. chandra: these challenges are ones only physicians can solve, because they are on the ground as providers. physicians enjoy the trust of their patients. they touch patients everyday. they can discourage their patients from asking for dubious therapies. In a world where fee-for-service is wholly or partially replaced by alternative payment models that reward higher quality and lower costs, physicians become the only party that makes these models successful. If physicians are working in bundled payments or are capitated, they have incentive to figure out which combination therapy is most beneficial, educate their patients, and steer them away from therapies of marginal value. Non-physicians could also do this, but it would result in a far more inferior outcome, with rigid guidelines and very little patient-centered care.
another example: In the long run, we must make hospitals into cost centers. Currently, capitated physician groups are the only ones with incentives to do this. If a patient goes to the hospital, it comes out of the payment to the capitated physician’s budget—so that’s an incentive for physicians to keep patients healthy or steer them to lower cost treatments. For non-capitated physicians, every time a patient goes to the hospital, the hospital gets a payment and so does the physician. We need to make it so that physicians lose money when they refer to the hospital. the hospital has become an end in itself—they’re social cost centers in search of revenue streams—but if our healthcare system were really good, we’d have fewer hospitals.
on the cover
The Healthcare Trilemma: access, Quality, and cost
continued on page 40
“In a world wherefee-for-service iswholly or partiallyreplaced byalternativepayment modelsthat reward higherquality and lowercosts, physiciansbecome the onlyparty that makesthese modelssuccessful.”

Summer 2016 capg health l 13
• Fast, accurate claims payments• Free eReferrals and online doctor-patient communications• Experienced RN case management for complex, time-intensive cases• Deep discounts on EPM and EHR solutions to help you meet the federal mandate• Easy preventive care and disease management reminders for patients• Extensive health resources that boost patient engagement• High consumer awareness that builds practice volume
At Hill Physicians, we continue to improve upon coordinated care, with remarkable results. We provide the tools and support that practices need to be financially successful and improve the coordinated care experience for their patients. Our advantages include:
That’s why nearly 4,000 independent primary care physicians, specialists and healthcare professionals have joined Hill. Feel confident in the future of your practice and your patients by affiliating with Hill Physicians Medical Group.
Hill Physicians’ nearly 4,000 healthcare providers accept HMOs and many PPOs from Aetna, Anthem Blue Cross, Blue Shield, Chinese Community Health Plan, CIGNA, Easy Choice, Health Net, Humana, SCAN, San Francisco Health Plan, United Healthcare WEST and Western Health Advantage. Medicare Advantage plans in all regions. Medi-Cal in some regions for physicians who opt-in.
Kelly Wong, M.D.Hill Physicians provider since 2014.
Uses Cozeva preventive care reminders, Hill inSite to review eClaims and eligibility and Hill EHR for a comprehensive solution to patient care, practice management and ePrescribing.
Confidence
For more about the advantages of affiliating, visit HillPhysicians.com/JoinUs.
The feeling you have when you are affiliated with Hill Physicians.

14 l capg health Summer 2016
hands-On or hands-Off: Balancing monitoring and Oversight at the State level
BY rUSSell D. FOSter aND SheIla a. StepheNS, WeISermazarS llp, aND BIll BarCellONa, CapG
the transition away from fee-for-service reimbursement to value-based payment models is accelerating rapidly across the United States as the triple aim takes hold. We have observed several lessons learned during our careers that provide a framework for this transition.
as physician groups and integrated delivery systems evolve into risk-based payment arrangements with government and commercial payers, regulatory monitoring and oversight is a necessary component to ensure program integrity, compliance, and the welfare of members served by managed care organizations. many states lack the necessary infrastructure to license and/or monitor provider entities that are moving into risk-based payments. as the Centers for medicare & medicaid Services (CmS) enables more organizations to form alternative payment models (apms) under the medicare access and ChIp reauthorization act (maCra), some form of state-level oversight infrastructure will be needed.
Whether the health plan and/or contracted provider risk-bearing entity (rBe) is a for-profit or not-for-profit entity, they must maintain sufficient administrative capacity to ensure efficient and cost-effective operations. additionally, they must maintain adequate financial reserves to protect members, providers, and other stakeholders—including the state agencies that regulate them—against the risk of insolvency due to poor business practices, network inadequacy, fraud, waste, abuse, or any number of other reasons.
It is not easy to regulate health plans and rBes these days. We are talking about large and complex organizations with hundreds of thousands or millions of members, participating in multiple lines of business, with different methods of operation and computer systems, and working with a variety of affiliated entities and/or outsourced vendors to meet their obligations. For a state regulator to have any reasonable understanding of what is happening inside a health plan or rBe, they must be engaged year-round and make a concerted effort to get into the heart of the organization to see how the licensee is actually operating.
Whether you love it or hate it, the affordable Care act (aCa) has resulted in millions of newly insured lives coming into the managed care system. and, with the surge in enrollment, significant strains have been placed on the administrative structures of most managed care organizations. It is not uncommon to see longer claims turnaround times; higher error rates on paid claims; more provider disputes; late claims with interest and penalties due, grievances, and appeals; difficulty managing the high volume of complex cases; staffing challenges; and, from a financial perspective, difficulty in estimating incurred but not reported (IBNr) claims liability.
None of these strains are beyond the health plan or rBe’s ability to correct over time, and most are, in fact, moving quickly to restore compliance. however, not all health plans and rBes have the same knowledge and expertise. monitoring
policy Briefing
Bill Barcellona
Russell D. Foster
Sheila A. Stephens

Fall 2015 capg health l 15
“The only real answer is for regulators to have more ‘hands-on’ involvement throughout the year—and it has to be more than a cursory involvement to be meaningful.”
continued on next page
and oversight by regulatory agencies is necessary to ensure that all licensees are held to the same standards, and that each is working diligently to resolve areas of noncompliance while striving to improve patient care and operational efficiency and effectiveness.
We fully recognize that managed care organizations already believe there is too much regulatory oversight and feel like they are drowning at times under audits by CmS, state regulatory agencies or, in the case of rBes, their health plan partners. We agree the number of audits often is too many, and some effort needs to be made to reduce the burden on the health plans and rBes while producing the kinds of audit results necessary to ensure stakeholders’ interests are protected. Focused audits of the claims or utilization management departments, and annual independent financial audits are helpful and provide useful information. Yet all these audits have limited value when trying to understand the organization and interdepartmental dependencies at a detailed operational level and attempting to identify and address underlying systemic issue(s) that may be at the root of many noncompliance issues.
For those who say it’s not the role of government to run the managed care organization or tell them what to do, we say, you are absolutely right. regulators are not supposed to run the businesses they regulate; rather, they exist to ensure compliance with laws, rules, and regulations, and to make recommendations for improvement. however, to those critics who advocate for less regulatory oversight (“hands off”), you need to live through a failure or two to understand the potential risks and impact of a business failure or series of repeated process failures. thousands of members have been or could be thrown into a state of uncertainty because their care has been disrupted, providers suddenly refuse to provide care due to non-payment, or they’ve lost confidence in a system that is supposed to protect them.
although the market is experiencing fewer health plan or rBe failures than in previous years, largely due to industry consolidation, we have all seen or heard about failures of large institutions. allowing a bank or an automobile manufacturer to fail or to receive a bailout is a matter of public policy, but letting a large health plan or rBe fail is a completely different matter. that has the potential to cost lives or at least impair the health and well being of
thousands of members, which is something that regulators must not allow to happen in the public interest. Waiting for a failure to occur and then responding to the fallout that will invariably happen (i.e., Why didn’t you know? Why didn’t you do more or take action sooner?) is not where regulators want to end up. the only real answer is for regulators to have more hands-on involvement throughout the year—and it has to be more than cursory involvement to be meaningful.
a short list of options is available to states considering how to implement regulatory oversight of a growing industry of risk-bearing entities in a value-based payment environment:
• all managed care functions (licensing, monitoring and oversight, auditing, reporting and enforcement) should be consolidated under one agency. Silos only increase the probability that monitoring and
oversight activities will be less than optimal.
• State regulatory teams need educated and trained staff that understand the managed care business and possess specific levels of expertise in how managed care organizations operate.
• regulatory standards must be enforced consistently across all licensees in order to ensure program integrity and consistency in enforcement actions.
• On-site audits need to be more comprehensive (e.g., plan-wide) and, at least periodically, include a deep dive into the plan’s entire operation, so there is a more complete understanding of its administrative capacity, staffing and financial strengths, and weaknesses. Joint audits are preferred over separate financial and medical audits. Not only is it less intrusive on the licensee, a joint audit enables examiners to confer with each other during the exam, which usually results in a better audit.
• regulators should allow health plans to consolidate their compliance and oversight activities to prevent the need for every health plan to audit every rBe every year. Duplication of effort is expensive, time consuming, and a waste of valuable resources. audit/compliance exceptions, when found, should lead to a universal corrective action plan (Cap) that all plans can monitor to ensure compliance.

• although regulators ultimately hold health plans accountable for the financial solvency and administrative capacity of their delegated entities, regulators need to look more closely at rBes too, because through delegation rBes are often contractually obligated to provide many or most of the same services the health plan would normally provide. In our experience, there has been a wide variation in the level of administrative competence at the rBe/management services organization (mSO) level. rBes also tend to have lower enrollment levels and are therefore subject to higher risks than their health plan partners, which can lead to a higher rate of failure.
the healthcare industry has embraced the triple aim: improvement in the health of populations, improvement in the experience of healthcare, and lower per capita costs. to ensure success, regulators need to play an important role in making the triple aim a reality—that is, by making sure licensees do what is necessary to ensure that the health of their enrolled populations improves, members see improvement in their individual experiences of healthcare, and health plans and rBes strive to find ways to operate in an efficient and cost-effective manner and ensure their financial viability going forward.
Our purpose in writing this article is to stimulate discussion about regulatory oversight and to highlight ways in which state regulatory agencies can help ensure health plans and rBes in their states perform at optimal levels. the three of us have worked through the impacts of failed entities during our careers, including shutdowns and turnarounds. We have collaborated on strategies to save troubled entities, and managed transitions when insolvency couldn’t be remedied. each of us remains enthusiastic about health reform in the U.S. an effective oversight and monitoring program will also ensure that managed care continues to build trust among all stakeholders and that quality and cost efficiency remain the driving forces for change. o
Russell D. Foster is a Principal with WeiserMazars LLP. He has more than 35 years’ experience in developing and managing healthcare systems. Sheila A. Stephens, a Principal with WeiserMazars LLP, has logged 30 years in healthcare, with particular focus on services and quality management. Bill Barcellona is Senior VP for Governmental Affairs at CAPG, and a former Deputy Director of the California Department of Managed Healthcare, with 30 years of experience as an attorney.
Sure, the Santa Cruz Health Information Exchange is one of the oldest HIEs in the country but that was just the beginning. For almost two decades we’ve diversified beyond our IPA roots to include a connectivity LLC, and even an insurance service for individuals and businesses in health care.
IT’S JUST ONEOF THE THINGS WE DO.
PMGSCC.COM/CAPG
16 l capg health Summer 2016
Monitoring and Oversight...continued from page 15

Andy SlavittActing Administrator, Centers for Medicare& Medicaid Services (CMS)
Francis J. Crosson, MDChairman, Congressional Medicare AdvisoryCommission (MedPAC)
Robert M. Pepper, DOFamily physician and endurance trainer
Neera TandenPresident and CEO, Center for American Progress and Center for American Progress Action Fund
Panel—MIPS or APMs:Which MACRA Option is Right for You?Moderated by Mara McDermott, VP of Federal Affairs, CAPG
Panel—Alternative PaymentModels in Action: What WorksModerated by Donald H. Crane, President and CEO, CAPG
Featured sessions include:
Panel—The Politics of Healthcare in an Election YearSheila P. Burke Faculty research fellow, Malcolm Wiener Center for Social Policy and faculty member,Kennedy School of Government, Harvard University; Chair of Federal Public Policy, Baker, DonelsonDouglas Holtz-Eakin President, American Action ForumLen M. Nichols, PhD Director, Center for Health Policy Research and Ethics; Professor of HealthPolicy, George Mason University
Colloquium 2016Building Successful
AlternativePayment Models
September 28–30, 2016 Hyatt Regency on Capitol Hill, Washington, DC
REGISTER NOW! capgcolloquium.com

Work-life Balance, Part 2
18 l capg health Summer 2016
BY amY NGUYeN hOWell, mD, mBa, ChIeF meDICal OFFICer, CapG
It has been almost two years since my article on work-life balance was published in CAPG Health. In this follow-up, I talk about my real-life challenges and offer some tips to help motivate you to find your balance. more importantly, I would like to discuss a current topic that’s been in the news—an issue important for all industry leaders, particularly physician executives.
as I continue to pursue my professional dreams in this fast-paced healthcare environment, I find myself challenged as I juggle childcare and career, traveling and hustling from one city to the next. When my work schedule permits, I go on same-day trips that allow me to get home in time to read a few short stories about trucks and taco-eating dragons with my youngest son before I tuck him into bed. When in Washington, DC, for CapG’s Colloquium, I bring my family along, so we can enjoy the dinosaur exhibit at the National museum of Natural history. also, we try to enjoy some poolside r&r in San Diego during CapG’s annual Conference. Savoring these special moments with my family allows me to have a sense of fulfillment as a multifaceted person—medical professional, mom, and wife.
It’s hard to discuss work-life balance without addressing the important issue of gender pay equality. harvard economics professor Claudia Goldin explains the reason is due to the high cost placed on temporal flexibility. In a recent interview on National public radio, she said, “Disproportionately, women, particularly those who are mothers or who are taking care of others, would like greater predictability in their hours. they would like less on-call hours.” those jobs with longer hours and less predictability are often associated with higher income occupations. Dr. Goldin goes on to say, “temporal flexibility is giving someone the ability not just to work fewer hours but to work their hours and not get a big hit for it or to work hours that are more predictable. a physician, let’s say, could work 50 hours a week but work the days that they would like to work and not be on call. they’ll probably get less than someone who is working the graveyard shift or who was on call...that’s true in a lot of fields. and it’s also as true at the top as it is at the bottom.”
however, other research out of harvard Business School attributes gender pay inequality to discrimination. In a recent paper titled, “equal Opportunity? Gender Gaps in CeO appointments and executive pay,” researchers systematically tried to present a logical explanation for the gender gap, aside from unmeasurable factors like chauvinism. they mostly failed because they found a significant gap in top corporate positions, in both the number of female executives and how much money they make compared to men. It seems there isn’t much women can do to close that gap—no matter how talented, educated, skilled, lucky, ambitious, or genetically gifted—unless they can figure out a way to thwart discrimination.
But, in failing to find a quantifiable explanation, the harvard researchers succeeded in challenging a commonly held notion that the corporate gender gap can be attributed to observable, measurable, controllable factors such as a woman’s intelligence level, the amount of time she takes off to raise children, or the quality of her network connections.
“As I continue to pursue my professional dreams in this fast-paced healthcare environment, I find myself challenged as I juggle childcare and career, traveling and hustling from one city to the next.”
continued on page 42

Summer 2016 capg health l 19
REDEFINING WE ARE REDEFINING
THE WAY DOCTORS AND INTEGRATED DELIVERY
SYSTEMS MANAGE MEDICAL MALPRACTICE RISK.
We relentlessly defend, protect, and reward
the practice of good medicine.
Our revolutionary approach is seamless and cost-effective.
As the nation’s largest physician-owned medical malpractice
insurer and an innovator in creating solutions for organizations
like yours, we have the resources and experience to meet your
unique needs. We’re already providing medical malpractice
insurance to a range of integrated delivery system models
across the country—supporting thousands of physicians.
Learn more about our sophisticated, flexible risk solutions.
CALL OUR LOS ANGELES OFFICE AT 888.536.5346 OR VISIT WWW.THEDOCTORS.COM
5517_CA_CAPG_Health_IDS_Red_3rdQtr2015_flat_f_ISSUU.indd 1 8/10/15 10:27 AM

It has been just over a year since Congress passed and president Obama signed into law the medicare access and ChIp reauthorization act (maCra). In the early days following its passage, the primary focus was on the repeal of the Sustainable Growth rate (SGr) formula. to be sure, SGr had plagued the health industry for years—the formula resulted in a cycle of proposed cuts and patches, forcing blunt cuts to the healthcare industry year after year. ending this cycle was truly something to be celebrated.
and yet, the repeal of the flawed SGr formula was just the beginning of maCra’s significance to physicians. Now proposed to begin in 2017, maCra puts in place a new system of potential rewards and penalties for physicians in traditional medicare. the law gives physicians two options: the merit-Based Incentive payment System (mIpS) or alternative payment models (apms). the vast majority of medicare part B payments will fall into these two categories, with very few exceptions.
In april, the Centers for medicare & medicaid Services (CmS) released the proposed rule that advances maCra implementation. the final rule is expected this fall.
MiPs: Fee-FOr-service WiTH PayMenT Tied TO value
the mIpS path will continue to pay physicians fee-for-service in traditional medicare, with a greater percentage
of that payment tied to value over time. the mIpS path is intended to consolidate fragmented quality measurement programs in the existing
medicare part B program. today, physicians in traditional medicare participate in three separate
programs: the physician Quality reporting System (pQrS), meaningful use of electronic health records technology, and the value-based payment modifier program.
maCra intends to combine and streamline these three separate programs into a single mIpS score. the mIpS score will comprise the three existing program elements and will add a fourth category of clinical practice improvement activities. In the early days of maCra implementation, physicians may receive up to a 4% incentive or 4% cut to their payment depending on their mIpS score across the four components. this percentage increases over time, with an additional bonus for exceptional performers. the mIpS program, in general, is budget neutral. there will be winners and losers, and the money to pay the winners comes out of the pockets of the losers.
BY mara mCDermOtt, Vp OF FeDeral aFFaIrS, CapG
Federal Updateadvancing risk-Based Coordinated Care through Federal advocacy
20 l capg health Summer 2016
“CAPG is working in Washington, DC, to create a system of incentives for physician groups engaged in APMs in Medicare Advantage.”
MIPS
PQRS
ValueModifier
MeaningfulUse
ClinicalPractice
Improvement
continued on page 22

Summer 2016 capg health l 21
Allscripts solutions advance clinical and financial results by enhancing care coordination, patient engagement and analytics. A global leader in healthcare technology, we connect people, places and data throughout the process of care to help meet unique population health challenges. We help drive the evolution in healthcare delivery.
The power to collaborate. That’s the Power of Allscripts.
Innovations that inspire smarter care.
Cop
yrig
ht ©
201
6 A
llscr
ipts
Hea
lthca
re S
olut
ions
, Inc
.
Learn more about Allscripts at www.allscsripts.com

22 l capg health Summer 2016
alTernaTive PayMenT MOdels: TOWard a value-Based PayMenT sysTeM
a second option creates an incentive payment for physicians who participate in advanced alternative payment models (apms), which are intended to move traditional medicare away from its reliance on fee-for-service, volume-based reimbursement. maCra contemplates a set of risk-bearing apms that will receive a
5% bonus for a period of time. the statute sets out criteria, including specific models such as the medicare Shared Savings program (mSSp), models tested by the CmS Innovation Center, and demonstrations required by federal law. these apms must meet specific criteria, including bearing “more than nominal financial risk.” With this option, Congress intended to encourage physicians to move into risk-bearing apms that will transform traditional medicare.
maCra’s implementation poses an exciting opportunity to move significantly more medicare payments into value-based arrangements. Yet, substantial work remains to ensure that implementation achieves the lofty goals of delivery system reform. three specific issues for CapG members to consider are:
1. WHaT is THe rOle OF Medicare advanTage in Macra?
maCra overlooks the role of medicare advantage in delivery system reform. to achieve the 5% apm incentive payment, a physician must have a percentage of their traditional medicare revenue in an apm. participating in an apm in medicare advantage alone will not be enough— a significant source of frustration to CapG members who may have a substantial portion of medicare advantage revenue in percent of premium capitation or other risk-bearing arrangements. CapG is working in Washington, DC, to create a system of incentives for physician groups engaged in apms in medicare advantage. Our strategy of legislative and regulatory options is aimed at leveling the playing field for apms in medicare advantage.
2. WHaT are BOnus-eligiBle aPMs?
to be eligible for the 5% maCra bonus, advanced apms must meet specific criteria. In its proposed rule, CmS defines a narrow set of qualifying apms: the medicare Shared Savings program tracks 2 and 3, Next Generation
aCO model, Comprehensive primary Care plus, Oncology Care model two-sided risk arrangement, and comprehensive eSrD care lDO arrangement. Within this definition, upside-only risk models, like the mSSp track One accountable Care Organizations, would not qualify for the maCra bonus incentive; they would have to participate in mIpS.
maCra provides a significant opportunity to move the delivery system along the continuum toward risk. While very few risk-bearing providers exist in traditional medicare today, maCra was designed to dramatically change the landscape. Its goal is to provide that incentive to change behavior going forward. Consistent with this view, we are encouraging CmS to consider other options to incent participation in risk-bearing arrangements in medicare and transform the delivery system. these options include both incentive payments and regulatory relief for risk-bearing models. regulatory relief may include simplified quality reporting gates, streamlined approaches to electronic health records (ehr) certification, and waiving restrictive and burdensome fee-for-service requirements.
3. are THere suFFicienT aPM OPTiOns in TradiTiOnal Medicare?
Finally, we are encouraging CmS to continue to develop advanced, risk-bearing apm options, including capitation. We believe that maCra’s success will largely rely on CmS’s risk-bearing medicare aCOs: the mSSp and Next Generation aCO.
We were pleased to see the introduction of the Next Generation aCO model, which represents a positive step in the evolution of medicare aCOs. the Next Generation aCO provides new payment models, including prepaid capitation and stronger incentives for beneficiary engagement in the model. even so, participation in the program is likely to be relatively limited. It is a test model through the CmS Innovation Center with a limited application period closing in may 2016.
this means that the medicare Shared Savings program and its risk-bearing tracks may be the best available option for physician groups that want to participate in the maCra apm pathway. We continue to work with CmS and Congress to improve the mSSp aCO program, as well as to develop new advanced apm options.
Macra’s enacTMenT is JusT THe Beginning
maCra presents the opportunity for significant advancement of traditional medicare away from a flawed, volume-based incentive system toward a forward-looking system that pays for the value of care delivered. But maCra’s implementation will be critical to defining this path going forward. CapG will continue to play a central role in representing america’s risk-bearing physician organizations as the law is implemented. We look forward to representing you in Washington, DC, through this exciting and pivotal time. o
BonusEligibleAPM
Specificmodels
Quality
CertifiedEHR
NominalRiskorQualifyingMedicalHome
RevenueThresholds
Advancing Risk-Based Care...continued from page 20

QUALITY FOCUSPROCESS IMPROVEMENT
TECHNOLOGY EFFICIENCY
MED
ICA
L E
XPEN
SE
REV
EN
UE
AD
MIN
IST
RA
TIV
E E
XPEN
SE
ANALYTICS CARE QUALITY
[email protected], option 4
© 2016 HealthCare Information Management, Inc. All Rights Reserved.
CAPABILITIES
Are you ready to transition to the new value-based healthcare model?
Our Strategic Consultants are ready to architect and guide you through your blueprint for transformation.

CA
PG
M
EM
BE
RS
24 l capg health Summer 2016
ORGANIZATIONAL MEMBERS
accountable Health care iPaGeorge m. Jayatilaka, mD, CeODruvi Jayatilaka, Vice president
advanced medical management, inc.kathy hegstrom, president
access medical Group/access Senior health Care • California Ipa • Community Care Ipa • Future Care Ipa • mediChoice Ipa • premier Care Ipa • Seoul medical Group
adventist Health Physicians network iPaarby Nahapetian, mD, CmOJim agronick, Vp, Ipa Operations
affinity medical Grouprichard Sankary, mD, presidentScott ptacnik, COO
alameda Health PartnersWilliam peruzzi, mD, ChairmanDavid Cox, treasurer/CFO
allcare iPa*matt Coury, CeOrandy Winter, mD, president
allied Physicians of californiathomas lam, mD, CeOkenneth Sim, mD, CFO
allina Health systemrod Christensen, mD, Vp of medical OperationsBrian rice, mD, Vp Network/aCO Integration
altamed Health services corporation*Castulo de la rocha, JD, president and CeOmartin Serota, mD, CmO
applecare medical Group, inc.*Vinod Jivrajka, mD, president/CeOtrish Baesemann, president
austin regional clinicNorman Chenven, mD, CeO and Founderkerry rosker, executive administrative Coordinator
bakersfield family medical centerCarol l. Sorrell, rN, COO Ju hwan lee, mD, medical Director
bayhealth Physician alliance, llcevan W. polansky, JD, executive DirectorJoseph m. parise, DO, medical Director
beaver medical Group*John Goodman, CeOraymond Chan, mD, Vp, medical administration and CmO
brown & toland Physicians*richard Fish, CeO
california Pacific Physicians medical Group, inc.Dien V. pham, mD, CeOCarol houchins, administrator
caremore medical GroupSachin Jain, CeOtom tancredi, Dir. of practice Operations
catholic Health initiatives*Don lovasz, president, Clinically Integrated NetworkChris Stanley, mD, Vp of Care management
cedars-sinai medical Group*Stephen C. Deutsch, mD, Chief medical DirectorJohn Jenrette, mD, executive Vp, medical Network
central ohio Primary care Physicians, inc.J. William Wulf, mD, CeOmichael ashanin, COO
children’s Physicians medical Groupleonard kornreich, mD, president and CeO
chinese american iPaGeorge liu, mD, phD, president and CeOpeggy Sheng, COO
chinese community Health care associationJohn m. Williams, pharmD, CeOpolly Chen, Director of Operations
choice medical Groupmanmohan Nayyar, mD, presidentmarie langley, Ipa administrator
cigna medical Groupedward kim, president and General managerkevin ellis, DO, CmO
citrus valley independent PhysiciansGurjeet kalkat, mD, executive medical Directormartin kleinbart, Dpm, Chief Strategy Officer
colorado Permanente medical Group, P.c.margaret Ferguson, mD, president and executive medical DirectorDan a. Oberg, CFO and Vp Corporate Development
conifer Health solutionsmegan North, CeO
altamed health Services • exceptional Care medical Group • Family Choice medical Group • Family health alliance • mid Cities Ipa • OmniCare medical Group • premier Care of Northern California • Saint agnes medical Group
continucare corporationalfredo Ginory, mD, CmOGemma rosello, Vp
DcHs medical foundationDean m. Didech, mD, CmO
Desert oasis Healthcaremarc hoffing, mD, medical DirectorDan Frank, COO
Dignity Health foundationBruce Swartz, SVp, physician Integration
edinger medical Groupmatthew C. Boone, mD, executive medical DirectorDenise mcCourt, COO
el Paso integral care, iParafael armendariz, DO, presidenttony martinez, administrator
empire Physicians medical Group*Steven Dorfman, mD, presidentYvonne Sonnenberg, executive Director
everett clinic, P.s., the*adrianne Wagner, Quality Improvement Consultant managerShashank kalokhe, associate administrator of Value-Based Contracting and Coordinated Care
facey medical foundation*James m. Slaggert, CeOerik Davydov, mD, medical Director
Golden empire managed care, inc.*michael myers, president and CeO
Good samaritan medical Practice associationNupar kumar, mD, medical Director
Greater newport Physicians medical Group, inc.*Diane laird, CeOadam Solomon, mD, CmO
Guthrie medical GroupJoseph a. Scopelliti, mD, president and CeOFrederick J. Bloom, mD, president
Healthcare Partners*Don rebhun, mD, National medical DirectorJim rechtin, SVp Corporate Strategy
Heritage Provider network*richard merkin, mD, presidentrichard lipeles, COO
affiliated Doctors of Orange County • arizona priority Care plus, az • Bakersfield Family medical Group • California Coastal physician Network • California Desert Ipa • Coastal Communities physician Network • Desert Oasis healthcare • Greater Covina medical Group • healthCare partners, Ipa, az & NY • heritage physician Network • heritage Victor Valley medical Group • high Desert medical Group • lakeside Community healthcare • lakeside medical Group • regal medical Group • Sierra medical Group
High Desert medical GroupCharles lim, mD, FaCp, medical Directoranthony Dulgeroff, mD, assistant medical Director
Hill Physicians medical Group, inc.*David Joyner, CeOtom long, mD, CmO
Horizon medical Group, PcJames Olver, CeOkristen vanDuynhoven
John muir Physician network lee huskins, president and CaOravi hundal, mD, CFO
lakeside community HealthcareJonathan Gluck, Counsel
lakeside medical Group, inc.
lakewood iPaJean Shahdadpuri, mD, mBa, CmOVarsha Desai, COO
alamitos Ipa • St. mary Ipa • Brookshire Ipa
leon medical centers, inc.rafael mas, mD, SVp and CmOJulio G. rebull, Jr., SVp
loma linda university Health careJ. todd martell, mD, medical Director
maverick medical GroupWarren hosseinion, mD, Chairmanmark C. marten, CeO
meD3000lynn Stratton haas, CeOGary proffett, mD, medical Director
SeaView Ipa • Valley Care Ipa
medPoint managementkimberly Carey, presidentrick powell, mD, CmO
accountable health Care Ipa • Bella Vista medical Group Ipa • Centinela Valley Ipa • el proyecto Del Barrio, Inc. • Global Care medical Group Ipa • healthCare la Ipa • Jewish home for the aging Ipa • pioneer provider Network, a medical Group, Inc. • premier physicians Network • prospect medical Group, Inc. • redwood Community health Network • Watts healthcare Corporation
memorialcare medical Group*mark Schafer, mD, CeOlaurie Sicaeros, COO, Vp of physician alignment
memorial Hermann Physician network - mHmDChristopher lloyd, eVp and CeO Shawn Griffin, Chief Quality and Informatics Officer
mercy Health Physiciansrandall Curnow, mD, presidentmichele montague, COO
meritage medical networkWojtek Nowak, CeOJ. David andrew, mD, medical Director
mid-atlantic Permanente medical Group, PcBernadette loftus, mD, associate executive Director for maSJessica locke, Special assistant
molina medical centers* keith Wilson, mD, CmO Gloria Calderon, Vice president of Clinic Operations
monarch Healthcare*Bart asner, mD, CeOray Chicoine, president and COO
mso of Puerto ricorichard Shinto, mD, CeOraul montalvo, mD, president
muir medical Group, iPa Ute Burness, rN, CeOSteve kaplan, mD, president
namm california*leigh hutchins, president and COOVerni Jogaratnam, mD, CmO
Coachella Valley physicians of primeCare • mercy physicians medical Group • primary Care associated medical Group • primeCare medical Group of Chino • primeCare medical Network • primeCare of Citrus Valley • primeCare of Corona • primeCare of hemet Valley • primeCare of Inland Valley • primeCare of moreno Valley • primeCare of redlands • primeCare of riverside • primeCare of San Bernardino • primeCare of Sun City • primeCare of temecula • redlands Family practice medical Group* Indicates 2015 - 2016 Board members

Summer 2016 capg health l 25
new West Physicians, Pcruth Benton, CeOthomas m. Jeffers, mD, president and Chair
northwest Permanente, P.c.harry Stathos, Vp and CFO
northwest Physicians network of Washington, llcrick macCornack, phD, CeOScott kronlund, mD, CmO
omnicare medical Grouptoni Chavis, mD, presidentashok raheja, mD, medical Director
the Permanente medical Group, inc. oakland (north)*michelle Caughey, mD, associate executive DirectorSuketu Sanghvi, mD, associate executive Director
Physicians Datatrustkathi toliver, Vp of Ipa administration lisa Serratore, COO
Greater tri-Cities Ipa • Noble ama Ipa • St. Vincent Ipa
Physicians choice medical Group of san luis obispoJohn Okerblom, mD, presidentBarbara Cheever, executive Director
Physicians medical Group of santa cruz countymarvin labrie, CeONancy Greenstreet, mD, medical Director
Physicians choice medical Group of santa mariaJohn Okerblom, mD, presidentBarbara Cheever, executive Director
Physicians of southwest Washington, llcmelanie matthews, CeOGary r. Goin, mD, president
PiH Health Physiciansrosalio J. lopez, mD, SVp and CmOramona pratt, rN, COO, Group Operations
Pioneer medical Group, inc.*John kirk, CeOJerry Floro, mD, president
Preferred iPa of californiamark amico, mD, medical Directorzahra movaghar, administrator
ProHealtH care associatesDavid Cooper, mDWalter leStrange, eVp and COO
Prospect medical Group*Jason Barker, CeOJeereddi prasad, mD, president and acting CmO
amVI/prospect medical Group • Genesis healthcare of Southern California, a medical Group • Nuestra Familia medical Group • pomona Valley medical Group • prospect healthSource medical Group • prospect medical Group • prospect NWOC medical Group • prospect professional Care medical Group • prospect provider Group rI, llC • prospect provider Group Ct - eChN, llC • prospect provider Group Ct - Waterbury, llC • prospect provider Group NJ, llC • prospect health Services tX • StarCare medical Group • Upland medical Group, a professional medical Corporation
Providence Health & servicesJames m. Slaggert, CeO
Providence medical management servicesphil Jackson, Chief Integration and transformation Officer
korean american medical Group • providence Care Network
renaissance Physician organizationClare hawkins, mD, Ipa Board ChairWhitney horak, Vp
river city medical Group, inc.keith andrews, mD, medical Directorkendrick t. Que, COO
riverside medical clinicSteven larson, mD, ChairmanJudy Carpenter, president and COO
riverside Physician network howard Saner, CeOpaul Snowden, COO
st. Joseph Heritage Healthcare*kevin manemann, president and CeOkhaliq Siddiq, mD, CmO
hoag medical Group • mission heritage medical Group • St. mary high Desert medical Group
st. vincent iPa medical corporationJeffrey hendel, mD, presidentleesa Johnson, Director of Ipa Operations
san bernardino medical GroupJames malin, CeOthomas hellwig, mD, president
sansum clinic*kurt ransohoff, mD, president and medical DirectorVince Jensen, COO
santa clara county iPa (scciPa)*J. kersten kraft, mD, president of the Boardlori Vatcher, CeO
santé Health system, inc Scott B. Wells, CeODaniel Bluestone, mD, medical Director
scripps coastal medical centeranthony Chong, mD, CmOtracy Chu, assistant Vp of Operations
scripps Physicians medical GroupJoyce Cook, CeOJames Cordell, mD, medical Director
sharp community medical Group*paul Durr, CeOChristopher mcGlone, COO
arch health partners • Graybill medical Group
sharp rees-stealy medical Group*Stacey hrountas, CeOalan Bier, mD, president
southeast Permanente medical Group, inc., themichael Doherty, mD, executive medical Director and Chief of Staff
southern california Permanente medical Group*Diana r. Shiba, mD, Comprehensive Opthamologist Dept.James malone, medical Group administrator
southwest medical associatesrobert B. mcBeath, mD, president and CeOGreg Griffin, COO
summit medical Group, PaJeffrey le Benger, mD, Chairman and CeOJamie reedy, mD, Vp of population health and Quality
sutter Health foundations & affiliated Groups*Jeffrey Burnich, mD, SVp and executive Officer, Sutter medical Network
Central Valley medical Group • east Bay physicians medical Group • Gould medical Group • marin headlands medical Group • mills-peninsula medical Group • palo alto Foundation medical Group • palo alto medical Foundation • peninsula medical Clinic • physician Foundation medical associates • Sutter east Bay medical Foundation • Sutter Gould medical Foundation • Sutter Independent physicians • Sutter medical Foundation • Sutter medical Group • Sutter medical Group of the redwoods • Sutter North medical Group • Sutter pacific medical Foundation
swedish medical Groupmeena mital, mD, medical DirectorBela Biro, admin. Director, accountable Care Services
synergy Healthcare, llcJames Jones, mD, Chairman of the BoardChris h. keffer, Vp, Network Operations
synermed*James mason, president and CeOGeorge ma, mD, medical Director
alpha Care medical Group • angeles Ipa • Crown City medical Group • ehS Inland Valleys Ipa • ehS medical Group – Central Valley • ehS medical Group – los angeles • ehS medical Group – Sacramento • employee health Systems • Ipa of Georgia • multiCultural Ipa • pacific alliance medical Center • Southern California Children’s Network
tenet HealthcareJacob Furgatch, CeOronald kaufman, CmO
the vancouver clinic, inc., P.s.mark mantei, CeOalfred Seekamp, mD, CmO
torrance Health iPaNorman panitch, mD, presidentJohn mcNamara, mD, CmO
triad Healthcare network, llcthomas C. Wall, mD, executive medical DirectorSteve Neorr, Vp, executive Director
uc irvine Healthmanuel porto, mD, president and CeO, Sr. associate Dean of Clinical affairspat Dolphin, Chief ambulatory Officer and executive Director of University physicians and Surgeons
ucla medical Group*Sam Skootsky, mD, CmOkit Song, mD, medical Director of Surgical Services
usc care medical Group, inc.Donald larsen, mD, CmO
valley organized PhysiciansWilliam torkildsen, mDSarah Wolf
verity medical foundationDean m. Didech, mD, CmOmathew abraham, CaO
Wellmed medical Group, P.a.George m. rapier III, mD, Chairman and CeOCarlos O. hernandez, mD, president
CORPORATE PARTNERSabbvieanthem Blue Cross of CaliforniaathenahealthBoehringer Ingelheim pharmaceuticals, Inc.evolent healthhumana, Inc.merck & Co.Novartis pharmaceuticalsNovo Nordiskpatient-Centered primary Care CollaborativeQuest DiagnosticsSanofi, USSCaN health plan
ASSOCIATE PARTNERSarkrayarrohealthastellas pharma US, Inc.astrazeneca pharmaceuticalsavanir pharmaceuticals, Inc.Bayer healthCare pharmaceuticalsBio-reference laboratories, Inc. Daiichi Sankyoeasy Choice health plan, Inc. Genentech, Inc.Gilead SciencesIncyte CorporationJohnson & Johnson Family of Companieskaufman, hall & associateskindred healthcare, Inc.lumara health, a Division of amaG pharmaceuticalspfizer, Inc.ralphs Grocery CompanySunovion pharmaceuticals Inc.Surgical Care affiliates, Inc. takeda Oncology the Doctors CompanyVitas healthcare Corporation of California
AFFILIATE PARTNERSable healthaetion, Inc. alignment healthcare alturaaSpira laBSaxene health partnersCal INDeXChildren’s hospital los angeles medical GroupCVhCareGlobal transitional Carehonormills peninsula medical GroupmyWoundDoctor, Inc.Nifty after Fifty monarch llC partners in Care Foundationpharmacyclics, Inc.psycheanalytics, Inc.redlands Community hospitalSaint agnes medical GroupSullivanluallin GroupVentegra, llC

26 l capg health Summer 2016
Welcome Home: using Mobile Technology to reduce Hospital readmissions BY JaNet appel, DIreCtOr OF INFOrmatICS aND pOpUlatION health, Sharp reeS-StealY meDICal GrOUp
Sharp rees-Stealy medical Group in San Diego, part of San Diego’s Sharp healthCare, is focusing on a new strategy to provide patients with extended support and peace of mind after an acute hospital stay. patients receive personalized follow-up communication that allows them to engage in their own recovery, increase quality of life, and ultimately avoid hospital readmission.
the program, aptly named Welcome home, sends timed, daily text messages to reiterate post-treatment instructions, identify early warning signs of potential issues, and promote behavioral change. During the pivotal few weeks post-hospitalization, patients are being tended to with the utmost care and attention. the digital platform serves as a two-way communication tool, giving patients personalized access to their care team at the touch of a button.
With this innovative program, primary care physicians, rN clinical case managers, and non-clinical staff can stay in close contact with patients for a remarkable 90 days post-discharge. this is a substantial increase from previous post-discharge care, which is generally limited due to lack of resources. the daily text message reminders put healthcare at the top of patients’ minds
during what is arguably the most critical window of time during recovery—empowering them to ask questions about their recovery from a comfortable environment by simply sending a reply text message.
“the relationship between provider and patient is shifting toward feedback and collaboration, ultimately increasing patient engagement and satisfaction,” says Dr. parag agnihotri, medical Director, Continuum of Care, Sharp rees-Stealy.
this direct line of communication allows clinical case managers from Sharp rees-Stealy’s population health department to spend more time answering specific patient questions than traditional means of follow-up previously allowed. patients appreciate the direct link to clinical staff so they may get their questions answered and concerns addressed in a timely manner.
If necessary, the clinical case managers will contact the patient’s primary care physician, thereby providing immediate intervention for any impending issues that could lead to readmission. patient medical records are easily accessible by the entire care team, allowing decisions to be made as a shared effort between patient, primary care physician, and clinical case manager. this real-time communication maximizes the collaboration between medical departments while
“With this innovative program, primary care physicians, RN clinical case managers, and non-clinical staff can stay in close contact with patients for a remarkable 90 days post-discharge.”

Summer 2016 capg health l 27
One call does it all.
Contact June Simmons, CEO818-837-3775 [email protected]
For coordinated services that address the social determinants of health.
• Regional network of community-based organizations• Culturally diverse providers with local expertise• HomeMeds medication reconciliation• Care transitions coaching• Health self-management education• In-home assessments• Wraparound services like meals and transportation• Proven results – quality and cost
simultaneously monitoring patient outcomes.
Since the program’s introduction, Sharp rees-Stealy nurses in almost every associated clinic have increased capacity to care for 25% more patients with minimal budget increases. hospital readmissions are low, quality of care is in the top percentile for California, and patients show a 78% engagement rate in Sharp rees-Stealy programs. the texting platform allows the group to derive greater value from the case management resources already in place, eliminating the need to increase the budget for additional staff.
to create the Welcome home texting platform, Sharp rees-Stealy teamed up with agile health, a healthcare technology vendor, and mCG, part of the hearst health network. Welcome home uses care guidelines and related expertise from mCG to help ensure that the message content incorporated in the program is evidence based and aligns with patient care plans.
Sharp rees-Stealy has already found great success with its first texting program to help patients manage chronic illnesses such as diabetes, chronic obstructive pulmonary disease, and heart disease. the success has led to similar texting initiatives in two other departments. the Sharp-rees Stealy pharmacy plans to develop a medication-adherence texting program and the Center for health management recently launched a pediatric obesity program incorporating texting.
the impact of the Welcome home initiative has increased Sharp rees-Stealy’s patients’ personal experience of care, improved the quality of care for the post-discharge population, and reduced costs for healthcare delivery. Using new technology to communicate with patients the way they prefer is just one way San Diego’s oldest multispecialty medical group continues to provide outstanding, coordinated, cost-effective care. o

Integrating behavioral health into primary care is receiving attention as an intervention with the potential to achieve the Quadruple aim of improving health outcomes, patient experience of care, and the experience of providers and staff delivering care, while efficiently using healthcare resources. this
article addresses three key questions often raised by those working on integration:
• What is behavioral health integration (BhI)?
• Why is BhI important as we move into a healthcare world of paying for value rather than volume?
• how can my organization successfully implement BhI?
BHi: develOPing a deFiniTiOn
the agency for healthcare research and Quality organized an effort to develop a consensus definition of BhI. the lexicon for Behavioral health and primary Care Integration was developed by a large group that included experts on BhI, as well as patients and family members, using an iterative process1. the group settled on the following definition:
Integrated behavioral healthcare is the care that results from a practice team of primary care and behavioral health clinicians, working together with patients and families, using a systematic and cost-effective approach to provide patient-centered care for a defined population.
this care may address mental health and substance abuse conditions, health behaviors (including their contribution to chronic medical illnesses), life stressors and crises, stress-related physical symptoms, and ineffective patterns of healthcare utilization.
It is worth noting that this definition is very broad in terms of the application of integration to healthcare problems and does not limit the scope of integration to the care of common mental health conditions, such as depression and anxiety.
THe iMPOrTance OF inTegraTiOn
the evidence is clear that co-morbid behavioral health conditions worsen the outcomes and increase the costs of care for common chronic physical health conditions2. there is increasing evidence that some approaches to integrating behavioral health and primary care can lead to better outcomes at a reasonable cost—increasing the value of care2,3. a recent actuarial report for the american psychiatric association showed that even modest improvement in the outcomes of chronic illness care as a result of BhI could lead to cost savings equal to the total amount spent on behavioral health care in the U.S. in a year4.
iMPleMenTing BHi
Implementing BhI involves a basic change in the way a practice thinks about and approaches common medical conditions. One way to structure a discussion about how to implement BhI is to use the “three Worlds” approach described by C.J. peek, phD5. Dr. peek suggests that implementation requires attention to the clinical, operational, and financial aspects of the service. here is how mainehealth, a vertically integrated healthcare system, has approached each of those aspects:
clinical: Our initial goal was to create a sustainable model of integration that improved access by primary care patients to behavioral healthcare and improved communication between behavioral health and primary care. Our approach has been to use primarily licensed clinical social workers (lCSWs) as integrated behavioral health clinicians (BhCs), because of their scope of practice and affordability. the lCSW is in the practice at least 20 hours a week in all except the smallest practices. the BhC sees patients with any condition, based on primary care provider (pCp) determination that behavioral health might be helpful.
Clinically, the team uses a focused treatment approach, employing evidence-based, brief treatment models. most patients are seen between three to six times. patients who need longer-term or more intensive treatment are assisted by the BhC to find such services in the community. BhCs are also involved as informal consultants to pCps and other staff members.
28 l capg health Summer 2016
Behavioral Health integration demands Multifaceted approachBY NeIl kOrSeN, mD , mSC , meDICal D IreCtOr, maINehealth
continued on page 44

Fall 2015 capg health l 29
CAPG Annual Conference 2016Sharing the Lessons of Innovative Payment ModelsManchester Grand Hyatt, San Diego
CAPG thanks our premier Conference sponsors for their support!
Diamond SponsorsAetna
Anthem Blue Cross
Blue Shield of California
Cigna
Health Net of California
Humana, Inc.
Molina Healthcare
Novo Nordisk
UnitedHealthcare
OptumCare
Platinum SponsorsAbbVieAlignment HealthcareAllscriptsBlueCross BlueShield Association RowdMap, Inc.
Gold SponsorsathenahealthBoehringer IngelheimJohnson & Johnson Family of CompaniesL.A. Care Health PlanSheppardMullinTalix

30 l capg health Summer 2016
colon cancer screening: Home Testing increases Patient activationBY khUram arIF, mD , mBa; DON hUFFOrD, mD; aND reNee DeBOSe , mD
In the United States, approximately 95,270 new cases of colon cancer are diagnosed annually1. physicians recommending colonoscopies face an uphill battle as patients continue to be concerned about inadequate pain control2. For several years, mercy medical Group (mmG), a Sacramento-based multispecialty medical group working with its partner Dignity health medical Foundation (DhmF), has educated patients in office visits and sent reminder letters for colon cancer screening. Western health advantage (Wha) a well-established health plan in Northern California, has in turn tried mail and phone reminder programs to activate patients. Both efforts met with only modest success.
kaiser permanente, meanwhile, has shown that, within an integrated health system, making testing “easy to do” improves colon cancer screening rates3. Our medical group could see that barriers to colon cancer screening were high, while the health plan realized that patients needed to hear the message from their own physicians. last year mmG/DhmF partnered with Wha to help their difficult-to-activate patients complete colon cancer screening at home. this article will describe our efforts, challenges and results.
We began by identifying a cohort of Wha patients who needed colon cancer screening. these folks had not completed either a fecal occult blood test in the prior year, a sigmoidoscopy in the prior five years, or a colonoscopy in the prior 10 years. they received a letter from their primary care provider (pCp) stating they were due for screening. each letter included a link to colon cancer screening information and phone numbers to schedule educational classes offered by mmG gastroenterologists (GI). patients who did not follow through received two additional reminders over the following four months.
a total of 1,660 patients took no action in response to these educational/reminder letters. We decided to study whether increasing testing convenience might help activate patients to complete colon cancer screening. the concept seemed simple. We would mail the patient a fecal immunochemical test (Quest InSure FIt™) kit to complete at home and mail back to our lab. the lab would process the test and through allscripts (ehr) inform the ordering provider, who would assume the responsibility of follow-up.
We quickly realized that several pieces first had to fall into place. We started with mmG GI providers who enthusiastically supported using FIt. It helped that the Integrated healthcare association accepts use of the FIt as appropriate annual screening. We then worked with primary care leadership to gain support of this concept. the process
“In the United States, approximately 95,270 new cases of colon cancer are diagnosed annually. Physicians recommending colonoscopies face an uphill battle as patients are concerned about inadequate pain control.”

Summer 2016 capg health l 31
involved GI providers who would enter the 1,660 lab orders and schedule appointments for patients with positive (abnormal) FIt results. primary care providers would be copied on abnormal FIt results.
Simultaneously we worked with our lab vendor, Quest Diagnostics, to supply easy-to-understand instructions for patients so they could successfully complete the FIt kit at home. Quest also arranged for mailing to a central facility and kept their personnel informed of this project. Breathlessly, we sent a sample kit through the process. It was mailed to a volunteer, who sent it into Quest. the result went onto allscripts, which notified the ordering provider. everything happened like clockwork! Now all we had to do was execute for all our patients.
all primary care physicians were informed at department meetings about this project. they also received a co-branded letter from mmG/DhmF and Wha. this was important because when patients called their doctor with questions, we wanted physicians in turn to encourage patients to complete the test. Over two weeks, our GI team laboriously entered 1,660 lab orders into allscripts. all lab orders were printed and signed before being sent via hIpaa-secure courier to Wha, who would support us with the mailing. the medical group and the health plan then worked together to design co-branded patient-friendly mailers. patients first received a co-branded card titled “an exam at home” so they would expect FIt kits in the mail. Shortly after, the mailers from the medical group/health plan, with the FIt kit, easy-to-read instructions, a return envelope, and a printed lab requisition from the doctor began to arrive at patients’ homes during Colon Cancer awareness month.
then, nervously, we waited. In the first six weeks we received 128 completed FIt kits. encouraged, over the following three months we sent patients two more reminder letters to complete the FIt kits. Over the next five months we received 281 completed FIt kits for a response rate of 19% in this difficult-to-activate population. We found 16 patients with abnormal FIt results. all patients were notified and 10 patients came in to complete colonoscopies. Interestingly, even among patients with negative FIt tests, another 30 patients came in to complete colonoscopies. the colonoscopy completion rate was 14% in the cohort that received a FIt kit mailed to their home. Of the 10 colonoscopies completed, five had adenomas; the remainder had conditions such as gastritis or internal hemorrhoids, which would not usually lead to cancer (table 1).
Five patients had adenomas, which have variable malignant potential4. If we had saved even one of those patients from developing colon cancer, this project was worthwhile. Since these patients were capitated, and we used our sub-capitated lab vendor (Quest Diagnostics), the FIt kit was
essentially free. Furthermore, in light of a 2009 study that showed mean total colon cancer cost per medicare patient was $29,1965 at one year post-diagnosis, in terms of cost the project was a no-brainer.
Our results showed that colon cancer screening using FIt kits mailed to patients increased activation rates by 17% for completion of a FIt kit. In this subset, 14% patients completed a colonoscopy. Once the necessary legwork to harness synergies has been undertaken, medical groups and health plans can execute successfully on such projects to improve the health of populations.
the feedback comment from one patient says much: “I didn’t know there was something other than colonoscopy; this was so easy.” Currently we are sending out FIt kits for the 2016 year. o
Khuram Arif, MD, MBA, is Medical Director, Managed Care, and Renee Debose, MD, is Division Chief, Gastroenterology, Mercy Medical Group. Don Hufford, MD, is Chief Medical Officer, Western Health Advantage.
We would like to acknowledge Laura Monteil, RN, Health Promotion and Disease Management Manager at WHA, for her invaluable support of this project.
References:
1. Colorectal cancer: Epidemiology, risk factors and protective factors. Macrae, F. UpToDate, Mar 29, 2016.
2. A prospective controlled assessment of factors influencing acceptance of screening colonoscopy. Gavin et al. The American J of Gastroenterology (2002) 97.
3. Colorectal cancer screening: preventing a deadly disease. Kaiser Permanente Policy Stories, Vol 4, No. 1.
4. Approach to the patient with colonic polyps. Ahnen et al. UpToDate, Feb 06,2015.
5. Colon cancer treatment costs for Medicare and dually eligible beneficiaries. Zhehui et al. Health Care Financing Review, Fall 2009/Volume 31, Number 1.
table 1. colon cancer screening using Home mailing fit kits
Metric Totals
patients mailed a FIt kit 1660
patients who returned the completed FIt kit 281
patients with negative FIt results who completed colonoscopy
30
positive FIt results – Colonoscopies completed
– Colonoscopies with adenomas (tubular, tubolovillous, villous or hyperplastic)
– Colonoscopies with other findings
– patients with positive FIt results who didn’t complete colonoscopy
1610
5
5
6

32 l capg health Summer 2016
CapG member Spotlight40 Years in the Wilderness: a medical Group’s managed Care Journey
austin regional Clinic (arC) brought managed care to Central texas in 1980 when we contracted with pruCare, the health maintenance organization (hmO) division of the prudential Insurance Company of america. Back then, prudential was the equivalent of
Unitedhealthcare today—the largest and most dominant commercial health insurance company across the country.
at that time, prudential was developing group model hmOs in Sun Belt cities, like austin, that had never been exposed to any payment mechanism other than fee-for-service (FFS). Consequently, no one in austin, texas, even knew how to spell “hmO.” Nevertheless, the moment was right and patients and employers embraced the concept.
arC spent the next two decades providing high-quality, cost-effective, capitated care to our community. at the peak of our hmO contracting, we served approximately 80,000 commercial lives through six national and regional hmO contracts.
But by 1999-2000, the bloom was off the rose. hmO jokes were de rigueur for every stand-up comedian in the country and closed panel health plans were in retreat everywhere. arC found ourselves increasingly isolated in the medical community as specialty groups and hospital systems exited managed care reimbursement mechanisms to return to pure FFS contracts that relieved them of the risk and responsibility of managed care arrangements.
By the year 2000, we made the decision to methodically reduce our exposure to capitation and return to a FFS universe. We were able to negotiate generous FFS reimbursements by virtue of our size, market share, and a physician culture that tilted towards evidence-based and cost-effective care. By 2001-2002, arC had exited all of
our capitated arrangements. the decade of the “aughts” (2001-2010) was spent growing our medical group under FFS contracts.
It was back to the future in 2011, following the passage of the affordable Care act (aCa), when arC was presented with the opportunity to participate in a very large commercial patient-centered medical home (pCmh) and a hospital-sponsored medicare pioneer accountable Care Organization (aCO). the key in both of those opportunities was our ability to negotiate for care management fees that allowed us to begin rebuilding the necessary infrastructure to manage cost and quality that we had abandoned a decade earlier.
In mid-2011, the arC medical home Department, with five staff members, was commissioned to develop the It infrastructure of a clinical data repository in order to receive and blend claims data from health plans and medicare with clinical data from epic, our electronic medical records system. We added nursing staff to educate and provide navigation for at-risk patients and outreach staff, with the goal of utilizing our recently purchased customer relations management software to contact patients and close care gaps.
Over the past five years, we’ve grown our pCmh and aCO patient population to approximately 160,000 attributed patient lives embedded in 10 different contracts. We’ve had the good fortune to have negotiated and received care management fees of almost $12 million over a five-year period, allowing us to develop a robust 65-person medical home department.
We have saved medicare, employers, and payers over $40 million (in aggregate) through these arrangements. arC has received approximately $11 million in cost-of-care savings payments. We are currently positioned to increase our pCmh population from the current 160,000 patients to nearly 190,000 by year-end 2016.
regardless of these giddy numbers, there is a need for sober reflection. the $11 million in cost-of-care savings we’ve received over the past five years only represents
BY NOrmaN h . CheNVeN, mD , aUSt IN reGIONal Cl IN IC
continued on page 46

Summer 2016 capg health l 33

Pharmacists on the interdisciplinary care Team
the myriad of evidence available to support pharmacist integration into interdisciplinary care teams has called CapG and ralphs pharmacy into action. as the leading association nationwide representing physician organizations practicing coordinated care, CapG has chosen to play a principal role in elevating awareness and understanding of the expansive and valuable role pharmacists play in improving health, as well as lowering healthcare costs. as a result, CapG has initiated a project entitled pharmacists on the Interdisciplinary Care team: the Value pharmacists Bring to Improving health & healthcare. the mission is to communicate the proven impact pharmacists make on patient health, cost of care, and healthcare quality in chronic disease and medication management. through new collaborations with partners to expand this network, we hope to identify promising pharmacy practices within integrated care teams to initiate and develop these relationships.
Community pharmacy practice has evolved from a traditional role of medication dispensing to direct involvement in critical patient care decisions. pharmacists now conduct health and wellness screenings, provide clinical services (travel medicine, disease management, naloxone), and work with members of an integrated healthcare team.1 as medication experts, pharmacists offer valuable medication and disease management services in coordinated, integrated care teams.
pharmacist-provided direct patient care has resulted in favorable therapeutic and safety outcomes for disease management. this involvement has also improved medication adherence, patient education, and quality of life.2 healthcare models that incorporate clinical pharmacy services, such as comprehensive medication management (Cmm), further exemplify the value of pharmacists in a team-based approach. a study with the USC School of pharmacy and altamed health Services showed that when pharmacists were incorporated into practice and provided Cmm services with full prescriptive authority, they were able to identify and resolve additional medication-related problems. Similarly, pharmacists working within the Greater Newport physicians ambulatory Care team achieved impressive therapeutic goals through medication management and therapy changes.3 In a subsequent study exploring the economic outcomes related to team-based care, a pharmacist-managed anticoagulation service resulted in $3,697 savings per patient.4
ralphs pharmacy has been a pioneer in promoting services that advocate the collaboration of the patient-physician-pharmacist triad. For example, the american pharmacists association (apha), medimergent and the U.S. Food and Drug administration (FDa) have a created a novel platform titled the National medication Safety, Outcomes, and adherence program (NmSOap). ralphs pharmacy, as part of a larger chain of kroger pharmacies, has been an initial retail chain partner for NmSOap. NmSOap brings patients, pharmacists, physicians and regulators together to improve safety, adherence, and health outcomes with novel oral anticoagulants through pharmacist-reviewed patient experience surveys. the platform will also be expanding to other drug classes in the near future, including medications used to treat hypertriglyceridemia.
34 l capg health Summer 2016
paid sponsorship
karIN kharlOUBIaN, USC/ralphS pharmaCY reSIDeNt | reBeCCa CUpp, rph, Vp OF pharmaCY, ralphS GrOCerY COmpaNY | lOrD
SarINO, pharmD, ClINICal SaleS maNaGer, ralphS pharmaCY | elISSa k. maaS, mph, prOJeCt DIreCtOr , pharmaCIStS ON the
INterDISCIplINarY Care team: the ValUe pharmaCIStS BrING tO ImprOVING health & healthCare

Summer 2016 capg health l 35
ralphs pharmacy has also taken the initiative to further expand the role of community pharmacists in promoting healthcare quality and defining payment models for outcome-based mtm services. ralphs pharmacy has contracted with Inland empire health plan (Iehp) in their pay-for-performance (p4p) program, one of the first large-scale pharmacy p4p programs in the US. With p4p, pharmacies are incentivized for positive performance on a predefined task or goal, similar to physician payment structures. Iehp utilizes pharmacy Quality Solutions for measurement metrics that are endorsed by CmS for part D Star ratings. ralphs pharmacy understands the importance of outcomes-based care management in validating the role of community pharmacists as interdisciplinary care team members and in promoting a cost-effective delivery system.
this current, CapG-led, physician-pharmacist collaboration will lead to high quality, coordinated, patient-centered care with positive patient outcomes. With support from CapG members, associated organizations, and pharmacist associations, pharmacists being part of interdisciplinary care teams will become a new standard of healthcare.
references
1 F.Isasi and E. Krofah. The Expanding Role of Pharmacists in a Transformed Health Care System. National Governors Association Center for Best Practices. Washington, D.C., January 13, 2015.
2 Chisholm-Burns MA, Lee JK, Spivey CA, et al. US Pharmacists’ Effect as Team Members on Patient Care. Systematic Review and Meta-Analyses. MedCare. 2010; 48(10): 923-33.
3 Butler A, Dehner M, Gates RJ, Shane P, Chu M, DeMartini L, Stebbins M, Nunez de Ybarra JM, Peck C, McInnis T, Chen S. 2015. California Department of Public Health. Comprehensive Medication Management Programs: Description, Impacts, and Status in Southern California, 2015. Sacramento, California.
4 Hall D, Buchanan J, Helms B, et al. Health Care Expenditures and Therapeutic Outcomes of a Pharmacist-Managed Anticoagulation Service Versus Usual Medical Care. Pharmacotherapy 2011; 31 (7): 686-694.
TAKE ON RISK:HOW TO THRIVE INRISK-BASEDCOORDINATED CARE
What do you need to know to take on risk?
Gain hard-earned insights from highly
experienced physicians and executives.
October 27, 2016 • 9:00am-4:00pm Hyatt Regency O’Hare, Chicago
REGISTER NOW!capg.org/symposium

36 l capg health Summer 2016
improving Medication adherence and Patient Health using the appointment-Based Model
medication adherence is critical in managing patients with chronic disease, not only to improve health outcomes but also to reduce healthcare costs. pharmacies are able to help reduce medication non-adherence rates by implementing a strategic refill process referred to as the appointment-based model (aBm). aBm is a patient care program designed to engage and help patients better manage their health through medication adherence. Instead of passively filling prescriptions as patients call in medications, pharmacy staff utilize a procedure called medication synchronization to proactively care for patients’ medication and health needs. Further, unlike traditional medication synchronization programs, aBm includes greater participation and better patient care from the pharmacy staff and assists physicians in managing their patients’ health.
the aBm workflow begins with a phone call to the patient four to seven days before a patient’s “sync date,” a set date in which all of the patient’s chronic medications are synchronized and ready for pick up. During the phone call, a pharmacy staff person reviews all the medications the patient is currently taking in a comprehensive manner. this allows the pharmacist to
inquire about any medication changes, new or discontinued prescriptions, and medication adherence. If a patient states that a chronic medication is “not needed,” the pharmacist can delve further and assess for possible non-adherence. additionally, this conversation with the patient allows time to further address any medication issues such as side effects or concerns about the patient’s current medication regimen. acknowledgement of all medications needed prior to the patient’s sync date provides the pharmacist with time to contact prescribers only once for any refill authorizations and to acquire any out-of-stock medications.
Traditional Model (Left): passively refill prescriptions as patient calls them in. Appointment Based Model (Right): actively synchronize and refill prescriptions for patients each month.
there are a number of benefits to aBm for physicians, patients, pharmacies and health plans. aBm helps physicians by consolidating contact with the pharmacy, improving medication adherence, and opening avenues of communication between the patient, pharmacist, and physician regarding adverse events. In addition, having a single sync date each month is convenient for the patient since it reduces the number of phone calls for refills, trips to the pharmacy each month, and stress associated with managing medications. aBm benefits the pharmacy by streamlining workflow, increasing prescription volume, reducing “waiters,” reducing out-of-stock issues, reducing medications not picked up, and allowing more time for clinical services such as independently furnishing naloxone, medication therapy management, providing travel clinic and smoking cessation consultations, and administering immunizations. lastly, health plans benefit by increasing adherence of life-saving medications, and achieving quality measures such as Star ratings.
thrifty White, a pharmacy chain in the midwestern United States, performed a study that measured medication adherence in patients enrolled in aBm. proportion of days covered (pDC) was used as a surrogate measure for medication adherence (as is a standard in these studies). pDC is measured as a ratio of days covered by medication received divided by the number of days in the period being measured. Six chronic medication classes were included and more than 600 hundred patients were enrolled in aBm. the average pDC for regular patients was 0.61 whereas for aBm patients it was 0.84 (p <0.01)1.
continued on page 46paid sponsorship
BellamaY mONteSa | COreY eDWarDS | lOrD SarINO, pharmD, ClINICal SaleS maNaGer, ralphS pharmaCY | reBeCCa CUpp, rph,
Vp OF pharmaCY, ralphS GrOCerY COmpaNY

Summer 2016 capg health l 37
EARLEarl doesn’t just love to ride, he lives to ride. After multiple visits to the hospital for numerous
chronic conditions, Earl needed a solution to improve his health. The solution was InnovAge Care Management (ICM). ICM worked with his providers to assess and coordinate
his care needs. They improved his medication adherence and appointment compliance, which resulted in reduced hospital re-admissions. ICM even coordinated therapeutic riding
lessons to improve his strength. Today Earl is back in the saddle. This is life on your terms.
InnovAge Care Management• Comprehensive Case Management• Care Assessments and Planning• Medication Management• Interdisciplinary Team (IDT) Consultation• Transitional Care Management • Re-admission Reduction
855.487.6768MyInnovAge.org
YOUR PARTNER TO REDUCE COSTS AND IMPROVE OUTCOMES
Paid Actor Portrayal
To le
arn m
ore,
please
visit
us
at the
Inno
vAge
exhib
it sp
ace
Booth
#508

38 l capg health Summer 2016
Primary care at a crossroadsBY marC mertz , mha , FaCmpe, Ge healthCare CamDeN GrOUp
most primary care practices still operate based on a model developed decades ago: the hours of operation, appointment scheduling rules, staffing, patient flow, and office design were all determined based on physician preference. In an attempt to provide physicians with a more convenient practice model, we created a system that forced patients to accept long waits for appointments, inefficient office flow, and limited ability to communicate with their physicians outside of the exam room.
Yet physicians hardly fared any better in these offices that were actually designed with them at the center. Complex appointment scheduling rules and templates inherently led to mistakes and double booking, phone messages piled up, administrative work increased, patient appointment ran behind, and physicians inevitably spent hours working in the clinic long after patients had left.
While the typical primary care practice doesn’t really work for patients or physicians, in the absence of alternatives, we came to accept this model for what it was. But times are changing. a plethora of new providers are entering the primary care marketplace, and their growing popularity is as much an indictment on traditional physician-centric primary care practices as it is a reflection of new reimbursement models and rising consumerism.
retail clinics, concierge practices, virtual visits, urgent/immediate care clinics, and even home visits are popping up everywhere. they offer patients everything that yesterday’s primary care practice doesn’t: immediate access, expanded hours, high levels of service, advanced technology, and the ability to communicate freely with physicians. more and more patients are choosing to receive primary care and, in some cases, specialty care, from these new providers. as they do, the traditional primary care office is at risk.
primary care practices today are at the proverbial fork in the road. they can choose to continue on the path they are on, or they can choose to veer off and adapt to a changing environment. patients now expect more—which is only natural as high-deductible plans require they pay more of the bill. and patients now compare the service they receive in their doctor’s office to other industries, including retail, hotels, restaurants, and other consumer services. they want to access their doctor when, where, and how they want. they want to email or text their doctor and actually hear back from her or him. they want options and choice. No one is going to wait three weeks for an appointment anymore. they aren’t going to take a day off of work for their annual physical. they will simply get care somewhere else, and they might not come back.
So where should a practice start? the short answer is everywhere. the longer answer is to start with office operations, because an office that runs smoothly and on time is the foundation for happy patients, staff, and physicians. and there is no sense in increasing patients’ access to an office that doesn’t work. Start by conducting time studies. assess the workflow and processes in your office to identify ways to reduce waste and bottlenecks. push work down so that everyone is working to the top of his or her license or ability. physicians should be leading care teams that comprise nurses, medical assistants, nurse practitioners, physician assistants, pharmacists, social workers, care coordinators, and more. Design new work flows with patients in the center so that staff, equipment, and physicians come to them rather than having patients move around the office.
Consider the physical layout of your office and whether it contributes to efficiency or causes a barrier. What impression does your office décor make on patients? While a full-office
“Primary care practices have changed little in a half century, while the world around them changes every day. The reality is, many new providers are lining up to take care of your patients.”

Summer 2016 capg health l 39
renovation may not be feasible, consider opportunities to improve the ambiance and functionality. Bring equipment and supplies to the patient. Consider open facility designs that are efficient, but also provide a more pleasing environment.
Once operations are improved, think about how patients access care. today, the only way most patients can access a physician is to call the office to schedule an appointment for days or weeks in the future. that is no longer acceptable in a market where patients have alternatives for immediate access to care. Implement a patient portal to allow patients to freely communicate with your office and to schedule—not just request—appointments. primary care practices need to reconsider how they schedule and if the process does or doesn’t work, restricts access, or creates needless extra work for the staff. If patients have questions, allow them to email the office and ensure they get a response quickly, including from physicians. In a delegated model, this is good medicine and business. In a fee-for-service environment, exchanging emails with patient might avoid a revenue-generating office visit, but it gives patients faster access to care and it may avoid potentially losing them to one of the new providers. and chances are plenty of other patients need an appointment that day.
Consider technology that enables virtual visits, especially for after-hours or weekend care. In a risk-based contracting
environment, this can be less expensive than urgent care or the emergency department. Fee-for-service contracts may not allow virtual visits today, but contracts can be negotiated, especially if a practice can demonstrate better care and lower cost. If the costs associated with creating virtual visit capabilities are prohibitive, consider partnering with one of the existing virtual providers. the same model may work for home visits. Your practice may not have the resources to see patients in their home, but home visit providers are expanding in major markets. Why not partner rather than compete with them?
primary care practices have changed little in a half century, while the world around them changes every day. the reality is, many new providers are lining up to take care of your patients. the time has come to transform primary care practices to provide patients with immediate and convenient access to the care they need. In doing so, clinic redesign that addresses broken work flows and surrounds physicians with a care team will allow you to focus on patient care in a more rewarding environment. o
For more information on how to redesign your primary care practice, please contact Marc Mertz, Vice President, GE Healthcare Camden Group, at 310.320.3990 or [email protected].
reserve your sPace in tHe colloQuium sPecial eDition
fall 2016 / colloQuium sPecial eDitiontheme: healthcare policy and alternative payment modelseditorial & advertising Due Friday, august 5
DISCOUNTS AVAILABLE FOR EARLY BIRD RESERVATIONS AND CAPG MEMBERS.
for editorial guidelines contact Daryn kobata [email protected] editorial Departments: Upcoming Events | Names in the News | Member Spotlight
for advertising information : [email protected] Okunami, Publisher 916-761-1853
CA
PG
20
16
Co
llo
qu
ium
is
su
e

40 l capg health Summer 2016
Getting ready to take on risk or already in it?CAPG Consulting can help you accelerate your journey. Our team is composed of executives with
decades of success in risk-based care delivery at leading physician organizations.
consulting
To learn more and get connected with one of our experts, please contact Nelson Maldonado at 213.239.5041 or [email protected]. Visit us online at capg.org/consulting.
C.R. BURKE MARIELLA CUMMINGS ROBERT J. MARGOLIS,MD DONNA J. MILLS CHARLES E. PAYTON,
MD, MBA ROBERT SEVERS BART WALD,MD, MBA
caPG Health: What about accountable care organizations—can they help physicians address quality and cost?
Dr. chandra: the fundamental flaw with aCOs is that they have the hospital at their heart. With this model, hospitals are buying out physician groups, getting bloated, and not improving patient well being, so capitated physician groups aren’t winning. again, physician-based capitation will help a lot in the areas of quality and cost. In the long run, the kaiser permanente model is ideal: massive physician groups holding risk. I’d much prefer experimenting with bundled payments before going straight to aCOs. I can agree with some of the logic of aCOs, but they can’t address market competition—for example, in a city with two aCOs, why would there be any price competition?
caPG Health: You’ve emphasized capitation a few times. Do you believe that’s the answer to the trilemma?
Dr. chandra: Capitation is the key to better healthcare—it is the goal, but we need to start with bundled payments. We must crawl before we walk. as doctors are willing to work under risk-based capitation, physician groups will start looking like insurance companies holding risk, which
The Healthcare Trilemma...continued from page 12 is good—it creates the right incentives. Because of our employer-based healthcare system, the vast majority of risk holders are large employers, but they have no expertise in it—and so we end up spending way too much. at present, private health plans do not hold risk; they only manage claims and that has got to change.
caPG Health: Is there anything we can do to ease physicians’ transition to alternative payment models—bundled payments and ultimately capitation?
Dr. chandra: absent a wave of physician leadership that’s deeply committed to patient value and work, the future is not terribly optimistic for american medicine. We need physicians who are smart and idealistic but pragmatic—those who can stay the course and guide healthcare to where we want it to be in five to 10 years, and are okay with taking small steps to improve quality.
Big-thinking visionaries have a terrific narrative, but that’s not what we need. We need physicians who are willing to change and improve things like orthopedic care, and cancer care. Not ones who are interested in bringing supermarkets to the inner city. We have no idea how to do that, or to get patients to change their behavior, so I’d much rather we stick to improving the things we know and the things in our control. o

Ventegra, Inc., a California Benefi t Corporation450 North Brand Boulevard, Suite 600, Glendale, California 91203858.551.8111, Ext. 109 • www.ventegra.com
Turn to Ventegra for empowerment and transparency.
In your quest for healthcare integration, Ventegra can make the path to becoming yourown PBM painless and profi table. It starts with empowerment and transparency. Our comprehensive suite of programs, including pharmaceutical rebates and discounts, pharmacy network, claims processing, formulary management and customer support allows you to create and manage your own Pharmacy Benefi t Program.
• Ventegra passes along 100% of all rebates/discounts.
• We guarantee – contractually – cost transparency. That’s a given.
• Our claims system seamlessly integrates pharmacy and medical information.
• Our formularies support not only quality care and affordability, but choice, too.
• Through a single, fully-integrated system, we support compliance with both 340B and non-340B programs.
Ventegra, Inc., is a California Benefi t Corporation. We’re the fi rst and currently onlyBenefi t Corporation in the U.S. in the Pharmacy Services Administration space.
To tap into the “new class-of-trade” solution, tap into Ventegra. We not only believe in truth and integrity. We deliver it.
Client: Ventegra #2410Created by: GSS Communiqations, 323.939.1181Publication: CAPGDimensions: 8 1/8” x 10 7/8” trimAgency contact: Andrea Graham [email protected] contact: Marc Shur [email protected] contact: Peggy Frank ([email protected])
Aspiring to become your own PBM?

42 l capg health Summer 2016
So how does this gender pay gap apply to work-life balance? It’s related because female executives share equal attributes and competencies with their male counterparts; however, they are not getting compensated equally because of the time they choose to be away from the office to raise their children. Whether this is fair or not is apparently not relevant to most Fortune 500 corporations. It seems what is relevant is the evaluation of the company by their shareholders.
“Our results point towards the possibility that male and female executives sharing equal attributes neither have the same probability of reaching the top, nor are they paid equally,” the researchers at harvard write. looking at data from the Swedish Companies registration Office and Statistics Sweden, they found that male executives earn 27% more than female executives, on average. the pay gap is smaller at the very top of the C-suite; male CeOs earn only 7.1% more than female CeOs. But while 21% of senior executives in Sweden are women, they account for only 8% of CeOs.
While the study focuses on a single nation, the researchers believe the findings can be generalized to other countries, including the United States. Widely cited for its management practices, Sweden has 24 companies on the Forbes Global 2000 list of largest companies in the world, and on a per capita basis, substantially more Swedish companies are on the list than U.S. companies.
Given these studies and expert testimony, how am I to “lean in” as Sheryl Sandberg recommends in her widely publicized book, Lean In: Women, Work, and the Will to Lead? perhaps if I could afford my own nanny, chef,
personal assistant, and other luxurious amenities, I could “lean in” and have some semblance of a work-life balance. thus, I agree with anne-marie Slaughter in her highly disputed 2012 article, “Why Women Still Can’t have It all”–unless you have a husband like hers who takes on the primary parenting role, and who wrote in the fall of last year about “Why I put my Wife’s Career First.” andrew moravcsik reflected on being a lead parent and not wanting to regret what most men do at the end of life—that they did not lead the caring and connected life they wanted, but rather the career-oriented life expected of them.
I hope that more men will embrace fatherhood as mr. moravcsik does, and perhaps the millennials and generations to come will have a different perspective on work-life balance that will help steer society to believe that such sacrifice and leadership can bridge gender gaps and executive equality and opportunity in our top industries. Otherwise, we will not have progressed as a society and will continue to teach our children to maintain archaic expectations. as Slaughter eloquently stated, “men and women take care of their children, their parents, or indeed their spouses out of the love they bear them. But this love is not treated equally at all, in the workplace or indeed in society as a whole.”
although it may not be easy to lead a purposeful, balanced life at work and at home, one must strive for this each and every day. I try to integrate my work travel schedule into my family’s fun time, so we can make memories together. What I can share with you are three things to motivate you when you’re overwhelmed by work, kids, your spouse/partner, or other life demands:
• ShOW Up—no matter how hard it is to get out of bed, fight traffic, etc. Just show up.
• FOrGIVe YOUrSelF for minor mistakes and errors—they’re bound to occur when you’re maximizing your efforts and trying to do everything for everyone at the same time.
• GIVe—of your time, your money, your ideas, so that you get the benefit of helping yourself. You’ll feel good about yourself, and this will lead to positivity in other areas of your life.
I would like to envision a day when we reduce the cost of temporal flexibility, and more and more people in the workforce demand flexible hours and a work-family balance. Only then will we possibly move to equality for all working americans—both in compensation and in having a balanced career that doesn’t sacrifice family and personal needs. o
WOMEN IN S&P 500 COMPANIES
CEOS
4.0%
BOARD SEATS
19.2%
EXECUTIVE/SENIOR•LEVELOFFICIALS AND MANAGERS
25.1%FIRST/MID•LEVEL
OFFICIALS AND MANAGERS
36.8%
S&P 500 LABOR FORCE
45.0%
Sources
Catalyst, Women CEOs of S&P 500 (2015)
Catalyst, 2014 Catalyst Census Women Board Directors (2015)
U.S. Equal Employment Opporttunity Commission (EEOC). “2013 EEO-1 Survey Data.”
S&P 500 is owned by S&P Dow Jones Indices LLC.
This work is licensed under a Creative CommonsAttribution-NonCommercial 4.0 International License
catalyst.org
Women in S&P 500 Companies
Work-Life Balance...continued from page 18

Working With PAs in Team Practice
New Legislation in 2016 Means Working with PAs Has Never Been Easier! Documentation Requirements Are
Now Customizable and Streamlined.
CONTACT US
Learn More About Adding a PA to Your Practice!
Teams may now decide if medical record review meetings, chart review or a combination of both are best suited for their particular setting and team.
As of January 2016, physicians may choose to countersign a minimum of 20% of CII medical records (reduced from 100% previously) when the PA has completed a Controlled Substances Education Course, such as CAPA’s.
Post a Job at www.capanet.org
California Academy of PAs2318 S. Fairview St., Santa Ana, CA 92704-4938Ph: (714) 427-0321 Fax: (714) 427-0324 www.capanet.org

Behavioral Health Integration...continued from page 28
BhCs receive supervision from an experienced lCSW monthly and as needed and also meet with a consulting psychiatrist monthly to discuss challenging patients. In addition, BhCs gather as a group quarterly for a day designed to add to their clinical skills and to develop camaraderie and learn from each other.
operational: Successful implementation of BhI depends on attention to important operational details before the integrated BhC arrives, during the early days of integration, and ongoing for years. Our approach has been to work with practice operational staff throughout the process, with the goal of maintaining shared responsibility for the success and growth of the BhI program.
Before integration starts, our job is to help practice staff understand what the BhC can (and can’t) do, and what the BhC’s role will be in the practice. Some staff members will have to learn specifics about billing and scheduling for behavioral health services. the integrated BhC may need to be credentialed with one or more health plans.
Once the integrated BhC begins working in the practice, some of the operational focus has to be on helping the BhC with the clinical model of focused treatment, which may be different from how they are used to providing care. primary care operational leadership continues to be closely involved in monitoring and troubleshooting implementation. In each region, program leadership meets monthly with regional leaders and practice leaders to review program performance.
these monthly meetings sometimes include review of data about the program. available data about productivity, access and show rate has been limited. We are working on developing a broader dashboard of measures to understand how the integrated BhCs are being used and what impact they are having on the value of care. Our goal is to add measures of clinical outcomes, experience of care (for patients and providers/staff) and cost of care.
financial: Integrated BhCs are hired by maine Behavioral healthcare, a regional behavioral health organization that is part of mainehealth. they are then contracted to practices for,in most cases, 20 to 40 hours per week. the practices bill for services, assisted by our staff, with the goal of collecting enough to cover their costs. We charge the practice organization a management fee for our role in implementing and supporting the BhI service.
most billing uses mental health codes. Some providers use health and behavior codes, which are specifically designed to use when a BhC is providing treatment for the behavioral or emotional aspects of physical health problems. Unfortunately, there are limits that vary by health plan on which types of clinicians can bill these codes. that makes the use of these otherwise important codes challenging for primary care organizations.
nexT sTePs: clinical PaTHWays
Our BhI program faces two important directions in the next few years. One is to develop clinical pathways targeting high-priority populations that might benefit from behavioral health input. We are starting with people with common behavioral health conditions comorbid with common chronic physical health conditions, as well as those with chronic pain and substance abuse problems. Other target populations will be identified over time.
We are also increasingly being asked to integrate behavioral health services in specialty settings. this partly overlaps with the focus on common chronic illnesses, with diabetes and heart failure being two of the populations we are being asked to serve in specialty settings. these initiatives recognize that people with serious illnesses experience psychosocial issues and might benefit from behavioral health services.
Behavioral health integration is an important and feasible approach to being ready for a pay-for-value world. attention to the clinical, operational, and financial aspects of implementation will help you to do so successfully. and successful implementation will lead to better care experiences and better outcomes.
the ahrQ playbook — a resource that can be helpful to your organization, if you are thinking about or working on integrating behavioral health into ambulatory care settings—will soon be available on the ahrQ academy for Integrating Behavioral health and primary Care website. this interactive set of tools will guide your organization through the process of planning and operationalizing integration6. o
Neil Korsen, MD, MSc, is Medical Director, Behavioral Health Integration Program, at MaineHealth. He will present a CAPG Annual Conference breakout session, “Integrating Behavioral Health into Primary Care,” on Saturday, June 18, at 2:15 pm.
references
1. Peek, CJ and the National Integration Academy Council—”Lexicon for Behavioral Health and Primary Care Integration: Concepts and Definitions Developed by Expert Consensus,” AHRQ Publication No. 13 – IP001-EF. Rockville, MD,Agency for Healthcare Research and Quality. 2013. Available at: http://integrationacademy.ahrq.gov/sites/default/files/Lexicon.pdf
2. Kathol, deGruy, and Rollman. Value-Based Financially Sustainable Behavioral Health Components in Patient-Centered Medical Homes. Annals of Family Medicine 2014: pp.172-175.
3. Butler, Kane, McAlpine et al. Integration of Mental Health/Substance Abuse and Primary Care. NO. 173 (Prepared by the Minnesota Evidence-based Practice Center under Contract No. 290-02-0009) AHRQ Publication No. 09-E003. Rockville, MD. Agency for Healthcare Research and Quality, October 2008.
4. Melek, Norris, and Paulus. Economic Impact of Integrated Medical-Behavioral Healthcare: Implications for Psychiatry. Prepared for the American Psychiatric Association by Milliman, Inc. Accessed at https://www.psychiatry.org/psychiatrists/practice/professional-interests/integrated-care .
5. Peek and Henrich. Building a Collaborative Healthcare Organization: From idea to invention to innovation. Family Systems Medicine 1995: Volume 13, pp.327-342.
6. https://integrationacademy.ahrq.gov/
44 l capg health Summer 2016

WELCOME BACK TO HEALTH CARE
As a physician, balancing value-based care with fee-for-service business can feel like navigating the uncharted West.
Evolent Health partners with physician groups and health systems to navigate the changing terrain of health care, enabling physicians to design and lead a new model of quality care delivery. Yes, you can overcome operational obstacles and seize opportunities to accelerate success in this new value landscape. We can help you put patients back at the center of care.
Embrace the adventure of value. Visit Evolent at the CAPG Annual Conference or at evolenthealth.com/CAPG
Changing reimbursement models. Shifting payer-provider relationships. Emerging government mandates.

46 l capg health Summer 2016
a similar study, conducted at ralphs pharmacy, compared medication adherence rates of patients on chronic medications for hypertension, diabetes, or dyslipidemia between the aBm program and automatic medication refill process. automatic refill is a more traditional method for using pharmacy software to increase adherence. this process was designed to passively fill medications three to five days before they are due. It is losing favor due to several reasons, however, including: 1) maintaining staggered dispensing schedules, 2) reduced personal touch, 3) an emphasis on sales as opposed to appropriate medication use, and 4) the frequency of discontinued medications being refilled.
the results of this investigation demonstrated significantly greater mean pDC for patients on aBm than those on automatic refill (0.9-0.91 vs. 0.96-0.97, p-values < 0.05) (table 1). Furthermore, the percentage of patients who were considered adherent to therapy (i.e. pDC ≥ 0.8) was greater in the aBm group than patients on automatic refill, achieving the Centers for medicare & medicaid Services (CmS) five-star goal for adherence to raSa therapy, statin therapy, and oral diabetes medication therapy (Figure 1). It was also observed that influenza immunizations were doubled for patients in the aBm group, though recommending flu shots was not in the aBm protocol. this is a likely benefit of actively reviewing therapy and having regular contact with patients about their care.
table 1. Proportion of Days covered
autofill aBmpn pDC
(mean ± SD)n pDC
(mean ± SD)
raSa therapy 122 0.91 ± 0.16 41 0.97 ± 0.09 0.02
Statin therapy 109 0.91 ± 0.15 47 0.96 ± 0.07 0.03
Oral Diabetes therapy
77 0.90 ± 0.15 35 0.96 ± 0.10 0.04
Improving Medication Adherence...continued from page 36
about 1% of our top line revenue. this is not a business model to write home about.
• the attribution logic for each of our 10 contracts is unique to each payer, and we are unable to audit their logic or performance.
• the quality metrics we are held to include dozens and dozens of different parameters and, as if to add insult to injury, the heuristics utilized for the same parameters often vary from plan to plan. What that means is that we spend more energy managing the contracts than we spend managing patient care.
• We have concluded that pCmh and aCO models are transitional models at best. Unfortunately, the premium available from medicare advantage in austin is low; thus, there is not adequate arbitrage to make medicare
40 Years in the Wilderness...continued from page 32 advantage the foundation for a managed care program, as it is for many of the most successful managed care groups.
In summary, austin regional Clinic is currently in the 36th year (1980-2016) of our quest to manage the cost and quality of the healthcare we deliver to our patients. It’s been a rollercoaster ride from managed care to fee-for-service and back to managed care, but arC hasn’t yet arrived at the promised land.
and so the journey continues. o
Norman H. Chenven, MD, founder and CEO of the Austin Regional Clinic, can be reached at [email protected] or 512.231.5514. He will present a breakout session, “40 Years in the Wilderness: One Medical Group’s Managed Care Journey,” at the CAPG Annual Conference on Saturday, June 18, 10:45 am.
figure 1. Percent of Patients adherent to therapy
percent of patients adherent to raSa therapy (CmS 5-Star Goal ≥ 85%)
percent of patients adherent to statin therapy (CmS 5-Star Goal ≥ 83%)
percent of patients adherent to oral diabetes therapy (CmS 5-Star Goal ≥ 81%)
the value of the aBm program on medication adherence is evident in these studies as the monthly phone call to the patient provides an opportunity to educate, engage, problem solve, and reinforce the importance of adherence. Furthermore, the workflow benefits of efficient communication between physicians and pharmacies lead to greater patient satisfaction and health. the appointment-based model allows patients, physicians, and pharmacists to work together to solve any medication-related problems and improve medication adherence as well as health outcomes. o
References
1. Holdford, David and Inocencio, Timothy. Appointment-Based Model (ABM) Data Analysis Report. Prepared for Thrifty White Pharmacy. Virginia Commonwealth University.

DermatologyGastroenterologyRheumatology
Building a better tomorrow today Janssen Immunology: Finding a path forward togetherAs an established immunology category leader, we are committed to fi nding new ways to improve patient outcomes and economic results with our immunology products and expertise.
Janssen has unbranded resources and category expertise to help you manage your immunology patient population. To learn more, please contact your Janssen Account Management Director.
© Janssen Biotech, Inc. 2016 03/2016 047044-160208

Value Based Care: Today and Tomorrow The healthcare industry has been moving from “volume to value,” placing more emphasis on coordinating care and delivering better outcomes in the most appropriate and cost effective settings.
That’s a good thing. Improving quality and reducing costs is not a trend at Brown & Toland Physicians. It’s part of our DNA. As one of the first medical groups in the country to implement electronic health records in our physicians’ offices, we have developed system-wide population health management programs and delivered positive results.
Taking a team approach, our managers work closely with our physicians to develop successful programs and education for specific patient groups. These programs have helped improve preventive screening rates, reduced hospital stays, and have resulted in fewer hospital readmissions.
Using predictive population health analytics, Brown & Toland Physicians has advanced care in a variety of accountable care programs for HMO and PPO patient populations. We will continue to provide proprietary solutions to help our physicians deliver value-based care, as this type of care is good for our patients today, as well as tomorrow.
To learn more about Brown & Toland Physicians, please visit our website at brownandtoland.com.
Keeping the San Francisco Bay Area healthy for more than 20 years
brownandtoland.com