-
Seediscussions,stats,andauthorprofilesforthispublicationat:http://www.researchgate.net/publication/40847354
ThecriticalroleofvitaminB12.ARTICLEinTHEPHYSICIANANDSPORTSMEDICINEDECEMBER2008ImpactFactor:1.49DOI:10.3810/psm.2008.12.9Source:PubMed
DOWNLOADS32
VIEWS169
1AUTHOR:
IliaVolkovBen-GurionUniversityoftheNegev15PUBLICATIONS94CITATIONS
SEEPROFILE
Availablefrom:IliaVolkovRetrievedon:18June2015
-
THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December 2008,
No. 1, Volume 36 1
CLINICAL FOCUS: NUTRITION
IntroductionVitamin B12 plays a functional role in a growing
list of various organs and body systems. Vitamin B12 deficiency is
a common problem. Early detection of vitamin B12 deficiency is
essential in order to prescribe opportune treatment, and there is
evidence that such deficiency occurs more frequently than expected.
Vitamin B12 deficiency can occur in individuals with dietary
patterns that exclude animal food products and patients who are
unable to absorb vitamin B12. Vitamin B12 deficiency has many
causes, and pernicious anemia has been described as a widespread
cause of vitamin B12 deficiency. Current studies on vitamin B12
deficiency, including more precise definitions and the description
of new etiologies of vitamin B12 deficiency, such as insufficient
dietary intake,1 food-vitamin B12 malabsorption syndrome,27 and
hereditary vitamin B12 metabolism diseases, such as
Imerslund-Grasbeck syndrome,8 show that hematological abnormalities
are generally incomplete, as compared with historical
descriptions.
Persons with B12 deficiency may be asymptomatic, but in patients
presenting with myelopathy, cognitive decline, neuropathy,
psychiatric disturbances, or specific hematological signs and
symptoms, vitamin B12 deficiency should be suspected.
The author will demonstrate the critical roles of vitamin B12 by
surveying and analyzing available reports, as well as reporting
personal clinical experience.
Vitamin B12 and DevelopmentMany research studies emphasize the
health complications of nutritional vitamin B12 deficiency and a
necessity of clinical, biochemical, and metabolic monitoring in
infants born to mothers with a vita-min B12 deficiency. Dietary
deficiencies of vitamin B12 during pregnancy and lactation may
result in health problems in exclusively breastfed infants.
Physical examinations of these children often reveal psychomotor
retardation, apathy, muscular hypotonia, irritability, anorexia,
abnormal movements, and failure to thrive. Laboratory analyses show
hematological abnormalities, such as a megaloblastic anemia, low
levels of vitamin B12, high levels of homocysteine and
methylmalonic acid, and methylmalonic aciduria. Magnetic resonance
imaging (MRI) of the brain reveals diffuse
frontotemporoparietal
The Critical Role of Vitamin B12
Ilia Volkov, MD
Abstract: Vitamin B12 affects the peripheral and central nervous
systems, bone marrow, skin and mucous membranes, bones, and
vessels, as well as the normal development of children. Although
there is undoubtedly an association between vitamin B12 and
homo-cysteinemia, their relative influence on cardiovascular events
is controversial.
Some large studies confirm that a supplementation with group B
vitamins did not reduce the risk of major cardiovascular events
or all-cause mortality in patients with vascular disease. The
outcomes of these and similar trials could have been different had
the
researchers considered the following points: Using vitamin B12
or B-complex as secondary prevention of cardiovascular events
for
patients with irreversible changes of blood vessels is probably
in error. Rather, vitamin B12 or B-complex should be used as
primary
prevention. Also, using high doses of vitamin B12 will probably
be more effective than using low doses of group B vitamins.
The effect of vitamin B12 on the proliferation of malignant
cells has been examined in vivo and in vitro in numerous studies.
Their
results indicate that methylcobalamin inhibits the proliferation
of malignant cells and propose the possibility of methylcobalamin
as
a candidate of potentially useful agents for the treatment for
some malignant tumors.
There are many articles indicating the increasing prevalence of
low vitamin B12 level in different segments of general
population.
In order to prevent serious health problems, vitamin B12 routine
fortification should be seriously considered and discussed.
Keywords: vitamin B12; homocysteine; malignancy; vitamin B12
routine fortification; recurrent aphthous stomatitis
Ilia Volkov, MD1
1Department of Family Medicine, Faculty of Health Sciences,
Ben-Gurion University of the Negev, Beer-Sheva, Israel
Correspondence: Ilia Volkov, MD Hogla Street 6,
Lehavim, 85338, Israel Tel: 972-8-6431530 Fax: 972-8-6413135
E-mail: [email protected]
Conflict of Interest Statement: Ilia Volkov, MD
discloses no conflicts of interest.
-
Ilia Volkov
CLINICAL FOCUS: NUTRITION
2 THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December
2008, No. 1, Volume 36
atrophy and retardation of myelination.9 Some studies have shown
a relationship between maternal vitamin B12 status and birth
weight. One extends those findings directly in terms of neonatal
vitamin B12 status and birth weight. Vitamin B12 status in the
mother was related to neonatal vitamin B12 status as measured by
cord serum vitamin B12 concentra-tion. In addition, low neonatal
vitamin B12 concentrations were adversely associated with low birth
weights.10 Marginal maternal vitamin B12 status increases the risk
of an offspring with spina bifida.11
Children have specific and increased nutritional require-ments
in comparison with adults. Rapid growth and enhanced energy
expenditure explain these differences. Any diet devia-tion will
increase exposure to the risk of nutritional deficiency along with
corresponding health consequences. Whenever a diet restriction for
children is required for medical reasons, particular attention must
be paid to the food regimen in order to avoid any health problems,
especially growth retardation.12
Vitamin B12-Responsive Neuropsychological ConditionsThe only
function that has been indicated as unique for vitamin B12 is the
synthesis of myelin, a component of the sheaths that protect nerve
fibers. Vitamin B12 deficiency can cause peripheral neuropathy and
combined system diseases involving demyelination of the dorsal
columns and the corticospinal tract. A wide variety of
neuropsychological symptoms and signs have been encountered, such
as ataxia, loss of cutaneous sensation, muscle weakness, diminished
or hyperactive reflexes, spasticity, urinary or fecal incontinence,
orthostatic hypotension, loss of vision, dementia, psychoses, and
disturbances of mood. Multiple neurological syndromes were often
seen in a single patient. Severity of neurological dysfunction
before treatment is clearly related to the duration of symptoms
prior to diagnosis.13
Multiple sclerosis (MS) and vitamin B12 deficiency share common
inflammatory and neurodegenerative pathophysi-ological
characteristics. Due to similarities in the clinical presentations
and MRI findings, the differential diagnosis between vitamin B12
deficiency and MS may be difficult. Additionally, low or decreased
levels of vitamin B12 have been demonstrated in MS patients.
Moreover, recent studies sug-gest that vitamin B12, in addition to
its known role as a cofac-tor in myelin formation, has important
immunomodulatory and neurotrophic effects. These observations raise
questions
of possible causal relationship between the two disorders, and
suggest further studies of the need to closely monitor vitamin B12
levels in MS patients, as well as possibly requiring
supplementation of vitamin B12 alone or in combination with the
immunotherapies.14 Interferon-beta is a mainstay therapy of
demyelinating diseases, but it has only a partial effect on MS in
humans and in several animal models of the disease. In a recent
report, the author demonstrated a dramatic improve-ment in the
clinical, histological, and laboratory parameters of disease in in
vivo mouse models of demyelinating disease. This was seen following
combination therapy with inter-feron (IFN)-beta and vitamin B12
cyanocobalamin (B12CN) in nonautoimmune primary demyelinating ND4
(DM20) transgenic mice and in acute and chronic experimental
auto-immune encephalomyelitis in mice. Clinical improvement,
manifested as near normal motor function, was associated with
reduced astrocytosis and demyelination. Interferon-beta-B12CN
combination therapy may be promising for the treatment of MS.15
The association of vitamin B12 deficiency with psychiatric
illness has been studied and debated since the vitamin was first
discovered in the 1940s. The clinical relevance of this deficiency
remains the subject of investigation and academic discussion.
Vitamin B12 has fundamental roles in brain function. Intracel-lular
vitamin B12 is converted to adenosylcobalamin, coenzyme for
methylmalonyl-CoA mutase and to methylcobalamin, coenzyme for
methionine synthase, which mediates conver-sion of homocysteine to
methionine. Consequently, there is an increase in the level of
homocysteine (Hcy) in B12 deficiency. Homocysteine has been
implicated as a risk factor for vascular disease, as well as brain
atrophy. There is evidence to implicate Hcy in increased oxidative
stress, DNA damage, and the triggering of apoptosis and
excitotoxicity, all of which are important mechanisms in
neurodegeneration. Homocysteine is also prothrombotic and
proatherogenic, causes damage to the vessel wall, and is related to
brain atrophy and possibly to white matter hyperintensities in the
brain. Epidemiological evidence and longitudinal data support the
finding that Hcy is a risk factor for cognitive impairment and
Alzheimers dis-ease. 1618 This may be due to cerebrovascular as
well as direct neurotoxic mechanisms.
As well as cognitive impairment, the common psychiatric symptoms
of vitamin B12 deficiency are continuous depression,19 psychotic
symptoms,20 mania, and obsessive compulsive disorder. The
neuropsychiatric severity of vitamin B12 deficiency
-
Critical Role of Vitamin B12
CLINICAL FOCUS: NUTRITION
THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December 2008,
No. 1, Volume 36 3
and the therapeutic efficacy depends on the duration of signs
and symptoms. Therefore, the consideration of vitamin B12
deficiency and testing for serum B12 levels is recommended in all
patients with organic brain syndrome, atypical psychiatric
symptoms, and fluctuation of symptomatology.
Relationship of Vitamin B12 and Homocysteine: Is Their Function
in Cardiovascular Events Obvious?Vitamin B12 deficiency and
homocysteinemia are undoubt-edly related,21,22 but their
synergistic or separate role in the development of atherosclerosis
and influence on cardiovas-cular events is nevertheless
controversial. In observational studies, elevated plasma total
homocysteine levels have been positively associated with ischemic
stroke risk.2325 Numer-ous retrospective and prospective studies
have revealed a consistent, independent relationship between mild
hyper-homocysteinemia and cardiovascular disease or all-cause
mortality. Starting at a plasma homocysteine concentration of
approximately 10 mmol/L, the risk increase follows a linear
dose-response relationship with no specific threshold level.
Hyperhomocysteinemia, as an independent risk fac-tor for
cardiovascular disease, is thought to be responsible for
approximately 10% of the total risk. Elevated plasma homocysteine
levels ( 12 mmol/L; moderate hyperhomo-cysteinemia) are considered
cytotoxic and are found in 5% to 10% of the general population and
in up to 40% of patients with vascular disease. Based on various
calculation models, reduction of elevated plasma homocysteine
concentrations may theoretically prevent up to 25% of
cardiovascular events. Treatment of hyperhomocysteinemia is
recommended for the apparently healthy general population.26 Some
large studies confirm that a supplementation with group B vitamins
did not reduce the risk of major cardiovascular events or all-cause
mortality in patients with vascular disease.27,28 The outcomes of
these and similar trials could have been different if the
researches had used vitamin B12 or B-complex for primary prevention
of cardiovascular events for patients with high risk of developing
atherosclerosis. Also, using high doses of vitamin B12 will
probably be more effective than using group B vitamins as a rule
presented by a set of various vitamins of this group in low doses.
For example, using folic acid alone for prevention of
cardiovascular diseases has been proven to be ineffective,29 while
very high doses of vitamin B12 (60 mg
every day for 6 months) has been used effectively without any
toxic side effects for the treatment of other diseases.30
What about Hematological Abnormalities?Hemopoesis is the process
in which new blood cells are produced and in which vitamin B12,
folate, and iron have funda-mental roles. New erythrocytes replace
the oldest erythrocytes (normally about 1%) that are phagocytosed
and destroyed each day. Erythroblasts require folate and vitamin
B12 for proliferation during their differentiation. Deficiency of
folate or vitamin B12 inhibits purine and thymidylate syntheses,
impairs DNA synthesis, and causes erythroblast apoptosis, resulting
in megaloblastic anemia from ineffective eryth-ropoiesis. The
presence of macro-ovalocytes having a high mean corpuscular value
(MCV), anisocytosis, poikilocytosis and hypersegmented neutrophils,
anemia, leukopenia, and thrombocytopenia or pancytopenia suggests a
megaloblastic disorder associated with a nutritional deficiency,
ie, vitamin B12. The usual presentation accompanies symptoms of
anemia. Asymptomatic patients can be identified by routine
hema-tologic investigations. Vitamin B12 deficiency produces the
classic picture of macrocytic anemia, with a MCV 100 fL. The MCV
correlates with estimated vitamin B12 level: MCV of 80 to 100 fL
indicates 25% probability of vitamin B12 defi-ciency; MCV of 115 to
129 fL indicates a 50% probability; MCV 130 indicates 100%
probability.31 It is a classic textbook picture of vitamin B12
deficiency, but usually the clinical picture looks different.
Hematological abnormalities, such as anemia or macrocytosis, may be
absent at the time of neurological presentation.32 It is well known
that vitamin B12 deficiency may be accompanied by iron deficiency,
and this associa-tion can mask the macrocytosis.33,34 There are no
generally accepted guidelines for the definition, diagnosis,
treatment, and follow-up of patients with vitamin B12 deficiency.
Total serum vitamin B12 may not reliably indicate vitamin B12
status. Probability of functional vitamin B12 deficiency decreases
upon increasing the blood level of vitamin B12. To increase
specificity and sensitivity in diagnosing vitamin B12 deficiency,
the concept of measuring Hcy, methylmalonic acid (MMA) is intended.
Lately, for the solution of this problem, an evaluation of
holotranscobalamin II has aroused great interest.35
Vitamin B12 deficiency may also influence the granulocyte and
platelet lines and may be mistaken for leukemia.36 In all cases,
the important practical indicator is positive response to vitamin
B12 treatment.
-
Ilia Volkov
CLINICAL FOCUS: NUTRITION
4 THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December
2008, No. 1, Volume 36
Known Cutaneous and Mucous Manifestations of Vitamin B12
Deficiency and the Novel Use of Vitamin B12 in DermatologyThe
characteristic dermatological sign of vitamin B12 deficiency is
cutaneous pigmentation,3740 which can be reversed by
admin-istration of vitamin B12. Increased cutaneous pigmentation is
especially accentuated in palmar creases, on the dorsa of hands and
feet, in intertriginous areas, on oral mucosa, and in recent scars.
The mechanism of hyperpigmentation is unexplained. Histology shows
an increase of melanin in the basal layer. In an electron
microscopic study, many melanosomes were observed in melanocytes
and surrounding keratinocytes. There is supposition that the
dominant mechanism of hyperpigmen-tation due to vitamin B12
deficiency is not a defect in melanin transport, but is rather an
increase in melanin synthesis.
The author investigated and reported a case of the paradoxical
disappearance of chronic erythema nodosum,41 which had persisted
for more than 6 months in spite of a prolonged treatment with
nonsteroidal anti-inflammatory drugs. When the patient complained
of paresthesias, a blood test for vitamin B12 was performed and a
prominent vitamin B12 deficiency was discovered. Since treatment
was initiated with intramuscular vitamin B12 injections, not only
did the par-esthesias disappear, but the erythema nodosum did as
well. The patient continued to receive maintenance therapy with
vitamin B12 without recurrence of erythema nodosum.
Recurrent aphthous stomatitis (RAS) is one of the most common
oral mucosa lesions seen in primary care. Most treatments given to
patients suffering from RAS achieve short-term therapeutic goals,
such as alleviation of pain, reduction of ulcer duration, and
recovery of normal oral function. Just a few reported treatments
have achieved long-term therapeutic goals, such as reduction of the
frequency and severity of RAS and maintenance of remission.
Although the precise role of vitamin B12 deficiency in the
pathogenesis of RAS is unclear, suppression of cell-mediated
immunity and changes in the cells of the tongue and buccal mucosa
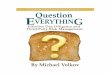
have been reported.42,43 We have reported previously the successful
treatment with vitamin B12 of RAS patients (Figure 1).44,45
According to the authors 6 years of clinical experience, vitamin
B12 treatment achieves long-term therapeutic goals and can be
effective for patients suffering from RAS, regardless of their
serum vitamin B12 level. The author and his colleagues have
finished a randomized, double-placebo, controlled clinical trial,
and received results to confirm their previous clinical
observations.
Potential Role and Uses of Vitamin B12 in Previously Uncommon
AreasA possible correlation between vitamin B12 and fertility
problems, which indicates vitamin B12 deficiency as one of cause of
recurrent abortions and the use of vitamin B12 in initial
treatments in order to prevent these conditions, has been debated
for a long time.4648 In a statistical meta-analysis
Figure 1. Frequency of recurrent aphthous stomatitis (RAS)
episodes prior to and during vitamin B12 treatment (episodes per
month).
1.5
0.13
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
Treatment status
Prior to treatment
During treatment
-
Critical Role of Vitamin B12
CLINICAL FOCUS: NUTRITION
THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December 2008,
No. 1, Volume 36 5
performed on 5 studies in which serum B12 was assayed in women
suffering from early recurrent abortions (ERA), a significant
relationship was found between ERA and vitamin B12 deficiency.49 No
difference was noticed between cases and controls for folate.
Vitamin B12 evaluation should be considered in women with ERA
regardless of whether or not hematological or neurological
abnormalities are present.
Osteoporosis is a widespread problem, which frequently has
devastating health consequences because of its association with
fragility fractures. The total number of fractures, and hence the
cost to society, will increase dramatically over the next 50 years
as a result of demographic changes in the number of elderly people.
Thus, prevention of osteoporosis by identifying risk factors or
risk indicators, as well as developing new treatment strategies, is
a major health issue. Recent data suggest that vitamin B12 affects
bone metabolism, bone quality, and fracture risk in humans.50
Strokes increase the risk of subsequent hip fracture by 2 to 4
times. Hyperhomocysteinemia is a risk factor for both ischemic
stroke and osteoporotic fractures in elderly men and women. In a
population with a high baseline fracture risk, combined treatment
with folate and vitamin B12 has been shown to be safe and effective
in reducing the risk of a hip fracture in elderly patients
following stroke.51 The relationship of Hcy and vitamin B12 with
bone turnover mark-ers, broadband ultrasound attenuation (BUA), and
fracture incidence in healthy elderly people was studied by
researchers who found that high homocysteine and low vitamin B12
con-centrations were significantly associated with low BUA, high
markers of bone turnover, and increased fracture risk.52 A
preventive vitamin B12 supplementation for healthy people with
mandatory risk factors for osteoporosis and a treatment with
vitamin B12 of patients suffering from osteoporosis could be a
promising treatment for this serious problem. Controlled clinical
trials should be conducted to confirm the safety and effectiveness
of vitamin B12 therapy for osteoporosis.
Vitamin B12 carrier proteins, the transcobalamins (TC), are
elevated during trauma, infections, and chronic inflammatory
conditions. This remains unexplained. It is proposed that such TC
elevations signal a need for vitamin B12 central to the resolution
of inflammation.53 Vitamin B12 is an effective scavenger of nitric
oxide (NO).54 Septic shock has an extremely high mortality rate,
with approximately 200 000 people dying from sepsis annually in the
US. The high mortality results partially from severe hypotension
secondary to high serum NO concentrations. Reducing NO levels
should be beneficial
in sepsis; a possible approach in reducing NO levels in sepsis
is the use of an NO scavenger, which would leave sufficient free NO
for normal physiological functions. Animal and human clinical data
suggest that high-dose vitamin B12 may prove a promising approach
to systemic inflammatory response syn-drome (SIRS), sepsis, and
septic and traumatic shock.
Drugs which directly counteract NO, such as endothelial receptor
blockers, NO-synthase inhibitors, and NO-scavengers, not only may
be effective in the acute treatment of migraine, but also are
likely to be effective in migraine prophylaxis. The first
prospective, open study indicated that intrana-sal hydroxocobalamin
may have a prophylactic effect in migraine.55
A number of studies have demonstrated that vitamin B12 is
important in maintaining differentiation, proliferation, and
metabolic status of cells. Nitric oxide can cause both apoptosis
and necrosis, making it a good candidate for anti-tumor therapy.
Initially, vitamin B12 was proposed for use as a scavenger and
cytoprotective agent to bind and inactivate NO. The use of vitamin
B12 as a carrier to deliver NO into tumor cells is novel. One
investigational study showed that complex NO-vitamin B12 inhibited
tumor growth in vivo and in vitro by activating the extrinsic
apoptotic pathway.
Researchers have attempted to correlate vitamin B12 with
malignancy ever since the multifunctional role of vitamin B12 has
begun to be understood. There are many hypotheses about the role of
vitamin B12 in growth of malignancy. What is the explanation for
elevation of vitamin B12 level in oncological patients? Is it a
marker of malignancy? Elevated levels of serum vitamin B12 may be a
sign of a serious, even life-threatening, disease. Hematologic
disorders, like chronic myelogeneous leukemia, promyelocytic
leukemia, polycythemia vera, and hypereosinophilic syndrome can
result in elevated levels of vitamin B12. Not surprisingly, a rise
of the vitamin B12 concentration in serum is one of the diagnostic
criteria for the latter two diseases. Several liver diseases, like
acute hepatitis, cirrhosis, hepatocellular carcinoma, and
meta-static liver disease, can also be accompanied by an increase
in circulating vitamin B12. This phenomenon is caused predominantly
by vitamin B12 release during hepatic cytolysis and/or decreased
vitamin B12 clearance by the affected liver. Altogether, it can be
concluded that an observed elevation of vitamin B12 in blood merits
a full diagnostic examination to assess the presence of
disease.56
-
Ilia Volkov
CLINICAL FOCUS: NUTRITION
6 THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December
2008, No. 1, Volume 36
Maybe an elevated level of vitamin B12 is a sign that the body
is fighting disease and that, as result of this battle, there is a
mobilization of resources and an attempt to compensate by
activating biologically active substances for repair of
defects.
Carmel et al (1977) studied 139 patients with non-hematologic
malignancy in order to define the incidence of vitamin B12-related
abnormalities and correlate them with clinical findings. A high
serum vitamin B12 level usually implied a poor prognosis in a
patient with cancer. However, while most such patients had hepatic
and other metastases, hepatic involvement was not universal nor did
most of the patients with hepatic disease have high vitamin B12
levels.57
The relationship between vitamin B12 levels and survival was
studied in a group of 161 terminally ill cancer patients. Their
average age was 74.7 years. The length of survival decreased with
the increase in serum vitamin B12 levels. In multivariate analyses,
C-reactive protein (CRP) was the most important prognostic factor
in this population, and vitamin B12 provided information
independent of CRP in predicting survival. These data indicate that
an elevated serum vitamin B12 level is a predictive factor for
mortality in patients with cancer, independent of CRP or other
factors.58
The effect of vitamin B12 on the proliferation of malignant
cells has been examined in vivo and in vitro in numerous
studies.5961 Methylcobalamin inhibited the proliferation of
androgen-sensitive SC-3 cells (a cloned cell line from Shionogi
mouse mammary tumor, SC115) in culture at the concentration of 100
to 300 g/mL. An inhibitory activity of methylcobalamin on the
proliferation was also observed in other cell lines
(estrogen-sensitive B-1F cells from mouse Leydig cell tumor and
MCF-7 cells from human mammary tumor) at the concentration of 500
g/mL. Moreover, large doses of methylcobalamin injected
intraperitoneally (100 mg/kg body weight/day) were nontoxic and
suppressed the tumor growth of SC115 and B-1F cells in mice fed a
vitamin B12-deficient diet. These results indicate that
methylcobalamin inhibits the proliferation of malignant cells in
culture and in vivo and propose the possibility of methylcobalamin
as a candidate of potentially useful agents for the treatment for
some malignant tumors.59
Every system in mechanics and nature seeks some sort of balance.
The human body is no exception. Upon an imbalance or disease, the
organism tries to compensate by the mobilization of its inner
resources. There is an ongoing process of accumulation of
biologically active substances
to fight disease. Unfortunately, this battle for balance is not
always successful. Being stressed, the organism shows us signs of
distress and calls for help.
The author proposes that a high level of vitamin B12 in
oncological diseases is such a sign.62 The basis for such a
proposal can be summarized as follows:
1. The well-known fact that a high level of vitamin B12 is
present in different kinds of malignancy.
2. There is a positive correlation between level of vitamin B12
and the severity of the disease; the more severe the disease, the
higher the level of vitamin B12.
3. A number of the experimental laboratory studies indi-cate an
inhibition in the growth of malignant cells upon use of vitamin
B12.
4. There are no experimental results indicating that vitamin B12
stimulates growth of malignant cells.
5. There is no data about toxic effect of vitamin B12 in the
treatment of various diseases. Sometimes it is necessary to use
very high doses to achieve therapeutic effect.30 Vitamin B12 is the
only known vitamin that does not have any toxic effect.
The author has not yet been able to find another explanation for
high levels of vitamin B12 in oncology patients other than that it
is a compensatory mechanism.
Necessity of New Approach to the Problem of Vitamin B12We know
that not only can individuals with special prob-lems and
vegetarians suffer from vitamin B12 deficiency, but also patients
with low meat intake. There are many articles indicating the
increasing prevalence of low vitamin B12 levels in different
segments of general population.6368 In the past decade, it has
become evident that vitamin B12 deficiency occurs commonly in
industrial countries at different levels of economic and social
status. A high prevalence of symptomatic vitamin B12 deficiency was
discovered in a pre-urban Bedouin area in Southern Israel due to
low intake of animal products.63 Dietary vitamin B12 deficiency is
a severe problem in India, Mexico, Central and South America,64 and
selected areas in Africa.65 For example, at least 40% of the
population in Central and South America has deficient or marginal
plasma vitamin B12 concentrations in almost all areas and in all
age groups.66 As a rule, it appears to be prevalent in 30% to 40%
of those in the lower socioeconomic levels. The authors clinic
serves middle to upper-middle class populations, and,
-
Critical Role of Vitamin B12
CLINICAL FOCUS: NUTRITION
THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December 2008,
No. 1, Volume 36 7
according to data received in that clinics study,69 frequency of
deficient or marginal vitamin B12 level ( 250 pg/mL) was about 35%.
The author cannot extrapolate the finding to general population in
this area, because the study population is a selected sample, but a
prevalence of low level of vita-min B12 in the overall population
may be similar. Today there is a tendency in modern society to
change habits, for example cessation of smoking, fighting with
obesity, accen-tuating physical exercise, and adopting correct
eating habits. The author concludes that as a result of media
information disseminating the relationship between meat and
cholesterol/cardiovascular diseases, consumption of
meatparticularly beefhas decreased. The author hypothesizes that
the decrease of level of vitamin B12 in the population with higher
educational level is caused by a premeditated decrease in
consumption of animal products. Also, in modern society, there is a
tendency for ideological motives, particularly among the younger
generation, to be vegans. Changes in lifestyle among segments of
the population with high socioeconomic level on one hand, and the
existence of poverty on the other, are two main factors in the
decreasing consumption of animal products (particularly red meat).
This causes a decrease in the level of vitamin B12 in general
population; as a consequence, this will increase pathology due to
vitamin B12 deficiency (such as neurological and hematological
disorders). As mentioned, vitamin B12 defi-ciency has various and
serious health effects. In lieu of these possible developments and
in order to prevent serious health problems, vitamin B12 routine
fortification should be seriously considered and discussed.
References 1. Narayanan MN, Dawson DW, Lewis MJ. Dietary
deficiency of vitamin B12
is associated with low serum cobalamin levels in
non-vegetarians. Eur J Haematol. 1991;47(2):115118.
2. Andrs E, Loukili NH, Noel E, et al. Vitamin B12 (cobalamin)
deficiency in elderly patients. CMAJ. 2004;171(3):251259.
3. Kaptan K, Beyan C, Ural AU, et al. Helicobacter pyloriis it a
novel causative agent in Vitamin B12 deficiency? Arch Intern Med.
2000;160(9):13491353.
4. Bauman WA, Shaw S, Javatilleke E, Spungen AM, Herbert V.
Increased intake of calcium reverses vitamin B12 malabsorption
induced by metfor-min. Diabetes Care. 2000;23(9):12271231.
5. Andrs E, Noel E, Goichot B. Metformin-associated vitamin B12
deficiency. Arch Intern Med. 2002;162(19):22512252.
6. Howden CW. Vitamin B12 levels during prolonged treatment with
proton pump inhibitors. J Clin Gastroenterol. 2000;30(1):2933.
7. Termanini B, Gibril F, Sutliff VE, Yu F, Venzon DJ, Jensen
RT. Effect of long-term gastric acid suppressive therapy on serum
vitamin B12 levels in patients with ZollingerEllison syndrome. Am J
Med. 1998;104(5):422430.
8. Grsbeck R. Imerslund-Grsbeck syndrome (selective vitamin B12
malabsorption with proteinuria). Orphanet J Rare Dis.
2006;1:17.
9. Smolka V, Bekrek V, Hldkov E et. Metabolic complications and
neurologic manifestations of vitamin B12 deficiency in children of
vegetarian mothers. Cas Lek Cesk. 2001;140(23):732735.
10. Muthayya S, Dwarkanath P, Mhaskar M, et al. The relationship
of neonatal serum vitamin B12 status with birth weight. Asia Pac J
Clin Nutr. 2006;15(4):538543.
11. Groenen PM, van Rooij IA, Peer PG, Gooskens RH, Zielhuis GA,
Steegers-Theunissen RP. Marginal maternal vitamin B12 status
increases the risk of offspring with spina bifida. Am J Obstet
Gynecol. 2004;191(1):1117.
12. Brasseur D. Excessive dietetic restrictions in children. Rev
Med Brux. 2000;21(4):A367A370.
13. Healton EB, Savage DG, Brust JC, Garrett TJ, Lindenbaum J.
Neurologic aspects of cobalamin deficiency. Medicine (Baltimore).
1991;70(4):229245.
14. Miller A, Korem M, Almog R, Galboiz Y. Vitamin B12,
demyelination, remye-lination and repair in multiple sclerosis. J
Neurol Sci. 2005;233(12):9397.
15. Mastronardi FG, Min W, Wang H, et al. Attenuation of
experimental auto-immune encephalomyelitis and nonimmune
demyelination by IFN-beta plus vitamin B12: treatment to modify
notch-1/sonic hedgehog balance. J Immunol.
2004;172(10):64186426.
16. Sachdev PS. Homocysteine and brain atrophy. Prog
Neuropsychopharmacol Biol Psychiatry. 2005;29(7):11521161.
17. Corder EH, Beaumont H. Susceptibility groups for Alzheimers
disease (OPTIMA cohort): Integration of gene variants and
biochemical factors. Mech Ageing Dev. 2007;128(1):7682.
18. Reynolds E. Vitamin B12, folic acid, and the nervous system.
Lancet Neurol. 2006;5(11):949960.
19. Wolters M, Strhle A, Hahn A. Cobalamin: a critical vitamin
in the elderly. Prev Med. 2004;39(6):12561266.
20. Masalha R, Chudakov B, Muhamad M, Rudoy I, Volkov I, Wirguin
I. Cobalamin-responsive psychosis as the sole manifestation of
vitamin B12 deficiency. Isr Med Assoc J. 2001;3(9):701703.
21. Spence JD, Bang H, Chambless LE, Stampfer MJ. Vitamin
Intervention for Stroke Prevention trial: an efficacy analysis.
Stroke. 2005;36(11):24042409.
22. Krajcovicov-Kudlckov M, Blazcek P. Nutritional determinants
of homocysteinemia. Cas Lek Cesk. 2002;141(13):417420.
23. Homocysteine Studies Collaboration. Homocysteine and risk of
ischemic heart disease and stroke. JAMA. 2002;288(16):20152022.
24. Del Ser T, Barba R, Herranz AS, et al.
Hyperhomocyst(e)inemia is a risk factor of secondary vascular
events in stroke patients. Cerebrovasc Dis. 2001;12(2):9198.
25. Boysen G, Brander T, Christensen H, Gideon R, Truelsen T.
Homocysteine and risk of recurrent stroke. Stroke.
2003;34(5):12581261.
26. Stanger O, Herrmann W, Pietrzik K, et al. DACH-LIGA
homocystein (German, Austrian, and Swiss homocysteine society):
consensus paper on the rational clinical use of homocysteine, folic
acid and B-vitamins in cardiovascular and thrombotic diseases:
guidelines and recommendations. Clin Chem Lab Med.
2003;41(11):13921403.
27. Lonn E, Yusuf S, Arnold MJ, et al. Homocysteine lowering
with folic acid and B vitamins in vascular disease. N Engl J Med.
2006;354(15):15671577. Erratum in: N Engl J Med.
2006;355(7):746.
28. Bnaa KH, Njlstad I, Ueland PM, et al. Homocysteine lowering
and cardiovascular events after acute myocardial infarction. N Engl
J Med. 2006;354(15):15781588.
29. Bazzano LA, Reynolds K, Holder KN, He J. Effect of folic
acid supplemen-tation on risk of cardiovascular diseases: a
meta-analysis of randomized controlled trials. JAMA.
2006;296(22):27202726.
30. Kira J, Tobimatsu S, Goto I. Vitamin B12 metabolism and
massive-dose methyl vitamin B12 therapy in Japanese patients with
multiple sclerosis. Intern Med. 1994;33(2):8286.
31. Singh NN, Thomas FP, Diamond AL, et al. Vitamin B12
Associated Neurological Diseases. eMedicine Website.
http://www.emedicine.com/neuro/TOPIC439.HTM. Updated January 29,
2008. Accessed December 1, 2007.
-
Ilia Volkov
CLINICAL FOCUS: NUTRITION
8 THE PHYSICIAN AND SPORTSMEDICINE ISSN 0091-3847, December
2008, No. 1, Volume 36
32. Solomon LR. Cobalamin-responsive disorders in the ambulatory
care setting: unreliability of cobalamin, methylmalonic acid, and
homocysteine testing. Blood. 2005;105(3):978985.
33. Hash RB, Sargent MA, Katner H. Anemia secondary to combined
deficiencies of iron and cobalamin. Arch Fam Med.
1996;5(10):585588.
34. Carmel R. Prevalence of undiagnosed pernicious anemia in the
elderly. Arch Intern Med. 1996;156(10):10971100.
35. Herrmann W, Obeid R, Schorr H, Geisel J. Functional vitamin
B12 deficiency and determination of holotranscobalamin in
populations at risk. Clin Chem Lab Med. 2003;41(11):14781488.
36. Aitelli C, Wasson L, Page R. Pernicious anemia:
presentations mimicking acute leukemia. South Med J.
2004;97(3):295297.
37. Mori K, Ando I, Kukita A. Generalized hyperpigmentation of
the skin due to vitamin B12 deficiency. J Dermatol.
2001;28(5):282285.
38. Srivastava N, Chand S, Bansal M, Srivastava K, Singh S.
Reversible hyper-pigmentation as the first manifestation of dietary
vitamin B12 deficiency. Indian J Dermatol Venereol Leprol.
2006;72(5):389390.
39. Simek OP, Gn N, Gmrk F, Cetin M. A child with vitamin B12
deficiency presenting with pancytopenia and hyperpigmentation. J
Pediatr Hematol Oncol. 2004;26(12):834836.
40. Sabatino D, Kosuri S, Remollino A, Shotter B. Cobalamin
deficiency presenting with cutaneous hyperpigmentation: a report of
two siblings. Pediatr Hematol Oncol. 1998;15(5):447450.
41. Volkov I, Rudoy I, Press Y. Successful treatment of chronic
erythema nodosum with vitamin B12. J Am Board Fam Pract.
2005;18(6):567569.
42. Field EA, Speechley JA, Rugman FR, Varga E, Tyldesley WR.
Oral signs and symptoms in patients with undiagnosed vitamin B12
deficiency. J Oral Pathol Med. 1995;24(10):468470.
43. Weusten BL, van de Wiel A. Aphthous ulcers and vitamin B12
deficiency. Neth J Med. 1998;53(4):172175.
44. Volkov I, Rudoy I, Abu-Rabia U, Masalha T, Masalha R. Case
report: Recurrent aphthous stomatitis responds to vitamin B12
treatment. Can Fam Physician. 2005;51:844845.
45. Volkov I, Rudoy I, Peleg R, Press Y. Successful treatment of
recurrent aphthous stomatitis of any origin with vitamin B12
(irrespective of its blood level). The Internet Journal of Family
Practice. 2007;5(1).
46. Kumamoto Y, Maruta H, Ishigami J, et al. Clinical efficacy
of mecobalamin in the treatment of oligozoospermiaresults of
double-blind comparative clinical study. Hinyokika Kiyo.
1988;34(6):11091132.
47. Bennett M. Vitamin B12 deficiency, infertility and recurrent
fetal loss.J Reprod Med. 2001;46(3):209212.
48. Chatterjee S, Chowdhury RG, Khan B. Medical management of
male infertility. J Indian Med Assoc. 2006;104(2):74,7677.
49. Reznikoff-Etivant MF, Zittoun J, Vaylet C, Pernet P, Milliez
J. Low Vitamin B(12) level as a risk factor for very early
recurrent abortion. Eur J Obstet Gynecol Reprod Biol.
2002;104(2):156159.
50. Herrmann M, Widmann T, Herrmann W. Homocysteinea newly
recognised risk factor for osteoporosis. Clin Chem Lab Med.
2005;43(10):11111117.
51. Sato Y, Honda Y, Iwamoto J, Kanoko T, Satoh K. Effect of
folate and mecobalamin on hip fractures in patients with stroke: a
randomized controlled trial. JAMA. 2005;293(9):10821088.
52. Dhonukshe-Rutten RA, Pluijm SM, de Groot LC, Lips P, Smit
JH, van Staveren WA. Homocysteine and vitamin B12 status relate to
bone turnover markers, broadband ultrasound attenuation, and
fractures in healthy elderly people. J Bone Miner Res.
2005;20(6):921929.
53. Wheatley C. A scarlet pimpernel for the resolution of
inflammation? The role of supra-therapeutic doses of cobalamin, in
the treatment of systemic inflammatory response syndrome (SIRS),
sepsis, severe sepsis, and septic or traumatic shock. Med
Hypotheses. 2006;67(1):124142.
54. Broderick KE, Feala J, McCulloch A, et al. The nitric oxide
scavenger cobinamide profoundly improves survival in Drosophila
melanogaster model of bacterial sepsis. FASEB J.
2006;20(11):18651873.
55. van der Kuy PH, Merkus FW, Lohman JJ, ter Berg JW, Hooymans
PM. Hydroxocobalamin, a nitric oxide scavenger, in the prophylaxis
of migraine: an open, pilot study. Cephalalgia.
2002;22(7):513519.
56. Ermens AA, Vlasveld LT, van Marion-Kievit JA, Lensen CJ,
Lindemans J. The significance of an elevated cobalamin
concentration in the blood. Ned Tijdschr Geneeskd.
2002;146(10):459464.
57. Carmel R, Eisenberg L. Serum vitamin B12 and transcobalamin
abnormali-ties in patients with cancer. Cancer.
1977;40(3):13481353.
58. Geissbhler P, Mermillod B, Rapin CH. Elevated serum vitamin
B12 levels associated with CRP as a predictive factor of mortality
in palliative care cancer patients: a prospective study over five
years. J Pain Symptom Manage. 2000;20(2):93103.
59. Nishizawa Y, Yamamoto T, Terada N, Fushiki S, Matsumoto K,
Nishizawa Y. Effects of methylcobalamin on the proliferation of
androgen-sensitive or estrogen-sensitive malignant cells in culture
and in vivo. Int J Vitam Nutr Res. 1997;67(3):164170.
60. Liteplo RG, Hipwell SE, Rosenblatt DS, Sillaots S, Lue-Shing
H. Changes in cobalamin metabolism are associated with the altered
methionine auxotrophy of highly growth autonomous human melanoma
cells. J Cell Physiol. 1991;149(2):332338.
61. Fiskerstrand T, Christensen B, Tysnes OB, Ueland PM, Refsum
H. Development and reversion of methionine dependence in a human
glioma cell line: relation to homocysteine remethylation and
cobalamin status. Cancer Res. 1994;54(18):48994906.
62. Volkov I. The master key effect of vitamin B12 in treatment
of malignancya potential therapy? Med Hypotheses.
2008;70(2):324328.
63. Masalha R , Rudoy I, Volkov I, Yusuf N, Wirguin I, Herishanu
YO. Symptomatic dietary vitamin B(12) deficiency in a nonvegetarian
popula-tion. Am J Med. 2002;112(5);413416.
64. Stabler SP, Allen RH. Vitamin B12 deficiency as a worldwide
problem. Annu Rev Nutr. 2004;24:299326.
65. Savage D, Gangaidzo I, Lindenbaum J, et al. Vitamin B12
deficiency is the primary cause of megaloblastic anaemia in
Zimbabwe. Br J Haematol. 1994;86(4):844850.
66. Allen LH. Folate and vitamin B12 status in the Americas.
Nutr Rev. 2004;62(6 Pt 2);S29S33.
67. Fora MA, Mohammad MA. High frequency of suboptimal serum
vitamin B12 level in adults in Jordan. Saudi Med J.
2005;26(10):15911595.
68. Dagnelie PC. Nutrition and healthpotential health benefits
and risks of vegetarianism and limited consumption of meat in the
Netherlands. Ned Tijdschr Geneeskd. 2003;147(27):13081313.
69. Volkov I, Rudoy I, Machagna M, et al. Modern society and
prospects of low Vitamin B12 intake. Ann Nutr Metab.
2007;51(5):468470.