Embed Size (px)
Citation preview

Chiang Mai Med J 2008;47(1):39-44.
Address requests for reprints: Suraphong Lorsomradee, M.D., Department of Anaesthesia, Faculty of Medicine,Chiang Mai University, Chiang Mai 50200, Thailand. E-mail:[email protected]
Received 17 January, 2008 and in revised form 26 March, 2008
Case report
VOLATILE INDUCTION AND MAINTENANCE OFANAESTHESIA IN A PATIENT WITH ADVANCED
EPIDERMOLYSIS BULLOSA
Sratwadee Lorsomradee, M.D., Suraphong Lorsomradee, M.D.
Department of Anaesthesia, Faculty of Medicine, Chiang Mai University
Abstract Epidermolysis bullosa dystrophica is characterized by cutaneous bullae forma-tion and subsequent scarring caused by relatively minor trauma to the skin and mucousmembranes. These patients grow up with more complicated sequelae that pose multiplechallenges to anaesthetists. There is a paucity of data concerning perioperative manage-ment in patients with advanced epidermolysis bullosa dystropica, who present with airwayproblems, particularly when coinciding with seizures from severe electrolyte disturbance,and lack of venous access. Therefore, we report perioperative anaesthetic management byusing the volatile induction and maintenance of anaesthesia in a patient with advancedepidermolysis bullosa dystropica. Chiang Mai Medical Journal 2008;47(1):39-44.
Keywords: epidermolysis bullosa, volatile induction and maintenance of anaesthesia
Epidermolysis bullosa dystrophica (EBD)is an autosomal recessive disorder, which ischaracterized by mechanically induced bullaeformation caused by minor friction followedby subsequent scarring.(1) It is an importantdisease for anaesthetists because unfortunatesequelae may occur during anaesthesia if thenecessary precautions are not taken. Patientsfrequently present with anaemia, hypopro-teinaemia, and electrolyte imbalance, whichrequire preoperative correction. Intubation inpatients with advanced EBD might be difficultbecause of mouth contractures, poor denta-
tions, and intraoral bullae, which can impedelaryngoscopy. Trauma from adhesive tape,blood pressure cuffs, or adhesive ECG elec-trodes may cause new bullae formation.Anaesthetic management of patients withadvanced EBD is directed toward avoidingeven minor friction to the skin and mucousmembranes. However, there is a paucity ofdata in the literature concerning the periopera-tive management in patients with advancedEBD, who present with accumulative problemsin the upper airway, particularly when coincid-ing with seizures due to severe electrolyte

40 Lorsomradee S, Lorsomradee S.
disturbance, and preoperative status can notbe corrected because of failure of preopera-tive venous access. Therefore, we report thevolatile induction and maintenance of anaes-thesia in a patient with advanced EBD.
Case reportA 20-year-old female patient (20 kg, 120
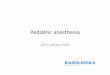
cm), with a background of EBD since birth,presented with a five-day history of severediarrhoea and vomiting, and developed gener-alized tonic clonic seizures due to hyponatrae-mic dehydration. Because of poor coopera-tion and failure in multiple attempts to estab-lish venous access for fluid resuscitation, shewas scheduled for central venous accessunder general anaesthesia. On physical exami-nation, her body surface was covered withnumerous blisters and fresh and scatteredbullae, particularly involving the face, exten-sor sides of the extremities, and around themouth and nose. There was evidence of mi-crostomia, poor dentations, intraoral bullae andlimitation of temporomandibular joint mobility.There were also flexion contractures andfusion of the fingers of both hands (Fig. 1).Capillary blood sampling demonstrated severeanaemia (haemoglobin 3.2 g/dL), prolongedpartial thromboplastin time (2.1 times controlvalue), and severe hyponatraemia (119 mEq/l). She had been treated with corticosteroidsin the past, but at the time of admission shewas taking phenytoin and applying 0.5%hydrocortisone ointment to her lesions.
She was taken to the operating room afteran adequate fasting period without premedi-cation. The respiratory circuit was primed for3 minutes using 8% sevoflurane in 100% oxy-gen with 6-l/min fresh gas flow. Her face andchin, gloves and the anaesthetic face mask
were well lubricated with hydrocortisone oint-ment. Spare laryngoscope blades, airways andintubating forceps were also well lubricated.A pulse oximeter probe was positioned on theleft earlobe. Anaesthesia was induced withvital capacity induction using the face maskwith sevoflurane starting at 8% in 100% oxy-gen, with fresh gas flow decreasing from 6-l/min to a 3-l/min during maintenance (50% oxy-gen), with up to 3.5% sevoflurane. Spontane-ous breathing via the face mask was main-tained throughout the whole procedure.
After induction of anaesthesia, needle elec-trodes were applied subcutaneously to theextremities for electrocardiographic monitor-ing, and non-invasive blood pressure was mea-sured with paraffin gauze covering under thecuff of the sphygmomanometer. Her eyes werecarefully closed with a gel pad. A centralvenous catheter was then inserted into the rightinternal jugular vein and sutured to the skin.During the procedure, the Trendelenburgposition and passive leg raising were used tofacilitate central venous access and treathypotension associated with hypovolaemia.The total anaesthesia time was 30 minutes.There was no new bullae formation and peri-operative complication. After her level of con-sciousness gained to preoperative level, shewas transferred back to the intensive care unit.Her initial postoperative course was notablefor the requirement of extensive fluid resusci-tation, blood component replacement, and elec-trolyte balance. Her recovery was uneventfuland she was discharged on the sixth postop-erative day.
DiscussionEBD is a group of inherited disorders char-
acterized by mechanically induced blistering

VIMA in epidermolysis bullosa 41
Figure 1. Photograph shows a 20-year-old female patient (20 kg, 120 cm), with advanced epidermolysisbullosa dystrophica.

42 Lorsomradee S, Lorsomradee S.
and bullae formation occurring immediatelybelow the lamina densa of the basement mem-brane. These blisters heal with atrophic scarformation.(1) This structural abnormality affectsthe stratified squamous epithelium of the skin,oropharynx and upper oesophagus, while theciliated columnar epithelium of the larynx andtrachea is spared. Certain precautions andmeticulous attention to several details arerequired throughout the operation to avoidanaesthetic related morbidity. Although directpressure to the skin is not as damaging as fric-tional or shearing forces, all persons involvedin handling the patients before, during andafter an operation must be made aware of theextreme vulnerability of their skin.
Routine monitoring is not always possible,so these patients are often poorly monitored.(2)
Pulse oximetry is the preferred method ofmonitoring pulse rate and there have been nocomplications reported with its use. Electro-cardiogram monitoring is not easy because theadhesive tapes can cause friction at applica-tion or removal. In our patient, needle elec-trodes were placed subcutaneously, and non-invasive blood pressure was measured withparaffin gauze covering without new bullaeformation.
Chronic anaemia resulting from chronicblood loss associated with frequent wounddressing is an additional problem for periopera-tive management. Red cell preparation andreplacement should be considered in a majoroperation. However, in accordance with a pre-vious review,(3) minimal blood loss associatedwith this procedure was not a major problem.
Airway patency may be a problem in somepatients with advanced EBD because ofmicrostomia, poor dentations, severe strictures,webbing, or large bullae in the oropharynx,
which can make intubation impossible. How-ever, several cases, without intraoral bullae,have been reported, in which endotrachealintubation was performed successfully with noadverse sequelae after extubation.(4-7) The useof a laryngeal mask airway (LMA) during theprocedure has also been described.(8) Never-theless, a review of 44 patients over a 10 yearperiod has warned against the risks.(9) If tra-cheal intubation is necessary, it is important toensure that both laryngoscopy and intubationare non-traumatic. A well-lubricated laryngo-scope and endotracheal tube are preferred toavoid trauma. A retrospective study reportedthat a minority of these patients requiredfiberoptic endotracheal intubation secondary tolimited opening of the mouth and contracturesin the neck. However, these intubations wereachieved with a intravenous anaesthesia.(10) Inour patient, failure of preoperative venousaccess and poor cooperation were reasons toanaesthetize the patient with the VIMA tech-nique. Fresh intraoral bullae proved on impor-tant problem for airway manipulation. How-ever, because the procedure had a non-airwayinvolvement and a relatively short duration, lessoropharyngeal manipulation was achieved us-ing gentle application of a well-lubricated facemask, and spontaneous breathing was keptthroughout the procedure, without airway com-plication. By using sevoflurane, postoperativeinvoluntary movements and shivering wereminimal, with less risk of inadvertent frictionand trauma,(8) and this was preferable inpatients with difficult or no venous access.(11)
Because of coagulation abnormality, a rightinternal jugular approach for central venousaccess was planned instead of a subclavianone, in which bleeding or haematoma is lesscontrollable. The perioperative challenge in this

VIMA in epidermolysis bullosa 43
patient was the haemodynamic compromisefrom anaesthesia together with preoperativehypovolaemia. However, the position requiredin this procedure was trendelenburg, whichsuited the patient’s status. In addition, furthervolume requirement was treated with gentlepassive leg raising. The haemodynamic situa-tion was within the preoperative range, andawakening to the level of preoperative con-sciousness was fast and uncomplicated.
In conclusion, as a result of the findings inthis and other case reports, anaesthetic man-agement in patients with advanced EBD shouldinclude careful airway manipulation, reductionof mucocutaneous contacts, prevention ofpressure or friction skin trauma, appropriatehaemodynamic balance, and the use of non-adhesive material. We successfully managedthe anaesthesia in a patient with advancedEBD.
References1. Fine JD, Eady RA, Bauer EA, et al. Revised classi-
fication system for inherited epidermolysis bullosa:report of the second international consensus meet-ing on diagnosis and classification of epidermolysisbullosa. J Am Acad Dermatol 2000;42:1051-66.
2. Holzman RS, Worthen HM, Johnson KL. Anaes-thesia for children with junctional epidermolysis
bullosa (letalis). Can J Anaesth 1987;34:395-9.3. Iohom G, Lyons B. Anaesthesia for children with
epidermolysis bullosa: a review of 20 years’ experi-ence. Eur J Anaesthesiol 2001;18:745-54.
4. Milne B, Rosales JK. Anaesthesia for correction ofoesophageal stricture in a patient with recessiveepidermolysis bullosa dystropica: case report. CanAnesth Soc J 1980;27:169-71.
5. Tomlinson AA. Recessive dystrophic epidermoly-sis bullosa. Anaesthesia 1983;38:485-91.
6. Ozkose Z, Celebi H, Pampal K, Altuntas B. Anes-thesia for correction of esophageal stricture in apatient with epidermolysis bullosa: a case report. JAnesth 2000;14:211-3.
7. Toda Y, Yokoyama M, Morimatsu H, et al. Generalanesthesia in a patient with dystrophic epidermoly-sis bullosa. J Anesth 2006;20:138-40.
8. Ames WA, Mayou BJ, Williams K. Anaestheticmanagement of epidermolysis bullosa. Br J Anaesth1999;82:746-51.
9. Griffin RP, Mayou BJ. The anaesthetic manage-ment of patients with dystrophic epidermolysisbullosa. A review of 44 patients over a 10 yearperiod. Anaesthesia 1993;48:810-5.
10. Lin YC, Golianu B. Anesthesia and pain manage-ment for pediatric patients with dystrophic epider-molysis bullosa. J Clin Anesth 2006; 18:268-71.
11. Herod J, Denyer J, Goldman A, Howard R. Epider-molysis bullosa in children: pathophysiology, ana-esthesia and pain management. Paediatr Anaesth2002;12:388-97.

44 Lorsomradee S, Lorsomradee S.
การนำสลบและรกษาระดบความลกของการสลบดวยยาดมสลบในผปวยโรค epidermolysis bullosa ชนดรนแรง
สรตวด หลอสมฤด, พ.บ., สรพงษ หลอสมฤด, พ.บ,
ภาควชาวสญญวทยา คณะแพทยศาสตร มหาวทยาลยเชยงใหม
บทคดยอ Epidermolysis bullosa dystrophica เปนโรคทางพนธกรรมทมลกษณะเดน คอ มผวหนงและเยอบตางๆ เปราะบางตอแรงเสยดทาน แมเพยงการสมผสหรอขดถผวหนงเพยงเบาๆ กอาจกอใหเกดผวหนงหรอเยอบแยกชนจนเกดบาดแผลชนด bullae เมอทำการรกษาบาดแผลจนกระทงหายดกยงคงมปญหาจากการเกดแผลเปนตามมา โดยผปวยทมอายมากขนมกจะมรองรองของแผลเปนมากขน จนทำใหเกดการดงรงอวยวะตางๆ หรอแขนขา และเปนอปสรรคสำคญตอการเปดทางเดนหายใจทางวสญญวทยา โดยมรายงานผปวยดวยโรคนทมารบบรการทางวสญญวทยา เกยวกบเทคนควธการบำบดทางวสญญวทยานอยมาก โดยเฉพาะผปวยผใหญทมแผลเปนมากและมปญหาในการเปดทางเดนหายใจ อกทงยงม severe electrolyte disturbance แตไมสามารถแกไขใหดกอนมาผาตดไดเนองจากไมสามารถหาเสนเลอดเพอเปดหลอดเลอดดำไดเลย ดงนนจงขอรายงานเทคนคทางวสญญวทยาคอ volatile induction and maintenance of anaesthesia ในการบำบดผปวย advancedepidermolysis bullosa dystropica เชยงใหมเวชสาร 2551;47(1):39-44.คำสำคญ: epidermolysis bullosa, volatile induction and maintenance of anaesthesia