Embed Size (px)
Citation preview

insightVol. XX No. 3 NOVEMBER 2002
Scientific Journal ofMEDICAL & VISION RESEARCH FOUNDATIONS
18, COLLEGE ROAD, CHENNAI - 600 006, INDIA
Editorial
Perspective — Wavefront Technology— Iyer Geetha Krishnan and Srinivas K Rao
Rapid Resolution of Posterior Scleritis following IntravenousMethylprednisolone Therapy — Rupak Kanti Biswas and Jyotirmay Biswas
Bilateral Retinal Vascular Occlusion Secondary to Septic Emboli arising froma Scrotal Ulcer in A Child - A Case Report— Amit Nagpal, Jyotirmay Biswas and Kannan M Narayanan
X-Chrom Contact Lens — S Premnandhini
Retinoblastoma mimicking Orbital Cellulitis — Manisha Agarwal,Jyotirmay Biswas, Krishna Kumar and Mahesh P Shanmugam
Last Page - Perimetry Update — R Krishna Kumar
External clinical photograph depicting left orbital cellulitis
13
2
This issue of Insight comes to you as Sankara Nethralaya enters it's 25th year inservice.
Ophthalmology is fast becoming a technology-based specialty. Phacoemulsifi-cationfor cataract surgery, lasers for refractive surgery and of course, the technology drivenvitreoretinal surgery exemplify this fact adequately. Adding to the list is the Wavefronttechnology, the current buzzword after LASIK in refractive surgery. Drs. Geetha Iyer andSrinivas K Rao explain the basics and effects on this technology on refractive surgery.
On the technology front again is the article on perimetry by R.Krishna Kumar whichdeals with the future of perimetry. This issue also has its complement of scientific articlesincluding one on x-chrom contact lenses.
Dr Mahesh P ShanmugamDr Arun Narayanaswamy
Editors
EDITORIAL
INSIGHT & EYELIGHTS are now available on line athttp://www. sankaranethralaya.org/publication.htm
3
Perspective:
Wavefront TechnologyIyer Geetha Krishnan and Srinivas K Rao
Refractive surgery for correcting theoptical aberrations of the eye aims to makethe eye optically perfect. In the past, thepreoperative goal has been 20/20 uncorrectedvisual acuity with zero residual power. Thenew goal is 20/10 uncorrected visual acuitywith aberration free postoperative vision.
Although recently introduced toophthalmology, wavefront technology has beenused for more than three decades to measurethe quality of optical lenses, such as thoseused in astronomy. Data derived fromwavefront technology allows the descriptionand calculation of optical errors, and offersthe promise of better understanding andtreating human visual disorders.
WAVEFRONTWavefront describes the curve corres-
ponding to multiple light rays emanating fromthe point source in the foveola after exitingthe eye having passed through the differentoptical elements of the eye and are visualizedthrough the pupil. Thus the wavefrontdescribes the surface shape of theimperfections of the eye's optical system. In aperfect optical system, there are no distortionsinduced by the lens system. Such an idealwavefront of an optical system with noaberrations is in one plane. A wavefront thatis not free of distortions is said to haveaberrations, which can be quantifiedmathematically using certain types ofmathematical functions. Wavefront error is thedifference between the actual and the idealwavefront.
OPTICAL ABERRATIONS
When light rays pass from the tear filmon to the cornea to the retina, they are bentand distorted by all the structures in the eye.The optical aberrations are classified aschromatic and monochromatic types. The
degradation of image caused by the chromaticaberration is not analysed by theaberrometers. The monochromatic aberrationsare measurable and are defined and quantifiedin terms of what are known as Zernicke'spolynomials (ZP) consisting of Zernicke's terms(ZT).
The classic spherocylindrical correctionof refractive errors that correct the opticalaberration of defocus equals sphericalcorrection (Zernicke term 4) and astigmatism(ZT 3 and 5) are familiar.
The so-called higher order aberrations areall the other aberrations except defocus (ZT4)and astigmatism (ZT3, 5) combined.
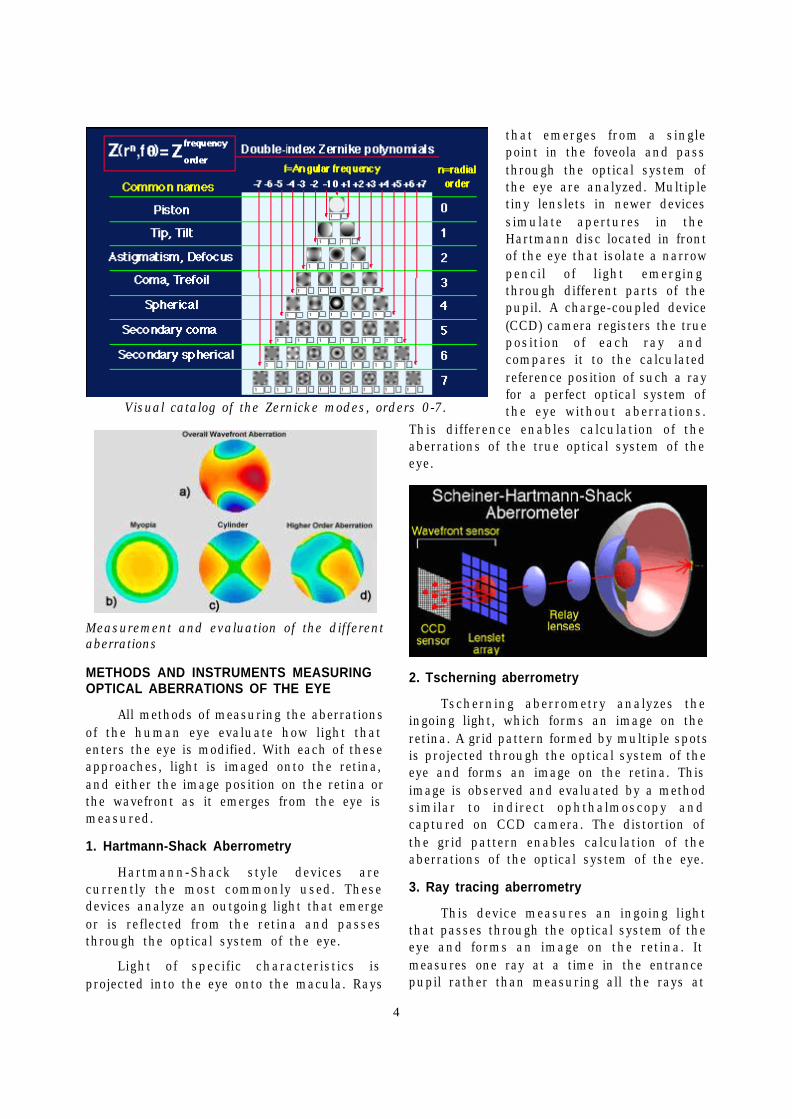
The most important and commonly usedare the first 4 orders of ZP consisting of 14terms of ZP, as follows:
0-order ZP (piston) - Term ZT0
1-order ZP (prism) - Term ZT1, 2 (tilt)
2-order ZP (spherocylinder) - TermZT3, 5 (astigmatism), and ZT4(defocus, sphere)
3-order ZP (coma) - Term 6, 9 (trefoil)and term ZT7, 8 (coma)
4-order ZP - Term ZT10, 14(quadrafoil) and term ZT 11, 12, 13(spherical aberration)
5-order ZP (secondary coma) - TermsZT 15, 16, 17, 18, 19, 20 and so forth
In normal human eyes of young patients,third order ZP aberrations (ZPA) areresponsible for approximately 40%, fourthorder ZPA for 25%, and fifth to sixth orderZPA for 30% of higher order aberrations ofthe eye.
4
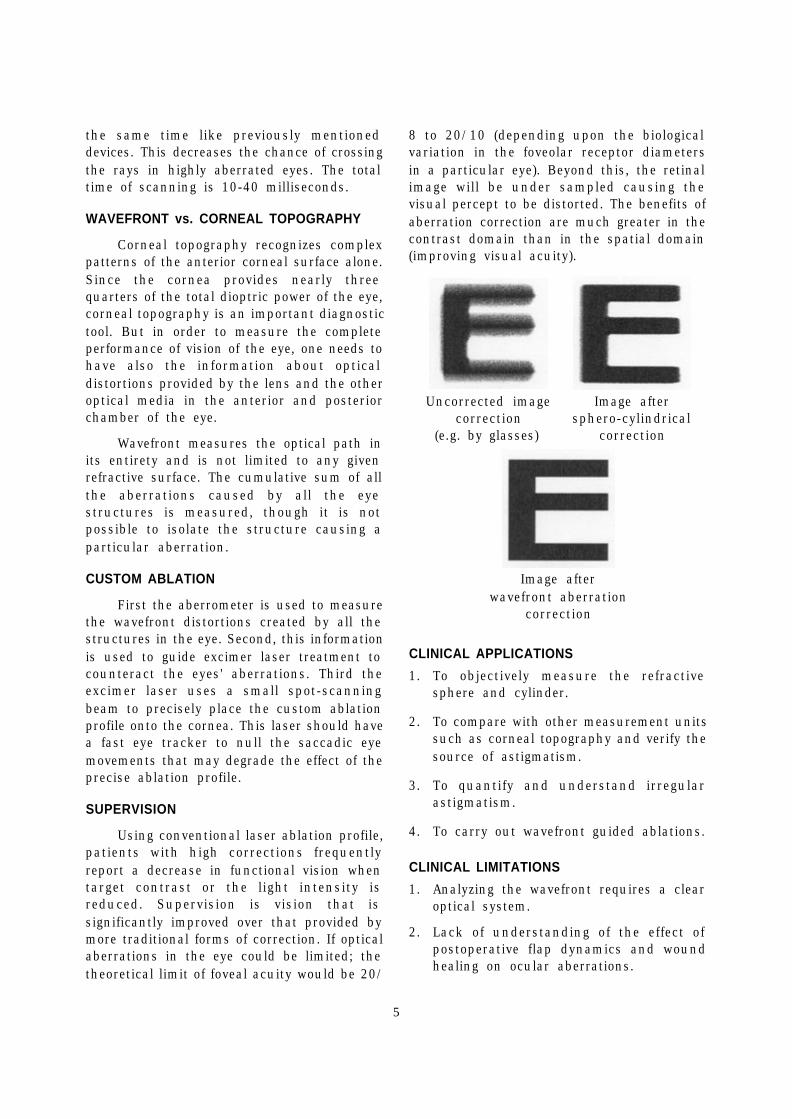
Measurement and evaluation of the differentaberrations
METHODS AND INSTRUMENTS MEASURINGOPTICAL ABERRATIONS OF THE EYE
All methods of measuring the aberrationsof the human eye evaluate how light thatenters the eye is modified. With each of theseapproaches, light is imaged onto the retina,and either the image position on the retina orthe wavefront as it emerges from the eye ismeasured.
1. Hartmann-Shack Aberrometry
Hartmann-Shack style devices arecurrently the most commonly used. Thesedevices analyze an outgoing light that emergeor is reflected from the retina and passesthrough the optical system of the eye.
Light of specific characteristics isprojected into the eye onto the macula. Rays
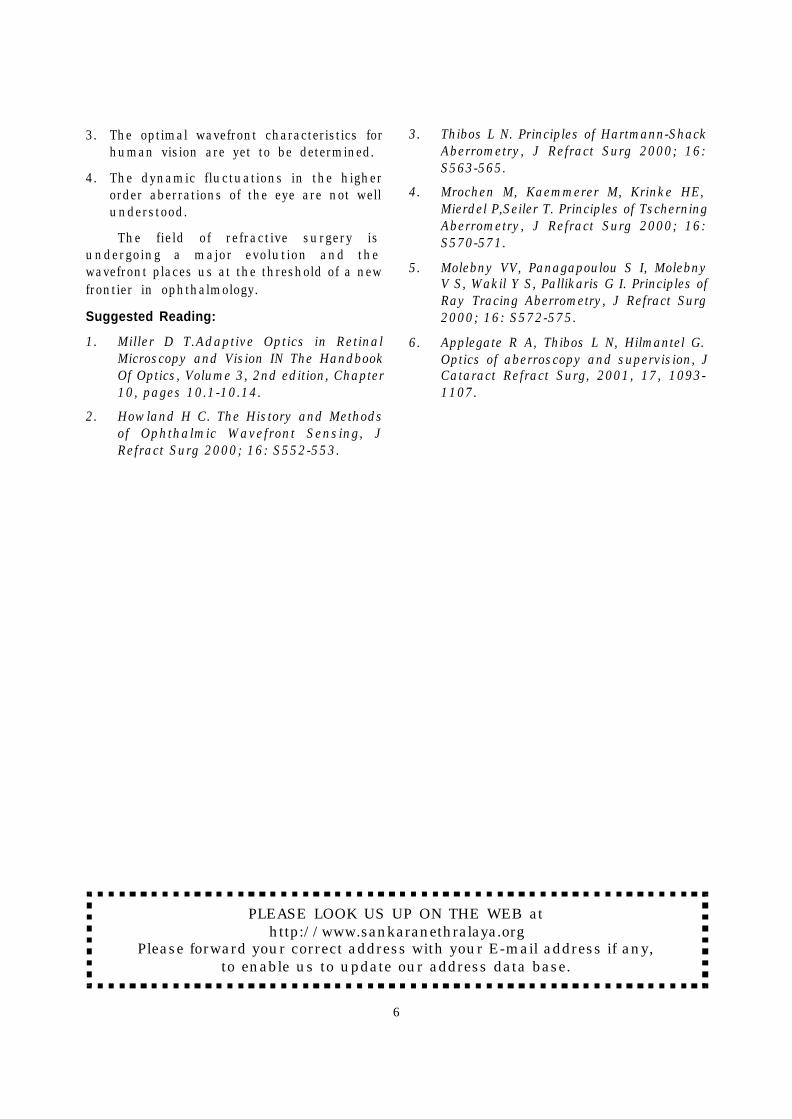
that emerges from a singlepoint in the foveola and passthrough the optical system ofthe eye are analyzed. Multipletiny lenslets in newer devicessimulate apertures in theHartmann disc located in frontof the eye that isolate a narrowpencil of light emergingthrough different parts of thepupil. A charge-coupled device(CCD) camera registers the trueposition of each ray andcompares it to the calculatedreference position of such a rayfor a perfect optical system ofthe eye without aberrations.
This difference enables calculation of theaberrations of the true optical system of theeye.
2. Tscherning aberrometry
Tscherning aberrometry analyzes theingoing light, which forms an image on theretina. A grid pattern formed by multiple spotsis projected through the optical system of theeye and forms an image on the retina. Thisimage is observed and evaluated by a methodsimilar to indirect ophthalmoscopy andcaptured on CCD camera. The distortion ofthe grid pattern enables calculation of theaberrations of the optical system of the eye.
3. Ray tracing aberrometry
This device measures an ingoing lightthat passes through the optical system of theeye and forms an image on the retina. Itmeasures one ray at a time in the entrancepupil rather than measuring all the rays at
Visual catalog of the Zernicke modes, orders 0-7.
5
the same time like previously mentioneddevices. This decreases the chance of crossingthe rays in highly aberrated eyes. The totaltime of scanning is 10-40 milliseconds.
WAVEFRONT vs. CORNEAL TOPOGRAPHY
Corneal topography recognizes complexpatterns of the anterior corneal surface alone.Since the cornea provides nearly threequarters of the total dioptric power of the eye,corneal topography is an important diagnostictool. But in order to measure the completeperformance of vision of the eye, one needs tohave also the information about opticaldistortions provided by the lens and the otheroptical media in the anterior and posteriorchamber of the eye.
Wavefront measures the optical path inits entirety and is not limited to any givenrefractive surface. The cumulative sum of allthe aberrations caused by all the eyestructures is measured, though it is notpossible to isolate the structure causing aparticular aberration.
CUSTOM ABLATION
First the aberrometer is used to measurethe wavefront distortions created by all thestructures in the eye. Second, this informationis used to guide excimer laser treatment tocounteract the eyes' aberrations. Third theexcimer laser uses a small spot-scanningbeam to precisely place the custom ablationprofile onto the cornea. This laser should havea fast eye tracker to null the saccadic eyemovements that may degrade the effect of theprecise ablation profile.
SUPERVISION
Using conventional laser ablation profile,patients with high corrections frequentlyreport a decrease in functional vision whentarget contrast or the light intensity isreduced. Supervision is vision that issignificantly improved over that provided bymore traditional forms of correction. If opticalaberrations in the eye could be limited; thetheoretical limit of foveal acuity would be 20/
8 to 20/10 (depending upon the biologicalvariation in the foveolar receptor diametersin a particular eye). Beyond this, the retinalimage will be under sampled causing thevisual percept to be distorted. The benefits ofaberration correction are much greater in thecontrast domain than in the spatial domain(improving visual acuity).
Uncorrected image Image aftercorrection sphero-cylindrical
(e.g. by glasses) correction
Image afterwavefront aberration
correction
CLINICAL APPLICATIONS
1. To objectively measure the refractivesphere and cylinder.
2. To compare with other measurement unitssuch as corneal topography and verify thesource of astigmatism.
3. To quantify and understand irregularastigmatism.
4. To carry out wavefront guided ablations.
CLINICAL LIMITATIONS
1. Analyzing the wavefront requires a clearoptical system.
2. Lack of understanding of the effect ofpostoperative flap dynamics and woundhealing on ocular aberrations.
6
3. The optimal wavefront characteristics forhuman vision are yet to be determined.
4. The dynamic fluctuations in the higherorder aberrations of the eye are not wellunderstood.
The field of refractive surgery isundergoing a major evolution and thewavefront places us at the threshold of a newfrontier in ophthalmology.
Suggested Reading:
1. Miller D T.Adaptive Optics in RetinalMicroscopy and Vision IN The HandbookOf Optics, Volume 3, 2nd edition, Chapter10, pages 10.1-10.14.
2. Howland H C. The History and Methodsof Ophthalmic Wavefront Sensing, JRefract Surg 2000; 16: S552-553.
3. Thibos L N. Principles of Hartmann-ShackAberrometry, J Refract Surg 2000; 16:S563-565.
4. Mrochen M, Kaemmerer M, Krinke HE,Mierdel P,Seiler T. Principles of TscherningAberrometry, J Refract Surg 2000; 16:S570-571.
5. Molebny VV, Panagapoulou S I, MolebnyV S, Wakil Y S, Pallikaris G I. Principles ofRay Tracing Aberrometry, J Refract Surg2000; 16: S572-575.
6. Applegate R A, Thibos L N, Hilmantel G.Optics of aberroscopy and supervision, JCataract Refract Surg, 2001, 17, 1093-1107.
PLEASE LOOK US UP ON THE WEB athttp://www.sankaranethralaya.org
Please forward your correct address with your E-mail address if any,to enable us to update our address data base.
7
Posterior scleritis remains one of theunder diagnosed treatable conditions inophthalmology. Awareness of the entity,typical clinical features, ancillary tests likefundus fluorescein angiography and inparticular ultrasonography can establish thediagnosis in majority of cases. The varioustreatment modalities described are retrobulbarinjection of corticosteroid, oral steroid, non-steroidal anti-inflammatory agents (NSAIDs)and systemic immunosuppressive agents 1.Intra venous methylprednisolone (IVMP) hasbeen described in severe uveitis, but its rolein posterior scleritis has been reported rarelyin literature. Mc clauskey et.al reportedsuccessful resolution of 13 cases of severeanterior scleritis and 1 case of posteriorscleritis2. We report a case of posterior scleritiswith profound, painless visual impairment,which resolved successfully following a courseof 3 days of IVMP.
Rapid Resolution of Posterior Scleritisfollowing Intravenous MethylprednisoloneTherapyRupak Kanti Biswas and Jyotirmay Biswas
CASE SUMMARY:
A 49year old female presented withsudden onset of decreased vision in right eyeof 1 day duration, which was not associatedwith pain or redness. She was alsocomplaining of seeing black area in centralregion of the right eye. There was no complaintin left eye. Her past history did not revealany systemic diseases like diabetes,hypertension. There was no history of jointpain, skin rashes, erythema or lymph nodeenlargement.
On examination her best-corrected visualacuity was counting finger at ½ meter, <N36in right eye and 6/6, N6 in left eye. Pupillaryreaction was brisk and well sustained in botheyes with no relative afferent pupillary defect.Slit lamp examination revealed unremarkablefindings except early posterior subcapsularcataract in both eyes. There were no active
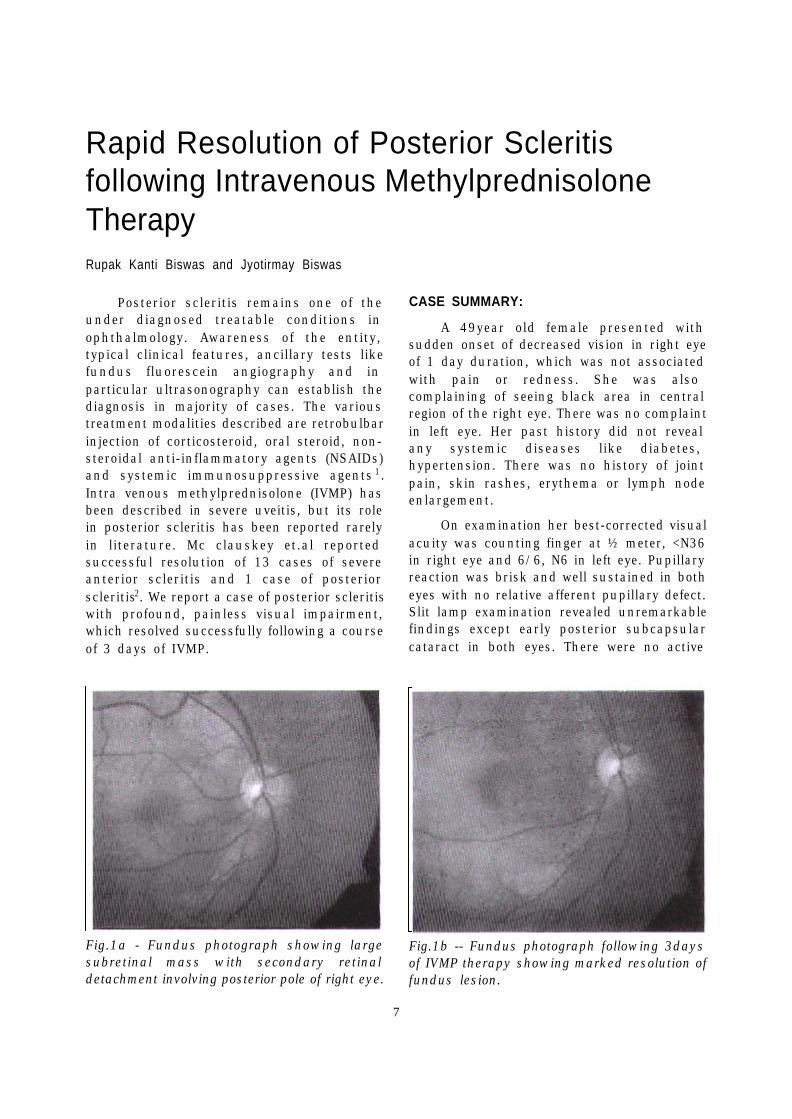
Fig.1a - Fundus photograph showing largesubretinal mass with secondary retinaldetachment involving posterior pole of right eye.
Fig.1b -- Fundus photograph following 3daysof IVMP therapy showing marked resolution offundus lesion.
1 2
8
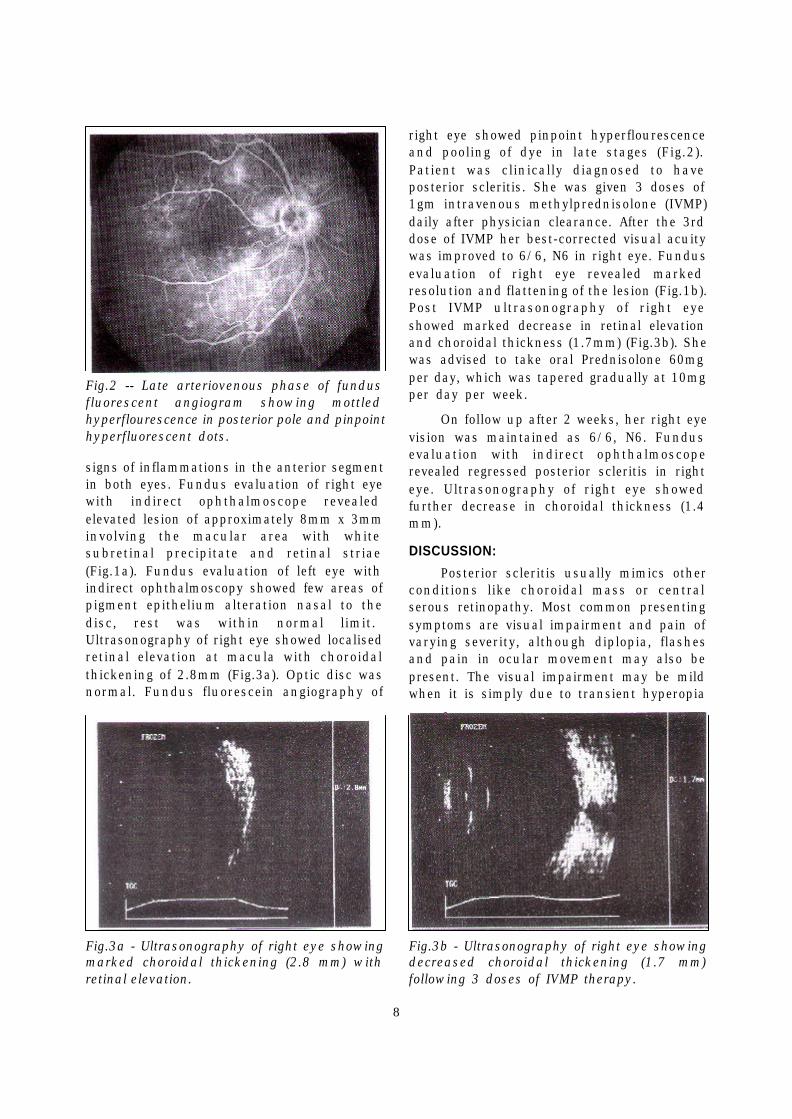
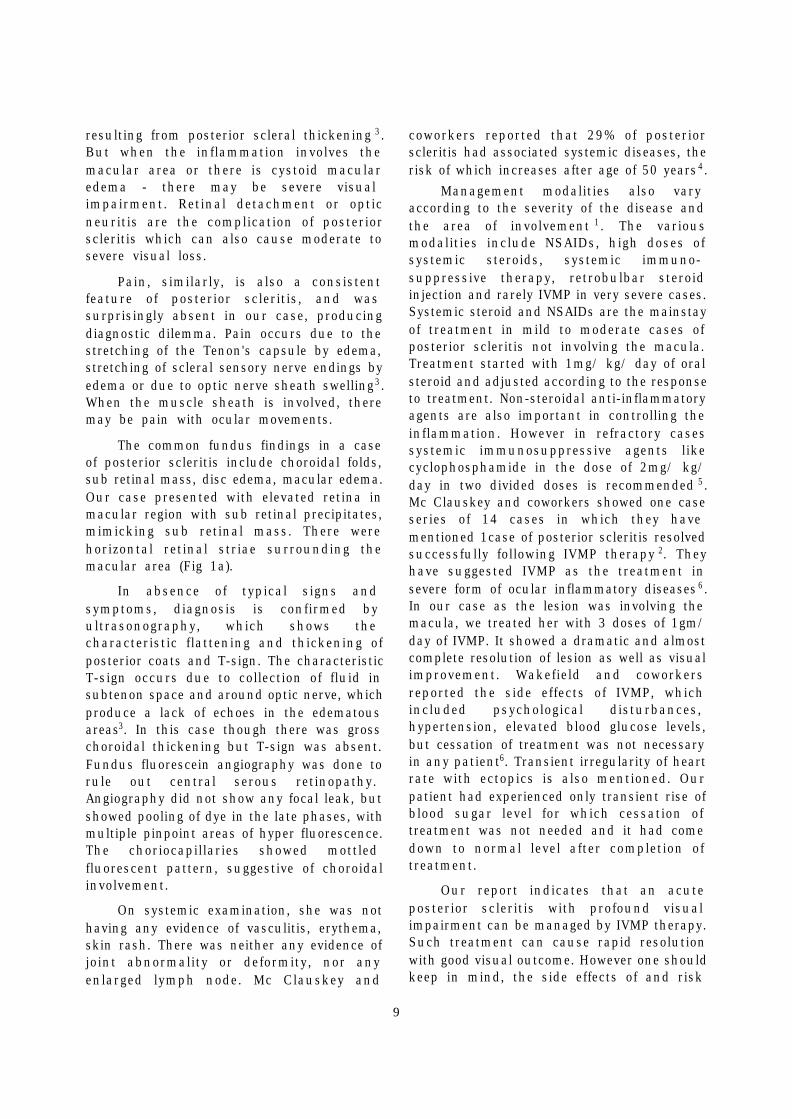
right eye showed pinpoint hyperflourescenceand pooling of dye in late stages (Fig.2).Patient was clinically diagnosed to haveposterior scleritis. She was given 3 doses of1gm intravenous methylprednisolone (IVMP)daily after physician clearance. After the 3rddose of IVMP her best-corrected visual acuitywas improved to 6/6, N6 in right eye. Fundusevaluation of right eye revealed markedresolution and flattening of the lesion (Fig.1b).Post IVMP ultrasonography of right eyeshowed marked decrease in retinal elevationand choroidal thickness (1.7mm) (Fig.3b). Shewas advised to take oral Prednisolone 60mgper day, which was tapered gradually at 10mgper day per week.
On follow up after 2 weeks, her right eyevision was maintained as 6/6, N6. Fundusevaluation with indirect ophthalmoscoperevealed regressed posterior scleritis in righteye. Ultrasonography of right eye showedfurther decrease in choroidal thickness (1.4mm).
DISCUSSION:
Posterior scleritis usually mimics otherconditions like choroidal mass or centralserous retinopathy. Most common presentingsymptoms are visual impairment and pain ofvarying severity, although diplopia, flashesand pain in ocular movement may also bepresent. The visual impairment may be mildwhen it is simply due to transient hyperopia
Fig.2 -- Late arteriovenous phase of fundusfluorescent angiogram showing mottledhyperflourescence in posterior pole and pinpointhyperfluorescent dots.
Fig.3a - Ultrasonography of right eye showingmarked choroidal thickening (2.8 mm) withretinal elevation.
Fig.3b - Ultrasonography of right eye showingdecreased choroidal thickening (1.7 mm)following 3 doses of IVMP therapy.
signs of inflammations in the anterior segmentin both eyes. Fundus evaluation of right eyewith indirect ophthalmoscope revealedelevated lesion of approximately 8mm x 3mminvolving the macular area with whitesubretinal precipitate and retinal striae(Fig.1a). Fundus evaluation of left eye withindirect ophthalmoscopy showed few areas ofpigment epithelium alteration nasal to thedisc, rest was within normal limit.Ultrasonography of right eye showed localisedretinal elevation at macula with choroidalthickening of 2.8mm (Fig.3a). Optic disc wasnormal. Fundus fluorescein angiography of
3
45
9
resulting from posterior scleral thickening 3.But when the inflammation involves themacular area or there is cystoid macularedema - there may be severe visualimpairment. Retinal detachment or opticneuritis are the complication of posteriorscleritis which can also cause moderate tosevere visual loss.
Pain, similarly, is also a consistentfeature of posterior scleritis, and wassurprisingly absent in our case, producingdiagnostic dilemma. Pain occurs due to thestretching of the Tenon's capsule by edema,stretching of scleral sensory nerve endings byedema or due to optic nerve sheath swelling3.When the muscle sheath is involved, theremay be pain with ocular movements.
The common fundus findings in a caseof posterior scleritis include choroidal folds,sub retinal mass, disc edema, macular edema.Our case presented with elevated retina inmacular region with sub retinal precipitates,mimicking sub retinal mass. There werehorizontal retinal striae surrounding themacular area (Fig 1a).
In absence of typical signs andsymptoms, diagnosis is confirmed byultrasonography, which shows thecharacteristic flattening and thickening ofposterior coats and T-sign. The characteristicT-sign occurs due to collection of fluid insubtenon space and around optic nerve, whichproduce a lack of echoes in the edematousareas3. In this case though there was grosschoroidal thickening but T-sign was absent.Fundus fluorescein angiography was done torule out central serous retinopathy.Angiography did not show any focal leak, butshowed pooling of dye in the late phases, withmultiple pinpoint areas of hyper fluorescence.The choriocapillaries showed mottledfluorescent pattern, suggestive of choroidalinvolvement.
On systemic examination, she was nothaving any evidence of vasculitis, erythema,skin rash. There was neither any evidence ofjoint abnormality or deformity, nor anyenlarged lymph node. Mc Clauskey and
coworkers reported that 29% of posteriorscleritis had associated systemic diseases, therisk of which increases after age of 50 years4.
Management modalities also varyaccording to the severity of the disease andthe area of involvement 1. The variousmodalities include NSAIDs, high doses ofsystemic steroids, systemic immuno-suppressive therapy, retrobulbar steroidinjection and rarely IVMP in very severe cases.Systemic steroid and NSAIDs are the mainstayof treatment in mild to moderate cases ofposterior scleritis not involving the macula.Treatment started with 1mg/ kg/ day of oralsteroid and adjusted according to the responseto treatment. Non-steroidal anti-inflammatoryagents are also important in controlling theinflammation. However in refractory casessystemic immunosuppressive agents likecyclophosphamide in the dose of 2mg/ kg/day in two divided doses is recommended 5.Mc Clauskey and coworkers showed one caseseries of 14 cases in which they havementioned 1case of posterior scleritis resolvedsuccessfully following IVMP therapy 2. Theyhave suggested IVMP as the treatment insevere form of ocular inflammatory diseases 6.In our case as the lesion was involving themacula, we treated her with 3 doses of 1gm/day of IVMP. It showed a dramatic and almostcomplete resolution of lesion as well as visualimprovement. Wakefield and coworkersreported the side effects of IVMP, whichincluded psychological disturbances,hypertension, elevated blood glucose levels,but cessation of treatment was not necessaryin any patient6. Transient irregularity of heartrate with ectopics is also mentioned. Ourpatient had experienced only transient rise ofblood sugar level for which cessation oftreatment was not needed and it had comedown to normal level after completion oftreatment.
Our report indicates that an acuteposterior scleritis with profound visualimpairment can be managed by IVMP therapy.Such treatment can cause rapid resolutionwith good visual outcome. However one shouldkeep in mind, the side effects of and risk
10
involved in intravenous methylprednisolonetherapy.
REFERENCES:
1. Mc Clauskey P, Wakefield D: Currentconcepts in management of scleritis: AustN Z J Ophthalmol 1988 Aug; 16: 169- 176.
2. Mc Clauskey P, Wakefield D.: Intravenouspulse methylprednisolone therapy inscleritis: Arch Ophthalmol 1987; 105: 793-797.
3. The Sclera: C. Stephen Foster, Maite Sainzde la Maza: Springer- Verlag, New York1994: page 112-124.
4. Mc Clauskey P, Watson PG, Lightman S,Haybittle J, Restori M, Branley M: Posteriorscleritis: Clinical features, systemicassociations and outcome in a large seriesof patients: Ophthalmology 1999 Dec; 106:2380-2386.
5. Joseph A, Biswas J, Sitalakshmi G, GopalL, Badrinath S.S.: Surgically InducedNecrotising Scleritis (SINS) - Report of twocases: Ind J Ophthalmol 1997; 45: 43-45.
6. Wakefield D, Mc Clauskey P, Penny R:Intravenous pulse methylprednisolonetherapy in severe inflammatory eyedisease: Arch Ophthalmol 1986 Jun; 104:847-851.
CME PROGRAMMES FOR THE SILVER JUBILEE YEAR 2002 – 2003
This Academic Year being the “Silver Jubilee Year” of Sankara Nethralayaattracts special significance and importance. Apart from the continuous effortsdirected towards improvement of Patient’s Care and Patient’s Education onprevention and cure, the foundation has also lined up various CME Programmesfor Ophthalmologists and Optometrists for updating their skill and knowledge.
Sl.No. Topics Date
1. Update in Neuro-ophthalmology 26.10.2002 to 27.10.2002
2. Low Vision Aids 30.11.2002
3. Small Incision Cataract Surgery 14.12.2002 & 15.12.2002
4. Cornea 07.03.2003 to 09.03.2003
5. Revision course in ophthalmology for 25.06.2003 to 01.07.2003FRCS / MRCS exam going students
6. Paediatric Ophthalmology 05.07.2003 & 06.07.2003
7. Vitreo-retina 07.09.2003 & 08.09.2003
8. Glaucoma 06.12.2003 & 07.12.2003
The programmes are aimed to provide continuing medical education to the practisingOphthalmologists, Residents in Ophthalmology and to the Optometrists.
FOR MORE DETAILS, PLEASE CONTACT
Mr. N. SivakumarThe Academic Officer
SANKARA NETHRALAYA18, College Road, CHENNAI – 600 006
Fax: 91-44-8254180 Email: [email protected]
11
Bilateral Retinal Vascular Occlusion Secondaryto Septic Emboli arising from a Scrotal Ulcer inA Child – A Case ReportAmit Nagpal, Jyotirmay Biswas and Kannan M Narayanan
ABSTRACT
A 4-year old child with features ofbacterial septicemia and a scrotal ulcer of 20days duration presented with acute onsetprofound bilateral loss of vision. Examinationrevealed central retinal vein occlusion in oneeye and branch retinal artery occlusion in theother eye. The child received intravenousmethyl prednisolone, antibiotics and ACTH.At 3 months follow up there was partial visualrecovery in one eye.
This retrospective interventional casereport illustrates that pediatric patientspresenting with retinal vascular occlusionshould be thoroughly examined for the septicfoci. Aggressive therapy with intravenoussteroids and antibiotics may be useful inrestoring functional vision.
INTRODUCTION
There are a few isolated case reports ofcombined retinal vascular occlusions in theliterature.1-5 In most of these instances the
occurrence was unilateral. One third of thesecases are reported to be due to retrobulbarinjection6. Other causes reported includevasculitis, neoplastic infiltration of optic nerveand septic emboli from sources like infectiveendocarditis. We further report a case ofbilateral vascular occlusion in a 4 year oldchild, in whom there were concomitantfeatures of bacterial septicemia secondary toa scrotal ulcer. There was partial visualrecovery in one eye at 3 month follow up.
CASE REPORT
A 4-year old boy was referred to us withthe complaint of sudden painless profoundloss of vision in both eyes. He had fever,erythematous maculopapular rash, anasarca,multiple generalized lymphadenopathy,hepatosplenomegaly and a scrotal ulcer forthe last 20 days. Echocardiography was doneto rule out infective endocarditis. A diagnosisof gram-negative septicemia was made andintravenous antibiotics; ceftazidime, ofloxacin
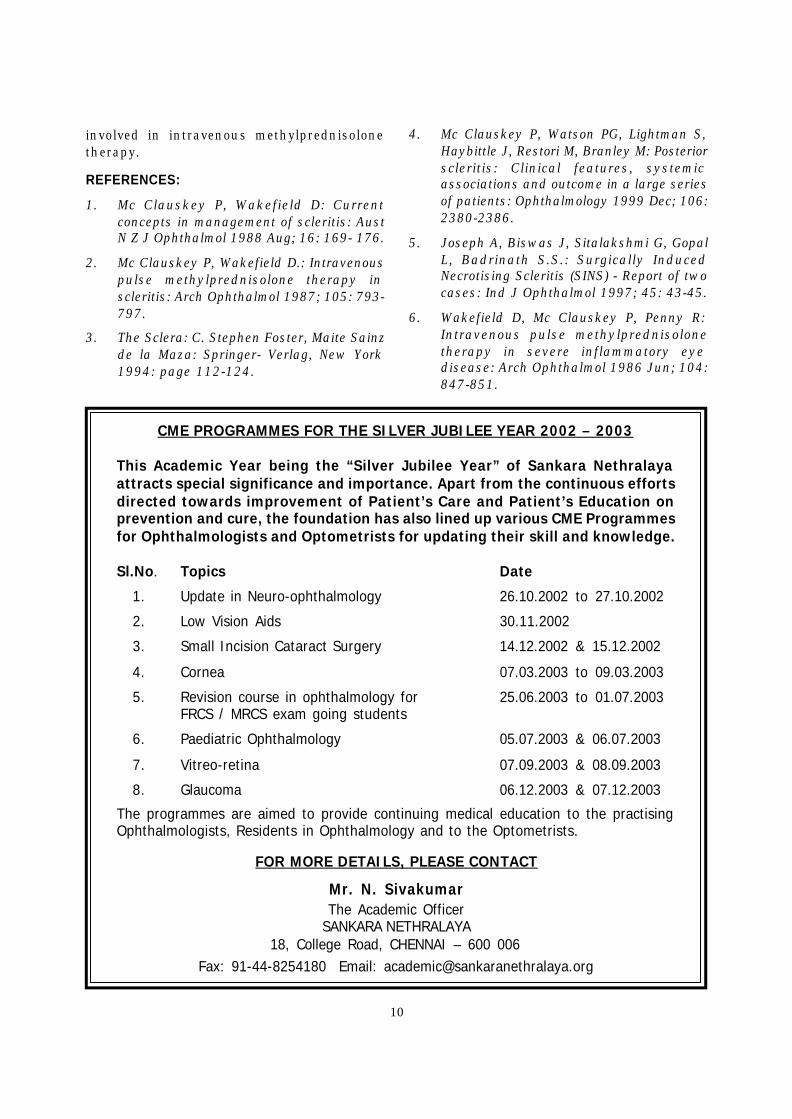
FIG 1: Fundus photograph of right eye at thefirst presentation, suggestive of central retinalvein occlusion.
FIG 2: Fundus photograph of the left eye atthe first presentation, suggestive ofinferotemporal branch retinal artery occlusionsecondary to arteritis.
67
12
and metronidazole were administered,following which he developed sudden loss ofvision in both the eyes for which he was givenintravenous methyl prednisolone and ACTH.A computerized tomography scan of brain wasdone which was with in normal limits.
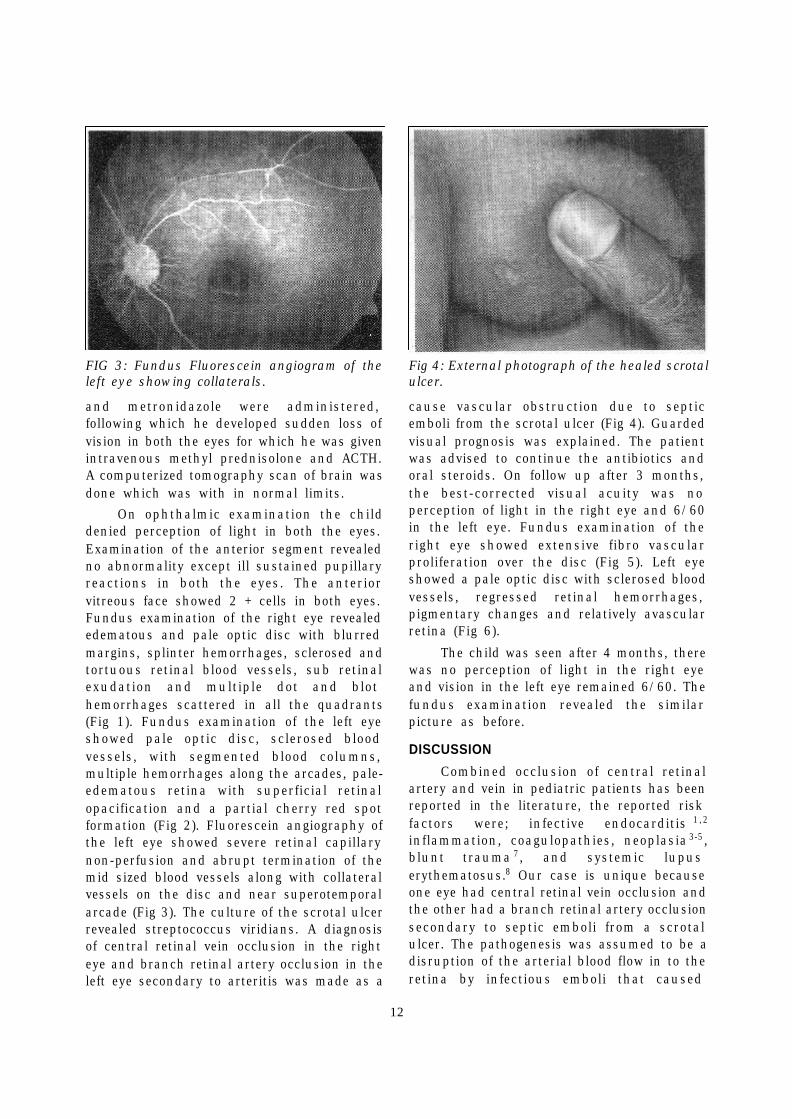
On ophthalmic examination the childdenied perception of light in both the eyes.Examination of the anterior segment revealedno abnormality except ill sustained pupillaryreactions in both the eyes. The anteriorvitreous face showed 2 + cells in both eyes.Fundus examination of the right eye revealededematous and pale optic disc with blurredmargins, splinter hemorrhages, sclerosed andtortuous retinal blood vessels, sub retinalexudation and multiple dot and blothemorrhages scattered in all the quadrants(Fig 1). Fundus examination of the left eyeshowed pale optic disc, sclerosed bloodvessels, with segmented blood columns,multiple hemorrhages along the arcades, pale-edematous retina with superficial retinalopacification and a partial cherry red spotformation (Fig 2). Fluorescein angiography ofthe left eye showed severe retinal capillarynon-perfusion and abrupt termination of themid sized blood vessels along with collateralvessels on the disc and near superotemporalarcade (Fig 3). The culture of the scrotal ulcerrevealed streptococcus viridians. A diagnosisof central retinal vein occlusion in the righteye and branch retinal artery occlusion in theleft eye secondary to arteritis was made as a
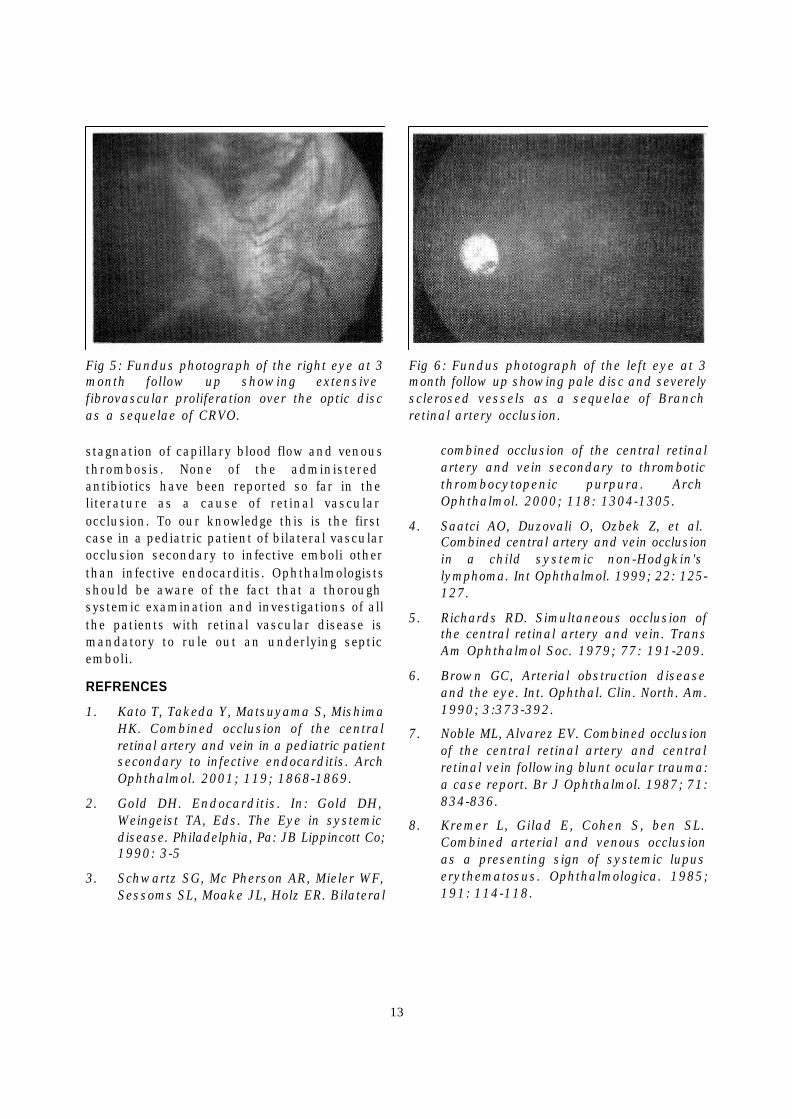
cause vascular obstruction due to septicemboli from the scrotal ulcer (Fig 4). Guardedvisual prognosis was explained. The patientwas advised to continue the antibiotics andoral steroids. On follow up after 3 months,the best-corrected visual acuity was noperception of light in the right eye and 6/60in the left eye. Fundus examination of theright eye showed extensive fibro vascularproliferation over the disc (Fig 5). Left eyeshowed a pale optic disc with sclerosed bloodvessels, regressed retinal hemorrhages,pigmentary changes and relatively avascularretina (Fig 6).
The child was seen after 4 months, therewas no perception of light in the right eyeand vision in the left eye remained 6/60. Thefundus examination revealed the similarpicture as before.
DISCUSSION
Combined occlusion of central retinalartery and vein in pediatric patients has beenreported in the literature, the reported riskfactors were; infective endocarditis 1,2
inflammation, coagulopathies, neoplasia 3-5 ,blunt trauma 7, and systemic lupuserythematosus.8 Our case is unique becauseone eye had central retinal vein occlusion andthe other had a branch retinal artery occlusionsecondary to septic emboli from a scrotalulcer. The pathogenesis was assumed to be adisruption of the arterial blood flow in to theretina by infectious emboli that caused
FIG 3: Fundus Fluorescein angiogram of theleft eye showing collaterals.
Fig 4: External photograph of the healed scrotalulcer.
8 9
13
stagnation of capillary blood flow and venousthrombosis. None of the administeredantibiotics have been reported so far in theliterature as a cause of retinal vascularocclusion. To our knowledge this is the firstcase in a pediatric patient of bilateral vascularocclusion secondary to infective emboli otherthan infective endocarditis. Ophthalmologistsshould be aware of the fact that a thoroughsystemic examination and investigations of allthe patients with retinal vascular disease ismandatory to rule out an underlying septicemboli.
REFRENCES
1. Kato T, Takeda Y, Matsuyama S, MishimaHK. Combined occlusion of the centralretinal artery and vein in a pediatric patientsecondary to infective endocarditis. ArchOphthalmol. 2001; 119; 1868-1869.
2. Gold DH. Endocarditis. In: Gold DH,Weingeist TA, Eds. The Eye in systemicdisease. Philadelphia, Pa: JB Lippincott Co;1990: 3-5
3. Schwartz SG, Mc Pherson AR, Mieler WF,Sessoms SL, Moake JL, Holz ER. Bilateral
combined occlusion of the central retinalartery and vein secondary to thromboticthrombocytopenic purpura. ArchOphthalmol. 2000; 118: 1304-1305.
4. Saatci AO, Duzovali O, Ozbek Z, et al.Combined central artery and vein occlusionin a child systemic non-Hodgkin'slymphoma. Int Ophthalmol. 1999; 22: 125-127.
5. Richards RD. Simultaneous occlusion ofthe central retinal artery and vein. TransAm Ophthalmol Soc. 1979; 77: 191-209.
6. Brown GC, Arterial obstruction diseaseand the eye. Int. Ophthal. Clin. North. Am.1990; 3:373-392.
7. Noble ML, Alvarez EV. Combined occlusionof the central retinal artery and centralretinal vein following blunt ocular trauma:a case report. Br J Ophthalmol. 1987; 71:834-836.
8. Kremer L, Gilad E, Cohen S, ben SL.Combined arterial and venous occlusionas a presenting sign of systemic lupuserythematosus. Ophthalmologica. 1985;191: 114-118.
Fig 5: Fundus photograph of the right eye at 3month follow up showing extensivefibrovascular proliferation over the optic discas a sequelae of CRVO.
Fig 6: Fundus photograph of the left eye at 3month follow up showing pale disc and severelysclerosed vessels as a sequelae of Branchretinal artery occlusion.
1110
14
Introduction:
Colour vision plays a crucial role in ourday today living. Though a concept taken forgranted it has enormorous clinicalapplications. Colour vision appears to be welldeveloped soon after birth, by the age of 2 or3 months, the infant has good colourdiscrimination ability as that of adults1.
Most clinicians are aware that colourvision is anomalous in a relatively largepercentage of the male population and a muchsmaller percentage of women. About 1 in 12males and 1 in 200 females have anomalouscolour vision of the Red-green type, but only1 in every 50,000 males & females haveinherited anomalous Blue-Yellow vision2. Thisdefect is inherited constant throughout lifeand cannot be cured in the usual clinicalsense.
As colour vision is being used more inthe work place, poor performance in a jobmay be related to defective colour vision.Mostly the hereditary linked colour visiondeficiency goes undetected, as the person willbe 'asymptomatic'. Mostly, its only during thetime of vision screening that many get to knowabout their colour deficiency, sometimes itmight be during a crucial time of a jobselection.
The current increased relevance of colourvision in the workstation demands a parallelincrease in interest in assisting persons withcolour defects. One of the popular ways ofassisting is the use of x-chrom contact lens.
Background knowledge:Dichoptic colour experiments were
performed with colour normals and withprotanopes and deutranopes. Experimentsindicate that the cortical perception achievedby summing input of each eye when one eyehas a filter in front of it may aid colourdiscrimination for dichromats3.
X-Chrom Contact LensS Premnandhini
The red filter when used gives brighteningof reds relative to other colours. These changesin relative brightness can of course be seenby any person whether his colour vision isnorma or defective. With the red filters, thegreen becomes darker and red remains bright.For colour-normal person, this tells him littlemore than he had already seen, but for thedichromat this is new information and he canmake the Red-Green distinctions, which hecouldn't make before4.
It should be noted that, the colouredfilters enables to differentiate betweencertain colours and are definitely not"cures" for colour defects. There is no knownfilter that allows a colour defective to have anormal colour vision.
X - Chrom contact lens:
The best-known filter that is specificallypromoted as an aid for colour defectivepatients is the X-Chrom lens, which isavailable as a hard and soft contact lens.Indeed, the X-Chrom contact lens is a redlens that allows some blue light transmission.In 1971 Zeltzer introduced the hard X-chromcontact lens in polymethyl meth acrylate forwear on one eye5. The lens is not only intendedto produce differences in intensity betweenthe two eyes6,7. The lens helps colour defectivepatients whose occupation calls fordifferentiating browns, greens, oranges, reds,purples and blues. Its usefulness probablyresults from the brightness difference cuesfor different colours in each eye, thestereolustre effect that occurs when objectson one eye are very different from the otherand small chromaticity (colour) shifts that anbe produced by this filter.
The X-Chrom contact lens is worn onthe non-dominant eye of colour deficientindividuals (dichromats & anomaloustrichromats). The fitting procedure is the sameas that of any conventional contact lens.
15
Clinicians are cautioned that the clearimprovement of performance on Ishihara,Drorine and AO pseudoisochromatic plateswith this lens, or infact most red filters, doesnot reflect comparable improvement in colourdiscrimination in the real world. The improvedperformance in the test plates can beattributed to the fact that a red filteressentially destroys the carefully balanceddesign of these test plates2.
X-Chrom lens can be extremely helpfulin distinguishing colours in an array andsimply doesn't give an overall improvement incolour discrimination.
Points To Remember:
u Care should be taken not to disrupt thebinocular vision when prescribing X-Chrom lens in one eye
u Patient should be cautioned aboutwearing the lenses at night
u The patient may experience a falsedistance preception of any and allobjects in motion; this phenomenon iscalled pulfrich phenomenon8.
u Due to the intensity difference betweenthe eyes, patient may report a lustre orglittering appearance of red objects. Thepatient can learn this and otherchromatic and brightness differentials.
For totally colour-blind patients, filtersthat cut out short wavelengths (blue) can beextremely effective in improving outdoorvision2.
Case 1:
A 30 year old man came to our outpatientclinic with difficulty in colour perception. Healso reported that he was denied a governmentjob due to this deficiency. There was nohistory of any systemic illness. His bestcorrected visual acuity was 6/6+; N6 in eacheye. Anterior and posterior segment did notreveal any abnormality.
His colour vision recorded with thepseudo-isochromatic chart was noted asfollows:
OD: 1/14 (correct response)OS: 2/14 (correct response).
An X-chrom contact lens was fitted inhis non-dominant eye (OS) and the responserecorded was OU: 8/14 (correct response)
The lens maintenance and handling wasexplained and the patient was instructed touse the X-chrom contact lens only during thetime of need.
Case 2:
A 27 year old male reported to our clinicwith complaint of difficulty in colourperception. As the patient had an occupationalneed, he was interested to go in for X-chromcontact lens.
His initial colour vision was 0/14 (eithereye), tested with Ishihara's test plates. Withred filter in either eye (OD / OS) the correctresponse was noted as 1/14 (measuredbinocularly).
With red filter in both eyes, colour visionwas noted as 14/14 correct response.
Usually a X-chrom contact lens will befitted only in one eye (non-dominant eye). Case1 obeys this rule whereas in Case 2,interestingly, the patient improved only withX-chrom contact lenses in both eyes.
The speciality of colour vision is vast andthe use of X-chrom contact lens is only at itsincipient stage in our country. The secondcase presented in this paper makes us wonderabout the complexities involved in colourvision and more research is needed in thisarea.
References:
1. Banks MS, Salapatek P. Infant VisualPerception. In: Haith M, Campos J, eds.Biology and infancy. Hand book of ChildPsychology. New York: John Wiley & Sons,1983: 435-571
2. Amos.J.F. Diagnosis and Management invision care, Butterworths:1987;671
3. Leonard Polizzotto, Dichoptic colourperception & the X-Chrom lens 1981;58(12) 1180 - 671
16
4. Wilson JA, Robinson JO, Binocular Filtersas an Aid to color Discrimination byDichromats, Amer Journal of Optom &physiol optics 1980; 57: 893 - 901
5. Zeltzer H, the X-Chrom lens. Journal ofAmerican Optometric Association1971;42:933-999
6. Zeltzer H.I, The X-Chrom contact lens &colour deficiency, Opt J Rev Optom, 1973:110 (5); 15-19
7. Zeltzer HI, A Typical case study correctingcolor deficiency. J Am Optom Assos 1975;46(6): 622 - 626
8. Reading R.W, Binocular Vision Foundation& Applications, Butterworths, Boston,1983; 151-154
AN APPEALA lot of things in this world depend on money - security, shelter, education and evenhealth. But at Nethralaya, money has ceased to be a pre-requisite for sight.Day after day, year after year, Nethralaya treats hundreds of patients absolutely freeof cost and gives them back their sight. Treatment is provided free of cost to allpatients with a monthly income below Rs.1,750/-.Yet there is no discrimination between the free patient and the one who pays. Apartfrom the treatment, food, medicines and travel expenses are absolutely free.Those free patients depend on Nethralaya, and Nethralaya depends on you.So, come and join the OPHTHALMIC MISSION TRUST.For questions about tax exempt status and contributions, please contact:
Mr S V Acharya,Treasurer
Ophthalmic Mission Trust Inc. (OM Trust)14613, Pommel Drive, Rockville,
MD 20850, U.S.A.Phone: (301)251 0378
INTERNET e-mail : [email protected]
For those of you in India and elsewhere, please contact:Dr S S Badrinath,
President & ChairmanSankara Nethralaya
(UNIT OF MEDICAL RESEARCH FOUNDATION)18 College Road, Chennai 600 006
Phone: 826 1265, 827 1616Fax: (044) 825 4180, 821 0117
INTERNET e-mail : [email protected] US UP ON THE WEB at http://www.sankaranethralaya.org
http://www.omtrust.orgGIVE ONLINE @ www.icicicommunities.org
COME, GIVE THE GIFT OF SIGHT

17
increased corneal diameter with iris adherentto posterior corneal surface, ciliary bodyatrophy and disorganization, presence of largeundifferentiated basophilic tumor cellsinterspersed with extensive areas of necrosis,calcification, haemorrhage and fibrous tissue.Tumor cells extended till the posterior cornealsurface involving the angle, which was closed.Focal choroidal and pre-laminar optic nerveinvasion was present.
The child was lost to follow up andexamined again after a month, with righteyelid edema, chemosis, mucopurulentdischarge, steamy cornea and shallow anteriorchamber. Histopathological examination of theenucleated right eye showed poorlydifferentiated and markedly necrotic tumorfilling the vitreous cavity with ciliary bodynecrosis, choroidal and extrascleral invasion.The child was referred to the local cancerhospital for chemotherapy and radiotherapy.
Case-2In 1995, a 1-year-old male was brought
to us after the parents noticed a white reflexin the left eye, following a fall. The left eyeshowed signs of orbital cellulitis such asperiorbital edema, proptosis, conjunctivalchemosis, buphthalmos, corneal edema,extensive rubeosis with dilated andnonreacting pupil, leukocoria and no view ofthe fundus. IOP could not be assessed due toperiorbital edema. Right eye fundus showedReese Ellsworth stage 5B retinoblastoma.Ultrasound and CT- Scan of left eye showedevidence of retinoblastoma with suspicion ofextraocular extension.
Left eye was enucleated which onhistopathological examination showed closedangle, poorly differentiated and extensivelynecrotic tumor filling the vitreous cavity, irisnecrosis, iris and ciliary body haemorrhage,focal choroidal invasion, post-laminar opticnerve invasion and no extrascleral extension(Figure-1). The patient underwent externalbeam radiation for the right eye, following
IntroductionRetinoblastoma commonly presents as
leukocoria and strabismus; rarely as uveitis,spontaneous hyphaema, preseptal cellulitis,pseudohypopyon, secondary glaucoma andphthisis bulbi. 1 Orbital cellulitis likemanifestation, though rare has beenpreviously reported by Shields et al 2 andMullaney et al,3 the prevalence being 1.3% in450 cases and 4.8% in 292 cases respectively.Many previously described cases ofretinoblastoma presenting as orbital cellulitis,have had marked associated anterior segmentinvolvement, including corneal opacificationand enlargement, glaucoma, uveitis, andrubeosis iridis. 2,3
We report the clinical and histopatho-logical features of four retinoblastoma patientspresenting with orbital cellulitis. The orbitalcellulitis like picture may be misdiagnosed tobe of infective etiology leading to impropermedical treatment, delaying institution ofappropriate treatment such as enucleation.This clinical implication and the rarity of sucha presentation make it important to recognizeorbital cellulitis like presentation ofretinoblastoma.
Case reportsCase -1
In 1991, a 21-month-old male childpresented to us with diminution of vision, lidedema and ecchymosis, steamy cornea,shallow anterior chamber, minimal hyphaemaand low intraocular pressure (IOP) in the righteye, of 3 weeks duration. His left eye wasbuphthalmic with corneal vascularization,multiple macular opacities, anterior chambercalcific deposits and normal IOP. Fundusexamination could not be done in either eyedue to corneal opacity. Ultrasound and CT-Scan examination of orbit showed intraocularmass lesions with calcification suggestive ofretinoblastoma. The child underwentenucleation of his left eye. Histopathologicalexamination of the enucleated eye showed
Retinoblastoma mimicking Orbital CellulitisManisha Agarwal, Jyotirmay Biswas, Krishna Kumar and Mahesh P Shanmugam
18
which the tumor regressed. The child wassubsequently lost for follow up.
Case-3In 1998, a 3- month- old male child
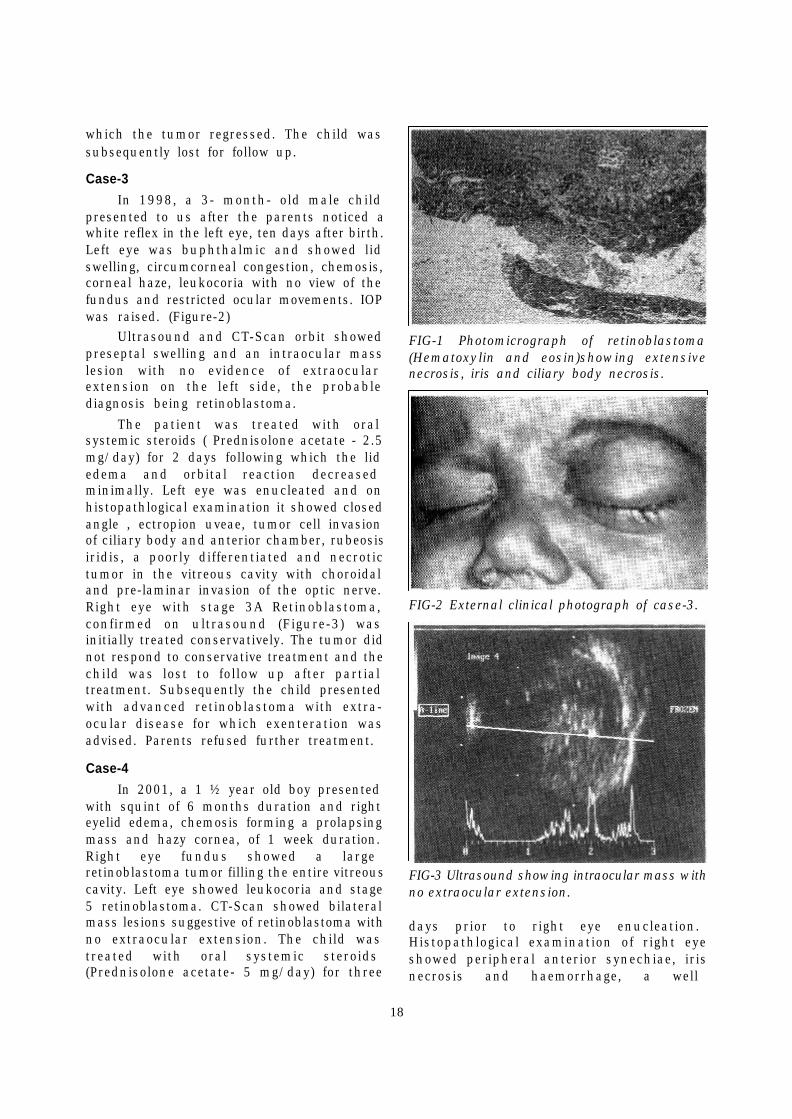
presented to us after the parents noticed awhite reflex in the left eye, ten days after birth.Left eye was buphthalmic and showed lidswelling, circumcorneal congestion, chemosis,corneal haze, leukocoria with no view of thefundus and restricted ocular movements. IOPwas raised. (Figure-2)
Ultrasound and CT-Scan orbit showedpreseptal swelling and an intraocular masslesion with no evidence of extraocularextension on the left side, the probablediagnosis being retinoblastoma.
The patient was treated with oralsystemic steroids ( Prednisolone acetate - 2.5mg/day) for 2 days following which the lidedema and orbital reaction decreasedminimally. Left eye was enucleated and onhistopathlogical examination it showed closedangle , ectropion uveae, tumor cell invasionof ciliary body and anterior chamber, rubeosisiridis, a poorly differentiated and necrotictumor in the vitreous cavity with choroidaland pre-laminar invasion of the optic nerve.Right eye with stage 3A Retinoblastoma,confirmed on ultrasound (Figure-3) wasinitially treated conservatively. The tumor didnot respond to conservative treatment and thechild was lost to follow up after partialtreatment. Subsequently the child presentedwith advanced retinoblastoma with extra-ocular disease for which exenteration wasadvised. Parents refused further treatment.
Case-4In 2001, a 1 ½ year old boy presented
with squint of 6 months duration and righteyelid edema, chemosis forming a prolapsingmass and hazy cornea, of 1 week duration.Right eye fundus showed a largeretinoblastoma tumor filling the entire vitreouscavity. Left eye showed leukocoria and stage5 retinoblastoma. CT-Scan showed bilateralmass lesions suggestive of retinoblastoma withno extraocular extension. The child wastreated with oral systemic steroids(Prednisolone acetate- 5 mg/day) for three
FIG-1 Photomicrograph of retinoblastoma(Hematoxylin and eosin)showing extensivenecrosis, iris and ciliary body necrosis.
FIG-2 External clinical photograph of case-3.
FIG-3 Ultrasound showing intraocular mass withno extraocular extension.
days prior to right eye enucleation.Histopathlogical examination of right eyeshowed peripheral anterior synechiae, irisnecrosis and haemorrhage, a well
14
13
12
19
differentiated, extensively necrotic tumor withinvasion of anterior chamber and pre-laminaroptic nerve without extraocular extension. Thechild was advised chemotherapy for left eye.Two months later the left eye tumor remainedactive with secondary retinal detachment andvitreous haemorrhage. He was advisedenucleation, which the parents refused andwas then lost for follow up.
DiscussionOrbital cellulitis is an uncommon
presentation of retinoblastoma.2Thepathogenesis of this response is unknown.Shields et al have suggested that theinflammatory signs could be secondary to anecrotic tumor that outgrows its blood supplyor the tumor in one eye induces an immuneresponse which may lead to necrosis of thetumor in the fellow eye.2
Large necrotic tumors have a tendencyto present with orbital cellulitis like picture.3Anterior segment involvement by the tumorhas commonly been found in patients withRetinoblastoma presenting as orbitalcellulitis. 3 Meir et al and Haik et al have
suggested anterior segment involvement withnecrosis of iris and ciliary body as a triggerto inflammation in adjacent orbital softtissues.4,5 Tumor necrosis with leaching ofnecrotic products has been suggested as amechanism by Mullaney et al. 3
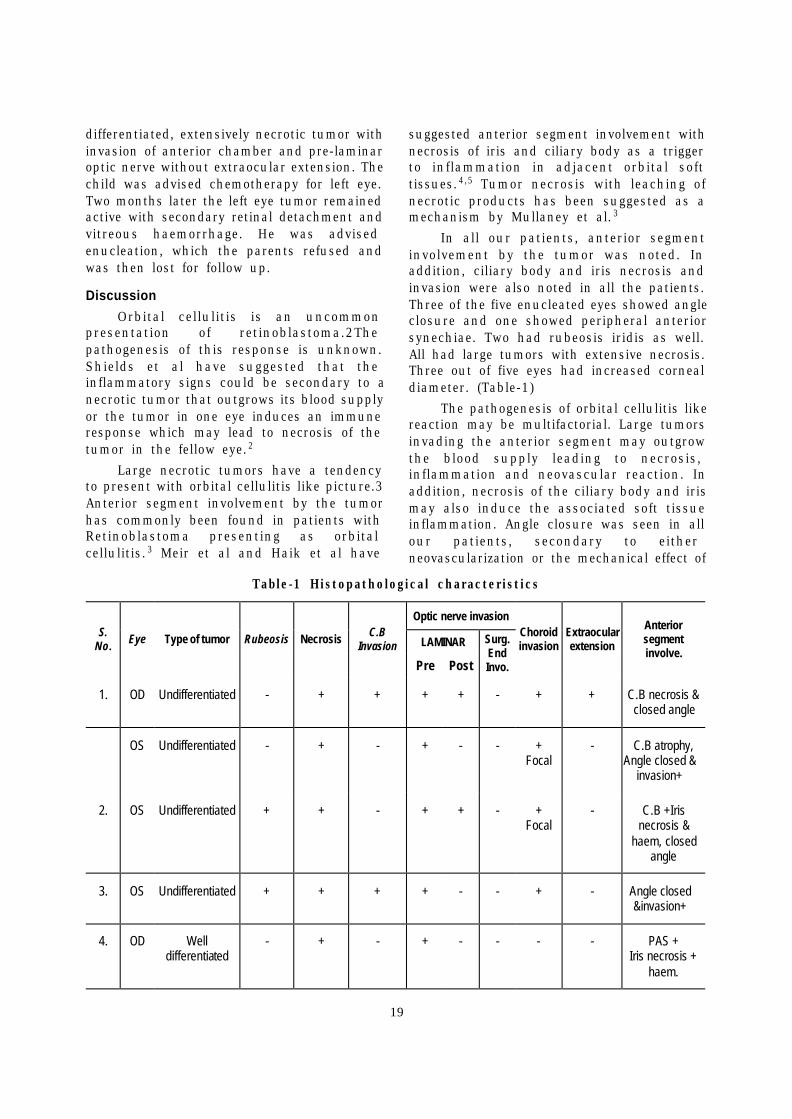
In all our patients, anterior segmentinvolvement by the tumor was noted. Inaddition, ciliary body and iris necrosis andinvasion were also noted in all the patients.Three of the five enucleated eyes showed angleclosure and one showed peripheral anteriorsynechiae. Two had rubeosis iridis as well.All had large tumors with extensive necrosis.Three out of five eyes had increased cornealdiameter. (Table-1)
The pathogenesis of orbital cellulitis likereaction may be multifactorial. Large tumorsinvading the anterior segment may outgrowthe blood supply leading to necrosis,inflammation and neovascular reaction. Inaddition, necrosis of the ciliary body and irismay also induce the associated soft tissueinflammation. Angle closure was seen in allour patients, secondary to eitherneovascularization or the mechanical effect of
Table-1 Histopathological characteristics
Optic nerve invasion
LAMINAR S.
No. Eye Type of tumor Rubeosis Necrosis C.B Invasion
Pre Post
Surg. End Invo.
Choroid invasion
Extraocular extension
Anterior segment involve.
1. OD Undifferentiated - + + + + - + + C.B necrosis & closed angle
OS Undifferentiated - + - + - - + Focal
- C.B atrophy, Angle closed &
invasion+
2. OS Undifferentiated + + - + + - + Focal
- C.B +Iris necrosis &
haem, closed angle
3. OS Undifferentiated + + + + - - + - Angle closed &invasion+
4. OD Well differentiated
- + - + - - - - PAS + Iris necrosis +
haem.

20
the tumor pressing the iris-lens diaphragmforwards. This may lead to increased IOPcausing further ischaemia and necrosis of thetumor, thereby setting up a vicious cycle. Thusthe combination of raised IOP and extensiveinflammation due to extensive tumor necrosis,ciliary body and iris necrosis may give rise toorbital cellulitis like reaction. Despite most ofthe previously reported cases of orbitalcellulitis not having extraocular invasion,oneeye in our series and one reported by Mullaneyet al showed extraocular disease. Hence acareful pre-operative orbital imaging with CT-Scan or MRI is very essential to rule outextraocular disease in these patients.
Most of the children with orbital cellulitislike reaction present with a hazy mediaobscuring fundus details. The presence ofpseudohypopyon, anterior segment inflam-matory signs may also mimic an inflammatoryetiology and not retinoblastoma. Thedifferentiating features are absence of systemicsymptoms such as high fever, history offrontoethmoidal sinusitis, normal pupils andfundi on examination, leukocytosis, positiveblood culture and cloudy sinuses oninvestigation.2 However in all children withorbital cellulitis like presenting picture wherethe fundus could not be seen, an imagingstudy is essential to rule out intraocularretinoblastoma. The difference on CT-Scanbeing that retinoblastoma appears as anintraocular mass lesion often with calcificationand in cases of true infectious cellulitis thesoft-tissue swelling is confined to the anteriorportion of the orbit adjacent to a cloudysinus.2 Delay in the diagnosis ofretinoblastoma can lead to possibleextraocular spread.
The orbital cellulitis like reaction isusually managed with 3 days of oralcorticosteroids resulting in reduction of theperineural soft-tissue edema which is oftenresponsible for false-positive interpretation ofthe tumor invasion into the optic nerve onCT-Scan.6 Intravenous prednisolone in thedose of 1mg/kg which can be increased to1.5mg/kg if the resolution is slow, has alsobeen advocated.3 In most of the children theinflammation decreases after 5 days oftreatment to enable enucleation. It is essential
to decrease the associated orbitalinflammation preoperatively to facilitateenucleation and obtaining a long optic nervestump.
In conclusion, advanced necroticretinoblastoma often involves the anteriorsegment and can give rise to orbital cellulitislike picture. It is essential to differentiate thisfrom infective orbital cellulitis to enable propermanagement.We recommend that all childrenpresenting with signs of orbital or ocularinflammation should have a completeophthalmic examination including a fundusexamination. If the fundus is not visible or incase of doubt, ultrasonography, CT-Scan orMRI should be performed to exclude thediagnosis of retinoblastoma.
However one should not presume theabsence or presence extraocular extension ofthe retinoblastoma based on only clinicalfindings.
References:
1. Mullaney PB, Karcioglu ZA, al-Mesfer S,Abboud EB. Presentation of retinoblastomaas phthisis bulbi. Eye 1997; 11(Pt 3): 403-8.
2. Shields JA, Shields CL, Suvarnamani C,Schroeder RP, Potter PD. RetinoblastomaManifesting as Orbital Cellulitis. Am JOphthalmol 112:442-449,October 1991.
3. Mullany PB, Karcioglu ZA, Huaman A,Mesfer SA. Retinoblastoma associatedorbital cellulitis. Br J Ophthalmol 1998;82:517-521.
4. Meir AB, Bardenstein DS, PeifferRl.Retinoblastoma presenting with orbitalcellulites: A mechanistic hypothesis. InvestOphthalmol Vis Sci 1995; 36:S492.
5. Haik BG, Dunleavy SA, Cooke C, et al.Retinoblastoma with anterior chamberextension. Ophthalmology 1987; 94:367-70.
6. Atchaneeyasakul LO, Murphree AL.Retinoblastoma. In: Ryan SJ, Ogden TE,Hintson DR, Schachat AP. St.Louis. C.VMosby ; 2001.Vol 1,p 513-570.

21
geniculate body. Most ganglion cells in themagnocellular lamina of the lateral geniculatebody give a more transient and phasicresponse and are sensitive to motion. Theretinal ganglion cells that project to themagnocellular lamina (M cell) usually havelarger cells. M cells constitute approximately10% of the total number of retinal ganglioncells and have less redundancy than the Pcell. When a low spatial-frequency sinusoidalgrating undergoes high temporal-frequencycounter phase flicker, the grating appears tohave twice as many light/dark bars and itsspatial frequency appears to be doubled. Thisphenomenon is known as the frequencydoubling illusion. The illusion is believed toreflect the function of a subset of M cells 3.Recent studies of glaucomatous pathologyhave demonstrated that the retinal ganglioncells with larger cell bodies are selectivelydamaged earlier in the disease process ofglaucoma4. Frequency doubling perimetry(FDP) operates based on the frequencydoubling illusion. A prototype device (WelchAllyn, USA) is available for the FDPmeasurements. The FDP device randomlypresents a sinusoidal grating in 1 of the 17test areas located within the central 20degrees radius of the visual field. Thesinusoidal grating has a spatial frequency of0.25 cycles per degree and undergoes a 25 -Hz counter phase flicker. An advantage offrequency doubling technology perimetry is itsshorter time, primarily the results are lessaffected by blur, pupil size differences and ithas lower test-retest variability than white onwhite perimetry and SWAP.
4. High -Pass Resolution perimetry:
Midget ganglion cells which project to theparvocellular layers of the lateral geniculatenucleus are the most numerous, comprising70 % of the total of ganglion cells. These cellshandle acuity and resolution tasks and preferstimuli with low temporal frequencies andhigh spatial frequencies, along with color.High-Pass Resolution perimetry resolutiontask developed by Lars Frisen, using the
Ophthimus High-Pass Resolution perimeter(High Tech Vision, Malmo, Sweden) is a testthat is designed to measure the response ofparvocellular mechanisms2. The test presentsspatially filtered rings across 50 test locationsin a 30-degree visual field. Fourteen differentring step sizes are used, with thresholddesignated as the smallest ring size that canbe resolved by the patient. This method iscomparable with standard fields for detectingvision loss and is superior for identifyingchange over time 5. It is user-friendly test,takes approximately 5 minutes and givesfeedback for correct responses. Hereby we cansee a sample High -Pass resolution perimetryreport depicting field defect (Fig).
6. Flicker perimetry:The ability to detect a rapidly flickering
stimulus is believed to be mediated bymagnocellular mechanisms. It is consideredto be a strategy to detect early glaucomatousdamage. Studies by a number of investigatorshave shown that flicker is able to detect earlydamage that is not demonstrated byconventional automated perimetry 2. Flickerperimetry has been implemented in acommercial perimeter, the Medmont M600(Medmont Pty Ltd., Camberwell, Victoria,Australia). The flicker stimulus has a fixedcontrast level, whereas its luminance is variedto obtain threshold. The major advantage isthat flicker perimetry is more resistant tooptical degradation (Blur, Cataract, etc) thanconventional perimetry 6.
7. Motion perimetry:
The ability of detecting motion has beena visual function of interest for detection ofglaucoma because of the reports that M-cellsand large-diameter fibers may be preferentiallydamaged early in glaucoma. Evidence frommany investigators indicates that thisprocedure is effective in detectingglaucomatous visual loss and that thesedeficits precede those found with conventionalperimetry 7. There are several methods ofperforming motion perimetry. The procedureemployed by Fitzke, Johnson and othersinvolves detection of the direction of motion
(contd. on page 24)

22
of a single dot or line stimulus. This proceduredetermines the minimum displacement of thestimulus necessary to detect movement.Motion perimetry has several advantages.First, motion is a very salient stimulus forperipheral vision, thereby making this a testthat is relatively easy for patients to perform.Second, like flicker perimetry, motionperimetry is highly resistant to opticaldegradation produced by blur or scatteredlight from cataract or corneal opacities. Third,large changes in pupil size do not appear tohave much effect on motion perimetrythresholds. Finally, motion perimetry is lessaffected by background luminance andcontrast than other visual functions7. Howeverat present time commercial version of thismethod is not available.
8. Multifocal visual evoked potential:
Multifocal visual evoked potential is anobjective measurement of the visual field.
There are two Multifocal techniques that arepresently being used, the Multifocalelectroretinogram, which measures the localelectrical responses of the retina throughoutthe central visual field and the Multifocalvisual evoked potential, which measures thelocalized electrical responses from the primaryvisual portion of the brain for the centralvisual field. The usefulness of the multifocalelectroretinogram is yet to be studied. Recentinvestigations of the Multifocal visual evokedpotential have indicated that it can providean objective determination of glaucomatousvisual field loss that shows very goodcorrespondence with standard automatedperimetry. Multifocal perimetry seems to be apromising new technique for objectivelyassessing the central visual field and willprobably be most useful for patients who aredifficult to test with conventional perimetricprocedures.
Figure: High-Pass resolution perimetry report showing inferior arcuate defect
23
At the present time, these new techniquesare able to supplement conventionalautomated perimetry by providing someadditional capabilities. In future, as thesetechniques are refined, they may possiblybecome the standard for visual field testing.
References:
1. Bengtsson B,Olsson J,Heijl A. Evaluationof new threshold visual field strategy,SITA,in normal subjects ActaOphthalmol.1998;76:165-169.
2. Pamela AS,Chris AJ. FunctionalAssessment of Glaucoma.J Glaucoma.2001;10:49-52.
3. Maddess T,Hemmi JM,James AC.Evidencefor spatial aliasing effects in the Y-like cellsof the magnocellular visual pathway. VisRes 1998; 38:1843-59.
4. Johnson C,Cioffi G,Van BuskirkE.Frequency doubling technology perimetryusing a 24-2 stimulus presentationpattern.Optom Vis Sci 1999;76:571-81.
5. Chauhan B,House PH,McCormick TA,etal.Comparision of conventional and high -pass resolution perimetry in a prospectivestudy of patients with glaucoma andhealthy eyes.Arch Ophthalmol1999;117:24-33.
6. Zhang L,Drance SM,Douglas GR.The abilityof Medmont M600 automated perimetry todetect threats to fixation.J Glaucoma1997;6:259-62.
7. Murray F,Thomas LL.Primary Care of theGlaucomas.2nd ed.St.Louis:McGraw-Hill;2001.
8. Chris AJ. Recent developments inautomated perimetry in glaucoma diagnosisand management.Ophthalmol 2002;13:77-84.
Editors : Dr Mahesh P Shanmugam & Dr Arun Narayanaswamy For Private Circulation Only
(contd. on page 21)
Last Page
Perimetry UpdateR Krishna Kumar
Perimetry is useful clinical tool for thedetection of ocular and neurological pathology,differential diagnosis of eye disease and follow-up of the disease. The introduction ofautomated static perimetry, which occurredsome 15 years ago, has changed the way ofthe management of ocular disease, especiallyglaucoma. The present perimetricmethodology, however, has some drawbacks:like long examination time and inefficiency indetecting early glaucomatous changes. In thisarticle, we discuss few of the developmentsthat address these issues.
1. White-on White automated perimetry:
To reduce the test time, the recentHumphrey field analyzer (HFA-II), has 2 newthreshold strategies: SITA standard (Swedishinteractive thresholding algorithm) and SITAfast. The SITA standard strategy matches theprecision of the full threshold strategy whilereducing test time by half 1. Both SITA andSITA fast use four methods for reducing time:reducing time between presentations, startingthe examination of each location with a betterestimate of the expected threshold, reducingthe testing performed at each test point, andreducing the time spent in catch trials. Inaddition to blind spot monitoring in HFA-I,HFA-II has gaze-tracking capability that willmonitor fixation continuously during theexamination.
Tendency Oriented Perimetry (TOP) is anefficient test strategy that has been developedfor the Octopus 101 and 300 Series perimeters(InterZeag Ac, Schlieren, Switzerland). It uses
This issue of Insight is sponsored by:
Rampion Eyetech Pvt. Ltd., Kalash, New Sharda Mandir Road, Paldi, Ahmedabad - 380 007Apex Laboratories Pvt. Ltd ., 44, Gandhi Mandapam Road, Kotturpuram, Chennai - 600 085Pharmacia & Upjohn India Pvt. Ltd., SCO 27, Sector 14, Gurgaon 122 001, Haryana
Medical & Vision Research Foundations thank the above sponsors for their generosity.
a staircase procedure, but does so bysequentially evaluating neighboring locationsso that each location is tested only once. Thevisual field is divided into squares of fourneighboring test locations and the firstlocation in each square is tested with theinitial stimulus intensity .The stimulusintensity for the second presentation isadjusted according to whether or not thepatient responded to the first stimulus. Thesecond location in the square is tested withthe new stimulus intensity, a similarprocedure is employed for the third and fourthmembers of the square and a thresholdestimate is thus obtained after 4 stimuluspresentations. TOP is four time faster thanconventional staircase threshold procedures.
2. Blue-on-yellow (B/Y) perimetry or shortwavelength automated perimetry (SWAP)
Blue-on-yellow perimetry or shortwavelength automated perimetry is used todetect glaucomatous visual field changesmuch earlier than the conventional white-on-white perimetry does. The blue-on-yellowperimetry is incorporated with the HumphreyField Analyzer. It uses blue stimuli (440 nmwavelength), narrow band, 1.8-degree targetof 200 milliseconds projected on a brightyellow background (530 nm-cutoff-filtered,315 apostilb) to test selectively the short -wavelength sensitive pathway. The smallbistratified ganglion cells mediate the patientresponse to this test. These cells are few,comprising 6% to 10 % of retinal ganglioncells. The major drawback to this testingmethod is the test time of 15 minutes. It isalso influenced by significant cataract 2.
3. Frequency Doubling Perimetry
Visual information derived from theretinal ganglion cells project to the lateral












![Leitthema - Springer · (2002) [58]x x x x x x x x Brune (2002) [23]x xx xx x xx Burmester (2014) [24]x x x Butollo (2012) [25]x xx x xx xx Casal (2005) [26]xx x xx x Claassen (2005)](https://img.pdfslide.us/doc/110x75/605f28310469a1434626bf30/leitthema-springer-2002-58x-x-x-x-x-x-x-x-brune-2002-23x-xx-xx-x-xx-burmester.jpg)