Embed Size (px)
Citation preview

Vocational Rehabilitation
and Social Reintegration
of the
Leprosy Affected in India
Navin Chawla

Vocational Rehabilitation and
Social Reintegration of the
Leprosy Affected in India
Navin Chawla I.A.S.

Preface
During the course of meetings and field visits undertaken for
this study, I was frequently asked by leprologists and social
workers alike how it was that an administrator should have
become interested in so remote a subject. In actual fact my
interest in leprosy arose in 1975. During the course of getting
acquainted with Mother Teresa and her world of destitutes, I
chanced upon the situation of leprosy patients and their families
living in Seemapuri in East Delhi. The opportunity, however, to
make a study of different facets of their situation - the etiology,
the social problems, control measures and rehabil i tat ion
measures - presented itself two years ago, when the Government
of India generously accepted my proposal to devote a period of
time to examine these factors in some detail, and present a
Report. It goes without saying that the conclusions arrived at are
entirely my own.
This paper is intended to share with policy makers several
policy options from the perspective of an administrator. The
leprosy affected are a community stigmatised by tradition.
However, it is not difficult to reverse this trend. I believe that it is;'
necessary for rehabilitation policy to be shaped to complement
the control measure that are al ready being implemented
particularly in the leprosy endemic districts in the country. The
stress is on evolving low-cost community-based methodologies.
With better coordination, the existing infrastructure can be
suitably modified, and hard pressed resources can be applied to
programme content instead of to the creation of administrative
apparatus.
I have used the words "leprosy affected" in most parts of this
Report for several reasons. The use of the word "leper" has
acquired a pejorative meaning and I have eschewed the word
except in some specific references as for example to the Indian
Lepers Act of 1898, the repeal of which I have affirmed. Some
papers and books have relied on the term "leprosy patient" but
with such usage a distinction needs to be drawn between
"patients" and "ex-patients". Persons with deformities are often

taken to be "patients", when in fact they may be non-infectious
and not undergoing treatment at all. Certain books rely on the
word "leprosy afflicted" which, while perfectly acceptable does
sugges t a l i f e - long problem which does not t ake in to
consideration recent medical advances. With the controlled use
of drugs such as Rifampicin, non -infectivity is rendered
sometimes in a matter of a week or two. Nor does this term take
into consideration the plight of family members, who while they
may not themselves suffer from the disease, share its socio-
economic consequences. I have in mind particularly the healthy
children of leprosy patients, especially the residents of Madipur,
who made my access to Seemapuri more meaningful. For all
these reasons, I have preferred to use the words "leprosy affected", as
a summation of a particular socio-economic as well as clinical
condition.
Navin Chawla, I.A.S
4. Jaipur Estate,
Nizamuddin East,
New Delhi-110013.

ACKNOWLEDGEMENTS
The Government of India is unique in permitting its civil servants time off to pursue their academic interests through formal or non-informal prescriptions. This opportunity was presented to me when I returned from an assignment with the International Labour Organisation in Thailand. The nine months of study leave that I availed of enabled me to obtain an Insight into the situation of the leprosy affected. For this unique opportuni ty. I am gra tefu l . I am gra tefu l a l so to the International Labour Organisation, and in particular to its Director-General Mr. Francis Blanchard who supported the project from its inception. I am also appreciative that the International Development Research Centre, New Delhi, provided inputs for research, and made the printing of this text possible.
Returning to a semi-academic structure after a space of many years. I turned to Professor K.D.Gangrade, Head of the Social Work Department, in the Delhi School of Social Work, and Pro- Vice Chancellor of Delhi University, for guidance and assistance. During the course of the last two years he has acted as my Supervisor, and I am indebted to him for his time and patience.
For a student wishing to read further about the rehabili tation aspects of this subject, I soon found that there is no cohesive library. However, thanks to the generosity of a number of leprologists and social scientists, I was assisted with material. Including their own papers.
A special word of thanks is due to Prof. RK. Mutatkar of Pune University and Dr. M. S. Nilakanta Rao, President, National Leprosy Organisation who shared their deep knowledge of the subject whenever I sought them out. Together with Dr. Clive Wing, they also looked over the drafts in its various stages and offered souna advice. My gratitude is also due to Dr. Kunal Saha and Dr. K.N. Rao of the Patel Chest Institute of Delhi University who together with Dr. N.N. Chawla of 'Coordination' Delhi so generously helped with the sample survey. My gratitude is also due to the following who so unhesitatingly provided me

access to research papers, seminar, conferences, projects and
their own rich experiences:
1. Mr. Anees Ahmad, Assistant Director General, ILO, Geneva. 2. Mr. A.G. Chaphekar, Udyog Dham, Talegaon, Maharashtra. 3. Dr. N.S. Dharmashaktu, Dy. Asstt. Director General
(Leprosy), Government of India. 4. Ms. Pushpika Freitas, Rehabilitation Consultant
(North India), German Leprosy Relief Association. 5. Dr. Ernest Fritschi. Director, (Retd.), Schieffelin Leprosy
Research and Training Centre, Karigiri, Tamilnadu. 6. Dr. R. Ganapati. Director, Bombay Leprosy Project. 7. Dr. S.D. Gokhale, Chairman, Gandhi Memorial Leprosy
Foundation, Wardha. 8. Shri Purshottam Goyal, Chairman, Metropolitan Council,
Delhi. 9. Mr. Sunil Guha, Director. ILO Office, New Delhi. 10. Mr. Lakshmi Jain, Industrial Development Services,
New Delhi. 11. Dr. E. Max, Department of Economics, Pondicherry
University. 12. Dr. J.M. Mehta, Hony. President, Pune District Leprosy
Committee. 13. Dr. P.N. Neelan, Director, CLTRI, Chengalpattu, Tamil Nadu. 14. Dr. S.K. Noordeen, Chief Medical Officer (Leprosy), WHO,
Geneva. 15. Prof. T.K. Oomen, Centre for the Study of Social Systems,
Jawahar Lal University, Delhi. 16. Shri Vijay Pande, Director, IDRC, New Delhi. 17. Dr. C.K. Rao, Deputy Director General (Leprosy), Government
of India (Retd.) 18. Dr. M.S. Nilakanta Rao. Specialist in Leprosy - WHO
Consultant. 19. Dr. Patricia L Rosenfield, Special Programme for Research
and Training in Tropical Diseases, WHO, Geneva. 20. Sh. C. Anthony Samy, Director, Worth Trust, Katpadi,
Vellore. 21. Mr. Shankar Narayan, Director, (Retd.) ILO Office, New Delhi. 22. Dr. Lila Soni. 23. Sh. S.P. Tare, Organising Secretary, National Leprosy
Organisation, Wardha. 24. Dr. R.H. Thangaraj, Director of Southern Asia, The Leprosy
Mission (Retd.). 25. Dr. M.V. Yellapurkar, Joint Director of Health Services,
(Maharashtra).

TABLE OF CONTENTS
Page No.
A. Recommendations 1
B. The State of the Art 10
1. Introduction 10
2. History 12 3. Leprosy as a disease 13 4. What leprosy is not 13 5. What leprosy is 14 6. Leprosy control 15 7. Community participation 17 8. Treatment 18 9. Rehabilitation as a factory in leprosy control 21
C. Stigma in Leprosy 23 D. The Global Situation 28 E. The Indian Scenario 41 F. Leprosy and the Law 69
G. The Rehabilitation Factor 75
1. Rehabilitation Policy -- the raison d'etre 75 2. The parameters of the situation 77 3. The prevention of "dehabilitation" 79
(i) Survey, Education and Treatment 81 (ii) Education 82 (iii) Education by demonstration 84 (iv) The attitude of medical community 85 (v) Reconstructive surgery 89
4. The role of institutions in rehabilitation 90
5. The role of the voluntary sector in rehabilitation 92 6. Rehabilitation measure in "free" or self-settled colonies 97

Page No.
7. The role of mass communication 98
8. An assessment of the proposed
rehabilitation strategy 99
H. Training and Placement Services 104
I. Vocational Training and Employment as the
principal means of Rehabilitation 117

A . R e c o m m e n d a t i o n s
These recommendations are specific to or have an important
bearing on rehabilitation aspects.
Employment Policy in the Government Sector
Employment
The 3% reservation for categories C & D of the handicapped
for employment in the Government sector (including the Public
Sector) is not being adequately enforced. The leprosy affected are
not getting their due share of the Reservation Policy on account of
leprosy; some of the leprosy disabled are considered eligible on
account of other effects of leprosy such as blindness or
orthopaedic disability.
1. Leprosy should be treated as a separate category of the
handicapped, and should not be placed under its side effects.
2. All leprosy patients with established signs of nerve
damage or its consequences as specified in the WHO Disability
Grading (Grade I, Grade II and Grade III) should fall under this
category.
3. Those that are having (a) partial or complete blindness
(b) other handicaps apart from the consequences of nerve
damage, e.g. shortening of fingers due to the concentric atrophy of
bones, bone disintegration as sometimes occurs in the ankles etc.
should also come under the category of the handicapped and be
provided suitable jobs.
4. Wherever possible, and in MDT districts in particular,
the leprosy affected especially carrying disability, should be
given certain responsibilities which include the manning of
railway crossings, guard duties, duties of night watchmen and
gardening functions. Certain agricultural jobs e.g. poultry farm-.
ing and animal husbandry may also be considered.
1

Medical Leave
5. For those already employed, the advent of leprosy
should not be considered to be a ground for their suspension,
termination, discharge or dismissal. Medical leave on full pay
should be granted until such time as the clinic/hospital/medical
expert certifies that the patient can rejoin his work without
causing a public health problem. Certification should be made
uniform for the Union Government and State Governments. No
person should be allowed to lose employment on grounds of
leprosy, whether ox not handicapped, whether or not infectious.
This should apply to civilian and military posts alike.
6. Where complications develop, the patient should be
allowed additional leave on full pay upon production of a medical
certificate from clinic/hospital/medical expert for the course of
his treatment.
7. For the leprosy affected seeking employment, while
physical disability may prohibit candidates from performing
certain jobs, physical deformity should not be a ground for non-
consideration.
8. The Special Employment Exchanges should make
efforts to enlarge the number of negative leprosy patients for
registration and placement.
9. Despite Grade II or Grade III disability, the leprosy
affected can perform usefully in a number of occupations i.e. as
railway gangrnen, railway and other gate keepers, and as
gardeners. For these occupations, very rudimentary training is
needed and such placements would go far in the successful
Implementation of a rehabilitation policy.
Incentives for Employment in the Private Sector.
10. Where private enterprise has been enlightened enough to
appoint handicapped persons, they have met with good results.
2

However, it is essential for Government to devise a distinct package of incentives and tax concessions for the private sector.
(a) Government should provide 100 percent tax exemption to employers for the salary they pay to a leprosy employee.
(b) Government should provide 100 percent tax exemption in the event of donations made to enhance the cause of leprosy.
The Role of Employers ' and Trade Union Organisations.
11. The Directorate General of Employment and Training
in the Union Ministry of Labour should convene an annual
tripartite conference to discuss employment policy for the
handicapped, in which the problems faced by the leprosy affebted
should be afforded a distinct identity. The tripartite machinery Is already well developed by the Ministry of Labour.
12. The terms of reference may include devising of trairiing
programmes, drawing up of an employment schedule and
discussing related on-the-job problems for the handicapped
including the leprosy affected. Principal Employers Organisa-
tions and Trade Union Organisations should share in a joint
effort towards an employment strategy for the handicapped.
13. This should act as the nodal Ministry and invite participation at sufficiently senior levels from all concerned Ministries/Departments including the Minist ries/ Departments of Law, Health, Social Welfare Information and Broadcasting and Industry among others. It is only then that a coordinated strategy can be fashioned and difficulties felt by the Employers and Trade Union Organisations be discussed with a view to remedial action.
3

Assistance by Financial Institutions
14. A Finance Corporation should be established to assist all
categories of handicapped persons to obtain financial assistance
towards self-employment schemes.
15. It is difficult for the leprosy affected to obtain bank loans.
They face difficulty in obtaining guarantors. both because of
their depressed economic status as well as societal attitudes. A
recommendation from any recognised voluntary agency working
in the field of leprosy should suffice as bank guarantee. The DRI
scheme or any other scheme for the weaker sections should be
specifically extended to cover the leprosy affected seeking self-
employment.
The Role of Mass Media
16. Stigma affects al l aspects of leprosy control and
rehabilitation. It also sets the leprosy affected apart from other
categories of the handicapped. A significant part of the leprosy
eradication programme lies in the need to educate the population
about the basic facts about the disease, in order that myths and
superstitions be removed. A campaign to remould public
attention needs to be initiated. It needs to be sustained at several
levels. (In the MDT districts in particular, detailed information
needs to be disseminated regarding aspects relating to the
availability of services).
17. Administratively, the Ministries of Information and
Broadcasting, Health, Social Welfare. Labour & Employment and
Industry need to formulate a joint strategy at the apex level.
Strategies need to be devised for State and District levels.
especially in MDT districts.
18. A media mix would need to be devised by experts.
Communication methods and range of coverage have made
s igni f icant advances in the las t few years . Televis ion
transmission now covers practically the whole country.
Acceptability ratios vary. Cinema, radio and the press may have
higher acceptability levels in some areas. Exhibitions and
4

festivals also have a role to play in other areas and during certain
times of the year.
19. It is necessary to associate representatives of the
voluntary agencies in the field of rehabilitation, as well as some
eminent leprologists and social scientists with the development
of a communication strategy at different levels.
Legislation
20. The Indian Lepers Act 1898 has been repealed by the
Central Government and is no longer applicable to centrally
administered areas. However, it has been repealed by only eight
S t a t e Governmen ts . I t s r epea l b y the remain ing S ta t e
Governments should be vigorously urged by the Central
Government, and effected within a time-bound frame.
21. The Law Commission should undertake a compre-
hensive study of Central and State Legislation affecting the
conditions of work and other rights of the leprosy affected.
Wherever discriminatory and outdated enactments exist, these
should be repealed or amended in keeping pace with medical
advancement and the scientific temper of the day. The Law
Commission may also suggest specific legal measures whereby the
working situation of the leprosy affected within the organised
sector can be improved.
22. It would be desirable to provide free legal aid to those
leprosy patients who apply for their legitimate constitutional
rights.
Education and Syllabi
23. Correct factual information about leprosy needs to be
imparted from the primary level uato the undergraduate level.
This may be transmitted both through science lessons as well as
lessons in the humanities. The National Council for Education
5

Research and Training (NCERT) should be associated with
developing an appropriate strategy.
24. The general apathy of the medical profession continues
to remain an impediment on the control side. Government and
private practitioners alike lack clinical confidence in diagnosis
and treatment. The Swaminathan Committee had observed that
"unless medical students are made to learn leprosy as a part of
their curriculum, by including compulsory questions on leprosy
in their examination, inadequate interest in leprosy work among
doctors in service, and general medical practitioners, will
continue". There has not been sufficient improvement in this
direction.
Travel Concessions
25. The leprosy affected who have bilateral Grade II
disability or unilateral Grade III disabilit y should be made
eligible for travel concession similar to those provided to the
orthopaedically or the visually handicapped.
26. The Railways do provide travel concessions to several
categories of the handicapped. These should be enlarged to
include free travel to leprosy patients who need to travel to obtain
treatment. This is especially important for patients undergoing
MDT treatment in districts where MDT has been introduced.
Old Age Pension
27. Leprosy patients with bilateral Grade II disability or
unilateral Grade III disability should be made eligible for old age
pensions, if they are destitute and above the age of 60. Old age
pensions are being provided by the Central Government and some
State Government for certain categories only, but these should be
extended to the leprosy affected categories above.
6

Training Schemes
28. The DGET under the Union Ministry of Labour has
es t ab l i sh e d
Voca t io na l Rehab i l i t a t i on Cen t res fo r t he
Handicapped. The total number of negative leprosy patients
admitted, evaluated and rehabilitated is small, both in absolute
terms and in terms of other categories of the handicapped. This
situation urgently needs to be remedied.
29. Emphasis must shift from sheltered institutions to low-
cost community-based self-employment schemes and domici-
liary rehabilitation schemes. Rural Vocational Rehabilitation
Centres for the Handicapped under the Ministry of Labour as well as
voluntary effort should provide training in self-employment schemes.
30. This should be initiated in all Multi Drug Therapy
(MDT) districts. These programmes should be organised by the
Ministry of Social Welfare in close coordination with the
Ministries of Health, Industry, Information & Broadcasting and
Labour (DGE&T). The programme should minimise expenditure
on infrastructural and administrative costs so that at least 60
percent of funding is made available for programme content. The
programmes must aim to be community-based and low-cost.
Wherever possible it would be of advantage to base them near the
centres where MDT health programmes are being administered.
31. Training modules, especially non-formal training
modules and skill development training programmes, are al -
ready being implemented by the VRCH administered and run by
the D.G.E &T. in the Ministry of Labour. Closer coordination
should be developed between the Ministry of Health's control
programme. DGET'S training programmes and the Ministry of
Social Welfare's rehabilitation programmes, so that a common
strategy be adopted and duplication avoided to the extent
possible. Emphasis whenever possible. should be laid on rural
schemes. The propagation of new methods and techniques in
agriculture and animal husbandry will help enlist greater
7

participation. It should be combined with training in small scale diversified agriculture, the use of appropriate technology and of natural energy (solar, wind power and simple treddle machines.)
32. The 11 Rural Rehabilitation Extension Centres so far
established at Block level, under five selected VRCH, should make
special efforts to include the leprosy affected cases as a special
category of the handicapped. Many of them require prosthetic
and other appliances.
33. Training should not necessarily be geared for the cities.
The high social cost of living in the cities presents it own
difficulties. Agriculture-based training programmes involving
new techniques in the production of food, fruit, vegetables, milk
and poultry as well as small scale diversified agriculture and uses
of appropriate technology would be helpful.
34. The Khadi and Village Industries Commission have
specialised rural-based schemes to encourage self-employment.
These schemes should be devised to suit the particular problems
of the leprosy affected.
35. In the case of cities where there are already large
'free' colonies, usually located near leprosy institutions and
hospitals, existing self-employment schemes, albeit in the voluntary
sector should be strengthened. In many cities their full potential
is not being explored. Mini-VRCH shquld be started near the
biggest urban leprosy centres especially in Bombay,
Calcutta and Madras.
36. In urban areas, a few mini VRCH should be opened near
the principal leprosy settlements with a view to enable the
leprosy affected to avail of evaluation, training and placement
services. The healthy children of the leprosy affected should also
be allowed to avail of such training programmes.
8

37. The 3% reservation for all categories of the handicapped in
the Industrial Training Institute should be strictly enforced. The
leprosy affected are not getting their due share of the
reservation policy on account of leprosy. Non-infectious leprosy
cases should be encouraged to join the training schemes.
38. Training instruments for negative leprosy cases bearing
deformity or suffering anaesthetic limbs should be devised to
ensure that they are within their thresholds of tolerance.
39. A policy needs to be devised for the healthy children of
leprosy patients. They encounter stigma if their parentage or
local address becomes known especial ly at the t ime of
prospective employment or interviews. The 3% reservation in
ITI's and other training institutions should permit any surplus
seats left over (after the needs of the physically handicapped have
been met), to this category of the socially handicapped.
40. Training institutions run both by Government and the
voluntary sector, should not be allowed to covert themselves into
sheltered workshops for a permanent few thereby blocking the
training chances of other aspirants and losing their own raison
d'etre. They should run on business-like lines and, as far as
possible, grow into self-supporting units.
41. Sheltered workshops employing the leprosy affected
should be treated on a different footing from other workshops
falling under the Industrial Disputes Act.
9

B. The State of the Art
1. Introduction:
The rehabilitation of the leprosy-affected can be looked on
both as a formidable problem as well as a formidable challenge.
As a problem its dimensions may seem Insurmountable.
Society with its deep-rooted ignorance and prejudice has
traditionally tended to view leprosy not merely as a disease but as a
sub-human condition. Myths have abounded. Some have
viewed the condition as a manifestation of previous sinful life,
others have believed it to be hereditary and without a cure.
There have been a host of difficulties on the control side as well.
not the least of which has been that the disease has not always
been diagnosed irutime,91-1 properly, nor has it always been
adequately treated. Avoidable deformities, have continued to
occur, fostering prejudice, attracting ostracism and continuing to
cause "dehabilitation". Despite significant advances on the
medical side, traditional prejudices have continued to retain
their grip on common perceptions. The net result is that in some
countries the problem in absolute terms has been increasing
Instead of decreasing.
It is, however, as a challenge that we need to view, the
rehabilitation of the leprosy affected. Several new insights about The
curability of the disease have opened fresh dimensions on how
both the disease and those affected by it should be treated cared for.
In recent years this has led to renewed efforts to cure the
affected, as well as rehabilitate those cured with respect to the
patients' sense of dignity. This attitude alone can temper despair
with hope, and bring about a comprehensive package to eliminate
the manifestations of the disease - physical, psychological and
social - within the foreseeable future
The word "dehabilitation” is etymologically incorrect . Its usage is unique to the leprosy situation and signifies the casting away from society.
10
•

Rehabi l i tat ion means a return to a s tate of complete
normalcy. This definition encompasses the need for social and
psychological assimilation as a necessary complement to
economic independence. There are therefore twin aspects to be
met - the establishment or re-establishment of economic
productivity, and equally important re-assimilation in society.
If only the former is met, the affected is vocationally settled but
not rehabilitated. The WHO has defined leprosy rehabilitation
most succinctly : "By rehabilitation is meant the physical and
mental restoration as far as possible, of all treated leprosy
patients to normal activity, so that they may be able to resume
their place in the home, society and industry. To achieve this,
treatment of the physical disability is obviously necessary but it
must be accompanied by education of the patient, his family and
the public, so that not only can he take his normal place, but
society will also be willing to accept him and assist in his
complete rehabilitation".
The problems of rehabilitation for the leprosy affected go
beyond those of other handicapped categories, chiefly because
such categories as the visually handicapped, orthopaedically
handicapped, the deaf and dumb and other handicapped groups
are neither stigmatised nor uprooted.. They may be considered
'different' from the able-bodied, but they do largely remain
w i t h i n t h e i r ow n en v i r onm ent . Th e l ep r os y a f f ec t ed ,
particularly after the development of deformity, are often
physically uprooted, with consequent psychological impairment.
Damage to hands and feet often enough requires the acquisition
of new skills. Rehabilitation in such cases goes beyond the
traditional ambits and takes on a deeper shade of meaning.
Leprosy rehabilitation as an instrument of policy, i s a
co mp a r a t i v e l y n ew co n cep t , and mu s t n eces sa r i l y b e
multi-dimensional in its framework. A distinction also needs to
be made between rehabilitation effort and rehabilitation policy.
Voluntary effort has indeed been pioneering and has created a
number of pools of excellence. Some extremely interesting and
rewarding experiments are also being carried out. By definition
11

however this can neither be enough or complete. It has now become necessary for Government to play its role in coordinating the manifold spheres involved-medical, social, economic and legislative. These have to be judiciously combined and shaped into an instrument of policy.
This need has become all the more pronounced because Government Is clearly against the "free" colony approach, a consequence of which is the stigmatizing process by society. Society at large does not favour the proliferation of beggars, although it does not realize that in the case of lepros
y it is sometimes the last
psychological barrier of shame that an affected person must cross when he is left with little or no option for survival. Whatever its causes, the phenomena cannot be wished away. The problems of the leprosy beggars need to be comprehensively examined and the parameters of the situation defined. However, it needs to be stated that while the dimensions of the situation are not overwhelmingly large, stigma renders this a difficult area of rehabilitation.
2. History:
Leprosy is a disease which has been with us for many centuries. The oldest Hindu scriptures and the Bible make references to it. Ayurvedic texts of the 6th Century BC had noted the symptoms of leprosy, and Manusmriti took cognizance of leprosy while discussing the regulation of marriage. It is all the more ironic that a disease with its centuries-long association with humankind should be so little understood —indeed misunderstood - in all its aspects including its etiology, causation, means of transmission and its curability. The principal reason for fear is that it is a disabling and disfiguring disease, which had no cure until comparatively recently.
The deformities that change the identity of a patient is the principal cause of social stigma. In every society there prevails an aesthetic concept of physical beauty. Health is indeed an Important aspect of culture, and attempts to change belief and
12

behavior regarding health and disease, therefore seek to change the cultural traditions of people. It is the deformities of the leprosy-affected that have traditionally caused repugnance, and in the absence of any understanding about cause and cure, the leprosy affected were viewed, in a number of societies, as objects of divine punishment and leprosy as a visitation of past sins.* Contagion was the great dread and as traditional medicine offered no cure for leprosy, society's attitude remained, over the centuries, one of outcasting of the leprosy-affected. The disease continues to this day to be the most dreaded of all (with the possible and recent exception of AIDS). In many spheres of life the process of outcasting continues to take place. although on an increasingly diminishing scale as awareness grows that new and powerful drugs can render complete non-infectivity sometimes in as little as one week.
3. Leprosy as a disease:
While leprosy is a disease like any other and requires to be shorn of the body of myth that surrounds it, it must be said that medical opinion does not yet provide unequivocal answers as to its cause or its etiology. Although the bacillus has been known since 1873 when it was identified by Dr. Hansen, its agent has yet to be effectively cultured, and answers are still awaited as to exact mode of transmission. Nor has medical research led to any conclusive vaccine, although field tests are now being carried out In India and elsewhere.
4. What Leprosy is not :
Myths and distortions, however, need to be corrected by comprehensive and sustained effort. There are a number of things that leprosy is not. It is not hereditary, it has nothing to do with impure blood, it is not a poverty-related disease, it does not call for isolation, nor are all leprosy patients infectious. Infection is probably not spread by food and water; indeed it is
R K. Mutatkar " Society and Leprosy".
13

a highly infectious disease. It is neither a difficult disease to diagnose nor is treatment per se difficult, although regularity of treatment is necessary. It does not require to be treated in specialised institutions. All persons are not susceptible to the disease, although insanitary conditions, malnutrition and lack of personal hygiene may "invite" the leprosy bacillus as such conditions might do for a host of other diseases and infections. It is not a fatal disease, but there must be few other diseases that cause its victims as much psychological and social damage.
5. What leprosy is :
Leprosy is a chronic bacterial infection affecting mainly the nerves, skin and mucosa. It is known largely to be a human disease, in that the human body is the principal reservoir of the causative germ the Mycrobacterium leprae. We do not yet have all the answers on the transmission of the disease, but it is known that transmission occurs through close contact between a person who suffers the infectious form of the disease, and who transmits the lepra bacilli through nasal discharge, or skin ulceration to healthy persons. Where the disease is not treated early, adequately or comprehensively, it can lead to primary or secondary deformities. An important factor in its early neglect is the absence of pain, itching and so on.
Manifestations of the disease appear to vary according to geographical variations and host responses. Leprosy does not give any forewarning, but early clinical signs may take the form of oily, shining skin surfaces or one or more faintly discoloured patches on the skin, which become anaesthetic and lose sensation. This removes the protective panoply of discomfort or of pain. It can have an incubation period ranging from 3-5 years or longer. Neglect over a prolonged period may lead to deformity and secondary pyogenic infection causing destruction mainly to hands and feet, loss of eyebrows and depressed noses. Injuries caused to anaesthetic parts invite ulceration; because it is frequently painless, neglect leads to sepsis.
14

There are two main varieties of the disease -lepromatous and non-lepromatous. It is the lepromatous group, which comprises about 15-20% of the leprosy-affected, which causes the spread of infection when left untreated or inadequately treated, Upto 80-85% of all cases are only feebly infectious, and do not generally transmit infection to others. In India the vast majority of the affected, who may often develop deformity, are in fact non-infectious. The majority of leprosy-affected beggars fall within this category. Quite a number of beggars are usually burnt-out cases. The vast majority of the population has sufficient defence mechanisms 2nd does rot develop the disease. To further amplify the point, in a hyper-endemic district of 30/1000. 97% of the population do not contract the disease. Of the 30, 80% i.e. 22.5 patients contract the non-infectious type of leprosy. Therefore, of a population of 1000, 970 do not get the disease and 22.5 contract its non-infectious form. Only 7.5 persons contract the infectious form. The incidence in such an area will be 3 per 1000 i.e. 3 new cases would crop up each year. The chances therefore, of getting the disease would be 3 per 1000, or 0.3%
.. This
would be the pattern in an area where no treatment is given. If, however, all the patients; in the area are systematically treated, the incidence would be further reduced. Should general health and socio-economic conditions improve, the incidence rate could be expected to fall further, consequently reducing the chances of getting the disease.*
Leprosy control :
Prior to the introduction of Dapsone, there was no known t reatment, and isolat ion of the pat ient into asylums. institutions or colonies were the only recourse that society felt it was open to. Isolation after the manifestation of the obvious signs of the disease did not prevent the infectious category of patients from spreading the disease during the early periods of infectivity.
D r . M . S . N i l a ka n t h a R a o — D i s c u s s i o n s
15

Despite the availability of new and powerful drugs. the
problems created by the fact that leprosy is a disease with a long
Incubation period, remain. It has been sometimes known to take a
few years before patients become aware of the manifestations of
the disease and start to take remedial action. Then, as now,
early detection is essential to the success of the control
programme, for on it is dependent timely treatment and cure, the
prevention of transmission of the disease in the family and
community, the prevention of the development of physical
deformity, and, finally, the prevention of "dehabilitation".
Following the introduction of Dapsone, control programmes
took the form of the SET model, comprising house-to-house
surveys for case detection, treatment in out-patient clinics, and
health education. With local variations, control programmes are
based on this model, with varying survey methods being
adopted, using medical and para-medical workers, health
educators and social workers, teachers, social volu nteers,
medical students and so on. There are several at tendant
problems, including the reluctance of people to cooperate with
household surveys, and hesitation to attend leprosy clinics, both
of which methods might single them out for attention and
ostracism. Medical practitioners often enough lack clinical
confidence in dealing with leprosy and instead of being able to
deal with cases in the comparative anonymity of their (often)
general practices, refer suspicious cases to specialised clinics,
which the patient might wish to avoid in the first place.
Whatever may be the nature of difficulties, it is imperative to
widen the scope and intensity of early detection methods. Well-
integrated mass education campaigns using an optimum media
mix are necessary to encourage voluntary reporting. It has been
frequently demonstrated that where such campaigns have been
Intensively launched, especially in control areas of leprosy
hospitals and clinics, an understanding of the disease and its
manifestations is greater, and patients come forward for
16

identification and treatment. It has been suggested earlier* and
needs to be reiterated, that an offer of cash incentives or
Incentives in kind would assist in this effort. Such incentives
would also off-set wage loss and travel expenditure.
Widespread educational campaigns need to precede more
organised population surveys. In some places, these may be
limited in scope. Voluntary agencies working in this field are
constantly involved in this effort. Many of them have well
defined control areas, and undertake surveys of specialised
groups as school children, factory workers. slum dwellers
etc. Such surveys are preceded by educational campaigns where
publ ici ty materials (hand -outs , posters , f i lms etc. ) are
distributed. The general experience of such campaigns is that
they are followed by a spurt of voluntary reporting. However, in
endemic districts particularly, there can be no substitute for
house-to house surveys of the entire population. This needs to be
done by leprosy or general health workers, properly t rained to
detect the earliest clinical manifestations. Such exercises also
need to be preceded by comprehensive educational campaigns, in
order to assuage abnormal fears, and to help bring the facts about
the nature of the disease out of the closet.
Community Participation :
This is where community participation also comes in. It is
vital to the success of an anti -leprosy programme that the
community at large accepts the disease like any other disease.
and its patient as any other chronic patient. The irony lies that
given deep-rooted traditional fears, such an attitude will have to
be taught. Health education is now being undertaken in India on a
much more systematic and sustained basis that in previous
years. However, changes in behaviour patterns do take time. The task
is uphill but it must be attempted. Programmes need to be
shaped in accordance with cultural variations, using local
languages, and a media mil: found most acceptable to local and
* Report of the Working Group on the Eradication of Leprosy- Ministry of Health and Family Welfare, Government of India. (1982)
17

regional populations. The use of religious sentiment can be an
important factor and should be taken into consideration. It is
also necessary to involve communi ty elements - youth
organisations, student organisations, organisations of teachers
as well as formal and informal community leaders. It has not
been sufficiently recognised that social scientists need to play
(what can amount to) a very significant role in community
understanding. For leprosy extends beyond being simply a
medical problem. It encompasses important social and cultural
issues, which are closely interwoven in the matrix of community
life.
It is not enough to encourage a few sociological studies. What
requires to be done is to encourage social scientists to integrate
their understanding with control mechanisms, and to tackle the
problem of leprosy as an integrated whole. Indeed, in its final
analysis, social scientists might convincingly argue that the very
word "leper" which has come to acquire a pejorative meaning,
should be discarded in favour of the term 'leprosy patient', and
indeed that the word "leprosy" itself be replaced by a less pointed
and more neuro-dermatological definition.
Treatment :
The scientific and technological advances in the fields of
leprosy treatment during the last three decades have resulted in a
major change in outlook towards the disease.
Treatment for several decades was dependent on a single drug-
Dapsone. In the last few years new and more powerful drugs such as
Rifamipicin, Clofazimine and others, which have powerful
bactericidal action against the leprosy bacillus are now available for
application in chemotherapy, as a measure of leprosy
control. These drugs, now often used in varying
combinations with Dapsone, are faster acting. This has helped
both to reduce the period of infectivity and has also dramatically•
brought down the length of treatment. Additionally, they have
provided a much needed answer to a major problem that was
18

developing with Dapsone chemotherapy, that of dapsone resistance in a percentage of cases. There is no doubt that these are now powerful weapons in the leprosy control programme.
The administration of the multi -drug treatment or regimen(MDT) is not without its difficulties. It is much more expensive than single drug therapy (Dapsone) and it also requires to be administered under close medical supervision throughout. This in turn has necessitated the need for adequate numbers of medical and para-medical personnel, as well as adequate training and retaining facilities. An important factor is the availability of the drugs in sufficient quantities, either by means of indigenous production or by import.
Wherever MDT has been launched a number of issues relating to regimen, supervision, regularity and continuity have to be worked out in advance. Regimens are worked out on the basis of age and whether cases are paucibacillary (those that have very few number of bacilli), which require a prescribed regimen for about six to nine months, or multibacillary (having large number of bacilli in their bodies), which prescribed regimen extends to an average of two years. Treatment must be supervised throughout and continuity and regularity need to be maintained. On the part of the control staff, it also means the careful monitoring of the effect of treatment and toxicity of the drug regimens by regular clinical and laboratory investigation as well as the requirement of maintaining proper records of cases.
Irregular treatment is a major problem in leprosy control. A contributory factor lies in the length of the disease as well as the length of the treatment involved, necessitating patience and regularity. Ironically and sadly, many patients become regular only after nerve damage or deformity has occurred. Prior to the Introduction of MDT, or in those areas where Dapsone monotherapy is still continuing, absenteeism in Nepal has been reported to range from 45% in some districts to 75% in others. In Sri Lanka, the average absenteeism rate is about 50%.
19

There is at present no alternative to early and regular
treatment. Research is however, being carried out in a number of
areas to see whether the action of the drugs presently in use
cannot be prolonged or their frequency of administration
reduced. Answers are also required on how to make the best use of
the available chemotherapy involving new combinations of
available drugs. The search must go on for newer and more
powerful agents. Advances in the medical sciences lends hope to
speedier and more efficacious control mechanisms.
The Special Programme for Research in Tropical Diseases
under the World Health Organisation (WHO) has been engaged in
developing a vaccine based on the lepra bacilli. This vaccine is
presently undergoing field trials in various countries. A pro-
posal to start field trials of this vaccine in India is presently
under consideration. Indian scientists have also been working
for several years on the development of vaccines, having
Immunological similarity with Mecrobacterium laprae. Field
tests are presently been undertaken in Maharashtra. These are
likely to take about five years before the efficacy of the vaccine,
which has had fairly positive results in a limited controlled
context, can be assessed. The Talwar vaccine has had success in
the t reatment of lepromatous cases of pronounced skin
condition, but is not in its true sense a prophylactic. The
vaccine developed by the Indian Cancer Research Centre is likely
to soon start field trials. However, the prognosis regarding these
developments and field tests must remain guarded, for it
remains to be seen whether they might actually help the
leprometous type of patients is developing immunity. Not all
vaccines that have been developed have shared equal success.
The Polio vaccine is a case in point. Whereas the vaccine against
Smallpox was invented in 1796 the eradication of Smallpox has
only recently become a reality. Nevertheless, the prophylaxis of
leprosy through a vaccine should in every way be encouraged, as
its success would spell an important advance in the quest to
control the disease.
20

Rehabilitation as a factor in leprosy control :
The need for rehabilitation of the leprosy affected cannot be
taken as an end product in an assembly-line approach involving
different components such as community survey, community
education, public health measures and treatment. To present an
everyday example, a beggar bearing leprosy deformity is almost
automatically taken to be suffering from the disease: the fact that
he may no longer be a carrier of the Mycrobacterium laprae and
that deformity arose out of earlier neglect, is not often realised.
In the eyes of the average person he remains a "leper". Leprosy is
therefore one disease where the need of rehabilitation
sometimes begins at the stage of diagnosis and treatment, and
requires to be continued unt il such time as the affected is
vocationally settled (or re-settled), and socially accepted in the
community to which he belongs. More than for any other
disease, the leprosy eradication programme requires an
integrated approach, involving both the medical control aspects
as well as 'inputs to counter problems of sociological displace-
ment and possible psychological impairment.
Everyone is agreed that there can be no substitute for early
detection and treatment. If leprosy were diagnosed early and
treated adequately, deformity would be prevented and leprosy
would soon divest itself from the whole body of misapprehension
that has inculcated itself into the religious, cultural and
sociological matrix of society. Sadly, however, leprosy is not
always diagnosed early and transmission and disabili ties
continue to occur.
It therefore becomes essential for the leprosy control
mechanism to step in at a sufficiently early stage in order to
prevent initial impairment and early disability from becoming a
major handicap leading to "dehabilitation" and its possible
consequences.
The control strategy must aim not merely at prevention as a
part of treatment, involving as this does public health and
21

specialised educational campaigns, but physical and vocational
r eh ab i l i t a t i on s chem es as w e l l . Th i s cou ld fo r es t a l l
"dehabilitation" avoiding not only individual tragedy, but also a
potential problem for the State.
The essence of a viable rehabilitation policy is not only that it
should be integrated into the leprosy control policy, but that it
should aim to be community-based and low cost. It is now
widely realized that the institution-based approach is neither
economical, nor indeed is it possible to isolate the numbers
involved behind walls of one kind or another. Nor is this
approach desirable, because it only perpetrates stigma instead of
dismantling it. For rehabilitation to be possible on the scale
required in many countries, it must be inexpensive and its
ad m i n i s t r a t i o n s h o u l d b e t i m e l y e n o u gh t o p r e v e n t
displacement, within the parameters of limited resources, it is
necessary to integrate measures of leprosy rehabilitation with
community education, public health, and treatment.
22

C. Stigma in Leprosy
Goffman describes a stigmatized person as one with a “spoiled identity'. Stigma in its dictionary meaning is variously a stain, taint or defect, a sign of moral blemish, a reproach caused by dishonorable conduct or as in an earlier age, a mark caused by a branding iron, as in aspects of slavery or criminality. Stigma takes on differing degrees of intensity which vary from and within societies and situations. Stigma is attributed to physical and social characteristics as well as aberrations in character. Deformity is the obvious physical characteristic. Character infirmities include deviant behaviour, imprisonment and frequent unemployment cycles. Sociologically, stigma is principally associated with race, colour, religion and, in India, caste as well. Stigma however recognizes hierarchy. The physically handicapped in general are less stigmatized than, say, the mentally ill. Physical disability caused by war or a similar patriotic function is usually quite acceptable. Social strata affects acceptability. A mentally ill or physically handicapped person is more acceptable if the person belongs to the upper classes or is wealthy. There is however, a sharp distinction between the leprosy-handicapped and other handicapped
persons.* While most handicapped persons are viewed as some what less than normal, they remain within their own milieu, homes, vocations and envoirnment. The leprosy- affected, on the other hand, have traditionally been ostracised to the extent of being excommunicated by society.
That stigma should have been attached to leprosy from early times because neither causation nor cure were known till a hundred years ago can perhaps be understood; that stigma still persists in many countries, and community understanding and cooperation is far from satisfactory is a matter of deep concern. Community attitudes vary in different countries, and indeed even in different regions in the same country. In some areas the occurrence of the earliest skin patches starts the cycle of fear,
* S. D. Gokhale " Social Aspects of Rehabilitation of leprosy Affected persons"
23

concealment, neglect and deformity; in others where there may
have been educational campaigns or easier availability of
treatment and cure, there may be a greater degree of tolerance
even to deformity. Paradoxical as it may seem, it is generally
accepted that attitudes and behaviour of the blue and white-
collared educated urban dwellers, is more stigmatizing than is
evident in rural areas.*
Leprosy therefore continues to be considered the most
stigmatised disease of all, barring the recent Acquired Immune
Deficiency Syndrome (AIDS). It was because it was viewed as
divine retribution that Missionary activity applied itself to the
"upliftment" of the leprosy-affected. Again, every society has its
concept of aesthetics, beauty and form. Into none of these could
leprosy ever fit, " its victim altering with the advancement of
the disease from normality into deformity. For much the same
reasoning there was much less stigma attached to tuberculosis or
smallpox. People did fear tuberculosis but there was little
stigma, because there was a long-term cure, and there were no
outward manifestations of the disease. Smallpox in India was
dreaded, but viewed as a visitation of the Mother Goddess, a
disease which was either fatal or cured within a specific time
limit. Although it left its mark behind, it was not viewed by
traditional societies in India as a progression the object of which
needed to be distanced. In the case of leprosy, however, stigma
was and cont inues to be perpetuated by ignorance and
misapprehension, that assumes contagion or infectibili ty,
whereas in most cases there is none. Even the literate equates
deformity with infectivity.
The common urban perception of leprosy are beggars on the
streets bearing deformity or ulceration in the hands and feet,
often without eyebrows and with depressed noses. Ironically such
• Dr. M.V. Yellapurkar, Deputy Director, Health Services (Leprosy), Govt. of Maharashtra - 'The Leprosy Control Programme in Maharashtra in Relation to Rehabilitation". Vocational Rehabilitation of Leprosy Patients. Report on the 1LO/DANIDA Asian Regional Seminar, Geneva, 1982.
R.K. Mutatkar, "Society and Leprosy." Chapter 1.
24

cases are most often not infectious, the infectious cases being relatively harder to identify.
Self-perception is quite identical to society's general perception, and follows from it. When a person discovers that he (or she) has contracted leprosy, lie begins to view himself as he viewed the leprosy affected in general, that is with some degree of dread or contempt. Upon discovery of the disease, his aspirations record a change. A defensive mechanism often develops in order to protect his immediate family from the humiliation of public discovery. There may be a daughter to marry, or a son to settle, a myriad of human accommodations yet incomplete. Too often to recount, he hides the disease until its outward manifestations became obvious, by which time conventional treatment cannot disguise deformity. Severe psychological damage, personality changes and deviancy often result. The logical end in such cases, happily less frequent now, was to leave home and as far as possible from known environs, to spare loved ones the "shame", or to protect oneself from the humiliation of being outcasted by family, friends, neighbours and the community.
An important difference between the stigma attached to
leprosy and that attached to caste or colour, is that in the case of the latter, the incumbent is attached to his respective group at birth.
* Moreover, his physical and emotional needs continue to be
fulfilled within his own social grouping. The incumbent continues to play the familiar roles of father, mother, child or sibling. The person's occupation or role in the family community or society remains undisturbed. He continues to derive a level of fulfillment from whatever job or task was being fulfilled. But in t h e ca s e o f l ep ro s y t h e re i s a m a r k ed ch an ge , f r om a comparatively higher status in to which he was born, to a situation sans status. It can sometimes be a dramatic social death, which applies equally to the work situation and, often pitilessly, to the domestic situation. Ironic as it may seem, even practitioners of medicine are sometimes reticent to accord him
• R.K. Mutatkar `The Leprosy Affected and their problems"
25

the status of a patient, which is given to persons suffering from more "acceptable" diseases.
There is a body of opinion that believes that the medical profession continues, by and large, to remain aloof from the medical problem. In terms of sheet numbers , medical practitioners working in the field are far outnumbered by para-medical and social workers. Doctors continue to display a lack of clinical confidence.' and body of knowledge about the disease. Several practitioners are unwilling to handle leprosy patients, sometimes for fear that this may not be tolerated by the bulk of their cl ientele. This too is st igma, and has the effect of strengthening society's misapprehensions, instead of the reverse. Conversely, fear of identification causes patients to shy away from specialised leprosy clinics and hospitals. Nor do they always welcome being contacted at home by leprosy technicians or workers. With stigma being so deeply ingrained, a view has been taken that it is self-defeating to maintain special leprosy clinics and hospitals. Some social scientists and leprologists advocate change in terminology used, such as "leprosy hospitals". leprosy projects, or even the word "leprologist". and would wish to see the National Leprosy Eradication Programme integrated with general health services.
Legislation too, in more countries than one continues to support stigma. Legislation concerning leprosy had its basic assumptions in the beliefs of incurability and infectivity. In many countries such legislation was enacted in the 19th century and sought to enforce compulsory segregation. In India, too, the Leprosy Act of 1898 reflected the social perceptions of the time, and was based on the premise that leprosy was incurable and that all cases were infectious. This Act and the Railway Act of 1890 as well as other legislation, affected a number of areas of segregation including the use of transport, presence of the leprosy affected in public places, as well as in the personal sphere affecting marriage, divorce, and inheritance. The Leprosy Act of 18.
c.‘.8 has since been repealsed by the Govt. of India in all Union
RK. Mulatkar-"Society and Lcprosy"
26

Territories. Eight State Governments have also repealed it. but it
continues to remain on the statute book in most States. Although
i t would appear that i t s provisions are no longer being
implemented vigourously, its presence on the statute book is
reflective of the casual attitude adopted towards the situation by
society at large.
27

D. The Global Si tuation
It must be stated at the outset that there are no accurate
statistics available. It is also difficult to compile global estimates
when the quality of data varies considerably from and within
regions. Enumeration of cases in some regions is less complete
than in others and registered cases represent only a proportion of
total estimated cases. The WHO's current global estimate is
between 10-12 million estimated cases. 10 million is an estimate
that may be considered conservative by many, who arc more
likely to place the figure nearer to 20 million.
There is a major difference between registered and estimated
cases. The WHO believes that only about 50% of the total
estimated cases are ever registered. Registered figures in
themselves have to be carefully considered. Patients rendered
inactive may continue to be retained on registers for a variety of
reasons. There are problems of duplicate registration in some
places. Not all registered persons take their treatment with
requisite regularity. It is true that wherever the multi -drug
regimen has been introduced, it has become necessary to keep
more scrupulous records, but this regimen has yet to be
comprehens ively in t roduced in many count r ies . Whi le
information on registered cases is by definition much more
reliable, it does not particularly help us to arrive at an accurate
compilation of total estimated cases.
The figures of registered cases are therefore only a part of the
total scenario. Equally important is the prevalence rate, which
demonstrates the intensity of the disease in the total population. A
prevalence rate of 1 case per 1000 persons is considered to be a
serious public health problem. It is estimated by the WHO that
approximately 1.6 billion people live in areas where prevalence
is over 1 case per 1000. Such areas constitute serious public
health problems, and the populat ions in these areas are
considered to be at risk.*
* Dr. S. K. Noordeen and L. Lopez Bravo 'The World Leprosy Situation".
28

Table 1 complied by the WHO presents a distribution of
registered cses, prevalence rates and the proportion of cases WHO-
region wise for upto 1985. Table 1 needs to be read in conjuction
with Table 4 because the WHO Regions are quite distinct from the
normal definition of geographical regions. According to this
estimate, South East Asia contributes the largest share of
registered cases (69.6%), with Africa at second place (18.4%),
followed by America including South America (5.7%). the
Western Pacific which includes Australia and several Asian
countries (4.6%), the Eastern Mediterranean Region including
Egypt, the Arab World and Afghanistan (1.4%), and Europe
including Morocco and Turkey (0.3%)
Keeping in view the WHO definition of Regions, Table 2 shows
the number of registered cases for 1966, 1976 and 1985. The
bracketted figures indicate the number of countries from which
the figures have been compiled, making strict comparisons
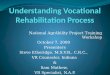
difficult. However, Table 2 does demonstrate that the South-
East Asia Region has contributed the preponderant number of
cases, with a sharp upward swing from 1,748,468 (for eight
countries) in 1976 to 3,737,159 (for nine countries) in 1985.
Equally significant Africa has shown a downward swing from
1.398,220 (for 38 countries) in 1976 to 987.607 (for 43 countries) in
1985.
Table 3 renders comparison somewhat easier in that it
presents the number of registered cases in 92 countries over the
same period. The African region has shown a decline of 23.9%
from 1966 to 1976 and again a decline of 28.2% from 1976, to
1985. These figures may be questioned as to their accuracy; for
instance it is not certain whether they might represent a certain
proportion of reduced case finding, but nevertheless the figures
are accepted to represent a declining trend. The South-East Asia
region however has shown a corresponding increase of 117.2%
and 113.3%. respectively. The single largest contribution to the
figures of the South East Asia region is from India. with a
registered leprosy population of 3.2 million, and an estimate
variously placed above 4 million.
29

Some countries have, however, achieved complete coverage.
and in these prevalence has declined. These include Australia.
Japan, Malaysia, the Philippines, the Republic of Korea, Sri
Lanka and Thailand, as well as several smaller countries such as
the Pacific Island countries of Fiji, Gaum, Solomon Islands,
Tonga and Vanuatu as well as Hongkong and Singapore. The
situation in several other Asian countries however continues to
generate concern. In Bangladesh there are 35,802 registered cases In
a population of 96.7 million. Only 22% of the total estimated
cases have so far been registered. The treatment default rate is
estimated to be as high as 40%. Burma with a population of 37.6
million has about 253.000 registered cases, of which about
87.6% are under regular treatment. In China the registered
number of cases is stated to be 1,00,000, in a total population of
1000 million. These figures are stated to have been identified
through mass screening surveys and care is largely organization or
institution-based. Indonesia has 127,870 registered cases in a population of 161.6 million.
Nepal with a population of 15 million has almost 35,000
cases with a prevalence rate ranging in different zones from 3.2 to
8.7 per 1000. Sri Lanka with a population of 15 million has
10,520 registered cases with an overall prevalence of .67/1000.
Malaysia with a population of 13 million has approx. 7500
registered cases, and the leprosy control programme is well
integrated with the general health services. Thailand represents
another success story in this field as indeed it does in other areas
such as family planning and general health services. In 1963
there were an estimated 1,40,000 number of cases with an
overall prevalence of 5/1000 of population. Since then the
country has developed a very well-organised structure and
programme involving government, voluntary and International
effort. Today Thailand has come down to 46,000 registered cases
in a population of 50 million. Prevalence in the whole country
has been below 1/1000 since 1976 and was 0.9/100G in 1979.
According to an evaluation survey made by WHO over a ten. year
interval in the Khonkaen province, prevalence fell from a high
of 12.37/1000 in 1962, by as much 70% over the next ten years.
30

Thailand as well as a number of these countries have effectively
integrated the leprosy control effort into their general health
services.
The American region has shown an increase in the periods
reviewed in Tables 2 and 3. This is largely due to increases in
Brazil . There has also been an increase in prevalence of
registered cases in the Eastern Mediterranean region, but
country-wise prevalence is below 1 per 1000 of the population and
therefore does not constitute a risk. There is virtually no
prevalence in Western Europe. North America and New Zealand.
31

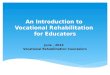
TABLE I
TABLE 1. DISTRIBUTION OF REGISTERED LEPROSY CASES BY WHO REGION, 1985
Registered cases
WHO Region Population latest official estimate (000)
Number Prevalence rate
per 1000 Proportion of cases to the total
(%)
Africa 421782 987607 2.34 18.4
Americas 654958 305999 0.47 5.7
South-East Asia 1130605 3737157 3.31 69.6
Europe 633838 16794 0.03 0.3
Eastern Mediterranean 290277 74802 0.26 1.4
Western Pacific 1359562 245753 0.18 4.6
Total 4491022 5368202 120 100.0
Or for the most recent year for which data are available
Population data from World Health Statistics Annual 1985.
32

TABLE 2
REPORTED REGISTERED LEPROSY CASES BY WHO REGION FOR THE YEARS 1966, 1976 AND 1985
WHO Region
Number of registered cases (Number of countries)
1966 1976 1985
Africa 1685526 (38) 1398220 (38) 987607 (43)
Americas 177813 (47) 241248 (40) 305999 (41)
South-East Asia 790851(6) 1748468(8) 3737157 (9)
Europe 19589 (20) 20452 (20) 16794 (10)
Eastern Mediterranean 40963 (10) 63236 (20) 74892 (21)
Western Pacific 117003 (30) 128325 (22) 245753 (27)
Total 2831745 (151) 3599949 (148) 5368202 (151)
• Or the most recent year for which data are available.
33

TABLE 3.
REGISTERED 'LEPROSY PATIENTS IN 92 COUNTRIES IN 1966, 1976 AND
1985, BY WHO REGION
Number of Number of Percentage Number of Percentage registered cases registered cases (or decrease) registered cases (or decrease)
WHO Region (Number of countries) 1966 1976 1985
Africa (26) 1460962 1111714 -23.9 798148 -28.2
Americas (34) 176514 238901 35.3 303607 27.1
South-East-Asia (5) 790851 1717415 117.2 3662657 113.3
Europe (8) 9377 13113 39.8 14463 10.3
Eastern Mediterranean (4) 885 3546 300.7 5350 50.9
Western Pacific (5) 79279 104829 32.2 101438 -.
-3.2
Total (92)
2517868
3189518
26.7
4885663
532
34

TABLE 4
REGISTERED LEPROSY CASES IN THE WORLD, BY WHO REGION
Countries or areas
AFRICA
Population estimate
(000)*
Number
Number of registered eases
Prevalence Year rate per 1000
Algeria 20500 ….
……
….…..
…. Angola 8540 300160 1975 3.51. Benin 3825 21469 1981 5.61 Botswana 1051 198 1982 0.19 Burkina Faso 6582 33478 1981 5.09
Burundi 4537 4828 1981 1.06 Cameroon 9432 23738 1985 2.52
Cape Verde 296 781 1979 2,64 Central African Rep;ublic 2442 8350 1983 3,42 Chad 4901 13113 1983 2.68 Comoros 421 1308 1979 3.11 Congo 1695 9920 1985 5.85 Cotc d' Ivoire 9300 49051 1984 5.27 Equatorial Gunca 300 ... Ethiopia 33680 70809- 1984- 2.10 Gabon 1146 3885 1984 3.39 Gambia 696 2414 1981 3.47 Ghana 12700 15331 1981 1.21 Guinea 5301 48557 1979 9.16 Guinea Bissau 810 2879 19891 3.55 Kenya 19536 8301 1981 0.42
Lesotho
35

Countries or areas
Population estimate
(000). Number Year
Prevalence rate per 1000
Liberia 2109 4202 1979 1.99
Madagascar 9400 35930 1979 3.82 Malawi 6839 17925 1981 2.62 Mali 7719 81657 1982 10.58 Mauritania 1832 699 1981 0.38 Mauritius 1011 E6 1981 0.07 Mozambique 12615 12829 1979 1.02 Namibia 1507 ... Niger 5686 16205 1982 2.8.5 Nigeria 92037 281601 1982 3.06 Reunion 532 227 1983 0.43 Rwanda 5757 1400 1983 0.24 Sao Tome & Principe 94 20 1981 0.21 Senegal 6316 15728 1981 2.49 Seychelles 53 1979 0.82 Sierra Leone 3600 12915 1979 3.59 South Africa 31586 16030 1975 0.51
Swaziland Togo
605 2747
123 11573
1980 1982
0.20 4.21
Uganda
15150 15309 1981 1.01 United Republic of Tanzania 21062 35097 1983 1.67 Zaire 30261 56648 1982 1.87 Zambia 6242 16642 1982 2.67 Zimbabwe 7980 5892 1979 0.74
Total 421782 987607
2.34
AMERICAS
Anguilla 9 5 1984 0.56 Antigua and Barbuda 79 47 1984 0.59 Argentina 29627 12506 1984 0.42
Bahamas 231 41 1984 0.18
36

Population
Prevalence
estimate rate per 1000 Countries or areas (000). Number Year
Barbados 252 33 1984 0.13
Belize 156 … … … Bermuda 56 1 1984 0.02 Bolivia 6082 1834 1983 0.30 Brazil 129660 206081 1983 1.59 Canada 25150 186 1983 0.01
Cayman Islands Chile
19 11780 10 1984 0.00
Colombia 28776 20737 1983 0.72
Costa Rica Cube
2467 10059
642 57 16
1984 1984
0.26 0.57
Dominica 77 19 1984 0.25
Dominican Republic Ecuador
El Salvador
6416 9257 4999
5132 22 12
184
19 84 1984
19 84
0.80 0.24
0.04
French Guiana 73 255 1984 3.49
Grenada Guadeloupe
112 332
281 115
1984 1983
0.25 3.47
Guatemala 7740 422 1983 0.05 Guyana 4 793 243 1984 0.31
Haiti Honduras
453185 72
948 103
1984 1984
0.18 0.02
Jamaica 2 190 802 1984 0.37
Martinique Mexico
327 78524
1804 16448
19 83 1984
5.52 0.21
Montserrat 12 4 1984 0.33 Netherlands Antilles 250 Nicaragua 3058 142 1964 0.05 Panama 2134 145 19 84 0.07 Paraguay 3278 4963 1984 1.51 Peru 29698 33 59 1980 0.17 Saint Christopher and Nevis 45 14 1984 0.31
Saint Lucia 134 217 1984 1.62
37

Population
Prevalence
estimate rate per 1000 Countries or areas (000)* Number Year Saint Vincent & the Grenadines Saint-Vincent-et-Grenadines 124 48 1984 0.39 Suriname 364 2311 1982 6.35 Trinidad & Tobago 1149 141 1983 0.12 Turks & Caicos Islands _ 7 18 1984 2.57 United States of America 2 36681 4330 1982 0.0 Uruguay 2990 688 1984 0.23 Venezuela 16851 12032 1984 0.71 Virgin Islands (British) 12 ... ... ...
Virgin Islands (USA) 104
Total 654958 305099 0.47
SOUTH -EAST ASIA
Bangladesh 96730 35802 1982 0.37 Bhutan 1388 2365 1985 1.70
Burma 37614 253285 1985 6.73 Democratic Peoples Republic of Korea 19630 0 1985 0.00
India 730540 3225302 1985 4.41 Indonesia 161632 127870 1985 0.79 Maldives 180 1183 1985 6.57 Mongolia 1866 0 1985 0.00 Ncpi1 15023 35150 1985 2.34 Sri Lanka 15606 10520 1985 0.67 Thailand 50396 45680 1985 0.91
Total 1130605 3737157 331
EUROPE
France 54947 Germany, Federal Republic of 61089 53 1975 0.00 Israel 4244 242 1979 0.06 Italy 57024 540 1980 0.01
Malta 360 195 1983 0.54
38

Countries or areas
Population estimate
(000). Number Year
Prevalence rate per 1000
Morocco 20420 3485 1981 0.17 Netherlands 14443 600 1978 0.04 Portugal 10164 2278 1983 0.22 Spain 38228 5109 1982 0.13 Turkey 48265 3967 1980 0.08 United Kingdom 49654 325 1984 0.01 USSR 275000 ... ...
Total 633838 16794 0.03
EASTERN MEDITERRANEAN
Afghanistan 17672 1346 1985 0.08 13ahrain 400 41 1985 0.10 Cyprus 657 156 1984 0.24 Democratic Yemen 2225 205 1980 0.09 Djibouti 3330 69 1975 0.21 Ekrpt 45915 23736 1984 0.52 Iran (Islamic Republic of)
. 43414 11192 1985 0.26 Iraq 14110 500 1980 0.04
Jordan 2779 0 1985 0.00 Kuwait 1695 0 1985 0.00 Lebanon 2644 45 1984 0.02 Libyan Arab Jamahiriya - 3637 644 1975 0.18 Oman 1181 275 1980 0.23 Pakistan 93286 21533 1981 0.23 Qatar 257 Saudi Arabia 10824 1670 1985 0.15 Somalia 5423 3056 1985 0.56 Sudan 20564 8790 1982 0.43 Syrian Arab Republic 9934 124 1985 0.01 Tur,loia 6886 153 1978 0.02 United Arab Emirates 1206 29 1984 0.02 Yemen 5238 1331 1983 0.25
Total 299277 74892
0.26
39

Population
Prevalence
estimate rate per 1000 Countries or areas (000). Number Year
WESTERN PACIFIC
American Samoa 34 73 1983 2.06 Australia 15544 2661 1982 0.17 Brunei Darussakun 214 China 1036040 100066 1983 0.10 Cook Islands 17 26 1982 1.53 Democratic Kampuchea - 7149 FIJI 686 375 1984 0.6.6 French Polynesia 167 298 1980 1.78 Gaum. 116 26 1982 0.22 Hong Kong 5579 1638 1983 0.29 Japan 120018 8944 1983 0.07 Kiribati 62 118 1983 1.90 Lao People's Democratic Republic 3585 2988 1984 0.83 Macao 343 % 1984 0.28
Malaysia 13393 7443 1983 0.56 Nauru 7 40 1981 5.71 New Caledonia 147 487 1983 3.31 New Zealand 3300 52 1975 0.02 Pacific Islands (Trust Territory) - 142 1469 1984 10.35 Papua New Guinea 3190 8851 1983 2.77 Philippines 53351 37397 1983 0.70 Republic of Korea 40578 27148 1984 0.67 Samoa 159 137 1984 0.86 Singapore 2544 7882 1983 3.10 Solomon Islands 221 7C0 1982 3.17 Tonga 99 23 1982 0.23 Tuvalu 7 10 1983 1.43 Vanuatu 128 258 1981 2.02 Viet Nam 52742 36616 1983 0.69
Total 1359562 245753
0.18
40

E. The Indian Scenario
Leprosy continues to remain a major health problem in
India. With 3.16 million cases on record in March, 1988, and an
estimated total slightly above 4 million, India accounts for
nearly a thi rd of the world 's leprosy cases. The avera ge
prevalence rate is estimated to be 5.72 per thousand, though in
some States prevalence is well above the national average.
Present estimates also indicate that nearly 1/4 to 1/5 of cases are
infectious and that 15 to 20 per cent suffer from disabilities such
as anaesthesia, noticeable deformity of hands/feet, ulceration,
depressed noses, blindness, or a combination of these. Sadly 20 -
25% of all cases occur in children below 14 years of age.*
National level data is, however, not available with regard to the
proportion of crippled patients, or those having correctable
deformities or those needing vocational rehabilitation. Studies
are needed to collect this information.
There was a very sizeable increase in case detection during the
Sixth Plan period accounting for 41. 5 per cent of the total case
detection thus far (21.44 lakhs out of 51.70 lakhs).**
While this
is unmistakably an indicator used for the assessment of
performance in case detection, it also indicates that in certain
States the inherent problem is perhaps of a dimension not fully
accounted for. There are marked inter-State variations ; the
district-wise data collected for 1984-85 indicates that 201
districts had a high endemic prevalence rate of 5 and above per
thousand. According to 1987 figures, 201 out of 430 districts in
the country continue to have disease endemicity of 5 and more
per 1000 of population. The number of cases on record in June,
1987 was 3,301,969 ; the number of cases under treatment and
discharged in June, 1987 were 3,043. 705 and 2,474,967
respectively. (Table 14). The 1981 census placed 58% of the
country's population (400 million) at risk. In March 1988 an
estimated 2.7 million were undergoing treatment.
* Leprosy - Status Report 1985-86 - Leprosy Division, DGHS (p.3) ** Ibid (p.42)
41

Until a few decades ago, there was a surprisingly remarkable coincidence in the approach to the problem of the leprosy- affected adopted both by society at large and by Government. The attitude was at best one of benign neglect. The disease was treated largely as a social problem, and the affected were outcast socially and physically. Some institutions, asylums and leprosoriums, were started mainly by voluntary effort where a few thousand patients were interned. Leprosy colonies mushroomed in urban outskirts and elsewhere as an answer to society's requirement that the leprosy affected live without being seen.
The advent of Christian missionary effort in the 19th century brought the first reasonably organised efforts as well as a humane attitude to leprosy work. This coincided with the discovery in 1874 by Hansen of the leprosy bacillus as the causative organism. At about this point hydnocarpus oil became the first specific form of treatment of the disease. Segregation however continued to remain the main method of control. The first known asylum in India appears to have been established in Calcutta in the early 19th Century. However, there is evidence that Raja Kali Sankar from Bengal established a Leper Asylum in Benares in 1810, which he later handed over to the Church to administer.
It was not until the introduction in the mid 1940's of sulphones as method of control that it became possible to think of effective domiciliary-based treatment. For as the size and dimension of the problem became known, it had become clear that large scale segregation was not even feasible. The reservoir of leprosy in the country was enormous, and segregation of such a large affected population was not possible either in terms of its infrastructural dimensions, or its financial implications or. Indeed, even in terms of the human resources that such a policy would entail. There would be social problems as well, and instead of encouraging the affected to remain within the community, the reverse would result. Meanwhile patients would have a tendency to hide the disease for as long as they were able.
42

Side by side with the early Christian missionary effort, pioneering work was also undertaken by several other voluntary bodies, not least among which was the innovative work of the Gandhi Memorial Leprosy Foundation (GMLF) at Wardha in developing the early SET model. This later came to be adopted by Government, and eventually led to the introduction of organised leprosy control in the national health programme. The start of organised leprosy work, however, began with the establishment of the Indian Council of the British Empire Leprosy Relief Association in 1925 (renamed the Hindu Kusht Nivaran Sangh in 1947). In 1941 the Government of India appointed a Committee w h i ch r ev i ew ed t h e ex t en t o f t h e p r o b l em an d m ad e recommendations. In the 1940's the GMLF experimented and refined the method that has come to be known by its different stages - Survey, Education and Treatment ( S E T ) of the population at large in endemic areas. In 1954. the Government's Expert Committee adopted this model and developed it into the National Control Programme (NLCP). Immediately prior to this, emphasis was placed on treatment, and the work was largely in the voluntary sector. A total of 152 institutions provided 142.6 beds per 10,000 estimated cases. The Statewise distribution was uneven. Equally uneven was outpatient clinical care. 1203 clinics in the country provided a ratio of an average of 1 clinic per 300,000 population. The First Plan (1951 -56) covered a cumulative population of 20 lakhs
. detected 17,000 cases and its
total allocation of expenditure was Rs. 35 lakhs. The NLCP coincided with the Second Plan (1956-61) and while it did not see a very high figure in terms of cumulative cases detected (1,12,000), the cumulative population sought to have been covered was appreciably higher at 1,47,000 and expenditure allocated had dramatically increased to 529 lakhs, all of which was provided by the Central Government. The Plan documents of 1951, 1956, 1961 and 1969-74 focussed on inputs to be provided in rural areas with high and moderate endemicity. In its earlier years, the programme suffered from several constraints, not the least amongst which were non-availability of potent drugs as well as the high degree of social stigma that came to be encountered. It
* 1 lakh represents 100,000
43

was only from the Fifth Plan period that the programme gained
sharper focus. Expenditure in the Fifth Plan (1974-79) was 2023
lakhs compared to 286 lakhs during the the Fourth Plan (1969-
74) and Rs. 63 lakhs each year during the Annual Plans (1966-69).
In 1976 the programme was made performance-oriented; each
Stale was given targets for case detection, treatment and
discharge after treatment and cure. More systematic effort was
emphasized for survey and case detection, registration of cases,
domiciliary sulphone treatment and community education. An
Important assumption made was that this was a disease of rural
incidence and urban prevalence. It was during the Fifth Plan
that the programme was extended to urban areas as well.
By the end of the Fourth Plan (1969-74) only one third of the
endemic population had been covered. During the Fifth Plan
(1974-79) coverage had increased to three fourths of the endemic
population. It had taken over a decade to iron out a number of bottle-
necks not the least of which were the need for several infrastructural
and financial arrangements. These factors made possible a
significantly high rate of increase in case detection during the
Sixth Plan Period (1980-85). Equally important was the factor of
treatment. By 31st March 1985, of the 3.24 million cases on
record, 3.02 million (or 93.2%) had been brought under treatment.
Since 1955, a total number of 1.93 million cases had been
discharged due to cure or death.
Upto 1968-69 the NLCP was a Centrally aided programme,
and i t was developed, managed and f inanced b y S ta t e
Governments, with assistance from the Central government.
From 1969-70 however i t became a Centrally sponsored
programme and total expenditure was charged to the Union
Government, with implementation by the States according to the
guidelines laid down by the Centre. During the Fifth Plan
expenditure was sought to be shared. The Sixth Plan reverted to
the programme being entirely Centrally aided. The Sixth Plan
r e f l e c t e d G o v e r n m e n t ' s r e n e w e d d e t e r m i n a t i o n t o
eliminate leprosy. The programme had been renamed the
44

National Leprosy Eradication Programme (NLEP) and allocation
of f inancia l r esources doubled to Rs . 4120 l akhs . The
infrastructural base was enlarged to create additional posts for
450 full-time doctors and 3200 additional field staff. There was a
significant increase of several related physical factors.
In 1982. a working group was set up by the Government under the
Chairmanship of Dr. M.S. Swaminathan with a number of
eminent leprologists. distinguished public health experts and
social scientists and scien tists to formulate a strategy to
eradicate leprosy by the end of the century. The Committee would
take into account the "great advances in the chemotherapy of
leprosy, the extended reach of the mass media, the promise of
recent medical research and other relevant factors". The terms of
reference were wide ranging and included the control aspects (the
chemotherapy to include the indigenous production of anti -
leprosy drugs and its delivery system). the sociological, legal and
rehabilitation dimensions, the role of the voluntary sector and
medical education.
This landmark report was submitted to Government in
February 1982. Its recommendations were for the most part
immediately accepted, and culminated in a policy statement
calling for the eradication of leprosy in India by the year 2000
AD. The NLCP was renamed the National Leprosy Eradication
Programme, and was declared time bound and target oriented.
The desire to see an end to leprosy came to be reflected in the
Twenty Point Programme.
The winds of change began to reflect themselves in other
related spheres. The Indian Leprosy Act of 1898, long an eyesore
on the Statute Book, was repealed by the Union Government in its
application to the Union Territories with effect from January.
1984. Repeal was urged on the State Governments.' A National
The Act has so far been repealed by the State Governments of Arunachal Pradesh, Kerala, Madhya Pradesh, Maharashtra, Mizoram, Orissa, Tamil Nadu and Tripura. It Is not applicable to Rajasthan and Sikkim. It is likely to be repealed by Karnataka and Uttar Pradesh soon.
45

Leprosy Eradication Commission was set up under the
Chairmanship of the Union Health Minister for Programme
Policy guidance, and a National Leprosy Eradication Board was
set up under the Chairmanship of the Union Health Secretary, for
monitoring the activities of the Programme. This consequently
necessitated the strengthening of the organisational structure
from its foundation upwards.
A far reaching recommendation of the Swaminathan
Committee was the need to speedily undertake a massive country
wide campaign to supplement dapsone monotherapy with bact-
ericidal drugs. and to establish the pre-requisites for such a
campaign in the form of population surveys, recruitment and
training of essential staff, health education and other necessary
infrastructural arrangements. A programme of combined
therapeutic regimen was launched in 1982 with SIDA assistance
and introduced in 12 highly endemic districts covering a total
population of 37.0 million. The number of districts placed under
coverage has since grown. While it is proposed to gradually cover all
201 districts having endemicity of 5 and more per 1000, by
March, 1988, 48 endemic districts covering a population of 100
million with an estimated leprosy case load of 1.34 million are
under coverage (see Table 15).
The efficacy of MDT has become clear. In 7 of the 12 districts an
intensive phase of five years was completed in July, 1987 on a total
population of 171.32 lakhs bearing a case load of 3.25 lakhs. The
prevalence rate in these seven highly endemic districts has reflected a
percentage decline of as much as 78%.
46

S.. District Prevalence Rate
No. before MDT
Prevalence Rate
in July, 1987 Percentage
Decline
1. Wardha 11.1 1.8 83.8
2. Purulia 19.2 7.7 60.0 3. Srikakulam 18.0 2.6 85.6 4. Ganjim 13.8 2.4 82.6 5. Viziangaram 13.6 2.4 82.4 6. North Arcot 18.1 4.3 77.8
7. Baroda 5.2 1.4 77.0
Maintenance activities to complete treatment, as well as detection
and treatment of new cases will continue for another five years,
when it is likely that the leprosy control activities in these
districts will be integrated with the basic health services during
the closing years of maintenance. The progress made in these and
other endemic districts may be seen in Table 16.
Until the point of integration is reached, the NLEP operates as a
vertical programme. One SET Centre with one para medical worker
for 25,000 population and one Leprosy Control Centre for every 4.5
lakh population would cover rural areas. In urban areas the ratio of an
LCC is to every 50,000 population besides hospitalization facilities.
In areas of endemicity below 5 per 1000, one SET Centre has been
established within the framework of the primary health care
infrastructure.
By December, 1987 the country wide Infrastructure had grown to 601
Leprosy Control Units, 919 Urban Leprosy Centres, 7000 SET
Centres. 215 District Leprosy Units and 294 Temporary
Hospitalisation Wards. 3.30 million leprosy cases were detected and
recorded; of these 3.04 million were brought under treatment. A total
of 2.47 million cases had either been discharged as cured or had
migrated or had died since the inception of the programme (see Table
14). Skilled manpower includes 2200 medical officers and 20.000
para medical staff
47

under the NLEP besides an additional 1100 trained medical and
3410 paramedical staff in the voluntary sector.
The role of the voluntary organisations in rehabilitation has
been treated in Chapter G. In statistical terms, there are
presently about 100 voluntary organisations actively engaged in
leprosy relief services. They are together estimated to provide
SET services to a population of 59 million spread over areas
with wide variation in the prevalence rate (1 to 32 per thousand).
of a total of 8.5 lakhs cases on their records. 7 lakhs had been
b r o u gh t u n d e r r e g u l a r t r e a t m en t .* M o s t o f t h em a r e
multifunctional. 82 are providing SET activities. 70 provide
curative as well as rehabilitation services. 14 are additionally
engaged in the organisation of training courses for medical
personnel, and some also provide referral courses.
Rehabil i tat ion service have hitherto been largely the
preserve of the voluntary agencies, which have developed along
different lines. Many of them have developed extremely
Interesting and useful models. The Swaminathan Committee, in
its list of recommendations, noted that it was essential for
rehabilitation to become an integral part of leprosy control.
Towards this end it suggested that coordinated efforts by the
Ministries or Departments of Health, Education and Social
Welfare, as well as by voluntary organisations was necessary.
with the Ministry of Health and Family Welfare as the nodal
point. A beginning is now proposed to be made. In the seven
MDT districts that have completed the intensive phase, it is
proposed to establish one Rehabilitation Centre each to provide
corrective surgery and vocational training to 3000 cured leprosy
patients with Grade-II (and above) deformity. It is proposed to
mix them with other non-leprosy handicapped. It is broadly
envisaged that the training programme should not have a very
long span. This may be about six months. During the training
period, each trainee would receive a stipend as well as food. The
vocational trainiiig courses would be developed to assist in re-
* Figures current for June. 1987. Ministry of Health and Family Welfare, Government of India.
48

integration at the community level. In order to provide for re-constructive surgery wherever it is needed, a local institution providing such facilities would be identified and used for referral services. There are presently 75 surgical units functioning under the NLEP. The number of leprosy rehabilitation units are only 11 and there are 45 training centres for medical personnel.
The emergence of several highly effective bactericidal drugs coincided with firmer political commitment, and gave a fillip to leprosy control. This was strengthened by the call given by the then Prime Minister Shrimati Indira Gandhi to Indian scientists to develop an eradication strategy. Indeed, it is widely acknowledged by the small and fraternal community engaged in leprosy control and rehabilitation services in India, that Shr imat i Ind i ra Gandhi had genuine s ympath y fo r disadvantaged groups in general, and the plight of the leprosy affected amongst them. Indeed it was her understanding of the helplessness of the lives of the leprosy affected that led her to confer her patronage to leprosy institutions the country over.
49

TABLE 5
Prevalence of Leprosy in India
Year Population
(millions) Estimated
No. of leprosy patients ( ,000)
'
Prevalence
rate (per 1000 popu- lation)
1871 198.291 108.8i 0.55 1881 216.679 128.09 0.59 1891 274.334 126.24 0.46 1901 294.361 97.36 0.33 1911 315.156 109.09 0.35 1921 318.942 102.51 0.32 1931 324.753 159.80 0.49 1951 360.958 1,374.01 3.81 1961 439.118 2,561.60 5.83 1971 547.958 3,200.90 5.84 1981 685.185 3,919.337 5.72
For data prior to 1971 Mohammad Ali. P. (1963) Facts and Figures about leprosy in India. Leprosy In India, 35, 10-26
• Table 5 to 12 are from Leprosy Status Report 1985-86, DOHS, Ministry of Health and Family Welfare, New Delhi.
50
Source :

TABLE 6
Distribution of Prevalence Rates of Leprosy by States/UTs
Prevalence rate States and UTs
1951 1961 1971 1981
Less than 1 (very low) 1 6 7 6
1-4 (low) 6 4 8 14 5-9 (moderate) 3 5 8 6 10-20 (high) 1 3 3 3 20-over (very high) 0 2 3 2
Total
11
20*
29*
31*
*for others data not available
1. Government of India, Ministry of Health (1955) Report of the Committee for Control of Leprosy. Government of India Press, Calcutta.
51

TABLE 7
Endemicity and Prevalence Rates of Leprosy in India - Statewise
S. N0.
State/ U.T. Estimated case load (lakhs)**
1951 1961 1971 1981
1 2 3 4 5 6
1. Andhra Pradesh 1.90 (4.84) 5.41 (14.44) 6.28 (14.43) 6.20 (11.58)
2. Assam 0.40 (4.4) 0.10 (0.84) 0.12 (0.81) 0.15 (0.75) 3. Bihar 1.23 (3.0) 2.80 (6.02) 3.39 (6.02) 3.80 (5.44) 4. Gujarat - 0.10 (0.48) 0.13 (0.48) 1.00 (2.93) 5. Haryana - - 0.01 (0.09) 0.01 (0.08) 6. Himachal Pradesh 0.07 (7.8) 0.06 (4.41) 0.15 (4.33) 0.07 (1.64)
7. Jammu & Kashmir - 0.04 (1.12) 0.05 (1.08) 0.05 (0.83)
8. Karnataka - 1.40 (5.93) 1.74 (5.93) 2.22 (5.98) 9. Kerala - 0.07 (0.41) 0.75 (3.51) 0.75 (2.95) 10. Madhya Pradesh 0.85 (3.0) 0.25 (0.77) 0.32 (0.76) 1.20 (2.30) 11. Maharashtra 1.04 (3.3) 2.20 (5.9) 2.80 (5.9) 4.00 (6.37) 12. Manipur - 0.02 (2.6) 0.06 (5.60) 0.08 (5.63) 13. Meghalaya - 0.06 (5.93) 0.06 (4.55) 14. Nagaland - - 0.17 (32.69) 0.05 (6.49) 15. Orissa 0.81 (7.50) 1.90 (10.82) 2.37 (10.80) 3.20 (12.14) 16. Punjab 0.01 (0.11) 0.03 (0.14) 0.02 (0.14) 0.20 (1.19) 17. Rajasthan - - 0.10 (0.38) 0.10 (0.29) 18. Sikkim - - - 0.025 (7.81)
19. Tamil Nadu 3.08 (8.4) 6.62 (8.99) 7.841 (19.00) 7.33 (15.14)

TABLE 7 (CONTD) Endemicity and Prevalence Rates of Leprosy in India - 8tatewise
S. No.
State/U.T. Estimated case load (lakhs)**
1951 1961
1971 1981
1 2 3 4 5 6
20. Tripura 0.02 (1.75) 0.10 (6.41) 0.10 (4.88)
21. U.P. 0.80 (1.4) 1.40 (1.89) 1.68 (1.90) 4.10 (3.70) 22. West Bengal 3.55 (b14.1)
(14.1
)
3.01 (8.01) 3.60 (8.12) 4.30 (7.88)
23. A & N Islands 0.003 (2.50) 0.01 (5.26) 24. Arunachal Pradesh 0.01 (2.12) 0.01 (1.59) 25. Chandigarh N.A. 26. D & N Haveli 0.001 (1.43) 0.001 (1.00)
27. Delhi 0.005 (0.12) 0.01 (0.16) 28. Goa, Daman & Diu O.04 (6.34) 0.05 (5.81) 0.05 (4.59) 29. Lakshadweep 0.01 (25.0) 30. Mizoram 0.01 (3.03) 0.01 (2.04) 31. Pondicherry 0.15 (40.54) 0.19 (40.42) 0.10 (31.67)
TOTAL
13.74 (3.81) 25.62 (5.83) 32.01 (5.84) 39.19 (5.72)
**Figures in brackets are rates per 1000 population.
Source: Mohammad Ali, P. (1963)., Loc. cit., Government of India, Ministry of Health and Family
Planning, DGHS, Leprosy Cell.

TABLE 8
No. of districts by leprosy prevalence rates by State/UT
S.
No.
State/UT 10+ 5 to 9.9 <5 Total
1. Andhra Pradesh 15 8 0 23
2. Assam 0 1 15 16 3. Bihar 11 11 9 31 4. Gujarat 0 6 13 19 5. Haryana 0 0 12 12 6. Himachal Pradesh 0 0 12 12 7. J & K 0 0 5
r 0
8. Karnataka 2 6 11 19 9. Kerala 2 8 4 14
10. Madhya Pradesh 1 16 28 45 11. Maharashtra 7 12 11 30 12. Manipur 0 3 5 8 13. Meghalaya 0 0 5 5 14. Nagaland 1 1 5 7 15. Orissa 8 5 0 13 16. Punjab 0 0 12 12 17. Rajasthan 0 0 25 25 18. Sikkim 0 4 0 4 19. Tamil Nadu 12 3 0 15 20. Tripura 0 2 1 3 21. Uttar Pradesh 6 24 26 56 22. West Bengal 7 9 0 16
1. A & N Islands 0 0 2 2
2. Arunachal Pradesh 0 3 4 7 3. Chandigarh 0 0 1 1 4. D & N Haveli 0 0 1 1 5. Delhi 0 0 1 1 6. Goa. Daman & Diu 0 3 0 3 7. Mizoram 0 0 3 3 8. Lakshadweep 1 0 0 1 9. Pondicherry 3 0 0 3
76 125 211 412
54

TABLE 9
List of Hyper Endemic Districts Statewise in India-1985
S. Name of state/ Name of districts Name of districts No. UT with prevalence with prevalence
rate 10/1000 rate 5 to 9.9/1000 and above
1 2 3 4
1. Andhra 1. Srikakulam 1. Adilabad
Pradesh 2. Vizianagaram 2. Hyderabad 3. Visakhapatnam 3. Kliammam 4. East Godavari 4. Krishna 5. West Godavari 5. Mahboob Nagar 6. Nellore 6. Nizamabad 7. Chittoor 7. Pralcasam 8. Karim Nagar 8. Rangarcddy 9. Warangal 10. Nalgonda 11. Medak 12. Kurnool 13. Anantapur 14. Guntur 15. Cuddapah
1.
2.
Karbi Anglong
Assam
3. Bihar 1. Patna 1. Gaya
2. Nawadah 2. Aurangabad 3. Pumea 3. Giridih 4. Siwan 4. Bhagalpur 5. Sitamarhi 5. Mongher 6. Darbhanga 6. Begusarai 7. Madhubani 7. Gopalganj 8. Katihar 8. Dumka (Santhal P) 9. Muzaffarpur 9. Nalanda 10. Rohtas 10. Hazaribagh 11. Singhbhum 11. West Champaran
55

S. Name of state/ Name of districts Name of districts No. UT with prevalence with prevalence
rate 10/1000 rate 5 to 9.9/ 1000 and above
1 2 3 4
4. Gujarat 1. Valsad
2. Surat 3. Dangs 4. Bharoch 5. Vadoclara 6. Panch Mahals
5. Karnataka 1. Raichur 1. Bellary
2. Bidar 2. Gulbarga 3. Mysore 4. Bijapur 5. Dharwar 6. Belgaum
6. Kerala 1. Kasargode 1. Trivandram
2. Palghat 2. Alleppey 3. Trichur 4. Malappuram 5. Kozhilcode 6. Cannanore 7. Quilon 8. Ernakulam
7. Madhya 1. Raigarh 1. Raipur
Pradesh 2. Rewa 3. Datia 4. Bilaspur 5. Barwani 6. Durg 7. Dhar 8. Bastar 9. Chhatarpur 10. Rajnandgaon 11. Gwalior 12. Ratlam 13. Chhindwara
56

Name of districts with prevalence rate 10/1000 and above
Name of districts with prevalence rate 5 to 9.9/ 1 000
1 2 3 4
14. Bhind
15. Khandwa (E.Nimar) 16. Shandol
8. Maharashtra '1. Greater Bombay 1. Thane
2. Wardha 2. Raigad 3. Latur 3. Satara 4. Gadchiroli 4. Sholapur 5. Nanded 5. Parbh ant 6. Osmanabad 6. Beed 7. Chandrapur 7. Akola 8. Arnravati 9. YeoUnal 10. Nagpur 11. Bhandara 12. Buldhana
9. Manipur 1. Bishanpur
2. Tamenglong 3. Tenganoupal
10. Nagaland 1 .
Mon 1. Tuensang
11. Orissa 1. Ganjam 1 . Keonjhar
2. Balasore 2. Koraput 3. Cu ttack 3. Kalahandi 4. Dhenlcanal 4 . Phulbani 5. Puri 5. Sundargarh 6. Mayurbhanj 7. Sambalpur 8. Balangir 12. Sikkim 1. East District 2. South District 3. North District 4. West District
57
S. Name of state/
No. UT

S. Name of state/ Name of districts Name of districts No. UT with prevalence with prevalence
rate 10/1000 rate 5 to 9.9/1000 and above
1 2 3 4
13. Tamil Nadu 1. Chingleput 1. Coimbatore
2. North Arcot 2. Tirunelveli 3. South Arcot 3. Kanyakurnari 4. Salem 5. Dharmapuri 6. Madurai 7. Tanj avur 8. Tiruch irapalli 9. Ramanathapu ram 10. Puddukotai 11. Periyar 12. Madras. 14. Tripura 1. North Tripura 2. South Tripura 15. Uttar 1. Hardoi 1. Rampur Pradesh 2. Pilibhit 2. Uttar Kashi 3. Sitapur 3. Azamgarh 4. Tehri 4. Basti 5. Faizabad 5. Badaun 6. Kanpur 6. Banda 7. Ballia 8. Barabank1 9. Bahraich 10. Bareilly 11. Etawa 12. Fatehpur 13. Ghazipur 14. Gonda 15. Gorakhpur 16. Hameerpur 17. Jalaun 18. Varanasi 19. Deoria 20. Rai Barelly 21. Shajahanpur
58

S. Name of state/ Name of districts Name of districts N o . J r with prevalence with prevalence
rate 10/1000 rate 5 to 9.9/ / 000 and above
1 2 3 4
22. 23. 24.
Unnao
Mirzapur
Lucknow
1 6 . West Bengal 1. Purulia 1. Howrah
2. Bankura 2. Hoogly 3. Midnapur 3. Malda 4. Birbhum 4. Coach Bihar 5. Burdwan 5. Murshidabad 6. Jalpaiguri 6. Nadia 7. West Dinajpur 7. 24 Praganas s. Darjeeling
9. Calcutta
17. Arunachal 1. Siang West
Pradesh 2. Tirap 3. Siang East
18. Goa, Daman 1. Goa
& Diu 2. Daman 3. Diu
19. Lakshadweep 1. Lakshadweep
20. Pondicherry 1. Pondicherry
2. Yenam
3. Karaikal
59

F . Leprosy and the Law
There are three pertinent observations that need to be made
,concerning the enactments affecting the leprosy afflicted in
various statute books across the country: —
(1) such legislation was devised at a time when there was no
known cure for leprosy and reflected concern for the welfare
of the 'healthy' majority. The assumption was that leprosy
was incurable, and that all affected persons spread the
disease.
(ii) with the medical advances made over the last three
decades, such enactments have lost their raison d'etre, and
(iii) until such times as these enactments are not repealed,
the movement for equal rights for the leprosy affected will
not come of age. Special legislation concerning the leprosy
affected will always put them into a category apart. These
observations are amplified briefly, in order not to be
repetitive.
Leprosy has been recognised over the centuries as an
affliction without cure, a disease which permitted the practice of
ostracism even within the parameters of the nuclea r and
extended families. In order to protect 'healthy' individuals and
the community, persons were separated, willingly or otherwise.
Ostracism was practised either in part or in whole. Relationships
were curtailed. The leprosy affected lost their right to participate in
social and religious functions, often immediately upon
recognition of the disease. The emotional divide was often in the
nature of the act of a guillotine. The cultural beliefs regarding the
disease coincided with the medical beliefs of the 18th and 19th
centuries, when there was no known scientific cure for leprosy.
Isolation was the only remedy that scientific opinion could
endorse as a means of protecting the interests of the 'healthy'
mass from those individuals unfortunate enough to have crossed
the line into a world subjected to the myths of traditional society.
60

Following shortly in the steps of the medical opinion of the time was the
law, which also stepped in to protect the interest of society as a whole
from its 'diseased minority. The law did at the time what the law was
expected to do-to safeguard and to protect. In so doing it could only echo
the medical opinion of the time, and to that extent it was 'scientific'.
What it also did, not surprisingly, was it endorsed the time worn
body of myth, superstition, prejudices and fears of the community at large.
A review of legislation concerning the leprosy affected reveals the
community view of the time, concealed in the clauses of various
enactments. It reflected, however inadvertently, the stigma perpetuated
by the body politic of the community. With the aim of protecting the
community at large, legislation contributed directly or indirectly to
the harassment faced by those unfortunate enough to be affected, by
giving legal sanctity to myth and superstition already buttressed by medical
opinion.
A number of countries passed legislation at the end of the 18th
century and in the early 19th century. They related to some form of
compulsory segregation, restrictions on use of transport and public
places and affected marriages , divorce and inheritance. In some
countries these enactments have since been revoked. In others, they
have not been formally repealed but are no longer vigorously implemented.
Similarly, a number of laws came to be enacted between 1898 and 1939
which put numerous restrictions on the physical movement of leprosy
patients and several legal impediments in social mobility as well.
Sadly, some enactments equated a leprosy affected individual's status
with that of a beggar and a- pauper and cast on him the overtones of
criminality, which made for a separate sub-culture.
N o r e s e a r c h h a s e v e n b e e n c o n d u c t e d t o s t u d y
comprehensively the gamut of Central and State legislation, to confront
discriminatory enactments and offending clauses with the scientific and
legal temper of the present day. Instead act upon discriminatory act has
been allowed to remain on the
61

statute book, cobwebbed perhaps by patchy applicability, but a blot
nevertheless on the painstaking advances made by the dedicated
band of scientists, leprologists, social workers and field specialists in
India, who have worked with what can only be described as
missionary zeal, to assist the affected to maintain and resume
'normal lives. It would be in the fitness of things if the Law
Commission might have such diverse legislation studied, so that a
logical first step could be taken to list such legislation that is now
anachronistic, and after, this necessary preliminary step, to plan for its
dismantling.
Some of the principal enactments on the statute book are: —
(1) The Indian Lepers Act 1898.
(2) The Hindu Marriage Act 1956.
(3) The Special Marriages Act, 1954
(4) The Muslim Marriages Act. 1939.
(5) The Indian Christian Marriage Act, 1872.
(6) The Indian Railway Act, 1890. (7) The
Motor Vehicles Act, 1979.
Apart Worn-these there are a number of other discriminatory areas
relating to elect ion rules , mil i tary service rules , employment and
reservation policies.
The Motor Vehicles Act of 1979 disqualifies a leprosy patient from
obtaining a licence to drive a vehicle, despite the fact that not all leprosy
patients have sensory loss of their limbs. Until very recently, life
insurance premiums were higher for the leprosy affected on the wholly
incorrect premise that the leprosy affected had shorter life spans. Military
service is not always open to the leprosy affected, even when the form of
leprosy is negative. Election booths in some places are separately
established for the leprosy affected, and sometimes manned by the
leprosy affected! Leprosy beggars are frequently transported in separate
municipal vehicles, lodged in leprosy homes apart
The expression "negative leprosy" has been used here as well as in other chapters to mean the non-infectious type of leprosy.
62

from other beggars, and some municipalities even separate them
In death by cremating them in separate crematoria.
The earliest legal enactment was the Indian Lepers Act of
1898. First enacted in Bengal, it was later made applicable to the
whole country. It is a federal law which was adopted by most of
the State Governments. Its underlying assumptions were that
leprosy was both an incurable disease, as well as a poverty-
related disease, for it reduced the leprosy affected to the status of a
pauper. To a considerable extent this Act endorsed the common
notion that leprosy was confined to the lowest economic strata.
This Act was largely employed for :--
(i) segregating beggars suffering from leprosy.
(ii) disallowing leprosy patients from preparation for sale, or
sale or handling of eatables, drinks, drugs, clothing etc.
(iii) forbidding leprosy patients from using public wells.
tanks, taps, etc. for purpose of bathing or washing.
(iv) restricting leprosy patients from working as barbers,
cooks, domestic servants etc.
(v) disallowing leprosy patients from using public
vehicles or transport. (vi) debarring leprosy patients from inheriting ancestral
properties.
The Act when it was passed could not have been expected
to make any distinction between infectious and non-infectious
types of leprosy. It was based on the premise that the leprosy
afflicted were afflicted for life. It is only against such a
background that one can hope to understand the rationale for
such stringent clauses as Sections 9 & 11. Section 9 of the Act
prohibits leprosy patients from preparing food and drinks or
even the sale of food, drinks or clothes, from using public wells,
dr iving or t ravel l ing in any publ ic conveyance or any
transportation which might affect public health. It provides
penalties which include cash fines and even imprisonme4 for
infringing any of its sections. Section 11 holds an employer
responsible for giving jobs to leprosy patients punishable by
63

Jaw. The Act provides for the establishment of segregation
camps for such patients as are found to be in notified areas.
The Indian Railways Act of 1890 bars the leprosy affected
from travelling by trains, regardless of infectivity. Similarly. the
various local self government enactments passed in the
nineteen thirties forbade entry of the leprosy affected from
public places and utilities with the emphasis on keeping urban
areas free of the disease. While the various marriage acts
provide legal cover for divorce on grounds of leprosy, (which was
confirmed by the Supreme Court in a case as late as 1973), in the vast
majority of cases, particularly in rural areas, the leprosy affected
spouse is merely "abandoned". Customary practice coming to the
fore, the abandoned half, more often than not the wife, is unable to
assert any legal right.
It was against these offending arid anachronistic clauses that
scientific and enlightened opinion began to protest, particularly against
the clauses equating leprosy with pauperism. The Fifth International
Congress of Leprosy in 1948 passed a unanimous resolution that the use
of term 'leper' be discarded, and the term 'leprosy patient' which was
much more in keeping with the dignity of human life, be employed
instead.
The Government of India constituted a Sub Committee of the
Leprosy Advisory Committee to advise on the modification of the
Lepers Act of 1898. The Committee expressed unanimously that
various clauses of the 1898 Act had been framed on the then existing
knowledge of leprosy. Moreover, the provision for its treatment and
control was dependent upon the means available at that time. Hence,
all those provisions that did not fit the then current requirement, could
no longer be considered valid in the light of the then knowledge
about the disease. However, the Committee advised that
infectious cases should be segregated from the non-infectious and
able bodied.
Even in Maharashtra, perhaps the most progressive State in the
battle against leprosy, it took more than three decades of
relentless effort before the offending portions could be
64

dismantled. The word 'pauper was deleted yet the word 'leper'
remained in title and substance. It was not until October 1,
1983 that the Act was finally repealed in Maharashtra. It was
repealed by the Central Government in its application to the
Union Territories three months later.
This is not to say that the Act has everywhere been repealed.
Only eight State Governments have additionally repealed the
Act. They are Maharashtra, Madhya Pradesh, Orissa, Arunachal
Pradesh, Tripura and Kerala, Mizoram and Tam il-Nadu.
Karnataka and Uttar Pradesh are likely to repeal it shortly.
There is no doubt that special legislation on leprosy has
helped to make leprosy a case apart . The World Health
Organisation would like to see leprosy treated by the law
makers, as by everyone else, as any other communicable
disease. Some people would prefer the legal scenario concerning
leprosy to remain stationary in the belief that the more the pot
is stirred, the more controversial the issue will become, leading
many of the leprosy affected to go "underground", thereby
retarding the rate of treatment and control.
There may be some validity in this point of view in the short run.
For the long run, however, it is necessary to amend or remove
such outmoded and clearly discriminatory legislation wherever it
exists in however effective or non-effective a form. It is equally
essential to provide for positive legislation to prevent 'dehabilitation'
and accelerate the process of rehabilitation. It is no longer enough,
if we intend to eradicate the problem in a decade, to do away
with negative legislation. Law is an important social
institution, and although it is from time to time overtaken by
traditional customs, belief and folklore, it does nevertheless
establish societal trends. To help break 4 centuries of stigma it is
essential as a first step to dismantle the old apparatus. Thereafter,
some degree of protection should be built in to accelerate the process
of rehabilitation.
65

G The Rehabilitation Factor in Leprosy in India
1. Rehabilitation Policy - the raison d'etre
Leprosy today is as much, if not more, a social problem, as it is
a medical problem. Unlike a host of other diseases where
suffering ends with the termination of the disease, the leprosy
affected suffer during and after their affliction. It is a moot
point whether the affected suffer more when the disease is in
progress or after the disease is arrested, because stigma
continues to operate and segregation continues to manifest itself
in a number of spheres in varying degree. It is this unique factor
that even after the leprosy affected are completely cured, they
may still be shunned by 'healthy' society, especially if they bear
any previous manifestation of the disease, such as apparent
deformity. Unable to retain or obtain employment, many
patients find no alternative to begging; unable to find shelter
even in urban ghettos, they have no recourse but to set up clusters
of their own. These account for the "free" leprosy colonies that
are spread unevenly through the rural and increasingly urban
kaleidoscope. Perhaps more than for other categories of the
handicapped (who are not ostracized), it has become imperative to
bring all aspects of the disease out into the open and to shape
Instruments of rehabilitation policy that must go hand in hand
at each stage with control policy, if we wish to see an end to the
disease in the reasonably foreseeable future. What is therefore
needed is an integrated approach to leprosy containment, which
must involve a nation-wide programme comprising detection,
t r e a t m e n t , ed u c a t i o n a s w e l l a s r e h ab i l i t a t i o n . T h e
rehabilitation component should involve new methods of
service delivery which should essentially be low-cost, able to
reach out to the maximum numbers within a given time frame
and, as far as possible, be community or domiciliary rather than
Institution-based.
There are two important concepts in rehabilitation. The first is
to understand and accept the need to help establish or re -
establish economic productivity. Marked as it frequently is by
66

loss of employment after the discovery of the disease, it becomes
very difficult for the patient to re-obtain employment whether
after infectivity or after the disease is 'arrested. Whereas many
'healthy persons find it hard to obtain employment, it is doubly
difficult for the handicapped and even more so for the leprosy
affected. Many have no alternative but to depend on charity.
Others are left with no recourse but to cross the last barrier of
human dignity and enter into the twilight world of begging or
Illegal activities such as illicit distillation, illicit trading or
smuggling.
The second is co-terminus with the first and lies in integrated
efforts to restore the 'dehabilitated' leprosy affected to his
family, or his community or to some form of domici liary
arrangement that might enable him, if not to be restored to his
roots, at least to be able to spring new ones. Social workers have
often come across cases where prolonged periods of separation
f rom the fami l y do no t l end themse lves eas i l y t o re -
attachments. Again, pressures on land and family holdings (all
too often in normal families as well) causes some family
members to relocate elsewhere, so it may not always be
necessary to ascribe the moving away from family land holdings
to st igma alone. Economic pressures together with the
fragmentation of land holdings are always at play, and should •
be taken into account in an overall policy statement.
Right, not charity, nor even compassion, must be the
hallmark of such a rehabilitation policy. Experience ha s
demonstrated time and again that the leprosy affected like other
handicapped or disadvantaged groups, are willing and able to
adapt old skills or learn new ones despite anesthetic limbs and
even deformity. Voluntary agencies the country over bear
witness to efforts which have successfully trained patients to
convert their disabilities into abilities. Employers have been
able to testify that most of the handicapped, including the
leprosy affected, work as hard if not harder than their 'normal'
employees. That stigma and misconceived beliefs should single
out the leprosy affected for a life time of disqualification should
not render a policy statement with any overtones of pity or
67

charity. It must instead recognize that in order to counter
misapprehension and myth, and at a stroke to remedy a
historical accumulation of discrimination. it is necessary to
enunciate a chapter that recognizes their ability to learn and to
adapt. This in order to contribute productively into the human
resources pool, and in so doing also provide momentum to the
national effort towards leprosy eradication in its most practical
sense.
It is then imperative to accept the definition of rehabilitation in
its fullest sense as going beyond economic productivity into
being re-assimilated in society. For this to happen we have no
alternative but to strengthen broad policy perspectives in which
rehabilitation must form an integral and not a peripheral part.
2. The parameters of the situation
It needs to be reiterated that there are no precise figures to go
by, but that approximations arrived at may not be considered
unreasonable. There is known to be a total estimated population
of 4.1 million leprosy affected in India. This figure may be
divided into two main categories which qualify for varying
degrees of rehabilitation services. The first are those who are
physically handicapped because of leprosy. It is accepted by the
Ministry of Health that 15% to 20% of the leprosy affected suffer
from disabil i t ies of one kind or another . This therefore
approximates figures ranging from 615,000 to 820,000 requiring
(and to an extent receiving) attention. The second category
comprises a less easily definable figure, that of the s ocio-
economically affected discussed below.
It is widely accepted by the Ministry of Health and eminent
leprologists and social scientists working in the field, that as
many as 90% of the affected are now living within their own
milieu. That would leave an estimated 10% who continue to
remain displaced, giving a tentative figure of 410,000 who are in
need of medical care and some degree of rehabilitation services.
This estimate may be considered to be on the high side, but in the
absence of any national sample survey it may be best to err on
the high side while planning integrated delivery services. This
68

estimate would comprise a number of broad categories of the affected including (a) those living in institutions of varying kinds, (b) inmates of "free" colonies (c) the leprosy affected beggar population, and (d) those who may have congregated singly or en-famille to live under the broad aegis of a specialised leprosy institution, hospital or rehabilitation centre, and may have been assisted to rebuild their lives under some community-based domic i l i a r y s chem e . No t a l l h owev er wou ld r equ i re rehabilitation services or even welcome them. It would be unreasonable to expect persons who have crossed working age to be drawn into any such scheme. Major deformity, serious orthopaedic handicap or visual deformity may also preclude serious consideration, and such persons would perhaps require shelter not rehabilitation. Leprosy affected beggars are also a category that are difficult to rehabilitate. Having once crossed a certain psychological human barrier, they are unlikely to wish to give up earning perhaps Rs. 20 or more a day in comparative freedom, to enter a situation where they may be bound to a regimen that might pay them considerably less for a full working day, This is not to say that this category should not be rehabilitated. It may be said about leprosy beggars that being perhaps the hardest to rehabilitate, scarce resources should be concentrated on such other categories as may welcome rehabilitation efforts and join in them as willing partners. This view may certainly reflect a measure of truth. However, the argument in favour of rehabilitation measures for this group is that community stigma levels rise highest on the sight of beggars bearing deformity, often causing burnt out non-infectious cases to be treated as infectious ones. Ideally the aim should be to prevent adding to the leprosy affected beggar problem by timely application of rehabilitation delivery services at earlier stages. It may also be useful to take into the policy framework two other categories of persons - viz - (e) patients undergoing treatment in control clinics who may yet be living at home, but who may have been d i sp l aced f rom thei r work s i t uat ion and ( I) t he undetermined number of persons in an intermediate zone who have not yet begun treatment and have yet not been forced out of employment. It might then be realistic to consider in this category a figure between 200,000 to 300,000, out of 410,000
69

affected persons who might hope to benefit from rehabilitation
services.
Combined with the leprosy affected physically handicapped,
the total population of both categories might vary from 815.000
to 1.120,000. There have already been established under the
National Leprosy Eradication Programme, centres for the
prevention and correction of physical deformities and the
fitting of prosthetic and protective appliances, to render patients
now able to benefit from the available package of services.
Several voluntary organisations are also providing correctional
services, and several too are duly recognized by Government,
and have their delivery costs reimbursed.
In the total context these figures should not be considered
Insurmountable. With determination and a comprehensive
policy and delivery package that closely integrates both
Government and voluntary effort and resources, it would be
possible to phase out the problem, without duplication of scarce
inputs, within a foreseeable span.
3 The prevention of "dehabilitation"
The term "dehabilitation" is etymologically incorrect but has
been succinctly described as a downgrading process which leads
to almost total disability from the socio-economic standpoint.
Because the problem in terms of numbers as well aS the
Indices of human misery is already large, the primary step in
the total package of rehabilitation services is to prevent further
"dehabilitation". Measures taken to contain the problem in its
early stages are easier to devise and implement, and given the
size of the situation, it is the only cost-effective method that is
available.
If the prevention of edehabilitation' is not treated as a major
instrument of rehabilitation policy, then on present estimates a
significant segment of persons will be displaced annually, to be
70

dispersed between peripatetic employment, movement into
"free" colonies and leprosy institutions, and begging.
Institutionalisation of the entire leprosy affected population is
patently impossible. Apart from the heavy financial burden
Involved, institutions have negative features that go alongside
their positive ones, not least of which is that institutions cannot
provide those important psychological inputs that the patient
can receive while living with his own family while obtaining
medical attention.
The rehabilitation of the leprosy affected beggar is perhaps
the most difficult of tasks. An interesting distinction has been
made between two categories of beggars* - the compulsive beggar
who himself rejects society, and a second category that has been
rejected by society. At this point let it suffice to say that once an
Individual who has been "dehabilitated" crosses the threshold
Into begging, it is not easy to bring him back, and the effort that must
be put into reclamation is many times more than it would have
taken to prevent his leaving society in the first place.
"Free" leprosy colonies too , are a mani fes ta t ion of
"dehabilitation". Everyone seems to be agreed that "free"
colonies should be "phased out". However, the larger cities in
particular face chronic housing shortages. The leprosy affected,
once they are displaced from their (often rural) communities,
have little choice but to settle in their own clusters or colonies.
This is chiefly because, as is well known, dwellers of 'healthy'
slum tenements do not easily permit entry to the leprosy
affected. As there is frequently no alternative means available
to this unfortunate segment. it is necessary to take this factor
into consideration in an overall policy framework.
"Dehabilitation" owes itself to a number of different causes
which vary in intensity depending on a number of regional and
local factors. In major measure this has been due to the
intractability of existing entrenched attitudes that result in
varying degrees of stigma. An important contributory factor in
* Dr. E.P. Fritschi "Surgical Reconstruction and Rehabilitation in Leprosy".
71

the past has ironically enough been the attitude of the medical
profession, although there is reason to believe that there has
been improvement in this area since the recommendations of
the Swaminathan Committee were accepted. Finally, the
current regulations pertaining to fitness certificates has also
Inadvertently led to the accentuation of problems of "dehabilitation".
It could well be argued that remedial action is being
simultaneously undertaken What is needed, however, is a
coordinated preventive campaign that is defined and recognised
as such, with interwoven strands complementing one another.
without being taken on an individual piece meal basis. Such a
policy package would go a long way in preventing "dehabil -
itation", in itself the first step of a rehabilitation policy. The
components of such an integrated package are listed below and
are discussed in some detail.
(1) Survey. Education and Treatment, particularly in
endemic areas, with due emphasis on public health
measures.
(2) closer involvement of the medical community.
(3) changing of fitness regulations.
(4) physiotherapeutic and surgical facilities for the
prevention and timely correction of deformities.
(i) Survey, Education and Treatment (SET)
The experiences of a number of countries have demonstrated
that whenever the SET Programme has been introduced, the
incidence of disability and deformity have been reduced
commensurate with the degree of programme development.
There is no doubt that this has proved to be a much more cost-
effective scheme, both in terms of the considerably lower per
capita cost per patient vis-avis institutionalisation, as well as in
terms of efficacy. In India, the Gandhi Memorial Leprosy
Foundat ion was a pioneer in th i s impor tan t area . The
Government of India appointed an Expert Committee in 1954
72

which adopted this model and developed it into the National Leprosy Control Programme (NLCP) in 1955.
Surveys are not conducted without attendant difficulties. It has been found that surveys often work less well in the urban situation, owing to the possible economic "dehabilitation" of infectious patients who are likely to be brought to light through surveys.* Nonetheless it is a well accepted fact that case detection, particularly in areas of high endemicity must rest primarily on population surveys.
On a rule of thumb basis, experienced leprologists are of the opinion that at least 25% of para-medical workers develop a deep sense of commitment to the cause of leprosy eradication, and this goes well beyond factors of their status and remunerative package. There is something about leprosy which, while it causes most workers to either work routinely or even apathetically, has the reverse effect on a not insignificant percentage of others. It is difficult to assess at the point of recruitment who is likely to develop in which direction, but one area of possible future recruitment in this field could well be the healthy offspring of the leprosy affected. This might mean that minimum educational qualifications might have to be relaxed to facilitate their recruitment, which could be considered. This would have a dual advantage. It might provide an understanding cadre of para medical workers; it would also give the healthy offspring an opportunity to break into the employment market with a considerable degree of security, which they are unlikely to have enjoyed in their early lives.
(ii) Education
Education is the principal long term means of preventing "dehabilitation". Twin questions arise - whom to educate and how is this best achieved at minimal cost.
There is little doubt that it is essential to combat the widespread body of myth and ignorance, which applies as much to the incipient patient, as it does to general community
* Discussions with Dr. M.S. Nilakantha Rao.
73

attitudes. With the former as a target, it is incumbent on policy
planners to break the vicious circle of late diagnosis and delayed
treatment, by teaching the incipient patient to recognize the
early signs of the disease, to understand that at the earlie st
stages, damage to peripheral nerves can be prevented and
disability entirely avoided by taking timely treatment. As part
of a daily public health campaign, the scientific facts about the
disease need to be succinctly conveyed. An important but not
cogently recognized factor, (but one that became apparent after
talking to a number of patients), is the need for such educational
campaigns to indicate precisely where the incipient patient or
person in doubt can go to for advice, reassurance or treatment.
Such programmes need to be suited to regional and local needs.
They would help in the prevention of the concealment of cases
and in taking timely treatment.
With the community as a target, the orientation of education
must change. It is vital to bring the stientific facts about the
disease out into the open. The new chemotherapy used in
treatment, which is not even particularly well known to many
members of the medical community let alone lay persons, must
be understood at least to the extent that infectivity can be curbed
within a matter of weeks by the administration of multi -drug
regimen. The age-old superstitions which are an important
ingredient of stigma, need to be attacked continuously by a
number of selected means.
Community attitudes develop early, for which reason it is
most important to introduce a few basic facts about disease and
treatment into school curricula. A few paragraphs about the
causation and cure by multi drug therapy, placed in science and
other lessons in secondary schools would educat e whole
generations to grow up with a proper understanding. It would
decisively lower stigma levels in society. It would also be useful
to draw on local community leaders, school teachers and
religious leaders to simultaneously assist both patients and
members of the community into developing more rational
attitudes. It is an alarming fact that there is surprisingly little
difference between the attitude of more educated and less
74

educated people on this subject. Indeed it is probably true to say
that the attitudes of people living in highly endemic tural areas is
perhaps more tolerant than that of urban conglomerations.
Even in urban areas, there is often less tolerance at the more
educated end of the spectrum.
From the point of preventing "dehabilitation", two specific
groups that need to be addressed are employers and trade unions.
Both groups reflect the common social misapprehensions
towards the disease. However, both groups play crucial roles
regarding employment and job retention. It is only to be
expected that if patients are denied the opportunity of economic
participation, or are driven out of employment, it contributes to
creating a parasitic class. Alternatively the leprosy affected are
driven to illegal or antisocial activity, sometimes carried out
with impunity in "free colonies" where even the law enforcement
agencies choose to ignore for fear of infection. The importance
of the role of the trade unions and employers organisations is
a m p l i f i e d l a t e r i n t h e t e x t a n d f o r m s a n i m p o r t a n t
recommendation.
Sometimes where an understanding management may be
willing to consider taking back a cured patient, trade unions
have been known to oppose the move and vice versa. Because
both managements and unions have a crucial role in the area of
employment, it would certainly help if the integrated education
campaign aims to educate these important groups through a
special educational programme designed for trade union
leadership and employers organisations.
(iii) Education by Demonstration
Community attitudes are shaped in little or greater degree by
the demonstration effect, especially where the example is set by
persons whom the public at large respects.
Sadly, there have been only a handful of pace setters in this
area. Father Damien who chose to live with leprosy patients on
the island of Molokai well before the advent of anti-leprosy
75

drugs, Roul Follereau, a French journalist, who after meeting by
chance a group of leprosy patients in Africa and seeing their
appalling living conditions, dedicated his life to awakening
public consciousness around the world, are the classic examples.
Gandhiji nursed a leprosy patient in his Sewagram Ashram,
and by this one deed inspired a number of voluntary agencies in
India to take to the field.* Demonstration, however, does not
necessari ly mean a l ifetime of dedication. When Queen
Elizabeth II of England visited Vellore in the 1960's she made it a
point to shake the hand of a leprosy patient, which gesture did not
pass unnoticed. If prominent persons in our society - judges and
journalists, administrators arid academics, politicians and
professionals were to understand that leprosy is not contagious
and were to shake a deformed hand, that in itself would go a long
way in convincing others that leprosy too is an "acceptable"
disease.
(iv) The Attitude of the Medical Community
It is ironic that the attitude of the medical profession as a
whole to the subject of leprosy should be a subject of concern.
Even six years after the submission of the Swaminathan
Committee Report, the attitude of the medical profession
remains apathetic. The Committee's findings, briefly were as
follows:
"Unless medical students are made to learn leprosy as part of
their curriculum, by including compulsory questions on leprosy
In their examination, inadequate interest in leprosy work
among doctors in service, and general medical practitioners will
continue .. . . . , the recommendations of the Mukhopadhaya
Committee of the Medical Council of India on teaching of
leprosy to undergraduate medical students be immediately
implemented."
* The selfless service of Baba Amte for the leprosy stri cken is well known throughout India. The dedication of Mother Teresa and her Missionaries of Charity in the cause of the destitute, and for the leprosy afflicted in particular, has been acclaimed the world over.
76

This is not to say that there has not been some improvement.
The Medical Council of India has issued instructions on the
teaching of the subject and has encouraged leprologists to deliver
lectures in medical colleges. However, leprosy continues to be a
low priority area and medical students continue to confer their,
priorities on the socially more 'fashionable' or 'acceptable'
diseases. It is also not entirely their fault, because leprosy as a
subject continues to be inadequately taught. The result
sometimes is that medical practitioners fail to recognize the
early clinical manifestations of the disease. It is quite usual in
city hospitals for the doctors not to wish to treat the leprosy
affected, and to refer them to leprosy centres instead. This may
in some measure be the doctors own reluctance, or it may be
because 'normal' patients are offended and in some measures it
continues to be because doctors have been inadequately trained
to treat the disease. It is this aspect that first needs to be
addressed.
The reasons are not far to seek. The subject matter relating to
the disease taught for the M.B.B.S. examination, is at best taught
inadequately; because there is no particular emphasis in its
teaching, there is a corresponding low priority in its learning.
Greater attention needs to be paid to the curricula in medical
schools, schools of nursing as well as to the training of
paramedical and other health staff. Wherever possible, orienta-
tion and refresher courses should be conducted.
The dispari t y between th e direct ives of the Central
Government and that of one of the otherwise most progressive
State Governments viz. Maharashtra, may be seen in the fact that
whereas the Central.Government Directive No. 1700/1/1974
of 5/4/1974 provides that an employee may be permitted
to resume duty provided he has remained bacteriologically
negative for three consecutive examinations carried out at
monthly in tervals af ter an in i t i a l negat ive s tage , the
Maharashtra Government requires negativity for no less than
twelve months. Meanwhile, the time period required to reach
negativity under dapsone rnonotherapy is lengthy in itself. In
77

places where monotherapy is being administered it can range
from three to five years: where the multi-drug regimen has been
launched the duration is considerably less, but these districts
are still comparatively few in number. In effect, affected persons
in employment are unable to resume duty till their skin smears
show constant negativity for upto one year after they reach the
threshold of initial bacterial negativity.
Instead, it makes more sense to take into account the factor
of the patients' morphological index, coupled with the basic
requirement of non-infectivity. A complete absence of germs
should not be considered any longer necessary especially, as in
smear positive cases, there is no longer any danger of infectivity,
especially if treatment is being taken with regularity. "If a
leprosy patient is taking treatment regularly, the chances of
anyone corning into contact with the patient 3-6 months after
the commencement of treatment is most unlikely to contract
the disease." *
In a depressed economy with high unemployment arid under
employment, where the handicapped are unable to compete with
the able-bodied, it makes no sense to expel or repel those
affected. What makes sense is to provide leave and encourage
treatment until infectivity Is eliminated and then permit the
patient to resume his work activity. This gives the employer a
much better chance of ensuring regularity of treatment, and
indeed provides a greater impetus to the patient to do the same.
Such a worker would in all probability be discharging non-
viable bacilli. In the present-day scenario, however, there is
every likelihood that the patient might wish to suppress his
discovery and may wander from pillar to post to find alternative
employment (in the event of his affliction coming out into the
open at his current work place), all the while placing his
colleagues at greater risk than would otherwise be the case.
It is, therefore, important to create a climate where fear is
lessened, and where the nature of the disease can be known. If
• Dr. M.S. Nilakanta Rao - Newsletter, National Leprosy Organisation, Vol. III No. 1, P. 6 (1974).
78

the disease is non-infectious the patient should be encouraged by
his employer to continue in his job while taking treatment. If he is
infectious he can be provided leave of absence or alternative
employment until negativity is el iminated. In a survey
conducted by the Ackworth Leprosy Hospital in Bombay*
between 1965-1970, it was found that out of 770 patients (of
whom 30.6% belonged to the smear - positive group) 29.4% only
resumed work after varying periods of treatment. Interestingly
enough, most of these were railway employees, who benefited
from the facility of free travel to clinics for follow-up.
* Dr. R. Ganapati , "Dehabil i tat ion of smcar — posi t ive leprosy patients: Experience in an Urban Centre". "Vocational rehabilitation of leprosy patients". Report on the ILO/DANIDA Asian Seminar .Geneva, 1982.
79

(iv) Reconstructive Surgery
Physiotherapy, reconstructive surgery, the provision of
protective footwear for ulcers, the case of insensitive hands and
feet are each concurrent parts of any leprosy rehabilitation
programme. This is an important aspect that is involved in the
prevention of "dehabilitation". Even where deformity has been
allowed to occur, its timely correction by reconstructive surgery
does prevent displacement from employment and community
life, especially in cases where patients themselves are motivated to
present a pleasant appearance, as for example reconstruction of
flattened noses, or replacement of eyebrows, or a desire to learn
new skills or retain existing ones.
Reconstructive surgery however should aim to be practical
and relevant to the attitude and work of a patient. It should be an
ancillary to rehabilitation and not become an end in itself. •
Care needs to be taken that this treatment is not so prolonged
that it serves to displace the patient altogether, for which reason
the periods of hospitalisation should, whenever possible, be
timed to coincide with seasonal unemployment or periods of
leave or holiday.
Surger y a lone cannot br ing about soc io -economic
rehabili tation, which needs vocational training, and an ancillary resettlement package. That it can and does play and - important role both functionally and in terms of community "acceptance" is understood. However, it must consciously be related to vocational rehabilitation. Dr. J. M. Mehta ** a renowned reconstructive surgeon, writi ng from his own experience as Honorary President of the Poona district Leprosy Committee (PDLC) had this to say:
"Starting as a reconstructive surgeon my original interest
was in the correction of the various deformities caused by
• Dr. EP Fritschi "Surgical Reconstruction and Rehabilitation in Leprosy"
•• Dr. J. M. Mehta "Social and Vocational Rehablitation of Leprosy Patients". Leprosy Research-Rehabilitation, social Medical"
80

leprosy. After this initial enthusiasm, I felt rather shaken when I
found that patients who were so operated on and who now had
good functional hands could not find employment because of the
leprosy stigma resulting in their total "dehabilitation" to a state
of penury and begging". While the PDLC has since come a long
way in terms of providing rehabilitation delivery services, the
proposition essentially continues to remain valid.
4. The role of institutions in rehabilitation
It is helpful to establish the distinction between traditional
leprosariums, rehabilitation centres and residual care homes.
When the only known "treatment" for leprosy was to isolate its
patients, the leprosarium was the institution where patients were
admitted for treatment and care. These were usually as far
isolated from the city, town or community as was possible.
Patients were provided with some form of activity suitable to the
advance of the disease, and in turn were provided with
maintenance. Their discharge depended on their cure, or if some
alternative rehabilitation became available. A rehabilitation
centre is an institution for the temporary housing of a disabled
person, where the patient or ex-patient can undergo training
or any other preparation for his or her ultimate return to society
as a self-supporting member of the community. The residual care
home, as the term implies involves primarily care, not
rehabilitation. It is the "substitute family" the patient does not
have. This is not to say that such homes do not provide activity.
Light occupations to keep idleness at bay are provided. "It must be
remembered that such patients have usually had more than their
share of suffering in life. They have experienced rejection, they
have known what it is to be unwanted, they have hungered and
thirsted physically as well as emotionally. The home should
offer to them not merely food and shelter, but a place where they
can, in the-eventide of their troubled life experience ....... peace at
last"*. There is a case for residual care homes and there is a small
percentage of ex-patients frequently with disability, who are
* Dr.EP Fritschi "Surgical Reconstruction and Rehabilitation in Leprosy"
81

destitute. Certain criteria are usually followed in making such
admissions. These include a high degree of disability, no known
relative, no shelter of their own and no or practically no source of
income. There are in-built difficulties in the administration of several
such homes. By definition such residual homes impose an unfamiliar
situation on frequently elderly and handicapped persons with
problems of personality interactions. They also call for a particularly
intense devotion and a special grace. There is sometimes a high
capital investment that is also involved. Not infrequently, they
function in isolation. and cut off the inmates both emotionally and
psychologically from the community. Residual care homes are
institutions of the last resort, for advanced patients who can no longer
hope to be independently productive.
Rehabilitation centres should first aim to prevent
dehabilitation, and encourage self employment schemes, or
community-based projects involving a low capital base wherever
possible. Experience has also long since reflected that such
institutions should avoid segregating of the leprosy affected, both for
treatment and in-house rehabilitation. Judicious combinations of the
leprosy affected with other sick and disabled, helps to break down
barriers of stigma. The repeated tragedy of several institutions lies in
the inability of the inmates to face the market place or community,
after getting used to the institution that has segregated then from the
every day world outside it. Compassion and charity make the inmate
welfare- conscious and reduces his independence.
Some rehabilitation institutions provide medical facilities together
with work opportunities, and although their inmates live in small
cottages within the confines of the institution, they are sometimes
reduced to a work camp. This is still a half way house situation, in that
it does not train the inmate to live outside the commune. In some
situations the leprosy affected_ who may have become alcoholics,
provide a greater dimension of difficulty in rehabilitation. In such cases
group rehabilitation methods have been tried with some success and
have provided an
82

answer for unskilled patients with limited capabilities, or where
physical disabilities ha 'e necessitated a division of labour.
Reconstructive surgery is available in a growing number of
insti tutions. Its appl ication must stem from a felt need.
Reconstructive surgery is an ancillary to rehabilitation and
should not become an end in itself. It requires to be practical and
relevant to the work that the patient wishes to perform. Under
the Sixth Plan, the N.L.E.P. has established four leprosy
rehabilitation promotion units on a trial basis, which includes
the prevention and correction of physical deformities and the
application of prostethetic appliances as well as protective
devices, so that the patient is better able to benefit from the
rehabilitation services available. For them to embark on the
road to reconstructive surgery, and have the road come to a
sudden end, is a doubly frustrating experience.
There are a number of institutions in the country, some run
by Central or State Governments, others by voluntary agencies,
each providing a range of services with differing emphasis, each a
product of their own innovation and environment. Sheltered
mixed employment, where it has grown, promises hope and a
balance between normal work culture which sometimes assists
in breaking barriers of isolation.
Outside the aegis of the traditional institution several
agencies have developed forms of domiciliary rehabilitation of
leprosy patients in surroundings familiar to them and as far as
possible without disturbing their own environment. They are
assisted to re-activate traditional-occupations, or start fresh
ones. They are assisted with bank loans, helped in obtaining
academic places or courses and assisted in their settlement
according to felt needs, capacities and at titudes. Continuous
follow-up is needed to develop and strengthen the relationship
between social worker anti patient.
5. The role of the voluntary sector in rehabilitation
It is everywhere acknowledged that the voluntary sector has
played a pioneering role in planning and developing rehabili-
tation programmes for the leprosy affected. In view of the high
83

cost involved in terms of time, patience and devotion, as well as the
need to provide multi faceted services - medical, sociological and
psychological - often over long periods, the voluntary sector must
continue to remain the principal pillar of support, and must in turn
continue to be strengthened in every way. For leprosy, because of the
prevailing high levels of stigma operating in society - is not everyone's cup
of tea. and even staunch social w o r k e rs b au l k a t t h e p r os pec t o f
en t e r in g t h i s f i e l d . Administrative impulses cannot be expected to
be very different from societal reaction, and therefore those who are
already working in this field or wish to do so, must be encouraged.
Voluntary effort in leprosy in India has always been
commended not least by the Government itself. The relationship with
Government has become somewhat more secure over the last few
years. There is now an annual dialogue in the shape of a meeting of
voluntary organisations engaged in leprosy work covered by the
Ministry of Health. This relationship between the voluntary agencies
and the Ministry is sometimes uneasy with arguments that can be
adduced on either side. The problems usually relate to financial support.
The voluntary organisations are quite often original and creative in their
line of thinking and approach; indeed the S.E.T. model was itself
devised by the G.M.L.F. to be later adopted by the Government.
Voluntary agencies also have a more flexible administrative structure,
and make for more sustained community participati on in their
specific spheres of activity and limited geographical areas.
However, they are not without weaknesses which include
differing perspectives and priorities of work, not especially
attractive service conditions for their workers, and of course the -seemingly
constant problem of financial constraints. This problem also
arises between donors and agencies in that resources are
sometimes raised for a particular purpose, but may be spent in other
areas, often equally deserving, but which then lead to accounting and
administrative difficulties.
There are other problems too. A major difficulty is the lack of
any meaningful coordination between the voluntary agencies
84

themselves, with the result that there is some duplication of
resources. More significantly, the innovative work of voluntary
organisations. and the developing results thereof are not
properly documented. It is sometimes the case that voluntary organisations
located not far from one another are hampered by their own
constraints of time and resources from engaging in meaningful
dialogues with one another. With rising salaries in the open market,
there is the problem of adequately trained manpower, which is
not attracted to comparatively lower salaries, and those too in an
area which is not viewed too highly on the employment spect rum.
It therefore has become increasingly difficult to establish
cost-effective projects especially with salaries and mounting
administrative costs eating into project funding.
Having said this, the role of the voluntary sector in the area of
rehabilitation has been, and indeed continues to remain
pioneering, because there is no substitute for a pioneering sense of
commitment. National as well as international voluntary
organisations provide a very wide matrix of services, and in view of
the 'high costs involved, it is important that they should continue to
receive a broad spectrum of support from the Government.
The relationship between the voluntary sector taken as a whole
and Government is not always an easy one, although there are some
splendid examples of cooperation. Much has been and continues to be said
on the subject, but it may broadly be stated that there are limitations
on both sides, and not to understand them does not in the final
analysis help matters. It is necessary for voluntary agencies to understand
the broad financial and administrative rules that govern the dispersal of
grants-in-aid, and perhaps it would assist if such rules are explained
to the voluntary agencies. Indeed, by and large, administrative details
and financial statements are not always the forte of the
voluntary agencies, and nor are many of them able to afford even a small
administrative apparatus. However, my understanding of the situation
is that if a cell in the concerned Ministry or State
85

Government could be set up to assist voluntary agencies to
understand and comply with the financial rules of Government,
especially accounting procedures and the time frame involved.
many of the existing irritants could be ironed out. This is
necessary because unless the role of the voluntary sector in the
field of rehabil i tat ion is not enlarged and strengthened,
rehabilitation will continue to lag behind the medical control
aspects of leprosy eradication.
Voluntary agencies have diversified into a number of facets of
rehabilitating the leprosy affected. These include the fitting of
prosthetic appliances and the correction of deformities,
vocat ional t ra ining programmes , rura l and agro -based
occupational programmes, self employment schemes, assistance in
the ob ta in ing o f bank loans , p rovis ion of footwear
appliances, sponsorship programme for children, and progr -
ammes for the healthy children of the leprosy affected, and
others besides. The areas covered by the voluntary sector now
Include centres for reconstructive surgery, training centres, craft
training institutes, sheltered workshops, counselling services,
placement services and so on. Most agencies have and continue
to achieve quantitatively significant results, but financial
constraints cause most of them to be selective in their choice of
objectives. With the total problem being as large as it is, and
voluntary agencies largely working on slim budgets, the answer
must lie closer to developing cost-effective, community-based
projects, with a small training span and relatively quick results. I
have come across attempts made to compare projects in the
voluntary sector with those of Government run projects. Such
comparisons serve no useful purpose. In this area of service,
wherever rehabi l i t a t ion schemes ex is t , they should be
strengthened. Effective linkages should be developed, duplication
of resources avoided, and innovative projects should be
encouraged. Better coordination is also called for between
voluntary agencies working in leprosy with other sectors of
disability and rehabilitation. A movement away from this
vertical approach is beginning to take place.
86

Among State governments, Maharashtra has itself played a
pioneering role, having long ago realized that it is the voluntary
sector that can more effectively tackle the problem of leprosy
rehabilitation. The Government provides financial assistance in
the form of grants in aid. The present rate is Rs. 95 per patient.
Goods produced by institutions such as bandages, gauze etc. are
purchased by all Government hospitals, and price preference is
given to them.
The attitude of employers is usually no different f rom the
general social attitude, with the additional thrust that employer
objectives being profit oriented, they are usually unlikely to
embark on a venture that may place profitability at risk.
Another consideration is the belief that they may put other
workers at 'risk' or otherwise antagonise them, especially when
there is high unemployment. The attitude of workers and trade-
unions towards an affected fellow worker is also much the same,
and there are far too many cases where ex-leprosy patients have
been thrown out of ( temporary) employment , o r where
permanent employees (as in Government) who were patients, find
themselves isolated at work, with colleagues refusing to share
their food with them, or otherwise reflecting hostility.
The elimination of leprosy by the concerted and twin efforts
of health care and rehabilitation are doubtful in the foreseeable
future without major contributions from the voluntary sector.
The recent past has witnessed the evolution of the role of the
voluntary agencies from the care of the disabled and social
support system, to the establishment of more comprehensive
projects involving health educat ion aids , rehabi l i tat ion
measures and promotion of the cause of leprosy alleviation at
decision making levels.- With all their disabilities (differing
priorities and perspectives, resources problems etc), the
voluntary sector has sustained contact through community
participation often in a limited geographical area of operation,
with the advantages of their more flexible administrativ e
structures and better inter personal relationships. One draw
87

back in their functioning is perhaps the paucity of participation by
the afflicted or ex-patients themselves.
6. Rehabilitation measures in 'free' or self-settled colonies
There are said to be some 300 'free' colonies of the leprosy
affected in the country, with an estimated population of 30,000
upwards. However, in the absence of any national survey, the
figures cannot be relied upon to any great degree. The fact
remains that there are a sufficient number of such clusters.
established by the leprosy affected themselves, to warrant serious
attention in terms of the provision of public health services,
vocational training and rehabilitation.
The clusters, large and small, have grown in numbers because of
an array of sociological and economic factors, not least
amongst which, in the case of those in the metropolitan and
other urban areas, is the magnetism of the cities. This is despite the
housing shortages which the leprosy-affected encounter in an even
more pronounced degree than 'healthy' destitutes. Not always
able find a place in leprosy institutions, clusters of the leprosy
affected usually come up near leprosy hospitals or treatment
centres. A contributory factor is that as urban slum colonies do
not welcome them, prevailing stigma pushes them into clusters of
their own.
In one sense this phenomenon should not be unwelcome
because it makes the task of identification and subsequent
ameliorative action easier. This is not to say that such colonies are
to be encouraged: it is merely a recognition of an existing fact.
Because such clusters do exist, it is essential to single them out for
special treatment including general health measures, leprosy control
measures, and rehabilitation services.
Certain steps need to be initiated in these colonies. In order
that public hygiene be introduced, which would help raise
general health standards, these colonies should be given priority for
their regularisation. Civic amenities such as provision of
88

clean drinking water, electricity and other facilities extended by
slum departments would improve sanitation and general health
especially of children. Outpatient clinics are needed in the larger
of such colonies. They should provide general medical facilities,
which would include first aid and family planning services
Wherever possible The healthy children of leprosy patients, arid
child patients should get the benefit of the Integrated Child
Development Scheme (ICDS). The district or zonal education
officer should ensure that healthy children, and those child
patients no longer infectious, are not refused school admissions.
7. The role of mass communication
Before any mass communication or major media effort is
launched, it is important to ensure infras truclural arrange-
ments, for it is to be expected that demands would be generated
with higher levels of public awareness, and these should be
catered for, particularly in terms of availability of drugs and
trained manpower to administer them. Without such ground
level arrangements, a major media programme would probably
be counter-productive.
There is no other means of "attacking" the centuries of stigma
that has flowed from one generation to another, in a compara-
tively short span of time, without creating the correct media
mix, adequate softwear, as well as without setting up proper
institutions down to the district levels, particularly in the
districts where the multi drug regimens have been introduced.
Three approaches should be adequate to start with. The first is
the more generalist approach which should be applied to
tackling the body of superstition and myth that have grown over
the centuries. It is necessary to explain precisely what leprosy is,
and what leprosy is not, as well as facts about its infectivity and
curability. These should be presented by the media in the
course of features on public health. Into this category may also
be placed items of important and real demonstrative value that
may swing public opinion away from its fear and consequent
89

stigmatising attitude. This approach would help to develop
positive attitudes and practices, and assist In raising tolerance
levels. The second approach should aim to enlist more active
participation from the vocal cross section of people including
school children, their leaders, youth organizations, volunteer
groups. university students and so on, but before this should be
done, a blue print would need to be prepared to channelise the
effort that is volunteered. Finally, a media mix should be devised
especially for the MDT districts, using regional and local
languages. According to the endemnicily of the districts, this
should aim to serve the twin purposes of health education, and to
disseminate specific information regarding leprosy control and
rehabilitation centres, available in each MDT district. Messages
need to be directed towards society at large (about the basic
misapprehensions about leprosy), to the patient himself (on
facilities being offered and where) as well as to non-patients
(family, friends, employers and co-workers), so that each group
may develop a positive attitude. The media mix would vary
between the rural and urban matrix. The relative usage of the
press, radio, television and cinema-would also need to be
evaluated by experts in the field.
8. An assessment of the proposed rehabilitation strategy
The emphasis hitherto has been on control measures, under-
standable in the context of the large accumulated pool of
infectivity, the length of sulphone treatment and its side effects
in a proportion of cases. Understandable, too, is the fact that the
leprosy strategy has, for a number of reasons already discussed,
developed unevenly. The voluntary sector has however,
convincingly demonstrated over the last decade and more the
efficacy of interweaving control measures with rehabilitation.
Voluntary insti tutions had realised that the only way to
overcome the dimension of social stigma and the patients' own
sense of failure and mental depression, was to equip them for a
job - to assist them in either obtaining one, or help them obtain
loans towards self employment and self sufficiency. Their efforts
have included the provision of optimum nutrition wherever
90

possible, as well as care for the healthy offspring of patients and ex-
patients.
The Swaminathan Report in 1982 firmly recommended that
rehabilitation should become an integral part of leprosy control. The
Committee fell that rehabilitation facilities be augmented or created
for all categories of the handicapped, including cured as well as non-
infective patients. They also recommended a joint action plan to be
undertaken by the Ministries of Health, Social Welfare. Education.
Labour and Employment and others, with the Ministry of Health
acting as the nodal Ministry. The underlying belief was that a
practical programme should emerge and that the benefits should be
reaped by the maximum members possible. It was recognized that no
rehabilitative programme could be a success unless public health and
nutritional aspects were not also addressed. This was particularly so
for the "free" colonies and "jhuggi jhonpri" clusters which were often
enough located near traditional leprosy homes and hospitals. The
Committee recommended that these were suitable locations for the
establishment of vocational training and production centres.
Today, the emphasis needs to be rapidly placed on positive
rehabilitation measures. IL is difficult to accept the view that
rehabilitation measures should wait until the patient has developed
deformities and is unable to retain his job. Prevention of
"dehabilitation" should be an important goal at the commencement of
chemotherapy itself.
An integrated rehabilitation plan is under consideration of the
Government, to be started in seven districts that have completed six
years of MDT treatment. There are Vizianagaram, Ganjam, Purulia,
North Arcot, Srikulum, Chingelpet and Wardha. The proposal,
presently in its blueprint stage, envisages the establishment of a
Vocational Training Centre in each district. While largely for the
leprosy affected, they would also include some proportion of other
handicapped persons. In a district with a population of approximately
1.5 million, it has been estimated that where the prevalence rate is 15
per
91

thousand, 22.500 patients are in need of MDT. It is also estimated that
an average 3,000 patients with grade II disability would require some
form of vocational rehabilitation, with a proportion also requiring
corrective and reconstructive surgery. In due course, it is proposed to
introduce MDT in other highly endemic districts by 1990, and in all
201 endemic districts by 1995. The assumption is that the scope of the
rehabilitation package would also be extended to all MDT districts.
The objectives of the scheme lay emphasis on community- based
vocational rehabilitation services. These would be appropriate to the
cultural and social milieu of the people of these districts. The
objectives would be to prevent disabilities from occurring, and where
deformities have already developed, to assist with reconstructive
surgery. This would better enable patients to be equipped to gain some
means of livelihood, which in turn would assist them to gain or regain
respect in their families and community.
The blueprint intends that the district rehabilitation centre would-
function for four years before shifting its services to another eligible
district. Within each district an institution providing for surgical
facilities would be identified, and those in need of reconstructive
surgery would be referred there. The entire cost of surgery and related
costs of transportation including a subsistence allowance would not be
borne by the patient. The envisaged number of cases requiring surgery
etc. is roughly estimated to be 3,000 in a district of the size and
prevalence rate mentioned above.
A list of 10 vocations - tailoring, weaving, carpet making; hand pump
set repairs, candle making, mats and basket weaving, pot making.
vegetable farming, furniture making and making of electrical circuits -
has been prepared. A package of seven trades • would be applied to a
district. At the district level, a committee to oversee and coordinate the
activities of the Leprosy "Rehabilitation Centre would be established
under the chairmanship of the District Magistrate. This Committee
would
92

also have on it the district Social Welfare Officer, the district level
chiefs of two nationalised banks, the district Health Officer, the
district Leprosy Officer and the Rehabilitation Officer. The latter
would function as the member-secretary to the group. This
Committee would meet once in six months. Reviews would be
conducted at regular intervals.
Before these proposals are finalised it would be useful to
examine these in the light of the experiences of voluntary agencies
which have been working both in control and rehabilitation
measures. Many of these organisations have, over the years, refined
their methodologies and acquired sharper focus. The scheme makes
no provision for social workers. The presence of the social worker
with some training in psychology and an understanding of local
community values, would be a definite asset. The experience of
several voluntary agencies has shown the crucial linkages between
trained social workers and patients. This is especially true after the
training period is over, when the patient is expected to function
independently in his new vocation. The self doubts, the problems of
adjustment, problems of loan servicing all require close monitoring
for several months. In the final analysis it would be self-defeating if
the patient having undergone vocational training is unable to fend for
himself. It would not only lead to degrees of rejection within family
arid community, but it may affect the success of the scheme as a
whole.
The problems of the healthy children of the leprosy affected need
to be treated as a special case because stigma attaches to them
especially when it becomes known that they are the (albeit healthy)
off-spring of the leprosy affected. It is not enough to only train the
patient or ex-patient with Grade II disability. The training of these
healthy young men and women would, give them the chance to
move out of the "free" leprosy colonies, and obtain jobs elsewhere.
Their situation is unlike that of the children of any other
handicapped category, and requires to be treated with special
attention.
93

The district surveys would also throw up cases of the leprosy affected (ex-patient) destitutes. These would include cases of Grade III disability, as well as old, infirm and 'burnt-out' cases. Most of them would fall outside the pale of vocational training either on account of advanced age or disabilities., There is the additional factor which may be taken into account. After a particular point, the human spirit breaks, and it is difficult to readjust such personalities to accept a training regimen. The old and infirm need a sheltered environment but it is not physically possible to match supply with demand. However, it would induce family and community acceptability if the aged and destitute be covered by a pension scheme. Even a small monetary amount would go a long way in making the leprosy affected more welcome, because he would then be a contributory member to the family fund. This need not be envisaged as a long term measure. It would take care of the aged leprosy population, while the younger elements would fall within the ambit of the training schemes.
94

H Training and Placement Services
The Directorate General of Employment and Training (DGET) in
the Ministry of Labour operates several training schemes to
ensure a regular supply of skilled manpower at different levels.
T h e s e i n c l u d e t h e C r a f t s m e n T r a i n i n g S c h e m e , t h e
Apprenticeship Training Scheme. Crafts Instructors Training
Scheme, training of highly skilled craftsmen under the Advanced
Vocational Training Scheme, as well as special training
programmes for women and training for several categories of the
handicapped through its Vocational Rehabilitation Centres for
the Handicapped. Some of the t raining programmes are
implemented by the State Governments and Union Territories,
some are implemented exclusively by the Central Government,
and some are implemented jointly.
The Directorate General of Employment and Training
provides training and employment services for several categories
of the handicapped, viz. the visually handicapped, the deaf and
dumb, the orthopaedically handicapped, the negative leprosy
affected and the mild mentally retarded. Largely through the
instrument of the 16 Vocational Rehabilitation Centres for the
Handicapped, the DGET has been admitting a number of
handicapped persons including a small percentage of negative
leprosy cases. Through 23 Special Employment Exchanges, one
each in most metropolitan cities, vocational guidance and placement services are provided. Special cells for the physically
handicapped, with special placement officers attached to the
employment exchanges ent i rely funded by the Central
Government, are also in the process of being established under
the aegis of the Ministry of Welfare.
There are 16 Vocational Rehabilitation Centres for the
Handicapped (VRCH), one each at Ludhiana, Delhi, Kanpur,
J aba lpur . Ahmed ab ad , Gauh a t i , Bomb a y, Ban ga lo re ,
Trivandrum, Madras, Hyderabad, Calcutta, Bhubaneswar,
Jaipur, Agartala and Baroda. One Vocational Rehabilitation
Centre is exclusively for the women handicapped. Two were
95

opened in 1968; thereafter others have been opened gradually over the following two decades. (In this context it is to be noted that the total achievement should be quantified in relation to the number of existing VRCH).
The VRCH are designed to provide rehabilitation services to
handicapped persons to suit their physical and psychological
capacities. The following services are offered
(i) Medical Evaluation: Handicapped persons are
referred to medical boards,
attached to rehabilitation
centres both to determine
their residual work
capacities, and suggest
curative and remedial
measures.
Handicapped persons are
interviewed for the purposes of
obtaining information about
their socio-economic
background, attainments
etc., and are also tested to
assess their intelligence,
aptitude, manual dexterity, and
personality traits.
The working capacity of each
handicapped person is tested on
the shop floor in workshops
attached to the centres, in units
that include metal assembly,
carpentry, radio as sem bl y,
t a i l o r in g and cutting,
typewriting, drawing and
painting, This assists the
vocational instructors to
96
(ii) Psychological and Social Evaluation
(iii) Vocational
Evaluation

help in assessing vocational skills
and potential. During the period of
evaluation, a stipend is paid for
upto a month. The handicapped
are also given training in work
adjustment. Counselling and
motivation for taking appro-
priate decisions in personal and
vocational areas, are also
provided.
After completion of various
evaluations, these reports are
discussed by officers and evalua-
ting staff, in a case conference
where decisions regarding the
vocational plans of the handi-
capped persons are taken. These
conferences are frequently attended
by medical specialists,
employment officers of Special
Employment Exchanges and by
employers.
Those handicapped persons who
are willing to undergo training, are
assisted in securing admissions
in Industrial Training Institutes
according to their suitability. For
others, shop floor training in
industry, as well as at
rehabilitation centres, is arranged.
At the VRCH, where skill training
workshops have been provided,
training is provided in various
vocations, to improve their skills
and to
97
(iv) Vocational Plans
(vi) Skill Development

make them more suitable for
wage or self employment. During
the period of training,
scholarships amounting to Rs.
170/- a month are provided by
the Union Ministry of Welfare.
Some of the handicapped
persons who can take up direct
employment, are assisted in
placement against vacancy notices
received from organisations under
the Central Government and State
Governments . The VRCH
direct ly receive vacancy
notifications for posts reserved
for physically handicapped
persons. Rehabilitation officers
are usually also in contact with
private industry to help promote
the employment of handicapped
persons in the private sector. To
assist with self-employment
schemes, the rehabilitation officers
are in touch with banks, financial
Institutions and the District
Industries Centres. Recently, case
workers have been placed for client
counselling, and they take up cases
after evaluation and skill training
stages, to assist in helping clients to
adjust to employment, as well as
help with follow-up services.
98
(vi) Rehabilitation and
Placement

The VRCH have been recognised
by the Government as agencies to
assist handicapped persons with
the fitting of orthotic and
prosthetic aids and appliances.
The Ministry of Welfare
provides financial assistance to
these Centres for this purpose.
An Advisory Board consisting of
representatives of Government .
i n d u s t r y, em p l o ye r s ' an d
workers and voluntary
organisations. medical specialists
and social workers have been set
up at each VRCH to advise
them on matters relating to
rehabilitation services and the
welfare of the physically
handicapped. The term of each
Advisory Board is three years.
Some physically handicapped
persons are not able to avail of
institutional and apprenticeship
training facilities in the absence of
requisite educational qualifications
for such courses. In such cases,
non-formal training is also
available at some of the
VRCH. These provide skill
development services. They do not
provide any formal certification
after he training. At present there
are seven Skill Training Work-
shops (STWs) in operation.
99
(vii) Fitting of Aids
and Appliances :
(vii) Advisory Boards
(ix) Skill Training
Workshops :

The training modules include
refrigeration and aircondition
ing, motor-mechanics, dress
making, printing and book-
binding. clock and watch
repairing, screen printing and
basic courses in electronics.
993 handicapped persons have
been trained by the Skill Training
Workshops, attached to seven
Vocational Rehabilitation Centres
by December 1987. Table 19
reflects the progress of training at
these workshops. There is no
specific break-up of the categories
of handicapped persons.
In order to provide services in
rural areas and to extend the
training facilities currently
available at the VRCH. eleven
Rural Rehabilitation Extension
centres have so far been
established at block level under
five selected VRCH .The details
are given below :
100
(X) Rural Rehabilita-
tion Extension
Centres at VRCs:

VOCATIONAL TRAINING AND EMPLOYMENT AS
THE PRINCEPAL MEANS OF REHABILITATION
The twin aspects of rehabi l i tat ion namely economic
productivity and social reassimilation must complement each
other if we are to accept the definition of rehabilitation in its real sense. Vocational
(formal or non-formal) training. employment, •
placement and follow-up by community and case workers are each a part of the complex matrix that spell the challenges of the
rehabilitation problem. Today a considerable part of the
rehabilitation effort is in the voluntary sector. The Government
has indeed established Vocation Rehabilitation Centres for the
Handicapped (VRCH), but as the figures reveal, the total number of
negative leprosy cases rehabilitated is negligible when compared
to other ca tegories of the handicapped who have been
rehabilitated. Meanwhile, the leprosy situation has grown in
complexity and it cannot be handled by voluntary effort alone. It
Is, therefore, incumbent on Government to strengthen and
enlarge its role of training and rehabilitation specific to the
situation of the leprosy affected, as well as to reinforce the
voluntary sector. It is also necessary to provide networking
services which Government alone can effectively establish.
While it is not always fair to place the major burden of all
problems on Government, leprosy is a disease which has special
problems, which is why if Government is not to enlarge its role in
the rehabilitation aspects of the leprosy eradication programme,
there will be little chance that the private sector will agree to
enlarge its role as a potential employer.
The situation as it presently exists is that most of the training
and rehabilitation effort is being provided by voluntary agencies.
Different voluntary agencies have been attending to different
facets of the problem. Some are able to provide rudimentary
training programmes along with medical services, on which the
emphasis has been largely placed. Only a few of the largest
organisations are now able to provide broad spectrum services
101

which include control aspects as well as a package of training and
placement services.
Voluntary effort, despite its pioneering and praiseworthy
role, is by definition fragmented, with each organisation often a
small pool of excellence. Until recently the relationship of
voluntary organisations with Government was largely confined
to efforts to obtain funding. It is only comparatively recently that
the Ministry of Health took the initiative in establishing an
annual conference of voluntary agencies working in the field of
leprosy control and rehabil i tat ion. This now provides a
meaningful dialogue between the Ministries of Health and Social
Welfare, with the voluntary agencies, and also between the
voluntary agencies themselves. This annual conference has
come to play a significant role in taking stock and in assessing
difficulties and developments.
However, it is not sufficient only to provide a sounding board
for current developments. In view of the fact that training
resources in the voluntary and Government sectors together
continue to be limited, it is essential to ensure that a well
coordinated networking arrangement is developed which will
computerise the total extent of facilities available under the
various agencies. This networking arrangement might usefully
fall within the purview of either the Ministry of Health or the
Ministry of Welfare. As spelled out in the following chapter, the
Directorate General of Employment and Training (DGET) under
the Union Ministry of Labour is already providing some training
programmes for negative leprosy cases through the Vocational
Rehabilitation Centres for the Handicapped (VRCH), and, in a
more limited way, under the general 3% reservation category for
the handicapped through the 1887 Industrial Training Institute
(I.T.Is) in the country. These apart, a number of voluntary
agencies are also providing a multitude of services, which
sometimes include training programmes as well as employment
and follow-up services. These need to be enumerated and,
wherever possible, strengthened. It must be recognised that while
the disabled leprosy affected account for only 0.7% of the world's
102

disabled population, they do represent a very difficult group to
rehabilitate, because stigma persists beyond the point of actual
cure. Several studies have already revealed that a serious
dimension of the problem of the leprosy affected is economic. It,
therefore, becomes necessary to tabulate the different kinds of
programmes available both in the Government and voluntary
sectors, to strengthen these wherever possible by providing new
methods of service delivery, and a new approach to employment
aspects. All avenues of employment after training need to be
strengthened. These include self-employment schemes: bank and
other institutional lending arrangement which are inescapably
l i n k ed w i t h s e l f - e m p l o ym en t s c h e m e s : em p l o ym en t
opportunities provided by sheltered workshops: employment
provided under the aegis of Government under rehabilitation
schemes for the handicapped: or open employment in factories
and other units of commercial production. The need for training
is doubly necessary for the leprosy affected, not only because it
can lead to employment, but in so doing it enables them to rise
above their predicament and gain a sense of equality, which
today only the employment market can effectively provide. It is
well established that in a depressed economy wi th high
employment or underemployment, the physically handicapped,
specially the unskilled, are not able to compete with the able bodied
for employment, and the leprosy patient has even less of 'chance than
other categories of the handicapped. This is not to sa y t h a t
s t i gm a d i s ap p ear s w i t h t he o b t a i n i n g o f t he
employment. Employers and workers do continue to reflect
prejudice in the same measure as open society reflects it.
However, with the growing awareness in the community at large
that the disease is curable and is usually non-infectious, the
leprosy affected is increasingly able to demonstrate that he is no
worse off for his affliction than other categories of handicapped
people. The need for a well devised and sustained communication
strategy has been spelled out elsewhere in this paper. A powerful
national campaign will further change attitudes as awareness
grows that multi-drug therapy is today available to effect
complete non-infectivity, often within a matter of a few weeks.
103

Training opportunities provided by the Government for the
handicapped has been discussed in the following chapter. Tables
17 and 18 provide figures of negative leprosy cases admitted,
evaluated and rehabilitated. The figures are very small to make
any worthwhile impact on the total scenario. If we are to see an
end to the problem in the foreseeable future; it is necessary to
expand the base of existing training opportunities. It is quite well
known (and the figures in the Tables amplify) that the range of
training that even the orthopaedically handicapped can
undertake is fairly wide. Until many more of the affected
population, with or without deformity. are not taken into the
t ra in ing pool t hey cannot s e r ious l y hope to en te r the
employment market . While the other categories of the
handicapped are well dispersed in the community, the leprosy
affected often live together in clusters or "free" colonies. Under
these c i rcumstances , i t should not be so d i f f i cu l t for
rehabilitation officers or para medical staff or community
workers to make special effort to enlist them into the training
pool. The network of Industrial Training Institutes is expected to
provide 3% reservation for handicapped persons. It would be
helpful if a small number of seats are reserved for leprosy cases.
on the criterion that stigma operates against leprosy. It would be seen
in Table 18 that the percentage of negative leprosy clients admitted
from the inception of VRCH till December 1987 is only 1,391
against a total of 1,41,757 handicapped persons admitted to t he
p rogramme. The nega t ive l ep ros y c l i en t s f i nal l y
rehabilitated for this entire period is 223 of a total of 42,400
clients rehabilitated, representing 0.53% of the total numbers
rehabilitated. While actual placement for other categories of the
handicapped are not unacceptable, the total number of
placements of the leprosy affected are low. The total number of
clients listed in the live, registers also represent a fraction of
those requiring placement assistance. The figure of 426 in
Table B of Chapter H is not in itself surprising, for reasons of
stigma at various levels. Often, leprosy patients are themselves
wary of coming forward, and special efforts need to be made to
draw them out. Until this not seen to be done, the private sector
will not overcome its reluctance to follow suit, although it must
104

that some enlightened employers in the private sector have set
notable examples not merely in employing the leprosy affected,
but also in purchasing their products.
It is worthwhile to briefly illustrate the operation of stigma
in the purchase of finished goods. A well known leprosy
rehabili tation centre in the voluntary sector received an
important order for wooden packaging crates from a leading steel
mill. However, when the workers at the steel mill learned that
the crates were being manufactured by leprosy affected persons.
they were adamant in their refusal to receive or touch them. It
was wi th cons iderable d i f f i cu l t y that the en l ightened
management of the mill was able to persuade their unions and
workers that there was no health risk whatsoever in the ir
handling of the wooden crates. However, they boycotted the
workers f rom the rehabi l i t at ion cent re , who were sent
periodically to accompany the consignments. It took several
visits spread over a period of years before hostility towards the
workers from the rehabilitation centre gave way to some form of
acceptance by the workers in the steel mill.
Employment
The vast majority of the leprosy affected and handicapped
l ive in the informal sector . It i s clearly impossible for
Government or voluntary effort to provide sheltered employment
to all. The answer must lie in self-employment schemes, which
may include the opening of small shops (provisions, tailoring or
trading) or agricultural work or poultry or cattle rearing.
A major consideration by Union and State Governments is
the help that should be provided in giving interest-free loans, or
loans at nominal rates of interest. Despite the relatively easy
availability of loans for the non-handicapped, the leprosy
handicapped, especially those bearing deformity continue to face a
number of problems. They have often experienced difficulty in even
obtaining the loans forms, particularly in cases of those who
bear deformity, or on occasions when their background
105

becomes known to bank staff. The experience is that unless there is
a voluntary organism ton acting for such clients, or unless a
bank manager is especially sympathetic, individual applicants
soon give up any desultory efforts in this direction.
Aware of these realities, some voluntary organisations have
developed a good rapport with banks, whom they approach after
first motivating the client to undertake some form of economic
activity. It is necessary for the individual to feel an inner need.
An occupation thrust on the individual does not usually fructify.
Some studies and surveys have shown that the loans taken by the
leprosy affected have on the average a good repayment record.
However, banking institutions should themselves be more
forthcoming in their assistance. This would help in measures for
self-employment in the agricultural sphere, particularly in the
informal sector. This trend should be encouraged alike by State
Governments, voluntary effort and financial institutions,
because it helps to reduce 'dehabilitation' and eases the pressure
on the cities.
Capital-intensive schemes and sheltered workshops do
provide employment, but to a very few, which is why they may be
advocated in positive cases, or in cases with severe physical and
mental disabilities or in cases of special categories, such as young
destitute women who need to be provided with a sheltered
situation. Wherever possible, however, such schemes should be
used as a training ground and designed to enable an 'apprentice' to
move out of a sheltered situation as early as possible. In general,
however, high investment per capita is not a desirable goal for
countries which have a major leprosy problem.
Rehabilitation and Adjustment
If rehabilitation is to succeed in its true sense, the thrust of
enlightened advisory services must equally be on the re -
orientation of the mind, with the need to emphasize to the
patients' their strengths, not their weaknesses; their abilities,
not their disabilities. The approach should not be in the 19th
106

century charitable mould: it needs to be one where the patient can-I
be taken as an equal partner in the country's developmental
programme and equipped to hold his own, albeit in a competitive
world where jobs are scarce. Into such a category usually fit only
the relatively young and those without major disability. It is this
category that voluntary agencies can successfully hope to train or re-
train. It often becomes necessary to begin with the training of minds to
accept a course of life where they need to aim to become a useful
part of the social and economic fabric, and not opt out into the
seemingly comparative freedom of the sub-cultures of begging,
illicit distillation of liquor, delinquency or crime. This approach is
already being followed by voluntary action in greater or
lesser measure. But as voluntary effort has also
demonstrated, where this is not consciously attempted and
pursued, there is often a slideback because of the difficulties that
arise in the struggle for economic rehabilitation. It is not enough
that the disease is halted and the patient vocationally trained.
There are several psychological difficulties involved in the "re-
entry" process into society.
These difficulties are faced on both sides of the fence. Society
cont inues to ref lec t i t s suspicions about leprosy in i t s
stigmatising attitude. The patient, on the other hand, having
been hurt in varying degree by family, friends, neighbours, co-
workers and other members of the community (including
possibly even members of the medical profession) is wary about
leaving his new community of fellow leprosy affected (within the
sheltered institution, hospital or leprosy colony as the case may
be). No rehabilitation programme can entirely succeed unless the
psychological impairment. if any, is not first treated, and this
requires continuous follow-up by social and case workers who
should be able to guide and help the ex-patient, as he struggles to take
his initial steps in the outside, unsheltered world.
There would appear to be marked improvement in attitudes
towards the disease as a direct result of Governmental and
voluntary effort in the last decade. Hostility remains, but it
appears to be less than in earlier years. In the field survey that
107

the author conducted in 1987, which represents a broad spectrum
of areas in North. West and South India, the family reaction of
192 patients sampled indicated that upon the first discovery of
the disease. in 98 cases (51.04%) the reaction was cordial. There
was indifference in 23 cases (11.97%). There was a negligent
attitude in 41 cases (21.35%) and boycott in 19 cases (9.89%). In
11 cases (5.72%) the individual did not disclose his or her disease.
Combining negligence and boycott as representative of a hostile
attitude, it may be seen that in 31.24% of cases, patients
encountered a hostile attitude from family members upon the
discovery of the disease. In 51.04% of the cases, however, family
members accepted the disease without affecting hostility.
In the cases of friends, the patients met with a much lower
degree of cordiality. Of the 192 cases sampled, in only 54 cases
(28.12%) did relations with friends remain cordial. Friends
reflected indifference in 28 cases (14.58%) and negligence in 43
cases (22.39%). Boycott, too, was higher at 25 cases (13.02%). Not
unexpectedly, the disease was not disclosed in a much higher
number of cases at 42 (21.87%).
An interesting and healthy development lay in the sample
conducted on the patients' initial exposure to doctors and other
members of the medical profession. Of the 192 cases sampled, in
as high as 165 cases (85.9%) the patient found the attitude of
doctors helpful; in 19 cases (9.89%) there was indifference, and
negligence was reflected in only 5 cases (2.6%). It needs however to
be stated that the samples were taken largely in controlled
areas near leprosy hospitals, or of groups under regular
treatment.
The imperatives of training
Training resources are scarce. With the need to stretch them as
far as possible, training should be applied wherever returns are
likely to be 'highest'. Within the age group of 15-45, the
incumbents probably have a higher degree of motivation to
acquire skills than in higher age groupings. The younger age
108

group are also more likely to have had a basic school education
but no automatic job opportunity. There is also greater
likelihood that skills, having been acquired. may be shaped into
economic livelihood, given other assumptions (bank loans.
ava i l ab i l i t y o f app ara tus e t c . ) . Econ o mic and soc i a l
rehabilitation would in such cases become a possibility. What
has to be res i s t ed i s t he t endency fo r t r a in ing and/o r
rehabilitation institutes to convert themselves into permanent
abodes for a chosen few, which ren ders the pol i cy o f
rehabilitation self-defeating. In these cases such institutions
become place of sheltered employment for a few. There is indeed a
case for sheltered employment, but the distinction between a
training institution, and an institution intended to provide
sheltered employment, and a residual care home for destitute
cases needs to be maintained.
Training must come early, it must be reasonably short in
duration, and it should be purposefully shaped to provide for the
type of employment, as far as possible to suit the milieu from
which the incumbent sprang. It is unlikely that the very disabled
or old would take to training. Training as an input in currently
held occupations if any. may be preferable. There is also little use in
preparing specifically for the cities. In an environment where
there are a host of difficulties arising from factors such as the
rising cost of living, the problems of housing and a quicker urban
pace, it would make it even more difficult for the incumbent to
compete with the able bodied. In a situation where there is a good
rapport with industry, persons may be trained specifically to suit
certain jobs openings.
It needs to be stated that employment in open industry is
difficult to obtain. However, whether, the end result aims for
industry or self-employment, the incumbent trained to operate a
lathe or machine in the light engineering industry, would stand a
better chance than his untrained counterpart . Machine
operators well trained in the use of such machines are usually in
demand and the pay is good. A pre-requisite may be a high school
level of general education. The problems with large scale
109

industry are however compounded by competitive entrance
procedures and higher educational qualifications demanded, not to
mention the problems of living in large cities including
transport, housing and schooling costs. Barring exceptions.
aiming for large industry should not be the goal. Small
industries are a better alternative. Although the problem is that
employment here is relatively temporary in nature, at the same
time entrance qualifications are also simpler, they are less
structured and bureaucratic, and their technology is also usually
simpler. Training should therefore aim for the small industry
segment of the employment market.
In selecting an occupation the patient's physical handicaps
must necessarily be taken into account. Work involving heat or
friction is unsuitable for anaesthetic hands because the patient
cannot feel to establish his or her threshold of tolerance. Those
patient trainees whose hands and feet are not anaesthetic can be
given a wide range of t ra ining: those whose hands are
anaesthetic but fingers are intact may be given training where the
Implements they handle or the machines they use bear no sharp
edges, or are not hot, and where implements are rubber coated.
Sharp tools can be used with a relatively higher degree of safety
over tools that involve heat or friction because a patient with
anaesthetic hands can see the sharpness, and does not need to
rely on feeling to warn him of danger. For those whose feet are
anaesthetic and who should not stand for too long, there may be
need for special footwear as well. While light engineering
workshops and fabrica t ion uni ts should safeguard the
patient/trainees from molten metal, welding, metal casting etc.,
some voluntary agencies provide excellent training schemes that
Include a wide range of engineering skills.* It is interesting to
see, given the basic safeguards, how quickly highly motivated
young trainees are able to adapt themselves to such training and
usually remain accident free in the process.
* The Worth Trust at Katpadi near Ve l lore, Tamilnaclu, runs two l ight engineering units on commercial lines staffed largely by handicapped workers, chiefly the leprosy affected. It also runs a training centre for handicapped. youth
110

The training imparted by some of the larger voluntary
agencies represent pools of excellence. Since most of the affected live in
rural areas, training could advantageously be agriculture- based, involving
the production of food, fruit, vegetables, milk or poultry. However, dairy
farming and animal husbandry should be in general confined to
patients who have the necessary land and family help to be self
employed. It could be combined with training in small scale
diversified agriculture, the use of appropriate technology and of
natural energy (solar, wind power and simple treddle machines). In self-
employment schemes, the importance of traditional occupations
especially in the rural context, is significant. If the patient has to acquire
his own raw materials and market his products, he needs the
cooperation of other related trades people. Alternatively, the
rehabilitating agency should undertake to supply raw materials, and
assist in the marketing of finished goods. The Khadi and Village
Industries Commission have specialised in rural-based schemes to
encourage self-employment, and these can be designed around the
leprosy affected. The Vocational Rehabilitation Centres for the
Handicapped and the Industrial Training Institutes provide -broad
spectrum training schemes ranging from plumbing, basic electrical
engineering and repair works, motor mechanics, tailoring, typing,
sewing, printing and cloth dyeing, in all of which training modules are
well developed, relatively simple and fairly inexpensive. Their
applicability to the leprosy affected needs to be intensified.
The importance of case workers to the leprosy situation cannot
be emphasised enough. Rehabilitation is an area where patients or
trainees face insecurity problems. Where patients have the outward
manifestation of the disease, they need a father figure to help them
overcome a host of problems arising from their lack of self-confidence.
The case worker is also a counsellor. Someone trained and experienced
must be available to share the trainee's fears and to answer his doubts. There
are patients who have lost the Jobs held before the advent of the disease and
are perhaps unable to get
111

re-employed. Re-employment as near as possible to previous or
traditional occupation is of advantage. This is particularly important in
India and elsewhere in South Asia where strong cultural and social
traditions often allow only a limited degree of freedom of occupation.
There are voluntary agencies that have refined the case worker
method, especially those engaged in domiciliary rehabilitation. Here
the primary task of case workers is to identify the person requiring
help and to assess his felt need in the context of his Immediate
environment. After helping to prepare the profile of the unit that is
intended to be established, they assist with a bank loan, or project seed
money from the voluntary agency. Follow-up visits continue through
the initial periods of teething problems, until self-sufficiency is gained
and repayment of the loan begins.
Training centres do need to be established on business like lines.
They should, wherever possible, aim to grow into self supporting
units. The philosophy of self reliance must permeate itself to its
incumbents. It is an advantage if training is conducted, wherever
possible, to the standard syllabi approved by State or Central
Government. Training should invariably be administered with an eye
to placement, because to use scarce resources and then not have them
applied to gainful employment means not simply wasted resources,
but also an increased measures of frustration that persons caught up in
this intricate social web must endure.
Re-training needs to be thought about not in the sense of refresher
training, but in the sense of learning a new trade. An incumbent who
may have been trained for a particular vocation, may have had to lose
it owing to growing disability of hands or feet, and an inability to use
anaesthetic hands or feet. In such cases it is not usually a simple case
of re-training in a new profession; training for adjustment formally or
informally is quite often a pre-requisite, for the mind must be
sometimes also prepared to accept a 'lower skill, before its application
can actually be translated into successful rehabilitation. Leprosy can
seldom be accepted as merely a medical problem; it has vital
112

psychological and social facets, and unless social and case
workers are present alongside the medical and para medical
workers, to tackle the problems of the mind alongside the body, it is
difficult to visualise a solution in the short term.
Voluntary agencies working in this area have demonstrated
time and again that after training, a moderately deformed
patient can acquire several skills with a reasonably high degree
of proficiency, including light engineering skills on a wide range of
machines. Where such training is provided in a mixed milieu, as
at the Worth Trust in Katpadi in Vellore where either the
leprosy handicapped are mixed with other categories of
handicapped, or with the non-handicapped, integration emerges
more easily. However, in the case of self-employment schemes, it
is frequently the case that the leprosy affected often face
considerable difficulty in the marketing of produce because of
stigma, and therefore it once again becomes necessary for the
State or the voluntary agency to attempt to direct the acquisition of
skills into those areas where the final product can find itself a
ready market. With a regular income, re-integration becomes a
possibility, and economic independence a viable shield against
stigma.
As the statistics in Tables 17 and 18 make clear, the number
of negative leprosy persons being trained under the VRCH is few.
Those being placed are fewer. The reasons are clear. The sheer
numbers of handicapped persons are overwhelming. With high
levels of unemployment and under employment, employers have
no special reason to wish to employ handicapped persons when
they can get non-handicapped workers for equal wages. The
employer's priorities are frequently in conflict with those of the
leprosy handicapped, the case worker and the rehabilitation
agency. The employer looking to investment and the reduction of
his costs is unlikely to continue with or accept afresh what he
may view as a medical risk. There are employers who may
themselves be sympathetic but are afraid of industrial action
which might be initiated by the employment of an ex-leprosy
patient. Nor are the employers presently receiving any incentive
113

of tax remission f rom the Government for employing
handicapped persons, especially ex-leprosy patients. Stigma
prevails at every level in the community, and there is no special
reason to believe that employers or for that matter personnel
that man employment exchanges and training programmes are
excluded from the general fear or misapprehension of this
disease.
Under these difficult but comprehensible conditions, the task
remains a daunting one, especially in view of actual placements
recorded. The answer must lie in strengthening training
schemes whenever they are found reasonably well structured.
Training schemes and placement services (and in some cases.
follow-up activities by professional case workers), are well
developed in several voluntary agencies . These should be
identified and reinforced. It is necessary to appraise voluntary
work annually, but it will be self-defeating to be overly critical,
or to unduly delay grants-in-aid. At the same time, Government
in the Ministries of Health, Social Welfare and Labour should
computerise all training and placement services, and update
these annually. An annual compendium should be published on
training programmes and services offered. Their per capita
costing should be established, together with placements (if any)
achieved. The results of follow-up on placements should be
determined. This would form part of the larger networking
arrangement, which would also ensure the preparation of a
manual of jobs for the handicapped.
The total package must necessarily lie in going beyond the
control dimension alone into the economic, sociological and
psychological factors that govern society's attitudes. Medical
control policy must be accompanied by a comprehensive,
relatively inexpensive and easily adaptable methodology that
aims in the first instance for the prevention of "dehabilitation";
or where "dehabilitation" has already occurred, to establish a
policy for vocational rehabilitation leading gradually to social
reintegration. Only with the recognition of this fact, and tne
acceptance and adoption of a policy leading to economic and
social rehabilitation, will the eradication of leprosy in its widest
sense begin to become a reality.
114