Embed Size (px)
Citation preview

CONFIDENTIAL
Jefferies Autumn 2015 Global Healthcare Conference Vivek Ramaswamy, Chief Executive Officer
Statements made in this presentation contains forward-looking statements, including statements regarding Axovant’s expectations about timing of the Phase 3 registration program for RVT-101, planned clinical studies of nelotanserin, and other elements of its clinical development and regulatory strategy. Forward-looking statements can be identified by the words “believes,” “expects,” “plans,” “potential,” “intends,” “will,” “should” and other similar expressions that are predictions or indicate future events, trends or prospects. Forward-looking statements are subject to risks and uncertainties that could cause actual results to differ materially and reported results should not be considered as an indication of future performance. These risks and uncertainties include, but are not limited to: risks associated with the success, cost and timing of our product development activities and clinical trials; the approval and commercialization of our product candidates RVT-101 and nelotanserin; and increased regulatory requirements. These statements are subject to the risk that clinical trial data are subject to differing interpretations, and regulatory agencies, medical and scientific experts and others may not share Axovant’s views of the clinical study data. There can be no assurance that the clinical programs for RVT-101 or nelotanserin will be successful in demonstrating safety and/or efficacy, that we will not encounter problems or delays in clinical development, or that any of our product candidates will ever receive regulatory approval or be successfully commercialized. For a further description of the risks and uncertainties that could cause actual results to differ from those expressed in these forward-looking statements, as well as risks relating to Axovant’s business in general, see the “Risk Factors” section of our quarterly report on Form 10-Q filed with the Securities and Exchange Commission on November 2, 2015, and other filings that Axovant makes with the SEC from time to time. These forward-looking statements are based on information available to Axovant as of the date of this presentation and speak only as of the date of this presentation. Axovant disclaims any obligation to update these forward-looking statements, except as may be required by law.
November 2015
Forward-Looking Statements
2
• Become the leading company focused on the treatment of dementia by addressing all forms and aspects of the condition
Vision: Dementia Solutions
• Build a late-stage pipeline of CNS drugs in a capital-efficient manner: deliver value to patients and to shareholders
Mission: Create Value for Patients and Shareholders
• RVT-101 is one successful pivotal phase 3 study away from approval by FDA and EMA in Alzheimer’s disease
Lead Drug: RVT-101 in Phase 3
• Current global leader in Lewy Body Dementia including both RVT-101 and nelotanserin
Rapidly Expanding our Pipeline
Axovant Sciences – The Dementia Solutions Company
3
Management Team
Vivek Ramaswamy* Chief Executive Officer
Mark Altmeyer* President & Chief Commercial Officer
Lawrence Friedhoff, M.D., Ph.D.* Chief Development Officer
Gregory Weinhoff, M.D., M.B.A.* Chief Financial Officer
Christine Mikail* Chief Administrative Officer & General Counsel
Marianne Romeo** Head, Global Transactions & Risk Management
Vivek Ramaswamy
Lawrence Olanoff, M.D., Ph.D.
Atul Pande, M.D.
Berndt Modig
Ilan Oren
Marianne Romeo
Directors
Axovant team includes developers of both Aricept (Dr. Friedhoff) and Namenda (Dr. Olanoff)
*Employee and officer of Axovant Sciences, Inc., a wholly-owned subsidiary of Axovant Sciences Ltd. **Employee and officer of Axovant Sciences Ltd.
Experienced Leadership
4
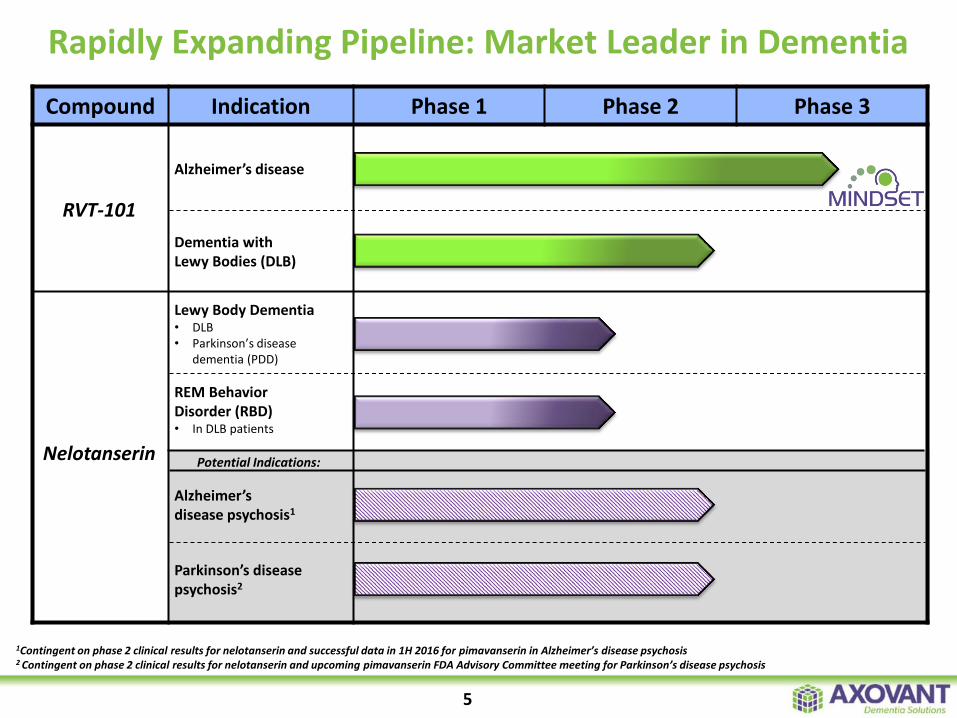
Rapidly Expanding Pipeline: Market Leader in Dementia
Compound Indication Phase 1 Phase 2 Phase 3
RVT-101
Alzheimer’s disease
Alzheimer’s disease psychosis1
Nelotanserin
Lewy Body Dementia • DLB • Parkinson’s disease
dementia (PDD)
Dementia with Lewy Bodies (DLB)
REM Behavior Disorder (RBD) • In DLB patients
Parkinson’s disease psychosis2
1Contingent on phase 2 clinical results for nelotanserin and successful data in 1H 2016 for pimavanserin in Alzheimer’s disease psychosis 2 Contingent on phase 2 clinical results for nelotanserin and upcoming pimavanserin FDA Advisory Committee meeting for Parkinson’s disease psychosis
Potential Indications:
5
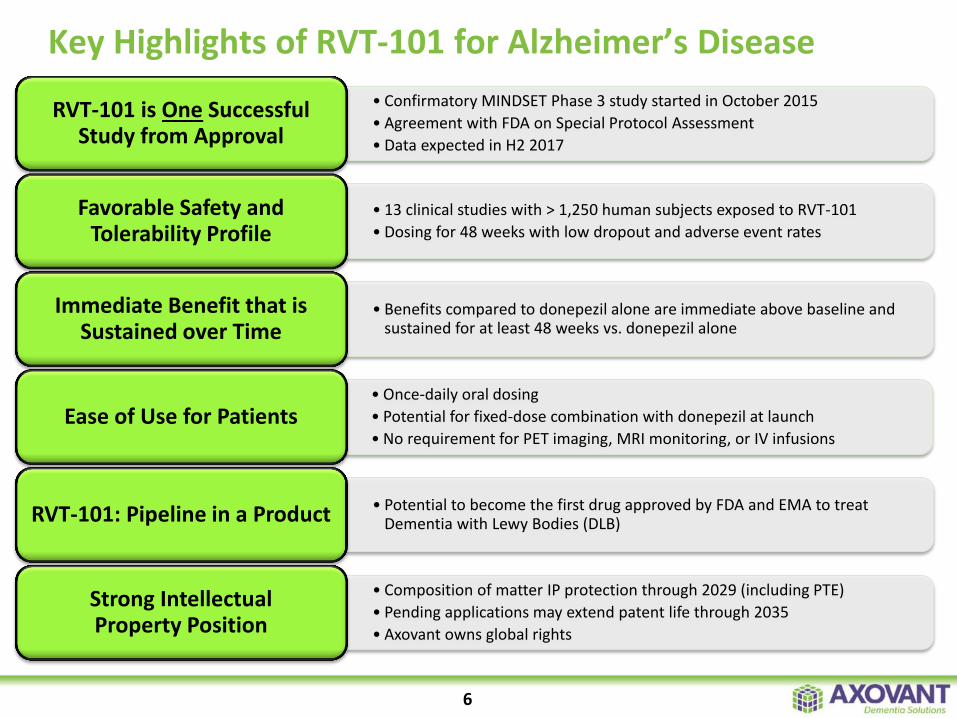
Key Highlights of RVT-101 for Alzheimer’s Disease
• Confirmatory MINDSET Phase 3 study started in October 2015
• Agreement with FDA on Special Protocol Assessment
• Data expected in H2 2017
RVT-101 is One Successful Study from Approval
• 13 clinical studies with > 1,250 human subjects exposed to RVT-101
• Dosing for 48 weeks with low dropout and adverse event rates
Favorable Safety and Tolerability Profile
• Benefits compared to donepezil alone are immediate above baseline and sustained for at least 48 weeks vs. donepezil alone
Immediate Benefit that is Sustained over Time
• Once-daily oral dosing
• Potential for fixed-dose combination with donepezil at launch
• No requirement for PET imaging, MRI monitoring, or IV infusions Ease of Use for Patients
• Potential to become the first drug approved by FDA and EMA to treat Dementia with Lewy Bodies (DLB) RVT-101: Pipeline in a Product
• Composition of matter IP protection through 2029 (including PTE)
• Pending applications may extend patent life through 2035
• Axovant owns global rights
Strong Intellectual Property Position
6
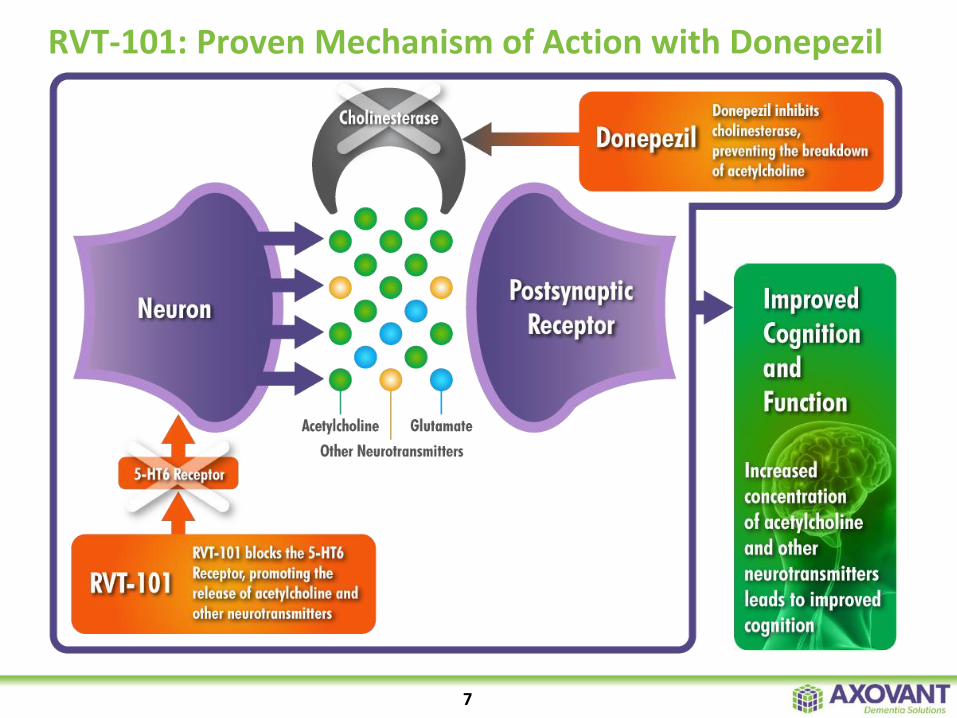
RVT-101: Proven Mechanism of Action with Donepezil
7
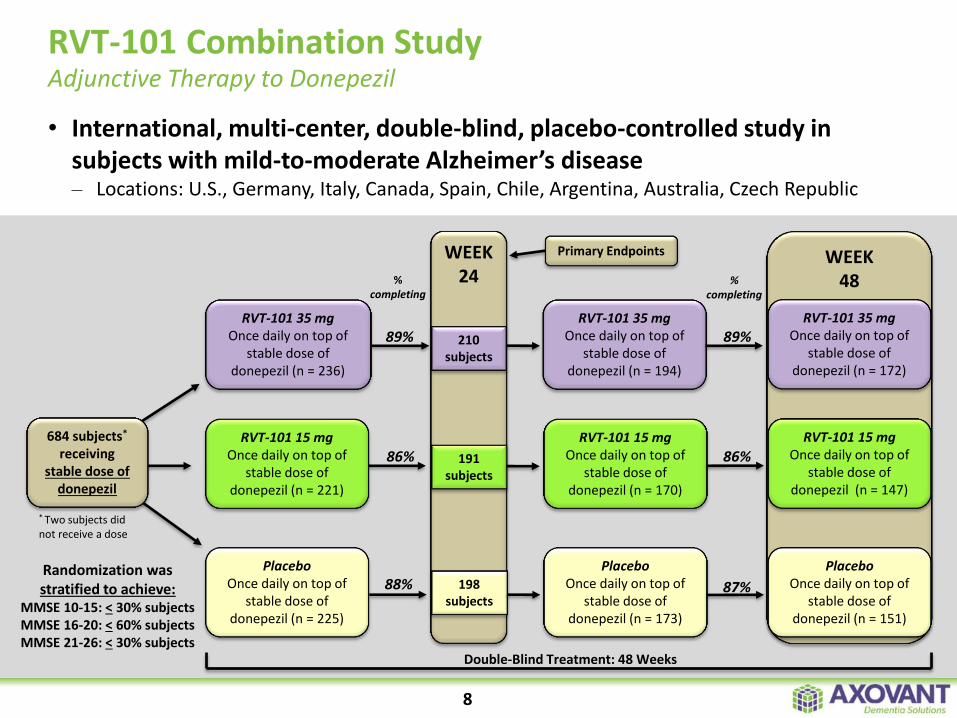
RVT-101 Combination Study Adjunctive Therapy to Donepezil
8
Randomization was stratified to achieve:
MMSE 10-15: < 30% subjects MMSE 16-20: < 60% subjects MMSE 21-26: < 30% subjects
684 subjects* receiving
stable dose of donepezil
* Two subjects did not receive a dose
RVT-101 35 mg Once daily on top of
stable dose of donepezil (n = 236)
Placebo Once daily on top of
stable dose of donepezil (n = 225)
% completing
89%
86%
88%
WEEK24
210 subjects
191 subjects
198 subjects
Double-Blind Treatment: 48 Weeks
RVT-101 35 mg Once daily on top of
stable dose of donepezil (n = 194)
RVT-101 15 mg Once daily on top of
stable dose of donepezil (n = 170)
Placebo Once daily on top of
stable dose of donepezil (n = 173)
WEEK 48
% completing
89%
86%
87%
RVT-101 35 mg Once daily on top of
stable dose of donepezil (n = 172)
RVT-101 15 mg Once daily on top of
stable dose of donepezil (n = 147)
Placebo Once daily on top of
stable dose of donepezil (n = 151)
RVT-101 15 mg Once daily on top of
stable dose of donepezil (n = 221)
Primary Endpoints
• International, multi-center, double-blind, placebo-controlled study in subjects with mild-to-moderate Alzheimer’s disease – Locations: U.S., Germany, Italy, Canada, Spain, Chile, Argentina, Australia, Czech Republic
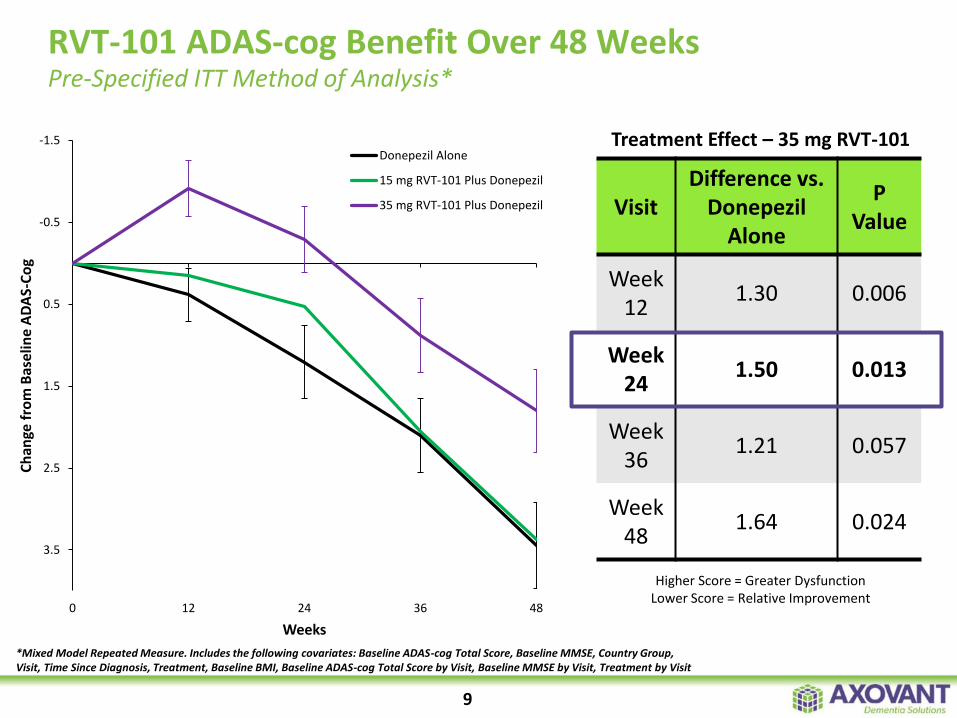
RVT-101 ADAS-cog Benefit Over 48 Weeks Pre-Specified ITT Method of Analysis*
Treatment Effect – 35 mg RVT-101
Visit Difference vs.
Donepezil Alone
P Value
Week 12
1.30 0.006
Week 24
1.50 0.013
Week 36
1.21 0.057
Week 48
1.64 0.024
-1.5
-0.5
0.5
1.5
2.5
3.5
0 12 24 36 48
Ch
ange
fro
m B
ase
line
AD
AS-
Co
g
Weeks
Donepezil Alone
15 mg RVT-101 Plus Donepezil
35 mg RVT-101 Plus Donepezil
Higher Score = Greater Dysfunction Lower Score = Relative Improvement
9
*Mixed Model Repeated Measure. Includes the following covariates: Baseline ADAS-cog Total Score, Baseline MMSE, Country Group, Visit, Time Since Diagnosis, Treatment, Baseline BMI, Baseline ADAS-cog Total Score by Visit, Baseline MMSE by Visit, Treatment by Visit
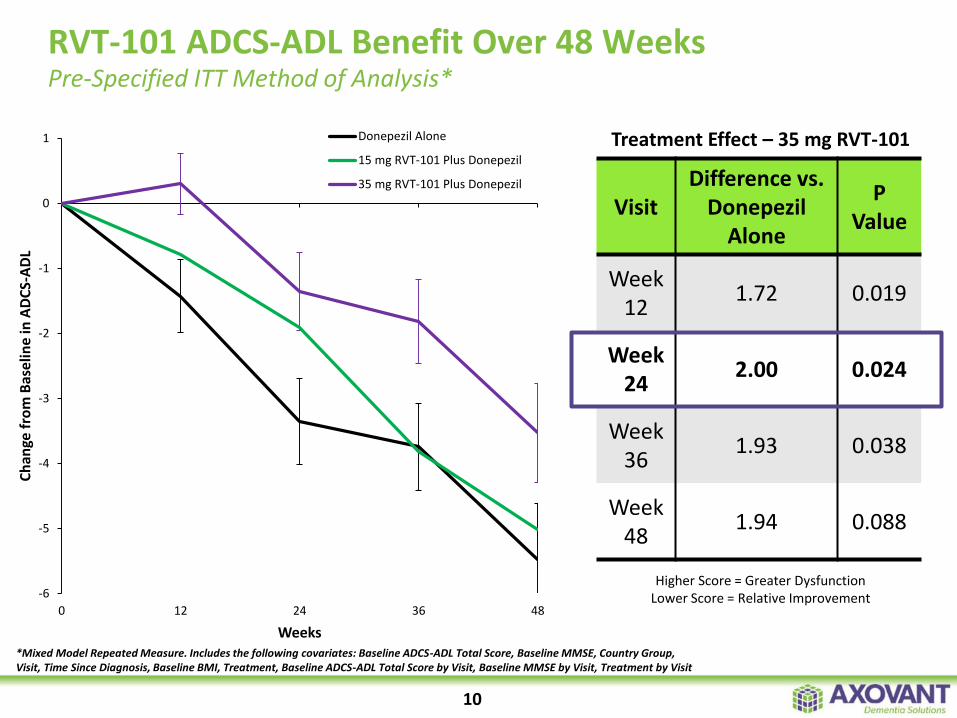
RVT-101 ADCS-ADL Benefit Over 48 Weeks Pre-Specified ITT Method of Analysis*
-6
-5
-4
-3
-2
-1
0
1
0 12 24 36 48
Ch
ange
fro
m B
ase
line
in A
DC
S-A
DL
Weeks
Donepezil Alone
15 mg RVT-101 Plus Donepezil
35 mg RVT-101 Plus Donepezil
10
Treatment Effect – 35 mg RVT-101
Visit Difference vs.
Donepezil Alone
P Value
Week 12
1.72 0.019
Week 24
2.00 0.024
Week 36
1.93 0.038
Week 48
1.94 0.088
Higher Score = Greater Dysfunction Lower Score = Relative Improvement
*Mixed Model Repeated Measure. Includes the following covariates: Baseline ADCS-ADL Total Score, Baseline MMSE, Country Group, Visit, Time Since Diagnosis, Baseline BMI, Treatment, Baseline ADCS-ADL Total Score by Visit, Baseline MMSE by Visit, Treatment by Visit
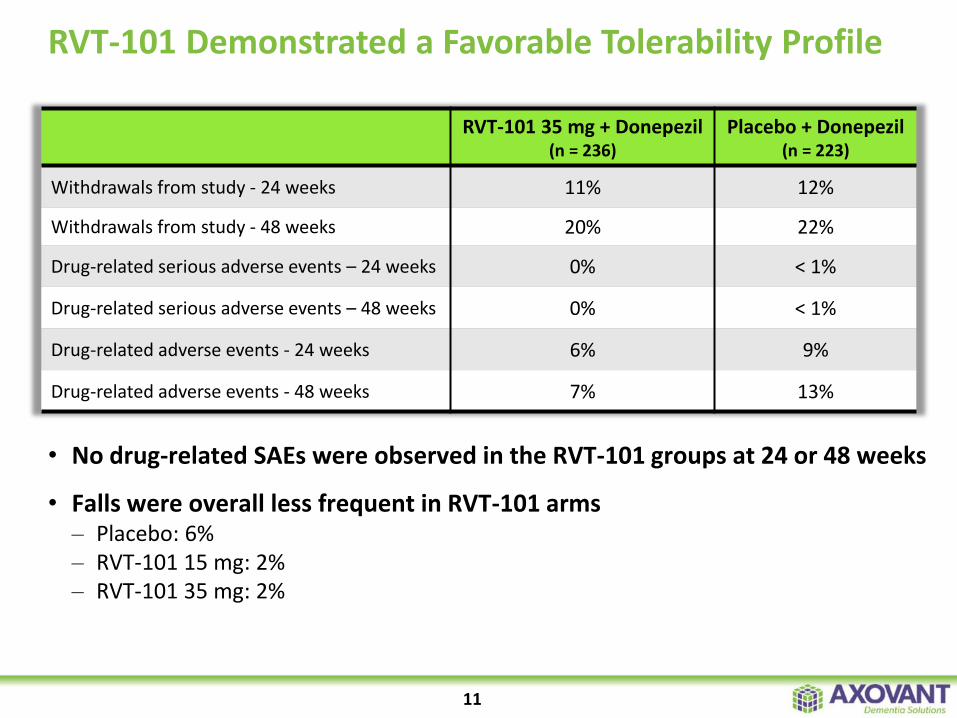
• No drug-related SAEs were observed in the RVT-101 groups at 24 or 48 weeks
• Falls were overall less frequent in RVT-101 arms – Placebo: 6% – RVT-101 15 mg: 2% – RVT-101 35 mg: 2%
RVT-101 35 mg + Donepezil (n = 236)
Placebo + Donepezil (n = 223)
Withdrawals from study - 24 weeks 11% 12%
Withdrawals from study - 48 weeks 20% 22%
Drug-related serious adverse events – 24 weeks 0% < 1%
Drug-related serious adverse events – 48 weeks 0% < 1%
Drug-related adverse events - 24 weeks 6% 9%
Drug-related adverse events - 48 weeks 7% 13%
RVT-101 Demonstrated a Favorable Tolerability Profile
11
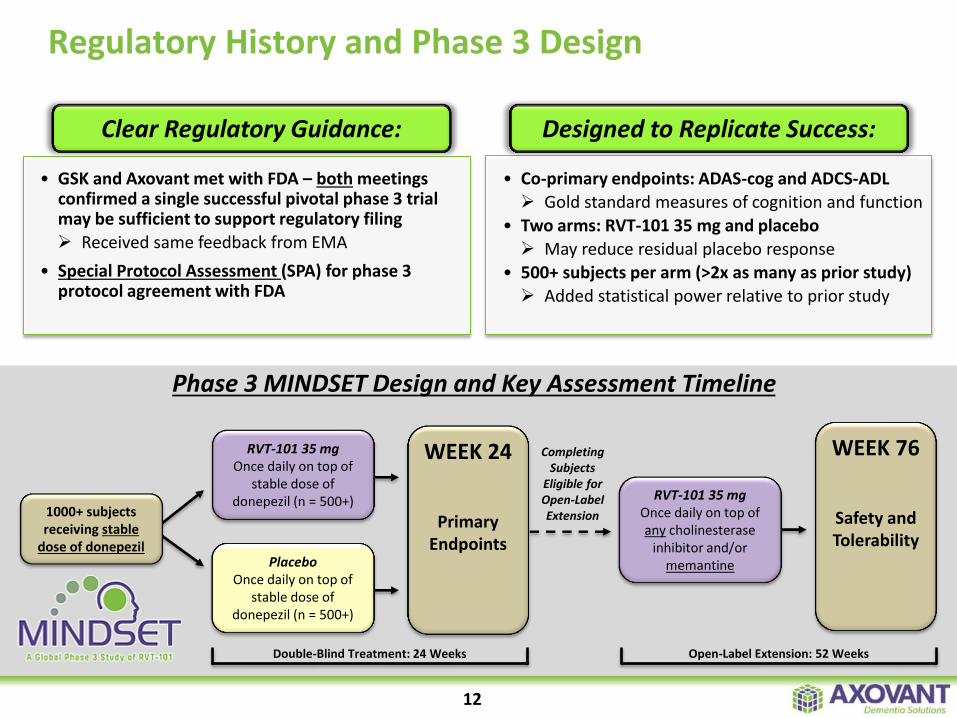
Regulatory History and Phase 3 Design
12
RVT-101 35 mg Once daily on top of
stable dose of donepezil (n = 500+)
Placebo Once daily on top of
stable dose of donepezil (n = 500+)
WEEK 24
Primary Endpoints
Double-Blind Treatment: 24 Weeks
1000+ subjects receiving stable
dose of donepezil
RVT-101 35 mg Once daily on top of any cholinesterase
inhibitor and/or memantine
Open-Label Extension: 52 Weeks
WEEK 76
Safety and Tolerability
Completing Subjects
Eligible for Open-Label Extension
Phase 3 MINDSET Design and Key Assessment Timeline
• GSK and Axovant met with FDA – both meetings confirmed a single successful pivotal phase 3 trial may be sufficient to support regulatory filing
Received same feedback from EMA
• Special Protocol Assessment (SPA) for phase 3 protocol agreement with FDA
• Co-primary endpoints: ADAS-cog and ADCS-ADL
Gold standard measures of cognition and function
• Two arms: RVT-101 35 mg and placebo
May reduce residual placebo response
• 500+ subjects per arm (>2x as many as prior study)
Added statistical power relative to prior study
Clear Regulatory Guidance: Designed to Replicate Success:
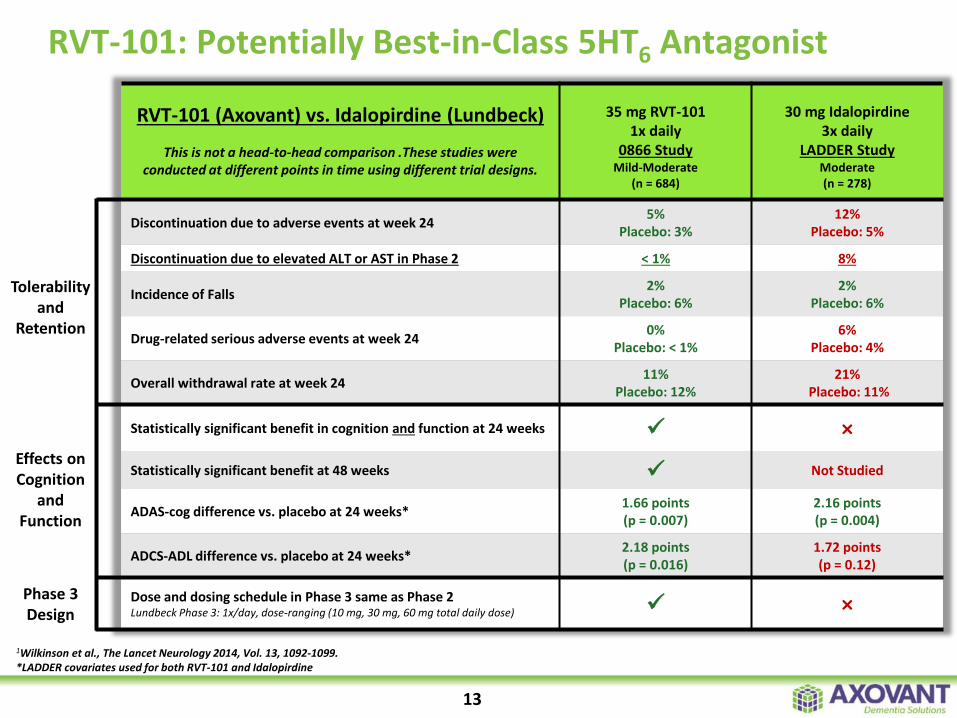
RVT-101: Potentially Best-in-Class 5HT6 Antagonist
13
Tolerability and
Retention
Effects on Cognition
and Function
Phase 3 Design
RVT-101 (Axovant) vs. Idalopirdine (Lundbeck)
This is not a head-to-head comparison .These studies were conducted at different points in time using different trial designs.
35 mg RVT-101 1x daily
0866 Study Mild-Moderate
(n = 684)
30 mg Idalopirdine 3x daily
LADDER Study Moderate (n = 278)
Discontinuation due to adverse events at week 24 5%
Placebo: 3% 12%
Placebo: 5%
Discontinuation due to elevated ALT or AST in Phase 2 < 1% 8%
Incidence of Falls 2%
Placebo: 6% 2%
Placebo: 6%
Drug-related serious adverse events at week 24 0%
Placebo: < 1% 6%
Placebo: 4%
Overall withdrawal rate at week 24 11%
Placebo: 12% 21%
Placebo: 11%
Statistically significant benefit in cognition and function at 24 weeks ×
Statistically significant benefit at 48 weeks Not Studied
ADAS-cog difference vs. placebo at 24 weeks* 1.66 points (p = 0.007)
2.16 points (p = 0.004)
ADCS-ADL difference vs. placebo at 24 weeks* 2.18 points (p = 0.016)
1.72 points (p = 0.12)
Dose and dosing schedule in Phase 3 same as Phase 2 Lundbeck Phase 3: 1x/day, dose-ranging (10 mg, 30 mg, 60 mg total daily dose) ×
1Wilkinson et al., The Lancet Neurology 2014, Vol. 13, 1092-1099. *LADDER covariates used for both RVT-101 and Idalopirdine
Pipeline Expansion Creates Global Leadership in Development of Lewy Body Dementia Therapies
• Potential best-in-class 5HT2A receptor inverse agonist
• Pursuing a larger potential market than pimavanserin
• Differentiated profile relative to pimavanserin and other competitors
Acquired Global Rights to Nelotanserin
• Expected study initiation: Q1 2016
• Potentially only one study required for approval in DLB*
• Opportunity for additional meaningful effects at higher doses
Initiating RVT-101 Phase 2b Study in DLB
• Axovant is developing the two leading programs in LBD
• Potential for RVT-101 and nelotanserin to become the first two drugs approved by FDA and EMA to treat DLB
• Multiple catalysts expected in 2016 and 2017
Significant Synergies Across Programs
*If the results of this study are successful, we believe that in conjunction with the Alzheimer’s disease NDA package it could serve as the basis to seek approval of RVT-101 in DLB.
14
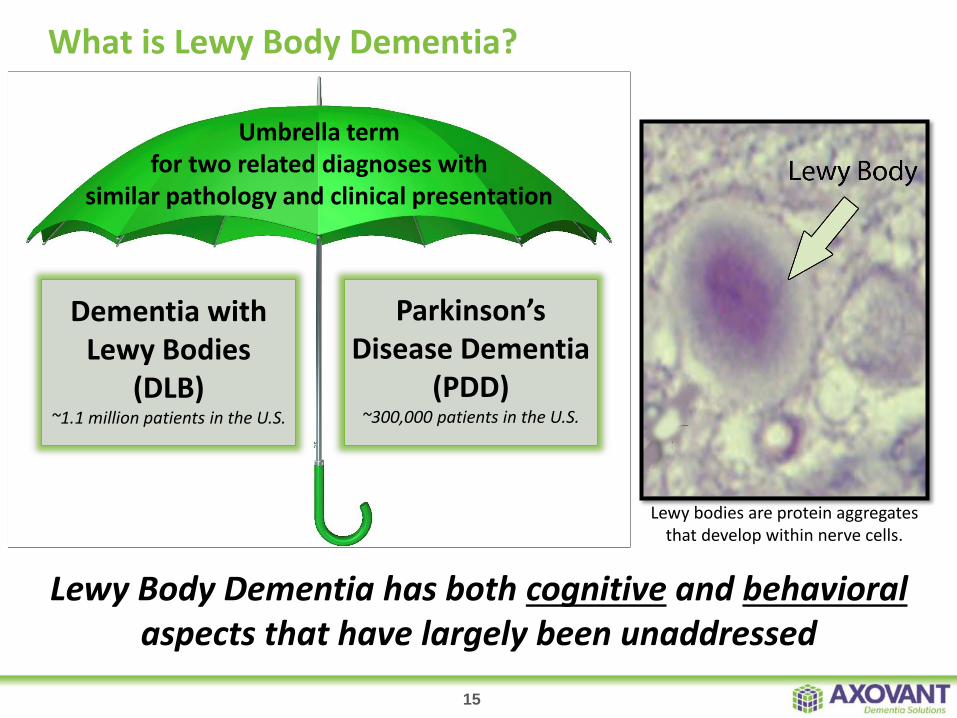
Lewy Body Dementia has both cognitive and behavioral aspects that have largely been unaddressed
What is Lewy Body Dementia?
Dementia with Lewy Bodies
(DLB) ~1.1 million patients in the U.S.
Umbrella term for two related diagnoses with
similar pathology and clinical presentation
Parkinson’s Disease Dementia
(PDD) ~300,000 patients in the U.S.
15
Lewy bodies are protein aggregates that develop within nerve cells.
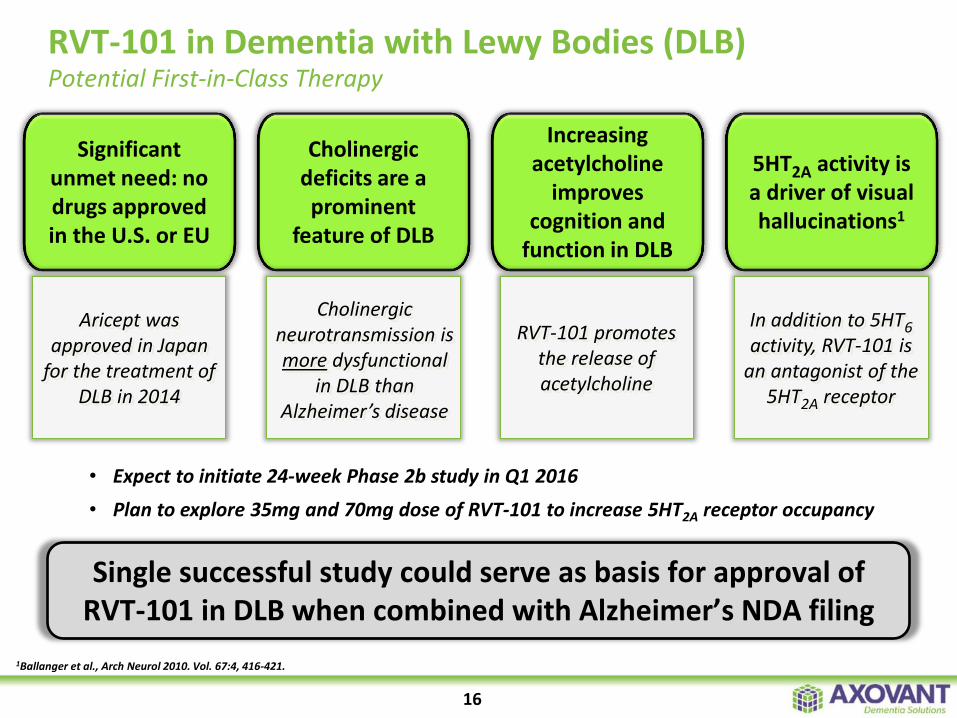
• Expect to initiate 24-week Phase 2b study in Q1 2016
• Plan to explore 35mg and 70mg dose of RVT-101 to increase 5HT2A receptor occupancy
RVT-101 in Dementia with Lewy Bodies (DLB) Potential First-in-Class Therapy
Cholinergic deficits are a prominent
feature of DLB
Cholinergic neurotransmission is more dysfunctional
in DLB than Alzheimer’s disease
RVT-101 promotes the release of acetylcholine
Increasing acetylcholine
improves cognition and
function in DLB
Significant unmet need: no drugs approved in the U.S. or EU
Aricept was approved in Japan
for the treatment of DLB in 2014
5HT2A activity is a driver of visual hallucinations1
In addition to 5HT6 activity, RVT-101 is
an antagonist of the 5HT2A receptor
1Ballanger et al., Arch Neurol 2010. Vol. 67:4, 416-421.
Single successful study could serve as basis for approval of RVT-101 in DLB when combined with Alzheimer’s NDA filing
16
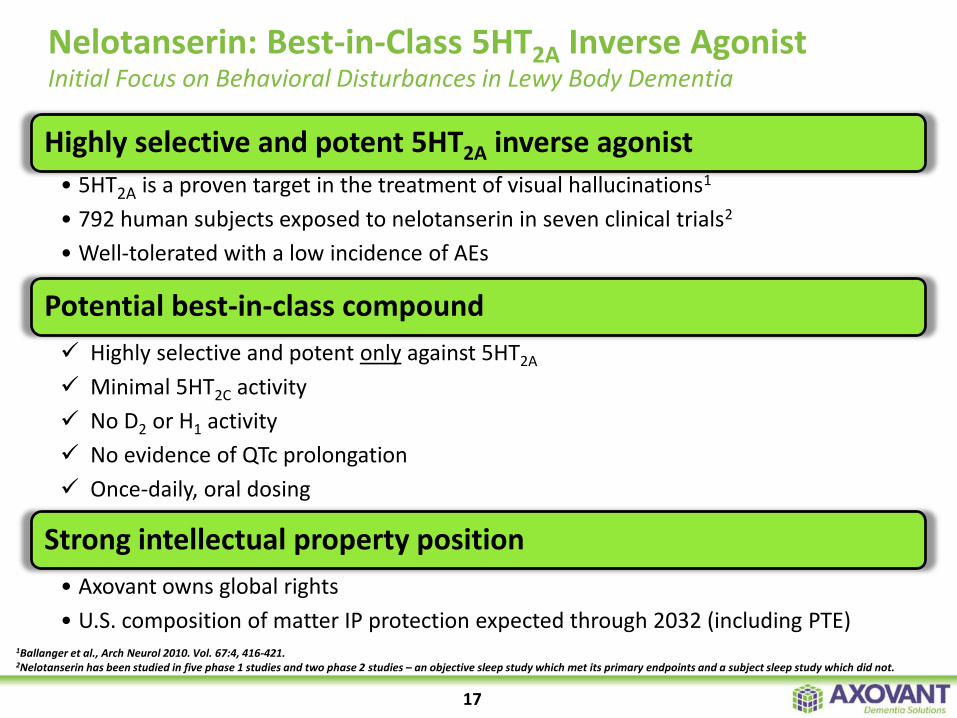
Highly selective and potent 5HT2A inverse agonist
• 5HT2A is a proven target in the treatment of visual hallucinations1
• 792 human subjects exposed to nelotanserin in seven clinical trials2
• Well-tolerated with a low incidence of AEs
Potential best-in-class compound
Highly selective and potent only against 5HT2A
Minimal 5HT2C activity
No D2 or H1 activity
No evidence of QTc prolongation
Once-daily, oral dosing
Strong intellectual property position
• Axovant owns global rights
• U.S. composition of matter IP protection expected through 2032 (including PTE)
Nelotanserin: Best-in-Class 5HT2A Inverse Agonist Initial Focus on Behavioral Disturbances in Lewy Body Dementia
17
1Ballanger et al., Arch Neurol 2010. Vol. 67:4, 416-421. 2Nelotanserin has been studied in five phase 1 studies and two phase 2 studies – an objective sleep study which met its primary endpoints and a subject sleep study which did not.
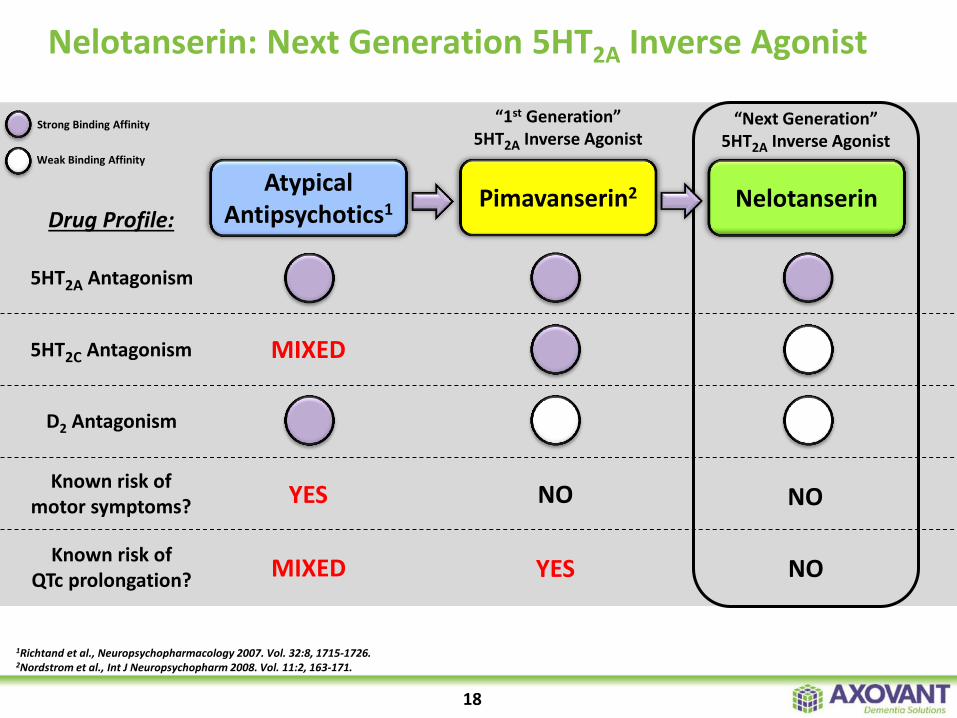
Nelotanserin: Next Generation 5HT2A Inverse Agonist
5HT2A Antagonism
5HT2C Antagonism
Known risk of motor symptoms?
D2 Antagonism
Nelotanserin
NO
“Next Generation” 5HT2A Inverse Agonist
Atypical Antipsychotics1
YES
Strong Binding Affinity
Weak Binding Affinity
Pimavanserin2
NO
“1st Generation” 5HT2A Inverse Agonist
Known risk of QTc prolongation? MIXED YES NO
Drug Profile:
MIXED
18
1Richtand et al., Neuropsychopharmacology 2007. Vol. 32:8, 1715-1726. 2Nordstrom et al., Int J Neuropsychopharm 2008. Vol. 11:2, 163-171.
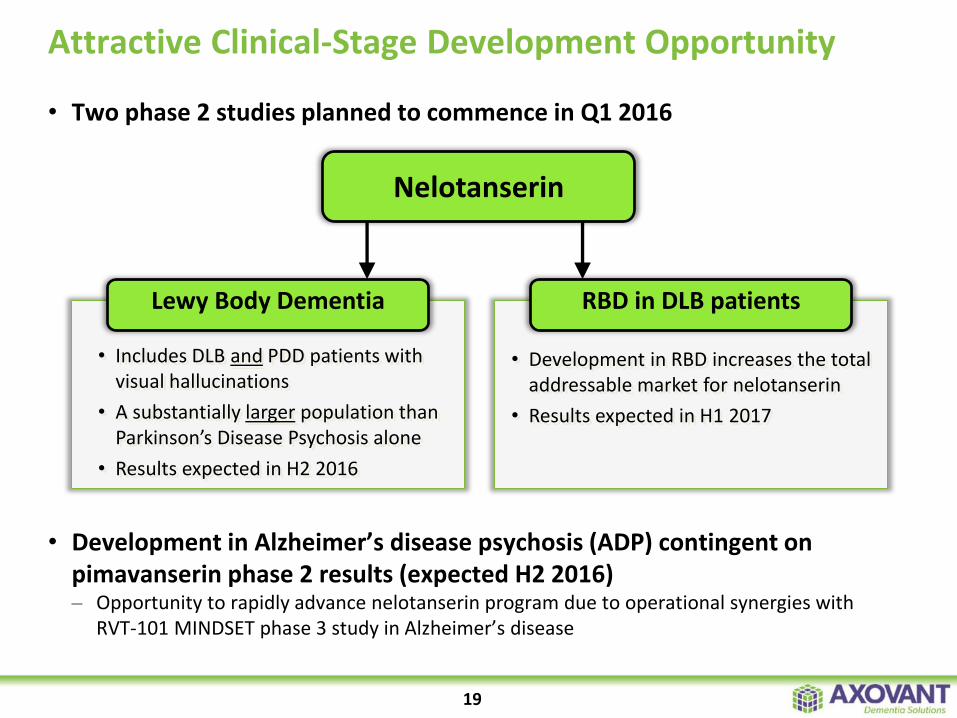
• Two phase 2 studies planned to commence in Q1 2016
• Development in Alzheimer’s disease psychosis (ADP) contingent on pimavanserin phase 2 results (expected H2 2016) – Opportunity to rapidly advance nelotanserin program due to operational synergies with
RVT-101 MINDSET phase 3 study in Alzheimer’s disease
Attractive Clinical-Stage Development Opportunity
• Includes DLB and PDD patients with visual hallucinations
• A substantially larger population than Parkinson’s Disease Psychosis alone
• Results expected in H2 2016
19
• Development in RBD increases the total addressable market for nelotanserin
• Results expected in H1 2017
Lewy Body Dementia RBD in DLB patients
Nelotanserin
Progress in Building a Dementia Solutions Company
Axovant: The Leader in Lewy Body Dementia
20
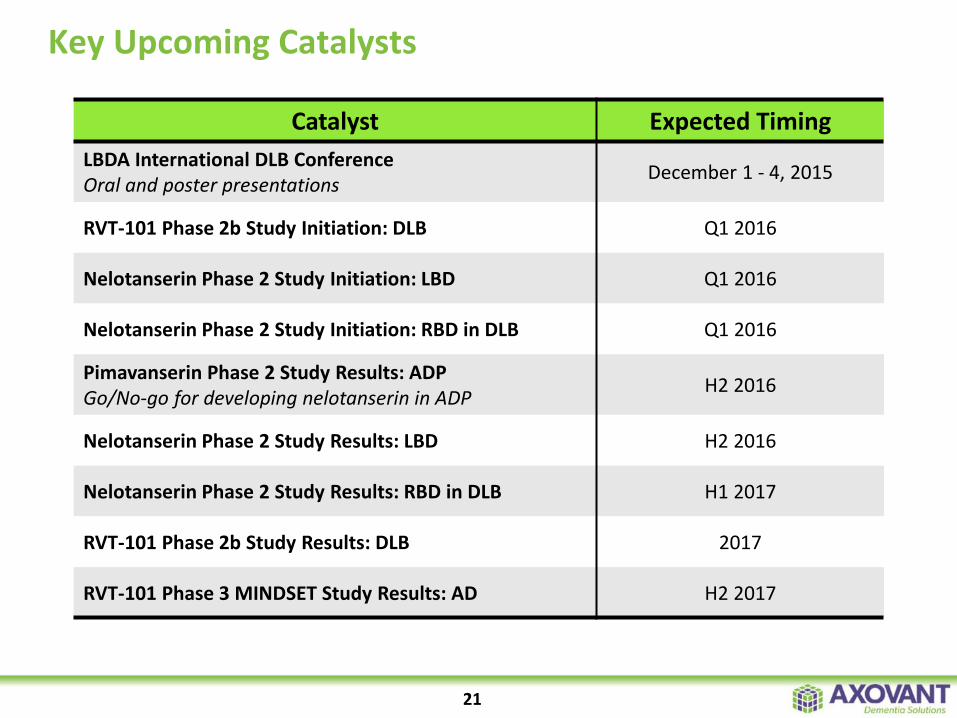
Key Upcoming Catalysts
Catalyst Expected Timing
LBDA International DLB Conference Oral and poster presentations
December 1 - 4, 2015
RVT-101 Phase 2b Study Initiation: DLB Q1 2016
Nelotanserin Phase 2 Study Initiation: LBD Q1 2016
Nelotanserin Phase 2 Study Initiation: RBD in DLB Q1 2016
Pimavanserin Phase 2 Study Results: ADP Go/No-go for developing nelotanserin in ADP
H2 2016
Nelotanserin Phase 2 Study Results: LBD H2 2016
Nelotanserin Phase 2 Study Results: RBD in DLB H1 2017
RVT-101 Phase 2b Study Results: DLB 2017
RVT-101 Phase 3 MINDSET Study Results: AD H2 2017
21

CONFIDENTIAL