Embed Size (px)
Citation preview

Vitamin D
Simon Pearce
Consultant Endocrinologist, RVI, Newcastle

Vitamin D
• Basic background
• Public health
• Cases & Clinical scenarios

Synthesis, activation & action
Skin Liver Kidney
Active vitamin D hormone
Calcium & skeletal
homeostasis
Immune system tissues
Metabolic & vascular
tissues
CellularHomeostasis& apoptosis

Vitamin D- natural sources
• Ergocalciferol– ‘Vitamin D2’– UV irradiated fungi/ yeast
• Colecalciferol– ‘Vitamin D3’– UV irradiated plankton– UV irradiated animal skin/ fur

• >90% of humankind’s vitamin D comes from UV-B exposure of skin
• 20-30 min of direct skin exposure to midday sun on face and arms, 2 or 3 times weekly provides sufficient for a fair-skinned person
• Above 43oN, the angle of sun to atmosphere filters out useful UV wavelengths between October and April.
Vitamin D- natural sources

• Sun block lotion SPF-8 prevents 95% of dermal vitamin D synthesis
• Wearing a hat, veil or head scarf very substantially reduce skin vitamin D synthesis
• Pigmented skin or elderly (thin skin) needs more exposure for same vit D production
• Impossible to overdose on skin synthesised vitamin D; possible to sunburn
Vitamin D- natural sources

Scale of the public health problem
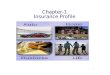
• Seasonal & geographic variation in prevalence of 25-OHD <40nmol/L• MRC 1958 birth cohort at age 45yrs =7437 whites• Spring nadir for 25OHD <20 nmol/L =16%
<50 nmol/L =50%
Hyppönen & Power 2007

Vitamin D- natural sources
• Food– Oily fish (top of the marine ecosystem)– Salmon, trout, mackerel, herring, fresh tuna, sardines,
pilchards, anchovies– Fish oils (cod liver oil)
• 2 portions of oily fish weekly (100-125g) sufficient to provide sufficient Vit D
• Less Vitamin D in farmed fish• Heavy metals in some sea fish

Vitamin D- natural sources• Common misconceptions
– Negligible amount of vit D in milk– None in green vegetables
• Small amounts in Egg yolk (20 yolks per day sufficient)
• Small amount in mushrooms (100 per day sufficient)• Small amounts in animal liver (inc. seal liver)
• Statutory supplementation in UK– Infant milk formula (500 IU/l)– Margarines (150-300 IU/100g)

How to determine vitamin D status?
• Measure serum 25 hydroxyvitamin D (25-OHD)– Robust marker of vit D stores– Half-life 3-4 weeks
• Don’t measure 1,25 dihydroxyvitamin D– Active ‘D hormone’– Circulating levels reflect PTH action and calcium
supply– Often falsely normal or even elevated in D
deficiency

How to determine vitamin D status?
25-OHD
(nmol/l)
Vit D status Manifestation Action
<25 Deficient Rickets
Osteomalacia
Treat with
high dose D
25-50 Insufficient Associated with disease risk
Supplement with vit D
50-75 Adequate Healthy Lifestyle advice
>75 Optimal Healthy None

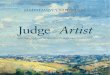
Interpretation of serum 25-OHD
Hypponen & Power 2007
Men (n=3725)
Women (n=3712)
• UK-wide white cohort born 1958

Interpretation of serum 25-OHD
Hypponen & Power 2007
Men (n=3725)
Women (n=3712)
• UK-wide white cohort born 1958

Case 1

35 yo, Pakistani-born Lady
• Living in Fenham for 11 yrs
• Migratory aches and pains, hips, legs, back during 3rd pregnancy
• GP re-assured, but ? Depressed
• 4/12 post partum-feels low, aches and pains persist= Fluoxetine 20mg od
• Presents limping, with pain in R hip

GP did blood tests
• Calcium =1.89 mmol/l (2.12-2.6)
• Alk Phos = 231 KIU/l (<120)
• Rh factor negative
• Refer endocrinology

Endocrinology blood tests
• PTH 684 ng/l
• 25-OH vitamin D = 7 nmol/l
• Diagnosis = Osteomalacia

Generalised Aches & Pains =not always depressionSievenpiper J et al. BMJ

Treatment
• Oral ergocalciferol 10,000 IU daily for 3 months
• Feels a lot better, aches and pains gone, smiling in clinic
• But……..

• After topping up her vitamin D levels, she will need long-term maintenance
– 1000 to 2000 IU calciferol daily– Regular sunlight exposure
• Don’t forget the baby: who was slow to walk and had rickets with tibial deformities

NICE antenatal care guideline

Case 2

20 month old girl
• Mother reports lower limb deformity
• 4th child, term birth, no problems
• Breast fed until 8 months
• Pain on walking, difficulty climbing stairs
• Nigerian mother, asylum seeker housed in tower block
• 3 older brothers born in Nigeria, no problems

• Ca 1.92 mmol/l (2.3-2.7)• PO4 1.26 mmol/l (1.1-1.85)• Alk Phos 1077 KIU/l (<375)
• Treatment
• Ergocalciferol oily solution, 3,000 IU/ml. 2mls daily
• Mother and brothers, also to take supplements: Dalivit 0.6 mls daily

Healthy Start/ Sure Start
• The UK health departments recommend a daily dose of vitamins A, C and D for:– breastfed infants from 6 months (or from 1 month if there is any doubt
about the mother's vitamin status during pregnancy)– formula-fed infants who are over 6 months and taking less than 500
ml infant formula per day– children under 5 years of age
• This recommendation is particularly important for children who are picky or fussy eaters, those of Asian, African, Afro-Caribbean or middle eastern origin and those living in northern areas of the UK.


Case 3

45 yo woman
• Multiple sclerosis diagnosed age 29
• Only 2 major attacks
• Feeling increasingly weak for 30 months• Painful to move legs, can’t stand up• Using wheelchair, even in house• Needs husband to pull her out of bed in
morning

Fell out of bed one day• Wedge # of L2 vertebral body
• BMD measured; T score -3.4 at spine
• Bone chemistry• (PTH 43)
• Treated with calcichew D3 one daily
Serum Feb April
Calcium 2.60 2.30
PO4 1.11 0.77
Alk Pase 62 48
25-OHD 10 11

• Allergic to fish; none since teenager
• Not really leaving the house due to mobility
• No overseas holiday for 5 yrs

Treatment• Oral colecalciferol 20,000 IU capsules, 3 per week
(Dekristol; pharmacy special order, approved by APC)
• Vomiting and diarrhoea (contains fish oil!)
• IM ergocalciferol 300,000 IU monthly for 3 months, • Oral vitamin D3 2 x 25ug capsules daily (2000 IU)
from Holland and Barrett
• 1 year later; walks unaided up to 200 m, no pain

How to determine vitamin D status?
25-OHD
(nmol/l)
Vit D status Manifestation Action
<25 Deficient Rickets
Osteomalacia
Treat with
high dose D
25-50 Insufficient Associated with disease risk
Supplement with vit D
50-75 Adequate Healthy Lifestyle advice
>75 Optimal Healthy None


Also OTC Boots (12.5 ug capsules) £2.99 for 90Holland & Barrett (25 ug capsules) £6.99 for 100

Dosing issues
• 100 IU calciferol daily increases serum 25-OHD by 2.5 nmol/l
• RDA is 400 IU (10 ug)• Increase serum 25-OHD by 10 nmol/l
• Typical Newcastle patient with vitamin D insufficiency has levels between 20 and 30 nmol/l
• Need to aim for 70 nmol/l or better• Toxicity seen at levels of 500 nmol/l or higher• 1- 2000 IU daily is appropriate maintenance dose
(Adults)

Tips on treatment
• Most people who you suspect are D deficient, are D deficient
• Supplementation is not the same as treatment
• If a child has rickets, the siblings and mother should also be treated
• Compliance with calcium containing preparations (calcichew D3) is poor, better to prescribe D only compounds for longterm use

The End

Questions
• Is it worth screening all new patients from overseas at risk of vit D?
-When people first arrive, they aren’t deficient
-Probably takes 5 years or a pregnancy to manifest severe D deficiency
-Worth giving dietary/sunlight exposure advice to all at risk groups

Questions
• Treatment- injection vs oral medication and how long for?
-Oral is better (all round); but current supply issues.
-In severe deficiency a short course of monthly IM insures treatment is received
-If GI problem, IM worthwhile

Questions
• How often to monitor bloods once on treatment?
-Depends on manifestations, but maybe never or once in a year until dietary intake is no longer an issue
-If Alk. Phos raised, recheck in 3 and 6 months; although it may take longer to normalise

Questions
• When to refer?- and who to endocrine vs bone clinic
- Doubt about diagnosis; conflicting biochem (eg. Hypercalcaemia)
- Failure to respond to treatment- Other nutritional issues (IDA frequently co-exists)- Childhood with bone disease- Vitamin D is actually a hormone

Questions
• Patients with aches and pains and confirmed vit D def- should we be x-raying joints
I generally don’t, unless there is very localised pain (not generalised aches & pains)
Pain not improved by 3 months treatment should trigger an X-ray

Dosing of colecalciferol in Autumn
From Heaney RP et al.
Placebo
10,000 U/d
5,000 U/d
1,000 U/d