-
8/20/2019 Vitamin D _ NEJMGroup_Collection
1/35
Vitamin DTo Supplement, orNot to Supplement?
https://collections.nejm.org/http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
2/35
the new england
journal of medicine
nejm journal watch
Cardiology
Dermatology
Emergency Medicine
Gastroenterology
General MedicineHospital Medicine
Infectious Diseases
Neurology
Oncology and Hematology
Pediatrics and Adolescent Medicine
Physician’s First Watch
Psychiatry
Women’s Health
nejm careercenter
nejm knowledge+
VITAMIN D COLLECTION
Too often in medicine (and life) definitive answers prove
elusive. Having some guidance allows
us to proceed down an uncertain road. Our collections are meant
to provide such guidance, and
so we begin with vitamin D — a topic that confuses and
confounds.
The thrust of this collection addresses topics relevant to
non-specific vitamin D supplementation
in broad populations who don’t have symptoms clearly known to
reflect deficiency (e.g., bone
pain not otherwise explained) or conditions known to be
associated with low vitamin D levels
(e.g., gastrointestinal malabsorption). Obviously, clinicians
should measure vitamin D levels in
those sorts of cases.
Observational studies have looked for — and discovered —
correlations between various chronicdiseases and low vitamin D
levels, but these are generally plagued by not being able to
establish
causality with certainty. Short-term randomized trials have
asked whether supplementation prevents
various conditions, ranging from upper respiratory
infections to asthma exacerbations to progres-
sion of knee osteoarthritis. These trials have generally found
no benefit from supplementation.
An ongoing trial — the VITAL study (NCT01169259) — may well
settle the question of whether
to supplement routinely or not. In that study, some 26,000
people aged 50 and older are receiving
2000 IU of vitamin D daily or placebo to determine whether
supplementation can lower the
incidence of cancer or cardiovascular disease. Unfortunately,
the results are still about 5 years
away. So, although vitamin D’s importance to health is
unquestioned, no one has shown exactly
how much the human body requires or exactly who would benefit
from routine supplementation.
The collection includes articles from NEJM Journal Watch, the
New England Journal of Medicine , and
Physician’s First Watch. (The editors of NEJM Journal Watch
survey, summarize, and comment on
studies from a wide range of journals; Physician’s First Watch
is our news arm.)
Our selection raises some questions that cannot yet be answered
definitively. Nevertheless, we
believe that this material will help practicing clinicians
navigate the uncertainty and controversy
surrounding vitamin D with more confidence.
— Joe Elia
Contributing writer, Physician’s First Watch
Host, Clinical Conversations
— Allan S. Brett, M.D.
Editor-in-chief, NEJM Journal Watch General Medicine
Professor of Medicine,
University of South Carolina School of Medicine
— Clifford J. Rosen, M.D.
Associate Editor, New England Journal of Medicine
Director of Clinical and Translational Research,
Maine Medical Center
July 2015
http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
3/35
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
4/35
4
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Back to Table of Contents
Clinical Collections — Vitamin D
14 Revisiting Variability in Measurement of Vitamin D
Levels On average, serum 25- hydroxyvitamin D levels differed
by 5 ng/mL across two assays.
NEJM Journal Watch General Medicine Apr 10, 2012
What’s the Threshold for Serum 25-OH Vitamin D
Levels below Which Thereis an Association with Lower Bone Density
or Abnormalities in Bone Turnover?
15 At What Level of Vitamin D Does Fracture Risk Rise? In
older men, fracture risk was elevated only among those with serum
25-hydroxyvitamin D levels
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
5/35
5
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
What Does the U.S. Preventive Services Task Force
(USPSTF) Have to Sayabout Screening for Vitamin D Deficiency in the
General Population?
23 USPSTF: Evidence Is Insufficient to Recommend Routine
Screening for Vitamin DDeficiency
Physician’s First Watch Jun 24, 2014
FINAL OVERVIEW AND LESSONS FROM THE CLINIC
25 NEJM Clinical Practice: Vitamin D Insufficiency
New England Journal of Medicine Jan 20, 2011
32 Correspondence: Vitamin D Insufficiency New
England Journal of Medicine Apr 7, 2011
http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
6/35
Back to Table of Contents
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Clinical Collections — Vitamin D Source: Te New England
Journal of Medicine
WHAT’S THE BOTTOM LINE ON VITAMIN D SUPPLEMENTS?
The VITAL Study may well settle the question of whether to
supplement or not. In that study, some
26,000 men and women aged 50 and older are receiving vitamin D
supplements or omega-3 fatty acids (or
both, or placebos) to determine whether they show a change in
risk for cancer and cardiovascular disease.
Unfortunately, the VITAL Study’s results are roughly 5 years
away.
The watchword here is “wait,” in the meantime we have some
information to help you cope.
6
Skin
Liver
Kidney
Food(vitamins D2 and D3)
Provitamin D3 Previtamin D3
Vitamin D3
25-Hydroxylase (CYP2R1)
24-Hydroxylase(CYP24R1)
1α-Hydroxylase(CYP27B1)
25(OH)D3
Increased PTH,decreasedphosphate
FGF-23 Calcitriol
Biologic Activity
24,25(OH)2D3
– +
Sunlight
+ ––
l
:
i
i l
i
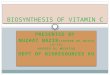
Figure 1. Synthesis and Metabolism of Vitamin D.
Vitamin D is initially generated in the skin from the non-
enzymatic conversion of provitamin D3 to previtamin
D3.Dietary intake of vitamin D is usually relatively limited,
since few foods, with the exception of certain kinds of
fish, contain sizable amounts; supplements are com-
monly used. Vitamin D is either stored in adipose tis-sue or
converted in the liver by the enzyme 25-hydroxy-
lase to 25-hydroxyvitamin D3 (25[OH]D3), the form
that circulates in the highest concentration and reflectssolar
and dietary exposure. It is converted to the active
metabolite, 1,25-dihydroxyvitamin D (1,25[OH]2D), or
calcitriol, in the kidney, although other tissues
have1α-hydroxylase enzymatic activity. The synthesis of
calcitriol is enhanced (+) by increasing levels of para-
thyroid hormone (PTH), which rise in response to lowerlevels of
serum calcium. Reduced levels of serum phos-
phate can also increase (+) the production of calcitriol.
Its synthesis is suppressed (–) by the production of fi-broblast
growth factor 23 (FGF-23), which is secreted
by osteocytes in the bone matrix. Calcitriol inhibits the
activity of 1α-hydroxylase (CYP27B1) and stimulates the
activity of 24-hydroxylase (CYP24R1), an enzyme that pro-motes
production of 24,25(OH)
2D3, a vitamin D prod-
uct that is not biologically active. In CYP2R1, CYP27B1,
and CYP24R1, CYP denotes cytochrome P.
Source: NEJM Clinical Practice ar ticle“Vitamin D Insuff
iciency” on page 26
http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
7/35
7
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Vitamin D Supplementation Prevents FracturesA meta-analysis
suggests benefit at a dose of >800 IU daily, but factors
relating to treatment adherencecould have biased the results.
Bischoff-Ferrari HA et al. A pooled analysis of vitamin D dose
requirements for fracture prevention. N Engl J Med 2012 Jul 5;
367:40.
( http://dx.doi.org/10.1056/NEJMoa1109617)
Heaney RP. Vitamin D — Baseline status and effective dose. N
Engl J Med 2012 Jul 5; 367:77.
( http://dx.doi.org/10.1056/ NEJMe1206858)
ARTICLE SUMMARY
Clinical trials have not consistently confirmed that vitamin D
supplementation in older adults prevents fractures.
To reconcile conflicting data, researchers pooled
participant-level data from 11 randomized controlled trials of
vitamin D supplementation that involved 31,000 older
people (age, ≥65).
In intent-to- treat analyses, vitamin D supplementation lowered
risks for hip fracture (hazard ratio, 0.90; P=0.07)
and any nonvertebral fracture (HR, 0.93; P=0.03), but these
reductions were not significant (for statistical rea-
sons, a P -value of 0.0125 was considered significant).
However, the researchers conducted additional
analyses that incorporated treatment adherence and supplement
use outside the trial: Participants in the highest
quartile of daily vitamin D intake (median, 800 IU; range,
792–2000) did have significantly lower risks for both
hip fracture (HR, 0.70) and any nonvertebral fracture (HR, 0.86)
, compared with controls. In contrast, partici-
pants in the lowest three quartiles did not benefit from vitamin
D supplementation. Some trials also involved
calcium supplementation, but the vitamin D findings were
independent of additional calcium intake. Vertebral
fractures were not documented consistently in these trials.
COMMENT
These data suggest a threshold dose of about 800 IU of vitamin D
daily for fracture prevention in older adults. The
pooling of participant-level data, plus the incorporation of
information on adherence and supplement use outside
the trial, distinguish this analysis from previous ones.
However, the departure from intent-to-treat analysis could
be a problem here. The subgroup with the highest vitamin D
intake was compared with all controls; thus, the
analysis probably compared a high-adherence population to a
mixed-adherence population and, if adherence is amarker for better
health or healthier behaviors, this fact could confound the
results. An editorialist adds that, for
any given dose of supplemental vitamin D, a person with baseline
deficiency is more likely to benefit than a person
whose baseline vitamin D status is adequate.
— Allan S. Brett, MD
University of South Carolina School of Medicine, Columbia
NEJM Journal Watch General Medicine , published July
10,2012
WHAT CAN VITAMIN D DO, AND WHAT CAN’T IT DO?
Does Vitamin D Supplementation Lower Risk of Fractures?
Although the meta-analysis summarized below suggests that it
does, the results were generally of borderline
significance — and thus not 100 percent decisive.
http://www.jwatch.org/cgi/content/full/2012/0/JW201207100000001?ijkey=fjSFnjqr7nHk.&keytype=ref&siteid=jwatchhttp://www.nejmgroup.org/http://www.jwatch.org/cgi/content/full/2012/0/JW201207100000001?ijkey=fjSFnjqr7nHk.&keytype=ref&siteid=jwatch
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
8/35
8
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
When It Comes to Bone, Vitamin D Supplementation Falls ShortIn a
large meta-analysis, vitamin D supplementation generally did not
increase bone-mineral density.
Reid IR et al. Effects of vitamin D supplements on bone mineral
density: A systematic review and meta-analysis. Lancet 2013
Oct 11;
[e-pub ahead of print].
( http://dx.doi.org/10.1016/S0140-6736(13)61647-5 )
ARTICLE SUMMARY
Calcium supplements, which are taken by nearly half of U.S.
adults for skeletal benefits, often include vitamin D.
However, the role of vitamin D supplementation itself in
maintaining bone quality remains unclear: Vitamin D
supplements have not lowered fracture risk, and their effect on
bone-mineral density (BMD) has varied. In a
meta-analysis, investigators combined data from 23 randomized
controlled trials (4082 adult participants; 92%
women) in which BMD was a measured outcome and in which
inclusion or dose of vitamin D varied. Studiesdiffered in patients’
mean baseline 25-hydroxyvitamin D level, vitamin D dose and
duration, and concomitant
interventions (primarily calcium supplementation).
Patients who took vitamin D supplements had significantly
greater increases in BMD at the femoral neck but not
at the total hip, lumbar spine, forearm, or total body. Vitamin
D supplementation was associated with significant-
ly greater increases in BMD at the total hip in studies where
mean baseline 25-hydroxyvitamin D level was 20 ng/mL do not require
supplementation.
— Bruce Soloway, MD
Montefiore Medical Center, New York
NEJM Journal Watch General Medicine , published October 22,
2013
Does Vitamin D Supplementation Improve Bone Density?
http://www.jwatch.org/na32572/2013/10/22/when-it-comes-bone-vitamin-d-supplementation-falls-shorthttp://dx.doi.org/10.1016/S0140-6736(13)61647-5http://www.nejmgroup.org/http://dx.doi.org/10.1016/S0140-6736(13)61647-5http://www.jwatch.org/na32572/2013/10/22/when-it-comes-bone-vitamin-d-supplementation-falls-short
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
9/35
9
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Vitamin D Appears to Prevent Falls in Some High-Risk
SubgroupsThe benefit appeared limited to those who received >800
IU of vitamin D daily.
Murad MH et al. The effect of vitamin D on falls: A
systematic review and meta-analysis. J Clin Endocrinol
Metab 2011 Oct;
96:2997. (http://dx.doi.org/10.1210/jc.2011-1193)
ARTICLE SUMMARY
Some, but not all, studies have shown that vitamin D
supplementation reduces risk for falls in elders, presumably
through direct effects on muscle function. Researchers performed
this meta-analysis of 26 randomized controlled
trials of vitamin D supplementation that reported falling as one
outcome. The mean age of the 46,000 participants
was 76, 78% of participants were women, and median duration of
vitamin D administration was 1 year. Baseline
risk for falling was high in these trials.
Vitamin D was associated with a significant reduction in risk
for falling (odds ratio for risk of at least one fall,
0.86). In prespecified subgroup analyses, this benefit was seen
primari ly in patients who also received calcium
supplementation and in those with vitamin D deficiency at
baseline (but definitions of deficiency varied across
studies). Although the benefit appeared limited to those who
received >800 IU of vitamin D daily (compared
with lower doses), the interaction between dose and falls did
not reach statistical significance.
COMMENT
This analysis suggests that vitamin D supplementation —
administered with calcium — reduces risk for falling,
particularly among older vitamin D– deficient women who are at
high baseline risk for fall ing. The findings thus
support selective use of vitamin D in such patients. However,
the authors believe that the quality of the evidence is
low to moderate due to publication bias, heterogeneity across
studies, and several other factors.
— Allan S. Brett, MD
University of South Carolina School of Medicine, Columbia
NEJM Journal Watch General Medicine , published October 27,
2011
Does Vitamin D Supplementation Prevent Falls in Elderly
People?
Based on results of some clinical trials, there is general
belief that vitamin D supplements reduce risk of falls
in elderly patients — presumably through an effect on muscle
function. Yet even here, the evidence is con-
troversial. For example, the meta-analysis summarized on this
page suggested a statistically significant 14%
reduction in falls among patients receiving vitamin D treatment,
while the meta-analysis on the next page
showed a 5% reduction that was not significant. If any benefit
exists, it is likely to be relatively modest and
limited to vitamin-D-deficient patients with high baseline risk
for falling.
http://www.jwatch.org/cgi/content/full/2011/0/JW201110270000006?ijkey=927IpU0ljl6WY&keytype=ref&siteid=jwatchhttp://www.nejmgroup.org/http://www.jwatch.org/cgi/content/full/2011/0/JW201110270000006?ijkey=927IpU0ljl6WY&keytype=ref&siteid=jwatch
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
10/35
10
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Back to Table of Contents
Clinical Collections — Vitamin D Source: NEJM Physician’s
First Watch
No Effect of Vitamin D Supplements for Fall Risk
Boland MJ et al. Vitamin D supplementation and falls: a trial
sequential meta-analyses. Lancet Diabetes Endocrinol 2014;
2:573.
(http://www.thelancet.com/journals/landia/article/PIIS2213-8587%2814%2970068-3/abstract)
ARTICLE SUMMARY
Vitamin D supplementation does not appear to reduce the risk for
falls in older adults, a trial sequential analysisin the Lancet
Diabetes & Endocrinology finds. This is contrary to
guidance from the U.S. Preventive Services Task
Force.
Nearly 30,000 older adults participated in 20 randomized trials
that looked at the effect of vitamin D supplemen-
tation — with or without calcium — on the risk for falls.
Vitamin D supplementation did not reduce the incidence
of falls by 15% or more (the prespecified threshold for clinical
relevance). Calcium also had no effect.
The authors write that there is “little justification” for using
vitamin D for fall prevention. Commentators con-
clude that until a large trial is conducted among adults who are
particularly vulnerable to falls, “we are left with
uncertainty about the benefits of vitamin D supplementation for
reduction in fall risk.”
— Kelly Young
Physician’s First Watch , published April 24, 2014
http://www.jwatch.org/fw108748/2014/04/24/no-effect-vitamin-d-supplements-fall-riskhttp://www.nejmgroup.org/http://www.jwatch.org/fw108748/2014/04/24/no-effect-vitamin-d-supplements-fall-risk
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
11/35
11
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
No Benefit of Vitamin D Supplementation for Knee OsteoarthritisA
2-year study might have been too short, but results still are
discouraging.
McAlindon T et al. Effect of vitamin D supplementation on
progression of knee pain and cartilage volume loss in patients
with
symptomatic osteoarthritis: A randomized controlled trial.
JAMA 2013 Jan 9; 309:155. (http://jama.jamanetwork.com/
article.aspx?articleid=1556148)
ARTICLE SUMMARYDisruption of normal bone architecture in knee
osteoarthritis (OA), combined with certain epidemiologic obser-
vations, led investigators to study the potential benefit
of vitamin D supplementation in 146 adults with knee OA
(mean age, 63; mean baseline 25-hydroxyvitamin D [25(OH)D]
level, 22 ng/mL; most with knee malalignment
and moderate-to-severe joint space narrowing and sclerosis).
Participants were randomized to cholecalciferol
(vitamin D3; 2000 IU daily) or placebo. Dosages in the
intervention group were adjusted to achieve 25(OH)D
levels >36 ng/mL; doses as high as 6000 –8000 IU daily were
required in several participants.
More than 80% of each group completed the 2-year trial, at which
time knee pain was diminished slightly in both
groups. No difference was found between the groups in pain,
function, or loss of cartilage volume.
COMMENT
Perhaps 2 years was too little time, or the participants’
baseline vitamin D levels were not low enough, or their
os-teoarthritis was too severe to permit detection of benefit —
still, epidemiologic studies published during this study
were less positive than those that inspired it in the first
place. Although bone metabolism was the biological basis
for exploring the benefit of vitamin D on knee OA, an
alternative explanation that merits further study is the ef-
fect of vitamin D on neuromuscular fitness (which might help
protect the knee before or during the onset of OA).
— Thomas L. Schwenk, MD
University of Nevada School of Medicine
NEJM Journal Watch General Medicine , published January 15,
2013
Is There Evidence that Vitamin D Supplementation Improves
Nonspecific Pain?
In one trial, supplements didn’t improve knee pain; in another
trial, supplements didn’t improve diffuse
musculoskeletal pain; and in an observational study, low vitamin
D levels were not highly correlated with back
or lower-extremity pain.
http://www.jwatch.org/jw201301150000002/2013/01/15/no-benefit-vitamin-d-supplementation-knee?ijkey=RlGofjRr5SA9c&keytype=ref&siteid=jwatch&variant=full-texthttp://www.nejmgroup.org/http://www.jwatch.org/jw201301150000002/2013/01/15/no-benefit-vitamin-d-supplementation-knee?ijkey=RlGofjRr5SA9c&keytype=ref&siteid=jwatch&variant=full-text
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
12/35
12
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Are Low Vitamin D Levels Associated with Nonspecific Pain?The
results of two studies argue against any simple relation between
diffuse pain and vitamin Ddeficiency.
Hicks GE et al. Associations between vitamin D status and pain
in older adults: The Invecchiare in Chianti Study. J Am Geriatr
Soc
2008 May; 56:785.
Warner AE and Arnspiger SA. Diffuse musculoskeletal pain is not
associated with low vitamin D levels or improved by treatment
with
vitamin D. J Clin Rheumatol 2008 Feb; 14:12.
ARTICLE SUMMARY
Observational data have suggested that vitamin D deficiency
might be a common cause of otherwise unexplained
musculoskeletal pain ( Mayo Clin Proc 2003 Dec; 78:1463).
In two new studies, researchers addressed this problem.
In a cross-sectional population-based study, researchers
examined the relation between vitamin D status and pain
in the back, hips, knees, and feet in 958 randomly selected
older adults (age, ≥65) in Italy. Women with low levels
of 25-hydroxyvitamin D (
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
13/35
13
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Measuring Serum Vitamin D Is ProblematicClinicians should be
cautious about drawing conclusions from a single 25-OHD
measurement.
Binkley N et al. Assay variation confounds the diagnosis of
hypovitaminosis D: A call for standardization. J Clin
Endocrinol Metab
2004 Jul; 89:3152-7.
Hollis BW. The determination of circulating 25-hydroxyvitamin D:
No easy task. J Clin Endocrinol Metab 2004 Jul;
89:3149-51.
ARTICLE SUMMARY
Data suggest that vitamin D status is suboptimal among many
adults. Accordingly, some experts advise that clini-
cians measure patients’ serum 25-hydroxyvitamin D (25-OHD)
levels to guide supplementation. How accurate
are such measurements? Researchers approached this question in
several ways:
• Serum from 59 postmenopausal women was sent to either of two
national laboratories. In one laboratory, nearly
all levels were higher than 30 ng/mL; in the other, nearly all
levels were lower than 30 ng/mL.
• Serum from each of 10 healthy young adults was sent to six
different commercial and research laboratories.
One lab measured 25-OHD levels using the gold standard method
(high-pressure liquid chromatography); the
other five used radioimmunoassays and chemiluminescent assays.
The group’s mean 25-OHD level ranged from
17 ng/mL to 36 ng/mL, depending on the laboratory.
• These same 10 specimens were “spiked” with 20 ng/mL of
additional 25-OHD; in the gold-standard lab, spiking
led to an appropriate mean 18 ng/mL increment in the serum
level, but the mean increment was as small as
8 ng/mL in another lab.
COMMENT
Because of substantial variation in laboratory measurement of
25- hydroxyvitamin D levels, accurate diagnosis
of hypovitaminosis D is problematic. Until better
standardization is achieved, clinicians should be cautious
about
drawing conclusions from a single 25-OHD measurement. An
editorialist discusses some of the reasons why
measuring vitamin D accurately is difficult. — Allan S.
Brett, MD
University of South Carolina School of Medicine, Columbia
NEJM Journal Watch General Medicine , published August 13,
2004
WHAT ABOUT VITAMIN D LEVELS?
How Accurate Are the Measurements?
We tend to assume that laboratory measurements of
25-hydroxyvitamin D are accurate, but studies show that
results can vary across labs — sometimes substantially. There’s
no evidence favoring serial measurements of
vitamin D; but if that’s done, we should try to use the
same lab each time, and we shouldn’t make too much
of small fluctuations in blood levels.
http://www.jwatch.org/jw200408130000002/2004/08/13/measuring-serum-vitamin-d-problematic?ijkey=gpMNVGfSLljhY&keytype=ref&siteid=jwatch&variant=full-texthttp://www.nejmgroup.org/http://www.jwatch.org/jw200408130000002/2004/08/13/measuring-serum-vitamin-d-problematic?ijkey=gpMNVGfSLljhY&keytype=ref&siteid=jwatch&variant=full-text
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
14/35
14
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Revisiting Variability in Measurement of Vitamin D LevelsOn
average, serum 25-hydroxyvitamin D levels differed by 5 ng/mL
across two assays.
Barake M et al. 25-hydroxyvitamin D assay variations and impact
on clinical decision making. J Clin Endocrinol Metab 2012
Mar;
97:835. ( http://dx.doi.org/10.1210/jc.2011-2584)
ARTICLE SUMMARY
A 2004 study demonstrated that measurements of serum
25-hydroxyvitamin D (25[OH]D) levels are considerably
variable across different assays. Now, researchers at
Lebanon’s American University of Beirut have revisited this
issue. They measured 25(OH)D levels in each of 494 adults using
both a radioimmunoassay (Immunodiagnostic
Systems RIA; Boldon, U.K.) and an automated chemiluminescent
immunoassay (DiaSorin Liaison; Stillwater,
Minnesota).
Mean 25(OH)D levels were significantly lower with DiaSorin
Liaison than with IDS-RIA (21 vs. 26 ng/mL), and
the proportion of people with serum levels measuring
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
15/35
15
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
At What Level of Vitamin D Does Fracture Risk Rise?In older men,
fracture risk was elevated only among those with serum
25-hydroxyvitamin D levels
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
16/35
16
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Vitamin D Levels and Bone Loss in Older MenIn men older than 75,
25(OH)D levels lower than 20 ng/mL were associated with accelerated
bone loss.
Ensrud KE et al. Serum 25-hydroxyvitamin D levels and rate of
hip bone loss in older men. J Clin Endocrinol Metab 2009
Aug;
94:2773.
ARTICLE SUMMARY
Osteoporotic Fractures in Men is a prospective study of healthy
aging — with a focus on osteoporosis — in
6000 older U.S. men (age, ≥65). In a previous report from that
study, one quarter of participants exhibited
25 hydroxyvitamin D [25(OH)D] levels lower than 20 ng/mL. Now,
the researchers report on the relation
between vitamin D levels and bone loss.
About 1300 participants underwent baseline measurement of serum
25(OH)D and bone-mineral density at the
hip, followed by repeat bone density testing about 4 years
later. After adjustment for potentially confounding vari-
ables, men with baseline 25(OH)D levels
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
17/35
17
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Another Comparison of Vitamin D2 and Vitamin D
3 Supplementation
D3 was somewhat more effective in raising serum levels of
total 25-hydroxyvitamin D.
Lehmann U et al. Bioavailability of vitamin D2 and D
3 in healthy volunteers, a randomized placebo-controlled
trial.
J Clin Endocrinol Metab 2013 Nov; 98:4339.
(http://dx.doi.org/10.1210/jc.2012-4287)
ARTICLE SUMMARY
Vitamin D that is produced naturally from sunlight exposure is
vitamin D3. However, both D
3 (cholecalciferol)
and D2 (ergocalciferol) are available as supplements. In
the U.S., supplemental vitamin D
2 is usually a 50,000 IU
prescription medication, whereas D3 is available over-the-
counter in various doses. With D
3 supplementation,
essentially all measured serum 25-hydroxyvitamin D (25[OH]D) is
hydroxylated D3
. In contrast, with D2
supple-
mentation, total serum 25(OH)D is the sum of supplemental
D2 plus endogenous D
3. Some, but not all, studies
have suggested that supplemental D3 raises total serum
25(OH)D more than supplemental D
2 does.
Researchers randomized 107 healthy volunteers in a northern
German community to receive daily 2000 IU doses
of vitamin D2, vitamin D
3, or placebo during winter months. At 8 weeks, the mean
increase in total 25(OH)D was
significantly greater with D3 supplementation than with
D
2 supplementation (18 vs. 12 ng/mL). Interestingly, the
D2 group’s 12 ng/mL increase in total 25(OH) D reflected
the net result of a 20 ng/mL increase in D
2
but an 8 ng/mL decrease in D3.
COMMENT
In this study, vitamin D3 supplementation raised total
serum 25-hydroxyvitamin D levels more effectively than did
vitamin D2
supplementation. D2
supplementation appeared to suppress endogenous D3
, thus offsetting some of the
expected increment in total serum 25(OH)D. The authors conclude
that D3 should be used for supplementation.
— Allan S. Brett, MD
University of South Carolina School of Medicine, Columbia
NEJM Journal Watch General Medicine , published December
12, 2013
Is There Any Difference between Giving D2 or D
3 Supplements?
http://www.jwatch.org/cgi/content/full/2013/dec12_3/NA33047?ijkey=I1xcD86i8qIFM&keytype=ref&siteid=jwatchhttp://www.jwatch.org/cgi/content/full/2013/dec12_3/NA33047?ijkey=I1xcD86i8qIFM&keytype=ref&siteid=jwatchhttp://www.jwatch.org/cgi/content/full/2013/dec12_3/NA33047?ijkey=I1xcD86i8qIFM&keytype=ref&siteid=jwatchhttp://www.nejmgroup.org/http://www.jwatch.org/cgi/content/full/2013/dec12_3/NA33047?ijkey=I1xcD86i8qIFM&keytype=ref&siteid=jwatch
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
18/35
18
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Which Vitamin D Supplement Boosts Levels More — D2 or D
3?
D3 (cholecalciferol) has the edge.
Binkley N et al. Evaluation of ergocalciferol or cholecalciferol
dosing, 1600 IU daily or 50,000 IU monthly in older adults.
J Clin Endocrinol Metab 2011 Apr; 96:981.
( http://dx.doi.org/10.1210/jc.2010-0015)
Heaney RP et al. Vitamin D3 is more potent than vitamin
D2 in humans. J Clin Endocrinol Metab 2011 Mar;
96:E447.( http://dx.doi.org/10.1210/jc.2010-2230)
ARTICLE SUMMARY
In the U.S., vitamin D supplements are available over-the-
counter as D3 (cholecalciferol; usually in 400–1000 IU
doses) and by prescription as vitamin D2 (ergocalciferol;
Drisdol and others; often prescribed at 50,000 IU doses).
In previous research, D3 supplements raised blood levels of
25-hydroxyvitamin D (25[OH]D) more than D
2 did at
equivalent doses. In two new studies, researchers reach the same
conclusion.
In a randomized trial, 64 older adults received daily D2 or
D
3 (1600 IU) or monthly D
2 or D
3 (50,000 IU). Mean
25(OH)D levels were about 33 ng/mL at baseline. At 1 year, mean
25(OH)D levels had increased by 9 ng/mL in both
the daily and monthly D3 groups; mean levels increased by 6
and 4 ng/mL in the daily and monthly D
2 groups, re-
spectively. The increase was significantly greater with
D3 than with D2.
In another randomized trial, 33 adults received 50,000 IU weekly
of either D2 or D
3; mean baseline 25(OH)D was
about 28 ng/mL. After 12 weeks, increases in 25(OH)D levels were
significantly greater with D3 than with D
2 (in-
crease from baseline, about 40 vs. 22 ng/mL) .
COMMENT
On average, oral supplemental vitamin D3 — the form made
naturally after exposure to sunlight — raises 25(OH)
D blood levels more than does vitamin D2. The authors of the
second study conclude, with good reason, that D
3
is preferable for correcting vitamin D deficiency. Note,
however, that U.S. clinicians often give D2 by
prescription
to vitamin D– deficient patients: One reason might be the
availability of high-dose D2 capsules that can be taken
weekly or monthly; another might be a mistaken impression that
prescription D2 is “stronger” than an equivalent
dose of D3.
— Allan S. Brett, MD
University of South Carolina School of Medicine, Columbia
NEJM Journal Watch General Medicine , published April 26,
2011
http://www.jwatch.org/cgi/content/full/2011/0/JW201104260000008?ijkey=nl9JitqCxFBHY&keytype=ref&siteid=jwatchhttp://www.jwatch.org/cgi/content/full/2011/0/JW201104260000008?ijkey=nl9JitqCxFBHY&keytype=ref&siteid=jwatchhttp://www.jwatch.org/cgi/content/full/2011/0/JW201104260000008?ijkey=nl9JitqCxFBHY&keytype=ref&siteid=jwatchhttp://www.nejmgroup.org/http://www.jwatch.org/cgi/content/full/2011/0/JW201104260000008?ijkey=nl9JitqCxFBHY&keytype=ref&siteid=jwatch
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
19/35
19
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Response to Oral Vitamin D Supplementation in Obese
AdultsDespite a dose-response effect on average, individual
responses vary widely.
Drincic A et al. 25-hydroxyvitamin D response to graded vitamin
D3 supplementation among obese adults. J Clin Endocrinol
Metab
2013 Dec; 98:4845. (http://dx.doi.org/10.1210/jc.2012-4103)
ARTICLE SUMMARY
On average, obese people have lower serum vitamin D levels and
require higher doses of supplemental vitamin D
to correct deficiency than do nonobese people. To examine
dose-response effects, researchers randomized 62
adults with high body-mass index (BMI; (30–58 kg/m2) to receive
1000, 5000, or 10,000 IU of oral vitamin D3
daily for 5 months. The study was conducted during winter months
in Nebraska (when skin synthesis of vitamin
D is minimal ). At baseline, mean serum hydroxyvitamin D
(25[OH]D) level was 23 ng/mL.
A dose-response effect was noted. Mean serum 25( OH)D levels
increased by 12 ng/mL, 28 ng/mL, and 48 ng/mL
in the 1000, 5000, and 10,000 IU groups, respectively. However,
participants varied widely in individual responses:
The ranges of increase in serum 25(OH)D in the three dosing
groups were 2 to 39 ng/mL, 13 to 46 ng/mL, and 16
to 83 ng/mL, respectively. The incremental response to a given
vitamin D dose varied inversely with BMI, but vi-
tamin D dose was more important than BMI in predicting response
to supplementation.
COMMENT
This study provides information on the response to vitamin D
supplementation in obese patients. The wide range
of individual responses might reflect genetic variability in
binding proteins and in vitamin D hydroxylation. In
comparing these results to previous findings in nonobese
cohorts, the authors estimate that the response to a given
vitamin D dose is roughly 30% lower in obese than in
nonobese people — presumably because vitamin D is diluted
in body tissue mass.
— Allan S. Brett, MD
University of South Carolina School of Medicine, Columbia
NEJM Journal Watch General Medicine , published January 30,
2014
Is There Any Difference in the Effect of Supplements on Vitamin
D Levels in Obese
versus Non-Obese People?
http://www.jwatch.org/cgi/content/full/2014/jan30_4/NA33376?ijkey=Sd9w4MhuYMvCo&keytype=ref&siteid=jwatchhttp://www.nejmgroup.org/http://www.jwatch.org/cgi/content/full/2014/jan30_4/NA33376?ijkey=Sd9w4MhuYMvCo&keytype=ref&siteid=jwatch
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
20/35
20
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Optimizing Postmenopausal Vitamin D3 Supplementation
For white women, 600 IU of vitamin D3 daily appears to be
sufficient.
Gallagher JC et al. Dose response to vitamin D supplementation
in postmenopausal women: A randomized trial. Ann Intern
Med
2012 Mar 20; 156:425.
(http://www.annals.org/content/156/6/425.full)
ARTICLE SUMMARY
Vitamin D deficiency is defined as a serum 25-hydroxyvitamin D
(25[OH]D) level of
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
21/35
21
Back to Table of Contents
Clinical Collections — Vitamin D
Source: NEJM Journal Watch
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Vitamin D–Binding Protein Levels Are Lower in Blacks than in
WhitesBlack patients with low levels of total 25-hydroxyvitamin D
might have normal bioavailable levels.
Powe CE et al. Vitamin D–binding protein and vitamin D status of
black Americans and white Americans. N Engl J Med 2013
Nov 21; 369:1991. (http://dx.doi.org/10.1056/NEJMoa1306357)
ARTICLE SUMMARY
Compared with whites, blacks have lower 25-hydroxyvitamin D
levels but higher bone- mineral density and lower
risk for fragility fractures. How can we explain this apparent
paradox? A new study of about 2000 middle-aged
adults in Baltimore suggests that the answer might lie in
vitamin D–binding protein. Black and white participants
(about 1000 each) were closely matched for age, sex, and
body-mass index.
Mean total 25-hydroxyvitamin D levels were substantially lower
in blacks than in whites (16 vs. 26 ng/mL). How-
ever, the mean level of vitamin D–binding protein in blacks was
half that in whites, resulting in similar levels of
bioavailable, or free, 25-hydroxyvitamin D in blacks and whites.
Polymorphisms in the vitamin D– binding pro-
tein gene differed in frequency among blacks and whites; these
polymorphisms explained most of the variation in
vitamin D–binding protein levels.
COMMENT
The clinical implication of this study is that 25-hydroxyvitamin
D levels might not accurately reflect the bioavail-
able component. Blacks in particular are more likely to be
predisposed genetically to low levels of binding protein,
resulting in low total — but sufficient bioavailable —
25-hydroxyvitamin D levels. This observation might be why
we often see bone-density preservation in blacks with low levels
of total 25-hydroxyvitamin D.
— Allan S. Brett, MD
University of South Carolina School of Medicine, Columbia
NEJM Journal Watch General Medicine , published November
21, 2013
Why Are Black Patients So Often Diagnosed as Having
Vitamin D Deficiency?
Although blacks tend to have lower vitamin D levels than whites,
their bone densities are not (on average) lower.
Traditionally, it has been thought that the low levels in blacks
are related to lower levels of synthesis in the
skin, but this study suggests that binding proteins also have a
role, and that bioavailable vitamin D may in fact
be adequate in some blacks with low serum levels.
http://www.jwatch.org/cgi/content/full/2013/nov21_6/NA32739?ijkey=1xP2oO77opss6&keytype=ref&siteid=jwatchhttp://www.nejmgroup.org/http://www.jwatch.org/cgi/content/full/2013/nov21_6/NA32739?ijkey=1xP2oO77opss6&keytype=ref&siteid=jwatch
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
22/35
22
Back to Table of Contents
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Clinical Collections — Vitamin D
What Did The Institute of Medicine Say about Vitamin
D?
An IOM report from 2010 warned that the only health benefit
firmly associated with vitamin D (and calcium
as well) is bone health.
Most people in North America, according to the analysis, receive
enough vitamin D despite the fact that average
intake falls below requirements. The difference is probably made
up by sunlight exposure. Elderly people living
in institutions and those with dark skin may be at higher risk
for vitamin D insufficiency.
Dietary Reference Intakes for Calcium and Vitamin D
CALCIUM VITAMIN D
Estimated
Average
Requirement
(mg/day)
Recommended
Dietary
Allowance
(mg/day)
Upper-Level
Intake
(mg/day)
Estimated
Average
Requirement
(IU/day)
Recommended
Dietary
Allowance
(IU/day)
Upper-Level
Intake
(IU/day)
19–30 years old 800 1,000 2,500 400 600 4,000
31–50 years old 800 1,000 2,500 400 600 4,000
51–70 year old males 800 1,000 2,000 400 600 4,000
51–70 year old females 1,000 1,200 2,000 400 600 4,000
>70 years old 1,000 1,200 2,000 400 800 4,000
Source: Reprinted with permission from Dietary Reference
Intakes for Calcium and Vitamin D, 2011 by the National
Academy of Sciences, Courtesy of theNational Academies Press,
Washington, D.C.
(http://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdf )
http://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdfhttp://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdfhttp://www.nejmgroup.org/http://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdfhttp://www.iom.edu/~/media/Files/Report%20Files/2010/Dietary-Reference-Intakes-for-Calcium-and-Vitamin-D/Vitamin%20D%20and%20Calcium%202010%20Report%20Brief.pdf
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
23/35
23
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Back to Table of Contents
Clinical Collections — Vitamin D Source: NEJM Physician’s
First Watch
USPSTF: Evidence Is Insufficient to Recommend Routine
Screeningfor Vitamin D Deficiency
For the USPSTF recommendation statement: Le Fevre et al. Ann
Intern Med 2015; 162:133.
http://annals.org/article.aspx?articleid=1938935
For the USPSTF evidence review:
http://annals.org/article.aspx?articleid=1938934
And for the USPSTF grade definitions:
http://www.uspreventiveservicestaskforce.org/Page/Name/grade-definitions
ARTICLE SUMMARY
The U.S. Preventive Services Task Force has concluded that the
current evidence is inadequate to weigh thebenefits and harms of
screening for vitamin D deficiency in community-dwelling,
nonpregnant adults.
The so-called “I” statement, published in the Annals of Internal
Medicine, applies to those who are being treated
in primary care settings, have no signs of vitamin D deficiency,
and have no conditions for which vitamin D
supplementation may be recommended.
Based on its review of the evidence, the task force notes:
• There’s no consensus on the definition of vitamin D
deficiency, nor is there agreement on the optimal blood level
of 25-hydroxyvitamin D.
• No studies have assessed the direct benefits or harms of
screening for vitamin D deficiency.
• Adequate evidence suggests that treating asymptomatic adults
with vitamin D deficiency offers no benefit in terms
of cancer, diabetes, or mortality outcomes. Treatment also does
not affect fracture outcomes in those not at high
fracture risk.
— Amy Orciari Herman
Physician’s First Watch , published June 24, 2014
What Does the U.S. Preventive Services Task Force (USPSTF)
Have to Say about
Screening for Vitamin D Deficiency in the General
Population?
http://www.jwatch.org/fw108975/2014/06/24/uspstf-draft-recommendation-routine-screening-vitamin-dhttp://www.jwatch.org/fw108975/2014/06/24/uspstf-draft-recommendation-routine-screening-vitamin-dhttp://www.nejmgroup.org/http://www.jwatch.org/fw108975/2014/06/24/uspstf-draft-recommendation-routine-screening-vitamin-dhttp://www.jwatch.org/fw108975/2014/06/24/uspstf-draft-recommendation-routine-screening-vitamin-d
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
24/35
24
Back to Table of Contents
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Clinical Collections — Vitamin D
FINAL OVERVIEW AND LESSONS FROM THE CLINIC
To conclude this collection, we offer a widely-cited
Journal review article — now freshly annotated by
the
author. This review reminds us of the lessons we’ve learned from
both the bench and the clinic.
http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
25/35
25
Back to Table of Contents
Clinical Collections — Vitamin D
Source: The New England Journal of Medicine
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
clinical practice
This Journal feature begins with a case vignette
highlighting a common clinical problem.Evidence supporting various
strategies is then presented, followed by a review of formal
guidelines,
when they exist. The article ends with the author’s clinical
recommendations.
An audio versionof this articleis available at
NEJM.org
Vitamin D Insufficiency
Clifford J. Rosen, M.D.
From the Maine Medical Center ResearchInstitute, Scarborough.
Address reprint re-quests to Dr. Rosen at Maine Medical Cen-ter
Research Institute, 81 Research Dr.,Scarborough, ME 04074, or at
[email protected].
N Engl J Med 2011;364:248-54.
Copyright © 2011 Massachusetts Medical Society.
A healthy 61-year-old white woman is concerned about a low
vitamin D level detectedduring an assessment of her skeletal
health. Her menopause began at 54 years of age.
She has no history of falls, and there is no family history of
hip fracture. She takes nomedications or supplements. Her height is
157.5 cm (5 ft 2 in.), and her weight 59.1 kg
(130 lb). The results of a physical examination are
unremarkable, and the findings onlaboratory studies are normal. The
T score for bone mineral density at the hip is −1.5,
and the serum level of 25-hydroxyvitamin D is 21 ng per
milliliter (53 nmol per liter). What do you advise?
The Clinical Problem
Whereas frank vitamin D deficiency (serum level of
25-hydroxyvitamin D below 10 ng
per milliliter [25 nmol per liter]) has long been recognized as
a medical condition
characterized by muscle weakness, bone pain, and fragility
fractures, vitamin D
“insufficiency,” characterized as a serum level of
25-hydroxyvitamin D of 10 to 30 ng
per milliliter (25 to 75 nmol per liter), without overt clinical
symptoms, has re-
cently become a concern on the part of physicians and
patients.1 Increased atten-
tion to this new “syndrome” and its potential complications has
led to a substantial
increase in testing for the metabolite 25-hydroxyvitamin D, the
best clinical mea-
sure of vitamin D stores. The number of 25-hydroxyvitamin D
assays performed by
one major reference laboratory increased by 50% in the fourth
quarter of 2009 ascompared with the same quarter in 2008, and it is
expected that several million
tests will be performed this year.2
The implications of vitamin D levels that are below the normal
reference range
but not markedly reduced and the value of supplementation are
incompletely un-
derstood. Vitamin D is critical for skeletal mineralization, and
numerous observa-
tional studies have linked low levels of 25-hydroxyvitamin D to
fractures.3-7 There-
fore it is not surprising that most observational and
randomized, placebo-controlled
trials concerning vitamin D insufficiency have focused on
skeletal health outcomes.
In the past several years, attention has turned to nonskeletal
effects of vitamin D
insufficiency, particularly in relation to cardiovascular
disease, diabetes mellitus,
cancer, and immune dysfunction.8-11 This review summarizes
the current under-
standing and uncertainties regarding vitamin D insufficiency and
the effects of
vitamin D supplementation on health outcomes.
Strategies and Evidence
Defining Vitamin D Insufficiency
Interpreting the import of a serum level of 25-hydroxyvitamin D
in the “insuffi-
cient” range (i.e., 10 to 30 ng per milliliter) is challenging
for several reasons. First,
most reference laboratories have raised the lower boundary of
the normal range to
http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMcp1009570http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMcp1009570http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMcp1009570http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMcp1009570http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMcp1009570mailto:rosenc%40mmc.org?subject=mailto:rosenc%40mmc.org?subject=mailto:rosenc%40mmc.org?subject=http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMcp1009570http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMcp1009570http://www.nejmgroup.org/mailto:rosenc%40mmc.org?subject=mailto:rosenc%40mmc.org?subject=http://www.nejm.org/stoken/default+domain/ClinicalCollections-PDF/full?redirectUri=/doi/full/10.1056/NEJMra070553
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
26/35
26
Back to Table of Contents
Clinical Collections — Vitamin D
Source: The New England Journal of Medicine
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
This is further
complicated by
recent studies
suggesting that
“free” 25(OH)D may
be a more accurate
measure of bioactiv-
ity, and that total
25(OH)D does notfully reflect “free”
levels.
30 ng per milliliter. Second, although there areseveral ways to
measure 25-hydroxyvitamin D
(radioimmunoassays, enzyme-linked assays, andliquid
chromatography with mass spectrometry),
the precision and accuracy of the assays, especial-ly in
nonreference laboratories, remain problem-atic.12 Third,
25-hydroxyvitamin D levels change
with the seasons, exposure to sunlight, and di-
etary intake. For example, in northern latitudes,serum levels of
25-hydroxyvitamin D decline by20% from late summer to midwinter,
whereas
30 minutes of full-body exposure to the sun dur-ing the summer
rapidly generates vitamin D.Regular exposure to sunlight (depending
on its
strength) can increase the serum level of25-hydroxyvitamin
D.3
What does a serum 25-hydroxyvitamin D levelrepresent? Vitamin D
is produced by the nonen-
zymatic conversion of provitamin D to previtaminD in the skin
during exposure to sunlight emit-ting ultraviolet radiation in the
narrow band of
290 to 315 nm (Fig. 1). Some vitamin D also comesfrom food
sources (between 100 and 200 IU per
day). Vitamin D is converted in the liver to25-hydroxyvitamin D,
a partially water-soluble
form with a shorter half-life than vitamin D thatcirculates
bound to vitamin D–binding protein.About 40 to 50% of circulating
25-hydroxyvita-
min D is derived from skin conversion.1,3 The
active form of vitamin D is 1,25-dihydroxyvita-
min D, which is generated primarily in the kid-ney. It
circulates in lower concentrations than
Skin
Liver
Kidney
Food(vitamins D2 and D3)
Provitamin D3 Previtamin D3
Vitamin D3
25-Hydroxylase (CYP2R1)
24-Hydroxylase(CYP24R1)
1α-Hydroxylase(CYP27B1)
25(OH)D3
Increased PTH,decreasedphosphate
FGF-23 Calcitriol
Biologic Activity
24,25(OH)2D3
– +
Sunlight
+ ––
l
:
i
i l
i
I
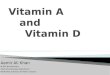
Figure 1. Synthesis and Metabolism of Vitamin D.
Vitamin D is initially generated in the skin from the non-
enzymatic conversion of provitamin D3 to previtamin D
3.
Dietary intake of vitamin D is usually relatively limited,since
few foods, with the exception of certain kinds of
fish, contain sizable amounts; supplements are com-
monly used. Vitamin D is either stored in adipose tis-
sue or converted in the liver by the enzyme 25-hydroxy-lase to
25-hydroxyvitamin D3 (25[OH]D
3), the form
that circulates in the highest concentration and reflectssolar
and dietary exposure. It is converted to the active
metabolite, 1,25-dihydroxyvitamin D (1,25[OH]2D), or
calcitriol, in the kidney, although other tissues have
1α-hydroxylase enzymatic activity. The synthesis ofcalcitriol is
enhanced (+) by increasing levels of para-
thyroid hormone (PTH), which rise in response to lower
levels of serum calcium. Reduced levels of serum phos-phate can
also increase (+) the production of calcitriol.
Its synthesis is suppressed (–) by the production of fi-
broblast growth factor 23 (FGF-23), which is secretedby
osteocytes in the bone matrix. Calcitriol inhibits the
activity of 1α-hydroxylase (CYP27B1) and stimulates the
activity of 24-hydroxylase (CYP24R1), an enzyme that pro-
motes production of 24,25(OH)2D3, a vitamin D prod-uct that is
not biologically active. In CYP2R1, CYP27B1,
and CYP24R1, CYP denotes cytochrome P.
http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
27/35
27
Back to Table of Contents
Clinical Collections — Vitamin D
Source: The New England Journal of Medicine
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
In addition, it
appears thatAfrican-Americans
may have
differences in
free vitamin D
as well as total.
25-hydroxyvitamin D but has much greater affin-
ity for the vitamin D receptor and is biologically
more potent. Low levels of 1,25-dihydroxyvita-
min D do not reflect low levels of 25-hydroxyvi-
tamin D but result from other causes, most com-
monly renal insufficiency and less frequently
oncogenic osteomalacia.
The serum 25-hydroxyvitamin D level is thebest indicator of
overall vitamin D status because
this measurement reflects total vitamin D from
dietary intake and sunlight exposure, as well as
the conversion of vitamin D from adipose stores
in the liver.13,14 According to the National Health
and Nutrition Evaluation Survey (NHANES), in the
United States, the average dietary intake of vita-
min D (including supplements) may be as low as
200 IU per day (with differences according to
age).15 Skin-derived synthesis of vitamin D is
quite variable, depending on pigmentation, lati-
tude, season, clothing, age, sunscreen use, and
local weather conditions. Levels of 25-hydroxyvi-
tamin D are considerably lower among blacks
than among whites because of greater pigmenta-
tion in blacks. In healthy whites, serum levels of
25-hydroxyvitamin D may vary according to en-
vironmental, hormonal, genetic, and nutritional
factors.3,14 The body-mass index (BMI), for exam-
ple, is inversely related to the serum 25-hydroxy-
vitamin D level, and obese patients typically
have levels in the range of 10 to 20 ng per milli-
liter (25 to 50 nmol per liter); these differences
may be due in part to lower levels of exercise and
sunlight exposure in obese persons than leanpersons. Several
conditions cause very low serum
levels of 25-hydroxyvitamin D (i.e., below 10 ng
per milliliter), including poor dietary intake of
vitamin D coupled with negligible sun exposure;
malabsorption due to inflammatory bowel dis-
ease, gluten enteropathy, gastric surgery, biliary
disease, or intestinal overgrowth; use of anti-
seizure medications (e.g., phenobarbital or phe-
nytoin); and long-term use of glucocorticoids.1,3
Defining a level of serum 25-hydroxyvitamin D
as low or insufficient depends on the level that is
defined as normal. Previously, according to the
World Health Organization, levels below 10 ng permilliliter were
considered deficient and levels
below 20 ng per milliliter were classified as in-
sufficient.16 However, with the recent changes in
laboratory reference ranges, a normal level is now
typically defined as a serum level of 30 to 76 ng
per milliliter (75 to 190 nmol per liter). When that
range is used, the estimated prevalence of vita-
min D insufficiency is as high as 50 to 80% in the
general population.17,18 According to the NHANES
for 2005 and 2006, the mean 25-hydroxyvitamin
D level among several age groups was 24 ng per
milliliter (60 nmol per liter), a level considered
to be insufficient according to some standards.15
There are two rationales for setting the low endof the normal
range for 25-hydroxyvitamin D at
30 ng per milliliter: one, put forward in studies
published in the past several years, suggests that
levels of parathyroid hormone (PTH) rise when
levels of 25-hydroxyvitamin D fall below 30 ng per
milliliter3,13,19; the other, proposed in earlier stud-
ies, suggests that active calcium absorption is op-
timal when the level of 25-hydroxy vitamin D is
30 ng per milliliter.20 However, both tenets are
now being questioned.14 Data indicate that the
relationship of PTH and 25-hydroxy vitamin D is
not curvilinear, and there is substantial variation
in PTH levels when 25-hydroxyvitamin D levels
are between 20 and 30 ng per milliliter. There is
no absolute threshold level of serum 25-hydroxy-
vitamin D at which PTH levels rise.13,19 Further-
more, although the information derived from
dual isotope analysis is the most accurate mea-
sure of calcium absorption, there are too few
studies to establish an absolute cutoff for levels
of 25-hydroxyvitamin D above which calcium ab-
sorption is not enhanced. Generally, peak absorp-
tion of calcium occurs at levels between 20 and
30 ng per milliliter.
Vitamin D and Bone Health
Although recent attention has focused on the non-
skeletal effects of vitamin D, it is well established
that vitamin D is critical for bone mineraliza-
tion.1,8-11 Therefore, it is not surprising that most
studies of vitamin D have assessed outcomes for
skeletal health.
Several observational studies of the associa-
tions between serum levels of 25-hydroxyvitamin
D and skeletal health have had conflicting re-
sults. A report from Ottawa on 15 studies (3 pro-
spective cohort studies and 12 case–control stud-
ies) concluded that associations between serum25-hydroxyvitamin
D concentrations and fractures,
falls, and performance measures (tests of gait,
stability, and activity) among postmenopausal
women or elderly men were inconsistent.21 A more
recent report from the Agency for Healthcare
Research and Quality (AHRQ) and Tufts Medical
http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
28/35
28
Back to Table of Contents
Clinical Collections — Vitamin D
Source: The New England Journal of Medicine
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
More-recent meta-nalyses have confirmed
hat vitamin D alone has
ttle if any benefit on
racture risk and bone
mineral density
Reid et al. Lancet 2013).
Center, analyzing the same observational stud-
ies, concluded that there was fair, or reasonable,
evidence of an association between lower serum
concentrations of 25-hydroxyvitamin D and an
increased risk of falls among institutionalized
elderly persons.22
Randomized, controlled trials of vitamin D
supplementation have addressed its effects onskeletal outcomes,
but most of these trials in-
volved supplementation with both vitamin D and
calcium, making it impossible to separate out
the effects attributable specifically to vitamin D.
The results of a 2007 meta-analysis of 29 trials
of supplementation with both calcium and vita-
min D or with calcium alone suggested that daily
supplementation with 1200 mg of calcium and
at least 800 IU of vitamin D resulted in reduced
rates of fracture and a modest increase in bone
mineral density, but the relationship between se-
rum 25-hydroxyvitamin D levels and skeletal out-comes was not
assessed.23 A 2009 Cochrane
meta-analysis of 10 trials testing the effects of
vitamin D supplementation alone and 8 trials test-
ing the effects of vitamin D plus calcium showed
no significant relationship between vitamin D
supplementation alone and a reduction in the risk
of fracture.24 However, the study confirmed the
conclusion of the 2007 meta-analysis that calci-
um plus vitamin D was marginally effective in
reducing the risk of fracture in older persons as
compared with no supplementation (odds ratio,
0.89; 95% confidence interval, 0.80 to 0.99).
Despite the observational data suggestingan inverse association
between serum levels of
25-hydroxyvitamin D and the risk of falls among
institutionalized elderly persons, the evidence is
inconsistent, with some studies showing a benefit
and others showing no effect of vitamin D sup-
plementation on the risk of fractures or falls in
various populations.22,25 Similarly, a randomized
study conducted by the Women’s Health Initiative
showed a nonsignificant reduction in hip frac-
tures among women receiving a total of 700 IU
of vitamin D and more than 2000 mg of calcium
per day.26 However, the high baseline intake of
calcium (an average of 1100 to 1200 mg per day)and vitamin D
(approximately 300 IU per day) in
the placebo group may have limited the ability of
the investigators to detect effects of supplemen-
tation. Subgroup analyses of women over 60 years
of age and of those who adhered to their supple-
mentation regimen showed a significant reduc-
tion in hip fractures with supplementation, but
these results must be interpreted with caution.
Randomized trials of supplementation with vita-
min D2 or D
3 (with daily doses ranging from 400
to 822 IU) published after the AHRQ–Tufts analy-
sis also failed to show significant effects of vita-
min D supplementation on the risk of fracture or
falls in older populations.27,28 However, in one ofthose
trials, vitamin D supplementation at a dose
of 400 IU daily improved gait speed and reduced
body sway.27
Several large observational studies have ad-
dressed the question of whether there is a thresh-
old level of 25-hydroxyvitamin D below which ad-
verse skeletal outcomes are more likely to occur.
In one study of elderly men, levels below 16 ng
per milliliter (40 nmol per liter) were associated
with a greater risk of fracture, whereas in an-
other study, men with levels below 20 ng per
milliliter had greater rates of femoral bone lossthan men with
higher levels.29,30 In a longitudi-
nal study, Osteoporotic Fractures in Men (MrOs),
older men with serum levels of 25-hydroxyvita-
min D that were less than 20 ng per milliliter
had a higher risk of hip fracture than men with
higher levels.31 In a prospective study of older
women, 25-hydroxyvitamin D levels between 24
and 26 ng per milliliter (60 to 65 nmol per liter)
were associated with the lowest risk of hip frac-
ture; no additional risk reduction was noted
above that level.32 However, in a study of older
New Zealand women, levels of 25-hydroxyvita-
min D below 20 ng per milliliter were not asso-ciated with an
increased risk of fracture during
5 years of follow-up.33
Vitamin D and Other Health Effects
Observational studies in large cohorts have shown
significant associations between low levels of
25-hydroxyvitamin D (i.e., below 20 ng per milli-
liter) and an increased risk of metabolic, neo-
plastic, and immune disorders such as type 1
diabetes mellitus and multiple sclerosis.7-11 The
two conditions most often connected with low
levels of vitamin D are atherosclerosis and diabe-
tes mellitus.34-36 For example, a significantly in-creased
risk of type 2 diabetes has been reported
among persons with levels of vitamin D that are
insufficient (below 30 ng per milliliter), even after
adjustment for BMI and percentage of body fat.8,35
Similarly, another prospective study showed that
levels of serum 25-hydroxyvitamin D below 20 ng
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2813%2961647-5/abstracthttp://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2813%2961647-5/abstracthttp://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2813%2961647-5/abstracthttp://www.nejmgroup.org/http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2813%2961647-5/abstract
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
29/35
29
Back to Table of Contents
Clinical Collections — Vitamin D
Source: The New England Journal of Medicine
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
Such a trial is under way
in non-institutionalized
elders. Called the STURD
Trial, it is sponsored by t
National Institute on Ag
(NCT02166333).
per milliliter were associated with an increased
risk of cardiovascular disease.10 However, there
are not enough data from large, randomized, con-
trolled trials to assess whether vitamin D supple-
mentation reduces the risk of chronic diseases
other than osteoporosis.
Areas of Uncertainty
The dynamics of vitamin D storage and reentry
into the circulation remain poorly understood,
particularly in obese persons.37 Optimal dosage
regimens for vitamin D remain uncertain. In
general, for every 100 IU of vitamin D taken in,
there is an increase of roughly 1 ng per milliliter
(3 nmol per liter) in the serum level of 25-hydroxy-
vitamin D; the lower the baseline level of 25-
hydroxyvitamin D, the greater the rise with vita-
min D supplementation. Most trials assessing the
association between 25-hydroxyvitamin D levelsand the risk of
fractures and falls have used daily
doses of vitamin D between 400 and 1000 IU.
Data are scarce on the effects of long-term supple-
mentation with doses greater than 1000 IU per
day. In a recently published randomized, placebo-
controlled trial involving elderly persons not liv-
ing in institutions, those who received an oral
dose of 500,000 IU of vitamin D once a year for
3 years had a significantly increased rate of falls
and fractures, as compared with those who re-
ceived placebo, particularly in the first 3 months
after dosing.38 These results suggest that high
intermittent doses of vitamin D, as compared
with daily doses, may be metabolized and used
differently. Finally, data are lacking from large
randomized, controlled trials designed to deter-
mine whether vitamin D supplementation reduces
the risk of other major diseases, such as colon
cancer, for which there are observational data
suggesting a reduction in risk with supplementa-
tion. The ongoing Vitamin D and Omega-3 Trial
(VITAL; ClinicalTrials.gov number, NCT01169259),
a 5-year, randomized, placebo-controlled trial in-
volving 20,000 U.S. men and women is examin-
ing vitamin D supplementation (2000 IU per day), with or
without supplementation of n–3 fatty acids,
for the primary prevention of cancer and cardio-
vascular disease.
Toxicity from vitamin D supplementation is
rare and consists principally of acute hypercalce-
mia, which usually results from doses that ex-
ceed 10,000 IU per day; associated serum levels
of 25-hydroxyvitamin D are well above 150 ng
per milliliter (375 nmol per liter).39 The tolerable
upper level of daily vitamin D intake recently set
by the Institute of Medicine (IOM) is 4000 IU.14
The long-term effects of supplementation at doses
above 4000 IU per day are not known, and risks
cannot be ruled out. Recent observational stud-ies have
suggested associations between serum
levels of 25-hydroxyvitamin D above 60 ng per
milliliter (150 nmol per liter) and increased risks
of pancreatic cancer, vascular calcification, and
death from any cause,34,40,41 but the observational
nature of these studies precludes an assessment
of cause and effect. More longitudinal studies
and controlled trials are needed.
Several studies have suggested that vitamin D
supplementation may be most effective in reduc-
ing fractures and falls in institutionalized elderly
persons, in whom serum levels of 25-hydroxyvi-
tamin D are often below 20 ng per milliliter.42-44 Yet the
optimal replacement dose in this popula-
tion is still not known. A large, long-term, ran-
domized trial is warranted to examine the ef-
fects of several different doses of vitamin D on
physical performance measures and the incidence
of falls and fractures in the institutionalized el-
derly population.
Guidelines from
professional societies
At an international workshop on vitamin D held
in 2007, there was agreement that most of the
world’s population is not getting an amount of
vitamin D sufficient to maintain healthy bone
mass and minimize the risk of fracture. The work-
shop members also agreed that vitamin D insuf-
ficiency decreases muscle strength and increases
the risk of falls.45 The recommendation from
that group, made on the basis of available obser-
vational data, was that the minimum desirable
serum level of 25-hydroxyvitamin D is 20 ng per
milliliter. Three years later, Osteoporosis Canada
issued a report stating that the 25-hydroxyvita-
min D level should be at least 30 ng per milliliterand that
vitamin D insufficiency should be de-
fined as a level of 10 to 29 ng per milliliter.46 In
2010, the International Osteoporosis Foundation
issued a position statement on vitamin D status,
also based on observational data, recommending
a target serum level of 25-hydroxyvitamin D of
30 ng per milliliter in all elderly persons and
https://clinicaltrials.gov/ct2/show/NCT01169259?term=NCT01169259&rank=1https://clinicaltrials.gov/ct2/show/NCT01169259?term=NCT01169259&rank=1http://www.nejmgroup.org/https://clinicaltrials.gov/ct2/show/NCT01169259?term=NCT01169259&rank=1
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
30/35
30
Back to Table of Contents
Clinical Collections — Vitamin D
Source: The New England Journal of Medicine
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
The U.S. Preventive Services
Task Force recently declared
that there was insufficient
evidence to supportwidespread screening with
serum 25(OH)D, thus raising
doubts about setting an
absolute level to target for
most individuals.
stating that vitamin D intakes as high as 2000 IUper day may be
necessary to attain the recom-
mended level in some persons.47 In contrast, theIOM report,
based on evidence from observational
studies and recent randomized trials, suggests thata serum level
of 20 ng per milliliter of 25-hydroxy-
vitamin D would protect 97.5% of the population
against adverse skeletal outcomes such as frac-tures and
falls.14
Conclusions a nd
Recommendations
The woman described in the vignette is a healthypostmenopausal
woman with slightly low bonemineral density and a 25-hydroxyvitamin
D level
of 21 ng per milli liter. Although the laboratorythat performed
the measurement, and many
other laboratories, would label that level as in-sufficient, she
is certainly not def icient in vita-
min D. According to the Fracture Risk Assess-ment Tool (FRAX)
developed by the WorldHealth Organization, the probability that
she
will sustain a hip fracture over the next 10 yearsis less
than 1%. Moreover, she is not at high risk
for falls and is unlikely to have osteomalacia.48 Hence,
for patients such as this one, I would
recommend an exercise program and a total cal-cium intake of
1200 mg per day. There remains
uncertainty about whether vitamin D supple-mentation is
appropriate for her, and if so, what
the dose should be, although the recent IOM
guidelines recommend 600 IU daily for a post-menopausal woman
who is not at high risk for
fractures or falls and 800 IU daily for persons who have a
very high risk of osteoporosis or
who are older than 70 years of age.14 I wouldexplain
that despite the recent focus in the me-
dia on the potential role of vitamin D in reduc-ing the risk of
various chronic diseases, thishypothesis requires testing in large,
randomized,
controlled trials, and vitamin D cannot current-ly be
recommended for the purpose of reducing
the risk of heart disease or cancer.
Dr. Rosen reports serving as an unpaid consultant for
LexiconGenetics and serving on the Vitamin D Subcommittee for
theIOM, for which he received reimbursement for travel expenses.No
other potential conf lict of interest relevant to this art icle
wasreported.
Disclosure forms provided by the author are available with
thefull text of this article at NEJM.org.
References
1. DeLuca HF. Overview of general physi-ologic features and
functions of vitamin D.Am J Clin Nutr 2004;80:Suppl:1689S-1696S.2.
Parker-Pope T. The miracle of vitaminD: sound science or hype? New
York Times,Feb. 1, 2010.3. Holick MF. Vitamin D deficiency.
N Engl J Med 2007;357:266-81.4. Dawson-Hughes B. Serum
25-hydroxy-
vitamin D and functional outcomes in theelderly. Am J Clin
Nutr 2008;88:537S-540S.5. van Schoor NM, Visser M, Pluijm
SM,Kuchuk N, Smit JH, Lips P. Vitamin D de-ficiency as a risk
factor for osteoporoticfractures. Bone 2008;42:260-6.6. Kenny AM,
Biskup B, Robbins B, Mar-cella G, Burleson JA. Effects of vitamin
Dsupplementation on strength, physicalfunction, and health
perception in older,community-dwelling men. J Am GeriatrSoc
2003;51:1762-7.7. Trivedi DP, Doll R, Khaw KT. Effect offour
monthly oral vitamin D3 (cholecal-ciferol) supplementation on
fractures and
mortalit y in men and women living in thecommunity: randomised
double blind con-trolled t rial. BMJ 2003;326:469.8. Pittas AG, Lau
J, Hu FB, Dawson-Hughes B. The role of vitamin D and cal-cium in
type 2 diabetes: a systematic re-
view and meta-analysis. J Clin EndocrinolMetab
2007;92:2017-29.9. Giovannucci E, Liu Y, Rimm EB, et al.
Prospective study of predictors of vitaminD status and cancer
incidence and mor-talit y in men. J Natl Cancer Inst
2006;98:451-9.10. Dobnig H, Pilz S, Scharnagl H, et al.Independent
association of low serum25-hydroxyvitamin D and 1,25-dihydroxy-
vitamin D levels with all-cause and car-diovascular
mortality. Arch Intern Med2008;168:1340-9.11. Hewison M. Vitamin D
and innate im-munity. Curr Opin Investig Drugs 2008;9:485-90.12.
Binkley N, Krueger D, Lensmeyer G.25-Hydroxyvitamin D measurement
2009:a review for clinicians. J Clin Densitom2009;12:417-27.13.
Heaney RP. The vitamin D require-ment in health and disease. J
Steroid Bio-chem Mol Biol 2005;97:13-9.14. IOM report on calcium
and vitamin D.Washington, DC: Institute of Medicine,2010.
(http://www.iom.edu/vitaminD.)15. National Health and Nutrition
Exami-
nation Survey. What we eat in America,2005-2006.
(http://www.ars.usda.gov/ba/bhnrc/fsrg.)16. WHO Scientific Group on
the Preven-tion and Management of Osteoporosis.Prevention and
management of osteopo-rosis: report of a WHO scientific
group.Geneva: World Health Organization, 2003.17. Holick MF, Siris
ES, Binkley N, et a l.
Prevalence of vitamin D inadequacy amongNorth American
postmenopausal womenreceiving osteoporosis therapy. J Clin
En-docrinol Metab 2005;90:3215-24.18. Ginde AA, Liu MC, Camargo CA
Jr.Demographic differences and trends of
vitamin D insufficiency in the US popula-
tion, 1988-2004. Arch Intern Med 2009;169:626-32.19.
Steingrimsdottir L, Gunnarsson O,Indridason OS, Franzson L,
Sigurdsson G.Relationship between serum parathyroidhormone levels,
vitamin D sufficiency, andcalcium intake. JAMA 2005;294:2336-41.20.
Chapuy MC, Preziosi P, Maamer M,et al. Prevalence of vitamin D
insufficiencyin an adult normal population. OsteoporosInt
1997;7:439-43.21. Cranney A, Horsley T, O’Donnell S,et al.
Effectiveness and safety of vitamin Din relation to bone health.
Evidence report/technology assessment no. 158. Rockville,MD: Agency
for Healthcare Research andQualit y, 2007.
22. Chung M, Balk E, Brendel M, et al. Vi-tamin D and calcium: a
systematic reviewof health outcomes. Evidence report/tech-nology
assessment no. 183. Rockville,MD: Agency for Healthcare Research
andQualit y, 2009.23. Tang BM, Eslick GD, Nowson C,Smith C,
Bensoussan A. Use of calcium orcalcium in combination with vitamin
D
http://www.nejmgroup.org/
-
8/20/2019 Vitamin D _ NEJMGroup_Collection
31/35
31
Back to Table of Contents
Clinical Collections — Vitamin D
Source: The New England Journal of Medicine
Downloaded from collections.nejm.org. For personal use only. No
other uses without permission.
Copyright © Massachusetts Medical Society. All rights
reserved.
supplementation to prevent fractures and
bone loss in people aged 50 years and
older: a meta-analysis. Lancet 2007;370:
657-66.
24. Avenell A, Gillespie WJ, Gillespie LD,
O’Connell D. Vitamin D and vitamin D
analogues for preventing fractures asso-
ciated with involutional and post-meno-
pausal osteoporosis. Cochrane Database
Syst Rev 2009;2:CD000227.25. Bischoff-Ferrari HA,
Dawson-Hughes
B, Willett WC, et al. Effect of vitamin D
on falls: a met a-analysis. JAMA 2004;291:
1999-2006.
26. Jackson RD, LaCroix AZ, Gass M, et al.
Calcium plus vitamin D supplementation
and the risk of fractures. N Engl J Med
2006;354:669-83. [Erratum, N Engl J Med
2006;354:1102.]
27. Bunout D, Barrera G, Leiva L, et al.
Effects of vitamin D supplementation and
exercise training on physical performance
in Chilean vitamin D deficient elderly sub-
jects. Exp Gerontol 2006;41:746-52.
28. Salovaara K, Tuppurainen M, Kark-
kainen M, et al. Effect of vitamin D3 and
calcium on fracture risk in 65- to 71-year-old women: a
population based 3-year ran-
domized controlled trial — the OSTPRE-
FPS. J Bone Miner Res 2010;25:1487-95.
29. Melhus H, Snellman G, Gedeborg R,
et al. Plasma 25-hydroxyvitaminD levels
and fracture risk in a community-based
cohort of elderly men in Sweden. J Clin
Endocrinol Metab 2010;95:2637-45.
30. Ensrud KE, Taylor BC, Paudel ML, et al.
Serum 25-hydroxyvitamin D levels and rate
of hip bone loss in older men. J Clin Endo-
crinol Metab 2009;94:2773-80.
31. Cauley JA, Parimi N, Ensrud KE, et al.
Serum 25-hydroxyvitamin D and the risk
of hip and nonspine fractures in older
men. J Bone Miner Res 2010;25:545-53.
32. Cauley JA, Lacroix AZ, Wu L, et al. Se-
rum 25-hydroxyvitamin D concentrations
and risk for hip fractures. Ann Intern Med
2008;149:242-50.
33. Bolland MJ, Bacon CJ, Horne AM, et al.
Vitamin D insufficiency and health out-
comes over 5 y in older women. Am J Clin
Nutr 2010;91:82-9.34. Wang TJ, Pencina MJ, Booth SL. Vita-
min D deficiency and risk of cardiovascu-
lar d isease. Circulation 2008;117:503-11.
35. Pittas AG, Harris SS, Stark PC, Dawson-
Hughes B. The effects of calcium and vita-
min D supplementation on blood glucose
and markers of inflammation in non dia-
betic adults. Diabetes Care 2007;30:980-6.
36. Giovannucci E, Liu Y, Hollis BW,
Rimm EB. 25-Hydroxyvitamin D and risk
of myocardial infarction in men. Arch In-
tern Med 2008;168:1174-80.
37. Koch TR, Finelli FC. Postoperative
metabolic and nutritional complications
of bariatric surgery. Gastroenterol Clin
North Am 2010;39:109-24.
38. Sanders KM, Stuart AL, Williamson EJ,et al. Annual high dose
vitamin D and
falls and fractures in older women: a ran-
domized controlled tr ial. JAMA 2010;303:
1815-22. [Erratum, JAMA 2010;303:2357.]
39. Jones G. Pharmacokinetics of vitamin
D toxicity. Am J Clin Nutr 2008;88:582S-
586S.
40. Stolzenberg-Solomon RZ, Jacobs EJ,
Arslan AA, et al. Circulating 25-hydroxy-
vitamin D and risk of pancreat ic cancer:
Cohort Consortium Vitamin D Pooling
Project of Rarer Cancers. Am J Epidemiol
2010;172:81-93.
41. Melamed ML, Michos ED, Post W, As-
tor B. 25-Hydroxyvitamin D levels and the
risk of mortality in the general popula-
tion. Arch Intern Med 2008;168:1629-37.
42. Chapuy MC, Arlot ME, Duboeuf F, et al.
Vitamin D3 and calcium to prevent hip
fractures in the elderly women. N Engl J
Med 1992;327:1637-42.
43. Lyons RA, Johansen A, Brophy S, et al.