-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
1/22
Official reprint from UpToDate www.uptodate.com 2014
UpToDate
AuthorMadhusmita Misra, MD,MPH
Section EditorsKathleen J Motil, MD, PhDMarc K Drezner, MD
Deputy EditorAlison G Hoppin, MD
Vitamin D insufficiency and deficiency in children and
adolescents
All topics are updated as new evidence becomes available and our
peer review process is complete.Literature review current through:
Aug 2014. | This topic last updated: Jul 21, 2014.
INTRODUCTION Vitamin D is an essential nutrient that plays an
important role in calcium homeostasisand bone health. Severe
deficiency of vitamin D causes rickets and/or hypocalcemia in
infants and childrenand osteomalacia in adults or adolescents after
epiphysial closure; severe vitamin D deficiency may also
beassociated with hypocalcemia, which may cause tetany or seizures.
These disorders occur with the highestfrequency among children in
malnourished populations and in children with chronic illnesses.
Rickets alsooccurs in children in developed nations if sufficient
vitamin D intake is not ensured through the use ofsupplements and
fortified foods, particularly if exposure to sunlight is limited.
The clinical evaluation andtreatment of a child with rickets is
discussed separately. (See "Overview of rickets in children" and
"Etiologyand treatment of calcipenic rickets in children", section
on 'Nutritional rickets'.)
The clinical consequences of mild vitamin D deficiency are less
well established. However, chronically lowvitamin D levels are
associated with the development of low bone mineral density and
other measures ofreduced bone health, even in the absence of
rickets. The definition, causes, and prevention of vitamin
Ddeficiency in children, and the treatment of vitamin D deficiency
in the absence of rickets will be reviewedhere.
The causes and treatment of vitamin D deficiency in adults are
discussed in separate topic reviews. (See"Causes of vitamin D
deficiency and resistance" and "Vitamin D deficiency in adults:
Definition, clinicalmanifestations, and treatment".)
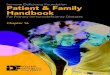
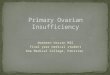
METABOLISM AND FORMS OF VITAMIN D Vitamin D is a prohormone that
is synthesized in the skinafter exposure to ultraviolet radiation.
Less than 10 percent of vitamin D comes from dietary sources in
theabsence of food fortification or use of supplements. The
prohormone is then converted to the metabolicallyactive form in the
liver and kidneys (figure 1). (See "Overview of vitamin D", section
on 'Metabolism'.)
EPIDEMIOLOGY Vitamin D deficiency in children in the United
States and several other developednations has been reported with
increasing frequency since the mid 1980s [2-5]. In the United
States, the
Cholecalciferol, or vitamin D3, is formed when ultraviolet-B
(UV-B) radiation (wavelength 290 to 315nm) converts
7-dehydrocholesterol in epidermal keratinocytes and dermal
fibroblasts to pre-vitamin D,which subsequently isomerizes to
vitamin D . This is the form of vitamin D found in animal products
andsome vitamin D supplements.
3
Ergocalciferol, or vitamin D2, is formed when ergosterol in
plants is exposed to irradiation. This is theform of vitamin D
found in plant dietary sources and in most vitamin D
supplements.
Vitamin D (cholecalciferol produced in the skin or ingested, or
ergocalciferol ingested) is bound tovitamin D-binding protein (DBP)
and transported to the liver, where it undergoes 25-hydroxylation
to 25-hydroxyvitamin D [25(OH)D], the storage form of this vitamin,
also known as calcidiol.
In the kidney, 25(OH)D undergoes 1--hydroxylation to form
1,25(OH) vitamin D [1,25(OH) D], theactive form of the vitamin,
also known as calcitriol. This process is driven by parathyroid
hormone(PTH) and other mediators, including hypophosphatemia and
growth hormone. There are many sites of1--hydroxylation, including
lymph nodes, placenta, colon, breasts, osteoblasts, alveolar
macrophages,activated macrophages, and keratinocytes, suggesting an
autocrine-paracrine role for 1,25(OH) D [1].
2 2
2
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
2/22
overall prevalence of vitamin D deficiency or insufficiency
(defined in these studies as 25(OH)D
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
3/22
vitamin D binding protein, which account for a large proportion
of the variation in serum total 25(OH)D levels.(See "Vitamin D
deficiency in adults: Definition, clinical manifestations, and
treatment", section on 'Definingvitamin D sufficiency'.)
Children Standards for defining vitamin D sufficiency in healthy
children are not well established. Inchildren, radiological changes
of rickets and low bone density have been reported at 25(OH)D
levels of
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
4/22
The latitude of residence and season are also important
determinants of cutaneous vitamin D synthesis.During the winter
months at high latitudes there is greater scatter and absorption of
UV-B because of theoblique angle at which sunlight traverses the
atmosphere and its longer path through the atmosphere. As
aconsequence, beyond a latitude of 40 and during winter, little or
no UV-B radiation reaches the surface ofthe earth. Therefore, while
vitamin D deficiency is relatively uncommon at the end of the
summer months, it isvery common at the end of winter. In the
Northern hemisphere, vitamin D levels typically reach their nadir
inFebruary and March. Even in the summer, excessive use of sunblock
can cause a persistence of low vitaminD levels [53]. One study from
Iowa (41N) reported that 25(OH)D levels were less than 11 ng/mL
(27.5nmol/L) in 78 percent of unsupplemented breast-fed infants
during winter, compared to only 1 percent in thesummer [54]. In
Edmonton, Canada (52N), 34 percent of children presenting to an
emergency department atthe end of winter had 25(OH)D levels less
than 16 ng/mL (40 nmol/L), and 6 percent had levels less than
10ng/mL (25 nmol/L) [55]. Similarly, the prevalence of low vitamin
D levels (
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
5/22
vitamin D deficiency [68]. One study that included Black and
White infants estimates that most breast-fedinfants need to be
exposed to sunlight for at least 30 minutes/week while wearing only
a diaper in order tomaintain 25(OH)D levels at >20 ng/mL (50
nmol/L) [46]. This amount of sun exposure is unlikely givencurrent
recommendations to limit sun exposure in infants younger than six
months old. (See 'Exposure tosunlight' below.)
One study reviewed 166 published cases of rickets in children 4
to 54 months old between 1986 and 2003,and reported that 96 percent
of the affected children were breast-fed [2]. In another study from
Alaska, 98percent of infants with 25(OH)D levels
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
6/22
Osteomalacia In older adolescents and adults, growth is
complete, epiphyseal plates are fused, and thereis usually reserve
mineral, all of which help prevent bony deformities. Impaired
mineralization in olderchildren and adults causes osteomalacia,
which may be asymptomatic or manifest as isolated or
generalizedmuscle and bone pain.
Biochemical changes Vitamin D deficiency reduces intestinal
calcium and phosphorus absorption.Parathyroid hormone (PTH)
increases, leading to mobilization of calcium from bone so that
serum calciumlevels remain normal or are moderately decreased.
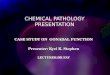
Biochemical changes that characterize early, moderate, and
severe vitamin D deficiency are outlined in thetable (table 1).
With more severe vitamin D deficiency, calcium and phosphorus
levels are normal ormoderately decreased, 25(OH)D levels decrease,
and PTH and ALP levels increase. 1,25(OH) D levelsinitially
increase in response to rising levels of PTH, but may subsequently
decrease because its substrate25(OH)D is limited.
Low serum phosphorus levels may cause muscle weakness and
discomfort, and children may have difficultystanding or walking.
Low phosphorus also prevents apoptosis of hypertrophic
chondrocytes, causingdisorganization of the growth plate. The
reduced serum levels of calcium and phosphorus lead to a
lowercalcium-phosphorus product and the subsequent mineralization
defects in growing children that arecharacteristic of rickets. (See
"Overview of rickets in children", section on 'Laboratory
findings'.)
Patients with advanced vitamin D-deficient rickets may develop
severe hypocalcemia especially duringperiods of very rapid growth,
such as infancy and adolescence, when increased calcium
mobilization frombone from rising levels of PTH and 1,25(OH) D is
unable to keep pace with increased calcium needs. Thiscan lead to
seizures or tetany, or may present as apneic spells, stridor,
wheezing, hypotonia, andhyperreflexia, particularly in very young
children.
RECOMMENDATIONS FOR VITAMIN D INTAKE The following
recommendations for vitamin D intakeare endorsed by the Institute
of Medicine, the Endocrine Society and the American Academy of
Pediatrics(AAP) [75-77]:
These recommendations reflect an increase over previous
guidelines, which recommended intake of 200 int.units daily in
infants and children. The intake of 200 int. units daily was
designed to ensure serum 25(OH)Dlevels >11 ng/mL (27.5 nmol/L).
However, this target serum level was considered inadequate because
theselevels are not sufficient for preventing all cases of florid
rickets [36,37,80], and because the risk of ricketsdecreases
substantially when 25(OH)D levels exceed 15 ng/mL (37.5 nmol/L)
[42]. (See 'Children' above.)
There is limited evidence that fracture risk is associated with
low levels of vitamin D intake. However, onelarge observational
study found that vitamin D intake was associated with reduced risk
of stress fracturesamong preadolescent and adolescent girls,
particularly those participating in at least one hour/day of
high-impact activity [81]. After adjusting for confounders, the
risk of developing a stress fracture among girls in thehighest
quintile of vitamin D intake (mean intake 663 int. units daily) was
50 percent lower than the risk ingirls with the lowest quintile of
vitamin D intake (mean intake 107 int. units/day). Although this
study does notestablish a causal association between vitamin D
intake and fracture risk, the findings lend support to
therecommended daily intake level of 600 int. units daily. Children
who are obese and those on anticonvulsants,glucocorticoids, and on
medications for HIV infection may require higher doses of vitamin D
to maintain theirvitamin D levels in the sufficient range. (See
'Obesity' above and 'Medications' above.)
PREVENTION
Vitamin D supplementation for infants All exclusively breast-fed
infants should receive 400 int. units per
2
2
All infants, including those who are exclusively breast-fed 400
International Units (10 micrograms)daily, beginning within a few
days after birth [1,78]. This intake is considered sufficient to
prevent ricketsand to maintain 25(OH)D levels at >20 ng/mL (50
nmol/L) in most infants [1,79]. Supplementation forpremature
infants is discussed separately. (See "Management of neonatal bone
health", section on'Vitamin D'.)
Healthy children 1 to 18 years of age 600 International Units
(15 micrograms) daily
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
7/22
day of Vitamin D supplements, as outlined above [1,75,76,78].
This recommendation is based on the lowvitamin D content of breast
milk, the inconsistency and unpredictability of cutaneous vitamin D
synthesis fromsun exposure, and the disproportionately high
frequency of rickets among exclusively breast-fed infants.
(See'Exclusive breast feeding' above.)
Many formula-fed infants should also receive vitamin D
supplements. Currently, fortification practices in theUnited States
ensure that infant formulas contain 40 to 100 int. units of vitamin
D per 100 kcal of formula,providing at least 400 int. units per
liter. Thus, formula-fed infants who consume at least 1 liter (33
oz) offormula daily meet the current AAP standards for vitamin D
intake. However, most infants who are onlypartially formula-fed,
and many infants who are fully formula-fed will consume less than
this amount offormula, and should therefore receive supplemental
vitamin D.
Of concern, it appears that few infants in the United States are
receiving sufficient vitamin D to meet the AAPrecommendations. This
is partly because pediatric health care providers in the United
States are not routinelyadvising Vitamin D supplements for
predominantly breast-fed infants. In one study, only 36 percent
ofresponding clinicians indicated that they routinely recommended
Vitamin D supplementation in predominantlybreastfed infants [82].
In addition, an even smaller percentage of parents are actually
giving vitamin Dsupplements to their infants. In the study cited
above, 67 percent of parents indicated that they believedbreast
milk has all necessary nutrients, and only 3 percent gave
supplements to their children [82]. Anotherstudy from the United
States concluded that only 1 to 13 percent of infants received
supplements per AAPrecommendations [83]. In this study, only 5 to
13 percent of breast-fed infants, 9 to 14 percent of
mixed-fedinfants, and 20 to 35 percent of formula fed infants met
the 2008 AAP recommendations for intake of VitaminD
supplements.
Awareness of and adherence to national recommendations for
vitamin D supplementation also appears to bea problem in the United
Kingdom [84-87]. Adherence is better in some other countries. In a
Canadian study,74 percent of mothers who exclusively breast-fed
their infants indicated compliance with Canadianrecommendations for
vitamin D intake (also 400 int. units daily) [88]. Other reports
describe that supplementsare given as recommended to 59 percent of
breast fed infants in Norway and 64 percent of those in
Sweden[89,90].
Of note, vitamin D supplementation may rarely trigger idiopathic
infantile hypercalcemia (IIH), which ischaracterized by
hypercalcemia, failure to thrive, vomiting, dehydration, and
nephrocalcinosis. The disorderhas been attributed to mutations in
the gene encoding CYP24A1, an enzyme involved in vitamin
Dmetabolism [91]. The effect is dose-related, and the disorder is
uncommon among infants given standardsupplement doses of vitamin D.
The risk and speed of developing symptomatic IIH appears to be
greater ininfants given bolus dosing of vitamin D (eg, 600,000 int.
units every three months, as has been done in somecountries).
The current lack of information about the frequency of CYP24A1
mutations precludes a universal screeningrecommendation for IIH in
infants given standard doses of vitamin D. However, infants should
be evaluatedfor the possibility of IIH if they develop suspicious
symptoms or have a family history of hypercalcemia. Thefirst step
in the evaluation is to measure serum 25(OH)D and calcium levels.
If these levels are elevated (eg,25(OH)D>50 ng/mL [72 nmol/L],
calcium >the upper limit of normal for age), then vitamin D
supplementsshould be stopped and the infant should be further
evaluated for evidence of IIH, which includes suppressedparathyroid
hormone, hypercalcuria, and nephrocalcinosis.
Another strategy to raise vitamin D levels in exclusively
breast-fed infants without feeding them supplementsis to administer
high doses of vitamin D (4000 to 6400 int. units per day) to the
lactating mother [79,92]. Thisintervention sufficiently increases
the vitamin D content of breast milk to allow sufficient vitamin D
intake bythe infant without causing hypervitaminosis D in the
mother. More moderate vitamin D doses (eg, maternalintake of 1500
to 2000 int. units daily during pregnancy and lactation) are
generally sufficient to maintainblood levels of vitamin D of >30
ng/mL in the mother and will improve the infant's vitamin D status
at birth.However, these doses may not result in sufficient vitamin
D in breast milk to meet the infants needs, andsupplementation may
still be necessary for the infant. (See 'Vitamin D supplementation
of pregnant women'below.)
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
8/22
Vitamin D fortification of milk and other foods In the United
States, milk and orange juice are fortifiedwith 400 int. units of
vitamin D per liter. Consumption of at least one liter of fortified
formula or beveragesdaily is usually sufficient to meet at least
two-thirds of the current guidelines for daily vitamin D intake
(600int. units daily for children one year and older). However,
many children do not consume this quantity offortified beverages
and may need supplementation to meet guidelines for vitamin D
intake. This is particularlytrue if juice intake is limited because
of its high content of sugar and calories, which have been
implicated inthe development of childhood obesity.
Milk is not routinely fortified with vitamin D in many countries
outside of the United States. Fortificationpractices and vitamin D
intakes vary widely among European countries [93], and nearly 45
percent ofchildren and adolescents across Europe have vitamin D
insufficiency or deficiency (serum 25(OH)D 30 ng/mL (75 nmol/L) and
maintainthese levels over a year long period [97,98]. The Canadian
Pediatric Society recommends supplementationwith 800 int. units
daily of vitamin D for breast-fed infants living in northern
communities during the winter[99]. The requirement for vitamin D
may be even higher for infants of dark skinned mothers (unless
thesemothers received adequate vitamin D supplementation through
pregnancy), and those who live in the higherlatitudes.
Vitamin D supplementation of pregnant women To optimize an
infants vitamin D status and bonehealth at birth, it is important
to ensure that the pregnant mother has sufficient vitamin D intake
throughoutpregnancy. This is because maternal vitamin D crosses the
placental barrier and builds up fetal stores ofvitamin D,
particularly during the third trimester. This is of greater concern
in dark skinned women, thoseliving in higher latitudes, and those
whose cultural and religious practices include complete skin
cover.
In pregnant and lactating women, the recommended dietary
allowance for vitamin D is 600 int. units daily,which is the same
as for women who are not pregnant [75]. However, some studies
suggest that this intakemay not be adequate: One study of pregnant
women in Finland found that 71 percent were vitamin Ddeficient
(25(OH)D levels 20 ng/mL (50 nmol/L) in pregnant women,
particularly in dark skinned women[101-108]. (See "Vitamin D
deficiency in adults: Definition, clinical manifestations, and
treatment", section on'Pregnancy'.)
Exposure to sunlight Sun exposure allows for cutaneous Vitamin D
synthesis. During most seasons, 10to 15 minutes of sun exposure
near midday is sufficient for adequate vitamin D synthesis in
light-skinnedindividuals [1]. However, darker skin pigmentation,
winter season, or northern latitudes can markedly reduceskin
synthesis of vitamin D and increase the need for dietary sources.
(See 'Decreased synthesis' above.)
The advantage of sun exposure in providing vitamin D needs to be
balanced against the potential risk for skincancer from excessive
exposure to ultraviolet radiation, particularly melanoma, which is
one of the mostcommon forms of cancer among young adults [109]. The
latter is particularly concerning in light skinnedindividuals
during the summer months, especially if there is a family history
of skin cancer. These concernshave led to recommendations that
direct sunlight exposure should be avoided for infants younger than
sixmonths old, and that sun exposure should be limited in older
children, through the use of protective clothingand sunscreen
[110,111]. Deliberate exposure to sun or artificial sources of
ultraviolet radiation should beavoided; outdoor activities should
be encouraged for their value in providing exercise, but sun-safety
shouldbe emphasized [111]. Studies are necessary to assess the
impact of these recommendations in dark skinnedchildren, and it is
possible that relaxation of these measures in dark skinned children
will allow for sufficient
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=P
9/22
cutaneous Vitamin D synthesis in the summer months, particularly
in lower latitudes.
SCREENING FOR VITAMIN D DEFICIENCY Screening is recommended in
populations at risk for vitaminD deficiency, but not for the
population at large. The best test for assessing vitamin D status
is to measure25(OH)D levels using a reliable assay. This may be a
radioimmunoassay, HPLC, or LC-MS/MS. (See'Vitamin D assays'
above.)
We suggest screening the following patient groups, each of which
has increased likelihood of rickets orosteopenia [1]:
Some centers also routinely screen obese children for vitamin D
deficiency. One guideline also suggestsroutine screening of
patients at risk for low bone density, such as those with
amenorrhea, immobilization,chronic kidney or liver disease, and for
those who are pregnant or lactating [113].
ADDITIONAL EVALUATION
The possibility of rickets should be considered in growing
children with vitamin D levels below 20 ng/mL (50nmol/L). For these
children who are at higher risk for rickets, the evaluation should
include measurements ofserum calcium, phosphorus, ALP, and
parathyroid hormone (PTH) (table 1). Radiographic evaluation
forrickets should be performed if the child is young or if there is
a high clinical suspicion of rickets, based on riskfactors or
physical signs. (See "Overview of rickets in children", section on
'Clinical manifestations'.)
Rickets can be further classified as calcipenic (hypocalcemic)
or hypophosphatemic rickets. Isolated vitaminD deficiency typically
causes calcipenic rickets, but other causes of rickets may coexist
in the same patientand should be considered. The detailed
evaluation of a patient with rickets is discussed in a separate
topicreview. (See "Overview of rickets in children".)
TREATMENT
Dosing and forms
Vitamin D deficiency or insufficiency Vitamin D replacement
therapy is necessary for childrenpresenting with low vitamin D
levels (25(OH)D 500 int. units/L in neonates or>1000 int.
units/L in children up to 9 years of age; ALP levels tend to
decrease after puberty) [112] (See'Biochemical changes' above.)
Infants
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
10/22
For children who do not achieve therapeutic concentrations of
25(OH)D following this regime, higher doses of25(OH)D will be
necessary. The specific dose of vitamin D required to raise 25(OH)D
levels into thetherapeutic range remains under investigation, but
in general depends on the severity of the deficiency andindividual
factors that potentially include vitamin D absorption and
degradation of 25(OH)D. One study foundno increase in 25(OH)D
levels following administration of 200 or 1000 int. units of
vitamin D3 for 11 weeks tohealthy adolescents whose 25(OH)D levels
were >20 ng/mL at baseline [116]. Another study reported that
adaily dose of 5000 int. units of vitamin D3 was more effective
than a dose of 2000 int. units over three monthsat achieving
25(OH)D >30 ng/mL in adults with 25(OH)D levels 30 ng/mL.
Multiple dosing regimens have been shown to be effective. The
cumulative amount of vitamin Dsupplementation appears to be more
important than the dosing frequency. As an example, one study
inadults found that the same cumulative dose given daily (1500 int.
units), weekly (10,500 int. units), or monthly(45,000 int. units)
resulted in similar increments in serum 25(OH)D concentration
[118]. (See "Vitamin Ddeficiency in adults: Definition, clinical
manifestations, and treatment", section on 'Dosing'.)
For patients with elevated levels of parathyroid hormone (PTH)
or clinical evidence of rickets, calcium shouldbe supplemented
along with vitamin D. This is because vitamin D replacement and a
normalization of PTHlevels can precipitate hypocalcemia by
suppressing bone resorption and from increased bone
mineralization,also referred to as the "hungry bone" syndrome.
Hence, calcium replacement is necessary along with vitaminD
replacement and should be given at doses of 30 to 75 mg/kg/day of
elemental calcium given in two to threedivided doses for two to
four weeks, until vitamin D doses have been reduced to maintenance
levels of 600 to1000 int. units daily. (See "Etiology and treatment
of calcipenic rickets in children", section on 'Treatment'.)
In children with symptomatic hypocalcemia (including seizures or
tetany), one or more intravenous boluses ofcalcium gluconate may be
necessary at a dose of 10 to 20 mg/kg of elemental calcium
administered slowlyintravenously over 5 to 10 minutes (1 to 2 mL/kg
of 10 percent calcium gluconate) [119].
Vitamin D may be administered as vitamin D2 (ergocalciferol) or
as vitamin D3 (cholecalciferol). The potencyof vitamin D3 in
relation to vitamin D remains somewhat controversial. Typically,
the two forms of vitamin Dare used interchangeably, although some
studies indicate that vitamin D3 may be more potent than vitaminD2
and cause two to three-fold greater storage of vitamin D [120,121].
Liquid vitamin D preparationscontaining 8000 int. units/ mL of
Vitamin D2 are available, as are gelatin capsules containing 50,000
int.units.
Short-term administration of high dose vitamin D, known as stoss
therapy, is an effective alternative. Asingle dose of 600,000 int.
units of vitamin D as an intramuscular injection is an excellent
solution forpersistent non-compliance; however, this vitamin D
preparation is no longer available in the US. Somestudies have
reported administering 100,000 to 600,000 int. units of vitamin D
orally over a period of one tofive days for infants and children
older than one month of age [122,123], followed by maintenance
dosing. Ifsuch an approach is chosen, it is important to use oral
preparations that do not contain propylene glycolbecause this can
be toxic in high concentrations. Tablets containing 25,000 to
50,000 int. units of vitamin Dmay be crushed, or a 50,000 int.
units capsule soaked in water to soften this before administering
thesoftened capsule in blended food. Liquid preparations often
contain propylene glycol, and should be avoidedfor stoss
dosing.
Administration of calcitriol (1,25(OH) D) is not necessary,
except in conditions of severe vitamin D deficiency
Children >12 months old: 2000 int. units/day for six weeks,
or 50,000 int. units per week for six weeks[114], followed by
maintenance dosing of 600 to 1000 int. units/day.
Children with obesity, malabsorptive diseases, or those on
medications that impact vitamin Dmetabolism may require higher
replacement doses (two to three times higher than in children
withoutthese conditions), followed by higher maintenance dosing
[76] (see 'Obesity' above and 'Malabsorptionand other medical
conditions' above and 'Medications' above). Much higher doses may
be necessary inconditions such as cystic fibrosis [115]. (See
"Cystic fibrosis: Nutritional issues", section on 'Vitamin D'.)
3
2
2
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
11/22
with severe symptomatic hypocalcemia. In such situations,
calcitriol administration at a dose of 20 to 100ng/kg/day with
intravenous calcium gluconate and high doses of vitamin D may
normalize plasma calciumlevels more rapidly than standard vitamin D
treatments. However, calcitriol plays no role in building upvitamin
D stores.
Borderline vitamin D levels As discussed above, vitamin D levels
above 20 ng/mL have not beenassociated with adverse clinical
effects in children. However, studies in adults have shown impaired
calciumabsorption and lower bone density at 25(OH)D levels between
20 and 30 ng/mL (50 to 75 nmol/L), andadditional studies are needed
to examine these issues more carefully in children. (See 'Defining
vitamin Dsufficiency' above.)
Based on currently available data, we do not usually give
vitamin D replacement therapy to infants or childrenfor low-normal
vitamin D levels (25(OH)D between 20 and 30 ng/mL (50 to 75
nmol/L)), unless there areother signs of vitamin D deficiency or
important risk factors (eg, very low nutritional intake or
perinatal riskfactors) (see 'Causes of vitamin D deficiency'
above). However, the diets of such children should bereviewed, and
vitamin D supplements should be given as needed to meet current
intake recommendations.We also suggest monitoring 25(OH)D levels in
these children periodically, and initiating treatment if levels
fallbelow 20 ng/mL (50 nmol/L). (See 'Recommendations for vitamin D
intake' above.)
Follow-up Patients with rickets require close follow-up to
document radiographic healing, normalization ofserum 25(OH)D, PTH,
calcium and phosphorus levels, and long-term maintenance of vitamin
D sufficiency.Recovery is associated with an initial increase in
serum phosphate, alkaline phosphatase (ALP) and1,25(OH) D levels,
followed by a gradual normalization of ALP; PTH; 1,25(OH) D; and
25(OH)D levels. (See"Etiology and treatment of calcipenic rickets
in children", section on 'Monitoring'.)
Patients without rickets but with low vitamin D levels and
biochemical changes such as elevated ALP levelsor PTH levels should
also be monitored to ensure treatment adherence. We generally check
serum 25(OH)Dlevels and other chemistries after six to eight weeks
of high-dose therapy, then again after several months ofmaintenance
therapy, then annually thereafter. It is important to monitor
25(OH)D levels to ensure thatvitamin D requirements continue to be
met after vitamin D deficiency has been treated, particularly in
highrisk population groups.
Patients presenting with only low levels of vitamin D and no
other biochemical changes or evidence of ricketsrequire less
intense monitoring. In our practice, we generally check 25(OH)D
levels after two to three months,then as needed thereafter,
depending on the adequacy of the patients intake and adherence to
maintenancesupplements.
INFORMATION FOR PATIENTS UpToDate offers two types of patient
education materials, The Basicsand Beyond the Basics. The Basics
patient education pieces are written in plain language, at the 5 to
6grade reading level, and they answer the four or five key
questions a patient might have about a givencondition. These
articles are best for patients who want a general overview and who
prefer short, easy-to-read materials. Beyond the Basics patient
education pieces are longer, more sophisticated, and moredetailed.
These articles are written at the 10 to 12 grade reading level and
are best for patients who wantin-depth information and are
comfortable with some medical jargon.
Here are the patient education articles that are relevant to
this topic. We encourage you to print or e-mailthese topics to your
patients. (You can also locate patient education articles on a
variety of subjects bysearching on patient info and the keyword(s)
of interest.)
SUMMARY AND RECOMMENDATIONS
2 2
th th
th th
Basics topic (see "Patient information: Vitamin D for babies and
children (The Basics)")
Groups at risk for vitamin D deficiency include premature
infants or exclusively breast-fed infants(unless they are reliably
taking supplements of 400 int. units daily), dark-skinned children
on vegetarianand unusual diets, children living at higher
latitudes, and children with conditions of malabsorption orthose
who are taking certain medications. (See 'Causes of vitamin D
deficiency' above.)
For infants and children with the above risk factors, we suggest
laboratory screening for vitamin D
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
12/22
Use of UpToDate is subject to the Subscription and License
Agreement.
REFERENCES
1. Misra M, Pacaud D, Petryk A, et al. Vitamin D deficiency in
children and its management: review ofcurrent knowledge and
recommendations. Pediatrics 2008; 122:398.
2. Weisberg P, Scanlon KS, Li R, Cogswell ME. Nutritional
rickets among children in the United States:review of cases
reported between 1986 and 2003. Am J Clin Nutr 2004; 80:1697S.
3. McAllister JC, Lane AT, Buckingham BA. Vitamin D deficiency
in the San Francisco Bay Area. J PediatrEndocrinol Metab 2006;
19:205.
4. Mylott BM, Kump T, Bolton ML, Greenbaum LA. Rickets in the
Dairy State. WMJ 2004; 103:84.5. Shah M, Salhab N, Patterson D,
Seikaly MG. Nutritional rickets still afflict children in north
Texas. Tex
Med 2000; 96:64.6. Mansbach JM, Ginde AA, Camargo CA Jr. Serum
25-hydroxyvitamin D levels among US children aged
1 to 11 years: do children need more vitamin D? Pediatrics 2009;
124:1404.7. Saintonge S, Bang H, Gerber LM. Implications of a new
definition of vitamin D deficiency in a
multiracial us adolescent population: the National Health and
Nutrition Examination Survey III.Pediatrics 2009; 123:797.
8. Gordon CM, Feldman HA, Sinclair L, et al. Prevalence of
vitamin D deficiency among healthy infantsand toddlers. Arch
Pediatr Adolesc Med 2008; 162:505.
9. Willer CJ, Dyment DA, Sadovnick AD, et al. Timing of birth
and risk of multiple sclerosis: populationbased study. BMJ 2005;
330:120.
deficiency (Grade 2C). Screening is accomplished by measuring
25(OH)D levels. (See 'Screening forvitamin D deficiency'
above.)
Standards for defining vitamin D status in healthy children are
not well established. The most commondefinitions are (see 'Defining
vitamin D sufficiency' above):
Vitamin D sufficiency: 25(OH)D 20 ng/mL (50 nmol/L)
Vitamin D insufficiency: 25(OH)D between 16 and 20 ng/mL (40 to
50 nmol/L)
Vitamin D deficiency: 25(OH)D 15 ng/mL (37.5 nmol/L)
All infants and children (including adolescents) should receive
at least 400 International Units (int. units;IU) daily of vitamin D
beginning soon after birth. The Institute of Medicine now
recommends a higherintake of 600 int. units of vitamin D daily for
healthy children between 1 and 18 years of age. High riskgroups may
have a higher requirement of vitamin D to maintain 25(OH)D levels
in the sufficient range.(See 'Recommendations for vitamin D intake'
above.)
For exclusively breast-fed infants we recommend vitamin D
supplementation providing 400 int. unitsdaily (Grade 1B). Infants
who are partially formula-fed usually also require supplementation
unless theirformula intake is >1000 mL (33 oz) daily. Use of
supplements in purely breast-feeding neonates andinfants may be
avoided if maternal intake of vitamin D is 4000 to 6000 int.
units/day. (See 'Vitamin Dsupplementation for infants' above.)
For infants and children with 25(OH)D levels below 20 ng/mL (50
nmol/L), we recommend vitamin Drepletion (Grade 1C). In our
practice, we use a six-week course of vitamin D replacement at
dosesranging from 1000 to 2000 int. units per day, depending on the
degree of deficiency and the age of theindividual, followed by
maintenance dosing of 600 to 1000 int. units/day. Some children may
requirehigher doses. Either vitamin D2 (ergocalciferol) or vitamin
D3 (cholecalciferol) may be used. A variety ofother dosing schemes
are also effective for children older than one year, including use
of 50,000 int.units weekly for six weeks. (See 'Dosing and forms'
above.)
After treatment for vitamin D deficiency, follow-up laboratory
testing is important to verify response andadherence to treatment,
and that normal vitamin D levels are sustained on maintenance
dosing. (See'Follow-up' above.)
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
13/22
10. Willis JA, Scott RS, Darlow BA, et al. Seasonality of birth
and onset of clinical disease in children andadolescents (0-19
years) with type 1 diabetes mellitus in Canterbury, New Zealand. J
PediatrEndocrinol Metab 2002; 15:645.
11. Merlino LA, Curtis J, Mikuls TR, et al. Vitamin D intake is
inversely associated with rheumatoid arthritis:results from the
Iowa Women's Health Study. Arthritis Rheum 2004; 50:72.
12. Cantorna MT, Munsick C, Bemiss C, Mahon BD.
1,25-Dihydroxycholecalciferol prevents andameliorates symptoms of
experimental murine inflammatory bowel disease. J Nutr 2000;
130:2648.
13. Mersch PP, Middendorp HM, Bouhuys AL, et al. Seasonal
affective disorder and latitude: a review ofthe literature. J
Affect Disord 1999; 53:35.
14. Rsnen P, Hakko H, Jrvelin MR. Prenatal and perinatal risk
factors for psychiatric diseases of earlyonset. Results are
different if seasons are categorised differently. BMJ 1999;
318:1622.
15. Bodiwala D, Luscombe CJ, French ME, et al. Susceptibility to
prostate cancer: studies on interactionsbetween UVR exposure and
skin type. Carcinogenesis 2003; 24:711.
16. Garland CF, Comstock GW, Garland FC, et al. Serum
25-hydroxyvitamin D and colon cancer: eight-year prospective study.
Lancet 1989; 2:1176.
17. Garland FC, Garland CF, Gorham ED, Young JF. Geographic
variation in breast cancer mortality in theUnited States: a
hypothesis involving exposure to solar radiation. Prev Med 1990;
19:614.
18. Grant WB. An ecologic study of dietary and solar
ultraviolet-B links to breast carcinoma mortality rates.Cancer
2002; 94:272.
19. Pritchard RS, Baron JA, Gerhardsson de Verdier M. Dietary
calcium, vitamin D, and the risk ofcolorectal cancer in Stockholm,
Sweden. Cancer Epidemiol Biomarkers Prev 1996; 5:897.
20. Tuohimaa P, Tenkanen L, Ahonen M, et al. Both high and low
levels of blood vitamin D are associatedwith a higher prostate
cancer risk: a longitudinal, nested case-control study in the
Nordic countries. Int JCancer 2004; 108:104.
21. Reis JP, von Mhlen D, Miller ER 3rd, et al. Vitamin D status
and cardiometabolic risk factors in theUnited States adolescent
population. Pediatrics 2009; 124:e371.
22. Ginde AA, Mansbach JM, Camargo CA Jr. Association between
serum 25-hydroxyvitamin D level andupper respiratory tract
infection in the Third National Health and Nutrition Examination
Survey. ArchIntern Med 2009; 169:384.
23. Science M, Maguire JL, Russell ML, et al. Low serum
25-hydroxyvitamin D level and risk of upperrespiratory tract
infection in children and adolescents. Clin Infect Dis 2013;
57:392.
24. Fox AT, Du Toit G, Lang A, Lack G. Food allergy as a risk
factor for nutritional rickets. Pediatr AllergyImmunol 2004;
15:566.
25. Allen KJ, Koplin JJ, Ponsonby AL, et al. Vitamin D
insufficiency is associated with challenge-provenfood allergy in
infants. J Allergy Clin Immunol 2013; 131:1109.
26. Muehleisen B, Gallo RL. Vitamin D in allergic disease:
shedding light on a complex problem. J AllergyClin Immunol 2013;
131:324.
27. Camargo CA Jr, Clark S, Kaplan MS, et al. Regional
differences in EpiPen prescriptions in the UnitedStates: the
potential role of vitamin D. J Allergy Clin Immunol 2007;
120:131.
28. Brehm JM, Celedn JC, Soto-Quiros ME, et al. Serum vitamin D
levels and markers of severity ofchildhood asthma in Costa Rica. Am
J Respir Crit Care Med 2009; 179:765.
29. Gupta A, Bush A, Hawrylowicz C, Saglani S. Vitamin D and
asthma in children. Paediatr Respir Rev2012; 13:236.
30. Holick MF. Vitamin D status: measurement, interpretation,
and clinical application. Ann Epidemiol 2009;19:73.
31. de la Hunty A, Wallace AM, Gibson S, et al. UK Food
Standards Agency Workshop Consensus Report:the choice of method for
measuring 25-hydroxyvitamin D to estimate vitamin D status for the
UKNational Diet and Nutrition Survey. Br J Nutr 2010; 104:612.
32. Hollis BW. Circulating 25-hydroxyvitamin D levels indicative
of vitamin D sufficiency: implications forestablishing a new
effective dietary intake recommendation for vitamin D. J Nutr 2005;
135:317.
33. Bischoff-Ferrari HA, Dietrich T, Orav EJ, Dawson-Hughes B.
Positive association between 25-hydroxyvitamin D levels and bone
mineral density: a population-based study of younger and older
adults. Am JMed 2004; 116:634.
34. Heaney RP, Dowell MS, Hale CA, Bendich A. Calcium absorption
varies within the reference range forserum 25-hydroxyvitamin D. J
Am Coll Nutr 2003; 22:142.
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
14/22
35. Vieth R, Ladak Y, Walfish PG. Age-related changes in the
25-hydroxyvitamin D versus parathyroidhormone relationship suggest
a different reason why older adults require more vitamin D. J
ClinEndocrinol Metab 2003; 88:185.
36. Kreiter SR, Schwartz RP, Kirkman HN Jr, et al. Nutritional
rickets in African American breast-fedinfants. J Pediatr 2000;
137:153.
37. Spence JT, Serwint JR. Secondary prevention of vitamin
D-deficiency rickets. Pediatrics 2004;113:e70.
38. Outila TA, Krkkinen MU, Lamberg-Allardt CJ. Vitamin D status
affects serum parathyroid hormoneconcentrations during winter in
female adolescents: associations with forearm bone mineral
density.Am J Clin Nutr 2001; 74:206.
39. Jones G, Blizzard C, Riley MD, et al. Vitamin D levels in
prepubertal children in Southern Tasmania:prevalence and
determinants. Eur J Clin Nutr 1999; 53:824.
40. Jones G, Dwyer T, Hynes KL, et al. Vitamin D insufficiency
in adolescent males in Southern Tasmania:prevalence, determinants,
and relationship to bone turnover markers. Osteoporos Int 2005;
16:636.
41. Pettifor JM, Isdale JM, Sahakian J, Hansen JD. Diagnosis of
subclinical rickets. Arch Dis Child 1980;55:155.
42. Goel KM, Sweet EM, Logan RW, et al. Florid and subclinical
rickets among immigrant children inGlasgow. Lancet 1976;
1:1141.
43. Cheng S, Tylavsky F, Krger H, et al. Association of low
25-hydroxyvitamin D concentrations withelevated parathyroid hormone
concentrations and low cortical bone density in early pubertal
andprepubertal Finnish girls. Am J Clin Nutr 2003; 78:485.
44. Holick MF. Photosynthesis of vitamin D in the skin: effect
of environmental and life-style variables. FedProc 1987;
46:1876.
45. Callaghan AL, Moy RJ, Booth IW, et al. Incidence of
symptomatic vitamin D deficiency. Arch Dis Child2006; 91:606.
46. Specker BL, Valanis B, Hertzberg V, et al. Sunshine exposure
and serum 25-hydroxyvitamin Dconcentrations in exclusively
breast-fed infants. J Pediatr 1985; 107:372.
47. Stein EM, Laing EM, Hall DB, et al. Serum 25-hydroxyvitamin
D concentrations in girls aged 4-8 y livingin the southeastern
United States. Am J Clin Nutr 2006; 83:75.
48. Harkness L, Cromer B. Low levels of 25-hydroxy vitamin D are
associated with elevated parathyroidhormone in healthy adolescent
females. Osteoporos Int 2005; 16:109.
49. Binet A, Kooh SW. Persistence of Vitamin D-deficiency
rickets in Toronto in the 1990s. Can J PublicHealth 1996;
87:227.
50. Gordon CM, DePeter KC, Feldman HA, et al. Prevalence of
vitamin D deficiency among healthyadolescents. Arch Pediatr Adolesc
Med 2004; 158:531.
51. Cosgrove L, Dietrich A. Nutritional rickets in breast-fed
infants. J Fam Pract 1985; 21:205.52. Cole CR, Grant FK, Tangpricha
V, et al. 25-hydroxyvitamin D status of healthy, low-income,
minority
children in Atlanta, Georgia. Pediatrics 2010; 125:633.53.
Sullivan S, Rosen C, Chen T, et al. Seasonal changes in serum
25(OH)D in adolescent girls in Maine
[meeting abstract]. J Bone Mineral Res 2003; 18(Suppl
2):S407.54. Ziegler EE, Hollis BW, Nelson SE, Jeter JM. Vitamin D
deficiency in breastfed infants in Iowa.
Pediatrics 2006; 118:603.55. Roth DE, Martz P, Yeo R, et al. Are
national vitamin D guidelines sufficient to maintain adequate
blood
levels in children? Can J Public Health 2005; 96:443.56.
Sullivan SS, Rosen CJ, Halteman WA, et al. Adolescent girls in
Maine are at risk for vitamin D
insufficiency. J Am Diet Assoc 2005; 105:971.57. Matsuoka LY,
Ide L, Wortsman J, et al. Sunscreens suppress cutaneous vitamin D3
synthesis. J Clin
Endocrinol Metab 1987; 64:1165.58. Tangpricha V, Turner A, Spina
C, et al. Tanning is associated with optimal vitamin D status
(serum 25-
hydroxyvitamin D concentration) and higher bone mineral density.
Am J Clin Nutr 2004; 80:1645.59. Del Arco C, Riancho JA, Luzuriaga
C, et al. Vitamin D status in children with Down's syndrome. J
Intellect Disabil Res 1992; 36 ( Pt 3):251.60. Bowman SA.
Beverage choices of young females: changes and impact on nutrient
intakes. J Am Diet
Assoc 2002; 102:1234.61. Greer FR, Krebs NF, American Academy of
Pediatrics Committee on Nutrition. Optimizing bone health
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
15/22
and calcium intakes of infants, children, and adolescents.
Pediatrics 2006; 117:578.62. Hollis BW, Wagner CL. Vitamin D
deficiency during pregnancy: an ongoing epidemic. Am J Clin
Nutr
2006; 84:273.63. Lee JM, Smith JR, Philipp BL, et al. Vitamin D
deficiency in a healthy group of mothers and newborn
infants. Clin Pediatr (Phila) 2007; 46:42.64. van der Meer IM,
Karamali NS, Boeke AJ, et al. High prevalence of vitamin D
deficiency in pregnant
non-Western women in The Hague, Netherlands. Am J Clin Nutr
2006; 84:350.65. Greer FR. Fat-soluble vitamin supplements for
enterally fed preterm infants. Neonatal Netw 2001; 20:7.66.
Henderson A. Vitamin D and the breastfed infant. J Obstet Gynecol
Neonatal Nurs 2005; 34:367.67. SECTION ON BREASTFEEDING.
Breastfeeding and the use of human milk. Pediatrics 2012;
129:e827.68. Specker BL, Tsang RC, Hollis BW. Effect of race and
diet on human-milk vitamin D and 25-
hydroxyvitamin D. Am J Dis Child 1985; 139:1134.69. Gessner BD,
Plotnik J, Muth PT. 25-hydroxyvitamin D levels among healthy
children in Alaska. J
Pediatr 2003; 143:434.70. Wortsman J, Matsuoka LY, Chen TC, et
al. Decreased bioavailability of vitamin D in obesity. Am J
Clin
Nutr 2000; 72:690.71. Harel Z, Flanagan P, Forcier M, Harel D.
Low vitamin D status among obese adolescents: prevalence
and response to treatment. J Adolesc Health 2011; 48:448.72.
Pazianas M, Butcher GP, Subhani JM, et al. Calcium absorption and
bone mineral density in celiacs
after long term treatment with gluten-free diet and adequate
calcium intake. Osteoporos Int 2005;16:56.
73. Lehmann B, Rudolph T, Pietzsch J, Meurer M. Conversion of
vitamin D3 to 1alpha,25-dihydroxyvitaminD3 in human skin
equivalents. Exp Dermatol 2000; 9:97.
74. Pettifor JM. Nutritional and drug-induced rickets and
osteomalacia. In: Primer on the Metabolic andBone Diseases and
Disorders of Bone Metabolism, 6th ed, Favus MJ (Ed), American
Society for Boneand Mineral Research, Washington, DC 2006.
p.399.
75. Institute of Medicine, Food and Nutrition Board. Dietary
reference intakes for calcium and vitamin D.National Academy Press,
Washington, DC 2010. Available at:
http://books.nap.edu/openbook.php?record_id=13050. (Accessed on
December 14, 2010).
76. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al.
Evaluation, treatment, and prevention of vitamin Ddeficiency: an
Endocrine Society clinical practice guideline. J Clin Endocrinol
Metab 2011; 96:1911.
77. Dietary reference intakes for calcium and vitamin D.
Pediatrics 2012; 130:e1424.78. Braegger C, Campoy C, Colomb V, et
al. Vitamin D in the healthy European paediatric population. J
Pediatr Gastroenterol Nutr 2013; 56:692.79. Wagner CL, Hulsey
TC, Fanning D, et al. High-dose vitamin D3 supplementation in a
cohort of
breastfeeding mothers and their infants: a 6-month follow-up
pilot study. Breastfeed Med 2006; 1:59.80. Greer FR. Issues in
establishing vitamin D recommendations for infants and children. Am
J Clin Nutr
2004; 80:1759S.81. Sonneville KR, Gordon CM, Kocher MS, et al.
Vitamin d, calcium, and dairy intakes and stress
fractures among female adolescents. Arch Pediatr Adolesc Med
2012; 166:595.82. Taylor JA, Geyer LJ, Feldman KW. Use of
supplemental vitamin d among infants breastfed for
prolonged periods. Pediatrics 2010; 125:105.83. Perrine CG,
Sharma AJ, Jefferds ME, et al. Adherence to vitamin D
recommendations among US
infants. Pediatrics 2010; 125:627.84. Update on Vitamin D:
Position statement by the Scientific Advisory Committee on
Nutrition. The
Stationery Office, London, 2007. Available
at:http://www.sacn.gov.uk/pdfs/sacn_position_vitamin_d_2007_05_07.pdf
(Accessed on December 14,2010).
85. Williamson S, Greene S. Rickets: Prevention message is not
getting through. BMJ 2007; 334:1288.86. Ahmed SF, Franey C,
McDevitt H, et al. Recent trends and clinical features of childhood
vitamin D
deficiency presenting to a children's hospital in Glasgow. Arch
Dis Child 2011; 96:694.87. Davies JH, Shaw NJ. Preventable but no
strategy: vitamin D deficiency in the UK. Arch Dis Child 2011;
96:614.
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
16/22
88. Gallo S, Jean-Philippe S, Rodd C, Weiler HA. Vitamin D
supplementation of Canadian infants:practices of Montreal mothers.
Appl Physiol Nutr Metab 2010; 35:303.
89. Lande B, Andersen LF, Baerug A, et al. Infant feeding
practices and associated factors in the first sixmonths of life:
the Norwegian infant nutrition survey. Acta Paediatr 2003;
92:152.
90. Dratva J, Merten S, Ackermann-Liebrich U. Vitamin D
supplementation in Swiss infants. Swiss MedWkly 2006; 136:473.
91. Schlingmann KP, Kaufmann M, Weber S, et al. Mutations in
CYP24A1 and idiopathic infantilehypercalcemia. N Engl J Med 2011;
365:410.
92. Basile LA, Taylor SN, Wagner CL, et al. The effect of
high-dose vitamin D supplementation on serumvitamin D levels and
milk calcium concentration in lactating women and their infants.
Breastfeed Med2006; 1:27.
93. Mensink GB, Fletcher R, Gurinovic M, et al. Mapping low
intake of micronutrients across Europe. Br JNutr 2013; 110:755.
94. Gonzlez-Gross M, Valtuea J, Breidenassel C, et al. Vitamin D
status among adolescents in Europe:the Healthy Lifestyle in Europe
by Nutrition in Adolescence study. Br J Nutr 2012; 107:755.
95. Lehtonen-Veromaa M, Mttnen T, Leino A, et al. Prospective
study on food fortification with vitamin Damong adolescent females
in Finland: minor effects. Br J Nutr 2008; 100:418.
96. Hower J, Knoll A, Ritzenthaler KL, et al. Vitamin D
fortification of growing up milk prevents decrease ofserum
25-hydroxyvitamin D concentrations during winter: a clinical
intervention study in Germany. EurJ Pediatr 2013; 172:1597.
97. El-Hajj Fuleihan G, Nabulsi M, Tamim H, et al. Effect of
vitamin D replacement on musculoskeletalparameters in school
children: a randomized controlled trial. J Clin Endocrinol Metab
2006; 91:405.
98. Maalouf J, Nabulsi M, Vieth R, et al. Short- and long-term
safety of weekly high-dose vitamin D3supplementation in school
children. J Clin Endocrinol Metab 2008; 93:2693.
99. Vitamin D supplementation: Recommendations for Canadian
mothers and infants. Paediatr ChildHealth 2007; 12:583.
100. Viljakainen HT, Saarnio E, Hytinantti T, et al. Maternal
vitamin D status determines bone variables inthe newborn. J Clin
Endocrinol Metab 2010; 95:1749.
101. Brooke OG, Brown IR, Bone CD, et al. Vitamin D supplements
in pregnant Asian women: effects oncalcium status and fetal growth.
Br Med J 1980; 280:751.
102. Cockburn F, Belton NR, Purvis RJ, et al. Maternal vitamin D
intake and mineral metabolism in mothersand their newborn infants.
Br Med J 1980; 281:11.
103. Delvin EE, Salle BL, Glorieux FH, et al. Vitamin D
supplementation during pregnancy: effect onneonatal calcium
homeostasis. J Pediatr 1986; 109:328.
104. Heaney RP, Davies KM, Chen TC, et al. Human serum
25-hydroxycholecalciferol response toextended oral dosing with
cholecalciferol. Am J Clin Nutr 2003; 77:204.
105. Mallet E, Ggi B, Brunelle P, et al. Vitamin D
supplementation in pregnancy: a controlled trial of twomethods.
Obstet Gynecol 1986; 68:300.
106. Maxwell JD, Ang L, Brooke OG, Brown IR. Vitamin D
supplements enhance weight gain and nutritionalstatus in pregnant
Asians. Br J Obstet Gynaecol 1981; 88:987.
107. Vieth R, Chan PC, MacFarlane GD. Efficacy and safety of
vitamin D3 intake exceeding the lowestobserved adverse effect
level. Am J Clin Nutr 2001; 73:288.
108. Grant CC, Stewart AW, Scragg R, et al. Vitamin D during
pregnancy and infancy and infant serum 25-hydroxyvitamin D
concentration. Pediatrics 2014; 133:e143.
109. Balk SJ, Council on Environmental Health, Section on
Dermatology. Ultraviolet radiation: a hazard tochildren and
adolescents. Pediatrics 2011; 127:e791.
110. Ultraviolet light: a hazard to children. American Academy
of Pediatrics. Committee on EnvironmentalHealth. Pediatrics 1999;
104:328.
111. Council on Environmental Health, Balk SJ. Ultraviolet
radiation: a hazard to children and adolescents.Pediatrics 2011;
127:588.
112. Wharton B, Bishop N. Rickets. Lancet 2003; 362:1389.113.
Harel Z, Cromer B, DiVasta AD, Gordon CM. Recommended vitamin D
intake and management of low
vitamin D status in adolescents: A position statement of the
Society for Adolescent Health andMedicine. J Adolesc Health 2013;
52:801.
114. Malabanan A, Veronikis IE, Holick MF. Redefining vitamin D
insufficiency. Lancet 1998; 351:805.
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
17/22
115. Boas SR, Hageman JR, Ho LT, Liveris M. Very high-dose
ergocalciferol is effective for correctingvitamin D deficiency in
children and young adults with cystic fibrosis. J Cyst Fibros 2009;
8:270.
116. Putman MS, Pitts SA, Milliren CE, et al. A randomized
clinical trial of vitamin D supplementation inhealthy adolescents.
J Adolesc Health 2013; 52:592.
117. Diamond T, Wong YK, Golombick T. Effect of oral
cholecalciferol 2,000 versus 5,000 IU on serumvitamin D, PTH, bone
and muscle strength in patients with vitamin D deficiency.
Osteoporos Int 2013;24:1101.
118. Ish-Shalom S, Segal E, Salganik T, et al. Comparison of
daily, weekly, and monthly vitamin D3 inethanol dosing protocols
for two months in elderly hip fracture patients. J Clin Endocrinol
Metab 2008;93:3430.
119. Root AW, Diamone FB. Disorders of mineral homeostasis in
the newborn, infant, child, and adolescent.In: Pediatric
Endocrinology, 3rd ed, Sperling MA (Ed), Saunders, Philadelphia
2008. p.699.
120. Armas LA, Hollis BW, Heaney RP. Vitamin D2 is much less
effective than vitamin D3 in humans. J ClinEndocrinol Metab 2004;
89:5387.
121. Heaney RP, Recker RR, Grote J, et al. Vitamin D(3) is more
potent than vitamin D(2) in humans. J ClinEndocrinol Metab 2011;
96:E447.
122. Hochberg Z, Bereket A, Davenport M, et al. Consensus
development for the supplementation of vitaminD in childhood and
adolescence. Horm Res 2002; 58:39.
123. Shah BR, Finberg L. Single-day therapy for nutritional
vitamin D-deficiency rickets: a preferred method.J Pediatr 1994;
125:487.
Topic 14590 Version 26.0
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
18/22
GRAPHICS
Pathways of vitamin D synthesis
Metabolic activation of vitamin D to calcitriol and its effects
on calciumand phosphate homeostasis. The result is an increase in
the serumcalcium and phosphate concentrations.
UV: ultraviolet.
Graphic 65360 Version 4.0
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
19/22
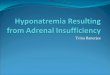
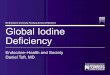
Vitamin D deficiency rickets in a child
Characteristic findings of rickets in children often include
radiographicevidence of decreased mineralization around the
epiphyses and bowingof the lower extremities.
http://www.asbmr.org.
Graphic 53635 Version 2.0
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
20/22
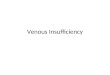
Anteroposterior radiograph of the wrist and hand in a child
withrickets
(A) Rickets. Anteroposterior radiograph of the wrist and hand in
a 3-year-old child withnutritional rickets. The child had been put
on a strict diet without dairy products. Note thewidening, cupping,
and fraying of the distal radius (arrowhead) and ulna metaphyses
with anassociated increase in the thickness of the growth plate
(arrow). These changes are theconsequence of disordered
endochondral growth. (B) Normal. Radiograph of the hand of a
healthy 3-year-old child, without rickets.
Panel A reproduced with permission from: Rao SB, Crawford AH.
Traumatic and Acquired WristDisorders in Children. In: The Wrist
and its Disorders, Lichtman DM, Alexander AH (Eds), WBSaunders,
1999. Copyright 1999 Elsevier. Panel B courtesy of: Lachlan Smith,
MD.
Graphic 80989 Version 6.0
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
21/22
Biochemical manifestations of different stages of vitamin
Ddeficiency, as compared with deficiencies of calcium or
phosphorus
PlasmaCa
PlasmaPO
ALP PTH 25(OH)-D
1,25(OH) -D
X-raychanges
Vitamin D deficiency
Early N or N or N Osteopenia
Moderate N or Rachiticchanges +
Severe or N or Rachiticchanges++
Calciumdeficiency
N or N
Phosphorusdeficiency
N or N or N
N: normal; ALP: alkaline phosphatase; PTH: parathyroid hormone;
25(OH)D: 25-hydroxyvitamin D;1,25(OH) D: 1,25-dihydroxyvitamin
D.
Data from: Levine MA, Zapalowski C, Kappy MS. Disorders of
calcium, phosphate, parathyroidhormone, and Vitamin D. In: Kappy
MS, Allen DB, and Geffner ME (Eds). Principles and Practice
ofPediatric Endocrinology. Charles C. Thomas Co, Springfield,
2005.
Graphic 56687 Version 4.0
++4
2
2
-
24/9/2014 Vitamin D insufficiency and deficiency in children and
adolescents
http://www.uptodate.com.ezproxy.uniandes.edu.co:8080/contents/vitamin-d-insufficiency-and-deficiency-in-children-and-adolescents?topicKey=
22/22
Disclosures: Madhusmita Misra, MD, MPH Nothing to disclose.
Kathleen J Motil, MD, PhDConsultant/Advisory Boards: NPS
Pharmaceuticals [Short gut syndrome (Teduglutide)]. Marc KDrezner,
MD Nothing to disclose. Alison G Hoppin, MD Employee of UpToDate,
Inc.Contributor disclosures are reviewed for conflicts of interest
by the editorial group. When found, theseare addressed by vetting
through a multi-level review process, and through requirements
forreferences to be provided to support the content. Appropriately
referenced content is required of allauthors and must conform to
UpToDate standards of evidence.Conflict of interest policy
Disclosures