Embed Size (px)
Citation preview

INATIONAL CENTER Series 4
For HEALTH STATISTICS Number 3
VITAL and HEALTH STATISTICS
DOCUMENTS AND COMMITTEE REPORTS
Report of the
International Conference
on the Perinatal and Infant
Mortality Problemof the
United StatesSuinrnary of the presentations and discussions at the International Con-
ference on the Perinatal and Infant Mortality Problem of the United
States, Washington, D. C., May 13 and 14, 1965, under the sponsorship
of the National Center for Health Statistics, Public Health Service, U.S.
Department of Health, Education, and Welfare.
Washington, D,C. June 1966
U.S. DEPARTMENT OF
HEALTH, EDUCATION, AND WELFARE Public Health Service
John W. Gardner Wil Iiam H. Stewart
Secretary Surgeon General

Public Health Service Publication No. I()(ltl.series .LNO. :3

NATIONAL CENTER FOR HEALTH STATISTICS
FORREST E. LINDER, PH. D., &%C~07
THEODORE D.WOOLSEY, lkjwy Director
OSWALD K. SAGEN, PH. D., ~$f;@z?z~ ~&C~O?’
WALT R. SIMMONS, hLA., Statistical Advi-ror
3EICE M. WATERHOUSE, M. D., Medical Advi.ror
JAMES E. KELLY, D.D.S., Dental Advisor
LOUIS R. STOLCIS, hf. A., Executive Ojicer
OFFICE OF HEALTH STATISTICS ANALYSIS
IWAO AM.MORIYAMA, PH. D., Chief
DIVIS1ON OF VITAL STATISTICS
ROBERT D. GROVE, PH. D., Chief
DIVISION OF HEALTH INTERVIEW STATISTICS
PHILIP S. LAWRENCE, Sc. D., Chief
DIVISION OF HEALTH RECORDS STATISTICS
MONROE G. SIRKEN, PH. D., Chief
DIVISION OF HEALTH EXAMINATION STATISTICS
ARTHUR J. MCDOWELL, Chief
DIVISION OF DATA PROCESSING
SIDNEY BINDER, Chiej
Public Health Service Publication No. 1000-Series 4-No. 3
Library of Congress Catalog Card Number 66-60073

CONFERENCE PARTICIPANTS
Julie E. Backer, Ph.D.Consultant, Research DepartmentCentral Bureau of Statistics of NorwayOslo, Norway
Katherine Bain, M.D.Assistant Chief for International CooperationChildren’s BureauWelfare AdministrationU.S. Department of Health, Education, andWelfare
Washington, D.C.
James F. Donnelly, M.D.Director, Personal Health DivisionNorth Carolina State Board of HealthRaleigh, North Carolina
Charlotte A, Douglas, O.B.E., M.D., D.P.H.Edinburgh, Scotland
Charles Gershenson, Ph.D.Associate Director, Division of ResearchChildren’s BureauWelfare AdministrationU.S. Department of Health, Education, andWelfare
Washington, D.C.
Bernard G, Greenberg, Ph.D.Professor and Head, Department of BiostatisticsSchool of Public HealthUniversity of North CarolinaChapel Hill, North Carolina
J, H. de Haas, M.D.Department of Swial HygieneNetherlands Institute for PreventiveMedicine
Leiden, The Netherlands
J. H. de Haas-Posthuma, M.D.Department of Social HygieneNetherlands Institute for PreventiveMedicine
Leiden, The Netherlands
Katherine M. Hirst,Reading, England
O.B.E., M.B., D.P.H.
Arthur J. Lesser, M.D., M.P.H.Deputy Chief, Children’s BureauWelfare AdministrationU.S. Department of Health, Education,and Welfare
Washington, D.C.
Forrest E. Linder, Ph.D.Director, National Center for Health StatisticsPublic Health ServiceU.S. Department of Health, Education,and Welfare
Washington, D.C.
I. M. Moriyama, Ph.D.Chief, Office of Health StatisticsAnalysis
National Center for Health StatisticsPublic Health ServiceU.S. Department of Health, Education,and Welfare
Washington, D.C.
Edith L. Potter, M.D., Ph.D.Pathologist, Chicago Lying-In HospitalChicago, Illinois
Richard A. Prindle, M.D., M.P.H.Chief, Division of Public Health MethodsPublic Health ServiceU.S. Department of Health, Education,and Welfare
Washington, D.C.
Franz W. Rosa, M.D., M.P.H.Acting Director, Congenital MalformationsProgram
National Institute of Child Health andHuman Development
Public Health ServiceU.S. Department of Health, Education, andWelfare
Bethesda, Maryland
III

Edward R. Schlesinger, M. D., M.P.H.
Assistant Commissioner of SpecialHealth Services
New York State Department of HealthAlbany, New York
William J. Schull, Ph.D.Department of Human GeneticsUniversity of Michigan Medical
School
Ann Arbor, Michigan
Sam Shapiro, B.S.Director, Division of Research
and StatisticsHealth Insurance Plan of GreaterNew York
New York, New York
William A. Silverman, M.D.
Associate Pediatrician, Babies
HospitalColumbia-Presbyterian MedicalCenter
New York, New York
William H. Stewart, M.D.
Assistant to Special Assistant(Health and Medical Affairs)
Office of the SecretaryU.S. Department of Health, Education,
and Welfare
Washington, D.C.
Dyre Trolle, M.D.
The University Department of Obstetricsand Gynecology
RigshospitaletCopenhagen, Denmark
Myron E. Wegman, M. D., M.P.H.Dean, School of Public Health
University of Michigan
Ann Arbor, Michigan
Jacob Yerushalmy, Ph.D.Director, Cooperative Study ofChild Development
University of CaliforniaOakland, California
NATION’iL CENTER FOR HEALTH STATISTICS—,CONFERENCE STAFF
Helen C. Chase, Dr.P.H.
Statistician, Office ofHealth Statistics Analysis
Barbara J. van den Berg, M.D.
Visiting ScientistOffice of Health StatisticsAnalysis
Elizabeth W. Curran, A .B.Statistician, Office ofHealth Statistics ,inalysis
Iv

-—. .——. .— .
CONTENTS
Introduction ----------------------------------------------------------
Greetings— Dr. Forrest E. Linder ---------------------------------------
Opening Remarks—Dr. Iwao M. Moriyama, Chairman ---------------------
Major Findings of the Forei~Stqdies -----------------------------------Scotland—Dr. Charlotte A. Douglas -----------------------------------England and Wales —Dr. Katherine M. Hirst ---------------------------Norway— Dr. Julie E. Backer ----------------------------------------Denmark—Professor Dyre Trolle ------------------------------------Netherlands—Dr. J. H. de Haas -------------------------------------
Infant Mortality Problems in the United States—Mr. Sam Shapiro ---------Discussion ---------------------------------------------------------
Differential Factors in Infant Mortality ---------------------------------Statistical Artifacts-Dr. Bernard G. Greenberg ----------------------
Table 1.
2,
3,
Change in period of gestation for which fetal death registrationis required: 10 States of the United States, 1950-63------------Change in ratio of fetal deaths by week ofgestation to all fetaldeaths 20 weeks and over, and the relative changein reporting,when minimum period of gestation required for registrationwas lowered: 10 States of the United States, 1950-63-----------Percent of live births of 2,500 grams or less: Minnesota andNorth Dakota, 1955-59----------=--------------------------
Discussion ----------------------------------------------------------Socioeconomic Factors–Dr. Barbara J. vanden Bergand Dr. Arthur J.
Lesser -----------------------------------------------------------Medical Factors—Dr. William A. Silverman ---------------------------
Table +$. Index of fetal maturity ---------------------------------------
Suggestions for Further Smdy ------------------------------------------Definitions and Registration Practices---- ----------------------------Determinantsof InfantMortaliW --------------------------------------Medical Factors Related to Infant Mortality ----------------------------
Summary -------------------------------------------------------------
Page
1
1
2
334567
910
1010
11
12
14
15
1516
16
18181920
21

VI
IN THIS REPOR T a summavy of the international conference on theperinatal and infant morbidity and mortality problem in the UnitedStates is presented. The conference was held in Washington, D. C., onMay “13 and 14, 1965 under the sponsorship of the National CenteY forHealth Statistics. The major findings of studies presented at the con-ference by investigators from DenmaYk, Englana!and Wales, the Nether-lands, Norway, Scotland, and the United States are summarized here.T~ends over the past 30 years as well as the cw?’ent situation in peri-
natal and infant movtality are described. Statistical social, demographic,and medical artifacts associated with infant mortality are discussed in
an effozt to deteymine the reasons fov the mortality differences betweenthe United States and the WesteYn Euvopean countries. Suggestions avemade foy futuye study of vayious aspects of the infant mortality pvoblem.
The infant mortality rates have decreased impressively during the past
30 yeavs; however, in the 1950’s the rates of decline for fow of thecountyies, including the United States, slowed down. The vate of declinein the United States decyeased the most, and the deceleration startedearliev than it did in most of the other countries. The infant” mortalityvates in Denmavk and the Netherlands are still declining with no apparentintem-uption.
Lavge Deductions in infant deaths have been attributed to declines in in-
fectious disease moytality. There have been limited reductions in deaths
from diseases of eavly infancy and congenital malformations, and an in-creasing incidence of perinatal deaths attributed to disoyders of uncer-tain etiology. All investigators descyibed incveasinguse of hospitals fovdeliveyy. There has been an increasing incidence of low-birth-weightinfants in the United States. In countvies wheve some measure of socio-economic level is available infant mortality is highev in the lower classes,and the mortality differential between the upper and lowev classes isincreasing.
Comparison of statistical, demographic, and medical parameters of in-
fant mo~tality showed no clear-cut explanation of the significant inter-
national differences. Further research of infant and perinatal mortalitypvoblems was wged.
SYMBOLS
Data not available------------------------ ---
I Category not applicable------------------- . . . IQuantityzero ---------------------------- -
I Quantitymore than O but less than 0.05---- 0.0 IFigure does not’meet standards of
reliability or precision ------------------ *
L

REPORT OF THEINTERNATIONAL CONFERENCE ON THE
PERINATAL AND INFANT MORTALITY PROBLEM
OF THE UNITED STATESElizabeth W. Curran, O~Ce of Health Statistics Analysis
INTRODUCTION
Two features were noted about the infantmortality rate in the United States in theIQ50’S: (1) the virtual halt in the rate of declineof infant mortality after a Iong period of rapiddecline,1 and (2) the unfavorable position ofUnited States’ infant mortality compared withthat of many other countries. 2 These two pointswere viewed with concern because health authori-ties had for many years pointed with pride to thehigh rate of decrease in infant mortality in theUnited States. In an attempt to illuminate theproblem areas related to infant mortality in theUnited States, a comprehensive study of perinataland infant mortality in several Western Europeancountries of similar social and economic develop-ment was arranged. These countries were Den-mark, England and Wales, the Netherlands.Norway, and Scotland. They were selected becauseof the low infant mortality rates in these countriesover a long period of time, and because of theweH-developed vital statistics systems with rel-ativel y stable definitions and reporting require-ments.
The National Center for Health Statisticssponsored, on May 13 and 14, 1965, a conferenceon the perinatal and infant mortality problem of
lhforiynmrt, I. hi.: Recent change in infant mortality trend.Pub. Hca2th Rep. 75:391-405, hiay 1960.
~Shupiro, S,, and Moriyarna, I. M.: International trends in
infwt mortulity and their implications for the United States.Am. J. Pub. Health. 53:747-’760, May 1963.
the United States. The participants included theforeign investigators and various workers in theUnited States concerned with the problem of infantmortality, The purpose of the conference was todetermine the reasons for the position of the infantmortality rate in the United States.
Following is a summary of the conferenceproceedings.
GREETINGS
DY. Fon’est E Li~eY
In one respect this meeting is a ratherunique event for the National Center for HealthStatistics. The Center and its component partshave had a long history of meetings on a nationalbasis with some international participation forconsidering questions of mortality classificationand other technical questions related to the wholerange of health statistics. However, this is thefirst time that we have called together an inter-national group that is focusing its work on themeaning of United States figures, and on whetherthe apparent substantive indications of the num-bers have validity in terms of interpretations thatmight be given to them. I think this is a forwardstep in our program in the National Centerfor Health Statistics and I hope it is a precursorof other fruitful conferences of this kind in thefuture.
We will look upon this conference as es-tablishing a pattern which we hQpe to repeat, andwhich we hope will be effective in bringing aboutcloser collaboration between the statisticians in
1

this country and those in countries that havesimilar types of problems in vital and healthstatistics.
It is ~ot on the agenda of this meeting todiscuss what might be done in a public healthprogram about finclings shown by the figuresor the causative situations that are indicated byour discussions here,. The problem is to explorethe validity and the meaning of the infant mortalityrate in the United States to see whether thecomparisons of that figure with other countriesare technically valid, and to what extent thediscrepancies and the differences are attributableto either technical questions or to social, demo-graphic, or economic features. It will then be theresponsibility of program directors in the variouspublic health and medical agencies to developrequired and appropriate action programs.
OPENING REMARKS
Dr. Iwao M. MoYiyama,Chairman
LTpto about 15 years ago, the infant mortalityrate in the United States was among the lowestin the world. In the period 1935 to 1950, the infantmortality rate declined at an accelerated pace inthe United States and in other countries of lowmortality, but in the 1950 decade, the rate ofdecline of infant mortality in the United Statesbegan to slow down. Incidentally, the change inmortality conditions was not peculiar to the periodof infancy. The rate at other ages also leveledoff in the United States, but these changes cameseveral years after the beginning of the decelera-tion in the infant mortality rate.
The rapid decline in the infant mortality ratein the late 1930’s and the 1940’s appears to be duemainly to a reduction in deaths from the infectivediseases. This was also generally true for theolder ages. Although further reductions in thedeath rates for the infective diseases are stillpossible, the gains to be made through infectiousdisease control are limited. However, the infantmortality rate for the Unitedabout 20 percent lower todaypneumonia had been eliminated.
2
States would beif deaths from
One of the intriguing questions is why therate of decline of infant mortality rates forcountries such as the United States, Englandand Wales, and Norway has been checked, whereasthe rates for Denmark and the Netherlands havecontinued to decline without apparent interruption.
This situation would not be tcm surprising ifthe level of the rate for Denmark and theNetherlands were considerably higher than thatfor the other countries; however, the contrary istrue. Indeed, the recorded infant mortality ratefor the Netherlands is now among the lowest inthe world. If the present movement of the deazhrates were to continue, there would be no questionin the future as to the country with the lowestperinatal and infant mortality rates.
Obviously, the decline in mortality ratescannot continue indefinitely; at some point theirreducible minimum must be reached. Theirreducible minimum is anybody’s guess, but it issignificant to us that the recorded infant mortalityrate for the Netherlands at this point in time isabout 15 per 1,000 live births, whereas the rate forthe United States is about 25. The position of theUnited States has worsened in relation to that ofother countries. What is more, the gap is widening.
I find this to be a distressing situation onlyif it means that this country is suffering un-necessary infant loss, and one of our main taskshere is to determine whether international dif-ferentials in mortality are real or apparent. Weneed to take a critical look at the situation andrule out, as far as possible, the effects ofartifacts on the comparisons. If the observeddifferences are real, we would like to identify thereason for the differences, and if we are unableto determine the reasons for the differences-andthis is likely in many cases—I hope that we cansuggest studies that will provide the answers.
It seems to me that there are two promisingleads that should be examined concerning theproblem of the relatively high infant mortality ratein the United States. One relates to the differencebetween the rates for the United States and thoseof other countries. The other relates to themarked decrease in the rate of decline for theififant mortality rate in the United States. Eitheror both of these factors might provide the reasonsfor the present unfavorable international pxitionof the United States with respect to the infantmortality rate.

MAJOR FINDINGS
OF THE FOREIGN STUDIES
Scotland
DY. Charlotte A. Douglas
In Scotland there had been impressive de-clines in maternal, fetal, and infant mortalityfrom 1935 until the early 1950’s when the decline inthe mortality rates became more gradual. Sincethen there have been only slight improvements.Dr. Douglas attributed the decline to the compara-tively low birth rate plus the increased avail-ability and utilization of maternity hospitals andmaternal and child care. Today, 80 percent ofthe live births, 90 percent of the fetal deaths, and90 percent of the premature births are deliveredin maternity institutions. The average stay in thehospital is 9 days.
Fetal death registration was instituted in1939, and since then the fetal death rate has de-creased 55 percent. Improvement has been great-est for deaths due to difficult labor, ill-definedconditions, and toxemias.
In general, neonatal mortality is the resultof intra-uterine conditions and birth hazards.‘Ihese causes are responsible for 98 percent offirst-day deaths, 95 percent of first-week deaths,and 90 percent of first-month deaths. Postneonatalmortality, however, is chiefly caused by respira-tory diseases and congenital abnormalities.
Illegitimacy in Scotland is more a socialproblem than a medical one. Now, the illegitimacyratio is 5.2 percent of live births. Although thesechildren are a social problem which may persistin following generations, the effect on the overallinfant mortality rate is comparatively low.
Dr. Douglas placed great emphasis on there-lationship between social class and fetal andinfant mortality. For statistical purposes, thesocial class of the infant is determined by thefather’s occupation. There are five. definedclasses, ranging from professional and man-agerial occupations (class I) to unskilled workers(class V). Although the infant morta.&.y rates inall five classes have declined over the past 30years, the distinction between classes I and V haswidened. In 1939, the fetal death rate of class V
was 11/4 times as high as that of class I; in 1963,it was about 21/3 times as high as that of class I.Neonatal mortality shows a similar trend in classdistinction. In 1939, class I had a neonatalmortality rate of 25.9 and class V of 39.9,whereas in 1963, class I had a neonatal mortalityrate of 9.5 and class V of 22.3. The gap betweenthese two social classes” is greatest in the post-neonatal period; and instead of closing, this gaphas widened throughout the years, for in 1939,the deaths in class V were 6 times that of class1, whereas in 1963 they were 13 times as great.
The Scottish Registrar General’s Report for1943 included an appendix analyzing infant mor-tality and fetal deaths by social class for the year1939, Another tabulation was published in thereport for 1944, and these statistics have beenpublished every year since then. In 1943 ProfessorRichard Titmuss drew attention to the inequalitiesin infant mortality rates in the different socialclasses. His findings were confirmed by Morrisand Heady in 1956. In France, similar mortalitydifferentials were found by CroZe, and in Hungaryby Gzabady.
For some time in Aberdeen, Baird, Kincaid,and others have been working on the problem ofreproductive efficiency and have established thefact that there is an association between maternalstature and pregnancy outcome. The measure ofmaternal stature was used as an index of the“biological fitness” of the mother. They haveshown that for each social class, as a generalrule, the taller the woman the less likely is sheto produce a fetal death or an early neonataldeath.
This tendency to show a widening differencebetween the social classes is difficult to under-stand in a country where medical care is availableto all and where there is ample maternity hospitalaccommodation for any woman requiring expertcare. It is true that the more intelligent womentend to seek prenatal care earlier in pregnancythan do women who may be careless about theirhealth, and who are also overburdened withheavy household duties and the care of otherchildren. This situation, might be expectedto explain to some extent the differingmortalities between the classes, since antenatalcare, however good, cannot be the whole explana-tion. It is true that family size with the concomitantextra burdens on the mother can be exhausting.
3

Should the pregnancies be too rapid, depletion ofthe mother’s reserves of iron may lead tobiological and physical exhaustion. However, onlyabout 11 percent of the women in this country nowhave more than four children, and” the averagefamily size is only 2.5 children. So, some furtherexplanation must be sought.
It would appear that the woman’s growthis influenced not only by heredity but also bynutrition, housing, economic conditions, and theway of life of her parents. It has been foundthat there is a relationship between the numberof siblings in the mother’s parental house andher future reproductive capacity. In nonmanualworkers there is an increase in perinatal mortalityonly when the mother was one of five or morechildren; while in the unskilled classes there is anincrease when the mother had only one sibling.
These facts appear to lead to the generaliza-tion that the smaller the family the better will bethe education and upbringing of the future mother.There is also a continual process of social selec-tion and the usual tendency is for the averagewoman to rise out of her social class or remainwithin it. In this way, as the women with betterreproductive potentialities move upwards, thoseremaining in classes IV and V are biologicallyand physically less able to produce and rearchildren successfully. Probably as these lowerclasses lose more and more women who arereproductive y efficient, the perinatal and infantmortality rates will remain above the average.
England and Wales
Dr. Katherine M Hirst
In England and Wales the total infant mortalityhas declined through the years, but it began tolevel off during the 1950’s as did that of theUnited States. Perinatal mortality began to leveloff at the end of the 1940’s; but in the midfiftiesfetal mortality began to fall again, while first-day mortality remained stationary. Postneonatalmortality appeared to start rising in the midfifties.
Three main causes of death were discussed—infections, diseases of early infancy, and congen-ital malformations. Infant mortality from infec-tions has decreased steadily since 1935. While,in general, deaths from infective conditionscontinued ta lessen during the 1950’s, deathsfrom pneumonia and bronchitis and from gastro-
enteritis stopped declining and began to level offaround 1957.
Diseases of early infancy, which includeimmaturity, birth injuries, and asphyxia andatelectasis, are responsible for 75 percent offirst-day mortality. In this cause group, im-maturity appears to be a strong factor in neonataldeaths, as half of the deaths ascribed to birthinjuries and two-thirds of those ascribed toasphyxia are associated with immaturity. Therehas been no decline in first-day deaths (mainlycaused by diseases of early infancy) since 1950.
There has been virtually no change in themortality rate for congenital malformations dur-ing the fifties.
Low-birth-weight babies constitute one of theimportant high-risk components of infant mor-tality. In England and Wales the proportion ofbabies weighing 2,500 grams or less at birth isabout 6.6 percent of all live births. This percentagehas remained unaltered for the past 10 years. Also,the proportim of babies weighing 1,500 grams orless at birth has remained at 11 percent of thetotal of low-birth-weight babies for the past 10years. Neonatal mortality of low-birth-weightbabies has decreased from 155 neonatal deathsper 1,000 live births of 2,500 grams or lessin 1953 to 128 in 1963; however, mortality ofinfants under 24 hours old has remained almostat a standstill.
There are geographical factors in infant ,andperinatal mortality in England and Wales, in thatthere is a southeast to northwest gradient withthe lower fetal and infant mortality rates in thesoutheast. However, the gap is gradually closing.The urban and rural areas both show this south-east to northwest gradient.
As in Scotland, there is a fairly steep gradientfrom socioeconomic class I to socioeconomicclass V which does not seem to be narrowing.Despite the fact that the gap between the incomeswithin these classes has been decreasing, thedifferences in the infant mortality rates betweenclasses I and V have increased slightly. Dr. Hirstpointed out that one reason for the wideningdisparity is that cultural customs of a group donot necessarily change as rapidly as do economicsituations. One of the most important stepsin lowering infant mortality is the acceptance ofnew ideas, such as receiving antenatal care earlyin pregnancy or being hospitalized for birth;
4

however, changes in attitudes and ways of lifetake time.
Migration between classes may tend to keepthe disparity evident, For example, families withpoor health may drift into the lower socioeconomicclasses. On the other hand, in connection with thematernal stature and infant mortality correlationsdiscussed by Dr. Douglas, the woman who marriesinto a higher social class will, on the average, betaller, will have a better standard of education,and, if she is working, will have a better occupa-tional status than the woman who marries into alower social class. These attributes carry a lowerperinatal mortality.
In conclusion, Dr. Hirst pointed out that thefuture outcome of pregnancy will depend on twoviews—the long-term view, which is the genera-tion effect of a mother’s background, and theshort-term view, which uses parameters ofpregnancy to define the immediate risk to themother. It is important to realize that theimmediate risk is evident because of the mother’sbackground. At any one point in time the mother’sbackground cannot be changed, but action can betaken to minimize the immediate risks involvedin parturition. For England and Wales this meansselection for hospital confinement. At present, 65percent of the pregnant women are hospitalized forbirth. This is the national average, with wide localvariations. On the basis of high risk groups —wom -en over the age of 35, those with four or morechildren, those who require admission on socialgrounds, all primigravidae, and all women withmedical or obstetric abnormalities—hospital ac -commodation should be provided for at least 70percent of the pregnant women in all areasthroughout the country.
Norway
Dr. Julie E. Backev
The infant mortality rate for Norway hasdeclined from 91.1 infant deaths per 1,000 livebirths in 1901 to 16.9 in 1963. The rate ofreduction has varied considerably from period toperiod, For instance, the downward trend wasrelativelyto an end
rapid in the thirties, but came almostduring the Second World War. During
the first decade after the war the relative declimof the infant mortality was the greatest experi-enced in Norway during this century. But in themiddle of the 1950’s this rapid downward trendwas again leveling out, and lately the annual re-duction ratio has been about the same as in theyears just before the Second World War.
Perinatal mortality has declined 39.5 percentin the last 30 years; mortality of infants 7 to27 days old was 70 percent lower in 1961-62than during 1931-35; and deaths of infants 1 to 11months were 75 percent lower. While in 1900,38 percent of all perinatal and infant deaths oc-curred before delivery, during delivery, or be-fore the end of the first week of life, in 1961-62,75 percent of the perinatal and infant deaths oc-curred before the end of the first week of life.
In 1962, 80 percent of the perinatal deathsoccurred before or within 24 hours after birth,This relationship has remained unchanged duringthis century. However, with the better obstetricalservices more infants, especially premature andnot viable, which in years past would have diedprior to or during birth, now have been born aliveand die during the first day of life.
Tuberculosis, the common infectious dis-eases, diarrhea, and enteritis have been prac-tically eliminated as causes of infant deaths. Also,mortality from pneumonia and other diseases ofthe respiratory organs has been considerablyreduced.
As infections caused by external factors havebecome better controlled, deaths from congenitalmalformations and diseases of early infancy havebecome increasingly prominent. While only 27percent of all infant deaths in 1900 were causedby this group, 76 percent of the infant deaths in1962 were caused by it.
As with England and Wales, immaturity hasbeen the most frequently reported of the causesof early infant deaths. Not only has immaturitybeen linked with approximately one-third of alldeaths assigned to congenital malformations anddiseases of early infancy since 1930, but it hasalso frequently been mentioned as a subsidiarycause of death for other diagnoses. In the last 10years, immaturity has been reported by physicianseither as a pyimary or as a secondary cause ofdeath for 64 percent of all infant deaths in thefirst month of life which were classified to dis -
5

eases of early infancy. Of’ the deaths whichoccurred after the first month of life 34 percenthave been attributed to or Iinked with immaturity.
Dr. Backer indicated that, as in other coun-tries, the illegitimate child in “the,.first year oflife has always had a greater risk” of death, butthe proportion of illegitimate babies in Norwayhas not been sufficiently high to affect thenational level of infant mortality.
There. is a direct relationship ~etween themother’s age and the mortality of a baby beforeor during delivery. In a study of “this relation-ship among legitimate births, it was found that therisk of a fetal death increases with the age of themother. Among mothers aged 40-45 years thefetal death rate was 28 per 1,000 live births andfetal deaths—almut three times the rate formothers in their early twenties. In all age groupsof mothers, the fetal death rate was considerablyhigher for first-born infants; however, during thelast 20 years, the fetal death rate for first-borninfants has decreased relatively more than that forchildren born later.
Dr. Backer attributed the great declines inNorway’s infant mortality to general improvementin environmental factors, which cause infections,and in socioeconomic conditions. The increasingincome of the families and the decreasing numberof children per family implied better nutrition,housing, environmental and personal hygiene, inshort, a more healthful standard of living. Theeconomic progress also provided a basis for theintroduction of a comprehensive system of socialsecurity and advances in public health and medicalservices with special bearing on the welfare ofthe’ mother and child. One indication has beenthe increasing number of births occurring inhospitals and maternity homes—from 75 percentin 1951 to 96 percent in 1963. As a rule, the
“.midwife delivers the child without medical as-sistance, but in hospitals and clinics a doctoris always available. Therefore, in”all cases wherecomplications of labor may be expected, themother is sent to a hospital.
Among the different legal measures whichhave contributed largely to the reduction of thematernal and infant mortality and morbidity inNorway are the introduction of national sicknessinsurance in 1911, in 1936 the provision for leaveof absence from work of pregnant women beforeand after delivery., and in 1946 special ,a~low~”ce
for all breadwinners supporting more than onechild.
Denmark
Professor Dyve Trolle
Denmark’s infant and perinatal mortalityrates have decreased by varying degrees. Duringthe period 1921 to 1962, the fetal death ratedecreased 52 percent to 11.9 per 1,000 livebirths and fetal deaths; the perinatal mortalitydecreased 44 percent to 24.9; and the total infantmortality under 1 year of age declined 74 percentto 20.0 per 1,000 live births. While late neonatalmortality of 7 days-1 month decreased 80 percentand postneonatal mortality declined 90 percent,early neonatal mortality under 7 days declinedonly 35 percent.
The relative declines by age have changed asfollows :
I Percent
Under 1 year -- 39 ;; 31Under 1 month-1-11 months--- H 60 ;;
The smaller decline for deaths of infants under1 month old is due to the fact that neonatal deathsare dominated by causes of death which have beensubjected to limited reductions such as congenitalmalformations, birth injuries, and immaturity.The large decreases in mortality have been mostconspicuous for infective and parasitic diseasesand for diseases of the respiratory and digestivesystems. There has been an excess mortalityfrom. most causes of death and in all age groupsat death for males.
The number of infants born out of wedlockdecreased from 1930 to the end of the 1950’s;however, the number has increased since then.In 1962, 8 percent of the live-born infants wereillegitimate. Illegitimate births are considered
6

among the high risk groups, and the excess mor-tality for illegitimate births in Denmark is seenfor all causes except congenital malformationsand hemolytic diseases.
Infant mortality in relation to parity and themother’s marital status shows increasing mor-tality with higher parity for infants of 2,500 gramsor less of both unmarried and married mothers.For infants weighing over 2,500 grams at birth,mortality is lowest for second parity. In allcases mortality is higher for infants of unmarriedmothers.
Since 1945, all women have been allowed ninefree consultations during pregnancy. Three ofthese are with a physician at the followingrecommended intervals: (1) as early as possible,(2) in the 25th week, and (3) in the 34th to the 36thweek of pregnancy. The other six are to be witha midwife in the 20th, 30th, 33d, 37th, 38th, andthe 39th weeks. The proportion of live-born infantswhose mothers take advantage of these free visitshas been increasing over the last 16 years.
Delivery of infants in hospitals has beenincreasing in Denmark. In 1962, 46 percent of thebirths were delivered at home and three-quartersof these were attended by a physician. Otherwise,10 percent of the deliveries were at private clinics,21 percent were at general hospitals, and 23percent were at obstetric departments.
Since 1937, when a health service law forprevention of disease and death during the firstyear of life was enacted, specially trained nurses,the so-called public health nurses, have beenemployed to supervise infants under 1 year inprivate homes. In 1962, there were 658 publichealth nurses employed, a ratio of approximately118 live births per nurse. Although their numberis increasing, there are still many rural districtswith no public health nurses.
Immediately after delivery, the midwife ordoctor notifies the public health nurse and shortlythereafter she pays her first visit to the homein question. In 1962, two-thirds of all infantswere supervised in this way. Euring the infant’sfirst year of life, the nurse pays 12 visits, mostof them during the first month. At these visits,the nurse advises the mother on nursing andfeeding, recommends free prophylactic medicalexaminations, and advises visits to a physicianat symptoms of any diseases. Since 1963 she has
also routinely made examination for phenyl-ketonuria. In addition, under an act of April1946, each child less than 7 years old may beexamined nine times free of charge by a physician,three of which are during the first year of lifeat the ages of 5 weeks, 5 months, and 10 months.
Netherlands
Dr. J. H. de Ham
For three reasons the Netherlands standsin a special position with respect to infant loss:(1) the rates are low compared with othercountries, (2) hospitalization at birth is extremelylow, and (3) infant care has a relatively longtradition. The medical demography of the Nether-lands is characterized by a relatively high birthrate, low mortality rates, and a disappearance ofcommon infectious diseases of childhood andtuberculosis.
In contrast to the experience of the UnitedStates, England and Wales, and Scotland, fetal andinfant mortality rates in the Netherlands havecontinued to fall since 1950. Infant mortalityhas decreased from a rate of 51 infant deaths per1,000 live births in 1930 to 29 in 1948, to 20 in1956, to 15 in 1964.
Before World War H fetal mortality was onthe average 50 percent higher than first-weekmortality, and since 1950 about 30 percent. Theposition of early neonatal mortality (deaths ofinfants under 7 days in age) has changed relativeto postnatal mortality (deaths of infants 1-51weeks in age). In the early 1920’s, postnatalmortality was three times as high as first-weekmortality, and at present, first-week mortality istwice as high as postnatal mortality.
In the first week of life, birth injuries,immaturity, and congenital malformations havebeen the dominant causes of death, From 1953-54 to 1961-62 they decreased by 20-25 percent.Other diseases of early infancy have been fourth inimportance, and have more than halved duringthese 8 years. During the same period totalfirst-week mortality decreased by 25 percent.
In the postnatal period congenital malforma-tions are the main cause of death and the ratesare scarcely decreasing.defined and other causes”
The subgroup “ill-occupies the second
7

place, and pneumonia and other respiratory dis-eases the third place. The rates for both ofthese groups are rapidly decreasing.
As medical certificates do not exist in theNetherlands, the exact distributions of birthweights and period of gestation are not available.However, independent surveys have been con-ducted in order to determine the extent ~fprematurity. In 1954 it was estimated that 5?2percent of the live ‘births were premature. As inall other countries, prematurity is of paramountsignificance in perinatal mortality. During thefilst week of life, the risk of dying is about20 times higher for premature infants than forinfants born at term.
Infant mortality rates in the Netherlands stillshow the classical picture, as in Scotland andEngland and Wales, of a wide range by socialclass. In 1961-62 first-week and postnatal mor -tal:.ty of class I (free professions and higherofficials) were 15 percent lower, and those ofclass V (nonfarm laborers—skilled and unskilled)were 10 percent higher than the average of thewhole country.
After World War II, the Netherlands becameone of the Western European so-called welfarestates—social security for the great masses,little unemployment, moderate wages with in-creasing standard of living, no real poverty com-pared with prewar conditions, no serious alco-holism, and at last but not least, an averagenutrition of reasonable quality and quantity. TheHealth Insurance Act of 1941 made health insur-ance compulsory under a certain level of income,giving the laborers and their families the legalright to medical care—family doctor, hospital,medicines, and so forth.
Obstetric care in the Netherlands has hadthree characteristics which are interrelated:(1) domiciliary confinement by general practi-tioners and midwives is far more usual thaninstitutional confinement; (2) midwives give pre-natal and natal care as independent practitioners;and (3) a special organization provides maternitycare and help in the household for the family,By tradition, the place of delivery has been athome. In the Netherlands only 20 percent of the
live births in 1950 were delivered in a hospital;and in 1963, 30 percent of the live births occurredin hospitals. The proportion of fetal deathsdelivered in hospitals amounts to about 60 percent.Perinatal mortality in home deliveries is verylow—in a decade decreasing from 22 to 12 per1,000—compared with that in hospital deliveries—decreasing in the same period from 65 to 53 per1,000—because pathological cases are concen-trated in hospitals. At present, obstetric aidis entrusted to midwives in 35 percent, togeneral practitioners in 45 percent, and toobstetricians in 20 percent of all births.
To offset low hospitalization, an organizationhas been founded to provide care to the motherand the newborn infant during childbirth and totemporarily manage the household duties, In 1950,this organization covered one-fourth and in 1963half of all home deliveries, Perinatal mortalityin the group with maternity-home help is halfthe national rate.
For the past 60 years, infant welfare centershave been set up throughout the Netherlands to giveperiodic examinations to infants. In 1930, therewas one infant welfare center per 450 live births,while in 1960 there was one per 100. At present,the average number of examinations in the firstvear of life is 10 to 11.
In conclusion, Dr. de Haas stated that:
the Netherlands belongs to the privileged
group of small industrialized countries withlow rates of infant loss. This favorablesituation was not reached because of evalua-tion and planning (at least not before 1950) butbecause of a long tradition of basic infantcare in the family supplied by district nursesand welfare centers and supported by ele-mentary social security and a rising standardof living.
The expectation is warranted that in 1970,fetal deaths will be reduced to 10-11 per1,000, first-week mortality to 8-9 per 1,000,postnatal mortality to 3-4 per 1,000, perinatalmortality to 18-20 per 1,000, and infantmortality to 11-13 per 1,000.
8

INFANT MORTALITY PROBLEMS
THE UNITED STATES
My. San2 Sha@YO
IN
Mr. Shapiro opened with a brief backgroundof the 1950 demographic and socioeconomicpicture in the United States, Hepointed out thatthe leveling off of the infant mortality rate inthe United States came earlier than it did in mostof the other countries with which comparisonswere being made. Furthermore, in more recentyears the leveling off has resulted in higherneonatal and postneonatal mortality rates in theUnited States than inmost of these other countries.
The United States has always had a com-paratively low fetal mortality rate; however, therate of decline appears to have slowed down morethan for other countries. The perinatal mortalityrate (fetal deaths of 28 weeks’ and over gestationand deaths of infants under 1 week old) maintaineda comparatively middle position in the postwarperiod. Currently it is one of the highest amongthe countries under discussion.
Mr. Shapiro next turned to discuss the issueof risk factors and what has been happening in theUnited States in relation to them. The male-femaledifferential in infant mortality has changed verylittle over the past 25 years. At the present time,there is an excess of 30 percent in the mortalityamong male births.
It is apparent that the rate of decline for boththe white and nonwhite populations decreased dur-ing the 1950 decade. Although the overall picturethat is found for white and nonwhite persons com-bined is reflected in the situation for the white,the decrease in the rate of decline was moreserious in the nonwhite population, During the1950’s and 19(j0’s the differentials increased sothat in 1962 the rate for nonwhite infants wasabout 85 percent higher than that for white infants.
During the 1950 decade, infant mortalitydecreased more rapidly in the nonmetropolitanareas than in the metropolitan areas, and todaythere is only about an 11 percent differentialbetween their rates. It is believed that about 50years ago urban areas had a higher infant mor-tality rate than did rural areas. Subsequently,
there was a crossing over with urban areas havinga lower rate. In the early fifties the urbanareas again had infant mortality rates slightlyhigher than those of the rural areas. Interestinglythough, this reversal or converging of the urban-rural infant mortality rates in recent years is dueentirely to what has been happening to the whitepopulation; the nonwhite infant mortality rate hasremained lower in urban areas than in rural areas.
The situation in large cities has drawn con-siderable attention. The infant mortality rate inmany of the large cities has remained unchangedin the white population, and has increased in thenonwhite population. Part of the speculation aboutthis phenomenon is that there has been a migrationamong white persons from these large cities intothe surrounding urbanized areas with an importantsocial class selectivity factor operating. There,the speculation is that as the higher social classis moving away from the central city into thesuburban area, a more adverse risk group of thewhite population has remained in the cities. In thenonwhite population the phenomenon has beendifferent. There has been a migration into thecities and hence a very substantial increase ofthe nonwhite population in many of the cities.
Prior pregnancy history is another risk factorinvolved in the outcome of the current pregnancy.If a mother has a prior fetal loss in her back-ground, there appears to be at least a doublingin the risk of a fetal death in the current preg-nancy. There is also an elevated risk of a pre-mature birth among women who previously havehad a prematurely born infant.
This introduces the factor of birth weightIn the United States in 1950, the first year forwhich there are national data, 7.5 percent of thelive births weighed 2,500 grams or less—7.2percent of white and 10.4 percent of nonwhitebirths. The proportion of births at low birthweights has increased to 8.2 percent (1963)due almost entirely to a sharp increase in therate among the nonwhite population.
There is a fairly clear indication fromdata for Upstate New York that the neonatalmortality rate, from the late 1940’s to theearly 1950’s, decreased among both babiesweighing 2,500 grams or less and those weighing
9

over 2,500 grams at birth; however, there hasbeen no decrease in the neonatal mortality rateamong the low-birth-weight infants since then.
It is generally. accepted that socioeconomicclass is a very important discriminating factorin infant mortality. However, there are no dataavailable for the United States as a whole on thisissue. Dr. Helen C. Chase has reported on theexperience in New York State (excluding NewYork City) for 1950-52. One point of interestrelates to the comparatively modest variations inperinatal mortality (defined as infant deaths under28 days of age and fetal deaths of 20 weeks’ ormore gestation) by social class based on thefather’s occupation. A one-third gradient in theloss rate was found between the professionalcategory and the laborer category (nonagricul-tural).
There are many difficulties in drawing in-ferences from cause-of-death information be-cause of the great variation that may exist amongcountries in the way cause of death is assigned.Nevertheless, from the standpoint of internationalcomparisons it would appear that the UnitedStates cannot single out any one or two particularcauses of death to which to attribute the dif-ferentials in either neonatal or postneonatalmortality. The United States seems to havean elevated infant mortality in the great majorityof the causes of death.
The final point made was that very recentevents indicate that the infant mortality rate inthe United States is still declining very slowly.However, no segment of the population is ex-periencing a large-scale reduction in the rate.
Discussion
The discussion that followed Mr. Shapiro’sreport centered on the problem of social classdifferentials. It was pointed out that data fromNew York State, exclusive of New York City,of mortality differentials by social class, asdefined by the father’s occupation, became moreapparent in the postneonatal and early child-hood periods. The chance of a low-birth-weightbaby being born dead or of dying within the firstmonth of life was shown to be the same for alloccupational groups, but the chance of the low-
birth-weight baby surviving later was quitemarked by social class. Professor Trolle re-marked that in Denmark, on the other hand,social class differences were seen both in theoccurrence of low-birth-weight babies and in theirneonatal mortality.
The fact that social class is indeed a dif-ficult factor to analyze was emphasized. Problemsof family disorganization, medical status beforepregnancy, and the nature of prenatal care allcontribute to make this a highly complex situation.Mr. Shapiro suggested that this view was supportedby data from a study of births in New York Cityin 1955. In this study, births were classifiedby whether the mother was hospitalized as ageneral service ward patient or as a privatepatient. The results showed that nonwhite patientsof private physicians had a perinatal loss whichwas very similar to the loss among white patientsadmitted to the general service ward. This wouldseem to indicate that a simple dichotomy betweenprivate care and general service ward care, or,for that matter, any single measure of socialclass will not entirely explain the situation.
DIFFERENTIAL FACTORS IN
INFANT MORTALITY
Statistic I Art if acts
Dr. Bernavd G. Greenberg
Dr. Greenberg led the discussion on statis-tical artifacts which might possibly affect inter-national comparisons of infant mortality. Heconcentrated on three possible artifacts: (1)definitions and requirements for reporting, (2)registration and notification practices, and (3)coding and tabulating practices. Dr. Greenbergalso summarized the significance of variousdemographic factors in relationship to inter-national comparisons of infant mortality.
For alI practical purposes, live births andfetal deaths are defined alike in the United Statesand in the Western European countries under dis-cussion. However, requirements for repxtingfetal deaths vary according to the period of ges-
10

tation for which registration and/or notificationis stipulated by law. The participating foreigncountries require that all fetal deaths after the28th week of gestation be reported. In the UnitedStates, each State determines its own laws forregistration of vital events. Most of the Statesuse the minimum gestation period equal to orgreater than 20 weeks; one State, Pennsylvania,requires that fetal deaths greater than 16 weeks’gestation be registered, and nine States and NewYork City require that fetal deaths of all periodsof gestation be registered.
The variation in registration requirementsmay be responsible in part for the variation in thefetal death ratios. The gestation period at whichreporting is required will affect not only thetotal number of fetal deaths, but also the distribu-tion of fetal deaths by gestation periods above theminimum level required. Dr. Greenberg showedthat in certain States of the United States regis-tration at 20-27 weeks’ gestation was increasedwhen the minimum period was lowered.
For example, within the past 13 years, 10States changed their registration requirementsso that the minimum gestation period for whichfetal deaths must be registered was lowered. Inone case, South Dakota, this requirement waschanged back to its former level in 1959. Table1 shows the year the change was effected andindicates the change. Analysis of differences in thedistributions of fetal deaths of 20 weeks’ gestationor more showed that after the registration changethe proportion of reported fetal deaths of 20-27weeks’ gestation increased in each State. Theoverall weighted average ratio for the 20-27week interval increased from 21.2 to 29.3 (anarithmetic change of 8.1 as shown in table 2).
In order to determine whether this trendoccurred in other States where no change wasmade in the minimal period for which a fetaldeath must be reported, Dr. Greenberg looked atthe trend for Upstate New York. Here the require-ments for. registration remained at 20 weeks ormore. Data for the years 1950-56 were compared
Table 1. Change in period of gestation for which fetal death registration is required: 10 States
Area
Arkansas -------
Colorado -------
Ge~rgia--------
Hawaii---------
Mai.ne----------
Missi.ssippi----
Oregon---------
Pennsylvania---
South Dakota---
Virginia---- ---
Year ofchange
1960
1954
1954
1960
1955
1952
19521
1954
195319591
19601
of the United States, 1950-63
Change in minimum gestation period required for registration
From
Although defined for all periodsof gestation, reporting limitedto 20 weeks’ gestation or more
20 weeks’ gestation or more
20 weeks’ gestation or more
No specified gestation
20 weeks’ gestation or more
20 weeks’ gestation or more
20 weeks’ gestation or more
20 weeks’ gestation or more
20 weeks’ gestation or moreAll products of conception
20 weeks’ gestation or more
To
All periods of gestation
All products of conception
All products of conception
All periods of gestation
All products of conception
All products of conception
All products of conception
16 weeks’ gestation or more
All products of conception20 weeks’ gestation or more
All products of conception
lChanged requirement July 1; all other States changed requirement January 1.
11

Table 2. Change in ratio of fetal deatha by week of gestation to all fetal deatha 20 weeka and over,and the relative change in reporting, when minimum periodlowered: 10 Statea of the United States, 1950-63
of gestation required for registration waa
Arithmetic change in ratio by week of gestationRelative changein reporting offetal deatha~213Weeksl
Yearsprior tochange
Yearsafterchange &36
weeks
Area20-27weeka
28-35weeks
36weeks
-1.1
+8.2
+9.0
+1.5
-0.5
-0.4
-0.8
-2.2
-1.7
-2.5
37-39weeka
-0.1
+9.5
+4.6
+2.6
+0.1
+0.6
+3.1
+1.3
+0.6
+0.4
40weeks
-3.2
-30.2
-18.3
-9.4
-3.4
-7.7
-7.2
-4.1
-3.7
-7.5
241weeka
-0.6
+3.5
+1.4
-0.1
+0.1
-0.1
+1.6
+0.8
-1.1
-0.2
Arkanaaa--------
Colorado--------
Georgia---------
Hawaii----------
Maine-----------
Mississippi------
0regon2---------
Penmaylvania----
South Dakota2’~--
Virginia2-------
1956-59
1950-53
1950-53
1952-59
1950-54
1950-51
1950-51
1950-53
1950-521960-63
1950-59
1960-63
1954-63
1954-63
1960-63
1955-63
1952-63
1953-63
1954-63
1953-58
1961-63
...
+4.9
+13 .3
+10 .5
+3.0
+3.6
+8.3
+11.2
+5.8
i-7.3
+10.2
+8.1
+0.1
-4.3
-7.1
+2.6
-0.7
-0.7
-7.8
-1.5
-1.5
-0.8
-2.5
-5.0
-9.0
-3.4
-5.5
-2.9
-7.6
-3.3
-4.3
-5.8
-9.4
-5.6
1.1649
1.0344
1.0469
1.0381
0.8758
1.0311
1.1657
1.0370
1.0371
1.0472
Weighted average +0.7 +2.1 -9.1 +0.8 1.0435. . .
lRelative change= Observed fetal cleat”s after changeExpected fetal cleats after changeY where expected fetal deatha after change =
(adjustment factor for decline in fetal death ratio)x(observed fetal death ratio before change)x(livebirths after change).
Qchanged requirement July 1; all other Statea changed requirement January 1.
aData for the perioda 1950-52 and 1959-63 were combined because registration requirements were theaame. The minimal registration requirement was lowered only for the period 1953-58 (table 1).
with those of 1957-63, andthefollowingarithmetic
changes in the proportion of fetal deaths byges-tation period were found:
These changes seem trivial compared withthose for States that lowered their registrationrequirements. It would seem then, thatthechangein the distribution of fetal deaths of 20 weeks ormore that occurred after registration require-ments lowered the minimum gestation periodisreal and not merely a function of time.
However, a second question arises. Did theincrease in the-interval 20-27 weeks result fromcases that were formerly unreported or was itashifting of fetal deaths within the total groupfrom one gestation interval to another? Tocheckthis, Dr. Greenberg looked at Upstate New Yorkagain and computed how much the fetal deathratio had changed during this 14-year period. Hefound that it decreased about 10 percentin the7
ChangePeriod of gestation in
ratio
20-27 weeks ---------------------28-35 weeks ---------------------36 weeks and over ---------------36 weeks ------------------------37-39 weeks ---------------------40 weeks ------------------------41 weeks and over ---------------
+1.6-0.5-1.1-0.5+1.5-2.0-0.2
12

years from the midpoint of 1950-56 to the mid-point of 1957-63. This was the same rate ofdecline observed in the total fetal death ratiofor the United States. In order to adjust the de-cline in the fetal death ratios of the other Statesso that a true assessment of the change couldbe made, Dr. Greenberg assumed that the periodafter the registration change should have a fetaldeath ratio lower than that prior to the changeat a rate of about 10 percent for every 7 years.This gave him an expected fetal death ratiowhich, when multiplied by the live births afterthe change, resulted in the expected number offetal deaths.
Next, he computed a relative increase basedupon the observed fetal deaths during the periodafter the change over the expected fetal deaths.Increases in the ratio of observed to expectedfetal deaths would indicate a real change in thetotal number of fetal deaths reported at 20 weeksor more. Table 2 shows the relative changes.Nine of the States increased, some as little as 3percent, and two as much as 16 percent.
Dr. Greenberg concluded that if the Europeannations were to lower the minimum reportingperiod to less than 28 weeks, the total number offetal deaths would probably increase by as muchas 4.35 percent. Since the United States registersfetal deaths of 20 weeks or more, any comparisonof fetal deaths 28 weeks and over with theEuropean countries would be biased against theUnited States. When the fetal deaths of 28 weeksand more are examined in order to compare theUnited States with some of the European nations,the fact that the United States has a lower re-porting period influences the fetal death ratios.
A second source of variation in the fetaldeath ratio arises from differences in determiningthe period of gestation. Four registration areas inthe United States base gestation upon the specifieddate of last menses, while other areas base iton the weeks of gestation as reported. WhenNew York City changed its method of recordinggestation in 1957 and requested that the data ofthe first day of the last menstrual period (LMP)be reported, so that the length of gestation couldbe more accurately and consistently calculated,the fetal death ratio at 20 weeks’ or more ges-tation increased 24 percent. At the same time,
however, the proportion of “not stated” gestationperiods increased. Discussion brought out thequestion of whether other factors added to thissharp increase, such as the concentrated cam-paign for better registration which was beingconducted by New York City. However, it wasresolved that this study was concerned withthe immediate effect of the change in reporting theage of the fetus at a time when the influenceof the campaign for complete registration waswaning. The point to be further studied is thatif data for the United States—New York City tobe specific —can be increased by as much asone-fourth because of a change in the methodof reporting period of gestation, then how isgestation period determined in foreign countriesand how does the measurement compare withthat of the United States?
Dr. Greenberg next discussed tabulationprocedures. In the United States, England andWales, Scotland, and Norway, first-day mor-tality includes deaths within 24 hours after birth.However, in Denmark and the Netherlands, first-day mortality includes only deaths occurring onthe calendar day of birth. In order to appraise theeffect of this tabulation difference, Dr. Greenbergcalculated a separation factor from the distribu-tions of (1) births by hour of birth for a 24-hourperiod, and (2) deaths by hour of death amongthose infants dying within the first 24 hoursafter birth. This separation factor was simplythe percent of babies which die within 24 hoursafter birth ,and which do not die on the snmecalendar day of birth. Based on 108,000 live birthsin Indiana in 1957 and on the assumption, verifiedby North Carolina data, that the distribution offirst-day deaths approximately follows a simpleexponential curve, he estimated the separationfactor to be approximately 22 percent. Otherwisestated, deaths within 24 hours after birth exceeddeaths occurring on the same calendar day ofbirth by about 28 percent.
However, from Norwegian data of 1949-51and 1959-61 deaths were tabulated for the peri-ods of 24 hours after birth and for the samecalendar day of birth. The two groups of dataindicated that 28.5 percent of the deaths withinthe first 24 hours of life did not occur on thesame calehdar day of birth. AS a compromise,
13

Dr. Greenberg felt thatof death under 24 hours
the mortality ratesshould be reduced by
25 percent before comparison with data in theNetherlands and Denmark for first-day mor-tality. Conversely, deaths under 1 calendar dayfor the Netherlands and Denmark should be in-creased by 33 1/3 percent so that the data forfirst-day mortality would be more comparableto the United States, England and Wales, Norway,and Scotland.
If ~irst-day mortality is increased in certaincountries, then deaths tabulated as 1-6 days ofage must be decreased correspondingly.
The general conclusion at this point wasthat these statistical artifacts were not suf-ficiently large to account for all the differences infirst-day and first-week mortality between theUnited States and the European nations under in-vestigation here.
Next, Dr. Greenberg summarized the in-cidence and significance of demographic fac-tors such as age of mother, birth order, andbirth weight which were discussed by Dr. vanden Berg in a paper distributed at the conference.He concluded, in concurrence with Dr. van denBerg, that although the distributions of live birthsby the mother’s age and by birth order are notfavorable in the United States compared withthose in the Western European countries, they donot account for the total differences in the neo-natal mortality rates.
Emphasis was placed on the significantlyhigher incidence of low-birth-weight babies in theUnited States. While the United States had 8.2percent live births of 2,500 grams or less in1963, England and Wales had 6.6 percent. The
Netherlands estimated about 5.5 percent in aspecial survey in 1954; and Norway currentlyestimates about 5-6 percent. Even though neonatalmortality of these low-birth-weight babies maybe essentially the same for the various countries,the fact that the United States appears to have agreater proportion of these births has a signifi-cant effect on its neonatal mortality rate. A lookat registration practices and other factors suchas sex ratio, plurality of birth, illegitimacy, ageof mother, and birth order indicated that theydo not seem to account for the observed inter-national differences in the incidence of low-birth-weight infants.
Dr. Greenberg continued the discussion oflow birth weight by considering whether the highincidence of small babies in the United States wasgenetic or cultural. He looked at the data for twoStates with high proportions of people of Scand-inavian background. Within the two States, Min-nesota and North Dakota, he compared the pro-portion of low-birth-weight babies in the countieswith the highest percentage of Scandinavians tothat of counties with the lowest percentage asdetermined by 1960 Census data. In Minnesota,the Scandinavian background was defined to in-clude Norwegian, Swedish, and Danish stock. InNorth Dakota it included Norwegian and Swedishbackgrounds only. In order to obtain meaningfuldata, Dr. Greenberg combined data for the years1955-59. The data showed that the counties withthe highest percentage of Scandinavian stock hada lower proportion of births of 2,500 grams orless than did the counties with the lowest pro-portion of Scandinavian stock (table 3).
Table 3. Percent of live births of 2,500 grams or less: Minnesota and North Dakota,1955-59
I
Place Nor thMinnesota Dakota
Entire State ------------------------------------------------------- 5.7
Counties with highest proportion of Scandinavian stock ----------- 5.1
Counties with lowest proportion of Scandinavian stock ------------ 5.6
6.3
6.0
6.4
Entire State minus counties with highest proportion ofScandinavian stock ---------------------------------------------- 5.8 6.3
14

Although these data are notpresent an interesting pointgation.
Discussion
Discussion concentrated
conclusive, they dofor further investi-
on the problems ofdefinition and underregistration. Although thedefinition of live birth officially appears to bethe same for the United States and the othercountries involved in the comparison, registra-tion practices do seem to differ. For example,Denmark, and until recently, England and Walesused only the criterion of breathing to determinea live birth, while other countries used the cri-terion of any signs of life, such as, breathing,pulsation of umbilical cord, heart beat, move-ment of voluntary muscles, and so forth.
Based on discussion of underregistration inthe United States and in the Western Europeancountries, it was concluded that some under-registration and undernotification do indeed exist,but the extent to which they exist has never beenexactly determined. Dr.. de Haas’ estimated under-registration in the Netherlands to be about 10percent, but the other European countries feltthat their registration was fairly complete. Thediscussion ended here with the general impressionthat more study was needed.
Socioeconomic Factors
Dv. Barbara J. van den Berg andDr. Arthur J. Lesser
L)r. van den Berg summarized the data avail-able on social class differentials, referring tostudies in the United States which showed ahigher percentage of low-birth-weight babiesamong the less favorable socioeconomic classes,and hence a higher neonatal mortality rate inthese lower social classes. She stated that in theUnited States a greater part of the population ismore “severely handicapped by unfavorable con-ditions than are the people in the Scandinavian
countries and some of the Westerncountries.” The indications cited were:
European
unemployment, education, illiteracy, andhousing conditions . . . . Unfavorable economicconditions of families in the United Statesare intensified by the fact that medical careis not as freely available to them as it is insome of the European countries and no ma-ternity allowances are given to cover theextra financial burden of a delivery and nomaternity benefits are given to working preg-nant women.
Dr. Lesser emphasized the need for bettermedical care facilities for the low-income fami-lies. Recognizing the fact that there is a positiveassociation between family income and infantmortality, Dr. Lesser described the worseningsituation within cities over 500,000 populationin the. United States. As there has been an influxof lower income and higher infant mortality riskgroups to the large cities, there has been acorresponding increase in the number of peoplewho are dependent upon tax supported medicalservices. Compounding the problem is the factthat this same group seeks prenatal care late inpregnancy or not at all, and at the same time thisis the group with an excessive rate of low-birth-
weight babies.Together with these worsening social factors
is the increasing cost of hospital care, with adecrease in “the ability of voluntary hospitals toprovide free prenatal and hospital delivery care.The result has been an increase in the numberof deliveries in’ tax-supported hospitals withoutan increase in hospital capacity. These hospitalshave become overcrowded and the length of stayat the time of delivery in a hospital has beenshortened. Discussion brought out that a newmaternity and infant care program with an appro-priation this year of $15 million from Federalfunds has been started to respond to these needs.Also, there have been an increasing number ofmaternal-child-healtn clinics. In order to remedythe decreasing number of personnel available forobstetric care, several programs for trainingnurses in midwifery have been initiated.
In conclusion, it was mentioned that al-though it is recognized that many infant deaths
15

occur in the low socioeconomic groups, theextent to which these deaths affect the total in-fant mortality rate is not known. Further studyis needed here.
Medical Factors
Dr. William A. Silverman
Dr. Silverman opened the discussion onmedical factors associated with the differentialinfant mortality by raising a series of pertinentand provocative questions. First, he questionedthe adequacy of birth weight as a measure of sur-vival. As a single criterion it tends to obscurethe fact that fetal growth is influenced by manyfactors. such as fetal malnutrition or fetal in-fections. Hence, low-birth- weight babies havedifferent chances of survival. It would be im -portant to obtain good standards of fetal growthso that aberrations could be confidently identifiedat birth.
In response to this comment, Dr. Yerushalmydiscussed his study in which a 5-point classifi-cation system of both birth weight and gestationage as an index of fetal maturity was devised
(~able 4). The study showed that in both neonataland postneonatal periods mortality increasedfrom group 5 to group 1; however, the gradientwas more pronounced in the neonatal deaths. Inthe low-birth-weight group (3!i-5k pounds), infantswith the shorter gestation period experienced ahigher mortality risk, while those with the longergestation period had a greater risk of being con-genitally malformed.
Lengthy discussion followed pointing out thevarious problems with the criteria of birth weightand gestation age, partially in response to Dr.Silverman’s question of whether there truly weredifferences in the rate of fetal growth M differentethnic groups. Points made were that the medianbirth weight does vary for different groups andthis consequently would affect the point at whicha baby is considered low in,birth weight. Optimumbirth size (the birth size at which both the babyand the mother have the greatest chance of sur-vival) varies. For example, in the United Statesthe optimum size for a white birth is between3,500-4,000 grams, whereas it is 500 grams lessfor a nonwhite infant.
The general conclusion reached at this con-ference, however, was that, in spite of theseproblems, birth weight is certainly the moreimportant criterion. However, as we are notdealing with a uniform population when consideringintact survival, additional measurements must beconsidered. It was at this point that Dr. Silver-man urged that the first day of last menstrualperiod be used actively as a more accurate andconsistent measure of gestation age.
Dr. Silverman’s next series of questionsrevolved around the problem of mechanisms whichare responsible for major perinatal disorders ofuncertain etiology. Is the incidence of hyalinemembrane disease indeed lower in the Scandina-vian countries than in the United States? Is therean indicator, such as socioeconomic differences,which could be used to predict the prematurerupture of membranes in various populations?How much is the distribution of causes affected
Table 4. Index of fetal maturity
DescriptionGroup
Birth weight Period of gestation
3 lbs. 8 oz. or less; 3 lbs., 9 OZ. -5 lb.8 C)z,
3 lbs. 9 OZ. -5 lb.8 OZ.
: 5 lbs. 9 oz. or more5 5 lbs, 9 oz. or more
All gestation periodsUnder 37 weeks37 weeks or moreUnder 37 weeks37 weeks or more
16

by the relativity of the diagnoses within thevarious colmtries?
These questions led to a discussion of thegrowing problem of the etiology of mechanicalsuffocation, or the so-called crib death. Severaltheories of the true nature of these deaths werediscussed; however, no agreement was reachedabout the etiology,
Dr. Silverman next turned to look at the issue
of national differences in medical practices. Towhat extent are these practicesrelated to preg-
nant y outcome and what changes in practiceshave occurred during the period under study?For example, during one recent period in theUnited States there was a change in the practiceof the administration of oxygen to low-birth-weight infants, and as a result the incidence ofretrolental fibroplasia decreased when oxygenwas given sparingly. What has been happening inthe foreign countries ? How is pregnancy out-come affected by the use of drugs and othermedical methods used to induce labor? How isthe severely involved fetus identified? In ‘short,there have been marked changes in the policyof fetal care and delivery over the past decades.How have these changes affected infant mortality,and how do they compare internationally?
Dr. Silverman’s questions stimulated othersin response. In reaction to the comment that theUnited States is aggressively using active resus-
citation, it was surmised that possibly resuscita-tion of the newborn infant was used more ofienwhere” the use of anesthetics and analgesia wasmore common, On the other hand, the advisa-bility of such active intervention was questioned.
Another point raised was whether almrtionacted as a means of preventing some infantdeaths. The Netherlands and Denmark felt thatthe number of abortions in a year would not affecttheir total infant mortality rate. However, thereis no way to tell now. In order to answer thisquestion there would have to be a study of the riskfactors related to women having abortions.
These questions were raised not only as animpetus to spur on discussion, but also as ameans to point out the real difficulty in comparinginternational medical practices in connection withinfant mortality. They indicate that additional workis needed tointernationalmeaningful.
understand basic practices beforecomparisons can be reliable and
Dr. William J. Schull of the University ofMichigan Medical School took time during thisdiscussion to cite some of his work showing the
effects of heredity on mortality. He stated, in
agreement with Dr. Moriyama. that there is in-deed an irreducible, nojzzeJ’o minimum in infantmortality. One reason is that there will always
be in every culture what may he termed theiatrogenic death. “Every culture, regardless
of how primitive it has been or how sophisticatedit may become, will have to pay a price for theadministrations of its medicine men. ” Secondly,a substantial body of biological evidence showsthat a significant portion of infant deaths is ofgenetic origin.
Ultimately, the chances of survival in a pop-ulation are limited by its genetic load— “theprice that any population, human or otherwise.pays for maintaining genetic variability ’’—andthis load may differ from nation to nation. Dr.SchuH showed how the “concealed load ,“ thegenetic burden of a population apparent upon
inbreeding, can affect the shape of a population.
The principal source of information on the “con-cealed load” stems from studies among the child-ren of parents biologically related to one another.
Such studies in Japan in 1956 and 1958-60
showed that increased inbreeding had as a result(1) smaller babies, (2) increased infant mortality,but (3) less childlessness.
Dr. Schull also reported that in Hiroshima
and Nagasaki socioeconomic status was loweras a function of inbreeding. He reported that
school performance of children diminished with
inbreeding; that is to say, the child of biologicallyrelated parents was a poorer performer in allaspects of school work. Here, Dr. Schull pointedout that possibly the parents of these children
were of a lower socioeconomic status becausethey were inherently poorer illustrations of thegenetic potential of Japan. This may tie in withthe socioeconomic differentials in infant mor-tality reported by Great Britain.
Finally, Dr. Schull observed that animaIstudies suggest that child survival is apt to be a
function not only of the child’s own genetic con-stitution, but also of the genetic constitution ofhis mother. This was seen in studies with cattleand swine where mortality increased with in-breeding in the offspring and inbreeding in themother, regardless of the father’s background.

SUGGESTIONS FOR FURTHER STUDY
No clear-cut explanations of the significantinternational differences in infant mortalityemerged from the discussions of the conference.It was generally agreed that the international mor-tality differentials could not be attributed to aparticular statistical artifact or difference indemographic distributions. However, it could notbe said with any certainty that the cumulativeeffects of all these factors would not account forthe difference in mortality.
Although mention was made throughout thecourse of the conference of the need for furtherstudy into the various aspects of the infant mor -tality problem, provision was made in the programfor a specific discussion of needed research onproblems of infant mortality. Suggestions forfurther study fall under the following generalheadings: (1) basic problems of definitions; (2) reg-istration practices; (3) determinants of perinataland infant mortality; and (4) medical factors re-lated to perinatal and infant mortality.
Definitions and Registration Practices
Definitions of live bivtk and fetal death. —AHof the countries involved in the discussion haveadopted the definitions of live birth and fetaldeath recommended by the World Health Organiza-tion. An integral part of these definitions is thecriteria of life, namely, breathing or otherevidence of life such as beating of the heart, pul-sation of umbilical cord, or definite movementof voluntary muscles. If a child breathes or showsany other evidence of life after complete expulsionor extraction from its mother, even though it beonly momentary, it is required that the event beregistered as a live birth and also as an infantdeath. This registration requirement is a changefrom that of the past in Sweden, for example, whenbreathing was the only criterion for determiningwhether an event should be registered as a fetaldeath or live birth,
Although no information is available, it ispossible that some small immature infants bornalive are registered as fetal deaths rather than asa live birth and infant death. These events wouldnot have any significant effect on the live birthtotals, but could have a marked influence on the
fetal death rate or the infant mortality rate, Foraccurate international comparisons, it is im-portant to determine how precisely the criteria oflife are being applied by the attendant at birth inthe registration of live birth and fetal death.
Two approaches were suggested in the studyof this problem. One method was to follow backon a sample of birth records with a questionnaireor an interview and obtain from the attendant atbirth information on the criteria which were usedin determining whether a specific event was a livebirth or a fetal death. The other proposal was toreview hospital records in order to determine thecriteria that were applied. The proportion ofdeliveries occurring in institutions would be oneof the controlling factors in the choice of methods.
Registration completeness. —There is verylittle quantitative information available on regis-tration completeness. The last test of birth regis-tration completeness in the United States wasmade in 1950, and showed that 2.1 percent of thelive births were not registered.
There have been no national tests of com-pleteness of death registration for the UnitedStates or for other countries. However, there havebeen several local studies in the United Statesfrom which estimates of underregistration havebeen made. Using data from records of theEmergency Maternity and Infant Care Program inNew York City (1943-45), Baumgartner et al. foundthat 14 percent of the fetal deaths occurring in thethird trimester of pregnancy were not registered.’]Schlesinger et al. estimated that in OnondagaCounty, New York (1951 -52) about 7 percent ofthe fetal deaths of 28 weeks’ or more gestationwere underregistered; however, these particulardata were records from hospitals in an urbanizedcounty where physicians and hospitals should bemore aware of reporting requirements,4 The totalUnited States would probably show a higher pro-portion of underregistered fetal deaths, sincethese studies used limited samples. Nevertheless,these are rather high estimates of underregistra-tion and indicate that national study is needed.
3Baumgartner, L., Wallace, H. M., Landsberg, E., and Pcs-sin, V.: The inadequacy of routine reporting of fetal deaths,Am.J.Pub.HeaZth. 39:1549-1552, Dec. 1949.
4Schlesinger, E. R., Beecroft, R. K., Silverman, H. F., andAll away, N. C.: Fetal and early neonatal deaths in Onondagacounty, New York. Pub. Health Rep. 74:1117-1122; Dec. 1959.
18

As more attention is shifted from infant mor-t:dity to perinatal mortality, the problem of fetalthmth unclerregistration becomes increasinglyimportont, Incomplete reporting of fetal deathsmokcw occurat eassessrnentof pregnancy wastagedifficult, and hampers investigation of the riskthctcws influencing perinatal mortality.
l’recise regional orinternational comparisonof fetal and perinatal death rates isalso impaired.For instance, the United States shows a late fetaldeath rate lower than any of the Western Europeancountries. In 1~62, the fetal death rates for theScandinavian countries and the Netherlands wereapproximately 15 percent higher than the rate forthe United States. The rate for Great Britain wasabout SOpercent higher. Part of these differencescan he attributed to incomplete registration; how-ever, the extent to which this is so needs to bedetermined.
(he recommended method of study into theproblem of underregistration was to follow acohort of recently married couples to the termina-tion of the first pregnancy, in order to determineij :md how the event was registered. Anotherpossibility is to establish some kind of pregnancyroster from information from maternity clinics,and to follow the individuals on the roster throughto the termination of the first pregnancy. It wassuggested that if international comparisons wereto bv made, an international sample should beselected, and standard forms and protocols beuseL1.
Determinants of Infant Mortality
Birth M@@t. —The incidence of low-birth-wcight infants remains largely unknown in coun-tries outside the United States. However, fromspecial surveys conducted in England and Wales,the Netherlands, and Norway the estimates seemto indicate that the United States has a higherincidence of low-birth-weight babies. Further-more, in the LTnited States the proportion hasbeen slowly increasing since 1950.
Tow-birth-weight infants have a much greaterchance Or dying, and hence contribute significantlym neonatal mortality. Yet, there has been nonut ionwide e~amination of this problem sincelL]S~, In view of the retardation in the rate of
decline in the infant mortality rate, there is a realneed to obtain national data on the relationshipbetween birth weight and infant mortality. It wassuggested that one type of study be made bymatching infant death certificates to their respec -tive birth records. From the birth certificate canbe obtained baseline information such as birthweight. A study of this type was launched in 1960in the United States; however, the results of thisstudy are not yet available.
For purposes of international comparisons,additional efforts would have to be made sincebirth weight does not routinely appear on thecertificates of the foreign countries representedat this conference, except Denmark, which onlyrecently added birth weight to its statisticalrecords. Other sources were suggested fromwhich data could be drawn for comparison withvital event records. In areas where prenatal carerecords exist in sufficient accuracy and com-pleteness, they could be matched to birth, fetaldeath, and infant death certificates. Hospitalrecords could be used in countries where a largeproportion of deliveries occur in hospitals; and ininstances where midwives attend most of thedeliveries, their records would be a source ofbasic information.
Socioeconomic status. —The investigators inGreat Britain have studied the relationship be-tween socioeconomic ,class and infant mortality.Socioeconomic class, as determined by the ,occu-pation of the infant’s father, has evidently had asignificant effect on the newborn infant’s pros-pects of survival. They have found that lowerinfant mortality rates occur in the higher classesand that there is a large gap between the highestand lowest class. Moreover, the gap has beenwidening.
It has been noted in the United States and inEngland and Wales that the proportion of low-birth-weight infants is higher in the lower socio-economic classes. The question arises whetherthis higher proportion is responsible for thehigher infant mortality rate in the lower socio-economic classes. Or, is socioeconomic statusa factor more important for determining thelevel of infant mortality? What are the problemsassociated with low- birth-weight (and premature)neonates born to women in the lower socialclasses?
19

In considering the socioeconomic situation,the problem of adequate measures by which todefine a socioeconomic class was raised. Sincethe mother’s background has an important effecton her reproductive capacity, is the occupationof the infant’s father a sufficient measure ofsocial class? Which aspects of social class have.an important relationship to pregnancy outcome?
Except for local studies in New York Stateand California, little recent information has beencollected on the relationship of infant mortalityand social class. More information is needed onthis subject ip the United States.
Ethnic background. —During the conferencethere was discussion of the relationship of ethnicbackground to pregnancy outcome. It was shownin a preliminary investigation that in Minnesotaand North Dakota ethnic background may havean effect on the incidence of low-birth-weightinfants. It has also been indicated that Orientalinfants have lower mortality rates than do whiteinfants in the United States. However, furtherstudy is needed to determine more exactly therelationship between infant mortality and ethnicorigin. For instance, how do the infant mortalityrates of different ethnic groups compare by socio-economic class ? What effect does ethnic back-ground have on the size of the infant at birth?What influences do immigrant groups have on thetotal infant mortality rate?
Medical Factors Related to Infant Mortality
Medical care. —There are important differ-ences in the provision of prenatal and natal carein the various countries; however, no evidencewas presented to suggest that the level of ob-stetrical and pediatric care pey se accounts fora large part of the international differences ininfant mortality. The effects of prenatal, natal,and neonatal care are important to the study ofinfant mortality, yet little is known almut them.It was suggested that the relationship of prenataland obstetric care, including the use of anesthesia,drugs, and hormones, to pregnancy outcome beexamined. For instance, how are complicatedpregnancies treated, and how does the treatmentrelate to the outcome?
Several factors connected with the medicalcare of the mother and infant before and afterbirth were mentioned as important for study. For
example, women in the lower socioeconomicstrata are less apt to secure early prenatal care,and at the same time are more likely to experiencepoor pregnancy outcome. A study of mothers, in-tegrating information on socioeconomic classlevel during their early life as well as at thetime of delivery, and details of prenatal carewould be important to the study of factors corre-lated with infant mortality.
The incidence of congenital malformationsrelated to prenatal factors such as drugs takenduring pregnancy and maternal infections couldbe inspected in countries with high proportionsof hospital deliveries. Such a study would involvethe integration of prenatal, hospital, and pediatricrecords.
The question was raised during discussionabout benefits to be derived from large-scalrresuscitation of the newborn infant. What is therelationship of active resuscitation of the neonateto his well-being? This type of investigation couldbest be conducted in the hospital setting.
In the United States the average hospital stayat the time of delivery is about 4 days; whereasin Scotland it is about 9 days, 10 days in Englandand Wales, and 11-12 days in the Netherlands.However, the effect of hospital stay on the neo-nate is unknown. Study of the relationship ofpostnatal hospital stay to neonatal mortalitycould be conducted by combining birth, hospital,and death information.
Diseases peculiar to early infancy.- Theneonatal death rate has been leveling off duringthe past decade in the United States, yet thischange has not been occurring to the same ex-tent in the European countries. Mortality ratesfor the major causes of neonatal death have beendeclining; however, the death rate for diseasespeculiar to early infancy has been increasing inthe United States and England and Wales, whiledecreasing in the Western European countries.Part of this increase appears to be IYom the in-creased reporting of hyaline membrane diseaseand respiratory distress syndrome. It was sug-gested that a detailed investigation of thesediseases be made in order to determine themeaning of this upward trend.
Incidence of infections. —The postneonatalmortality rates for many countries have been cutapproximately in half since 1950. However, thepostneonatal mortality rate for the United States
20

has declined very slowly and is now at a rela-tively high level compared with the rates forother countries of low mortality.
In 1959-61 over 43 percent of the posmeo-natal deaths in the United States were attributedto infectious diseases. Further reductions inmortality from this cause are still possible;however, study of the epidemiological and medicalaspects of infections is urged in order to deter-mine the underlying factors of these diseases.
Major diso~.devs ofwzcertainet iology.-Con-tern over the increasing frequency of major dis-orders of uncertain etiology prompted proposalfor thorough study of the incidence of sudden andunexpected deaths, and mechanical suffocationin bed or cradle with or without reference to thecertifying physician. What mechanisms are re-sponsible for these disorders?
In 1963 there were 2,998 accidental deathsamong the infants between 28 days and 1 year ofage in the United States. Of these, over 25 per-cent were ascribed to suffocation in bed orcradle. These deaths have been under question asthere is evidence that most of these deaths arenot due to accidental mechanical sul%cation, butare a result of some fulminating infection orallergic reaction. A study needs to be made whichwould include pathological evaluation of the va-lidity of the clinical diagnosis.
In recent years, attention has been calledto the sudden and unexpected deaths. Some ofthese deaths appear to be due to respiratory in-fections. Epidemiological investigations couldbe made of these deaths with special attentionto infections among them.
Incidence of nonfatal handicapping con-ditions. —Improved fetal and infant survival mayresult in an increase in infants with handicappingneurosensory conditions. It was proposed thatexamination of this ~ssibility be made. A studyof this relationship would require cooperativeinvestigations by a number of hospitals withfollowup pediatric and psychological examina-tions.
SUMMARYIn an effort to explain the infant mortality
situation in the United States, a significant num-ber of problem areas in the study of infant andperinatal mortality were brought into focus at
this 2-day conference. Among the areas con-sidered were the problems in the interpretationof international data arising from variations indefinitions and in registration and statisticalpractices. Risk factors, such as the incidenceof low-birth-weight babies, the socioeconomicbackground of the mother, the age of the mother,the birth order of the infant, and the genetic back-ground of the mother and child were discussed.Questions were raised about such medical careaspects as the effect on the infant’s chance ofsurvival of adequate and inadequate prenatal care,of hospital stay at the time of birth, and of theadministration of drugs to the mother before andduring parturition. Further questions were raisedabout the increasing incidence of perinatal deathsattributed to diseases of early infancy and todisorders of uncertain etiology.
There seemed to be no simple, conciseexplanation for the leveling off or for the unfavor-able position of the infant mortali~ rate in theUnited States. No single statistical, demographic,or medical factor appeared to account for theinternational differences observed in the perinataland infant mortality rates. However, it was notpossible to assess the relative portion con-tributed by each factor. In some areas, especiallythose associated with medical aspects, data werenot available for the evaluation of their impacton infant and perinatal mortality.
As the perinatal and infant mortality ratesdecrease, the relative effectg of artifacts such asunderregistration of fetal and infant deaths anddifferences in definitions and statistical practicesincrease. More information on these factors isneeded for the various countries for future com-parative studies. Also, data are needed on fac-tors associated with infant mortality such associoeconomic conditions, mortality rates among”low-birth-weight infants, and the effect of pre-natal care and obstetrical practices on perinataland infant mortality. According y, suggestionsfor future research have been made.
Unless some major change in the infantmortality rates takes place in the United States,the situation with respect to other countries willonly worsen. It is hoped that serious study willbe given to the problems of perinatal and infantmortality, and action taken to achieve greatersavings of infant lives.
00021
* U. S. @OVERNMZNT PRINTING OFFICE - 1S70 - 435.U57 P. 0. 1

Series 1.
Series 2.
Series 3.
Series 4.
SeVies 10.
SeYies 11.
SeYies 12.
SeVies 20.
Sevies 21.
Series 22.
OUTLINE OF REPORT SERIES FOR VITAL AND HEALTH STATISTICS
Public Health Service Publication No. 1000
Progvams and collection procedures. —Reports which describe the general programs of the NationalCenter for Health Statistics and its offices and divisions, data collection methods used, definitions, andother material necessary for understanding the data.
Reports number 1-4
Rata evaluation and methods Yesearch .—Studies of new statistical methodology including: experimentaltests of new survey methods, studies of vital statistics collection methods, new analytical techniques,objective evaluations of reliability of collected data, contributions to statistical theory.
Reports number 1-18
Analytical studies. — Reports presenting analytical or interpretive studies based on vital and health sta-tistics, carrying the analysis further than the expository types of reports in the other series.
Reports number 1-4
Documents and committee re~orts.—Final reports of major committees concerned with vital and healthstatistics, and documents such as recommended model vital registration laws and revised birth nddeath certificates.
4
Reports number 1-3
Data From the Health Interview Survey .—Statistics on illness, accidental injuries, disability, use ofhospital, medical, dental, and other services, and other health-related topics, based on data collected ina continuing national household interview survey.
Reports number 1-29
Data From the Health Examirration Survey .—Statistics based on the direct examination, testing, andmeasurement of national samples of the population, including the medically defined prevalence of spe-cific diseases, and distributions of the population with respect to various physical and physiologicalmeasurements.
Reports number 1-16
Data Fvom the Health Records .%vuey. —Statistics from records of hospital discharges and statisticsrelating to the health characteristics of persons in institutions, and on hospital, medical, nursing, andpersonal care received, based on national samples of establishments providing these services andsamples of the residents or patients.
Reports number 1-4
Data on mortality. —Various statistics on mortality other than as included in annual or monthly reports-special analyses by cause of death, age, and other demographic variables, also geographic and timeseries analyses.
Number 1 wtd 2
Data on natality, mavriage, and divorce. —Various statistics on natality, marriage, and divorce otherthan as included in annual or monthly reports— special analyses by demographic variables, also geo-graphic and time series analyses, studies of fertility.
Reports number 1-9
Data From the National Natality and Mortality .% ’veys. —Statistics on characteristics of births anddeaths not available from the vital records, based on sample surveys stemming from these records,including such topics as mortality by socioeconomic class, medical experience in the last year of life,characteristics of pregnancy, etc.
Reports number 1 and 2
For a list of titles of reports published in these series, write to: National Center for Health StatisticsU.S. Public Health ServiceWashington, D.C. 20201











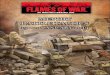
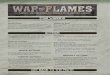

![Louis F Fow Consulting Presentation 2009 [Autosaved]](https://img.pdfslide.us/doc/110x75/55be04aabb61eba7108b45c9/louis-f-fow-consulting-presentation-2009-autosaved.jpg)