Embed Size (px)
Citation preview
INATIONAL CENTER Series 11For HEALTH STATISTICS Number 6
VITAL and HEALTH STATISTICS
DATA FROM THE NATIONAL HEALTH SURVEY
HeartDisease
in Adults
United States. 1960-1962
A description of the examination and diagnostic pro-
cedures with maior findings by age, sexz and race..
DHEW Publication No. (HRA) 76-1254
U.S. DEPARTMENT OFHEALTH, EDUCATION, AND WELFARE
Public Health ServiceHealth Resources Administration
National Center for Health StatisticsRockville, Maryland 20852
Vital and Health Statistics Series 11, No. 6
For sele by the Superintendent of Documents, Government Printing OfficeWashington, D.C., 20402
NATIONAL CENTER FOR HEALTH STATISTICS
DOROTHY P. RICE, Director
ROBE RT A. ISRAEL, Acting Deputy DirectorJACOB J. FELDMAN, Ph.D., Associate Director for Andy.sk
GAIL F. FISHER, Associate Director for the Cooperative Healfh Statistics SystemELIJAH L. WHITE, Associate Director for Data Systems
ROBERT C. HUBER, Acting Associate .Directorfor ManagementPETER L. HURLEY, Acting Associate Director for Operations
JAMES M. ROBEY, Ph.D., Ass;ciate Director for Program DevelopmentALICE HAYWOOD, Information Officer

CONTENTSPage
The Cardiovascular Evaluation --------- --------- --------- -
The Medical History- - -------- -------- -------- -------- --
The Cardiac Examination --------- --------- --------- ----Blood Pressure Measurement ---------------------------Other Parts of the Examination -------------------------Comparison With Clinical Examination -------------------
Heart Disease Diagnosis ---------------------------------Interpretation of the X-ray and Electrocardiogram- --------Classification and Criteria -----------------------------Dia~osis ---------------------------------------------
Major Findings ------------------------------------------Sex---------------------------------------------------Race -------------------------------------------------Age --------------------------------------------------Multiple Diagnosis -------------------------------------Other Heart Disease -----------------------------------Heart Findings ----------------------------------------
Summary -----------------------------------------------
Detailed Tables ------------------------------------------
Appendix I. Medical History Questions Related to Cardio-vascular Disease ---------- ------------ ------------------
Appendix II. Forms Used in Recording FindingsonthePhysicalExamination -------------------------------------------
Appendix III. Electrocardiographic Readings ---------------Criteria and Classification ------------------------------ECG Code Sheet ---------------------------------------
122233
4456
77889
1112
12
14
17
21
282832
CONTENTS—Continued
Page
Appendix IV. Interpretation of Chest X-ray -----------------Form Used in Puhnonary Reading -----------------------Form Used in Cardiovascular Reading -------------------Pulmonary Readers ------------------------------------Cardiovascular Readers --------------------------------Final Evaluation ---------------------------------------
Appendix V. Diagnostic Review ---------------------------
Appendix W. Statistical Notes ----------------------------The Survey Design --------------------------- --------- -Reliability improbability Surveys ------------------------Sampling and Measurement Error -----------------------Small Numkrs ----------------------------------------Tests of Significance -----------------------------------Demographic Terms -----------------------------------
333334353536
39
41414141424243
SYMBOLS
Data not available ------------------------ ---
Category not applicable ------------------ . . .
Quantity zero --------- ------------------ -
Quantity morethan Obutless than O.OS----- 0.0
Figure doesnot meet standards ofreliabilityor precision ------------------ *
HEART DISEASE IN ADULTS
Tavia Gordon, Division of Health Examination Statistics
The National Health Survey uses threemethods for obtaining information about thehealth of the U.S. population. The first is ahousehold interview in which persons are askedto give information relating to their health orto the health of other household members. Thesecond is the collection of data from availablehealth records. The third is direct examination.The Health Examination Survey was organized touse the third procedure, drawing samples of thepopulation of the United States and, by medicalexamination and with various tests and measure-ments, undertaking to characterize the populationunder study.
The initial enterprise of the Health Examina-tion Survey was the examination of a nationwideprobability sample of 7,710 persons aged 18-Wyears. Its purpose was to obtain informationon the prevalence of cardiovascular disease,arthritis, diabetes and certain other chronicdiseases, on dental health, and on the distributionof a number of anthropometric and sensorycharacteristics. Altogether, 6,672 persons wereexamined during the course of the Survey whichwas begun in October 1959 and completed inDecember 1962. Sample persons received astandard examination, lasting about 2 hours,performed by medical and other staff members ofthe Survey in specially designed mobile clinics.
This is one of a series of reports describingand evaluating the plan, conduct, and findings ofthe first cycle of the Health Examination Survey.The description of the general plan 1 and of thesample population and response 2 has been pub-lished. These provide general background for allreports of findings. In this report the cardiovascu-lar examination is outlined and those parts of the
examination relating to the diagnosis of heartdisease are discussed. An account is given of themethd of evaluating the findings and of the pro-cedures used in arriving at diagnoses. The preva-lence of heart disease in adults is summarized,for total heart disease and for specific diagnoses.
THE CARDIOVASCULAR
EVALUATION
The cardiovascular evaluation included thefollowing:
1. A medical history2. A cardiovascular examination performed
by a fellow or first-year resident ininternal medicine witha.
b.
c.
d.
e.
f.
g.
Three measurements of blood pres-sureExamination of the cxxlar fundi withan ophthalmoscopeExamination of the neck for venousengorgementInspection and palpatio; of the pe-ripheral arteriesExamination of the extremities forevidence of edemaExamination of the heart by auscul-tation and palpation for thrills, heartsounds, or murmursOther observations which might con-tribute to differential diagnosis, suchas a set of serological tests for syphi-lis and evidences of thyroid enlarge-ment, congenital malformations, phy-sical impairments, and residuals ofcerebrovascular accidents.
1

3. A 12-lead electrwardiogram4. A chest X-ray— 14 by 17 inches in size,
taken at a 6-foot distance
The Medical History
The cardiovascular examination began with aself-administered medical history. After a briefinterview by a receptionist, the examinee wasasked to complete a medical history form. Thereceptionist remained available to provide theexaminee with any assistance necessary. Includedamong the questions were some concerning cardi-ovascular symptoms or disease. These are shownin Appendix I. The examinee was then offered adrink which included 50 grams of glucose, unlesshe was under treatment for diabetes, and aftercompleting the self-administered history wasasked a few additional questions by the recep-tionist. The6e included questions about physicalhandicaps, major health problems, and operationsand were designed to elicit relevant medical in-formation that had not appeared in response tothe more specific questions on the history. Thereceptionist, at the same time, reviewed the his-tory both for completeness and for consistencyand queried the examinee further where anydeficiencies were evident.
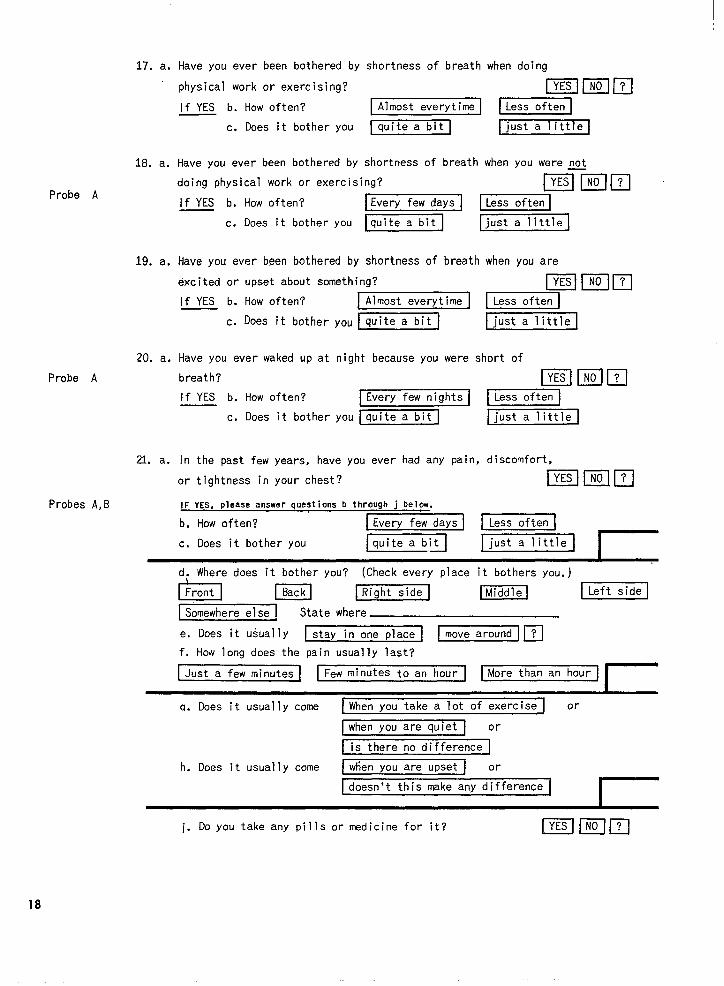
The examining physician reviewed the medi-cal history before beginning the physical exami-nation. He attempted to correct any incomplete-ness or inconsistency remaining in the record andwhere the examinee had been uncertain in hisanswer attempted to arrive at a definite “yes”or “no” by further questioning. In some caseshe could not. For most of the cardiovascularquestions the physician was instructed to ask forfurther information if an answer of “yes” or “?”had been checked, or if the examinee had indi-cated that he did not know the answer. A seriesof standard probes were used (Appendix I) andthe answers to these were recorded. When theseprobes were completed the physician was freeto further question the examinee until he wassatisfied that he had all the relevant informationthat could be obtained in a single session.
Among the cardiovascular questions two wereof especial importance for the diagnosis of heartdisease-questions 21 and 22 (Appendix I). Thesedealt with chest pain and heart pain. It was on
the basis of the response to these questions andthe associated probes that a diagnosis of anginapectoris was made. Responses to the othercardiovascular questions on the medical historyform were also of assistance in, although notsufficient in themselves for, heart disease diag-nosis.
The Cardiac Examination
After reviewing the medical history, thephysician began the physical examination. In-cluded in this was a standardized examinationof the heart, undertaken without exercise. Theprecordium was palpated for thrills with theexaminee first sitting upright, then leaning for-ward. This was first done with the examineebreathing normally and then repeated with theexaminee holding his breath in expiration. Aus-cultation was done with a stethoscope, using boththe bell and the diaphragm, and proceeded fromthe apex upward along the left sternal borderand then to the pulmonic and aortic areas. Itwas done with the examinee upright, first breath-ing normally and then hoMing his breath in ex-piration. Next, palpation and auscultation wererepeated with the examinee supine. Finally, herolled over on his left side and was examinedwith the bell and palpated for thrills.
Findings from this examination were re-corded on a standard form (Appendix II). If am~rmur was noted. it was described in specificterms, as to intensity, time, pitch, quality, andduration. 3 Intensity was graded on a five-pointscale, from very faint (grade 1) to very loud(grade 5).
Blood Pressure Measurement
Three blood pressure measurements weremade, the first just after the physician met theexaminee; the second midway in the examination,after completing the auscultation of the heartin the sitting position; and the third at the endof the examination. Blood pressures were takenwhile the examinee was sitting on the examiningtable. The nurse placed the middle of the cuff overthe bulge in the upper left arm. The cuff wasleft on the arm between the first and secondmeasurements, removed after the. second, and
returned for the third. The physician held thearm at the level of the atrium, with the nurseholding the Baumanometer at the physician’seye level. Using the bell of his stethoscope,the physician noted the pressure when the soundfirst was heard, when it first became muffled,and when it disappeared. All three measurementswere recorded. The point at which the Korotkovsounds disappeared was taken as the diastolicpressure. If the sounds did not disappear, thepoint of muffling, if distinctly heard, was used.Since the Baumanometer is scaled in intervalsof 2 mm., measurements were so recorded.Some results from this examination have alreadybeen reported.~ 5
Other Parts of the Examination
For the chest X-ray, a posterior-anteriorview was taken at a 6-foot distance and recordedon a 14 by 17 inch film. The exposure was taken ininspiration but was not timed for a fixed phaseof the heart cycle. The electrocardiogram wasobtained by a Twin Viso machine (model 60-1300):Twelve leads were recorded: I, H, HI, AVR, AVL,AVF, V1-V6.
The other aspects of the cardiovascularexamination, while not leading to the diagnosisof heart disease as such, were helpful either inevaluating the signs of heart disease or indetermining a specific etiology. Thus, the pres-ence of congenital abnormalities might contributeto the differential diagnosis of congenital heartdisease. The finding of a positive serologicaltest for syphilis was required in order to makea diagnosis of syphilitic heart disease.
Comparison With Clinical Examination
The uniform, single-visit examination usedfor the Health Examination Survey differed inboth objectives and procedures from the usualclinical examination. In clinical practice theobjectives are evaluation and medical manage-ment of the individual patient. Usually the patientis being studied because of some complaint forwhich he has sought medical advice. If the diag-nosis or treatment seems obvious on clinicalgrounds, the workup may be minimal. On the
other hand, if the diagnostic clues are equivocal,there may be an extended series of tests andconsultations and the patient may be under obser-vation for an appreciable period before diagnosis.Diagnosis may be modified by the patient’s re-sponse to treatment, by his subsequent clinicalhistory, or by new findings. There is, in short, avariable diagnostic workup and an extended oppor-tunity to confirm or reject the original impres-sions.
On the other hand, the purpose of the HealthExamination Survey is to characterize a popu-lation group. The cardiovascular examinationwas designed to provide reliable diagnostic in-formation insofar as such information could beobtained during a single visit. Since there was noresponsibility for patient care, persons withmedical complaints need not be diagnosed ashaving disease if the findings were equivocal ornonspecific. Since persons did not presentthemselves for medical care but because theywere members of a population sample, theabsence of complaints gave no assurance that therewas no disease. Therefore, a standardized exami-nation was given to every examinee.
Prior to beginning the first cycle of the HealthExamination Survey, a special study was under-taken under the direction of Dr. Jeremiah Stam-ler. G Its purposes were to design a single-visitcardiovascular examination which would yielddiagnoses in accord with current survey practice,to compare diagnoses obtained by this examinationwith diagnoses obtained for the same individualsby a replicate of this examination, and to comparediagnoses made by the single-visit examinationwith diagnoses arrived at in clinical practice.The single-visit examination developed for thisstudy was later adopted, with minor modifications,by the Health Examination Survey for use in itsexamination of adults.
While there is a distinct contrast between thestandardized single-visit examination and a clini-cal examination, the study did not find large dif-ferences between the two in diagnostic results.The chief discrepancies were with respect tocoronary heart disease. The diagnosis of anginapectoris was more common on the single-visitexamination than on the clinical, whereas minorelectrocardiographic abnormalities were more
3
likely to lead to a diagnosis of coronary heartdisease on the clinical examination than on thesingle-visit examination.
HEART DISEASE DIAGNOSIS
Several intermediate steps were involvedin progressing from examination findings toheart disease diagnoses. The first step wasinterpreting the chest X-ray film and the elec-trocardiographic tracing. The second was con-structing a set of diagnostic criteria. The thirdwas developing a procedure for translating thefindings from the examination and the interpre-tation of the X-ray and electrocardiogram intospecific diagnoses. How these steps were takenfor the Health Examination Survey is discussedin the following sections.
Interpretation of the X-ray
and Electrocardiogram
Both the electrocardiogram and the chestX-ray were interpreted independently by severalspecialists. These interpretations were madewithout any other information about the examinee.
The electrocardiogram was read independ-ently by three cardiologists according to criteriaagreed upon in advance. These criteria arespecified in Appendix III, which also contains areproduction of the preceded form on which thefindings were entered. For all major findingsallowance was made for designating any electro-cardiographic abnormality observed by the elec-trocardiographic reader even though the specifiedcriteria for that abnormality were not satisfied.After completion, the three independent determi-nations were compared. Where they all agreed,the unanimous decision was used for subsequentdiagnosis. In the event that there was any disa-greement, the three met with Dr. Michael A.Corrado, who served as coordinator for this work,and together they came to a final decision. Thisfinal decision was the one used in such cases.
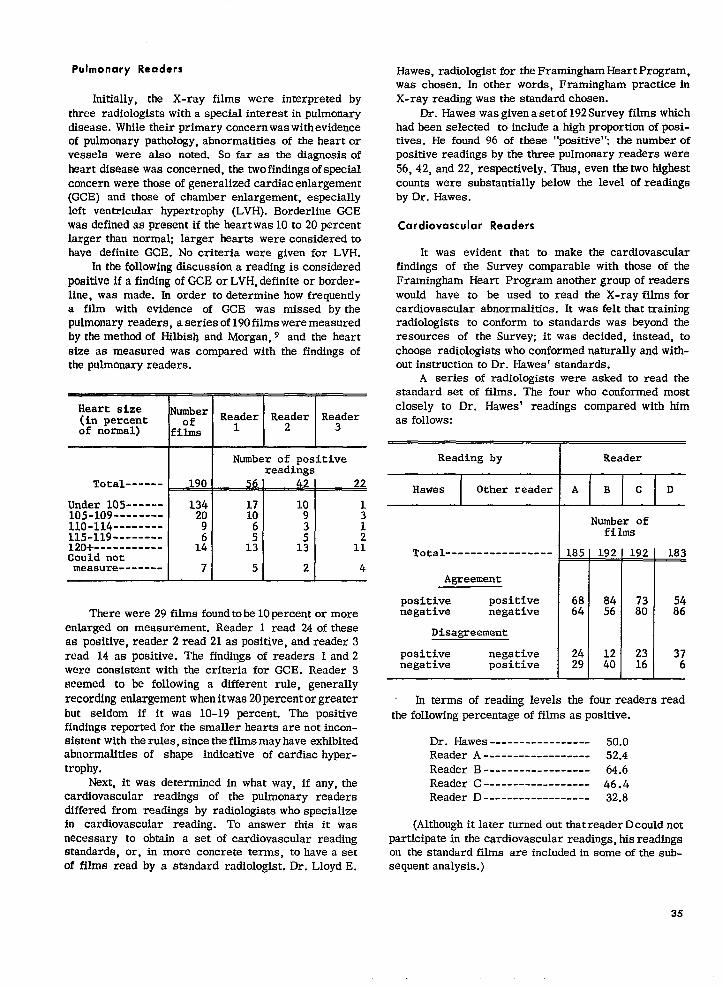
The evaluation of the chest X-ray was a some-what more complicated undertaking. Initially,arrangements were made to have the X-ray filmsinterpreted by radiologists specializing in pul-monary disease. In addition to noting evidence of
pulmonary disease, the “pulmonary readers”were requested to record evidence of distinctcardiovascular abnormality. As had been antici-pated, this led to an estimate of the prevalence ofcardiovascular abnormalities which was muchlower than is ordinarily found in cardiovascularsurveys. Another group of radiologists was there-fore employed to reexamine the films for evidenceof cardiovascular abnormality. These ‘‘cardi-ovascular readers” were chosen on the basis ofstandards set by Dr. Lloyd E. Hawes, radiologistfor the Framingham Heart Study. A set of filmsfrom the Health Examination Survey was readfirst by him and then by a number of differentradiologists. Three were found to employ aboutthe same standards as Dr. Hawes and were chosento read the Health Examination Survey films forcardiovascular abnormalities. Each was given arandom third of the films to read. The forms usedin recording the radiological findings for both the“pulmonary readers” and the “cardiovascularreaders” are reproduced in Appendix IV.
The reading procedure was designed as fol-lows. A finding of general cardiac enlargement orleft ventricular hypertrophy, definite or possible,was considered “positive.” All films were read bytwo pulmonary readers and one cardiovascularreader. The determination of the two pulmonaryreaders provided a preliminary evaluation. Ifboth considered the film “positive” a decision ofenlargement was made whatever the findings of thecardiovascular reader. If they disagreed and thecardiovascular reader considered the film posi-tive, the decision was that enlargement was pres-enq otherwise a second cardiovascular readerinterpreted the film and his decision was final.If the two pulmonary readers considered the film“negative” and the cardiovascular reader agreedwith them, the decision was that no enlargementwas presenq otherwise a second cardiovascularreader examined the film and his decision wasbinding. All decisions were made independentlyand no reconciliation of differences was under-taken.
The rationale for this procedure is too com-plicated to be discussed at this point. It is partlyexplained in Appendix IV. The effect was toproduce reading results which conformed well,both in level of abnormalities found and in
attributions tostandards of the
specific individuals, with theFramingham Heart Study.
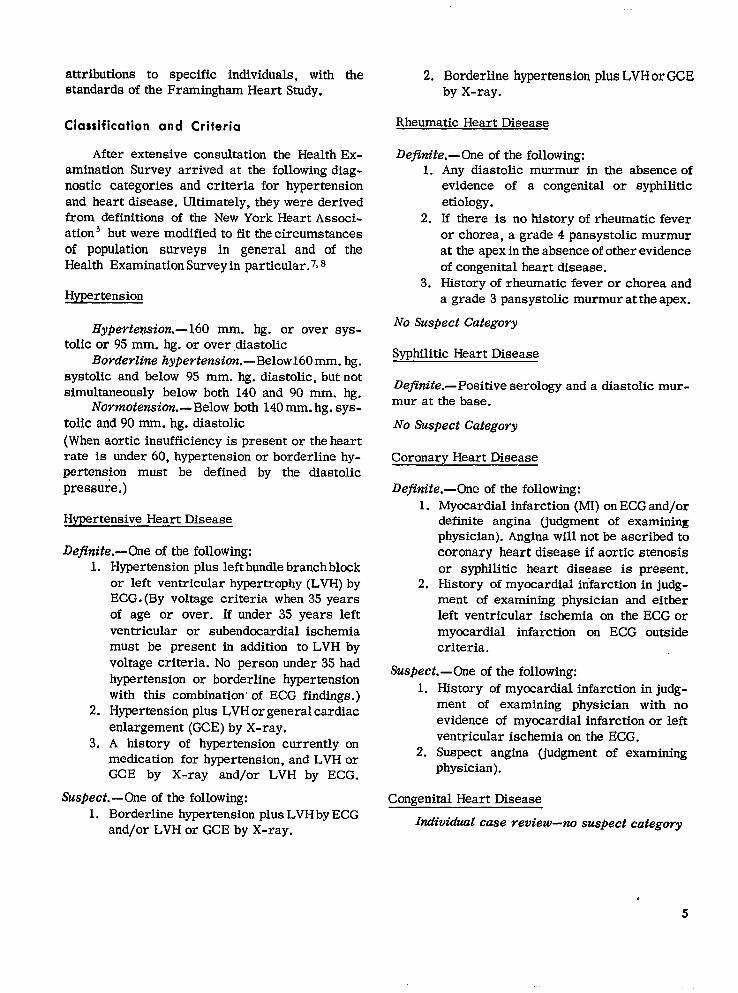
Classification and Criteria
After extensive consultation the Health Ex-amination Survey arrived at the following diag-nostic categories and criteria for hypertensionand heart disease. Ultimately, they were derivedfrom definitions of the New York Heart Associ-ation 5 but were modified to fit the circumstancesof population surveys in general and of theHealth Examination Survey in particular.7, 8
Hypertension
Hyperte@on.— 160 mm. hg. or over sys-toIic or 95 mm. hg. or over diastolic
Borderline hype? feneion.-Belowl6O mm. hg.systolic and below 95 mm. hg. diastolic, but notsimultaneously below both 140 and 90 mm. hg.
Normotension.— Below both 140 mm, hg. sys-tolic and 90 mm. hg. diastolic(When aortic insufficiency is present or the heartrate is under 60, hypertension or borderline hy-pertension must be defined by the diastolicpressure,)
Hypertensive Heart Disease
Defltdte.-One of the following:1. Hypertension plus left bundle branch block
or left ventricular hypertrophy (LVH) byECG. (By voltage criteria when 35 yearsof age or over. If under 35 years leftventricular or subendocardial ischemiamust be present in addition to LVH byvoltage criteria. No person under 35 hadhypertension or borderline hypertensionwith this combination” of ECG findings. )
2. Hypertension plus LVH or general cardiacenlargement (GCE) by X-ray.
3. A history of hypertension currently onmedication for hypertension, and LVH orGCE by X-ray and/or LVH by ECG.
Suspect. -One of the following:1. Borderline hypertension plus LVH by ECG
and/or LVH or GCE by X-ray.
2. Borderline hypertension plus LVHor GCEby X-ray.
Rheumatic Heart Disease
Dejinite.— One of the following:1. Any diastolic murmur in the absence of
evidence of a congenital or syphiliticetiology.
2. If there is no history of rheumatic feveror chores, a grade 4 pans ystolic murmurat the apex in the absence of other evidenceof congenital heart disease.
3. History of rheumatic fever or chores anda grade 3 pans ystolic murmur at the apex.
No Suspect Category
Syphilitic Heart Disease
Definite.- Positive serology and a diastoIic mur-mur at the base.
No Suspect Category
Coronary Heart Disease
Definite.-One of the following:1. Myocardial infarction (MI) on ECG and/or
definite angina (judgment of examiningphysician). Angina will not lx ascribed tocoronary heart disease if aortic stenosisor syphilitic heart disease is present.
2. History of myocardial infarction in judg-ment of examining physician and eitherleft ventricular ischemia on the ECG ormyocardial infarction on ECG outsidecriteria,
Suspect.—One of the following:1. History of myocardial infarction in judg-
ment of examining physician with noevidence of myocardial infarction or leftventricular ischemia on the ECG.
2. Suspect angina (judgment of examiningphysician).
Congenital Heart Disease
Individual case veview-no suspect categovy
.
5

Other Heart Disease
Defim”te.-One of the following:
1.
2.3.4.5.
Medical examinationAortic stenosis (a systolic ejection mur-mur accompanied by a thrill at the basewith diminished or absent A2 in theabsence of other etiology).
ECG findingsLeft bundle branch blockComplete heart blockAtrial fibrillationLVH including left ventricular ischemiaor subendocardial ischemia
Suspect.—One of the following:
1.
2.3.4.5.6.
X-ray findingsCardiomegaly (LVH or GCE)
ECG findingsRight bundle branch block (complete)Partial A-V blockAtrial ~utterRight ventricular hypertrophyIsolated left ventricular ischemia
There are some omissions from this list.Because sample persons had to visit the mobilecenter for examination two manifestations ofheart disease were automatically omitted. Thefirst were acute clinical episodes. The secondwere episodes which run a rapid fatal course—in particular, coronary heart disease first mani-festing itself as “sudden death. ” Moreover, pastmanifestations which left only equivocal evidencewere also undiagnosed.
In addition, the Survey chose to ignore twoimportant clinical manifestations of heart dis-ease. It was thought that the examination was notadequate for diagnosing cases of congestiveheart failure. To be sure, most such cases werediagnosed as some form of heart disease, anyhow,because of other findings in the examination,but a few cases did elude diagnosis. Cor pulmonalewas also omitted, again because it was decidedthat the examination was inadequate for differ-ential diagnosis. Again a few cases of heart dis-ease were not diagnosed because of this omission.
In diagnosing rheumatic, congenital, andsyphilitic heart disease no provision was madefor a category of suspect disease, chiefly becausesuch diagnoses depend on quite subtle differ-entiations of heart sounds and murmurs. It wasthought that without verification of the examiningphysician’s impressions it would be unwise toplace great weight on such evidence; thereforethe Survey considered it preferable to omitsuspect categories for these diseases.
Diagnosis
After all the findings were available, thefinal step was to arrive at a diagnosis. Even infavorable circumstances this is a difficult prw-ess to standardize. In the Health ExaminationSurvey, it was more difficult than usual. Therewere 62 different examining physicians. To relyon their consistent use of the same diagnosticstandards and criteria was clearly impossible.What is more, they did not have available thespecialist judgments on the electrocardiographictracing and the chest X-ray or the findings fromthe serological tests for syphilis. Thus, thoughthe examining physician was requested to enterhis diagnostic impressions, these were used onlyas indicators; the final diagnoses were made bythe permanent staff of the Survey, with consultanthelp in difficult cases.
The first step in this procedure was to supplya set of rules suitable for diagnosis by computer,which would convert the coded information fromthe medical record and from the interpretationof the X-ray film and the electrocardiogram intoa diagnostic decision. An example of the computeroutput is given in Appendix V. Some of thesedecisions were then subject to review. For thefirst few hundred cases all computer diagnoseswere reviewed by Dr. Alice M. Waterhouse,medical advisor to the National Center forHealth Statistics. These reviews made it evidentthat many diagnostic decisions did not require aspecial medical review and the classes of casessubject to review were finally narrowed to thefollowing:
1. Cases with significant murmurs.2. Cases with a diagnosis of angina pectoris.3. Cases where the diagnosis depended on a
4.
!5.
history of hypertension or a history ofmyocardial infarction.Cases with electrocardiographic findingsof myocardial infarction outside of cri-teria or of left ventricular ischemia,where a diagnosis of definite coronaryheart disease had not been made.Cases diagnosed as having heart diseaseby the examining physician but not bythe computer.
This omitted from review those cases with a clearand definite diagnosis of heart disease on theavailable evidence and those cases where therewas no possibility of diagnosing heart diseasefrom the available evidence.
In most cases where the computer diagnosiswas reviewed, the diagnostic decision made bythe computer was unaltered. In a few instances,however, there was a diagnostic change on thebasis of review. Where a review decision seemedto require specialist judgment the case was re-ferred to Dr. Abraham Kagan of the FraminghamHeart Program for a final decision. The discussionof the details of these decisions is not feasible,but in general equivocal evidence of heart dis-ease was treated as nondiagnostic, although it wasrecognized that some of these cases wouldwarrant medical supervision.
The review procedure did more than arriveat final diagnoses. It also submitted the diagnostic
criteria to repeated scrutiny. In the balance theyappear to be both reasonable and conservative.
MAJOR FINDINGS
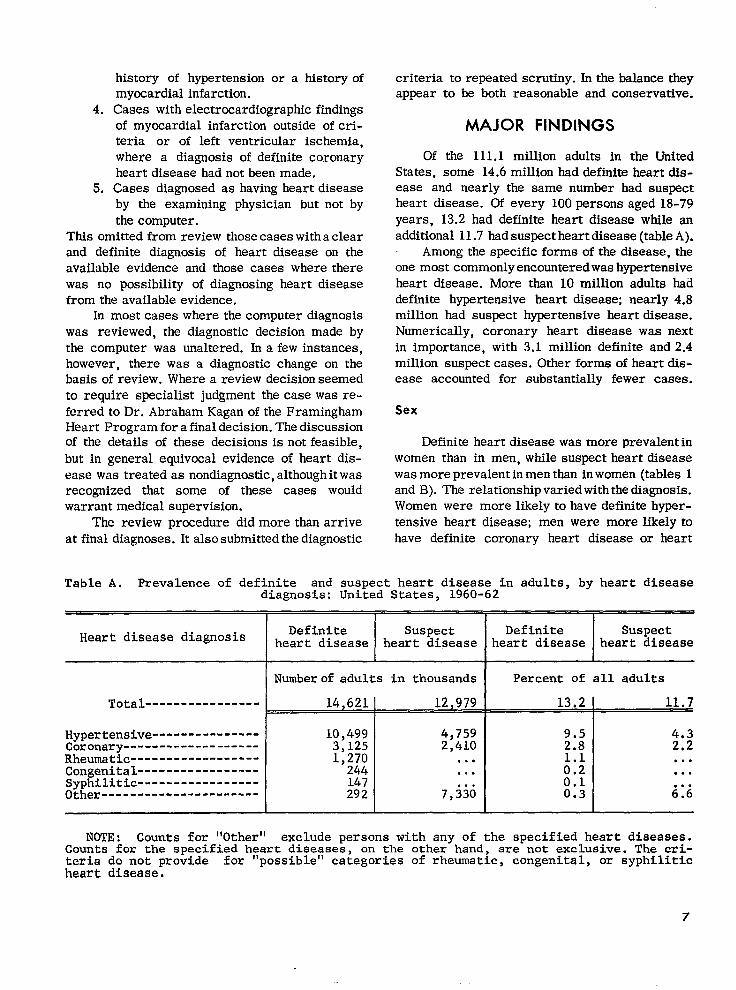
Of the 111.1 million adults in the UnitedStates, some 14.6 million had definite heart dis-ease and nearly the same number had suspectheart disease. Of every 100 persons aged 18-79years, 13.2 had definite heart disease while anadditional 11.7 had suspect heart disease (table A).
Among the specific forms of the disease, theone most commonly encountered was hypertensiveheart disease. More than 10 million adults haddefinite hypertensive heart disease; nearly 4.8million had suspect hypertensive heart disease.Numerically, coronary heart disease was nextin importance, with 3.1 million definite and 2.4million suspect cases. Other forms of heart dis-ease accounted for substantially fewer cases.
Sex
Definite heart disease was more prevalent inwomen than in men, while suspect heart diseasewas more prevalent in men than in women (tables 1and B). The relationship varied with the diagnosis.Women were more likely to have definite hyper-tensive heart disease; men were more likely tohave definite coronary heart disease or heart
Table A. Prevalence of definite and suspect heart disease in adults, by heart diseasediagnosis: United States, 1960-62
Heart disease diagnosis Definite Suspect Definite Suspectheart disease heart disease heart disease heart disease
I Number of adults in thousands I Percent of all adults
Total ---------------- 14,621 I 12,979 13.2 I 11.7I
Hypertensive ---------------Coronary -------------------Rheumatic ------------------Congenital -----------------SyphiM.tic -----------------Other ----------------------
10,4993,1251,270
244147292
4,7592,410
. . .
. . .
. . .7,330
9.52.8
k:;0.10.3
;.;●
✎ ✎ ✎
✎ ✎ ✎
✎ ✎ ✎
6.6
NOTE: Counts for “Other” exclude persons with any of the specified heart diseases.Counts for the specified heart diseases, on the other hand, are not exclusive. The cri-teria do not provide for “possible” categories of rheumatic, congenital, or syphiliticheart disease.
7
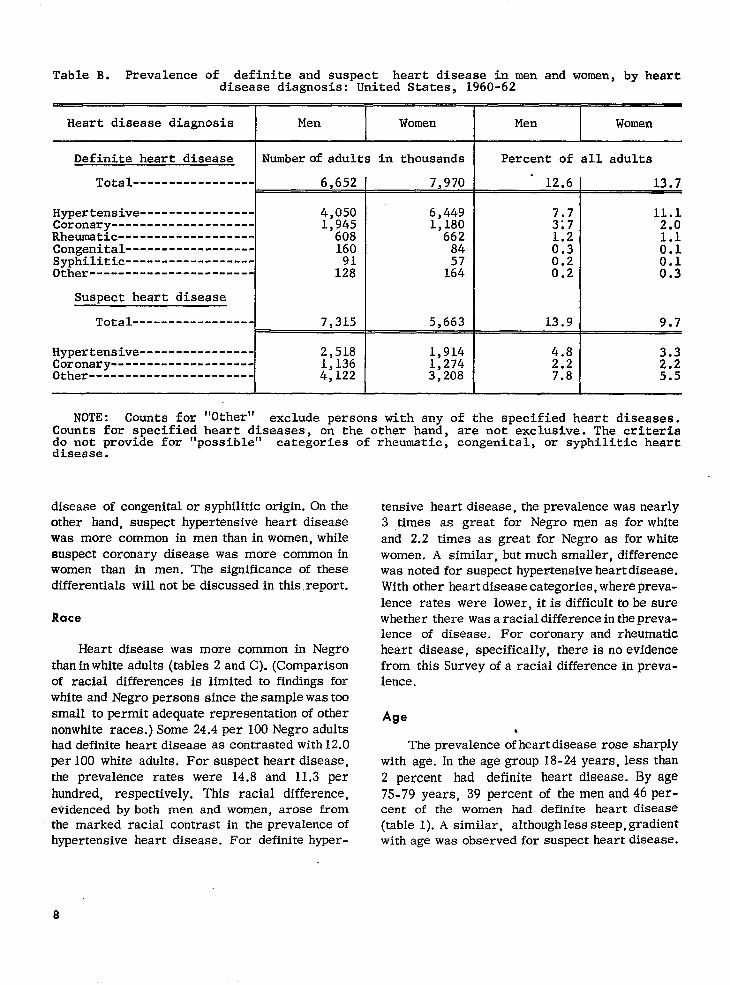
Table B. Prevalence of definite and suspect heart disease in men and women, by heartdisease diagnosis: United States, 1960-62
Heart disease diagnosis Men Women Men Women
Definite heart disease Numberof adults in thousandsI
Percent of all adults
Total-----------------.
6,652 I 7,970 12.6
IHypertensive---------------- 4,050Coronary-------------------- 1,945Rheumatic------------------- 608Congenital------------------ 160Syphilitic------------------Other----------------------- 1%
6,4491,180
66284
la
Suspect heart disease I I ITotal----------------- 7,315 5>663 13.9
Hypertensive---------------- 2,518Coronary-------------------- 1,136Other----------------------- 4,122
1,914 4.81,274 2.23,208 7.8
13.7
11.12.0
k:
u
9.7
3.32.25.5
NOTE: Counts for “Other” exclude persons with any of the specifiedheart diseases.Counts for specifiedheart diseases, on the other hand, are not exclusive.The criteriado not provide for “possible” categories of rheumatic, congenital, or syphiliticheartdisease.
diseaseofcongenitalor syphiliticorigin.On theotherhand,suspecthypertensiveheartdiseasewas more common inmen thaninwomen, whilesuspectcoronarydiseasewas more commoninwomen than in men. The significanceof thesedifferentialswillnotbe discussedinthis.report.
Race
Heartdiseasewas more common in Negrothaninwhiteadults(tables2 andC).(Comparisonof racialdifferencesis limitedto findingsforwhiteandNegropersonssincethesamplewastoosmalltopermitadequaterepresentationofothernonwhiteraces.)Some 24.4per 100Negroadultshaddefiniteheartdiseaseas contrastedwith12.Oper100 whiteadults.For suspectheartdisease,the prevalencerateswere 14.8and 11,3per
hundred,respectively.This racialdifference,evidencedby both men and women, arosefromthemarked racialcontrastin theprevalenceofhypertensiveheartdisease.For definitehyper-
tensiveheartdisease,theprevalencewas nearly3 ,timesas great for Negro men as forwhiteand 2.2 timesas greatforNegro as forwhitewomen, A similar,butmuch smaller,differencewas notedforsuspecthypertensiveheartdisease.Withotherheartdiseasecategories,wherepreva-Iencerateswere lower,itisdifficulttobe surewhethertherewasaracialdifferenceinthepreva-lenceof disease.For coronaryand rheumaticheartdisease,specifically,thereisno evidencefrom thisSurveyofa racialdifferenceinpreva-lence.
Age
The prevalenceo;heartdiseaserosesharplywithage.Intheagegroup18-24years,lessthan2 percent had definiteheartdisease.By age75-79years,39 percentof themenand46 per-cent of the women had definiteheartdisease(table1).A similar,althoughlesssteep,gradientwithagewas observedforsuspectheartdisease.
8
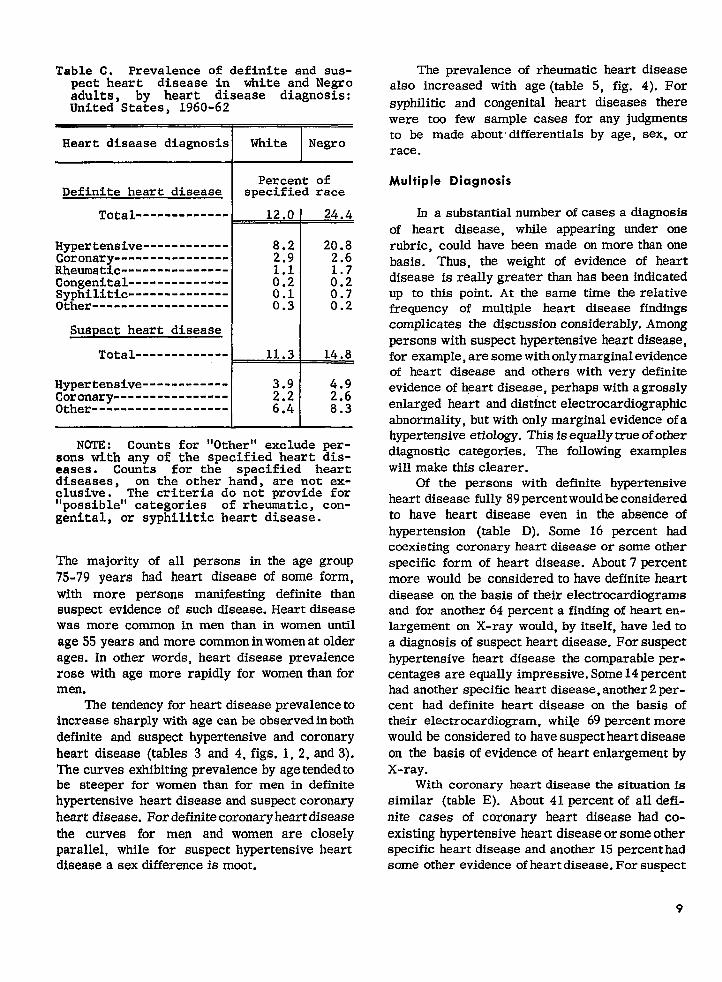
Table C. Prevalence of definite and sus-pect heart disease in white and Negroadults, by heart disease diagnosis:United States, 1960-62
Heart disease diagnosis White Negro
Percent ofDefinite heart disease specified race
Total------------- 12.0 24.4
Hypertensive ------------ 8.2 20.8Coronary ---------------- 2.9 2.6Rheumatic ---------------Congenital -------------- ::: MSyphilitic -------------- 0.1Other------------------- 0.3 ::;
Suspect heart disease
Total ------------- 11.3 14.8
Hypertensive ------------ 3.9 4.9Coronary ---------------- 2.6Other ------------------- ::: 8.3
NOTE: Counts for “Other” exclude per-sons with any of the specified heart dis-eases. Counts for the specified heartdiseases, on the other hand, are not ex-clusive. The criteria do not provide for“possible” categories of rheumatic, con-genital, or syphilitic heart disease.
The majority of all persons in the age group75-79 years had heart disease of some form,with more persons manifesting definite thansuspect evidence of such disease. Heart diseasewas more common in men than in women untilage55 years and more common inwomenatolderagea. In other words, heart disease prevalencerose with age more rapidly for women than formen.
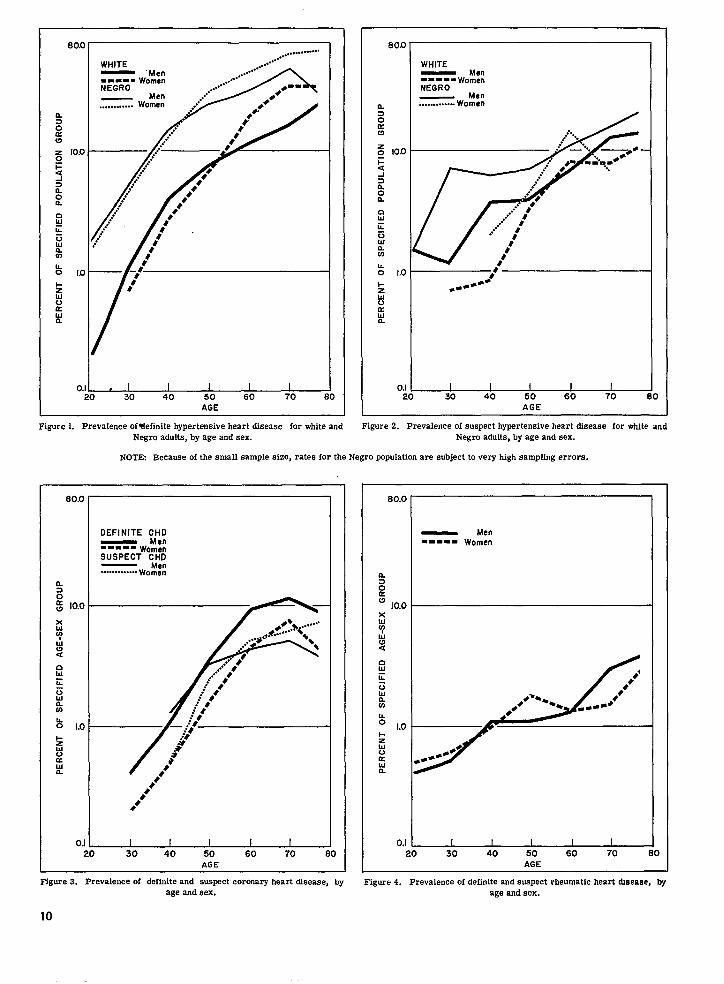
The tendency for heart disease prevalence toincrease sharply with age canbe observedinbothdefinite and suspect hypertensive and coronaryheart disease (tables 3 and 4, figs. 1,2, and3).The curves exhibiting prevalence byage tendedtobe steeper for women than for men in definitehypertensive heart disease and suspect coronaryheart disease. For definitecoronary heartdiseasethe curves for men and women are closelyparallel, while for suspect hypertensive heartdisease a sex difference is moot.
The prevalence of rheumatic heart disease
also increased with age (table5, fig. 4). For
syphilitic and congenital heart diseases therewere too few sample cases for any judgmentsto be made aboutdifferentials by age, sex, orrace.
Multiple Diagnosis
In asubstsntial number ofcases a diagnosisof heart disease, while appearing under onerubric, could have been made on more tbanonebasis. Thus, the weight of evidence of heartdisease is really greater than has been indicatedup to this point. At the same time the relativefrequency of multiple heart disease findingscomplicates the discussion considerably. Amongpersons with suspect hypertensive heart disease,forexample,are somewithonly marginalevidenceof heart disease and others with very definiteevidence of heart disease, perhaps with agrosslyenlarged heart and distinct electrccardiographicabnormality, but with only marginal evidence ofahypertensive etiology. Thisisequallytrueofotherdiagnostic categories. The following exampleswill make this clearer.
Of the persons with definite hypertensiveheart disease fully 89percentwould reconsideredto have heart disease even in the absence ofhypertension (table D). Some 16 percent hadcoexisting coronary heart disease or some otherspecific form of heart disease. About 7 percentmore would be considered to have definite heartdisease on the basis of their electrocardiogramsand for another64 percent a finding of hearten-largement on X-ray would, by itself, have ledtoadiagnosis of suspect heart disease. Forsuspecthypertensive heart disease the comparable psx-centages are equally impressive.Some 14percenthsd another specific heart disease, anotber2per-cent had definite heart disease on the basis oftheir electrocardiogram, whfle 69 percent morewouldbe considered to havesuspect heartdiseaseon the basis of evidence of heart enlargement byX-ray.
With coronary heartdiseasethesituationis
similar (tableE). About 41 percentof alldefi-nite cases of coronary heart disease had co-existing hypertensive heartdiseaseor someotherspecific heart disease and another 15 percenthadsome other evidence ofheartdisease. Forsuspect
9
. . .
WHITE— ‘Men---=9 w~m~”NEGRO
... .........aa
Ewg 10.0
FaA3noa
au~u!+!mLo Kl —1-fl0auL
o.,~30 40 50 60 70
AGE
EiiGw0.mL01-Zw0
:
WHITEMen
----.wom~”NEGRO
Men- Women
O;.-O
AGE
Figure 1. Prevalence of?lefinite hypertensive heart diseaee for white and Figure 2. Prevalence of suspect hypertensive heart disease for white andNegro adults, by age and sex. Negro adults, by age and eex.
NOTE Because of the small eample size, rates for the Negro ppukdfon are subject to very high sampffng errors.
10.0
1.0
OJd
DEFINITE CHD— Men-mm -- womenSUSPECT CHD
Men.. ....... .. .. Women
,?0
tiGF
80.0
0.1 I I I I I) 30 40 50 60 70
AGE----
Figure 3. Prevalence of definite and suspect coronary beart disease, by Figure 4. Prevalence of definite and saapect rheumatic heart disease, byage and sex.
10
age and sex.
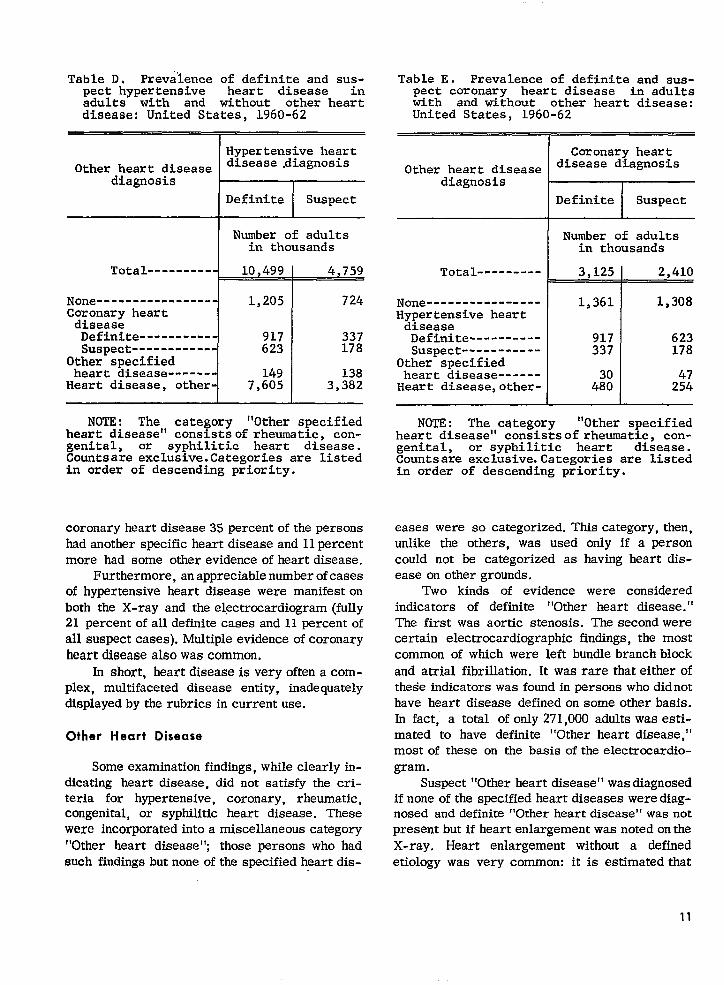
Table D. Prevalence of definite and sus-pect hypertensive heart disease inadults with and without other heartdisease: United States, 1960-62
Hypertensive heartOther heart disease disease diagnosis
diagnosis
-
Table E. Prevalence of definite and sus-pect coronary heart disease in adultswith and without other heart disease:United States, 1960-62
I
Other&%Number of adults
in thousandsNumber of adults
in thousands
Total ---------~
None ----------------i
1,205 724Coronarv heart
diseas;Defini.te ----------
i917 337
SuaDect ------------ 623 178Other-specified
heart disease ------{
149 138Heart disease, other- 7,605 3,382
NOTE: The category “Other specifiedheart disease” consistsof rheumatic, con-genital, or syphilitic heart disease.Countsare exclusive.Categories are listedi.n order of descending priority.
coronary heart disease 35 percent of the personshad another specific heart disease and llpercentmore had some other evidence of heart disease.
Furthermorejan appreciablenumber ofcasesof hypertensive heart disease were manifestoboth the X-ray and the electrocardiogram (fully21 percent of all definite cases and 11 percentofall suspect cases). Multiple evidence ofcoronaryheart disease also was common.
In short, heart disease is very often acorn-plex, multifaceted disease entity, inadequatelydisplayed bythe rubrics uncurrent use.
Other Heart Disease
Some examination findings, while clearly in-dicating heart disease, did not satisfy the cri-teria for hypertensive, coronary, rheumatic,congenital, or syphilitic heart disease. Thesewere incorporated into a miscellaneous category“Other heart disease”; those persons who hadsuch findings but none of the specified heart dis-
Total --------- 3,125 I 2,410I
None ---------------- 1,361 1,308Hypertensive heart
diseaseDefimite ---------- 917 623Suspect ----------- 337 178
Other specifiedheart disease ------
Heart disease,other- 4% 2:;
NOTE: The category “Other specifiedheart disease” consistsof rheumatic, con-genital, or syphilitic heart disease.Countsare exclusive. Categories are listedin order of descending priority.
eases were so categorized. This category, then,unlike the others, was used only if a personcould not be categorized as having heart dis-ease on other grounds.
Two kinds of evidence were consideredindicators of definite “Other heart disease.”The first was aortic stenosis. The second werecertain electrocardiographic findings, the mostcommon of which were left bundle branch blockand atrial fibrillation. It was rare that eitherofthese indicators was found in persons who didnothave heart disease defined on some other basis.In fact, a total of only 271,000 adults was esti-mated to have definite “Other heart disease,”most of these on the basis of the electrocardio-gram.
Suspect ’’Other heart disease’’ wasdiagnosedifnone of the specified heart diseases werediag-nosed and definite “Other heart disease” was notpresent but ifheart enlargement was notedontheX-ray. Heart enlargement without a definedetiology was very common: it is estimated that
11
6,910,000 adults had this finding using the Surveystandards. Electrocardiographic findings indi-cating suspect “Other heart disease” were muchless common. Most cases diagnosed on thesegrounds had either right bundle branch block orleft ventricular ischemia, with the cases beingevenly divided between these two categories. Aswith other findings included in “Other heart dis-ease ,“ left ventricular ischemia was much morecommonly found with other evidence of specificheart disease than it was as an isolated finding.
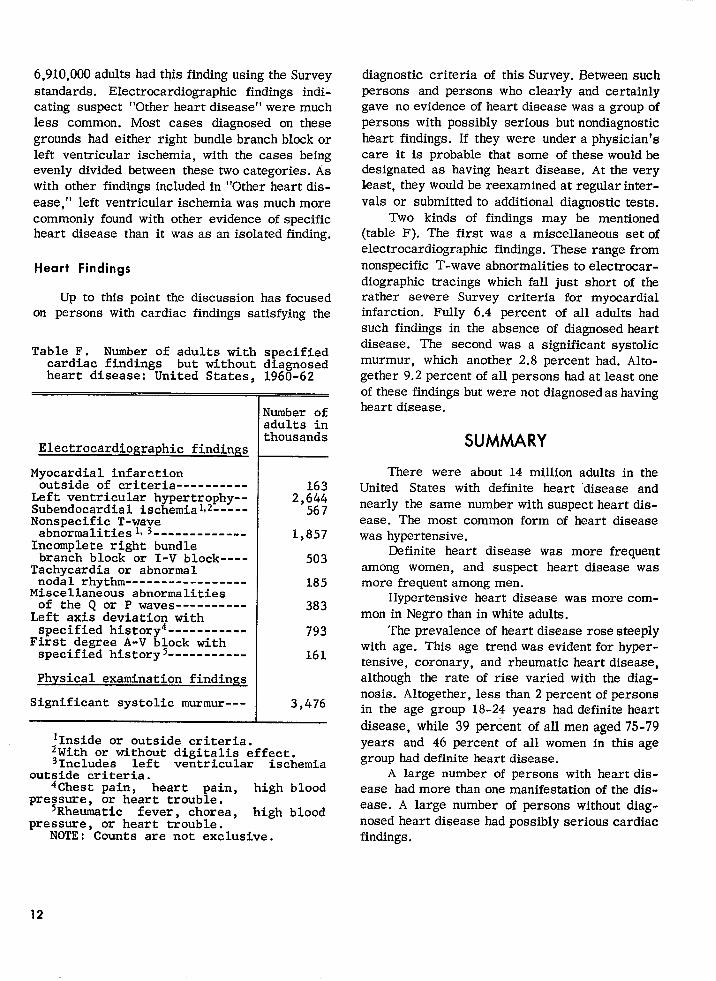
Heart Findings
Up to this point the discussion has focusedon persons with cardiac findings satisfying the
Table F. Number of adults with specifiedcardiac findings but without diagnosedheart disease: United States, 1960-62
Electrocardiographic findings
Myocardial infarctionoutside of criteria ----------
Left ventricular hypertrophy--Subendocardi.al ischemialtz -----Nonspecific T-wave
abnormalities, s-------------Incomplete right bundle
branch block or I-V block----Tachycardia or abnormalnodal rhythm -----------------
Miscellaneous abnormalitiesof the Q or P waves ----------
Left axis deviation withspecified history4-----------
First degree A-V block withspecified history5-----------
Physical examination findings
Significant systolic murmur---
Number ofadults inthousands
1632,644
567
1,857
503
185
383
793
161
3,476
lInside or outside criteria.~With or without digitalis effect.31ncludes left ventricular ischemia
outside criteria.4Chest pain, heart pain, high blood
pressure, or heart trouble.5Rheumatic fever, chores, high blood
pressure, or heart trouble.NOTE: Counts are not exclusive.
diagnostic criteria of this Survey. Between suchpersons and persons who clearly and certainlygave no evidence of heart disease was agroupofpersons with possibly serious butnondiagnosticheart findings. If they were under aphysician’scare it is probable that some of these wouldbedesignated as having heart disease. At the veryleast, they would be reexamined at regularinter-vals or submitted to additional diagnostic tests.
Two kinds of findings may be mentioned(table F). The first was a miscellaneous setofelectrocardiographic findings. These range fromnonspecific T-wave abnormalities toelectrocar-diographic tracings which fall just short of therather severe Survey criteria for myocardialinfarction. Fully 6.4 percent of all adults hadsuch findings in the absence of diagnosed heartdisease. The second was a significant systolicmurmur, which another 2.8 percent had. Alto-gether 9.2 percent ofall persons hadat least oneofthese findings but were not diagnosedashavingheart disease.
SUMMARY
There were about 14 million adults in theUnited States with definite heart “disease andnearly the same number with suspect heart dis-ease. The most common form of heart diseasewas hypertensive.
Definite heart disease was more frequentamong women, and suspect heart disease wasmore frequent among men.
Hypertensive heart disease wasmorecom-mon in Negro than in white adults.
The prevalenceof heart disease rose steeplywith age. This age trend was evidentforhyper-tensive, coronary, and rheumatic heart disease,although the rate of rise varied with the diag-nosis. Altogether, less than 2 percent of personsin the age group 18-24 years had definite heartdisease, while 39 percent ofallmenaged 75-79years and 46 percent of all women in this agegroup had definite heart disease.
A large number of persons with heart dis-ease had more than one manifestation of the dis-ease. A large number of persons without diag-nosed heart disease had possibly serious cardiacfindings.
12
1U.S. National Health Sutvey: Plan sndinitial progrnm oftbe
Health Examination Survey. Health Statistic.s. PHSPub. No. 584-A4. Public Health Service. Washington. U.S. Government PrintingOffice, May 1962.
2National Center for Health Statistics: Cycle Ioftbe HesltbExaminationSurvey, ssmple and response. VitaIand Health Statis-
fits. PHS Pub. No. 1000-Series 11-No. .l. Public Health Service.Washington. U. S. Gmemment Printirrg Office, Apr. 1964.
3N=W York Heart A,socia&n: Nomenclature and Ctiteria f?l
Diagnosis o/Diseases of the Heariand Blood Vessels. New YorkHeart Association, 1955.
4National Centet for Health Statistics: Blood pressure of
adulte”by age and sex. Vital and HeaWr Statistics, pHS .Pub. No.1000-Series II-No. 4. Public Herdth Service. Washington. U.S.Govern ment Printing Office, June 1964.
5National Center for Health Statistics: Blood pressure of
adults by tsce end stea. Vifal andHealth Statistics. PHS Pub. No.
1000-Series 11-No. 5. ,Public Healtb Service. Washington. U.S.Governmen tPrintingOffice, July 1964.
6U.S. National Healrb Survey: Evaluation of a single-visit
cardiovascular exsraination. Herr2ih Statistics. PHS Pub. No. 584-D7. Public Health Service. Washington. U.S. Government PrintingOffice, Dec. 1961.
7National Heart Institute: Reporto/the Conference on Longi-
tudinaI Cardiovascular Studies. Bethesda, Md., 1957.
8PolIack, H.,, snd Kreuger, D. E., eds.: Epidemiologyof Cardi-
.ovas.culsr diseases-hypertension snd stteriosclerosis. Supplementm Am. ]. Pub. Health, Vol. 50, No. 10, 1960.
9Hilbish, T. F., and Morgarr, R. H.: Cardiac mensuration byroentgermlogic methods. Am. J. M. Sc. 224(5) :58G596, Nov. 1952.
000
13
DETAILED TABLESPage
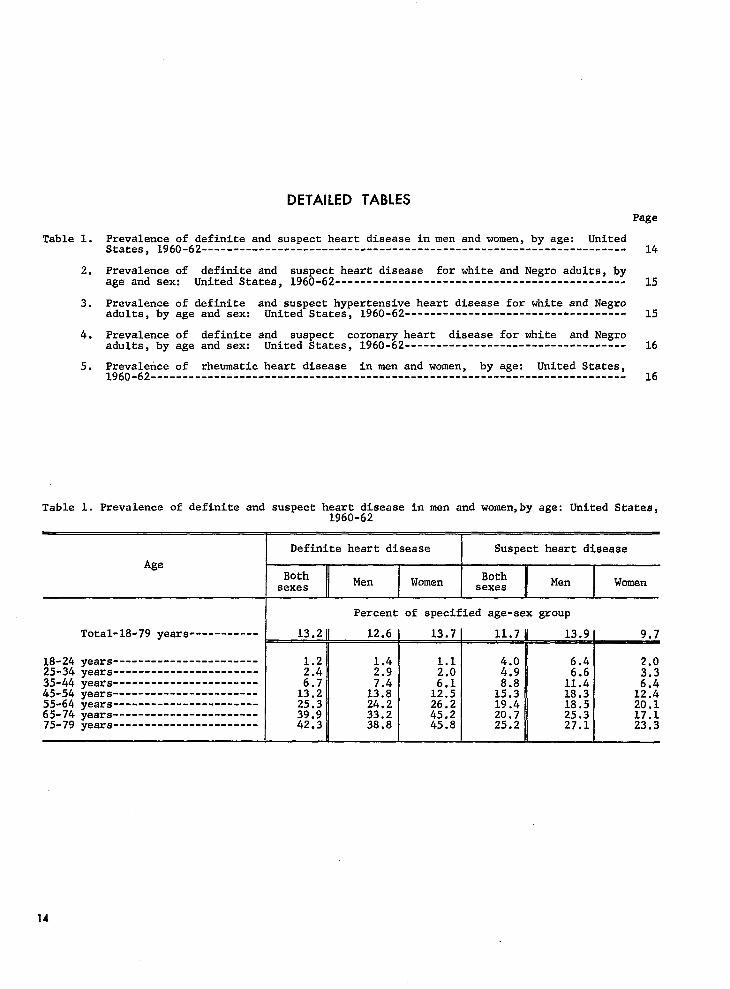
Table 1. Prevalence of definite and suspect heart disease in men and women, by age: UnitedStates, l96O-62------------------------------------------------------------------- 14
2. Prevalence of definite and suspect heart disease for white and Negro adults, byage and sex: United States, 1960-62........-------------------------------------- 15
3. Prevalence of definite and suspect hypertensive heart disease for white and Negroadults, by age and sex: United States, 1960-62----------------------------------- 15
4. Prevalence of definite and suspect coronary heart disease for white and Negroadults, by age and sex: United States, 1960-62----------------------------------- 16
5. Prevalence of rheumatic heart disease in men and women, by age: United States,l96O-62--------------------------------------------------------------------------- 16
Table 1. Prevalence of definite and suspect heart disease in men and women,by age: United States,1960-62
Definite heart disease Suspect heart disease
AgeBoth
Men Women Both
1Mensexes sexes Women
Total-18-79 years-----------
years-----------------------years-----------------------years-----------------------years-----------------------years-----------------------years-----------------------years-----------------------
13.2-
;::
1!:;25.339.942.3
Percent of specified age-sex group
12.6 I 13.71 11.71 13.9[ 9.7
I I n I1.4 1.1 4.0 6.42.9 4.9 R
::! 8.8 1!::1;:$ 12.5 15.3 18.3 1::224.2 26.2 19.4 18.5 20.133.2 45.2 20.7 25.338.8
17.145.8 25.2 27.1 23.3
14
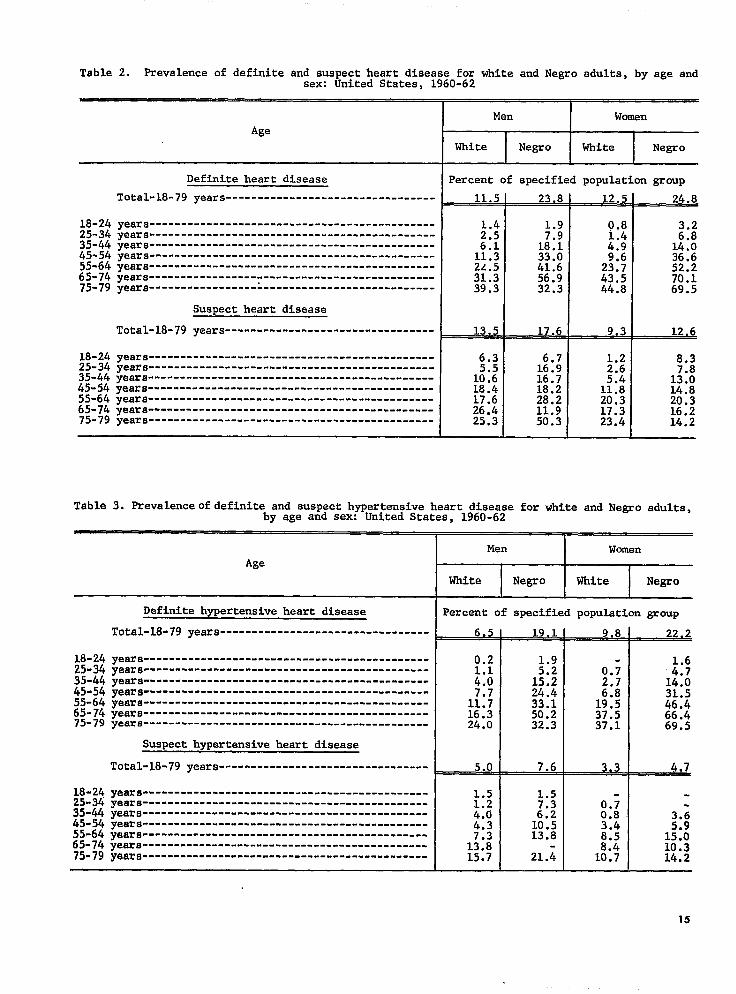
Table 2. Prevalenceof definiteand suspectheart diseasefor white and Negro adulta, by age andsex: United Statea, 1960-62
Age
Definiteheart disease
Total-18-79years---------------------------------
18-24 years---------------------------------------------25-34 years---------------------------------------------35-44 yeara---------------------------------------------45-54 years---------------------------------------------55-64 yeara ---------------------------------------------65-74 years-----------------;---------------------------75-79 years ---------------------------------------------
Suspectheart disease
Total-18-79years---------------------------------
18-24yeara---------------------------------------------25-34 yeara---------------------------------------------35-44 years-----------------------------------------------45-54 yeara---------------------------------------------55-64 yea~s ---------------------------------------------
65-74 yeara ---------------------------------------------75-79years---------------------------------------------
Men Women
White Negro White Negro
Percent of specifiedpopulationgroup
11.5
;::
1:::2.4.531.339.3
__XLJl
6.3
1::::;.;
26:425.3
23.8
+:;18.133.0;;.;
32;3
~
6.716.916.718.228.211.950.3
12.5
0.8
::;
23:743.544.8
9.3
;::
1?::20.317.323.4
24.8
:::14.036.652.270.169.5
12.6
8.3
1;::14.820.316.214.2
Table 3. Prevalenceofdefiniteand suspecthypertensiveheart disease for white and Negro adults,by age and sex: United Statea, 1960-62
Age
18-2425-3435-4445-5455-64~:-;$
18-2425-3435-4445-5455-64;;-;:.
Definitehypertensiveheart disease
Total-18-79years----------------------------.----
yeara ---------------------------------------------
yeara ------------------ --.--..S-- ------------------years --------------------------- --------- .........yeara ---------------------------------------------yeara ---------------------------------------------
yeara---------------------------------------------yeara---------------------------------------------
Suspecthypertensiveheart disease
Total-18-79years---------------------------.-----
years---------------------------------------------years----------------------------------------------
~ears---------------------------------------------ye~ra ---------------------------------------------
years---------------------------------------------yeara --------------------------- ------------------
Men Women
White Negro White Negro
Percentof specifiedpopulationgroup
6.5
0.21.14.0
1::;16.324.0
5.0
::;15.224.433.150.232.3
-L1.5
H 7.34.04.3 1;:;
13.81;::15.7 21.4
1.6
1:::31.546.466.469.5
4,7
3.65*9
15.010.314.2
15
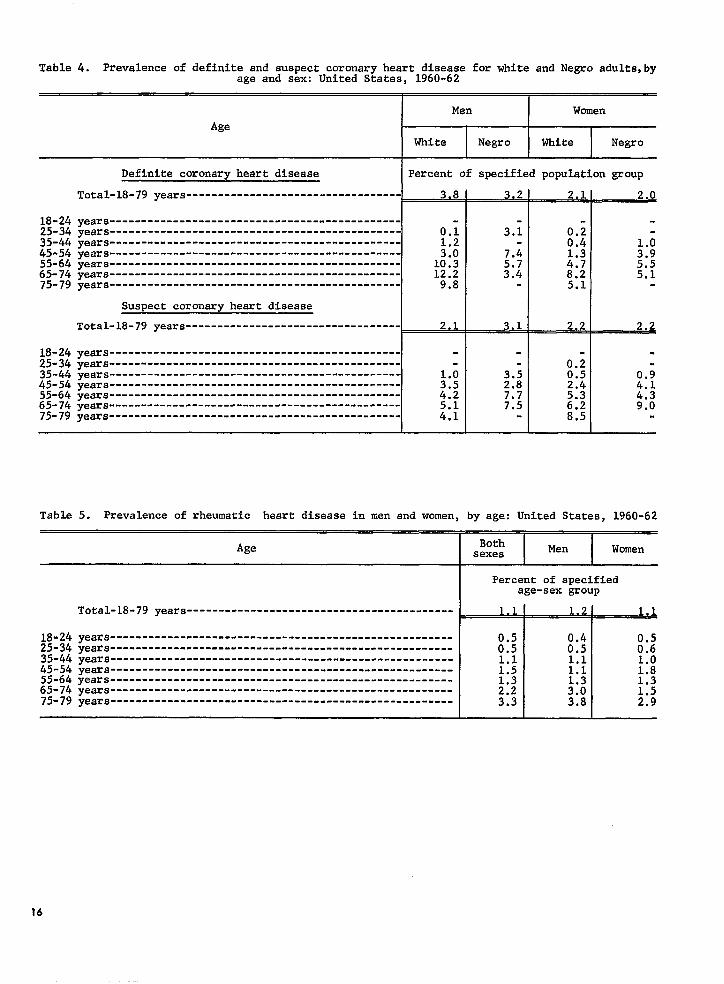
Table 4. Prevalenceof definiteand suspectcoronaryheart diseasefor white and Negro adults,byage and sex: United States, 1960-62
Ken Women
Age
White Negro White Negro
Definitecoronaryheart disease Percentof specifiedpopulationgroup
Total-18-79years----------------------------------w
18-24years----------------------------------------------25-34 years
L
-------------------------------.--------------35-44 years
0.;---------.........----------------------------
45-54 years---------------------------------------------- $:55-64 years----------------------------------------------10,365-74 years----------------------------------------------75-79years
12.2---------------------------------------------. 9.8
Suspect coronary heart disease
Total-18-79 years---------------------------------- 21
18-24years--------------------------------------.-------25-34 years---------------------------------------------- -35-44 years----------------------------------------------45-54 years---------------------------------------------- ;::55-64 years----------------------------------------------65-74 years
4.2----------------------------------------------
75-79 years---------------------------------------------- ::;
3.2
3.1
3,1
;::7.77.5
2.1
0.20.4
::;8.25.1
2.2
0.;0.52.4
::;8.5
2.0
i:5.55.1
2.2
.
.0.94.14.39.0
Table 5. Prevalence of rheumatic heart disease in men and women, by age: United States, 1960-62
Age
18-2425-3435-4445-5455-6465-7475-79
Total-18-79years-----------------------------------------y-
ears ------------------------------------------------------years--------.---------------------------------------------years------------------------------------------------------years------------------------------------------------------years------------------------------------------------------years------------------------------------------------------years------------------------------------------------------
Both I Men I WomensexesI I
Percent of specifiedage-sex group
0.50.51.1
H2.23.3
1,2
0.40.51.11.1
M3.8
~
:::1.01.81.31.52.9
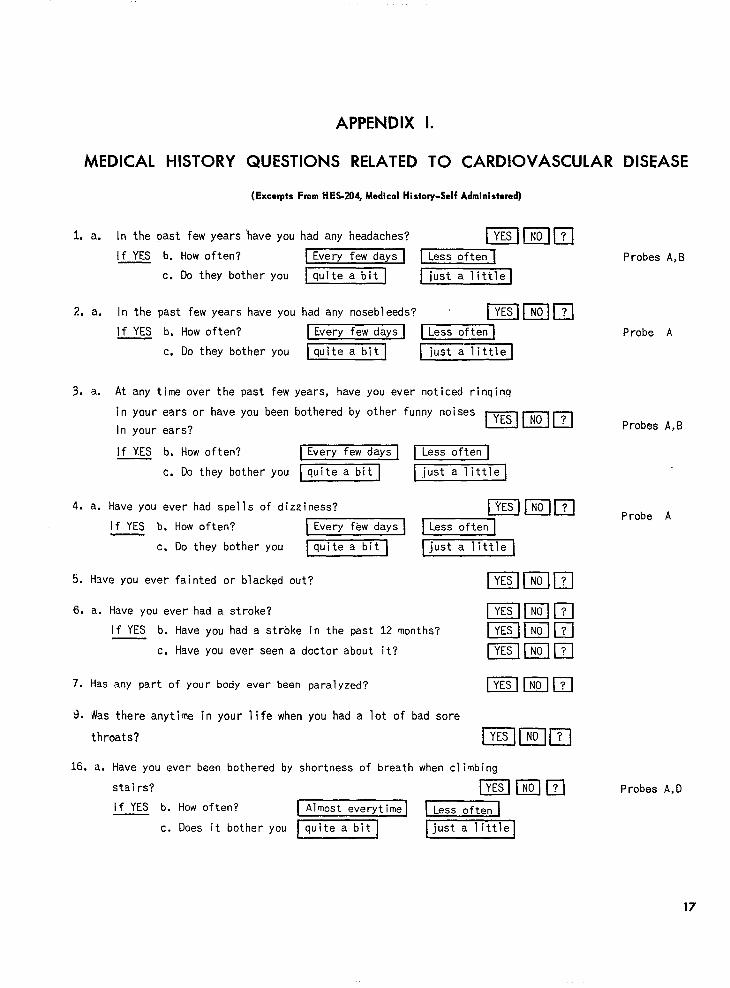
APPENDIX 1.
MEDICAL HISTORY QUESTIONS RELATED TO CARDIOVASCULAR DISEASE
(Excqrts From HES.204, Medical Hi.tory-Self Administered)
1.
2.
3.
4.
5.
6.
7.
9.
16.
a.
a.
a.
a.
In the past few years “have you had any headaches?
[f YES b. How often? Every few days
c. Do they bother you ~
In the past few years have you had any nosebleeds?
If YES b. How often?
c. Do they bother you
At any time over the past few
in your ears or have YOU been
In your ears?
If YES b. How often?
c. Do they bother you
DEHEKIl~iust a littlel
Probes A,B
Emillzl\Every few days-1~
~ just a little
years, have you ever noticed rinqinq
bothered by other funny noisesmmml
Every few days 1~
quite a bit just a little]
Have you ever had spells of dizziness?
If YES b. How often? Every few days
c, Do they bother you@EZZKl
Have you ever fainted or blacked out?
Ellmlzl~just a little
a. Have you ever had a stroke?
If YES b. Have you had a stroke in the past 12 months?
c, Have you ever seen a doctor about it?
Has any part of your body ever been
Was there anytime in your life when
throats?
paralyzed?
you had a lot of bad sore
a,
EmmlElmlElEEltmlzlIEllmm
EElmEl
EHEllzlHave you ever been bothered by shortness of breath when climbing
stai rs? EmlZl
Probe A
Probes A,B
Probe A
Probes A,D
If YES b. How often? Almost everytime ~
c. Does it bother you~~
17
Probe A
Probe A
Probes A,B
4-I -Al.
18.
19.
20.
21.
a.
a.
a.
a,
a.
Have you ever been bothered by
physical work or exercising?
If YES b. How often?
c. Does it bother you
Have you ever been bothered by
shortness of breath when doing
m13Klm
Almost everytime ~
lquitea bitl just a little[
shortness of breath when you were not—
doing physical work or exercising? m mm
If YES b. How often? Every few days ~,
c. Does it bother you Iquite a bit ] Ijust a little]
Have you ever been bothered by shortness of breath
excited or upset about something?
If YES b. How often? Almost everytime
~c. Does it bother YOU quite a b[t
Have you ever waked up at night because you were short of
breath?
If YES b. How often?
c, Does
In the past few
or tightness in
Every few nights
it bother you 1-[
years, have you ever had any pain,
your chest?
EHEIEI~just a little[
discomfort,
m@zlm
IF YES, Please answer questions b through j belw.
b. How often? ~
c. Ooes it bother you ~~~
d. Where does it bother you? (Check every place it bothers you.)
bFront m Iz@Glz2 m -
Somewhere else! State where
e. Does it usually stay in one place ~lzlf. How long does the pain usually last?
bJust a few minutes Few minutes to an hour [More than an hour
I
q. Does it usually come When you take a lot of exercise or
h. Does it usually
when you are quiet 1 or
is there no difference
come wlien you are upset or
doesn’t this make any difference rj. Do you take any pills ornedicine for it? EIEIm
18
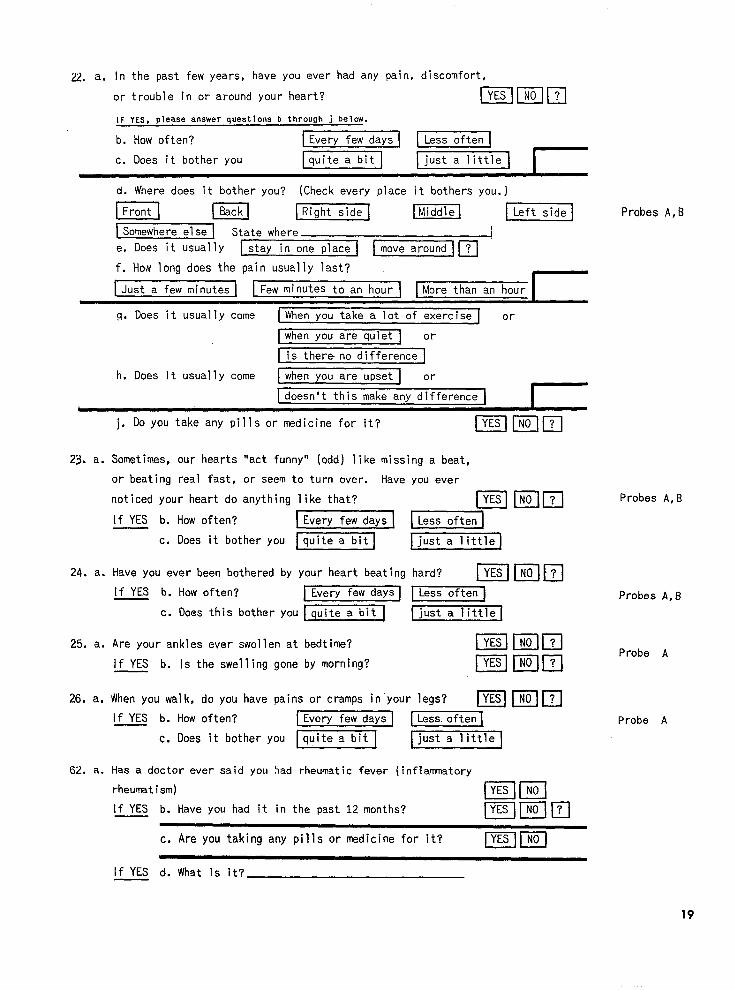
2 a. In the past few years, have you ever had any pain, discomfort,
or trouble in or around your heart? Ellzlm
IF YES, please answer questions b through j below.
b. How often? Every few daysL____l~
c, Does it bother you ~ just a little Id. Where does it bother you? (Check every place it bothers you. )
m El EImEl miEEl LzmElSomewhere else State where !
e. Does it usually stay in one place I ~m
f. How long does the pain usually last?
Just a few minutes
Probes A,B
g. Does it usually come When you take a lot of exercise or
when you are quiet 1 or
is there no difference 1
h. Does it usually come when you are upset I or
doesn’t this make any differenceI I
j. Do you take any pills or medicine for it? m
Sometimes, our hearts “act funny” (odd) like missing a beat,
you ever
m
-
just a little
or beating real fast , or seem to turn over. Have
noticed your heart do anything like that?
If YES b. How often? Every few days
c. Does it bother you ~1
Have YOU ever been bothered by your heart beating
Probes A,B
hard? Immm24. a.
Probes A,BIf YES b. How often? Every few daysL___J~
c. Does this bother you [-1
Imlmlzl25. a.
26. a.
Are your ankles ever swollen at bedtime?Probe A
mEmlIf YES b. Is the swelling gone by fnorning?
When you walk, do you have pains or cramps in your legs? IX!lmm
Probe AIf YES b. How often? Every fewdsys ~
c. Does it bother you 1-1~
62. a. Has a doctor ever said you +ad rheumatic fever (inflammatory
rheumatism)
[f YES b. Have you had it in the past 12 months?ElmEmmI
c. Are you taking any pills or medicine for it? Blzz
lfYES d. What is it?
19
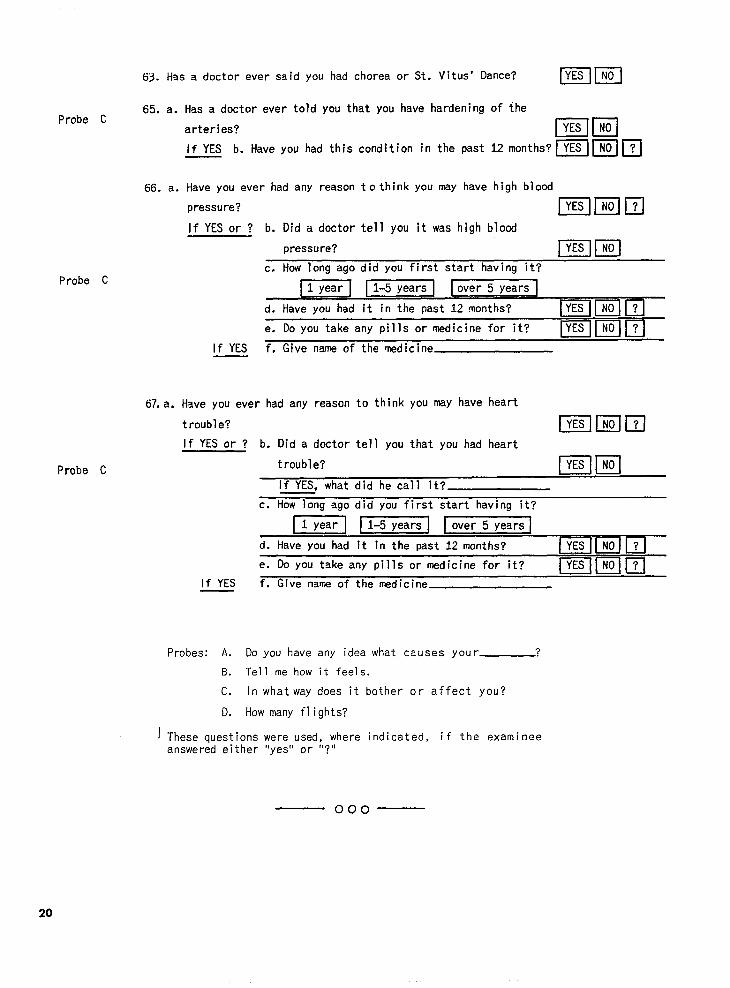
63. Has a doctor ever said You had chores or St. Vitus’ Dance? mm
65. a. Has a doctor ever told you that you have hardening of theProbe C
arteries? mm
If YES b. Have you had this condition in the past 12months?~l~]~l
66. a. Have you ever had any reason tcthink you may have high blood
Probe C
67. a.
Probe C
pressure? Bl@lIl
lf YES or? b. Dida doctor tell you it was high blood
pressure? mmc. How long ago did you first start having it?
1 year~
d. Have you had it in the past 12 months?~ & _
e. Do you take any pills or medicine for it?mm 1
If YES f. Give name of the medicine
Have you ever had any reason to think you maY have heart
trouble? Bmm
lfYES or ? b. Did a doctor tell you that you had heart
trouble?mm
If YES, what did he call it?
c. How long ago did you first start having it?
m-~
d. Have you had it in the past 12 months?
e. Do you take any pills or medicine for it?mlIzlm
if YES f. Give name of the medicine
Probes: A. Do you have any idea what causes your ?
B. Tell me how it feels.
c. In what way does it bother or affect you?
D. How many flights?
lThesequestions were used, where indicated, if the examineeanswered either “yes” or “?”
— 000
20
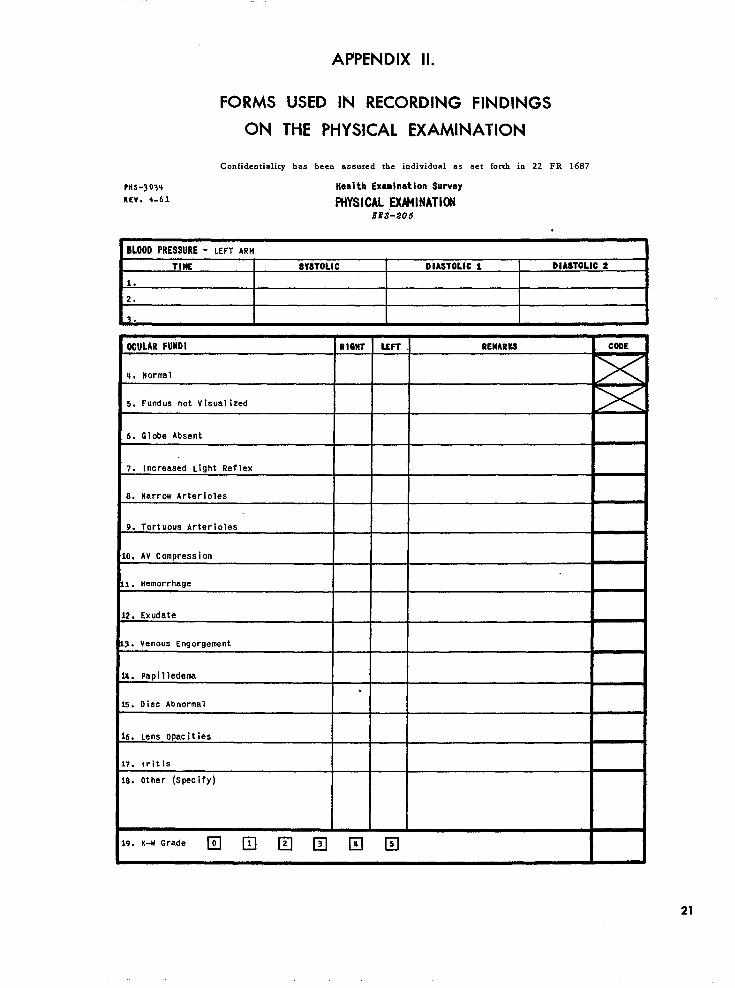
FORMS
ON
Confidentiality
PHs-j03~
REV. 4-61
APPENDIX Il.
USED IN RECORDING FINDINGS
THE PHYSICAL EXAMINATION
has been assured the individual as
Wealth Examination Suwey
FMYSICAL EXMNATICN
set forth in 22 FR 1687
lfES-205
.
BLOOD PRESSURE - LEFT ARM
TIME ! SWTOLIC I DIASTOLIC 1 ! OIASTOLIC 2
OOULAR FUNOI RIGHT LEFr . REMARKS COOE
u. Normal
S. Fund us not V isual ized
6. Globe Absent
7. Increased Li9ht Reflex
6. Narrow Arterioles
9. TOrt UoUS Arterioles
O. AV Compression
1. Hemorrhage
2. Exudate
1. Venous Engorgernent
t. Papilledema
.
5. Disc Abnormal
5. Lens opacities
7. Iritis
9. Other (Specify)
‘“’-”’”de IZl ❑ E lZl IZl ❑
21
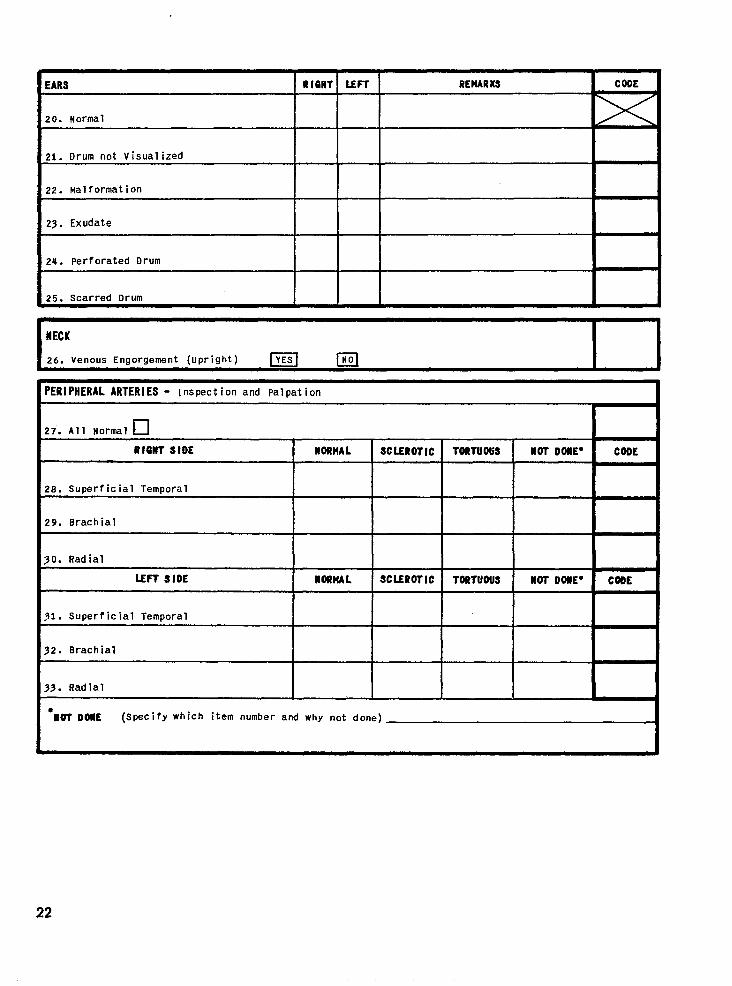
EARS U 16HT LEFT REHARKS CODE
20. Itormal
21. Drum not Visualized
22. Malformation
23. Exudate
24. Perforated Drum
25. Scarred Drum
HECK
26. Venous Enaoraement (uoright) m m
PERIPHERAL ARTERIES - Inspection and palpation
❑27. All Normal
RlanTslDE SCLEROTIC
28. Superficial Temporal
29. Brachial
SO. Radial
LEFT SIDE
~1. Superficial Temporal
32. Brachial
IIORHAL
IIORHAL SCLEROTIC
33. Radial
*
I
●WTOWE (Specify which item number and why not done)
22
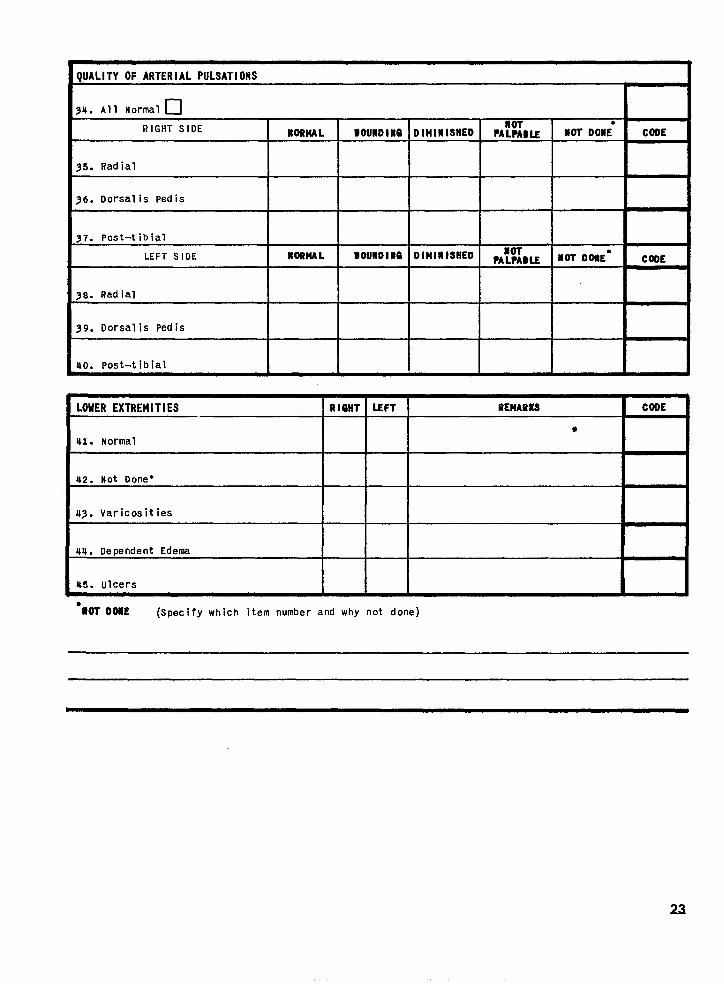
QUALITY OF ARTERIAL PULSATIONS
94. All Normal •1
RIGHT SIDE I IIORHAL I OOUHDl#O
35. Radial I I
36. Dorsalis pedis I I
==+4==38. Radial I I
39. Dorsalis pedis
40. Post-t ibial I I
T HOT DOME”
NOT DONE*
CODE
CDBE
LOWER EXTREMITIES R leHT LEFT REHARKS COOE
*41. Normal
42. Not Done*
43. Varicositiesr
44. Dependent Edema
45. ulcers\
“MT DOIIE (Specify which item number and why not done)
23
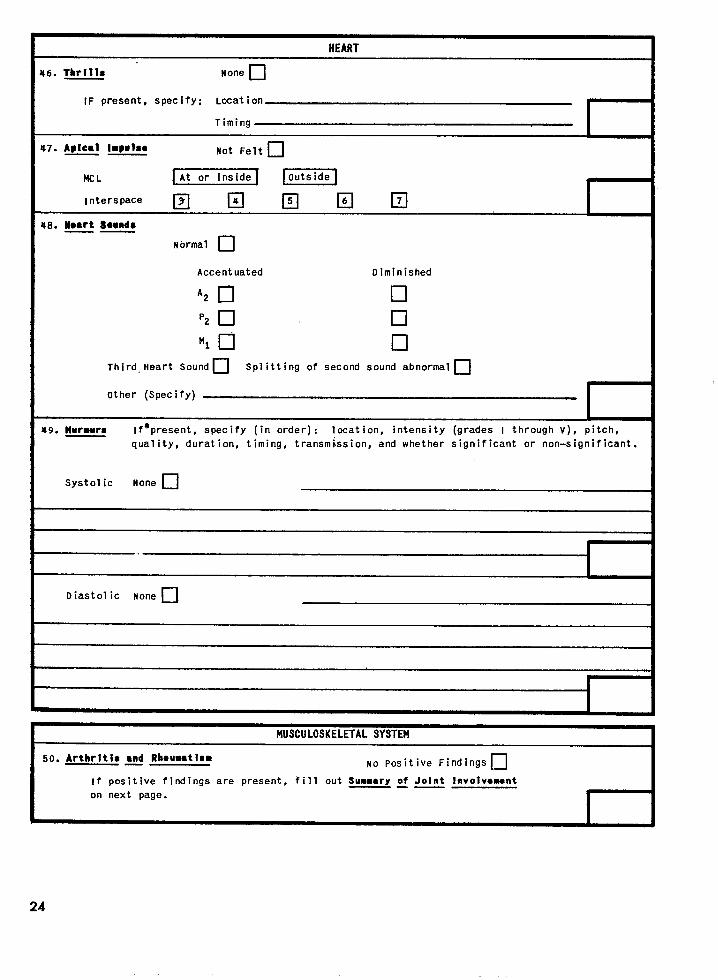
HEART
46. Thrills None ❑
IF present, spec ify: LoCat ion
Timing
47. A@ical hPMhO—— Not Felt ❑
MC L At or inside EzEl
InterspaceIZIIIIEIKIEI
*8. W08rt Sosnd8.—
Normal •1
Accent uated Diminished
‘2 •1 •1
P2 •1 •1
‘1 •1 •1
Third Heart Soundn Splitting of second sound abnormaln
Other (Specify)
49. Iturmurs If*present, specify (in order): location, intensity (grades I through V), I
quality, duration, timing, transmission, and whether significant or non-sigl
Systolic None •1
Diastolic None •1
I
1
pitch,
nificant.
F
MUSCULOSKELETAL SYSTEM
50. Arthritis ●nd Rboumatlam—— No Positive Findings n
if positive findings are present, fill out Summary of Joint Involvount—— —
on next page.
I
# I I
24
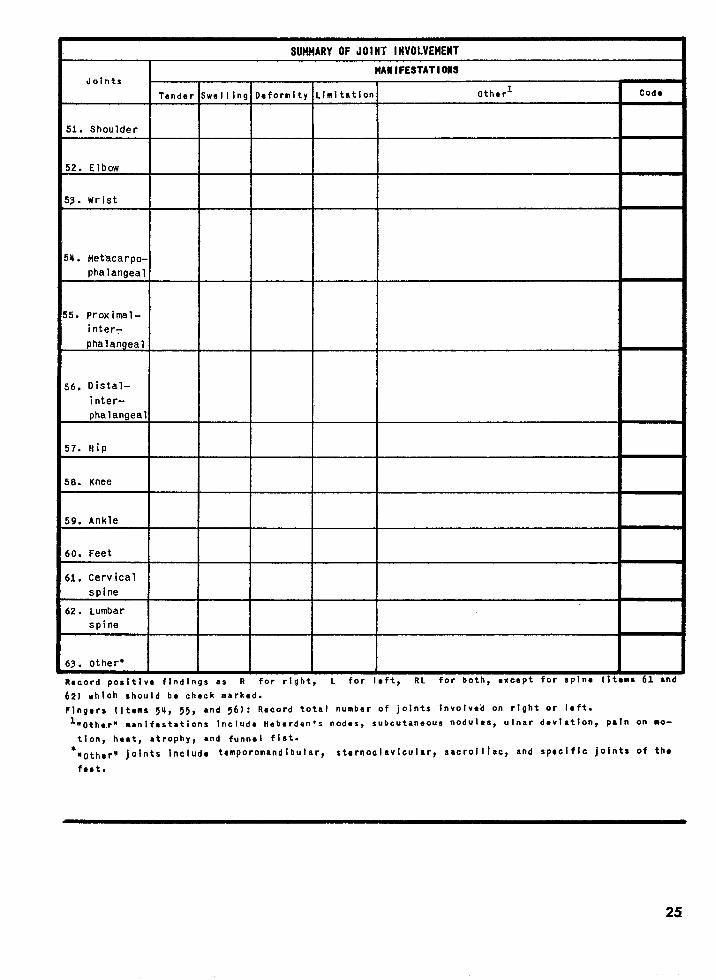
SUMMARY OFJOIHT INVOLVEMENT
JointsMAIIIFESTATIOM
Tender Swelling Deformity Ll!sitatlon Othorl Cods
51. Shoulder
i2. Elbow
i3. Wrist
4. Metacarpo-
phalangealI
5. proximal-
inter=
phalangeal
,6, Distal-
inter-
phalangeal
i7. Hip
i8. Knee
;9. Ankle
iO. Feet
il. Cervicalspine
i2. Lumbar
spine
i3. other”. -. . . .. . . , ... —— .. -— .
Racord posltivc findings as R for right, L for I@ft, RL tor aozn, ●xcapz Tor spin* IIc*ms OL ana
62J which should ba check marked.
Flngars (Items 54, 55, and 56): Record total number of joints Involved on right or left.
l-othc.rn manifestations Include Heberden”s nodes, subcutaneous nodules, ulnar devl~tion, Pain on ● O-
tlon, hsst, ●trophy, and funnal fist.
*mothcrn IOlnts Include temporomandlbular~ aternoclavicular, sacroiliac, and spoclflc joints of th~
fast.
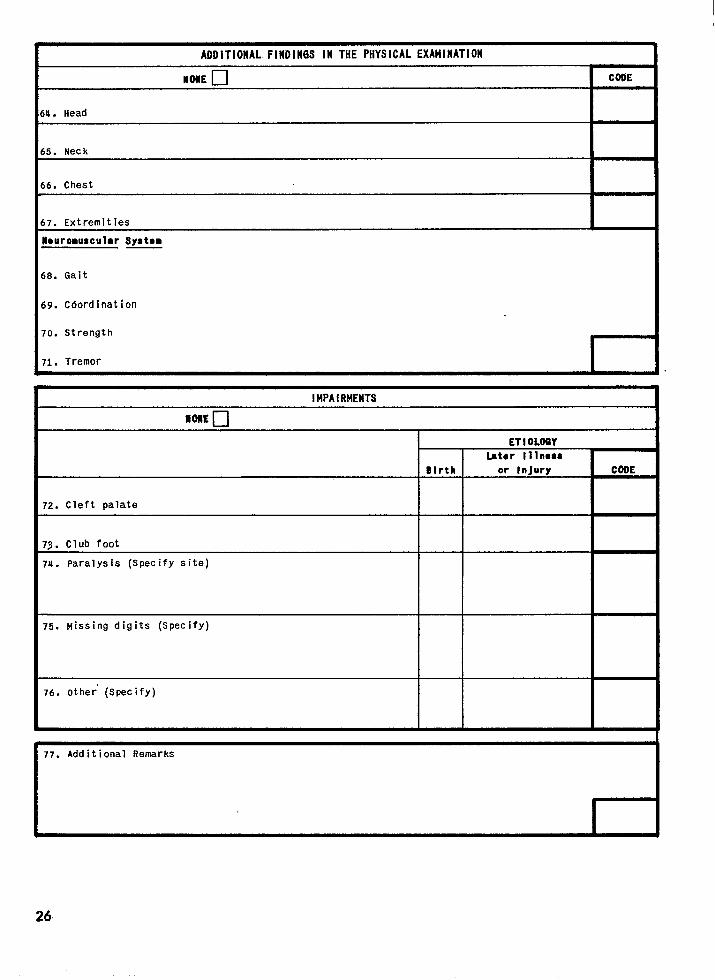
ADDITIONAL FIHDIN6S Ill THE PHYSICAL EXAtilHATIOH
u. Head I
5. Neck
6. Chest I
7. Extremities I
Iouroauscular Sy8tom
8.
19.
‘o.
‘1.
Gait
Coordination
Strength
Tremor r
I14PAIRMENTS—
NONE u
72. Cleft palate
73. Club foot
74. Paralysis (Specify site)
75. Missing digits (Specify)
76. other’ (SpeCify)
ET 10LOGY
F COOE
77. Additional Remarks
I
26
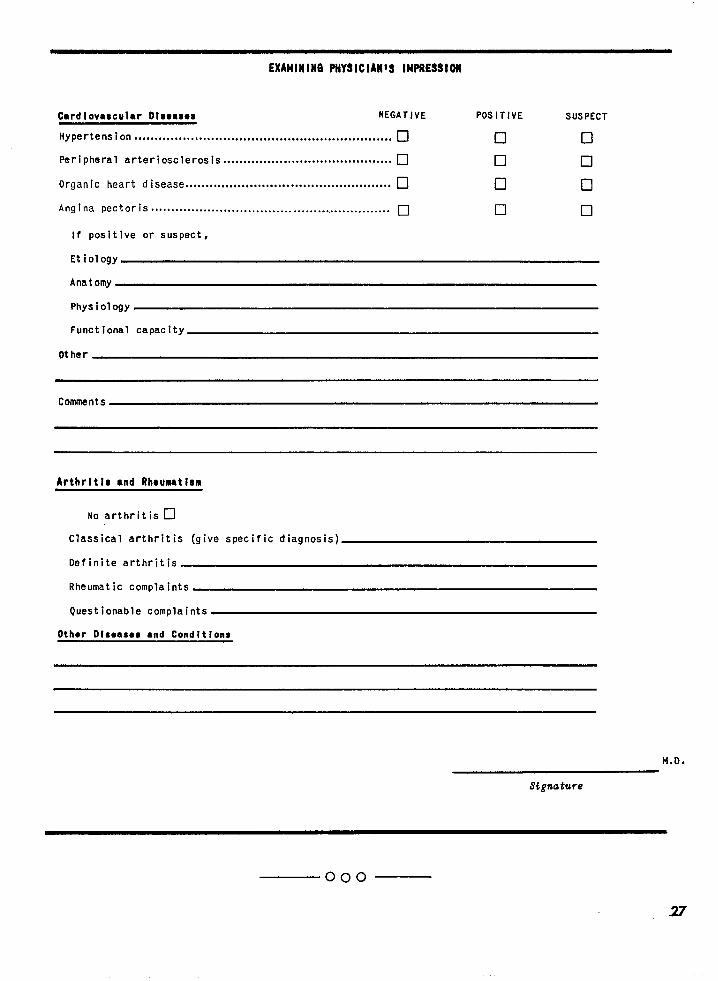
EXAkllHll16 PtlYSICIAH~S IMPRESSIM
Cardiovascular Dlsomes NEGATIvE PoSITIVE SUSPECT
Hypertens ion ................................................................ •1 •1 •1
Peripheral arteriosclerosis .......................................... •1 •1 ❑
Organic heart disease ................................................... •1 •1 •1
Angina pectoris ............................................................ •1 •1 ❑
If positive or suspect,
Etiology
Anatomy
Functional capacity
Other
Comments
Arthrltls ●nd Rh.umtlsm
No arthritis ❑
Classical arthritis (give specific diagnosis)
Definite arthritis
Rheumatic complaints
Questionable complaints
Other Dlsoasoa tnd Condltlons
M.D.
Signature
000
27
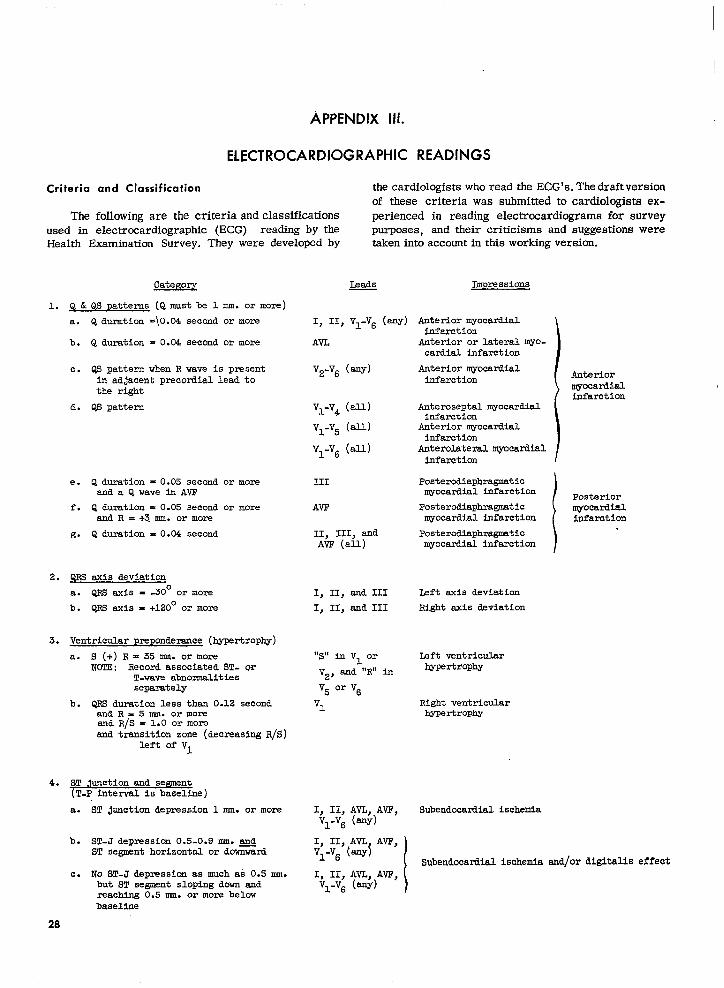
APPENDIX ui.
ELECTROCARDIOGRAPHIC
Criteria
Theused in
and Classification the cardiologistswho read theECG’S.The draftversion
of these criteriawas submittedto cardiologistsex-
followingare the criteriaand classifications perienced in reading electrocardiogramsfor survey
electrocardiographic(ECG) readingby the purposes, and their‘criticismsand suggestionswereThey were developedby takenintoaccountinthisworkingversion.Health Examination Survey.
CateKoq
1. Q&QSP atterns(Qmustbe 1 mm. or more)
a. Q duration=\O.04secondor more I, II, V1-V6(my)
b. Q duration= 0.04secondor more AVL
c. QS patternwhenR wave is present V2-V6(w)in adjacentprecordialleadtothe right
d. QS pattern V1-V4(all.)
V1-V5(all)
V1-V6(all)
III
AVF
II, 111,andAVT (all)
e. Q duration-0.05 secondanda Qwavei.nAVP
f. Q duration= 0.05secondand R = +3.mm. or more
g. Q duration= 0.04second
or more
or more
2.
3.
4.
QRs axisdeviation
a. QRS axis= -30°or more
b. QRS axis= +120°or more
1, II,and III
I, II,sad III
Ventricularpreponderance(hypartrophy)
a. S (+)R = 35 mm. or more “S” in V1 orNCTE: RecordassociatedST- w
T-waveabnoznmlities V2* and “R” in
separately V5 or V6
b. QRS durationlessthen0.12second V1andR.5mm. or momend.R/S = 1.0 or moreand transitionzone
leftof VI(decreasing R/S)
ST junction and segment(T-Pintervalis baseline)
a. ST junctiondepression1 mm. or more I, II,AVL,AVP,V1-V6(any)
b. ST-Jdepression0.5-0.9m. and I, 11,AVL AVF,ST segmenthorizontalor dcw%%ni V1-V6(W1
c. No ST-Jdepressionas muchas 0.5mm. I, II,AVL,AV7?,but ST segmentslopingdownand V1-V6(any)reachingO.5mn. or morebelowbaseline
Impressions
Anteriormyowmd.ielinfarction
Anterioror lateralmYO-cazdie.1infarction
Anterior myocardialinfarction
Anteroseptelqyocardialinfarction
Anteriormyocardialinfarction
Anterolateralmyocatiialinfarction
Anteriormyocardialinfarction
Posterodiaphragmaticmyocardialinfarction ) PosteriorPosterodiaphrwustic
}myocardial
~ocardla.1infarction Infarction
Posterodiaphragmticmyocafiialinfarction
Leftaxisdeviation
Righta%isdeviation
Leftventricularhypertrophy
Rightventricularhypertrophy
Subendocardial.ischemia
1Subend.ocardielischemiaend/ordigitaliseffect
28
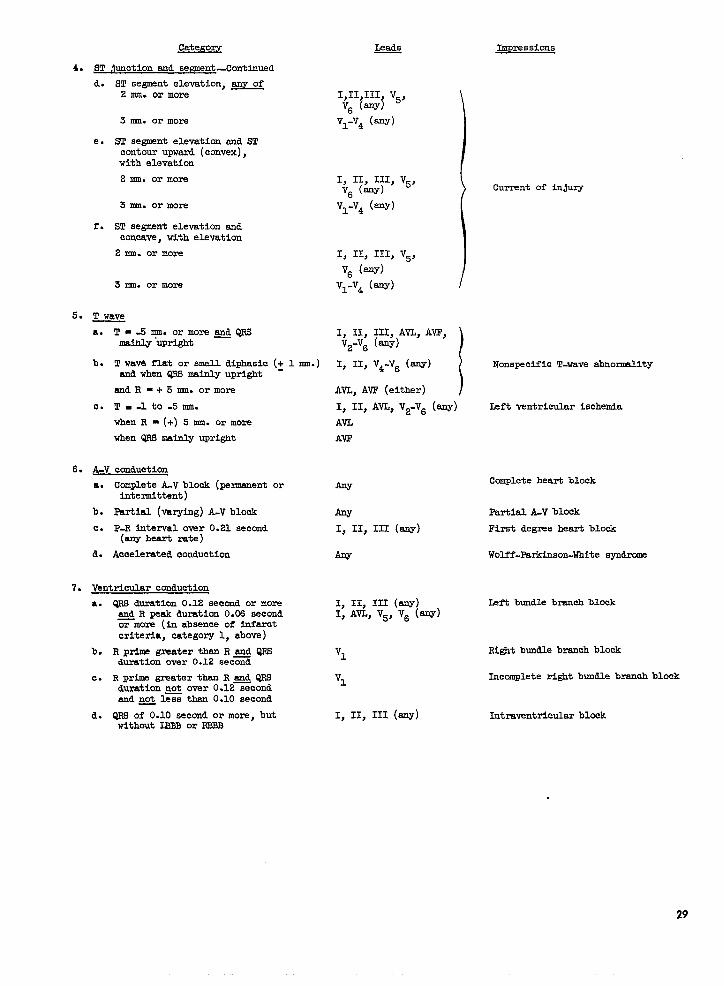
Categoqy
4. ST ,Iunction eud segment-Continued
d.
e.
r.
ST ee~nt elevation,anY of2 mm. or more
3 mm. or more
S9!.9egmentelevationand STcontourupward(convex),withelevation
2 mm. or more
3 mm. or more
S9!segmentelevationCMconc&, withelevation
2 mm. or more
3 nm. or more
5. T We.ve
a.
b.
c.
6. ~
T=-5nmhormores&QF5malhly “upright
T wav4 flat or smell diphasic(~ 1 mm.)andwhenQRSmainlyupright
aMR=+5mn. or more
!l!-.lto-5 mm.
whenR = (+)5 cmI.or more
whenQRSmainlyupright
conduction
a. Complete A-V block (permanent orIntermittent)
b. Partial (varying)A-V block
c. P-R intervalover0.21second(enyheartrate)
d. Acceleratedconduction
7. Ventricularconduction
a.
b.
c.
d.
QRS duration0.12secondor moreQ R peakduration0.06secondor more (inabsenceof tifarctcriteria,category1, above)
R primegreaterthanR md QRSdumtion over 0.12 sec=d
R pr~ greaterthanR & QRSdurationnot over0.12secondandpQ 1= than0.10second
C&S of 0.10secondor more,butwithoutIBB2or RBB2
Leads
1)11)111 V5SV6 (aw~ \
V1-V4 (any)
1> II> 111> ‘J5>V6 (w)
VI-VA (aY)
Impressions
Currentof in.juzy
I, II, 111,AVL,AVF,V2-V6(fW’) )I, II,V4-V6(any)
\Nonspecific T-wave abnormality
AVL,AVF (either)
1$ llJ‘~$ ‘2-V6AVL
AVF
m
m’I, II, III (my)
w
I, II, III (anY)v (-)I>A% v5~ 6
V1
V1
I, II, III (any)
Ieftventricularischemla
Complete heart block
Partial A-V block
Firstdegreeheartblock
Wolff-Parkinson-Whitesyndrome
Left bundle branch block
Rightbundle branchblock
Incompleterightbundlebranchblock
Intraventricular blak
29
Categoq
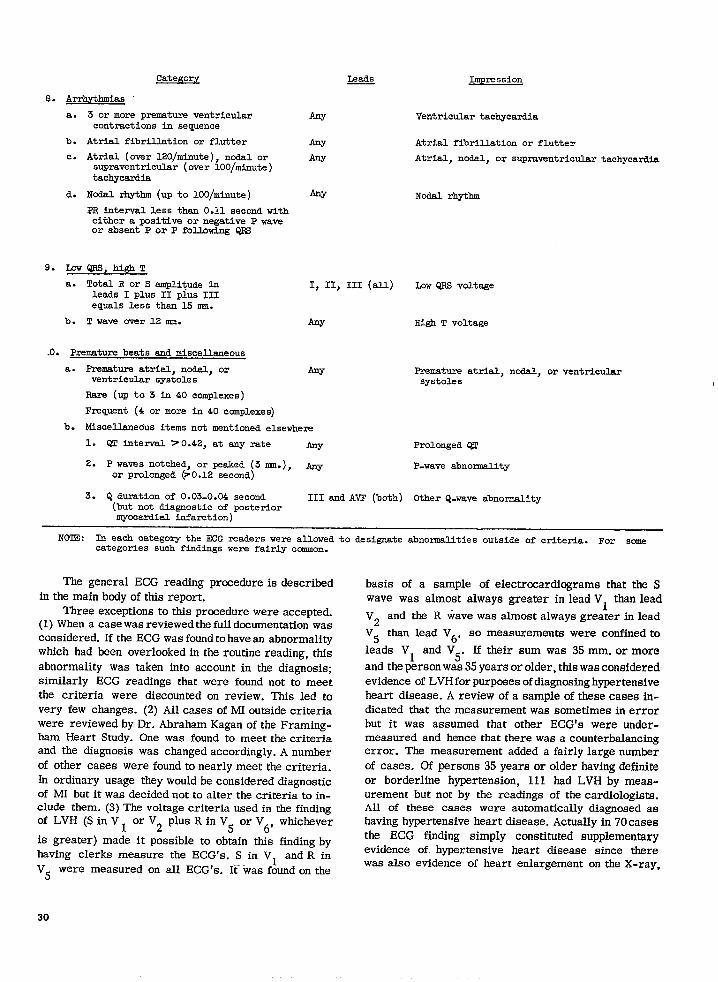
8. Arrhythmias
Impression
a.
b.
c.
d.
3 or more prematu~ ventricularcontractions in sequence
Atrial fibril.lationor flutter
Atrial (over 120/minute), ncdal orsupraventricular (over 100/minute)tachycardia
Nodal rhythm (up to 100/minute)
PR interval.less thsn O.11.second witheither a positive or negative P waveor absent P or P following Q16
9. LOW QRS, high T
a. Total R or S eunplitudeinleads I plus II plus IIIequals less than 15 nro.
b. T waw over 12 mm.
.0. Premature beats and miscellaneous
a. Premature atrial, nodal, orventricular systoles
Rare (up to 3 in 40 complexes)
Frequent (4 or more in 40 complexes)
ArJY
mw
w
Ventricular tachycardia
Atrial fibrillation or flutter
Atrial, no3al.,or supraventricular tachycardia
Nodal rhythm
I, II, III (all) Lcw QRS voltage
m High T voltage
Aw Premature atrial, nodal, or ventricularsystoles
b. Miscel.lanedusitems not mentioned elsewhere
1. QT interval 70.42, at my rate Any Prolonged QT
2. P waves notched, or peeked (3 mm.), @or prolonged &O. 12 second)
P-wave abnormality
3. Q duration of 0.03-0.04 second III and AVF (both) Other Q-wave abnormality(but not diagnostic of posteriormyocardial infarction)
NOTE: In each catego~ the ECG readers were allcwed to designate abnormalities outside of criteria. For somecategories such findings wers fairly common.
The general ECG reading procedure is described
in the main body of this report.Three exceptions to this procedure were accepted.
(1) When a case was reviewed the full documentation wasconsidered. If the ECG was found to have an abnormalitywhich had been overlooked in the routine reading, this
abnormality was taken into account in the diagnosis;similarly ECG readings that were found not to meetthe criteria were discounted on review. This led tovery few changes. (2) All cases of MI outside criteriawere reviewed by Dr. Abraham Kagan of the Framing-ham Heart Study. One was found to meet the criteriaand the diagnosis was changed accordingly. A number
of other cases were found to nearly meet the criteria.In ordinary usage they would be considered diagnosticof MI but it was decided not to alter the criteria to in-clude them. (3) The voltage criteria used in the findingof LVH (S in V ~ or V2 plus R in V5 or V
6’whichever
is greater) made it possible to obtain this finding byhaving clerks measure the ECG’S. S in VI and R in
V5 were measured on all ECG’S. It- ‘was found on the
basis of a sample of electrmardiograms that the Swave was almost always greater in lead VI than lead
V2 and the R wave was almost always greater in lead
V5 than lead V6, so measurements were confined to
leads VI and V5. If their sum was 35 mm. or more
and the person was 35 years or older, this was consideredevidence of LVH for purposes of diagnosing hypertensiveheart disease. A review of a sample of these cases in-dicated that the measurement was sometimes in errorbut it was assumed that other ECG’S were under-measured and hence that there was a counterbalancingerror. The measurement added a fairly large number
of cases. Of persons 35 years or older having definite
or borderline hypertension, 111 had LVH by meas-urement but not by the readings of the cardiologists.All of these cases were automatically diagnosed ashaving hypertensive heart disease. Actually in 70 casesthe ECG finding simply constituted supplementaryevidence of. hypertensive heart disease since therewas also evidence of heart enlargement on the X-ray,
30
and in only 7 of these cases was the diagnosis changedfrom suspect to definite hypertensive heart disease asa consequence of the ECG measurement. In the re-maining 41 cases, however, a new diagnosis of hy-pertensive heart disease resulted—in 23 cases definite,and in 18 suspect. The net effect of the ECG measure-ment was to raise the prevalence of hypertensive heartdisease by approximately 9 percent.
The distributions of LVH findings by the readersfor persons 3S years and over against the combinedsum of the S in VI and the R in V
5were as follow:
s (vyY (V5)
Under 35 mm-----35 nml-----------36 mm-----------37 lmn-----------38 mn-----------39 mm-----------40 nm-----------41 mm-----------42 mm-----------43 m-----------44 nml-----------45i- mm----------
Number of electrocardiograms
Total
3,9036253
%3322222718
i%’
=l=E3,858
:;262217129
This tableincludesallsample persons,whatevertheir
blood pressure.If aperson hadnormal blood pressure, no account
was taken in thisreportofdiscrepanciesbetweenthe
electrmardiographicreadingsand the measurements
for LVH. Had this been done, the numixw ofpersonsconsidered to have had significant but nondiagnosticcardiac findings would have been increased by about10percent.
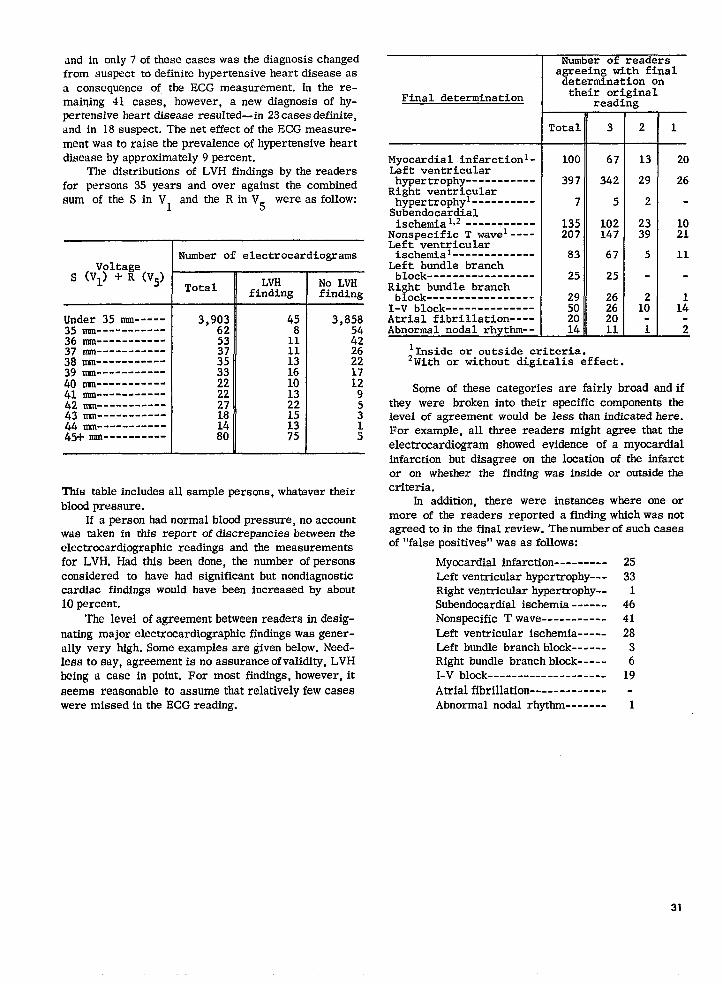
The level ofagreement between readers indesig-nating major electrocardiograpbic findings was gener-ally very high. Some examples are given below. Need-Iesstosay, agreement is noassuranceof validity, LVHbeing a case in point. For most findings, however, itseems reasonable to assume that relatively few caseswere missed intheECG reading.
Final determination
Myocardial .infarcti.on1-Left ventricularhypertrophy-----------
Right ventricularhypertrophyl----------Subendocardialischemial,z-----------
Nonspecific T wavel----Left ventricularischemial-------------
Left bundle branchblock-----------------
Right bundle branchblock-----------------
I-V block--------------Atri.alfibrillation---A-bnormal nodal rhythm--
Number of readersazreeinz with finalileterm~nationon
their originalreading
Total
100
397
7
135207
83
25
29502014
3
67
342
5
102147
67
25
26262011
+
21
13 20
29 26
2-
llnside or outside criteria.Zwith or without digitalis effect.
Some of these categories are fairly broad and ifthey were broken into their specific components thelevel of agreement would be less than indicated here.For example, all three readers might agree that theelectrocardiogram showed evidence of a myocardialinfarction but disagree on the location of the infarctor on whether the finding was inside or outside thecriteria.
In addition, there were instances where one ormore of the readers reported a finding which was notagreed tointhe final review. Thenumberofsuchcaseeof “false positives” was as follows:
Myocardial infarction ---------Left ventricular hypertrophy---Right ventricular hypertrophy--Subendmardial ischemia ------Nonspecific Twave -----------Left ventricular ischemia -----Left bundle branch block ------Right bundle branch block -----I-V block --------------------Atrial fibrillation ----- --------Abnormal nodal rhytbm -------
2533
1464128
36
19
1
31
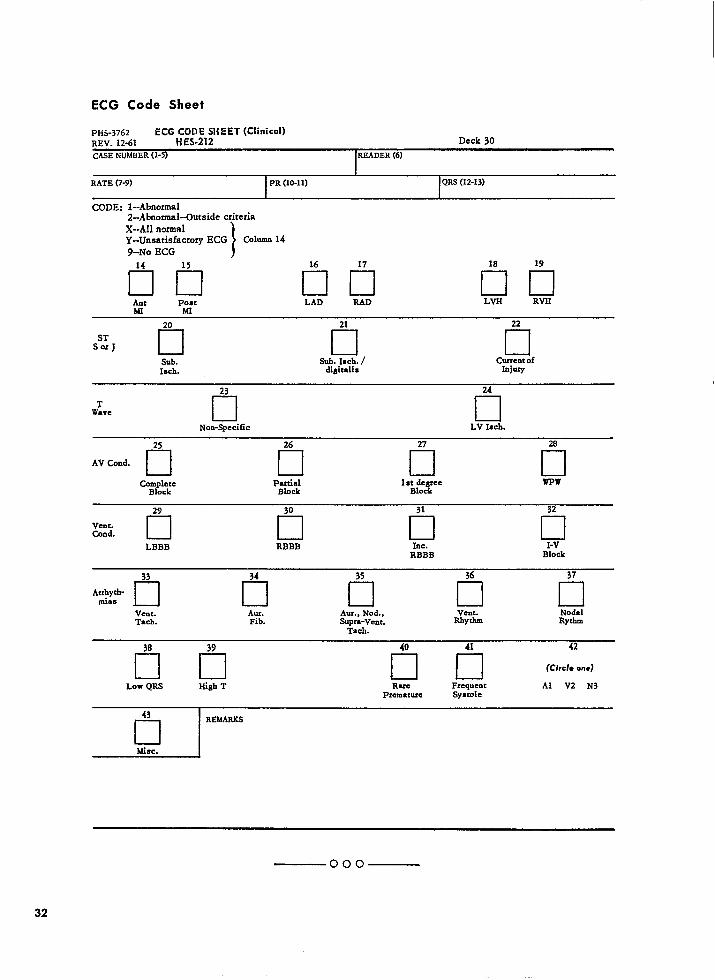
ECG Code Sheet
PH5-3762 ECG #::,~14EET (Clinical)REv. 12-61 Deck 30
cASE NUMBER (1-5) READER (6)
1
RATE (7-9; PR (10-11) QRS (12-13)
CODE: I--Abnormal2--Abnmmsl--Outside criteria
X--AH normalY--Unsatisfactory ECG
\
Column 14
%-No ECG
rln on 00Am PO# LAD RAD LV33
MI
RVH
20 21 22
S% J ❑ •1 ❑Sub. Sub. 18ch. / Current of
Isch. digitalis Injury
23 24
TWave
•1 •1Non-Specific LV IICh.
25 26 27 28
AV Cond.•1 •1 •1 •1
co;::: P8u&?.. 1s~;:yee WIw
29 30 31 32
Vent.Cond. ❑ •1 •1 •1
LBBB RBBB Inc. l-vRBBB Block
33 34 35 36 37
Arrhyth-mias n ❑ •1 •1 ❑
Vent. Aur. Aur., Nod., vent. NodalTach. Fib. Supr8-Vent. Rhythm Rytbm
Tach.
On tln42 (CfrcI*one)
Low QRS High T Rare Frequent Al V2 N3Premature Sysmle
32
43
❑REMARKS
Misc.
—ooo —
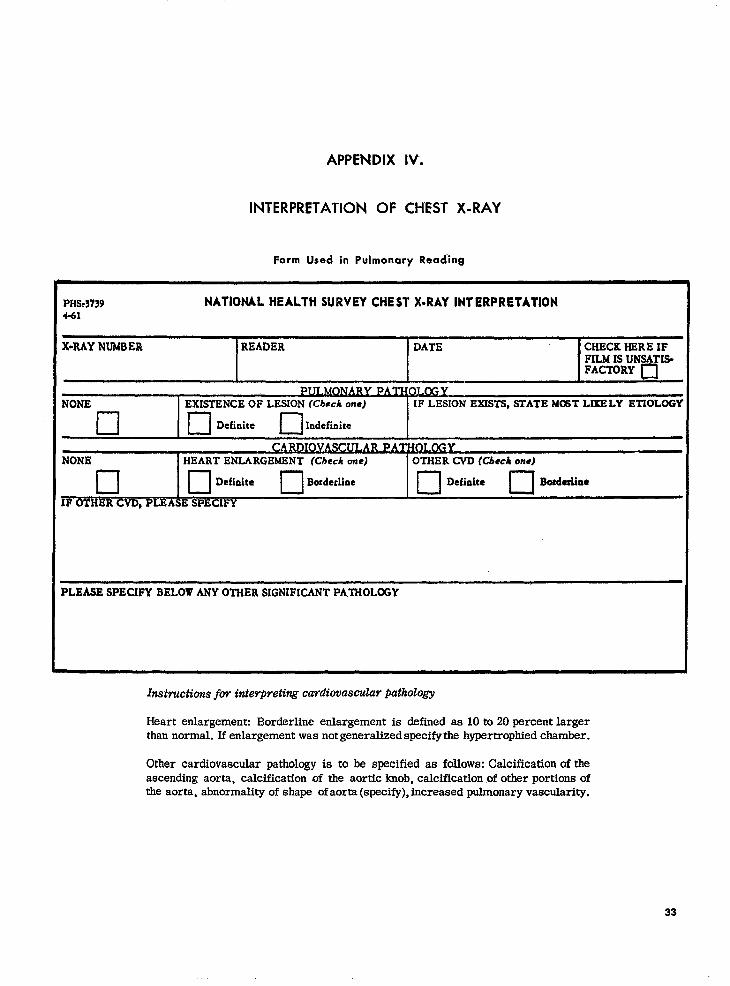
APPENDIX IV.
INTERPRETATION OF CHEST X-RAY
Form Used in Pulmonary Read”ing
PHS,3739 NATIONAL HEALT’H SURVEY CHEST X-RAY INTERPRETATION4-61
X*RAYNUMBER READER DATE CHECKHEREIFFILMISUNSATI$FACTORY❑
Pu~@GYNONE EXISTENCEOF LESION(Check one) IF LESION EXISTS, STATE MOST LIKELY ETIOLOGY
c1 ❑ Definitec1
Indefinite
IOVASCNONE [ HEART ENLARGEMENT(Check anej OTHER CVD (Check one)
c1 10Definiten
Borderline10
Defiiitec1
Bosdetliae
IF OTHER CVD,PLEASESPECIFY
PLEASESPECIFYBELOWANY OTHERSIGNIFICANTPA,TliOLfflY
Instructions for interpreting cardiovascular pathology
Heart enlargement: Borderline enlargement is defined as 10 to 20 percent largerthan normal. If enlargement was not generalized specify the hypertrophied chamber.
Other cardiovascular pathology is to be specified as follows: Calcification of theascending aorta, calcification uf the aortic knob, calcification of other portions ofthe aorta, abnormality of shape of aorta (specify), increased pulmonary vascularity,
33
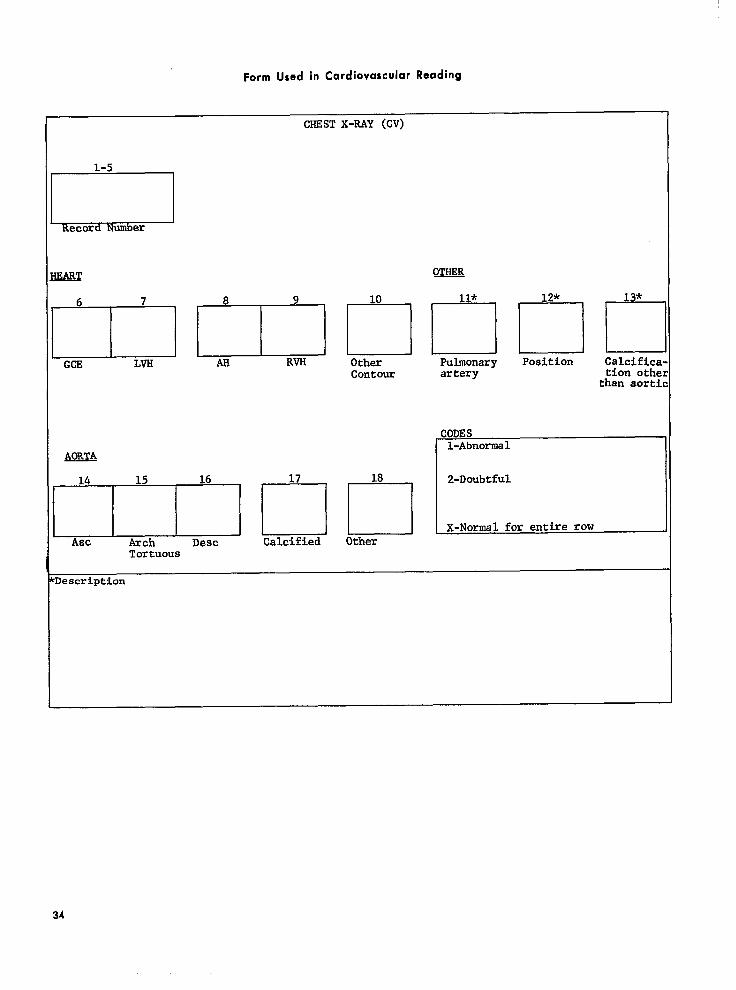
Form Used in Cardiovascular Reading
CHESTX-RAY (CV)
1-5
Record Number
us
6 7
I
GCE LVH
AORTA
14
Asc
EAH RVH
10
OtherContour
15,16,,17,1181
Arch Desc Calcified OtherTortuous
11*
ElPulmonaryartery
IlrPosition Calci.fic~
tion oth~than sort:
20DESl-Abnormal
2-Doubtful
X-Normal for entirerow
Ieacription
34
Pulmonory Readers
Initially, the X-ray films were interpreted bythree radiologists with a special interest in pulmonarydisease. While their primary concern was with evidenceof pulmonary pathology, abnormalities of the heart orvessels were also noted. So far as the diagnosis ofheart disease was concerned, the two findings of specialconcern were those of generalized cardiac enlargement(GCE) and those of chamber enlargement, especiallyleft ventricular hypertrophy (LVH). Borderline GCEwas defined as present if the heart was 10 to 20 percentlarger than normal larger hearts were considered tohave definite GCE. No criteria were given for LVH.
In the following discussion a reading is consideredpositive if a finding of GCE or LVH, definite or border-line, was made. In order to determine how frequentlya film with evidence of GCE was missed by thepulmonary readers, a series of 190 films were measuredby the method of Hilbish and Morgan, 9 and the heartsize as measured was compared with the findings ofthe pulmonary readers.
Heart size(in percentof normal)
Total ------
~~o;05--------------
11o:114--------115-119--------120+-----------Could notmeasure -------
lumber Reader Reader Readerof“ilms 1 2 3
Number of positivereadinga
190 56 42 22
134 17 10 120 10 9 39
; : ;1: 13 13 11
7 5 2 4
There were 29 films found to belOpercent or moreenlarged on measurement. Reader 1 read 24 of theseas positive, reader 2read21 appositive, and reader 3read 14 as positive. The findings of readers land2were consistent with the criteria for GCE. Reader 3seemed to be following a different rule, generallyrecording enlargement whenitwas20percent orgreaterbut seldom if it was 10-19 percent. The positivefindings reported for the smaller hearts arenot incon-sistent with therules, since the films mayhsve exhibitedabnormalities of shape indicative of cardiac hyper-trophy,
Next, it was determined in what way, if any, thecardiovascular readings of the pulmonary readersdiffered from readings by radiologists who specializein cardiovascular reading. To answer this it wasnecessary to obtain a set of cardiovascular readingstandards, or, in more concrete terms, to have a setof films read by a standard radiologist. Dr. Lloyd E.
Hawes, radiologist forthe Framingbsm Heart Program,was chosen. In other words, Framingham practice inX-ray reading was the stsndard chosen.
11.r.Haweswasgiven asetof192Survey films wbichhad been selected toinclude abighproportion ofposi-tives. He found 96 of these “positive”; the number ofpositive readings by the three pulmonary readers were56, 42, and 22, respectively. Thus, even the two highestcounts were substantially below the level of readingsby Dr. Hawes.
Cardiovascular Readers
It was evident that to make the cardiovascularfindings of the Survey comparable with those of theFramingham Heart Program another group of readerswould have to be used to read the X-ray films forcardiovascular abnormalities. It was felt that trainingradiologists to conform to standards was beyond theresources of the Survey, it was decided, instead, tochoose radiologists who conformed naturally and with-out instruction to Dr. Hawes’ standards.
A series of radiologists were asked to read thestandard set of films. The four who conformed mostclosely to Dr. Hawes’ readings compared with himas follows:
Reading by
Hawes I Other reader
Total -----------------
Armeement
positive positivenegative negative
DLs.agreement
positive negativenegative positive
Reader
Number off ihs
192_
:;
2316
183_
1%
376
In terms of reading levels the four readers readthe following percentage of films as positive.
Dr. Hades ----------------- 50.0Reader A ------------------ 52.4Reader B ------------------ 64.6Reader C------------------ 46.4Reader D------------------ 32.8
(Although itlater tumedout thatreader Dcouldnotparticipate in the cardiovascular readings, his readingson the standard films are included in some of the sub-sequent analysis. )
35
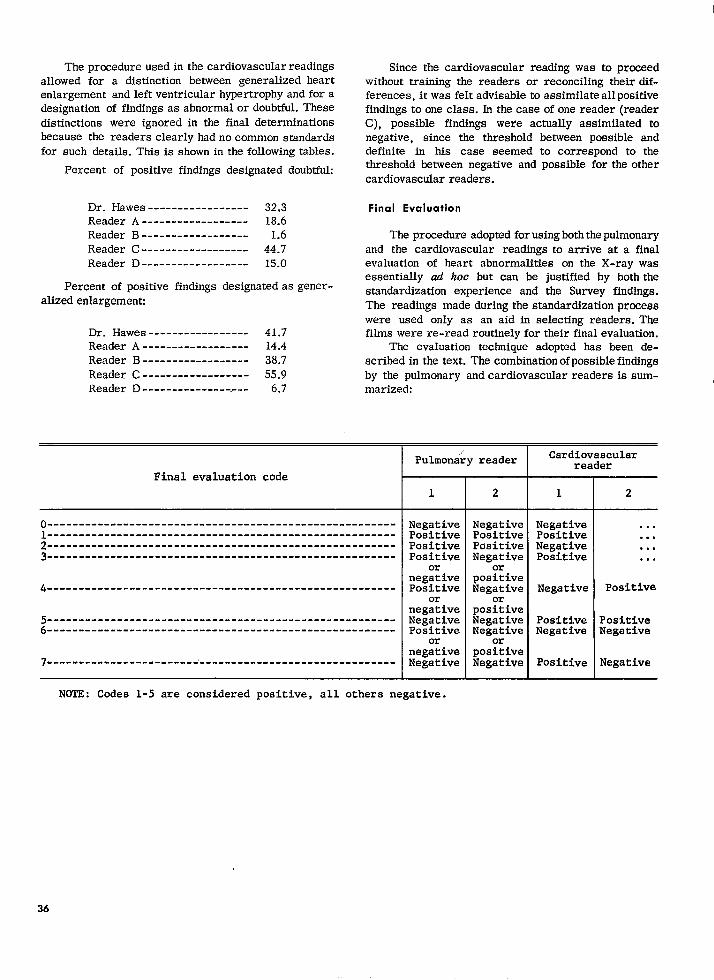
The prccedure used in the cardiovascular readingsallowed for a distinction between generalized heartenlargement and left ventricular hypertrophy and for adesignation of findings as abnormal or doubtful. These
distinctions were ignored in the final determinationsbecause the readers clearly had no common standardsfor such details. This is shown in the following tables.
Percent of positive findings designated doubtful:
Dr. Hades ----------------- 32.3Reader A------------------ 18.6Reader B------------------ 1.6Reader C------------------ 44.7Reader D------------------ 15.0
Percent of positive findings designated asgener-alizedenlargemenh
Dr. Hades ----------------- 41.7Reader A------------------ 14.4Reader B------------------ 38.7Reader C------------------ 55.9Reader D------------------- 6.7
Since the cardiovascular reading was to prmeedwithout training the readers or reconciling their dif-ferences, itwasfelt advisable toassimilate allpositivefindings to one class. Inthe case of onereader (readerC), possible findings were actually assimilated tonegative, since the threshold between possible anddefinite in his case seemed to correspond to thethreshold ktween negative and possible for the othercardiovascular readers.
Final Evaluation
The procedure adopted forusingboththe pulmonaryand the cardiovascular readings to arrive at a finalevaluation of heart abnormalities on the X-ray wasessentially ad hoc but can be justified by both thestandardization experience and the Survey findings.The readings made during the standardization processwere used only as an aid in selecting readers. Thefilms were re-read routinely fortheir final evaluation.
The evaluation technique adopted has been de-scribed in the text. The combinationofpossiblefindingsby the pulmonary andcardiovascular readers is sum-marized:
Final evaluation code
o-------- ------------- ---------- ------------------ -------------- ------------ --------------------------- --------
; --------- --------- --------------------------- --------- -3-------- -------- -------- -------- -------- -------- -------
4 -------- -------- --.----- -------- ---------------- .------
-------- -------- -------- -------- .------- -------- --..---:-------------------------------------------------------
7--------- . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . ------------
Pulmonary reader I Cardiovascularreader
1
NegativePositivePositivePositive
ornegativePositive
ornegativeNegativePositive
ornegativeNegative
2 I 1
Negative NegativePositive PositivePositive NegativeNegative Positive
poa~iveNegative Negative
pos~iveNegative PositiveNegative Negative
orpositive
2
,... . .. . .. . .
Positive
PositiveNegative
Negative
NOTE: Codes 1-5 are considered positive, all othera negative.
36
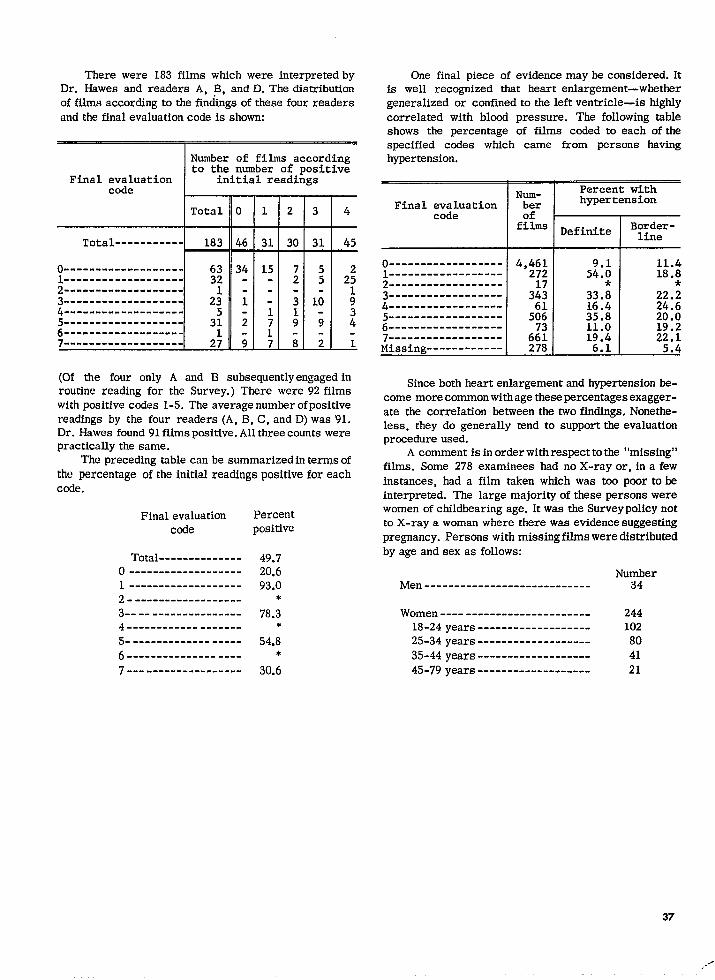
There were 183 films which were interpreted byDr. Hawes and readers A, B, and D. The distributionof films according to the fin&ngs of these four readersand the final evaluation code is shown:
Number of films accordingto the number of positive
Final evaluation initial readingscode
t-Total
Total ----------- 183
0 . . . . . . . ----------- . 63-------- -------- ---
L------------------32
-------- -------- --- 2;;-------------------
-------- -------- --- 3::-------------------7-----.--- --------- - 2;
—
o—
46—
34
i
;
i.
(Of the four only A and B subsequentlyengagedinroutine reading for the Survey.) There were 92filmswith positive codes 1-5. The average number of positivereadings by the four readers (A, B, C,and D)was 91.Dr. Hawesfound 91filmspositive.Allthreecounts werepractically the same.
The preceding table can be summarized intermsofthe percentage of theinitial readings positive for eachcode.
Final evaluation Percent
code positive
Total -------------- 49.70 ------------------- 20.61 ------------------- 93.02 . -------- -------- -- *
3-- -- --------------- 78.34 -------- ---- ------- *
5------------------- 54.86 --------------- ---- *
7 ..- -------- -------- 30.6
One final piece of evidence maybe considered. Itis well recognized that heart enlargement-whethergeneralized or confined totheleft ventricle-is highlycorrelated with blood pressure. The following tableshows the percentage of films coded to each of thespecified ccxles which came from persons havinghypertension.
Num-Percent with
Final evaluation ber hypertension
code
‘:La-
0------- --.---- ----1--.----- -------- --
-------- ----------L-----------------4 -------- ----------
-.------ -------- --2------------------7-------- -------- --Miasing ------------
33.816.435.811.019.4
6.1
11.418.8
22.;24.620.019.222.1
5.4
Since both heart enlargement and hypertension be-come morecommon withage these percentages exagger-ate the correlation between the two findings. Nonethe-less, they do generally tend to support the evaluationprocedure used.
A comment is in order with respect to the “missing”films. Some 278 examinees had no X-ray or, in a fewinstances, had a film taken wbfch was too poor to beinterpreted. The large majority of these persons werewomen of childbearing age. It was the Survey policy notto X-ray a woman where there was evidence suggestingpregnancy. Persons with missing films were distributedby age and sex as follows:
NumberMen ---------------------------- 34
Women ------------------------- 24418-24 years ------------------- 10225-34 years ------------------- 80
35-44 years ------------------- 4145-79 years ------------------- 21
37
..6

The missing films were treated as negative in this re-port. Judging from the small number of persons withmissing X-rays who had hypertension (15 definite,17 borderline) this decision seems reasonable. It isunlikely that treating the missing X-rays as negativeresulted in an appreciable understatement of heartdisease prevalence. Some of these persons were diag-nosed as having heart disease even without the evidenceof the X-ray, but even if this were not the case therewould seem to be no alternative to the procedure chosen.
Finally, some note should be made of the unusualnature of the X-ray evaluation procedure. The use ofa screening prccedure which picks up all suspiciousfindings initially and then, at a second stage of evaluation,applies more stringent rules to the cases selected isnot uncommon. The Survey procedure was the reverse.The initial (pulmonary) screening was the more con-servative, the final (cardiovascular) reading the lessconservative. Actually the contrast between the tworeadings is greater than appears from the standard
films. Since these films included an unusually largeproportion of very large hearts, there would be moreagreement on them than on a purely random sample ofthe population. The contrast for the Survey films as awhole was much greater, the cardiovascular readersfinding 27.9 percent positive on their initial reading, thepulmonary 8.2 percent.
Why, then, were the pulmonary readings used?There were three reasons. First, they were alreadylargely available at the time the cardiovascular stand-ards were finally chosen. Second, the y were relevan~clearly heart enlargement found on the pulmonaryreadings was meaningful in terms of the cardiovascularstandards. Third, it was possible by using them todevise a more economical and secure cardiovascularreading system than would otherwise have been possi-ble. While it is not suggested that the procedure usedwas the optimum one, it seems to have worked quitesatisfactorily.
ooo —
38
APPENDIX V.
DIAGNOSTIC REVIEW
The prxedure used in case review has beendescribed in the text. Briefly, every case was firstdiagnosed by the computer. The key information wasthen printed out and this machine record served as aconvenient summary of the case record, as well as aplace for entering decisions made in a subsequent re-view, if there were such a review.
There were two important points at which the phy-sician’s judgment was seldom modified by review.These were the diagnosis of angina pectoris and theevaluation of a murmur.” Findings of angina pectoriawere reviewed, chiefly to verify the coding of the phy-sician’s judgment. The description of a significantmurmur was reviewed to see if it was consistent withthe physician’s evaluation of it.
The question arises as to what was done when aphysician’s findings at these points appeared to divergefrom the usual. This became a serious question ontwo occasions.
At one stand both examining physicians reported anunusually large number of cases of angina pectoris.Since both physicians had conducted examinations atother stands and at these had found an average amountof angina pectoris, it was felt that their judgments hadto be accepted where they found an unusual amount.Their descriptions of angina pectoris were reviewedand where the wording indicated less certainty thanappeared in the coded diagnosis, the coding was alteredto conform. It is likely that the review of cases fromthis stand was more critical than usual, but in principleit was the same as the review of similar cases fromother stands. Having admitted most of the cases fromthis stand, it is nonetheless suspected that the chestpain described for these cases was frequently notdue to coronary heart disease but arose from someother cause.
The other set of unusual findings was a largenumber of murmurs considered diagnostic of rheumaticheart disease that was reported by one examining phy-sician. On the average, slightly less than two cases ofrheumatic heart disease were reported by other phy-sicians for each 160 persons examined. This physician
reported 19. Since he examined persons at two standaand since the other examining physician at each ofthese stands (a different one at each) reported only theusual number of cases of rheumatic heart disease, theprevalence of rheumatic heart disease among MS ex-aminees could hardly be attributed to the populationsexamined. Three choices seemed open. (1) To selecta subsample of the rheumatic heart disease cases re-ported by this physician, controlling to the usualprevalence reported in the Survey. (2) To ignore thepopulation examined by this physician for the purposeof computing rheumatic heart disease prevalence. (3)To accept the cases as reported. Of the three alterna-tives the first appeared the best and the third theworst. In effect, a random selection of cases wasmade by controlling to the usual prevalence, with aprobability of selection by age and sex proportional tothe distribution of rheumatic heart disease by age andsex as reported by the other examining physicians.This obviously was a choice among evils.
The review procedure was altered and becamemore efficient as staff experience accumulated. In thelast seven standa reviewed, there were 1,116 cases.Of these 181 were reviewed. In 23 cases a change wasmade in the computer diagnosis as a result of thereview.
One set of review cases warranta special notice.These are the cases in which the impression of theexamining physician was that heart disease was pres-ent but the computer did not diagnose heart disease.ht the review of cases from the last seven stands 36 ofthe 181 cases reviewed fell in this category. Inspectionof the case records revealed that the physician arrivedat his diagnostic impression in one of two ways. Eitherhe interpreted the electrocardiogram as abnormal whenthe Survey readers did not, or he placed more diagnosticweight on findings from the physical examination, suchas significant systolic murmurs, than the Survey cri-teria allowed.
It would he misleading, however, to emphasizethe diagnostic “misses” by the examining physicianand ignore the “hits.” In fact,’80 percent of all cases
39
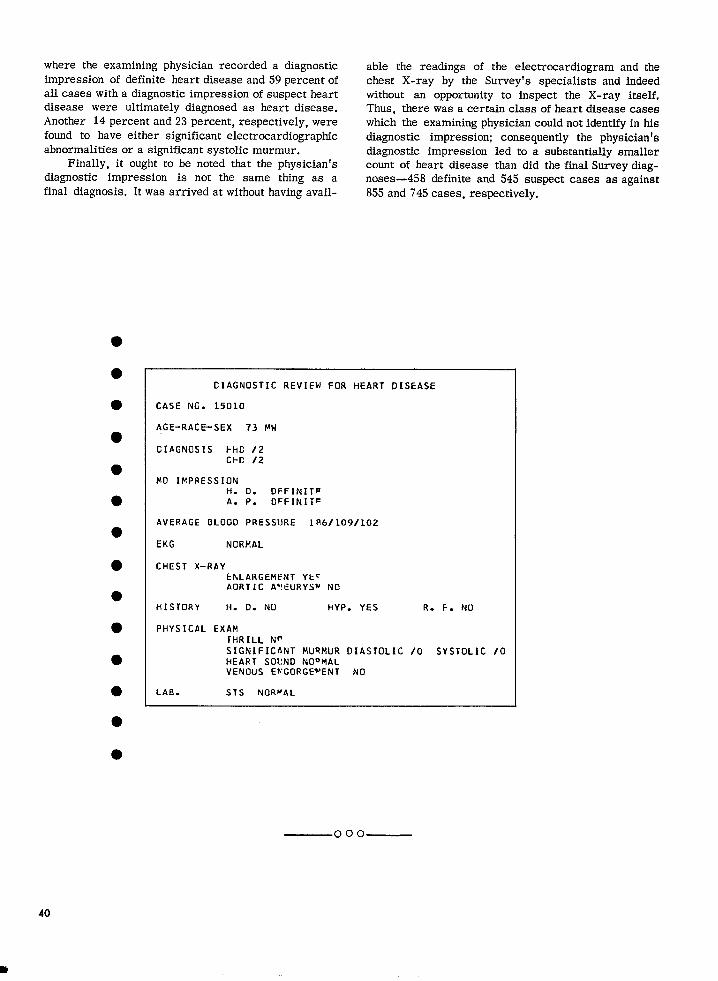
where the examining physician recorded a diagnosticimpression of definite heart disease and 59 percent ofall cases with a diagnostic impression of suspect heartdisease were ultimately diagnosed as heart disease.Another 14 percent and23percent, respectively, werefound to have either significant electrocardiographicabnormalities or a significant systolic murmur.
Finally, it ought to be noted that the physician’sdiagnostic impression is not the same thing as afinal diagnosis. Itwasarrived atwithout having avail-
able the readings of the electrmardiogram and thechest X-ray by the Survey’s specialists and indeedwithout an opportunity to inspect the X-ray itself.Thus, there wasacertain class ofheart disease caseswhich the examining physician could not identify in hisdiagnostic impression; consequently the physician’sdiagnostic impression led to a substantially smallercount of heart disease than did the final Survey diag-noses—458 definite and 545 suspect cases as against855 and 745 cases, respectively.
CIAGNOSTIC REVIEW FOR HEART DISEASE
CASE NG. 15010
AGE-RACE-SEX 73 NW
131hGNOSIS t-hC /2C1-’c /2
$!0 IMPRESSIONH. D. OFFINIT~A. P. OFFINITE
AVERAGE BLOGO PRESSIJRE lR6/109/102
EKG NORMAL
CHEST X-RAYENLARGEMENT Yt~AORTIC A*IEURYSW NO
HISTORY H. O. NU HYP. YES R. F. NO
PHYSICAL EXAMJHRILL N~SIGNIFICflNT MURMUR OIASTOLIC /0 SYSTOLIC /0HEART SOVNO NOOMALVENOUS E~GORGE~ENT NO
LAB. STS NOR~AL
ooo—
40
m
APPENDIX W.
STATISTICAL NOTES
The Survey Design
The Health Examination Survey is designed as ahighly stratified multistage sampling of the civilian,noninstitutional population, aged 18-79 years, of theconterminous United States. The first stage of the planis a sample of the 42 primary sampling units (PSLPS)from 1,900 geographic units into which the UnitedStates has been divided. A PSU is a county, two orthree contiguous counties, or a standard metropolitanstatistical area. Later stages result in the randomselection of clusters of about four persons from asmall neighborhood within the PSU. The total sampleincluded 7,710 persons in the 42 PSU’S in 29 differentStates. The detailed structure of tbe design and theconduct of the Survey have been described in previousreports. 1. 2
Reliability in Probability Surveys
The methodological strength of the Survey derivesespecially from its use of scientific probability samplingtechniques and of highly standardized and closely con-trolled measurement prccesses. This does not implythat statistics from the Survey are exact or withouterror, Data presented are imperfect for three im-
portant reasons: (1) results are subject to samplingerror, (2) the actual conduct of a survey never agreesperfectly with the design, and (3) the measurementprocess itself is inexact, even when standardized andcontrolled. The faithfulness with which the study designwas carried out has been analyzed in a previous report. 2
Of the total of 7,710 sample persons, 86 percent or6,672 were examined. Analysis indicates that the ex-
amined persons are a highly representative sample of
the adult civilian, noninstitutional population of theUnited States. Imputation for the nonrespondents wasaccomplished by attributing to nonexamined personsthe characteristics of comparable examined persons.The specific procedure used 2 consisted of inflatingthe sampling weight for each examined person to com-pensate for nonexamined sample persons at the samestand and of the same age-sex group.
While it is impossible to be certain that the preva-lence of heart disease was the same in the examined andthe nonexamined groups, the available evidence indi-cates that it was. One source of information on thisquestion is a special inquiry sent to the physicians ofnonexamined persons and to the physicians of a match-ing set of examined persons. The heart disease preva-lence reported for the examined and for the nonex-amined groups was in close agreement. For furtherdetails on this subject see Vital and Health Statistics,Series 11. No. 1.
Sampling , and Measurement Error
In this report and its appendices, several refer-ences have been made to efforts to evaluate both biasand variability of the measurement techniques. Theprobability design of the Survey makes possible the
calculation of sampling errors, Traditionally the roleof the sampling error has been the determination ofhow imprecise the survey results may be because theycome from a sample rather than from measurement ofall elements in the universe.
The task of presenting sampling errors for a studyof the type of the Health Examination Survey is compli-
cated by at least three factors, (1) Measurement error
and “pure” sampling error are confounded in the data;
41
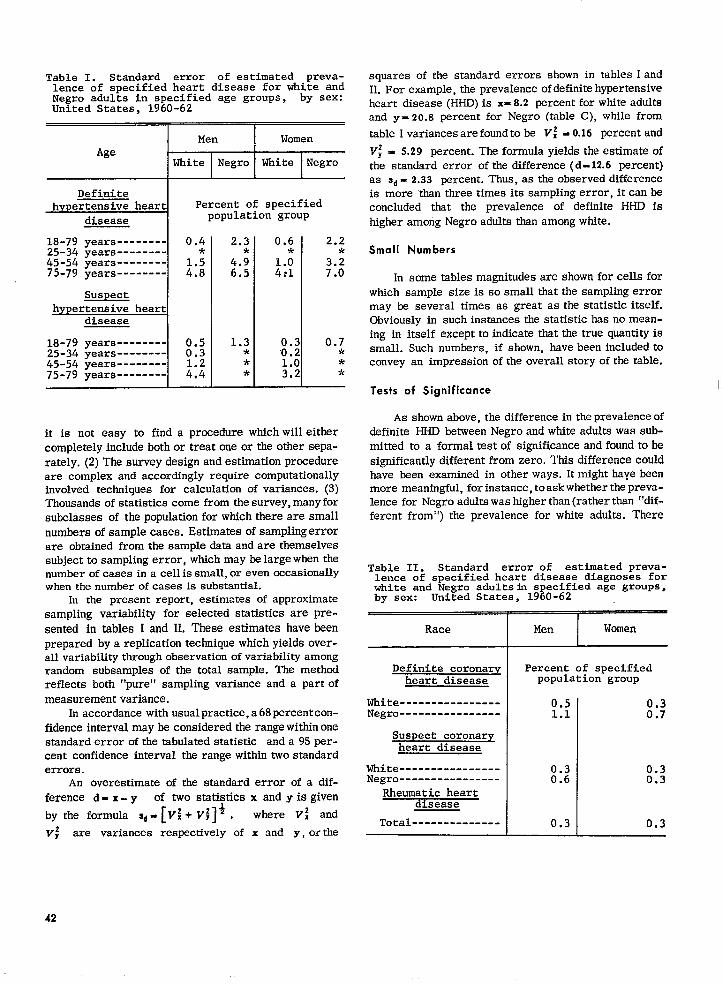
Table 1. Standard error of estimated preva-lence of specified heart disease for white andNegro adults in specified age groups, by sex:United States, 1960-62
~
* ‘opulatiOngroupPercent of specified
1S-79 years -------- 0.425-34 years -------- *45-54 years --------75-79 years -------- M
Suspecthypertensive heart
disease
18-79 years -------- 0.525-34 years -------- 0.345-54 years --------75-79 years -------- M 1
2.3 0.6*
4.;6.5 :;:
1.3 0.3* 0.2* 1.0* 3.2
2.2*
;::
0.7***
it is not easy to find a procedure whichwill eithercompletely include both or treat one or the other sepa-
rately. (2) The survey design and estimation procedureare complex and accordingly require computationallyinvolved techniques for calculation of variances. (3)Thousands of statistics come from thesurvey, manyforsubclasses of the population for which there are smallnumbers of sample cases. Estimates of samplingerrorare obtained from the sample data and are themselvessubject to sampling error, which may belargewhen thenumber of cases in a cell is small, or even occasionallywhen the number of cases is substantial.
In the present report, estimates of approximatesampling variability for selected statistics are pre-
sented in tables I and II. These estimates have beenprepared by a replication technique which yields over-all variability through observation of variability amongrandom subsamples of the total sample. The methodreflects both “pure” sampling variance and a part of
measurement variance.In accordance with usualpractice,a 68percentcon-
fidence interval maybe considered the range witbin onestandard error of the tabulated statistic anda 95per-cent confidence interval the range within two standarderrors.
An overestimate of the standard error of a dif-
ference d- x- y of two statistics x and yis given
by the formula s,= [vi+ vj]* , where Vi and
v; are variances respectively of x md y, or the
squares of the standard errors shown in tables IandH. For example, the prevalence of definite hypertensiveheart disease (HHD) is x=8.2 percent for white adultsand y=20.8 percent for Negro (table C), while from
table I variances are found to be V: = 0.16 percent and
V; = 5.29 percent. The formula yields the estimate ofthe standard error of the difference (d-12.6 percent)as Sd= 2.33 percent. Thus, as the observed differenceis more ‘than three times its sampling error, itcanbeconcluded that the prevalence of definite HHD ishigher among Negro adults than among white.
Small Numbers
h some tables magnitudes are shown for cells forwhich sample size is so small that the sampling errormay he several times as great as the etatistic itself.Obviously in such instances the statistic has no mean-ing in itself except to indicate that the true quantity issmall. Such numbers, if shown, have been includedtoconvey an impression of the overall story of the table.
Tests of Significance
As shown above, the difference in the prevalence ofdefinite HHD between Negro andwhite adults was sub-mitted to a formal testof significance and found tobesignificantly different from zero, This difference couldhave been examined in other ways. It might haye beenmore meaningful, for instance, to ask whether the preva-lence for Negro adults was higher than (rather than “dif-ferent from”) the prevalence for white adults. There
Table 11. Standard error of estimated preva-lence of specified heart disease diagnoses forwhite and Negro adultsfn specified age groups,by sex: united states, 1960-62 .
Race Men Women
Definite coronary Percent of specifiedheart disease population group
White ----------------Negro ----------------
0.51.1
0.30.7
Suspect coronaryheart disease
White ---------------- :.; 0.3Negro ---------------- . 0.3
Rheumatic heartdmease
Total -------------- 0.3 0.3
42
is much evidence indicating this, and the test foraone-sided hypothesis is more powerful than the testfor a two-sided hypothesis. Alternatively, the questionmight have been, “Is the prevalence higher for Negroadults than for white adults if age is held constant?”Conceivably, the age-sex-specific means could beidentical for the two groups but a larger proportion ofolder people in one group could lead to an overallhigher prevalence for that group.
This last version of the hypothesis can be testeddirectly from table 3, with the use of a table for thebinomial variable. The prevalence of definite HHD ishigher for Negro adults in every age-sex group. The
chances of 14 heads out of 14 tosses of a true coin are0.00006.
Demographic Terms”
Age.—The age recorded for each person is theage a~ast birthday.
Race .—Race is recorded as “White,” “Negro,”or “Other. “ “Other” includes American Indian, Chinese,Japanese, and so forth. Mexican persons are includedwith “White” unless definitely known to be Indian orother nonwhite race.
ooo —
*U.S. GOVERNMENT PRINTING OFFICE: 1976—210.981:40
43
VITAL AND HEALTH STATISTICS PUBLICATION SERIES
Formerly Public Health Service Publication No. 1000
Series 1.
Swies 2.
Series 3.
Swies 4.
Swies IO.
Series 11.
Swies 12.
Swies 13.
Swies 14.
Swies 20.
Swies 21.
Swies 22,
Programs and collection procedures. — Reports which describe the general programs of the National
Center for Health Statistics and its offices and divisions, data collection methods used, definitions,and other material necessary for understanding the data.
~ta evohmtion and methods research. — Studies of new statistical methodology including: experi-
mental tests of new survey methods, studies of vital statistics collection methods, new analyticaltechniques, objective evaluations of reliability of collected data, contributions to statistical theory.
Analytical studies .—Reports presenting analytical or interpretive studies based on vital and health
ststisttcs, carrying the analysis further than the expository types of reports in the other series.
Documents and committee vepovts. — Final reports of major committees concerned with vital and
health statistics, and documents such as recommended model vital registration laws and revisedbirth and death certificates:
Do to from the Health Interview Swve v. —Statistics on illness, accidental injuries, disability, useof hospital, medical, dental, and other services, and other health-related topics, based on data
collected in a continuing national household interview survey.
Data from the Health Examination Survey. —Data from direct examination, testing, and measure-
ment of national samples of the civilian, noninstitutional population provide the basis for two types
of reports: (1) estimates of the medically defined prevalence of specific diseases in the UnitedStates and the distributions of the popularion with respect to physical, physiological, and psycho-
logical characteristics; and (2) analysis of relationships among the various measurements withoutreference to an explicit finite universe of persons.
Data porn the Institutional Population Surveys — Statistics relating to the health characteristics ofpersons in institutions, and their medical, nursing, and personal care received, based on nationalsamples of establishments providing these services and samples of the residents or patients.
Data porn the Hospital Discharge Survey. —Statistics relating tc li~cl-?rged patients in short-stayhospitals, based on a sample of patient records in a national sample of hospitals.
Dab on health resources: manpower and facilities. —Statistics on the numbers, geographic distri-bution, and characteristics of health resources including physicians, dentists, nurses, other healthoccupations, hospitals, nursing homes, and outpatient facilities.
Data on mortality. — Various statistics on mortality other than as included in regular annual ormonthly reports— special analyses by cause of death, age, and other demographic variables, also
geographic and time series analyses.
Data on natulity, marriage, and divorce. —Various statistics on nataliry, marriage, and divorce
other than as included in regular annual or monthly reports-special analyses by demographicvariables, also geographic and time series analyses, studies of fertility.
Datu from the National Natality and Mortality SurL,eys. - Statistics on chai-acteristics of birthsand deaths not available from the vital records, based on sample surveys stemming from theserecords, including such topics as mortality by socioeconomic class, hospital experience in thelast year of life, medical care during pregnancy, health insurance coverage, etc.
For a list of titles of reports published in these series, write to: Scientific and Technical Information
Branch
National Center for Health Statistics
Public Health Service, HRA
Roekville, Md. 20852
U.S. DEPARTMENT OF
HEALTH, EDUCATION, AND WELFARE
Public Health Service
Health Resources Administration
5600 Fishers Lane
Rockville, Md. 20852
POSTAGE AN1) F’F.LSF’AII)U.S. DEPARTMENT OF IIEW
HEV/ 390
THIRD CLASS
BLK. RATE
E)*U. S.MAIL
OFFICIAL BUSINESSPenalty for Private Use, $300