Embed Size (px)
Citation preview

Visual Impairment Corrected Via Cataract Surgery and5-Year Survival in a Prospective Cohort
CALVIN SZE-UN FONG, PAUL MITCHELL, ELENA ROCHTCHINA, TANIA DE LORYN, AVA GRACE TAN, ANDJIE JIN WANG
� PURPOSE: To compare mortality risk between cataractsurgical patients with corrected and persistent visualimpairment.� DESIGN: Cohort study.� METHODS: A total of 1864 consecutive patients, aged‡64 years, undergoing phacoemulsification surgery atWestmead Hospital were followed annually for 5 yearspostoperatively. Visual impairment status in the surgicaleye was categorized as none (presenting visual acuity[VA], ‡20/40), mild (VA<20/40-20/60), or moderate-severe (VA <20/60). All-cause mortality was obtainedfrom the Australian National Death Index.� RESULTS: Of 901 patients with moderate-severe visualimpairment before surgery, 60.4% (n [ 544), 15.5%(n [ 140), and 24.1% (n [ 217) had no, mild, ormoderate-severe visual impairment in the surgical eye,respectively, 1 month postoperatively. Age-standardized5-year mortality rates were nonsignificantly lower inpatients with either mild (24.7%, 95% confidenceinterval [CI] 16.5%-32.9%) or no visual impairment(24.1%, 95% CI 19.9%-28.4%) post surgery comparedto that in patients whose moderate-severe visual impair-ment persisted (30.6%, 95% CI 23.3%-37.9%). Afteradjusting for age, sex, smoking, body mass index, andindividual comorbid conditions, such as hypertension,diabetes, angina, myocardial infarction, stroke, transientischemic attack, and kidney disease, patients with novisual impairment 1 month postoperatively had a lowermortality risk (HR 0.73, 95% CI 0.52-1.01) comparedto those with persistent moderate-severe visual impair-ment after surgery. This finding was significant (HR0.71, 95% CI 0.51-0.99) after additional adjustmentfor number of medications taken (continuous variable)and number (‡3 vs <3) of comorbid conditions.� CONCLUSION: Correcting moderate-severe visualimpairment in older patients with phacoemulsification
See accompanying Editorial on page 7.Accepted for publication Aug 21, 2013.
From the Centre for Vision Research, Department of Ophthalmologyand Westmead Millennium Institute, University of Sydney, Sydney,Australia (C.S.F., P.M., E.R., T.d.L., A.G.T., J.J.W.); and Centre forEye Research Australia, Department of Ophthalmology, University ofMelbourne, Melbourne, Australia (J.J.W.).
Inquiries to Professor Jie Jin Wang, Centre for Vision Research,Department of Ophthalmology, University of Sydney, WestmeadHospital, Hawkesbury Road, Westmead, NSW 2145, Australia; e-mail:[email protected]
0002-9394/$36.00http://dx.doi.org/10.1016/j.ajo.2013.08.018
� 2014 BY ELSEVIER INC.
surgery was associated with a lower mortality risk,compared to surgical patients whose visual impairmentpersisted postoperatively. (Am J Ophthalmol2014;157:163–170. � 2014 by Elsevier Inc. All rightsreserved.)
PREVIOUSSTUDIESHAVEREPORTEDTHATOBJECTIVELY
measured visual impairment (visual acuity [VA]<_20/40) was associated with a 20%-90% increased
mortality risk.1–4 The Salisbury Eye Evaluation (SEE)project reported a 53% reduction in 6-year mortality riskin participants who had a gain of >_2 lines in binocularpresenting VA 2 years after baseline examinationscompared to those whose presenting VA was unchanged,after multivariable adjustment.5 Approximately half ofthose with a presenting VA gain had undergone cataractsurgery during the follow-up period while the rest werelikely to have had refractive correction.5
The BlueMountains Eye Study (BMES) found that older(>_49 years) persons with cataract-related visual impair-ment corrected by cataract surgery had a 40% reductionin 15-year mortality risk after multivariable adjustment,compared to those who remained visually impaired becauseof cataract and did not have surgery.6 We aimed, using anindependent, older cataract surgical cohort, to assessa similar question to the BMES report,6 that correctingmoderate-severe visual impairment using phacoemulsifica-tion surgery is associated with better survival among olderpeople with visual impairment attributable to cataract,compared to that in patients who remained visuallyimpaired after their cataract surgery.
METHODS
THE AUSTRALIAN PROSPECTIVE CATARACT SURGERY AND
Age-related Macular Degeneration study is a prospectivecohort study of patients, aged >_64 years, recruited for cata-ract surgery at Westmead Hospital, Western Sydney,Australia. Westmead Hospital is a major public, tertiaryhospital that provides public services to the WesternSydney region. All patients provided written informedconsent. The study adhered to the tenets of the Declarationof Helsinki and was approved by the Human ResearchEthics Committees of the University of Sydney, the Sydney
163ALL RIGHTS RESERVED.

West Area Health Service, and the Australian Institute ofHealth and Welfare. Details of the Australian ProspectiveCataract Surgery and Age-related Macular Degenerationstudy are described elsewhere.7,8
� PARTICIPANTS: During 2004-2007, 1864 consecutivepatients had phacoemulsification surgery at WestmeadHospital. They were recruited into the study either preop-eratively or shortly after surgery. The eye that was to beoperated on during the study recruitment period wasdefined as the surgical eye of the patient. The better eyewas defined as either the surgical eye, if fellow eye datawere not available, or the better of the 2 eyes, irrespectiveof surgical eye status, with regard to presenting VA levels.Study participants had VA assessment (with and withoutpinhole) and retinal photography at preoperative and 1-,6-, and 12-month postoperative visits.
� MEASUREMENTSANDDEFINITIONS: In brief, presentingVA in both eyes was assessed using a retroilluminated loga-rithm of the minimal angle of resolution (logMAR) chartread at 2.4 m with current distance glasses, if worn. Present-ing VA was defined as the number of letters read correctlyfrom zero to 70 and converted to a Snellen fraction.Presenting visual impairment was defined using eitherthe surgical eye or the better of the 2 eyes andcategorized as none (presenting VA >_20/40), mild(presenting VA <20/40-20/60), or moderate-severe(presenting VA <20/60). For eyes reading fewer than54 letters (<20/40) using current distance correction, VAwas further assessed with a pinhole aperture. Under-corrected VA was defined as presenting VA that wascorrected with a pinhole aperture by >_3 lines. Pseudo-phakic status was confirmed from photographs of the ante-rior segment of the eye, taken using a Canon CF-60DSidigital fundus camera (Canon Inc, Tokyo, Japan). Retinalphotographs, obtained with the digital camera, wereassessed by a trained grader for the diagnosis of retinalconditions that could have contributed to poor vision post-operatively. Adjudication of the photographs was obtainedby a senior researcher (J.J.W.) and a retinal specialist(P.M.). The International Classification and GradingSystem for Age-related Maculopathy and Age-relatedMacular Degeneration9,10 and the modified EarlyTreatment Diabetic Retinopathy Study classificationsystem11 were closely followed for the diagnosis of these2 conditions.
Demographic and anthropomorphic data were collectedat baseline visits. Regular medications and history of eyedisease and comorbid conditions, including hypertension,diabetes mellitus, angina, myocardial infarction, transientischemic attack, stroke, and kidney disease, were recordedduring interview and confirmed from hospital patientmedical records. Categorized number of comorbid condi-tions (>_3 vs <3) included any of the following medicalconditions: hypertension, diabetes mellitus, angina,
164 AMERICAN JOURNAL OF
myocardial infarction, transient ischemic attack, stroke,and kidney disease. Body mass index (BMI) at baselinewas calculated as weight in kilograms divided by the squareof height in meters, with BMI less than 20 kg/m2 defined aslow. Current smokers included persons who had stoppedsmoking within the past year.The main outcome was death since the preoperative or
1-month-postoperative examinations (if preoperativedata were not available), up to October 13, 2011 (meanfollow-up period 5.7 years, range 4-8 years), informationthat was obtained via data linkage to the AustralianNational Death Index (NDI) dataset. A probabilisticrecord linkage package was used to cross-match the 2 data-sets, based on characteristics that included given andfamily names, sex, date of birth, and the name of the suburbof residence. Causes of death were provided by the NDI,which records causes documented on death certificates,based on the International Classification of Diseases, NinthRevision,12 and the International Statistical Classificationof Diseases, Tenth Revision.13 Australian NDI data havebeen validated previously, with an estimated sensitivityof 93.7%-95.0% and specificity of 100% for all-causedeaths.14,15 Seven patients identified as having nonexactmatching could not be ascertained from either theirmedical records or family members, and thus wereexcluded, leaving 1857 patients for study analyses.
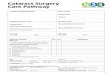
� STATISTICAL ANALYSIS: After excluding 839 partici-pants (45.2% of 1857) with preoperative presenting VA>_20/60 and 117 (6.3% of 1857) with VA data missingat either the preoperative or 1-month-postoperative visits,901 participants with preoperative presenting VA <20/60were included in the primary analysis of this report, for theassociation between visual impairment correction andimproved survival among cataract surgical patients(Figure, left panel). Presenting VA, or VA using the partic-ipants’ current distance correction, was used in all analysesas this represents the daily vision that these persons used intheir everyday activities.Statistical software (SAS version 9.2; SAS, Cary,
North Carolina, USA) was used to perform survival anal-yses. Five-year mortality rates by visual impairment statusat 1-month-postoperative visits, defined using the surgicaleye, were calculated after direct age standardization to theAustralian Prospective Cataract Surgery and Age-relatedMacular Degeneration study population (n ¼ 1857).These primary analyses were performed to assess the
association between visual impairment correction via cata-ract surgery and 5-year survival. Mortality risk was assessedand compared between patients with mild or no visualimpairment in the surgical eye 1 month postoperativelyand those remaining with moderate-severe visual impair-ment in the operated eye at the same visit, using Coxproportional hazard regression models. Patients in thesevisual impairment groups were censored to either thecensus date (October 13, 2011) or date of death. Three
JANUARY 2014OPHTHALMOLOGY

FIGURE. Patient selection for mortality analysis in patients with phacoemulsification surgery and postoperative visual acuity data inthe Australian Prospective Cataract Surgery and Age-related Macular Degeneration study. VA, visual acuity.
Cox regression models were used: Model 1 adjusted forbaseline age and sex; Model 2 additionally adjusted forsmoking status: current (including persons who had stoppedwithin the past year) vs past or never smokers, low BMI,and history of hypertension, diabetes, angina, myocardialinfarction, stroke (including transient ischemic attack),and kidney disease; Model 3 adjusted for all variablescontained in the second model plus indicators of poorgeneral health and frailty:16 the number of medicationstaken (as a continuous variable) and the number (>_3 vs<3) of comorbid conditions. Co-variables were checkedfor violation of the proportional hazard assumption usingSchoenfeld residuals. As age was found to violate thisassumption, we defined 3 age-group strata (64-69, 70-79,and 80þ years) in the Cox models. Mortality hazard ratios(HRs) are presented with 95% confidence intervals (CIs).
Supplementary analyses were performed comparingmortality risk between patients with no or mild visualimpairment after cataract surgery to those with persistingmoderate-severe visual impairment, defined using the betterof the 2 eyes, irrespective of whether the assessed eye wasthe surgical eye or not. Two different VA criteria wereused in the supplementary analyses; first, using VA thatwas measured 1 month postoperatively, and second, usingVA that was measured from the latest visit within the 12-month-postoperative period. These supplementary analysesaimed to assess the visual impairment–mortality associationin a larger sample of participants who had VA data out of
VOL. 157, NO. 1 IMPROVED VISION WITH CATARACT
the 1857 surgical patients, using the better of the 2 eyesregardless of whether it was the surgical eye or not. Analysesusing both 1-month- and cumulative 12-month-postopera-tive visual impairment status are to confirm the robustnessof the findings. Of the 1857 participants, 1785 (96.1%)had VA data for the better eye 1 month postoperativelyand 1801 (97.0%) had VA data from the latest visit withinthe 12-month follow-up period (Figure, right panel).
RESULTS
OF THE 901 PATIENTS WITH VA DATA IN THE SURGICAL
eye 1 month postoperatively, 60.4% (n ¼ 544), 15.5%(n¼ 140), and 24.1% (n¼ 217) had no visual impairment,mild visual impairment, and moderate-severe visualimpairment, respectively. Patients with no visual impair-ment were younger, had a higher proportion of women,and had a lower prevalence of diabetes than the groupwith moderate-severe visual impairment (Table 1). Therewere no other significant differences in the proportionswith chronic conditions, with >_3 comorbid conditions, ortaking >_6 medications (Table 1). Table 2 shows the knowncauses of visual impairment among the 217 cases withpersistent moderate-severe visual impairment shortly aftersurgery. Of the 901 surgical eyes, 64.9% (n ¼ 585) and33.5% (n ¼ 302) were the better and worse of the paired
165SURGERY AND BETTER SURVIVAL

TABLE 1. Baseline Characteristics of the Australian Prospective Cataract Surgery and Age-related Macular Degeneration StudyPatients, Based on Their Cataract Surgery and Visual Impairment Status at 1-Month-Postoperative Visits
Characteristics
Visual Impairment Status in Surgical Eye at the 1-Month-Postoperative Visit
Na
Presenting VA <20/60
N ¼ 217
Presenting VA <20/40 to >_20/60
N ¼ 140
Presenting VA >_20/40
N ¼ 544
n (%) n (%) P Valueb n (%) P Valuec
Age, mean (SD), y 901 76.1 (6.7) 75.2 (6.9) .21g 74.4 (5.8) .0001g
Female 901 111 (51.2) 72 (51.4) .87h 320 (58.8) .02h
Previous cataract surgery 901 53 (24.4) 38 (27.1) .56 150 (27.6) .38
Current smokerd 895 23 (10.7) 22 (15.8) .15 84 (15.6) .08
Body mass index <20 kg/m2 777 17 (9.1) 7 (6.3) .44 30 (6.3) .20
Hypertension 901 134 (61.8) 92 (65.7) .45 322 (59.2) .52
Diabetes mellitus 901 82 (37.8) 44 (31.4) .22 144 (26.5) .002
Cardiovascular diseasee 901 41 (18.9) 39 (27.9) .05 126 (23.2) .20
Strokef 901 36 (16.6) 19 (13.6) .44 65 (12.0) .09
Kidney disease 901 21 (9.7) 18 (12.9) .35 55 (10.1) .86
>_3 comorbid conditions 901 98 (45.2) 62 (44.3) .87 224 (41.2) .32
>_6 regular medications 901 71 (32.7) 53 (37.9) .32 172 (31.6) .77
VA ¼ visual acuity.aExcludes missing data.bAge-sex-adjusted P value for comparison between ‘‘VA <20/60’’ and ‘‘20/60<_ VA <20/40.’’cAge-sex-adjusted P value for comparison between ‘‘VA <20/60’’ and ‘‘VA >_20/40.’’dIncludes participants who gave up smoking less than a year prior to the baseline examinations.eIncludes either angina or myocardial infarction.fIncludes either stroke or transient ischemic attack.gSex-adjusted P value.hAge-adjusted P value.
eyes, respectively, and 1.6% (n ¼ 14) were the only eyewith data available.
By October 2011, 232 of the 901 patients (26%) haddied. The age-standardized mortality rates were marginallylower in patients with either no visual impairment (24.1%,95% CI 19.9%-28.4%) or mild visual impairment (24.7%,95%CI 16.5%-32.9%) at the 1-month-postoperative visits,compared to those with persistent moderate-severe visualimpairment (30.6%, 95% CI 23.3%-37.9%) after surgery.However, these differences were not significant (P ¼ .12and P ¼ .056, respectively). Of the 232 patients who haddied in the 5-year follow-up period, only 24% (n ¼ 55)had data on cause of death. In this small number of cases,there was a higher incidence of cardiovascular death inthe group with visual impairment remaining after surgery(69.6%, 16/23) compared to those with visual impairmentcorrected by cataract surgery (40.6%, 13/32; P ¼ .034).Age, low BMI, and history of angina, myocardial infarction,stroke, and kidney disease were significantly associated withincreasedmortality (P< .05) inModel 2, and the remainingco-variables were not significant in the model but wereforced into the model. After adjusting for all the variablesinModel 2 (age, sex, smoking, BMI, hypertension, diabetes,angina, myocardial infarction, transient ischemic attack,stroke, and kidney disease) and grouped indicators ofgeneral health and frailty (number of medications used
166 AMERICAN JOURNAL OF
and number of comorbid conditions), patients with novisual impairment postoperatively had a significantly lowermortality risk (HR 0.71, 95% CI 0.51-0.99, P ¼ .044)compared to those with persistent moderate-severe visualimpairment at 1-month-postoperative visits. Patients withmild visual impairment postoperatively had nonsignifi-cantly lower mortality risks compared to those with persis-tent moderate-severe visual impairment postoperatively(P > .06, Table 3).For supplementary analyses, of the 1785 patients with
VA data of the better eye from the postoperative1-month visits, 80.2% (n ¼ 1432), 11.9% (n ¼ 213), and7.9% (n ¼ 140) had no, mild, and moderate-severe visualimpairment, respectively. Of this group, 22% (n ¼ 391)had died by October 2011. Patients with no visual impair-ment (21.2%, 95% CI 18.8%-23.7%) had a similarage-standardized mortality rate to those with mild present-ing visual impairment (23.4%, 95% CI 17.0%-29.9%) buta lower age-standardized mortality rate than those withmoderate-severe presenting visual impairment (30.2%,95% CI 21.1%-39.4%, P ¼ .021) in the better eye. Afteradjusting for age, sex, smoking, BMI, hypertension, dia-betes, angina, myocardial infarction, transient ischemicattack, stroke, kidney disease, number of medications,and number of comorbid conditions (Model 3), the groupwith no visual impairment in their better eye had a 33%
JANUARY 2014OPHTHALMOLOGY

TABLE 2. Known Causes of Visual Impairment Among 217Cases With Persistent Moderate-Severe Visual Impairment
(Presenting Visual Acuity <20/60) 1 Month After Cataract
Surgery
Characteristic
Frequency, % (N)
(N ¼ 217)
Nonoperative
Under-corrected VAa 33.2 (72)
AMD 21.2 (46)
Glaucoma 16.1 (35)
Diabetic retinopathy 13.4 (29)
Epiretinal membranes 8.3 (18)
Myopic retinopathy 1.4 (3)
Optic disc atrophy 1.4 (3)
Previous retinal tear 0.9 (2)
Corneal lesion 0.9 (2)
Intraoperative or postoperative
Posterior capsular tear 5.5 (12)
Anterior vitrectomy 6.0 (13)
Iris trauma 3.2 (7)
Any intraoperative complicationb 9.7 (21)
Untreated posterior capsule
opacification
6.5 (14)
Cystoid macular edema (not associated
with diabetic retinopathy)
3.2 (7)
Otherc 1.4 (3)
No known nonrefractive caused 36.4 (79)
AMD ¼ age-related macular degeneration; VA ¼ visual acuity.aCases with VA that was corrected with a pinhole aperture by
>_3 lines.bIncludes posterior capsular tear, anterior vitrectomy, or iris
trauma.cOne case each of previous penetrating eye trauma, branch
retinal vein occlusion, or amblyopia.dNonrefractive causes include AMD, glaucoma, diabetic reti-
nopathy, epiretinal membranes, myopic retinopathy, optic disc
atrophy, previous retinal tear, previous penetrating eye trauma,
corneal lesion, branch retinal vein occlusion, amblyopia, intrao-
perative complication, posterior capsule opacification, or cystoid
macular edema.
lower mortality risk (HR 0.67, 95% CI 0.47-0.94)compared to the group who had moderate-severe visualimpairment in their better eye 1 month postoperatively(Table 4). After multivariable adjustments in Models2 and 3, the group with mild visual impairment in theirbetter eye also had lower mortality risks (Model 2, HR0.70, 95% CI 0.45-1.09; Model 3, HR 0.69, 95% CI0.45-1.07) compared to the group with moderate-severevisual impairment in their better eye 1 month postopera-tively, but the difference was not significant (Table 4).
Supplementary analyses using the latest VA from cumu-lative visits within the 12-month-postoperative periodshowed similar but attenuated associations. After multivar-iable adjustment in Models 2 and 3, the group with novisual impairment in the better eye had a lower mortality
VOL. 157, NO. 1 IMPROVED VISION WITH CATARACT
risk compared to the group whose moderate-severe visualimpairment persisted in the better eye during cumulativevisits in the 12 months after cataract surgery (Model 2,HR 0.77, 95% CI 0.52-1.15; Model 3, HR 0.72, 95% CI0.48-1.08), but the difference was marginally nonsignifi-cant. There was no difference in mortality riskbetween the mild visual impairment group and themoderate-severe visual impairment group in these analyses(Models 2-3, Table 4).Fourteen percent of the study sample had missing BMI
data. Exclusion of the BMI variable from Model 3 allowedthe inclusion of a larger number of participants in thesupplementary analyses. The estimate for the mortalityassociation between those with no visual impairment vsthose with moderate-severe visual impairment becamesignificant if participants with missing BMI data wereincluded: HR 0.69 (95% CI 0.48-0.99), using cumulative12-month VA.
DISCUSSION
IN THIS OLDER SURGICAL COHORT, WE FOUND THATOLDER
persons with moderate-severe visual impairment that wascaused by cataract and corrected by cataract surgery hada 30% lower mortality risk over 5 years, independent ofage, sex, many individual variables defining chronic condi-tions, and grouped indicators of health and frailty,compared to older persons who had also undergone cataractsurgery but had persistent moderate-severe visual impair-ment after surgery. This finding complements our observa-tion from a different study sample (the BMES) that personswith cataract-related presenting visual impairment thatwas corrected by cataract surgery had a 40% lower15-year mortality risk, compared to those who remainedvisually impaired because of cataract and who did nothave cataract surgery.6
Although our previous findings from the BMES hadadjusted for many comorbidities,6 we could not excludethe possibility that poor general health prevented someolder persons from having cataract surgery, and that itwas the poor health status that contributed to, andthus explained, poor survival in the nonsurgical groupwith persistent visual impairment over the follow-upperiod. In this current study we recruited cataractsurgical patients only, implying that these patientswere in reasonable general health that enabled themto undergo cataract surgery. However, there was stilla possibility that reasons associated with persistingmoderate-severe visual impairment after cataractsurgery contributed to poor survival. We collected infor-mation about common comorbid conditions and use ofregular medications from this surgical cohort, and wereonly able to document a slightly younger mean age(74.4 years), a higher female proportion (58.8%), and
167SURGERY AND BETTER SURVIVAL

TABLE 3. Five-Year Mortality Hazard Ratios of 901 Patients who Had Either Mild (Defined as Visual Acuity<20/40-20/60) or No VisualImpairment (Visual Acuity >_20/40) Versus Those With Moderate-Severe Visual Impairment (Visual Acuity <20/60) in the Surgical Eye
1 Month Postoperatively, the Australian Prospective Cataract Surgery and Age-related Macular Degeneration Studya
1-Month-Postoperative VA Statusa Patients, n
Died,
n (%)
Model 1: Age- and
Sex-Adjusted
HR (95% CI)
Model 2:
Multivariable-Adjusted
HR (95% CI)b
Model 3:
Multivariable-Adjusted
HR (95% CI)c
Moderate-severe visual impairment (<20/60) 217 71 (32.7) 1.0 1.0 1.0
Mild visual impairment (<20/40-20/60) 140 36 (25.7) 0.71 (0.47-1.06) 0.70 (0.44-1.11) 0.67 (0.42-1.06)
No visual impairment (>_20/40) 544 125 (23.0) 0.76 (0.57-1.02) 0.73 (0.52-1.01) 0.71 (0.51-0.99)
BMI ¼ body mass index; CI, confidence interval; HR ¼ hazard ratio; VA ¼ visual acuity.aPresenting VA data are used.bAdjusted for sex, baseline age, smoking, low BMI, and history of hypertension, diabetes, angina, myocardial infarction, transient ischemic
attack, stroke, and kidney disease.cAdjusted for all the variables in Model 2 plus number of medications taken (as a continuous variable) and number (>_3 vs <3) of comorbid
conditions (which included history of hypertension, diabetes, angina, myocardial infarction, transient ischemic attack, stroke, and kidney
disease).
TABLE 4. Five-Year Mortality Hazard Ratios of Post–Cataract Surgical Patients who Had Either Mild (Defined as Visual Acuity
<20/40-20/60) or No Visual Impairment (Visual Acuity >_20/40) Versus Those With Moderate-Severe Visual Impairment (Visual Acuity<20/60) in the Better Eye Postoperatively, the Australian Prospective Cataract Surgery and Age-related Macular Degeneration Studya
Patients, n
Died,
n (%)
Model 1: Age- and
Sex-Adjusted
HR (95% CI)
Model 2:
Multivariable-Adjusted
HR (95% CI)b
Model 3:
Multivariable-Adjusted
HR (95% CI)c
Patients with 1-month-postoperative VAa
Moderate-severe postoperative visual
impairment (<20/60)
140 46 (32.9) 1.0 1.0 1.0
Mild postoperative visual impairment
(<20/40-20/60)
213 53 (24.9) 0.71 (0.48-1.05) 0.70 (0.45-1.09) 0.69 (0.45-1.07)
No postoperative visual impairment
(>_20/40)
1432 292 (20.4) 0.68 (0.50-0.93) 0.70 (0.50-0.98) 0.67 (0.47-0.94)
Patients with VA from cumulative visits over the 1-year-postoperative perioda
Moderate-severe postoperative visual
impairment (<20/60)
111 34 (30.6) 1.0 1.0 1.0
Mild postoperative visual impairment
(<20/40-20/60)
235 72 (30.6) 0.96 (0.63-1.44) 1.03 (0.65-1.63) 1.01 (0.64-1.61)
No postoperative visual impairment
(>_20/40)
1455 289 (19.9) 0.72 (0.50-1.03) 0.77 (0.52-1.15) 0.72 (0.48-1.08)
BMI ¼ body mass index; CI, confidence interval; HR ¼ hazard ratio; VA ¼ visual acuity.aPresenting VA data are used.bAdjusted for sex, baseline age, smoking, low BMI, and history of hypertension, diabetes, angina, myocardial infarction, transient ischemic
attack, stroke, and kidney disease.cAdjusted for all the variables in Model 2 plus number of medications taken (as a continuous variable) and number (>_3 vs <3) of comorbid
conditions (which included history of hypertension, diabetes, angina, myocardial infarction, transient ischemic attack, stroke, and kidney
disease).
a lower diabetes prevalence (26.5%) in the groupwithout visual impairment compared to those whoremained with moderate-severe visual impairment(age, 76.1 years, P ¼ .0001; female proportion, 51.2%,P ¼ .02; diabetes prevalence, 37.8%, P ¼ .002)(Table 1). We acknowledge that there are many factorsassociated with visual impairment that we had notmeasured and controlled for, including social support and
168 AMERICAN JOURNAL OF
emotional well-being factors, that could partly explainthe observed association.The Salisbury Eye Evaluation project reported that
participants with a >_2-line gain in binocular presentingVA, resulting from either cataract surgery or refractivecorrection over 2 years, had a 53% adjusted mortality riskreduction over 6 years.5 In our primary analysis, we addressa slightly different question in this study, which is whether
JANUARY 2014OPHTHALMOLOGY

correcting cataract-related visual impairment by phaco-emulsification surgery is associated with better survivalamong older persons whose visual impairment was consid-ered to be caused by the cataract. Further, in supplementaryanalyses we document a lower mortality risk in olderpersons with no visual impairment compared to thosewith moderate-severe visual impairment in their bettereye regardless of cataract surgery. Findings from the SEEand our studies can be viewed as providing additionalcomplementary evidence supporting the visual impair-ment–mortality association, documented previously inmany population-based studies.1–5,17
Previous studies have also shown that visual impair-ment may be linked to mortality via indirect path-ways.5,17–19 In our study, adjustment for BMI did notchange the direction of the protective associationbetween corrected visual impairment and lowermortality, but the significance level was attenuated forthe mild visual impairment group (Table 3). This couldbe attributable to either a smaller sample size (14% ofpatients with missing BMI data were excluded from theanalysis with BMI in the model) or a partial confoundereffect on the mortality association: low BMI levels maybe associated with mortality-related systemic conditions.Our study findings cannot be interpreted as a direct orcausal association between visual impairment and highermortality, or between no visual impairment and bettersurvival. It is highly likely that other factors (such associal connections, emotional well-being status, andself-perceived health status) associated with visualimpairment may explain the observed association.
Older age per se is associated with increasing healthproblems. Although we have adjusted for a large numberof health conditions, the adjustment for age and markersof aging and frailty may not have completely resolved theimbalance in distribution of many health problemsbetween groups with and without visual impairment,even though the difference in mean age was less than2 years among the visual impairment groups in our sample.
In our analyses of surgical eyes and better eyes ofpatients, two thirds of the surgical eyes overlapped withthe better of paired eyes or were the only eye with dataavailable in our sample. Hence, we assessed mortality riskaccording to the better-eye group in 2 ways: first, using
VOL. 157, NO. 1 IMPROVED VISION WITH CATARACT
VA status of the better eye 1 month after cataract surgery;second, using VA measures from the latest visit within the12-month-postoperative period. The similarity in findingsfrom analyses using either the surgical eye or the bettereye at 1-month-postoperative visits (Table 4) confirmsthe robustness of these findings. Although the significancelevel of analyses using the better-eye data within the12-month-postoperative period was attenuated, it did notchange the direction of the protective association betweencorrected visual impairment and lower mortality.The strengths of our study include its prospective design,
the relatively large sample size of surgical patients withless than 10% dropout rate at the 1-month-postoperativevisits, the use of standardized protocols to measure VA,and the use ofAustralianNDI data to obtainmortality infor-mation. Limitations of our study include its relatively shortfollow-up period (around 5 years) and the possibility that wecould have missed other confounding factors, such as socialconnection, optimism and self-reported health status, thatwere not measured in our study. Although there was likelyto be progress of age-related eye diseases, such as age-relatedmacular degeneration, glaucoma, and diabetic retinopathy,in the long term after cataract surgery, postoperative visionin the Australian Prospective Cataract Surgery and Age-related Macular Degeneration study cohort was relativelysustained for at least 2 years post surgery.20 We had previ-ously reported that approximately 70% of 1294 patientswith sufficient VA data had presenting VA >_20/40 at boththe 1- and 24-month-postoperative visits.20
In conclusion, in this older cataract surgical cohort wewere able to confirm findings observed in an olderpopulation-based sample (the BMES) that correctingmoderate-severe cataract-related visual impairment bycataract surgery was associated with a 30% lower mortalityrisk, compared to that of older persons whose moderate tosevere levels of visual impairment persisted, independent ofother known mortality risk factors. These new findings,strengthened by including cataract surgical patients onlyand comparing patients with and without visual impair-ment correction after cataract surgery, complementprevious evidence found from multiple studies document-ing a link between visual impairment and poor survivalamong older persons,1–4,21 even though this association islikely to be indirect.
ALL AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OF INTEREST.P.M. serves on Advisory Boards for Abbott, Novartis, Bayer, and Bausch & Lomb and has received consultancy fees and payment for lectures from Abbott,Novartis, and Bayer. J.J.W. is funded by a National Health &Medical Research Council Senior Research Fellowship (2005-2014). The Australian Prospec-tive Cataract Surgery andAge-relatedMacular Degeneration study was supported by theNational Health&Medical Research Council, Canberra, Australia(Grant No 302010, 2004-2006), Retina Australia (2005), and NHMRC Centres for Clinical Research Excellence (Identification No 529923, 2009-2013).Contributions of authors: study design (J.J.W., P.M.); conduct of the study (T.d.L., C.S.F.); data collection (T.d.L., A.G.T., C.S.F.); management of thestudy (J.J.W., P.M.); statistical analyses (E.R.); analysis and interpretation of data (E.R., J.J.W., C.S.F.); drafting the manuscript (C.S.F., J.J.W.); reviewof the article (J.J.W., P.M., E.R., T.d.L., A.G.T., C.S.F.); and approval of the final version of the article, including changes made in the subsequent revision(J.J.W., P.M., E.R., T.d.L., A.G.T., C.S.F.). The authors wish to thank Ms Mireille Moffitt and Ms Kirsten Jakobsen (Centre for Vision Research, Depart-ment of Ophthalmology and Westmead Millennium Institute, University of Sydney) for, respectively, grading retinal photographs and editing the article.
169SURGERY AND BETTER SURVIVAL

REFERENCES
1. Wang JJ, Mitchell P, Simpson JM, Cumming RG, Smith W.Visual impairment, age-related cataract, and mortality. ArchOphthalmol 2001;119(8):1186–1190.
2. Borger PH, van Leeuwen R, Hulsman CA, et al. Is therea direct association between age-related eye diseases andmortality? The Rotterdam Study. Ophthalmology 2003;110(7):1292–1296.
3. Clemons TE, Kurinij N, Sperduto RD. Associations ofmortality with ocular disorders and an intervention ofhigh-dose antioxidants and zinc in the Age-Related EyeDisease Study: AREDS Report No. 13. Arch Ophthalmol
2004;122(5):716–726.4. Knudtson MD, Klein BE, Klein R. Age-related eye disease,
visual impairment, and survival: the Beaver Dam Eye Study.Arch Ophthalmol 2006;124(2):243–249.
5. Freeman EE, Egleston BL, West SK, Bandeen-Roche K,Rubin G. Visual acuity change and mortality in older adults.Invest Ophthalmol Vis Sci 2005;46(11):4040–4045.
6. Fong CS, Mitchell P, Rochtchina E, Teber ET, Hong T,Wang JJ. Correction of visual impairment by cataract surgeryand improved survival in older persons: the Blue MountainsEye Study Cohort. Ophthalmology 2013;120(9):1720–1727.
7. Cugati S, de Loryn T, Pham T, Arnold J, Mitchell P,Wang JJ.Australian prospective study of cataract surgery andage-related macular degeneration: rationale and method-ology. Ophthalmic Epidemiol 2007;14(6):408–414.
8. Wang JJ, Fong CS, Rochtchina E, et al. Risk of age-relatedmacular degeneration 3 years after cataract surgery: pairedeye comparisons. Ophthalmology 2012;119(11):2298–2303.
9. Klein R, Davis MD, Magli YL, Segal P, Klein BE, Hubbard L.The Wisconsin age-related maculopathy grading system.Ophthalmology 1991;98(7):1128–1134.
10. Bird AC, Bressler NM, Bressler SB, et al. An internationalclassification and grading system for age-related maculopathyand age-related macular degeneration. The InternationalARM Epidemiological Study Group. Surv Ophthalmol 1995;39(5):367–374.
170 AMERICAN JOURNAL OF
11. Early Treatment Diabetic Retinopathy Study ResearchGroup. Grading diabetic retinopathy from stereoscopic colorfundus photographs-an extension of the modified AirlieHouse classification (Report No. 10). Ophthalmology 1991;98:786–806.
12. International Classification of Diseases, Ninth Revision,Clinical Modification (ICD-9-CM) Geneva: World HealthOrganization; 1991.
13. International Statistical Classification of Diseases AndRelated Health Problems, Tenth Revision (ICD-10) Geneva:World Health Organization; 1992.
14. Powers J, Ball J, Adamson L, Dobson A. Effectiveness of theNational Death Index for establishing the vital status of olderwomen in the Australian Longitudinal Study on Women’sHealth. Aust N Z J Public Health 2000;24(5):526–528.
15. Magliano D, Liew D, Pater H, et al. Accuracy of the Austra-lian National Death Index: comparison with adjudicated fataloutcomes among Australian participants in the Long-termIntervention with Pravastatin in Ischaemic Disease (LIPID)study. Aust N Z J Public Health 2003;27(6):649–653.
16. Klein BE, Klein R, Knudtson MD, Lee KE. Frailty, morbidityand survival. Arch Gerontol Geriatr 2005;41(2):141–149.
17. Foong AW, Fong CW,Wong TY, Saw SM, Heng D, Foster PJ.Visual acuity and mortality in a Chinese population. TheTanjong Pagar Study. Ophthalmology 2008;115(5):802–807.
18. Lee DJ, Gomez-Marin O, Lam BL, Zheng DD. Visual acuityimpairment and mortality in US adults. Arch Ophthalmol2002;120(11):1544–1550.
19. Tournier M, Moride Y, Ducruet T, Moshyk A, Rochon S.Depression and mortality in the visually-impaired,community-dwelling, elderly population of Quebec. ActaOphthalmol Scand 2008;86(2):196–201.
20. Fong CS, Mitchell P, Rochtchina E, de Loryn T, Hong T,Wang JJ. Sustainability of visual acuity in the first 2 years aftercataract surgery. Br J Ophthalmol 2011;95(12):1652–1655.
21. Cugati S, Cumming RG, Smith W, Burlutsky G, Mitchell P,Wang JJ. Visual impairment, age-related macular degenera-tion, cataract, and long-term mortality: the Blue MountainsEye Study. Arch Ophthalmol 2007;125(7):917–924.
JANUARY 2014OPHTHALMOLOGY

Biosketch
Calvin Sze-un Fong, MBBS, graduated in medicine from the University of New South Wales, Australia, in 2005. He
subsequently completed his medical internship at Westmead Hospital, in Sydney. He is currently undertaking a PhD at
the Centre for Vision Research, University of Sydney, under the supervision of Professor Jie Jin Wang and Professor
Paul Mitchell.
VOL. 157, NO. 1 170.e1IMPROVED VISION WITH CATARACT SURGERY AND BETTER SURVIVAL