Embed Size (px)
Citation preview

Visual Conditions in Veterans Followed at a VA Polytrauma
Network Site Thomas R Stelmack, O.D.1,3,4, Theresa Firth, O.D.2;
Dennise VanKoevering, M.A.2, Steve Rinne2, MA, Barbara Hunt2, Ph.D., Joan A Stelmack, O.D., MPH2,3,4
1 Jesse Brown VAMC, 2 Hines VAH, 3 Illinois College of Optometry 4 University of Illinois

War
• Brain and eye injuries are well recognized consequences of war. The etiology of these injuries reflects the “wounding patterns of the war.”
• Over 1.5 million U.S. military personnel have been deployed to Iraq or Afghanistan since military operations were initiated in 2001.
• Service members from Operation Enduring Freedom (OEF) and Operation Iraqi Freedom (OIF) have survived injuries that would have been fatal in previous wars because of speedy evacuation, timely acute trauma care and improvements in protective body armor.

Blast injuries
• are the most common wound in the current conflicts.
• soldiers may be exposed to multiple blast waves during deployment.
• account for two thirds of army war zone evacuations.
Blast wave injuries occur from
• changes in atmospheric pressure (overpressures)
• collision with objects carried by the blast wave
• personnel set in motion hitting a stationary object.

Traumatic Brain Injury
• primary neuropathology of TBI diffuse axonal injury caused by shearing forces that disrupt axons and small vessels during sudden deceleration– focal brain edema– anoxia– hematoma Sandia Corp
brain-model shear 1 msecred 30 blue 1 atmospheres

TBI
• The news media has also reported a high incidence of traumatic brain injury (TBI) caused by blasts noting rates as high as 18% based on interviews with military officials
• The provision of medical care and rehabilitation for those soldiers injured in the current conflict is a major priority for the Department of Veterans Affairs, Veterans Health Administration (VHA).
• VHA created an infrastructure referred to as the “Polytrauma System of Care” to guide medical care and rehabilitation of injured veterans and active duty service members.
VA System
• Polytrauma Rehabilitation Centers (PRCs)
• Regional Polytrauma Network Sites (PNS)
• Polytrauma Support Clinic Teams (PSCTs)Polytrauma Points of Contact (PPOCs)
• Mandates screening all OEF / OIF participants for TBI.
Polytrauma Rehabilitation Centers (PRCs)
• Minneapolis, MN • Palo Alto, CA
• Richmond, VA • Tampa, FL• San Antonio, TX
provide acute inpatient medical and rehabilitation care
Regional Polytrauma Network Sites (PNS)
post-acute sequelae of polytrauma
• interdisciplinary evaluation• care coordination for inpatient and outpatient rehabilitation• day programs• transitional rehabilitation
21 Centers distributed nationwide
Polytrauma Support Clinic Teams (PSCTs)
Polytrauma Points of Contact (PPOCs)
• support by managing those who are medically stable• provide regular follow-up visits• respond to new programs• coordinate with the Polytrauma Network Sites
130 Nationwide
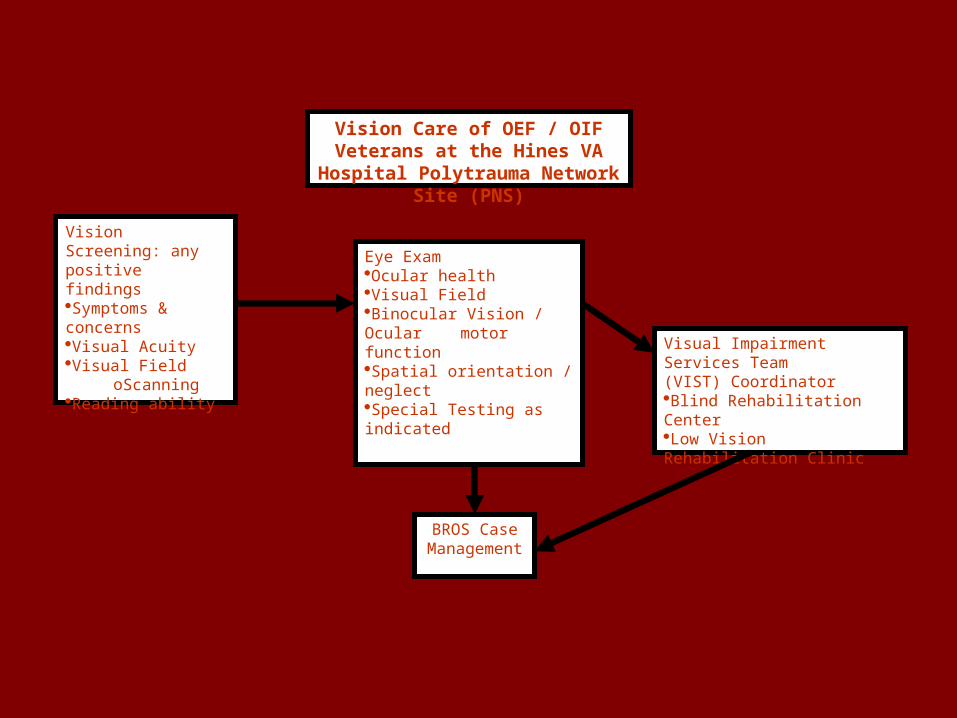
Vision Screening: any positive findingsSymptoms & concernsVisual AcuityVisual Field
oScanningReading ability
Eye ExamOcular healthVisual FieldBinocular Vision / Ocular motor functionSpatial orientation / neglectSpecial Testing as indicated
Visual Impairment Services Team (VIST) Coordinator
Blind Rehabilitation CenterLow Vision Rehabilitation Clinic
BROS Case Management
Vision Care of OEF / OIF Veterans at the Hines VA Hospital Polytrauma
Network Site (PNS)
TBI mandated screening
• Exposure– Blasts– Wounds– Falls– MVA– Amnesia– LOC
• Symptoms• Neurobehavioral inventory

TBI mandated screening
• Exposure• Symptoms
– Poor memory – Balance / dizziness– Photophobia– Irritability– HA– In (hypo) somnia
• Neurobehavioral inventory
TBI mandated screening
• Exposure
• Symptoms
• Neurobehavioral inventory– 5 point scale– Extent to which symptoms have disturbed
them since trauma

TBI mandated screening• Neurobehavioral inventory
– Feeling dizzy– Loss of balance– Poor coordination, clumsy– Headaches– Nausea– Vision problems, blurring, trouble seeing– Sensitivity to light– Hearing difficulty– Sensitivity to noise– Numbness or tingling on parts of my body– Changes in taste or smell– Loss of appetite or increased appetite– Poor concentration, can’t pay attention, easily distracted– Forgetfulness, can’t remember things– Difficulty making decisions– Slowed thinking, difficulty getting organized, can’t finish things– Fatigue, loss of energy, getting tired easily– Difficulty falling or staying asleep– Feeling anxious or tense– Feeling depressed or sad– Irritability, easily annoyed– Poor frustration tolerance, feeling easily overwhelmed by things

Visual Function Polytrauma
• Goodrich et al from Palo Alto Polytrauma Rehabilitation Center (Optometry Dec 04 – Nov 06)
– 50 records TBI • 50% explosive devices (IED, RPG, mortars etc)• 44% penetrating injuries• 74% self reported visual complaints• 14% legal blindness• 10% visual impairment (20/63-20/100)• >2x prevalence visual sxs with blast injury
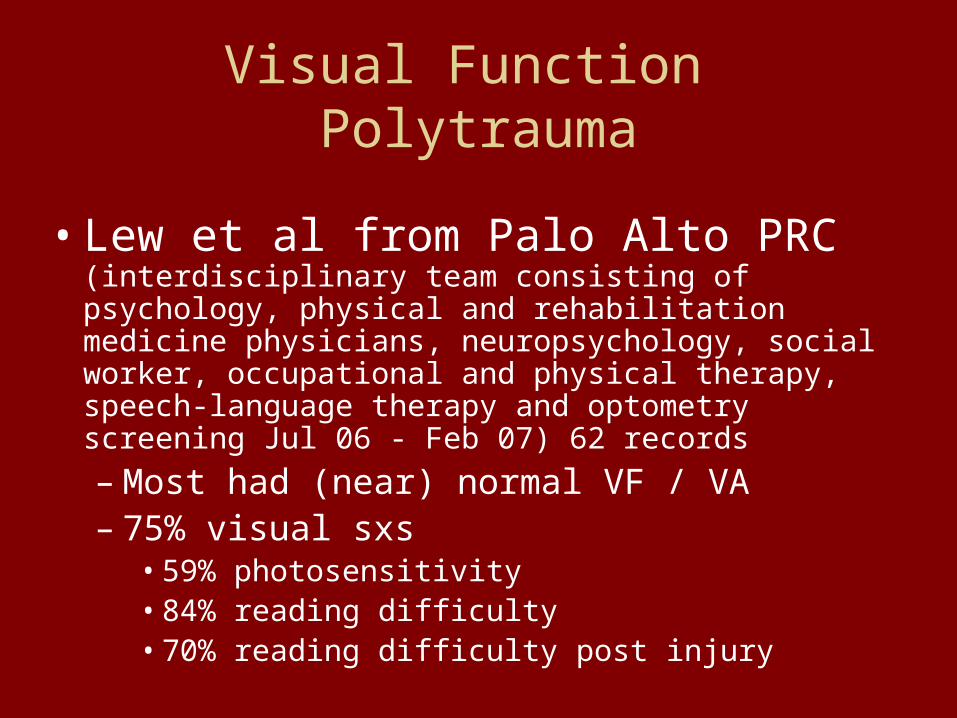
Visual Function Polytrauma
• Lew et al from Palo Alto PRC (interdisciplinary team consisting of psychology, physical and rehabilitation medicine physicians, neuropsychology, social worker, occupational and physical therapy, speech-language therapy and optometry screening Jul 06 - Feb 07) 62 records
– Most had (near) normal VF / VA– 75% visual sxs
• 59% photosensitivity• 84% reading difficulty• 70% reading difficulty post injury

Visual Function Polytrauma
• Lew et al from Palo Alto PRC • 70% oculomotor• Binocular vision problems
– 46% convergence– 25% pursuits / saccades (different neuro control)– 21% accommodation– 11% strabismus– 5% fixational / strabismus– Other
» 66% Visual disturbance» 42% balance» 40% dizziness (? Vertigo vs light headed)
Methods
• A retrospective review of VA electronic medical records was conducted to identify patients flagged as POLYTRAUMA and those with a confirmed diagnosis of TBI who were seen at the Hines PNS. – 103 patients with POLYTRAUMA seen in clinics from
October, 2005 – March, 2008 – 88 patients with TBI seen in the TBI Clinic from
December, 2007 – March, 2008. The level of TBI was not routinely available in the electronic medical record.

Demographics
• Polytrauma– 96% male– 30 years mean age– 85% OEF / OIF
• 77% injury in theatre• 23% US or other
countries
– 46% TBI
• TBI– 92% male– 31 years mean age– 88% OEF / OIF injury
in theatre– 95% non penetrating

Basic Visual assessment
• Polytrauma– Mean visual acuity was .04 log MAR (Snellen Equivalent 20/20)– bilateral no light perception (3%)– legally blind (4%)– visually impaired 1% (VA less than 20/63 to 20/100)– self-reported visual symptoms (76% )
• TBI– mean .04 log MAR (20/20 Snellen Equivalent)– legally blind (1%) – visually impaired (visual acuity less than 20/63 to 20/100) (0%)– self-reported visual symptoms (67%)
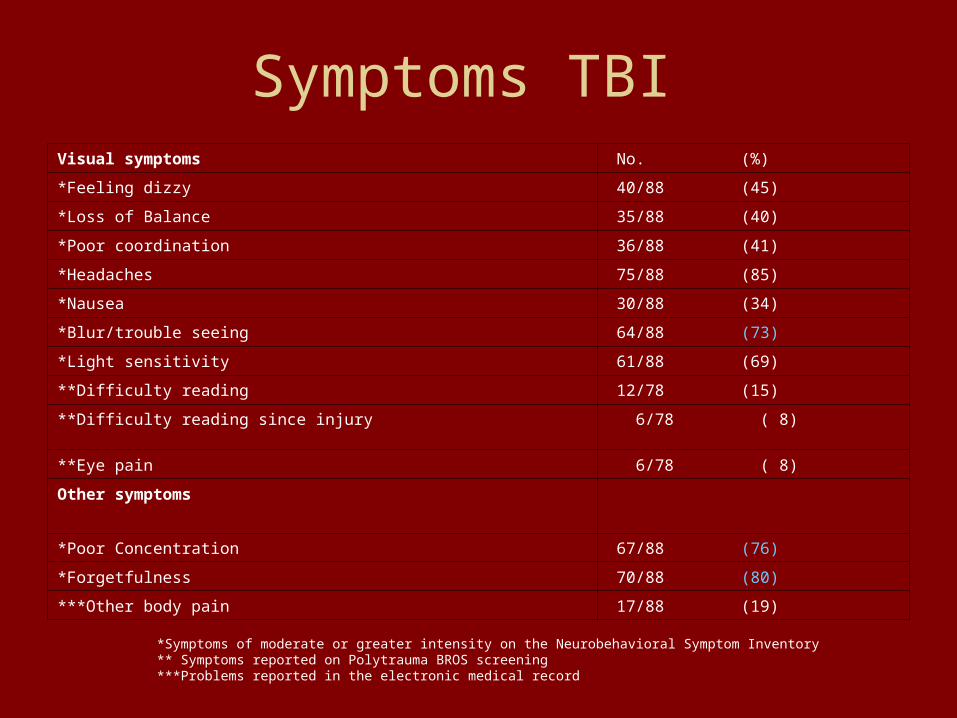
Symptoms TBI Visual symptoms No. (%)
*Feeling dizzy 40/88 (45)
*Loss of Balance 35/88 (40)
*Poor coordination 36/88 (41)
*Headaches 75/88 (85)
*Nausea 30/88 (34)
*Blur/trouble seeing 64/88 (73)
*Light sensitivity 61/88 (69)
**Difficulty reading 12/78 (15)
**Difficulty reading since injury 6/78 ( 8)
**Eye pain 6/78 ( 8)
Other symptoms
*Poor Concentration 67/88 (76)
*Forgetfulness 70/88 (80)
***Other body pain 17/88 (19)
*Symptoms of moderate or greater intensity on the Neurobehavioral Symptom Inventory ** Symptoms reported on Polytrauma BROS screening***Problems reported in the electronic medical record
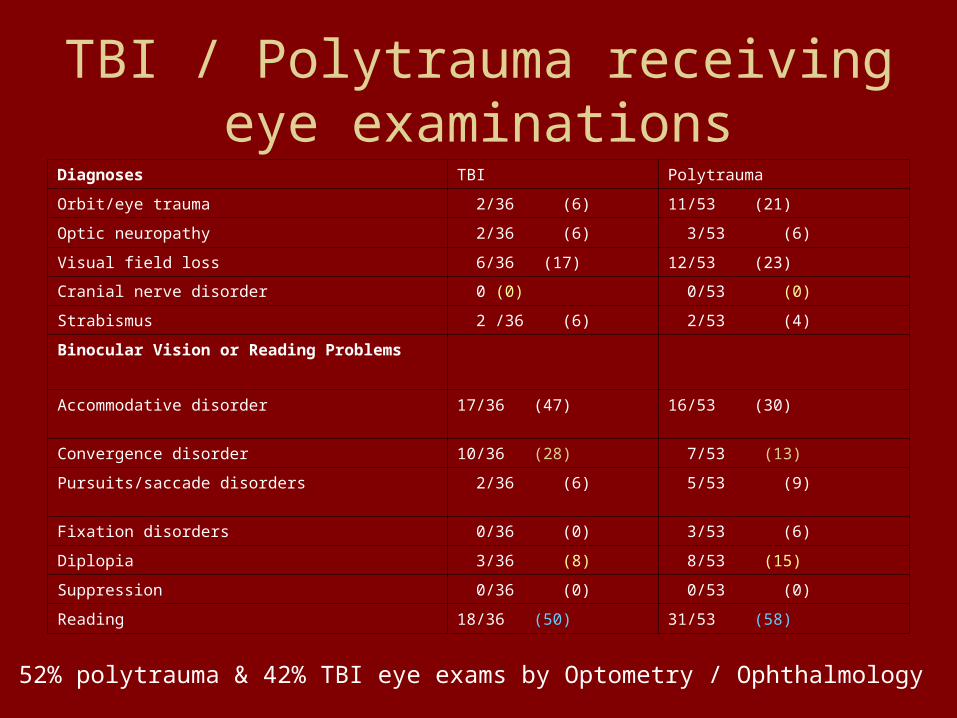
TBI / Polytrauma receiving eye examinations
Diagnoses TBI Polytrauma
Orbit/eye trauma 2/36 (6) 11/53 (21)
Optic neuropathy 2/36 (6) 3/53 (6)
Visual field loss 6/36 (17) 12/53 (23)
Cranial nerve disorder 0 (0) 0/53 (0)
Strabismus 2 /36 (6) 2/53 (4)
Binocular Vision or Reading Problems
Accommodative disorder 17/36 (47) 16/53 (30)
Convergence disorder 10/36 (28) 7/53 (13)
Pursuits/saccade disorders 2/36 (6) 5/53 (9)
Fixation disorders 0/36 (0) 3/53 (6)
Diplopia 3/36 (8) 8/53 (15)
Suppression 0/36 (0) 0/53 (0)
Reading 18/36 (50) 31/53 (58)
52% polytrauma & 42% TBI eye exams by Optometry / Ophthalmology

Visual treatments Polytrauma or TBI
Treatment TBI Polytrauma
Ocular surgery 0/36 (0) 2/52 (4)
Contact Lenses 1/36 (3) 1/52 (2)
Spectacles 28/36 (78) 33/52 (63)
Vision Therapy 5/36 (14) 4/52 (8)
Blind Rehabilitation 0/36 (0) 5/52 (10)
Low Vision Rehabilitation 1/36 (3) 1/52 (2)

Other conditions Hines patients
TBI with
diagnoses of – PTSD (58%) – depression
(26%)– depression &
PTSD (40%)
Polytrauma with diagnoses of• TBI (46%)• PTSD (50%)• depression (32%)• depression &
PTSD (18%)
Center differences in severity
• Patients seen at the Palo Alto Polytrauma Rehabilitation Center were more likely to have vision loss from moderate to total blindness as a result of visual acuity, visual field loss, and or bilateral enucleation (38%) compared to patients at the Hines PNS (8% of patients with TBI and 18% of patients with polytrauma).
• Patients admitted to the PRCs are severely injured and require acute care and rehabilitation in a hospital setting.
What we’ve learned What is needed
• Hines VA Hospital and the Palo Alto Health Care System are both Polytrauma Network Sites. – A high percentage of patients self-reported visual symptoms at
both sites• 70% Hines TBI patients, 78% Hines polytrauma patients• 75% Palo Alto patients
– Binocular vision screening • Palo Alto indicated that oculomotor problems were found in 70 % of
patients screened by optometry• Hines found these problems in 83% of patients with TBI and 70% of
patients with polytrauma who received an eye examination.
• These statistics emphasize the importance of including vision screening and examinations within the Polytrauma System of Care.
What we’ve learnedWhat we’ve learned What is neededWhat is needed
• VHA does not have a national directive that establishes a protocol for OIE/OEF eye examinations
• a VA directive establishing a protocol for eye examinations, screenings and reporting is needed to facilitate research on the incidence, natural course of recovery and outcomes of brain injury treatment in soldiers returning from the war
• disciplines comprising the Polytrauma team, vision screening procedures and eye examination protocols vary making it difficult to combine or compare data from different sites

What we’ve learned What is neededWhat is needed
• A VA TBI workgroup was formed for optometrists to share information and experiences working with OEF/OIF veterans during regularly scheduled conference calls.
Reported Binocular Vision Problems:VA vs non military TBI
• Ciuffreda et al. reported in his retrospective analysis of 160 patient records that 90% of patients with TBI had oculomotor dysfunction– accommodative (56.3%)– vergence deficits (56.3%)
• Kowal reported from a series of 161 closed head injury patients – 16% had poor accommodation– 14% convergence insufficiency– 19% pseudomyopia

Reading difficulty co-morbidities concentration & memory
• Palo Alto– 84% self reported
reading difficulty
• Hines– 50% self reported
reading difficulty (TBI) 25% (polytrauma)
– exam 50% TBI & 40% polytrauma had reading problems
Reading ability has concentration and memory components.Despite unknown pre morbid conditions, Hines TBI self reported
80% memory 76% concentration difficulty; which is consistent with known TBI data.

Natural course & success of treatment
• Civilian population: – 85 – 90% attention & memory problems associated
with neural damage from mild TBI resolve within weeks to months.
– Remainder persist for year and are associated with compensation / medical disability.
• Military population:– Statistics may not apply given frequent association
with PTSD.– 43.9% OEF / OIF reporting LOC had TBI had sxs
sufficient for PTSD dx
Natural course & success of treatment
• AMA study (PTSD, depression etc) mental illness – 19.1% OEF / OIF– 11.3% Afghanistan
• Depression etc known to exacerbate attention & memory.
• Natural vs. treated course will be difficult to follow as many opt out of treatment for convergence / accommodative disorders.
VA benefits
• All OIF/ OEF veterans serving in the armed forces, Reserves or National Guard are entitled to 5 years of free care for most conditions through the VA.
• Veterans with service-related conditions must file a claim to have their diagnoses service-connected in order to obtain lifelong medical care from the VA.
References
• Warden D. Military TBI during the Iraq and Afghanistan wars. J Head Trauma Rehabil 2006;21:5:398-402.• Hoge CW, McGurk D, Thomas JL, Cox AL, Engel CC, Castro CA. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med
2008;358:453-463.• Warden DL, Ryan LM, Helmick KM, et al. war neurotrauma: The Defense and Veterans Brain Injury Center (DVBIC) experience at Walter reed Army
Medical Center (WRAMC) [abstract]. J. Neurotrauma. 2005;22910):1178.• Alexander MP. Mild traumatic brain injury: Pathophysiology, natural history and clinical management. Neurology 1995;45(7):1253-1260.• Lew HL, Cifu DX, Sigford B, Scott S, Sayer N, Jafee MS. Team approach to diagnosis and management of traumatic brain injury. J Rehabil Res Dev.
2007;44:vii-xi. • Lew HL, Poole JH, Vanderploeg RD, Goodrich GL, Dekelboum S, Guillory SB, Sigford B, Cifu DX. Program Development and defining characteristics of
returning military in a VA Polytrauma Network Site. J Rehabil Res Dev. 2007;44;1027-1034.• Goodrich GL, Kirby J, Cockerham G, Ingalla SP, Lew H L. Visual function in patients of a Polytrauma Rehabilitation Center: A descriptive study. J
Rehabil Res Dev. 2007; 44(7):929-936.• Department of Veterans Affairs, Veterans Health Administration. Screening and evaluation of possible traumatic brain injury in Operation Enduring
Freedom (OED) and Operation Iraqi Freedom (OIF) Veterans. VHA Directive 2007-013. Washington, D.C.: Department of Veterans Affairs, April, 2007.• Ciuffreda KJ, Kapoor N, Rutner D, Suchoff IB, Han ME, Craig S. Occurrence of oculomotor dysfunctions in acquired brain injury: A retrospective
analysis. Optometry 2007;78:155-161.• Kowal L. Ophthalmic manifestations of head injury. Clinical and Experimental Ophthalmology 2007;20(1);35-40.• Dikmen S, Mc Lean A, Temkin N. et al. Neuropsychological and psychosocial consequences of minor head injury. J Neurol Neurosurg Psychiatry
1992;49:1227-1232.• Evans RW. The Post-concussive syndrome: 130 years of controversy. Semin Neurol 1994; 14:32-39.• Padula WV, Wu L, Vicci V, Thomas J, Nelson C, Gottlieb D, Suter P, Politzer T, Benabib R. Evaluating and treating visual dysfunction. In:Zasler ND,
Katz DI, Zafonte RD, Editors. Brain injury medicine principles and practice. N.Y., N.Y.: Demos; 2006:511-528. • Suchoff IB, Ciuffreda KJ, Kapoor N, Editors. Visual & vestibular consequences of acquired brain injury. Santa Ana, CA: OEP Foundation; 2001:1-244.• Carroll LJ, Cassidy JD, Peloso PM. et al. Prognosis for mild traumatic brain injury: results of the WHO Collaborating Centre Task Force for mild
traumatic grain injury. J Rehabil Med 2004;43:Suppl:84-105.• National Center for Injury Prevention and Control. Report to Congress on mild traumatic brain injury in the United States: steps to prevent a serious
public health problem. Atlanta: Centers for Disease Control and Prevention, 2003.• Hoge, CW, Auchterlonie JL, Miliken CS. Mental health problems, use of mental health services and attrition from military service after deployment to
Iraq or Afghanistan. JAMA.2006;295:1023-1032.• Keram E. PTSD in Afghanistan and Iraq war veterans. Sonoma Medicine.http://www.sonic.net/scp/sm06/keram.html. accessed 8/15/08• Grieger TA, Cozza SJ, Ursano RJ, Hoge C, Martinez PE, Engel CC, Wain HJ. Posttraumatic stress disorder and depression in battle-injured soldiers.
Am J Psychiatry 2006;164 :1777-1783.• Veterans Administration. Combat veterans now eligible for five year no-cost VA medical care. Chevron 2008;68(16):8.• Department of Veterans Affairs, Veterans Health Administration. Determining combat veteran eligibility. VHA Directive 2005-020. Washington, D.C.:
Department of Veterans Affairs, June 2, 2005.• Department of Veterans Affairs, Veterans Health Administration. VA Handbook 4550. Washington, D.C.: Department of Veterans Affairs, April 24, 1997.
Thank you
To
Those who have served to defend our freedom !!!!