Embed Size (px)
Citation preview

Vision Screening Pilot Project
Prepared By
Oregon Lions Sight & Hearing Founda on
For
Oregon Department of Educa on Contract #8921 – Final Report
February 15, 2011
503‐413‐7399 or [email protected]

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
1
Vision Screening Pilot Project Summary The 75th Oregon Legislative Assembly, 2010 Special Session through House Bill 3626, directed the Oregon Department of Education (ODE) to establish a Vision Screening Pilot Project. The Oregon Lions Sight & Hearing Foundation (OLSHF), an Oregon based 501(c)(3) nonprofit, was awarded Contract #8921 and provided the following objectives:
Arrange and conduct vision screenings in three Oregon school districts
Screen all students in grades one through eight in those districts
Provide parents or guardians of students an “opt out” option for the vision screenings
Conduct background checks on all staff and volunteers
Establish a system of documentation and tracking of:
o the school districts where vision screening occurred
o number of students screened and the results of those screenings
o which grades were screened
o the number of students who, based on the vision screenings, were:
referred to an ophthalmologist or an optometric physician for an eye exam;
identified as requiring vision correction or treatment; and
provided vision correction or treatment
The estimated cost for the students who received vision screenings
Make recommendations for how to fund and implement statewide a program that provides students with vision screenings
Submit an Interim Report due by December 1, 2010 providing an update on the progress of the Vision Screening Pilot Project
Provide a final written report, no later than February 15, 2011, with information requested to be reported to the Legislature as part of HB 3626
Since 1959, the Oregon Lions Sight & Hearing Foundation has provided vision and hearing related services to those in need. In 1994, OLSHF created a health screening program designed to identify vision and hearing impairment. The program’s mission was to provide access to resources for vision and hearing care in rural and underserved areas of Oregon. Initially focused on adults, school based vision and hearing screenings now represent over 86% of all OLSHF screening events. OLSHF provides vision screenings to over 25,000 children and 5,000 adults annually throughout the state of Oregon. It is the largest program of its kind in the state.

OLSHF restudentssocial anchild modevelopmoutlook f
Experts Howeveractually screeningeyeglasse
In the OrSight & HidentifyinperformaOregon sClubs, OrOLSHF coreferred
Thank yo
Or
ecognizes thwith visual d emotionaore opportument, the eafor correctio
estimate vir, research shave themgs, an alarmes.
regon DeparHearing Founng students ance. OLSHFschool distriregon Healthoordinated sfor eye exam
ou for this op
regon Depart
e importancimpairmentl developmeunity for edarlier vision ion or improv
sion probleshows that . Even wheming 40% to
rtment of Edndation (OLSthat may h
F provided victs from Seh & Science screenings amination. OL
pportunity.
tment of Educ
Febr
ce of vision sts. Visual prent of childreducational simpairmentsvement of th
ems affect 2only 10% o
en children o 67% do n
ducation (ODSHF) has prohave vision vision screenept. 13 throuUniversity’sand follow‐uLSHF provide
cation Contra
ruary 15, 2011
screening prroblems can en. Early detsuccess. Becs are diagnohe child’s we
25% of all of children 9with vision ot receive
DE) Vision Sovided an evproblems t
ning for 6,82ugh Nov. 19s Casey Eye Ip contact wes the follow
act #8921 – Fi
rograms in sc and do affetection of vicause visionosed and treaell‐being.
school chil9 to 15 yeaproblems recommend
creening Pilvidence‐basethat interfer23 school ch9, 2010. WoInstitute andwith the parewing final rep
inal Report
chools to asect the physision problen loss may ated, the mo
dren in thers old who are identifided follow‐u
ot Project, ted, cost‐effere with learhildren in graorking with pd Prevent Blents or guarport to ODE.
sist in identsical, intellecms can provimpede no
ore favorabl
e United Stneed eyegled during vup eye exam
the Oregon ective methorning and scades 1 to 8 partners at indness Amerdians of chi.
2
ifying ctual, vide a ormal e the
tates. asses vision ms or
Lions od for chool in six Lions erica, ldren

Detailed
1. T
The scho
Lincoln C
and Unio
screening
of childre
OLSHF w
eight usi
complete
the follow
Klamath
Bonanza
Bonanza
Brixner J
Chiloquin
Chiloquin
Falcon H
Ferguson
Or
d Findings
he School D
ool districts
County Scho
on School D
gs for childr
en in Oregon
was tasked to
ng space w
ed all screen
wing 37 scho
County Sch
Elementary
Jr/Sr
r
n Elementar
n Jr/Sr
eights
n
regon Depart
s of Object
Districts Whe
where visio
ol District, C
District. OLSH
ren. Public sc
n.
o screen the
within each s
nings as defi
ool locations
ool District
y
y
tment of Educ
Febr
ives
ere Vision Sc
on screenin
Cove School
HF understa
chools prov
e vision of a
school facilit
ned by Cont
s in Oregon:
Gearhart
Gilchrist E
Gilchrist J
Henley Ele
Henley M
Keno
Lost River
cation Contra
ruary 15, 2011
creenings Oc
gs occurred
District, Elg
ands that sc
ide an oppo
pproximatel
ty where po
tract #8921
Elementary
r/Sr
ementary
iddle Schoo
r Jr/Sr
act #8921 – Fi
ccurred
d were Klam
gin School D
chools are t
ortunity to sc
ly 7,000 stud
ossible. On
for the Visi
l
inal Report
math County
istrict, Imble
the critical s
creen the la
dents in gra
November
on Screenin
Malin
Merrill
Peterson
Sage Comm
Shasta
Stearns
y School Dis
er School Di
setting for v
argest popul
ades one thr
19, 2010, O
g Pilot Proje
munity
3
strict,
istrict
vision
ation
rough
OLSHF
ect at

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
4
Lincoln County School District
Crestview Heights
Eddyville
Isaac Newton Magnet
School
Newport Intermediate
Newport Prep
Oceanlake
Olalla
Sam Case Elementary
Siletz
Taft Elementary
Taft 7‐12
Toledo Elementary
Toledo Jr/Sr
Cove School District, Elgin School District, Imbler School District And Union School District
Cove Elementary
Imbler Elementary
Stella Mayfield Elementary
Union Elementary
In order to coordinate efforts with each school district, OLSHF contacted school nurses,
principals, and other school personnel. OLSHF introduced the project and its objectives,
requested assistance with:
identifying and reserving space in each school facility,
requested class rosters and other student information,
recruiting volunteers, and
distributing an “opt out” option to each parents or guardians.
Reserving Space ‐ Each school in Klamath County School District, Cove School District, Elgin
School District, Imbler School District and Union School District was able to reserve space within
their schools for screenings to take place. Schools used gymnasiums the majority of the time.
Lincoln County School District (LCSD) was unable to provide space and requested the use of the
OLSHF screening vehicle. The space exception request was approved by the ODE prior to
screenings. In LCSD, OLSHF provided a semi‐truck and trailer on which screening stations were
set up and conducted in the same manner as the in‐school locations.
Student Information ‐ In order to track individual student results and to match those results
with follow up care, OLSHF requested student information from each district. The requested
information included student first and last name, date of birth, gender, grade, teacher, parents
or guardians name, and parents or guardians contact information. This information was
consolidated into a database and each student was assigned a unique identifier solely for the
purposes of this project. All identifying information is confidential and will be securely
destroyed per contractual requirements upon completion of the project.
Volunteers ‐ OLSHF worked with each school district and with local organizations to recruit and
train volunteers. One or two OLSHF staff was on site for set up, training, managing the
screening process, and data collection. In addition, OLSHF estimated a need for a minimum of
eight volunteers for the duration of each screening. Members of the local Lions Clubs, PTA,

school st
shift of v
OLSHF p
America
Blindness
screening
children'
Each vol
Oregon S
check pr
checks co
All volun
voluntee
removed
having t
fingerpri
Voluntee
Or
taff and OHS
ision screen
professional
(PBA) in Un
s America
gs. PBA scr
s eye care p
unteer who
State Police
ocess. In all,
onducted th
teers who w
er for the pr
d for a DUI fr
their dog o
nted backgr
ers Cleared i
regon Depart
SU nursing s
ing at one o
screening s
nion County
has a nati
reening proc
rofessionals
o participate
or was verif
, OLSHF clea
hat returned
were found t
oject. To be
rom their di
off of the
ound checks
in Backgrou
tment of Educ
Febr
students, we
or more scho
staff coordi
y School Dist
onal progra
cedures are
s and researc
es in the pr
fied to have
ared 163 vol
an “In Proc
o have an “I
e clear, these
stant past a
leash. In a
s through th
nd Checks
cation Contra
uary 15, 2011
ere asked to
ools.
nated volun
trict and in
am that tr
e recommen
chers.
oject under
e gone throu
lunteers. Th
cess” result,
n Process” r
e were not
and another
addition, al
e Oregon St
act #8921 – Fi
1
o volunteer f
nteer traini
Lincoln Cou
ains and c
nded by ma
rwent a bac
ugh a specifi
ere were an
meaning th
result were i
criminals. Fo
was remove
ll OLSHF st
tate Police D
inal Report
for no less t
ngs with Pr
unty School
certifies peo
any of the
ckground ch
ic school dis
n additional
hat a record
informed th
or example,
ed based on
taff passed
Department.
han a three
revent Blind
District. Pre
ople to con
nation's lea
heck through
strict backgr
four backgr
had been fo
at they coul
one person
n a convictio
comprehe
5
hour
dness
event
nduct
ading
h the
round
round
ound.
d not
n was
on for
ensive

2
“Opt Ou
screening
about th
T
“o
T
2. The num
6,823 stu
further e
16 years)
Summary
Student a
being scr
Students
Or
ut” ‐ Schoo
g. Only four
e “opt out”
he form was
opt out” opt
he form was
o One p
screen
conta
mber of stude
udents rece
eye examina
).
y of Student
absenteeism
reened in the
s Absent/No
regon Depart
ls were pro
r of the for
letter includ
s redundant
tion that inc
s confused a
parent was re
ning when th
ct clarified t
ents who re
ived vision
tions (16.5%
ts Screened
m among oth
e six school
ot Screened
tment of Educ
Febr
ovided a fo
rms were re
ded:
as schools r
ludes screen
as an “opt in”
eported to h
hey had sign
he parent’s
ceived visio
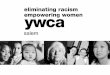
screening. 5
%). This is co
: Vision Pass
her factors re
districts.
by School D
cation Contra
uary 15, 2011
rm to be s
eturned and
reported tha
nings such as
” by a small
have said the
ned and subm
intent and t
on screening
5,698 passe
onsistent wit
sed and Refe
esulted in ap
District
act #8921 – Fi
1
sent home
d collected.
at student en
s vision scre
number of p
ey were exc
mitted the “
the student w
gs
ed (83.5%) a
th prior OLS
erred by Sch
pproximately
inal Report
with each
Feedback f
nrollment fo
eenings; and
parents or g
ited for thei
“opt out” for
was able to
and 1,125 w
HF screenin
hool District
y 804 (10.5%
student prio
rom school
orms include
guardians.
r child’s visio
rm. The scho
be screened
were referre
gs (over the
t
%) students
6
or to
staff
ed an
on
ool
d.
ed for
e past
not

3. T
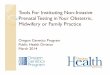
Overall V
See Lesso
the three
Or
he number
a. Refer
exam
Vision Refer
ons Learned
e smaller sch
regon Depart
of students
red to an op
ination
rals By Scho
and Conclu
hool districts
tment of Educ
Febr
who were
phthalmolog
ool District
sions on pag
s listed in the
cation Contra
uary 15, 2011
gist or an op
ge 21 for an
e chart abov
act #8921 – Fi
1
ptometric ph
analysis of t
ve.
inal Report
hysician for
the significa
an eye
nt differenc
7
es in

Overall V
Or
Vision Refer
regon Depart
rals by Scho
tment of Educ
Febr
ool
cation Contra
uary 15, 2011
act #8921 – Fi
1
inal Report
8

Accordin
successfu
above. F
standard
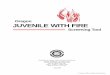
First grad
screened
Figure 1
Screener
“critical
helped th
have cor
Screener
repeated
based on
based on
Referrals
Note that th
are not capa
Or
i.
g to curren
ully pass the
irst graders
ds. The line t
ders were sc
d using a HO
1 ‐ Example o
rs selected o
line”. This g
he eye adjus
rrectly ident
rs first teste
d the proces
n Distance V
n the Distanc
s based on D
he total screene
able of completi
regon Depart
The numb
t medical st
e Distance Vi
below six y
that a stude
creened usin
TV chart.
of LEA Symb
one symbol
gave younge
st to the fon
ified at leas
ed the right
ss for the le
Visual Acuity
ce Visual Acu
Distance Visu
ed for Distance V
ing an individual
tment of Educ
Febr
ber of studen
tandards, th
isual Acuity
ears of age
nt must suc
ng a LEA Sym
bols and HOT
or letter fro
er children
nt becoming
st four out o
eye (while
eft eye. The
y. Of the 6,7
uity screenin
ual Acuity b
Visual Acuity is s
l portion of the s
cation Contra
uary 15, 2011
nts referred
he vision cha
screening is
were tested
ccessfully rea
mbols chart a
TV Distance
om each lin
practice at
g smaller on
of five of th
the left eye
e following c
770 student
ng.
y School Dis
slightly lower th
screening (for ex
act #8921 – Fi
1
for Distanc
art line the
20/30 for st
d to the 20/
ad at is refe
and second t
e Vision Scre
e of the cha
identifying
the chart. T
he symbols o
e was “occlu
chart shows
ts screened,
strict
han the total ove
xample, languag
inal Report
e Visual Acu
child must
tudents that
/40 line acco
erred to as t
through eigh
eening Chart
art on the w
the symbo
To pass a lin
or letters at
uded” or bl
s referrals b
, 698 (10.3%
erall screened b
ge barriers or sp
uity problem
read in ord
t are ages six
ording to cu
the “critical
hth graders
ts and Scree
way down to
ls or letters
e, the child
t the critical
ocked) and
by school di
%) were refe
because some st
ecial needs stud
9
ms
der to
x and
urrent
line”.
were
ening
o the
s and
must
line.
then
istrict
erred
tudents
dents.)

Referrals
Or
s based on D
regon Depart
Distance Visu
tment of Educ
Febr
ual Acuity b
cation Contra
uary 15, 2011
y Individual
act #8921 – Fi
1
l Schools
inal Report
10

In additio
problems
age child
reverse a
academic
problems
Amblyop
students
screening
and untr
The follo
Of the 6,
Referrals
Note that th
capable of c
Or
ii.
on to the ne
s for a child
dren in Am
amblyopia. If
c achieveme
s leading to
pia is detect
are using b
gs focuses o
eated, ambl
Figure 2
owing chart s
782 student
s based on S
he total screene
completing an in
regon Depart
The numb
problems
eed for pres
d is amblyop
erica suffer
f it is not rev
ent. A child
o socioecono
ed through
both eyes to
on identifyin
yopia can le
‐ Example o
shows stude
ts screened,
Stereo Vision
ed for Stereo Vis
ndividual portion
tment of Educ
Febr
ber of studen
scription eye
pia (also kno
from ambl
versed, perm
d with amb
omic disadv
Stereo Visio
ogether effe
ng eye cond
ead to perma
of the "3D" c
ent referrals
534 (7.87%)
n Screening
sion is slightly lo
n of the screenin
cation Contra
uary 15, 2011
nts referred
eglasses, on
own as “lazy
lyopia. Early
manent impa
lyopia may
antages and
on screening
ectively usin
ditions such
anent vision
cards used f
by school d
) were refer
by School D
ower than the t
ng (for example,
act #8921 – Fi
1
for Stereop
e of the mo
y eye”). Thre
y detection
airment may
then exper
d a significa
g. The Stere
ng “3D” card
as amblyop
loss.
for the Stere
district based
red based o
District
otal overall scre
language barrie
inal Report
psis or depth
ost pervasive
ee to four p
and treatm
y result lead
rience othe
antly reduce
eo Vision scr
ds. Primarily
pia. As state
eopsis Scree
d on Stereo
n Stereo Vis
eened because s
ers or special nee
h perception
e but overlo
percent of sc
ment can us
ding to decre
r developm
ed quality of
reening che
y this part o
ed, if undete
ening
Vision scree
sion screenin
some students a
eds students.)
11
n
ooked
chool
sually
eased
mental
f life.
cks if
of the
ected
ening.
ng.
are not

Referrals
Or
s based on S
regon Depart
Stereo Vision
tment of Educ
Febr
n Screening
cation Contra
uary 15, 2011
by Individua
act #8921 – Fi
1
al Schools
inal Report
12

Student v
appeared
further c
A
o
B
sq
C
u
The follo
Complain
ABCs of s
Referrals
Note that th
completing
Or
iii
vision scree
d, behaved,
are.
Appearance s
r infection, o
ehaviors ca
quinting or f
omplaints ca
nusual sensi
owing chart
nts screenin
screening.
s based on A
he total screene
an individual po
regon Depart
. The numb
(ABCs)
ning began
or complai
signs can inc
or possible i
n include a
frowning, or
an include h
itivity to ligh
t shows ref
g. Of 6,762
Appearance/
d for ABCs is slig
ortion of the scre
tment of Educ
Febr
ber of studen
with Appea
ned of a vis
clude crosse
njury.
rigid body,
excessive b
headaches, b
ht.
ferrals by sc
total studen
/Behavior/C
ghtly lower than
eening (for exam
cation Contra
uary 15, 2011
nts referred
rance/Behav
sion or eye
ed eyes, wat
thrusting h
linking.
blurred or do
chool distric
nts screened
Complaints (
n the total overa
mple, language b
act #8921 – Fi
1
for Appeara
vior/Compla
problem, th
tering or red
head forwar
ouble vision,
ct based on
d, only 265
(ABCs) by Sc
ll screened beca
barriers or specia
inal Report
ance/Behav
aints screen
he student
d eyes, droo
d or backwa
, burning or
n Appearan
were referr
chool Distric
ause some stude
al needs student
vior/Compla
ings. If a stu
was referre
oping eyelid,
ard, tilting h
scratchy eye
nce / Behav
red based o
ct
ents are not cap
ts.)
13
aints
udent
ed for
sties
head,
es, or
vior /
n the
pable of

Referrals
Or
s based on A
regon Depart
Appearance/
tment of Educ
Febr
/Behavior/C
cation Contra
uary 15, 2011
Complaints (
act #8921 – Fi
1
(ABCs) by In
inal Report
ndividual Schhools
14

As part
PediaVisi
used to
measure
Accordin
Plusoptix
deploym
referral t
additiona
Summary
The $10,
time that
it has dif
and Hisp
device is
language
of childr
them. It
anything
technolo
manual s
to refer t
3. T
Students
guardian
received
student
families
detected
attempte
Or
iv.
of the Visio
ion Plusoptix
take a digi
ments from
g to doctor
x camera in
ent in a wid
to an eye c
al screening
y of the Res
000 PediaVi
t make it a l
fficulty meas
panic eyes) a
s particular
e barrier ma
en. The Ped
is completel
other than
ogy, we foun
screening. M
them anywa
he number
b. Identi
s referred fo
s that detai
a “Refer” fo
in for a com
that might
d a total of
ed to contac
regon Depart
Students a
on Screenin
x SO9 autor
tal image o
the image t
rs at Queen’
n detecting
despread sch
care special
was used to
sults of Pedia
sion photo s
less attractiv
suring the p
and may no
ly attractive
kes it more
diaVision de
ly objective
n open their
nd that the d
Many more c
y based on o
of students
ified as requ
or comprehe
iled the resu
or any of the
mprehensive
require fina
f 1125 stud
ct each hom
tment of Educ
Febr
also screene
g Pilot Proj
efractor. Th
of the stude
to indicate t
’s University
amblyopiog
hool screen
ist can be m
o double che
aVision Scre
screener OLS
ve option fo
upil when a
ot be effectiv
e, however,
difficult for
evice takes a
and does no
r eyes and r
device was c
children pas
our tradition
who were
uiring vision
ensive eye e
ults of the s
e screenings
e eye exam
ancial assist
ents who w
me three tim
cation Contra
uary 15, 2011
ed with Pedi
ject, OLSHF
is objective,
ents’ eyes.
he presence
y, Kingston,
genic factor
ing program
made at th
eck the resul
eenings
SHF purchas
r school scre
child has da
ve when us
, when scre
the screene
a digital pic
ot require th
remain still.
calibrated at
sed the Ped
nal screening
correction o
exams were
screenings (s
s, parents or
m. OLSHF’s c
ance with a
were referre
mes when it
act #8921 – Fi
1
iaVision Plus
screened 3
, non‐invasiv
The compu
e of a variety
Ontario, Ca
rs appears
m. Immediat
e time of t
lts of the ma
sed for this p
eenings. The
ark irises (in
sed under h
eening pre‐
er to commu
cture of a p
he screener o
In our first
t a very diff
diaVision do
g protocols.
or treatmen
provided a
see page 2
r guardians w
contact info
an eye exam
ed for a co
had a telep
inal Report
soptix autor
395 student
ve compute
ter softwar
y of eye and
anada, “The
sufficiently
e determina
the screenin
anual screen
project has l
e device is n
n particular A
alogen type
‐verbal child
unicate with
person’s eye
or child bein
t attempt a
ferent bar th
uble check
nt
referral lett
of Appendix
were encour
rmation wa
m and/or ey
omprehensiv
phone for th
refractor
ts vision us
rized system
re processed
vision prob
e accuracy o
high to fu
ation of nee
ng process.”
ning process
imitations a
not ideal bec
African Ame
e light bulbs
dren or wh
h a child or g
es and diagn
ng screened
t using this
han our stan
but OLSHF c
ter to paren
x A). If a stu
raged to tak
s also note
yeglasses. O
ve exam. O
hat househo
15
ing a
m was
d the
lems.
of the
urther
ed for
” This
.
at this
cause
erican
. The
hen a
group
noses
to do
new
ndard
chose
nts or
udent
ke the
d for
OLSHF
OLSHF
old. It

also used
follow up
Summary
Summary
Of those
schedule
During d
errors of
passed o
able to r
the follow
form was
21 for an
Summary
OLSHF p
eye exam
only 101
eye exam
were dis
require
Or
d email or m
p contact wit
y of Parents
y of Parents
households
ed.
ata collectio
f a total of
or incorrectly
review each
w up proces
s sent home
n analysis of
y Totals of I
i.
rovided 400
m using OHS
consent for
m. The eye e
tributed by
financial as
regon Depart
mail when a
th 51.9% of
s or Guardia
s or Guardia
s contacted,
on, OLSHF w
6823 scree
y referred. L
student’s re
ss, OLSHF co
e with docum
documentat
dentified Do
The numb
by Casey E
0 randomly s
SU’s Casey
rms (see App
exams were
OLSHF to p
ssistance. Th
tment of Educ
Febr
telephone n
households
ns Follow U
ns Reported
over 50% re
was able to
ened. A sma
Less than in
esults form
ontacted pa
mentation er
tion errors.
ocumentatio
ber of studen
Eye Institute
selected stu
Eye Institut
pendix B) we
offered free
parents or g
he exams w
cation Contra
uary 15, 2011
number was
whose child
p Effort and
d Exam Statu
eported that
specifically
all percenta
nitially prese
to identify a
rents or gua
rrors. See Le
on Errors
nts referred
e staff
dents the o
e medical p
ere returned
e of charge a
guardians alo
were perfo
act #8921 – Fi
1
s not availab
dren were re
d Response R
us
t an eye exam
identify and
ge of stude
ented in the
actual docu
ardians of th
essons Learn
d for a comp
opportunity
professionals
d giving OLS
and results,
ong with a
rmed by C
inal Report
ble. OLSHF w
eferred for e
Rate
m had occur
d correct 94
ents (1.4%)
e Interim Re
mentation e
hose studen
ned and Con
prehensive d
for a compr
s and techn
HF permissi
as well as a
resource lis
Casey Eye I
was able to m
eye exams.
rred or was b
4 document
were incorr
port, OLSHF
errors. As pa
nts whose re
nclusions on
dilated eye e
rehensive di
nicians. Of t
on to condu
any prescript
t should fam
nstitute me
16
make
being
tation
rectly
F was
art of
esults
page
exam
ilated
hose,
uct an
tions,
milies
edical

professio
Lincoln C
The Case
this proje
that in 6
student w
on page
Summary
3. T
Of the h
them dur
Summary
4. T
The estim
$15.93 p
per stud
methodo
accounte
The actu
OLSHF’s
Vision Sc
involved
Or
onals and te
County Schoo
ey Eye Instit
ect accurate
cases a stu
was referred
21 for an an
y of Casey E
he number
c. Provid
ouseholds c
ring their co
y of Parents
he estimate
mated cost
per student.
ent cost. Ne
ology for sc
ed for a cons
al cost to sc
current me
creening Pilo
in running a
regon Depart
echnicians o
ol District. Ex
tute exam re
ely passed o
dent was pa
d and no vis
alysis of the
Eye Institute
of students
ded vision co
contacted, 3
omprehensiv
s or Guardia
ed cost per s
per studen
However, v
ew equipme
creening, fol
siderable pe
reen per stu
thod. This c
ot Project de
a nonprofit o
tment of Educ
Febr
on site at T
xams occurr
esults demo
r referred a
assed when
sual impairm
ese results.
Exam Resu
who were
orrection or
33.9% report
ve eye exam.
ns Reported
student for t
nt screened
vision screen
ent (PediaV
llow‐up call
rcentage of
udent (witho
cost does no
etailed above
organization
cation Contra
uary 15, 2011
Taft, Toledo,
red on Decem
onstrate that
student at
a visual imp
ment existed
lts
r treatment
ted that a p
.
d Prescriptio
the students
for the OLS
ning actually
ision Plusop
s to parent
the $15.93 p
out the study
ot include s
e. This figure
.
act #8921 – Fi
1
, and Sam
mber 3 and
t the manua
least 76% of
pairment did
d. See Lesso
prescription
on Status
s that receiv
SHF Vision
y accounted
ptix photo s
ts, follow‐up
per student
y) is approxi
services pro
e does includ
inal Report
Case Eleme
10, 2010.
al screening
f the time. T
d exist and 1
ons Learned
for eyeglas
ved vision sc
Screening P
d for only pa
screener), te
p eye exam
cost howev
imately $10
ovided by th
de all allocat
entary schoo
g process us
The exams f
18 cases wh
and Conclu
ses was give
creenings
Pilot Project
art of the $1
esting the O
ms and repo
er.
per student
he OLSHF fo
ted indirect
17
ols in
ed in
found
ere a
usions
en to
t was
15.93
OLSHF
orting
t with
or the
costs

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
18
Conclusions
5. Recommendations for how to fund and implement statewide a program that provides students with vision screenings
Oregon has mandated that school districts screen the vision and hearing of school children for many years but the regulation is neither well defined nor enforced consistently throughout the state. The state mandates vision and hearing screening as part of several other health care regulations regarding schools but it does not provide funds for school districts to provide these services.
“581‐022‐0705 Health Services:
(1) The school district shall maintain a prevention oriented health services program for all students which provides:
(f) Vision and hearing screening;
Stat. Auth.: ORS 326 & ORS 342 Stats. Implemented: ORS 326.051 Hist.: 1EB 19‐1980, f. 6‐17‐80, ef. 9‐1‐80; 1EB 16‐1981 (Temp), f. & ef. 11‐3‐81; 1EB 12‐1982, f. & ef. 3‐24‐82; EB 21‐1988, f. & cert. ef. 4‐26‐88; EB 17‐1996, f. & cert. ef. 11‐1‐96”
In 1996, the nonprofit Oregon Lions Sight & Hearing Foundation began offering these services free of charge to schools in areas where Lions Clubs existed. This program has grown to the largest screening program in Oregon serving over 25,000 school children and 5,000 adults per year. The screenings are provided by paid staff coordinating lay volunteers, primarily Lions Club members.
It is important to recognize that a vision screening is different from a comprehensive exam by an eye care professional. Screening covers a baseline of important vision functions often including distance visual acuity, stereo vision as well as appearance, behavior and complaints. It may also cover near visual acuity. Results of a vision screening are used to assess whether a child needs to see an eye doctor. A comprehensive exam involves much more. In a full exam, a patient’s eyes would usually be dilated so an eye care professional can look inside the eye as well. According to Prevent Blindness America, a comprehensive eye examination includes an evaluation of the refractive state, dilated fundus examination, visual acuity, ocular alignment, binocularity, and color vision testing, where appropriate. An optometrist or ophthalmologist may check for additional eye problems including glaucoma, etc.
Only an eye doctor can diagnose and treat visual impairment, but vision screenings help find children who need a full eye exam. Children's vision screenings are an accurate, cost‐effective way to identify visual impairment in children. Children who need a full eye exam are referred to an eye doctor of the parent's choice.

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
19
Lessons Learned and Conclusions
1. A summary of results from the Vision Screening Pilot Project shows that:
a. 89.5% of children in grades one to eight in six school districts were screened
iv. 10.5 % of children were absent or not screened
b. 16.5% of children were referred over all for follow up exams (some children
were referred for more than one issue so the percentages below do not add up
to 16.5%)
c. 10.3% of children were referred for distance visual acuity
d. 7.9% of children were referred for stereo vision
e. 3.9 % of children were referred for ABCs (Appearance/Behavior/Complaints)
f. Parents or guardians reported 50.7% of the time the screening referral prompted
them to attend or schedule a comprehensive exam for their child
g. Based on parents or guardians reporting, 33.9% of the households contacted
report their child received a prescription for or obtained eyeglasses
2. Where possible, schools or the organization screening students should mail screening results home to parents or guardians instead of sending results home with the child usually in their backpacks. Children who do not pass the vision screening may not want to share the information with their parents out of fear that they “failed” or not wanting to go to the doctor or get eyeglasses. 21.1% of the parents or guardians OLSHF was able to contact reported they did not receive a copy of the screening results form. Too many results forms do not get to the parent or guardian if they are sent home with the child, and the child does not get the appropriate follow up vision examination or care. Vision screenings take time and money, approximately $10 per child in fact. The cost of an envelope and stamp may be the most important expenditures to make vision screening more effective.
3. The Vision Screening Pilot Project allowed OLSHF to evaluate its own screening process from top to bottom. During the project, OLSHF discovered an error rate of approximately 1.4% that the organization never knew it had. The mistakes are primarily human error when documenting the results of screening on paper forms. The screener may accidentally circle “pass” when they meant to circle “refer” or vice versa. These forms are later sent home to parents who may make decisions based in inaccurate information. OLSHF is told that the rate of error is typical and to be expected when using lay volunteers for vision screenings. However, OLSHF intends to do everything it can to improve these results. The error rate can be reduced by a simple quality control process that OLSHF is implementing. At the end of the screening day, the screening coordinator will go through every form to make sure the lay screeners filled them out correctly before they are sent home via the school administration. The coordinator will find a quiet place to take this final important step before completing the screening. OLSHF is also reviewing its forms to see if revisions can make the process more clear to volunteer screeners.

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
20
4. OLSHF can screen a student’s vision in approximately three to five minutes. With three “lanes” of screening, it can screen approximately 45 children an hour. In six hours of near nonstop screening, it can screen approximately 270 children in less than one school day. With additional volunteers, OLSHF has screened 400 students in one school day. This level of efficiency takes one lead person on site to train and coordinate the screening and at least 12 other volunteers to perform screening.
5. The lower referral rates at Union, Imbler and Cove School Districts are based on much smaller data sets. OLSHF and Children’s Vision Foundation (CVF) screened children at these schools for at least the past two years; however, that does not explain the significant difference in overall referral rates. OLSHF and CVF also screened recently in nearby Elgin School District which had higher referral rates, similar to the larger school districts, and OLSHF has screened in the past few years in the Lincoln and Klamath School Districts, where the rates were higher. While OLSHF cannot determine the reasons for the lower referral rates in Union, Imbler and Cove School Districts, the smaller data sets make these anomalies statistically unreliable.
6. For the Distance Visual Acuity screening, there are many methods to occlude or block vision in one eye while testing the other. Children naturally want to pass any “test”. It is very important that a child is not allowed to “peek” or see around the occluding device when the other eye is being tested. Some organizations recommend that occlusion be done with medical tape to completely cover the eye, but OLSHF found that this method was impractical when attempting to screen large quantities of school children in an efficient process. Alternately, OLSHF used a simple and inexpensive paper condiment cup. To avoid peeking, a child is asked to hold the cup over one eye with their hand over the cup so it is more difficult to peek. It is essential that the screener watch the child carefully so the child does not peek. To test these two methods, OLSHF used medical tape in Lincoln County School District (LCSD) and paper cups in Klamath County School District (KCSD). The distance visual acuity referral rate in LCSD was 10.71% and the referral rate in KCSD was 10.42%. Although a direct correlation cannot be drawn (there were different volunteer sets at each as well), it is of note that when the tape was used and that less children were able to peek, 0.29% more children were referred for eye exams. Since the difference was statistically irrelevant, OLSHF concluded the process of using the medical tape is too cumbersome and inefficient to recommend for large scale school screenings with lay volunteers.
7. Obtaining parental consent for follow up eye exams presented a significant challenge. Of the 400 parents and guardians OLSHF asked to sign permission slips to provide a free comprehensive eye exam for their child, only 101 parents or guardians gave consent.
8. The OHSU Casey Eye Institute exam results demonstrate that the manual vision screening process used in this project accurately passed or referred a student at least 76% of the time. The exams found that in 6 cases a student was passed when a visual impairment did exist and 18 cases where a student was referred and no visual impairment existed. There were three times more “false positives”. In screening, it may be better to be safe than sorry. The OHSU exam results also highlight the difference

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
21
between vision screening and examinations. For example, in screening, OLSHF might refer a student for red and watery eyes, but an examination might determine the cause to be allergies not visual impairment. An examination also looks for vision issues that student screening is not designed to detect such as glaucoma. The exams found three cases of suspected glaucoma, interestingly each of those students was correctly referred for an exam. The exam results also highlighted the need to potentially add Near Visual Acuity screenings to the recommended screening method. Four of the six cases where OLSHF methods incorrectly passed the student during screening were found to be hyperopic, or farsighted.
9. The PediaVision photo screener OLSHF purchased for this Pilot Project has limitations at this time that make it a less attractive option for school screenings. The device is not ideal because it has difficulty measuring the pupil when a child has dark irises (in particular African American and Hispanic eyes) and may not be effective when used under halogen type light bulbs. The device is particularly attractive, however, when screening pre‐verbal children or when a language barrier makes it more difficult for the screener to communicate with a child or group of children. The PediaVision device takes a digital picture of a person’s eyes and diagnoses them (see Appendix C). It is completely objective and does not require the screener or child being screened to do anything other than open their eyes and remain still. OLSHF plans to monitor this technology as it develops in the future and would be glad to demonstrate this device to ODE and legislators if an opportunity is provided.
10. For 16 years, OLSHF provided screening in two 64 foot tractor trailer trucks that obtained approximately 6 miles per gallon and required a coordinator who could drive a truck, as well as work well with children. For the Vision Screening Pilot Project, OLSHF compared the use of new vision screening kits that bring all the necessary equipment into the school for screening. The school must provide a dedicated space for vision screening such as the school gym, auditorium or multi‐purpose room. OLSHF found that the needed equipment can be transported in much more fuel efficient cars and that the lead staff person would not need to know how to drive a truck. This model is much less expensive and will allow OLSHF to screen in many more locations on the same day. This successful debut of the vision screening kit system has led OLSHF to develop a 2020 Vision Capital Campaign to revamp the entire program using this new model. To compare results, in Lincoln where a truck was used (see page 4 above for explanation), 18.8% of children screened were referred for follow up eye exams. In Klamath where kits were used in school buildings, 16.8% of children screened were referred for follow up eye exams. There is no clear explanation for the 2% difference in referral rates; however, screening is much more cost effective using kits inside schools. This new model will allow OLSHF to decrease its cost per student to provide screenings. In addition, there are advantages to keeping school children in the school environment where they are comfortable and more relaxed. In order to make this model work, schools will need to provide space for screenings.
11. OLSHF attempted to contact the parents or guardians of all 1,125 students referred for follow up vision exams. When appropriate, OLSHF used a native Spanish speaker to

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
22
make follow up calls to Spanish speaking households. Parents or guardians reported 50.7% of the time the screening referral prompted them to attend or schedule a comprehensive exam for their child. 33.9% of the households OLSHF was able to contact reported receiving a prescription for eyeglasses.
12. While some people were suspicious, most parents we spoke to were grateful for the follow up contact.
Here is one example: “Baylee was seen by an eye doctor on 1‐5‐11 to follow up on the results of her screening. Thank you for the follow up email and for the efforts you put into our community. Best Regards, Melissa Dieckhoff (her mom)”
Here is another example: “Thank you for the eye exam. I had no idea my daughter’s vision was bad. I had her examined and she’s already got her new glasses. Hopefully her reading will improve now. Teresa Erickson (Breana Erickson’s mom)”

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
23
Recommendations
1. Oregon should adopt regulations that set a minimal baseline to define vision screening based on the Prevent Blindness America model. Any methodology should include: Appearance/Behavior/Complaints, Distance Visual Acuity and Stereopsis screenings. A minimal standard would help create consistency in vision screening in the state. As an example, one very large school district that currently screens its own students through an Educational Service District (ESD), does not include stereo vision, potentially missing amblyopia in hundreds or even thousands of children each year.
2. Standards should define (1) methodology, (2) frequency and grades of children screened, (3) visual functions assessed, and (4) criteria for referral to an eye care professional.
3. As it may be impractical to screen every student in every grade every year, a minimum standard should require schools to screen students in kindergarten, first, third and fifth grades. This approach would allow for detection of solvable vision impairments at younger ages and help children to achieve educational success from the start. With amblyopia, the impairment must be detected and treated before age 10 or it is not treatable most of the time and the child loses vision in the affected eye. Amblyopia is a significant reason to screen children while they are younger.
4. The standard adopted should set minimum expectations for screening rather than perfect conditions so screening does not become too expensive for nonprofit organizations and school districts to perform. Several other states have set standards for vision screening (see Prevent Blindness America website for a list of all state regulations).
5. A state methodology should allow the screening organization or school district to add but not require near visual acuity to the screening process.
6. OLSHF recommends vision screening should test for stereopsis using the Random Dot E method. The Random Dot “E” screening is the only method recommended by Prevent Blindness America and Casey Eye Institute. This study found that this method is faster, less expensive and more effective than the Lang model that was previously used by OLSHF.
7. The focus of this project was only vision screening, but OLSHF recommends the state of Oregon consider hearing screenings for school children. Hearing is certainly important in a learning environment and it is equally mandated in Oregon regulations cited above in this report. There may be economies of scale to perform these screenings together. In a recent Portland Public School, MESD, OLSHF, Walmart and Prevent Blindness America partnership at seven schools, children had their vision, hearing and teeth screened at the same time.
8. Private nonprofit and other screening organizations face a major challenge helping school districts provide screening due to lack of access to follow up contact information

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
24
for the parents or guardians of children screened. When a student is referred for follow up examination, the screening organization should contact the parent or guardian to make sure they got the results form (preferably mailed) and ask if parents have questions or need assistance getting their child seen by an eye care professional. Schools, however, are hesitant to share parent data with outside organizations due to concerns about Family Educational Rights and Privacy Act (FERPA), Health Insurance Portability and Accountability Act (HIPAA) and the right to privacy. Unfortunately, schools often do not have the capacity, whether administrative personnel or school nurses, to do follow up with the parents of referred students. The result is a lack of follow up. OLSHF is often asked by potential funders how we follow up with parents of children who need further assistance. Direct follow up contact with parents is a key factor in the success of screening programs. Follow up is currently stymied by other legitimate interests such as the expectation of privacy. Unfortunately, a form requesting parental “consent to contact” them are not an easy answer since so many parents do not return these forms. Schools could address this issue by including a comprehensive waiver as part of their enrollment process allowing certain partner organizations to contact parents directly for healthcare reporting. In some ways, this is similar to the partnership between schools and PTAs. A qualified partnering organization would sign an agreement with the school or district that private information could only be used for legitimate reasons and never sold, traded or given away. Confidential information could be treated as such under established guidelines and data could also be destroyed after a certain period of time.
OLSHF recognizes the difficulty of resolving this problem. However, when contracting with ODE on this project, most school districts treated OLSHF as a partner and after some initial hesitation, shared data with OLSHF. In this instance, the contract between OLSHF and ODE gave the school districts an assurance that it was appropriate to share data. Perhaps ODE could create permanent nonprofit partners for this purpose going forward. OLSHF would be interested in contracting with ODE and school districts even when it is providing screening services free of charge to help overcome the problem of follow up.
Currently, OLSHF uses a triplicate results form with one copy going to parents, one to the school and one to our office so we can compile anonymous data on screening, such as what percentage of children are referred for follow up. Often times OLSHF is provided a blank form with screening results but no other student information. Some schools do this by attaching a label to the parent and school copy but not the OLSHF copy. An alternative option would be to share a unique student identifier such as a student ID that a partner organization cannot connect to a student’s identity without the school’s assistance. Then at least each record or form would be able to be traced back to a student by the school or school district should follow be requested by the partner.
9. Many studies have shown that children who have difficulty seeing have difficulty learning. OLSHF recommends the state of Oregon and school districts allocate funds to pay for a statewide vision screening program. Nonprofit organizations such as OLSHF can fund raise for private funds but this is an inconsistent model for funding such an

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
25
important healthcare and education program. OLSHF recommends the state offer to match dollars that nonprofits raise for vision screening in public schools dollar for dollar. This would provide an effective incentive for private funders creating a public‐private‐nonprofit collaboration to make sure Oregon school children receive critical vision screenings in kindergarten, first, third and fifth grades. An annual matching fund of approximately $400,000 per year would be a major step toward making sure school children are screened.
10. The state of Oregon should focus resources on vision screening at Title 1 schools perhaps based on percentage of students receiving free and reduced school lunch. Students at traditionally underserved schools statistically have far greater numbers of children who do not have health and vision insurance.
11. Screening organizations such as OLSHF, various ESDs, Children’s Vision Foundation, OHSU Casey Eye Institute and Pacific University should meet to discuss screening methodology and consider using a common reporting form available in multiple languages. At minimum, the form should include language translation of key parts such as the designation of Pass or Refer.
12. There are several options for screening students but all of the options recommended in this report require staffing, administration and coordination. The importance of experienced staff as part of a successful screening program cannot be overlooked. This requires professionals dedicated to working with schools and students to provide high quality screening events. In the past, most schools had a school nurse who was in charge of screening school children’s vision and hearing, but in the past 30 years, the number of school nurses has been drastically reduced. Schools often share a nurse (if they have one at all) who is only at the school for a very limited amount of time. This means that the school nurse often does not have the time to coordinate the entire screening process. In some areas, Educational Service Districts (ESDs) have taken on this role. The schools themselves usually do not have adequate personnel with appropriate training to provide screening on their own. The coordinating organization or agency needs to manage location, training, equipment, scheduling, volunteers, data collection and reporting, and more.

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
26
Options for School Based Vision Screening
There are several options in a menu of how schools can screen student’s vision. Whatever options are selected by the state, must be both affordable and scalable. Here are several examples estimated from least to most expensive:
1. For approximately, $250 each, school districts can purchase a vision screening kit from Prevent Blindness America (PBA). See the online store at www.preventblindness.org. The kit would include distance visual acuity charts ($15‐50), a Random Dot E Stereopsis kit for stereo vision testing ($110), a device for covering one eye at a time, measuring tapes to measure proper distance to the charts, and a vinyl bag to carry the equipment in. OHSU’s Casey Eye Institute provides a $500 kit for Head Start programs around the state that also includes a light box along with the equipment listed above.
It should be noted that any kit should include charts for both younger, pre‐alphabet children and older children. (OLSHF recommends using a LEA Symbols chart and an HOTV chart.) One major limitation to this approach is that the PBA kit does not include an electric light box to display the charts and to ensure equal and adequate light is provided for the screening (a light box is approximately $270 with a stand and it is heavier and more fragile). Another limitation is that this kit only provides equipment and does not resolve the issue of who will coordinate the actual screening process. School nurses, ESDs and PTAs can work together with this equipment but in all likelihood someone will have to be paid to coordinate the screening and recruit volunteers or it may not get done.
2. An attractive option is for the state of Oregon and ODE to partner with nonprofit organizations to provide vision screening. Nonprofits have the advantage of being able to attract grant funding to help pay for vision screening and they attract volunteers that help keep costs low. As stated above this would be most effective in a public‐private‐nonprofit partnership. OLSHF is currently able to screen school children for approximately $10 per child or $1,000 per day using this model. One option would combine an effective nonprofit organization with adequate infrastructure and equipment and school personnel such as school nurses to help schedule school space and dates, and PTA volunteers where possible.
a. The value of volunteer labor or soft costs cannot be overlooked in the nonprofit model. In a recent application to the Ford Family Foundation, OLSHF was asked to provide a realistic estimate of the value of the volunteer labor provided each year to this program. Using the Independent Sector’s model for valuing in‐kind or volunteer labor, OLSHF estimated the value of volunteer labor at $198,396 per year for a program that serves approximately 30,000 people annually. If OLSHF had to pay for this volunteer labor, the average cost to screen one child would increase from approximately $10 per child to over $16.60 per child. While lay screening with volunteers has limitations and challenges regarding training and consistency, it can be reliable and very cost effective.

Oregon Department of Education Contract #8921 – Final Report
February 15, 2011
27
3. ODE and the Oregon Legislature could review how ESDs are providing vision screenings in certain school districts. ODE could compare the costs and methods to screen using an ESD versus a nonprofit volunteer model. The Multnomah ESD successfully uses volunteers and paid professionals, as well as retired school nurses. However, Multnomah ESD should be strongly encouraged to add a stereo vision test in its current screening method. Without this element of screening, children with amblyopia will not be detected. If not treated at an early age, these children are at risk for losing vision in the affected eye. Multnomah ESD also does not use light boxes at screenings.
4. Another option is for ODE and school districts to contract with private for‐profit professionals to provide vision screening for schools. This option is likely to be cost prohibitive, however, because a profit margin would need to be built in, and a for‐profit company could not attract grant and charitable donations to help offset the costs of screening. In addition, a for‐profit company would be unlikely to offset its costs with volunteer labor that nonprofit organizations often use to keep costs low.
5. School Districts could also purchase high tech equipment such as the PediaVision photo screener at approximately $10,000 each but the equipment requires training and maintenance. A large school district would also have to purchase more than one device to cover a larger number of schools that would need to share these devices. Scheduling and training would have to be coordinated centrally. As prices drop and these devices become smaller and easier to use, this may become a good option, but this method is not recommended at this time.
OLSHF has initiated an Oregon School District Vision Screening Survey to determine the prevalence of vision screening in Oregon schools. The survey will help determine where gaps exist. With 25% (50 of 200 Districts) reporting so far, we have the following preliminary results to report. It should be noted that the self‐reporting districts that filled out the online survey in its first week may be more likely to be providing vision screening than those school districts that have not responded. OLSHF will follow up with calls to each District and report the results of this survey to ODE by May 1, 2011. One week into the survey, OLSHF has found thus far:
62% of school districts report they are screening student’s vision
9% do not screen and 29% screen at some but not all schools in their district
67% screen hearing (a slightly higher number than vision)
Grade one students are screened the most at 79% with kindergarten students second
highest at 70%. Each year after that the percentage decreases.
Most school districts that screen vision report that they do so annually
When asked who performs the screening, 42% said the school nurse, 29% said ESD, and
29% said a nonprofit partner
When asked if the school district utilizes volunteers, 64% said yes with 35% utilizing PTA
volunteers and 29% utilizing Lions Club members.

We concsignificandilated eAiden, inthe conseAiden hasomethinexam, Aiand his mAiden’s c
OLSHF issponsoreinformatfindings aODE and
Or
clude with ant way. OLSHeye exams tonsisted multent form andad been reng wrong wden was foumother havecondition rec
s pleased ted HB 3626 ion session and answersthe legislatu
regon Depart
story aboutHF worked wo 101 studeiple times thd the schooleferred throith his visiound to have e been proviceives treatm
to provide that led to for ODE ans questions. ure’s conven
tment of Educ
Febr
t one particwith OHSU’snts in Lincohat he needl worked witough the On but he disevere glauded follow ument and his
this Final Rthe Vision Sd state legiOLSHF wounience.
cation Contra
uary 15, 2011
cular child ths Casey Eye ln County. Oded to have th staff to tryLSHF screendn’t know wcoma, a rareup support as remaining
Report to OScreening Pilslators wheuld be please
act #8921 – Fi
1
hat was helpInstitute to On the finalan exam. Hy to obtain cning proceswhat. Upone condition and resourcvision is pre
ODE. Reprelot Project, re OLSHF ped to schedu
inal Report
ped by this provide free day of examHis mother hconsent to pss and he k performingin someonee informatioeserved.
esentative Thas expressresents a suule an inform
project in ae comprehems, one stuhad not retuperform an eknew thereg the dilatede so young. Aon to ensure
Tina Kotek, sed interest ummary of tmation sessi
28
a very ensive dent, urned exam. was d eye Aiden e that
who in an these on at

Name: Teacher: VSPPID: DOB: Gender: School: Grade:

Name: Teacher: VSPPID: DOB: Gender: School: Grade:

Name: Teacher: VSPPID: DOB: Gender: School: Grade:

Please check YES and sign below if you would like your child to be considered eligible
for this free dilated eye exam.
YES, I give my consent for my child to participate in this program. (In order to participate, you must complete the medical history form on the reverse)
NO, I do not give my consent for my child to participate in this program.
Signature of parent or legal guardian Date
Questions? Please contact Brenda Anderson or Mara Steen at 1‐800‐635‐4667 or [email protected].
This is a validation eye examination and does not establish an ongoing physician patient relationship.
OREGON LIONS SIGHT & HEARING FOUNDATION AND OHSU’S CASEY EYE INSTITUTE
Dilated Eye Exam Permission Form
Child’s Name: Date of Birth: School and Classroom:
Dear Parent/Guardian,
The Oregon Lions Sight & Hearing Foundation (OLSHF) and Casey Eye Institute are offeringcomprehensive dilated eye exams at no cost to a select group of students as part of theOregon Department of Education Vision Screening Pilot Project.
The eye exam includes the use of eye drops to dilate the pupils. These drops make the pupils larger. The drops will make vision blurry and eyes sensitive to light. This is normal and will usually go away by the next day. These are tests that an eye doctor would normally do as part of an exam if your child went to an eye doctor.
The OLSHF is conducting a research study on the results of these eye exams.
If you agree to participate in this free eye exam, the results will be entered into a computer database. These results will help determine if vision screenings are effective or if they need to be changed.
The OLSHF and Casey Eye Institute will maintain the confidentiality of your child’s information in accordance with all applicable state and federal laws and regulations. Any information that could identify your child and family will not be used without your permission and will be securely destroyed upon completion of the project.
ALL INFORMATION WILL BE KEPT CONFIDENTIAL.

OREGON LIONS SIGHT & HEARING FOUNDATION AND OHSU’S CASEY EYE INSTITUTE
EYE EXAM: YOUR CHILD’S MEDICAL HISTORY
Child’s Name:_________________________________ Child’s Date of Birth:___________________________
Has your child seen an eye doctor in the past year? YES NO Eye Dr. Name____________________ Has your child ever worn glasses? YES NO For how long?____________ Has your child ever complained of pain? YES NO Where?___________ Date of onset__________ List any allergies to medications_______________________________________________________________
List all current medications, including vitamins and supplements_____________________________________
__________________________________________________________________________________________
List any surgeries____________________________________________________________________________ Was your child premature? YES NO Birth weight__________ Complications? YES NO
DOES YOUR CHILD HAVE ANY PROBLEMS IN THE FOLLOWING AREAS? Please check all that apply
YES NO
Fever, unexplained weight loss or gain, tires easily
Ear, nose, throat (hearing, sinus, ear tubes, nose bleeds, etc)
Respiratory (asthma, pneumonia)
Gastrointestinal (reflux, diarrhea, pain)
Genital, kidney, bladder (urinary infections, pain)
Skin (rashes, acne, warts, unusual birth marks)
Muscles, bones, joints (arthritis, pain, swelling, lump)
Neurological (seizures, weakness, delayed development, brain shunt, cerebral palsy)
Behavioral (hyperactivity, depression, attention deficit, unusual anxiety)
Endocrine (diabetes, thyroid, growth hormone)
Blood (anemia, high cholesterol, poor clotting)
Allergy/Immunological (hay fever, eczema, hives, autoimmune)
Other?
IS THERE FAMILY HISTORY OF ANY OF THE FOLLOWING PROBLEMS? Please check all that apply
YES NO
Crossed, wandering, or lazy eyes?
Blindness?
Need for glasses other than reading glasses?
Glaucoma?
Migraines?
Family/Hereditary disease?
Other?
10.10