Embed Size (px)
Citation preview

Attachment 6
VISION 2020 UK – 2020 and beyond: building the foundations for the future of eye healthResponses from VISION 2020 UK committee members to prioritise research questions
Background
VISION 2020 UK held a ‘2020 and beyond’ seminar on 1 June 2015. The event was chaired by the joint Chairs of the VISION 2020 UK Eye Research Committee: Michele Acton, CEO of Fight for Sight and Richard Wormald, Consultant at Moorfields and Trustee of VISION 2020 UK. There were 50 attendees from the eye health and sight loss sectors.
The objectives of the seminar included:
To reach consensus on the questions that need to be answered to ensure the sector has the evidence required to inform long-term planning and service transformation in eye health.
Prioritise the questions that need to be addressed in a programme of research, including tactical and longer-term initiatives.
The questions identified during the seminar were expected to inform a programme of research to help inform future change in eye health services. In total 97 questions were compiled. A working group on behalf of VISION 2020 UK consisting of Richard Wormald, Anita Lightstone former Chief Officer of VISION 2020 UK, Mercy Jeyasingham, CEO of VISION 2020 UK and Mike Bowen, Director of Research at The College of Optometrists edited the list by removing duplication and questions
1_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
outside the scope of service transformation. The final list is comprised of 17 questions (Appendix 1).
VISION 2020 UK committees questioned
The questions were taken to the VISION 2020 UK Social Research Committee who have added the Beyond 2020 research to their work plan. They recommended comments be gathered on the questions from other VISION 2020 UK committees.
The questions were then circulated to the following VISION 2020 UK committees asking them to prioritise 5 questions and reasons for their selected questions:
VISION 2020 UK Charities Forum Committee; VISION 2020 UK Children & Young People with a Vision
Impairment Committee; VISION 2020 UK Dementia & Sight Loss Committee; VISION 2020 UK Eye Research Committee; VISION 2020 UK Ophthalmic Public Health Committee; VISION 2020 UK Learning Disability Committee.
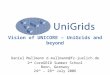
Results of prioritising questions
There were a total of 34 responses out of 152 committee members questioned. The table below shows the results for the questions prioritised by the committee members. The top five questions highlighted are as follows:
1. Question 8 – What is the relative cost effectiveness of different pathways into eye health services and what are the barriers within those pathways?
2. Question 7 – What are the true direct and indirect costs of vision impairment and severe vision impairment?
3. Question 5 – How do we improve early diagnosis for those at risk of sight loss?
4. Question 15 – What should be the care package of health and social care support offered to people with impaired vision?
2_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
5. Question 10 – What is the most cost effective service configuration for:
a) patients presenting with new ocular symptoms or visual disturbance; and
b) opportunistic detection of people with asymptomatic conditions which are a threat to eyesight?
Q1 Q2 Q3 Q4 Q5 Q6 Q7 Q8 Q9Q10
Q11Q12
Q13Q14
Q15Q16
Q170
2
4
6
8
10
12
14
16
18
20
76
89
13
8
16
18
4
1110
7
2
5
13
43
Responses for Beyond 2020 research questions
Number of responses
Research questions 1-17
Num
ber o
f res
pons
es
The comments for the questions chosen by the committee members are as follows:
Question 1 – What motivates people to have a sight test? Without this information, it will be very hard to fashion any sort of
effective intervention to encourage the uptake of sight tests. If we know what motivates some, I suspect this may inform what
could motivate others. There is not always an awareness among patients of the
association of eye health with regular eye examination. Some patients do attend regularly because they understand the ‘test’ includes examination of the inside of the eye to detect any ocular pathology, which may be symptomless, but many do not
3_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
appreciate that the signs of diseases such as diabetes may be detected during an eye exam. Some patients present simply wanting new spectacles, or with broken spectacles and some do not return on a regular basis because they feel they can see well enough. Children need regular checks to ensure the eyes are developing properly but many patients will comment that their child has never complained about their sight.
Sight tests; detection etc – This information could open up the potential for outreach work and help us get more people into primary care, meaning that those at risk are identified and referred that are currently being missed. Could be melded perhaps with question 12 below.
Question 2 – Is there evidence that screening for sight loss would be beneficial? What conditions causing sight loss might be included?
Screening is key for early intervention – identification and ensuring access to the right support from the start.
For adults, the conditions for which screening may be beneficial are Glaucoma and wet ARMD (this already happens for Diabetic Retinopathy).
Question 3 – Should children with learning disabilities be specifically targeted for sight loss screening?
Children with LD are often overlooked, often mis-diagnosed and often having the wrong priorities identified (physical vs sensory imp).
Children with sight impairment have the most years of living with sight loss and its learning implications ahead of them.
This is a relatively easy to answer question within this clearly defined and accessible population. Answering the question could lead to an intervention that would be relatively easy to argue for funding of, and relatively easy to implement.
There is compelling evidence that children living with learning disability are more likely to suffer vision problems. I would like to know if targeted interventions (carried out by whom?) actually work in case-finding and improving visual and quality of life outcomes.
4_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
Question 4 – Are there other hard to reach groups which should be specifically targeted?
We have an awareness that housebound citizens, homeless, and people in care have difficulties attending sight assessment and are often in great need this links to question 6.
Ethnic minority, Deaf/hard of hearing. By their very nature, hard to reach groups rarely access services
and when they do it tends to be at a late stage when treatment and/or support is more difficult. Identifying those at most need and understanding why they don’t access services will help us design services in the future which deliver the best outcomes for those most in need.
Sight tests, detection etc. – Though we know RNIB has done work on BME groups which tend to fall in here as well as work on inequalities being able to work out who is hard to reach vs. accessible gives a very clear picture and direction to focus general outreach vs. specialised outreach.
Question 5 – How do we improve early diagnosis for those at risk of sight loss?
Those who do not present for a sight test will suffer the greatest consequences should they acquire a sight-threatening condition, as the treatment will be later than it needs to be. Ensuring that a condition can be spotted earlier ensures that those who are less likely to present have a greater chance of keeping their sight if they actually do seek a sight test.
On the assumption that prevention is better than cure. Effective early diagnosis will increase the chance for effective
rehabilitation. Early diagnosis is key for maximising skills, learning and identifying
appropriate support and interventions – improving this will lead to greater identification of needs and better economic benefit for commissioners.
We believe early diagnosis gives the best chance of successful outcomes.
The question needs to address “do we fully understand who is at risk of sight loss?” Eye Health Examination Wales, with extended
5_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
categories, might go some way to addressing this. The question then is to explore what skills to aid detection and provisional diagnosis are available in primary care, how universal are these, and what variations are there in current practice? The forthcoming GOC Strategic Review of Education is perhaps timely in reviewing core competencies, skills and CPD (not CET) requirements for primary care optometrists.
Early diagnosis can be achieved by regular eye examination and referral and an awareness of genetic risk factors. The NHS pay for the eye exam for children, patients over 60 and those with or at risk of certain eye conditions. Encouragement of regular eye examination is vital.
Sight tests, detection etc – Hugely important in preventing avoidable sight loss.-the earlier the better.
Question 6 – How does the eye health sector access people in long term care?
With numbers in long term care increasing, and the possibility that eye care will be ignored as other co-morbidities become the priority (in particular conditions that affect mental capacity, such as dementia), it is important to look at how these people are accessing eye care in order to ensure that they are and that it is tailored for their needs.
There is a large and largely hidden number of elderly with age-related VBI need.
This is a group who have a clear need but can miss out on eye care.
Question 7 – What are the true direct and indirect costs of vision impairment and severe vision impairment?
Are we spending money on the right thing? I feel that there are far too many assumptions about this area and
yet it should lie at the foundation of service delivery models and help service providers to understand the “true” impact of sight loss.
This information will help to inform the cost-effectiveness of interventions and support the case for funding.
All groups targeting the support of people with a VI have to make better social-economic arguments in order to establish and
6_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
continue to provide services for people with VI. This will become an increasing challenge and we need strong research to support this.
Unless we know the true costs it’s difficult to promote and justify the level of investment required.
Without a true cost/benefit analyses it will be virtually impossible to secure new funding for VI.
I would welcome strong evidence-based, health economist appraisal of this; such information would make the business case for adequate, whole-systems, funding more compelling.
Question 8 – What is the relative cost effectiveness of different pathways into eye health services and what are the barriers within those pathways?
This very much links into question marked as number 3 here. [question 7 - I feel that there are far too many assumptions about this area and yet it should lie at the foundation of service delivery models and help service providers to understand the “true” impact of sight loss.] One forms the foundation and the other ultimately a beginning for a sustainable client centred structure.
Linked to 7 above, we need to determine the optimum pathways for effective eye health management.
I think it might be best to pick on major pathways here: Pareto Principle. Review pathways for glaucoma/OHT, cataract, diabetic retinopathy and retinal diseases.
The eye care sector would benefit generally from identifying the relative costs within different types of pathways.
Eye care services – Research into the cost effectiveness of different pathways into eye care services could also be useful. In some areas optometrists do still refer into eye clinics via a secondary appointment with a GP and this is a thoroughly wasteful approach. Diabetic eye screening often takes place outside of eye departments and represents another possible pathway into eye care services alongside referrals from optometrists.
7_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
Question 9 – What percentage of prevalent and incident sight loss is actually preventable?
I have to declare that I have submitted an NIHR research proposal related to question 9 in the list above and so, obviously I think that that is an important question.
Prevention is better than cure both for the individual and for the public pocket! By understanding what can and cannot be prevented, we can target resources more effectively.
Question 10 – What is the most cost effective service configuration for a) patients presenting with new ocular symptoms or visual disturbance and b) opportunistic detection of people with asymptomatic conditions which are a threat to eyesight?
We need to make decisions that give the best return on investment.
The wording of question 10 seems unnecessarily technical. These are two separate questions really. "Part b)" will be answered
as part of the 5th question I selected below. [Question 13 - It would be good to apply some robust epidemiology to this question, as has been done recently to dentistry, to answer this question from a public funding perspective for older people, but also from a privately funded perspective for the working age population.]
"Part a)" however is a separate and very timely question. Once you have set up a system like that being configured in Scotland since the revision of the GOS or that seen in Wales, it is hard then to tease out how cost-effective this is in a real world way. For example, if you have a PEARS / MECS scheme in operation, you can look at what proportion of their patients needed to be seen at all (ie had significant pathology). What you can't easily find out is whether, in real life, those patients with non-significant disease would have accessed other primary care (such as GP) or secondary care (such as an eye casualty), thereby incurring more costs or whether you are just causing lots of patients who would have previously self-managed with OTC medication to attend the scheme. We have the opportunity to answer this and other questions around the inception of MECS/PEARS schemes but this needs to be intentional research designed into service implementation which would need a national oversight to access sufficient quality of real world data from both GP and HES at
8_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
commencement of a scheme, and also ongoing monitoring to look for utility attrition. I think this is an essential question that we may miss the chance to answer if lots of poorly evaluated schemes get set up.
Question 11 – What is the evidence for the cost effectiveness of Low Vision Services? What are the alternatives for the location and delivery of these services?
What are the alternatives for the location and delivery of these services? –this sit in the context of older people and holistic assessment.
Outcomes here will provide the “meat on the bones”. This links to questions 4 and 7. What are the alternatives for the location and delivery of these
services? This is an under-researched area - we are busy doing LVA but could benefit from some more evidence base to support commissioning of those activities. It may be, like patching, that we are over-doing it - or it may be like preventative measures for AMD, that we are currently missing a trick. It would be good to investigate.
Low vision services are generally provided through the Hospital Eye Service and low vision aids issued on a free permanent loan basis to patients. The costs of providing such services are high in hospitals, where chair time and room space are relatively costly and waiting times for appointments can be several months. Some community optical practices offer LV services, sometimes in response to a request from the local hospital, as part of a local shared care scheme, or by independent optometrists or dispensing opticians. The dispensing of spectacles, spectacle mounted and complex LVAs to visually impaired patients are legally restricted to optometrists and dispensing opticians and both the College of Optometrists and the Association of British Dispensing Opticians offer specialist diplomas in low vision. Attending their local optical practice is often more convenient for patients than the hospital in terms of time and travelling or parking costs and an early appointment is likely. Regrettably, there is currently no GOS voucher scheme for LV patients towards the cost of spectacles or LVAs.
9_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
Question 12 – Can sight testing, eye health assessment and spectacle prescription be separated from the sale of spectacles?
This information would be helpful in exploring how alternative models of eye care delivery could realistically work in practice.
My previous research on reasons for non-attendance for sight tests means that I am keen to explore separate of clinical aspects of eye examinations from the commercial aspects of selling optical appliances.
This would be a very important public health policy question, but can this be done other than in specific pilot sites - it is a good question but in light of the serious negative impact on legitimate commercial enterprises it might prove difficult to design a study to investigate.
We feel that this question is worth exploring but would not necessarily be suitable for all groups, including children who attend special needs schools.
The comments on Q.1. above [There is not always an awareness among patients of the association of eye health with regular eye examination. Some patients do attend regularly because they understand the ‘test’ includes examination of the inside of the eye to detect any ocular pathology, which may be symptomless, but many do not appreciate that the signs of diseases such as diabetes may be detected during an eye exam. Some patients present simply wanting new spectacles, or with broken spectacles and some do not return on a regular basis because they feel they can see well enough. Children need regular checks to ensure the eyes are developing properly but many patients will comment that their child has never complained about their sight.] highlight the importance of the eye health exam. Separating the testing of sight from the eye health assessment is likely to endanger eye health because many patients may decline the eye exam in favour of a simple refraction for new spectacles, allowing any ocular pathology to go undetected. This would be particularly serious for children as the eye is still developing and more frequent checks are recommended. I have taken ‘separating the spectacle prescription from the sale of spectacles’ to mean having the spectacles made up by a third party, rather than at the practice of the prescriber. It is important to have spectacles made where all the relevant information is available. This includes the patient’s facial
10_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
measurements, for example many people have one eye higher than the other, one ear higher or further forward than the other, or possibly a head tilt, all of which may affect the fit of the spectacles, the effectiveness of the prescription and the type of lenses. Omitting to provide proper measurements can result in headaches and even double vision. It is not possible to provide measurements to a third party when the frame is not known.
Sight tests, detection etc – Sight testing and eye health assessment could be separated from spectacle sales but such a separation would be of no interest to optometrists/opticians and I don't think CCGs or NHS England are in a position to commission new services for sight testing across the UK. Anecdotally we have heard people who wear glasses are increasingly resorting to buying frames and lenses online to save money so I guess customer demand might eventually lead to such a separation anyway.
Question 13 – How frequently should adult sight tests be recommended?
Further evidence in this area could have a big impact on capacity, as it would allow sight test time to be directed to those ages and groups most in need, thereby helping to reduce health inequalities.
It would be good to apply some robust epidemiology to this question, as has been done recently to dentistry, to answer this question from a public funding perspective for older people, but also from a privately funded perspective for the working age population.
Question 14 – Should there be condition specific matrices for service delivery – i.e. AMD, Glaucoma, Cataract and Diabetic Retinopathy?
I don’t know enough (yet) about the clinical and/social pathways for each condition but it would make sense for these to be nationally agreed pathways.
Eye care services – This drew our attention because of the clear focus on the big four conditions which is the main focus of our work. However, we were also unsure what these matrices would be and which services they refer to. From a clinical point of view
11_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
there are clinical guidelines for all of these that set out parameters for clinicians and some of primary and tertiary care.
Question 15 – What should be the care package of health and social care support offered to people with impaired vision?
As part of the integration agenda. The Care Act assumes that health and social care will be properly
integrated and that VI needs will be attended to in an integrated and effective manner. Informed advice to LA's is needed to help make this a reality (or at least get closer to it).
Many people are still not receiving appropriate visual impairment rehabilitation services. This provision is vital for the individuals affected but can also be a way of reducing ongoing health and social care costs.
Social care – We’re not sure how much benefit additional research into the care package that should be offered to blind and partially sighted people could provide in the short term. We already have a baseline of the minimum level of rehabilitation and support that should be offered and it seems like the battle right now is in ensuring local authorities even maintain that basic standard of provision.
We believe ESI at RNIB (working with OPM) are also actively conducting research into the cost benefits of rehab and other support so there is already work ongoing in this area.We wondered what “care package” means here - does this include rehab and preventative support or long term care?There also isn’t really such a thing as one package of care for someone with visual impairment, it might be that it takes the form of different support - this is commonly a PA to help with reading mail, and cooking etc, or it could be that someone is given a personal budget that has allowed them to buy an expensive piece of kit to help them to do this. Some people use their PA to go shopping or the gym etc. So, if this question was to remain, it would need look more broadly at the different types of care, or areas of support that people need - as not one size fits all. This also would fit better in with the ethos of social care today, which is all about providing tailored support for that person, for example for one person not being sociable and seeing people have a severe
12_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
impact on their wellbeing, whilst someone else might not want to be around people - but by not cooking for themselves impacts on their wellbeing.We know that the number of blind and partially sighted people receiving long term care support has dramatically reduced, but we don’t know why - is it because of tight assessments, or people just not being deemed to have significant care needs, etc. To be honest we also don’t know if this an issue, what is the impact on people not receiving care support, what would receiving social care enable the person to do?We think that understanding the provision of long term care may be really useful, but it would be important to identify the most useful element to look at and why.
Question 16 – Where do patients prefer to be treated? Although Patient Reported Outcome and Experience Measures are
becoming more embedded into pathway redesign, unless we truly involve patients in the planning, delivery and quality improvement cycle of their care, we will not get sustainable, accessible services.
I am not aware of any recent surveys on this issue but anecdotally patients prefer to be treated locally. Some optometrists are now qualified to prescribe and treat certain ocular conditions at their own practices rather than having to refer patients into the Hospital Eye Service, saving the HES time and money. As mentioned in my comments on Q.11 (cost effectiveness, location and delivery of LV services) attending their local optical practice is often more convenient for patients than the hospital in terms of time and travelling or parking costs and an early appointment is likely.
Question 17 – What are the quality standards for optometric consultation and follow up and how can these be monitored?
Enhanced governance of optometry will lead to improved outcomes for the VI.
Eye care services – Being able to hold services to account and monitor how they are delivering care is important for us. We were not sure at this point if 'optometric' referred only to optoms or all of eye care? Again there are NICE quality standards for clinicians but we are not quite sure where things stand for primary care and how
13_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
far the guidelines stray into that territory (they often cover diagnosis and referral).
Overall comments
1. Questions 8, 10 and 14 are closely linked (as community services questions) and the importance of CCGs commissioning those (we would argue that there should be national commissioning with standardised pathways).
2. Questions 5 and 7 are broad questions for the whole sector to consider and of fundamental importance. As is 9 of course – I know that there are different interpretations of this.
3. Questions 5, 7, 9, 11 and 14 – It is difficult to prioritise the questions due to their conflicting nature. When you lay the 17 questions across the sight loss pathway there is a clear cause and effect between the majority of the questions, so depending on where your organisation continues to the pathway will heavily influence the response. It is therefore difficult to segregate the questions into importance depending on where they fall on the pathway. In addition the questions range from the tactical to the strategic and from identifying outputs to outcomes (value added) and therefore not easy to compare and contrast. The questions around value added and monitoring value are our preference (due to lack of confident prevalence data as a sector, a need for the sector to show value for funding and with our strategy in mind). Question 15 is potentially the next step from the outcome of question 14.
4. Questions 4, 5, 9, 10 and 14 – Glaucoma falls under preventable sight loss.
5. Questions 7, 9, 12, 13 and 16 – I do believe that eye tests offer the chance of picking up important eye conditions. I think people are currently put off by the fact that the person testing may wish to sell glasses. Separating the two would remove this. I am not sure what the evidence is for testing two yearly and given the cost of this believe it is important to establish. Finally much is made of patients not wishing to be treated in hospitals. Has this come from patients?
14_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
6. Questions 1, 4, 7, 8 and 16 – They are all based around bringing down barriers to healthcare as patients should get seen and care should be funded and costed to be appropriate and beneficial.
7. Questions 8, 10, 11, 12 and 15 – These are just the areas that I am most interested in personally to be honest.
8. Questions 7, 8 and 9 – The three questions are all related in terms of a need for health economics evidence to underpin eye care services. We need to understand the cost consequences (direct/indirect, tangible/intangible) of not preventing sight loss that is potentially preventable, to set against the cost of different interventions and models of care that could achieve benefits in terms of preventing preventable sight loss.
9. Questions 7, 8, 9, 10 and 15 – My reasons for many of these are financial implications as this is often the main driver of governments and without accurate costings this may prevent NICE/NHS England recommending specific new therapies.
It is disappointing that none of these questions have included anything about 'The Patient Voice' (very indirectly Q16).
10. It seems to me that many of these questions are interlinked or subcategories of other broader topics.
11. Questions 4, 7, 9, 10 and 15 – My reasons are that these questions seem to be the ones that most closely address V2020's big issue: V2020 appears wholly occupied with 'preventable' sight loss. The oft-quoted statistics are that there are "two million blind and partially sighted people in the UK and that half of this is preventable".
What does this mean? The Future Sight Loss document suggests that nearly half the 2 million is uncorrected refractive error - obviously preventable but there is no obvious strategy to tackle this. The rest of the unpreventable sight loss is untreated, treatable eye disease such as cataract and late-diagnosed glaucoma.
Answering question 9 would define the problem.
Question 4 (coupled with a bit of 3) might help understand why there is so much uncorrected refractive error; poverty, groups
15_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
unable to solve this themselves, eg children, people with learning disabilities, dementia or very frail older people etc. How much refractive error is actually a problem? What sort of action would solve the problem?
Qs 10 and 15 address important service issues but it is difficult (impossible?) to make a case for investment in health and social care services unless change can be demonstrated to be cost-effective and so Q7 is important to that end.
I have to say that I am terribly disappointed that (after apparently a year of discussion) there is still no mention of biomedical research. If uncorrected refractive error is taken out of the two million figure it exposes the fact that the vast majority of sight loss is NOT preventable or treatable - AMD, inherited retinal conditions, intractable glaucoma etc etc. I really do think that V2020 UK should do more in this area. At the very least V2020 needs to be clearer about the refractive error problem and openly address that as a target. At least then the true problem of incurable eye disease in this country would be made obvious.
12. I believe almost all of the seventeen questions posed to be valid and worthy of consideration. In prioritising I have tried to assign a priority value based on a number of matrices:
Lack of existing evidence base in literature. Ease of research versus burden of data collection and
analysis. Novelty value (has it been done before).
I have prioritised based on an attempt to build evidence around health promotion and prevention (children with LD), early diagnosis, access to services and treatment, efficacy of treatment, patient experience, and building evidence to fully support people living with sight loss (societal cost of sight loss). A pathway approach, aimed at maximising resource and impact across the system.
13. I'd have liked to have seen something more explicit on rehabilitation/habilitation and on emotional aspects of sight loss - perhaps the link between sight loss and symptoms of clinical depression.
16_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
14. Questions 2, 3, 5, 6 and 8 – We have made our choice taking into consideration global eye health as well as our professional interests.
15. We feel that some of the questions will bring a very wide range of responses, depending on individual responses including –
What motivates people to have a sight test? Where do patients prefer to be treated?
For example, we know that the answers above will be very different for people with learning disabilities.
We also feel that for some of the priorities listed, there is research already being undertaken, or there is plenty of research to confirm the answer already. We wondered if the working group had been through the 85 questions and shortlisted on this basis, but then there is still the question, should children with learning disabilities be specifically targeted for sight loss screening? which we know has been comprehensively researched and answered over the past few years. It was a surprise to see the children with learning disabilities question still shortlisted and we would be interested to know why.
The sector recently worked together to agree on a framework for testing children in special schools where it was also clinical opinion that “screening” should be avoided in preference to a full eye examination, as many children are unable to comply. For more information see the Task and Finish group framework paper for special schools https://www.seeability.org/uploads/files/Children_in_Focus_campaign/Framework.pdf and particularly Appendix A.
If you need us to list the academic pieces of research that confirm children with learning disabilities should be specifically targeted for eye examinations please let us know but just a selection as follows are:
Salt, A and Sargent, J (2014) “Common visual problems in children with disability”. Archives of Disease in Childhood. 08/2014 99(12).
Woodhouse JM et al. Ocular and visual status among children in special schools in Wales: the burden of
17_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
unrecognised visual impairment. Arch Dis Child (2013); 99(6):500-504.
Das M., Spowart K., et al. (2010). "Evidence that children with special needs all require visual assessment." Archives of Disease in Childhood 95(11): 888-892.
Next steps
The results of the prioritisation exercise will be discussed at the VISION 2020 UK Social Research Committee. The prioritised list of questions will then be discussed with Prof Gwyn Bevan of the London School of Economics, who can add a health economics perspective, and then a submission will be made to the National Institute for Health Research (NIHR). The NIHR will undertake a series of systematic reviews addressing these questions based on consultation from the attendees at the meeting and any additional relevant stakeholders.
Tayyaba KamalOperations Officer/PA to CEOVISION 2020 UK
October 2016
Appendix 1: Final questions to inform a programme of research 1. What motivates people to have a sight test?
2. Is there evidence that screening for sight loss would beneficial? What conditions causing sight loss might be included?
3. Should children with learning disabilities be specifically targeted for sight loss screening?
4. Are there other hard to reach groups which should be specifically targeted?
5. How do we improve early diagnosis for those at risk of sight loss?
18_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837

Attachment 6
6. How does the eye health sector access people in long term care?
7. What are the true direct and indirect costs of vision impairment and severe vision impairment?
8. What is the relative cost effectiveness of different pathways into eye health services and what are the barriers within those pathways?
9. What percentage of prevalent and incident sight loss is actually preventable?
10. What is the most cost effective service configuration for a) patients presenting with new ocular symptoms or visual disturbance and b) opportunistic detection of people with asymptomatic conditions which are a threat to eyesight?
11. What is the evidence for the cost effectiveness of Low Vision Services? What are the alternatives for the location and delivery of these services?
12. Can sight testing, eye health assessment and spectacle prescription be separated from the sale of spectacles?
13. How frequently should adult sight tests be recommended?
14. Should there be condition specific matrices for service delivery – i.e. AMD, Glaucoma, Cataract and Diabetic Retinopathy?
15. What should be the care package of health and social care support offered to people with impaired vision?
16. Where do patients prefer to be treated?
17. What are the quality standards for optometric consultation and follow up and how can these be monitored?
19_______________________________________________________VISION 2020 UK 2nd Floor, 105 Judd Street, London WC1H 9NEReg. Company No. 7850769 Charity No. 1146746/SC046837