Embed Size (px)
Citation preview

BEHAVIOR THERAPY 26, 547-554, 1995
Virtual Reality Graded Exposure in the Treatment of Acrophobia: A Case Report
BARBARA OLASOV ROTHBAUM
Emory Umverstty School o f Medtcme
LARRY F. HODGES
ROB KOOPER
Georgia Institute o f Technology
DAr~ OVDYKE
Georgw State Umverstty
JAMES S. WILLIFORD
lOlst Atrborn Division (Air Assault), Fort Campbell
M A X NOR T H
Clark Atlanta University
This is the first case report to test the efficacy of computer-generated virtual reality (VR) for the treatment of acrophobia (fear of heights). The subject was a 19-year-old undergraduate student with a fear of heights, particularly of elevators Twice weekly, sessions were conducted for 3 weeks, for a total of 5 sessions. Outcome was assessed on measures of anxiety, avoidance, attitude, distress, and included a behavioral avoid- ance test. VR graded exposure was successful in reducing fears of heights. VR graded exposure is proposed as a new medium for exposure therapy
Acrophobia, a simple phobia, is characterized by marked anxiety upon ex- posure to heights, avoidance of heights, and a resulting interference in func- tioning (American Psychiatric Association, 1987). Behavioral therapy of
Thanks to Drew Kessler, Kevin Mclnturff, and David Rodriguez for their help in modeling and monitoring equipment during sessions. This work was supported in part by a grant from the Emory/Georgia Tech Biotechnology Research Center, by an equipment grant from the Georgia Tech Foundation, and by a Research Experiences for Undergraduates Site Grant from the Na- tional Science Foundation.
Correspondence concerning this article should be sent to Barbara O. Rothbaum, Ph.D., Dept. of Psychiatry, The Emory Clinic, 1365 Clifton Road, Atlanta, GA 30322.
547 0005-7894/95/0547-055451 00/0 Copyright 1995 by Association for Advancement of Behavior Therapy
All rights of reproduction m any form reserved.

548 R O T H B A U M ET AL.
acrophobia usually includes some form of exposure. Systematic desensitiza- tion has long been found to be effective in treating individuals with simple phobias (Marks & Gelder, 1965), but a large body of evidence indicates that in vivo exposure has proven consistently effective for individuals with height phobias (Abelson & Curtis, 1989; Emmelkamp & Felten, 1985; Marshall, 1985; Williams, Dooseman, & Kleinfield, 1984; Williams, Turner, & Peer, 1985).
Exposures to heights usually require leaving the therapist's office, often proving to be difficult and expensive. Therefore, it is important to identify al- ternatives to these exposures. One variation effectively utilized lenses to mag- nify apparent height during in vivo exposure to allow more control and ex- posure to seemingly greater heights than was physically possible (Schneider, 1982). Another alternative may be in the form of virtual reality (VR).
VR integrates real-time computer graphics, body tracking devices, visual displays, and other sensory input devices to immerse a participant in a computer-generated virtual environment (VE; Kalawsky, 1993). Participants usually wear a head-mounted display fitted with an electromagnetic sensor. The user is presented with a computer-generated view of a virtual world that changes in a natural way with head and body motion. For some environments, users may also hold a second position sensor in their hand that allows them to manipulate a virtual hand to interact with the environment, for example, to push an elevator button and ascend.
As such a new technology, the applications of VR are still being explored. An uncontrolled report from Japan described the use of VR to simulate the sand play projective technique with autistic children. No data were presented, but the authors contended that the VR sand play was useful (Kijima, Shirakawa, Hirose, & Nihei, 1994). In a controlled study applying VR to the treatment of a psychological disorder, VR graded exposure (VRGE) was incorporated in the treatment of acrophobia (Rothbaum et al., 1995). Subjects were repeat- edly exposed to virtual foot bridges of varying heights and stability, outdoor balconies of varying heights, and a glass elevator that ascended 50 floors. VRGE was effective in significantly reducing fear of heights and improving attitudes toward heights, whereas no change was noted in the wait-list control group.
This paper represents the first known data-based case report of VR in the treatment of a psychological disorder. The purpose of this study was to ex- amine the efficacy of a treatment for acrophobia using VRGE. VRGE has the advantages of conducting time-consuming exposure therapy without leaving the office and offering more control over exposure stimuli. Thus, it may offer a time- and cost effective manner to conduct exposure therapy, with implica- tions for the treatment of many disorders, especially anxiety disorders.
Method Subject
The subject was a 19-year-old white male undergraduate student who indi- cated fear and avoidance of heights and a desire to participate in a treatment study. He was offered treatment after participating in the wait list control con- dition of a larger controlled study of VRGE in the treatment of acrophobia
VIRTUAL REALITY EXPOSURE 549
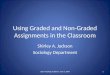
(Rothbaum et al., 1995). His pre- and post-wait list data appear in the group data reported elsewhere (Rothbaum et al.); this case report presents his re- sponse to treatment that does not appear elsewhere.
Measures
The Screening Questionnaire was constructed for use in the larger study and assessed inclusion and exclusion criteria. DSM-III-R criteria (APA, 1987) for simple phobia (i.e., fear of heights, avoidance of heights, belief that the fear is excessive, interference from fear), desire for treatment, desire to partic- ipate in a treatment study, presence of panic attacks, history of panic attacks, and presence of claustrophobia were assessed.
The Acrophobia Questionnaire (AQ; Cohen, 1977) describes 20 height situ- ations with rating scales for anxiety (0 to 6) and avoidance (0 to 3). The AQ yields a total score ranging from 0 to 180 and anxiety (0 to 120) and avoidance (0 to 60) subscale scores. Adequate consistency and test-retest reliability have been demonstrated, and it has been shown to discriminate between phobic and nonphobic subjects (Cohen). The questionnaire has been responsive to treatment and group effects in several studies (Cohen; Menzies & Clarke, 1993; Pendleton & Higgins, 1983; Rothbaum et al., 1995), and was more sensitive to treatment outcome than were behavioral tests (Cohen).
The Attitude Towards Heights Questionnaire contains six items assessing attitudes towards heights and was adapted from Abelson and Curtis (1989). These include the following dimensions rated on a 0 to 10 semantic differen- tial scale: good-bad, awful-nice, pleasant-unpleasant, safe-dangerous, threat- ening-unthreatening, and harmful-harmless.
One item was included from the Marks and Mathews' (1979) Fear Ques- tionnaire assessing the degree of distress related to the acrophobia, rated on a 0 to 8 scale.
A Behavioral Avoidance Test (BAT) was conducted pre- and posttreatment by the therapist. The subject and therapist ascended in a glass elevator at the Marriott Marquis Convention Hotel as high as the subject felt he could, with no encouragement by the therapist to push himself, rating his Subjective Units of Discomfort (SUDs) at various floors. However, the pretreatment BAT was confounded by the fact that an express elevator was inadvertently used, thereby ascending to higher floors than the subject would have chosen.
Apparatus Hardware for the creation of VEs for this study consisted of a Silicon
Graphics Reality Engine I computer graphics workstation, a head-mounted display (VR Flight Helmet) and an electromagnetic sensor that was used to track the head and right hand (Ascension Technology Flock System) so that the subject could interact with objects in the VE. Modeling was done using Wavefront software (Wavefront Technologies, 1989). The Simple Virtual En- vironment (SVE) software library (Kessler, Kooper, Verlinden, & Hodges, 1994) was used to create VEs from the models. To create a greater sense of realism, we integrated VR hardware and software with a 4 x 4 foot raised (6 inches) platform surrounded with railing. This aided exposure by giving the subject
5 5 0 ROTHBAUM E T A L .
railings to hold and an edge to approach, as well as keeping the subject within tracking range of the sensor. The hardware and software are described in greater detail elsewhere (Hodges et al., 1994). Although this equipment is costly, given current trends for increasing computer power in personal computers and decreasing VR hardware costs (driven by the game industry), we are confident that the VRGE system we are developing and testing in our lab environment on high-end equipment can be made available within 2 to 3 years for less than $5,000 per installation.
Procedure
The subjects were initially screened in large introductory psychology and computer classes at two universities in Atlanta via the Screening Question- naire for the larger study. Subjects who indicated a fear of height~ were con- tacted by telephone for further screening and to explain the study. The pretreat- ment assessment (PRE) was conducted in a group format in separate sessions for the treatment and the wait list groups. At that time, the study was explained, informed consent was gathered, and the subject completed all self-report scales. Treatment for this subject followed his WAIT condition. All subjects who par- ticipated in the wait list condition of the larger study were offered free treat- ment following the wait list period. However, that study terminated at the end of their academic quarter and so this is the only subject that accepted the offer of treatment. The posttreatment assessment (POST) consisted of the same battery of questionnaires administered at PRE and was conducted after three weeks of VRGE treatment. Treatment and assessments were provided free of charge.
Treatment
Individual VRGE was conducted in five sessions over 3 weeks. Sessions were 35 to 45 minutes long and conducted by an advanced clinical psychology graduate student, All sessions were video recorded and were reviewed by a licensed clinical psychologist in supervision. The subject was encouraged to spend as much time at each "floor" as needed for his anxiety to decrease and was allowed to progress at his own pace. SUDs were rated every 5 minutes during exposure on a 0 (no discomfort) to 100 (panic-level anxiety) scale. The therapist simultaneously viewed on a video monitor the VEs in which the sub- ject was interacting and therefore was able to comment appropriately. The therapist 's comments were essentially identical to what would be expected for conventional in vivo exposure, for example, "Can you try to let go of the railings?"; "Do you want to get closer to the edge?"; and "You're doing very well: your anxiety is coming down just by staying in the situation," as well as inquiring as to the subject's thoughts and physical feelings.
Photographic quality textures were fed into the computer to enhance the realism of the VEs. The glass elevator simulated the elevator at the Marriott Marquis Convention Hotel in downtown Atlanta, complete with balconies, artwork, and marble floor. The subject controlled the movement of the ele- vator via three "buttons" within the VE to move up, down, or stop. The ele- vator moved 49 floors, up to 147 meters at the top, and the floor number ap-
VIRTUAL REALITY EXPOSURE
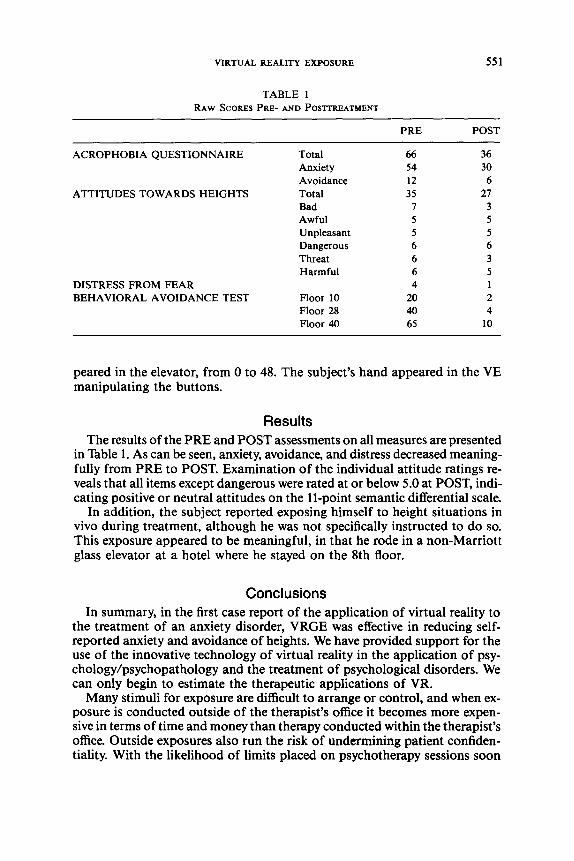
TABLE 1 RAW SCORES PRE- AND POSTTREATMENT
551
PRE POST
ACROPHOBIA QUESTIONNAIRE Total 66 36 Anxiety 54 30 Avoidance 12 6 Total 35 27 Bad 7 3 Awful 5 5 Unpleasant 5 5 Dangerous 6 6 Threat 6 3 Harmful 6 5
4 1 Floor 10 20 2 Floor 28 40 4 Floor 40 65 10
ATTITUDES TOWARDS HEIGHTS
DISTRESS FROM FEAR BEHAVIORAL AVOIDANCE TEST
peared in the elevator, from 0 to 48. The subject's hand appeared in the VE manipulating the buttons.
Results The results of the PRE and POST assessments on all measures are presented
in Table 1. As can be seen, anxiety, avoidance, and distress decreased meaning- fully from PRE to POST. Examination of the individual attitude ratings re- veals that all items except dangerous were rated at or below 5.0 at POST, indi- cating positive or neutral attitudes on the 11-point semantic differential scale.
In addition, the subject reported exposing himself to height situations in vivo during treatment, although he was not specifically instructed to do so. This exposure appeared to be meaningful, in that he rode in a non-Marriott glass elevator at a hotel where he stayed on the 8th floor.
Conclusions In summary, in the first case report of the application of virtual reality to
the treatment of an anxiety disorder, VRGE was effective in reducing self- reported anxiety and avoidance of heights. We have provided support for the use of the innovative technology of virtual reality in the application of psy- chology/psychopathology and the treatment of psychological disorders. We can only begin to estimate the therapeutic applications of VR.
Many stimuli for exposure are difficult to arrange or control, and when ex- posure is conducted outside of the therapist's office it becomes more expen- sive in terms of time and money than therapy conducted within the therapist's office. Outside exposures also run the risk of undermining patient confiden- tiality. With the likelihood of limits placed on psychotherapy sessions soon
552 ROTHBAUM E T A L .
in the new healthcare reforms, anything that can make the available sessions more efficient is a huge advantage. Being able to conduct exposures on air- planes for individuals with flying phobias or interstate highways for individ- uals with driving phobias, for example, within the therapist 's office will make better treatment available to more sufferers.
In addition, many patients have difficulty imagining and therefore would not be good candidates for imaginal exposure. VR exposure may provide the necessary images while still being able to program them specifically for that patient. An advantage of VR over the real world is that exposures can be made as extreme as necessary, providing for overcorrection of the fear and avoid- ance. Anecdotally, subjects appeared to respond to VRGE more as they do to in vivo exposure than to imaginal exposure. They appeared to remain en- gaged in the exposure exercise, looking around, "walking" around, and did not engage in much unrelated conversation. They reported physical sensations indicating anxiety and movement. There were a few comments by two sub- jects in the larger study that the scenes were not realistic, but usually these were made after the subjects had apparently habituated and seemed to be get- ting bored. Some sample comments from subjects participating in the larger study: " I 'm feeling a little weak in the knees. My chest is getting tight. My palms are sweaty. .... This is the first time I can look down and not get that weak-in-the-knees feeling." "As long as I keep looking at it, it gets better than it was before." " I f I don't see the rail, I feel like I 'm going to fall." "Feel like I 'm on the e d g e . . , don't like it." "Feel weak in the k n e e s . . , wanting to hold on for dear life."
It is interesting to note that although it was clear that the VR situation was not real, no subject, visitor to the lab, or investigator walked off the elevator into midair. A few investigators did so only after they were prompted to do so, and they were clear about the safety of doing so. This issue of the degree to which participants feel immersed in VEs is discussed in more detail else- where (Hodges et al., 1994).
It is also possible that therapists will be able to be present in the VE, al- lowing therapists unfamiliar with exposure therapy to be able to provide it to their patients. The ramifications of VR on training are far-reaching for psy- chology, psychiatry, and the medical field in general. Trainees may be able to interview, treat, and even operate on virtual patients with no risk, liability, or patient expense. Of course, care must be taken in the development and ap- plication of this new technology as applied to patients, but if used judiciously, it can be a tremendous tool for the therapist. This technology is currently limited by the cost of the equipment and the skills to program the application, but if the applications for VR become popular, one would hope it would become more accessible to the general public, much as calculators and PCs have become
The strengths of this case report include the collaboration of experts in their respective fields to transform the capabilities o f high technology VR into state- of-the-art treatment for anxiety disorders. A new modality of exposure treat- ment has now been launched: In addition to imaginal and in vivo, we now have virtual in vivo. The length of the treatment was sufficient, and the measures were sound.
VIRTUAL REALITY EXPOSURE 553
The weaknesses of this study center on the case report format with its limited generalizability and the absence o f follow-up data. The design is a simple pre- post uncontrolled application. It was felt that the nature o f the research ques- tion did not necessitate follow-up data. The hypothesis, namely, that VR graded exposure can reduce anxiety associated with heights, was tested and supported by the dependent measures used. Future research should focus on expanding the applications o f VR in the treatment o f psychological disorders. It is espe- cially applicable in the treatment o f anxiety disorders in which exposure-based treatments are recommended. It would be interesting to compare VRGE to an existing treatment modality. The reasonable applications and limits o f VR- assisted therapy must be established.
References Abelson, J. L., & Curtis, G. C. (1989). Cardiac and neuroendocrme responses to exposure therapy
m height phoblcs: Desynchrony within the "physiological response system "Behavtour Re- search and Therapy, 27, 561-565
American Psychiatric Association. (1987). Dtagnostw and stattstwal manual o f mental dtsorders (3rd ed., rev.). Washington, DC: Author.
Cohen, D. C. (1977). Comparison of self-report and overt-behavioral procedures for assessing acrophobia Behavtor Therapy, 8, 17-23
Emmelkamp, P. M., & Felten, M. (1985). The process of exposure m-vivo: Cognmve and psycho- logical changes during treatment of acrophobia. Behawour Research and Therapy, 23, 219-223.
Hodges, L. E, Rothbaum, B. O., Kooper, R., Opdyke, D., Meyer, T., de Graft, J. J., & Williford, J S. (1994). Presence as the definmg factor m a VR apphcatton: Vzrtual reahty graded ex- posure m the treatment ofacrophobta. (Tech. Rep. #GIT-GVU-94-6). Georgia Institute of Technology.
Kalawsky, R. S. (1993). The scwnce of vtrtual reahty and vtrtual envtronments. Reading, MA: Addison-Wesley.
Kessler, G. A., Kooper, R., Verhnden, J., & Hodges, L. E (1994). The stmple vtrtual envtronment (SVE) tool ktt. (Tech. Rep #GIT-GVU-94-46). Georgia InsUtute of Technology.
Kijima, R., Shirakawa, K., Hirose, M., & Nihel, K. (1994). Virtual sand box: Development of an application of virtual environment for the clinical medicine. Presence: Teleoperators and vtrtual enwronments, 3, 45-49
Marks, I M., & Gelder, M G. 1965 A controlled retrospective study of behaxaour therapy in phobic patients. Brtttsh Journal of Psychtatry, 111, 571-573.
Marks, I. M., & Mathews, A. M (1979). Brief standard self-rating for phobic paUents. Behavlour Research and Therapy, 17, 263-267.
Marshall, W L. (1985). The effects of variable exposure m flooding therapy. Behavtor Therapy, 16, 117-135.
Menzles, R G, & Clarke, J C. (1993) The euology of fear of heights and its relationship to seventy and m&vidual response patterns. Behavtour Research and Therapy, 31, 355-365.
Pendleton, M. G., & Hlggins, R L (1983). A comparison of negatwe pracUce and systematic desensitization m the treatment of acrophobia. Journal of Behavior Therapy and Experimental Psychtatry, 14, 317-323.
Rothbaum, B. O., Hodges, L. F., Kooper, R., Opdyke, D., Wllliford, J. S., & North, M. (1995). The efficacy of wrtual reahty graded exposure in the treatment of acrophobm Amerwan Journal o f Psychtatry, 152, 626-628.
Schneider, J. W (1982) Lens-assisted m-vwo desensmzation to heights. Journal of Behavtor Therapy and Experimental Psychtatry, 13, 333-336.
554 ROTHBAUM ET AL.
Wavefront Technologies, Inc (1989). Image user's manual , version 2.9. Los Angeles: Wavefront Technologies
Wllhams, S. L., Dooseman, G., & Kleinfield, E. (1984). Comparative effecUveness of guided mas- tery and exposure treatments for intractable phobias. Journal of Consulting and Chmcal Psychology, 52, 505-518.
Williams, S. L , Turner, S. M., & Peer, D. E. (1985). Guided mastery and performance desensm- zaUon treatments for severe agoraphobia. Journal of Consulting and Chmcal Psychology, 53, 237.
RECEIVED: April 12, 1994 ACCEPTED: September 12, 1994