Embed Size (px)
Citation preview
www.elsevier.com/locate/btBehavior Therapy 37 (2006) 80–90
Virtual Reality Exposure Therapy and Standard (in Vivo) ExposureTherapy in the Treatment of Fear of Flying
Barbara Olasov Rothbaum, Emory University School of Medicine, USA
Page Anderson, Georgia State University, USA
Elana Zimand, Virtually Better, Inc., USA
Larry Hodges, University of North Carolina–Charlotte, USA
Delia Lang, Emory University, USA
Jeff Wilson, Georgia Institute of Technology, USA
This controlled clinical trial tested virtual reality exposure(VRE) therapy for the fear of flying (FOF), a relatively newand innovative way to do exposure therapy, and comparedit to standard (in vivo) exposure therapy (SE) and a wait list(WL) control with a 6- and 12-month follow-up. Eighty-three participants with FOF were randomly assigned toVRE, SE, or WL. Seventy-five participants, 25 per group,completed the study. Twenty-three WL participants com-pleted randomly assigned treatment following the waitingperiod. Treatment consisted of 4 sessions of anxietymanagement training followed either by exposure to avirtual airplane (VRE) or an actual airplane at the airport(SE) conducted over 6 weeks. Results indicate that VRE wassuperior to WL on all measures, including willingness to flyon the posttreatment flight (76% for VRE and SE; 20% forWL). VRE and SE were essentially equivalent on standard-ized questionnaires, willingness to fly, anxiety ratings duringthe flight, self-ratings of improvement, and patient satisfac-
Drs. Rothbaum and Hodges receive research funding and areentitled to sales royalty from Virtually Better, Inc., which isdeveloping products related to the research described in this article.In addition, they serve as consultants to and own equity in VirtuallyBetter, Inc. The terms of this arrangement have been reviewed andapproved by Emory University and Georgia Institute of Technologyin accordance with their conflict of interest policies.
This study was supported by NIMH Grant #2-R42-MH58493-02. Thanks go to Edna Foa, Ph.D., for consultation during thisresearch, and Dan Whitaker, Ph.D., for statistical consultation.
Address correspondence to Barbara O. Rothbaum, Ph.D.,Department of Psychiatry and Behavioral Sciences, The EmoryClinic, 1365 Clifton Rd., Atlanta, GA 30322, USA; e-mail:[email protected]/06/080–090$1.00/0n 2006 Association for Behavioral and Cognitive Therapies. Published byElsevier Ltd. All rights reserved.
tion with treatment. Follow-up assessments at 6 and 12months indicated that treatment gains were maintained,with more than 70% of respondents from both groupsreporting continued flying at follow-up. Based on thesefindings, the use of VRE in the treatment of FOF wassupported in this controlled study, suggesting that experi-ences in the virtual world can change experiences in the realworld.
THE BEST E ST IMATE of fear of flying (FOF) is 10%to 40% (Dean & Whitaker, 1982; Van Gerwen &Diekstra, 2000), or approximately 25 millionadults in the U.S., many of whom avoid flyingentirely. As many as 20% of all flyers depend onalcohol or sedatives to reduce anxiety symptomsduring flights (Griest & Griest, 1981; Howard,Murphy, & Clarke, 1983). Since the September 11terrorist attacks, there has been a 10% to 30%decrease in airline travel, affecting the airlineindustry, the business community, and the overalleconomy (Ito & Lee, 2004).FOF treatment programs are increasingly popular
and lucrative. Most of these programs use a CBTapproach including both anxiety management (e.g.,relaxation training, cognitive restructuring, psy-choeducation) and exposure (i.e., flying) (VanGerwen, Spinhoven, Diekstra, & Van Dyck,2002). Many FOF programs affiliated with theairlines (see Van Gerwen & Diekstra, 2000, for areview) report positive outcomes but do not conductstandardized research, with the exception of VanGerwen et al. (2002).

81v irtual real i ty exposure therapy
Virtual reality (VR) has developed as one ofseveral new computer-based formats for the deliveryof exposure therapy (Anderson, Jacobs, & Roth-baum, 2004). The use of VR in the treatment ofanxiety disorders is receiving increasing scientific(Anderson, Rothbaum,&Hodges, 2000; Zimand etal., 2002; Zimand, Rothbaum, Tannenbaum, Fer-rer, & Hodges, 2003) and public (Carmichael,Kovach, Mandel, & Wehunt, 2001; Hoffman,2004; Szegedy-Maszak, 2004) attention. VR is ahuman-computer interaction paradigm in whichusers are active participants within a computer-generated three-dimensional virtual world. Tobecome part of the virtual world, the user wearsan immersive head-mounted display (HMD) thatconsists of a display screen for each eye, earphones,and a head-tracking device, while sitting or standingon a low platform atop a bass speaker, thus placingthe user within a multisensory, 360-degree environ-ment that can provide visual, auditory, and kines-thetic cues (i.e., vibrations). Natural body and headmotion by the user corresponds to changewithin thevirtual world. The image seen by the user in theHMD is displayed on a computer monitor for thetherapist to view.A sense of presence, essential to conducting
exposure therapy, distinguishes VR from aninteractive computer graphics display. Regen-brecht, Schubert, and Friedmann (1998) studiedthe sense of presence in which arousal is elicitedby the user “developing a mental representation ofthe virtual stimuli as one3s own environment” (p.246). Although the user3s experience is entirelycomputer-generated, the individual3s perceptionoverlooks the role of technology in the experience(Krijn, Emmelkamp, Olafsson, & Biemond,2004).There are several advantages to VR for FOF and
other exposures. VR exposure (VRE) takes place ina therapy office, which is more convenient andprovides an intermediate step between the therapyoffice and the real world (Botella, Osma, Garcia-Palacios, Quero, & Banos, 2004). As a result,researchers have suggested that VR exposure hasgreater appeal over in vivo exposure and may helpmore individuals who meet criteria for an anxietydisorder to seek treatment (Garcia-Palacios, Hoff-man, See, Tsai, & Botella, 2001). For FOF, it is lessexpensive to pay for VR sessions in a therapist3soffice than to purchase airline tickets and pay forthe therapist to accompany the client. Confidenti-ality can more easily be maintained relative to invivo exposure conducted in a public place. Finally,VR can effectively meet the basic criteria forexposure, including a high degree of control, theability to present anxiety-producing stimuli over
and over, and the ease of prolonging the exposurein order to achieve habituation (Foa & Kozak,1986; Foa, Steketee, & Rothbaum, 1989).A body of research is accumulating supporting
the use of VRE within a comprehensive treatmentprogram for anxiety disorders. Case studies supportthe use of VRE in the treatment of anxietydisorders, including specific phobia of flying(North, North, & Coble, 1997; Rothbaum,Hodges, Watson, Kessler, & Opdyke, 1996;Smith, Rothbaum, & Hodges, 1999; Wiederhold,Gevirtz, & Wiederhold, 1998), specific phobia ofspiders (Carlin, Hoffman, & Weghorst, 1997),claustrophobia (Botella et al., 1998; Botella,Banos, Villa, Perpina, & Garcia-Palacios, 2000),acrophobia (Choi, Jang, Ku, Shin, & Kim, 2001;Rothbaum et al., 1995b), and social anxiety(Anderson, Rothbaum, & Hodges, 2003). Twocase studies have reported that VRE was successfulat reducing PTSD symptoms: one in a Vietnamveteran (Rothbaum et al., 1999) and another in asurvivor of the 9/11 World Trade Center attacks(DiFede & Hoffman, 2002).These case studies were followed by successful
open clinical trials without comparison groups forcombat-related PTSD (Rothbaum, Hodges, Ready,Graap, & Alarcon, 2001), social anxiety (Ander-son, Rothbaum, Hodges, & Zimand, submitted forpublication), acrophobia (Emmelkamp, Bruynzeel,Drost, & van der Mast, 2001), post-earthquaketraumatic stress (Basoglu, Livanou, & Salcioglu,2003), and FOF (Botella et al., 2004). A recentapplication of VR to fear of driving (Wald, 2004)with five participants in a multiple-baseline across-subjects design yielded only modest outcome inanxiety reduction and did not result in generaliza-tion to actual driving behavior.Randomized clinical trials comparing VRE to
wait list (WL) control groups have been conductedfor several of the anxiety disorders. The firstpublished controlled study used VRE therapycompared to WL for the treatment of acrophobia(Rothbaum et al., 1995a). Another controlledstudy demonstrated the efficacy of VRE therapycompared to WL for reducing public speakinganxiety among university students (Harris, Kem-merling, & North, 2002). A drawback to thesestudies is the small sample sizes, ranging from 10 to20 participants.Several controlled trials using VRE for fear of
heights and flying have been conducted by inde-pendent researchers around the world. Emmelkampand colleagues (2002) compared in vivo exposurewith an exact replication of the environment in VRfor acrophobia (N = 33). Participants in bothtreatments reported reduced anxiety, avoidance,

82 rothbaum et al .
and distress, and were able to confront real-lifeheights situations following treatment, maintainingtreatment gains at 6-month follow-up. A drawbackto this study was the absence of a no-treatmentcontrol group.The same researchers tested VRE for acrophobia
in two different formats believed to vary in degreeof presence. VRE using a PC delivered through anHMD was compared to a computer automaticvirtual environment (CAVE), a multi-user projec-tion-based VR system in which the patient andtherapist were surrounded by stereoscopic comput-er-generated images on four sides of a room. Thesetwo active VRE interventions were compared to aWL control group (Krijn, Emmelkamp, Biemond, etal., 2004; N = 37). Findings indicated that bothactive treatments were equally effective in helpingindividuals overcome a fear of heights and bothwere more effective than the control group, butthere were a high number of dropouts (n = 10), allof whom reported less presence, the sense that theywere “there” and immersed in the virtual environ-ment. These results suggested that VR could beeffectively delivered through an HMD, which isexponentially less expensive than the CAVE system;however, individual users may differ in the extent towhich they can develop a sense of presence.VRE has been tested extensively for treatment of
FOF in well-controlled designs by independentresearchers. The first of these studies comparedVRE to standard in vivo exposure therapy (SE) andWL control (Rothbaum, Hodges, Smith, Lee, &Price, 2000;N = 45). Both treatments were found tobe equally effective and significantly better than thecontrol group. Treatment gainsweremaintained at a12-month follow-up with over 90% of respondentsreporting continuing to fly (Rothbaum, Hodges,Anderson, Price, & Smith, 2002). In another con-trolled study usingVR for FOF, long-term follow-up(i.e., 3 years) data suggested that VRE continued tobe more effective than imaginal exposure (Wieder-hold &Wiederhold, 2003; N = 30).Muhlberger and researchers (2001) compared
VRE with relaxation training (N = 30). Bothtreatments were found to be helpful related tonegative cognitions regarding flying, but VRE wasmore effective for specific flying-related behavior.In an attempt to dismantle the components oftreatment for FOF, these researchers compared: (a)cognitive therapy plus VRE with motion simula-tion, (b) cognitive therapy plus VRE withoutmotion simulation, and (c) cognitive therapyalone (Muhlberger, Wiedemann, & Pauli, 2003;N = 45). VRE with or without motion simulationwas more effective than cognitive therapy alone forFOF. Another group of researchers compared VRE
to attention-placebo group therapy (N = 45), whichconsisted of psychoeducation about flying andsharing of fears among group members (Maltby,Irving, Mayers, & Allen, 2002). VRE led to asignificant decline in FOF compared to the grouptherapy, although its superiority was not main-tained at 6-month follow-up. Results from all thesestudies suggested that VRE therapy is more effectivethan nontreatment control groups and at least aseffective as other forms of exposure therapy.The randomized controlled clinical trial reported
here is a replication and extension of a previousclinical trial completed by Rothbaum and collea-gues (2000). This study extends the previous studywith a larger sample size, 6- and 12-month follow-up data, and randomization of the WL group to thetwo active treatments following completion of theWL period. The following primary hypotheses weretested: VRE and SE would be equally effective andmore effective than WL control in reducingparticipants' fears of flying and avoidance behavior,and treatment gains would be maintained at 6- and12-month follow-ups.
Methodparticipants
Eighty-three participants met criteria for the studyand were randomly assigned to the three groups:VRE, SE, and WL. All participants were recruitedbroadly from the local community through news-paper advertising, posted flyers, and referral fromother mental health professionals. To participate inthis free clinical trial, participants met currentDSM-IV criteria for either specific phobia, situa-tional type (i.e., FOF; 88%, n = 73) or panicdisorder with agoraphobia in which flying was thefeared stimulus (11%, n = 9), or agoraphobiawithout a history of panic disorder, in which flyingwas the feared stimulus (1%, n = 1). All assessmentswere conducted by an Independent Assessor (IA),who was blind to the type of treatment received. Alldiagnostic assessments were videotaped and 15were randomly selected to be viewed independentlyby two viewers. To determine the level of agreementamong independent viewers, interrater reliabilitywas computed and resulted in a kappa coefficient of.94, indicating excellent interrater reliability. As inother studies treating participants with FOF, onlyparticipants who had flown at least once beforewere eligible.Demographic information, diagnostic character-
istics, and baseline scores on primary outcomemeasures are presented in Table 1. The sample wasrelatively wealthy and well educated with a meanlevel of education of 16.24 years and most
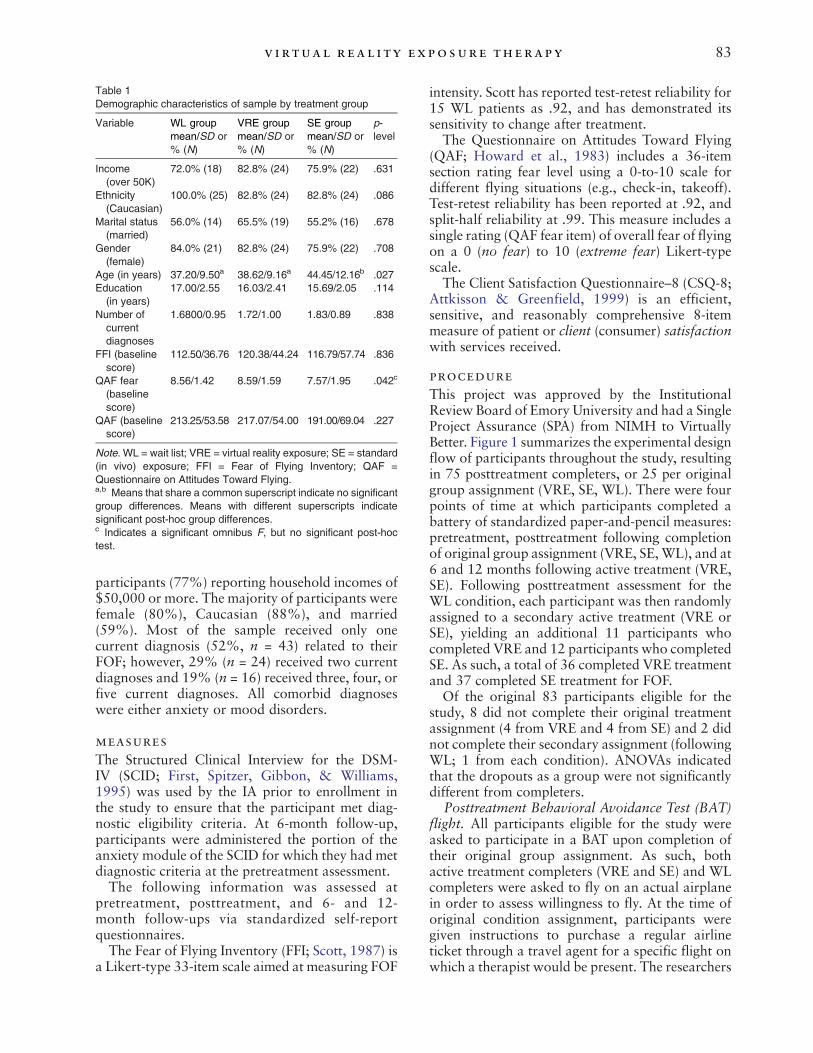
Table 1Demographic characteristics of sample by treatment group
Variable WL groupmean/SD or% (N)
VRE groupmean/SD or% (N)
SE groupmean/SD or% (N)
p-level
Income(over 50K)
72.0% (18) 82.8% (24) 75.9% (22) .631
Ethnicity(Caucasian)
100.0% (25) 82.8% (24) 82.8% (24) .086
Marital status(married)
56.0% (14) 65.5% (19) 55.2% (16) .678
Gender(female)
84.0% (21) 82.8% (24) 75.9% (22) .708
Age (in years) 37.20/9.50a 38.62/9.16a 44.45/12.16b .027Education
(in years)17.00/2.55 16.03/2.41 15.69/2.05 .114
Number ofcurrentdiagnoses
1.6800/0.95 1.72/1.00 1.83/0.89 .838
FFI (baselinescore)
112.50/36.76 120.38/44.24 116.79/57.74 .836
QAF fear(baselinescore)
8.56/1.42 8.59/1.59 7.57/1.95 .042c
QAF (baselinescore)
213.25/53.58 217.07/54.00 191.00/69.04 .227
Note. WL = wait list; VRE = virtual reality exposure; SE = standard(in vivo) exposure; FFI = Fear of Flying Inventory; QAF =Questionnaire on Attitudes Toward Flying.a,b Means that share a common superscript indicate no significantgroup differences. Means with different superscripts indicatesignificant post-hoc group differences.c Indicates a significant omnibus F, but no significant post-hoctest.
83v irtual real i ty exposure therapy
participants (77%) reporting household incomes of$50,000 or more. The majority of participants werefemale (80%), Caucasian (88%), and married(59%). Most of the sample received only onecurrent diagnosis (52%, n = 43) related to theirFOF; however, 29% (n = 24) received two currentdiagnoses and 19% (n = 16) received three, four, orfive current diagnoses. All comorbid diagnoseswere either anxiety or mood disorders.
measures
The Structured Clinical Interview for the DSM-IV (SCID; First, Spitzer, Gibbon, & Williams,1995) was used by the IA prior to enrollment inthe study to ensure that the participant met diag-nostic eligibility criteria. At 6-month follow-up,participants were administered the portion of theanxiety module of the SCID for which they had metdiagnostic criteria at the pretreatment assessment.The following information was assessed at
pretreatment, posttreatment, and 6- and 12-month follow-ups via standardized self-reportquestionnaires.The Fear of Flying Inventory (FFI; Scott, 1987) is
a Likert-type 33-item scale aimed at measuring FOF
intensity. Scott has reported test-retest reliability for15 WL patients as .92, and has demonstrated itssensitivity to change after treatment.The Questionnaire on Attitudes Toward Flying
(QAF; Howard et al., 1983) includes a 36-itemsection rating fear level using a 0-to-10 scale fordifferent flying situations (e.g., check-in, takeoff).Test-retest reliability has been reported at .92, andsplit-half reliability at .99. This measure includes asingle rating (QAF fear item) of overall fear of flyingon a 0 (no fear) to 10 (extreme fear) Likert-typescale.The Client Satisfaction Questionnaire–8 (CSQ-8;
Attkisson & Greenfield, 1999) is an efficient,sensitive, and reasonably comprehensive 8-itemmeasure of patient or client (consumer) satisfactionwith services received.
procedure
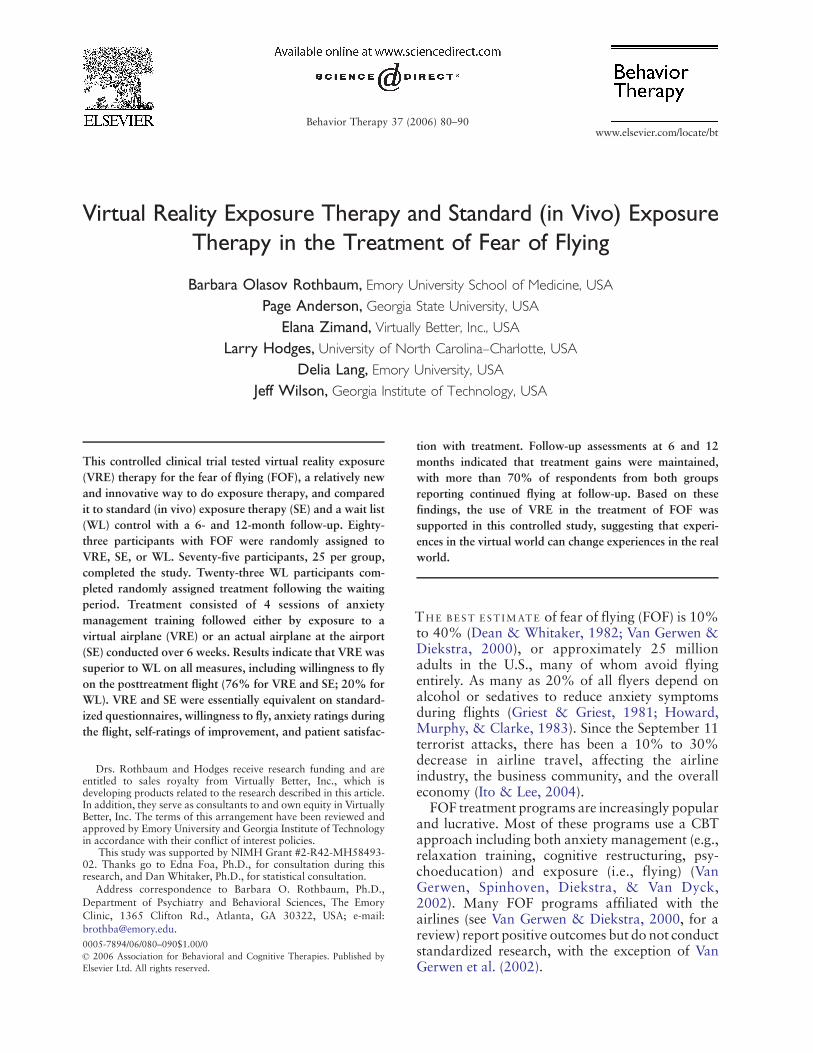
This project was approved by the InstitutionalReview Board of Emory University and had a SingleProject Assurance (SPA) from NIMH to VirtuallyBetter. Figure 1 summarizes the experimental designflow of participants throughout the study, resultingin 75 posttreatment completers, or 25 per originalgroup assignment (VRE, SE, WL). There were fourpoints of time at which participants completed abattery of standardized paper-and-pencil measures:pretreatment, posttreatment following completionof original group assignment (VRE, SE,WL), and at6 and 12 months following active treatment (VRE,SE). Following posttreatment assessment for theWL condition, each participant was then randomlyassigned to a secondary active treatment (VRE orSE), yielding an additional 11 participants whocompleted VRE and 12 participants who completedSE. As such, a total of 36 completed VRE treatmentand 37 completed SE treatment for FOF.Of the original 83 participants eligible for the
study, 8 did not complete their original treatmentassignment (4 from VRE and 4 from SE) and 2 didnot complete their secondary assignment (followingWL; 1 from each condition). ANOVAs indicatedthat the dropouts as a group were not significantlydifferent from completers.
Posttreatment Behavioral Avoidance Test (BAT)flight. All participants eligible for the study wereasked to participate in a BAT upon completion oftheir original group assignment. As such, bothactive treatment completers (VRE and SE) and WLcompleters were asked to fly on an actual airplanein order to assess willingness to fly. At the time oforiginal condition assignment, participants weregiven instructions to purchase a regular airlineticket through a travel agent for a specific flight onwhich a therapist would be present. The researchers
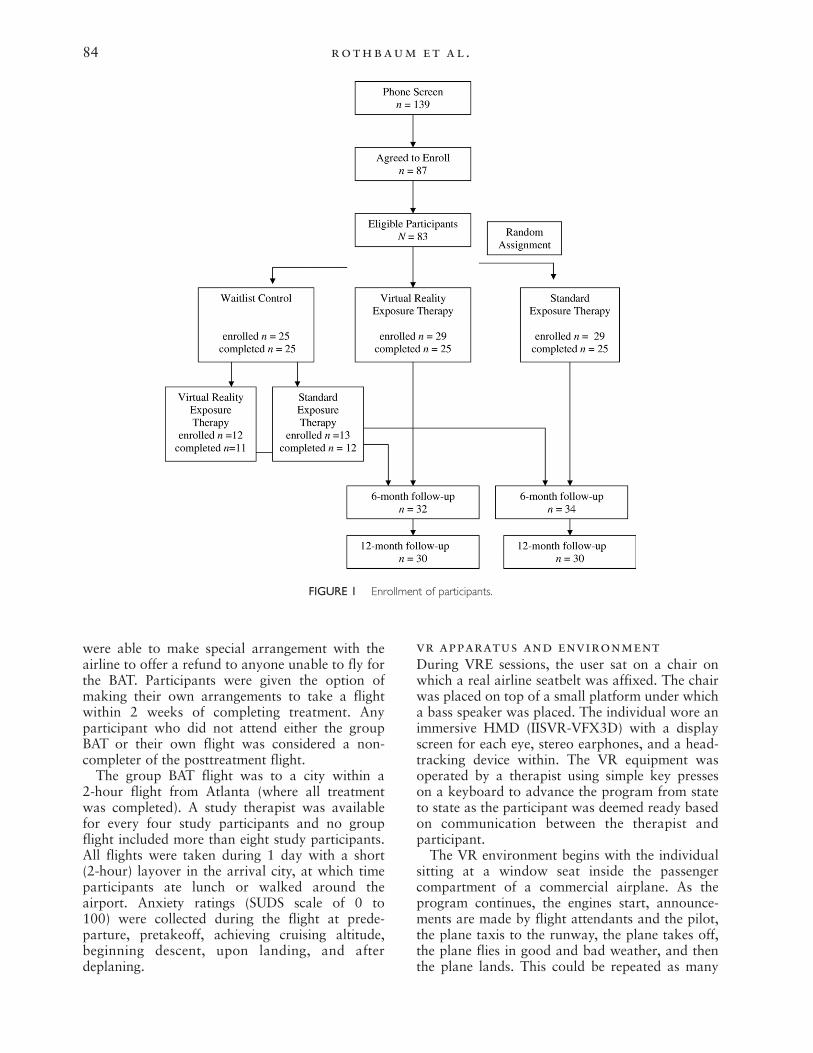
FIGURE 1 Enrollment of participants.
84 rothbaum et al .
were able to make special arrangement with theairline to offer a refund to anyone unable to fly forthe BAT. Participants were given the option ofmaking their own arrangements to take a flightwithin 2 weeks of completing treatment. Anyparticipant who did not attend either the groupBAT or their own flight was considered a non-completer of the posttreatment flight.The group BAT flight was to a city within a
2-hour flight from Atlanta (where all treatmentwas completed). A study therapist was availablefor every four study participants and no groupflight included more than eight study participants.All flights were taken during 1 day with a short(2-hour) layover in the arrival city, at which timeparticipants ate lunch or walked around theairport. Anxiety ratings (SUDS scale of 0 to100) were collected during the flight at prede-parture, pretakeoff, achieving cruising altitude,beginning descent, upon landing, and afterdeplaning.
vr apparatus and environmentDuring VRE sessions, the user sat on a chair onwhich a real airline seatbelt was affixed. The chairwas placed on top of a small platform under whicha bass speaker was placed. The individual wore animmersive HMD (IISVR-VFX3D) with a displayscreen for each eye, stereo earphones, and a head-tracking device within. The VR equipment wasoperated by a therapist using simple key presseson a keyboard to advance the program from stateto state as the participant was deemed ready basedon communication between the therapist andparticipant.The VR environment begins with the individual
sitting at a window seat inside the passengercompartment of a commercial airplane. As theprogram continues, the engines start, announce-ments are made by flight attendants and the pilot,the plane taxis to the runway, the plane takes off,the plane flies in good and bad weather, and thenthe plane lands. This could be repeated as many

85v irtual real i ty exposure therapy
times as necessary during the designated exposuresession using an exposure hierarchy developed bythe study participant together with the therapist.
treatment
Participants were treated for eight individualsessions over 6 weeks. VRE and SE groups receivedidentical treatment for Sessions 1 through 4, whichincluded information gathering and treatmentplanning, and training in anxiety managementtechniques, including breathing retraining, cogni-tive restructuring, thought stopping, and interocep-tive exposure.Exposure was conducted in Sessions 5 through 8.
VRE to sitting in an airplane, takeoffs and landingsin an airplane, and flying in both calm and stormyweather were provided twice weekly for 2 weeks inVirtually Better, Inc.’s office, according to atreatment manual developed by the authors (Roth-baum & Hodges, 1997). For SE sessions, in vivoexposure was conducted at the airport duringSessions 5 through 8. Due to the time required fortravel to and from the airport and cost associatedwith parking, Sessions 5 and 6 were combined intoone extended session, as were Sessions 7 and 8.Sessions 5 and 6 were spent at the airport exposingparticipants to the preflight stimuli (e.g., ticketing,trains, waiting area) and at a coordination centertower exposing patients to viewing planes andspeaking with knowledgeable airport personnel.Sessions 7 and 8 were spent on a stationary airplaneand conducting imaginal exposure on the plane.SUDS rating (0–100) were collected every 5 minutesduring both forms of exposure.
statistical analyses
Analyses included an intent-to-treat (ITT) using thelast value carried forward (LVCF) method tominimize the impact of missing data. Specifically,missing values at any follow-up point were imputedwith the participant's pretreatment score. Thisconservative method was selected in an effort tofurther minimize any potential inflation of post-treatment or follow-up scores. ITT analyses werecompared with results from analyses performed onthe nonimputed data yielding almost identicalresults. For purposes of consistency with priorpublications (Rothbaum et al., 2002), analysesusing the LVCF method are reported below.
Resultsequivalence of groups
Of the 83 participants randomized to the threeconditions, 25 were randomly assigned to the WLcontrol, and 29 to the VRE and SE therapies each.
At baseline, significant differences were foundbetween the WL and SE groups for age, with theSE group being significantly older (mean = 44.45;SD = 12.16) than the WL group (mean = 37.20;SD = 9.50). Additionally, age was significantlydifferent between the VRE and the SE groups, withthe VRE group being significantly younger(mean = 38.62; SD = 9.16) than the SE group(mean = 44.45; SD = 12.16). Due to this significantfinding, subsequent analyses included age as acovariate. Although one of the primary outcomevariables (QAF-fear item) resulted in a significantomnibus F (p = .042), subsequent post-hoc testsindicated no significant difference between thegroups on this variable. No other differences wereobserved for sociodemographic characteristics onany other primary outcome measures (Figure 1).
differences for ffi, qaf, qaf-fearitem using three groups
ANCOVA was utilized to compare differences atposttreatment between WL, VRE, and SE for eachof the three dependent variables, using age andpretreatment scores as covariates. Results indicate asignificant difference for each of the three outcomemeasures (FFI, F[2, 77] = 5.01, p = .009,eta2 = .115; power = .80; QAF, F[2, 77] = 9.27,p = .0001, eta2 = .194; power = .97; QAF-fear item,F[2, 74] = 11.23, p = .0001, eta2 = .233;power = .99). Post-hoc analyses indicate that, foreach outcome measure, both the VRE and SEgroups differed significantly from WL, but did notdiffer significantly from each other (Table 2).
analyses of 6- and 12-monthfollow-up data
Retention was high for the 6-month follow-up, withcompletion rates of 21/25 (84%) for the VR groupand 23/25 (92%) for the SE group. Retention rateswere similarly high for the 12-month follow-upwith19/25 (76%) for both VRE and SE participants.However, in order to maximize statistical power,onceWLparticipantswere randomized to one of thetreatment conditions as described in detail in theMethod section, a larger sample size resulted forboth the VRE and SE groups. Of the 25 WLparticipants, 23 completed treatment, yielding asample of N = 36 for VRE and N = 37 for SE. Thefollow-up data for the entire group who receivedactive treatment were analyzed using ANCOVA tocompare differences between VRE and SE at 6-month and 12-month follow-up, using age andpretreatment scores as covariates (Table 3). Resultsindicate a marginally significant group effect for FFIat 6 months, but no additional significant groupdifferences at either the 6-month follow-up
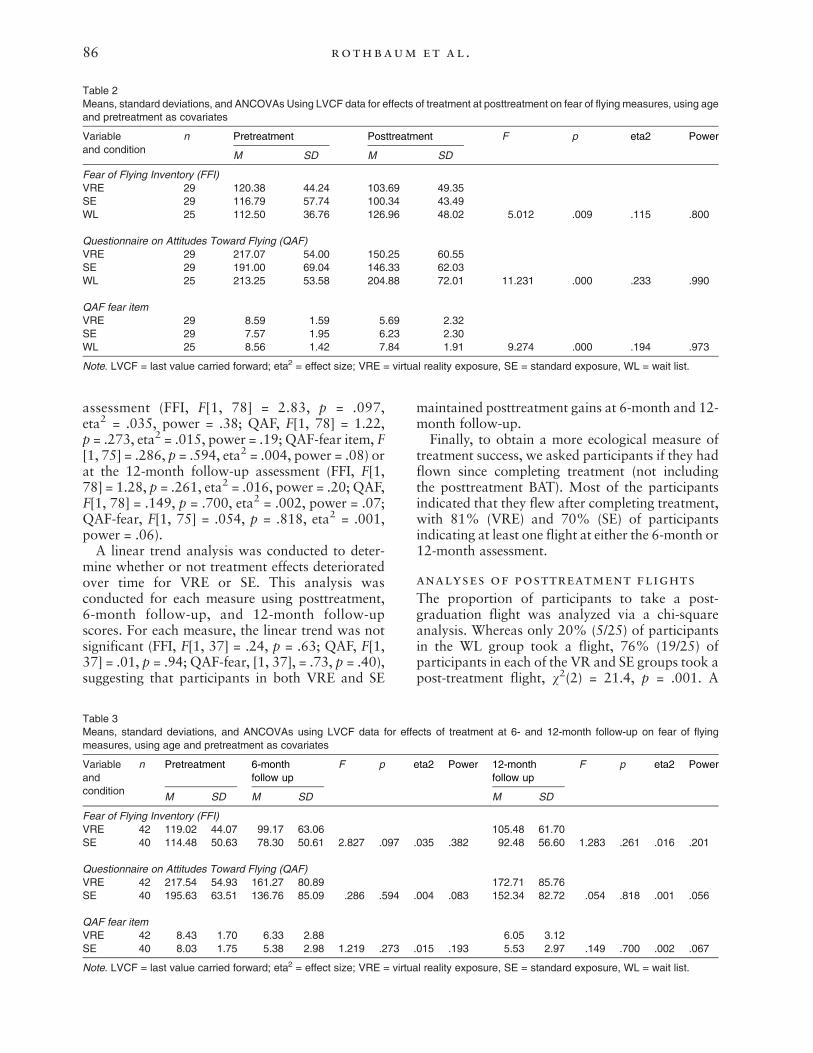
Table 2Means, standard deviations, and ANCOVAs Using LVCF data for effects of treatment at posttreatment on fear of flying measures, using ageand pretreatment as covariates
Variableand condition
n Pretreatment Posttreatment F p eta2 Power
M SD M SD
Fear of Flying Inventory (FFI)VRE 29 120.38 44.24 103.69 49.35SE 29 116.79 57.74 100.34 43.49WL 25 112.50 36.76 126.96 48.02 5.012 .009 .115 .800
Questionnaire on Attitudes Toward Flying (QAF)VRE 29 217.07 54.00 150.25 60.55SE 29 191.00 69.04 146.33 62.03WL 25 213.25 53.58 204.88 72.01 11.231 .000 .233 .990
QAF fear itemVRE 29 8.59 1.59 5.69 2.32SE 29 7.57 1.95 6.23 2.30WL 25 8.56 1.42 7.84 1.91 9.274 .000 .194 .973
Note. LVCF = last value carried forward; eta2 = effect size; VRE = virtual reality exposure, SE = standard exposure, WL = wait list.
86 rothbaum et al .
assessment (FFI, F[1, 78] = 2.83, p = .097,eta2 = .035, power = .38; QAF, F[1, 78] = 1.22,p = .273, eta2 = .015, power = .19; QAF-fear item, F[1, 75] = .286, p = .594, eta2 = .004, power = .08) orat the 12-month follow-up assessment (FFI, F[1,78] = 1.28, p = .261, eta2 = .016, power = .20; QAF,F[1, 78] = .149, p = .700, eta2 = .002, power = .07;QAF-fear, F[1, 75] = .054, p = .818, eta2 = .001,power = .06).A linear trend analysis was conducted to deter-
mine whether or not treatment effects deterioratedover time for VRE or SE. This analysis wasconducted for each measure using posttreatment,6-month follow-up, and 12-month follow-upscores. For each measure, the linear trend was notsignificant (FFI, F[1, 37] = .24, p = .63; QAF, F[1,37] = .01, p = .94; QAF-fear, [1, 37], = .73, p = .40),suggesting that participants in both VRE and SE
Table 3Means, standard deviations, and ANCOVAs using LVCF data for effemeasures, using age and pretreatment as covariates
Variableandcondition
n Pretreatment 6-monthfollow up
F p
M SD M SD
Fear of Flying Inventory (FFI)VRE 42 119.02 44.07 99.17 63.06SE 40 114.48 50.63 78.30 50.61 2.827 .097
Questionnaire on Attitudes Toward Flying (QAF)VRE 42 217.54 54.93 161.27 80.89SE 40 195.63 63.51 136.76 85.09 .286 .594
QAF fear itemVRE 42 8.43 1.70 6.33 2.88SE 40 8.03 1.75 5.38 2.98 1.219 .273
Note. LVCF = last value carried forward; eta2 = effect size; VRE = virtu
maintained posttreatment gains at 6-month and 12-month follow-up.Finally, to obtain a more ecological measure of
treatment success, we asked participants if they hadflown since completing treatment (not includingthe posttreatment BAT). Most of the participantsindicated that they flew after completing treatment,with 81% (VRE) and 70% (SE) of participantsindicating at least one flight at either the 6-month or12-month assessment.
analyses of posttreatment flights
The proportion of participants to take a post-graduation flight was analyzed via a chi-squareanalysis. Whereas only 20% (5/25) of participantsin the WL group took a flight, 76% (19/25) ofparticipants in each of the VR and SE groups took apost-treatment flight, v2(2) = 21.4, p = .001. A
cts of treatment at 6- and 12-month follow-up on fear of flying
eta2 Power 12-monthfollow up
F p eta2 Power
M SD
105.48 61.70.035 .382 92.48 56.60 1.283 .261 .016 .201
172.71 85.76.004 .083 152.34 82.72 .054 .818 .001 .056
6.05 3.12.015 .193 5.53 2.97 .149 .700 .002 .067
al reality exposure, SE = standard exposure, WL = wait list.

87v irtual real i ty exposure therapy
logistic regression revealed that participants inthe VR and SE groups were 12.7 times more likelyto fly than WL participants at posttreatment(OR = 12.7, 95% CI = 3.9, 41.0, p = .001).Furthermore, reported SUDS (range of 0–100, with0 indicating no anxiety and 100 indicating maxi-mum anxiety) during the actual BAT flight were lowfor all groups: 32.5 for VRE (range: 11–57,SD = 13.8), 32.2 for SE (range: 5–77, SD = 19.6),and 34.8 for WL (range: 14–60, SD = 16.8).
posttest rating of improvementvariables
On posttest rating of self-improvement (Likert scalefrom 1 to 7, where 1 = very much improved,4 = unchanged, and 7 = very much worse), asignificant difference between groups emerged, F(2,72) = 34.71, p = .0001, such that participants whoreceived either VRE (mean = 2.00, SD = .82) or SE(mean = 1.86, SD = .76) described themselves asimproved significantly more than WL participants(mean = 3.68, SD = .99). There were no significantdifferences between VRE and SE participants, whoreported themselves as “much improved” onaverage, whereas the WL participants reportedthemselves as “unchanged”.
posttreatment client satisfactionratings
An independent t test was conducted to test whetherthere were any significant differences between VREand SE participants on ratings of client satisfaction.Results indicate no significant difference for meansatisfaction scores between the VRE (mean = 29.56;SD = 3.39) and the SE (mean = 29.52; SD = 3.55)groups (t = .652, p = .517). The range of clientsatisfaction scores was from 18 (low satisfaction) to32 (highest possible satisfaction). The meansobtained from this sample indicate that both groupswere equally, highly satisfied with the treatmentthey received.
diagnostic status
Including the WL participants that were subse-quently treated, a total of 48 out of 66 individuals(73%) completed the diagnostic interview at the 6-month follow-up assessment to determine if theycontinued to meet DSM-IV criteria for flyingphobia. For the total VR group, 71% (22/32) andfor the total SE group, 76% (26/34) no longer metfull criteria.
DiscussionIn summary, VRE therapy was shown to beeffective as measured by standardized question-
naires, by the number of participants to actually flyon a real airplane following treatment, on self-ratings of improvement, and on a measure oftreatment satisfaction. Immediately posttreatment,both VRE and SE reported significantly less flyinganxiety. The two active treatments were equallyeffective on all measures. The gains observed intreatment were maintained at 6- and 12-monthsfollowing treatment with both active treatmentsleading to equivalent improvement. The use of VREtherapy for treatment of FOF was unequivocallysupported in this controlled study.This is the largest controlled clinical trial
comparing VRE to an active in vivo exposuretherapy to a control condition. The strengths of thecurrent study center on the methodological rigoremployed. Participants were randomly assigned totreatment condition. Clear eligibility requirementswere incorporated, including a DSM-IV diagnosis,and all diagnostic interviews were completed by anassessor masked to condition. Standard and psy-chometrically sound self-report measures wereused. Two active treatments were compared anddelivered by the same therapist, treatments werewell delineated, standardized, brief, and easilyreplicated, all leading to a high degree of treatmentintegrity. An equal, and very small, number ofparticipants dropped out from active treatment(n = 4 from each active treatment), and retentionrates were high at 6- and 12-month follow-upassessment (75% and above). A major strength ofthe study was the inclusion of an actual airplaneflight (BAT) following treatment to measure avoid-ance behavior and in vivo anxiety. Although apretreatment BAT flight was not incorporatedinto the design of this clinical trial for severalreasons, including the risk of sensitization, it wouldbe interesting to attempt to use a VR flight as apretreatment BAT tool.Despite these strengths and positive findings,
there are also areas of weakness within the designand implementation of the treatment package.Because two active treatments were compared, it isvery difficult to detect differences between them. Inpart, this is due to the high degree of overlap bet-ween the treatment packages. Both treatmentsincluded identical first componentswhich addressedanxiety-management techniques. As such, it is notpossible to determine the relative benefit of anxietymanagement to the entire treatment package and nodifferences were detected between the two types ofexposure.In addition, the exposures were not parallel, both
in terms of the number of therapeutic contacts andthe content of the exposure sessions. Although theamount of time with the therapist was kept constant

88 rothbaum et al .
during exposure sessions, two double sessions aredifferent from four single sessions. For one, there ismore time to integrate the information andexperience during the exposure sessions, and moretime to complete homework assignments betweenfour sessions than between two sessions. Further-more, the experience of a virtual flight, which canbe repeated many times during sessions, is verydissimilar to the experience of sitting on astationary plane and going through the airportroutines, including watching planes take off.Although in both circumstances, it can be easy toconvince oneself that the exposure is not “for real,”each contains very different sensory experiencesthat cannot easily be compared to one another. Itmay be that the combination of the two types ofexposure could yield even better outcomes for FOF,as they could potentially address different aspects ofan individual’s idiosyncratic fear.Another study limitation is the homogeneous
sample, which makes it difficult to generalize thesefindings. Although efforts were made to recruit adiverse sample, the current sample was highlyeducated, relatively well-off, Caucasian, female,and a little over half were married. Therefore, it isnot possible to predict whether this same treatmentwould be as effective with a more varied popula-tion. However, our clinical experience indicates thisis the typical patient presenting for treatment forFOF.In conclusion, what are the significant benefits
and disadvantages of developing and using VREin the treatment of anxiety? VRE may be cost-effective both to the therapist and the patient inthe treatment of anxiety. Because it allows thetherapist to conduct exposure in the office,eliminating travel time to in vivo settings, morepatients can be seen for the cost of a standardtherapy hour as opposed to extended sessiontimes that insurance companies do not usuallycover. In addition, VR is conducted within theprivacy and safety of the therapist's office, whichreduces risk and possible violations of confiden-tiality. Perhaps because it is still a relatively newtechnique, VR appears to have wide public appealand people seem to be less afraid to confront theirfears in VR as opposed to in real life.Though there is a growing body of literature
suggesting VR is useful for treatment of anxiety, westill know very little about who is likely to benefitfrom VRE. We know that VR does not benefiteveryone; some cannot achieve the suspension ofdisbelief needed to believe that it is “for real,” andothers require some in vivo exposure to assist in thegeneralizability of behavior change in real life. Asthe graphic displays become more sophisticated, it
may be easier to create greater immersion, andtherefore, increased benefit. However, these typesof improvements also add to the cost and timeneeded to develop VR applications, which makesthese systems very expensive and difficult for aclinician to afford outside of a research institution.In general, costs are coming down and the numberof VR applications is on the rise, which willcontribute to making these systems more affordableand thus more available to the public at large.However, VR environments are still limited in thenumber of disorders for which they can be used. Asnew applications are developed and tested, there isalways the need to balance the desire for thebroadest possible use, yet specific enough to addressan individual’s situation. It will be essential that VRenvironments continue to be designed and testedwith multiple applications to keep down costs andmake the tool more accessible to the generalclinician.
ReferencesAnderson, P., Jacobs, C., & Rothbaum, B. O. (2004).
Computer-supported cognitive behavioral treatment ofanxiety disorders. Journal of Clinical Psychology, 60,253−267.
Anderson, P., Rothbaum, B. O., &Hodges, L. F. (2000). Virtualreality: Using the virtual world to improve quality of life inthe real world. Bulletin of the Menninger Clinic Supplement,65, 78−91.
Anderson, P., Rothbaum, B. O., &Hodges, L. F. (2003). Virtualreality exposure in the treatment of social anxiety. Cognitiveand Behavioral Practice, 10, 240−247.
Anderson, P., Rothbaum, B. O., Hodges, L. F., and Zimand,E., (manuscript submitted for publication). Treating socialanxiety using virtual reality exposure: An open clinicaltrial.
Attkisson, C. C., & Greenfield, T. K. (1999). The UCSF clientsatisfaction scales: I. The Client Satisfaction Question-naire–8. In M. E. Maruish (Ed.), Use of psychologicaltesting for treatment planning and outcomes assessment(pp. 1333–1346), 2nd ed. Mahwah, NJ: LawrenceErlbaum.
Basoglu, M., Livanou, M., & Salcioglu, E. (2003). A singlesession with an earthquake simulator for traumatic stress inearthquake survivors. American Journal of Psychiatry, 160,788−790.
Botella, C., Banos, R. M., Perpina, C., Villa, H., Alcaniz, M., &Rey, A. (1998). Virtual reality treatment of claustrophobia:A case report. Behaviour Research and Therapy, 36,239−246.
Botella, C., Banos, R. M., Villa, H., Perpina, C., & Garcia-Palacios, A. (2000). Virtual reality in the treatment ofclaustrophobic fear: A controlled multiple-baseline design.Behavior Therapy, 31, 583−595.
Botella, C., Osma, J., Garcia-Palacios, A., Quero, S., & Banos,R. M. (2004). Treatment of flying phobia using virtualreality: Data from a 1-year follow-up using a multiplebaseline design. Clinical Psychology and Psychotherapy, 11,311−323.
Carlin, A. S., Hoffman, H. G., & Weghorst, S. (1997). Virtualreality and tactile augmentation in the treatment of spider

89v irtual real i ty exposure therapy
phobia: A case study. Behaviour Research and Therapy, 35,153−158.
Carmichael, M., Kovach, G. C., Mandel, A., & Wehunt, J.(2001, June 25). Virtual reality therapy. Newsweek, 53.
Choi, Y. H., Jang, D. P., Ku, J. H., Shin, M. B., & Kim, S. I.(2001). Short-term treatment of acrophobia with virtualreality therapy (VRT): A case report. Cyberpsychology &Behavior, 4, 349−354.
Dean, R. D., & Whitaker, K. M. (1982). Fear of flying: Impacton the U.S. air travel industry. Journal of Travel Research,21, 7−17.
DiFede, J., & Hoffman, H. G. (2002). Virtual reality exposuretherapy for World Trade Center post-traumatic stressdisorder: A case report. Cyberpsychology and Behavior, 5,529−536.
Emmelkamp, P. M. G., Bruynzeel, M., Drost, L., & van derMast, C. A. P. G. (2001). Virtual reality treatment inacrophobia: A comparison with exposure in vivo. Cyber-psychology and Behavior, 4, 335−345.
Emmelkamp, P. M. G., Krijn, M., Hulsbosch, L., de Vries, S.,Schuemie, M. J., & van der Mast, C. A. P. G. (2002). Virtualreality treatment versus exposure in vivo: A comparativeevaluation in acrophobia. Behaviour Research and Therapy,40, 25−32.
First, M. B., Spitzer, R. L., Gibbon, M., & Williams, J. B. W.(1995). Structured clinical interview for DSM IV (SCID.New York: New York State Psychiatric Institute, BiometricsResearch.
Foa, E. B., &Kozak,M. J. (1986). Emotional processing of fear:Exposure to corrective information. Psychological Bulletin,99, 20−35.
Foa, E. B., Steketee, G., & Rothbaum, B. O. (1989). Behavioral/cognitive conceptualizations of post-traumatic stress disor-der. Behavior Therapy, 20, 155−176.
Garcia-Palacios, A., Hoffman, H. G., See, S. K., Tsai, A., &Botella, C. (2001). Redefining therapeutic success withvirtual reality exposure therapy. Cyberpsychology &Behavior, 4, 341−348.
Griest, J. H., &Griest, G. L. (1981). Fearless flying: A passengerguide to modern airplane travel. Chicago: Nelson Hall.
Harris, S. R., Kemmerling, R. L., & North, M. M. (2002). Briefvirtual reality therapy for public speaking anxiety. Cyber-psychology & Behavior, 5, 543−550.
Hoffman, H. (2004). Virtual-reality therapy. Scientific Ameri-can, 291, 58−65.
Howard, W. A., Murphy, S. M., & Clarke, J. C. (1983). Thenature and treatment of fear of flying: A controlledinvestigation. Behavior Therapy, 14, 557−567.
Ito, H., & Lee, D., 2004. Assessing the impact of September 11terrorist attacks on U.S. airline demand. Retrieved February8, 2005, from Brown University Web site: http://www.brown.edu/Departments/Economics/Papers/2003/2003-16_paper.pdf
Krijn, M., Emmelkamp, P. M. G., Biemond, R., de Wilde deLigny, C., Schuemie, M. J., & van der Mast, C. A. P. G.(2004a). Treatment of acrophobia in virtual reality: The roleof immersion and presence. Behaviour Research andTherapy, 42, 229−239.
Krijn,M., Emmelkamp, P.M.G.,Olafsson, R. P.,&Biemond, R.(2004b). Virtual reality exposure therapy of anxiety dis-orders: A review. Clinical Psychology Review, 24, 259−281.
Maltby, N., Irving, K., Mayers, M., & Allen, G. J. (2002).Exposure therapy for the treatment of fear of flying: Acontrolled investigation. Journal of Consulting and ClinicalPsychology, 70, 1112−1118.
Muhlberger, A., Herrmann,M. J., Wiedemann, G., Ellgring, H.,& Pauli, P. (2001). Repeated exposure of flight phobics to
flights in virtual reality. Behaviour Research and Therapy,39, 1033−1050.
Muhlberger, A., Wiedemann, G., & Pauli, P. (2003). Efficacy ofa one-session virtual reality exposure treatment for fear offlying. Psychotherapy Research, 13, 323−336.
North, M. M., North, S. M., & Coble, J. R. (1997). Virtualreality therapy for fear of flying. American Journal ofPsychiatry, 154, 130.
Regenbrecht, H. T., Schubert, T. W., & Friedmann, F. (1998).Measuring the sense of presence and its relations to fear ofheights in virtual environments. International Journal ofHuman-Computer Interaction, 10, 233−249.
Rothbaum, B. O., & Hodges, L. F. (1997). Virtually Bettertherapist manual for fear of flying. Decatur, GA: VirtuallyBetter.
Rothbaum, B. O., Hodges, L. F., Alarcon, R., Ready, D.,Shahar, F., Graap, K., et al. (1999). Virtual reality exposuretherapy for PTSD Vietnam veterans: A case study. Journal ofTraumatic Stress, 12, 263−270.
Rothbaum, B. O., Hodges, L., Anderson, P. L., Price, L., &Smith, S. (2002). Twelve-month follow-up of virtual realityand standard exposure therapies for fear of flying. Journal ofConsulting and Clinical Psychology, 70, 428−432.
Rothbaum, B. O., Hodges, L. F., Kooper, R., Opdyke, D.,Williford, J., & North, M. M. (1995a). Effectiveness ofvirtual reality graded exposure in the treatment of acropho-bia. American Journal of Psychiatry, 152, 626−628.
Rothbaum, B. O., Hodges, L. F., Kooper, R., Opdyke, D.,Williford, J. S., & North, M. (1995b). Virtual reality gradedexposure in the treatment of acrophobia: A case report.Behavior Therapy, 26, 547−554.
Rothbaum, B. O., Hodges, L., Ready, D., Graap, K., &Alarcon, R. (2001). Virtual reality exposure therapy forVietnam veterans with posttraumatic stress disorder. Journalof Clinical Psychiatry, 68, 617−622.
Rothbaum, B. O., Hodges, L. F., Smith, S., Lee, J. H., & Price,L. (2000). A controlled study of virtual reality exposuretherapy for the fear of flying. Journal of Consulting andClinical Psychology, 68, 1020−1026.
Rothbaum, B. O., Hodges, L., Watson, B. A., Kessler, G. D., &Opdyke, D. (1996). Virtual reality exposure therapy in thetreatment of fear of flying: A case report. BehaviourResearch and Therapy, 34, 477−481.
Scott, W. (1987). A fear of flying inventory. In P. Kellar, & S.Hayman (Eds.), Innovations of clinical practice, vol. 7.Sarasota, FL: Professional Resource Exchange.
Smith, S., Rothbaum, B. O., & Hodges, L. F. (1999). Treatmentof fear of flying using virtual reality exposure therapy: Asingle case study. the Behavior Therapist, 22, 154−158.
Szegedy-Maszak, M. (2004, December 6). Conquering ourphobias: The biological underpinnings of paralyzing fears.U.S. News and World Report, 137, 66−74.
Van Gerwen, L. J., & Diekstra, R. F. W. (2000). Fear of flyingtreatment programs for passengers: An international review.Aviation, Space, and Environmental Medicine, 71,430−437.
Van Gerwen, L. J., Spinhoven, P., Diekstra, R. F. W., & VanDyck, R. (2002). Multicomponent standardized treatmentprograms for fear of flying: Description and effectiveness.Cognitive and Behavioral Practice, 9, 138−149.
Wald, J. (2004). Efficacy of virtual reality exposure therapy fordriving phobia: A multiple baseline across-subjects design.Behavior Therapy, 35, 621−635.
Wiederhold, B. K., Gevirtz, R., & Wiederhold, M. D. (1998).Fear of flying: A case report using virtual reality therapywith physiological monitoring. Cyberpsychology and Be-havior, 1, 97−103.

90 rothbaum et al .
Wiederhold, B. K., & Wiederhold, M. D. (2003).Three-year follow-up for virtual reality exposure forfear of flying. Cyberpsychology and Behavior, 6,441−445.
Zimand, E., Anderson, P., Gershon, J., Graap, K., Hodges, L.,& Rothbaum, B. O. (2002). Virtual reality therapy:Innovative treatment for anxiety disorders. Primary Psychi-atry, 9, 51−54.
Zimand, E., Rothbaum, B., Tannenbaum, L., Ferrer, M., &Hodges, L. (2003). Technology meets psychology: Integrat-ing virtual reality into clinical practice. The ClinicalPsychologist, 56, 5−11.
RECEIVED: September 29, 2004ACCEPTED: April 1, 2005Available online 24 Febuary 2006