Embed Size (px)
Citation preview
In thIs Issue
p. 4 What’s your incentive?Read how one organization offers incentives for good work. Also, see one facility’s incentives program on p. 5.
p. 6 Medicare occupational mix adjustmentFind out whether it’s serving its original purpose.
p. 8 Be through with poor throughputRead some best practices to relieve gridlock.
p. 11 Just catching upLearn how the University of North Carolina Health Care System is monitoring progress and reporting the results from its PFS process redesign.
It was only four years ago when Teresa Bassett became
the patient access director at Riverside Health System (RHS)
in Newport News, VA, and immediately recognized a few
disturbing trends. Bassett’s top objective was to reduce ac
counts receivable (A/R) by working with her registration
staff. However, the staff members weren’t yet performing
timeofservice (TOS) collections efforts, and when she
learned that the business office was touching 85% of every
thing that came out of registration, she knew that there
couldn’t be a quick fix. “It wasn’t just bad. It was way bad,”
said Bassett, who spoke during the NAHAM Annual Con
ference in May.
However, the business office now steps in only 24%
of the time, and these instances are rarely due to a reg
istration error. “It’s nice to know that we’re finally not
Case study
Virginia hospital system tackles A/R through registration quality
causing patient accounting additional work,” Bassett said.
The secrets to success: switching from manual to elec
tronic audits; studying quality reports; conducting frequent,
onthespot, informal training; launching a dedicated col
lections initiative, and receiving staff support.
up-front collections
RHS is a fourhospital system located in southeastern
Virginia. In 2004, RHS was in the same boat as most facil
ities. It wasn’t doing much to ensure TOS accuracy and
it had yet to look into incentives (e.g., bonuses and pay
scales) to motivate staff members to be more aggressive.
“Administration
was timid about
starting to collect
money,” Bassett
said. “We hadn’t done it before, and we’d have to teach
staff how to do it efficiently.” RHS started from scratch,
purchasing credit card machines and developing protocols
to indicate when TOS was due and when it wasn’t.
Although there was a learning curve, staff members got
it down and now excel at the process. “Now we have very
clear policies, and we’re on target to collect $3 million this
year,” she said.
RHS is aggressive in its collections efforts, but its registrars
always have their eyes on customer service. The organization
offers a 20% discount to patients who pay their copay and/
or deductible at the TOS. “It works wonderfully,” Bassett said.
Some patients naturally say they’ll pay later when a reg
istrar asks for the upfront money. “But when we tell them
about the discount, they’re usually happy to pay,” she said.
“We do it across the board for every patient.”
staff participation
RHS is fortunate to have maintained much of its reg
istration staff for years. But when candidates interview,
> continued on p. 2
August 2007 Vol. 4, No. 8
“ It wasn’t just bad. It
was way bad.”
—Teresa Bassett
Patient Access AdvisorPage �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
Registration quality < continued from p. 1
Bassett insists that they be comfortable with collecting
money. “It’s one of the most important aspects of the
job,” she said.
However, Bassett prefers applicants who don’t have
registration experience. “I prefer not to hire people with
old, ingrained philosophies from another facility,” she
said. “I’ve had much better luck hiring people without
experience.”
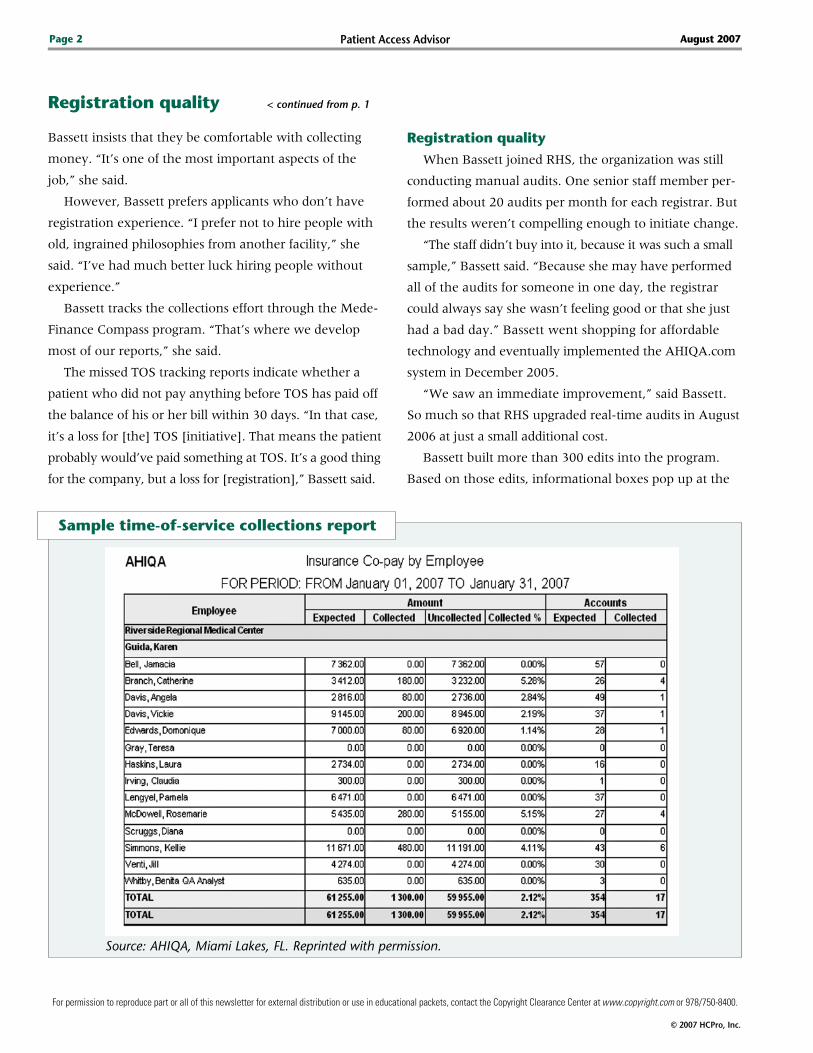
Bassett tracks the collections effort through the Mede
Finance Compass program. “That’s where we develop
most of our reports,” she said.
The missed TOS tracking reports indicate whether a
patient who did not pay anything before TOS has paid off
the balance of his or her bill within 30 days. “In that case,
it’s a loss for [the] TOS [initiative]. That means the patient
probably would’ve paid something at TOS. It’s a good thing
for the company, but a loss for [registration],” Bassett said.
Registration quality
When Bassett joined RHS, the organization was still
conducting manual audits. One senior staff member per
formed about 20 audits per month for each registrar. But
the results weren’t compelling enough to initiate change.
“The staff didn’t buy into it, because it was such a small
sample,” Bassett said. “Because she may have performed
all of the audits for someone in one day, the registrar
could always say she wasn’t feeling good or that she just
had a bad day.” Bassett went shopping for affordable
technology and eventually implemented the AHIQA.com
system in December 2005.
“We saw an immediate improvement,” said Bassett.
So much so that RHS upgraded realtime audits in August
2006 at just a small additional cost.
Bassett built more than 300 edits into the program.
Based on those edits, informational boxes pop up at the
sample time-of-service collections report
Source: AHIQA, Miami Lakes, FL. Reprinted with permission.

Patient Access Advisor Page �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
end of each registration to indicate incomplete or incor
rect information for the registrar to fix while the patient
is still in the registration area.
For example, the program networks with the U.S.
Post Office to verify addresses. “It doesn’t verify that it’s
the right address,” said Bassett. “But it verifies that it is a
valid address, and that is extremely useful.”
Bassett had realized that many of the registration
errors stemmed from Medicare policy numbers, which
have nine digits and an alpha character.
“The registrars were invariably leaving off that alpha
character,” she said. “Now it doesn’t happen at all
anymore.”
See “Sample employee error report” below for an
example of a registrar’s detailed field errors report. This
report helps Bassett identify where each registrar needs
additional training.
“We can run the reports whenever we want, so we’re
always on top of things,” she said.
Additional benefits
The AHIQA program also allows Bassett to moni
tor patient wait times. As part of the “lobby” function,
registrars check patients in and administer an electronic
signin sheet, and managers can track the movement of
patients.
“Managers used to have to walk around to monitor
patient volume in each registration area. Now they can sit
in their office and watch it on their computer screen. It’s
allowed us to immediately adjust staffing levels in the vari
ous registration areas based on the patient volume. At the
same time, it is allowing the managers to spend their time
more appropriately,” said Bennett.
“Do we need to call extra help in? Is our inpatient
area swamped and our outpatient area slow? If so,
can we move people around to help out the inpatient
area? We really take advantage of this at all of our
acutecare facilities and outpatient diagnostic centers,”
she added. n
sample employee error report
Source: AHIQA, Miami Lakes, FL. Reprinted with permission.

Patient Access AdvisorPage �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
teresa Bassett, the patient access director at Riverside
Health System (RHS) in Newport News, VA, knew that the
best way to make the organization’s aggressive time-of-ser-
vice (TOS) collections and registration quality initiatives fly
was to get staff members excited about them.
So in October 2005, well before many of its peers thought
to develop and implement an organized rewards program,
RHS began challenging staff members to perform their regis-
tration duties more efficiently by giving them an incentive to
be great at their jobs.
The results have been tremendous—RHS has seen in-
creased TOS collections, fewer registration mistakes, and
little staff turnover.
Certifications
First, Bassett set out to educate staff members about
their importance to the financial well-being of the organiza-
tion. All too often, registration staff members receive too
much of the criticism and not enough of the praise, she says.
“I wanted our staff to understand how important they are.
If they don’t do the job well, we won’t get paid timely or pos-
sibly at all,” Bassett says. “I wanted to build their confidence
and show that they are not just a registrar.”
To further this goal, RHS began offering $500 bonuses for
patient access staff members who passed the certified patient
access associate exam.
RHS paid the exam fee the first time for each staff member
who took the exam. Eighty percent of the system’s patient
access staff members took the exam, and 75% passed.
“Staff morale was dramatically increased,” Bassett says.
Random gratitude
RHS has worked diligently to create an environment in
which hard work is always noticed—and often rewarded.
“We have a manager’s toolbox filled with movie
passes, gift cards for our cafeteria, Starbucks gift certificates,
and other gifts we can use to reward staff that go above
and beyond,” says Bassett. “We want to continue encourag-
ing staff to work hard, and this is a great way to
do so.”
Incentive plans: Give a little, get a lot back
Incentives program
RHS also has a quarterly incentives program for up-front
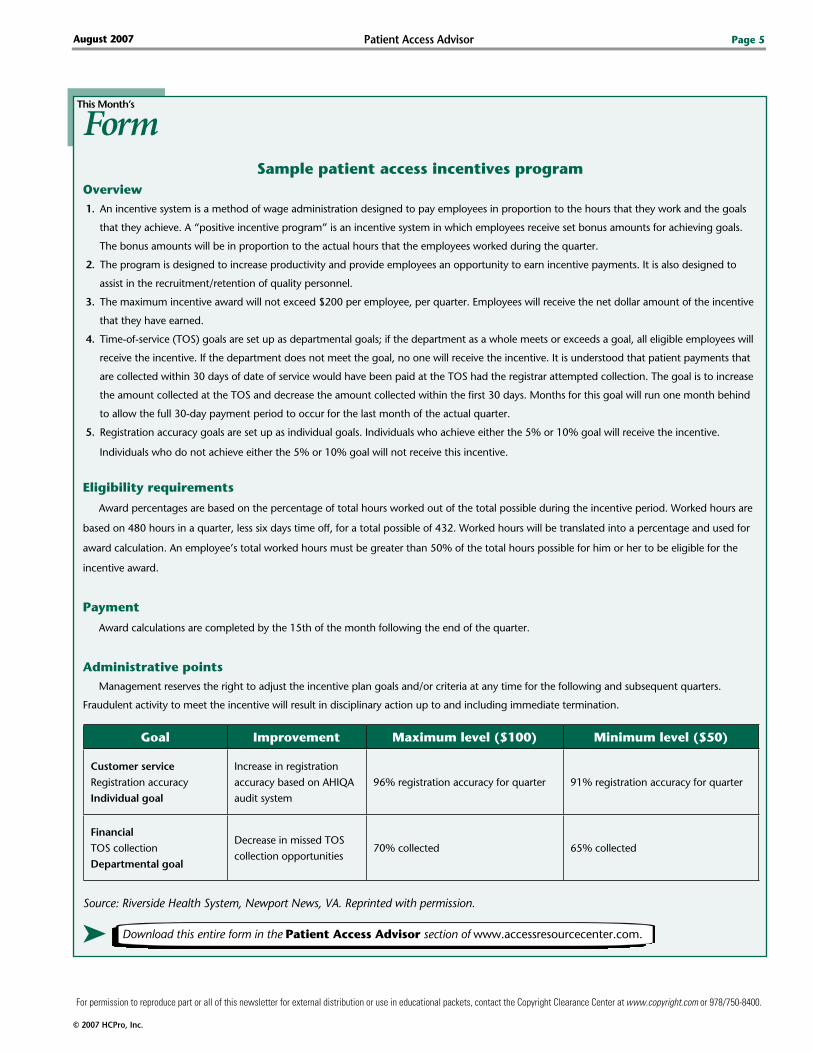
collections and registration accuracy. (See “Sample patient
access incentives program” on p. 5 to see a copy of the
policy.)
For up-front
collections, a
staff member
will receive a
$100 bonus for
collecting 70%
or more of all of
the TOS money due to the registrars for that quarter. If the
staff member collects between more than 65%–69.9% of all
the TOS money due to them for that quarter, he or she will
receive a $50 bonus.
For registration accuracy, a staff member will receive
a $100 bonus if he or she has an accuracy rate of 96% or
higher for the quarter. The staff member will receive a $50
bonus for an accuracy rate of 91%–95.9%.
Those parameters may need to change soon as RHS
registrars have gone from 65% accuracy to 98.7% during
the past few years. “We originally had the top goal at 85%
accurate, so I guess we’ll probably have to raise the bar
again,” Bassett says.
An easy sell
Don’t anticipate much pushback from administration,
Bassett says. “We collect probably 20-fold the amount that
we’re paying out,” she says. “Plus you can’t really put a dol-
lar amount on what the accuracy does on bills dropping
clean and no one needing to touch them.”
But Bassett insists that you need a legitimate registration
audit system to pull it off. “My feeling is providers are wast-
ing their time doing manual audits,” she says.
Just as important as the financial gains, Bassett says, is
that registration staff members are happier with their jobs
now. “They’re talking to us more, coming forward with sug-
gestions,” she says. “They just feel proud of their work. And
that’s very important.”
“ We originally had the top
goal at 85% accurate, so I
guess we’ll probably have
to raise the bar again.”
—Teresa Bassett
Patient Access Advisor Page 5
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
FormThis Month’s
➤ Download this entire form in the Patient Access Advisor section of www.accessresourcecenter.com.
sample patient access incentives programOverview1. An incentive system is a method of wage administration designed to pay employees in proportion to the hours that they work and the goals
that they achieve. A “positive incentive program” is an incentive system in which employees receive set bonus amounts for achieving goals.
The bonus amounts will be in proportion to the actual hours that the employees worked during the quarter.
2. The program is designed to increase productivity and provide employees an opportunity to earn incentive payments. It is also designed to
assist in the recruitment/retention of quality personnel.
3. The maximum incentive award will not exceed $200 per employee, per quarter. Employees will receive the net dollar amount of the incentive
that they have earned.
4. Time-of-service (TOS) goals are set up as departmental goals; if the department as a whole meets or exceeds a goal, all eligible employees will
receive the incentive. If the department does not meet the goal, no one will receive the incentive. It is understood that patient payments that
are collected within 30 days of date of service would have been paid at the TOS had the registrar attempted collection. The goal is to increase
the amount collected at the TOS and decrease the amount collected within the first 30 days. Months for this goal will run one month behind
to allow the full 30-day payment period to occur for the last month of the actual quarter.
5. Registration accuracy goals are set up as individual goals. Individuals who achieve either the 5% or 10% goal will receive the incentive.
Individuals who do not achieve either the 5% or 10% goal will not receive this incentive.
eligibility requirements
Award percentages are based on the percentage of total hours worked out of the total possible during the incentive period. Worked hours are
based on 480 hours in a quarter, less six days time off, for a total possible of 432. Worked hours will be translated into a percentage and used for
award calculation. An employee’s total worked hours must be greater than 50% of the total hours possible for him or her to be eligible for the
incentive award.
Payment
Award calculations are completed by the 15th of the month following the end of the quarter.
Administrative pointsManagement reserves the right to adjust the incentive plan goals and/or criteria at any time for the following and subsequent quarters.
Fraudulent activity to meet the incentive will result in disciplinary action up to and including immediate termination.
Source: Riverside Health System, Newport News, VA. Reprinted with permission.
Goal Improvement Maximum level ($100) Minimum level ($50)
Customer service
Registration accuracy
Individual goal
Increase in registration
accuracy based on AHIQA
audit system
96% registration accuracy for quarter 91% registration accuracy for quarter
FinancialTOS collection
Departmental goal
Decrease in missed TOS
collection opportunities70% collected 65% collected
Patient Access AdvisorPage �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
Medicare occupational mix adjustment: healthcare experts question whether it serves its original purposeby Tina Ford and Scott Besler
Congress enacted the Medicare occupational mix adjust
ment (MOMA) in federal fiscal year (FFY) 2005 as part of
the Benefits Improvement and Protection Act of 2000.
The MOMA is one component of the Medicare wage
index reimbursement methodology, which the federal
government uses as a mechanism to recognize the differ
ent wages hospitals in different geographic areas pay.
The general concept of MOMA is to control the effect
of a hospital’s employment choices on the wage index.
Currently, the MOMA methodology basically works this
way: If a labor market area’s nursing average hourly wage
is higher than the national average, a negative MOMA
applies and reduces the overall wage index factor for that
labor market area.
The reverse is true if a labor market area’s nursing
average hourly wage is lower than the national average;
the labor market experiences a positive MOMA, which
increases the labor market area’s wage index.
Therefore, the MOMA tries to adjust for hospital man
agement decisions rather than account for the geographic
difference in the cost of labor. With that said, one would
expect that a healthcare facility in New York City would
receive a higher Medicare wage index factor than one in
Mississippi.
This would be a result of the higher average hourly
wage in New York City. However, you’d be surprised
to discover that hospitals in New York City actually
receive positive MOMAs, whereas many other hospitals
located in rural areas receive negative MOMAs. To be
exact, onethird of rural hospitals currently receive a
negative MOMA.
MOMA is meant to benefit rural hospitals
To make sense of this, it is necessary to determine
which hospitals are supposed to benefit from MOMA.
Historically, rural healthcare associations have claimed
that there is an inequity in current wage index calcula
tions due to hospital employment choices.
Therefore, Congress enacted, and CMS implemented,
the MOMA to benefit rural hospitals. CMS has made
revisions to the MOMA methodology since its inception
in October 2004, and the same result has occurred each
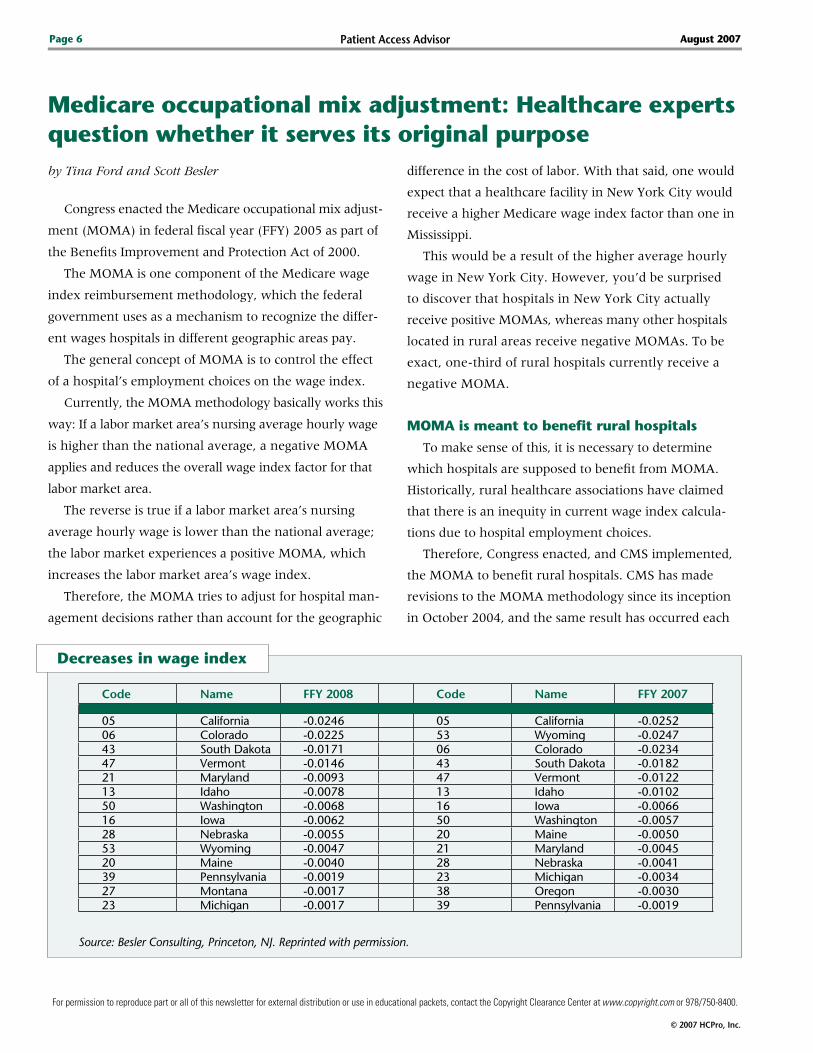
Decreases in wage index
Code Name FFY 2008 Code Name FFY 2007
05 California -0.0246 05 California -0.025206 Colorado -0.0225 53 Wyoming -0.024743 South Dakota -0.0171 06 Colorado -0.023447 Vermont -0.0146 43 South Dakota -0.018221 Maryland -0.0093 47 Vermont -0.012213 Idaho -0.0078 13 Idaho -0.010250 Washington -0.0068 16 Iowa -0.006616 Iowa -0.0062 50 Washington -0.005728 Nebraska -0.0055 20 Maine -0.005053 Wyoming -0.0047 21 Maryland -0.004520 Maine -0.0040 28 Nebraska -0.004139 Pennsylvania -0.0019 23 Michigan -0.003427 Montana -0.0017 38 Oregon -0.003023 Michigan -0.0017 39 Pennsylvania -0.0019
Source: Besler Consulting, Princeton, NJ. Reprinted with permission.

Patient Access Advisor Page 7
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
time—up to onethird of rural core based statistical areas
(CBSA) are affected negatively. (See “Negative MOMA in
rural areas” below for a list of rural areas that witnessed a
negative MOMA.)
As you can see from “Decreases in wage index”
on p. 6 many of the rural areas adversely affected in
FFY 2007 are adversely affected in the projected data
for FFY 2008. This is not much of a coincidence, as
CMS will also use the data from 2007 in 2008 (albeit
one additional quarter). The data are from the same cal
endar year (2006).
CMs rolls out full implementation of MOMA
But that is not the only change in the MOMA
methodology. The MOMA methodology applied begin
ning in FFY 2007 contained several changes from the
previous version that was in effect for FFY 2005 and
FFY 2006.
The most notable change was the full implementa
tion of the MOMA. The initial methodology (used in
FFY 2005 and FFY 2006) was implemented at only 10%
of CBSAs (the current methodology is implemented at
100%). In FFY 2006, 34 of the 47 rural CBSAs witnessed
a reduction of their wage index value as a result of the
MOMA. But as you can see in “Decreases in wage index”
on p. 6, the decreases to the wage index in FFY 2006
were not as severe as those in FFY 2007 and FFY 2008,
as shown previously.
MOMA’s success is still unclear
Is MOMA serving its purpose? It appears that CMS
may have answered that question in FFY 2005, when
it was obligated by statute to implement MOMA but
only did so at 10%. CMS kept MOMA at 10% until
a courtimposed mandate to implement at 100% in
FFY 2007.
Although CMS has the authority to revise the MOMA’s
methodology, it does not have the authority to imple
ment it at less than 100%. The answer to the question
of whether MOMA is serving its purpose lies with its
creators in Congress, as it will take a statutory change
to either eliminate or reduce the effect of MOMA.
Congress did pass the Tax Relief and Health Care Act
of 2006, which contains a statute for the Medicare Pay
ment Advisory Commission to study alternatives to the
current Medicare wage index methodology and issue a
report. n
Editor’s note: Ford is a senior manager and Besler is a man-
ager at Besler Consulting in Princeton, NJ.
negative MOMA in rural areas
RuralRural core based
statistical areas
10%
Implementation
Code Name FFY 2006*
12 Hawaii -0.003845 Texas -0.003244 Tennessee -0.003019 Louisiana -0.002904 Arkansas -0.002837 Oklahoma -0.002542 South Carolina -0.002411 Georgia -0.001913 Idaho -0.001901 Alabama -0.001951 West Virginia -0.001810 Florida -0.001826 Missouri -0.001825 Mississippi -0.001533 New York -0.001518 Kentucky -0.001549 Virginia -0.001435 North Dakota -0.001103 Arizona -0.001046 Utah -0.001014 Illinois -0.000834 No. Carolina -0.000732 New Mexico -0.000729 Nevada -0.000617 Kansas -0.000621 Maryland -0.000623 Michigan -0.000450 Washington -0.000315 Indiana -0.000308 Delaware -0.000316 Iowa -0.000328 Nebraska -0.000324 Minnesota -0.000236 Ohio -0.0001
* Previous methodology that CMs revised as a result of
the Bellevue v. Leavitt case.
Source: Besler Consulting, Princeton, NJ. Reprinted with permission.
Patient Access AdvisorPage 8
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
Patient throughput: Determine the severity of your problem and identify realistic solutions for your facility
Poor patient throughput is common in hospitals nation
wide—both large and small, rural and urban. EDs are
overcrowded, beds are scarce, space is limited, and quality
of care and customer service ratings are down significantly.
According to a study from The Lewin Group, there
were nearly 5.3 billion ED visits in 2004. In 1991, there
were only about 85 million visits. During this same time
period, the number of EDs dramatically decreased.
“This has created a significant problem causing capac
ity issues,” said Susan Werthem, RN, consulting man
ager for revenue management at IMA Consulting in
Chadds Ford, PA, who spoke during the NAHAM Annual
Conference in May. “The increased aged population, unin
sured, and boarded patients only compound the situation.”
Overcrowding directly results in diversion. It also frus
trates referring physicians, hospital staff members, and
patients and their families, Werthem said. To a patient
access professional, this is old news. However, there are
new bestpractice approaches, such as admissions units,
that can help you relieve this gridlock.
Determine whether you measure up
The first step is to measure key performance indica
tors (KPI) to determine the severity of the problem within
your organization. Werthem suggested that you take a
long, hard look at the following areas:
➤ The hours that your facility is on diversion.
Examine diversion by hour of day and day of week. Per
haps your facility is on diversion more often at a certain
time of day. “See if you can find a trend,” Werthem said.
Then calculate the ramifications of that trend.
Not only is it important to compile this information
to fuel any process change, The Joint Commission also
requires you to track patient throughput data (Joint Com
mission standard LD3.15.10). “You need to demonstrate
that you’re reviewing the data and discussing it on a regu
lar basis, resulting in quality improvement,” said Werthem.
The financial impact of diversion is not just from
the loss of ED patients. The loss of revenue is also seen
through the potential loss of ED admissions and market
share. “Determine the average ED revenue generated,”
Werthem said. “Then multiply that times the potential
number of lost ED patients due to diversion to determine
the financial impact.”
You can also calculate the same for potential ED
admissions, she added.
➤ Admissions. Measure ED and direct admissions by
time of day and day of week. “You’re looking for trends that
might suggest patients are waiting and beds aren’t available
because the discharges aren’t out on time,” Werthem said.
If that’s the case, Werthem said, work to communicate the
discharge time expectation to patients and the physicians
right from the start. “If people understand this, they are
more likely to follow through,” Werthem said.
➤ Average length of stay (LOS) for general acute
care. You’ll want to know whether patients of a particu
lar physician have a longer LOS than other physicians’
patients. If you know that, you can target particular prob
lems with staff members.
➤ Noon occupancy. Compare your noon census
with your midnight census. “That might help identify a
discharge problem,” Werthem said. Perhaps one end of
the throughput cycle is lagging.
➤ Wait times for inpatient beds. This tracks the
performance of patient access and illustrates how many
patients you are boarding. “Ask yourself if you’re utiliz
ing precious inpatient beds for lower reimbursement out
patient services,” said Werthem.
➤ Wait times from registration to ED bed. It’s
important to see whether patient access is part of the
problem or the solution. “Frequently the registration is
viewed as the bottleneck,” Werthem said. “Obtain the
data to identify registration opportunities for improve
ment or to dispel the myth.”
Patient Access Advisor Page �
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
➤ Average discharge time. It’s ideal for your dis
charge time to average close to 11 a.m. to keep with a
healthy discharge flow. “You need to set that expectation,
or else it won’t work,” said Werthem.
the effect on your bottom line
Poor throughput affects many people and, ultimately,
its greatest effect is on your patients and the organiza
tion’s finances. The following are several other sources
of lost revenue Werthem associated with throughput
problems:
➤ Cancelled surgeries and other procedures
➤ Outpatients occupying inpatient beds for less or no
reimbursement
➤ A discharged patient occupying a bed while waiting
for tests, a meal, or a ride home
➤ Diminished DRG profitability due to prolonged LOS
➤ Loss of market share
Werthem noted two longterm solutions. You can either
add more beds and staff members at increased costs, or you
can manage patient throughput to increase revenues and
open more of your existing beds. Before you consider pro
posing expansion to your administration, ask yourself:
➤ What kind of beds do I need?
➤ Can I find the nursing and technical staff we’ll need?
➤ Will I have consistent use of new beds, or will I be able
to use them only during crisis periods?
A more realistic approach is to manage throughput,
process to process, said Werthem. For starters, decrease
LOS through the following practices:
➤ Monitoring LOS by physician and DRG
➤ Enforcing discharge hours
➤ Discharging patients timely in the computer
➤ Ensuring timely turnaround from ancillary departments
Before you do anything, Werthem said your organi
zation should schedule crossdepartmental meetings to
discuss the capacity management from everyone’s view
point. These are hospitalwide problems. Make sure to
involve the following people and department representa
tives in the discussion:
➤ CEO
➤ CFO
➤ Chief operating officer
➤ Vice president of nursing
➤ ED nursing manager
➤ Medical director
➤ Patient access director
➤ PFS director
➤ Case management director
➤ Ancillary department directors
➤ Bed czar
➤ Bed board manager
➤ Nurse manager of discharge and LOS
Your source code: N0001
Name
Title
Organization
Address
City State ZIP
Phone Fax
E-mail address(Required for electronic subscriptions)
q Payment enclosed. q Please bill me.q Please bill my organization using PO # q Charge my: q AmEx q MasterCard q VISA
Signature(Required for authorization)
Card # Expires(Your credit card bill will reflect a charge to HCPro, the publisher of PARC.)
q Start my subscription to Patient Access Resource Center immediately.
Options No. of issues Cost Shipping Total
q 1 yr membership 12 issues $399 (PARC) $24.00
Sales tax (see tax information below)*
Grand total
Order online at www.hcmarketplace.com.
Be sure to enter source code N0001 at checkout!
*Tax Information Please include applicable sales tax. Electronic subscriptions are exempt. States that tax products and shipping and handling: CA, CO, CT, FL, GA, IL, IN, KY, LA, MA, MD, ME, MI, MN, MO, NC, NJ, NM, NY, OH, OK, PA, RI, SC, TN, TX, VA, VT, WA, WI, WV. State that taxes products only: AZ. Please include $27.00 for shipping to AK, HI, or PR.
Mail to: HCPro, P.O. Box 1168, Marblehead, MA 01945 Tel: 800/650-6787 Fax: 800/639-8511 E-mail: [email protected] Web: www.hcmarketplace.com
For discount bulk rates, call toll-free at 888/209-6554.
PARC Subscriber Services Coupon
> continued on p. 10

Patient Access AdvisorPage 10
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
Patient throughput < continued from p. 9
Admissions units
A 2002 Government Accountability Office survey
revealed that 90% of boarded patients in the ED waited
more than two hours for an inpatient bed. The Hospital
Advisory Board estimates that it takes eight hours to admit a
patient. Ideally, you should complete the admissions process
in two hours. “An admissions unit allows you to complete
paperwork, initiate medications, and ensure xrays are start
ed, all in that twohour window,” Werthem said.
Assigning the admissions functions to one unit allows
staff members to perform the admission quicker. The
familiarity with these tasks speeds up the process, just as
the sameday surgery staff is able to prepare a patient for
surgery quickly. “The work an admissions unit can per
form could potentially knock a half day off the [LOS] for
an individual patient,” she said.
Consider opening an admission and discharge center,
a selfcontained unit that provides initial clinical care
to patients for whom an admission order has already
been written. Location is additionally important, said
Werthem. Ideally, you should locate the unit near the
ED and the registration department. Your staff compli
ment for a 12bed unit may include about 9.5 fulltime
employees, including nurses, a nurse unit manager, a
bed czar, clinical technicians, and a unit secretary.
“If I bring my grandmother in, I can talk to admitting
while the IV is started,” she said. “Admitting has access
to the patient to finalize questions with my grandmoth
er. Additionally, financial issues can be discussed and
required signatures obtained prior to transfer to the floor.
Everyone is accessible there.”
Werthem recommends that you do not treat obstet
rics and psychiatric patients at the admission center.
The unit could also serve as a comfortable area in which
discharged patients can wait for transportation home,
get their prescriptions filled, and schedule followup
appointments.
“However, a facility may not be in the financial posi
tion to build an admissions unit,” she said. “When that is
the case, we have seen facilities create admissions nurses,
who go to the unit to admit the patient.”
An admissions unit is only one part of the solution.
Daily capacity management meetings, physician involve
ment, and strong leadership are also essential.
“Whatever solutions are put into place, you must be
proactive. Once you stop, people begin to return to their
old ways, as many do not like change,” said Werthem.
“Keep your eye on the ball.” n
Once you’ve determined that your facility has capacity management concerns, IMA Consulting recommends taking the fol-
lowing steps:
➤ Measure key patient-flow statistics and make them available to the executive leadership group
➤ Develop an administratively directed, high-level, physician-involved work group to address capacity problems
➤ Perform a financial impact study to determine revenue opportunities through improved capacity management
➤ Identify a high-level administrative leader with the ability to cross over department lines of authority to oversee daily patient
throughput
➤ Report capacity management progress objectively/statistically to the executive leadership group at least once per month.
➤ Engage a facilitator to assist the organization with overall implementation guidance
Source: IMA Consulting, Chadds Ford, PA. Reprinted with permission.
Capacity management steps to success
➤ Download this entire form in the Patient Access Advisor section of www.accessresourcecenter.com.
Patient Access Advisor Page 11
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
Follow-up
unChCs monitors initiative progress, reports resultsEditor’s note: PAA just completed a four-part series that
examined the significant patient financial process changes
that the University of North Carolina Health Care System
(UNCHCS) in Chapel Hill, NC, has made during the past year.
In this month’s series follow-up, PAA illustrates UNCHCS’
patient-focused collections efforts and progress monitoring and
reporting.
Over the past year, officials at UNCHCS thoroughly
examined every financial process. They considered cus
tomer service, financial viability, and staff burden, and
they drew up realistic changes that would keep each of
the system’s priority interests in mind.
In many cases, they tore down the process structure
and put up new walls from scratch.
When they completed their entire process redesign,
all that was left was a strategy to monitor progress and
report results, says Karen McCall, UNCHCS’ vice presi
dent of public affairs and marketing.
“It was important for us as a system to [track our
performance],” she says.
Instituting audits for charity applications
Officials made wholescale changes to the manner
in which the system screened patients for eligibility,
assisted patients in the process, and alerted patients
of the charity care program.
But the changes were no good if UNCHCS couldn’t
determine whether the new program worked.
UNCHCS designed and instituted an audit process
for all charity care applications and began tracking
the number of patients UNCHCS approved for finan
cial assistance every quarter.
Almost immediately, UNCHCS recorded a 20% in
crease in the number of applications patients filled out.
“It was a definite and noticeable increase for us,” says
McCall. “It told us the process was working.”
Assessing the availability of bilingual Medicaid
assistance counselors
To further the system’s efforts to reach out to the com
munity’s bilingual population, UNCHCS is working with
nine communitybased practices and their bilingual coun
selors to ensure that Spanishspeaking families have the
same access to financial counseling as Englishspeaking
families.
This is another
process that has
seen tremendous
results.
“Our Medicaid
applications are
now way up,”
McCall says. “We
haven’t gotten our Medicaid approvals up much, but our
applications are definitely up. And that’s a definite win
for the system.”
UNCHCS has also begun to use mystery shoppers to
test access to financial assistance.
Letting five principles shape the change
UNCHCS is monitoring progress but also emphasizing
to staff members the following key principles that evolved
from the process redesigns:
➤ Exhaust all third-party options to cover the
cost of care. At the end of fiscal year 2006, UNCHCS
had a staggering $290 million bottled up in accounts
“ We haven’t gotten our
Medicaid approvals
up much, but our
applications are definitely
up. And that’s a definite
win for the system .”
—Karen McCall
Contact Senior Managing Editor Corey Goodman
Telephone 781/���-187�, ext. �7�7
E-mail [email protected]
Questions? Comments? Ideas?
> continued on p. 12
Patient Access AdvisorPage 1�
© 2007 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
August �007
unChCs initiative < continued from p. 11
receivable. Now, prompt payments are the order of
the day.
“Our charity care program is only available when all
other options are exhausted. We had to clarify that,”
McCall says. “Things weren’t consistent in our system.
So much of this process was just being diligent to get
consistency throughout the system.”
➤ Ensure access to financial counselors. In 2006,
UNCHCS expanded eligibility requirements for its charity
care program. However, at the time, it didn’t bulk up its
staff to accommodate the additional business.
“Without sufficient staff, we really weren’t able to
keep our promise,” says McCall. So UNCHCS added five
financial counselors to the staff. The organization also
uses roving financial counselors, who bounce around
from clinic to clinic, going wherever there is a need.
Clerical staff members order a roving financial coun
selor through a program on UNCHCS’ Web site.
➤ Ensure that billing is accurate and easy to
read. This is probably the biggest challenge for UNCHCS.
“I think we’ll keep working on this the rest of our
lives,” McCall says. “Hospital and physician billing is so
complex that this will always be a challenge.”
UNCHCS relies on customer focus groups to shape
new ideas to simplify the bills. “People are still looking
for a MasterCard bill, and it’s just not that easy,” says
McCall. “I think the industry as a whole still has a long
way to go.”
➤ Ensure that patients understand their obliga-
tion to pay. One ongoing challenge is the fact that hos
pitalbased clinics have an opportunity to charge a facility
fee in addition to the physician charge.
This is because Medicare and Medicaid recognize that
large institutions have additional costs, because they
provide a level of testing to which a normal physician
office doesn’t have access. However, educating patients
as to why they’re receiving two bills isn’t easy. “We’ve
really given a great deal of effort to make sure the patient
doesn’t find this out as a surprise,” McCall says. “We send
letters to them ahead of time, and we include a notice on
the appointment slips to alert them to this.”
The notices also serve as a valuable tool in the cus
tomerfriendly collections efforts. “Patients are more than
willing to pay; they just don’t want to deal with our bill
ing system,” says McCall.
➤ Assist patients with payment plans. UNCHCS
has enlisted the assistance of its collection agencies to
offer nointerest loans.
“It just makes more sense to do what it takes to get
our principle paid back,” says McCall. “Before, we could
only allow patients to pay us over 36 months. Now, if
they need longer, we can make arrangements.” n
editorial Advisory Board Patient Access Advisor
Group Publisher: Lauren McLeod
Executive Editor: Lori Levans
Senior Managing Editor: Corey Goodman, [email protected],
781/6391872, Ext. 3737
Rose t. Dunn, RhIA, CPA, FAChe, FhFMA Chief operating officer, First Class Solutions, Inc., St. Louis, MO
Donna K. GilleyDirector of revenue cycle and regulatory compliance, LBMC Healthcare Group, Brentwood, TN
Amy harttVice president, VHA Southwest, Plano, TX
Diane Jepsky Healthcare consultant, Seattle, WA
steven OrvisSenior consultant, Sinaiko Healthcare Consulting, Los Angeles, CA
Joyce sourbeck, Ms, RnAssistant vice president for patient financial services, Washington Hospital Center, Washington, DC
David s. szabo Nutter, McClennen & Fish, LLP, Boston, MA
sandra J. Wolfskill, FhFMA President, Wolfskill & Associates, Inc., Chardon, OH
Joe Zebrowitz, MDExecutive vice president/senior medical director, Executive Health Resources, Newtown Square, PA
Patient Access Advisor (ISSN 1933-3307) is published monthly by HCPro, Inc., 200 Hoods Lane, Marblehead, MA 01945. Subscription rate: $399/year; back issues are available at $25 each. • Postmaster: Send address changes to Patient Access Advisor, P.O. Box 1168, Marblehead, MA 01945. • Copyright 2007 HCPro, Inc. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro, Inc., or the Copyright Clearance Center at 978/750-8400. Please notify us immediately if you have received an unauthorized copy. • For editorial comments or questions, call 781/639-1872 or fax 781/639-2982. For new subscriptions, renewals, change of address, back issues. billing questions, or permission to reproduce any part of PAA, call customer service at 800/650-6787, fax 800/639-8511, or e-mail: [email protected]. • Visit our Web site at www.hcpro.com. • Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to be included on this mailing list, please write to the Marketing Department at the address above. • Opinions expressed are not necessarily those of PAA. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions.
Patient Access Advisor is one of the resources from the Patient Access Resource Center from HCPro, Inc. For information, call 800/650-6787 or go to www.accessresourcecenter.com.
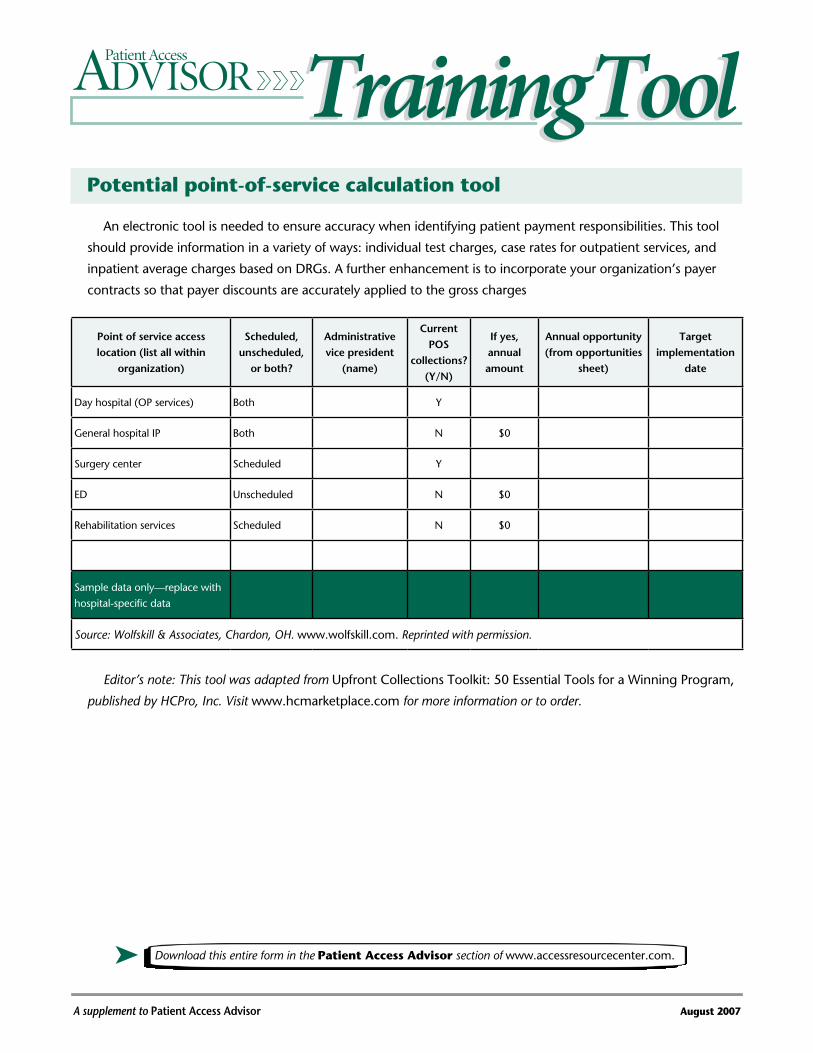
Potential point-of-service calculation tool
A supplement to Patient Access Advisor August 2007
Training ToolTraining ToolAn electronic tool is needed to ensure accuracy when identifying patient payment responsibilities. This tool
should provide information in a variety of ways: individual test charges, case rates for outpatient services, and
inpatient average charges based on DRGs. A further enhancement is to incorporate your organization’s payer
contracts so that payer discounts are accurately applied to the gross charges
Point of service access location (list all within
organization)
Scheduled, unscheduled,
or both?
Administrative vice president
(name)
Current POS
collections? (Y/N)
If yes, annual amount
Annual opportunity (from opportunities
sheet)
Target implementation
date
Day hospital (OP services) Both Y
General hospital IP Both N $0
Surgery center Scheduled Y
ED Unscheduled N $0
Rehabilitation services Scheduled N $0
Sample data only—replace with
hospital-specific data
Source: Wolfskill & Associates, Chardon, OH. www.wolfskill.com. Reprinted with permission.
Editor’s note: This tool was adapted from Upfront Collections Toolkit: 50 Essential Tools for a Winning Program,
published by HCPro, Inc. Visit www.hcmarketplace.com for more information or to order.
➤ Download this entire form in the Patient Access Advisor section of www.accessresourcecenter.com.