-
PRACTICAL THERAPEUTICS
Viral Encephalitis Diagnosis and Treatment
Richard J. Whitley
eNS Drugs 2 (5). 355-366. 1994
1172-7047/94/0011-0355/S0600/0
~.~.-~~-~~.~.~
© Adis International limited All rights reserved
Department of Pediatrics, University of Alabama at Birmingham,
Birmingham, Alabama, USA
Contents Summary 1. Pathogenesis 2. Epidemiology ... 3. Clinical
Manifestations and Diagnosis . 4. Representative Diseases and
Therapy.
4.1 Herpes Viruses . . .. ..... . 4.2 Other Viruses .... . ....
.
5. General Treatment Guidelines for Viral Encephalitis. 5.1.
Supportive Care
355 355 356 356 358 358 362 363 364 364 6. Conclusion .
Summary Viral infections of the eNS are typically associated
with mortality and mor-bidity. These infections are caused by a
variety of both DNA and RNA viruses, and occur in individuals of
all ages. Worldwide, disease burden is most frequently attributed
to herpes simplex virus, varicella zoster virus, cytomegalovirus,
Jap-anese encephalitis and measles infection of the eNS. The
epidemiology and pathogenesis of these infections varies according
to the organism and the locale of occurrence.
Importantly, therapy has only been identified for herpes simplex
encephalitis, varicella zoster virus and cytomegalovirus infections
of the eNS. The utilization of aciclovir l,lnd ganciclovir will
improve the morbidity and mortality for these diseases. For the
other eNS viral infections for which no therapy is presently
available, supportive care is essential.
Viral infections of the eNS have attracted the attention of
historians and physicians for millen-nia,lI,2] With the exception
of herpes simplex en-cephalitis (HSE)pA] identification of the
organ-isms that causes viral eNS syndromes has been difficult, if
not impossible. With the advent of anti-viral therapy, increased
attention has focused on prompt and specific diagnosis, and
implementation of treatment. This review focuses on the
pathogen-
esis of and general diagnostic approach to patients with
presumed eNS viral infections. The appropri-ate therapy of those
infections that are treatable is discussed.
1. Pathogenesis
Encephalitis is generally an unusual complica-tion of a common
viral infection,lS-71 Thus, of the
-
356
large number of individuals with systemic viral in-fection, very
few develop clinical CNS complica-tions. Most viral infections
cause either meningeal involvement, namely aseptic meningitis, or a
mild clinical syndrome of meningoencephalitis rather than
encephalitis.
In general, viral encephalitis can be subdivided into
distinctive categories on the basis of aetiology and pathogenesis.
There are 4 broad categories: (i) acute encephalitis; (ii)
post-infectious encepha-litis; (iii) slow viral infections of the
CNS; and (iv) chronic degenerative diseases of the CNS of presumed
viral aetiology. This review only dis-cusses acute viral
encephalitis.
In acute viral encephalitis, capillary and endo-thelial
inflammation of cortical vessels is a striking pathological
finding. It is accompanied by peri-vascular lymphocytic
infiltration and neuronopha-gia early in the disease and
astrocytosis and gliosis during later stages. Unique
histopathological fea-tures include Cowdry type A intranuclear
inclu-sions and Negri bodies associated with herpes vi-ruses and
rabies infections, respectively.
Access of viruses to the CNS generally occurs by one of 2
routes, either haematogenous or neuro-nal (reviewed in detail
elsewhere[2,5,6,8- 141) Haem-atogenous spread is most common and
can result in an altered blood-brain barrier,[1l,12,15, 161 as
ex-emplified by arthropod-borne viral disease)9, I 0, 16]
Alternatively, viruses can access the nervous sys-tem by
intraneuronal routes as occurs with herpes simplex virus (HSV)
accession from peripheral sites) 17, 18] It is not known whether
HSV can exist in a latent state within the CNS. Another example of
intraneuronal transmission of a virus to the CNS is rabies, with
ultimate involvement of the limbic system) 19]
Once a virus has reached the brain, subsequent replication can
remain intraneuronal or result in either cell-to-cell or
extracellular transmission.
2. Epidemiology
Many human viral pathogens cause CNS infec-tions,l21 The Centers
for Disease Control suggest that approximately 20 000 cases of
encephalitis oc-
© Adis International Limited. All rights reserved.
Whitley
cur in the US each year, most being mild. 120,211 The 2 endemic
causes of encephalitis in the US are HSV and rabies virus. Rabies
virus causes only encepha-litis and is more common in developing
countries. HSV accounts for approximately lO% of all en-cephalitic
cases in the US,l22,23] Japanese enceph-alitis is probably the most
common epidemic infec-tion outside North America. In China alone,
there are over lO 000 cases annually, despite childhood
immunisation. [9, 1 0]
The development of effective vaccines for con-trol of diseases
such as measles, mumps, rubella and yellow fever has significantly
decreased the inci-dence of both acute encephalitis and
post-infec-tious encephalitis in countries where vaccination is
routine. Vaccination has decreased significantly the incidence of
poliovirus infections of the CNS;[24] however, sporadic cases occur
as a con-sequence of vaccine-associated infection with type 2 or
type 3 virus.] 251
Other members of the picornavirus family clearly have the
potential to infect the brain, these includ-ing Coxsackie and Echo
viruses.[2,26-281 Usually, these latter agents cause a benign
aseptic meningitis.
The arthropod-borne viruses, that cause disor-ders such as St.
Louis encephalitis, Eastern equine encephalitis, Venezuelan equine
encephalitis and La Crosse virus infections, are causes of
spo-radic and epidemic CNS viral infection in the US. [12,29-311
Early identification and recognition of the specific infection may
lead to interventive strategies to prevent burgeoning mosquito
popula-tions that serve as vectors for transmission of in-fection.
[32]
3. Clinical Manifestations and Diagnosis
The hallmark of viral encephalitis is the acute onset of a
febrile illness. The clinical findings as-sociated with viral
encephalitis are shown in table I. These findings distinguish a
patient with enceph-alitis from one with viral meningitis, who
usually has only headache, nuchal rigidity and fever.
Clinical findings reflect disease progression and the cells of
the CNS that are infected. The tropism of select viruses for
different cell types illustrates
eNS Drugs 2 (5) 1994
-
Treatment of Viral Encephalitis
Table I. Clinical features associated with viral
encephalitis
Headache
Fever
Altered consciousness
Disorientation
Behavioural disturbances
Speech disturbances
Neurological signs (sometimes focal but generally diffuse) e.g.
hemiparesis and/or seizures
this point)2,5-7] For example, poliovirus preferen-tially
infects motor neurons, rabies selects neurons ofthe limbic system
and mumps can infect ependy-mal cells of neonates. Infection of
cortical neurons can lead to abnormal electrical discharges,
result-ing in seizures or focal neurological deficits.
De-myelination may follow destruction of oligo-dendroglia cells,
while involvement of ependymal cells can result in hydranencephaly.
The predispo-sition ofHSV for the temporal lobe leads to clinical
findings of aphasia, anosmia, temporal lobe sei-zures and focal
neurological findings)22]
The diagnosis of viral infections of the CNS is difficult at
best. Patient and general history may reveal a characteristic
epidemiology, such as a his-tory of an animal bite, season of year
and prevalent community diseases. The Morbidity and Mortality
Weekly Report identifies prevalent diseases and responsible
pathogens in the US and, therefore, may be valuable in the
identification of aetiologi-cal agents locally responsible for
encephalitic syn-dromes.
Physical examination usually does not lead to an aetiological
diagnosis. However, a few considera-tions are essential when
performing such an exam-ination. In patients with acute viral
encephalitis, the distinction between generalised and focal
neuro-logical findings is important. The most common cause of focal
encephalopathic findings is HSV.£33,34] However, when signs and
symptoms of patients with biopsy-proven HSE are compared with those
who did not have HSV infection, there are no dis-tinguishing
characteristics for patients ultimately proven to have HSE.£33]
Viruses that are usually responsible for diffuse encephalitic
diseases can,
© Adis International Limited. All rights reserved.
357
on occasion, localise to one area of the brain and, therefore,
mimic HSE (table 11))34,35] Apprecia-tion of these data is
essential for the development of diagnostic and therapeutic
approaches in such patients.
Evaluation of the cerebrospinal fluid (CSF) is essential, unless
its collection is contraindicated because of marked increased
intracranial pressure. Careful assessment of the CSF formula is
helpful. Findings indicative of encephalitis generally in-clude
pleocytosis, predominately mononuclear cells and elevated protein
levels (glucose levels are usually normal). Nevertheless, a small
percentage of patients (approximately 3 to 5%) with severe viral
infections of the CNS, such as HSE, have completely normal CSF)33]
Unfortunately, cul-tures ofCSF are of little value for isolation of
HSV, except under unusual circumstances (see section 4.1.1).[35]
However, cultures may be positive early after the onset of some
viral meningitis.
Neurodiagnostic tests, including the electro-encephalogram
(EEG), and computed tomographic (CT) technetium brain and magnetic
resonance im-aging (MRI) scans, can provide useful information for
the evaluation of patients with altered menta-tion and fever.
Laboratory confirmation of disease aetiology is of therapeutic
value for only a few pathogens, but is always of prognostic value.
For most diseases, antibodies identified in the CSF are not useful
diagnostically unless evaluated sequentially, in or-der to
demonstrate increasing quantities. Routine evaluation of acute and
convalescence sera (to as-sess seroconversion or seroboosting) is
of no prac-tical value in the decision to institute therapy for
viral CNS infections. Such studies may be helpful, retrospectively,
to clarify the aetiology of infec-tion, as has been done for
HSE.£35-37]
The development of new diagnostic assays that utilise CSF can
accelerate the diagnosis of viral infections of the brain. Japanese
encephalitis and HSE can be detected using these systems. An
enzyme-linked immuno-sorbent assay (ELISA) that detects
immunoglobulin M (IgM) antibodies in the CSF from patients with
presumed Japanese encephalitis
eNS Drugs 2 (5) 1994
-
358
Table II. Diseases found in 432 patients that mimic herpes
simplex encephalitis (reproduced from Whitley et al.,[34] with
permission)
Disease
Treatable diseases 1. Infection
Abscess or subdural empyema
bacterial
listerial
fungal
mycoplasmal
Tuberculosis
Cryptococcal
Rickettsial
Toxoplasmosis
. Mucormycosis
Meningococcal meningitis
2. Tumour
3. Subdural haematoma
4. Systemic lupus erythematosus
5. Adrenoleukodystrophy
Untreatable diseases 1. Nonviral
Vascular disease
Toxic encephalopathy
Reye's syndrome
2. Viral
Togavirus infection
St Louis encephalitis
Western equine encephalomyelitis
California encephalitis
Eastern equine encephalomyelitis
Other herpesvirus infections
Number of patients
38
5
1
2
2
6
3
2
1
1
5 2
1
6
57
11
5
1
7
3
4
2
Epstein-Barr virus 8
cytomegalovirus
Other
echovirus infection 3
influenza A 4
mumps 3
adenovirus infection 1
progressive multifocal leukoencephalopathy
lymphocytic choriomeningitis
subacute sclerosing panencephalitis 2
is sensitive and specific.£38] Most patients have IgM antibodies
at the time of hospitalisation and virtually all acquire them by
day 3 of illnessJ38,39] The polymerase chain reaction (PCR) has
been de-veloped to detect viral DNA in the CSF of patients with
HSE.£40-42] This assay is over 90% sensitive
© Adis International Limited. All rights reserved.
Whitley
and 90% specific within 3 days of the onset of ill-ness.
Nevertheless, if properly performed, brain bi-opsy remains the
most sensitive and specific means for diagnosis of HSE and diseases
that mimic HSE.£33-35] Brain tissue is submitted for culture,
histopathological and electron microscopic evalu-ations. Currently,
brain biopsy is generally re-served for patients who deteriorate on
aciclovir therapy and have an unknown abnormality on CT or MRI
evaluation.
4. Representative Diseases and Therapy
4.1 Herpes Viruses
4. 1. 1 Herpes Simplex
Incidence and Diagnosis HSE is the most common cause of
nonepidemic,
sporadic, acute focal encephalitis in the US. The estimated
incidence is 1 in 250 000 to 1 in 500 000 individuals per
year.£22,43] Occurring throughout the year, approximately one-third
of the cases of HSE develop in patients less than 20 years of age
and one-half in individuals over the age of 50 years)22] The
disease does not occur more com-monly in immunosuppressed
patients,[44] but may be increasing in individuals with HIV
infection.£45]
In the absence of antiviral therapy, the mortality for HSE is in
excess of 70%. Furthermore, only approximately 2.5% of untreated
individuals re-turn to normal functioning)46,47]
A distinction must be made between HSV infec-tions of the CNS
that occur during the neonatal and other periods. HSE in neonates
is caused either by HSV type 1 or type 2, while infection in older
chil-dren and adults is overwhelmingly the conse-quence of HSV type
1.£48,49] During the neonatal period, HSV type 2 infection of the
brain in patients with multi-organ disseminated neonatal HSV
in-fection is likely to be blood-borne. It is associated with a
diffuse encephalitic process, resulting in generalised
encephalomalacia)50] In contrast, when the disease only involves
the CNS of neonates, neuronal transmission of the virus to the CNS
tends to result in unitemporal and, then, bitemporal
eNS Drugs 2 (5) 1994
-
Treatment of Viral Encephalitis
disease as illness progresses. This latter pattern of evolution
is also encountered in older children and adults. Interestingly,
HSV type 2 (which is the most common cause of genital herpes and,
not in-frequently, viral meningitis) rarely results in
en-cephalitis in adults. The reasons for the differences in the
pathogenesis of HSV type I and type 2 are unknown.
HSV can be retrieved from the CSF of babies with encephalitis or
disseminated disease in ap-proximately 15 and 40% of patients,
respectively. [50] Thus, CSF viral cultures are indicated in
neonates. This is in contrast to older individuals in whom
isolation of the virus from this site is uncommon. In older
patients, it becomes necessary to obtain a brain biopsy or utilise
CSF for the detection of HSVby PCR.
Treatment Studies A series of trials has evaluated therapy of
HSE
in older children and adultsP2,46,47,51-53]
The first clinical trials to indicate therapeutic success used
vidarabine 15 mg/kg/day. Mortality was decreased from 70% in
placebo recipients to 28% in drug-treated patients 1 month after
institu-tion of therapy and to 44% 6 months later for pa-tients
with biopsy proven disease.l46]
However, the National Institute of Allergy and Infectious
Diseases Collaborative Antiviral Study Group and investigators in
Sweden found aciclovir to be superior to vidarabine.[52,53]
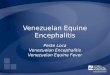
Mortality was reduced to 28% in the aciclovir-treated patients 18
months after the onset of treatment compared with 50% in vidarabine
recipients, as shown in figure l.l52] Three factors influenced
outcome with aciclovir therapy. First, a low level of
conscious-ness, as measured by a Glasgow coma score of 6 or less,
was associated with a poor therapeutic out-come. This was
irrespective of the age of the pa-tient (or the agent
administered). Secondly, if dis-ease was present for 4 days or less
before initiation of therapy, the likelihood of survival increased
from 72 to 92% during the 18 months following treatment. Finally,
patients less than 30 years of age had a more favourable outcome
than older in-dividuals.
© Adis International Limited. All rights reserved.
359
100
~ 80 ACV (n =32)
'" c: :~ 60 2: :::l !J)
i1 ARA·A n=37 CI> '@ 40 c. '0 0 z 20
o 3 6 9 12 15 18 Time (months)
Fig. 1. Comparison of survival in patients with biopsy-proved
herpes simplex encephalitis treated with vidarabine (ARA-A) or
aciclovir (ACV) [reproduced from Whitley et al.,[52] with
per-mission].
Two years after treatment, 30% of aciclovir re-cipients were
judged to be normal or to have mild impairment, 17% had moderate
neurological se-quelae (such as speech impediment and gait
distur-bance) and 53% were dead or had severe impairment. This
outcome was better than that of vidarabine re-cipients, of whom
only 15 to 20% were found to be neu-rologically normal on long-term
follow-up.l22,52-54] Obviously, these data indicate the need for
further improvement in therapy of HSV infections of the brain.
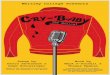
When vidarabine and aciclovir were compared directly in neonates
with HSV infection, no differ-ence in morbidity or mortality was
detected be-tween the 2 drugs (see fig. 2 and table III).l55,56]
Neonates with HSV infections can be classified as having disease
that is localised to the skin, eyes and mouth, affecting the CNS,
or that is disseminated.
In a comparative study, aciclovir was as effec-tive as (but not
superior to) vidarabine treatment in neonates with HSV infections
(fig. 2)[55] Overall, no baby with disease localised to the skin,
eyes or mouth died, while 18% of babies with CNS infec-tion and 55%
of those with disseminated infection died. Among babies with HSV
infections of the
eNS Drugs 2 (5) 1994
-
360 Whitley
Table III. Assessment of morbidity after 12 months in infants
with neonatal herpes simplex virus infection treated with
vidarabine or aciciovir (reproduced from Whitley et al.,155] with
permission)
Extent of disease Morbidity after 12 months (number of infants)
AI ive after 12 Dead within Total normal mild moderate severe
Skin, eye or mouth infection
Vidarabine 22 1 1 Aciclovir 45 0 0
eNS infection Vidarabine 13 1 5 11 Aciclovir 8 5 6 9
Disseminated disease Vidarabine 7 0 4 Aciclovir 3 0
Total 98 9 13 26
skin, eyes and mouth, 90% of those treated with vidarabine and
98% of those treated with aciclovir were developing normally 2
years after infection. The comparable values were 50% and 43%,
respec-tively, among babies surviving CNS infection (en-cephalitis)
and 62% and 57%, respectively, among babies surviving disseminated
infection.
Thus, unlike the results of therapy in older patients with HSE,
there were no significant differences in either morbidity or
mortality among infants treated with aciclovir and vidarabine.
Clearance of the virus was slower in babies who received aciclovir
than in immunocompromised adults, implying a require-ment for host
defense for recovery. To improve out-come, therapy must prevent
progression of infection to the CNS or disseminated disease.
Factors that influence outcome of CNS disease in neonates
include prematurity, level of conscious-ness at initiation of
therapy, HSV-I for mortality, and seizures and HSV-2 infection for
morbidity. As an example, differences in outcome are dependent on
the HSV type. Babies with HSV type 1 CNS infection have been
noted[46,47J to have a signifi-cantly better neurological outcome
than those with HSV type 2 infection of the brain,l52]
Therapeutic Recommendations Because of the ease of
administration and rela-
tive absence of toxicity, aciclovir is recommended by most
authorities as the medication of choice for
© Adis International Limited. All rights reserved.
subtotal months (morbidity 12 months unknown)
25 6 0 31 46 8 0 54
30 1 5 36 28 2 5 35
12 2 14 28 5 2 11 18
146 21 35 202
treatment of neonatal, child and adult HSV infec-tionJ48] It
should be administered intravenously at a dosage of 10 mg/kg 3
times daily for a period of 10 to 14 days. Longer periods of
administration and higher dosages of medication are being
investi-gated. There is no established therapeutic value to the
concomitant administration of steroids.
Relapse of HSV infection of the brain following either aciclovir
or vidarabine therapy has been doc-umented. From studies of
neonatal HSE, approxi-mately 8% of children who received aciclovir
had a documented virological relapse if treated for 10 days at a
dosage of 10 mg/kg every 8 hours. [55] The exact percentage of
adults with biopsy proven HSE who experience relapse is unknown.
However, re-ports have suggested that relapse can occur[57,58]
following therapy with either vidarabine or aciclovir, and may be
as high as 5%.[59,601
At this time, HSV isolates have not been routinely obtained from
patients with neurological deteriora-tion. In a few cases when HSV
isolates were obtained and tested for resistance to aciclovir, they
remained sensitive. Retreatment at a higher dosage of aciclovir (15
mg/kg every 8 hours) or in combination with vidarabine 15 mg/kg/day
has been utilised in a few patients and for a longer course (21
days).
4.1.2 Other Herpes Viruses Other herpes viruses can cause acute
encepha-
litic syndromes, including varicella zoster virus
eNS Drugs 2 (5) 1994
-
Treatment of Viral Encephalitis
(VZV), cytomegalovirus (CMV) and Epstein-Barr virus.l34] The
occurrence offocal encephalopathic disease caused by Epstein-Barr
virus is of particu-lar interest; recovery was complete without
treat-ment. The role of human herpesvirus-6 (HHV-6) as a cause of
encephalitis in under investigation. This entity is difficult to
diagnose and does not rou-tinely warrant therapy.
Varicella Zoster Virus VZV can result in CNS disease,
causing
symptoms including cerebellar ataxia, meningo-encephalitis,
transverse myelitis and aseptic meningitis. During chickenpox in
otherwise healthy individuals, cerebellar ataxia is a com-mon
clinical finding and is usually benign. In the US, between 200 and
400 child deaths yearly are attributed to chickenpox, many of which
in-volved the CNS. In older individuals, herpes zoster encephalitis
and granulomatous arteritis can occur.l7,61] This latter condition
has been re-ported following zoster ophthalmicus. Other CNS
syndromes associated with VZV infection include myelitis,
encephalitis, polyradiculitis, and cranial and peripheral nervous
palsies.
The diagnosis of VZV infection of the CNS re-sides, for the most
part, on supportive evidence of cutaneous clinical disease. The
patient with al-tered mentation or evidence of myelitis with either
chickenpox or shingles should be presumed to have VZV infection of
the CNS. Evaluation can include CSF examination, EEG and either CT
or MRI scans. A MRI scan can be useful in establishing the
diag-nosis of transverse myelitis and granulomatosis arteritis.
However, findings with other diagnostic tools may be nonspecific.
Assessment of CSF by PCR may detect VZV-DNA.
The treatment of VZV infections of the CNS with both aciclovir
and vidarabine has been evalu-ated in limited numbers of
patients.l62] The treat-ment of choice is aciclovir administered
intrave-nously at a dosage of 500 mg/m2 given every 8 hours for 7
to lO days.
Cercopithecine Herpes Virus 1 (8 Virus) B virus has caused
several cases of severe and
fatal encephalitis,[63] with fewer than 40 cases re-
© Adis International Limited. All rights reserved.
1.0
0.9
Cl 0.8 c .:;; .~
:::J 0.7
UJ
~ 0.6 Ql
~ 0.5 c.
15 0.4 c 0 t 0.3 0 c. e 0.2 0..
0.1
0 0
I!!I Skin, eye or mouth infection, vidarabine (n = 31) or
aciclovir (n = 54)
+ CNS infection, vidarabine (n = 36) • CNS infection, aciclovir
(n = 35) • Disseminated infection, vidarabine (n = 28) o
Disseminated infection, aciclovir (n = 18)
361
60 120 180 240 300 360
Survival (days)
Fig. 2. Survival of babies with neonatal herpes simplex viral
infection, according to treatment and extent of disease
(repro-duced from Whitley et al.,[55J with permission).
ported in the literature. This virus is transmitted by monkey
bite, and is a preventable disease if proper animal handling
precautions are employed.l63] In-fection can be confirmed by virus
isolation, a pro-cedure not routinely performed, or
seroconversion.
Aciclovir or ganciclovir may be of value in the therapy of CNS
disease; however, therapeutic ex-perience in this condition is
limited. Nevertheless, early therapy has resulted in survival in
the ab-sence of neurological impairment.[64] Because of the near
fatal outcome of CNS disease, therapy with aciclovir should be
initiated at dosages used for the treatment of HSE (see section
4.1.1). If disease progression occurs, treatment should be changed
to ganciclovir at 5 mg/kg administered intravenously every 12 hours
for at least 14 days. Because of the life-threatening potential
ofinfec-tion, some authorities recommend long term sup-pressive
aciclovir therapy (at a dosage of 250 mg/m2
3 times daily) for survivors of disease.
eNS Drugs 2 (5) 1994
-
362
Cytomegalovirus CMV infection of the CNS is most commonly
associated with congenital CMV infection, occur-ring with a
prevalence of approximated 1 % in de-veloped countries. However,
CMV also occurs in patients with HIV infection, and so CMV
neuro-logical disease is being reported more frequently in this
patient population.
One of 10 children with congenital CMV infec-tion will have
evidence of clinical symptoms, in-cluding microcephaly (50%),
psychomotor impair-ment (70%) and hearing loss (60%). Intracranial
calcification is also common. Disease is confirmed by isolation of
CMV from the urine within the first 2 weeks of life.
In the immunocompromised host, clinical find-ings are less
specific than in children. Meningitis, encephalitis and
polyradiculitis are all attributed to CMV infection of the CNS. The
appearance ofCSF proteinosis and leucocytosis in the absence of
bac-terial, parasitic or fungal evidence of disease and clinical
evidence of polyradiculitis is highly sug-gestive of CMV infection.
Disease can be con-firmed by PCR evaluation of CSF for CMV-DNA.
Ganciclovir therapy should be reserved for HIV-infected patients
instituted promptly at a dosage of 5 mg/kg every 12 hours for 21
days.
4.2 Other Viruses
4.2. 1 Rabies Rabies is of increasing concern worldwide, es-
pecially in the US in view of recent cases in New YorkV1 In the
Southeastern US, foxes and bats are most often infected with rabies
virus, while in Cali-fornia skunks are most often infected. In
South and Central America, dogs and cattle are the primary carrier
of rabies virus.l651 Infection is transmitted by the bite of a
rabid animal. The incubation period is quite variable, ranging from
days to months. While not all individuals bitten by a rabid animal
develop infection, if infection does occur, it is in-variably
fatal.[66,671
The best medical management is the prevention of infection by
utilisation of post-exposure vaccine and immune serum, particularly
in individuals bit-
© Adls International limited. All rights reserved.
Whitley
ten by an unprovoked animal.l68-701 The vaccine should also be
administered to animal handlers at risk. Post-exposure immunisation
is an essential feature of the imunoprophylaxis of rabies even for
individuals who have received pre-exposure rabies immunisation.
Most rabies exposures occur be-cause of unanticipated animal
contact (bite, scratch or mucosal contamination). In an
nonimmunised indi vidual, both rabies immune globulin (of human
origin) and rabies vaccine should be administered as appropriate
for the circumstances of exposure. Local care should include
aggressive cleaning of the wound. Active immunisation consists of
the hu-man diploid cell vaccine (HDCV) or rhesus diploid cell
vaccine (rabies vaccine absorbed) as a 1ml in-jection given
intramuscularly in the deltoid area on the first day of treatment,
with administration re-peated on days 3, 7, 14 and 28.
Recent vaccine advances, utilising rabies virus glycoproteins
produced by vaccine vectors, may be a better prophylactic
approach.[71-751 Vaccination of wild animals, to decrease
transmission in the animal community, has been considered. [76-781
No therapy for rabies exists at this time.
4.2.2 Arthropod-Borne Viruses Arthropod-borne viruses can be a
common cause
of sporadic and epidemic encephalitisV,79,801 These viruses
replicate in both vertebrate and nonverte-brate species, and
include members of the a-, flavi-and bunyavirus families. These
agents are transmit-ted by mosquitoes and ticks. Among the
a-viruses are those that cause Eastern, Western and Venezu-elan
equine encephalitis. The flaviviruses cause ei-ther mosquito- or
tick-borne encephalitis. Exam-ples of the former include Japanese,
St. Louis, Rocio, Murray Valley and West Nile encephalitis.
Examples of tick-borne diseases are Kyasuma For-est and Powassan
encephalitis. The bunyavirus family includes the most common causes
of arbo-viral disease in the- US, La Crosse virus, as well as
Jamestown Canyon and California encephalitis vi-ruses.
Japanese encephalitis is a major medical problem in China,
Southeast Asia and India where as many as 20 000 cases per year
have been reported.l9,81,821 The
eNS Drugs 2 (5) 1994
-
Treatment of Viral Encephalitis
major vector for Japanese encephalitis in humans appears to be
the colicine mosquito, which breeds in large numbers in the rice
fields of the Orient. Incubation in the mosquito, known as the
gesta-tional incubation period or the interval of time be-tween
ingestion of infected blood and spread from the mid gut to the
salivary glands, is inoculum-and temperature-dependent)lO] A
predictive fac-tor for outcome is the rapid appearance of
antibod-ies directed against Japanese encephalitis in the CSF.[38]
These antibodies apparently ameliorate disease severity)39]
Vaccination against Japanese encephalitis is effective.
No treatment exists for arboviral infections other than
supportive care.
4.2.3 Enteroviruses The infrequent but devastating occurrence
of
poliomyelitis caused by the type 2 or 3 strain polio-virus
following vaccination is of increasing con-cern)24,25,83-85] This
has led to numerous attempts to alter the vaccine)86,87]
Alternative vaccines, in-cluding an enhanced inactivated vaccine
and a genetically engineered vaccine, have been tested and debated
as potential solutions)87]
Perinatal acquisition of echoviruses and cox-sackieviruses can
lead to significant morbidity and mortality)88,89] In patients with
agammaglobulin-aemia, enteroviral CNS infections can be chronic and
lethal.l90]
Care of patients with enteroviral infection of the CNS is
supportive, as no drugs exist for treatment.
4.2.4 Retroviruses Human T-lymphotropic viruses (HTLV) are
known causes of CNS disease.l91 ,92] HTLV type I has been
associated with spastic pareses in Japan and Hawaii. HIV causes
dementia in nearly all pa-tients by the time of death)93-100] It is
likely that HIV encephalopathy will become the most com-mon cause
of CNS viral infection worldwide. Oral therapy with zidovudine
100mg 5 times a day may benefit CNS disease as it does other
systemic man-ifestations of HIV infection)lOl-103] This virus, as
well as other retroviral causes of CNS diseases, has been reviewed
extensively in other publica-tions )93-100,104-107]
© Adis International Limited. All rights reserved.
363
4.2.5 Miscellaneous Viruses Other viruses can also result in CNS
disease,
and these will only be briefly mentioned. Two paramyxoviruses,
mumps and measles, commonly caused CNS disease in the prevaccine
era. Vacci-nation in the US has nearly eliminated this prob-lem.
The arenaviruses, lymphocytic choriomenin-gitis and Lassa viruses,
are rare causes of CNS disease. Ribavirin, an antiviral licensed
for therapy of respiratory syncytial virus infection of infants,
has been reported to be efficacious in the treatment of Lassa
fever, using a dosage regimen of a 2g load-ing dose followed by 19
4 times a day for 4 days and then O.5g 3 times a day for 6
days)108]
5. General Treatment Guidelines for Viral Encephalitis
Of all the viral encephalitis currently identified, only those
caused by HSV, VZV and CMV are amenable to treatment. The
utilisation of aciclovir and ganciclovir in patients with these
infections is described in section 4.1.
The administration of aciclovir must be as a 1 hour infusion in
order to avoid potential local (thrombophlebitis) as well as renal
(tubular crystal deposition) complications. Adequate hydration must
be maintained and balanced against increased intracranial pressure
associated with cerebral oe-dema. Evidence of bone marrow
suppression, and bone marrow, hepatic and other organ dysfunction
is not usually encountered with the administration of aciclovir.
However, renal function must be moni-tored carefully, particularly
in patients for whom excessive fluid requirements may not be well
tol-erated.
Administration of ganciclovir of the treatment of CMV infection
is associated with significant bone marrow suppression. Medication
can usually be administered for a period of 10 to 14 days, with the
appearance of neutropenia and thrombocyto-penia in approximately 10
to 15% of patients. Thus, careful monitoring of blood cell
parameters should be employed in patients who receive this
therapy.
eNS Drugs 2 (5) 1994
-
364
5.1 Supportive Care
Individuals with infections of the eNS require meticulous
medical management. Since a common complication of infections of
the eNS is increased intracranial pressure, it is common for
patients to re-quire ventilatory support. Therefore, careful
atten-tion to pulmonary hygiene, adequate ventilation and judicious
use of antimicrobial agents to treat sec-ondary infections are all
indicate. Additionally, atten-tion to adequate nutritional status
is also required.
6. Conclusion
This review has focused on the pathogenesis, diagnosis and
treatment of common eNS viral en-cephalitides, with a particular
focus on those caused by herpes viruses. With the recognition that
at least one eNS viral disease is treatable, namely HSE, it is
likely that newer specific diagnostic tests and therapies for other
viral eNS infections will be de-veloped. However, it should be
noted that at pres-ent most viral encephalitides are not directly
treat-able with an antiviral drugs, and, therefore, care is
supportive.
Acknowledgements
Studies performed by the author and herein reported were
initiated and supported under a contract (NOI-AI-62554) with the
Development and Applications Branch of the Na-tional Institute of
Allergy and Infectious Diseases (NIAID), a Program Project Grant
(PO I AI 24009), by grants from the General Clinical Research
Center Program (RR-032) and the State of Alabama.
References I. Hughes SS. The virus. A history of the concept.
New York:
Science History Publications, 1977 2. Johnson RT, editor. Viral
infections of the nervous system. New
York: Raven Press, 1982 3. Smith MG, Lennette EH, Reames HR.
Isolation of the virus of
herpes simplex and the demonstration of intranuclear inclu-sions
in a case of acute encephalitis. Am J Pathol 1941; 17: 55-68
4. Zarafonetis CJD, Smodel MC, Adams JW, et a!. Fatal herpes
sim-plex encephalitis in man. Am J Patho11944; 20 (3): 429-45
5. Johnson RT, Mims CA. Pathogenesis of viral infections of the
nervous system. N Engl J Med 1968; 278: 23-92
6. Mims CA. The pathogenesis of infectious disease. London:
Academic Press, 1977
7. Griffin DE. Viral infections of the central nervous system.
In: Galasso GJ, Whitley RJ, Merigan TC, editors. Antiviral
agents
© Adis International Limited. All rights reseNed.
Whitley
and viral diseases of man. New York: Raven Press, 1990:
461-95
8. Weiner LP, Fleming JO. Viral infections of the nervous
system. J Neurosurg 1984; 61: 207-24
9. Johnson RT. The pathogenesis of acute viral encephalitis and
postinfectious encephalitis. J Infect Dis 1987; 155: 359-64
10. Rosen L. The natural history of Japanese encephalitis virus.
Annu Rev Microbiol 1986; 40: 395-414
II. Friedman HM, Macarak EJ, MacGregor RR, et a!. Virus
infec-tion of endothelial cells. J Infect Dis 1981; 143: 266-73
12. Johnson RT. Virus invasion of the central nervous system. A
study of Sindbis virus infection in the mouse using fluorescent
antibody. Am J Patho11965; 46: 929-43
13. Schlitt M, Chronister RB, Whitley RJ. Pathogenesis and
patho-physiology of viral infections of the central nervous system.
In: Scheid WM, Whitley RJ, Durack DT. editors. Infections of the
central nervous system. New York: Raven Press. 1991: 7-18
14. Whitley RJ. Viral encephalitis. N EnglJ Med 1990; 323:
242-50 15. Johnson KP, Johnson RT. California encephalitis. II.
Studies of
experimental infection in the mouse. J Neuropathol Exp Neu-rol
1968; 27: 390-400
16. Albrecht P. Pathogenesis of neutropic arbovirus infections.
Curr Top Microbiol Immunol 1968; 43: 44-91
17. Cook ML. Stevens JG. Pathogenesis of herpetic neuritis and
ganglionitis in mice: evidence of intra-axonal transport of
in-fection. Infect Immun 1973; 7: 272-88
18. JR Baringer. Herpes simplex virus infection of nervous
tissue in animals and man. Prog Med Virol 1975; 20: 1-26
19. Murphy FA. Rabies pathogenesis: a brief review. Arch Virol
1977; 54: 279-97
20. Beghi E. Nicolosi A. Kurland LT. et a!. Encephalitis and
aseptic meningitis. Olmsted. Minnesota. 1950-1981. I.
Epidemiol-ogy. Ann Neurol 1981; 16: 283-94
21. Summary of notifiable diseases in United States. 1987. MMWR
Morb Mortal Wkly Rep 1988; 36: I-59
22. Goldsmith SM. Whitley RJ. Herpes simplex encephalitis. In:
Lambert HP. editor. Infections of the central nervous system.
Philadelphia: B.C. Decker. 1991: 283-99
23. Olson LC. Buescher EL. Artenstein MS. Herpesvirus infections
of the human central nervous system. N Engl J Med 1967; 277:
1271-7
24. Melnick JL. Poliomyelitis vaccines: an appraisal after 25
years. Compr Ther 1980; 5: 6-14
25. Assaad F. Cockburn we. The relation between acute persisting
spinal paralysis and poliomyelitis vaccine - results of a ten-year
enquiry. Bull World Health Organ 1982; 60: 231-42
26. Melnick JL. Enteroviruses: polioviruses. coxsackieviruses.
echoviruses and newer enteroviruses. In: Fields BN. Knipe DM.
editors. Virology. 2nd ed. New York: Raven Press. 1990: 549-607
27. JR Modlin. Poliovirus. In: Mandell GL. Douglas Jr RG.
Bennett JE. editors. Principles and p,ractice of infectious
diseases. 3rd ed. New York: Churchill Livingstone. 1990: 1365-7
28. Modlin JE Coxsackievirus and echovirus. In: Mandell GL.
Douglas Jr RG. Bennett JE. editors. Principles and practice of
infectious diseases. 3rd ed. New York: Churchill Livingstone. 1990:
1367-83
29. Luby JP. St. Louis encephalitis. Epidemiol Rev 1979; I:
55-73 30. Monath TP. Tsai TE St. Louis encephalitis: lessons from
the last
decade. Am J Trop Med Hyg 1987; 37 Supp!. 3: 49S-59S 31. Shope
RE. Epidemiology: mechanisms of cause. distribution
and transmission of viral disease. In: Field BN. Knipe DM.
Chanock RM. et al.. editors. Virology. New York: Raven Press. 1985:
145-51
eNS Drugs 2 (5) 1994
-
Treatment of Viral Encephalitis
32. Eldridge BF. Strategies for surveillance. prevention, and
control of arbovirus diseases in Western North America. Am J Trop
Med Hyg 1987; 37: 77-86
33. Whitley RJ, Tilles J, Linneman Jr C, et al. Herpes simplex
en-cephalitis: clinical assessment. JAMA 1982; 247: 317-20
34. Whitley RJ, Cobbs CG, Alford CA, et al. Diseases that mimic
herpes simplex encephalitis: diagnosis, presentation and out-come.
JAMA 1989; 262: 234-9
35. Nahmias AJ, Whitley RJ, Visintine AN, et al. Herpes simplex
encephalitis: laboratory evaluations and their diagnostic
sig-nificance. J Infect Dis 1982; 145: 829-36
36. Longson M, Bailey AS. Early diagnosis and treatment of virus
infections of the central nervous system. Practitioner 1978;
221:47-56
37. Skoldenberg B, Jeansson S, Wolontis S. Herpes simplex virus
type 2 and acute aseptic meningitis: atypical features of cases
with isolation of herpes simplex virus from cerebrospinal flu-ids.
Scand J Infect Dis 1975; 7: 227-32
38. Burke OS, Nisalak A, Ussery MA, et al. Kinetics of IgM and
IgG responses to Japanese encephalitis virus in human serum and
cerebrospinal fluid. JInfect Dis 1985; 151: 1093-9
39. Burke OS, Loromrudee W, Leake CJ, et al. Fatal outcome in
Japanese encephalitis. Am J Trop Med Hyg 1985; 34: 1203-10
40. Rowley A, Lakeman F, Whitley R, et al. Rapid detection of
herpes simplex virus DNA in cerebrospinal fluid of patients with
herpes simplex encephalitis. Lancet 1990; 335: 440-1
41. Aurelius E, Johansson B, Skoldenberg B, et al. Rapid
diagnosis of herpes simplex encephalitis by nested polymerase chain
reaction assay of cerebrospinal fluid. Lancet 1991; 337: 189-92
42. Schlesinger Y, Tebas P, Gaudreault-Keener M, et al. Herpes
simplex type 2 meningitis in the absence of genital lesions:
improved recognition using the polymerase chain reaction. Ann
Intern Med. In Press
43. Institute of Medicine. New vaccine development establishing
priorities: disease of importance in the United States.
Wash-ington, DC: National Academy Press, 1985: 280-312
44. Whitley RJ, Lakeman AD, Nahmias AJ, et al. DNA
restriction-enzyme analysis of herpes simplex virus isolates
obtained from patients with encephalitis. N Engl J Med 1982; 307:
1060-2
45. Snider WD, Simpson OM, Nielson S. Neurological
complica-tions of the acquired immune deficiency syndrome. Analysis
of 50 patients. Ann Neuro11983; 14: 403-18
46. Whitley RJ, Soong S-J, Dolin R, et al. Adenine arabinoside
therapy of biopsy-proved herpes simplex encephalitis: Na-tional
Institute of Allergy and Infectious Diseases Collabora-tive
Antiviral Study. N Engl J Med 1977; 297: 289-94
47. Whitley RJ, Soong S-J, Hirsch MS, et al. Herpes simplex
en-cephalitis: vidarabine therapy and diagnostic problems. N Engl J
Med 1981; 304: 313-8
48. Whitley RJ, Nahmias AJ, Visintine AN, et al. The natural
his-tory of herpes simplex virus infection of mother and newborn.
Pediatrics 1980; 66: 489-94
49. Whitley RJ, Corey L, Arvin A, et al. Changing presentation
of neonatal herpes simplex virus infection. J Infect Dis 1988; 158:
109-16
50. Whitley RJ. Herpes simplex virus infections. In: Remington
JS, Klein JO, editors. Infectious diseases of the fetus and
new-born infant. 2nd ed. Philadelphia: WB Saunders Company, 1989:
282-305
51. Boston Interhospital Virus Study Group and the NIAID
Spon-sored Cooperative Antiviral Clinical Study. Failure of high
dose 5-deoxyuridine in the therapy of herpes simplex virus
© Adis International Lirnited. All rights reserved.
365
encephalitis: evidence of unacceptable toxicity. N Engl J Med
1975; 292: 600-3
52. Whitley RJ, Alford Jr CA, Hirsch MS, et al. Vidarabine
versus acyclovir therapy in herpes simplex encephalitis. N Engl J
Med 1986; 314 (3): 144-9
53. Skoldenberg B, Forsgren M, Alestig K, et al. Acyclovir
versus vidarabine in herpes simplex encephalitis: randomized
multi-center study in consecutive Swedish patients. Lancet 1984; I
(2): 707-11
54. Whitley RJ. Herpes simplex virus infections of the central
nerv-ous system: a review. Am J Med 1988; 85: 61-7
55. Whitley RJ, Arvin A, Prober C, et al. A controlled trial
compar-ing vidarabine with acyclovir in neonatal herpes simplex
vi-rus infection. N Engl J Med 1991; 324 (7): 444-9
56. Whitley RJ, Arvin A, Prober C, et al. Predictors of
morbidity and mortality in neonates with herpes simplex virus
infec-tions. N Engl J Med 1991; 324: 450-4
57. Van Landingham KE, Marstell HB, Ross Gw. Relapse of her-pes
simplex encephalitis after conventional acyclovir therapy. JAMA
1988; 259: 1051-3
58. Rothman AL, Cheeseman SH, Lehrman SN. Herpes simplex
encephalitis in a patient with lymphoma: relapse following
acyclovir therapy. JAMA 1988; 259: 1056-7
59. Davis LE, McLaren LE. Relapsing herpes simplex encephalitis
following antiviral therapy. Ann Neuro11983; 13: 192-5
60. Dix RD, Baringer JR, Panitch HS, et al. Recurrent herpes
sim-plex encephalitis: recovery of virus after Ara-A treatment. Ann
Neurol 1983; 13: 196-200
61. Whitley RJ. Varicella-zoster virus infections. In: Galasso
G, Merigan T, Whitley RJ, editors. Antiviral agents and viral
diseases of man. 3rd ed. New York: Raven Press, 1990: 235-63
62. Gnann J, Whitley RJ. Natural history and treatment of
varicella zoster in high risk populations. J Hosp Infect 1991; 18:
317-29
63. Whitley RJ. Cercopithecine herpes virus 1 (B Virus). In:
Fields BN, Knipe OM, Chanock R, editors. Virology. 2nd ed. New
York: Raven Press, 1990: 2063-75
64. Whitley RJ. Herpes simplex viruses. In: Fields BN, Knipe OM,
Howley PN, et al. Virology. 3rd ed. In press
65. Whitley RJ, Middlebrooks M. Rabies infections of the central
nervous system. In: Scheid WM, Whitley RJ, Durack DT, editors. New
York: Raven Press, 1991: 127-44
66. Baer GM, Bellini WJ, Fishbein DB. Rhabdoviruses. In: Fields
BN, Knipe OM, editors. Virology. 2nd ed. New York: Raven Press,
1990: 883-930
67. Murphy FA, Bauer SP, Harrison AK, et al. Comparative
patho-genesis of rabies and rabies-like viruses: viral infection
and transit from inoculation site to the central nervous system.
Lab Invest 1973; 28: 361-76
68. Centers for Disease Control. Rabies vaccine, absorbed: a new
rabies vaccine for use in humans. MMWR Morb Mortal Wkly Rep 1988;
37: 217-23
69. Immunization Practice Advisory Committee. Rabies preven-tion
- United States. MMWR Morb Mortal Wkly Rep 1984; 32: 393-402
70. Baer GM, Fishbein DB. Rabies post-exposure prophylaxis. N
Engl J Med 1987; 316: 1270-2
71. Melek LT, Soostmeyer G, Garvin RT, et al. The rabies
glyco-protein gene is expressed in Escherichia coli as a denatured
polypeptide. In: Chanock RM, Lerner RA, editors. Modern approaches
to vaccines. La Jolla, CA: Cold Spring Harbor Laboratory, 1984:
203-8
72. Macfarlan RI, Dietzschold B, Koprowski H, et al.
Localisation of the immunodomains of rabies virus glycoprotein.
In:
eNS Drugs 2 (5) 1994
-
366
Chanock RM, Lerner RA, editors. Modem approaches to vac-cines.
La Jolla, CA: Cold Spring Harbor Laboratory, 1984: 139-43
73. Dietzschold B, Wunner WH, Wiktor TJ, et al. Characterisation
of an antigenic determinant of the glycoprotein that correlates
with pathogenicity of rabies virus. Proc Natl Acad Sci USA 1983;
80: 70-4
74. Kieny MP, Lathe R, Drillien R, et al. Expression of rabies
virus glycoprotein from a recombinant vaccinia virus. Nature 1984;
312: 163-6
75. Lathe R, Kieny MP, Lecocq JP, et al. Immunization against
rabies using a vaccinia-rabies recombinant virus expressing the
surface glycoprotein. In: Lerner RA, Chanock RM, Brown F, editors.
Vaccines 85, molecular and chemical basis of re-sistance to
parasitic, bacterial and viral diseases. La Jolla, CA: Cold Spring
Harbor Laboratory, 1985: 157-62
76. Wiktor TJ, Macfarlan RI, Reagon KJ, et al. Protection from
rabies by a vaccinia virus recombinant containing the rabies virus
glycoprotein gene. Proc Natl Acad Sci USA 1984; 81: 71-94
77. Wiktor TJ, Macfarlan RI, Dietzschold B, et al. Immunogenic
properties of vaccinia recombinant virus expressing the rabies
glycoprotein. Ann Inst Pasteur 1985; 136: 105-9
78. Rupprecht CE, Dietzschold B, Koprowski H, et al.
Develop-ment of an oral wildlife rabies vaccine: immunization of
rac-coons by a vaccinia-rabies glycoprotein recombinant virus and
preliminary field baiting trials. In: Chanock RM, Lerner RA, Brown
F, editors. Vaccines 87, modem approaches to new vaccines:
prevention of AIDS and other viral, bacterial, and parasitic
diseases. La Jolla, CA: Cold Spring Harbor Lab-oratory, 1987:
389-92
79. Johnson RT. Arboviral encephalitis. In: Warren KS, Mahmoud
AAF, editors. Tropical and geographical medicine. 2nd ed. New York:
McGraw Hill, 1989: 691-700
80. Shope RE. Togaviruses. In: Fields BN, Knipe OM, Chanock RM,
et aI., editors. Virology. New York: Raven Press, 1985: 927-9
81. Monath TP. Flaviviruses. In: Fields BN, Knipe OM, editors.
Virology. New York: Raven Press, 1990: 763-814
82. Umenai T, Krzysko R, Bektimirov TA, et al. Japanese
enceph-alitis: current worldwide status. Bull World Health Organ
1985; 63: 625-31
83. Nathanson N. Epidemiologic agents of poliomyelitis
eradica-tion. Rev Infect Dis 1984; 6: 308-12
84. Centers for Disease Control. Poliomyelitis - United States,
1975-84. MMWR Morb Mortal Wkly Rep 1986; 35: 180-2
85. Almond JW, Burke KL, Skinner MA, et al. Redesigning
polio-virus for vaccine purposes. In: Norby SR, editor. New
antiviral strategies. London: Churchill Livingstone, 1988:
205-14
86. Almond JW. The attenuation of poliovirus neurovirulence. Ann
Rev Microbiol1987; 41: 153-80
87. Almond JW, Stanway GC, Cann AJ, et al. New poliovirus
vac-cines: a molecular approach. Vaccine 1984; 2: 174-84
88. Kaplan MH, Klein SW, McPhee J, et al. Group B coxsackie
virus infections in infants younger than three months of age. Rev
Infect Dis 1983; 5: 1019-32
89. Modlin JE Perinatal echovirus infection: insights from a
litera-ture review of 61 cases of serious infection and 16
outbreaks in nurseries. Rev Infect Dis 1986; 8: 918-26
90. McKinney RE, Katz SL. Chronic enteroviral
meningoenceph-alitis in agammaglobulinemic patients. Rev Infect Dis
1987; 9: 334-6
91. Roman Gc. The neuroepiderniology of tropical spastic
parapa-resis. Ann Neurol 1988; 23: 113-20
© Adls International limited. All rights reserved.
Whitley
92. Hinuma Y, Komoda H, Chosa T. Antibodies to adult T-cell
leu-kemia-virus associated antigens (ALTA) in sera from patients
with ALT and controls in Japan: a nationwide sero-epidemi-ologic
study. Int J Cancer 1982; 29: 631-5
93. Jordan BD, Navia BA, Petito C, et al. Neurological syndromes
complicating AIDS. Front Radiat Ther Onco11985; 19: 82-7
94. Navia BA, Price RW. The acquired immunodeficiency syn-drome
dementia complex as the presenting or sole manifesta-tion of human
immunodeficiency virus infection. Arch Neurol 1987; 44: 65-9
95. Comblath DR, McArthur JC, Kennedy PGE, et al. Inflamma-tory
demyelinating peripheral neuropathies associated with human
T-celllymphotropic virus type III infection. Ann Neu-rol 1987; 21:
32-40
96. Hollander H, Stringari S. Human immunodeficiency
virus-associated meningitis. Am J Med 1987; 83: 813-6
97. Appleman ME, Marshall OW, Brey RL. Cerebrospinal fluid
abnormalities in patients without AIDS who are seropositive for the
human immunodeficiency virus. J Infect Dis 1988; 158: 193-9
98. Hollander H. Cerebrospinal fluid normalities and
abnormalities in individuals infected with human immunodeficiency
virus. JInfect Dis 1988; 158: 855-8
99. Navia BA, Jordan BD, Price RW. The AIDS dementia complex: I.
Clinical features. Ann Neuro11986; 19: 517-24
100. Rance NE, McArthur JC, Comblath DR, et al. Gracile tract
degeneration in patients with sensory neuropathy and AIDS.
Neurology 1988; 38: 265-71
101. Richman DO. HIV and other human retroviruses. In: Galasso
GJ, Merigan TC, Whitley RJ, editors. Antiviral agents and viral
diseases of man. 3rd ed. New York: Raven Press, 1990: 581-649
102. Fischl MA, Richman DO, Grieco MH, et al. The efficacy of
azidothymidine (AZT) in the treatment of patients with AIDS and
AIDS-related complex: a double-blind, placebo-control-led trial. N
Engl J Med 1987; 317: 185-91
103. Pizzo PA, Eddy J, Fallon J, et al. Effect of continuous
intra-venous infusion of zidovudine (AZT) in children with
symp-tomatic HIV infection. N Engl J Med 1988; 319: 889-96
104. Epstein LG, Sharer LR, Oleske JM. Neurologic manifestations
of human immunodeficiency virus infection in children. Pe-diatrics
1986; 78: 678-87
105. Belman AL, Diamond G, Dickson D. Pediatric acquired
immu-nodeficiency syndrome: neurologic syndromes. Am J Dis Child
1988; 142: 29-35
106. Ho DO, Rota TR, Schooley RT. Isolation of HTLV-III from
cerebrospinal fluid and neural tissues of patients with neuro-logic
syndromes related to the acquired immunodeficiency syndrome. N Engl
J Med 1985; 313: 1493-7
107. Hollander H, Levy JA. Neurologic abnormalities and recovery
of human immunodeficiency virus from cerebrospinal fluid. Ann
Intern Med 1987; 106: 692-5
108. McCormick JB, King IJ, Webb PA. Lassa fever: effective
ther-apy with ribavirin. N Engl J Med 1986; 314: 20-6
Correspondence and reprints: Dr Richard J. Whitley, Univer-sity
of Alabama at Birmingham, Department of Pediatrics, Microbiology,
and Medicine, 616 Children's Hospital -ACC, 1600 Seventh Avenue
South, Birmingham, AL 35233, USA.
eNS Drugs 2 (5) 1994