-
10/27/2014
1
Going, Going, Not Quite Gone…The Race to End Perinatal HIV
TransmissionCarol A. Vincent, PhD, CRNP, AAHIVS
The Children’s Hospital of Philadelphia
Objectives
•
Describe how current trends in the HIV epidemic impact HIV in women and children in the United States
•
Discuss current standards of care for the prevention of mother to child HIV transmission.
•
Recognize psychosocial issues related to HIV testing and infection in pregnant women.
•
Using case scenarios, describe the Nurse Practitioner’s role in implementation standards of care in prevention of perinatal transmission and pharmacologic management of HIV prevention medications as they relate to the case scenarios.
-
10/27/2014
2
Percentages of HIV Cases Diagnosed Among Female Adults and
Adolescents, by Transmission Category
2010—46 States and 5 US-Dependent Areas
Note: Data include persons with a diagnosis of HIV infection regardless of their AIDS status at diagnosis. Data from 46 states with confidential name‐based HIV infection reporting since at least 2003. Data have been adjusted for reporting delays and missing risk‐factor information.*Heterosexual contact with a person known to have, or to be at high risk for, HIV infection.†Includes blood transfusion, perinatal exposure, and risk factor not reported or not iden
fied. Source CDC website
6
-
10/27/2014
3
Estimated Numbers and Percentages* of AIDS Cases Among Female
Adults and Adolescents
1985–2010—United States and Dependent Areas
Year of diagnosis
Cas
es,N
o.
Cas
es,%
20071985 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996
1997 1998 1999 2000 2003 2004 2005 20062001 2002 2008 2009 2010
Note: Data have been adjusted for reporting delays.*Percentage of all cases that were diagnosed among females.
5
AIDS Cases Among Female Adults and AdolescentsAttributed to
Injection Drug Use or High-Risk Heterosexual
Contact, by Region, 2003–2007—50 States and DC
4
Northeast Midwest South WestRegion
16
20
12
8
0
Note: Data have been adjusted for reporting delays and missing risk‐factor information. * Heterosexual contact with a person known to have, or to be at high risk for, HIV infection.
7
-
10/27/2014
4
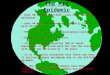
Global HIV Rates● There are an estimated 34 million people
infected with HIV● Worldwide, of people living with HIV, the
percentage of
women with HIV remains at 50%● Nearly 68% of all people with HIV
globally live in sub-
Saharan Africa ● 70% of AIDS deaths in 2011 occurred in
sub-Saharan Africa● In sub-Saharan Africa, women make up nearly 60%
of those
with HIV infection● Nearly 15 million children
-
10/27/2014
5
Female Health Disparities•
Females account for an increased proportion of HIV cases in U.S.
–
In 2010‐2011, 25% of HIV/AIDS patients were female–
Increased from 23% in 2007 and 14% in 1992
• Changes in transmission risk–
Increased heterosexual contact– Decreased IDU
•
Continued disproportionate impact on African American womenLifetime risk:
–
1 in 32 African American women (decreased in 2010)–
1 in 106 Hispanic women–
1 in 526 Caucasian women
Pediatric HIV Infection: Mother to Child Transmission
Pediatric AIDS Clinical Trials Group 076
A phase III randomized placebo-controlled trial of zidovudine
(ZDV) for preventing maternal-fetal HIV transmission.Treatment
Regimen
●Antepartum: 100 mg ZDV po 5x day, started at 14–34 weeks
gestation
●Intrapartum: During labor, 1-hour initial dose 2 mg/kg IV
followed by continuous infusion of 1 mg/kg until delivery
●Postpartum/Infant: 2 mg/kg po q 6 hr for 6 weeks, start 8–12
hours after birth
35
-
10/27/2014
6
Results of Pediatric AIDS Clinical Trials Group 076
● Intervention led to a 66% reduction in risk for transmission
(P=
-
10/27/2014
7
Research to Implementation: # of HIV‐infected Infants and MTCT Rate in NY State by year of delivery, 1997‐2011
•
Source: AIDS Institute, New York State Department of Health, 2012
We are doing better but…how do we get to zero?... and how do we stay
there?
HIV Cascade
-
10/27/2014
8
Prevention of Perinatal HIV ● With maternal diagnosis and
prophylaxis
during the perinatal period, perinatal HIV transmission is
usually preventable in all but 2% or less cases
● In order to reach this goal, HIV testing and antiretroviral
(ARV) prophylaxis and treatment are essential
11
PMTCT: More Than Just AntiretroviralsFour Pillar Prevention Strategy
•
Pillar 1 Prevention of HIV in Women•
Pillar 2 Prevention of Unintended Pregnancies in HIV + Women
•
Pillar 3 Prevention of MTCT from an HIV + Woman to her infant
•
Pillar 4 Support for HIV+ Mother and Family
• Wilcher, R, et.al Sex Trans Inf
2008: 84 (Supp2):iii54‐60.
What is Needed to Prevent MTCT: The PMTCT Cascade
• What it really entails
Credit: Lynne Mofenson MD NICHD
-
10/27/2014
9
Prevention Strategies in the US•
Planned conception•
Universal prenatal testing of all pregnant women•
Use of combination antiretrovirals during pregnancy to reliably and durably suppress viral load
•
Individualized laboratory management (CD4 count and HIV viral load)
• Infant antiretroviral prophylaxis•
Elective C‐section (Viral Load
-
10/27/2014
10
Reproductive Health Care:Goals of Preconception Counseling
Improve the knowledge, attitudes and behaviors of men &
women related to preconception health.
Assure all women of childbearing age in U.S. receive
preconception care that will enable them to enter pregnancy in
optimal health.Reduce risks indicated by previous pregnancy which
can prevent or minimize problems for mother and her future
children.Reduce the disparities in adverse pregnancy outcomes.
HIV Testing
Patients routinely tested for HIV should include:
• All patients aged 13‐64 years
•
All patients initiating treatment for TB
•
All patients seeking treatment for STDs during each visit for a new complaint, regardless of specific behavioral risks for HIV infectionCDC. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in healthcare settings. MMWR 2006;55(RR14);1-17.
HIV TestingHIV testing should be: •
Voluntary and with the patient's knowledge that HIV testing is planned
•
Provided as an opt‐out healthcare service•
Accompanied with information, including an oral and/or written explanation of HIV infection and the meanings of positive and negative test results
•
Consented for in the same way as other screening or diagnostic tests
•
Declinations should be documented in the medical record.
-
10/27/2014
11
HIV Testing•
Test all persons at high risk for HIV at least annually
–
High risk populations include: MSM or heterosexual persons who have had more than one sex partner since their last HIV test, injection‐drug users, sex workers, and sexual partners of people at high risk or with a diagnosis of HIV
•
For those at lower risk, repeat testing should be performed based on clinical judgment
•
Encourage patients and their prospective partners to be tested before initiating a new sexual relationship
HIV Testing in Pregnancy
•
Test women as early as possible during each pregnancy
•
A second HIV test during the third trimester, preferably
-
10/27/2014
12
HIV Testing in Labor and Delivery•
Women with undocumented HIV status in labor should be screened with a rapid/expedited HIV test
•
Women with unknown status after delivery should be screened immediately postpartum
•
If the rapid/expedited test is reactive, immediately initiate antiretroviral prophylaxis. Do not wait for the result of a confirmatory test.
Recommendations for 3rd Trimester Repeat HIV Testing
● In jurisdictions with an elevated incidence of HIV/AIDS among
women
● Women known to be at high risk for HIV
● Facilities that identify HIV infection in at least 1/1,000
women screened
● Women who have signs or symptoms of acute HIV infection (acute
retroviral syndrome)
19
Why Aren’t All Pregnant Women Tested?
• Provider• Language barriers • Late entry or no prenatal
care • Patient perceived as not at
risk• Provider does not strongly
recommend testing to all women
• Patient• Women’s reasons for not
being tested– Do not think they are at
risk– Have been tested
“recently”– Test not offered or
recommended
• Negative consequences of testing rarely mentioned
-
10/27/2014
13
Case Study #1
•
Lisa and her partner Joseph are expecting their first baby. Lisa is 11 weeks pregnant and this is her first visit. She reads a pamphlet in the waiting room.
•
When you offer HIV testing to Lisa as part of her prenatal testing she tells you “I don’t need HIV testing. I haven’t been with anyone but Joseph and I don’t do drugs”
• How do you proceed?•
If the case scenario changed and she accepted and said she tested negative, how would you proceed?
I’m HIV positive and pregnant…now what?
-
10/27/2014
14
Perinatal HIV Transmission● Without ARV drugs during pregnancy,
risk of
transmission from mother to infant is 1 in 4● Pediatric AIDS
Clinical Trials Group (PACTG) 076
found that by giving zidovudine (ZDV) to the pregnant woman
during pregnancy, labor, and delivery, and to her newborn,
transmission could be reduced to 8%
● The risk of perinatal transmission can now be less than 2% (1
in 50) with:● Highly effective ARV therapy (HAART)●Elective
Cesarean section as appropriate ●Formula feeding
13
Assuming No Interventions:
Reproductive Health Care:Preconception/Postconception
Opportunities
(ACOG, 2006)• Optimize maternal HIV stability.• Choose “safe”
ARV’s• Ed/Counsel HIV MTCT risks.• For HIV Discordant Couples
discuss
optimal risk reduction techniques.• Evaluate need for
vaccination/OI
prophylaxis.• Optimize Nutritional Health• PNV/Folic Acid.•
Genetic Screening/Compile OB History.
-
10/27/2014
15
Timing of Perinatal HIV Transmission: Non-Breastfeeding
Women
● Intrauterine (before 36 weeks) ~20% of cases● Virologic
detection of HIV in newborn at 1–2 days of life
● Peripartum ~80% of cases● Onset of placental separation●
Mother-to-fetus microtransfusions● Labor and rupture of
membranes
● Most transmission occurs close to or during labor and delivery
(L&D) 14
A Healthy Pregnancy: The Mother
HIV viral load monitoring •
Initial visit •
2‐4 weeks after ART is started or changed•
Monthly until HIV is undetectable•
Every 3 months throughout pregnancy•
At 34‐36 weeks gestation HIV drug‐resistance testing with ART initiation and regimen changesCD4 monitoring every trimester Selecting, monitoring, and changing ART
Monitoring and PlanningMonitoring •
Infant growth and development •
Maternal complications
Plan for Labor & Delivery•
Vaginal delivery recommended if HIV viral load 1,000 at 38 weeks•
IV zidovudine
(AZT) recommended (BIII) if HIV viral load >400•
Avoid procedures that increase transmission risk:
–
Rupture of membranes (natural or artificial) and labor onset–
Fetal scalp electrodes –
Forceps or vacuum extractor –
Episiotomy
-
10/27/2014
16
Factors Influencing Perinatal Transmission
● Maternal Factors●High HIV-1 RNA levels (viral load [VL])●Low
CD4+ lymphocyte count (“T-cells”) ●Co-infections: Hepatitis C,
cytomegalovirus
(CMV) bacterial vaginosis●Maternal injection drug use●No ARV
therapy or prophylaxis
15
Risk of MCT
• In studies prior to any therapy:–
Africa: 30‐45%– US: 20‐25%–
ECS: 13%
–
What were the factors influencing the large differences in world wide MCT?
Risk of MCT
• Possible hypothesis:– Breast feeding–
HIV strain differences–
Immune status of mother–
Co‐factors/Nutritional status–
Genetic factors of the host
-
10/27/2014
17
Reproductive Health Care: Vertical Transmission Protocol
• All pregnant HIV + women should be offered ART to maximally
suppress viral replication, reduce the risk of perinatal
transmission and minimize the development of resistant virus.
• Start ART at least by 28 wks gestation.• Include AZT if
possible.• Mother treated during pregnancy, IV AZT
antepartum and infant 6 wks after delivery.• Educate/counsel
breast milk transmission.
Review: Goals of ARV Therapy
● Suppress HIV to below the limits of detection or as low as
possible for as long as possible
● Prolong life and improve quality of life
● Preserve or restore immune function
● Reduce risk of perinatal transmission
41
-
10/27/2014
18
Resources for Clinicians
• Offering information on AIDS treatment, prevention, and
research
• Clinical guidelines for ARV treatment–
Perinatal/Mother-to-Child Transmission – Pediatrics– Adults and
Adolescents
• http://www.aidsinfo.nih.gov107
Summary of Current Knowledge on Factors Affecting
Mother-to-Child HIV-1 Transmission
Known risk factorsHigh maternal viral loadViral
genotype/phenotypeAdvanced maternal HIV diseaseLow CD4 count or
percentVaginal deliveryDuration of membrane rupture > 4
hoursPremature delivery (< 37 weeks)Breastfeeding
Factors for which evidence is suggestive but not
conclusiveGenetic factorsImmature immune system in infantIncreased
viral strain diversity Maternal neutralizing antibodyIllicit drug
use during pregnancyFrequency of unprotected sexual
intercourseMultiple sex partners during pregnancyMaternal
nutritional statusAnemia during pregnancy Cigarette smoking
ChorioamnionitisAbruptio placentaePlacental P. falciparum
infestationSyphilis and other STDFetal scalp electrodesEpisiotomy
and vaginal tears
The Infant: Preventing HIV infection
•
Prevention of Mother to Child Transmission does not end at delivery
-
10/27/2014
19
Perinatal ARV Guidelines
• USPHS Task Force Recommendations for the Use of ARV Drugs in
Pregnant HIV-1 Infected Women for Maternal Health and to Reduce
Perinatal HIV-1 Transmission in the United States
• Developed in 1994 in response to PACTG 076• Working group
meets monthly• Updated recommendations available online at
AIDSInfo website (http://www.aidsinfo.nih.gov)42
PREVENTION OF MCT
•
Starting therapy at birth still reduces the risk of transmission of HIV, from 20% to 13‐15%.
•
Therefore, women with no PNC, or no HIV testing on file, should be offered rapid HIV testing at presentation in active labor.
CARE OF THE HIV‐EXPOSED INFANT
•
At birth, begin ZDV therapy, based on weight and gestational age: for full term infants: 2mg/kg/dose 4x/day or 4mg/kg 2x/day
•
If high risk: if there was no maternal treatmentmaternal VL >1000PROM >8‐12hrsprematurity
-
10/27/2014
20
CARE OF THE HIV‐EXPOSED INFANT
•
If high risk: no maternal treatmentNICHD‐PACTG 1043Enrolled newborns when mom presented in labor on no
therapy:
Infant regimens/infection rate (including in‐utero)ZDV for 6 weeks
11%ZDV and NVP 3doses/72hrs
7.1%ZDV and 3TC/Nelfinavir for 2 weeks 7.4%
RISKS OF PERINATAL ANTIRETROVIRAL THERAPY
•
Blanche, et al. French Collaborative Study:Initial report of 2 deaths, related mitochondrial disease in HIV‐exposed uninfected infants. (perinatal rx
with ZDV/3TC).Later, report of possibly 8 children with less severe symptoms.
•
US meta‐analysis of >23,000 HIV‐exposed infants revealed no unexpected events
CARE OF THE HIV‐EXPOSED INFANT
Testing for the diagnosis:•
Use RNA qualitative assay
» False positive rate 1‐2%»
False negative rate 4% after 2 weeks of age
–
If mother is known to be HIV +, and infant at low risk:
•
PCR RNA at 2 weeks, 4wks and 4mon •
A negative RNA ql assay at 2 wks
and 4wks months indicates infant is presumptively HIV negative. A negative at 4months r/o HIV infection (as per CDC)
•
For high risk infants, additional tests at day 1 of life and at 8 weeks of age (along with tests at 2wks,4wks and 4months)
•
Follow HIV ab until infant becomes HIV ab negative, usually between 12 and 18 months of age.
-
10/27/2014
21
CARE OF THE HIV‐EXPOSED INFANT
•
At birth, begin ZDV therapy, based on weight and gestational age.
• Continue ZDV for 6 weeks.•
At 2 weeks, assess CBC, send HIV PCR QL•
At 4 wks send CBC, CD4, HIV PCR•
At 6 weeks,d/c ZDV and start TMP/SMZ if there is only one RNA test results available. If there are 2 neg(2 and 4wks), do NOT need to start TMP/SMZ
CARE OF THE HIV‐EXPOSED INFANT
Testing for the diagnosis:•
Use RNA qualitative assay
» False positive rate 1‐2%»
False negative rate 4% after 2 weeks of age
–
If mother is known to be HIV +, and infant at low risk:•
PCR RNA at 2 weeks, 4wks and 4mon •
A negative RNA qualitative assay at 2 wks
and 4wks months indicates infant is presumptively HIV negative. A negative at 4months r/o HIV infection (as per CDC)
•
For high risk infants, additional tests at day 1 of life and at 8 weeks of age (along with tests at 2wks,4wks and 4months)
•
Follow HIV ab until infant becomes HIV ab negative, usually between 12 and 18 months of age.
Breastfeeding by HIV‐infected women is not recommended in the United
States.•
Breastfeeding by HIV‐infected women (including those receiving ARV drugs) is not recommended in the United States where replacement feeding is affordable, feasible, acceptable, sustainable, and safe and the risk of infant mortality due to diarrheal and respiratory infections is low.
•
Importantly, although significantly lowering the risk of postnatal infection, neither infant nor maternal postpartum ARV prophylaxis completely eliminates the risk of HIV transmission through breast milk.
-
10/27/2014
22
Mixed feeding (breast + formula) is most dangerous.
•
Mixed feeding is the most dangerous method–
Formula feeding can irritate the lining of the baby's stomach
–
Irritation makes it easier for the HIV in breast milk to get in and cause an infection.
–
In a South African study of HIV‐positive women and their babies, 36 percent of babies who received mixed feeding were reported infected compared to about 25 percent of those who were exclusively breast‐fed and 19.5
percent of formula‐fed babies.
HIV-Positive Pregnant Women:Psychosocial Issues
● Stigma: in community and in health care ● Non-disclosure: to
partners, health-care team● Domestic partner violence● Mental
health ● Substance abuse● Worry about infection status of infant●
For more information, see http://www.aidsetc.org
or http://www.womenchildrenhiv.org102
Legal and Ethical Issues with Impact on HIV Care
● Confidentiality and HIV reporting● Non-disclosure to sexual
partners● Reproductive health and family planning● Immigration
issues● Access to prenatal/HIV care● For more information see:
http://www.aidsetc.org
and search on the topic of interest
103
-
10/27/2014
23
Perinatal Hotline – National Perinatal HIV Consultation and
Referral Service
• Around-the-clock advice on testing and care of HIV-infected
pregnant women and their infants
• Provides referral to HIV specialists and regional resources–
1-888-448-8765
– [email protected]
• For additional resources: http://www.nccc.ucsf.edu
Remaining Research Questions
•
Long term outcome of perinatal exposure to HAART (p219, SMAART)
•
Benefits of initiating treatment for infected neonates at 2 wks vs 1 or 3 months of age
•
Optimal treatment for HIV‐exposed neonates with no maternal pre‐treatment
Case Study #2
•
Linda is a 24 year old female who presents to L&D in active labor and delivers precipitously. She has never had and HIV test. She admits to active intravenous drug use. What other questions do you want to ask her?
•
What intervention would you recommend for her baby who was full term by dates
-
10/27/2014
24
Case Study #3
• Shantay
is a 30 year old woman who presents to the perinatal clinic. She is 30 weeks pregnant. When you ask her if she has had prenatal care, She tells you no. “this is my 4th
child and I know what I am doing“. She tests HIV positive at this visit.
What do you do next?
•
She delivers a healthy baby girl at 38 weeks. Shantay’sviral load is undetectable and her CD4 count is 550. What do you offer her next? What do you offer for the baby?
• Shantay
tells you she wants to breastfeed. How do you counsel her?
We are Citizens of the World
HIV Global Burden
-
10/27/2014
25
End PMTCT by 2015
Mississippi to Milan
• Mississippi baby• Milan Baby•
Aggressive treatment•
Thought to be cured….then a relapse.
Challenges: What’s Left to Do
• Challenges:–
Maintaining momentum costs money and utilizes many resources
–
Building into the Standard of Care
– Gaining “buy in” worldwide
– Public health and provider education
• Opportunity to use PMTCT to:–
Address other health threats
– Address maternal and child mortality
– Strengthen MCH services–
Ensure good health outcomes for mother, child and family
-
10/27/2014
26
Special Thanks to:
CHOP Family Care Center and Medical Director‐Dr. Rick RutsteinPennsylvania AIDS Education and Training CenterDr. Lynne Mofenson, NICHDDr. Kathleen Brady (Upenn/Philadelphia Department of Health)