Embed Size (px)
Citation preview

April 20, 2014
Linda G. Snetselaar, PhD, RDN, LDEditor-in-ChiefJournal of the Academy of Nutrition and Dietetics
Dear Dr. Snetselaar,
I am pleased to submit my manuscript entitled: “Natural Sleep Initiative Reduces the Incidence of Falls and Increases Patient Satisfaction Among Hospital Inpatients”, for consideration as a research article. This study follows a cross-sectional design frame, monitoring trends of inpatient falls and patients’ overall satisfaction with the service provided. Five months after the introduction of the initiative, the results showed a downward trend in inpatient falls and significant patient satisfaction.
The incidence of falls in hospitals nation-wide is a well-documented safety issue. Fall-risk reduction is a recognized National Patient Safety Goal of the Joint Commission. The aim of this research study was to explore alternate, non-pharmacologic sleep interventions as a primary means to reduce the likelihood of patient falls in the hospital.
This study was conducted in fulfillment of requirements of the Aramark Distance Learning Dietetic Internship. The study was conducted under the supervision of a registered dietitian at Einstein Medical Center Montgomery as well as an Aramark Dietetic Internship Director. The study was conducted with permission and grant funding from the Albert Einstein Society.
This manuscript has not been previously published and is not under consideration in the same form in any other peer-reviewed media. Thank you for your consideration of this manuscript.
Sincerely,
Heather Pavlik, BS (Corresponding Author)Dietetic Intern Aramark Healthcare Distance Learning Dietetic [email protected]
Cyndra Banta, MS, RD, LDRegional DirectorAramark Healthcare Distance Learning Dietetic [email protected]
Lisa DeHaven, MS, RD, LDNDirector of Patient ServicesEinstein Medical Center [email protected]
1

Natural Sleep Initiative Reduces the Incidence of Falls and
Increases Patient Satisfaction Among Hospital Inpatients
Key Words: Sleep, falls, hypnotics, cognitive-behavioral therapies
Word Count: 2,893
Heather Pavlik, Dietetic Intern
ARAMARK Dietetic Internship, Einstein Medical Center Montgomery
2

Natural Sleep Initiative Reduces the Incidence of Falls and Increases Patient
Satisfaction Among Hospital Inpatients
ABSTRACT
The incidence of falls in hospitals nation-wide is a well-documented safety issue.
Fall-risk reduction is a recognized National Patient Safety Goal of the Joint Commission.
It is also well recognized that sleep-inducing pharmacologic agents used in the hospital
setting play a large role as causative agents in patient falls. The aim of this initiative was
to explore alternate, non-pharmacologic sleep interventions as a primary means to
reduce the likelihood of patient falls in the hospital. This cross-sectional study was
conducted from October of 2013 to February of 2014 and included 6,109 subjects.
Subjects were selected based on two criteria: 1) patients who were considered at fall
risk and/or 2) patients receiving pharmacologic sleep agents. Descriptive statistical
procedures were utilized to analyze the effectiveness of the study. The results showed
that overall patients were satisfied with the study; 87% of patients were satisfied with
the services of the sleep initiative and 13% of patients were dissatisfied with the service.
Additionally, results indicated that there were 10 fewer total falls and 6 fewer falls of
patients on sleep agents after initiating the study. This was an 18% reduction in total
falls and a 40% reduction in falls of patients on sleep agents since the start of the study.
These successful outcomes demonstrate a downward trend in patient falls and an
upward trend in patient satisfaction since the initiation of the Natural Sleep Initiative in
October of 2013.
3

Natural Sleep Initiative Reduces the Incidence of Falls and Increases Patient
Satisfaction Among Hospital Inpatients
INTRODUCTION
The negative sequela stemming from patient falls in an institutional setting is well
recognized nationally and has been a primary area of focus for the Joint Commission for
Accreditation for some time now. Of the 10 Hospital Acquired Conditions (HACs) that
Centers for Medicare and Medicaid Services (CMS) looks at, “Falls with Trauma” is the
most frequently occurring class. The Pennsylvania Patient Safety Authority stated that
the incidence of falls with trauma in the state of Pennsylvania is 0.581/1000 patient
discharges. This is almost 3% greater than the national rate of 0.564/1000 patient
discharges.1
Five months prior to the start of the study, May to September of 2013, Einstein
Medical Center Montgomery (EMCM) has had 55 patient fall events. Five months after
the start of the initiative, October to February of 2013, there have been 45 patient fall
events. Falls can lead to patient injuries and prolonged hospital stays. Falls are the
most common type of inpatient hospital accident, reportedly accounting for up to 70% of
all inpatient accidents.2 The average additional cost attributed to a fall with serious injury
is $13,316 and the additional average length of stay increase is 6.3 days compared to
patients who did not fall.3 Due to the fact that many insurance providers will not pay for
injuries resulting from patient falls, there is a significant impact to the hospital’s fiscal
success in finding methods and processes to reduce or eliminate them. The Joint
Commission’s Provision of Care Standard, PC 01.02.07, drives institutions to monitor
and find ways to reduce or eliminate patient falls, not only by assessing the risk for falls,
4

but also by implementing interventions designed to reduce them. It is estimated that
25% of these fall injuries can be prevented.4
The elderly population is most susceptible to falls in an institution, but any patient
could experience a risk for falls, especially when centrally acting drugs such as
pharmacologic sleeping agents are used to promote sleep and treat insomnia. A
number of these falls can be attributed to the “hangover” effects from the use of
pharmacologic sleeping agents leading to cognitive and motor impairment. It is further
suggested that lack of effective sleep cycles can also lead to cognitive and motor
deficits, especially in the elderly.5, 6 It is well recognized that pharmacologic agents used
to induce sleep, both the benzodiazepine and non-benzodiazepine variety, lead to an
increased risk for not only falls, but death as well.
Hospitalized patients have increased rates of sleep disturbances, which have led
to the frequent prescription of hypnotic pharmacologic agents in the inpatient setting.7
The most common classes of approved sedative hypnotic drugs used to treat insomnia
include benzodiazepines (BZDs), benzodiazepine receptor antagonists (BzRAs),
antidepressants, melatonin receptor agonists, and histamine antagonists.8 Drugs
currently marketed as hypnotics have much more favorable side effects and a larger
therapeutic margin than the formerly prescribed barbiturates.9 According to data pulled
by Einstein pharmacists, the most frequently prescribed sleep medications at EMCM
over the past three months include zolpidem (Ambien), lorazepam (Ativan), alprazolam
(Xanax), trazodone (Depyrel), diphenhydramine (Benadryl), and mirtazapine
(Remeron). Lorazepam and alprazolam are classified as BZDs, zolpidem is classified as
a BzRA drug, trazodone and mirtazapine are sedative antidepressants, and
5

diphenhydramine is a sleep aid in over the counter sleep products. Zolpidem is the most
commonly prescribed hypnotic agent in the United States and is also one the most
frequently used in inpatient settings.7, 10 All sleep medications prescribed at Einstein
Medical Center Montgomery are administered to hospital inpatients for their sleep-
inducing effects.
There are many factors that are associated with and contribute to fall risk.
Hospital falls often occur during the nighttime, suggesting that factors related to
nighttime sleep may contribute to fall risk. These factors include waking at night, sleep
medications and hypnotic medications, untreated insomnia and other sleep problems,
and nocturia.11 Insomnia is a common occurrence in the hospital setting, even for those
with no history of it, secondary to unfamiliar surroundings, noises, interruptions, drug
side effects, and pain or discomfort from a procedure or disease process. Several
studies have been conducted within the past five years to determine if sleep
medications and hypnotics are, in fact, independently associated with the risk of
inpatient falls.7, 12-14
One study found that the fall rate among patients who were prescribed and
received zolpidem was significantly greater than among patients who were prescribed
but did not receive zolpidem, 3.04% versus 0.71%.7 Two separate studies measured the
balance and cognition of patients after middle-of-the-night awakening.12, 13 A study by
Frey et al. assessed balance using a tandem walk on a beam and cognition using
computerized performance tasks, such as mathematical addition problems. This study
found that zolpidem produced clinically significant balance and cognition impairments
upon awakening from sleep.12 The second study focusing on balance and cognition
6

detected balance and stability impairments using computerized dynamic posturography
(CDP), a clinical assessment technique used to quantify the central nervous
system’s adaptive mechanisms involved in the control of posture and balance. It was
found that bedtime administration of zolpidem lead to significant balance impairments,
indicating that pharmacological treatment of sleeplessness is a risk factor for patient
falls.13 Zolpidem was used as the test medication in the majority of falls studies related
to hypnotics administration due to its common prescription in the United States and its
ability to alter balance for up to 5 hours after administration.13 Recent media attention
has again raised awareness and even FDA mandated dosing changes have been made
to popular pharmacologic sleeping agents, like zolpidem (Ambien™), after studies
confirmed that drug levels, especially in females, can still be present in sufficient levels
to cause motor and cognitive impairment the day after these agents have been
consumed.
According to Kolla et al., non-pharmacological measures to improve the sleep of
hospitalized patients should be investigated as preferred methods to provide safe relief
from complaints of disturbed sleep.7 In the last decade, many publications on the
efficacy of pharmacotherapy versus various psychological and behavioral therapies for
insomnia have been released. To address the multitude of psychological and behavioral
factors at the root of sleeplessness, a multicomponent Cognitive-Behavior Therapy
(CBT) for insomnia emerged.15 Common behavioral therapies include sleep hygiene,
relaxation therapy, stimulus control therapy, and sleep restriction therapy. A variety of
studies conclude that both sleep medications and psychological and behavioral
treatments are effective for short-term treatment of insomnia, but psychological and
7

behavioral treatment alone is significantly more efficient for long-term treatment when
medicinal prescriptions are discontinued.16
The Natural Sleep Initiative is a program that will be put in place at Einstein
Medical Center Montgomery (EMCM) to reduce the use of pharmacologic interventions
to treat insomnia and provide alternate non-pharmacological means to ensure restful
sleep to patients. The initiative will utilize EMCM’s state-of-the-art GetWell Network to
promote the program and offer patients the ability to order the service from the comfort
of their own room. The purpose of this study will be to assess the effectiveness of the
Natural Sleep Initiative on patient satisfaction and the patient’s level of relaxation after
participating in the program. The study will also aim to evaluate the success of the
program on preventing or reducing the incidence of falls for patients receiving sleeping
medications and/or at fall risk at Einstein Medical Center Montgomery. Another goal,
established by the department of pharmacy, is to decrease the prescription and
administration of hypnotic sleep medications. The question at hand is as follows: will the
implementation of a Natural Sleep Initiative improve patient satisfaction, decrease the
administration of sleep medications, and reduce the incidence of inpatient falls?
METHODOLOGY
The Natural Sleep Initiative was a cross-sectional study that included inpatients
on the telemetry and medical/surgical floors of EMCM. Physicians, nurses, pharmacists,
and food service workers monitored for patients in need of sleep aids on a daily basis.
Once it was determined that a patient was experiencing insomnia, a consult for the
Natural Sleep Initiative services was placed and the food service workers initiated the
8

Natural Sleep services for the patient. The clinical pharmacist and physician monitored
for patients ordered pharmacologic sleep agents in the areas that the initiative was
being plotted. Medication record reports were used to capture and audit this. Patients
ordered sleeping agents on the floors included in the study were referred to the Natural
Sleep Initiative services upon approval by the physician. A nightly visit report captured
patients who were either on sleeping medications or at fall risk. The patients included in
the nightly visit report were offered the amenities of the Natural Sleep Initiative.
Patients, caretakers, and nursing staff were educated on the benefits of the non-
pharmacologic alternative treatment approach.
The goal of the Natural Sleep Initiative at Einstein Medical Center Montgomery
was to reduce the number of falls of patients on sleep medications and provide a
superior patient experience. This initiative incorporates a variety of the CBT treatments,
including sleep hygiene and relaxation therapy. Four per diem food service workers
offered a variety of decaffeinated herbal teas, tea cookies, and Sweet Dream Kits
between the hours of 6:00 PM and 8:00PM, seven nights per week. Sweet Dream Kits
included an eye mask, earplugs, a lavender pouch, and a small card with sleep tips.
The service will be offered seven days a week for a period of 6 months to one year,
which is to be determined.
Data was collected 5 months prior to the start of the initiative, May 2013 to
September 2013, and for the first 5 months after the start of the initiative, October 2013
to February 2014. Results of the Natural Sleep Initiative were determined using patient
surveys and assessment of fall reports before and after starting the initiative. Shortly
before a patient was discharged, they were prompted to participate in a survey
9

regarding the Natural Sleep Initiative on their GetWell television. The data gathered
from these reports determined overall patient satisfaction with the program. Food
service workers documented and tracked the number of patients visited each night and
the number of cookies, tea, and Sweet Dream Kits that were distributed. The
institution’s Quality Management department captured patient fall data as directed by
CMS and the PA Safety Authority (Act 13) reporting requirements. EMCM collected fall
data 5 months prior to the study, from May of 2013 to September of 2013 and this data
will be used as a baseline. Fall reports were analyzed monthly over the course of the
initiative to determine if there was an overall trend of declining rates of inpatient fall
incidences. Fall rates 5 months after the start of the initiative were analyzed. These data
collection tools were used to determine if there was an increase in patient satisfaction
and a reduction in the number of inpatient falls.
The Natural Sleep Initiative is a grant-funded innovative program that was
approved by the Albert Einstein Society in February of 2013. The start up costs for this
initiative include the costs of equipment, service ware, food, Sweet Dream Kits, labor,
and the healing videos on the GetWell Network. The total non-labor/non-personnel
costs for the initiative are estimated to be $14,800 and the personnel/labor costs are
estimated to be $47,800. The Natural Sleep Initiative will not generate revenue. The
total expenses for the initiative will be $62,600 and the total grant request was $40,000.
Funding will be provided on a quarterly basis to maintain the initiative.
10

RESULTS
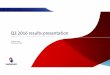
Over the course of 5 months after the initiation of the study, a total of 6,109 face-to-
face encounters were made with patients. On average, 1,222 encounters were made
each month and 41 patients were seen each night (Figure 1).
Figure 1. Monthly Face-to-Face Encounters
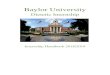
Patient satisfaction with the initiative was analyzed using patient surveys. The
data found that on average, 87% of patients offered the services of the study were
satisfied and 13% of patients were dissatisfied with the service (Figure 2). The data
displays that overall patients were satisfied with the services of the Natural Sleep
Initiative.
11
October NovemberDecember January February1000
1050
1100
1150
1200
1250
1300
1350
1400
1450
1230
11661189
1418
1106
Monthy Encounters
Face-to-Face
Month
Pat
ien
ts

Figure 2. Patient Satisfaction
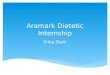
Patient falls data was collected by EMCM’s Quality Management department.
The mean of the fall rates for the 5 months prior to the start of the initiative was used as
the baseline for the study. The number of falls of patients on sleep agents was
compared to all other patient falls in the same timeframe. From May 2013 to September
2013, 55 total falls occurred in the inpatient setting. Of the 55 total falls, 15 (27%)
occurred in patients receiving sleep medications. This was the baseline fall rate used for
the study (Figure 3).
Figure 3. Patient Falls 5 Months Prior to the Study
12
27%
73%
May 2013 - September 2013
Falls in Patients on Sleep AgentsOther Falls
October November December January February0
10
20
30
40
50
60
70
86%91%
84% 85%90%
14%9%
16% 15%
10%
Were you satisfied with the Natural Sleep Initiative?
Dissatisfied PatientsSatisfied Patients
Months
Pat
ien
ts

The mean number of falls for the 5 months after initiating the study was also
analyzed to determine if there was a reduction in the number and percentage of falls of
inpatients on sleeping medications. From October 2013 to February 2014, 45 total falls
occurred. Of the 45 total falls, 9 (20%) occurred in patients receiving sleep medications
(Figure 4).
Figure 4. Patient Falls 5 Months into the Study
13
27%
73%
May 2013 - September 2013
Falls in Patients on Sleep AgentsOther Falls

On average, there were 10 fewer total falls after initiating the study and 6 fewer
falls of patients on sleep agents. This is an 18% reduction in total falls and a 40%
reduction in falls of patients on sleep agents. The data verifies that there was a
downward trend in patient falls since the initiation of the Natural Sleep Initiative.
DISCUSSION
This study examined the effectiveness of a sleep initiative on the reduction of
patient falls and improving patient satisfaction. The findings of the study indicate that the
implementation of a natural sleep initiative to promote relaxation and natural sleep
improved overall patient satisfaction and reduced the occurrence of inpatient falls. It
was anticipated that a nightly tea service would encourage healthy sleep behaviors and
sleep-conducive environmental conditions, which are the key elements of sleep hygiene
14
20%
80%
October 2013 - February 2014
Falls in Patients on Sleep AgentsOther Falls

treatment. The patient-centered approach of the initiative and its multiple constituents
improved both satisfaction and outcomes for the patients and the hospital.
The results of this study found that there was an 18% reduction in total falls and
a 40% reduction in falls of patients on sleep agents after the initiation of the study. This
data concurs with the findings of the study by Kolla et al. that sleep medications are
effective for short-term treatment of insomnia, but cognitive-behavioral treatment is
significantly more efficient for long-term treatment of insomnia in hospital patients. The
fact that there were falls at all in patients on sleep medications confirms the findings of
the study by Frey et al., which established that sleep agents cause balance and
cognitive impairments in patients upon awakening. This study solidified the notion that
the use of pharmacologic agents for promoting sleep is a risk factor for patient falls in
hospitals.
One strength of this study was the accuracy of the fall data that was collected by
EMCM’s Quality Management department, as directed by CMS and the PA Safety
Authority reporting requirements. Another strength was the large sample size of this
study; about 6,000 patients were visited over the course of the study and about 40
patients were visited each night. The magnitude of this study allowed for a greater
amount of data to be complied and analyzed. Registered nurses tracked the
administration of sleep medications using the hospital’s electronic medical records
system. This data was easily extracted from the system to accurately determine the
number of patients receiving pharmacologic sleep agents, another strength of the study.
A limitation of this study was the accuracy of record keeping by the tea service
workers. Each tea service worker was responsible for tracking the amount of tea,
15

cookies, and Sweet Dreams kits provided to patients each night of the service; human
error was likely a limitation. Another limitation of this study was the reliability of patients’
self-reporting proficiencies. Self-reported data, such as interviews, focus groups, or
questionnaires, contains several potential sources of bias and must be taken at face
external value. This study did not control variables such as a patient’s admitting
diagnosis and no historical information was provided about the patient other than their
room number, their name, and their diet order. A final limitation of this study was its
seclusion to one hospital facility. Expansion of the natural sleep initiative to other
Einstein Network facilities, or any other hospitals, may be advantageous for the
promotion of holistic sleep remedies in hospital settings.
Due to the innovativeness and currency of this research initiative, there was an
extreme lack of prior research on the specific topic. Very few studies have been
finalized that examine the effectiveness of CBT on patient relaxation and the reduction
of falls. Further research analyzing sleep medications versus natural sleep methods on
the reduction of patient falls in hospitals may be beneficial. It would also be beneficial to
provide ongoing education for healthcare professionals on the long-term benefits of a
natural sleep approach in a hospital setting.
CONCLUSION
The implementation of the natural sleep initiative at Einstein Medical Center
Montgomery produced successful results for the first five months of its operation and it
is anticipated to continue until October of 2014. Patients expressed overall satisfaction
with the service and the resulting fall counts steadily declined. The program exposed
16

patients to a new means of sleep induction and had a beneficial effect on patient
relaxation at bedtime. The findings of this research study demonstrate the crucial role
that a natural sleep approach plays in the reduction of hospital falls. With the incidence
of falls in hospitals on the rise, the incorporation of initiatives to reduce fall risk are more
pertinent than ever. Health care professionals from all fields that make up the
multidisciplinary team are key players in the safety and well being of their patients.
Through platforms for patient safety, such as the natural sleep initiative, hospitals and
healthcare facilities have the opportunity to be on the cutting edge of healthcare. The
expansion of the initiative to a multitude of hospitals and healthcare facilities across the
nation may not only help to reduce the incidence of falls, but may also reduced the
number of injuries resulting from falls, decrease patients’ lengths of stay, and improve
hospitals’ fiscal success.
17

REFERENCES
1. Gardner LAP. Pennsylvania Patient Safety Advisory. Pennsylvania Patient Safety
Authority. June 2012;Vol. 9, No. 2.
2. Sutton JC, Standen PJ, Wallace WA. Patient accidents in hospital: incidence,
documentation and significance. The British journal of clinical practice. Mar-Apr
1994;48(2):63-66.
3. Tzeng HM, Yin CY. Frequently observed risk factors for fall-related injuries and
effective preventive interventions: a multihospital survey of nurses' perceptions.
Journal of nursing care quality. Apr-Jun 2013;28(2):130-138.
4. Lohse GR, Leopold SS, Theiler S, Sayre C, Cizik A, Lee MJ. Systems-based
safety intervention: reducing falls with injury and total falls on an orthopaedic
ward. The Journal of bone and joint surgery. American volume. Jul 3
2012;94(13):1217-1222.
5. Ray WA, Thapa PB, Gideon P. Benzodiazepines and the risk of falls in nursing
home residents. Journal of the American Geriatrics Society. Jun 2000;48(6):682-
685.
6. Bloom HG, Ahmed I, Alessi CA, et al. Evidence-based recommendations for the
assessment and management of sleep disorders in older persons. Journal of the
American Geriatrics Society. May 2009;57(5):761-789.
7. Kolla BP, Lovely JK, Mansukhani MP, Morgenthaler TI. Zolpidem is
independently associated with increased risk of inpatient falls. Journal of hospital
medicine : an official publication of the Society of Hospital Medicine. Jan
2013;8(1):1-6.
18

8. Roehrs T, Roth T. Insomnia pharmacotherapy. Neurotherapeutics : the journal of
the American Society for Experimental NeuroTherapeutics. Oct 2012;9(4):728-
738.
9. Dikeos DG, Soldatos CR. The condition of insomnia: etiopathogenetic
considerations and their impact on treatment practices. Int Rev Psychiatry. Aug
2005;17(4):255-262.
10. Walsh JK, Schweitzer PK. Ten-year trends in the pharmacological treatment of
insomnia. Sleep. May 1 1999;22(3):371-375.
11. Wang PS, Bohn RL, Glynn RJ, Mogun H, Avorn J. Zolpidem use and hip
fractures in older people. Journal of the American Geriatrics Society. Dec
2001;49(12):1685-1690.
12. Frey DJ, Ortega JD, Wiseman C, Farley CT, Wright KP, Jr. Influence of zolpidem
and sleep inertia on balance and cognition during nighttime awakening: a
randomized placebo-controlled trial. Journal of the American Geriatrics Society.
Jan 2011;59(1):73-81.
13. Zammit G, Wang-Weigand S, Peng X. Use of computerized dynamic
posturography to assess balance in older adults after nighttime awakenings
using zolpidem as a reference. BMC geriatrics. 2008;8:15.
14. Shuto H, Imakyure O, Matsumoto J, et al. Medication use as a risk factor for
inpatient falls in an acute care hospital: a case-crossover study. British journal of
clinical pharmacology. May 2010;69(5):535-542.
19

15. Edinger JD, Carney CE, Wohlgemuth WK. Pretherapy cognitive dispositions and
treatment outcome in cognitive behavior therapy for insomnia. Behavior therapy.
Dec 2008;39(4):406-416.
16. Riemann D, Perlis ML. The treatments of chronic insomnia: a review of
benzodiazepine receptor agonists and psychological and behavioral therapies.
Sleep medicine reviews. Jun 2009;13(3):205-214.
20