Embed Size (px)
Citation preview

Submission to the Minster for Health and Children
Public Consultation on Proposed Health Information Bill
The Minister is proposing new legislation on the collection, use, sharing, storage, disclosure and transfer of personal health information as well as ensuring that the privacy of such information is appropriately respected
SUBMISSION BY GS1 [Global Standards 1(Ireland)) Limited]
(formerly EAN Ireland)
INTRODUCTION TO GS1
GS1 is a not for profit and neutral worldwide body comprising 109 Member Organisations (MO), dedicated to improving efficiency in the supply chain across the world by the adoption of Global Standards1 for commerce. More than 5 billion daily transactions (bar code scans/electronic messages) are carried out by 1.3 million companies in over 150 countries using the GS1Standards.
Globally, GS1 has been at the forefront in supporting the development of efficient and cost effective solutions for traceability for both food distribution and healthcare. Many Healthcare Authorities, Healthcare Regulators, Healthcare Providers and companies providing supplies and services to the Healthcare Sector around the world have already adopted the GS1 Standards for identification purposes – patients, staff, products and services– both in medical device and pharmaceutical sectors. (c.f. Appendix 1 for more details.)
GS1 Ireland (the local GS1 MO office) was established in 1980 and has around 3,000 members in the Fast Moving Consumer Goods, Healthcare and other sectors. Our Board is representative of leading local and international companies including a wide cross-section of healthcare stakeholders who use GS1 Standards in their supply chains and for other mission critical operations.
1 GS1 Global Standards are developed in collaboration with the International Standards Organisation ISO and United Nations Economic Commission for Europe UNECE. All GS1 published standards reference approved ISO Standards and CEFACT.
GS1 Response:
GS1 Ireland welcomes the proposed Health Information Bill.
(a) We support the proposal to have unique identifiers for patients and health care providers which, when implemented along with an electronic health record and other technologies, will make a huge contribution in terms of the accuracy and security of diagnosis, treatment selection and the care delivery process. The result will be a vast improvement in the quality, efficiency and safety of individual treatment episodes coupled with considerable extra clinical benefits including the ability to automatically capture data for patient records and comparative analysis on patient outcomes versus treatment choices.
(b) The discussion document reflects careful consideration of key issues to be addressed if the transformational changes required are to be supported by patients and the other stakeholders involved. If digital records are to be shared between the various professional providers in the course of a patient’s treatment journey, then the privacy and security of these records must be fully secured.
In summary, GS1 believes that the adoption of GS1 Standards can assist in the realisation of the main objectives of the Health Information Bill, which are: -
to establish a legislative framework to enable information –in whatever form- to be used to best effect to enhance medical care and patient safety throughout the health system;
to facilitate the greater use of information technologies for better delivery of patient services; and
to underpin an effective information governance structure for the health system generally

How can GS1 Standards help?
GS1 has over 30 years experience and knowledge of managing unique number banks and establishing the most widely used global standards by supply chain stakeholders in some 24 sectors including healthcare.
The GS1 Standards (see Appendix 2) today provide for:-
(a) Unique numbers for the identification of the following: - Patients and their individual treatment episodes; Healthcare providers (clinicians, nurses, pharmacists etc.); Products (medicines, medical implants, surgical instruments); and Services (medical procedures, lab tests etc.);
(b) Bar code and RFID standards for automatic identification and capture of patient, provider, product and other data (e.g. batch information and expiry data) using scanning technologies;
(c) Standards for secure exchange of information stored in distributed databases between trusted parties based on their particular rights of access - (EPCglobal Network);
(d) Secure e-Messaging standards for the communication of supply chain commercial and critical information;
(e) Using the Global Data Synchronisation Network GDSN, the exchange of product information for a wide variety of database applications i.e., supply chain, classification and clinical purposes;
Traceability standards have been developed in order to provide a basis for validating the effectiveness of solutions in the food and healthcare environment. Effective traceability reduces risk through certainty of identification of people, products, services and places and ensures tracking and tracing processes are operated in a timely manner.

Examples of Healthcare Solutions using GS1 Unique Numbers and Standards
(1) National Centre for Hereditary Coagulation Disorders (NCHCD)
The solution, approved and funded by the Department of Health and Children, was developed in response to the Lindsay Tribunal on the harm caused to Irish haemophilia patients due to the well documented failure to track and trace infected blood products.
This solution is a perfect example of the successful introduction of the GS1 Standards. Unique identifiers for patients, providers and products coupled with bar coding and an electronic patient record give real time visibility of all patient treatment episodes. The results have been dramatic in terms of patient safety, secure data exchange and patient satisfaction (100% per surveys). Each patient is uniquely identified by a GSRN (Global Service Relationship Number). Bar code scanning is used extensively to capture the unique identifiers and critical other data in real time. Manual recording and retention of paper records are no longer required, except for home treatment purposes. For the patient’s home or work, the use of mobile technology for the automatic data capture of treatment episodes has been fully tested. Homecare treatment accounts for more than 60% of the medication used for this patient group
The system provides for 100% product recall thanks to the GS1 unique identifier and serialisation of each patient pack within the barcode and the visibility of each storage location identified by a GS1 unique identifier. There has also been a marked improvement in the efficiency of clinical management procedures since the solution was rolled out.
The Haemophilia Electronic Patient Record also meets the aims of a national population health registry:
100% capture of cases (100% ascertainment) Prevents case duplication Can provide real time visibility of patient status including clinical data from home
treatment episodes.
For more details see Appendix 3

(2) “Bar Coding for Success” – The Department of Health in the UK
In February 2007, the Department of Health issued their policy document “Bar Coding for Success” which promoted the strategy to adopt the GS1 standards as the information standard for the NHS in England. The policy is being rolled out now with NHS Connecting for Health working closely with GS1 UK to assist NHS hospital Trusts implement the standards. 125 hospitals in England have already signed up for the standards.
The NHS in England is also introducing the GSRN for unique patient ID as part of its Connecting for Health Initiative.
GSRN Example - Newborn Screening Programme
Background: The newborn screening programme routinely offers blood spot teats, “heel prick test”, for all babies within the first few days of birth. The filter paper is sent to a laboratory for testing within to identify illnesses or conditions that would benefit from early treatment. One problem has been tracing babies through the system to ensure that they have been tested. Until recently this has only been possible by using names and other personal identifiers because the NHS number was typically not available at the age when screening was carried out (6-14 days). Since the introduction of the NHS Numbers For Babies in October 2002 it is possible to for tracing to be based on the NHS number because babies are now given their unique identifier after birth.
The Objective: is to make sure that the screening laboratory receives the blood spot filter paper test card with the NHS Number represented as a barcode as well as in a human readable format, it also contains basic birth and demographic details on a label.Specifically, the aim is to enable all maternity units to provide the mother with the NHS number before discharge from the maternity unit.
The labels provide enormous benefits , midwives do not have to handwrite all the basic birth and demographic details, thus saving time and reducing errors on both the writing and reading stages.

The use of bar-coded labels enables the NHS numbers to be used as a unique identifier within the screening process and also to track babies throughout the system. Being able to correctly identify and track the progress of babies is fundamental to reducing the risk of babies going untested or not being tested in a timely fashion. The NHS number is contained within the GS1 Standard GSRN., The GS1 data standards and bar code symbol were adopted by the NHS to optimize the solution.
For more details see Appendix 4

GS1 Ireland’s Proposal
Unique Healthcare Identifier
Having regard to the requirements described in Appendix 2 of the Health Information discussion paper, GS1 Ireland proposes that
1. The GSRN (Global Service Relationship Number) be adopted as the unique patient identifier for the entire healthcare service
2. All healthcare professionals should be identified by a GLN (Global Location Number).
The reasons for using the GSRN as the unique patient identifier are: -
Global Uniqueness
Numbers assigned using the GS1 Standards and structures are globally unique by virtue of how the GS1 Standards are deployed in over 150 countries world wide. There is no possibility of the same number being allocated to a different patient.
Non significant
The number itself is non-significant and contains no data about the patient. It is merely used as a unique index or key access data on a database for example an Electronic Health Record. Access to the data is restricted by secure healthcare practices for IT solutions.
Sharing Information
As the number is globally unique there is the possibility of sharing patient data between different applications at different sites without disclosing the patient’s identification. It can facilitate the sharing of data between Public and Private Healthcare Institutions without using the patient’s PPS number.
It would provide an appropriate solution for patients who don’t have PPS numbers, for example tourists.

Given the fact that every European citizen has the right to treatment in the country of their choice the GSRN would ensure uniqueness of identification not only locally but on a Community wide basis.
As with the NHS, the GS1 GSRN could be adopted as an EU wide identifier, given that each Member State has a GS1 office capable of providing support to their respective healthcare authorities.
Registry for Unique Patient and Provider Identification
GS1 would be happy to assist with the software solution for a registry of patient and provider identification which would be managed and controlled by a Body within the Healthcare System. The registry could be used to assign numbers to new born babies as well as all other citizens for the accurate identification of their treatment throughout the entire healthcare service.
Unique Identification of Healthcare Professionals
The recent report of the Commission on Patient Safety and Quality Assurance calls for a Group to collaborate on the scope, design and implementation of a credentialing system on a universal basis R6.20,
The assignment of a unique identifier (GLN) to each provider of healthcare services (doctor, nurse, pharmacist etc.) would provide certainty of identification for such a system.
Furthermore, R6.21 suggests that the Group should pro-actively participate in an EU-wide credentialing system, GS1 in Europe can provide the necessary globally unique numbering system for this purpose.
As previously stated GS1 Ireland proposes the adoption of the GLN for the purposes of accurate tracking and tracing of all healthcare professionals, the availability of a unique provider identification would assist in the management of an accurate credentialing system.

Appendix 1
GS1 Global Adoption
Healthcare
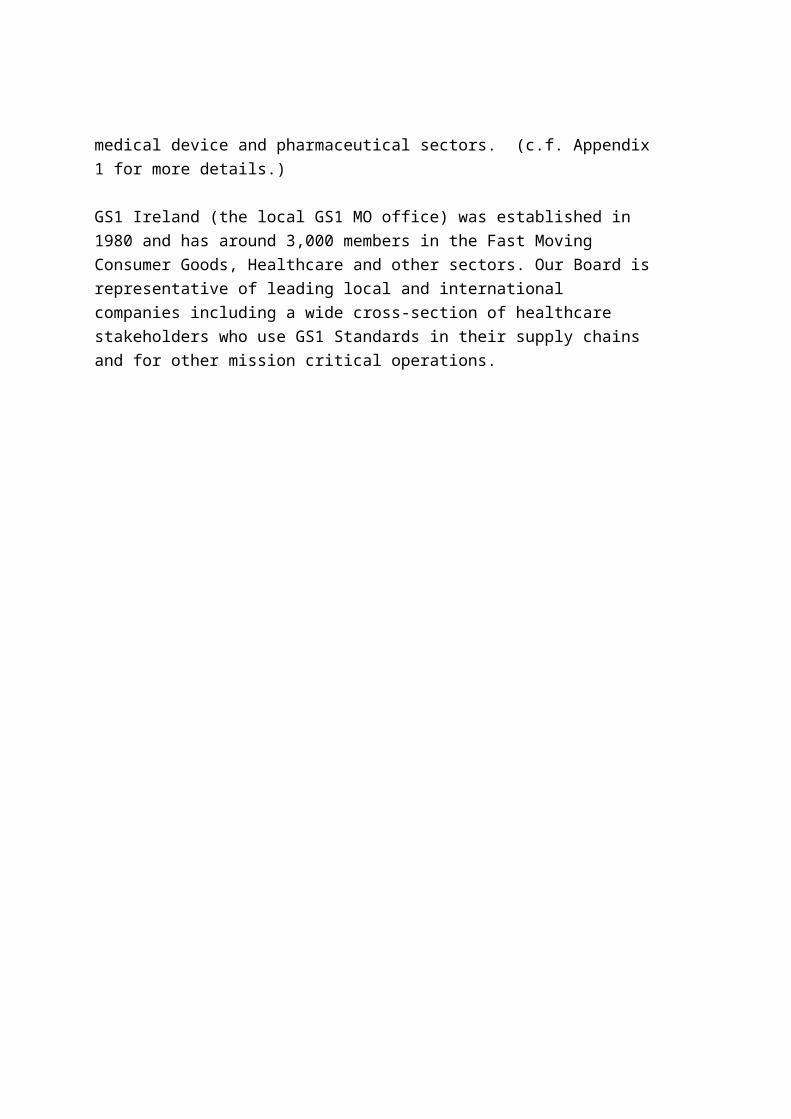
Regulations and policies by national and regional authorities

Region Scope Authority Citation Date Summary of Requirement
USA Pharmaceuticals US Food and Drug Administration
21CFR Parts 201, 606, 610
2/4/2004Requires a linear bar code on most prescription drugs and certain over-the-counter drugs commonly used in hospitals and dispensed under order. NDC must be coded in GS1 or HIBCC.
Although not stated as a requirement, FDA has indicated a recommendation for RFID.
Brazil Pharmaceuticals ANVISA (National
Health Surveillance Agency)
Resolution 802 10/8/1998Ministry of Health requires all medicines to have GS1-13 on their packages, and the GTIN must be informed in the application form for registering the medicine.
Brazil Pharmaceuticals ANVISA (National Health Surveillance Agency)
Resolution 32011/22/2002Lot number and expiry date of each pharmaceutical product delivered to the retailers must be informed in the invoice
Chile Pharmaceuticals Public System and the
Healthcare Minister Working on a pilot program to build a
proof of concept and benefits of the use of bar codes.
México Pharmaceuticals Instituto Mexico del
Seguro Social (IMSS)CANIFARMA
March, 1994
Requires a linear bar code (for all pharmaceuticals and medical devices) that dispatch and/or sale products to the IMSS and the CANMIFARMA.
México Medical Devices Instituto Mexico del Seguro Social (IMSS)CANIFARMA
March, 1994
Requires a linear bar code (for all pharmaceuticals and medical devices) that dispatch and/or sale products to the IMSS and the CANMIFARMA.
Belgium Pharmaceuticals Royal Decree Bar code, sequential code per sales unit,
only reimbursed pharmac. products
Croatia Pharmaceuticals
Ministry of Health
Regulation for GS1 coding on pharmaceutical products, however there is no reg
All pharmaceutical companies in Croatia barcode their products using GS1-13.

Region Scope Authority Citation Date Summary of Requirement
Former Republic of Macedonia
Pharmaceuticals Pursuant to the Article 48 of the Law on medicines, auxiliary medicinal remedies and medical accessories (" Official Gazette of the Republic of Macedonia", No.21 May 8th, 1998), all the pharmaceutical and medical products in the Republic of Macedonia must have the bar code GS1 13. All the pharmaceutical producers are members of GS1 Macedonia and they obligatory use the EAN-13 bar code.
Former Republic of Macedonia
Medical Devices
(See Pharmaceuticals) France Pharmaceuticals A decision has been taken in 2004 to
move to a GS1 13 system as of June 2006. Additionally CIP (association of wholesalers, industry and pharmacists) has recommended adopting an GS1 128 system.
Greece Pharmaceuticals National
Pharmaceuticals Organization
Doc. 1202/B amendment to A6A-18/26
8/4/04Requires a GS1-13 bar code (bearing the NPO registration number) on all pharmaceuticals in the Greek market (OTCs excluded).
Russia Pharmaceuticals
UNISCAN/EAN Russia and the Russian Health Ministry have a cooperation agreement on joint implementation of mandatory bar coding of pharmaceuticals with EAN/UCC GTINs.
The Russian Health Ministry uses a unified numbering system for pharmaceuticals and medical products. All medical products and pharmaceuticals imported or sold in Russia, independently of their origin, must have GTIN. Importers must present a document from their respective GS1 Member Organisation confirming the allocation of an GTIN. 100% of pharmaceutical products are coded with GS1 system.

Region Scope Authority Citation Date Summary of Requirement
Russia Medical Devices
Yes - UNISCAN/EAN Russia and the Russian Health Ministry have a cooperation agreement on joint implementation of mandatory bar coding of pharmaceuticals with EAN/UCC GTINs.
The Russian Health Ministry uses a unified numbering system for pharmaceuticals and medical products. All medical products and pharmaceuticals imported or sold in Russia, independently of their origin, must have GTIN. Importers must present a document from their respective GS1 Member Organisation confirming the allocation of an GTIN code. 100% of pharmaceutical products are coded with the GS1 system.
Poland Pharmaceuticals Ministry of Health
GS1 Poland assigned the Ministry of Health several 4-digit company prefixes, allowing the Ministry to allocate GTINs
Slovakia Pharmaceuticals
Law requires GS1 barcodes
Pharmaceutical products are numbered according to the GS1 structure
Spain Pharmaceuticals GS1 128 per October 2005. Currently
GS1- 13 system is used.
Spain Pharmaceuticals Ministry of Health Agreement with Farmaindustria and GS1 Spain
February the 29th. Of 1998
The GS1-13 become mandatory for almost all pharmaceuticals
Spain Medical Devices Ministry of Health RD 9/96 of January the 15th.
January the 15th. of 1996
To the above specifications products like "bandages, sticking plasters, splints, cotton, etc." were included on that date.
Spain Pharmaceuticals Ministry of Health A new amendment of the Real Decreto 725/2003 of June the 13th. on which some issues from the article 100 of the law 25/1990 of December the 20th. have been developed, is going to come out soon.
Working on it now.
Working with the Ministry of Health to develop the Real Decreto 725/2003 in order to make mandatory the use of GS1-128 in case and pallet.

Region Scope Authority Citation Date Summary of Requirement
Sweden Medical Devices Report Prepared by a
WG inside HSS, the official Swedish Standardization body for the Healthcare Industry
Recommend all articles bar coded by 6/14/1988
All articles shall be given an article identity according to GS1 standard. Bar-coded as GS1-13 for only product ID and GS1-128 if S/N, Lot No. or additional information is needed. A number of other regulations released after this document - none of them contradict this document.
Switzerland
Pharmaceuticals Swissmedic Loi sur les produits thérapeutiques
12/15/2000. Bar codes (including the registration number) are encouraged. 99% of the retail packs show a GS1-13. Narcotics have to be identified with GS1-13.
UK Pharmaceuticals and
Medical DevicesDepartment of Health Policy
statement16/02/07 Bar coding recommendation (GS1) for
all products in the pharma and medical device supply chain
Ukraine Pharmaceuticals GS1-13 required through law of Minister of Health and Trade
For all products in the pharmaceutical supply chain GS1-13 must be used.
Yugoslavia
Pharmaceuticals By Federal Law from 1993, each medicine must have an GS1
By Federal Law from 1993, each medicine must have a GS1 barcode.
Iran Pharmaceuticals All pharmaceutical products must be bar coded with GS1-13. At the current time, there are 51 pharmaceutical manufacturers using GS1-13 on their products.
South Africa
Pharmaceuticals Department of Health Department of Health requires GS1 bar code on all pharmaceutical items purchased by them through their tender process
Hong Kong
Pharmaceuticals Government Supplies Dept. of HK
GS1 - 128 with data content GTIN / batch no / expiry date, each sales unit must carry the bar code
Region Scope Authority Citation Date Summary of Requirement
Hong Kong
Medical Devices Government Supplies Dept. of HK
GS1-128 with data content GTIN / batch no / expiry date, each sales unit must carry the bar code
Japan Pharmaceuticals Ministry of Health and
Welfare GS1-128, all packaging levels, sterile
products = GTIN / batch no / expiry date, non-sterile = GTIN
Japan Medical Devices Ministry of Health and Welfare
GS1-128, all packaging levels, sterile products = GTIN / batch no / expiry date, non-sterile = GTIN
Korea
Pharmaceuticals In the healthcare sector, GS1 Korea has taken part in the implementation of EHCR in cooperation with Ministry of Health and Welfare. Government officially adopted GTINs for the identification of all pharmaceuticals distributed in Korea.
Most pharmaceutical companies have an GS1 manufacturer number. GS1 numbers are used in the health sector. The number 6 following the GS1 prefix 880 is reserved for Pharmaceutical industry. Pharmaceuticals have been bar-coded with EAN/UPC Symbology since July 2000
Taiwan
Pharmaceuticals
The Taiwan healthcare sector adopts GS1 standards
As a criterion in the forms of packaging: GS1-13/GS1-14. Selecting bar-code symbols according to operations demands: GS1-13/GS1-14/GS1-128. Over 13000 Medicines with GTINs have been registered in the e-Catalogue of GS1 Taiwan.
Thailand
Pharmaceuticals
Pharmaceutical products are mandated to be identified and bar-coded with the GS1-13 system.

Appendix 2
An Introduction to the GS1 Standards

In this section you will be introduced to the GS1 System: standards for identification, data carriers, electronic messages, data synchronisation and RFID.
Why Numbers?
The GS1 “system” relies on the use of numbers to securely identify products, people and places. Before going any further into how to use numbers for identification purposes, it is important to answer the question; “Why use numbers?” People differ in how they identify products so an alternative method of identification is needed - numbers. There are several reasons why numbers (particularly GS1 number banks) make better identifiers than names, including: Numbers are easily processed by computers. Numbers are not language dependant. Regardless of the language or script used numbers
are recognised all over the world making them a globally recognised language. GS1 numbers are unique to each product, person or place, i.e. a number that is assigned to
a product will identify it anywhere in the world. GS1 numbers eliminate misunderstandings surrounding product descriptions. GS1 numbers are secure, i.e. there is no other information contained in the number other
than the number itself.
Areas of Application for the GS1 System
The GS1 System is open to use by anyone who wishes to trade and communicate in a globally acceptable and understandable way. It is currently used by over 25 different industry sectors around the globe including, grocery and general merchandise retail, clothing & textiles, transport and logistics, healthcare, food traceability and defence. The GS1 System contains a powerful set of standard tools to enable a wide variety of applications in an open standards environment.

The GS1 System
The GS1 System is the complete set of global standards that include keys for the identification of objects, standards for data carriers (bar codes, RFID tags) and standards for exchanging electronic messages (e-Com).
The GS1 Standards are an integrated solution that facilitates trade by combining the unique identification keys with data carriers and electronic commerce processes resulting in efficient, accurate and timely business communications.
The application of GS1 Standards can result in significant improvements in logistics operations, a reduction in paperwork costs, shorter order and delivery lead times, increased invoice accuracy and better management of the whole supply chain. Enormous cost savings are realised daily by user companies who have adopted the GS1 Standards because they apply the same solution for communicating with all their trading partners.

The Components of the GS1 System
The GS1 System consists of the following distinct components:
GS1 Bar Codes comprising of:GS1 Identifiers Data Carriers
GS1 eCom: EANCOM XML Electronic MessagesAS1/AS2 Protocols
GS1 GPC: Global Product Classification
GS1 GDSN: Data Pooling and Synchronisation
GS1 EPCglobal: Electronic Product Codes and the EPC Network

GS1 Bar codes
GS1 Bar codes are made up of two distinct sub-components:
GS1 Identifiers Data carriers.
The GS1 Identifiers
The GS1 System relies on globally unique identifiers or keys. These identifiers enable the unique identification of products, services, assets, documents, locations and transactions.
The unique identifiers (or keys) are used for accessing information about an item (a product, service or any physical or non-physical item) on a computer database.
The structure of the GS1 System ensures that the identifiers are globally unique, contain no significance or meaning, are secure and are globally understood. The identifiers can be allocated to consumer or retail items, traded goods, logistics units, locations and many others items such as assets, services and documents.
The following GS1 identifiers are commonly used in retail and supply chain applications:
The Global Trade Item Number (GTIN) The Serial Shipping Container Code (SSCC) The Global Location Number (GLN)
In addition to the above, the GS1 identifiers below may be used by any company that adopts the GS1 Schema for more advanced applications.
The Global Individual Asset Identifier (GIAI) The Global Returnable Asset Identifier (GRAI) The Global Service Relationship Number (GSRN) The Global Document Type Identifier (GDTI) The Electronic Product Code (EPC)
These identifiers are beyond the scope of this guideline. Please contact GS1 for further information.
The Global Trade Item Number (GTIN)

The GTIN is a number used to uniquely identify trade items worldwide.
Note: A trade item is any item (product or service) upon which there is a need to retrieve pre-defined information and that may be priced, ordered or invoiced for trade between participants at any point in any supply chain.
The GTIN is most commonly used to identify consumer products and outer cases containing consumer products. The use of the GTIN enables the following:
retail point-of-sale scanning electronic ordering goods inwards goods inwards management and control sales analysis data alignment and a wide range of other business applications.
The Serial Shipping Container Code (SSCC)
The SSCC is a number used for the unique identification of logistic units such as cases, pallets and containers.
Note: A Logistic Unit is an item of any composition established for transport and/or storage which needs to be managed throughout the supply chain.
The SSCC is typically used: -
to facilitate logistical track and trace applications to improve supply chain efficiency through faster handling at goods inwards in warehouse management systems
The Global Location Number (GLN)
The Global Location Number (GLN) is a number used to identify individual organisational entities.
GLN’s are used as unique reference numbers for:-
e-Commerce to identify the sender and receiver of an electronic message Data alignment to identify the data suppliers and receivers To identify logistics organisations responsible for shipping, delivery and warehouse
management
By following the principles of the GS1 Identifiers, users can design applications to process data automatically with the guarantee that the identifiers used are globally unique and will not conflict. The most obvious example of this is scanning at the point of sale where a single GS1

Identifier in a bar code can be scanned in any country worldwide and will not conflict with any other item.
GS1 Data Carriers
The GS1 identification numbers (and other standard data) can be translated into a machine-readable form, better known as a bar code. Physically the GS1 identifier assigned to an object can travel with that object forming a link between the physical flow of goods and the associated information flow. A scanner is used to read the identification number and transmit it to a computer.
There are different types of data carriers (or bar code symbols) and their use depends upon a number of factors including:
• the environment in which the code will be scanned • the item to be identified and bar coded For point of sale applications, the following GS1 BarCodes may be used: -
• EAN-13• EAN-8 for very small items• UPC-A• UPC-E for very small items
The symbols can be read omni-directionally.
Note: : Please note that a new type of symbol GS1 DataBar will be added to the above list after 2010.

For Trade Items and Logistics Units not intended for the point of sale. The following GS1 BarCodes may be used: -
EAN-13 UPC-A ITF-14 GS1-128
GS1 eCOM, Standard Electronic Messages
The GS1 identification numbers are also used in e-Commerce (i.e. electronic data interchange (EDI) messages) to improve the speed and accuracy of data communicated between trading partners. GS1 has two suites of standards for electronic messages EANCOM and GS1 XML. In addition, a secure protocol has been prepared for Internet based communications called GS1 AS1/AS2.
The most commonly used e-COM standard in Ireland is Harmonised EDI, H-EDI which is based on EANCOM and includes the specific business and legal requirements agreed by Irish users. The H-EDI Guidelines are available for download from the GS1 Ireland website or may be ordered from GS1 Ireland Membership Services.
GS1 Global Product Classification
Global Product Classification (GPC) is an internationally agreed standard for product classification and is a key enabler for the Global Data Synchronisation Network (GDSN) and category management.
Note: The GPC Schema is aligned with the United Nations Standard Product and Services Classification (UNSPSC).

GS1 GDSN, Standards for Data Synchronisation and the GS1 Ireland Data Pool Service
The next component of the GS1 System is a suite of standards developed to facilitate the exchange of product and company information via a network of linked data pools across the globe called the Global Data Synchronisation Service (GDSN). The GS1 Ireland Data Pool Service, linked with the GDSN, will enable Irish companies to publish and to receive product information.
EPCglobal, Standards for Radio Frequency Identification (RFID) applications
The fourth component of the GS1 System is a set of standards for RFID applications packaged under the brand name EPCglobal. EPC stands for Electronic Product Code which is a unique identification key stored in an RFID tag which can then be applied to products to identify them and monitor their location and movement throughout the supply chain. In very simple terms, EPC acts like an electronic bar code. The EPC Code combined with the EPCIS (EPC Information Service) will enable real-time supply chain visibility and more effective track and trace.

Appendix 3
GS1 Ireland and the NCHCD

Overview
The accurate tracing of factor concentrate is a critical component in the safe delivery of haemophilia care as it supports rapid recall and identification of patients who receive “at risk products”. Prior to the project a combination of manual and electronic methods were used to trace factor concentrate. The project proposed to introduce a GS1 based data carrier system (bar code or radio frequency identification tags (RFID)) to support the complete electronic tracing of each vial of factor concentrate imported into the Republic of Ireland from point of entry to end user in both the hospital and home environment. The data carrier would be applied at point of importation into the country. The project would initially utilize the traditional barcode however once complete electronic tracing had been achieved the aim was to proceed to a detailed assessment of RFID tags. The data carrier (bar code and RFID tag) would contain all critical information needed to support the proposal. This information included, but was not limited to patient identification, product identification, logistics identification, batch number, unique vial number, kit serial number, and expiry dates.
Project Objectives
The key objectives of the proposed system were as follows:
Real time identification of the location of all CFC to facilitate rapid, accurate and validated product recall;
Real time identification of patients treatment history to allow rapid and accurate identification of all patients who have received an "at risk" product;
The capture of data to validate cold chain storage and delivery of factor concentrates; The provision of a system to ensure that the correct product is prescribed and
administered to the patient (electronic prescription and administration); The provision of a real-time stock management system which would allow: -
correct dispatch and delivery direct to the patient, hospital and ward; optimal stock management with specified re-order levels and stock rotation to
minimise wastage due to expiry dates limitations; real time stock consumption data with comparison of actual, budgeted and year to date
variance presented in stock and cost terms. Analysis of patient treatment data to ensure appropriate usage and to flag clinically
significant bleeding that requires hospital rather than home treatment. Decision support system to analyse the impact on stocks, the cost of prescribing
actions and future budget requirements. Invoicing system to support the receipt of invoice from the CFC supplier and
generation of invoices to customers/hospitals for CFC products Back-up processes and procedures, both manual and infrastructure, to manage
Information Technology risk.

Organisation
The project was overseen by an internal group including representatives from the National Centre for Hereditary Coagulation disorders, GS1 Ireland and the Irish Haemophilia Society.
External review, comments and suggestions were provided by the Global consultation group operating under the leadership of the WFH. This group included representatives from regulatory authorities (FDA,EMEA), clinicians, consumers (WFH,IPOPI), governmental agencies (DG, SANCO, HHS ), industry (PPTA) and the not for profit manufacturing sector (EFPIA). External review was an important component in optimising the application of the project in Ireland and in defining the potential application of this project and methodology in other countries.
What did GS1 Standards offer?
GS1 Global Standards for barcodes/RFID technology provided the ability to:
Identify patients, clinicians, locations and medications with unique barcodes Provide real-time ID and 100% track and trace of all medication (CFC) using Global
(GS1) standards Provide a stock management system incorporating Correct dispatch and delivery Optimal stock management with stock rotation to avoid wastage due to expiry dates Real time stock consumption data with comparison of actual, budget and year to year
variances
National Haemophilia Electronic Patient Record (EPR)
An Electronic Patient Record for patients with Haemophilia and related bleeding illnesses was established through the modification of a Cancer EPR system. The project team worked in partnership with the supplier to add disease specific information to the database. The EPR system enabled:
The migration of critical data from existing database. Interface to existing PAS/LIS systems Full Appointment Scheduling module for clinicians and patients Electronic Chart with up to date information Accessibility in any Haemophilia treatment centre throughout Ireland

Logistics
60% of Irish Haemophilia patients are treated in their own homes. Therefore it was critical that a secure, validated cold chain delivery system was put in place to manage home deliveries. The selected company had to:
Ensure quality of product using validated scheduled cold chain delivery (Home/Pharmacy/School)
Be licensed by the IMB Take charge of Home Fridge management (Temperature monitoring) Implement Bar code scanning
Current Status
The NCHCD project was launched by the Minister for Health in 2004. The following was the roll-out process:
The validated Cold Chain delivery system started in August 2004 Bar Coding of CFC’s began in August 2005 allowing for real-time track and trace
based on Bar codes Phase 1 of the EPR has been installed and went live in June 2005 to allow for move to
EPR The “in hospital solution” for stock movement and issuing CFC to the patient went
live in March ‘06 “In home solution” has been fully tested with successful trials on hand held PDAs for
use by patients Validation process is ongoing in Hospital, EPR/Cold Chain IT provider
Costs & Savings
It is estimated that the project cost in the region of €1 million. In the first year of operation, inventory was reduced by in excess of €1 million, product wastage reduced from €90,216 to zero in the year post service implementation, and Documentation errors were reduced from 12 to zero in the year post service implementation. Annual savings are now running in excess of €1 million from its operation.
As well as the monetary savings, patient satisfaction with the convenience of the new system was 100%, patient satisfaction with regard to privacy and confidentiality was rated at 99%, and patient’s overall satisfaction with the service was 99%.

Appendix 4
NHS Numbers For Newborn Screening

NHS Numbers for Newborn Screening
Output Based Specification for the Blood Spot Card Label

Version No: 1.0 FinalIssue Date: 13th July 2005

Purpose of this documentThe purpose of this document is to provide the output based specification for the production of ‘standard sticky labels’ so as to enable all maternity units to print such labels with the NHS number which will be given to the mother, usually before discharge from the maternity unit. This will allow the sticky label to be available in the home environment for use by community midwives (for example) to identify blood spot cards.
VERSION HISTORY
Version Date Issued Brief Summary of Change Owner’s Name0.1 First Draft Version for comment Glen Woodward0.2 Second Draft Version after review comments
received from NHS Numbers For Newborn Screening Project Board
Glen Woodward
0.3 Third Draft Version after review comments received from Kate Hall and David Isherwood
Glen Woodward
1.0 Final 13th July 2005 Updated to reflect sign-off by the UK Newborn Screening Programme Centre
Glen Woodward
For more information on the status of this document, please see the covering letter or contact:
Glen WoodwardNHS Connecting for HealthHexagon HousePynes HillRydon LaneExeterEX2 5SE
Tel: 01392 206915E-mail: [email protected]
Date of Issue 13th July 2005Reference NPFIT-FNT-TO-DPM-0405.01© Crown Copyright 2005

CONTENTS
1. INTRODUCTION...............................................................................................................51.1 SCOPE....................................................................................................................................................51.2 REFERENCES.........................................................................................................................................5
2. STRATEGIC CONTEXT...................................................................................................62.1 BACKGROUND........................................................................................................................................62.2 OBJECTIVES...........................................................................................................................................8
3. LABEL CONTENT AND FORMAT................................................................................103.1 CONTENT OVERVIEW..........................................................................................................................103.2 FORMAT OVERVIEW.............................................................................................................................22
4. BAR-CODE CONTENT AND FORMAT.........................................................................244.1 OVERVIEW............................................................................................................................................24
5. SYSTEM REQUIREMENTS...........................................................................................255.1 SYSTEM HANDLING OF THE BAR-CODE...............................................................................................255.2 DIMENSIONS.........................................................................................................................................255.3 SYMBOLOGY.........................................................................................................................................25
6. PRINTING REQUIREMENTS.........................................................................................266.1 CODE SETS..........................................................................................................................................266.2 LABEL PAGE FORMATS........................................................................................................................26
7. BAR-CODE VERIFICATION..........................................................................................277.1 VERIFICATION OVERVIEW....................................................................................................................277.2 VERIFICATION PROCESS......................................................................................................................287.3 TESTING PROCESS - MATERNITY SYSTEM SUPPLIERS.....................................................................297.4 TESTING PROCESS - SCREENING LABORATORY SYSTEM SUPPLIERS.............................................30
APPENDIX A - BLOOD SPOT LABEL SIGN-OFF FORM (P1)............................................31APPENDIX A - BLOOD SPOT LABEL SIGN-OFF FORM (P2)............................................32Appendix A - Blood spot label sign-off form (p3)....................................................................34

1. Introduction
Scope
This is the Output Based Specification (OBS) for the production of ‘standard sticky labels’ so as to enable all maternity units to print such labels with the NHS number both in numeric ‘3-3-4’ format and as a bar-code.
To ensure that the specification can be adequately followed, section 1.2 details the relevant documents that are required.
This OBS will be read by a number of differing system supplier communities (including Maternity System and Screening Laboratory System Suppliers) as well as being used by the UK Newborn Screening Programme Centre as the technical reference for the NHS Numbers For Newborn Screening Project.
It is strongly recommended that ALL System Suppliers read and comply with ALL sections of the specification, as detail regarding the label design is important to all supplier communities.
This document will also be the basis for more detailed guidance from the UK Newborn Screening Programme Centre regarding the implementation and training requirements of the Health Care Professionals, such as :
the midwifery community
laboratory staff
nurse specialists
Relating to the above point. this document does NOT detail such guidance on implementation, roll-out and training requirements.
References
Reference Title Version Date1 NN4B Birth Notification Data Set Version 4.0 10.08.20012 NN4B Maternity System Specification Version 4.0 01.08.20013 NN4B Message Specifications -
Maternity – CISVersion 4.0 01.08.2001
4 NHS Data Dictionary Version 2.0.0 May: 20045 General EAN.UCC Specification V5.0 Version 5.0 2004

2. Strategic Context
Background
The newborn screening programme routinely offers blood spot tests for phenylketonuria, and congenital hypothyroidism, and is expanding to include screening for sickle cell disorders and cystic fibrosis for all babies within the first few days of birth.
The blood spot screening test is often called the ‘heel prick test’ and is performed by pricking the heel of the baby’s foot and dropping the blood obtained onto a special filter paper card where it is dried as several blood spots.
These blood spots are sent to a newborn screening laboratory where they undergo a number of tests with the aim of picking up babies with illnesses or conditions that would benefit from early treatment.
One problem for this programme has been tracing babies through the system to make sure they have been tested. Until now, this has only been possible by using names and other personal identifiers because the NHS number was typically not available at the age when screening was carried out (6-14 days).
However, the introduction of NHS Numbers For Babies in October 2002 has made it possible for tracing to be based on the NHS number because babies are now given their unique identifier shortly after birth.
The UK Newborn Screening Programme Centre is working with both the UK Newborn Screening Laboratories Network (UKNSLN) and the NHS Information Authority to ensure that the benefits of early issue of NHS numbers to babies extend to newborn screening. Specifically, to ensure that the blood spot label is compliant with the newborn screening filter paper test card, provision of which is overseen by the UKNSLN, and to ensure that the delivered blood spot samples meet current laboratory standards and practices.
The UKNSLN was instrumental in developing and agreeing the blood spot card label design in February/March 2003, This OBS builds on this work by utilising the NHS Numbers For Babies Birth Notification Dataset (section 3.1.1 refers).
It is the intention that both the technical processes and over-riding procedures put in place to enable NHS Numbers for Newborn Screening will be implemented within the architecture of the National Programme for Information Technology (NPfIT). The following diagram illustrates the proposed model:

Diagram 1 - Proposed Model for Screening Systems within the NPfIT.

Objectives
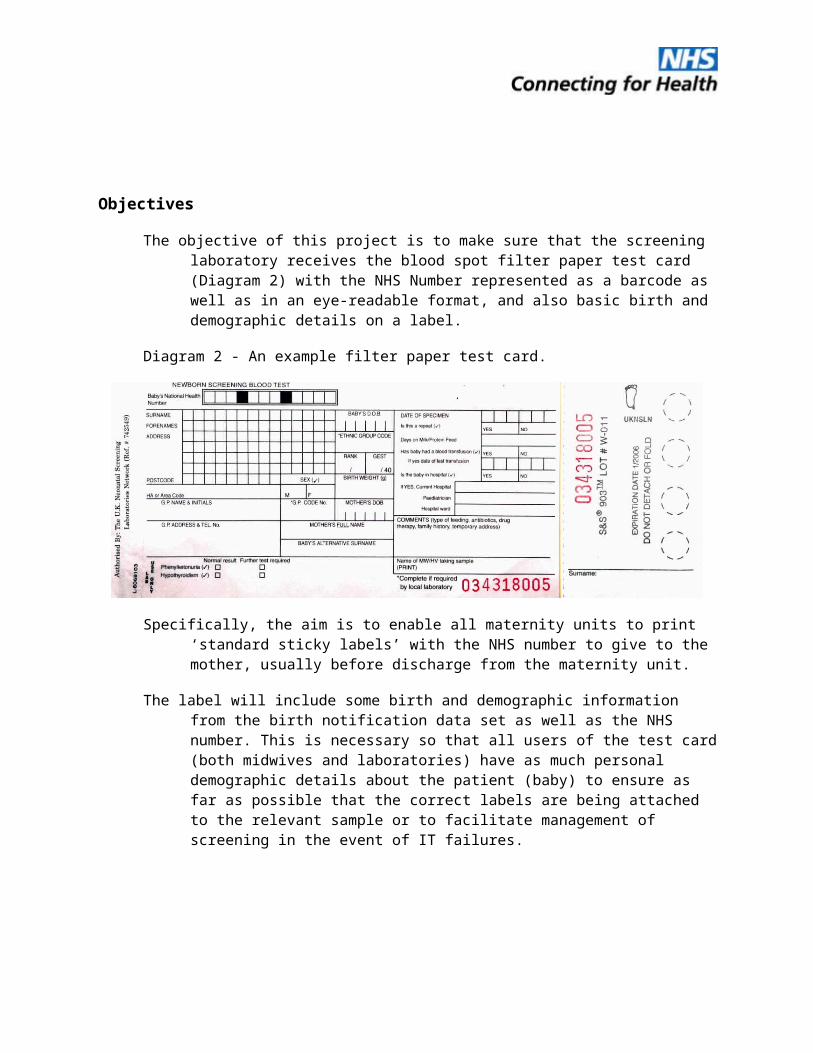
The objective of this project is to make sure that the screening laboratory receives the blood spot filter paper test card (Diagram 2) with the NHS Number represented as a barcode as well as in an eye-readable format, and also basic birth and demographic details on a label.
Diagram 2 - An example filter paper test card.
Specifically, the aim is to enable all maternity units to print ‘standard sticky labels’ with the NHS number to give to the mother, usually before discharge from the maternity unit.
The label will include some birth and demographic information from the birth notification data set as well as the NHS number. This is necessary so that all users of the test card (both midwives and laboratories) have as much personal demographic details about the patient (baby) to ensure as far as possible that the correct labels are being attached to the relevant sample or to facilitate management of screening in the event of IT failures.
The labels will bring about enormous benefits. Midwives will use these labels when they carry out the newborn blood spot test. Hence, they will not have to handwrite all the basic birth and demographic details, thus saving time and reducing errors on both the writing and reading stages. It is recognised, however, that parent(s) do move, and in such cases, demographic details will need to be manually updated when required.
The use of bar-coded labels will enable the NHS number to be used as a unique identifier within the screening process and be able to track babies throughout the system.

Being able to correctly identify and track the progress of babies is fundamental to reducing the risk of babies going untested or not being tested in a timely fashion.

3. Label CONTENT and Format
Content Overview
The contents of the label are derived from the existing NN4B Birth Notification Data Set (Reference 1).
As a result of the data items being derived from the above data set, then the validation for the data items detailed in this section of the specification MUST be consistent with the validation detailed in the NN4B Birth Notification Data Set. As an example, baby’s surname cannot be mandated in the following data set as it set as optional in the NN4B dataset.
If data items are present in the Birth Notification raised, then, if the data items appear in table 1, such data items MUST be printed on the label. Again, using the optional data item of baby’s surname (in the NN4B Birth Notification Data Set) …
if baby’s surname is present on the NN4B Birth Notification Data Set, then it MUST be printed on the label
if baby’s surname is not present on the NN4B Birth Notification Data Set, then, by default, the baby’s surname cannot be printed.
The data items, together with their format and status are detailed in table 1.
Notation used in Table 1
Field Description - description of the data item.
Defined in NHS Data Dictionary - Yes or No. (Data items marked with * (asterisk) are present in the NHS Data Dictionary but have a format that differs from the NHS Data Dictionary definition.
Status - The status identifies if the data is
M (mandatory - must be present in the message)
R (required - must normally be present but exceptional circumstances may prevent it)
O (optional - does not have to be present in the message but should be included by the sending system if available)
C (conditional - a rule specifying the circumstances in which the data must be present in the message. Details will be given in the Dependency Rule(s) column)
n/a (not applicable to this message transaction)
Format
a – alphabetic characters (letters a-z, A-Z, the <space> character, and all punctuation characters). Invalid characters are default HL7 delimiters and separators which are |^~\& (pipe, circumflex, tilde, backslash, ampersand)
n – numeric characters (values 0-9 only)
The form of representation that the data may take, according to the following notation:
a3 3 alphabetic characters, fixed length
n3 3 numeric characters, fixed length
an3 3 alpha-numeric characters, fixed length
a..3 up to 3 alphabetic characters
n..3 up to 3 numeric characters
an..3 up to 3 alpha-numeric characters
NN4B Central Issue System Validation - any conditions attached to the formatting etc.

Table 1 - Blood spot Card Label Data Items (derived from the NN4B Birth Notification)

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Bar-coded NHS Number
Submission Pending
Mandatory (subject to NHS Number being available at point of printing labels). If not issued, then blank field
UCC/EAN-128 bar-code symbology (defined later in this document)
Not present
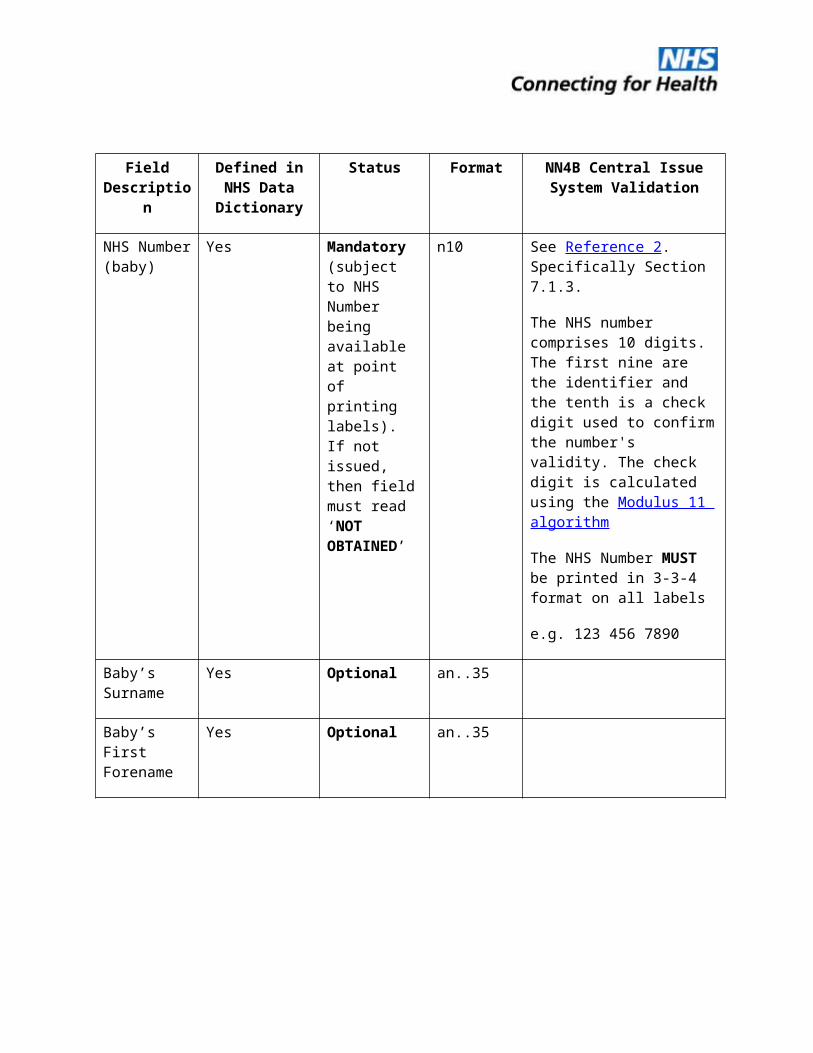
NHS Number (baby)
Yes Mandatory (subject to NHS Number being available at point of printing labels). If not issued, then field must read ‘NOT OBTAINED’
n10 See Reference 2. Specifically Section 7.1.3.
The NHS number comprises 10 digits. The first nine are the identifier and the tenth is a check digit used to confirm the number's validity. The check digit is calculated using the Modulus 11 algorithm
The NHS Number MUST be printed in 3-3-4 format on all labels
e.g. 123 456 7890
Baby’s Surname
Yes Optional an..35
Baby’s First Forename
Yes Optional an..35

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Birth Date (baby)
Yes Mandatory n8 CCYYMMDD
Formatted to be viewed/printed as dd mm ccyy. Date separator can be one of /.- (forward slash (ASCII 47), full stop (ASCII 46), hyphen (ASCII 45))
Sex Yes Mandatory n1 0 = Not known
1 = Male
2 = Female
9 = not specified
Baby’s Usual Address line 1
Yes Conditional an..35 Either address line 1 or address line 2 must be present
Baby’s Usual Address line 2
Yes Conditional an..35 Either address line 1 or address line 2 must be present
Baby’s Usual Address line 3
Yes Optional an..35
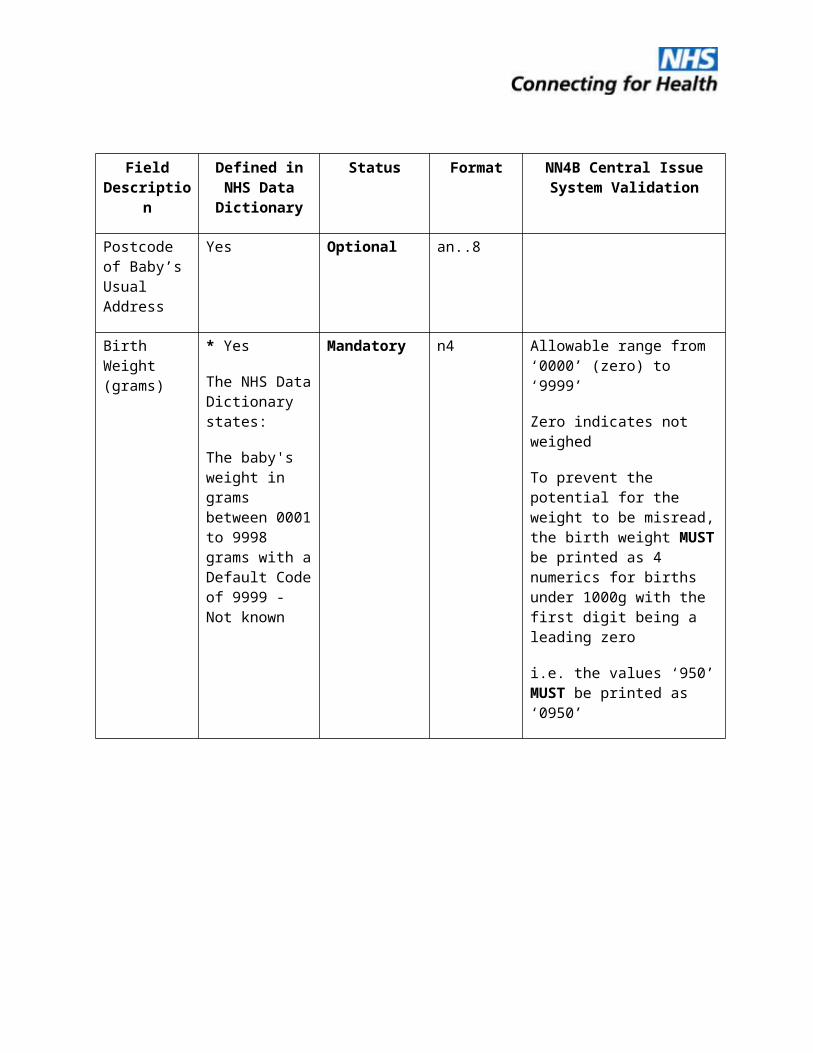
Postcode of Baby’s Usual Address
Yes Optional an..8

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Birth Weight (grams)
* Yes
The NHS Data Dictionary states:
The baby's weight in grams between 0001 to 9998 grams with a Default Code of 9999 - Not known
Mandatory n4 Allowable range from ‘0000’ (zero) to ‘9999’
Zero indicates not weighed
To prevent the potential for the weight to be misread, the birth weight MUST be printed as 4 numerics for births under 1000g with the first digit being a leading zero
i.e. the values ‘950’ MUST be printed as ‘0950’
Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Ethnic Category (baby)
Defined by mother, required for monitoring of service delivery
Yes Mandatory an2 The recommended classification is a single character defined from within the range A to Z and this should be stored in the first position of the field. (There is a further optional level of classification consisting of an additional character which may be used at local level if required) WhiteA = BritishB = IrishC = Any other White backgroundMixed D = White and Black CaribbeanE = White and Black AfricanF = White and AsianG = Any other mixed backgroundAsian or Asian British H = IndianJ = PakistaniK = BangladeshiL = Any other Asian backgroundBlack or Black BritishM = CaribbeanN = AfricanP = Any other Black backgroundOther ethnic groupsR = ChineseS = Any other ethnic groupZ = Not stated
Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Birth Order (if multiple)
* Yes
The NHS Data Dictionary states:
This records the sequence in which the baby was born, with 1 indicating the first or only birth in the sequence (i.e. singleton), 2 indicating the second birth in the sequence, 3 indicating the third, and so on with Default Codes of 8 - Not applicable 9 - Not known: a validation error
Conditional n1 Must be present if ‘Number of births in this confinement’ is greater than 1
Allowable range from ‘1’ to ‘9’
This data item will be combined with ‘Number of births in this confinement’ to produce the term of rank
Rank will be defined by the following notation:
Rank -Birth Order/No. of births this confinement
- with the separator being / (forward slash (ASCII 47))
i.e. Rank: 2/3- meaning the second birth out of three this confinement
For systems that do not record birth order for a singleton birth, then the field of rank MUST include a default of ‘1’ for birth order
i.e. although birth order can be null for a singleton birth, the rank MUST default to Rank: 1/1

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
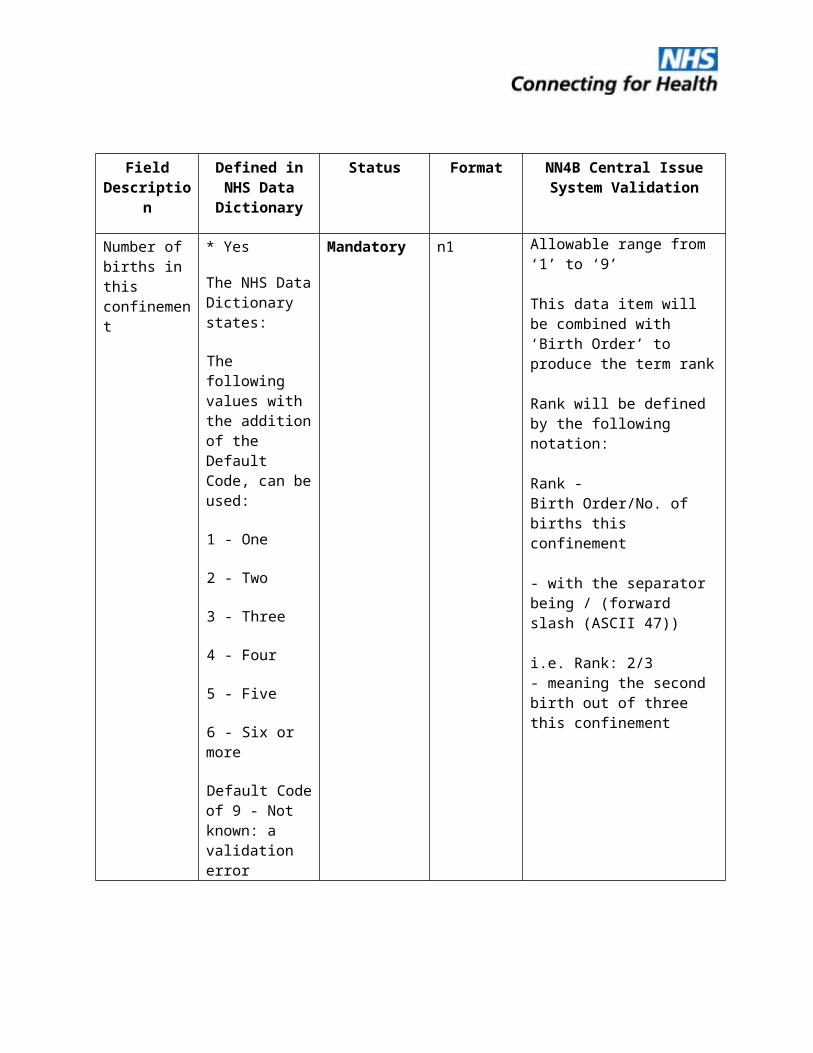
Number of births in this confinement
* Yes
The NHS Data Dictionary states:
The following values with the addition of the Default Code, can be used:
1 - One
2 - Two
3 - Three
4 - Four
5 - Five
6 - Six or more
Default Code of 9 - Not known: a validation error
Mandatory n1 Allowable range from ‘1’ to ‘9’
This data item will be combined with ‘Birth Order’ to produce the term rank
Rank will be defined by the following notation:
Rank -Birth Order/No. of births this confinement
- with the separator being / (forward slash (ASCII 47))
i.e. Rank: 2/3- meaning the second birth out of three this confinement
Gestation Length (weeks)
* Yes
The NHS Data Dictionary states:
Gestation Length records a period (if known) of between 10 to 49 weeks with a Default Code of 99 - Not known
Mandatory n2 Allowable range includes ‘00’ (zero) and from ‘10’ to ‘49’
Zero indicates unknown gestation length

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Mother’s Surname
Yes Mandatory an..35
Mother’s First Forename
Yes Mandatory an..35
Birth Date (mother)
Yes Conditional To be printed ONLY if NHS Number (mother) is NOT present on the birth notification
n8 MUST be present if Mother’s NHS Number is blank
CCYYMMDD
Formatted to be viewed/printed as dd mm ccyy. Date separator can be one of /.- (forward slash (ASCII 47), full stop (ASCII 46), hyphen (ASCII 45))
If both Birth Date (mother) and NHS Number (mother) are present on the birth notification, then the mother’s NHS Number MUST be printed in preference to the mothers’ date of birth

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
NHS Number (mother)
Yes Conditional To be printed if NHS Number (mother) is present on the birth notification
n10 The NHS number comprises 10 digits. The first nine are the identifier and the tenth is a check digit used to confirm the number's validity. The check digit is calculated using the Modulus 11 algorithm
The NHS Number MUST be printed in 3-3-4 format on all labels
e.g. 123 456 7890
If both Birth Date (mother) and NHS Number (mother) are present on the birth notification, then the mother’s NHS Number MUST be printed in preference to the mothers’ date of birth
GP Name Yes Conditional an..35 MUST be present if National GP Code is blank

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Organisation Name
Yes Conditional an..35 MUST be present if the Delivery Place Type Code is one of:0= In NHS hospital -
delivery facilities associated with midwife ward
2= In NHS hospital - delivery facilities associated with consultant ward
3= In NHS hospital - delivery facilities associated with GMP ward
4= In NHS hospital - delivery facilities associated with consultant/GMP/midwife ward inclusive of any combination of two of the professionals mentioned
5= In private hospital6= In other hospital or
institution7= In NHS hospital - ward
or unit without delivery facilities
PCT of Residence
Yes Mandatory for NHS CRS compliant systems
an..35 MUST be present if birth has been registered on an NHS CRS compliant Maternity System. To be derived from

Field Description
Defined in NHS Data
Dictionary
Status Format NN4B Central Issue System Validation
Date Printed N/A Mandatory CCYYMMDD
This is the date that the labels were printed
Formatted to be viewed/printed as dd mm ccyy. Date separator can be one of /.- (forward slash (ASCII 47), full stop (ASCII 46), hyphen (ASCII 45))
Format Overview
The format of the label design is as in Diagram 3
Diagram 3 - Blood spot Label Design.
All the data fields are shown for clarity. If data items are optional and are not present as part of the NN4B Birth Notification (e.g. baby’s surname), then the field should remain blank.
The data fields (underlined in the above diagram for illustrative purposes only and should not be printed as being underlined on the label) MUST have a text description preceding the field as follows:
NHS No:
Rank:
Label printed on:
Data fields requiring units (Birth Weight and Gestation length) MUST include the units following the field. Examples are:
3175 g - birth weight
40 weeks - gestation length
NHS No: 999 000 5451Baby Surname, Forename
Address lines 1, 2 and 3
Date of Birth Sex
Birth Weight
Rank: Birth Order/No. Births
Mother Forename Surname
GP name
Postcode
Ethnic Category (Baby)
Gestation Length
Mother NHS Number/DoB
Name of Hospital were bornLabel printed on: Date Printed

For systems that provide enhanced functionality for the data items referred to in 3.2.3 (i.e. imperial equivalents for weight; inclusion of days for gestation length) then this may be added to the design so long as it is an already recognisable label convention such as:
3175 g (7lb 0oz)
40 + 0 weeks
Mother NHS Number/DoB:
where a birth is notified to the Central Issue System which contains the Mothers’ NHS Number, then the Mother’s NHS Number MUST be printed (in 3-3-4 format) in preference to the mother’s date of birth.
where a birth is notified to the Central Issue System which DOES NOT contain the Mothers’ NHS Number, then the Mother’s Date of Birth shall be printed.

4. Bar-code content and format
Overview
Table 1 - Format of the Element String*
* Referenced from http://194.203.97.138/EANUCC/HTML_Files/03/03-06-55.html.
Notes:
Application Identifier (format of 4 numerics) - ‘8018’ - relates to a Service Relation Number (SRN) and indicates that the data field contains a Global Service Relation Number (GSRN).
EAN.UCC Company Prefix - UK Health and Social Care (format of 7 numerics) - ‘5050898’ allocated to the Service Provider (the NHS) and it makes the number (the NHS Number) GLOBALLY UNIQUE.
Service Reference (format of 10 numerics) - the NHS Number.
Check Digit (format of 1 numeric) - check digit and its verification, which must be carried out in the application software, ensures that the number is correctly composed. Details of the check digit calculation are available from http://194.203.97.138/EANUCC/HTML_Files/03/03a1-01.html.
N1 N2 N3 N4 N5 N6 N7 N8 N9 N10 N11 N12 N13 N14 N15 N16 N17 N18
Check Digit
8018
Application Identifier
EAN.UCC Company Prefix Service Reference
EAN.UCC Global Service Relation Number (GSRN)
Format of the Element String
e.g. element string ‘8018505089899900054513’ comprises …
‘8018’ - Application Identifier
‘5050898’ - EAN.UCC ‘Company’ Prefix - UK Health and Social Care Number (NHS Number)
‘9990005451’ - NHS Number 999 000 5451
‘3’ - Check Digit
5. System requirements
System handling of the bar-code
As the bar-coded NHS Number is a 22-digit element string, then systems will have to both validate and process the new format by …
recognising and discarding the application identifier (positions 1 to 4)
recognising the EAN.UCC Company Prefix (positions 5 to 11)
validating the bar-code check-digit (position 22) - this validation is done by the scanner. The check digit is not sent by the scanner to the host system
returning the 10-digit NHS Number (positions 12 to 21)
Dimensions
The minimum dimensions quoted by the e.centre for the UCC/EAN-128 bar-code are 46.7 mm long by 12 mm deep.
Specifically, the minimum symbol height indicated is for bar height only and does not include the Human Readable Interpretation. If the item is too small to accommodate the minimum, the minimum bar height is the greater of 15 percent of the symbol width including Quiet Zones or 12.7 mm (0.50 in.).
Symbology
The data carrier for the EAN.UCC Global Service Relation Number (GSRN) is the UCC/EAN-128 Bar Code Symbol. When encoding the GSRN, the UCC/EAN-128 Bar Code Symbol should be printed at an X-dimension between 0.25 mm (0.00984 in.) and 1.016 mm (0.040in.).

6. Printing requirements
Code sets
As the data encoded within the bar-code is purely numeric, then UCC/EAN-128 Code set C MUST be used so as to ensure minimum printed bar-code length.
The data carrier for the EAN.UCC Global Service Relation Number (GSRN) is the UCC/EAN-128 Bar Code Symbol. When encoding the GSRN, the UCC/EAN-128 Bar Code Symbol should be printed at an X-dimension between 0.25 mm (0.00984 in.) and 1.016 mm (0.040in.).
Label Page formats
Due to the multitude of label sheets, and also the myriad printers available, this specification cannot specify a particular type of label sheet or printer.
However, examples of some of the more popular label sheet formats in use are:
Avery A4 - L7159 - giving 24 labels (3 across by 8 down)
Avery A4 - L7160 - giving 21 labels (3 across by 7 down)
Avery A4 - L7161 - giving 18 labels (3 across by 6 down)
The following measurements are a guide as to the minimum and maximum label sizes recommended by the UKNSLN so as to be able to fit on the blood spot card:
Minimum dimensions: 6.35 cm wide by 3.81 cm deep
Maximum dimensions: 8.89 cm wide by 5.08 cm deep

7. Bar-code Verification
Verification Overview
Verification is the measuring and grading of the quality of a printed bar code in its final configuration. This is carried out to international standards and is particularly useful for quality control purposes.
The difference between symbol verification and symbol scanning is that verification measures and grades the quality of a bar code, and can provide information to help diagnose the cause of any problems. Scanning is the process of reading the data from the symbol and it provides no indication of a bar code’s quality.

Verification process
Any verifier used to check the quality of UCC.EAN bar codes should conform to the international standard ISO/IEC 15426-1, which will ensure that the codes are graded according to the standard ISO/IEC 15416.
The international specification for bar code print quality (ISO/IEC 15416) defines seven attributes.
For each scan the verifier produces an individual reflectance profile which measures the reflectance of each bar and space of the bar code. The verifier then takes nine different measurements from the reflectance profile, and grades seven of them individually.
The grade for the scan of the bar code will be the lowest grade for any one of these seven parameters. The overall symbol grade is obtained by averaging the grades of the ten individual scan reflectance profiles.
Each parameter is measured in percentage terms and this is then expressed as a numeric or alphabetic grade. The numeric grade will provide more precise figures, but as the alphabetic grades are still widely used a table showing how they compare is set out below:
Table 2 - Table relating numeric grading to alphabetic grading
Alphabetic Numeric range
A 3.5 - 4.0B 2.5 - 3.5C 1.5 - 2.5D 0.5 - 1.5F 0 - 0.5
All UCC/EAN-128 bar codes must have a grade of C (1.5) or better. In general symbols with higher quality grades can be expected to scan more easily and quickly than lower quality symbols of the same magnification. Larger magnification, the absence of truncation, and high print quality contribute to fast, effortless scanning.
Bar codes that fail verification may scan under ideal conditions, but badly or not at all in other environments. This is why a scanner cannot be used to test the quality of a bar code.
Testing process - Maternity System Suppliers
Once the System Supplier has developed their system to enable the functionality detailed in this specification, the Supplier will submit the following documentation as official conformation that the System is able to print bar-coded NHS Number labels from their system.
Written confirmation (on headed paper) from the supplier that bar-coding functionality has been implemented on their system
Written confirmation (on headed paper) of the verification process detailed in Section 7.2, together with written confirmation of their grading, together with details (make, model) of the verifier used.
Appendix A contains the sign-off form that MUST be completed by all parties detailed within the document.
All the above MUST be sent on completion to:
NN4NS Project ManagerNHS Connecting for HealthHexagon HousePynes HillRydon LaneExeterEX2 5SE- or e-mail it to [email protected]
Copies of Appendix A will be sent to all parties as part of the Project Testing process.

Testing process - Screening Laboratory System Suppliers
Once the System Supplier has developed their system to enable the scanning functionality detailed in this specification, the Supplier will submit the following documentation as official conformation that the System is able to print bar-coded NHS Number labels from their system.
Written confirmation (on headed paper) from the supplier that bar-coding functionality has been implemented on their system so as to successfully read the NHS Number bar-code and to populate the NHS Number field on the Screening Laboratory system.
Appendix A contains the sign-off form that MUST be completed by all parties detailed within the document.
All the above MUST be sent on completion to:
NN4NS Project ManagerNHS Connecting for HealthHexagon HousePynes HillRydon LaneExeterEX2 5SE- or e-mail it to [email protected]
Copies of Appendix A will be sent to all parties as part of the Project Testing process.
Appendix A contains the sign-off form that MUST be completed.
Appendix A - Blood spot label sign-off form (p1)Trust Name
Maternity Site Name
Maternity System Supplier
Maternity System Name and VersionScreening Laboratory System SupplierScreening Laboratory System Name and Version The above Maternity and Screening Laboratory Systems have been amended in accordance with the NHS Numbers for Newborn Screening Output Based Specification for the Blood spot label and have successfully completed to the satisfaction of all parties detailed in this document.
Such parties therefore consider the bar-coding software suitable for national implementation and recommends that unconditional/conditional approval status be granted.
Please include details of restrictions on page 3 if only conditional approval is recommended.

Appendix A - Blood spot label sign-off form (p2)Midwifery Representative Name
Position
Signature
Date
Maternity System Supplier Representative Name
Position
Signature
Date
Screening Laboratory System Supplier Representative Name
Position
Signature
Date
On behalf of the NHS Connecting for Health Authority, (Name)
PositionNN4NS Project ManagerSignature

Date
Appendix A - Blood spot label sign-off form (p3)Details of Restrictions
Item for Amendment Target Date for completion
1.
2.
3.
4.
5.
6.




















![P001-TR-0104764-R28 JAFZA STATION-13APR09[1]](https://img.pdfslide.us/doc/110x75/5571ff7d49795991699d5e0b/p001-tr-0104764-r28-jafza-station-13apr091.jpg)