Embed Size (px)
Citation preview

Quality in Health Care 1994;3:69-74
Views of survivors of stroke on benefits ofphysiotherapy
Pandora Pound, Michael Bury, Patrick Gompertz, Shah Ebrahim
AbstractObjective-To describe the components ofphysiotherapy valued by survivors of astroke.Design-Qualitative study using in-depthinterviews.Setting-Two adjacent districts in NorthEast Thames Regional Health Authority.Patients-82 survivors of stroke takenconsecutively from a stroke register whenthey reached the tenth month after theirstroke, 40 of whom agreed to be inter-viewed.Main measures-Content analysis ofinterviews.Results-Patients who agreed to theinterview were significantly less likely tobe disabled 12 months after stroke thanthose who did not. Twenty four patientshad received physiotherapy, and thesewere more disabled than those who hadnot. Patients appreciated physiotherapy.It was believed to bring about functionalimprovement; the exercise componentwas valued because it was perceived tokeep them active and busy and exerciseprogrammes to follow at home were alsovalued for the structure they gave to eachday; and therapists were considered asource of advice and information and asource of faith and hope.Conclusions-Many of the positiveaspects ofcaring which patients describedin the context of physiotherapy could beincorporated into the mainstream ofrehabilitation care and training. How-ever, health professionals need to becareful not to promote false expectationsabout recovery.Implications-The outcome of treatmentis of critical importance to patients andshould become a central dimension ofpatient satisfaction questionnaires. Theimpact ofphysiotherapy is not confined toreducing physical disability but may alsoaffect wellbeing. The choice of outcomemeasures in rehabilitation researchshould reflect this situation.(Quality in Health Care 1994;3:69-74)
IntroductionMost people admitted to hospital with strokereceive physiotherapy,' but a clear view on theimpact of this treatment has not yet emerged.Several trials have attempted to determine thevalue of physiotherapy after stroke, but theyare not easily comparable.2 3 Trials are rarely
randomised; settings are varied (for example,some study inpatient physiotherapy, some out-patient physiotherapy, and some domiciliaryphysiotherapy); and the content of thetreatment is not standardised.4 Moreover,outcome measures are not standardized anddo not reflect the full range of rehabilitationaims or include assessments of patient andcarer satisfaction.5 The most that can bedrawn from these studies is that physiotherapyseems to be associated with modest improve-ments (according to functional and physicaloutcome measures) in the first few monthsafter a stroke,3 6 although recent work suggeststhat there may also be benefits late after astroke.7A previous study of ours disclosed that six
months after their stroke 85% of people weresatisfied with the rehabilitation they had hadbut that only 46% were satisfied that they hadreceived enough rehabilitation.' However, thestudy was unable to explain why the majoritythought they needed more rehabilitation.Little is known about patients' attitudestowards rehabilitation, although Andersongained the impression that patients valuedtherapists' interest and positive approach.' Healso suggested that in the beginning therapistsencourage high hopes of recovery, but thatlater on many patients become disappointedbecause this recovery has not been achieved.Anderson did not ask patients systematicallyabout the service they received, but his insightoffers a possible explanation for the results ofour patient satisfaction survey.This paper examines in greater depth
the reasons why people thought they hadnot had enough rehabilitation. Explorations ofthis kind require the collection of data that arerich in information and these can often beobtained from a relatively small number ofinterviews. In depth, semistructured inter-views seemed the most appropriate way ofallowing people to talk freely about theirexperiences according to their own priorities.A qualitative method such as this is well suitedto exploring the complexity of peoples'experience9 ' and also has the potential tothrow light on the social contexts in whichpatients evaluate their health care. Survivors ofstroke may receive a combination of physio-therapy, occupational therapy, or speechtherapy, depending on the type of stroke theyhad. However, for simplicity the analysisconcentrates exclusively on physiotherapysince this is the most common form ofrehabilitation after stroke.
Department of PublicHealth and PrimaryCare, Royal FreeHospital School ofMedicine, LondonNW3 2PFPandora Pound, researchsociologistPatrick Gompertz,research fellowShah Ebrahim, professorof clinical epidemiologyDepartment of SocialScience and SocialPolicy, RoyalHolloway, Universityof London, EghamHill, SurreyTW20 OEXMichael Bury, professorof sociologyCorrespondence to:Ms PoundAccepted for publication10 May 1994
69
on 7 July 2018 by guest. Protected by copyright.
http://qualitysafety.bmj.com
/Q
ual Health C
are: first published as 10.1136/qshc.3.2.69 on 1 June 1994. Dow
nloaded from

Pound, Bury, Gompertz, Ebrahim
MethodsWe wanted to gain a representative sample ofpeople admitted to hospital with stroke, ratherthan structuring the sample to select onlypeople who had experience of physiotherapy.During nine months, consecutive patients in
the North East Thames stroke outcome study(NETSOS) stroke register (the same samplingframe used in the patient satisfaction survey),when they reached the tenth month after theirstroke, were invited to take part in aninterview. Those patients lost to follow up inthe outcomes study during the nine monthperiod, those who had moved out of the studyarea, those still inpatients at 10 months, andthose known to be unable to participate in anin depth interview owing to dementia (threepatients) or severe speech impairment (three)were excluded from the sampling frame.Additionally, because fewer women than menwere able to participate in the interviews,mainly for reasons of ill health, men wereexcluded from sampling during the last twomonths. The register contains data on allacute stroke admissions to the four majorhospitals in two adjacent health districts inNorth East Thames region between January1991 and March 1992. In the outcomes studysurvivors were followed up at six and 12months with a range of postally administeredquestionnaires, including the NottinghamExtended Activities of Daily Living (NEADL)scale," the Barthel activities of daily livingindex,'2 the Nottingham health profile,' theshort form of the geriatric depression scale,'and the patient satisfaction questionnaire.8The differences between those who
accepted and those who refused the invitationto participate in the in depth interviews wereinvestigated with Student's t test, the Mann-Whitney U test, and Pearson's x2, whereappropriate.The interviews were conducted an average
of ten months after the strokes. All (exceptone) were conducted in peoples' homes andtape recorded, and all were conducted,transcribed, and analysed by PP. Theinterviewer used a guide (see box) to ensurethat each conversation covered the samegeneral areas, but within subject areas theconversation was flexible so that issues couldbe explored in more depth by tailoringsubsequent questions to deal with eachperson's particular situation. The transcriptswere subjected to content analysis,'5 whichentails reading through the data, identifyingrecurrent themes or themes which seemimportant to the interviewees, and organisingthem into categories. This type of analysis wasused because as far as possible we wanted topresent the interviewees' views rather thanimposing our own. In the specific examplesgiven below the names of the intervieweeshave been changed to preserve anonymity.
ResultsSAMPLE POPULATIONOf the 82 patients invited to participate in anin depth interview, 40 accepted, a rate of 49%/o.The sample comprised 21 men and 19
women; 35 were white, three wereBangladeshi, and two were black Caribbean.The mean age at the time of interview was71-5 years (range 40-87 years). Twenty threepatients lived in council housing and five inwarden supervised accommodation, eightwere owner occupiers, two were living inprivately rented houses, one in bed andbreakfast accommodation and another wasstaying in her daughter's home at the time ofthe interview. Thirty nine patients identified amain carer, ofwhom 19 were spouses. Sixteenpeople lived alone.There were no significant differences six
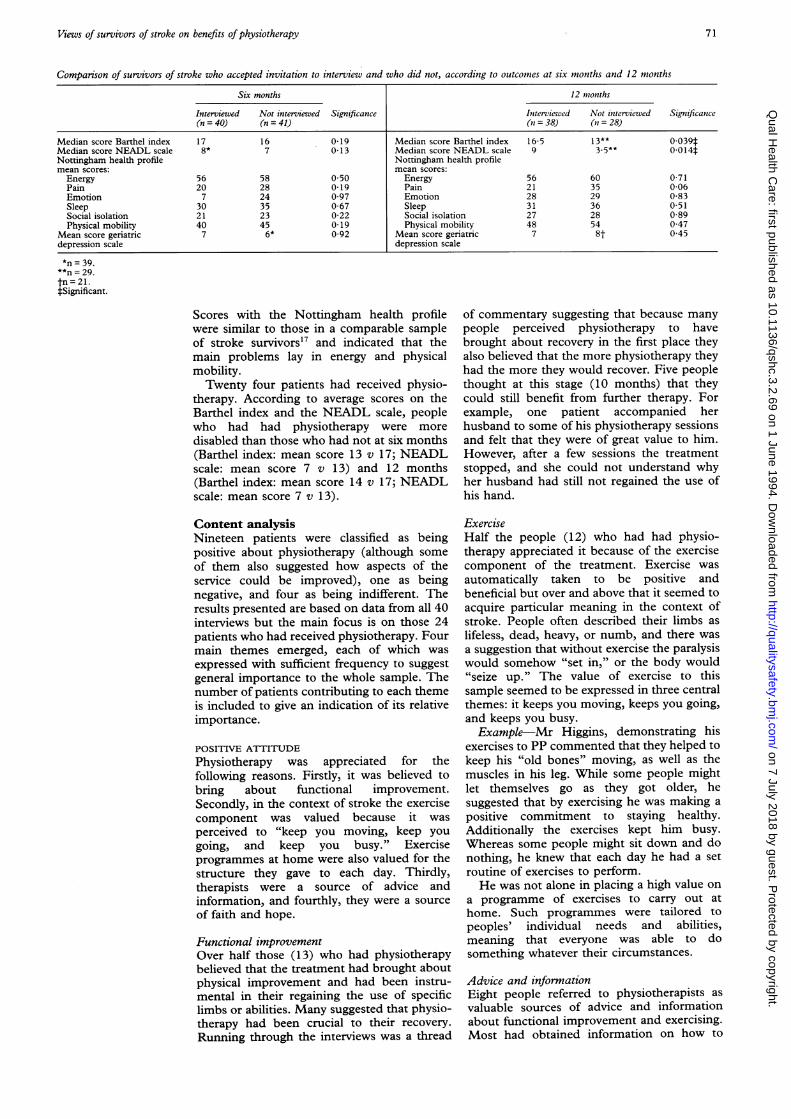
months after the stroke between those whoaccepted the invitation to be interviewed andthose who refused, either in terms of disability(with the Barthel index and the NEADL scale)or according to age at time of stroke, age leftfull time education, last employment (manualor non-manual), whether living alone, housingtenure, sex, or race. However, those whoaccepted were significantly less likely to bedisabled 12 months after the stroke than thosewho refused (table). At the same time,however, the patients in the sample had a fairlyhigh level and wide range of disability, as thescores indicate. The median Barthel score(range 0-20, 0 indicating greatest disability)for the sample was 17, six months after thestroke and 16-5 at 12 months (table),indicating that patients were moderatelydependent in basic activities of daily livingsuch as self care, using the toilet, and mobility.For extended activities of daily living (with theNEADL scale (range 0 to 22, 0 indicatinggreatest disability) the group scored a medianof 8 at six months after the stroke and 9 at 12months, suggesting the need for daily supportfrom a carer or from social services. With thegeriatric depression scale the sample scored a
mean of 7 at both six and 12 months,indicating a fairly high level of depression.'6
Interview guide* Could you tell me what happened the dayyou had your stroke?
* What happened when you got into hospital?* What do you think would have happened if
you had not gone into hospital?* How did the hospital help you? (if
appropriate)* Did you have any physiotherapy/speech
therapy/occupational therapy while inhospital?
* What did you think of it (type of therapy)?* Are you happy with the amount of therapy
you have had?
* Is there any treatment you feel you shouldhave had, that you were not offered?
* Thinking back to all the people you sawwhile you were in hospital which were themost useful to you? (Why was that?)
* You've been home for about 10 months.What would make the most improvement inyour life now?
70 on 7 July 2018 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
Qual H
ealth Care: first published as 10.1136/qshc.3.2.69 on 1 June 1994. D
ownloaded from
Views of survivors of stroke on benefits ofphysiotherapy
Comparison of survivors of stroke who accepted invitation to interview and who did not, according to outcomes at six months and 12 months
Six months 12 months
Interviewed Not interviewed Significance Interviewed Not interviewed Significance(n = 40) (n = 41) (1= 38) (in = 28)
Median score Barthel index 17 16 0-19 Median score Barthel index 16-5 13** 0-039tMedian score NEADL scale 8* 7 0-13 Median score NEADL scale 9 3-5** 0-014tNottingham health profile Nottingham health profilemean scores: mean scores:Energy 56 58 0 50 Energy 56 60 0-71Pain 20 28 0-19 Pain 21 35 0-06Emotion 7 24 0 97 Emotion 28 29 0-83Sleep 30 35 0-67 Sleep 31 36 0-51Social isolation 21 23 0-22 Social isolation 27 28 0-89Physical mobility 40 45 0.19 Physical mobility 48 54 0-47
Mean score geriatric 7 6* 0-92 Mean score geriatric 7 8t 0 45depression scale depression scale
*n = 39.**n = 29.tn =21.tSignificant.
Scores with the Nottingham health profilewere similar to those in a comparable sampleof stroke survivors'7 and indicated that themain problems lay in energy and physicalmobility.Twenty four patients had received physio-
therapy. According to average scores on theBarthel index and the NEADL scale, peoplewho had had physiotherapy were moredisabled than those who had not at six months(Barthel index: mean score 13 v 17; NEADLscale: mean score 7 v 13) and 12 months(Barthel index: mean score 14 v 17; NEADLscale: mean score 7 v 13).
Content analysisNineteen patients were classified as beingpositive about physiotherapy (although someof them also suggested how aspects of theservice could be improved), one as beingnegative, and four as being indifferent. Theresults presented are based on data from all 40interviews but the main focus is on those 24patients who had received physiotherapy. Fourmain themes emerged, each of which wasexpressed with sufficient frequency to suggestgeneral importance to the whole sample. Thenumber of patients contributing to each themeis included to give an indication of its relativeimportance.
POSITIVE ATTITUDEPhysiotherapy was appreciated for thefollowing reasons. Firstly, it was believed tobring about functional improvement.Secondly, in the context of stroke the exercisecomponent was valued because it wasperceived to "keep you moving, keep yougoing, and keep you busy." Exerciseprogrammes at home were also valued for thestructure they gave to each day. Thirdly,therapists were a source of advice andinformation, and fourthly, they were a sourceof faith and hope.
Functional improvementOver half those (13) who had physiotherapybelieved that the treatment had brought aboutphysical improvement and had been instru-mental in their regaining the use of specificlimbs or abilities. Many suggested that physio-therapy had been crucial to their recovery.Running through the interviews was a thread
of commentary suggesting that because manypeople perceived physiotherapy to havebrought about recovery in the first place theyalso believed that the more physiotherapy theyhad the more they would recover. Five peoplethought at this stage (10 months) that theycould still benefit from further therapy. Forexample, one patient accompanied herhusband to some of his physiotherapy sessionsand felt that they were of great value to him.However, after a few sessions the treatmentstopped, and she could not understand whyher husband had still not regained the use ofhis hand.
ExerciseHalf the people (12) who had had physio-therapy appreciated it because of the exercisecomponent of the treatment. Exercise wasautomatically taken to be positive andbeneficial but over and above that it seemed toacquire particular meaning in the context ofstroke. People often described their limbs aslifeless, dead, heavy, or numb, and there wasa suggestion that without exercise the paralysiswould somehow "set in," or the body would"seize up." The value of exercise to thissample seemed to be expressed in three centralthemes: it keeps you moving, keeps you going,and keeps you busy.Example-Mr Higgins, demonstrating his
exercises to PP commented that they helped tokeep his "old bones" moving, as well as themuscles in his leg. While some people mightlet themselves go as they got older, hesuggested that by exercising he was making apositive commitment to staying healthy.Additionally the exercises kept him busy.Whereas some people might sit down and donothing, he knew that each day he had a setroutine of exercises to perform.He was not alone in placing a high value on
a programme of exercises to carry out athome. Such programmes were tailored topeoples' individual needs and abilities,meaning that everyone was able to dosomething whatever their circumstances.
Advice and informationEight people referred to physiotherapists asvaluable sources of advice and informationabout functional improvement and exercising.Most had obtained information on how to
71 on 7 July 2018 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
Qual H
ealth Care: first published as 10.1136/qshc.3.2.69 on 1 June 1994. D
ownloaded from

Pound, Bury, Gompertz, Ebrahim
maximise recovery after discharge and wantedto make sure that they would not do thingswhich might impede recovery or cause furtherdamage. They had been advised about how tobehave once they were at home - for example,how to stand up "correctly," how to avoidpoor posture, or how to exercise their armsand legs. However not everybody received theadvice they desired.Example-Mr Weaver was confused about
several things. He showed the way hetransferred from his chair, but he was worriedin case he was not doing it correctly. He usedan electric massager on his weak leg and he feltthat this "toned it up" temporarily, but he hadbeen given no advice about exercising this leg.Furthermore, because one of his hands wasstill weak, he was wondering whether or not heshould try and strengthen it by squeezing on arubber ball.Some people indicated that they would
value feedback after discharge, in the form ofhome visits by physiotherapists. This was aservice that few had experience of, but whichwould apparently be much appreciated. Therealso seemed to be a desire for informationabout prognosis and for regular reviews ofprogress. Many people set their own goals,such as striving to be able to walk with a frameby six months after the stroke, and theyseemed to be asking for some form ofevaluation of their progress.
Faith and hopeThe accounts of seven patients suggested thatphysiotherapists were regarded as a source offaith or hope, or both. In those patients whohad given up on their bodies, and perhaps whohad lost the will to recover, physiotherapistswere described as having restored faith.Example-For six weeks after his stroke Mr
McCarthy lay in bed, resigning himself to thefact that he would never use his legs again,until a physiotherapist visited him and toldhim he could walk. Mr McCarthy describedthe event in terms of a miracle; he could barelybelieve that he was on his feet again, sayingthat he had "felt like Jesus walking on water."For those who already had the determi-
nation and will to get better, physiotherapistsseemed to be drawn on as a resource to helpthem in their struggle to recover.Example-Mrs Patten, although determined
enough to start the difficult task of walkingwith her frame, considerably appreciated theencouragement of her physiotherapist in doingthis and also in trying to start writing again,which she was more doubtful about. However,by the time she returned home Mrs Patten waspleased to have been able to sign and send outall her Easter cards herself.
NEGATIVE ATTITUDE
Only one person was negative about physio-therapy, because of the pain she endured as aresult of being encouraged to stand up.
INDIFFERENT ATTITUDEThe main reason why four patients wereindifferent towards physiotherapy was
because they were already able to carry outactivities that were important to them andconsidered that the treatment had nothingmore to offer.Example-When Mrs Samuels was asked
whether she thought more physiotherapywould be beneficial, her husband replied thatit did not really matter because she could nowmanage to get to the toilet on her own. MrsJacobs felt she could already walk satisfac-torily, and Mr White thought his besttreatment was to go out walking with hisdog.
PATIENTS WITHOUT EXPERIENCE OF
PHYSIOTHERAPY
Most of the patients who did not have physio-therapy did not express a wish that they hadhad it and most did not seem to have neededit. However, one patient who had had only aninitial assessment was told that he did notneed physiotherapy because the "feeling andactions" would come back naturally. This wasnot the case and he felt that if he had hadsome therapy he would not be experiencingthe problems he still had with his arm and leftleg. Another patient had contacted thehospital several times in an attempt to arrangephysiotherapy for her mother because shethought it would help to ease her pain.Ultimately the patient did her own exercises athome but seemed to feel a need forprofessional advice as to whether she wasdoing them properly.
DiscussionRESPONSE RATE
The main reasons given for non-participationwere the effects of ill health, which is notsurprising, given the population studied.Many of those who refused may have done sobecause they had already contributed a greatdeal to the outcomes study. Consideration ofthe demands on people in the main study wasalso a reason why non-responders were notfollowed up. However, despite the low take uprate for the interviews, those patients whoaccepted were no different from those whorefused, with the exception of being slightlyless disabled at 12 months. The interviewgroup were therefore probably slightly lessdisabled than a sample of all survivors wouldhave been, but their level and range ofdisability were still fairly high, as the medianscores with the Barthel index and NEADLscale indicate. The relatively low proportion ofpeople who received physiotherapy probablyreflects this slightly lower level of disability andthe fact that the study was of survivors and ofthose living at home.
PATIENTS VIEWS OF PHYSIOTHERAPY AND
IMPLICATIONS FOR PRACTICEFirst and foremost physiotherapy seemed to bevalued among this group of patients because itwas believed to be crucial to the recovery offunctional ability. Patients believed that themore therapy they had the more completetheir recovery would be. Whether this is trueclinically remains to be determined. A
72
on 7 July 2018 by guest. Protected by copyright.
http://qualitysafety.bmj.com
/Q
ual Health C
are: first published as 10.1136/qshc.3.2.69 on 1 June 1994. Dow
nloaded from

Views of survivors of stroke on benefits of physiotherapy
problem is that in this atmosphere ofuncertainty patients may foster unrealistichopes about the potential of physiotherapy.Though maintaining hope is often vitally
important, Hoffman argued that hospital staffunconsciously promote an extended belief inrecovery through various communicationstrategies (for example, being vague aboutprognosis) in order to deal with their ownfeelings that "nothing can be done" for peoplewho have had a stroke.'8 Davis, in an earlierstudy, noted the issue of maintaining"functional uncertainty" in managing chronicillness.'9 However, problems arise whentherapy ends.20 Patients may feel abandoned:they are left to deal with the recognition oftheir disability and to begin the lonely andpainful task of adjusting to it. Maintaining andpromoting "faith and hope" therefore needs tobe balanced against the reality of the disabilitythat stroke entails, although achieving thisbalance is not easy.Though patients are concerned with the
outcome of their treatment, this study suggeststhat they also gain a great deal from its process,as illustrated by their appreciation of exercise.Exercise has positive connotations generally,but it may take on particular meaning forsurvivors of stroke owing to the nature ofstroke itself. Stroke is a condition synonymouswith paralysis and inactivity, but exerciseimplies movement and animation. Thetreatment itself is active and physical. Thepatient often works together with theprofessional instead of being passive and actedupon. In this context then, the idea thatexercise keeps you moving has importantsymbolic value.The belief that exercise "keeps you going" is
perhaps specific to old age. Some people maywelcome old age, others may surrender to it,but many, as Williams points out,2' feel itshould be resisted. The moral component ofthe latter may be expressed through the ideathat others are wrong if they are "just sittingaround waiting to die."2' By engaging inexercise and remaining active in the face ofillness the negative features and stereotypesattached to old age may be resisted. Inemphasising the value of exercise, patients andtheir carers may also be expressing the need tobe seen in a positive light, in comparison withothers who have "given up." Thus exerciseand activity may simultaneously be anexpression of a continuing engagement in life,and of social distance.
Patients appreciated exercise for "keepingbusy" when the had been given a programmeof exercise to follow at home. After a stroke aperson may lose their physical independence,their autonomy, and they be unable to fulfilpreviously valued roles. The threat of"rolelessness" constitutes one of the mainchallenges of old age in modem societies22 andis reinforced by the aftermath of a conditionsuch as stroke. In this context then, theknowledge that a certain number of exercisesneeds to be done every day may provide apartial substitute for lost roles and lend avaluable structure to the day.
Clinical, nursing, and rehabilitation staffmight benefit from a deeper understandingand appreciation of the meaning of stroke andfrom a greater sensitivity to the particularexperience which stroke entails. Perhapsbecause of a preoccupation with the clinicalaspects of stroke, especially with neurologicaland functional outcomes, health professionalshave failed to recognise the importance, and insome cases the symbolic value, of the differentaspects of caring which stroke survivors havedrawn attention to here in the context ofphysiotherapy. Many of the positive aspects ofphysiotherapy which patients described couldwell be incorporated into mainstreamrehabilitation care and training.
IMPLICATIONS FOR RESEARCH
For these patients the primary concern seemedto be with the outcome of treatment, in teamsof physical recovery. However in research ofpatient satisfaction people are less commonlyasked for their views on the outcome of theirtreatment and what it means to them thanthey are for their views on the hotel aspects ofhealth care or the personal qualities ofstaff.23 25 Within rehabilitation research toothere is a popular myth that people enjoyphysiotherapy simply because physiotherapistsare "nice people." However this study suggeststhat the personal qualities of therapists are ofless importance to patients compared withtheir main priority, which is to get as muchtreatment as possible and to get better.Our findings also have implications for
rehabilitation research. These patientsindicated that they gained important benefitsfrom their physiotherapy in addition to therecovery of physical function, suggesting thatthe choice of outcome measures traditionallyused in rehabilitation research may have beenlacking in content validity. Measures havefocused almost exclusively on functionaloutcomes and have failed to reflect the otherbenefits which may be gained from physio-therapy, such as an increased feeling of well-being or a sense of self-worth.
Qualitative research has an important place inevaluating health care. It is capable of providinginsights into patients' priorities and predica-ments, which should bring about not only moresensitive care but also a deeper understandingof the way in which patients make theirevaluations of health care. Patient satisfactionmeasures are still relatively crude instrumentsand, although they are able to indicate generalareas needing attention, they are often unableto give the depth of understanding required tobring about sensitive change.Our findings were generated from a small
number of interviews with a relatively mildlydisabled group of stroke survivors. Theintention is that they should stimulate debateabout the process of rehabilitation rather thanthat they should be generalised. Ultimately,the ideas formulated here should be furtherexplored in a larger sample of stroke patientsbeing cared for both in hospital and in thecommunity with both qualitative andquantitative forms of assessment.
73 on 7 July 2018 by guest. P
rotected by copyright.http://qualitysafety.bm
j.com/
Qual H
ealth Care: first published as 10.1136/qshc.3.2.69 on 1 June 1994. D
ownloaded from

Pounild, Bunr, GJomipertZt, Ebrahloil
We acknowledge funding from the Stroke Association, theResearch Unit of the Royal College of Physicians of London,North East Thames Regional Health Authority's locallyorganised research scheme, and the generosity of all the peoplewe interviewed.
1 Anderson R. 7i'h a/teliath o' stroke. Cambridge:Cambridge Universitv Press, 1992.
2 FEffectivze Health ('arc. Stroke Rehabilitation. Leeds:University of Leeds, 1992. (Bulletin No 2)
3 Ebrahim S. The clinical cpidciniiologs of stroke. Oxford:Oxford Medical Publications, 1990.
4 Tallis R. Rehabilitation of the elderly in the 21st century.JR Coil Phvsicians Lond 1992;26:413-22.
5 Seale C, Davies P. Outcome measurement in strokerehabilitation research. International Disabilitv Stndic,1987;9:155-60.
6 Freemantle N, Pollock C, Sheldon TA, Mason JM, LongAF, Ibbotson S. Formal rehabilitation after stroke.QualityN in Health Carc 1992;1:134-7.
7 Wade D, Collen MC, Robb GF, Warlow CP. Physiotherapyintervention late after stroke and mobility. BAI71992;304:609- 13.
8 Pound P, Gompertz P, Ebrahim S. Patients' satisfactionwith stroke services. Clinical Rehabilitationi 1994;8:7- 1 7.
9 Chapman S. Unravelling gossamer with boxing gloves:problems in explaining the decline in smoking. BMJ1993;307:429-32.
10 Pope C, Mays N. Opening the black box: an encounter inthe corridors of health services research. BM7 1993;306:315-8.
11 Nouri FM, Lincoln NB. An extended activities of dailvliving index for stroke patients. Clinical Rehabilitation1987;1:301-5.
12 Mahones FI, Barthel DW. Functional esaluation: theBarthel index. ,'lZarvlcmd .Sta.t Altdical '7oinlo 1965;14:61- 5.
13 Hunt SM, McEswen J. McKenna SlP .\ lsiiriiig h/iclthstatus. London: Croom Helm, 1986.
14 Lum 0, Brink TL, Yesavage JA, Hecrsetma P, Ade YM,Rose TL. Screening tests for geriatric depression. (CliIGero)tol 1982;1:3- -43.
15 Patton MQ. Hoz' to itse qlliti /i/tis t'll -'ailitilrls.London: Sage Publications, 1 987.
1 6 Yesavage JA. Geriatric depression scale. J), ?/hush1i ii~icoho'Bulletin 1988;24:709-11.
17 Ebrahim S, Barer 1), Nourn F. Use of the NottinghamHealth Profile with patients after stroke. .I F'pidC;iniliCoi)niiiiiiiiito' Health 1986;40: 166-9.
18 Hoffman JE. "Nothing can be done:' social dimensions ofthe treatment of stroke patients in a general hospital.Ultban Life anid (l'ultmrni 1974;3(l ):50 70.
19 Dasvis F. Passage through cil'i's. Indianapolis: Bobbs-Merrill,1963.
21) Holbrook M. Stroke: social and emotional outcome.C(ill Phlsimcimais Lond 1982;16:100 4.
21 Williams R. A Protestant legacv: attitudes to death ailddllIms.cmiiiiii'st oleti) Abmdoniaiics. ()xford: C(larendon Press,199().
22 Riles' M"~', Foner A, Waring J. Sociology of age. In: SmelserNJ, ed. Handbook olf .Sociolo.gw. I ondon: Sage,1988:243-90.
23 Clear PD, McNeil BJ. Patient satisfaction as an indicatorof quality care. Inqnm'riv 1988;25:25 36.
24 Fitzpatrick R. Satisfaction with health care. In: FitzpatrickR, Hinton J, Newman S, Scambler F, 'T'hompson J, eds.Ihe cxpericem of illmoess. London: 'la stock, 1984.
25 Hall JA, Doman MC. What patients like about theirmedical care and hosw often these are asked: a meta-analhsis of the satisfaction literature. iSoc tmciSXlcd1988;27:935-9.
74
on 7 July 2018 by guest. Protected by copyright.
http://qualitysafety.bmj.com
/Q
ual Health C
are: first published as 10.1136/qshc.3.2.69 on 1 June 1994. Dow
nloaded from




![Classes of Ordinary Differential Equations Obtained for ... · distribution [19], bivariate Gompertz [20], Gompertz-power . Abstract — In this paper, the differential calculus was](https://img.pdfslide.us/doc/110x75/5c0865ae09d3f23a458c07be/classes-of-ordinary-differential-equations-obtained-for-distribution-19.jpg)
























