Embed Size (px)
Citation preview
Chapter 15b endocrine glands
1. Peripheral glands a. Thyroidb. Testicle and ovariesc. Adrenal gland
2. Endocrine glanda. Everything is under control of endocrine gland
i. Sleepii. Mood
iii. Appetiteiv. Sexual and emotional behaviorv. Happiness and sadness
vi. GIvii. Respiratory
viii. Heart ix. Reproductive
3. Hypothalamusa. Controls
i. Appetiteii. Sleep
iii. Body tempiv. Emotional and sexual behaviorv. Sympathetic and parasympathetic partially
vi. Endocrine systemvii. Memory and learning
b. Hypothalamus contains some nuclei which are involved in releasing of two types of hormonesi. Releasing hormones (RS)ii. Inhibit releasing hormone
4. Pituitary glanda. Has 3 lobes
i. Posteriorii. Anterior
iii. intermediateb. Has trophic cellsc. Has hypothalamic nuclei which release two things
i. Releasing hormonesii. Inhibit releasing hormone
d. Trophic cell stimulating hormone e. Blood carries stimulating hormones to peripheral glands
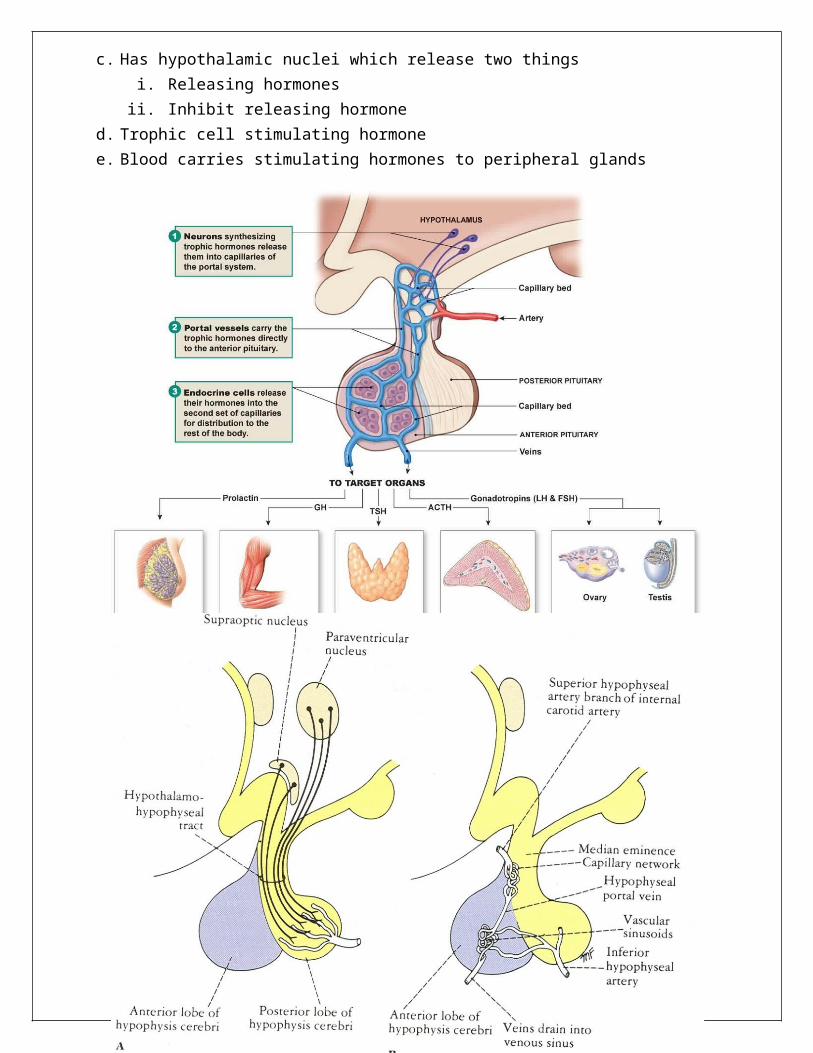
5. Connections between hypothalamus and Hypophysis cerebri (pituitary gland)a. Stimulation of anterior pituitary
i. Connection is by blood vessel called hypothalamic pituitary portal systemii. Releasing hormones stimulate tropic cells in anterior pituitar
iii. This causes secretion of stimulating hormone from anterior lobeiv. Stimulating hormone released into blood stream v. Carried to peripheral gland (such as thyroid gland, adrenal gland, testicle, ovary)
vi. 1st signal comes from hypothalamus, 2nd in pituitary glandb. Hormones from anterior lobe pituitary
i. Growth hormone (GH)ii. Adrenocorticotropic hormone (ACTH)
iii. Follicle -stimulating hormone (FSH)iv. Luteinizing hormone (LH)v. Thyroid -stimulating hormone (TSH)
vi. Prolactin (PL)c. Hormones from posterior lobe of pituitary
i. ADH (antidiuretic hormone) or vasopressin ii. Oxytocin
d. Connection between two nuclei from hypothalamus to posterior pituitaryi. Two nuclei are supraoptic and paraventricular produce two hormones
1. ADH (antidiuretic hormone) or vasopressin 2. Oxytocin
ii. Storage of these two hormones posterior pituitaryiii. When body needs these two hormones, then posterior pituitary releases these hormones
into blood stream which carries to target cell.
6. Inhibitory releasing hormonesa. These are neurotransmitters from hypothalamusb. Act as neurohormones such as
i. Dopamine1. Inhibits prolactin secretion from anterior lobe
ii. Somatostatin 1. Inhibits growth hormone secretion from anterior lobe
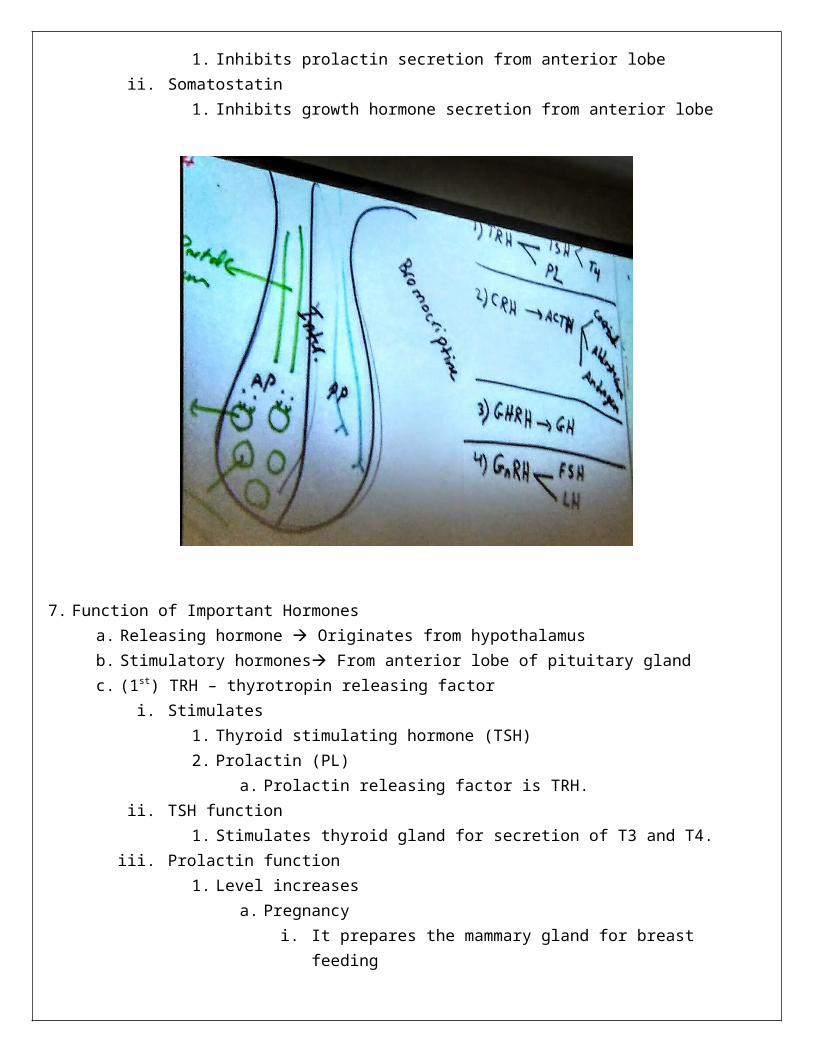
7. Function of Important Hormonesa. Releasing hormone Originates from hypothalamusb. Stimulatory hormones From anterior lobe of pituitary glandc. (1st) TRH – thyrotropin releasing factor
i. Stimulates 1. Thyroid stimulating hormone (TSH) 2. Prolactin (PL)
a. Prolactin releasing factor is TRH. ii. TSH function
1. Stimulates thyroid gland for secretion of T3 and T4. iii. Prolactin function
1. Level increases a. Pregnancy
i. It prepares the mammary gland for breast feeding ii. Suppresses sex hormone in pregnant female such as FSH (follicle
stimulating hormone) and LH (luteinizing factor)1. This causes pregnant females not to have menstruation and
ovulation during pregnancy2. Non-pregnant females and male have small amount of prolactin
a. In male controls emotional behavior and sexual behavior b. When prolactin level increases in male and nonpregnant female leads to
infertility in male or female because of suppression of FSH and LH by high prolactin level
3. Treatment for hyperprolactinemiaa. Synthetic dopamine which is called bromocriptine
d. (2nd) CRH – corticotropic releasing hormone i. Stimulates ACTH which is from anterior pituitary
1. ACTH stimulates adrenal cortex which leads to secretion Cortisol, aldosterone, and androgen from adrenal cortex.
8. (3rd) GHRH - Growth hormone releasing hormonea. GHRH leads to secretion of growth hormone (GH) from anterior lobe.
i. GH is also secreted by placenta in pregnant femaleb. Effect of GH (growth hormone)
i. Controls number and size of cellsii. Controls cell proliferation and cell growth of everything in fetus and child.
1. This includes, brain, heart, blood vessels, soft tissue. iii. GH level increases
1. In pregnancy 2. In childhood
iv. GH level decreases1. After puberty
v. Abnormal increased growth hormone in childhood causes giantism1. Means they are extremely tall2. Also have enlarged heart
vi. Abnormal secretion after puberty or in adult causes acromegaly1. Enlarged face, hands, and feet2. Important point
a. After puberty closure of epiphyseal plate in bone i. Closure activated by sex hormones
1. Testosterone in male2. Estrogen in females
b. For this reason, excess growth hormone doesn’t have any side effect on long bones because we already have closure.
c. The only bones affected are small bones such as i. Facial bone big faceii. Fingers of upper and lower limbs big hand and feet
iii. Soft tissuevii. Growth hormone controls fetal tissue development
viii. Deficiency of growth hormone1. Leads to dwarfism2. Treatment synthetic growth hormone
ix. Treatment for gigantism synthetic somatostatin
9. (4th) GnRH - Gonadotropin releasing hormone a. Stimulates follicle stimulating hormone (FSH) and luteinizing hormone (LH)b. Effect of FSH in female
i. Receptor in ovary ii. Controls development of follicle and ovum during first two weeks of menstrual cycle (28
days total)iii. 1st two weeks of cycle
1. FSH level increases which controls maturation or development of follicleiv. Midcycle day 13, 14, or 15
1. FSH level decreases2. LH level increases
a. LH functioni. LH takes over last steps of maturation of follicle after FSHii. LH causes
1. Rupture of follicle cell2. Elimination of ovum from follicle3. Migration of ovum toward fallopian tube4. It means, LH controls ovulation.
b. Good time for pregnancy is midcyclei. If there is any sperm during midcycle, 99.9% risk for pregnancy
v. After midcycle1. If there is no sperm and thus no pregnancy
a. Estrogen and progesterone level decreases b. Then we have rupture of blood vessels in endometrium and menstruation
occurs for 5 to 7 days. c. After menstruation, estrogen level increases which is important for repairing
and regeneration of endometrium. vi. If pregnancy occurs
1. The remaining of follicle cells secretes progesteronea. Progesterone is main hormone for pregnancyb. It prepares and maintains endometrial for implantation of fertilized ovumc. Decreased progesterone level in pregnant female leads to spontaneous
abortionc. Effect of FSH in male
i. FSH in male has receptor in testicleii. Controls development of sperm from germ cells in testicle
d. LH effect in Malei. LH has receptor in testicle on Leydig cells
1. LH binds to receptor on Leydig cells and stimulates testosterone secretionii. Function of testosterone
1. Important for intrauterine life2. Development of testicle in male fetus3. Development of genitalia organs in fetus and child4. Control descending of testicle from abdominal cavity to scrotum in fetus
iii. Deficiency of testosterone
1. Leads to infertility since testicle does not descend childiv. Testosterone controls secondary sex characteristics
1. Affects muscles2. Voice3. Libido4. Sexual activity
v. Other function of testosterone1. Controls body temp2. Increases rate of production of red blood cells3. Controls mood, sleep, appetite, body metabolism
vi. Deficiency of testosterone in fetus1. Leads to infertility in fetus
vii. Deficiency of testosterone in adult1. Depression in male
viii. Deficiency of estrogen in female1. Leads to depression
10. Posterior pituitary hormonesa. For storage of hormones ADH and oxytocinb. Aldosterone is sensitive to low blood pressure and sodium c. ADH is sensitive to blood osmolarity
i. ADH response to blood osmolarity1. Stimulation of osmoreceptor after dehydration2. Stimulation of cranial nerves 9 (glossopharyngeal) and CN 10 (vagus)3. Take information to hypothalamus4. Two nuclei in hypothalamus supraoptic and paraventricular
a. Secrete ADH5. Axon of neuron carries ADH and oxytocin into posterior pituitary gland6. Posterior part releases these into bloodstream carries ADH to nephron7. ADH binds to V2 receptors on nephrons8. This increases fluid retention by kidney
d. Oxytocini. Effect in female
1. Increases during delivery a. Causes contraction of uterusb. Relaxation of cervix of uterus.
2. Is controls contraction of myoendothelial cells in mammary gland and milk ejectionii. Effect in male
1. Controls ejaculation 2. Autism seems to be from hormone disorder of oxytocin
11. Adrenal glanda. Has two parts
i. Cortex 1. Is about 90% of gland (medulla is 10%)2. Cortex has 3 layers produce steroid hormones (cholesterol precursor)
a. Zona glomerulosa secretes aldosterone (mineralocorticoids)b. Zona fasciculata secretes cortisol (glucocorticoids)c. Zona reticulata secrete androgen, androstenedione,
dehydroepiandrosterone (sex hormones)3. Adrenal cortex is regulated by pituitary hormone ACTH
a. ACTH controls aldosterone, cortisol, androgenb. Hormones of adrenal cortex
i. Aldosterone secretion1. Process
a. Low blood pressure, low blood sodium, or low blood volume secretion of renin
b. Renin converts Angiotensinogen (Ag) into angiotensin 1 (Ag1)c. Angiotensin converting enzyme (ACE) converts Ag1 into Ag2d. Ag2 is vasodilatore. Ag2 acts on zona glomerulosa conversion of corticosterone to aldosteronef. Aldosterone has receptor on nephron
i. Increases reabsorption of sodium, chlorine, and waterii. Excretion of potassium and H+ into urine
iii. Absorption of bicarbonate2. Excess aldosterone secretion leads to
a. Hypokalemia b. Hypernatremia
ii. Cortisol (glucocorticoids)1. Maintains blood glucose 2. Stimulates appetite3. Degrades proteins increases protein catabolism4. Act as anti-inflammatory 5. Immunosuppressant suppresses immune system6. Stimulates gluconeogenesis7. Increases lipolysis8. Decrease glucose utilization9. Stress hormone
iii. Androgen1. Becomes active in females after puberty
a. Controls first sign of puberty in female which is axillary hair growth2. Increases androgen in female 3. Excess androgen
a. Suppresses female sex hormones which leads to infertility
12. Connection between hypothalamus pituitary gland
a. Connection with anterior lobe i. By a blood vessel called hypothalamo-pituitary portal systemii. Releasing hormones (RH) carried by portal system to the tropic cell
1. Tropic cells exist in anterior lobe of pituitary 2. Tropic cells release SH (stimulating hormones)
a. Stimulates the peripheral hormone secretions such as T3 and T4 from thyroidb. Connection to posterior pituitary
i. By axons of some neurons which come from two nuclei, supraoptic and paraventricular1. These are located in hypothalamus
ii. For production of oxytocin and ADH. 1. Posterior lobe is also for storage of these two hormones
c. There are two feedback systems i. (1) When peripheral hormone level decreases
1. Gives feedback to central hormones SH and RH increasing thema. Positive feedback
ii. (2) When peripheral hormone level increases1. Gives feedback is given to central hormones SH and RH decreasing them
a. Negative feedback
13. Two types of disordersa. Primary
i. Means cause exists peripheral gland1. Such as
a. Tumorb. Autoimmune c. Infectiond. Manipulation Young surgeon cuts part of gland
b. Secondaryi. Cause is else
1. Could be in central nervous system Hypothalamus or pituitary gland
14. Pathophysiologya. Addison’s disease could be either primary or secondary
i. Primary1. Due to destruction of adrenal cortex tissue due to
a. Tumorb. Infectionc. Autoimmuned. Manipulatione. Congenital
2. These lead to deficiency of three hormones from adrenal cortex3. Decreased aldosterone, cortisol, androgen
a. Give feedback to central hormones and increases ACTH and CRH
4. Signs and symptomsa. Low level of aldosterone patient has hypotensionb. Hyponatremia from low aldosteronec. Hyperkalemia from low aldosteroned. High level of H+ in blood so blood becomes acidice. Low level of cortisol gives hypoglycemiaf. Weak immune system from low cortisolg. Inflammation from low cortisolh. Low androgen lose body hair (in female especially)
5. In primary Addison’s disease onlya. Hyperpigmentation of skin especially face, lips, and nails, and palmar region
and dorsal region of handsb. Mechanism of hyperpigmentation in Addison’s disease
i. Low peripheral hormones from adrenal cortex increases ACTH and CRH (central hormones).
ii. Physiologically pituitary gland has three lobes, anterior, posterior, and intermediate lob.
1. Intermediate lobe has substance called POMC. iii. We can find small amount of POMC in anterior lobe. iv. POMC gives rise to different hormones
1. 1st is ACTH2. 2nd is Endorphin3. 3rd MSH – melanocyte stimulating hormone
v. In primary Addison disease, low level of peripheral hormones increases ACTH and POMC as well.
1. High POMC leads to increased ACTH and increases MSH.2. MSH is melanocyte stimulating hormone which controls
pigment cells. 3. This causes patient to have hyperpigmentation only in primary
Addison’s disease. THIS DOESN’T happen in secondary Addison’s.
6. Treatmenta. Replace all these three hormones and solve problemb. Remove tumor if problemc. Treat infection with antibioticd. Deal with autoimmune
ii. Secondary Addison’s disease Exists in hypothalamus or anterior lobe of pituitary1. Tumor2. Autoimmune3. Destruction4. Leads to decreased ACTH and CRH which decreases all three hormones from adrenal
cortex.
5. There is no feedback since no increase or decreases in peripheral hormones so no hyperpigmentation in patient
6. Treatment is to replace hormonesb. Cushing’s syndrome increases in hormones from adrenal cortex
i. Primary1. Patient has tumor in adrenal cortex which leads to over secretion of three hormones
(peripheral hormones).2. Increased peripheral decreases central hormones ACTH and decreases CRH
(corticotropin releasing hormone)ii. Secondary
1. Case is high level of ACTH or high level of CRH which lead to increase in three hormones.
2. CRH increases ACTH which increases three hormones from adrenal cortex. iii. Overproduction of adrenal cortex hormones in primary and secondaryiv. Signs and symptoms of primary and secondary
1. Increased aldosterone and cortisol – leads to hypertension2. Hypernatremia – from high aldosterone3. Hypokalemia – from high aldosterone4. Signs for hypertension
a. Headacheb. Vomitingc. Sleep disorderd. Vertigo
5. Hyperglycemia - from high cortisol6. In female patients high androgen leads to facial hair growth7. High androgen in female patient suppresses female sex hormones such as
estrogen.a. Low estrogen gives high testosterone which causes irregular menstruation,
ovulation, and infertility. v. Treatment
1. Treat hypertensiona. ACE blocker to block aldosterone pathwayb. Also could use Aldosterone receptor blocker
2. Remove tumor3. Treat infection
15. Conn’s disease tumor releasing just aldosterone - hyperaldosteronisma. Signs and symptoms
i. High level of aldosteroneii. Severe hypertension
iii. Hypernatremiaiv. Hypokalemiav. Headache
vi. Vomiting
16. Adrenal medullaa. Secretes two hormones adrenaline and noradrenaline (also called norepinephrine and
epinephrine)i. Glands not under control of pituitary gland or hypothalamus
1. Pancreas 2. Adrenal medulla 3. Parathyroid
ii. Norepinephrine 1. Can act as neurotransmitter2. NE and E act as neurotransmitter is because embryonic origin of adrenal medulla is
from ectoderma. Ectoderm gives rise to CNS, PNS, and adrenal medulla
3. Dopamine is precursor of NEa. Found in adrenal medulla and noradrenergic neurons
4. Norepinephrine depends on type of receptor alpha and betaa. Alpha 1
i. Vasoconstrictions of sphincterii. Contraction of smooth muscle
1. Increases blood pressureb. Alpha 2
i. Relaxation of smooth muscle ii. Dilation of sphincter
c. Beta 1i. Increases heart rate, contractility of myocardium, and conduction
velocity in neuronsii. Propranolol and atenolol are blockers
d. Beta 2i. Relaxes bronchiii. Albuterol acts like NE and relaxes bronchi
iii. Epinephrine1. Controls blood pressure2. Controls glucose formation and absorption in liver
b. Pheochromocytoma hypersecretion of NEi. Problem with adrenal medullaii. NE has alpha 1, alpha 2, beta 1, and beta 2 receptors
iii. Signs and symptoms1. Severe hypertension
iv. Treatment1. Control blood pressure2. Remove tumor
c. Precursor of adrenaline and noradrenaline are tyrosine DOPA dopamine NE E
17. Thyroid glanda. Is located between two cartilages
i. First is hyoid boneii. Second is first ring of trachea
b. Has two lobes, left and right lobesc. Blood supply
i. Superior part of thyroid1. Supplied by superior thyroid artery branch of external carotid artery
ii. Lower part of gland1. Supplied by inferior thyroid artery branch of thyrocervical trunk
a. This trunk is branch of subclavian arteryiii. Blood stream carries iodide which is precursor for iodine
d. Structure of thyroidi. A transverse section, we have follicular cells, which are a single layer. ii. Follicle cell membrane has cell surface receptor for TSH
iii. In center of follicle, we have colloid1. This colloid contains a protein called thyroglobulin which has tyrosine part
e. Synthesis of thyroid hormonesi. (1) Sodium carries iodide to follicle cells
1. After binding of TSH to TSH receptor on follicle cell membrane activates the follicle cells to uptake iodide
a. We call it iodide pump which occurs by sodium symportii. (2) Oxidation of iodide and conversion into iodine
iii. (3) When one iodine combines with tyrosine part of thyroglobulin forms MIT (monoiodotyorsine).
1. When two iodines combine with tyrosine part of thyroglobulin forms DIT (diiodotyrosine)
2. MIT and DIT are inactive form of T3 and T4. 3. Organification exam question
a. Formation of MIT and DIT from tyrosine incorporation into thyroglobuliniv. (4) One MIT fuses with one DIT to form T3 (triiodothyronine) (1+2-3).
1. Combination of DIT and DIT is T4 (thyroxine) (2+2=4). 2. T3 and T4 are active forms of thyroid hormones
a. Both are active and collaborate and have effect on target cell3. Example on collaboration
a. T4 is able to pass through placenta membrane, then is converted into T3 b. Then T3 controls CNS development in fetus and bone development in fetus.
f. T3 and T4 functionsi. Main effect is in fetal development
1. Maternal T3 and T4 and placental TSH in fetus controla. Thyroid gland development in fetus
b. CNS and bone development in fetusii. If there is issue to thyroid gland
1. Pregnancy is not good plan. 2. First solve issue because deficiency of maternal T3 and T4 leads to congenital
hypothyroidism in child. 3. Newborn will have mental retardation and bone growth retardation.
a. Speech and learning disorders. Motor disorder, sensory disorder, learning disorder.
iii. Treatment 1. Treatment should start hormonal replacement first day of child’s life
g. Congenital hypothyroidismi. In newborn is due to maternal thyroid hormone deficiency ii. When mother has hypothyroidism, it gives side effect to baby development
iii. In child we have1. Mental and bone growth retardation2. Heart problem3. Short stature4. Speech and learning disorder
h. Second effect of T3 and T4i. Increases sensitivity of alpha 1 and beta 1 receptors to NEii. Controls heart rate, blood pressure, and contractility of myocardium
18. Disorder of thyroid glanda. Hyperthyroidism in adults Over secretion of thyroid glands
i. Symptoms1. Hypertension2. Excess sweating3. Increased heart rate4. Heart problem5. Increased metabolic rate6. Lose weight because thyroid hormones control body metabolism7. Feel hot because thyroid hormone control body temp8. Increases oxygen consumption by different cells9. Nervousness because of CNS stimulation from thyroid hormones10. Sleep disorder
b. Hypothyroidism in adultsi. Low thyroid hormone levelsii. Symptoms
1. Gain weight obesity2. Hypotension3. Bradycardia4. Heart problem
5. In sever conditions, can lead to heart failure6. Feel cold7. Dry skin, dry hair8. In primary hypothyroidism decreased T3 and T4
a. Increases TSH (thyroid stimulating hormone) and TRH (thyroid releasing hormone) due to feedback
b. 2nd function of TRH stimulation of prolactin secretion causing high prolactin
i. In hypothyroidism in patient increased prolactin due to high TRH1. This causes suppression of sex hormones2. Nonpregnant female has irregular menstruation and ovulation
as well as infertilityc. Famous hyperthyroidism case Grave’s disease
i. This is primary hyperthyroidism issue is in peripheral 1. Graves is an autoimmune disease
a. The antibody recognizes TSH receptor and irritates the follicle cells in thyroid gland
b. This leads to over secretion and production of T3 and T4. 2. Signs and symptoms
a. Increases T3 and T4b. Increased blood antibodyc. Decreased TSH and TRH due to feedback
i. No high prolactin since not high TRH1. This only occurs in primary hypothyroidism (due to increase in
TRH from feedback from peripheral hormones) and secondary hyperthyroidism (increase in central hormones)
d. Palpitation tachycardiae. Hypertensionf. Heart diseaseg. Big eyes due to accumulation of antibody in retroorbital area.
i. Exo-orbitalh. Sweatingi. Losing weightj. Sleep disorder
3. Treatmenta. No specific treatment since its autoimmune
i. Control hypertensionii. Immune system
iii. Try to fix problemsd. Hashimoto's Thyroiditis
i. Inflammation of thyroid gland based on autoimmune diseaseii. 80% of this condition leads to hypothyroidism called post Hashimoto’s hypothyroidism
iii. 20% is converted tin hyperthyroidismiv. Signs and symptoms
1. Goiter inflammation of thyroid gland (can exist in hyper and hypothyroidism)2. Inflammation should be symmetric and bilateral
a. Tumor gives irregular margin and is unilateral or could be more than one tumor in different area of thyroid gland. Not the same as goiter
3. Tissue is tough and painful this means not cancer but just inflammation4. Viral and bacterial thyroiditis
a. pain in thyroid glandb. inflammationc. affects thyroid hormonesd. It is temporary
5. Treatmenta. For viral thyroiditis
i. Non-steroid anti-inflammatory such as aspirin and resting in bed can decreases inflammation
b. For bacterial thyroiditis antibiotics can be used as treatment6. Gestational thyroiditis due to pregnancy
a. This is also called silent thyroiditis since no signs or symptoms after pregnancy
7. Cancera. Diagnose in timeb. When there is tumor, remove the tumor
19. Other actions of thyroid hormonesa. TRH Stimulates TSH which stimulates T3 and T4
i. TSH should bind to cell surface receptor ii. T3 and T4 bind to nuclear receptors
iii. T3 and T4 require carrier protein in blood which is called thyroxine binding globulin (TBG)b. Metabolic effects
i. Increases glucose absorption ii. Increase glycogenolysis, gluconeogenesis, and glucose oxidation
iii. Increases lipolysisiv. Increase protein synthesis and degradation overall catabolic





























