- 1. Serving Special Populations Medical and Dental Homes
Children with Special Health Care Needs Washington Oral Health
Regional ForumAugust 1, 2008 Washington State Medical Home Project
Katherine TeKolste, MD - Co-Director
2. Washington StateMedical Home Project University of Washington
- CHDD
-
- Dept. Pediatric Dentistry
-
- MHLN Teams 21 Community-based teams
-
- Division of Genetics and Developmental Medicine, UW
-
- Family Voices of Washington
-
- Washington Family to Family Network
-
- Medical Assistance Administration
3. Medical Home: High-quality health care partnership
- Families, physicians and office staff working together to:
- Provide acute and preventive primary health care and a central
location for health records
- Set priorities and plan a childs care
- Identify medical and non-medical services needed to optimize
outcomes
- Coordinate specialty care & community services
- Connect with information resources
4. In a context of:
- Respect, mutual trust and collaborative decision-making in
health care encounters
- Respect for cultural and religious beliefs and personal
preferences
Originated in context of CSHCN.Evolved to include all children
and adults Endorsed by the AAP, AAFP, ACP, AOA 5. Oral Health
Issues: Prevalence in General Population
- Oral disease is the single most common chronic childhood
disease
- Five times more common than asthma
- 2% of 1-2 year olds have at least one tooth with decay
- 18% of 2-5 year olds in Head Start/ECEAP programs (WA) have
ECC
- Citizens Watch for Oral Health
- Washington State Smile Survey, 2005
6. Dental High-Risk Groups:
-
- Washingtons 1 yo are 5x and 2 yo twice as likely as children
nationwide to have dental decay(Citizens Watch for Oral
Health)
- Children from families with active dental disease(AAPD Caries
Risk Assessment Tool)
-
- Across all income levels, 2x as likely to have unmet oral
health needs as non-SHCN peers(Natl Maternal Child Oral Health
Resource Center)
-
- With severe dental decay, often need treatment in hospital
operating room(Citizens Watch for Oral Health)
7. PCP Steps:
-
- Reinforce importance of daily oral care
-
- Provide information on oral hygiene
-
- Innoculate against cavities review fluoride exposure,
supplement as needed
-
- Review diet and feeding practices that increase risk for caries
and gingivitis
-
- Review medications and dosage regimens to minimize oral health
side effects
- Monitor interactions of oral and systemic health
- Recognize and teach implications of poor oral health on overall
health across the lifespan
8. Bright Futures in Practice: Oral Health Pocket Guide
- To help health professionals implement specific oral health
guidelines during pregnancy, postpartum, infancy, early childhood,
middle childhood and adolescence
- Addresses risk assessment for caries, periodontal disease,
malocclusion and injury.
http://www.mchoralhealth.org/pocket.html 9.
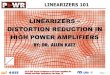
http://www.mchoralhealth.org/PediatricOH/index.htm 10. Cost Savings
of Early Oral Health Care for Preschool Children
- Over the course of 5-year study of N Carolina Medicaid children
enrolled at birth:
-
- Average cost per child who had a dental visit before 1 yo -
$262
-
- If childs first visit not until 4-5 yo, cost doubles to
$546
-
- Older age of first dental visit associated with increased
restorative and emergency visits for oral health
Savage MF et al.Pediatrics.2004. N=23 249 465 915 823 $492*
$339* $449* $262* $546* *Average cumulative dental expenditure per
child according to age at first dental visit Age at First Dental
Visit 11. Children/Youth with Special Health Care Needs
- Children who have or are at increased risk for a chronic
physical, developmental, behavioral, or emotional condition and
require health and related services of a type or amount beyond that
required by children generally
- 14% of population; 5-6% severe
- E.g. children and youth with:
-
- Cleft lip or palate; other craniofacial defects
-
- Intellectual or developmental disability
-
- Vision and/or hearing impairment
-
- Genetic and hereditary disorders
12. The Problem:
- CYSHCN -Higher risk for oral health problems
-
- Routine self-care may be difficult or impossible for a
child
-
-
- Motor disability such as seen in spastic quadriplegia
-
-
- Cognitive or behavioral impairment.
-
- The underlying disease may impact oral health
-
- The treatment of a chronic disorder may lead to secondary oral
health problems,
-
-
- Gingival hyperplasia with anticonvulsants, methotrexate,
immunosuppressants and calciuim channel blockers.
In surveys of the special needs population, parents and families
identify dental care asthe most common unmet health care needfor
their children. 13. CYSHCN:
- Need for dental care exceeds need for either preventive or
specialty medical care
- Individuals with a personal doctor/nurse (medical home) are
significantly less likely to have unmet dental needs
- Dental care should be an integral and explicitly stated part of
the comprehensive coordinated services that the medical home aims
to provide for CSHCN.
Lewis C et al.Pediatrics.2005. 14. Medical Home:Oral Health
Strategies
- Develop referral, tracking and follow-up protocols, including
oral health
- Establish collaborative relationships with oral health
professionals to ensure coordinated care
- Include oral health as part of routine health supervision
Natl Maternal and Child Oral Health Resource Center 15. The
Dental Home
- The dental home is the ongoing relationship between the dentist
and the patient, inclusive of all aspects of oral health care
delivered in a comprehensive, continuously accessible, coordinated,
and family-centered way.Establishment of a dental home begins no
later than 12 months of age and includes referral to dental
specialists when appropriate.
American Academy of Pediatric Dentistry
-
- American Dental Association
-
- Academy of General Dentistry
-
- American Academy of Pediatrics
16. Dental Home Concept:
- Oral health professionals helping families:
- Understand what care is needed
- Coordinate care with specialists and other health
professionals
17. Dental Home Provides:
- Acute and preventive services(AAPD schedules)
- Assessment for oral diseases/conditions
- Preventive dental health program based on risk assessment for
caries and periodontal disease
- Plan for acute dental trauma
- Information about care of teeth and gingivae
- Referral to dental specialists as needed
- Transition to adult dentist
AAPD 18. Dental Home for CSHCN:
- Provide appropriatepreventive and routinedental care
- Documentinformed consentas appropriate to patients special
needs
- Determine optimalcommunication methodsfor patient
- Appointment schedulingshould include determination of the
special needs, primary medical care provider, and need for
additional time or dental personnel to accommodate needs
- Know the patientsmedical history and updatesto prevent
aggravating a medical condition
- Consult with medical providers tocoordinate care
- Provide summaryof findings and recommendations
- Understandbehavior guidance* most patients with physical and
mental disabilities can be managed in the dental office
- Know and use community-based resourcesto assist with issues
from cultural and language preferences to transportation and
financial support.
- Work with insurers onfinancial coverage , especially in genetic
and congenital conditions with oro-facial malformations
AAPD Guideline on Management of Dental Patients with SHCN
http://www.aapd.org/media/policies.asp
*http://www.mchoralhealth.org/Special/mod5_0.htm 19. CSHCN -
Stories in the last 48 hours:
-
- Family of child with ID 2 pediatric dentists (unsuccessful) and
then Seattle Childrens community dentist referral.But graduates
from pediatric dentist at 21 yo.
-
- HMC used to have dental clinics for SHCN patients, but no
longer
-
- Need dental care from someone who speaks the same language as
the child/family
-
- Physician with 18 yo former preemie with CP, shunted HC, ID and
significant orthodontic needs (small jaw, crowded teeth, very high
arched palate) cannot access care at UW, CHRMC or private
orthodontist to date trying almost 2 years to get care for this
member of a Spanish-speaking family on Medicaid
-
- Childrens Village patients aging out at 18 years and no adult
program to serve the population (DECOD consultation in
progress)
-
- Very difficult to find dentists who accept adults on
Medicaid
20. CSHCN - Stories in the last 48 hours:
-
- Long-term consequences of oral health were not at the top of
the list: feeding issues, drooling, teeth grinding, biting, pica,
oral sensitivity, inadequate oral hygiene (difficult to brush,
impossible to floss) and dentist just doing the best (s/he) could
on q 6 mos cleaning; ended up with severe gum disease
-
- Physical access issues e.g. wheelchair
-
- There is a great need for the dentist or hygienist to take
adequate time to address oral sensitivity and sensory integration
issuesprivate room, quiet music, calm and pleasant voice,
explaining before doing -understand, ask and accommodate
-
- Privacy for individual who must wear a diaper and may need to
be changed while at the office
- Expenses and insurance coverage
-
- Medical vs dental coverage for maxillofacial problems; high
out-of-pocket expenses ($3,000-6,000 not uncommon), esp. in genetic
and congenital disorders with oro-facial manifestations
-
- Loss of family dental insurance with retirement move onto
Medicaid which few providers take
These themes are echoed in key informant interview (WA) and
survey (UT) 21. Access to a Dental Home:
- Fewer than half of US dental schools offer meaningful clinical
experiences in care of very young children/CSHCN
- Fewer than 1 in 10 general dentists regularly provide care for
children and youth with CP, ID or who are medically fragile
- (Natl Maternal and Child Oral Health Fact Sheet)
- In King County:(Smith RG, Lewis CW.Pediatr Dent . 2005.)
-
- 99% of dental offices seeing children would see a new 5 yo
patient, but only 15% would if on Medicaid
-
- 9% would see new under 1 yo, but only 3% would accept if on
Medicaid
22. Access?
- 136 Pediatric Dentists in WA (AAPD)
- At best: 4337 dentists licensed in WA (How many are general
dentists, active?)
-
- Dentists billing Medicaid 2008 (All seeing children?) 693
- WA 0-5 population 434,000(DOH, 4/1/2008)
- WA CSHCN population 214,600(CSHCN survey 2005-6)
23. How to provide care?
- 4,520 children per pediatric dentist
- 1,078 children per general and pediatric dentist who see
CSHCN
-
- 702 0-5yo + 376 with SHCN
- 936 children per Medicaid billing dentist
-
- 626 0-5yo + 309 with SHCN
- 97 children 0-5 per general dentist
- (assuming all are general dentists)
OR OROR 24. Other Providers:
- Dental Hygienists 4443 (2007)
-
- Sealants and some restorative
-
- Some prevention and education at WIC
- Primary Health Care Offices
-
- Anticipatory guidance, fluoride varnish
25. Washington Resources:
- UW Dental Education in the Care of Persons with Disabilities
(DECOD)
- Community Health Clinics (KGC)
- Yakima Childrens Village, Farm Workers Clinic
- Access to Baby & Child Dentistry-ABCD
26. 27. 28. 29. Practice Tools for Dental Offices Caring for
Special Needs Children:From The Maternal and Child Oral Health
Resource Center Special Care: Dental Office Considerations
ChecklistSpecial Care: Getting to Know Me Special Care: Family
Satisfaction Questionnaire 30. 31. http://www.scdonline.org/
- American Academy of Developmental Medicine and Dentistry
- AAPD Dental Home resource center
- International Assoc. for Disability and Oral Health
32. What will work for our future? 33. Issues:
- Workforce -numbers, distribution, capability/training
- Knowledge gap child development, family and social context,
behavior management, what families want from medical/dental
homes
- Willingness gap Ethics, social responsibility, reimbursement
enhancements, carrots?
34. Examine New Workforce Paradigms
- Medical Office Prevention Efforts
-
- (discussion of overlapping roles of medical and dental
homes)
- Oral Health Practitioners (MN)
- Nursing/Dental (NYU) synergistic relationship to improve
overall health
35. New paradigms:
- Special clinics Premier Health Program, NYC
- Centers of Oral Health Excellence
- Dental Internship requirements (NY 2007)
-
- Increased experience with complex problems
-
- Opportunity for hospitals to establish dental training
programs
36. Align With Referral Capacity :
- As a community, move for change improving dental outcomes for
young children and CSHCN is a priority; effective prevention will
leverage significant cost savings and alleviate unneeded
suffering
-
-
- Capacity esp. for subpopulations by age, ESL
-
- Establish referral criteria with local dental resources
-
- Other community resources
-
-
- WIC nutritional education
-
-
- PHD/LHD oral health specialists
37. Connecting Your Medical and Dental Community:
-
- Personal links your own doctor/dentist
-
- Local Medical and Dental Societies
-
-
- Washington State Dental Association, Medical Association, WC
AAP
-
-
-
- Oral health liaison, CSHCN Coordinator in LHJ
-
-
- Community Health Clinics, FQHCs
-
-
- Medical and Dental Schools, Faculty Contacts
38. Medical-Dental Linkage - Models
-
- 1:1::MD:DDS relationships fordirect patient referral
-
- Toll-free 211 referral hotline Idaho CareLine with rotating
list of dentists accepting patient on MD referral
-
- Smile Mobile; ABCD Program
-
- Referral system for adults w/HIV
-
- Pilot for access for pregnant women
-
- Initiation of Childrens Village/ DECOD Transition
collaboration
39. 40. 41. Take Home Messages:
- Break down silos for prevention
- Rejoice in children being embedded in families who work to make
it happen (may not be as true for other populations you will
discuss today). Leverage family power.
- Start to organize services at your community level
- Be open to examining new models.
42. Considerable work remains to define the health team
composition(including dental professionals) and technology
requirements, develop the optimal medical home [and dental home]
curricula and performance measures, and evaluate the effectiveness
and cost of coordinated services as well as their financing and
methods of provider compensation. Kenney MK et al.Parental
perceptions of dental/oral health among children with and without
special health care needs.Ambulatory Pediatrics.In press.