Embed Size (px)
Citation preview
J Am Acad Audiol 8 : 447-467 (1997)
Video Otoscopy in Audiologic Practice Roy F. Sullivan*
Abstract
Recent advances in endoscopic optics and miniature video camera technology have made video otoscopy (VO) accessible to audiologists in a practical way. Seven categories of VO applications are presented with clinical examples : (1) general examination of the earcanal and tympanic membrane, (2) physician communication/telemedicine, (3) hearing instrument selection and fitting applications, (4) patient education, (5) scope of practice reinforcement, (6) knowledge base/skill growth, and (7) cerumen management .
Key Words: Audiologist, audiology, canal, cerumen, concha, eardrum, external ear, fiber optics, hearing aid, otic pathology, otoscope, otoscopy, pinna, telemedicine, tympanic mem-brane, video, video otoscope, video otoscopy
T
he external ear is the gateway to the sense of hearing. In the profession of audiol-ogy, clinical details of visual examination
of the pinna, concha, external auditory canal (EAC), and tympanic membrane (TM) have received significantly less attention than func-tional assessment of auditory capacity using psychoacoustic, electroacoustic, and electrophysi-ologic techniques . Recent cost-effective develop-ments in endoscopic optics and miniature video camera technology have made video endoscopic otoscopy or video otoscopy WO) accessible to audiologists in a practical way. VO appears at a time of clinical need generated by (a) audiol-ogists fitting the majority of custom corrective amplification in all contexts, (b) audiologists fit-ting those hearing aids deeper within the EAC, (c) cerumen management emerging within the scope of audiologic practice, and, perhaps most significantly, (d) a growing recognition of audi-ology as a cost-effective resource for direct refer-ral of patients with suspected hearing loss by primary care physicians (PCPs), the "gate-keepers" of health care (Sullivan 1993, 1995a, b, 1997) .
Basic categories of VO applications for audi-ologic practice are shown in Table 1. These cat-egories may be appraised relative to their direct or indirect value for the patient, the PCP and ENT physician, and the audiologist . For exam-ple, VO benefits the audiologist by verifying acoustic and physical access to the EAC and TM for both hearing evaluation and hearing aid fitting. It can also be used in direct and referred
cerumen management . For example, with referred patients, the physician benefits from the high quality of clinical documentation provided by the audiologist . VO provides detailed clinical information correlating pathology and condi-tions observable in the EAC and at the TM with audiologic findings and the outcome of medical treatment. The patient may benefit specifically from a better understanding of their ear, of any observable otic condition that may exist requir-ing treatment, and in hearing aid fitting and ori-entation . The audiologist also benefits from an enhanced appreciation, by both physician and patient, of his or her technological skills demon-strated in the application of VO.
HISTORICAL ANTECEDENTS OF VIDEO OTOSCOPY
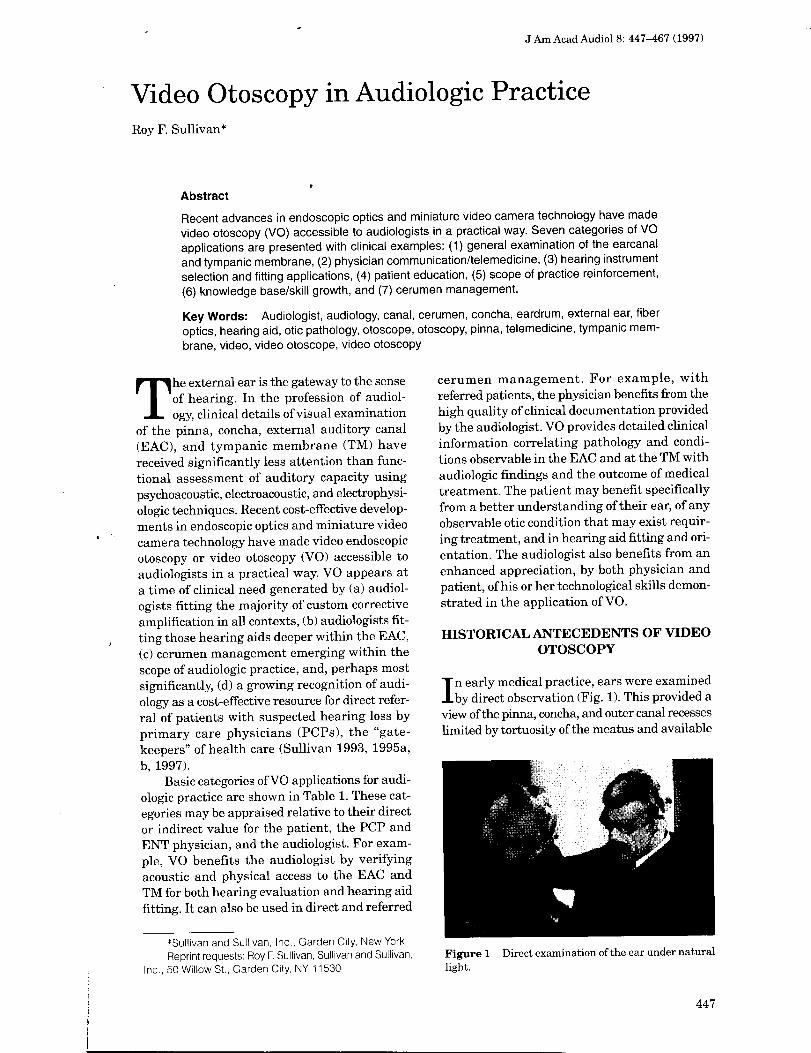
I n early medical practice, ears were examined by direct observation (Fig . 1) . This provided a
view of the pinna, concha, and outer canal recesses limited by tortuosity of the meatus and available
*Sullivan and Sullivan, Inc., Garden City, New York Reprint requests : Roy F. Sullivan, Sullivan and Sullivan,
Inc., 50 Willow St ., Garden City, NY 11530 Figure 1 Direct examination of the ear under natural light .
447
Journal of the American Academy of Audiology/Volume 8, Number 6, December 1997
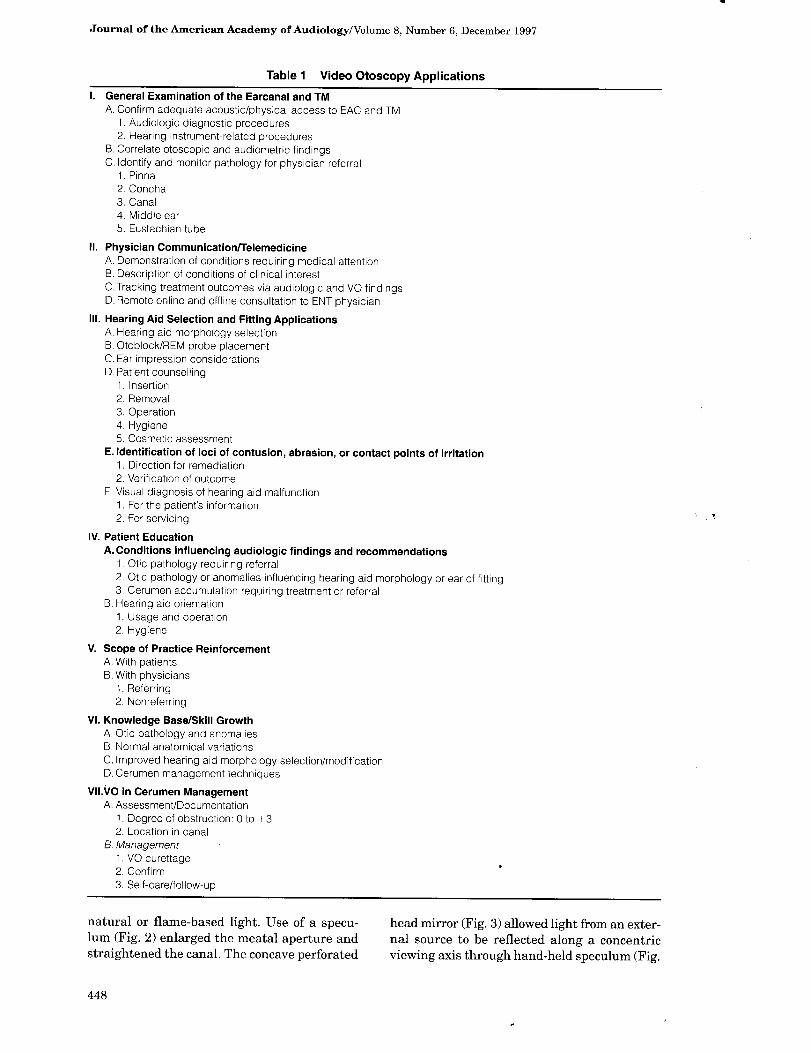
Table 1 Video Otoscopy Applications I . General Examination of the Earcanal and TM
A . Confirm adequate acoustic/physical access to EAC and TM 1 . Audiologic diagnostic procedures 2 . Hearing instrument-related procedures
B . Correlate otoscopic and audiometric findings C . Identify and monitor pathology for physician referral
1 . Pinna 2.Concha 3 . Canal 4 . Middle ear 5 . Eustachian tube
II . Physician CommunicationfTelemedicine A. Demonstration of conditions requiring medical attention B . Description of conditions of clinical interest C . Tracking treatment outcomes via audiologic and VO findings D . Remote online and offline consultation to ENT physician
III . Hearing Aid Selection and Fitting Applications A. Hearing aid morphology selection B . Otoblock/REM probe placement C . Ear impression considerations D . Patient counselling
1 . Insertion 2 . Removal 3 . Operation 4 . Hygiene 5 . Cosmetic assessment
E . Identification of loci of contusion, abrasion, or contact points of irritation 1 . Direction for remediation 2 . Verification of outcome
F. Visual diagnosis of hearing aid malfunction 1 . For the patient's information 2 . For servicing
IV. Patient Education A . Conditions influencing audiologic findings and recommendations
1 . Otic pathology requiring referral 2 . Otic pathology or anomalies influencing hearing aid morphology or ear of fitting 3 . Cerumen accumulation requiring treatment or referral
B . Hearing aid orientation 1 . Usage and operation 2 . Hygiene
V. Scope of Practice Reinforcement A . With patients B . With physicians
1 . Referring 2 . Nonreferring
VI . Knowledge Base/Skill Growth A . Otic pathology and anomalies B . Normal anatomical variations C . Improved hearing aid morphology selection/modification D . Cerumen management techniques
VILVO in Cerumen Management A . Assessment/Documentation
1 . Degree of obstruction : 0 to +3 2 . Location in canal
B . Management 1 . VO curettage 2 . Confirm 3 . Self-care/follow-up
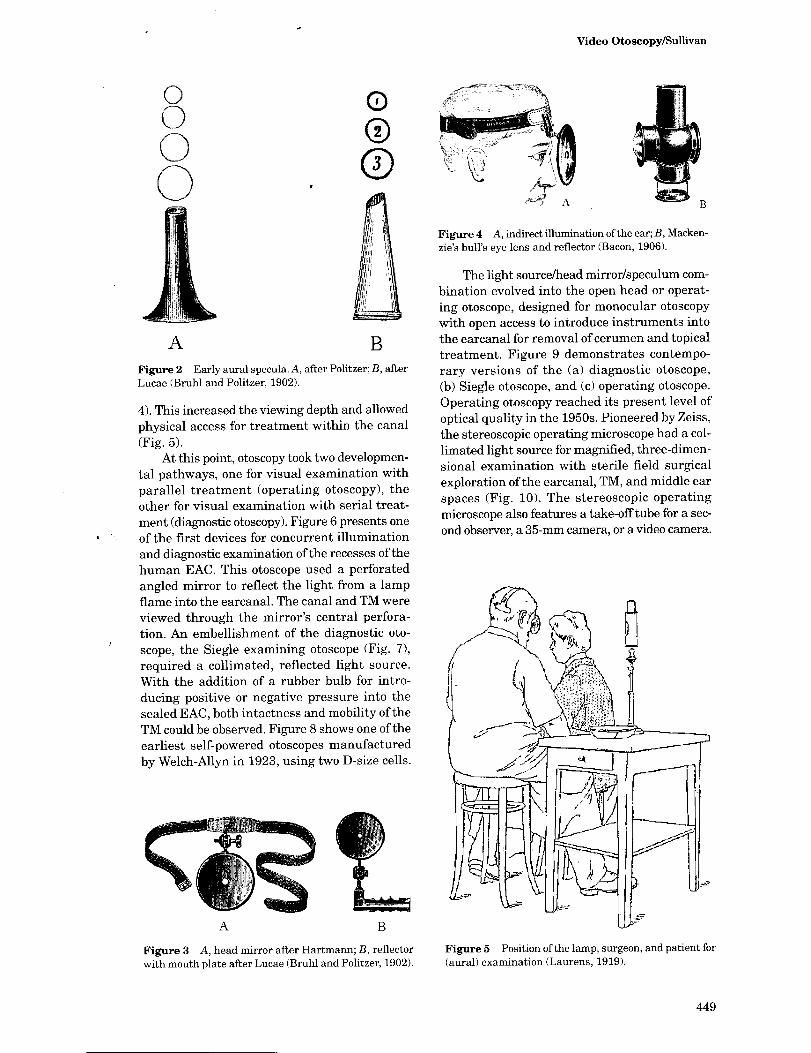
natural or flame-based light. Use of a specu-lum (Fig . 2) enlarged the meatal aperture and straightened the canal. The concave perforated
head mirror (Fig . 3) allowed light from an exter-nal source to be reflected along a concentric viewing axis through hand-held speculum (Fig .
448
Video Otoscopy/Sullivan
0 C-)
Figure 2 Early aural specula. A, after Politzer; B, after Lucae (Bruhl and Politzer, 1902).
4) . This increased the viewing depth and allowed physical access for treatment within the canal (Fig . 5) .
At this point, otoscopy took two developmen-tal pathways, one for visual examination with parallel treatment (operating otoscopy), the other for visual examination with serial treat-ment (diagnostic otoscopy). Figure 6 presents one of the first devices for concurrent illumination and diagnostic examination of the recesses of the human EAC. This otoscope used a perforated angled mirror to reflect the light from a lamp flame into the earcanal . The canal and TM were viewed through the mirror's central perfora-tion . An embellishment of the diagnostic oto-scope, the Siegle examining otoscope (Fig . 7), required a collimated, reflected light source . With the addition of a rubber bulb for intro-ducing positive or negative pressure into the sealed EAC, both intactness and mobility of the TM could be observed . Figure 8 shows one of the earliest self-powered otoscopes manufactured by Welch-Allyn in 1923, using two D-size cells.
A B
Figure 3 A, head mirror after Hartmann ; B, reflector with mouth plate after Lucae (Bruhl and Politzer, 1902).
Figure 4 A, indirect illumination of the ear; B, Macken-zie's bull's eye lens and reflector (Bacon, 1906) .
The light source/head mirror/speculum com-bination evolved into the open head or operat-ing otoscope, designed for monocular otoscopy with open access to introduce instruments into the earcanal for removal of cerumen and topical treatment. Figure 9 demonstrates contempo-rary versions of the (a) diagnostic otoscope, (b) Siegle otoscope, and (c) operating otoscope . Operating otoscopy reached its present level of optical quality in the 1950s. Pioneered by Zeiss, the stereoscopic operating microscope had a col-limated light source for magnified, three-dimen-sional examination with sterile field surgical exploration of the earcanal, TM, and middle ear spaces (Fig . 10). The stereoscopic operating microscope also features a take-off tube for a sec-ond observer, a 35-mm camera, or a video camera .
Figure 5 Position of the lamp, surgeon, and patient for
(aural) examination (Laurens, 1919).
449
Journal of the American Academy of Audiology/Volume S, Number 6, December 1997
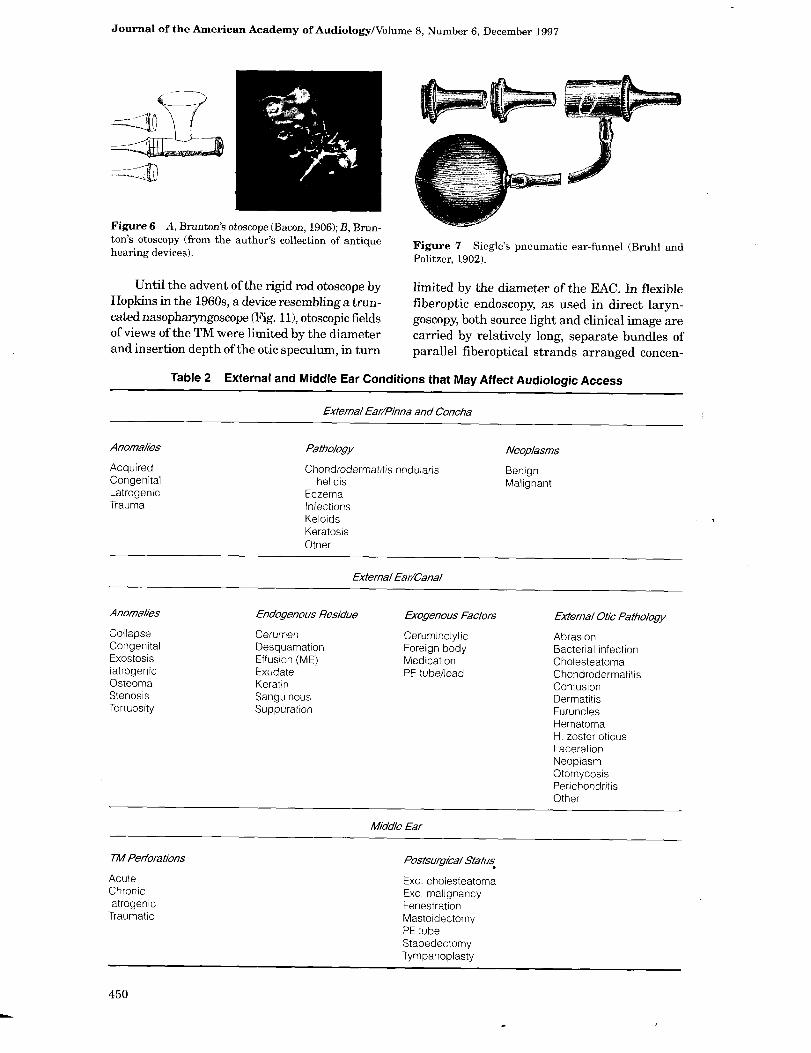
Figure 6 A, Brunton's otoscope (Bacon, 1906); B, Brun-ton's otoscopy (from the author's collection of antique hearing devices) .
Until the advent of the rigid rod otoscope by Hopkins in the 1960s, a device resembling a trun-cated nasopharyngoscope (Fig. 11), otoscopic fields of views of the TM were limited by the diameter and insertion depth of the otic speculum, in turn
rmatitis nodularis
Table 2 External and Middle Ear Conditions that May Affect Audiologic Access
External Ear/Pinna and Concha
Anomalies Patiho%gy
Acquired Chondrode Congenital helicis Latrogenic Eczema Trauma Infections
Keloids Keratosis Other
E
Anomalies Endogenous Residue
Collapse Cerumen Congenital Desquamation Exostosis Effusion (ME) latrogenic Exudate Osteoma Keratin Stenosis Sanguinous Tortuosity Suppuration
TM Perforations
Acute Chronic latrogenic Traumatic
xternal Ear/Canal
Figure 7 Siegle's pneumatic ear-funnel (Bruhl and Politzer, 1902).
limited by the diameter of the EAC. In flexible fiberoptic endoscopy, as used in direct laryn-goscopy, both source light and clinical image are carried by relatively long, separate bundles of parallel fiberoptical strands arranged concen-
Exogenous Factors
Ceruminolytic Foreign body Medication PE tube/lead
Middle Ear
Postsurgical Status
Exc . cholesteatoma Exc . malignancy Fenestration Mastoidectomy PE tube Stapedectomy Tympanoplasty
Neoo/asms
Benign Malignant
External Otic Patho%gy
Abrasion Bacterial infection Cholesteatoma Chondrodermatitis Contusion Dermatitis Furundes Hematoma H . zoster oticus Laceration Neoplasm Otomycosis Perichondritis Other
450
Video Otoscopy/Sullivan
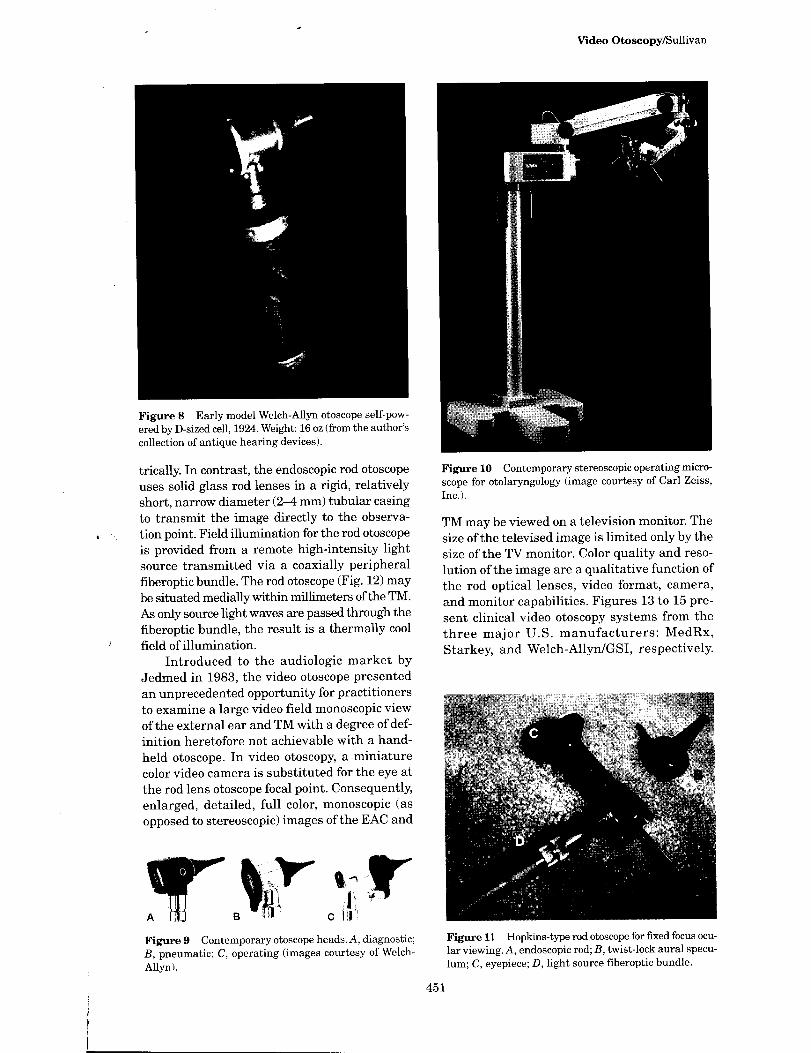
Figure S Early model Welch-Allyn otoscope self-pow-ered by D-sized cell, 1924 . Weight : 16 oz (from the author's collection of antique hearing devices) .
trically. In contrast, the endoscopic rod otoscope uses solid glass rod lenses in a rigid, relatively short, narrow diameter (2-4 mm) tubular casing to transmit the image directly to the observa-tion point. Field illumination for the rod otoscope is provided from a remote high-intensity light source transmitted via a coaxially peripheral fiberoptic bundle . The rod otoscope (Fig . 12) may be situated medially within millimeters of the TM. As only source light waves are passed through the fiberoptic bundle, the result is a thermally cool field of illumination .
Introduced to the audiologic market by Jedmed in 1983, the video otoscope presented an unprecedented opportunity for practitioners to examine a large video field monoscopic view of the external ear and TM with a degree of def-inition heretofore not achievable with a hand-held otoscope . In video otoscopy, a miniature color video camera is substituted for the eye at the rod lens otoscope focal point. Consequently, enlarged, detailed, full color, monoscopic (as opposed to stereoscopic) images of the EAC and
Figure 9 Contemporary otoscope heads. A, diagnostic ; B, pneumatic; C, operating (images courtesy of Welch-Allyn) .
Figure 10 Contemporary stereoscopic operating micro-
scope for otolaryngology (image courtesy of Carl Zeiss,
Inc.) .
TM may be viewed on a television monitor. The size of the televised image is limited only by the size of the TV monitor. Color quality and reso-lution of the image are a qualitative function of the rod optical lenses, video format, camera, and monitor capabilities . Figures 13 to 15 pre-sent clinical video otoscopy systems from the three major U.S . manufacturers : MedRx, Starkey, and Welch-Allyn/GSI, respectively.
Figure 11 Hopkins-type rod otoscope for fixed focus ocu-lar viewing. A, endoscopic rod; B, twist-lock aural specu-
lum; C, eyepiece; D, light source fiberoptic bundle .
451
Journal of the American Academy of Audiology/Volume 8, Number 6, December 1997
ROD OTOSCOPE CIRCU6IFERENTIAL FIBER OPTICS BUNDLE
ROD LENS
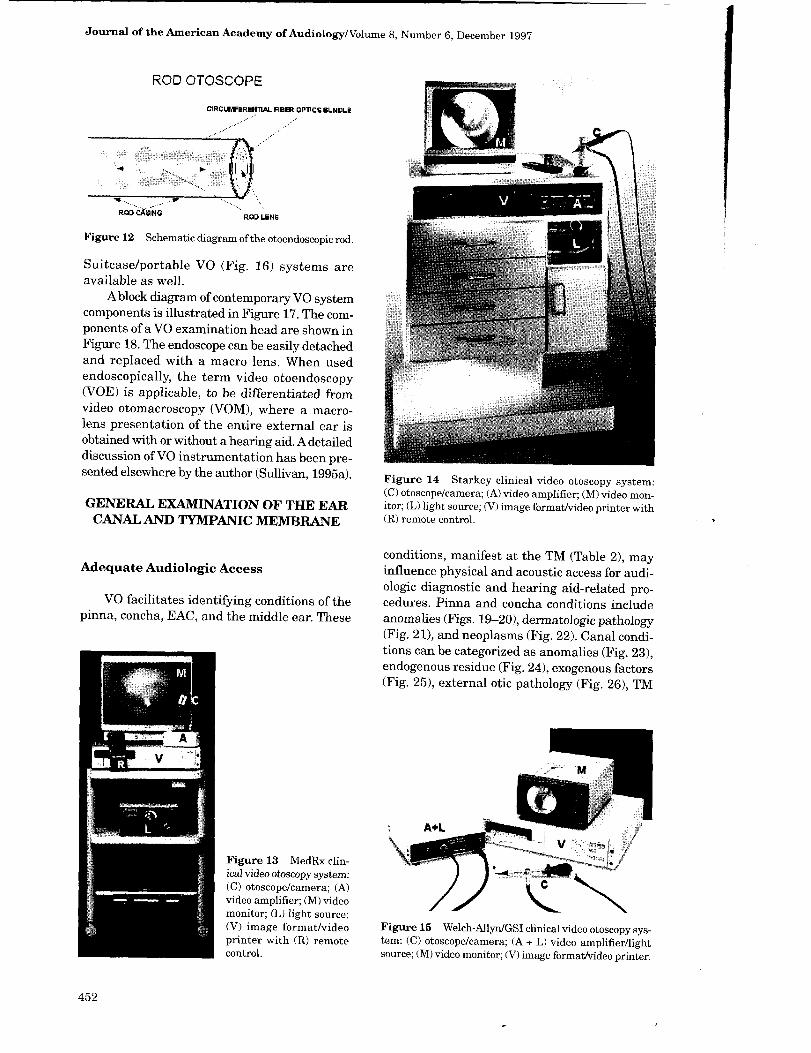
Figure 12 Schematic diagram of the otoendoscopic rod.
Suitcase/portable VO (Fig . 16) systems are available as well .
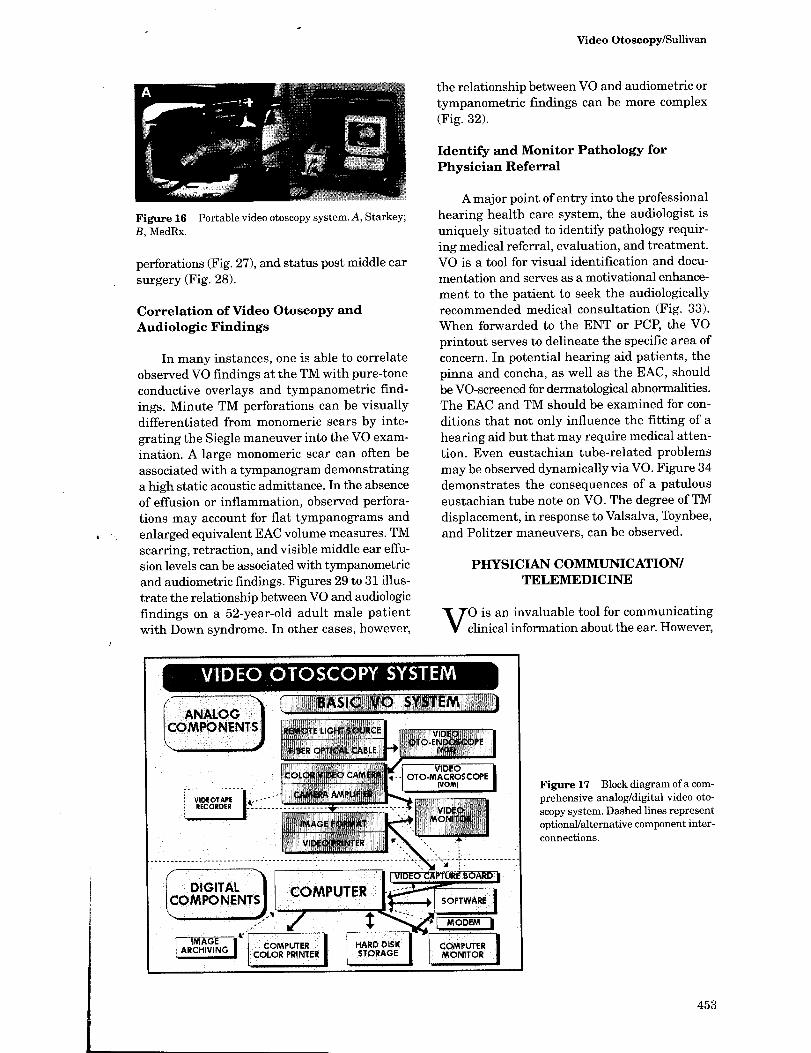
A block diagram of contemporary VO system components is illustrated in Figure 17 . The com-ponents of a VO examination head are shown in Figure 18. The endoscope can be easily detached and replaced with a macro lens . When used endoscopically, the term video otoendoscopy (VOE) is applicable, to be differentiated from video otomacroscopy (VOM), where a macro-lens presentation of the entire external ear is obtained with or without a hearing aid. A detailed discussion of VO instrumentation has been pre-sented elsewhere by the author (Sullivan, 1995a) .
GENERAL EXAMINATION OF THE EAR CANAL AND TYMPANIC MEMBRANE
Adequate Audiologic Access
VO facilitates identifying conditions of the pinna, concha, EAC, and the middle ear. These
Figure 13 MedRx clin-ical video otoscopy system : (C) otoscope/camera; (A) video amplifier; (M) video monitor; (L) light source; (V) image format/video printer with (R) remote control.
Figure 14 Starkey clinical video otoscopy system : (C) otoscope/camera; (A) video amplifier; (M) video mon-itor ; (L) light source; (V) image format/video printer with (R) remote control.
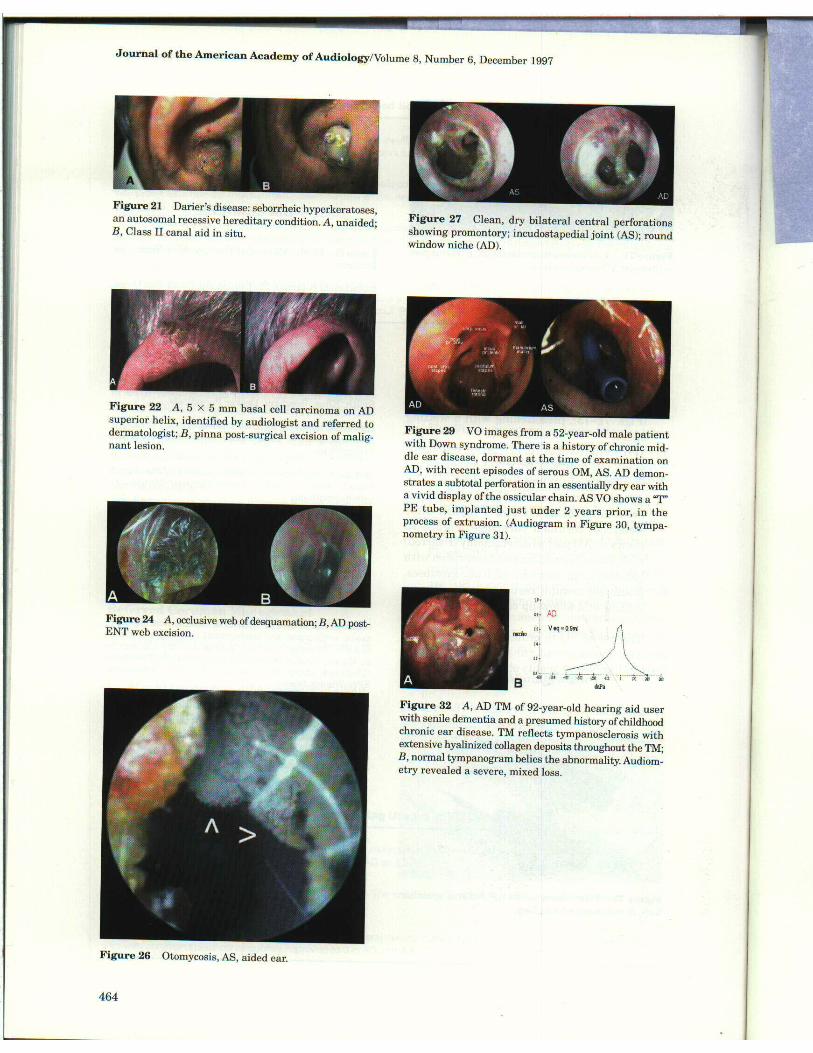
conditions, manifest at the TM (Table 2), may influence physical and acoustic access for audi-ologic diagnostic and hearing aid-related pro-cedures. Pinna and concha conditions include anomalies (Figs. 19-20), dermatologic pathology (Fig . 21), and neoplasms (Fig . 22). Canal condi-tions can be categorized as anomalies (Fig . 23), endogenous residue (Fig . 24), exogenous factors (Fig . 25), external otic pathology (Fig . 26), TM
Figure 15 Welch-Allyn/GSI clinical video otoscopy sys-tem: (C) otoscope/camera; (A + L) video amplifier/light source; (M) video monitor; (V) image format/video printer.
452
Video Otoscopy/Sullivan
Figure 16 Portable video otoscopy system. A, Starkey ; B, MedRx .
perforations (Fig. 27), and status post middle ear surgery (Fig . 28) .
Correlation of Video Otoscopy and Audiologic Findings
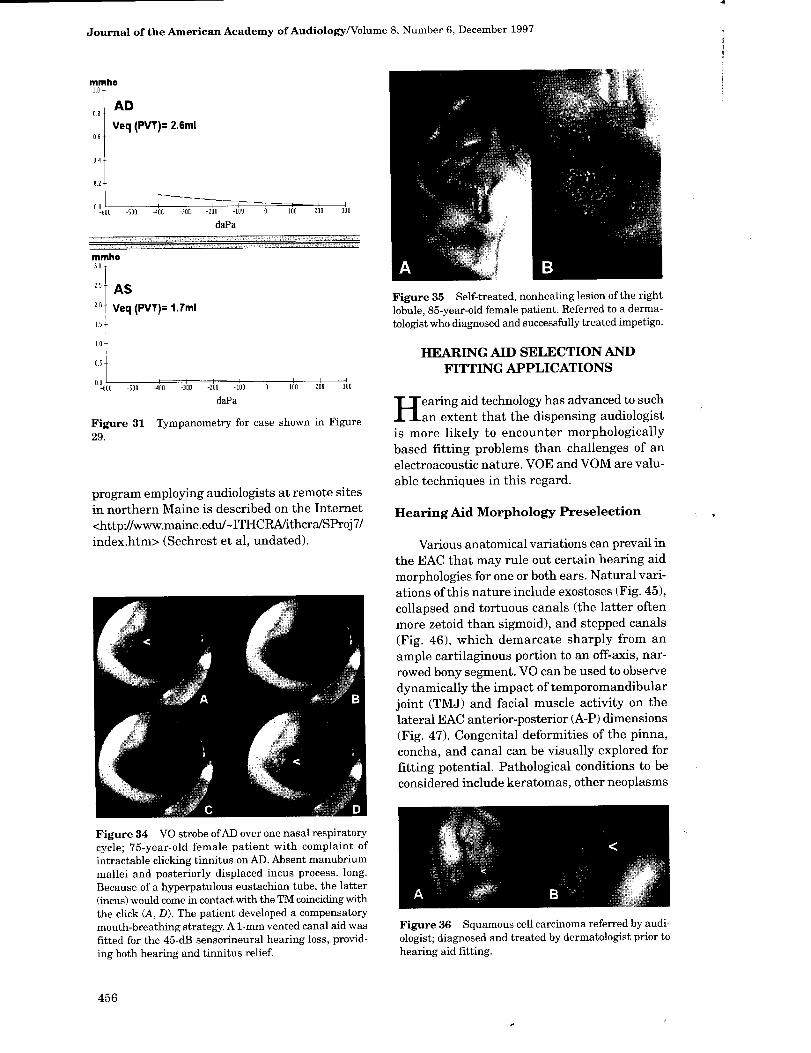
In many instances, one is able to correlate observed VO findings at the TM with pure-tone conductive overlays and tympanometric find-ings. Minute TM perforations can be visually differentiated from monomeric scars by inte-grating the Siegle maneuver into the VO exam-ination. A large monomeric scar can often be associated with a tympanogram demonstrating a high static acoustic admittance . In the absence of effusion or inflammation, observed perfora-tions may account for flat tympanograms and enlarged equivalent EAC volume measures . TM scarring, retraction, and visible middle ear effu-sion levels can be associated with tympanometric and audiometric findings . Figures 29 to 31 illus-trate the relationship between VO and audiologic findings on a 52-year-old adult male patient with Down syndrome . In other cases, however,
VIDEO} C3T JSCt PY
the relationship between VO and audiometric or tympanometric findings can be more complex (Fig . 32).
Identify and Monitor Pathology for Physician Referral
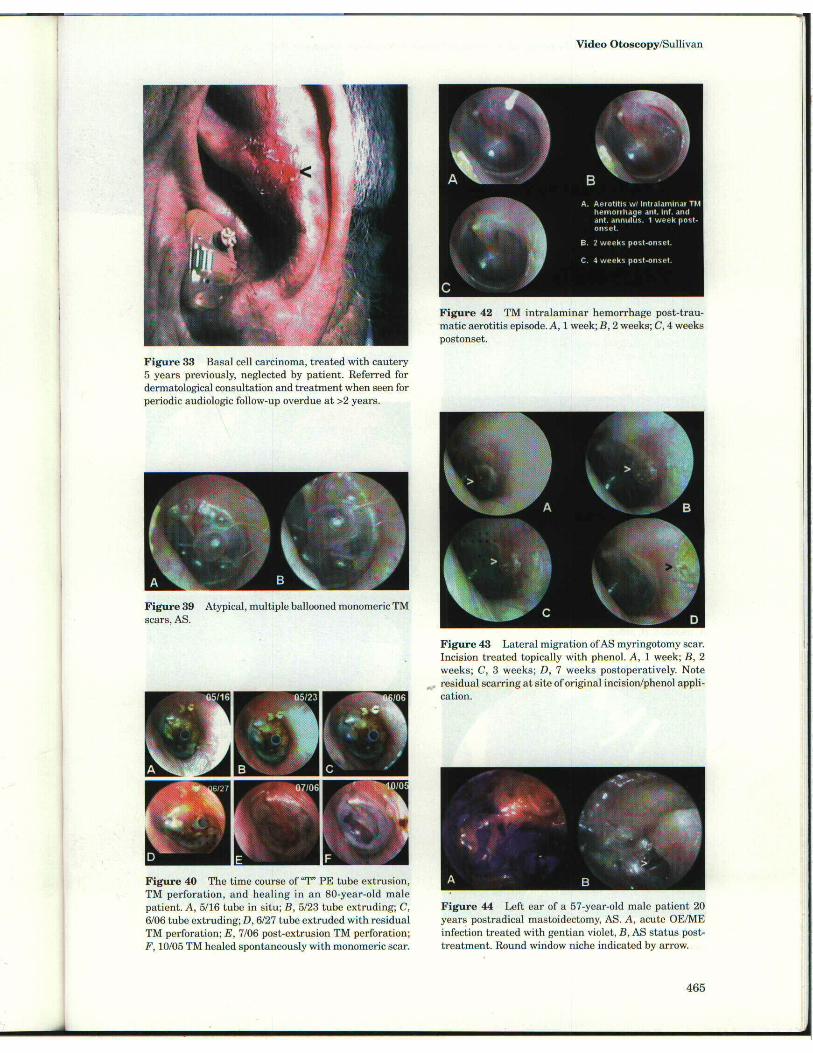
A major point of entry into the professional hearing health care system, the audiologist is uniquely situated to identify pathology requir-ing medical referral, evaluation, and treatment. VO is a tool for visual identification and docu-mentation and serves as a motivational enhance-ment to the patient to seek the audiologically recommended medical consultation (Fig. 33). When forwarded to the ENT or PCP, the VO printout serves to delineate the specific area of concern. In potential hearing aid patients, the pinna and concha, as well as the EAC, should be VO-screened for dermatological abnormalities. The EAC and TM should be examined for con-ditions that not only influence the fitting of a hearing aid but that may require medical atten-tion . Even eustachian tube-related problems may be observed dynamically via VO. Figure 34 demonstrates the consequences of a patulous eustachian tube note on VO. The degree of TM displacement, in response to Valsalva, Toynbee, and Politzer maneuvers, can be observed .
PHYSICL4,N COMMUNICATION/ TELEMEDICINE
O is an invaluable tool for communicating clinical information about the ear. However,
`STEM BASIC 1fO' SYSTEM`
VIDEO OTO-MACROSCOPE (VOM) Figure 17 Block diagram of a com-
prehensive analog/digital video oto-scopy system. Dashed lines represent optional/alternative component inter-connections.
IMAGE ARCHIVING COMPUTER
COLOR PRINTER' HARD DISK STORAGE ]
F-MODEM I
CC MPUTER
MONLTOR >MP
453
Journal of the American Academy of Audiology/Volume 8, Number 6, December 1997
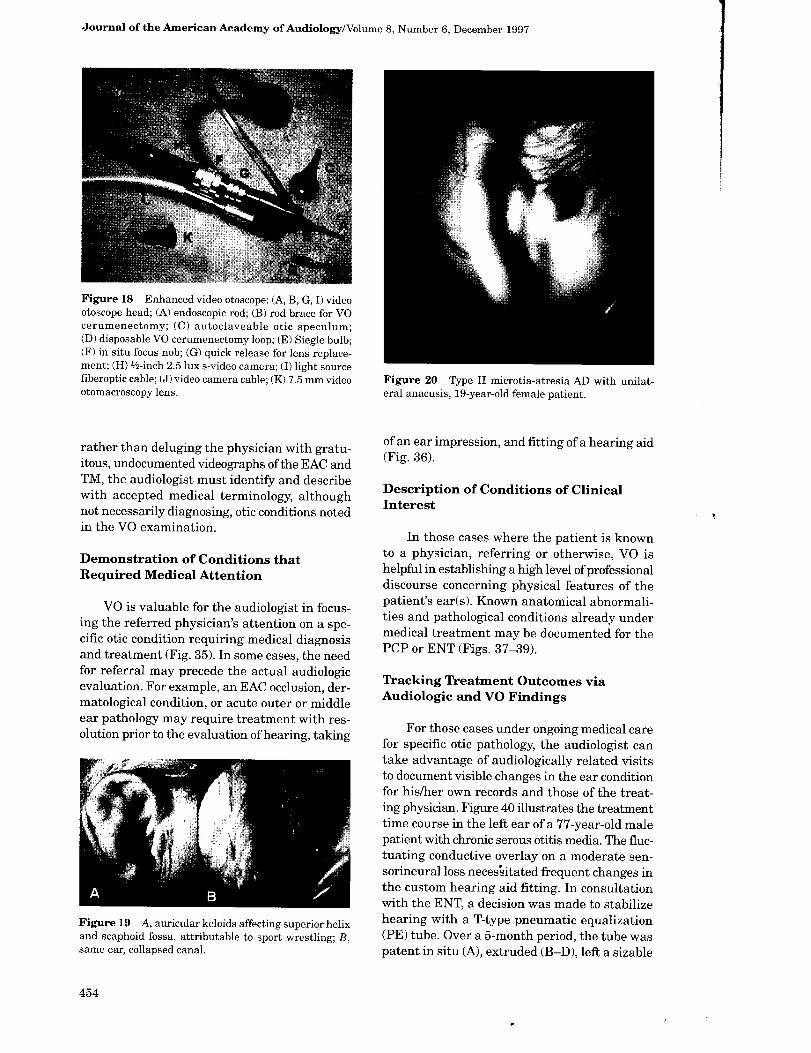
Figure 18 Enhanced video otoscope : (A, B, G, I) video otoscope head ; (A) endoscopic rod; (B) rod brace for VO cerumenectomy; (C) autoclaveable otic speculum ; (D) disposable VO cerumenectomy loop; (E) Siegle bulb ; (F) in situ focus nob; (G) quick release for lens replace-ment ; (H)'-/z-inch 2.5 lux s-video camera ; (I) light source fiberoptic cable; (J) video camera cable; (K) 7.5 mm video otomacroscopy lens .
Figure 20 Type II microtia-atresia AD with unilat-eral anacusis, 19-year-old female patient .
rather than deluging the physician with gratu-itous, undocumented videographs of the EAC and TM, the audiologist must identify and describe with accepted medical terminology, although not necessarily diagnosing, otic conditions noted in the VO examination.
Demonstration of Conditions that Required Medical Attention
VO is valuable for the audiologist in focus-ing the referred physician's attention on a spe-cific otic condition requiring medical diagnosis and treatment (Fig . 35). In some cases, the need for referral may precede the actual audio ogic evaluation . For example, an EAC occlusion, der-matological condition, or acute outer or middle ear pathology may require treatment with res-olution prior to the evaluation of hearing, taking
Figure 19 A, auricular keloids affecting superior helix and scaphoid fossa, attributable to sport wrestling; B, same ear, collapsed canal.
of an ear impression, and fitting of a hearing aid (Fig. 36).
Description of Conditions of Clinical Interest
In those cases where the patient is known to a physician, referring or otherwise, VO is helpful in establishing a high level of professional discourse concerning physical features of the patient's ear(s) . Known anatomical abnormali-ties and pathological conditions already under medical treatment may be documented for the PCP or ENT (Figs. 37-39) .
Tracking Treatment Outcomes via Audiologic and VO Findings
For those cases under ongoing medical care for specific otic pathology, the audiologist can take advantage of audiologically related visits to document visible changes in the ear condition for his/her own records and those of the treat-ing physician. Figure 40 illustrates the treatment time course in the left ear of a 77-year-old male patient with chronic serous otitis media. The fluc-tuating conductive overlay on a moderate sen-sorineural loss neces'sitated frequent changes in the custom hearing aid fitting. In consultation with the ENT, a decision was made to stabilize hearing with a T-type pneumatic equalization (PE) tube . Over a 5-month period, the tube was patent in situ (A), extruded (B-D), left a sizable
454
Video Otoscopy/Sullivan
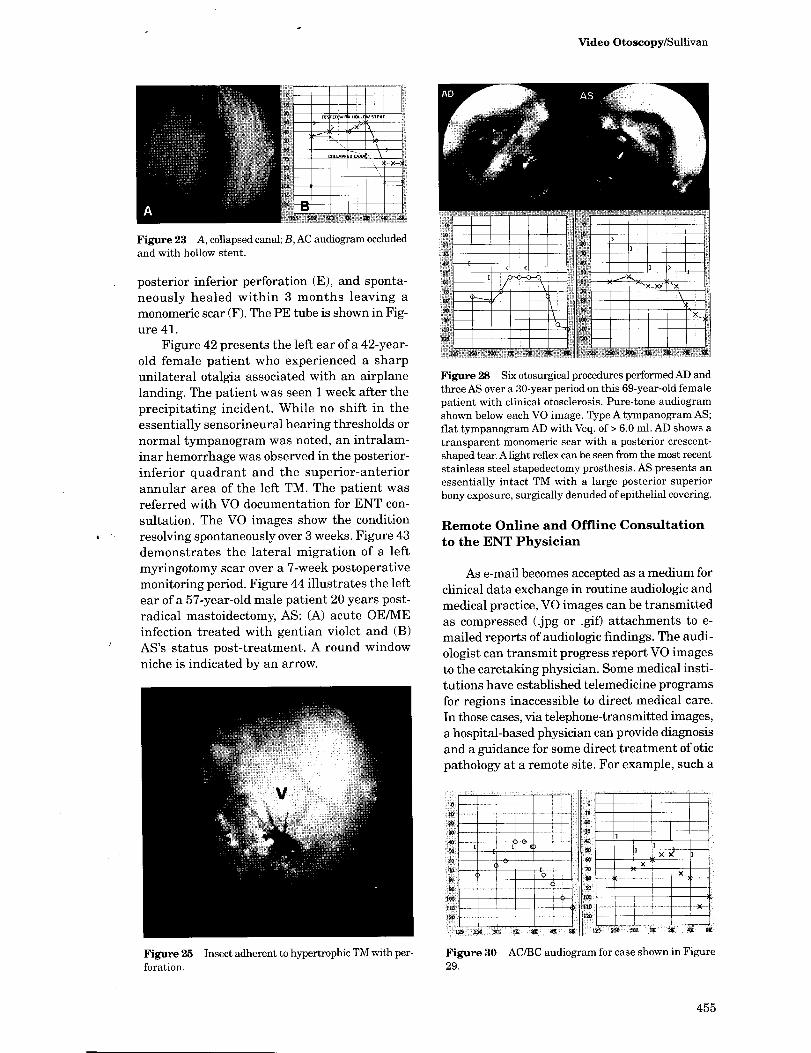
Figure 23 A, collapsed canal; B, AC audiogram occluded and with hollow stent.
posterior inferior perforation (E), and sponta-neously healed within 3 months leaving a monomeric scar (F). The PE tube is shown in Fig-ure 41 .
Figure 42 presents the left ear of a 42-year-old female patient who experienced a sharp unilateral otalgia associated with an airplane landing. The patient was seen 1 week after the precipitating incident . While no shift in the essentially sensorineural hearing thresholds or normal tympanogram was noted, an intralam-inar hemorrhage was observed in the posterior-inferior quadrant and the superior-anterior annular area of the left TM . The patient was referred with VO documentation for ENT con-sultation. The VO images show the condition resolving spontaneously over 3 weeks. Figure 43 demonstrates the lateral migration of a left myringotomy scar over a 7-week postoperative monitoring period. Figure 44 illustrates the left ear of a 57-year-old male patient 20 years post-radical mastoidectomy, AS: (A) acute OE/ME infection treated with gentian violet and (B) AS's status post-treatment . A round window niche is indicated by an arrow.
Figure 25 Insect adherent to hypertrophic TM with per-foration.
< < r
u
Figure 28 Six otosurgical procedures performed AD and three AS over a 30-year period on this 69-year-old female patient with clinical otosclerosis . Pure-tone audiogram shown below each VO image. Type A tympanogram AS; flat tympanogram AD with Veq. of > 6.0 ml . AD shows a transparent monomeric scar with a posterior crescent-shaped tear. Alight reflex can be seen from the most recent stainless steel stapedectomy prosthesis . AS presents an essentially intact TM with a large posterior superior bony exposure, surgically denuded of epithelial covering .
Remote Online and Offline Consultation to the ENT Physician
As e-mail becomes accepted as a medium for clinical data exchange in routine audiologic and medical practice, VO images can be transmitted as compressed (jpg or .gif) attachments to e-mailed reports of audiologic findings . The audi-ologist can transmit progress report VO images to the caretaking physician. Some medical insti-tutions have established telemedicine programs for regions inaccessible to direct medical care . In those cases, via telephone-transmitted images, a hospital-based physician can provide diagnosis and a guidance for some direct treatment of otic pathology at a remote site . For example, such a
Figure 30 AC/BC audiogram for case shown in Figure 29 .
455
Journal of the American Academy of Audiology/Volume 8, Number 6, December 1997
mmho 10,
AD Veq (PVT)= 2.6m1
-600 -50a -406 -300 -200 -109 a 100 200 300 daPa
mmho 30T
2 .5
2 .6
15
10
0.5
AS Veq (PVT)= 1.7m1
00600 -500 -400 -300 -200 100 0 100 200 30a daPa
Figure 31 Tympanometry for case shown in Figure 29 .
program employing audiologists at remote sites in northern Maine is described on the Internet <http://www.maine.edu/-ITHCRA/ithcra/SProj7/ index.htm> (Sechrest et al, undated) .
Figure 34 VO strobe ofAD over one nasal respiratory
cycle ; 75-year-old female patient with complaint of intractable clicking tinnitus on AD . Absent manubrium mallei and posteriorly displaced incus process. long . Because of a hyperpatulous eustachian tube, the latter (incus) would come in contact with the TM coinciding with the click (A, D) . The patient developed a compensatory mouth-breathing strategy. A 1-mm vented canal aid was fitted for the 45-dB sensorineural hearing loss, provid-ing both hearing and tinnitus relief.
Figure 35 Self-treated, nonhealing lesion of the right
lobule, 85-year-old female patient. Referred to a derma-
tologist who diagnosed and successfully treated impetigo .
HEARING AID SELECTION AND FITTING APPLICATIONS
H earing aid technology has advanced to such an extent that the dispensing audiologist
is more likely to encounter morphologically based fitting problems than challenges of an electroacoustic nature . VOE and VOM are valu-able techniques in this regard .
Hearing Aid Morphology Preselection
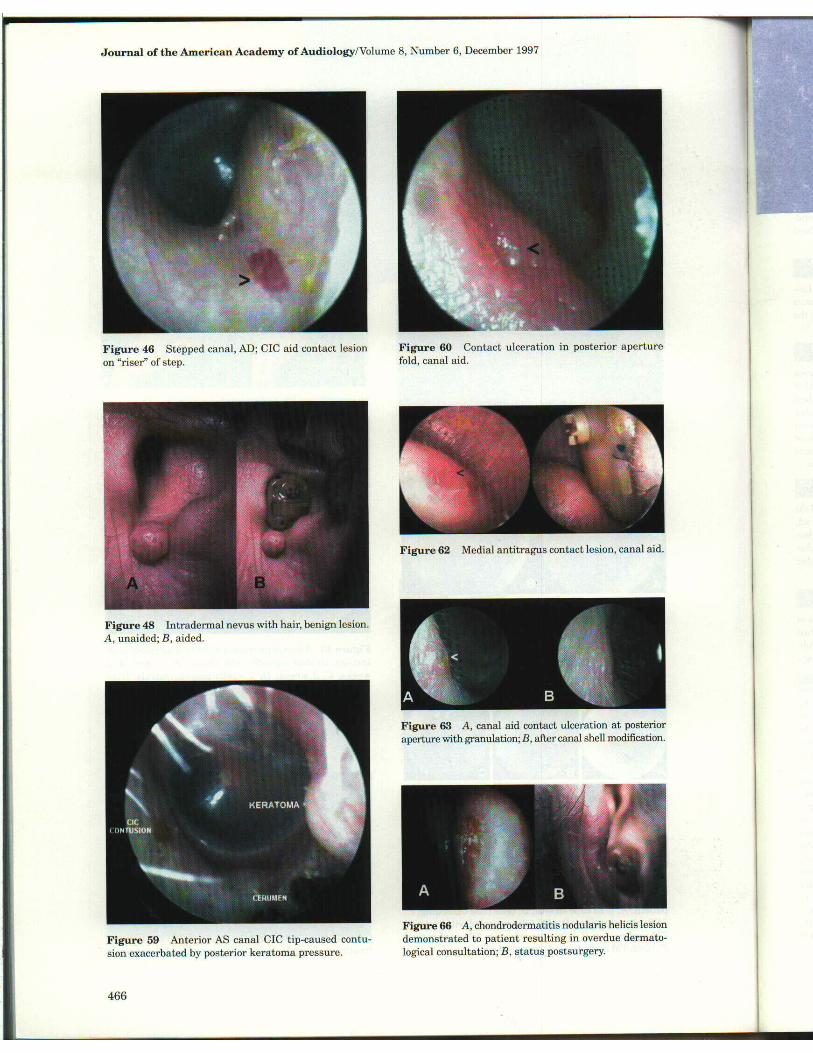
Various anatomical variations can prevail in the EAC that may rule out certain hearing aid morphologies for one or both ears . Natural vari-ations of this nature include exostoses (Fig . 45), collapsed and tortuous canals (the latter often more zetoid than sigmoid), and stepped canals (Fig . 46), which demarcate sharply from an ample cartilaginous portion to an off-axis, nar-rowed bony segment. VO can be used to observe dynamically the impact of temporomandibular joint (TMJ) and facial muscle activity on the lateral EAC anterior-posterior (A-P) dimensions (Fig . 47). Congenital deformities of the pinna, concha, and canal can be visually explored for fitting potential. Pathological conditions to be considered include keratomas, other neoplasms
Figure 36 Squamous cell carcinoma referred by audi-
ologist; diagnosed and treated by dermatologist prior to
hearing aid fitting .
456
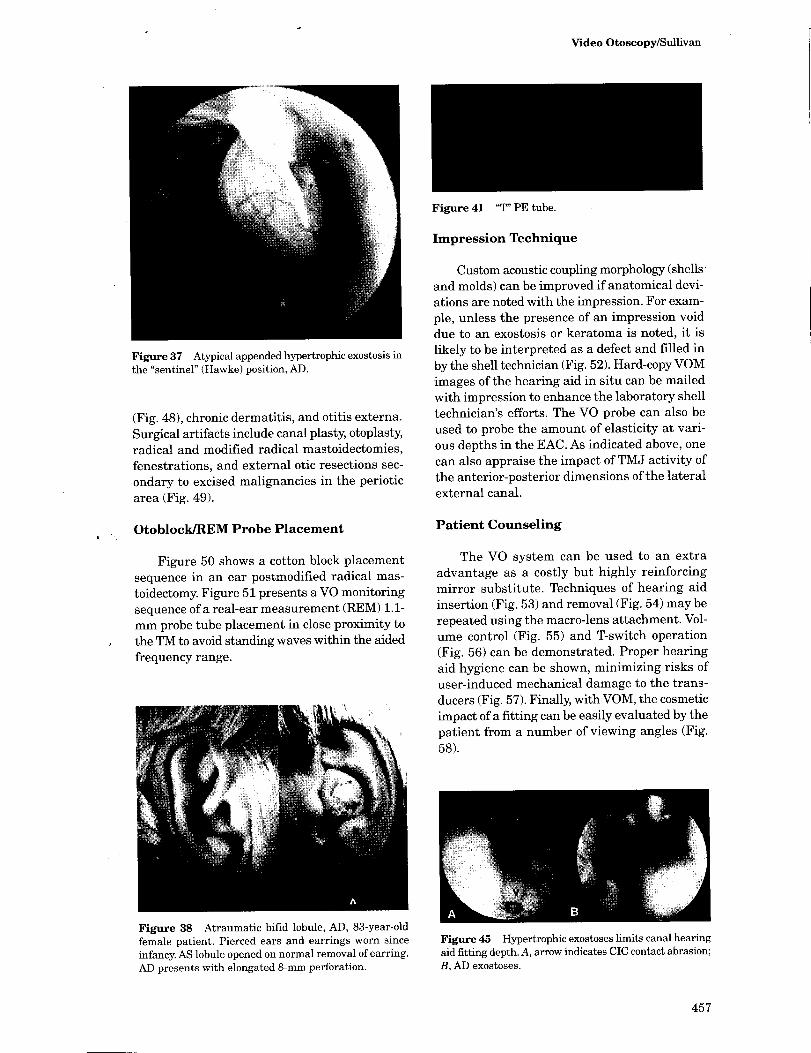
Figure 37 Atypical appended hypertrophic exostosis in the "sentinel" (Hawke) position, AD .
(Fig. 48), chronic dermatitis, and otitis externa. Surgical artifacts include canal plasty, otoplasty, radical and modified radical mastoidectomies, fenestrations, and external otic resections sec-ondary to excised malignancies in the periotic area (Fig . 49).
Otoblock/REM Probe Placement
Figure 50 shows a cotton block placement sequence in an ear postmodified radical mas-toidectomy. Figure 51 presents a VO monitoring sequence of a real-ear measurement (REM) 1.1-mm probe tube placement in close proximity to the TM to avoid standing waves within the aided frequency range.
Figure 38 Atraumatic bifid lobule, AD, 83-year-old female patient. Pierced ears and earrings worn since infancy. AS lobule opened on normal removal of earring. AD presents with elongated 8-mm perforation .
Video Otoscopy/Sullivan
Figure 41 "T" PE tube .
Impression Technique
Custom acoustic coupling morphology (shells and molds) can be improved if anatomical devi-ations are noted with the impression . For exam-ple, unless the presence of an impression void due to an exostosis or keratoma is noted, it is likely to be interpreted as a defect and filled in by the shell technician (Fig . 52). Hard-copy VOM images of the hearing aid in situ can be mailed with impression to enhance the laboratory shell technician's efforts. The VO probe can also be used to probe the amount of elasticity at vari-ous depths in the EAC. As indicated above, one can also appraise the impact of TMJ activity of the anterior-posterior dimensions of the lateral external canal.
Patient Counseling
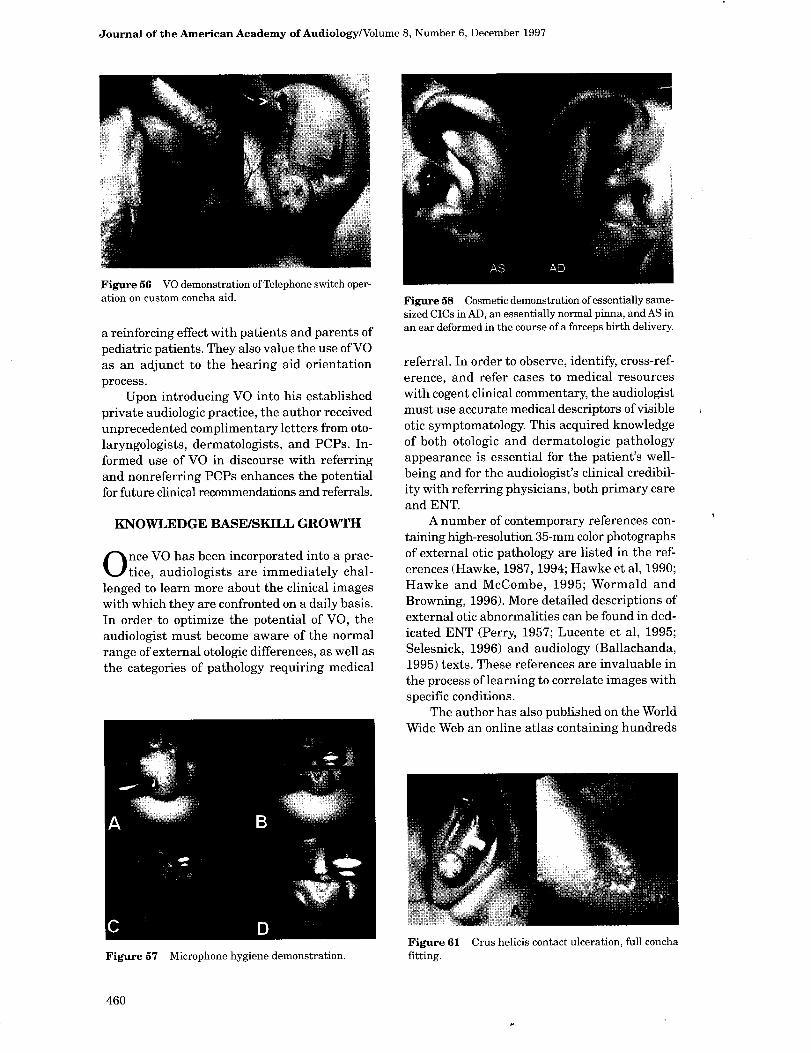
The VO system can be used to an extra advantage as a costly but highly reinforcing mirror substitute . Techniques of hearing aid insertion (Fig . 53) and removal (Fig . 54) may be repeated using the macro-lens attachment . Vol-ume control (Fig . 55) and T-switch operation (Fig . 56) can be demonstrated . Proper hearing aid hygiene can be shown, minimizing risks of user-induced mechanical damage to the trans-ducers (Fig . 57). Finally, with VOM, the cosmetic impact of a fitting can be easily evaluated by the patient from a number of viewing angles (Fig . 58).
Figure 45 Hypertrophic exostoses limits canal hearing
aid fitting depth. A, arrow indicates CIC contact abrasion ; B, AD exostoses.
457
Journal of the American Academy of Audiology/Volume 8, Number 6, December 1997
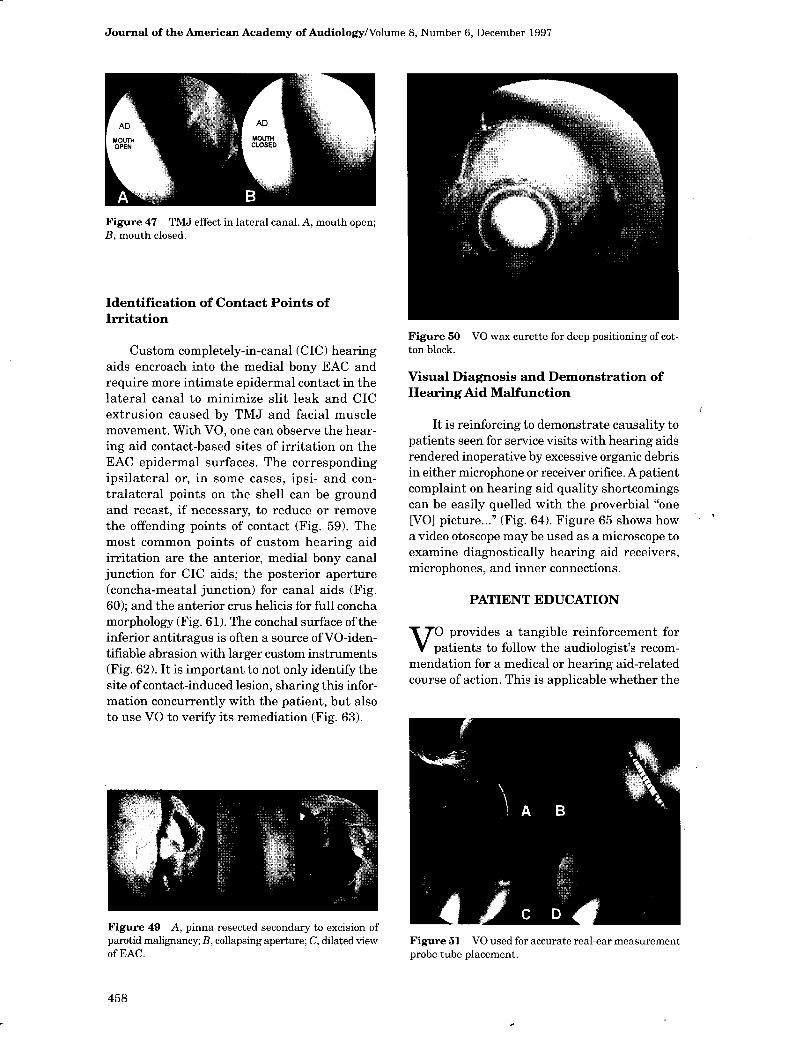
Figure 47 TMJ effect in lateral canal. A, mouth open ; B, mouth closed.
Identification of Contact Points of Irritation
Custom completely-in-canal (CIC) hearing aids encroach into the medial bony EAC and require more intimate epidermal contact in the lateral canal to minimize slit leak and CIC extrusion caused by TMJ and facial muscle movement . With VO, one can observe the hear-ing aid contact-based sites of irritation on the EAC epidermal surfaces . The corresponding ipsilateral or, in some cases, ipsi- and con-tralateral points on the shell can be ground and recast, if necessary, to reduce or remove the offending points of contact (Fig . 59). The most common points of custom hearing aid irritation are the anterior, medial bony canal junction for CIC aids ; the posterior aperture (concha-meatal junction) for canal aids (Fig . 60); and the anterior crus helicis for full concha morphology (Fig. 61). The conchal surface of the inferior antitragus is often a source of VO-iden-tifiable abrasion with larger custom instruments (Fig . 62). It is important to not only identify the site of contact-induced lesion, sharing this infor-mation concurrently with the patient, but also to use VO to verify its remediation (Fig . 63).
Figure 49 A, pinna resected secondary to excision of parotid malignancy; B, collapsing aperture ; C, dilated view of EAC .
Figure 50 VO wax curette for deep positioning of cot-ton block.
Visual Diagnosis and Demonstration of Hearing Aid Malfunction
It is reinforcing to demonstrate causality to patients seen for service visits with hearing aids rendered inoperative by excessive organic debris in either microphone or receiver orifice. A patient complaint on hearing aid quality shortcomings can be easily quelled with the proverbial "one [V0] picture. . ." (Fig. 64) . Figure 65 shows how a video otoscope may be used as a microscope to examine diagnostically hearing aid receivers, microphones, and inner connections.
PATIENT EDUCATION
V 0 provides a tangible reinforcement for patients to follow the audiologist's recom-
mendation for a medical or hearing aid-related course of action . This is applicable whether the
Figure 51 VO used for accurate real-ear measurement probe tube placement.
458
Video Otoscopy/Sullivan
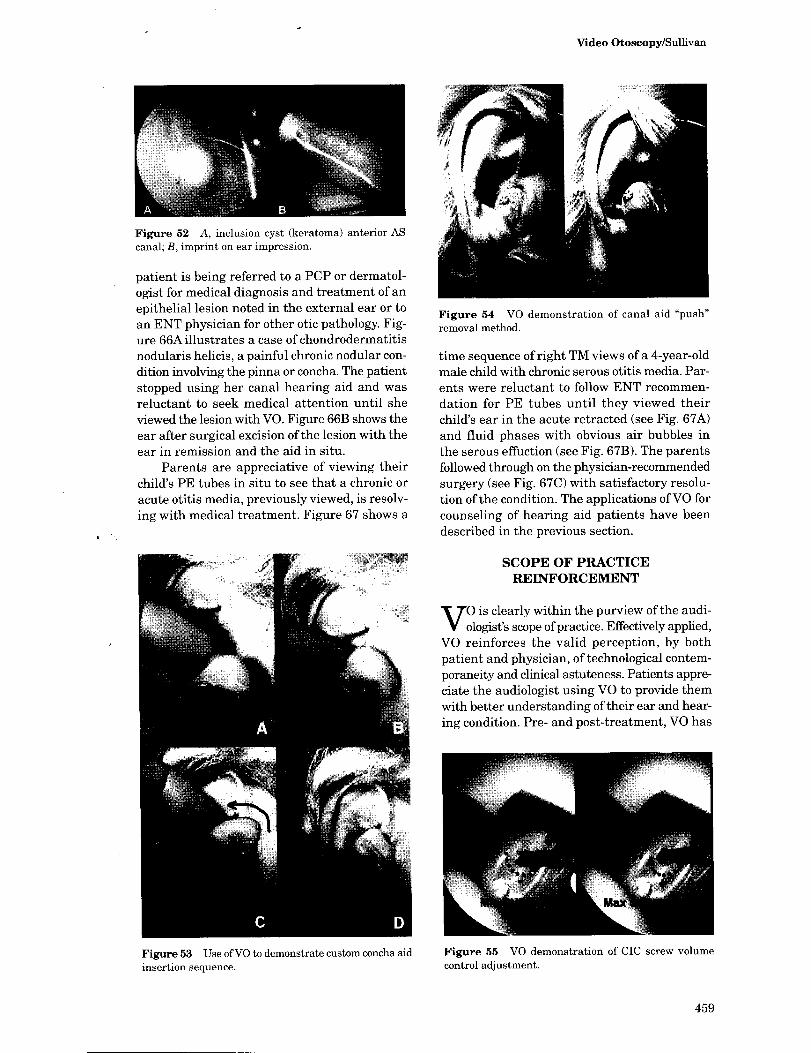
Figure 52 A, inclusion cyst (keratoma) anterior AS canal; B, imprint on ear impression .
patient is being referred to a PCP or dermatol-ogist for medical diagnosis and treatment of an epithelial lesion noted in the external ear or to an ENT physician for other otic pathology. Fig-ure 66A illustrates a case of chondrodermatitis nodularis helicis, a painful chronic nodular con-dition involving the pinna or concha . The patient stopped using her canal hearing aid and was reluctant to seek medical attention until she viewed the lesion with VO. Figure 66B shows the ear after surgical excision of the lesion with the ear in remission and the aid in situ .
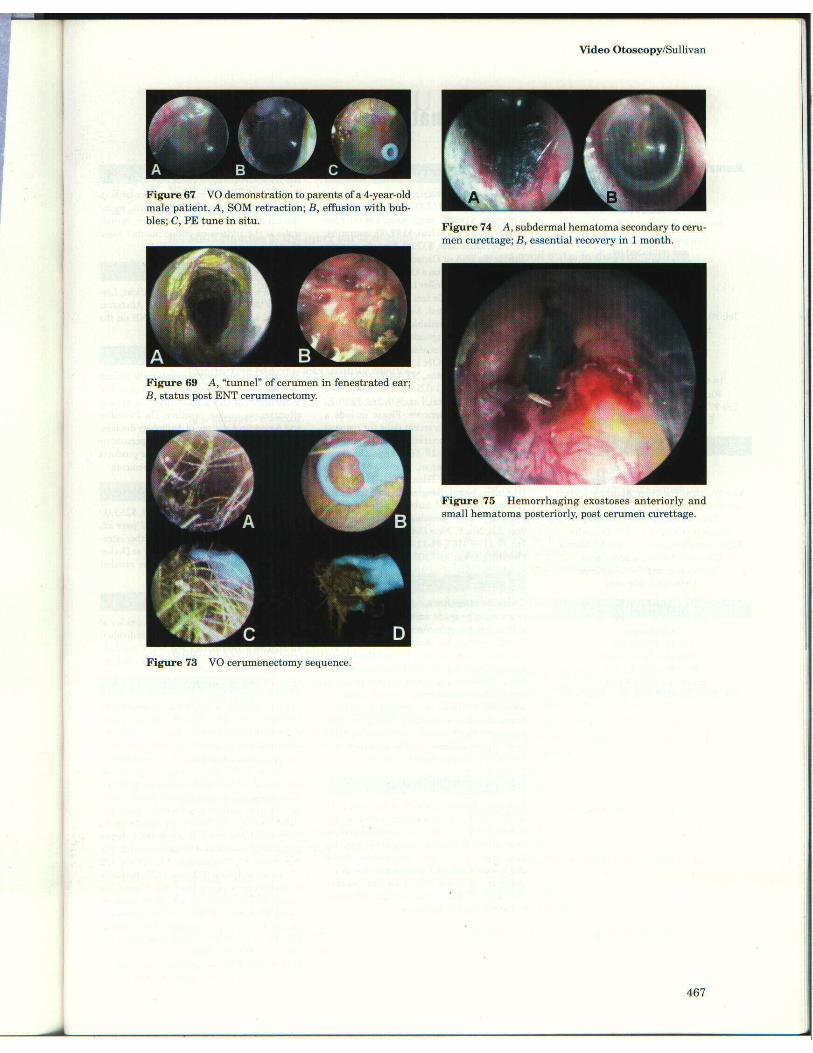
Parents are appreciative of viewing their child's PE tubes in situ to see that a chronic or acute otitis media, previously viewed, is resolv-ing with medical treatment. Figure 67 shows a
Figure 54 VO demonstration of canal aid "push" removal method .
time sequence of right TM views of a 4-year-old male child with chronic serous otitis media. Par-ents were reluctant to follow ENT recommen-dation for PE tubes until they viewed their child's ear in the acute retracted (see Fig. 67A) and fluid phases with obvious air bubbles in the serous effuction (see Fig. 67B). The parents followed through on the physician-recommended surgery (see Fig. 67C) with satisfactory resolu-tion of the condition. The applications of VO for counseling of hearing aid patients have been described in the previous section.
Figure 53 Use of VO to demonstrate custom concha aid insertion sequence .
SCOPE OF PRACTICE REINFORCEMENT
V is clearly within the purview of the audi-
001ogist's scope of practice . Effectively applied, VO reinforces the valid perception, by both patient and physician, of technological contem-poraneity and clinical astuteness . Patients appre-ciate the audiologist using VO to provide them with better understanding of their ear and hear-ing condition. Pre- and post-treatment, VO has
Figure 55 VO demonstration of CIC screw volume control adjustment .
459
Journal of the American Academy of Audiology/Volume 8, Number 6, December 1997
Figure 56 VO demonstration of Telephone switch oper-ation on custom concha aid.
a reinforcing effect with patients and parents of pediatric patients . They also value the use of VO as an adjunct to the hearing aid orientation process.
Upon introducing VO into his established private audiologic practice, the author received unprecedented complimentary letters from oto-laryngologists, dermatologists, and PCPs. In-formed use of VO in discourse with referring and nonreferring PCPs enhances the potential for future clinical recommendations and referrals .
KNOWLEDGE BASE/SKILL GROWTH
0 nce VO has been incorporated into a prac-tice, audiologists are immediately chal-
lenged to learn more about the clinical images with which they are confronted on a daily basis. In order to optimize the potential of VO, the audiologist must become aware of the normal range of external otologic differences, as well as the categories of pathology requiring medical
Figure 57 Microphone hygiene demonstration.
Figure 58 Cosmetic demonstration of essentially same-sized CICs in AD, an essentially normal pinna, and AS in an ear deformed in the course of a forceps birth delivery.
referral . In order to observe, identify, cross-ref-erence, and refer cases to medical resources with cogent clinical commentary, the audiologist must use accurate medical descriptors of visible otic symptomatology. This acquired knowledge of both otologic and dermatologic pathology appearance is essential for the patient's well-being and for the audiologist's clinical credibil-ity with referring physicians, both primary care and ENT.
A number of contemporary references con-taining high-resolution 35-mm color photographs of external otic pathology are listed in the ref-erences (Hawke, 1987, 1994 ; Hawke et al, 1990 ; Hawke and McCombe, 1995; Wormald and Browning, 1996). More detailed descriptions of external otic abnormalities can be found in ded-icated ENT (Perry, 1957 ; Lucente et al, 1995 ; Selesnick, 1996) and audiology (Ballachanda, 1995) texts. These references are invaluable in the process of learning to correlate images with specific conditions .
The author has also published on the World Wide Web an online atlas containing hundreds
Figure 61 Crus helicis contact ulceration, full concha fitting.
460
Video Otoscopy/Sullivan
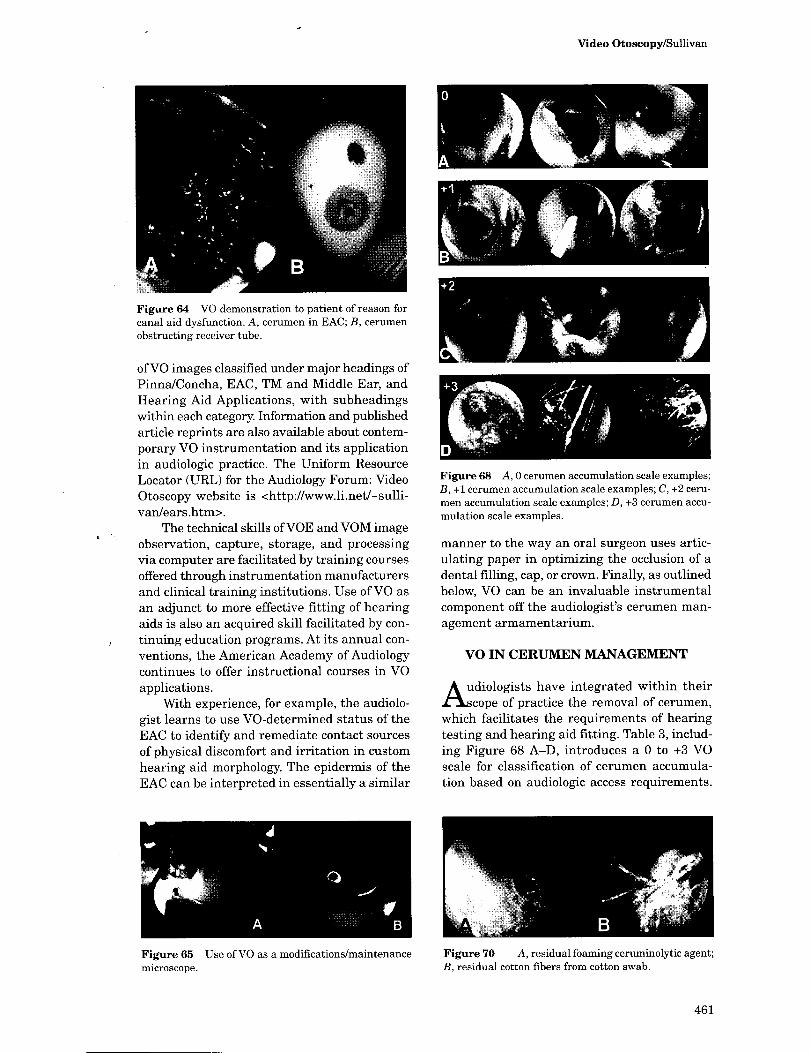
Figure 64 VO demonstration to patient of reason for canal aid dysfunction. A, cerumen in EAC; B, cerumen obstructing receiver tube .
of VO images classified under major headings of Pinna/Concha, EAC, TM and Middle Ear, and Hearing Aid Applications, with subheadings within each category. Information and published article reprints are also available about contem-porary VO instrumentation and its application in audiologic practice . The Uniform Resource Locator (URL) for the Audiology Forum: Video Otoscopy website is <http://www.li .net/-sulli-van/ears .htm>.
The technical skills of VOE and VOM image observation, capture, storage, and processing via computer are facilitated by training courses offered through instrumentation manufacturers and clinical training institutions . Use of VO as an adjunct to more effective fitting of hearing aids is also an acquired skill facilitated by con-tinuing education programs . At its annual con-ventions, the American Academy of Audiology continues to offer instructional courses in VO applications .
With experience, for example, the audiolo-gist learns to use VO-determined status of the EAC to identify and remediate contact sources of physical discomfort and irritation in custom hearing aid morphology. The epidermis of the EAC can be interpreted in essentially a similar
Figure 68 A, 0 cerumen accumulation scale examples ; B, +1 cerumen accumulation scale examples ; C, +2 ceru-men accumulation scale examples ; D, +3 cerumen accu-mulation scale examples .
manner to the way an oral surgeon uses artic-ulating paper in optimizing the occlusion of a dental filling, cap, or crown. Finally, as outlined below, VO can be an invaluable instrumental component off the audiologist's cerumen man-agement armamentarium.
VO IN CERUMEN MANAGEMENT
A udiologists have integrated within their ;cope of practice the removal of cerumen,
which facilitates the requirements of hearing testing and hearing aid fitting. Table 3, includ-ing Figure 68 A-D, introduces a 0 to +3 VO scale for classification of cerumen accumula-tion based on audiologic access requirements .
Figure 65 Use of VO as a modifications/maintenance microscope .
Figure 70 A, residual foaming ceruminolytic agent; B, residual cotton fibers from cotton swab .
461
Journal of the American Academy of Audiology/Volume 8, Number 6, December 1997
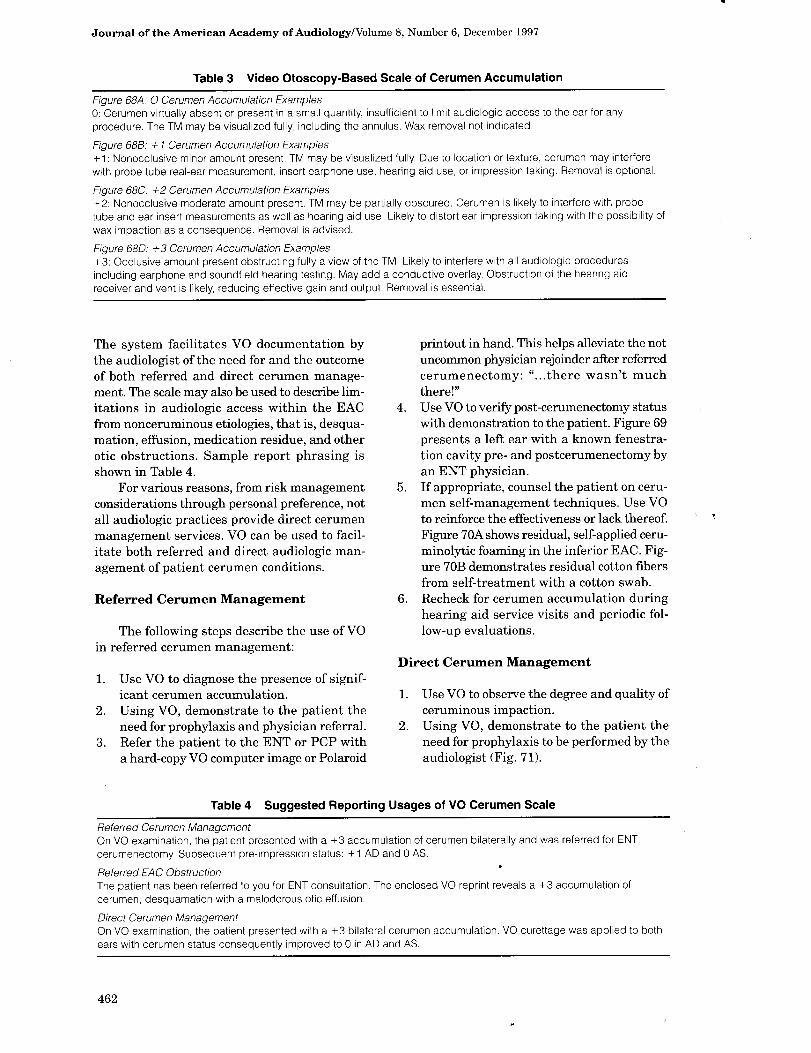
Table 3 Video Otoscopy-Based Scale of Cerumen Accumulation
Figure 68A. O Cerumen Accumulation Examples 0 : Cerumen virtually absent or present in a small quantity, insufficient to limit audiologic access to the ear for any procedure . The TM may be visualized fully, including the annulus . Wax removal not indicated .
Figure 688 : + 1 Cerumen Accumulation Examples +1 : Nonocclusive minor amount present . TM may be visualized fully . Due to location or texture, cerumen may interfere with probe tube real-ear measurement, insert earphone use, hearing aid use, or impression taking . Removal is optional .
Figure 68C: +2 Cerumen Accumulation Examples +2 : Nonocclusive moderate amount present . TM may be partially obscured . Cerumen is likely to interfere with probe tube and ear insert measurements as well as hearing aid use . Likely to distort ear impression taking with the possibility of wax impaction as a consequence . Removal is advised .
Figure 68D : +3 Cerumen Accumulation Examples +3 : Occlusive amount present obstructing fully a view of the TM . Likely to interfere with all audiologic procedures including earphone and soundfield hearing testing . May add a conductive overlay. Obstruction of the hearing aid receiver and vent is likely, reducing effective gain and output . Removal is essential .
The system facilitates VO documentation by the audiologist of the need for and the outcome of both referred and direct cerumen manage-ment . The scale may also be used to describe lim-itations in audiologic access within the EAC from nonceruminous etiologies, that is, desqua-mation, effusion, medication residue, and other otic obstructions . Sample report phrasing is shown in Table 4.
For various reasons, from risk management considerations through personal preference, not all audiologic practices provide direct cerumen management services . VO can be used to facil-itate both referred and direct audiologic man-agement of patient cerumen conditions .
Referred Cerumen Management
The following steps describe the use of VO in referred cerumen management :
1. Use VO to diagnose the presence of signif-icant cerumen accumulation .
2 . Using VO, demonstrate to the patient the need for prophylaxis and physician referral .
3. Refer the patient to the ENT or PCP with a hard-copy VO computer image or Polaroid
4.
5.
6.
printout in hand . This helps alleviate the not uncommon physician rejoinder after referred cerumenectomy: ". . .there wasn't much there!" Use VO to verify post-cerumenectomy status with demonstration to the patient. Figure 69 presents a left ear with a known fenestra-tion cavity pre- and postcerumenectomy by an ENT physician. If appropriate, counsel the patient on ceru-men self-management techniques . Use VO to reinforce the effectiveness or lack thereof. Figure 70A shows residual, self-applied ceru-minolytic foaming in the inferior EAC . Fig-ure 70B demonstrates residual cotton fibers from self-treatment with a cotton swab . Recheck for cerumen accumulation during hearing aid service visits and periodic fol-low-up evaluations .
Direct Cerumen Management
1.
2 .
Use VO to observe the degree and quality of ceruminous impaction. Using VO, demonstrate to the patient the need for prophylaxis to be performed by the audiologist (Fig . 71) .
Table 4 Suggested Reporting Usages of VO Cerumen Scale
Referred Cerumen Management On VO examination, the patient presented with a +3 accumulation of cerumen bilaterally and was referred for ENT cerumenectomy. Subsequent pre-impression status : +1 AD and 0 AS .
Referred EAC Obstruction The patient has been referred to you for ENT consultation . The enclosed VO reprint reveals a +3 accumulation of cerumen, desquamation with a malodorous otic effusion .
Direct Cerumen Management On VO examination, the patient presented with a +3 bilateral cerumen accumulation . VO curettage was applied to both ears with cerumen status consequently improved to 0 in AD and AS .
462

Video Otoscopy/Sullivan
Acknowledgment. Video otoscopy images accompany-ing this article remain the property of the author; copy-right 1995, 1996, 1997 . The Journal of the American Academy of Audiology is given permission to use these images in this context.
REFERENCES
Figure 71 A, +2 cerumen accumulation; B, status post audiologist VO cerumenectomy.
3 . Document with computer-stored or Polaroid image and secure patient approval for the procedure.
4. Based on VO observation, determine the most appropriate technique or combination of techniques for cerumen extraction, including curettage, lavage, suction, and VO curettage (Figs. 72-73), presoftening with a wetting agent.
5. Verify effectiveness of extraction and docu-ment the outcome with VO, especially if there was pain or bleeding in the EAC . Fig-ure 74 illustrates a sizable AD subdermal hematoma 24 hours and 1 month after (referred) cerumen curettage. Figure 75 shows an AD postcerumenectomy (referred) with a small hematoma and contusion with bleeding in an area with multiple exostoses.
6. Routinely monitor cerumen status during routine and follow-up office visits .
The use of VO in either referred or direct cerumen management enhances both the pro-fessional scope and quality of audiologic practice .
Figure 72 VO cerumen curettes . A, Sullivan speculum loop; B, rod-mounted wax loop .
Bacon G. (1906) . Manual of Otology. New York: Lea Brothers .
Ballachanda B. (1995) . The Human Ear Canal. San Diego: Singular Publishing Group.
Bruhl G, PolitzerA. (1902) . Atlas and Epitome of Otology. Philadelphia : WB Saunders .
Hawke M. (1987) . Clinical Pocket Guide to Ear Disease. Philadelphia : Lea and Febiger.
Hawke M. (1994) . Otitis Media: A Pocket Guide. Toronto: Smith, Kline, Beecham; Decker Periodicals.
Hawke M, Keene M, Alberti P. (1990) . Clinical Otoscopy: An Introduction To Ear Diseases. Edinburgh: Churchill, Livingstone.
Hawke M, McCombe A. (1995) . Diseases of the Ear: A Pocket Atlas. Starkey Laboratories, Manticore Communications .
Laurens G. (1919) . Oto-Rhino-Laryngology for the Student and Practitioner. New York: William Wood .
Lucente DF, Lawson W, Novick N. (1995) . The External Ear. Philadelphia: WB Saunders .
Perry E . (1957) . The Human Ear Canal. Springfield, IL: CC Thomas .
Sechrest A, Peacock M, Yonvitz A. Remote hearing diag-nosis: evaluation and assessment in remote settings (EARS) . [Internet abstract] . A project of the University of Maine, Orono; Dept. of Communication Disorders . (Undated) <http ://www.maine.edu/-ITHCRA/ithcra/ SProj 7hndex.htm>
Selesnick S, ed. (1996) . Diseases of the External Auditory Canal. Otolaryngology Clinics, 26, #5 . Philadelphia : WB Saunders .
Sullivan R. (1993) . How video otoscopy benefits hearing health care practice . Hear Instrum 44:14-17 .
Sullivan R. (1995a) . Audiologic applications of video oto-scopy. Hear J 48:10-ff.
Sullivan R. (1995b). Video otoscopy: basic and advanced systems. Hear Rev 2:12-16 .
Sullivan R. (1997) . Video otoscopy in hearing aid fitting . Hear J 50:40.
Wormald P, Browning G. (1996) . Otoscopy: A Structured Approach. San Diego: Singular Publishing Group.