Embed Size (px)
Citation preview

VICTORIAN ALCOHOL AND DRUG ASSOCIATION
CALD AOD Project:
Final report
March 2016
VAADA Vision
A Victorian community in which
the harms associated with drug
use are reduced and general
health and wellbeing is
promoted.
VAADA Objectives
To provide leadership,
representation, advocacy and
information to the alcohol and
other drug and related sectors.
Address: 211 Victoria Parade
Collingwood VIC 3066
P: 03 9412 5600
F: 03 9416 2085
www.vaada.org.au
ABN 19 039 293 679

2
Acknowledgements
The Victorian Alcohol and Drug Association (VAADA) wishes to thank all the people who have
been involved in and supported this project, without whom it would not have been possible to
proceed in any meaningful way. We would like to acknowledge the culturally and linguistically
diverse (CALD) liaison personnel and partner agencies who worked with us to identify the specific
health literacy needs of their respective communities. Without their efforts it would have been
extremely difficult to generate much interest in the project amongst the various CALD
communities, nor obtain much of the information we needed to meet the project objectives.
They include:
Nail Aykan, Ramzi Elsayed, Sheikh Moustapha Sarakibi and Ben Gresham (Islamic Council
of Victoria)
Dawood Baqiri and Tim Andrews (Primary Care Connect)
Tavale Ilalio and Adelle Levi (Bridging Worx)
Jose Consul Gonsalvez (African Communities Foundation Australia)
Bright Chinganya and Selba Luka (Carers of Africa)
Cam Nguyen, Tuong Nguyen and Kim Vu (Australian Vietnamese Women’s Association)
We would also like to recognise the contributions of all the alcohol and other drug (AOD), allied
health and CALD practitioners and other community representatives who participated in the
consultations and other activities undertaken during the project. Their contributions have been
invaluable.
We also thank members of the Project Reference Group (PRG) who we relied on for guidance,
advice and support throughout the project. They include:
Kieran Connolly (Deputy Director Research and Workforce Development – Turning Point
Alcohol and Drug Centre)
Johnny King (Regional Services Coordinator – North West, Centre for Multicultural Youth)
Michal Morris (General Manager – Centre for Culture, Ethnicity and Health and North
Richmond Community Health)
Rebecca Lorains (Chief Executive Officer/Clinical Director – Primary Care Connect)
Rachel Rowe (Senior Research Officer – Drug and Alcohol Multicultural Education Centre)
Joseph Szwarc (Manager, Research and Policy Program – Foundation House)
John Zika (Executive Director – VICSEG New Futures)
Finally, VAADA would like to acknowledge the Victorian Government for funding this project, and
recognise the Victorian Department of Health and Human Services for their support.
The findings contained in this report are indicative (not definitive), incorporating the views of a range of
stakeholders who participated in the project as well as findings drawn from the literature review and follow-up
analysis of available data.
VAADA recommends that you consider the sensitive nature of the material included as well as the potential for
reputational damage to those CALD communities cited if findings were to be misrepresented and taken out of
context.

3
Contents Page
1. INTRODUCTION 6
1.1 About VAADA 6
1.2 CALD AOD Project overview 6
2. EXECUTIVE SUMMARY 7
2.1 Project activities 7
2.2 Project findings 9
2.3 Summary of recommendations 10
2.4 Discussion 12
3. PROJECT ACTIVITIES 14
3.1 Information gathering 14
3.1.1 Targeted literature review 15
3.1.2 CALD and AOD practitioner consultations 16
3.1.3 Selection of target CALD populations and catchments 16
3.1.4 CALD liaison and development of ‘cultural inventories’ 18
3.1.5 Audit of consumer and worker resources 36
3.2 Supporting cross-sector collaboration 38
3.2.1 Initial roundtable discussions 38
3.2.2 Agency site visits 40
3.2.3 Crossing the Cultural Divide – CALD AOD forum 41
4. WORKER AND CONSUMER RESOURCES 42
4.1 AOD practitioner tip sheets 42
4.2 CALD consumer promotional materials 42

4
5. PROJECT FINDINGS AND RECOMMENDATIONS 43
5.1 Project findings and recommendations 43
5.2 Discussion 53
6. REFERENCES 59
APPENDICES
Appendix A Community profile templates (domains of enquiry)
Appendix B Initial roundtable discussions – summary of issues raised
Appendix C CALD AOD forum program and evaluation summary
Appendix D AOD practitioner tip sheets
Appendix E Crossing the Cultural Divide postcards
Appendix F Crossing the Cultural Divide poster
60 – 93

5
List of tables
Table 1. Selected CALD communities and catchments p. 17
Table 2. Initial roundtable discussion – overview p. 39
Table 3. Agency site visit calendar pp. 40 – 41
Table 4. ‘Culturally safe’ service delivery – key features of best practice pp. 55 – 59
Table 5. CALD AOD forum program p. 77
List of diagrams
Figure 1. CALD AOD Project activities overview p. 14
Figure 2. CALD AOD Project timeline p. 15
Figure 3. Cultural inventory structure p. 19

6
1. INTRODUCTION
While the available research indicates that alcohol and other drugs (AOD) use is generally lower
in culturally and linguistically diverse (CALD) communities compared to the general population,
this situation is not universal. Some CALD communities are at increased risk of experiencing AOD
related harms as they are subject to multiple risk factors including, but not limited to, low levels
of health literacy and pre- and post-migration stressors making it harder to adjust to a new
cultural environment. Despite this situation CALD communities are significantly
under-represented in the AOD treatment system.
In a bid to shed light on the reasons for this disparity, while providing insights into what can be
done to improve service outcomes for individuals and families in need of AOD treatment and
support, the Victorian Alcohol and Drug Association (VAADA) has undertaken the CALD AOD
Project.
This final report provides an in-depth overview of the two year project, from its beginning in
January 2014 through to its conclusion in December 2015. Included in the report is a description
of all the key activities undertaken throughout the project, a detailed overview of the findings
and a discussion of the key issues and learnings which have emerged.
At the conclusion of this report are a series of recommendations aimed at enhancing the capacity
of service providers to deliver culturally safe and responsive services to CALD communities, while
at the same time increasing the AOD health literacy of CALD community members.
1.1 About VAADA
VAADA is a peak organisation which aims to reduce the harms associated with AOD use in the
community. VAADA’s membership comprises agencies working in the AOD field, as well as those
individuals who are involved in, or have a specific interest in, prevention, treatment,
rehabilitation or research that minimises the harms caused by AOD.
1.2 CALD AOD Project overview
In January 2014 VAADA commenced work on the CALD AOD Project, a two-year initiative which
arose from the Victorian Government strategy – Reducing the alcohol and drug toll – Victoria’s
Plan 2013 – 2017.
The project aims to support Victorian AOD services to improve outcomes for individuals and
families from CALD communities who are affected by harmful AOD use. More specifically its
objectives were to:
1. Inform improved access to culturally appropriate drug and alcohol information and
services
2. Inform improved cultural competence of staff in AOD treatment services so they can
more effectively work in cross-cultural situations

7
The project was guided by a Project Reference Group (PRG) made up of key stakeholder
representatives and experts from both the CALD and AOD sectors. Membership was drawn from
a range of services across metropolitan and regional catchments, and included individuals with
relevant experience and expertise in the development of CALD AOD initiatives.
The PRG which met on a bi-monthly basis involved representatives from the following
organisations:
Centre for Culture, Ethnicity and Health
Centre for Multicultural Youth
Drug and Alcohol Multicultural Education Centre
Foundation House (also known as the Victorian Foundation for Survivors of Torture)
Primary Care Connect
Turning Point Alcohol and Drug Centre
VICSEG New Futures
Following an extensive consultation process with workers across the state, as well as a review of
the available research, the following five target populations were selected:
1. Afghan Hazara community
2. African communities
3. Arabic-speaking Muslim communities
4. Pacific Islander and Maori (‘Pasifika’) communities
5. Vietnamese community
Investigating the health needs of these communities would form the basis of the second half of
the project.
2. EXECUTIVE SUMMARY
2.1 Project activities
The CALD AOD Project was made up of two broad streams of activity Refer to Figure 1 (page 14) for an overview of these activities. A detailed description of each activity can be found in section 3 (pages 14 – 41). The first stream – information gathering – spanned the entire project and involved four key components:
1. Targeted literature review – used to establish a baseline of information including data on
AOD prevalence and patterns of use within CALD communities, specific health literacy
needs per community, gaps in existing research, service barriers and relevant best
practice initiatives
2. Follow-up consultations – interviews held with CALD and AOD practitioners across the
state (mostly face-to-face) to identify reported AOD patterns of use, identified ‘hot spots’
where substance use is prevalent, barriers and enablers to accessing AOD treatment, and
risk factors increasing the likelihood of AOD harms. Findings from this round of

8
consultations were documented in a report and distributed to participants
3. Selection of target CALD populations – drawing on findings from the literature review
and follow-up consultations, a needs based model was developed. This model was used
to select five target CALD populations (see Table 1 )
4. Development of ‘cultural inventories’ (community profiles) – including but not limited to
information on how each target population is structured (including networks,
communication channels and key organisations within the community), health beliefs
and perceptions of community members and experiences of community members who
have previously accessed AOD treatment (where available)
Note. As part of the follow-up consultations a training needs assessment was also undertaken, focusing on the professional development needs of frontline staff in both AOD treatment services and ethno-specific (CALD) agencies. AOD practitioners were asked to reflect on their cultural competency needs while CALD workers were asked to consider their AOD literacy needs. Findings are included the attached consultation report.
Table 1. Selected CALD communities and catchments
Selected community Catchment
Afghan community (Hazara group) Hume region of Victoria (centred on the City of Greater Shepparton)
African (including Sudanese, Ethiopian, Somali, Togolese and Congolese communities)
Outer east of Melbourne (centred on the City of Greater Dandenong)
Arabic speaking Muslim communities Inner and outer north of Melbourne (centred on the City of Hume)
Pacific Islander and Maori communities (including Maori, Fijian, Samoan and Tongan communities)
Outer south west of Melbourne (centred on the City of Wyndham)
Vietnamese community Inner east and north of Melbourne (centred on the City of Yarra)
The second stream of activity – supporting cross-sector collaboration – was undertaken during the final stage of the project, after the various target populations had been selected and each catchment was established. It included the following three components:
1. Initial roundtable discussions – CALD representatives (community leaders and practitioners) as well as key decision makers from the relevant local AOD agencies met to discuss issues related to the AOD service needs of CALD community members
2. Agency site visits – following the roundtable discussions, CALD representatives in four of the five catchments attended agency site visits (including a local assessment and intake hub, residential withdrawal units, a residential rehabilitation service and non-residential program)

9
3. CALD AOD forum – involving stakeholders from across the five catchments as well as other interested parties to review project findings, explore key issues raised during the project, network and formally launch consumer and worker resources due for release at the conclusion of the project
2.2 Project findings
Key project findings are listed below. These are drawn from a thematic analysis of the evidence
obtained during the literature review and follow-up consultations with AOD, CALD and allied
health practitioners, CALD community members and other interested parties.
A more detailed appraisal of the project findings can be found in section 5.1 (pages 43 – 53).
At present there is very limited data on the prevalence of AOD use within CALD
communities, and while much of the research suggests that levels of AOD use is low
compared to the general population, this situation is not universal. Some CALD communities
are at increased risk of experiencing AOD related harms as they are subject to multiple risk
factors (including, but not limited to, low levels of health literacy and pre- and post-
migration stressors making it harder to adjust to a new cultural environment)
Despite this situation CALD communities are significantly under-represented in the AOD
treatment system, with data showing only 5% of closed treatment episodes for Victoria in
2013 – 14 applied to clients born overseas (AIHW 2015). When we consider that in 2011
26% of Victoria’s population was born overseas, it is clear that the proportion of CALD clients
is very low
As noted above there are multiple ‘at risk’ groups within CALD communities who are subject to AOD harms, including asylum seeker and refugee populations (especially young people), people from CALD backgrounds who inject drugs and CALD women from a range of cultural backgrounds in need of pre- and post-natal support, to name but a few
Admission rates of CALD clients into AOD treatment are due to an under-utilisation of services rather than a lower need (Beyer & Reid 2000), which is to be expected given the broad range of service barriers and socio-cultural norms making it difficult for individuals and families to access treatment
For those individuals from CALD backgrounds who come into contact with AOD services, it is often due to their involvement in the criminal justice system, raising concerns about the numbers of individuals from CALD backgrounds who are effectively bypassing treatment services and other supports
Adjustment to a new culture places considerable pressure on migrants, who often experience feelings of dislocation, isolation and grief. When these are compounded by the shame and ‘loss of face’ associated with AOD use (especially illicit drug use), the impact can be overwhelming on the family as they attempt to keep things hidden from view. It is therefore critical that in working with CALD clients AOD practitioners also focus on the needs of their families

10
While the CALD AOD Project is focused primarily on the AOD health needs of migrants, it is clear that approaching some CALD communities directly about AOD matters is not culturally appropriate nor is it sensitive (due to the stigma and shame associated with AOD use). For this reason it may be necessary to focus on health and wellbeing more generally, with AOD use representing but one of the underlying issues for consideration
Those agencies which are able to work effectively with CALD clients in need of AOD support demonstrate one or more of the following four service characteristics
1. Assertive outreach and an emphasis on linkage and service navigation support 2. Longer timeframes for engagement and treatment as well as more flexible appointment
arrangements (e.g. drop-in services) 3. Recruitment and use of skilled bi-cultural workers as well as peer led models of service
delivery 4. Focus on community engagement and relationship building. Services which have
established and maintained a presence are more likely to build up a level of trust within the community
As a result of the recent reforms to the AOD sector (adult service system) some agencies have reported a decreased capacity to work effectively with CALD communities. Often cited is the reliance on centralised assessment and intake processes which effectively preclude CALD individuals and family members from treatment. Alternative entry pathways are urgently required
Improving the capacity of AOD agencies to provide culturally responsive services should not be done in isolation, with the emphasis merely on the professional development needs of frontline staff. What is required is a broader systemic approach, one which addresses the underlying service barriers making it difficult for CALD communities to access relevant information, treatment and support
Despite the shame and stigma associated with AOD use, and the reluctance of many to come forward, there is significant interest across a number CALD communities to engage more fully with treatment providers. Multiple opportunities have been identified to work collaboratively and build on the gains which are already in place
2.3 Summary of recommendations
For a more detailed appraisal of the following recommendations, including background
information, examples of best practice and rationales, refer to section 5.1 (pages 43 – 53).
Recommendation 1: That existing AOD screening and assessment tools utilised by Victorian AOD
practitioners be reviewed to examine their applicability to CALD populations, with the aim of:
More effectively identifying each person’s ethnicity and cultural background
Establishing more flexible and culturally sensitive screening and assessment processes
tailored to each cultural group

11
Recommendation 2: That further research and capacity building initiatives be conducted into
the prevalence of AOD use within CALD communities, as well as the health literacy needs of CALD
community members and the experiences of individuals and family members navigating the AOD
service system
Recommendation 3: That the existing AOD sector catchment based intake and assessment
system be reviewed and reworked (in consultation with CALD community leaders and other
representatives) to enable alternative referral and entry pathways for individuals and family
members from CALD backgrounds
Recommendation 4: That culturally specific AOD resources be developed for distribution by AOD
and allied health practitioners, bi-cultural workers, CALD community leaders and other
representatives, with priority given to the use of audio visual materials (catering for the needs of
community members with low language proficiency while providing more engaging and
contemporary sources of information)
Recommendation 5: That AOD education and health promotion campaigns be undertaken in
each of the catchments targeting specific CALD communities, utilising culturally appropriate
messaging, communication tools and media channels (e.g. multicultural radio and newspapers),
with priority given to:
Reducing stigma and shame associated with AOD use
Raising awareness of available AOD services, how to access them and how they operate
Increasing community members’ knowledge of the potential harms associated with AOD
use as well as appropriate harm reduction strategies
Rebuilding relationships and addressing family inter-generational conflict
Recommendation 6: That resources be directed to tailoring diversion programs aimed at
reducing the high proportion of individuals (especially young people) from CALD backgrounds
entering the criminal justice system for AOD related offences
Recommendation 7: That resources be directed into establishing CALD specific community
engagement positions (a team of bi-cultural workers per catchment) whose role will be to:
Engage CALD communities and agencies with the emphasis on relationship building and
cross-sector collaboration
Raise awareness of available supports while facilitating access to AOD treatment for
individuals and families from CALD communities
Liaise with CALD communities and/or representatives about their specific health literacy
needs, experiences navigating the AOD sector and ways to improve the system
Advocate and promote culturally appropriate models of service delivery while
strengthening ties between CALD communities, ethno-specific agencies and AOD services
Recommendation 8: That AOD agencies be supported to establish interagency partnerships and
protocols with CALD organisations, thus ensuring more accessible, holistic and culturally safe

12
services for individuals and family members impacted by harmful AOD use
Recommendation 9: That further resources and training be developed for AOD practitioners,
aimed at increasing workers’ capacity to engage and support individuals and family members
from CALD backgrounds in need of AOD treatment, with priority given to increasing participants’
knowledge of:
Pre- and post-migration stressors and how they impact on AOD use – differentiating
between established and new and emerging migrant communities (with particular
reference to asylum seeker and refugee populations)
Culturally appropriate AOD screening and assessment
Strategies and therapeutic approaches for working with individuals and families from
CALD backgrounds (applied to different treatment settings)
The use of language services support to address language barriers and other
communication difficulties
Recommendation 10: That a cross-sector leadership program be established targeting
designated AOD and allied health personnel, CALD community leaders, bi-cultural workers and
other stakeholders in each catchment, with a view to:
Promoting stronger ties between mainstream AOD and allied health services, CALD
communities and ethno-specific agencies
Enhancing male and female participants’ capacity to act as advocates/champions and
‘bridges’ into the AOD system
Identifying suitable capacity building initiatives and putting them into practice
Recommendation 11: That agencies be supported to develop culturally appropriate service
delivery models (in partnership with local CALD communities), incorporating each of the
following service characteristics:
1. Assertive outreach and an emphasis on linkage and service navigation support
2. Longer timeframes for engagement and treatment as well as more flexible appointment
arrangements (e.g. drop-in services)
3. Recruitment and use of skilled bi-cultural workers as well as peer led models of service
delivery
4. Focus on community engagement, relationship building and family inclusive practice
2.4 Discussion
This project has sought to shed light on what is an especially complex situation. Individuals and
families from CALD communities are under-represented in the AOD treatment system, attributed
to a range of service barriers and socio-cultural norms which make it difficult for individuals and
families affected by problematic AOD use to access relevant information, support and treatment.
It is clear that working with CALD clients in need of AOD support is not a simple undertaking,
requiring what is a targeted and multi-faceted approach. At present this appears to be

13
happening only on a piecemeal basis, with staff and agencies (CALD and AOD) limited in their
capacity to cater for the specific needs of individuals and families from CALD communities
affected by harmful AOD use.
While much attention has been paid to the cultural competence of staff and culturally
appropriate service delivery, it is VAADA’s view that a more meaningful and substantial approach
is required, one which places ‘cultural safety’ as a core feature of integrated care.
This approach focuses on services and practitioners embracing, rather than merely accepting, the
differences created by culture, with the emphasis on them as much as possible proactively
engaging CALD communities so they feel included and welcomed. Despite the shame and stigma
associated with AOD use, and the reluctance of many to come forward, it is important to note
there is significant interest across a number of CALD communities to engage more fully with
treatment providers.
With this in mind VAADA has put together a framework made up of nine key features of best
practice, including:
1. Taking into account of the person’s ethnicity, cultural identity, pre-migration and
settlement experience
2. Special attention paid to engagement, addressing confidentiality concerns and promoting
safety (building rapport and trust)
3. Providing language services support (where required)
4. Addressing gaps in health literacy while focusing on the client’s worldview and health
perceptions
5. Flexible service delivery – tailoring one’s approach to match clients’ help seeking
behaviours
6. Customising the physical environment
7. Working in partnership with CALD community leaders, bi-cultural workers and other
representatives
8. Using appropriate messaging and communication channels to reduce stigma and shame
and improve the health literacy of community members requiring AOD support or
treatment
9. Providing holistic and family sensitive care
For more information about these features of best practice refer to Table 4 in section 5.2 (pages
53 – 59).
It is VAADA’s intention that this framework be used by AOD and allied health service providers,
CALD community leaders, government and other interested parties as reference points –
providing a series of benchmarks which can be used to:
Promote stronger ties between mainstream AOD and allied health services, CALD
communities and ethno-specific agencies
Improve service access for CALD community members in need of AOD treatment
Enhance the skills and knowledge of AOD practitioners in working with individuals and
families from CALD backgrounds
Reduce stigma and shame associated with AOD use while increasing the health literacy
of CALD community members

14
3. PROJECT ACTIVITIES
The CALD AOD Project was made up of two broad streams of activity, including:
1. Information gathering 2. Supporting cross-sector collaboration
Figure 1 provides an overview of the key activities undertaken across the two streams, followed by Figure 2 (on the next page) which outlines when each activity was conducted.
Figure 1. CALD AOD Project activities overview
3.1 Information gathering
This first stream of activity – information gathering – spanned the entire project and involved five key activities:
1. Targeted literature review 2. CALD and AOD practitioner consultations 3. Selection of target CALD populations 4. Development of ‘cultural inventories’ 5. Audit of consumer and worker resources
Information gathering
Targeted literature review
CALD & AOD practitioner consultations
Selection of target CALD populations
Development of 'cultural inventories'
Consumer & worker resources audit
Supporting cross-sector
collaboration
Initial roundtable discussions
Agency site visits
CALD AOD forum

15
Figure 2. CALD AOD Project timeline
While the literature review provided a useful baseline it was clear more information was required
to bring about a more up-to-date and comprehensive analysis, one which factored in the
experiences of frontline and other operational staff. With this in mind VAADA commenced the
first round of stakeholder consultations with CALD and AOD practitioners.
Refer below (sections 3.1.1. – 3.1.5) for a more detailed appraisal of each information gathering activity.
3.1.1 Targeted literature review
During stage 1 of the project a literature review was conducted, using mostly Australian sources
from 2000 onwards (publications, journal articles, grey literature and other data).
The purpose of the literature review was to identify AOD prevalence rates and patterns of use
among CALD populations, risk factors contributing to problematic AOD use, gaps in existing
research and service barriers for CALD communities and relevant best practice initiatives.
Analysis of the literature highlighted four key issues:
1. There is limited data on the prevalence of AOD use within CALD communities
January - June 2014Stage 1
• Targeted literature review
• First round of CALD and AOD practitioner consultations commences
July - December 2014Stage 2
• Completion of CALD and AOD practitioner consultations (consultation report distributed to iiparticipants)
• Needs assessment and selection of target CALD populations and catchments
• Consumer and worker resources audit
January - June 2015 Stage 3
• CALD community consultations
• Partnerships established with CALD agencies and recruitment of CALD Liaison Workers
• Development of 'cultural inventories' (community profiles) commences
July - December 2015Stage 4
• Initial roundtable discussions
• Agency site visits
• CALD AOD forum
• Completion of 'cultural inventories' (community profilles)

16
2. There are a range of service barriers and socio-cultural norms making it difficult for
individuals and families affected by problematic AOD use to access relevant information,
support and treatment
3. Low admission rates of CALD clients into AOD treatment is due to an under-utilisation of
services rather than a lower need
4. In order to more effectively engage migrant populations health agencies (including AOD
service providers) will need to tailor their approaches accordingly
Note. To ensure it reflected the most up-to-date data the literature review was revised and updated in
February 2016.
See attached literature review for more information.
3.1.2 CALD and AOD practitioner consultations
Following the literature review, the CALD AOD Project Officer undertook a series of consultations
(mostly face-to-face) with AOD and CALD practitioners across Victoria to get their feedback on:
AOD use patterns within CALD communities
Service barriers
Ways to improve access to culturally appropriate AOD information and services
The professional development needs of respondents
In total 50 consultations were conducted involving 111 participants from 43 agencies across
Victoria. Consultations were generally run as a series of semi-structured interviews, covering a
range of topics while at the same time enabling respondents to raise other issues they considered
important.
Findings were documented in a consultation report and made available to respondents in
February 2015.
See attached consultation report for more information.
3.1.3 Selection of target CALD populations and catchments
In September 2014, data from the literature review was compared and contrasted to the
feedback received during the follow-up consultations with CALD and AOD practitioners. Drawing
on the findings five target populations were selected.
The selection process itself was based on a needs based model. Rather than selecting various
CALD communities or groups simply on the basis of raw numbers (i.e. population size) or current
demand for services (i.e. number of clients currently accessing AOD treatment), VAADA opted to
focus on the need for AOD treatment and support within different communities.
While population size and current demand for AOD treatment remained an important
consideration, it was recognised that this approach in isolation was insufficient. It did not
account for the service barriers making it difficult for some CALD groups in particular to access

17
the support they require, nor did it account for the impact on individuals and families when they
miss out.
A needs based approach to selection enabled VAADA, in collaboration with the project reference
group (PRG), to consider all the factors and variables, comparing level of need for each
community while reflecting on what is achievable.
The process was comprised of four steps:
1. Identification of the various CALD communities and groups under consideration (i.e. a
shortlist)
2. Assessment of each population’s level of need, taking into consideration the following
criteria –
a) AOD pattern of use, prevalence and associated harms for each CALD community or
group
b) Current level of AOD service involvement and the barriers limiting access to AOD
treatment and support for each CALD community or group
c) Risk factors increasing the likelihood of AOD harms for each CALD community or
group (including resettlement stressors, stigma, language barriers and other literacy
problems, family conflict, socio-economic disadvantage, mental health issues and
criminal justice system involvement)
3. CALD communities and/or groups selected (based on the needs assessment undertaken
in step 2)
4. Geographic locations (catchments) selected
Table 1 outlines the five target populations / communities selected, as well as the catchments VAADA would be operating in to deliver project outcomes.
Table 1. Selected CALD communities and catchments
Selected community Catchment
Afghan community (Hazara group) Hume region of Victoria (centred on the City of Greater Shepparton)
African (including Sudanese, Ethiopian, Somali, Togolese and Congolese communities)
Outer east of Melbourne (centred on the City of Greater Dandenong)
Arabic speaking Muslim communities Inner and outer north of Melbourne (centred on the City of Yarra)
Pacific Islander and Maori communities (including Maori, Fijian, Samoan and Tongan communities)
Outer south west of Melbourne (centred on the City of Wyndham)
Vietnamese community Inner east and north of Melbourne (centred on the City of Yarra)

18
In determining the various catchments VAADA, with advice from the PRG, prioritised those areas:
Which had been identified as ‘hot spots’ – locations where AOD use was considered
prevalent for each selected community
Where AOD services had demonstrated the capacity to work well with individuals and/or
families from CALD backgrounds in need of AOD support
Where linkages between CALD and AOD services and other stakeholders are well
established, or where there is an identified need to strengthen ties between CALD and
AOD services
Where CALD and AOD stakeholders had shown an interest in participating and supporting
the project
3.1.4 CALD liaison and development of ‘cultural inventories’
In order to more effectively document the specific health needs of each target population VAADA
sought the assistance of a range of CALD liaison personnel whose role was to:
Investigate and brief VAADA project staff on CALD community structures, networks and
‘gatekeepers’ within their target community
Introduce VAADA project staff and local service providers to CALD community members,
representatives and other service providers
Meet with CALD community members and workers using formal and informal networks
to raise awareness of the project and seek their perspective on CALD AOD issues
Participate in project seminars/forums/workshops to inform interested parties (CALD and
AOD) of issues arising from the project
Liaise with CALD community members and/or representatives about their health literacy
needs and experiences navigating the AOD sector, passing on this information to VAADA
project staff
Inform VAADA project staff on relevant initiatives undertaken by service providers in the
catchment
Provide advice and guidance on the development of consumer and worker resources
(ensuring they are culturally appropriate)
Recruit CALD community members to participate in project activities
These personnel, referred to as CALD Liaison Workers (CLWs), were sourced from a range of
ethno-specific and mainstream agencies working on behalf of the selected communities/target
populations, including:
Australian Vietnamese Women’s Association (AVWA) – working on behalf of the
Vietnamese community
Bridging Worx (BW) – working on behalf of Pacific Islander and Maori (‘Pasifika’)
communities
Carers of Africa (CoA) and the African Communities Foundation of Australia (ACFA) –
working on behalf of African communities
Islamic Council of Victoria (ICV) – working on behalf of the Arabic-speaking Muslim
community

19
Primary Care Connect (PCC) – working on behalf of the Afghan Hazara community
If the project objectives were to be met in the time allocated it was clear that handing over some
responsibility to CLWs was paramount. This would promote a greater sense of ownership and
respect while demonstrating VAADA’s commitment to working in partnership with the target
communities. While the project remained fundamentally a scoping exercise, information
gathering and relationship building exercise it was also clear that elements of a community
development approach were needed.
Based on the information provided by the CLWs in each catchment a series of ‘cultural inventories’ (community profiles) were developed. Figure 3 provides on overview of the structure of these cultural inventories. Figure 3. Cultural inventory overview
Each cultural inventory (community profile) is made up of four domains of enquiry:
1. CALD community structure and networks – including information on how each target
population is structured, as well as a description of the networks and organisations
within that community
2. Partner agency – providing an overview of the agency’s role, organisational structure,
services it provides and how agency staff communicate with community members
3. Perceptions and health beliefs of CALD community members – related to AOD use,
culturally appropriate treatment responses and ways CALD AOD issues are most
effectively communicated
4. Perceptions of past and current service users (where available) – based on a series of
short interviews with community members, adults 18 years and over, about their
CALD community structure & networks
Partner agency
Perceptions & health beliefs of
CALD community members
Perceptions of past & current service users

20
experiences navigating the AOD service system (including people within and outside of
the criminal justice system)
Note. In two of the catchments interviewing Afghan Hazara and African community members about their service user experiences was not possible. For the Afghan Hazara community it was considered too confrontational an issue and thus culturally insensitive, whereas for the African community access to adult community members with AOD service user experience was very limited.
To assist CLWs in this task VAADA developed four templates outlining specific issues and questions to be investigated. Refer to Appendix A (pages 60 – 67) for the community profile templates.
Below and on pages 21 – 36 we have included the five cultural inventories which have been developed.
Cultural inventory 1
Afghan Hazara community (City of Greater Shepparton catchment)
Afghan Hazara community in the City of Greater Shepparton
It is estimated that 135 families and 450 single Afghans (mostly male) reside in Shepparton, with a total population of approximately 1600 people. The oldest Afghan Hazara household in Shepparton settled in the region in 2001, with the community starting to form when many of the men came to Shepparton for work (i.e. to pick fruit).
It is also estimated that approximately 50% of the Afghan population arrived in Australia by boat, with many having spent time in detention prior to release.
According to the Afghani Community Profile, developed by the Ethnic Council of Shepparton and District Inc., 80% of Afghan people speak Hazaragi. Of this group 98% of adults are unable to read or write in their language of origin. It is also estimated that approximately 70% of Afghans in the area are able to speak some English but are not able to read or write. Pushto is also spoken in a small number of households.
Approximately 99% of Afghans are Muslim. The majority practice Shia Islam while a small number practice Sunni Islam (Pushto speakers and Tajiks).
Most Afghan men who are working are employed in farming occupations. Due to their low English proficiency employment opportunities for many community members are limited.
The father is traditionally head of the household and responsible for earning money to support the family. The mother’s prime responsibility is the care of children and management of the household. Afghan women tend to be quite isolated, not socialising outside of the family home, relying on their partners for transport and language support. A key priority raised by the community is the need for women in the community to be given opportunities to socialise and engage in physical activity.
While men are more active within the community there are a number of female leaders who are highly influential.
The Goulburn Valley Afghan Association (GVAA) is the only formal organisation representing Shepparton’s Afghan community. This organisation is governed by the President and seven other committee members. According to the Afghani Community Profile (cited above) in early 2015 community elections were held where the community resolved to elect a younger group of

21
Cultural inventory 1
Afghan Hazara community (City of Greater Shepparton catchment)
representatives, as it was believed that young educated community members would be better equipped to represent the community and advocate on their behalf.
Practitioners and service providers are advised to contact GVAA as the primary link to the community.
The Afghani Mosque in Shepparton serves as community centre and a key point of contact. As of October 2015, the mosque’s construction had almost been completed and was in use. Funding for its construction was raised entirely by the Shepparton Afghan community (in excess of $1 million).
The Afghani Mosque has been identified as an ideal place for service providers to establish connections with the community and perhaps run information sessions, but not specifically on AOD as this is considered too confrontational. Instead it is considered more appropriate to include AOD information as part of a wider health program. The mosque’s Imam is fundamental as “he is a useful source for spreading information and also knows more information about cultural and religious beliefs of the community”, as described by the catchment’s CALD Liaison Worker.
In terms of communication/media channels information is mostly disseminated via word of mouth or posters. Social media is also widely used, though this is largely the preserve of younger members of the community who are digitally literate. GVAA has recently set up a Facebook page which posts regular updates on issues pertinent to the community and the activities of community leaders. The community has also commenced work on a magazine (to be published on a monthly basis). Primary Care Connect
Primary Care Connect (PCC) is a community health service located in Shepparton. PCC operates more than 25 programs across a number of service areas, including:
Drug and alcohol
Primary health
Financial
Indigenous services
Counselling
Refugee services
PCC has strong links with the local Afghan community having recruited a number of community members to act as bicultural staff. In total, PCC employs more than 60 staff.
PCC is located at 399 Wyndham Street Shepparton VIC 3630 Ph: (03) 5823 3200
For more information about PCC go to: www.primarycareconnect.com.au Perceptions and health beliefs of CALD community members
Family is extremely important in Afghanistan and maintaining the family’s honour is a key influence on many community members’ behaviour. There is a strong belief in Afghan culture that what happens in the home remains private, as in many other cultures, thus sensitive issues such as those related to AOD use are generally not discussed in public.
AOD use is considered ‘haram’ (forbidden under Islamic law), however the use of medications is allowed.
Many parents are concerned that their children are rapidly changing as they are unduly influenced by Western norms and culture. They fear a loss of culture, identity and respect for parents and their

22
Cultural inventory 1
Afghan Hazara community (City of Greater Shepparton catchment)
traditions.
Given the high numbers of asylum seekers and refugees within the Afghan community, and high prevalence of trauma exposure, much of the attention with AOD centres on the misuse of prescription medications and lack of awareness regarding potential harms. Increasing community members’ awareness of the links between mental health and AOD use (e.g. providing information on medication safety) has been a key priority for a number of health service providers.
Community members experiencing AOD issues are most likely to keep it to themselves, largely due to the stigma and shame. Generally speaking, Afghan people would rather access a mainstream service in private rather than approach another community member. This is a difficult situation as they are often unaware of the services which are available.
For community members on bridging visas, where they have signed a code of conduct agreeing to obey all Australian laws and comply with all official health and immigration requests, the fear of legal sanctions is likely to dissuade them from coming forward about AOD misuse (especially related to illicit substances).
If a parent becomes aware of their child using substances they may try to deal with the situation by isolating the young person – keeping them at home. Many parents and other family members are at a loss to understand the issues or how to respond.
Cultural inventory 2
African communities (City of Greater Dandenong catchment)
African communities in the City of Greater Dandenong
The City of Greater Dandenong is the most culturally diverse locality in Victoria, and second most diverse in Australia, with residents from over 150 different birthplaces. Well over half of the population (60%) were born overseas. Based on Australian Bureau of Statistics (2011 census data) Dandenong had an estimated population of approximately 145,000 people.
Over the last few decades Africans have come to Australia primarily via two routes – as skilled migrants and as refugees . For refugees in particular adjusting to a new cultural environment has been challenging, including:
Difficulties in dealing with trauma histories which may have involved loss of family and friend and exposure to violence
Differing rates of adjustment between adults and young people resulting in family conflict
Lack of understanding about legal rights and responsibilities, including situations where racism and discimination has occurred
Socio-economic disadvantageunderpinned by high rates of unemployment, shortages in affordable housing etc
Practitioners and service providers are advised to contact one or more of the following organisations as they serve as primary links to the various African communities.
New Hope Foundation

23
Cultural inventory 2
African communities (City of Greater Dandenong catchment)
African Think Tank
Care Africa International
Sudanese Community Association of Australia
Horn of Africa Communities Network
Liberians for Empowerment and Development Inc
South Eastern Region Oromo Community Association
Congolese Community of Victoria
South Sudan Equatorians Association Inc
Sudanese Australia Youth Action Group
Carers of Africa
African Communities Foundation Australia
There is a broad agreement amongst community members that relationship building is a slow and incremental process, with investment needing to take place over the long term. One-off AOD information sessions will not suffice. The key is to work through community leaders – engaging and mobilising key representatives.
For many African community members print based materials are of limited use, as they come from a ‘low reading culture’. Other mechanisms for conveying information are recommended, including sharing information and stories through music and in face-to-face interactions at cultural and social events. Carers of Africa and the African Community Foundation Australia
Carers of Africa (CoA) is a not-for-profit charity located in Dandenong which was established in 2014. CoA’s purpose is to support disadvantaged members of the African refugee community in Victoria through the provision of a range of services, for example:
Volunteer services
Community Corrections Order Support
Domestic services
Healthcare services
CoA is located at 18 Mason Street Dandenong VIC 3175 Ph: (03) 9706 9887
For more information about CoA go to: www.carersofafrica.org.au The African Communities Foundation Australia (ACFA, formerly Eastern and Central Africa Communities Victoria and African Holistic Services) is a statewide organisation which aims to bring together African-Australians in Victoria who trace their genealogy mainly from various African countries as well as those who feel connected to Africa.
ACFA was established in 1988 to provide a forum where common issues of settlement could be collectively dealt with. Their mission is to support the integration of African migrants in Australia through the provision of culturally sensitive services.
ACFA is located at 241 Wellington Street Collingwood VIC 3066 (co-located with Neighbourhood Justice Centre) Ph: (03) 9948 8777
For more information about ACFA go to: www.africanfoundation.org.au Perceptions and health beliefs of CALD community members
Alcohol use, when consumed in moderation, is typically accepted across many African communities.

24
Cultural inventory 2
African communities (City of Greater Dandenong catchment)
However, when used to excess the individual may be perceived as having a mental illness. For some people (e.g. individuals from South Sudanese backgrounds) mental illness is regarded as a sign of weakness and therefore not an issue for open discussion (McLean 2005).
In some African cultures drug use is widely associated with criminal activity and violence.
It is widely acknowledged that there is often a cultural clash between African youth and their parents/elders. Australian drinking and substance use norms are viewed by some community members as too permissive when compared to their traditional cultural norms. In these circumstances conflict emerges where the young person adopts the drinking of his/her peers, while his/her parents focus their efforts on preserving traditional roles and values (CMY & MYAN 2011).
It was strongly recommended by community representatives that AOD treatment needs to be delivered in a holistic manner – moving beyond narrowly defined clinical interventions. A popularly held view amongst community representatives is that AOD treatment is anglo-centric (based on a western/white interpretation).
Cultural inventory 3
Arabic speaking Muslim community (City of Hume catchment)
Arabic speaking Muslim community in the City of Hume
It is estimated that the City of Hume has the second highest concentration of Muslims in Australia after Bankstown in New South Wales. According to the Australian Bureau of Statistics (2011 census data):
The majority of Muslims living in the City of Hume (n = 16952) are above 18 years of age
A large number of Muslims living in the City of Hume (35.4%) are from an Arabic speaking background, however the majority are from a Turkish speaking background (54.8%)
The Australian Muslim age profile is significantly younger when compared to the general population. In 2011, 67.2% of Muslims were below the age of 35 compared to 46.4% of the total Australian population, and only 3.4% of Muslims were 65 years and older compared to 14% of the total Australian population
Muslims in Australia come from 183 different countries around the world, making them one of the most ethnically diverse religious groups in Australia
Not all Arabic speakers living in Hume are Muslim. Non-Muslim Arabic speakers include Lebanese and Assyrian Christians. There are significant differences in language, culture and attitudes between Arabic speakers of different origin.
The Lebanese community, due to its size and length of time in Australia, is considered the most influential of all the Arabic speaking Muslim community groups.
As Islam places responsibility on the individual to practice his or her religion, there are personal and cultural variations which apply. A Muslim from Iran may have a different way of observing Islam when compared to a Muslim from West Africa.
Included below is some background information about the cultural nuances for working with Muslim clients.

25
Cultural inventory 3
Arabic speaking Muslim community (City of Hume catchment)
Cultural nuances for working with Muslim clients
Note. Much of the following information has been sourced from Health care providers’ handbook on Muslim patients (Second Edition 2010), developed by Queensland Health and Islamic Council of Queensland. Available from www.health.qld.gov.au/multicultural
The following sensitivities need to be observed when introducing oneself:
Many Muslims do not shake hands with members of the opposite sex, though some will shake hands but do so to avoid offending the other person. It is therefore important to wait for the other person to extend their hand first
Be considerate of personal space – many Muslim men and women feel uncomfortable with people of the opposite gender standing too close
Where possible, female staff should be made available for consultations and treatment of Muslim women. This also applies to male staff working with Muslim men. Having a male and female sitting in a room alone is strongly discouraged in Islam. Where this is unavoidable it is recommended that the door remains open, and that a room with windows is used so that others may look in.
Modesty is very important in Islam. The following dress codes are advocated:
Muslims may wear any national or chosen dress code so long as it loosely covers certain parts of the body (i.e. from the navel to the knees for men, and for women the whole body with the exception of the face, hands and feet). These areas of the body are referred to as Awrah
Some Muslim women may also wear a veil over their face (referred to as a niqab) and hold the view that it is also part of their Awrah
Muslim women may take off their hijab (veil) in front of other Muslim women, as well as their husbands and close family members
For some Muslims it is considered respectful and modest for men and women not to make direct eye contact
In terms of dietary requirements Muslims are required to follow a ‘halal’ diet. Halal means lawful and is used to designate food which is permitted in Islam. Halal requirements related to food, drink and fasting are as follows:
Islam does not permit the consumption of alcohol or pork
Muslims are not permitted to eat food which contains animal fat or animal by-product unless it is derived from animals slaughtered in the halal tradition
During Ramadan Muslims will fast (not eat or drink) from the break of dawn to sunset
Note. Ramadan occurs during the ninth month of the Islamic calendar, and is observed by Muslims worldwide as a month of fasting to commemorate the first revelation of the Quran to Muhammad.
Before prayer, a Muslim is required to perform ablution (a ritual purification wash) with water known in Arabic as wudhu. Washing with water is also required after urination or defecation. A full bath (ghusl) is required after seminal discharge or after menstruation and post-natal bleeding. It is therefore strongly advised that toilets be equipped with containers of water to assist with washing.
Muslims are required to pray five times a day. However those who are cognitively impaired are exempted. Prayers are performed while facing Mecca, which in Victoria is located west, north-west. Prayers are usually said on a prayer mat and includes various movements such as bowing, prostrating and sitting. If the person is ill it is not necessary for him/her to make all the prayer movements. In these circumstances prayers can be performed in bed or while seated.
Friday is a significant day to Muslims and a special prayer is performed at noon.

26
Cultural inventory 3
Arabic speaking Muslim community (City of Hume catchment)
There are two key days of festivities (known as Eid) which are celebrated by all Muslims around the world:
1. Eid al-Fitr – festival of the feast that takes place at the end of Ramadan 2. Eid al-Adha – festival of sacrifice that takes place at the time of the annual pilgrimage
to Mecca (referred to as the Hajj), approximately two and a half months after the first Eid Islamic Council of Victoria
The Islamic Council of Victoria (ICV) is a peak body for Victorian Muslim organisations, representing the interests of more than 150,000 Muslims across the state. Its membership base includes 47 Muslim organisations located throughout metropolitan Melbourne and rural and regional Victoria.
ICV is made up of 15 paid staff and currently 12 volunteers – including General Manager (head of operations), Services Manager, Prison Chaplains, youth workers and volunteers.
ICV provide a broad range of services, including but not limited to:
Advocacy and media liaison
Community Integration Support Program
Hospital chaplaincy
Office for Women
Muslim Leadership Program
Prison Chaplaincy
Muslim Connect – a post release rehabilitation program for Muslims exiting prison
No Interest Loans Scheme – interest free loans of up to $1000 to people on low incomes
Partnership and sponsorship of community events
Youth engagement programs
Zakat (local charity)
In terms of communication/media channels the ICV has a Communications Officer who is responsible for media releases, website updates and a weekly bulletin newsletter. ICV uses the following means to communicate with the community:
Newsletter (weekly bulletin) and media releases
Email networks – a member contact list including 47 member organisations and a general email list including individuals and organisations used by the Communications Officer to distribute the newsletter
Social media – including the ICV Facebook page and Twitter account
Friday prayers – religious sermons are held every Friday at the ICV central mosque. Announcements are often made at this time or messages incorporated into the sermon
Word of mouth
ICV is in regular contact with the Victorian Board of Imams as well as member organisations when giving a united message to the community
ICV has establishes a partnership with Al-Wasat newspaper (Arabic monthly newspaper)
Islamic Voice Radio
For more information about ICV go to: www.icv.org.auions and health beliefs of CALD community members Perceptions and health beliefs of CALD community members
Use of AOD is considered ‘haram’ – forbidden under Islamic law – though the use of medications is

27
Cultural inventory 3
Arabic speaking Muslim community (City of Hume catchment)
allowed.
For non-practicing Muslims alcohol is not considered as much of a concern as other substances (e.g. amphetamines), and social drinking is not considered a problem.
Community members experiencing AOD issues are most likely to keep it to themselves, due to the stigma and shame. Thus AOD issues are not openly discussed. Mental health issues are also considered taboo.
Individuals engaging in AOD use tend to distance themselves from the community, and in some cases have been disowned by other community members. It is commonplace for people who are using to be seen as harming their family and the community at large.
It has also been reported that for many community members there is not a distinction between the different patterns of use – you are either ‘using’ or ‘not using’.
For many community members, including practicing and non-practicing Muslims, AOD use is very much seen through a moral and religious prism. AOD use is often viewed as a moral failure, though this view is not universally supported.
Harm minimisation is not widely understood, with harm reduction messages considered to be challenging cultural norms. Nonetheless, there are avenues to engage the community, with the support of agencies such as ICV.
As many community members are unaware of the support available to them it is unlikely that they will contact AOD services. While community members are often reluctant to seek help from drug treatment services, there is significant interest from community leaders to establish relationships with AOD service providers.
For many community members there is significant concern about the involvement of individuals in the criminal justice system – often for drug-related crimes. As such, ICV has devoted significant resources to its prison chaplaincy and post release rehabilitation program for Muslims exiting prison. Perceptions of past and current service users
The following information is drawn from 13 participant interviews conducted by one of the ICV Prison Chaplains.
Participant A – Lebanese male aged 24 years. First contact with AOD services as an adolescent – AOD counselling on 9 – 10 occasions over a period of 4 – 5 weeks. Has not being engaged in AOD treatment since. Reports being directed to attend by a youth justice worker. Further reports being ‘somewhat satisfied’ as “they tried to do a good job”.
Participant B – Lebanese male aged 34 years. Reports being directed to attend a youth AOD service in his early twenties after being convicted for a drug related crime. Attended on six occasions. Has not received AOD treatment since. Further reports being ‘somewhat satisfied’ with the support he received at the time.
Participant C – Lebanese male aged 40 years. First contact with AOD services as an adolescent – including AOD counselling, withdrawal treatment and residential rehabilitation. Reported accessing services on more than 15 occasions. Further reports ‘no opinion’ regarding the support he received from AOD services. Stated that it is “up to you and faith. How string your faith is in not just from receiving support but using it to the best of your ability”. Did not offer a view regarding potential service improvements.

28
Cultural inventory 3
Arabic speaking Muslim community (City of Hume catchment)
articipant D – Lebanese male aged 40 years. Reported first coming into contact with AOD services as Participant D – Lebanese male aged 40 years. Reported first coming into contact with AOD servuces as an adolescent, but did not access treatment as he was placed on a waiting list. Further reports not receiving any assistance or linkage support at the time. No other details provided.
Participant E – Lebanese male aged 49 years. First came into contact with AOD services aged in his late forties. Reports attending AOD counselling 1 – 5 times. Has also been placed on a pharmacotherapy (methadone). Currently on the program for more than 12 months. Further reports being ‘very satisfied’ with the support he has received, as “it was the best thing I have done in my life … I feel great.”
Participant F – Egyptian male aged 27 years. First came into contact with AOD services as an adolescent. Currently incarcerated at Marngoneet Prison where he reports attending a 44 hour semi-intensive AOD psycho education program. Reports being ‘somewhat dissatisfied’ as he did not feel he benefitted from attending the program. Recommends more time and effort be put into working with the community.
Participant G – Lebanese male aged 32 years. First came into contact with AOD services upon release from youth prison aged 18 – 21 years. Reports attending voluntarily on two occasions but has not returned to an AOD service since. Further repots being ‘very dissatisfied’ with the support he received.
Participant H – Lebanese male aged 40 years. First came into contact with AOD services aged 22 – 34 years. Reports attending AOD counselling solely on one occasion while incarcerated at Marngoneet prison. Reports ‘no opinion’ about the support he received. No further details provided, other than noting he is unfamiliar with any AOD services located in the community.
Participant I – Lebanese male aged 34 years. Reports attempting to access residential withdrawal but felt “let down by the system” as he was unable to immediately access treatment (i.e. was placed on a waiting list). Has not sought AOD treatment since. Reports being ‘very dissatisfied’ with the support he received from AOD services. No further details provided.
Participant J – Lebanese male aged 23 years. First came into contact with AOD services aged 18 – 21 years. Reports attending AOD counselling 1 – 5 times while incarcerated. Further reports being ‘somewhat satisfied’ with the support he received – “they done a good job overall but in prison it is hard to get a lot of time with the counsellors.”
Participant K – Lebanese male aged 40 years. First came into contact with AOD services aged 35 – 44 years. Reports attending AOD counselling solely on one occasion, court ordered as one of his bail conditions. Has not accessed AOD services since. Further reports being ‘somewhat dissatisfied’ with the support he received, as the AOD counsellor was not well versed in his culture or religion. No other details provided.
Participant L – Lebanese male aged 46 years. First came into contact with AOD services aged 22 – 34 years. Reports voluntarily accessing medical support on two occasions with support from his family. No other details provided. Further reports being ‘very satisfied’ with the support he received as “it helped me a lot and I stayed off the ‘ice’ while I was on it.” Recommends AOD practitioners engage more fully with Muslims to raise awareness of the services they provide.
Participant M – Lebanese male aged 54 years. First came into contact with AOD services aged 45 – 54 years. Reports attending an AOD psycho education program whilst incarcerated (approximately 40 hours in length). Further reports being ‘somewhat satisfied’ with the support he received, though he experienced some communication difficulties due to language barriers.

29
Cultural inventory 4
Pacific Islander and Maori communities (City of Wyndham catchment)
Pacific Islander and Maori (‘Pasifika’) communities in the City of Wyndham
The City of Wyndham is currently the second-fastest growing local government area in Victoria. According to the Australian Bureau of Statistics (2011 census data), its residential population will exceed 245,000 people by 2021 and 300,000 by 2030. As of June 2013 its population was 189,618 representing a 6% annual growth rate (MyriaD Consultants 2014).
According to a local council report – Multicultural Policy Planning in Wyndham – published in November 2014, between 2006 and 2011 in Wyndham, the number of residents who were born overseas increased by nearly 17,000.
A review of the available data shows that it is difficult to identify the precise number of Pacific Islanders and Maori people living in Wyndham, however based on consultations with the catchment’s CALD Liaison Worker and others we know there has been a significant increase in the ‘Pasifika’ population over the past decade, with all the main cultures represented (Maori, Samoan, Tongan, Cook Islander, Fijian and Nieuan).
At the epicentre of Pasifika societies is a collectivist philosophy underpinned by strong family interdependence, holism and spirituality. Practicing cultural traditions and values are viewed as necessary for the maintenance of cultural identity as well as the preservation of wellbeing.
Of particular concern to the Pasifika community is the over-representation of adults and youth in the criminal justice system, resulting in organisations such as Bridging Worx (discussed below) establishing a range of pre- and post-release prison programs.
Another key concern is the impact of Federal legislation which came into effect in February 2001, denying New Zealand citizens residing in Australia access to unemployment benefits and other social security payments as well as other forms of government support (e.g. tertiary student loan schemes – FEE HELP and VET FEE HELP).
Practitioners and service providers are advised to contact the following organisations as they serve as primary links to the community.
Maori Wardens – not-for-profit volunteer organisation providing mentoring support to ‘at risk’ Pacific Islander and Maori youth
Victorian Samoan Advisory Council – organisation representing the Samoan community in Victoria
Charis Mentoring – not-for-profit organisation targeting Pasifika youth
Iron Armour Academy – Christian based not-for-profit organisation providing mentoring and sports development support to young people
United Pasifika Council of Victoria – peak body representing Pacific Islander and Maori communities
Bridging Worx (discussed below)
In addition, the City of Wyndham and its adjoining council in the City of Brimbank have both established Pasifika networks involving local agencies and community representatives which are also important conduits for engaging the community.
Christianity plays a pivotal role in Pasifika culture. With the increase in migration from the Pacific into Australia and New Zealand in the 1950s and 1960s, Pasifika peoples who left their island homelands quickly established churches in their new surrounds. This was done not only for religious education but for the purposes of cultural reinforcement. Churches are hubs which are used to strengthen extended family ties and educate young people about their cultural identity and heritage (South East Local Learning and Employment Network 2012). For these reasons it is strongly

30
Cultural inventory 4
Pacific Islander and Maori communities (City of Wyndham catchment)
recommended that AOD practitioners and service providers pay special attention to the role of (South East Local Learning and Employment Network 2012). For these reasons it is strongly recommended that AOD practitioners and service providers pay special attention to the role of churches and religious leaders as they engage the Pasifika community.
Word of mouth, face-to-face interactions and social media have been put forward as the most effective means to communicate with Pasifika people, whereas disseminating information in hard copy form is not considered particularly effective. Bridging Worx
Bridging Worx (BW) is a multicultural not-for-profit, non-government community organisation with strong links to the Pacific Islander and Maori community. BW aims to alleviate hardship through the provision of emergency care and services for people at risk, by:
Diverting young people and adults away from the criminal justice system
Reintegrating young people and adults back into the community with a view to becoming more productive members of society
Working to reduce the incidence of recidivism among this group
BW also aims to build capacity in the Pacific Islander and Maori community through their school programs to assist in addressing cultural differences, improve educational outcomes and enhance employability.
Founded in 2011 by a local Samoan businessman, the organisation was initially developed to service Pasifika communities located in the Northern suburbs of metropolitan Melbourne.
For more information about Bridging Worx go to: www.bridgingworx.org.au Perceptions and health beliefs of CALD community members
Many Pacific Islanders and Maori people do not respond to healthcare models which are inconsistent with traditional concepts of health and wellbeing. According to Sheridan (2015) these differ markedly from contemporary biomedical concepts.
For example, the Pacific ‘Fonofale’ model, which is based on the structure of a traditional meeting house, is made up of four pillars representing the various components of holistic health: physical, spiritual, mental and other (including gender, sexual orientation, age, social class, education and employment status), as well the house’s foundation and roof.
The foundation represents family, recognised as a fundamental building block on which Pasifika communities are organised and the basis on which health and wellbeing is built. The roof represents culture, perceived as a set of values which provide shelter for life.
Sheridan (2015, p. 9) notes:
This model serves to explain the holistic nature of Pacific identity and wellbeing, whereby all aspects are needed for the house to stand. Family not only provides social support, but is the mechanism through which values, beliefs, wisdom and traditional customs are shared; shared cultural values serve to provide identity, especially for a minority group subject to the influence of other cultures …
Against this backdrop it was strongly recommended by community representatives that AOD treatment needs to be delivered in a holistic manner – moving beyond narrowly defined clinical interventions. A popularly held view amongst Pasifika people is that AOD treatment is anglo-centric (based on a western/white interpretation).

31
Cultural inventory 4
Pacific Islander and Maori communities (City of Wyndham catchment)
Within this group AOD use is often viewed as a moral issue rather than a health issue. For those people who view it in moral terms AOD use is considered shameful.
Community members experiencing AOD issues are most likely to keep it to themselves, due to the stigma and shame. Thus AOD issues are not openly discussed. Mental health issues are also considered taboo.
There is a widespread belief that AOD issues need to be dealt with in private – connected to the view that one needs to show strength. Perceptions of past and current service users
The following information is drawn from 10 participant interviews undertaken by BW staff.
Participant A – young Maori/Samoan man aged 18 years. Involved in AOD use since his early teens. Sentenced to a Community Based Order (CBO) for crimes committed whilst under the influence. First contact with AOD services aged 22 – 34 years. Required to attend AOD counselling as a condition of his CBO. Attended AOD counselling for only one session – solitary occasion where he was engaged in AOD treatment. Reported that he did not feel comfortable at the time and was asked to see another AOD clinician but did not return for treatment.
Participant B – Cook Island/Australian male aged 32 years who was released from prison approximately 10 years ago. Reported history of trauma which led to heroin use. Introduced to methadone while in prison and continues to access methadone treatment post release. Also engaged in AOD counselling while incarcerated. Has accessed AOD services 11 – 15 times and being ‘very dissatisfied’ with the support he has received. Reports being skeptical of AOD service providers as “they don’t see the culture of people”, and prefers to work with someone from his own community.
Participant C – Samoan male aged 29 years. First contact with AOD services aged 22 – 34 years. Directed to attend AOD counselling by the court as part of a CBO. Attended three sessions over a six month period. Reports that he found it difficult to connect as his culture and family situation was not raised. Reports being ‘somewhat satisfied’ with the support he received, though when prompted noted that practitioners would benefit attending training in working with individuals and families from Pasifika communities.
Participant D – Samoan male aged 35 years. Currently in medium security prison – in and out of the prison system for the past 5 – 6 years for drug related offences. Commenced methadone program while in prison. Has also attended group and individual AOD counselling while incarcerated, though is unlikely to seek out AOD services post release as he is reluctant to retell his story. Further reports that he would have liked AOD and prison staff to know more about his culture.
Participant E – young Maori male aged 23 years. Currently residing in the community. First came into contact with AOD services aged 18 – 21 years as part of a Youth Justice Order. Reports attending four sessions, supported by his older sister. Noted that he was allowed to attend with his sister on a couple of occasions which was especially useful. Calls for more work to be done with the Maori community and families so they can better understand and support people in his situation.
Participant F – Samoan female aged 26 years. Reports supporting her older brother to access AOD counselling, who had been directed to attend by the court. Further reported that the process for her and her brother was not clearly explained, and that it was not inclusive of family members as service providers appeared hesitant to have her involved. Calls for AOD practitioners to be trained in working with families from Pacific Islander and Maori communities.

32
Cultural inventory 4
Pacific Islander and Maori communities (City of Wyndham catchment)
Participant G – young Samoan male aged 23 years. Reports being in and out of the youth and adult Participant G – young Samoan male aged 23 years. Reports being in and out of the youth and adult criminal justice system since he was 13 years of age. First came into contact with AOD services as an adolescent, as part of a Youth Justice Order. Has accessed AOD services 6 – 10 times. Reports being ‘very dissatisfied’ with the support provided by AOD services. Presented to the interview with an Acquired Brain Injury, reportedly due to ongoing substance use. Further reports mental health issues whilst in prison. Noted that his parents have always been supportive but often struggle to understand the system and his situation due to language barriers. Also stated that AOD use has isolated him from his community. Recommends that AOD services partner with churches and community leaders to learn more about working with Pasifika community members.
Participant H – Maori male aged 30 years. Reports first attending AOD counselling in his twenties, with support from his family (mainly brother and mother). Attended on 6 – 10 occasions. Reports being ‘somewhat satisfied’ with the support he received. Currently on the road to recovery, attributed to his family’s involvement in the process. Further reports his counsellor being open to discussing his culture though it was something he had to initiate.
Participant I – Tongan male aged 28 years. Reports coming from a very closed family and community who opts not to discuss these issues. First came into contact with an AOD service in his twenties. Attended residential withdrawal but was a “bad experience”. Reports finding the intake process very stressful and having to tell his story on a number of occasions before admission. Further reports being ‘very dissatisfied’ with the experience, as staff did not work hard to connect with him. Attended for a short period and has not accessed help since. Recommends that more work needs to be done with the Tongan community. Further recommends that staff attend training in working with people from his cultural background.
Participant J – young Samoan male aged 19 years. First contact with AOD services as an adolescent, initially directed to attend by a youth justice worker. Reports being ‘very satisfied’ with the support he received from a youth AOD counsellor, as he was able to discuss issues he had not previously disclosed. Reports feeling like he was talking with a friend. Though only required to attend four sessions he opted to attend a further two sessions. Acknowledges that he would have liked to discuss more about his culture.
Cultural inventory 5
Vietnamese community (City of Yarra catchment)
Vietnamese community in the City of Yarra
The Vietnamese community arrived in Australia in the mid to late 1970s, after Saigon fell to the Communist Government in the north during the Vietnam War, and settled as refugees in areas such as the City of Yarra, transforming the former inner-city working class shopping strip in Victoria Street Richmond into a Vietnamese cultural hub. This part of Melbourne is now often referred to as ‘little Saigon’.
According to the Yarra City Council Multicultural Policy 2010 – 2014, 11.8% of the population in Richmond North, 7.7% in Abbotsford and 7.5% in Collingwood are of Vietnamese birth.
In the early 1980s approximately 50% of Vietnamese immigrants were married but many arrived in Australia without their spouses and as a result often experienced feelings of extreme isolation (Reid et al. 2002). According to Reid et al. this experience of separation was for many deeply traumatic.

33
Cultural inventory 5
Vietnamese community (City of Yarra catchment)
While many people in the Vietnamese community have adjusted well to Australian society, a substantial number have experienced major problems adapting and achieving social acceptance. ‘Culture shock’ has been widely reported (Reid et al. 2012; Australian Institute of Family Studies 1995).
Of particular concern to the Vietnamese community is the over-representation of adults and youth in the criminal justice system, resulting in organisations such as the Australian Vietnamese Women’s Association (discussed below) establishing a support program for Vietnamese prisoners and their families.
Traditionally the father is head of the household – seen as the provider who holds the authority to make decisions of great importance, whereas the mother is primarily responsible for raising and educating children and taking care of financial matters (Tran 1984, cited in Australian Institute of Family Studies 1995). Usually parent-child relationships are based on the principle that children must obey their parents and are charged with looking after them in their old age.
According to Nguyen (1994) there is enough evidence to suggest that most Vietnamese refugees arrived in Australia with few material possessions. Because of economic necessity many Vietnamese women for the first time entered the workforce. This resulted in changes to their role in the home and status within the family. In other families, however, neither parent could find work.
Vietnamese culture is oriented towards the family and the group, where each individual is thought to represent the family as a whole. If an individual loses respect or status in the community, the whole family loses respect and status as well. This loss of face is a key driver dissuading Vietnamese people from reaching out for support.
In terms of communication/media channels the Vietnamese community is well served as they have access to Vietnamese radio and the Viet Times (Melbourne based Vietnamese newspaper). Australian Vietnamese Women’s Association
The Australian Vietnamese Women’s Association (AVWA), formerly known as the Australian Vietnamese Women’s Welfare Association, has been in operation since 1983. Its purposes are to:
Provide a framework for mainly Vietnamese women to collaborate and learn to lead and operate a not-for-profit organisation to assist the settlement and harmonious integration of refugees and migrants of Vietnamese and other backgrounds in Victoria.
Help Victorians, irrespective of age, gender, religion or ethnic background, obtain the information they need, know their rights, responsibilities, options and opportunities, realise their full potential and improve their health, happiness and wellbeing.
AVWA provide a wide range of services, for example:
Community Aged Care and Home Care Packages
Planned Activity Groups
Playgroups
Training services
Support program for Vietnamese prisoners in Victoria and their families
Gambling support services
AVWA (Richmond Office) is located at 30 – 32 Lennox Street Richmond VIC 3121 Ph: (03) 9428 9078
For more information about AVWA go to: www.avwa.org.au

34
Cultural inventory 5
Vietnamese community (City of Yarra catchment)
Perceptions and health beliefs of CALD community members
Oriental medicine, which incorporates traditional Chinese and Vietnamese medicine, is important in Vietnamese culture. Emphasis is placed on the balance of yang (male, positive energy, hot) and yin (female, negative energy, cold), and a proper balance is considered necessary for health to be maintained. Illness is believed to result from an imbalance of yin and yang.
Mental illness is generally considered shameful and is often associated with wrong-doing in a previous life, and is often not discussed in the family or community.
Much attention has been paid to the illicit drug use within the Vietnamese community, with particular reference to the use of opiates. The public housing estate in Richmond has long been identified as a ‘hot spot’ for injecting drug use, raising concerns within the community and general population about the impact of illicit drug use in public spaces.
Individuals engaging in AOD use tend to distance themselves from the community, and in some cases have been disowned by other community members. It is commonplace for people who are using to be seen as shaming their family and the community at large.
It has also been reported that for many community members there is not a distinction between the different patterns of use – you are either ‘using’ or ‘not using’. It is not uncommon for family members to seek a ‘quick fix’, with the expectation that the person using should be admitted into treatment to immediately cease their use.
For many community members AOD use is very much seen through a moral prism. Harm minimisation is not widely understood, with harm reduction messages considered to be condoning drug use and challenging cultural norms.
As many family members are unaware of the available AOD supports it is unlikely that they will contact AOD services. Perceptions of past and current service users
The following information is drawn from 15 participant interviews, conducted by North Richmond Community Health (NRCH) staff with Vietnamese clients accessing the NRCH needle and syringe program (NSP).
Participant A – Vietnamese male aged 45 years. First came into contact with AOD services aged in his thirties. Reports attending AOD services voluntarily on more than 15 occasions, including AOD counselling, withdrawal services (including private residential withdrawal facilities on two occasions), medical support from GPs and NSPs. Further reports a long term relationship with staff at NRCH. Reports being ‘very satisfied’ with the support he has received, though identified language issues when working with interpreters (i.e. need for interpreters to speak more clearly and slowly, and explain terms which he found difficult to understand). Suggests that a Vietnamese worker in the NSP would be beneficial.
Participant B – Vietnamese male aged 48 years. Reports attending AOD services voluntarily on more than 15 occasions, including AOD counselling, withdrawal services and NSPs. Disclosed his preference to work with staff not from a Vietnamese background, as he has had experiences with Vietnamese workers who responded in a judgmental fashion. Client discussed issues regarding opiate replacement – perceived negatively within the community, as well as heroin use which is considered evil amongst many Vietnamese community members.
Participant C – Vietnamese male aged 46 years. Initial contact with outreach AOD worker who arranged an appointment with a methadone prescriber (GP). Reports attending GP service on multiple occasions, with support from the NRCH outreach worker. Disclosed preference for working

35
Cultural inventory 5
Vietnamese community (City of Yarra catchment)
multiple occasions, with support from the NRCH outreach worker. Disclosed preference for working multiple occasions, with support from the NRCH outreach worker. Disclosed preference for working with people who are not Vietnamese, as he has felt judged in the past. Reports that pharmacotherapies are not considered appropriate by many Vietnamese community members, as the person is not deemed to be drug free.
Participant D – Vietnamese male aged 37 years. Reports accessing NRCH on a regular basis for wound care as well the mobile NSP outreach service. Also regular contact with local pharmacotherapy (methadone) prescriber. Has received some support from family. Further reports being ‘somewhat satisfied’ with the support he has received from AOD practitioners due to the differences in knowledge between workers. Client also noted that at times it would be useful to liaise with staff who were fluent in Vietnamese or Cantonese.
Participant E – Vietnamese male aged 46 years. Has voluntarily sought AOD counselling, medical support and NSP support. Reports being ‘very satisfied’ with the support he has received from AOD services. Noted that at times it has been difficult to liaise with an interpreter when he has not come across the interpreter before. Recommended that there be a greater mix of cultures working in the AOD field, and that workers spend more time with each client to build relationships.
Participant F – Vietnamese clients aged 50 years. Has voluntarily sought AOD counselling, withdrawal services and medical support. Has also regularly attended the NRCH NSP. Reports being ‘very satisfied’ with the support received from AOD services, noting they are “always friendly”. Further reported receiving some support from his sister. Recommended that more education be provided to older Vietnamese community members as “drug users are not bad people.”
Participant G – Vietnamese male aged 42 years. Reports attending multiple AOD services on more than 15 occasions, both voluntarily and directed to attend by the courts/police, including AOD counselling, withdrawal services, medical services and NSPs. Currently on a methadone maintenance program. Reports being ‘very satisfied’ with the support he has received from AOD services, though would prefer more access to interpreters as well as more culturally appropriate food when attending a residential withdrawal service.
Participant H – Vietnamese male aged 55 years. Reports attending multiple AOD services on more than 15 occasions, both voluntarily and directed to attend by the courts/police, including AOD counselling, withdrawal services, medical services and NSPs. Has obtained support letters from outreach staff for court and other service providers. Notes that at times he felt he could not be open or honest with staff for fear of being judged. Reports being ‘very satisfied’ with the support he has received from AOD services, though would prefer more access to interpreters. Also noted that he preferred to be seen by non-Vietnamese workers.
Participant I – Vietnamese male aged 34 years. Reports attending AOD counselling voluntarily at NRCH prior to the AOD sector reforms, and has attended residential withdrawal services. Regularly attends NRCH NSP – more than 10 times per month. Has received some support from family to access AOD services. Reports being ‘very satisfied’ with the support he has received from AOD services, though would have preferred to be served Vietnamese food when admitted into residential withdrawal.
Participant J – Vietnamese male aged 36 years. Reports attending AOD counselling voluntarily on a monthly basis for approximately 12 months. Has regularly attended the NRCH NSP service, citing that he would prefer to see its hours of operation extended as he is employed. Client has received support from family in accessing AOD services – with his sister making appointments on his behalf. Reports being ‘very satisfied’ with the support he has received from AOD services, though reports increased access to interpreters as a service improvement.

36
Cultural inventory 5
Vietnamese community (City of Yarra catchment)
Participant K – Vietnamese male aged 63 years. Reports attending multiple AOD services on more Participant K – Vietnamese male aged 63 years. Reports attending multiple AOD services on more than 15 occasions, generally on a voluntary basis, including AOD counselling, medical services and NSPs. Accesses GP services for general health, liver function tests and referrals to the Hepatitis C clinic. Reports seeking assistance from the AOD counsellor to access AOD services. Also reports being ‘very satisfied’ with the support he has received from AOD services. Notes that he would prefer to see a bilingual Vietnamese worker at NRCH main reception.
Participant L – Vietnamese male aged 26 years. Reports attending AOD services including AOD counselling, medical services and the NRCH NSP. Is currently on a methadone maintenance program. Has received support from NRCH staff to access AOD services. Reports being ‘very satisfied’ with the support he has received from AOD services, citing that they have been very helpful in accessing interpreters. Notes that he would prefer to be seen by non-Vietnamese staff as he will not be judged.
Participant M – Vietnamese male aged 50 years. Reports attending multiple AOD services voluntarily for the past 21 years including AOD counselling, medical services and NSPs. Supported by the NRCH outreach clinician to make appointments with the GP and clinic nurse for access to pharmacotherapy program and wound care. Reports being ‘very satisfied’ with the support he has received from AOD services, citing that he can always use the phone to make calls. Notes that he prefers to work with non-Vietnamese workers as he will not be judged.
Participant N – Vietnamese male aged 38 years. Reports attending multiple AOD services, both voluntarily and directed to go by the courts/police, including AOD counselling, withdrawal services, medical support and NSPs. Has worked with outreach staff for support while at court. Notes that he is happy to use a Vietnamese interpreter (over the phone), and would prefer to see a Vietnamese speaking pharmacotherapy prescriber. Reports being ‘very satisfied’ with the support he has received from AOD services, but would like to see more Vietnamese speaking workers, follow up and support calls, as well as more pharmacotherapy prescribers at NRCH rather than going to another service.
Participant O – Vietnamese male aged 47 years. Reports attending multiple AOD services on a voluntary basis, including AOD counselling, withdrawal services, medical support and NSPs. Attends NRCH NSP twice weekly. Has received assistance from NRCH outreach team for support with Centrelink and a referral to a residential withdrawal service. Reports being ‘very satisfied’ with the support he has received from AOD services. Notes that some workers require cultural training particularly related to working with Vietnamese clients, the stigma in the community of injecting drug use, how it impacts on the family and providing culturally appropriate support. Also noted that he is happy to work with a Vietnamese interpreter, so long as it is over the phone.
3.1.5 Audit of consumer and worker resources
In November 2014 a web-based search (audit) of CALD and AOD resources was conducted to
identify:
AOD materials specifically targeting CALD service users
Relevant practice guides or tools for staff working with CALD clients
Materials on the health literacy needs of CALD populations (related to AOD and other
health issues)

37
Government policies and other sector-related documentation
Sites where these resources could be found
Resources were identified using an on-line search and ‘snowball sampling’ method, targeting key
stakeholder agency websites prominent in the CALD AOD space (predominantly state and
national). For example:
Centre for Culture Ethnicity and Health website – www.ceh.org.au
Drug and Alcohol Multicultural Education Centre website – www.damec.org.au
Centre for Multicultural Youth website – www.cmy.net.au
Victorian Refugee Health Network website – www.refugeehealthnetwork.org.au
Health Translations Directory website – www.healthtranslations.vic.gov.au
Centre for Cultural Diversity in Ageing website – www.culturaldiversity.com.au
VICSEG New Futures website – www.vicsegenewfutures.org.au
Below is a summary of the findings from the consumer and worker resource audit, including
details regarding consumer resources, practice guides and tools for staff working with CALD
clients and government policies and other sector-related documentation.
See attached database for a detailed list of the resources covered in the audit.
Consumer resources
There are limited CALD AOD resources (translated or in English). Notable gaps include:
o Harm reduction materials targeting specific CALD community/groups (using
culturally appropriate terminology and messaging)
o Information on AOD services within each catchment, how to access them and how
they operate
o Harm reduction information pitched at CALD families – available information is
generally preventative in its focus and generic in content (text translated into
multiple languages)
Many of the available resources need updating. It is also uncertain whether many of
these resources have been ‘road tested’
Different formats have been used, though most are available in written form
(e.g. brochures and fact sheets). For IT literate consumers materials in audio visual
formats are available (highlighting use of digital media to communicate CALD clients’
lived experiences)
Practice guides and tools for staff working with CALD clients (including health literacy materials)
Multiple worker resources have been developed (including tip sheets, practice guides,
tools and other publications), though very few are AOD specific
Most of these materials focus on strategies related to effective communication (e.g.
using interpreters), recruiting bilingual staff and/or supporting CALD clients with
particular needs (e.g. settlement support)

38
Multiple health literacy resources have been developed though most are not AOD
specific (often targeting asylum seekers and refugees) in need of primary care or allied
health services
Government policies and other sector-related documentation
Multiple government policies and other sector-related publications are readily available
– establishing service standards and benchmarks for the development and
implementation of culturally responsive services
3.2 Supporting cross-sector collaboration
In the second half of the project VAADA operated in five locations across the state, targeting
specific CALD communities in each site, with a view to:
Use existing networks to bring together workers and others involved in the project to
discuss how AOD services can better meet the needs of individuals and families from the
selected CALD communities
Liaise with agencies to strengthen the ties between AOD and CALD services and the
communities thy work with
Work with communities and others to develop culturally appropriate resources
This second stream of activity – supporting cross-sector collaboration – was undertaken after the various target populations had been selected and each catchment established. It included the following three components:
1. Initial roundtable discussions 2. Agency site visits 3. CALD AOD forum
3.2.1 Initial roundtable discussions
In each of the five catchments CALD representatives (community leaders and practitioners) as well as key decision makers from the relevant AOD agencies were invited to come together to meet each other and participate in a roundtable discussion. Those attending:
Shared a meal while meeting with other participants
Discussed issues related to the AOD service needs of CALD community members, with the emphasis on giving and receiving targeting feedback and raising awareness of each party’s needs, expectations and perceptions
Shared their views, knowledge and experiences with other participants
Each roundtable discussion was divided into three parts. See Table 2 for details.

39
Table 2. Initial roundtable discussion – overview
PART 1
Welcome and introductions
CALD AOD Project – overview and findings
Participants provided with a brief overview of the CALD AOD Project, including:
History of the project
Aims, objectives and structure of the roundtable discussion
Project findings (pertaining to the target CALD population)
PART 2
Q&A session AOD treatment providers invited to respond to questions and issues put forward by community representatives
Q&A session Community representatives invited to respond to questions and issues put forward by AOD treatment providers
BREAK
PART 3
Site visits and resource development options
Scoping out site visit options (subject to community member interest and AOD service availability). Participants also invited to discuss consumer and worker resource development options
LUNCH
While all of the meetings followed this basic structure, each needed to be tailored to cater for the specific needs of the target CALD population. Notably:
All meetings involved male and female community members, however for the Afghan Hazara community the large group was divided into two gender specific groups (male and female). This was suggested by participants as the most effective way to ensure all viewpoints were heard
Where necessary on-site interpreters were also made available – applicable to the Afghan Hazara and Vietnamese roundtable discussions
Approaching the Afghan Hazara community directly about AOD matters is not culturally appropriate nor is it considered sensitive (due to the stigma and shame associated with AOD use). For this reason the decision was made to focus on health and wellbeing more generally, with AOD use representing but one of the underlying issues for consideration. As such, allied health practitioners were also invited to the meeting
Roundtable discussions took place from Tuesday 18th – Monday 31st August 2015. Feedback obtained and issues raised were documented and subsequently distributed to each meeting’s participants for review. Refer to Appendix B (pages 68 – 76) for a summary of the issues raised in each roundtable discussion.

40
3.2.2 Agency site visits
During each of the roundtable discussions CALD community representatives were invited to attend one or more agency site visits. Site visits were conducted in four of the five catchments (not including the City of Greater Shepparton – Afghan Hazara community), with the first agency visit taking place on Wednesday, 7th October and concluding on Thursday, 18th November 2015.
The purpose of the site visits was threefold:
1. Giving CALD community representatives the opportunity to familiarise themselves with each service’s operation while learning more about the various treatment options – differentiating between residential withdrawal, residential and non-residential rehabilitation, counselling and assertive outreach
2. Giving AOD practitioners the opportunity to liaise with CALD community members directly about their specific AOD needs and discuss ways treatment could be modified to better meet their needs
3. Strengthening the ties between CALD communities and local AOD service providers
The precise mix of site visits was determined by the participants in each catchment, subject to CALD stakeholder interest and AOD service availability. The format of each visit was determined in collaboration with CLWs and the individual service provider.
Table 3 outlines the schedule for agency visits.
Table 3. Agency site visit calendar
Date and time Service details – overview
Wednesday, 7th October 2015
6.00 – 8.00 pm
REVAL day program – Youth Support and Advocacy Service (Dandenong)
Structured program for young people aged 12 – 21 years with AOD issues. Running group programs including music, graphic design, fashion, adventure therapy, health and fitness – delivered with an emphasis on transitioning into education, employment or training
Thursday, 8th October 2015
9.00 – 10.00 am
Living Room – Youth Projects (Melbourne CBD)
Drop-in primary health service providing free healthcare and support to improve the physical, mental and social wellbeing of individuals who are homeless or at risk of homelessness, disadvantaged or marginalized, with complex health needs
Providing broad range of services (e.g. health care, shower and laundry, housing support, referral and legal support)

41
Date and time Service details – overview
Friday, 16th October 2015
1.30 – 3.00 pm
Youth Residential Withdrawal Service – Youth Support and Advocacy Service (Glen Iris)
Provides young people aged 12 – 21 years with intensive support to undergo respite or withdrawal from AOD use. Operating 5 beds for stays up to 14 days
Thursday, 22nd October
1.30 – 2.30 pm
Youth Residential Withdrawal Service – Youth Support and Advocacy Service (Fitzroy)
Fitzroy Youth Residential Withdrawal Service provides young people aged 12 – 21 years with intensive support to undergo respite or withdrawal from AOD use. Operating 8 beds for stays up to 14 days
Wednesday, 28th October 2015
10.00 am – 1.00 pm
UnitingCare ReGen – central office (Moreland)
Key AOD service provider operating across a number of catchments – Inner North, North and North West Melbourne
Provides a broad range of services, including intake and assessment, counselling, care and recovery (targeting individuals with complex needs), residential and non-residential withdrawal, non-residential rehabilitation, education programs etc
Thursday, 19th November 2015
10.00 – 11.30 am
Residential Therapeutic Community – Odyssey House (Lower Plenty)
Therapeutic community providing live-in treatment for adults, couples and parents with children (aged 0 – 12 years). Program offers a structured environment, with up to 97 residents and 30 staff
All residents participate in the decision making of the community. They are also expected to contribute through cooking, cleaning and working on property development and maintenance
3.2.3 CALD AOD forum
On Monday, 30th November 2015 stakeholders from across the five catchments as well as other interested parties came together for a full-day forum. The purpose of the Crossing the cultural divide forum was to:
Review the project’s findings and raise awareness of CALD AOD issues – exploring key issues raised during the project
Showcase examples of best practice currently in place within the catchments
Formally launch consumer and worker resources
Facilitate discussions on strategic approaches to working with CALD community members in need of AOD treatment, information and support
Promote networking and information sharing within and across CALD and AOD sectors

42
In total, 139 participants attended the forum including CALD representatives and practitioners, key personnel from the relevant AOD services located in each catchment, PRG members, Department of Health and Human Services staff and other interested parties. Refer to Appendix C (pages 77 – 81) for the CALD AOD forum program and evaluation summary.
4. WORKER AND CONSUMER RESOURCES One of the key activities undertaken by project staff (in collaboration with CALD liaison workers operating in each of the five sites) was to develop a number of CALD AOD resources, including:
Three AOD practitioner tip sheets
Five catchment specific postcards
Crossing the cultural divide poster
4.1 AOD practitioner tip sheets
The AOD practitioner tip sheets outline key issues for consideration for frontline staff when working with clients from CALD communities. Each tip sheet has been developed for use by clinical staff working in a specific AOD treatment setting, including Intake and Assessment, Residential Withdrawal and AOD Counselling. These guides draw on information obtained from the five CALD communities as well as consultations with key AOD and allied health service providers, and are intended to build on existing resources currently available to workers within and outside of the AOD sector.
See Appendix D (pages 82 – 87) for the following AOD practitioner tip sheets:
Cultural Cues: Working with cultural diversity in AOD Intake and Assessment settings
Cultural Cues: Working with cultural diversity in Residential Withdrawal settings
Cultural Cues: Working with cultural diversity in AOD Counselling
4.2 CALD consumer promotional materials In addition to the practitioner guides five postcards were developed, one per catchment with each postcard directed at one of the five target communities. Designed primarily for bi-cultural workers to hand out to individuals and/or family members within their respective communities, each card includes a plain language statement (in English, and on the reverse side its translation to the relevant community language), encouraging community members in need of AOD support to contact their local AOD service.
Using the same design language a poster was also developed. The poster is intended to be displayed in community health centres, mosques, GP settings and other public spaces where CALD community members are likely to be present. Like the postcards, the poster includes a

43
statement encouraging community members in need of AOD support to reach out for assistance. The poster is not catchment specific as it lists the contact details for DirectLine (statewide telephone information and referral service). Note. Design of the postcards and poster incorporate culturally specific motifs (themes) provided by the CLWs intended to represent the five target CALD communities. CLWs were also consulted with respect to the statements used in the postcards and poster to ensure they were both culturally appropriate and legible.
See Appendix E (pages 88 – 92) for the five Crossing the Cultural Divide postcards, and Appendix F (page 93) for the Crossing the Cultural Divide poster.
5. PROJECT FINDINGS AND
RECOMMENDATIONS
5.1 Project findings and recommendations
Key project findings are drawn from a thematic analysis of the evidence obtained during the
literature review and follow-up consultations with AOD, CALD and allied health practitioners,
CALD community members and other interested parties.
In order to address the issues raised in the findings we have also incorporated 11
recommendations. These recommendations identify specific actions which VAADA believes will,
if enacted, significantly enhance the capacity of AOD services to cater for the needs of individuals
and families from CALD backgrounds who are experiencing harms associated with AOD use.
Interspersed throughout this section are five examples of best practice demonstrating where
such measures have already been enacted.
a) Limited data on the prevalence of AOD use within CALD communities
At present there is very limited data available on the prevalence of AOD use within CALD
communities, and while much of the research suggests that levels of AOD use is low compared to
the general population, questions have been raised as to their validity, especially large scale
studies which do not specifically target a particular CALD community.
At the heart of this issue is how ‘ethnicity’ is defined. While ethnicity is a multidimensional
concept incorporating a range of variables, many of the studies rely solely on country of birth
and/or language spoken. Other factors, most notably self-identified ethnicity, migration or visa
status and year of arrival are generally not included in the data set, thus providing a narrow and
simplistic interpretation of CALD status.
Compounding this issue are the data collection tools currently used by AOD treatment agencies
to identify people from CALD backgrounds, which generally rely solely on country of birth and
preferred language spoken.

44
In addition, social taboos which are prominent in many CALD communities dissuade those
engaging in AOD use from coming forward for fear of being ostracized. As a result much of the
formal research is constrained by low participation rates (Beyer & Reid 2000; Browne et al. 2000).
Another consideration is the limited number of studies which have been conducted, many of
which were undertaken some time ago, raising questions about their applicability to the present
day. This is especially important when we consider the dynamic nature of drug use, affected by
fluctuations in the availability of different substances as well as the emergence of new drugs
(e.g. synthetic cannabis).
Recommendation 1: That existing AOD screening and assessment tools utilised
by Victorian AOD practitioners be reviewed to examine their applicability to CALD
populations, with the aim of:
More effectively identifying each person’s ethnicity and cultural background
Establishing more flexible and culturally sensitive screening and
assessment processes tailored to each cultural group
Recommendation 2: That further research and capacity building initiatives be
conducted into the prevalence of AOD use within CALD communities, as well as
the health literacy needs of CALD community members and the experiences of
individuals and family members navigating the AOD service system
b) Under-representation of CALD communities in the AOD treatment system
CALD communities are significantly under-represented in the AOD treatment system, with data
showing only 5% of closed treatment episodes for Victoria in 2013 – 14 applied to clients born
overseas (AIHW 2015). When we consider that in 2011 26% of Victoria’s population was born
overseas, it is clear that the proportion of CALD clients is very low.
Given the limitations of existing data collection tools, these figures are put forward merely as an
indicator of service utilisation.
Note. In 2013 – 14, Victorian AOD treatment agencies provided 52,848 closed treatment episodes. Of this
number 91% (n = 48,122) were provided to clients born in Australia, 5% (n = 2654) were provided to clients
born overseas and 4% (n = 2072) were provided to clients who did not state their country of origin (AIHW
2015).
c) Barriers to accessing AOD treatment, information and support
Admission rates of CALD clients into AOD treatment are due to an under-utilisation of services
rather than a lower need, which is to be expected given the broad range of service barriers and
socio-cultural norms making it difficult for individuals and families to access treatment. They
include:
Lack of trust in mainstream services
Lack of awareness of the available services and how they operate
Stigma, shame and fear of the consequences dissuading people from seeking assistance
Community perceptions that services are inflexible and insensitive to their cultural needs

45
Culturally inappropriate service delivery
Language barriers
Confidentiality concerns
Compounding these factors are the recent reforms to the Victorian AOD sector (adult service
system) which has decreased the capacity of many providers to work effectively with CALD
communities. Often cited is the reliance on centralised assessment and intake processes which
effectively preclude CALD individuals and family members from accessing services, as many
people from CALD backgrounds are reluctant to attend a specialist AOD service for fear of being
identified as a ‘drug user’. Other factors include a lack of awareness of available services and
how they operate, community perceptions that services are inflexible as well as a lack of trust in
mainstream service providers. Thus, alternative entry pathways are urgently required.
Recommendation 3: That the existing AOD sector catchment based intake and
assessment system be reviewed and reworked (in consultation with CALD
community leaders and other representatives) to enable alternative referral and
entry pathways for individuals and family members from CALD backgrounds
Recommendation 4: That culturally specific AOD resources be developed for
distribution by AOD and allied health practitioners, bi-cultural workers, CALD
community leaders and other representatives, with priority given to the use of
audio visual materials (catering for the needs of community members with low
language proficiency while providing more engaging and contemporary sources of
information)
Recommendation 5: That AOD education and health promotion campaigns be
undertaken in each of the catchments targeting specific CALD communities,
utilising culturally appropriate messaging, communication tools and media
channels (e.g. multicultural radio and newspapers), with priority given to:
Reducing stigma and shame associated with AOD use
Raising awareness of available AOD services, how to access them and how
they operate
Increasing community members’ knowledge of the potential harms
associated with AOD use as well as appropriate harm reduction strategies
Rebuilding relationships and addressing family inter-generational conflict
Best practice example 1
Catching Up – Turning Point Alcohol and Drug Centre and Multicultural
Centre for Women’s Health
Currently in its fourth year Catching Up is a project undertaken by Turning Point Alcohol and Drug Centre and the Multicultural Centre for Women’s Health, aimed at increasing awareness of Dual Diagnosis issues across five CALD communities, including:
Arabic speaking
Polish
Spanish speaking

46
Best practice example 1
Catching Up – Turning Point Alcohol and Drug Centre and Multicultural
Centre for Women’s Health
Sudanese
Spanish speaking
Sudanese
Vietnamese
A key feature of the project has been the support and training provided to community leaders and peers enabling them to engage fellow community members in various activities related to problematic AOD use and mental health. For example, the development and dissemination of consumer resources, announcements and discussions on ethnic radio as well as community education sessions delivered in the relevant language. Additionally, cross cultural training and capacity building activity has been undertaken in the Victorian AOD sector.
For more information about Catching Up go to: www.turningpoint.org.au or www.mcwh.com.au
d) Bypassing the AOD treatment system
For those individuals from CALD backgrounds who come into contact with AOD services, it is
often due to their involvement in the criminal justice system, raising concerns about the numbers
of individuals from CALD backgrounds who are effectively bypassing treatment services and other
supports.
Anecdotal feedback from CALD liaison staff, as well as case summaries provided by community
members regarding their AOD service user experience, reveal a high proportion of individuals
whose experience with AOD treatment either took place in a prison or another forensic setting.
Analysis of this data shows that of the 38 respondents 50% (n = 19) had been directed to attend
AOD treatment by the courts / police.
At the same time available data from the Australian Bureau of Statistics (ABS) in 2015 shows that
a number of CALD communities are subject to elevated imprisonment rates across the country,
including Sudan (767.7), Tonga (441.2), Samoa (419.2), Colombia (368.6) and Vietnam (362.2).
This compares to an imprisonment rate for the Australian born population of 237.5.
Note. Imprisonment rates are calculated per 100,000 adult population.
As of 30 June 2015 overseas born prisoners accounted for 25% (1,551 prisoners) of the Victorian prison
population. The largest number were from Vietnam (313 prisoners or 20% of the overseas born
population) followed by New Zealand (174 prisoners or 11% of overseas born prisoners) (ABS 2015).
Recommendation 6: That resources be directed to tailoring diversion programs
aimed at reducing the high proportion of individuals (especially young people)
from CALD backgrounds entering the criminal justice system for AOD related
offences

47
Best practice example 2
Police Youth Leaders Engagement Team – Victoria Police
The Police Youth Leaders Engagement Team (PYLET) is a targeted community policing program which was developed by the Police Multicultural Unit in Melbourne’s Southern Metro Region. It commenced operation in 2013 and focuses on building relationships with ‘at risk’ CALD youth in and around the City of Greater Dandenong. In 2014 the program was expanded to Frankston.
Using an assertive outreach model police officers patrol the streets on Friday and Saturday nights alongside volunteer youth leaders. Their aim is to prevent anti-social behaviour by proactively engaging young people and linking them into the relevant supports (where appropriate).
PYLET emerged in response to concerns regarding public drunkenness, violence and other anti-social behaviours, leading to multiple arrests and fines. As a result tensions arose between police and young people from CALD backgrounds who alleged they were being vilified and discriminated against.
Since its inception PYLET staff have worked closely with a range of local service providers, most notably the Youth Support + Advocacy Service, a local AOD treatment service, leading to many young people successfully engaging in AOD support while avoiding further legal sanctions and in some cases imprisonment.
For more information about PYLET go to: http://dandenong.starcommunity.com.au/journal/2014-07-28/team-helps-find-the-lost-generation/
e) Impact of socio economic disadvantage, pre- and post-migration stressors and other
risk factors
Adjustment to a new culture places considerable pressure on migrants, who often experience
feelings of dislocation, isolation and grief. When these are compounded by the shame and ‘loss
of face’ associated with AOD use (especially illicit drug use), the impact can be overwhelming on
individuals as well as their families as they attempt to keep things hidden from view. It is
therefore critical when working with CALD clients that AOD and other health providers also focus
on the needs of their families, taking into consideration a broad range of risk factors:
Socio economic disadvantage
Settlement experiences (pre- and post-migration) leading to difficulties adjusting to a
new cultural environment
Stigma associated with AOD use
Family conflict
Co-occurring mental health issues
Language barriers and low health literacy (including knowledge of AOD harms and
available supports)
Of these factors socio-economic disadvantage has been identified as most influential in increasing
the likelihood of problematic substance use, challenging the myth that ethnicity is the key factor
(Beyer & Reid 2000).

48
f) Populations considered most ‘at risk’
During the course of the project a number of CALD populations were identified as most ‘at risk’:
Individuals and families from newly arrived and emerging communities (with particular
reference to asylum seekers and refugees)
Young men and women from African communities, many of whom arrived as asylum
seekers and refugees
Younger and older men from different Pacific Islander and Maori communities
People who inject drugs (most notably younger and older Vietnamese, Cambodian and
Laotian men who are long term opiate users)
Arabic and Turkish speaking men and a range of different groups from the Middle East
from established communities as well as more recent arrivals
CALD women from a range of cultural backgrounds in need of pre- and post-natal support
International students from a range of different cultural backgrounds
Across all groups men were cited as those with the highest rate of problematic AOD use and
therefore most in need of AOD treatment. CALD women did not receive the same attention,
though it was generally accepted that they are by comparison a hidden population. Further
research and analysis is required to better understand the specific needs of women and the role
gender plays in relation to AOD use within CALD populations.
Best practice example 3
Peer Networker Program – Harm Reduction Victoria
The Peer Networker Program (PNP) is an initiative of Harm Reduction Victoria, a peer-based organisation working closely with people who use illicit drugs across the state. The aim of this program is to reduce the spread of hepatitis C and other blood borne viruses (BBVs) by increasing access to sterile injecting equipment, targeting those who inject drugs but who are not presenting to Needle and Syringe Programs (NSPs).
According to NSP statistics, young people (particularly women) as well as individuals from CALD and Aboriginal or Torres Strait Islander backgrounds are under-represented. In response, ‘peer networkers’ have been recruited from within these under-represented groups to distribute injecting equipment to their friends and associates while providing education and support about safer drug use.
Once recruited, peer networkers attend a training program and on completion are registered as volunteers and authorised NSP outreach workers. Training is delivered over five days and includes information on the program, overdose prevention and naloxone training, safer using and vein care, BBVs, how data is collected and confidentiality.
At present PNP operates across a number of sites – Footscray, Richmond, Braybrook, Geelong and Frankston. In each site peer networkers attend monthly meetings to provide status reports and alert program staff of any immediate risk issues, support each other and discuss possible health promotion campaigns.
When we consider the prevalence of injecting drug use within some CALD communities (with particular reference to Cambodian, Laotian and Vietnamese communities), and the associated harms, it is clear that PNP is an important initiative.
For more information about PNP go to: www.hrvic.org.au

49
g) Importance of community engagement and relationship building
Improving the capacity of AOD agencies to provide culturally responsive services is largely
predicated on their ability to engage with community members, at the individual, family and
community wide levels.
While there are exceptions, the ties between AOD service providers and CALD communities have
not been strong. For a number of reasons this continues to be the case. Of particular concern
are current AOD system arrangements which do not include community engagement or
relationship building as funded activities. At present most of the emphasis lies on the delivery of
treatment types which require the service user to present to an AOD service.
As noted previously, there are multiple barriers limiting access to AOD treatment. For agencies
to effectively address these barriers (e.g. mistrust in mainstream services or lack of awareness of
the supports available to them) it is incumbent on practitioners to reach out to the communities.
Assertive outreach is a model well suited to this task.
This view was articulated by a youth outreach worker operating in Melbourne’s outer east –
pertaining to working with hard to reach young people from CALD backgrounds.
If there’s a magic wand I would have all the NGOs (AOD and non-AOD) commit strongly to
having a focused assertive outreach team to take their work, their organisation, into the
space of young people in need, because a lot of them work in the traditional model of come
to our office. It doesn’t work. In spring and summer all the kids are out on the street. You
need all the organisations to be out there with them. Once you’ve established rapport and
built trust with the young person then bring them into the service and encourage them to
work through deeper issues. Kids are slipping through the gaps because they are simply not
going to attend a Western organisation and work in that framework. They need people to
come to them.
While the CALD AOD Project was focused primarily on the AOD health needs of migrants, it is clear that approaching some CALD communities directly about AOD matters is not culturally appropriate nor is it sensitive (due to the stigma and shame associated with AOD use). For this reason it may be necessary to focus on health and wellbeing more generally, with AOD use representing but one of the underlying issues for consideration. Another point is the importance of attending cultural events and social gatherings, identified as a
key priority across the various target CALD communities. The more time practitioners spend with
the community the greater the opportunities to establish trusting relationships. It is important to
note this is an intensive and incremental process, with investment needing to take place over the
long term.
In order to meaningfully engage with CALD communities it is also necessary to work in partnership. Identifying and seeking support from CALD community leaders, bi-cultural workers and other representatives is critical. This approach demonstrates respect while creating opportunities for seeking community input as well as a sense of community ownership in program design and service delivery.
Recommendation 7: That resources be directed into establishing CALD specific
community engagement positions (a team of bi-cultural workers per catchment)

50
whose role will be to:
Engage CALD communities and agencies with the emphasis on relationship
building and cross-sector collaboration
Raise awareness of available supports while facilitating access to AOD
treatment for individuals and families from CALD communities
Liaise with CALD communities and/or representatives about their specific
health literacy needs, experiences navigating the AOD sector and ways to
improve the system
Advocate and promote culturally appropriate models of service delivery
while strengthening the ties between CALD communities, ethno-specific
agencies and AOD services
Recommendation 8: That AOD agencies be supported to establish interagency
partnerships and protocols with CALD organisations, thus ensuring more
accessible, holistic and culturally safe services for individuals and family members
impacted by harmful AOD use
h) Professional development needs of CALD and AOD practitioners, allied health
professionals, community leaders and other representatives
During the course of the project consultations were held with both CALD and AOD practitioners.
For CALD practitioners much of the attention centred on ways to increase workers’ knowledge of
the available AOD services in their catchment, how to access them and how each service type
operates.
For AOD workers their professional development needs lay elsewhere, with the emphasis on
learning more about how to undertake culturally appropriate AOD screens and assessments,
tailoring how one works with CALD clients in different treatment settings, the cultural nuances of
working with individuals and families from different CALD backgrounds, working with interpreters
and how to engage communities as a whole to establish stronger ties and build partnerships.
See attached consultation report for more information.
Recommendation 9: That further resources and training be developed for AOD
practitioners, aimed at increasing workers’ capacity to engage and support
individuals and family members from CALD backgrounds in need of AOD
treatment, with priority given to increasing participants’ knowledge of:
Pre- and post-migration stressors and how they impact on AOD use –
differentiating between established and new and emerging migrant
communities (with particular reference to asylum seeker and refugee
populations)
Culturally appropriate AOD screening and assessment
Strategies and therapeutic approaches for working with individuals and
families from CALD backgrounds (applied to different treatment settings)
The use of language services support to address language barriers and
other communication difficulties

51
Recommendation 10: That a cross-sector leadership program be established
targeting designated AOD and allied health personnel, CALD community leaders,
bi-cultural workers and other stakeholders in each catchment, with a view to:
Promoting stronger ties between mainstream AOD and allied health
services, CALD communities and ethno-specific agencies
Enhancing participants’ capacity (CALD women and men) to act as
advocates/champions and ‘bridges’ into the AOD system
Identifying suitable capacity building initiatives and putting them into
practice
i) Need for a targeted and multi-faceted approach
It is clear that working with CALD clients in need of AOD support is not a simple undertaking,
requiring what is a targeted and multi-faceted approach. At present this appears to be
happening in a limited and fragmented way, with staff and agencies (CALD and AOD) constrained
in their capacity to cater for the specific needs of individuals and families from CALD communities
affected by harmful AOD use.
What is required are measures both at the micro and macro levels which recognise the specific
health literacy needs of different populations, leading to the development of suitable service
delivery models.
Recommendation 11: That agencies be supported to develop culturally
appropriate service delivery models (in partnership with local CALD communities),
incorporating each of the following service characteristics:
1. Assertive outreach and an emphasis on linkage and service navigation
support
2. Longer timeframes for engagement and treatment as well as more flexible
appointment arrangements (e.g. drop-in services)
3. Recruitment and use of skilled bi-cultural workers as well as peer led
models of service delivery
4. Focus on community engagement, relationship building and family
inclusive practice
Best practice example 4
Brimbank Young Men’s Project – Centre for Multicultural Youth and
Youth Support + Advocacy Service
The Centre for Multicultural Youth (CMY) and Youth Support + Advocacy Service (YSAS) are both well versed in working with young people from CALD backgrounds, especially those who are marginalised and difficult to engage.
A case in point is a pre-pathways engagement project they collaborated on in 2010 – 11 in the Western suburbs of Melbourne, known as the Brimbank Young Men’s Project. Targeting mostly young Sudanese men (aged 16 – 25 years), support was provided in areas such as education and training, recreation, social engagement and AOD treatment.

52
Best practice example 4
Brimbank Young Men’s Project – Centre for Multicultural Youth and
Youth Support + Advocacy Service
Most of the young men had been in Australia for some time (up to seven years), drawing the attention of local services, the broader community and the police. They had come to people’s attention for drinking heavily in groups in local parks and other public spaces.
A number of staff involved in this project were interviewed, including workers from both agencies (CALD and AOD). In one of the interviews an AOD practitioner made this statement, in reference to the first 6 – 12 months of the project:
It took a long time to build rapport and establish relationships within the group … the initial response varied, one or two would engage but initially most of the group were standoffish. Providing food and water was an integral tool in the process, because in their eyes it gave the outreach workers a reason for being there.
Eventually after much effort and preparation some of the young men were admitted into a residential withdrawal facility. To maximise the likelihood of success, a number of measures were put into place:
The young men were admitted into the unit as one group (sole residents at the time), which
made it a less intimidating experience
Recruiting peer facilitators who visited the young men in detox and provided encouragement
and support
Cultural information sessions delivered to residential withdrawal staff – giving them insight into
what was culturally appropriate for this group of African youth
Since that first group were admitted there have been a series of follow-up admissions, though on a smaller scale. Future episodes involved pairs of African young people entering the withdrawal unit.
This project is notable as it clearly demonstrates a person-centred approach to service delivery, involving a range of staff from different agencies (CALD and AOD) who collaborated strongly with each other while being prepared to adjust existing work practices to meet the specific needs of a particular cultural group.
For more information about the project go to: www.cmy.net.au/publications
Best practice example 5
Multicultural Health and Support Service – Centre for Culture, Ethnicity
and Health
The Multicultural Health and Support Service (MHSS) is a program of the Centre for Culture, Ethnicity and Health. MHSS works with refugees, asylum seekers, migrants and mobile populations in metropolitan Melbourne and regional Victoria to prevent new incidents and transmission of blood borne viruses (BBV) and sexually transmissible infections (STI). MHSS collaborates with priority communities to improve their access to information, testing, care and support. MHSS also works with service providers to build capacity in designing and implementing culturally competent and inclusive services that provide relevant care and support to refugee and migrant communities.
Its service delivery model includes:

53
Best practice example 5
Multicultural Health and Support Service – Centre for Culture, Ethnicity
and Health
Community education – raising communities’ understanding of BBV/STI issues and provide specialized community education sessions to priority communities and population groups
Community action – building the capacity of members from priority communities in planning, design, implementation and evaluation of community led BBV/STI projects
Support for connections and outreach – providing, on a time limited basis, appropriate support that assists a client’s journey through testing, diagnosis, treatment, care and support for BBV/STI
Organisational capacity building, advocacy and sector development – building capacity across sectors to enhance service coordination and improve culturally competent service delivery among organisations. MHSS is also collaborating in social research to understand the BBV/STI needs of communities, and advocating for the health rights of multicultural communities by influencing policy and enhancing evidence based practice
For more information about MHSS go to: www.ceh.org.au
5.2 Discussion
This project has sought to shed light on what is an especially complex situation. Individuals and
families from CALD communities are under-represented in the AOD treatment system, attributed
to a range of service barriers and socio-cultural norms which make it difficult for individuals and
families affected by problematic AOD use to access relevant information, support and treatment.
It is clear that working with CALD clients in need of AOD support is not a simple undertaking,
requiring what is a targeted and multi-faceted approach. At present this appears to be
happening only on a piecemeal basis, with staff and agencies (CALD and AOD) limited in their
capacity to cater for the specific needs of individuals and families from CALD communities
affected by harmful AOD use.
While it may be suggested that AOD services are not doing enough to cater for the specific needs
of CALD populations, it is worth noting that most mainstream health services struggle with this
issue. This was highlighted in a 2008 Victorian study which showed that while 90% of health and
welfare agencies come into contact with CALD clients, the overwhelming majority of this group
(89.3%) adopt a generalist approach (Renzaho 2008). Based on this and other findings one could
argue that many service systems are geared toward ‘fitting in’ consumers, rather than a needs-
based approach to service delivery.
As noted in the attached consultation report, improving the capacity of AOD agencies to provide
culturally responsive services should not be done in isolation, with the emphasis merely on the
professional development needs of frontline staff. What is required is a broader systemic
approach, one which addresses the underlying service barriers and socio-cultural norms making it
difficult for individuals and families from CALD backgrounds to access culturally appropriate
support and treatment.

54
While much attention has been paid to the cultural competence of staff and culturally
appropriate service delivery, it is VAADA’s view that a more meaningful and substantial approach
is required, one which places ‘cultural safety’ as a core feature of integrated care.
Cultural safety is a concept which emerged in the late 1980s as a key priority for the delivery of
health services to the Maori people in New Zealand. More recently, it has gained recognition as a
concept which is useful for the delivery of health services to Aboriginal and Torres Strait Islander
as well as CALD populations. A commonly used definition is that put forward by Williams (1999,
p. 213) who defines it as:
… an environment that is spiritually, socially and emotionally safe, as well as physically safe
for people; where there is no assault, challenge or denial of their identity, of who they are
and what they need. It is about shared respect, shared meaning, shared knowledge and
experience of learning together.
This approach focuses on services and practitioners embracing the differences created by culture,
with the emphasis on them as much as possible proactively engaging CALD communities so they
feel included and welcomed (Henderson & Kendall 2011). Despite the shame and stigma
associated with AOD use, and the reluctance of many to come forward, there is significant
interest across a number of CALD communities to engage more fully with AOD service providers.
As noted previously this can be an intensive and incremental process, with investment needing to
take place over the long term. Thus, for this to occur agencies and CALD communities need to be
supported.
With this in mind VAADA has put together a framework made up of nine key features of best
practice (see Table 5 on pages 55 – 59). The information detailed in Table 5 synthesises all the
key findings and learnings obtained during the project. It is VAADA’s intention that this
information be used by AOD and allied health service providers, CALD community leaders,
government and other interested parties as reference points – providing a series of benchmarks
which can be used to:
Promote stronger ties between mainstream AOD and allied health services, CALD
communities and ethno-specific agencies
Improve service access for CALD community members in need of AOD treatment
Enhance the skills and knowledge of AOD practitioners in working with individuals and
families from CALD backgrounds
Reduce stigma and shame associated with AOD use while increasing the health literacy
of CALD community members
As you read through the framework consider the impact of culture when working with people
from CALD backgrounds. It is important not to make assumptions. Just because a person comes
from a specific country or speaks a particular language or follows a certain religion does not
mean we automatically understand who they are. This response fails to appreciate the diversity
which exists within each community.

55
Table 5. Culturally safe service delivery – key features of best practice
Key features of best practice Explanation
1. Taking account of the person’s ethnicity, cultural identity, pre- migration and settlement experience
There are various ways to make sense of a person’s CALD background (such as country of birth and/or preferred language spoken). Ethnicity, however, is more complex, requiring a broader and more comprehensive appraisal.
This involves enquiring about how the person defines for themselves their ethnicity and cultural identity, which should be reflected in how data is collected and processed.
Inextricably linked is the person’s migration experience, including asking the client about their year of arrival (if born overseas), reasons for migrating and who they migrated with.
Also relevant is the person’s or their family’s post-migration experience, including difficulties they or those close to them have experienced in making the adjustment and whether this has contributed to their AOD use.
At the broader level collecting this data will allow service providers to establish more accurate information regarding the needs of CALD populations, thus guiding future program design and service delivery.
2. Special attention paid to engagement, addressing confidentiality concerns and promoting safety (building rapport and trust)
Building rapport and trust is especially important when working with people from CALD backgrounds, given the shame and stigma associated with AOD use and often what is a reluctance to come forward due to concerns about being identified in the community.
In the case of asylum seekers on bridging visas there is an added level of complexity, with the fear of legal sanctions and the loss of their visas being a key concern. Against this backdrop it is understandable if the client is reluctant to disclose. Workers are therefore advised to proceed with care.
To address these concerns it is important that client-worker confidentiality, client consent, choice and control are explained and emphasised. As a matter of priority ensure the client understands that you view AOD use as a health issue, not a moral or legal problem. Allowing more time for engagement is therefore likely to be required. For asylum seekers and refugees it is also important to be trauma aware. Be mindful that speaking about their pre- or post-migration experience may be overwhelming for the client. In these circumstances seek to validate their resilience and promote a sense of safety and stability. Workers are advised to draw on their knowledge of trauma informed models of practice.

56
Key features of best practice Explanation
3. Providing language services support (where required)
For clients with low English proficiency, it is important they are provided with language services support.
Telephone interpreters may be preferred for confidentiality reasons – especially if the person is from a small community or language group. In this situation an interpreter located elsewhere in the state may be required.
Where the client is admitted into a residential program language support via an interpreter may not be possible. In these circumstances bi-cultural workers are likely to be the best option.
Services are also advised to display the national interpreter symbol which will alert those in need of language support of the availability of interpreters.
4. Addressing gaps in health literacy while focusing on the client’s worldview and health perceptions
For many people from CALD backgrounds concepts such as counselling, harm reduction or other treatment specific terminology are entirely unfamiliar.
Practitioners are therefore advised to avoid jargon while explaining in as clear and concise a manner as possible any concepts or issues which will assist the client to make more informed decisions.
Practitioners are also advised to regularly check in with the client as to their worldview and health perceptions, while openly and respectfully acknowledging any differences. Be mindful that this can be challenging, as there may be points in the process where concepts or experiences you are trying to convey are not relatable to the client, or vice versa. When you have communication between people of different cultures, even if they share a common language, things can be misinterpreted.
5. Flexible service delivery – tailoring one’s approach to match clients’ help seeking behaviours
Many people from CALD backgrounds are either unaware of the existence of AOD supports or are reluctant to present for assistance.
If this problem is to be addressed, AOD agencies need to tailor their approach accordingly. Suitable measures include:
Offering to meet with the client and/or their family in a location of their choosing (where possible)
Making reminder calls before client appointments and where possible, offering drop-in appointments
Offering practical support – people from CALD backgrounds (most notably newly arrived migrants) will often need assistance with income support and material goods. Where possible, assist the client by

57
Key features of best practice Explanation
linking them into the relevant support services
While working through the various treatment options, encouraging the client to consider what is the ‘best fit’ for them, taking into consideration the agency’s capacity to cater for the client’s specific needs
Being aware of any cultural practices or norms which may challenge the client’s decision to cease or control their AOD use. Tailoring one’s relapse prevention messages accordingly is strongly advised
6. Customising the physical environment
It is important that the physical environment reflects a culturally diverse community, promoting a sense of welcome for clients who may otherwise feel alienated. This can be done in a number of ways, for example:
Providing signage and reading materials in multiple languages
Hanging artwork or imagery on the wall which is representative of diverse cultures
Where possible, setting aside a dedicated space for prayer and/or other traditional cultural/religious practices
7. Working in partnership with CALD community leaders, bi-cultural workers and other representatives
In order to meaningfully engage with CALD communities it is necessary to work in partnership. Identifying and seeking support from CALD community leaders, bi-cultural workers and other representatives is critical.
This approach demonstrates respect while creating opportunities for seeking community input as well as a sense of community ownership in program design and service delivery.
Examples of useful community engagement activities include:
Meeting with community representatives using formal and informal networks to raise awareness of available AOD supports while seeking their perspectives on CALD AOD issues
Attending community events and social gatherings to establish oneself in the community and build trusting relationships
Developing leadership programs to enhance the skills and knowledge of AOD and allied health personnel, CALD community leaders and bi-cultural workers
Liaising with community members about their health literacy needs and experiences navigating the AOD sector, feeding this back to senior management
Recruiting bi-cultural workers to facilitate access and

58
Key features of best practice Explanation
promote culturally appropriate models of service delivery
8. Using appropriate messaging and communication channels to reduce stigma and shame and improve the health literacy of community members requiring AOD support or treatment
Stigma and shame associated with AOD use are key factors dissuading CALD community members from coming forward. Compounding this problem is the lack of culturally appropriate consumer resources.
To address this AOD education and health promotion campaigns need to be conducted utilising culturally appropriate messaging, communication tools and media channels (e.g. multicultural radio, social media and word of mouth).
Of particular importance is the development of audio visual materials which allow for messages to be conveyed in an engaging format to audiences where print based materials are ineffective.
Establishing peer education programs where community members are supported to provide AOD education and support themselves is also critical.
9. Providing holistic and family sensitive care
Common critiques to biomedical approaches, ones which exclude social, spiritual and other cultural factors, are especially acute in the context of providing AOD treatment to CALD community members.
Practitioners are therefore advised to augment their biopsychosocial models by:
Considering any social customs or norms which may impact on the client’s preparedness and ability to engage in treatment
Seeking out opportunities to involve family members, elders and/or bi-cultural workers, wherever possible and with the client’s consent
Paying special attention to family dynamics – understand that in many CALD communities there is a divide between those whose views on AOD contradict traditional cultural values and norms, resulting in some people feeling torn between two cultures as they keep things hidden from their family, elders and others in the community. Family conflict often manifests itself as young people are influenced by the dominant culture but find it difficult to communicate with their parents/elders on matters such as AOD use
Exploring the cultural implications of providing AOD treatment. It is useful to keep in mind that your client may not have previously sought assistance from a service who treats their needs as distinct from their family

59
Note. In collectivist cultures confidentiality is viewed in more communal/familial terms (where treatment
providers are expected to share information with family, elders or others). In these circumstances the
rights of the individual may be overridden by a sense of duty and obligation to their family and community
as a whole. Workers may therefore need to manage family expectations on information sharing and
treatment planning.
6. REFERENCES
Australian Institute of Health & Welfare 2015, Alcohol and other drug treatment services in
Australia 2013 – 14: Report on the National Minimum Data Set, Drug treatment series no. 25,
Australian Institute of Health & Welfare, Canberra.
Beyer, L & Reid, G 2000, Drugs in a Multicultural Community: An Assessment of Involvement,
Department of Human Services, Public Health Division, Melbourne.
Browne, JL & Renzaho, A MN 2010, ‘Prevention of alcohol and other drug problems in culturally
and linguistically diverse communities’, Prevention Research Quarterly, Issues Paper no. 13, June
2010, pp. 1-13.
Henderson, S & Kendall, E 2011, ‘Culturally and linguistically diverse peoples’ knowledge of
accessibility and utilization of health services: Exploring the need for improvement in health
service delivery’, Australian Journal of Primary Health, vol. 17, no. 2, pp. 195-201.
MyriaD Consultants Pty Ltd 2014, Multicultural Policy Planning in Wyndham: A report on the
planning process undertaken to develop Council’s 2014-2018 Multicultural Policy and Action Plan,
November 2014, Wyndham City Council.
Renzaho, A 2008, ‘Re-visioning cultural competence in community health services in Victoria’,
Australian Health Review, vol. 32, no. 2, pp. 223-235.
Sheridan, SA 2015, Pathways to achieving complete social, emotional and spiritual wellbeing: The
Pasifika and Maori community vision for culturally safe mental health support services in south-
east Queensland, Pasifika and Maori Mental Health Forum, Official Report, Brisbane, June 2015.
South East Local Learning and Employment Network 2012, The Maori and Pasifika young people
of the South East Region of Melbourne, December 2012, South East Local Learning and
Employment Network, Melbourne.
Williams, R 1999, ‘Cultural Safety – what does it mean for our work practice?’, Australia and New
Zealand Journal of Public Health, vol. 23, no. 2, pp. 213-214.

60
Appendix A – Community profile templates (domains of
enquiry)
To assist CALD Liaison Workers (CLWs) in their role VAADA has developed four templates outlining
specific avenues (domains) of enquiry for the CALD AOD Project. These include:
Template 1 – CALD community structure and networks
Template 2 – Partner agency
Template 3 – Perceptions and health beliefs of CALD community members
Template 4 – Perceptions and experiences of past and current service users
These templates provide CLWs with clear criteria as to the information sought by VAADA project
staff.
Template 1 – CALD community structure and networks
The focus of these questions is to identify how your community structured, as well as provide a
description of the networks and key people within the community (centred on, but not limited to the
City of ……………………………………….).
Please identify the community leaders (e.g. religious leaders and elders)
representing/working on behalf of the community. In your response provide a brief
overview of their position within the community and any activities/initiatives that you are
aware of that they were/are involved in relation to AOD use in the community
In your response concentrate on the City of ………………………………. However, if there are
leaders of particular importance who are based elsewhere feel free to list them of well.
Your agency is a key service provider to the community in the City of ……………………………….
Please identify any other key organisations working with the community in this catchment
who you think may have a role in supporting community members experiencing AOD or
other related problems. In your response list the:
o Name of each organisation
o Name/s of key people operating in each agency (including their position titles)
o Contact details of the people identified
o A description of their roles and the services each agency provides
Please identify the various networks your agency is currently involved in. Focus on those
which are most likely to show an interest in the CALD AOD Project. If possible, provide an
overview of each network, including:
o Name, aims and objectives of each network
o Whether each network is auspiced by a particular agency, and if so whom

61
o Any initiatives undertaken via these networks directly/indirectly related to AOD use
(e.g. community forums or specific projects)
In your response do not limit yourself to networks based in and around the City of
……………………………. Also focus on those relevant AOD/non-AOD focused services within your
communities which are statewide, and if appropriate those which are national.
Please identify any key people operating within and outside of these networks (who may or
may not be community leaders). In your response focus on those individuals who are most
likely to show an interest in the CALD AOD Project.
Please identify any communication/media channels through which information is currently
disseminated specifically to the community (e.g. ethnic radio, newspapers, newsletters,
community TV etc). In your response please provide contact details.
Template 2 – Partner agency
This template focuses on the agency you work for – providing an overview of its role, organisational
structure, services it provides and how your agency communicates with community members.
As you provide an overview of the organisation take note of:
o The agency’s mission and role
o Organisational structure – including details of the size of the organization (number
and profile of staff), areas of operation and management structure
o Services provided (with particular reference to those focusing on the AOD and
health literacy needs of community members)
o How information is disseminated to clients, other stakeholders and the community
at large (e.g. word of mouth, newsletters, agency website, ethnic radio and media
releases)
o Current feedback loops with the community – enabling your agency’s leadership and
staff as well as those outside of the organization to keep abreast of community
issues, attitudes and perceptions
Note. Please limit your response to a maximum of 500 words (1 – 2 pages)
Here you may wish to provide VAADA with agency documentation (e.g. annual report, newsletter,
brochures, position papers and project reports).
Template 3 – Perceptions and health beliefs of CALD community
members
This template focuses on the perceptions and health beliefs of CALD community members related to
alcohol and other drug (AOD) use, culturally appropriate treatment responses and ways CALD AOD
issues are most effectively communicated within the community.

62
How are AOD issues generally perceived within the community?
In general terms, what is the perception of treatment for AOD use (legal and illegal drugs)
among community members?
To what extent is there consensus across the community about these issues? Have you
noticed any differences of opinion put forward by different people? If so, please explain. In
your response consider the perceptions and attitudes of:
o Community leaders
o Agency workers (within and outside of your agency)
o Younger and older people within the community
o Male and female community members
o Family members (parents and significant others)
o Those who use alcohol or other drugs
Are there differences between different ethnicities and/or nationalities in relation to these
issues and the way in which they could be approached? Is there scope for
information/education sessions on these issues?
How do community members’ views of alcohol differ, if at all, from other substances
(e.g. amphetamines, cannabis and prescription medications)? Do people’s attitudes and
perceptions differ in line with their gender, age or other demographics? If so, please
explain.
Please identify any traditional cultural/religious beliefs you think may influence community
members’ perceptions of AOD issues? To what extent are these beliefs
supported/followed? In your response consider the mix of people within the community
and how different people have responded.
How do family members or others within the community currently respond to AOD issues, if
someone they know is experiencing an AOD problem. Are they likely to:
o Keep it to themselves
o Seek assistance from an agency worker at your agency or another ethno-specific
agency
o Approach a drug treatment service for help
o Approach another health service (e.g. doctor at a GP service)
o Other
Based on your dealings with family members and others in need of AOD assistance what do
you think needs to happen to increase community members’ access to drug treatment?
What should AOD agencies do to become more welcoming of community members?
Please outline any strategies which would enhance the capacity of AOD treatment providers
to deliver culturally appropriate services to community members

63
Please identify any key messages which are important to consider when engaging
community members in need of AOD support, or developing culturally appropriate
consumer and worker resources
Template 4 – Perceptions of past and current service users
This template focuses on the perceptions of past and current service users (including people within
and outside of the criminal justice system) – identifying their experiences navigating the AOD service
system.
In total VAADA would like CLWs to undertake 10 – 15 interviews, canvassing the views of a range of
past and current service users (targeting adults, 18 years and over, from different age groups, males
and females, within and outside of the criminal justice system). It is anticipated that each interview
will run for up to 15 minutes (including the discussion beforehand to explain what is being asked of
them).
Refer below for the interview schedule.
At the conclusion of each interview draft a short case summary (1 – 2 paragraphs in length) outlining
the person’s experiences navigating the AOD system as well as their views about what needs to
change.
Before commencing the interview you will first need to take the participant through the attached
plain language statement (participant information sheet). Refer to page …
This statement outlines the name and aim of the project, what will happen to the feedback they
provide (how it will be used) and confidentiality arrangements.
It is critical that before you ask them any questions about their experiences navigating the AOD
sector they fully understand why they are being interviewed and what is involved. This will enable
them to consent to the process (fully aware of why they are being interviewed, how their feedback
will be used and that their participation is voluntary).
To assist you in this process we have also developed a checklist outlining the various steps. Refer to
page …
CALD AOD Project – interview questions
Gender: □ Male □ Female
Age: …….
Ethnicity: …………………………… Residential postcode: ……………………..
1. How old were you when you first came into contact with a drug and alcohol service?
□ < 18 yrs □ 18 – 21 yrs □ 22 – 34 yrs □ 35 – 44 yrs □ 45 – 54 yrs □ > 54 yrs

64
2. What type/s of drug and alcohol service have you accessed?
□ Drug and alcohol counselling
□ Help to withdraw from alcohol and/or another drug (e.g. attending a ‘detox’ unit)
□ Medical support (e.g. using methadone to help you manage opioid dependence)
□ Needle and syringe program
□ Other ……………………………………….
List details here …………………………………………………………………………………………………………………………....
……………………………………………………………………………………………………………………………………………………….
……………………………………………………………………………………………………………………………………………………….
3. Did you attend these services voluntarily or were you directed to go by the courts/police or both?
□ Attended voluntarily
□ Directed to go by the courts/police
□ Both
List details here …………………………………………………………………………………………………………………………....
……………………………………………………………………………………………………………………………………………………….
……………………………………………………………………………………………………………………………………………………….
4. How often have you accessed drug and alcohol services?
□ Only once □ 1 – 5 times □ 6 – 10 times □ 11 – 15 times □ > 15 times
List details here …………………………………………………………………………………………………………………………….
……………………………………………………………………………………………………………………………………………………….
……………………………………………………………………………………………………………………………………………………….
5. Have you received any assistance to access drug and alcohol services? □ Yes □ No
If yes, indicate who supported you and how
□ Family
□ Another person from my community

65
□ Support worker from an agency
□ Other
List details here ……………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………………………………
………………………………………………………………………………………………………………………………………………………
6. Looking back are you satisfied with the support you have received from drug and alcohol services?
□ Very dissatisfied
□ Somewhat dissatisfied
□ No opinion
□ Somewhat satisfied
□ Very satisfied
List details here ……………………………………………………………………………………………………………………………..
……………………………………………………………………………………………………………………………………………………….
………………………………………………………………………………………………………………………………………………………
7. Is there anything drug and alcohol services should do to better meet your needs and those of other people from African communities?
……………………………………………………………………………………………………………………………………………………….
.............................................................................................................................................................
.............................................................................................................................................................

66
CALD AOD Project – participant information sheet
You are invited to take part in an interview about your experiences accessing and receiving support
from drug treatment services.
This is part of the CALD AOD project which is currently being run by the Victorian Alcohol and Drug
Association (VAADA), working with agencies like the ……………………………………... The aim of this
project is to identify what needs to happen to improve services for people from culturally and
linguistically diverse (CALD) communities experiencing alcohol and/or other drug (AOD) problems.
VAADA acknowledges that it can be difficult for people from CALD backgrounds to get the help they
need. If this is to change drug treatment services need to better understand the needs of people
from CALD communities.
If you agree to participate you will be interviewed by ……………………………………………………….. You will
be asked questions about how you came into contact with drug and alcohol services, the type/s of
support you received, whether you feel you received the help you needed and what is required to
help people from your community who are experiencing AOD problems.
This interview should take no longer than 10 minutes to complete. The feedback you and others
provide will be put into a report describing your experiences and what you think needs to change.
To protect your right to confidentiality your name will not be included. We will also remove any
other references that might allow someone to guess your identity.
Your participation in this interview is entirely voluntary. You are not obliged to answer any of the
questions. At any point during the interview if you wish to stop just let ………………………………………..
…………………………… know.
At the end of the interview you will be given a gift for your time.
If you have any questions /concerns please feel free to speak with your interviewer. Otherwise, we
can arrange for you to speak with ……………………………………………………….

67
Interview checklist
□ Plain language statement presented to the participant
□ Seek the person’s consent to proceed, making sure they fully understand what is being asked of
them
□ Take note of their gender, age, ethnicity and residential postcode
□ Undertake the interview – focusing on how they came into contact with drug and alcohol
services, the type/s of support they received, whether they believe they received the support
they need and their views about service improvement
□ Provide the participant with a gift
□ Develop case summary – based on the information provided to you (1 – 2 paragraphs)

68
Appendix B – Initial roundtable discussions – summary of
issues raised
Arabic speaking Muslim community (City of Hume catchment)
Date: Tuesday, 18th August 2015
To what extent are family members involved in treatment?
o Assessments can be undertaken with a family member present, and while the needs of
the family are considered during the treatment planning process the service system is
not geared towards working specifically with families. Funding is an issue when it
comes to working with families
o Involving family members can be difficult, especially when English is not their first
language
o Important to note that treatment providers can’t give out any information without the
consent of the person seeking help
Noted that for those people who are coming into contact with AOD services, it is often due
to their involvement with police and the legal system. High proportion of forensic referrals.
Thus more needs to be done to intervene earlier
Are harsher penalties required for illegal drug use? Should treatment for alcohol and other
drugs (AOD) be mandatory (i.e. put into a locked treatment facility)?
o Noted that Switzerland has an excellent step down/step up model of mandatory
treatment but it’s incredibly expensive to set up and at present governments in this
country are not interested
o Courts can mandate people into treatment but this is different to putting someone into
a locked facility
o Other than provisions set out in Victoria’s Mental Health Act, which allows for
compulsory treatment and hospitalization of people who are at risk due to serious
mental health issues, people are not detained in treatment. There is, however, the
Severe Substance Dependence Treatment Act – which allows for people who are
considered at imminent risk of death due to their AOD use to be detained, but this is
only a temporary measure and an option of last resort
o Putting money into treatment is far more cost effective than imprisoning drug users.
Harsher penalties, including imprisoning people who use drugs, leads not only to
significant harms to that person but to the community as a whole
o Sometimes people engage in treatment on multiple occasions before anything changes
– which can be heartbreaking for families
o Fear of treatment is usually a key issue – though often they realise it isn’t what they
expected

69
Families are often shocked and traumatised to learn someone in their family is using and
often have trouble accepting it. Parents are concerned and often have no idea how to deal
with the situation
As community members are unaware of the support available to them it is unlikely that they
will contact AOD services – thus creating the impression that there isn’t demand. Other
issues cited include:
o Shame and stigma dissuading people from coming forward
o The Muslim community is constantly having to deal with issues related to terrorism
and discrimination, which can crowd out other social issues such as dealing with the
impact of AOD use
Broad agreement that more needs to be done to work with the Muslim community, to
educate parents and other family members, as well as those engaging in AOD use
Concerns raised by one community member (Lebanese background), however, that due to
the shame and stigma associated with drug use it is unlikely that that community members
would attend a forum / information session specifically about AOD. Suggestion that
community members be educated discreetly. However, other community representatives
noted that while there is shame associated with AOD use there is nonetheless widespread
interest in attending community forums on AOD
What is required is a multipronged approach, one which adopts a variety of measures. For
example:
o Working with religious leaders and other key community representatives (as they
are central points of contact) – building relationships with them to raise awareness
of the issues and skilling people up in terms of how to respond
o Looking for opportunities to work collaboratively with the community
o Supporting / recruiting Muslim bi-cultural staff
Multiple sites and communication channels identified (e.g. mosques, Islamic schools & social
media)
Acknowledgement from AOD service providers that while they do their best to
accommodate each person’s dietary and faith requirements, “we can’t always get it right”
AOD personnel expressed interest in learning more about cultural nuances (i.e. how to
engage and work with Muslim communities both on a micro & macro level)
Community representatives expressed interest in attending AOD services, as this would
assist them to learn more about the different types of treatment. Differentiating between
residential withdrawal (‘detox), residential rehabilitation (therapeutic communities),
counselling, assertive outreach support etc

70
African communities (City of Greater Dandenong catchment)
Date: Thursday, 20th August 2015
AOD providers acknowledged that the recommissioning process has had a negative impact
in terms of service access, especially when it comes to CALD populations. They are,
however, keen to work with African communities to improve the situation
Most adult AOD services are currently being accessed via a centralised intake service – often
with preliminary screening undertaken over the phone. This was acknowledged as a less
than ideal process
YSAS, however, has made significant gains working with African youth – attributed to their
service delivery model which allows for assertive outreach, drop-in services etc
Broad agreement that for those people who are coming into contact with AOD services, it is
often due to their involvement with police and the legal system. High proportion of forensic
referrals. Thus more needs to be done to intervene earlier
Community representatives identified a number of reasons why people from African
communities are not accessing AOD services. For example:
o The person may be in denial – “I don’t have a problem”
o Cultural belief that AOD issues need to be dealt with in private – connected with the
view that you need to show strength
o Lack of awareness of services & how they operate
Acknowledgement there is a cultural clash between African youth who were born in
Australia and those who came here in early adulthood or later in life – impacting on the
person’s attitude to AOD use as well as their preparedness to seek assistance
Broad agreement that relationship building is a slow and incremental process, with
investment needing to take place over the long term. One off information sessions will not
suffice. The key is to work through community leaders – engaging and mobilizing key
representatives
Focus needs to be on bringing people together to share food and participate in cultural
events
Healthy Living Program – information sessions on a range of topics (e.g. mental health)
delivered on a monthly basis. Identified as a potential vehicle for AOD providers to engage
with African communities
Recommendation by community representatives that treatment needs to be delivered in a
holistic manner – moving beyond narrowly defined clinical interventions (i.e. AOD
counselling, admissions to a residential withdrawal unit etc)

71
Noted that print based materials have limited applicability. For many community members
they come from a ‘low reading culture’. Other mechanisms for conveying information are
needed – Africans share information and stories through music and in face-to-face
interactions at cultural and social events
Afghan Hazara community (City of Greater Shepparton catchment)
Date: Monday, 24th August 2015
Most health and welfare services in the area provide access to interpreters, which is
important as there are few health professionals who themselves speak Pashtu or Dari.
There is one GP locally who speaks these languages
Depending on the issue community members may not want an interpreter, as the
interpreter may be known to them. Keeping issues private is really important. In this case a
telephone interpreter is preferred as it is much less likely that confidentiality breaches will
occur
While some community members can speak English they do not feel comfortable speaking
English in front of workers due to their level of confidence
Accessing an interpreter outside of a health or welfare service can be an issue. This has
occurred at court where the delay in accessing an interpreter has led to cases being
adjourned
Family, including children, are used as interpreters by some service providers which is
inappropriate and may cause distress and discomfort to the community members
Mental health and AOD issues are very sensitive topics – people would rather access a
mainstream service in private than approach another community member. This is a difficult
situation as they are often unaware of what is available
While there is stigma associated with mental health and AOD, community members are less
likely to discuss AOD issues. The stigma related to AOD is greater
If a parent becomes aware of their child using drugs they may try to deal with them by
isolating the young person – keeping them at home – which may have an impact on their
mental health. Parents and other family members are generally at a loss to understand the
issues or why the person is using. Parenting/education classes would be very useful
Services should use a range of activities to connect with the community and have more
contact (e.g. at TAFE, sewing groups, recreational activities, sport). They could also offer
work experience to community members to strengthen ties with the community
Setting up support groups where Afghan community members can practice English with
people from the general community is really important

72
Mosques are an ideal place for service providers to establish connections and perhaps run
information sessions, but not specifically on AOD as this is considered too confrontational.
Instead it is more appropriate to include AOD information as part of a wider health program
Services and community representatives should meet on a regular basis (e.g. every 6
months) to share information and build relationships
Facebook is well used especially by young people in the community – how can services use
this to engage with the community?
AOD misuse is not a problem in the Afghan Hazara community
Afghani women are quite isolated in the community as they tend not to socialise outside of
the home. Providing opportunities for them to meet and socialise with each other is a key
priority (e.g. swimming offered in a private women’s only space)
Noted that print based materials have limited applicability. Many community members do
not read or write English, nor are they literate in their first language
Pacific Islander and Maori communities (City of Wyndham
catchment)
Date: Wednesday, 26th August 2015
For those people who come into contact with alcohol and other drug (AOD) services it is
generally due to their involvement with police and the legal system. High proportion of
forensic referrals. Individuals and family members are generally not engaging with AOD
services on a voluntary basis. Situation applicable to ISIS Primary Care and Western Health
Noted by a large AOD provider that there are some people from the community presenting
voluntarily, however they often present with a range of complex needs. Key issue is family
violence
Community representatives identified a number of reasons why people from
‘Pasifika’ communities are not accessing AOD services:
o Widespread belief that AOD issues need to be dealt with in private – connected with
the view that you need to show strength which is also connected to a person’s sense
of pride. “We are a proud people”
o Language barriers
o Young people in particular find it difficult to engage, especially if they have had
negative experiences in the past

73
o The current system actively discourages CALD communities from accessing services
– phone intake and being moved from one agency to another identified as key
problems requiring attention
Coming forward exposes the family. People want help “but they know workers will take it to
another level … Polynesians, we’re designed to protect – nothing comes in and nothing gets
out”. We’re afraid to expose what happened and dishonour the whole family
Within Pacific Islander and Maori communities AOD use is often viewed as a moral issue
rather than a health issue. For those people who view it in moral terms AOD use is
considered shameful. Linked to the view that “something is wrong with you”
Within the Serbian community alcohol is not viewed as a drug, and in the Ukraine how
‘manly’ you are is determined by how much you can drink. For many in this community
family violence is okay so long as you are drunk at the time
Broad agreement that trust is of paramount importance and not something that is easy to
achieve. But once it’s established the whole relationship will change
Recommendation by community representatives that treatment needs to be delivered in a
holistic manner – moving beyond narrowly defined clinical interventions (i.e. AOD
counselling, admissions to a residential withdrawal unit etc). At present, the definition of
‘treatment’ is anglo-centric (based on a western / white interpretation)
“If you meet with the community as a professional the community will back off … go to them
as a person”
“Young people find it hard to connect & then stop looking” …. “Understanding the young
person’s journey is most important”
AOD providers acknowledged that in the adult system “we sit and wait for people to come
to us”. Unfortunately there is little scope to go out & actively engage the community, as
services are already in high demand
Community members will engage in services if programs are pitched from a broader health
and wellbeing perspective, rather than it being presented as AOD specific. Look at
rebranding (e.g. focusing on health, getting fit and spiritual connection).
It’s also about going to them, on their turf, where they feel safe – something which is
happening in the youth AOD space … not so much in adult services
Youth AOD provider identified that they’ve been working with the community for some time
– during ‘poly night’ workers on assertive outreach engage with youth on the street. This
has led to the ‘poly week detox’ where a group of young people were brought into the
residential withdrawal unit. A number of adjustments were made to the program, including
shortening the length of stay and increasing family visits. However the young people who
came into the unit “just wanted a break”

74
Noted that behaviour changes according to the individual’s beliefs – “right believing leads to
right living”
Recruiting and supporting bi-cultural workers identified as a key priority, whether they’re
located in a mainstream service or an agency such as Bridging Worx, whose purpose is to
specifically work with Pacific Islanders & Maoris. However, what is required is support to
make this work
Broad agreement that relationship building is a slow and incremental process, with
investment needing to take place over the long term. One off information sessions will not
suffice. The key is to work through community leaders – engaging and mobilizing key
representatives
As there are layers within the AOD system there are also layers in the community. For a
service to be successful it must establish relationships with those ‘go to people’. First, tell
your story to these go to people, and with their support you can access the family which will
then give you access to those people in need. “This is a different context … it’s a cultural
context”
Vietnamese community (City of Yarra catchment)
Date: Monday, 31st August 2015
Question directed to AOD personnel – “What is your experience working with
individuals and families from the Vietnamese community?”
o Harm Reduction Victoria (HRV) noted they work with people who inject drugs,
including individuals from the Vietnamese community. As part of the Peer
Networker Project they support and train individuals who are active users to
distribute injecting equipment and educate others about safer injecting as well as
the risks
o People from the Vietnamese community who inject drugs have traditionally been
very difficult to reach. At present, HRV are working with 2 Vietnamese peer
networkers – enabling them to reach this otherwise difficult to reach population
o On average HRV peer networkers come into contact with 20 individuals from the
Vietnamese community in need of support each week, many of whom are repeat
clients
Concerns raised by a number of community representatives that this approach – supplying
needles and other equipment through Needle Syringe Programs (NSPs) etc – encourages
people to use, which is not what many people in the Vietnamese community think should
happen

75
o In response, it was noted by HRV and other AOD providers that people accessing
NSPs or coming into contact with HRV are already using. The aim is to reduce the
harms by giving them access to sterile injecting equipment and working with them
to use more safely
o The number of people who inject drugs has not increased since the introduction of
NSPs, but it has led to a decrease in the spread of blood-borne viruses
Suggested by a community representative that treatment workers need to be aware of
Vietnamese cultural views of drug use. Not uncommon for family members to seek a ‘quick
fix’ – with the expectation that the person using should be admitted into treatment to cease
their use
For those people who come into contact with alcohol and other drug (AOD) services it is
generally due to their involvement with police and the legal system. High proportion of
forensic referrals. Individuals and family members are generally not engaging with AOD
services on a voluntary basis
Community members are unlikely to walk into a drug treatment service, because of the
shame and stigma associated with AOD use, whereas coming to a service such as the
Australian Vietnamese Women’s Association (AVWA) is much less problematic. “People can
walk into an organization such as AVWA because it provides a wide range of services and no
one knows why you’re there”
Question directed to AOD providers regarding the lengthy wait periods for treatment
(residential rehabilitation)
o Large AOD provider noted that wait times for a bed at the therapeutic community
can be anywhere from 3 – 5 months, due to the very slow turn over. Priority is
however given to certain groups (i.e. high-risk clients, forensic clients and Aboriginal
and Torres Strait Islander people)
o At present there are approximately 100 beds at the therapeutic community
o Important to note that residential services (including withdrawal and residential
rehabilitation) are the most expensive treatment types, and AOD services are in
need of more government funding to deal with the demand
o Service providers are dealing with this issue by setting up non-residential
rehabilitation programs. For example, Odyssey House Victoria have recently opened
a new 5 week day program in Werribee
Noted by AOD service providers that in addition to residential rehabilitation there are a
range of other services which are easier to access in terms of wait times – counselling,
pharmacotherapies etc. Going into a therapeutic community is usually something the
person does after having gone into other forms of treatment
Community representative noted that people find motivation to seek treatment but when
they have to wait multiple weeks they give up. “If treatment is available at the right time,
they’ll go … one day they’re doing well, but when treatment isn’t available motivation
disappears”

76
Most people within the Vietnamese community are unaware of how the drug treatment
system works, nor what services are available. Pointed out by AOD providers that this
situation also applies to other migrant communities as well as the general community. It
was agreed that government needs to come up with a better communication strategy for
Vietnamese as well as other CALD populations
Noted that many people in the Vietnamese community do not have a good understanding of
‘counselling’. Traditionally, you seek advice from elders and do not discuss personal issues
with outsiders, and are reluctant to approach outsiders for fear of confidentiality breaches
One agency representative recalled a 5 week AOD education program she delivered to a
group of Vietnamese women some years ago. She noted that over the course of the
program participants felt increasingly at ease, less fearful and intimidated by the prospect of
people using drugs in public spaces, as their knowledge of these issues increased
AVWA receiving many requests from concerned family members. Broad agreement that
more needs to be done to work with the Vietnamese community (especially those aged 40 –
60 years), to educate parents and other family members, as well as those engaging in AOD
use
Broad agreement that more could be done to strengthen the relationship between local
AOD service providers , Vietnamese community and AVWA

77
Appendix C – CALD AOD forum program and evaluation
summary
CALD AOD forum program
Table 5. CALD AOD forum program
Registrations and networking
9.30 – 10.20 am
Tea, coffee and finger food available on arrival
Minister introduced to CALD community representatives and project staff
Welcome to Country
10.20 – 10.30 am
Welcome to the CALD AOD forum and resources launch
10.30 – 10.45 am
Proceedings opened by the Honorable Martin Foley, Minister for Housing, Disability and Ageing, Minister for Mental Health, Minister for Equality, Minister for Creative Industries
Minister formally launches CALD AOD resources
Keynote speakers (CALD and AOD stories of inspiration)
10.45 – 11.35 am
Keynote speech focusing on overcoming the challenges of migrating to Australia followed by keynote speech focusing on story of AOD recovery
CALD AOD Project reflections
11.35 am – 12.00 pm
Reflections on the CALD AOD Project delivered by the CALD AOD Project Officer
LUNCH (12.00 – 12.40 pm)
CALD Liaison Worker (CLW) presentation and panel discussion
12.40 – 1.30 pm
A short audio visual presentation on the health needs of CALD communities presented by CLWs, focusing on the experiences of Afghan Hazara, African, Arabic speaking Muslim, Pacific Islander and Maori and Vietnamese community members
Moderated panel discussion involving CLWs and other CALD community representatives. Panelists invited to respond to questions put forward by the moderator and audience members
Examples of best practice
1.30 – 2.15 pm
Presentations by AOD and allied health service providers regarding best practice initiatives
Key issues for consideration and where to from here
2.15 – 2.35 pm
Overview of key issues informing the development of project recommendations and where to from here
Acknowledgements and close
2.35 – 2.45 pm
AFTERNOON TEA (2.45 – 3.00 pm)

78
CALD AOD forum evaluation summary
Total number of participants: 139 Total number of respondents: 65 1. Your role / position (please circle the correct response) CALD community member / bicultural worker / other CALD representative: 20 AOD practitioner: 17 Allied health practitioner: 4 Other interested party: 22 2. Please rate your overall agreement with the following statements: The forum was well prepared and run
My knowledge of CALD AOD issues has increased
2% (n = 1)5% (n = 3)
60% (n = 39)
34% (n = 22)
Stronglydisagree
Disagree Unsure Agree Strongly agree
2% (n = 1)6% (n = 4)
14% (n = 9)
55% (n = 36)
23% (n = 15)
Stronglydisagree
Disagree Unsure Agree Strongly agree

79
The forum provided me with the opportunity to network and share information with others
I am now more aware of the barriers making it hard for people from CALD backgrounds to access AOD support
The catering was suitable
3 (n = 2)6% (n = 4)
9% (n = 6)
52% (n = 34)
29% (n = 19)
Stronglydisagree
Disagree Unsure Agree Strongly agree
2% (n = 1)6% (n = 4)
9% (n = 6)
69% (n = 45)
14% (n = 9)
Stronglydisagree
Disagree Unsure Agree Strongly agree
2% (n = 1)
6% (n = 4)3% (n = 2)
38% (n = 25)
51% (n = 33)
Stronglydisagree
Disagree Unsure Agree Strongly agree

80
The venue was suitable
Overall, the forum was worthwhile attending
3. What did you find useful about today’s forum?
Useful to hear from a wide range of CALD communities represented
Powerful community voice – 2 keynote speakers were also very powerful
Project reflections – hearing about the key issues & findings, though would have like to hear more about this
Discussions around the need for community input and consultation with respect to AOD treatment program development
Video presentation and panel discussion
Depth of concern across ethnicities for clients to access services
Excellent catering
Best practice examples – finding out about what is currently taking place in this space
3% (n = 2)
17% (n = 11) 17% (n = 11)
45% (n = 29)
18% (n = 12)
Stronglydisagree
Disagree Unsure Agree Strongly agree
2% (n = 1)5% (n = 3)
54% (n = 35)
40% (n = 26)
Stronglydisagree
Disagree Unsure Agree Strongly agree

81
4. What could have been improved?
The venue – terrible acoustics. Sound was a real problem (echo and inconsistent volume). Microphone at times too loud and harsh
Allocating more time for questioning and group discussion (including small group discussion)
Table / group discussions with some specific questions they could focus on
More of a focus on how community organisations can educate and work with CALD communities
More time to move around
Have a panel with youth to answer why they don’t access services
Cultural performances during the break
Gender imbalance of panel (all males) was very disappointing
It felt rushed at times
More input from adult AOD service providers 5. Further comments / issues you would like to raise:
How do we continue these conversations in order to improve our practice?
Department (DHHS) needs to support this work. At present stats / funding DTAUs put pressure on services that makes it difficult to engage with communities that don’t fit into a service stream
Wanted to hear more about generational family issues – felt there was little emphasis on family interventions or addressing family structures … absence of domestic violence issues
Clearly a need for improvements in sector and a huge interest

82
Appendix D – AOD practitioner tip sheets

83

84

85

86

87

88
Appendix E – Crossing the Cultural Divide postcards

89

90

91

92

93
Appendix F – Crossing the Cultural Divide poster

94






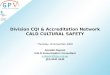
![· to begin a new course of study […] and resume working overseas. ... • Mr Brad Pearce, Victorian Alcohol and Drug Association (VAADA) • Mr Robert Stirling, Network of](https://img.pdfslide.us/doc/110x75/5f14e2f8a0e6787ca11a35a7/-to-begin-a-new-course-of-study-and-resume-working-overseas-a-mr-brad.jpg)





















