-
ADHD and AutismMaking Data-Based Eligibility Decisions
Association of School Psychologists of Pennsylvania &
Pennsylvania State University
2020 Virtual Fall ConferenceNovember 4 & 5, 2020
Amanda Zanko, M.Ed., Ed.S., NCSP
Victoria Petit, M.Ed.
Doctoral Students, The Pennsylvania State University
-
● Background Information: Review how ASD and ADHD fit into IDEA
criteria○ Provide information regarding symptoms of ADHD and ASD
and how these may overlap
● Objective 1: Provide school psychologists with the tools
needed to complete a comprehensive, multidisciplinary evaluation
to:
○ Gather the data needed to differentiate between ASD and ADHD ○
Make appropriate recommendations for programming and
interventions
● Objective 2: Develop critical-thinking skills needed to
analyze data to arrive at appropriate eligibility decisions
○ Take a look at real-life case data to apply these skills
● Objective 3: Provide recommendations for school-based and IEP
teams
What’s Ahead
-
ADHD & Autism:Two Common Neurodevelopmental Disorders &
Comorbidity
-
The Stats
Centers for Disease Control and Prevention (CDC, 2020)
● 6.1 million children aged 2-17 years had a diagnosis of ADHD
(2016)○ This has drastically increased from the
previous estimates of 4.4 million children aged 4-17 years old
in 2003
● 1 in 54 children are diagnosed with Autism○ This has increased
from 1 in 150 in 2000
● Both ASD and ADHD are more common in boys than girls
-
The dilemma… Is it ADHD? Autism? Both?
● ADHD is the most common comorbidity in children with ASD
(Antshel & Russo, 2019)○ 30-75% of students with ASD
have symptoms consistent with ADHD (Grzadinski, Dick, Lord,
& Bishop, 2016)
● 64% of children with ADHD have a comorbid diagnosis, including
autism (CDC, 2020)○ 14% of these children also have
a diagnosis of ASD● 20-60% of students with ADHD have
social difficulties similar to students with ASD (Grzadinski,
Dick, Lord, & Bishop, 2016)
● 21% of participants diagnosed with ADHD met criteria for
autism on the ADOS (Zablotsky, Bramlett, & Blumberg, 2020)
-
Attention Deficit/Hyperactivity Disorder (ADHD): Diagnostic
Criteria
● DSM-5: “A persistent pattern of inattention and/or
hyperactivity-impulsivity that interferes with functioning or
development”
○ Inattention: “Wandering off task, lacking persistence, having
difficulty sustaining focus, and being disorganized”
○ Hyperactivity: “Excessive motor activity when it is not
appropriate, or excessive fidgeting, tapping, or talkativeness”
○ Impulsivity: “Hasty actions that occur in the moment without
forethought and that have high potential for harm to the
individual”
● Must manifest in more than one setting● Presentations:
○ Predominantly Inattentive○ Predominantly
Hyperactive/Impulsive○ Combined
-
The Individuals with Disabilities Education Act (IDEA) and
ADHD
● OTHER HEALTH IMPAIRMENT (OHI)● “OHI means having limited
strength, vitality, or
alertness, including a heightened alertness to environmental
stimuli, that results in limited alertness with respect to the
educational environment, that -
○ (i) Is due to chronic or acute health problems such as asthma,
attention deficit disorder or attention deficit hyperactivity
disorder, diabetes, epilepsy, a heart condition, hemophilia, lead
poisoning, leukemia, nephritis, rheumatic fever, sickle cell
disease, anemia, and Tourette syndrome; and
○ (ii) Adversely affects a child’s educational performance.
-
IDEA and ADHD EMOTIONAL DISTURBANCE(i) Emotional disturbance
means a condition exhibiting one or more of the following
characteristics over a long period of time and to a marked degree
that adversely affects a child’s educational performance:
(A) An inability to learn that cannot be explained by
intellectual, sensory, or health factors.(B) An inability to build
or maintain satisfactory interpersonal relationships with peers and
teachers. (C) Inappropriate types of behavior or feelings under
normal circumstances.(D) A general pervasive mood of unhappiness or
depression.(E) A tendency to develop physical symptoms or fears
associated with personal or school problems.
(ii) Emotional disturbance includes schizophrenia. The term does
not apply to children who are socially maladjusted, unless it is
determined that they have an emotional disturbance under paragraph
(c)(4)(i) of this section.
https://sites.ed.gov/idea/regs/b/a/300.8/c/4/ihttps://sites.ed.gov/idea/regs/b/a/300.8/c/4/i/ahttps://sites.ed.gov/idea/regs/b/a/300.8/c/4/i/bhttps://sites.ed.gov/idea/regs/b/a/300.8/c/4/i/chttps://sites.ed.gov/idea/regs/b/a/300.8/c/4/i/dhttps://sites.ed.gov/idea/regs/b/a/300.8/c/4/i/ehttps://sites.ed.gov/idea/regs/b/a/300.8/c/4/ii
-
Autism Spectrum Disorder (ASD): Diagnostic Criteria
● DSM-5: “Essential features of ASD are persistent impairment in
reciprocal social communication and social interaction (Criterion
A), and restricted, repetitive patterns of behavior, interests, or
activities (Criterion B). These symptoms are present from early
childhood and limit or impair everyday functioning (Criteria C and
D).”
○ “Diagnoses are most valid and reliable when based on multiple
sources of information, including clinician’s observations,
caregiver history, and, when possible, self-report.”
■ Criterion A: Impaired use of language; deficits in
social-emotional reciprocity; deficits in nonverbal communicative
behaviors; and deficits in developing, maintaining, and
understanding relationships.
■ Criterion B: Simple motor stereotypies, repetitive use of
objects, repetitive speech, excessive adherence to routines,
ritualistic patterns of verbal and nonverbal behavior
-
IDEA and ASD
● AUTISM○ “Autism means a developmental disability
significantly affecting verbal and nonverbal communication and
social interaction, generally evident before age three, that
adversely affects a child’s educational performance. Other
characteristics often associated with autism are engagement in
repetitive activities and stereotyped movements, resistance to
environmental change or change in daily routines, and unusual
sensory responses to sensory experiences.”
-
When ADHD and Autism criteria collides...
ADHD?
Inattention
Social Skill Difficulties
Self-Regulation Difficulties
Hyperactivity
Pragmatic language difficulties
Autism Spectrum Disorder?
-
Questions to Consider...
● Are there self-regulation difficulties?○ If so…
■ Does the student demonstrate externalizing behaviors due to a
lack of impulse or self-control?
■ Does the student have difficulties tolerating changes in their
environment?
-
Questions to Consider...
● Are there social skill deficits?○ If so...
■ Are the social difficulties related to
hyperactivity/impulsivity or inattention?■ Are these difficulties
related to isolation and withdrawal typical of students
with Autism? Does the student have difficulty understanding
appropriate social interactions?
■ Is the student withdrawing due to other comorbidities (i.e.,
Anxiety and Depression)?
-
Questions to Consider...
● Hyperactivity can be misinterpreted as repetitive behaviors
seen in students with Autism○ Are the repetitive behaviors
generalized and related to hyperactivity and
a lack of self-regulation?○ Are the repetitive behaviors
stereotypical in nature?
-
Questions to Consider...
● Are there difficulties with pragmatic language skills?○ If
so…
■ Is the language stereotypical in nature?■ Is the language
restricted to the individual’s own interests?
-
Thoughts to Consider...
● Inattention is a diagnostic consideration for ADHD; AND●
Inattention is not uncommon in students with Autism
○ If students with Autism also meet criteria for ADHD, they meet
criteria for BOTH Autism and ADHD (Comorbid disorders)
○ In these cases, school teams may consider criteria for both
Autism and OHI in your eligibility decisions
-
Completing Comprehensive Evaluations
Case Planning
-
Gathering Background Information:
Interviews
● Interviews○ Parent interview○ Teacher interview○
Paraprofessional interview ○ Speech pathologist○ Student interview
○ Standardized/Structured
Interviews■ Autism Diagnostic Interview
- Revised (ADI-R)
-
Observations ● Direct Observations ○ Functional Behavior
Assessment (FBA)
■ Consider observations during direct instruction and
independent work, as well as observations when peer interactions
are likely to occur (i.e., lunch, recess)
■ Make note of teacher interactions, peer interactions, and any
repetitive behaviors/speech
■ Collect time-on task assessment during instruction and/or
independent work
-
Assessments for ADHD
Rating Scales
● Conners - Third Edition (Conners-3)○ Age 5 or below: DSM-5
Checklist
Direct Assessments
● Conners Continuous Performance Test - Third Edition
(CPT-3)
○ Kiddie Conners Continuous Performance Test - Second Edition (K
CPT 2)
○ Conners Continuous Auditory Test of Attention (Conners
CATA)
● NEPSY-II○ Attention and Executive Functioning Battery
● IQ Assessments
-
Assessments for Autism Rating Scales● Autism Spectrum Rating
Scales (ASRS)● Gilliam Autism Rating Scale - Third Edition
(GARS-3) ● Childhood Autism Rating Scale - Second
Edition (CARS-2)● Social Communication Questionnaire (SCQ)
Standardized Assessments
● Autism Diagnostic Observation Schedule - Second Edition
(ADOS-2)
○ COVID-19 Alternative: Brief Observation of Symptoms of Autism
(BOSA)
-
Additional Assessments to Consider
Rating Scales
● Behavior Assessment System for Children - Third Edition
(BASC-3)
○ Consider: Hyperactivity and Attention Problems scales;
Withdrawal and Atypicality
● Behavior Rating Inventory for Executive Function - Second
Edition (BRIEF-2)
● Social Skills Improvement System (SSiS) Rating Scales●
Adaptive Behavior:
○ Adaptive Behavior Assessment System - Third Edition
(ABAS-3)
○ Vineland Adaptive Behavior Scales - Third Edition
(Vineland-3)
Executive Functioning
● Delis-Kaplan Executive Function System (D-KEFS)● NEPSY-II
Sensory Evaluation
Achievement Measures
-
CASE STUDIES
-
Case Studies #1: Ivan YReferral: autism
Background information: ● 8th grade student● Previous
identification: OHI + SLI● Currently takes medication for ADHD,
OCD, and ODD:
- Concerta, 54mg- Strattera, 40mg- Clonidine ER, 0.2mg am/ 0.2
mg pm- Escitalopram, 5mg
Referral concerns:● Concerns with volatile words and actions,
impulses, lying, stealing, and arguing
(across settings)● Peer relations
Case Plan:
1. Rating scalesa. BASC-3b. Conners 3c. ASRS
2. CPT33. ADOS-24. Behavioral
Observations5. WISC-V6. KTEA7. Parent interview8. Child
interview
-
BASC-3
-
Conners 3 & CPT 3
-
ADOS-2 & ASRS
-
ResultsDiagnosis:
● ADHD● Anxiety● Depression
Identification recommendations:
● Other Health Impairment● Emotional Disturbance
Ruled out:
● Autism
-
Discussion Do these results surprise you?
What disability category would you recommend?
What would you recommend for treatment? Next steps?
-
Case Study #2: Collin SReferral: autism and math concerns
Background information:
● 7 years old, 2nd grade● Only child● Recently diagnosed with
dyscalculia and ADHD
Referral concerns:
● Hand flapping● Rocking in chair● Staring off into the
distance● Swinging legs in chair● Talks quickly and without
receiving a response● Has to go up and down aisles of the grocery
store in a certain order
Case Plan: YOUR TURN
1. What is your initial reaction?2. What information do you want
to
know?3. What assessments would you
give?
-
WISC-V
-
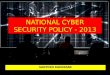
WIAT-IIISubtest/Composite Standard Score 90% Confidence Interval
Percentile Rank Classification
Listening Comprehension 105 95-115 63 Average
Oral Expression 103 94-112 58 Average
Oral Language 104 96-112 61 Average
Word Reading 102 98-106 55 Average
Pseudoword Decoding 109 105-113 73 Average
Basic Reading 104 101-107 61 Average
Reading Comprehension 114 107-121 82 High Average
Oral Reading Fluency 88 81-95 21 Low Average
Reading Comprehension and Fluency 101 95-107 53 Average
Total Reading 102 98-106 55 Average
-
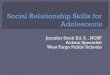
WIAT-III continued
Math Problem Solving 88 80-96 21 Low Average
Numerical Operations 74 67-81 4 Very Low
Mathematics 80 74-86 9 Low Average
Math Facts Fluency - Addition 66 55-77 1 Extremely Low
Math Facts Fluency - Subtraction 67 59-75 1 Extremely Low
Math Fluency
66 59-73 1 Extremely Low
Spelling 96 90-102 39 Average
Alphabet Writing Fluency 93 79-107 32 Average
Sentence Composition 88 80-96 21 Low Average
Written Expression 89 82-96 23 Low Average
Early Reading Skills 88 77-99 21 Low Average
Total Achievement 93 90-96 32 Average
-
BASC-3At-Risk:
● Subcategories○ Hyperactivity (mom, dad)○ Attention Problems
(dad, teacher)○ Atypicality (mom)○ Adaptability (mom, dad)○
Functional communication (all)○ Activities of daily living (mom,
dad)○ Social Skills (mom, dad)○ Leadership (mom, dad)
● Composites○ School Problems (teacher)○ Behavioral Symptoms
Index (mom)○ Adaptive Skills (mom, dad)
Clinically Significant:● Subcategories
○ Anxiety (dad)○ Attention Problems (mom)○ Atypicality (dad)○
Withdrawal (dad)
● Composites○ Internalizing Problems (dad)○ Behavioral Symptoms
Index
(dad)
-
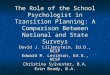
ASRSAreas DAD
T score (CI) PR
MOM T score (CI) PR
TEACHERT score (CI)
PR
ASRS Scales
Social/ Communication
(SC)
62 88 Slightly Elevated
53 62 Average
57 76
Average
Unusual Behaviors (UB)
73** 99 Very Elevated
64 92 Slightly Elevated
58 79 Average
Self-Regulation (SER)
69* 97 Elevated
62 88Slightly Elevated
53 62
Average
Total Score 71** 98 Very Elevated
61 86Slightly Elevated
57 76 Average
DSM-IV-TR Scale (DSM)
72** 99Very Elevated
60 84Slightly Elevated
59 82 Average
Peer Socialization 70** 98Very Elevated
56 73Average
55 69 Average
Adult Socialization 62 88Slightly Elevated
52 58Average
51 54
Average
Social/Emotional Reciprocity 62 88Slightly Elevated
55 69 Average
60 84Slightly Elevated
Atypical Language 71** 98Very Elevated
52 58 Average
64 92Slightly Elevated
Stereotypy 72** 99Very Elevated
58 79Average
60 84Slightly Elevated
Behavioral Rigidity 78** 99Very Elevated
74** 99Very Elevated
55 69
Average
Sensory Sensitivity 69* 97Elevated
53 62Average
57 76
Average
Attention 72** 99Very Elevated
67* 96Elevated
58 79Average
Areas DADT score (CI) PR
MOM T score (CI) PR
TEACHERT score (CI)
PR
-
Behavioral Observations
● Appropriate eye contact● Frequently turned around in his chair
to ask about pictures/posters on the wall● Swung his legs● Flapped
arms when he felt he got something correct● High-pitch inflection
of voice when he felt he answered correctly● Told stories about
friends, family, and pets● Eager to come back after the first test
session
-
Discussion What do you think? What data pointed you to that
conclusion?
What would you recommend?
Would you have collected more information?
-
ResultsDiagnosis:
● ADHD● SLD in math calculation
Identification:
● Primary: Specific Learning Disability● Secondary: Other Health
Impairment
Ruled out:
● Autism
-
CASE STUDY #3: Jackie B.Referral Question: SLD, Autism, ADHD,
SLI, ED
Background Information:
● 1st grade student; Retained in K● Attendance issues●
Environmental factors: Access to language ● 504 Service Agreement
for OT services● Previous evaluation in K - Found not eligible for
services
Referral Concerns:
● Academic concerns: Math and reading ● Inattentive during
instruction/independent work● Typically plays alone, enjoys playing
with paper/making hats to flap paper● Does not like raindrops
touching her● Fixated and obsessed with ideas/things (i.e., what
she is doing after school, ponytail)● Imitates the teacher●
Frequent mood swings, irritable
Case Plan: YOUR TURN
1. What is your initial reaction?2. What information do you want
to
know?3. What assessments would you
give?
-
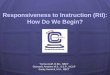
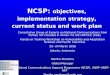
KBIT-2
Subscales Standard Score
(90% Confidence Interval)
Percentile Rank Qualitative Descriptor
Verbal 82 (75-91) 12 Very Low - Average
Nonverbal
102 (93-111) 55 Average – High Average
IQ Composite 91 (85-98) 27 Low Average - Average
-
WIAT-III
-
BASC-3
-
ASRS
-
Conners-3
-
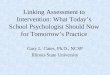
Conners CPT 3
Total of 8 atypical T-scores
● Associated with a very high likelihood of having a disorder
characterized by attention deficits
Profile of scores and response pattern indicate issues related
to:
● Inattentiveness (strong indication), sustained attention
(strong indication), and vigilance (strong indication).
ADOS-2
-
Discussion What do you think? What data pointed you to that
conclusion?
What would you recommend?
Would you have collected more information? What would you have
done differently?
-
ResultsIdentification:
● OHI (ADHD - Inattentive Type)
Ruled Out:
● Emotional Disturbance● Autism● Specific Learning
Disability
Do these results surprise you? Do you agree with these
conclusions?
What would you recommend for treatment? Next steps?
-
Recommendations
-
Treatment Options - ADHD
Medication:
● Stimulant vs. non-stimulant
*Consider as-needed versus daily dosage
Behavioral Intervention:● Organizational training●
Parent/teacher training● Therapeutic approaches
-
Medication
● Stimulant○ Methylphenidate (Ritalin/Concerta)○ Amphetamine
(Adderall)○ Lisdexamfetamine (Vyvanse)
● Non-stimulant○ Atomoxetine (Strattera)○ Guanfacine (Tenex)
-
ADHD Interventions
Behavioral Interventions:
● Parent/teacher training ○ Contingency management
● Organizational intervention
Other:
● Peer education● Cognitive Behavioral Therapy
(CBT)● Self-monitoring intervention
-
ADHD - Accommodations
Preferential seating
Brain breaks/movement breaks
Extended time to complete assignments
Testing accommodations
Repeating of directions/frequent teacher check-ins
Frequent teacher praise/redirection
Sensory interventions (Velcro, bouncy band)
-
Treatment Options - Autism
Applied behavior analysis (ABA)● Reinforcement (R+, R-)● Visual
schedules● Token economies● Social skills training● Life skills
training● Self-monitoring
Parent training● Home-school communication● Behavior management
in home setting● Home-based services
Classroom behavior management● Behavior-specific praise●
Reminders/pre-corrects● Modeling● Self-monitoring
Related Services● Speech Services● Occupational Therapy●
Physical Therapy● Assistive Technology
-
Overlapping Treatment Options
Behavior management
ABA
Parent training
Home-school communication
Structure/routines
Exercise
-
Reflection
What are some potential challenges that could come up regarding
the discussion of medication as a treatment option?
What are the stigmas for each diagnosis? What about
comorbidity?
How does ADHD present in females? Autism?
What might ADHD or autism look like in adults?
What is the benefit for comorbid diagnoses? Downsides?
-
Resourceshttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC4010758/
https://www.pbisworld.com/
https://www.classroomcheckup.org/
https://chadd.org/about-adhd/adhd-and-autism-spectrum-disorder/
https://www.autismspeaks.org/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4010758/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4010758/https://www.pbisworld.com/https://www.classroomcheckup.org/https://www.classroomcheckup.org/https://chadd.org/about-adhd/adhd-and-autism-spectrum-disorder/https://chadd.org/about-adhd/adhd-and-autism-spectrum-disorder/https://chadd.org/about-adhd/adhd-and-autism-spectrum-disorder/https://www.autismspeaks.org/
-
ConferencesNational Association of School Psychologists (NASP)
Annual Convention
● February 23–26 virtually
Teacher Educators for Children with Behavior Disorders
(TECBD)
● November 3, 10, 17, and 24 virtually
American Psychological Association (APA)● August 12-15
American Educational Research Association (AERA) ● April 9 –
April 12
15th Annual Autism Conference
● February 28–March 2, 2021 virtually
-
References
American Psychiatric Association. (2013). Diagnostic and
statistical manual of mental disorders (5th ed.). Washington, DC:
Publisher.
Antshel, K. M., & Russo, N. (2019). Autism Spectrum
Disorders and ADHD: Overlapping phenomenology, diagnostic issues,
and treatment considerations. Current Psychiatry Reports, 21,
1-11.
Centers for Disease Control and Prevention. (2020). Data and
statistics about ADHD. Retrieved from:
https://www.cdc.gov/ncbddd/adhd/data.html
Centers for Disease Control and Prevention. (2020). Data and
statistics on autism spectrum disorder. Retrieved from:
https://www.cdc.gov/ncbddd/autism/data.html
Baixauli Forteaa, I., Berenguer Forner, C., Colomer, C., Miranda
Casas, A., & Rosello Miranda, B. (2018). Communicative skills
in spanish children with autism spectrum disorder and children with
attention deficit hyperactivity disorder: Analysis through parents’
perceptions and narrative production. Research in Autism Spectrum
Disorders, 50, 22-31.
Cooper, J., Heron, T. and Heward, W., 2007. Applied Behavior
Analysis. 2nd ed. Upper Saddle River, NJ: Pearson.
Grzadinski, R., Dick, C., Lord, C., & Bishop, S. (2016).
Parent-reported and clinician-observed autism spectrum disorder
(ASD) symptoms in children with attention deficit/hyperactivity
disorder (ADHD): Implications for practice under DSM-5. Molecular
Autism, 7, 1-12.
https://www.cdc.gov/ncbddd/adhd/data.htmlhttps://www.cdc.gov/ncbddd/autism/data.html
-
References
Handen, B.L. et al. (2015). Atomoxetine, parent training, and
their combination in children with autism spectrum disorder and
attention-deficit/hyperactivity disorder. Journal of the American
Academy of Child and Adolescent Psychiatry, 54(11), 905-915.
Leitner, Y. (2014). The co-occurrence of autism and attention
deficit hyperactivity disorder in children - What do we know?
Frontiers in Human Neuroscience, 8, 268.
Individuals with Disabilities Education Act, 20 U.S.C. § 300.8
(2004).
Mikami, A. Y., Smit, S., & Khalis, A. (2017). Social skills
training and ADHD - What works? Current Psychiatry Reports,
19(93).
Zablostky, B., Bramlett, M. D., & Blumberg, S. J. (2020).
The co-occurrence of autism spectrum disorder in children with
ADHD. Journal of Attention Disorders, 24, 94-103.
-
Contact Information
Victoria Petit: [email protected]
Amanda Zanko: [email protected]
mailto:[email protected]:[email protected]