Embed Size (px)
Citation preview

Page 1 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Review
For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
AbstractIntroductionAn acoustic neuroma (also known as vestibular schwannoma) is an in-tracranial tumour of the vestibular nerve that is commonly treated by surgical resection. Following resec-tion, patients may experience a range of symptoms that include deficits in gaze stability, mobility and balance. Vestibular rehabilitation may be use-ful in reducing the severity and mini-mizing the impact of these symptoms.ObjectiveTo systematically review the clinical trial evidence for the effectiveness of vestibular rehabilitation interventions following resection of an acoustic neuroma and provide a concise syn-thesis useful for informing clinical re-habilitation of this patient population.Data sourcesElectronic databases including Cochrane, PubMed, CINAHL, Embase and AUSThealth were searched with no time restriction. Search terms included combinations of MeSH terms (‘acous-tic neuroma’, ‘vestibular schwannoma’, ‘acoustic neurinoma’, ‘acoustic neuri-lemoma’, ‘acoustic neurilemmoma’ or ‘acoustic schwannoma’) and (‘reha-bilitation’, ‘physiotherapy’ ‘physical therapy’, ‘adaptation’, ‘habituation’, ‘balance’, ‘exercise’ or ‘gaze stability’).
Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials
L Passier1, D Doherty1, J Smith1, SM McPhail2,3*
Study selectionRandomized clinical trials of rehabili-tation approaches following surgical resection of acoustic neuroma among adults were included. Studies with mixed populations that included bi-lateral vestibular loss or vestibular dysfunction of central or unknown aetiology were excluded. The 591 hits were screened by title, abstract and then full text by two independent researchers who reached a consen-sus on the eligibility of each study (a third researcher was available to arbitrate but was not required). Six clinical trials fulfilled the inclusion criteria.Data extractionThe characteristics of each study including the trial design, sample, intervention, outcome measures and summary of results were extracted and tabulated.Data synthesisMethodological quality was indepen-dently assessed by two researchers using the Physiotherapy Evidence Database scale. The heterogeneity of both interventions and outcome measures did not allow a valid meta-analysis.ConclusionThere is some evidence to support the use of adaptation exercises for this clinical group. Clinical trial evi-dence does not support the use of habituation exercises alone, although when combined with adaptation ex-ercises and balance and gait training, habituation exercises may have some benefit. Further research is required to determine the optimal combina-tion of vestibular rehabilitation inter-ventions as well as the volume and timing of interventions.
ReviewBackgroundAn acoustic neuroma (also known as vestibular schwannoma) is an intra-cranial tumour of the vestibular nerve that is most commonly treated by surgical resection. Following re-section, patients may experience a range of symptoms that include defi-cits in gaze stability, mobility and balance. The incidence and functional impact of these symptoms have varied across previous reports1–4. Although compensation through parallel sys-tems and central processing usually occurs relatively quickly post-surgery, these impairments can be long last-ing1,5,6. Deficits in measures of bal-ance and mobility have been found in patients at least three months post-resection of an acoustic neuroma who have not undergone vestibular rehabilitation6. Similarly, deficits in gaze control have been found in pa-tients at least three months post- resection of an acoustic neuroma5. Vestibular rehabilitation may be use-ful in reducing the severity and mini-mizing the impact of these symptoms.
A broad Cochrane review of the evidence for vestibular rehabilitation in patients with symptomatic unilat-eral vestibular dysfunction found evidence supporting the use of ves-tibular rehabilitation for symptom resolution and improvement of func-tion7. This review included multiple diagnostic groups including benign paroxysmal positional vertigo, ves-tibular neuritis, Meniere’s disease including endolymphatic hydrops, perilymphatic fistula, unilateral laby-rinthectomy or neurectomy (acoustic or vestibular). It compared vestibular rehabilitation to placebo or sham or
* Corresponding author Email: [email protected] Physiotherapy Department, Princess Alexandra
Hospital, Ipswich Road, Brisbane, Australia2 Centre for Functioning and Health Research,
Buranda Plaza, Corner Ipswich Road and Cornwall Street, Buranda, Brisbane, Australia
3 Queensland University of Technology, School of Public Health and Social Work and Institute of Health and Biomedical Innovation, Kelvin Grove, Brisbane, Australia

For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Page 2 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Review
usual care, vestibular rehabilitation to other kinds of management such as pharmacological and surgical in-terventions and one form of vestibu-lar rehabilitation to another form of vestibular rehabilitation. The review considered vestibular rehabilitation to include a variety of interventions including adaptation exercises, ha-bituation exercises, substitution ex-ercises and balance and gait training activities. Although the review con-cluded that there is moderate evi-dence for vestibular rehabilitation following surgical removal of an acoustic neuroma, there was consid-erable variation in the outcomes of the reported studies, making it diffi-cult to achieve clinical guidance for optimal rehabilitation protocols, in-cluding which elements of vestibular rehabilitation are the most effective for this diagnostic group.
The aim of this manuscript is to provide a systematic review of clini-cal trial evidence for vestibular reha-bilitation interventions following resection of an acoustic neuroma and provide a concise synthesis useful for informing clinical rehabilitation of this patient population.
Search strategyThis review investigated an acoustic neuroma, also known as vestibular schwannoma, acoustic schwannoma, acoustic neurilemoma or acoustic neu-rinoma. Searches were performed in April 2011 in the following data-bases: Cochrane, PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase and AUSThealth. Search syntaxes are pre-sented in Appendix 1.
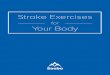
Study selectionA conventional four-stage approach for the identification of studies fulfill-ing the inclusion and exclusion crite-ria was adopted by two researchers (Figure 1). A third member of the re-search team was available to arbi-trate any disagreement between the two researchers, but his intervention
was not required. Studies were screened by title; non-relevant arti-cles and duplicates were removed. Article abstracts were then screened and the articles that did not fulfil the inclusion criteria were excluded. Finally, the full texts of the remaining articles were examined and articles that fulfilled the inclusion criteria were included in the review.
Inclusion and exclusionThe population being investigated was adults following the resection of an acoustic neuroma. Studies with mixed populations that included bi-lateral vestibular loss or vestibular dysfunction of central or unknown aetiology were excluded. Studies were included if the sample com-prised only post-resection of acoustic neuroma patients or a mixed diagno-sis, which included patients post- resection of an acoustic neuroma and patients with unilateral vestibular
loss with pathophysiological presen-tation and mechanism of recovery comparable with post-acoustic neu-roma resection. Only studies using randomized-controlled trial method-ologies were considered eligible for inclusion.
InterventionsThe review considered vestibular re-habilitation interventions that could include walking or gait training, exer-cise, balance training, or specific ves-tibular rehabilitation treatments such as adaptation exercises, habitu-ation exercises and substitution strategies. The authors found that this treatment is primarily delivered by physical therapists, although they may have also been delivered by other suitably qualified profession-als. Adaptation exercises use the er-ror signal created by retinal slip to induce adaptation of vestibulo- ocular reflex8. The ×1 and ×2 viewing
Data sourcesComputer search results Cochrane database (n = 1) PubMed (n = 291) Embase (n = 253) CINAHL (n = 37) AUSThealth (n = 9)
Outcome: 591 ar�cles
591 �tles screened Outcome: 77 ar�cles
Duplicates removed Outcome: 48 ar�cles
48 abstracts screened Outcome: 8 ar�cles
8 full text screened Outcome: 6 ar�cles
6 ar�cles included in final review
Excluded 514 ar�cles
Excluded 29 duplicates
Excluded 40 ar�cles
Excluded 2 ar�cles
Figure 1: Literature search and number of articles excluded at each stage dur-ing study selection.

Page 3 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Review
post-operative vestibular rehabilita-tion intervention or a randomized-controlled trial design.
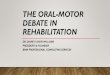
HeterogeneityThere was considerable diversity in methodological rigour between the six randomized-controlled trials. Quality scores using the PEDro scale ranged from 3–7 (Table 1). An inade-quate description of whether an intention-to-treat analysis was con-ducted and failure to specify the eligibility criteria were common limi-tations of the included investigations. Assessments were blinded in four of
total of 591 hits. Screened by title, 514 were removed at this stage as they were not relevant to this review. A further 29 were duplicates and were removed. Abstracts of the 48 re-maining articles were then screened and eight were identified as poten-tially fulfilling the inclusion criteria. The full text of these eight articles was then retrieved and assessed for eligibility, with two further articles removed as they did not fulfil the in-clusion criteria. For investigations of acoustic neuroma patients, the most common reason for the exclusion of articles was the absence of either a
paradigms8 are commonly used adap-tation exercises. In the ×1 viewing paradigm, the visual target is station-ary and, while maintaining visual fix-ation on the target, the patient moves the head back and forth. In the ×2 viewing paradigm, the target and head are moved in opposite direc-tions, again keeping the target in focus throughout. Both paradigms are generally performed using both a near and a far target. Habituation exercises use repeated exposure to provocative movements to produce a reduction in symptoms8. Substitution exercises rely on the utilization of other strategies, such as vision and somatosensory cues, to compensate for the loss of function8.
Data extraction and quality assessmentThe characteristics of each study including the trial design, sample, in-tervention, outcome measures and summary of results were extracted and tabulated. The methodological quality of the included studies was independently assessed by two re-searchers, after which the results were compared and a consensus was reached. A third researcher was avail-able to arbitrate any unresolved as-sessment disagreements. Each study was rated using the Physiotherapy Evidence Database (PEDro) scale. This scale consists of a checklist of 11 items designed to evaluate the meth-odological quality of clinical trials and has evidence to support its valid-ity and reliability for this purpose9–12. One item (eligibility criteria) relates to external validity and is not used in the calculation of the total PEDro score, which ranges between 0 and 10. The heterogeneity of both interven-tions and outcome measures used in the clinical trials did not allow a valid meta-analysis.
Search resultsAn overview of the literature search and study selection is shown in Figure 1. The searches returned a
Table 1 Quality scores (PEDro* scale) for included randomized trialsPEDro scale items Cakrt
et al., 2010
Cohen et al., 2002
Herdman et al., 1995
Herdman et al., 2003
Mruzek et al., 1995
Vereeck et al., 2008
1. Eligibility criteria specified†
0 1 0 1 0 0
2. Randomization 1 1 1 1 1 1 3. Allocation
concealed0 0 0 0 0 0
4. Groups similar at baseline
0 1 1 1 1 1
5. Blinding of subjects
0 0 0 1 0 0
6. Blinding of therapists
0 0 0 0 0 0
7. Blinding of assessors
0 1 1 1 0 1
8. Adequate follow-up
0 0 1 1 0 1
9. Intention-to-treat analysis‡
0 0 0 0 0 0
10. Between groups statistical comparison
1 1 1 1 1 1
11. Point and variability measures
1 1 1 1 1 1
Total 3 5 6 7 4 6*Range 0–10 points. †Eligibility criteria are related to external validity and not used in the cumulative total. ‡Intention-to-treat analysis may have been undertaken, but was not explicitly stated for all included studies. PED, Physiotherapy Evidence Database

For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Page 4 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Review
all of which reported positive find-ings. One of these17 found an im-provement in postural stability and reduction in the complaint of dis-equilibrium with the performance of adaptation exercises in the acute post-operative period (day 3–6). A further study by the same lead au-thor13 reported improvement in gaze stability in a mixed population of patients with unilateral vestibular hypofunction that included patients 2–17 weeks post-resection of an acoustic neuroma. A customized pro-gramme of vestibular rehabilitation that included both adaptation and habituation exercises was found to improve postural control, particu-larly in patients older than 50 years of age18.
Effect of ambulation and balance retrainingThree13,14,18 of six studies included ambulation (walking or gait) and balance training as a component of vestibular rehabilitation. Of the re-maining three studies, two16,17 in-cluded only ambulation training and one15 included only balance training. In four of the studies13,14,17,18, ambula-tion or balance was included in both the control and intervention groups. This did not allow conclusions to be drawn about the effect of these inter-ventions from those studies. One study18 implemented balance train-ing as part of a multi-faceted vestibu-lar rehabilitation intervention and although positive findings were re-ported, it was difficult to attribute improvement to any one facet of the intervention, such as ambulation and balance retraining exercises. Only one study15 specifically examined balance retraining in the acute post-operative period (day 5–14). This study found that patients who under-took balance retraining with visual biofeedback demonstrated better compensation and postural control than patients who performed bal-ance rehabilitation without visual biofeedback cues.
measured in five studies, although with variation in utilization, for ex-ample some studies considered the six Sensory Organisation Test condi-tions,14,15,17 while others considered only one of the six conditions16 or used a composite score14. Two stud-ies17,18 considered clinical measures of balance and gait and one study13 did not include any measures of pos-tural control or balance.
Effect of habituation exercisesThree studies14,16,18 included habitua-tion exercises in the interventions. One study16 implemented habituation exercises as the only primary inter-vention. Findings from this study did not demonstrate a benefit from ha-bituation exercises in the first week post-resection of an acoustic neu-roma for balance, vestibulo-ocular reflex function or spatial orientation. The other two studies14,18 investi-gated habituation exercises in con-junction with balance training. One of these14 reported findings that were similar to the habituation-only inves-tigation; however, the reduction in both motion sensitivity and self- perceived dizziness handicap was suggestive of more rapid improve-ment post-surgery. In contrast, the other reported early vestibular reha-bilitation including habituation, bal-ance and gaze stability exercises resulted in improved postural control for patients older than 50 years of age18. This discrepancy in findings across studies could be due to the ad-dition of gaze stability exercises alone or a combined effect of gaze stability exercises with habituation exercises and balance training. Alternatively, the difference may be reflective of the customization of ves-tibular rehabilitation programmes in one study18 compared with the pre-scriptive approach used in the other two studies14,16.
Effect of adaptation exercisesThe effect of adaptation exercises was investigated in three studies14,17,18,
six investigations. Two studies13,14 also included some patients with unilat-eral vestibular loss not caused by an acoustic neuroma, and all studies had small sample sizes (range, n = 15–65).
A variety of intervention types and duration were reported in the studies including adaptation exercises, ha-bituation exercises, range of motion exercises, balance training, walking, general instruction and social rein-forcement (Table 2). The intervention period in three studies15–17 was lim-ited to the acute post-operative period (day 1–14). In one study18, the inter-ventions commenced in the acute post-operative period (day 3–5) and continued until 12 weeks post-sur-gery. In another14, the interventions were commenced the day after hos-pital discharge and continued until eight weeks post-surgery. Follow-up periods ranged from six days post-operatively17 to 12 months18.
Monitoring of adherence to the intervention protocol varied across the studies. Observations of adher-ence were noted in five studies13,15–18 by the therapist treating each patient daily or through the use of a diary or a calendar. However, only one study13 described the level of adherence to the prescribed intervention and con-sidered a patient to be compliant if he/she completed more than 50% of the prescribed exercises.
There was considerable variation in the outcome measures used across the studies (Table 2). Patients in all except one study13–16,18 underwent tests of vestibular function such as calories, rotary chair testing and quantified dynamic visual acuity be-fore the surgery or interventions. Only three studies13,14,16 used any vestibular functions test as an out-come measure. The investigators in one trial17 decided against the use of some clinical assessment items (Table 2) because of the acuity of their participants and the potential risk of adverse events with more vigorous testing early in the post- operative period. Posturography was

Page 5 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Review
Tabl
e 2
Sum
mar
y of
stud
y de
sign
s, sa
mpl
es, i
nter
venti
ons,
out
com
e m
easu
res a
nd re
sults
of i
nclu
ded
stud
ies
Stud
ySt
udy
desi
gn a
nd
popu
latio
nIn
terv
entio
nO
utco
me
mea
sure
sSu
mm
ary
of re
sults
Cakr
t et
al.,
20
10
• RC
T•
Patie
nts u
nder
goin
g re
mov
al o
f ve
stibu
lar
schw
anno
ma
• Co
ntro
l gro
up
(n =
8)
• In
terv
entio
n gr
oup
(n =
9)
• In
terv
entio
n: D
ay
5–14
pos
t-sur
gery
• As
sess
men
t: pr
e-op
erati
ve, d
ay 5
an
d da
y 14
pos
t-su
rger
y
Cont
rol:
Reha
bilit
ation
with
out v
isual
bio
feed
back
• Id
entic
al e
xerc
ises t
o th
e in
terv
entio
n gr
oup
Inte
rven
tion:
Reha
bili t
ation
usin
g vi
sual
bio
feed
back
•
Shift
ing
cent
re o
f pre
ssur
e on
forc
e pl
atfor
m w
ith v
isual
targ
ets o
n m
onito
r sc
reen
Both
gro
ups:
Vesti
bula
r ada
ptati
on e
xerc
ises f
or
vesti
bula
r-ocu
lar r
eflex
•
×1 v
iew
ing
ex w
ith n
ear a
nd fa
r tar
get,
horiz
onta
lly a
nd v
ertic
ally
Dura
tion
of tr
eatm
ents
: In
crea
sed
grad
ually
from
min
utes
day
5
post
-sur
gery
, up
to 4
0 m
inut
es o
n th
e da
y of
disc
harg
e (d
ay 1
4 or
15
post
-sur
gery
)
• Po
stur
ogra
phy
– Ce
ntre
of
foot
pre
ssur
e pa
ram
eter
s du
ring
the
Clin
ical
Test
fo
r Sen
sory
In
tera
ction
of
Bal
ance
co
nditi
ons
(1–4
)
Firm
surf
ace
with
eye
s clo
sed:
Con
trol
and
inte
rven
tion
grou
ps si
mila
r
Foam
surf
ace
with
eye
s clo
sed:
Sta
tistic
ally
sign
ifica
nt
impr
ovem
ent i
n in
terv
entio
n gr
oup
in 5
out
of 7
cen
tre
of fo
ot p
ress
ure
para
met
ers (
p va
lues
0.0
08–0
.027
)
Sum
mar
yTh
ese
findi
ngs i
ndic
ate
visu
al b
ased
reha
bilit
ation
tr
eatm
ent i
mpr
oved
pos
tura
l con
trol
bett
er th
an
reha
bilit
ation
with
out v
isual
feed
back
Cohe
n
et a
l.,
2002
• RC
T•
Patie
nts s
ched
uled
fo
r res
ectio
n of
AN
(n
= 3
1)•
Cont
rol g
roup
(n
= 1
5)•
Inte
rven
tion
grou
p (n
= 1
6)•
Inte
rven
tion:
Day
1
post
-sur
gery
to
disc
harg
e da
y 5–
6 po
st-s
urge
ry•
Asse
ssm
ent:
pre-
oper
ative
, di
scha
rge,
ap
prox
imat
ely
3, 7
an
d 13
wee
ks p
ost-
surg
ery
Cont
rol:
Atten
tion
from
labo
rato
ry a
ssist
ant
• Ar
ousa
l and
psy
chol
ogic
al su
ppor
tIn
terv
entio
n:Se
en b
y th
erap
istDa
y 1:
• Pa
ssiv
e ra
nge
of m
otion
of h
ead
and
neck
in y
aw, p
itch
and
roll
whi
le ly
ing
sem
i rec
lined
in b
ed, y
aw li
mite
d by
dr
essin
g siz
e to
ope
rate
d sid
eDa
y 2
and
3:
• Pa
ssiv
e ra
nge
of m
otion
with
hea
d aw
ay fr
om b
ed fo
r ful
l ran
ge o
f moti
on;
activ
e ra
nge
of m
otion
as f
ast a
s po
ssib
le•
Perfo
rmed
sitti
ng in
bed
or c
hair
if po
ssib
leDa
y 3:
•
Pass
ive
rang
e of
moti
on w
ith h
ead
away
from
bed
for f
ull r
ange
of m
otion
;
• Ro
tary
cha
ir te
sting
– ve
stibu
lar-
ocul
ar re
flex
• Su
bjec
tive
verti
go in
tens
ity
and
freq
uenc
y•
Dyna
mic
po
stur
ogra
phy
– Se
nsor
y or
gani
satio
n te
st•
Path
inte
grati
on
test
Verti
go in
tens
ity a
nd fr
eque
ncy:
No
signi
fican
t diff
eren
ce b
etw
een
grou
ps
Vesti
bula
r-ocu
lar r
eflex
(VO
R) :
No
signi
fican
t effe
ct o
f age
, lev
el o
r ver
tigo
or
expe
rimen
tal g
roup
on
VOR
gain
, sym
met
ry o
r as
ymm
etry
Sens
ory
orga
nisa
tion
test
(Con
ditio
n 5)
:N
o sig
nific
ant d
iffer
ence
bet
wee
n ex
perim
enta
l gro
ups
Path
inte
grati
on:
No
signi
fican
t diff
eren
ce b
etw
een
expe
rimen
tal g
roup
s
Sum
mar
yN
o ev
iden
ce fo
r ves
tibul
ar re
habi
litati
on d
urin
g ac
ute
post
-ope
rativ
e w
eek
in te
rms o
f im
prov
ed V
OR
func
tion,
bal
ance
and
spati
al o
rient
ation
Rate
of c
ompe
nsati
on re
late
d to
tum
our s
ize(C
ontd
.)

For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Page 6 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Review
Tabl
e 2
(Con
tinue
d)St
udy
Stud
y de
sign
and
po
pula
tion
Inte
rven
tion
Out
com
e m
easu
res
Sum
mar
y of
resu
lts
Cohe
n
et a
l.,
2002
activ
e ra
nge
of m
otion
as f
ast a
s pos
sible
• Pe
rform
ed si
tting
in c
hair
• Co
mm
ence
d tr
unk
mov
emen
ts in
all
plan
es, c
ombi
ned
with
upp
er li
mb
reac
hing
mov
emen
ts re
quiri
ng p
atien
t to
turn
and
look
whi
lst re
achi
ng•
Wal
king
if to
lera
ted
Day
4 an
d 5:
•
Activ
e ra
nge
of m
otion
hea
d w
hile
sitti
ng•
Wal
king
long
er d
istan
ces f
rom
3 to
10
m a
s tol
erat
ed w
ith a
ugm
ente
d he
ad m
ovem
ents
in p
itch
and
yaw
Da
y 5
or 6
: •
Disc
harg
e at
surg
eon’
s disc
retio
n ba
sed
on m
edic
al st
atus
and
safe
mob
ility
. Bo
th g
roup
s:•
Patie
nts s
een
2× d
aily
• Du
ratio
n gr
adua
lly in
crea
sed
as
tole
rate
d fr
om 5
min
utes
of t
reat
men
t da
y 1
to 3
0 m
inut
es d
ay b
efor
e di
scha
rge
Herd
man
et
al.,
19
95
• RC
T•
Patie
nts s
ched
uled
fo
r res
ectio
n of
AN
(n
= 1
9)•
Cont
rol g
roup
(n
= 8
)•
Inte
rven
tion
grou
p (n
= 1
1)•
Inte
rven
tion:
co
mm
ence
d da
y 3
post
-sur
gery
• As
sess
men
t:
pre-
oper
ative
, dai
ly
post
-sur
gery
Cont
rol:
Smoo
th p
ursu
it ex
erci
ses (
with
out h
ead
mov
emen
t) p
erfo
rmed
:•
in b
oth
verti
cal a
nd h
orizo
ntal
di
recti
ons
• in
stan
ding
and
sitti
ng•
for 1
min
ute
each
, five
tim
es p
er d
ay,
for t
otal
of 2
0 m
inut
es p
er d
ayIn
terv
entio
n:Ex
erci
ses t
o in
crea
se v
estib
ular
gai
n (×
1 vi
ewin
g pa
radi
gm (h
orizo
ntal
and
ver
tical
he
ad m
ovem
ents
mai
ntai
ning
visu
al
fixati
on) p
erfo
rmed
:•
on n
ear t
arge
t (ar
ms l
engt
h) o
r far
ta
rget
(acr
oss t
he ro
om)
• in
stan
ding
and
sitti
ng
• VA
S fo
r ve
rtigo
and
di
sequ
ilibr
ium
• Ro
mbe
rg•
Qua
litati
ve g
ait
anal
ysis
• O
culo
mot
or te
st–
Spon
tane
ous
nyst
agm
us–
Gaze
evo
ked
nyst
agm
us–
VOR
to sl
ow
and
horiz
onta
l he
ad th
rust
s
Verti
go:
No
diffe
renc
e be
twee
n gr
oups
Dise
quili
briu
m:
At d
ay 1
–4 p
ost-s
urge
ryth
ere
was
no
diffe
renc
e be
twee
n gr
oups
At d
ay 5
and
6 p
ost-s
urge
ry th
e in
terv
entio
n gr
oup
expe
rienc
ed le
ss d
isequ
ilibr
ium
than
con
trol
gro
up
(p <
0.0
5)
Rom
berg
:At
day
3, 2
5% o
f con
trol
and
64%
of i
nter
venti
on g
roup
co
uld
perf
orm
with
eye
s clo
sed
At d
ay 6
, 57%
of c
ontr
ol a
nd 8
0% o
f int
erve
ntion
gro
up
coul
d pe
rfor
m w
ith e
yes c
lose
d

Page 7 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Review
• fo
r 1 m
inut
e ea
ch, fi
ve ti
mes
per
day
, fo
r a to
tal o
f 20
min
utes
a d
ayBo
th g
roup
s:Am
bula
tion
• Po
stur
ogra
phy
– Pe
ak to
pea
k an
terio
r–po
ster
ior
sway
– To
tal s
way
pa
th–
Freq
uenc
y of
sw
ay
Qua
litati
ve g
ait a
naly
sis:
At d
ay 3
, all
subj
ects
had
wid
e ba
se o
f sup
port
, m
inim
al–m
oder
ate
atax
ia a
nd re
duce
d he
adm
ovem
ent.
Thre
e of
8 in
con
trol
gro
up a
nd 3
of 1
1 in
th
e in
terv
entio
n gr
oup
need
ass
istan
ce o
f one
per
son
for s
afe
ambu
latio
nAt
day
6, a
ll of
the
cont
rol g
roup
and
40%
of
inte
rven
tion
grou
p w
ere
cons
ider
ed to
hav
e an
abn
orm
al g
ait.
All o
f the
con
trol
and
50%
of
inte
rven
tion
grou
p ha
d so
me
atax
ia o
r ata
xia
with
hea
d tu
rns w
hilst
wal
king
No
signi
fican
t diff
eren
ce b
etw
een
gait
on d
ay 6
pos
t-op
erati
vely
and
any
pre
-ope
rativ
e cl
inic
al a
sses
smen
t
Gaze
evo
ked
nyst
agm
us (r
oom
ligh
t):
At d
ay 3
, 88%
of t
he c
ontr
ol a
nd 9
1% o
f the
inte
rven
tion
grou
p ha
d ga
ze e
voke
d ny
stag
mus
At d
ay 6
, 71%
of t
he c
ontr
ol a
nd 7
3% o
f the
inte
rven
tion
grou
p ha
d ga
ze e
voke
d ny
stag
mus
VOR
(clin
ical
) to
slow
hea
d ro
tatio
ns:
At d
ay 3
, 25%
of t
he c
ontr
ol a
nd 5
5% o
f the
inte
rven
tion
grou
p ha
d cl
inic
ally
nor
mal
VO
RAt
day
6, 2
9% o
f the
con
trol
and
73%
of t
he in
terv
entio
n gr
oup
had
clin
ical
ly n
orm
al V
OR
Post
urog
raph
y:
At d
ay 3
, the
re w
as n
o di
ffere
nce
in p
eak
to p
eak
sway
be
twee
n pr
e- a
nd p
ost-s
urge
ry m
easu
res o
n te
sts
1–3
for c
ontr
ol o
r int
erve
ntion
gro
ups.
The
re w
as a
di
ffere
nce
(p <
0.0
5) b
etw
een
pre-
and
pos
t-sur
gery
on
test
s 4–6
for b
oth
cont
rol a
nd in
terv
entio
n gr
oups
.At
day
6, t
here
was
no
diffe
renc
e be
twee
n pr
e- a
nd
post
-sur
gery
on
test
s 1–3
for c
ontr
ol o
r int
erve
ntion
gr
oups
. The
re w
as a
sign
ifica
nt d
iffer
ence
(p <
0.0
2)
betw
een
pre-
and
pos
t-sur
gery
on
test
4–6
for t
he
cont
rol g
roup
. The
re w
as a
sign
ifica
nt d
iffer
ence
(p
< 0
.04)
bet
wee
n pr
e- a
nd p
ost-s
urge
ry fo
r tes
t 5 a
nd
6 bu
t no
diffe
renc
e on
test
4 fo
r int
erve
ntion
gro
up
Sum
mar
y:Ve
stibu
lar a
dapt
ation
exe
rcise
s dur
ing
the
initi
al p
ost-
surg
ical
per
iod
faci
litat
es ra
te o
f rec
over
y of
pos
tura
l(C
ontd
.)

For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Page 8 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Review
Tabl
e 2
(Con
tinue
d)St
udy
Stud
y de
sign
and
po
pula
tion
Inte
rven
tion
Out
com
e m
easu
res
Sum
mar
y of
resu
lts
stab
ility
, dec
reas
es e
xper
ienc
e of
dise
quili
briu
m a
nd
impr
oves
VO
R cl
inic
ally
Herd
man
et
al.,
20
03
• RC
T•
Patie
nts w
ith
unila
tera
l ves
tibul
ar
loss
refe
rred
to
labo
rato
ry fo
r as
sess
men
t
• Co
ntro
l gro
up
(n =
8)
• In
terv
entio
n gr
oup
(n =
13)
• In
terv
entio
n:
4–5
wee
ks
• As
sess
men
t: pr
e-in
terv
entio
n,
2-w
eek
inte
rval
s aft
er c
omm
enci
ng
inte
rven
tion
Cont
rol:
Vesti
bula
r neu
tral
exe
rcise
s•
Sacc
adic
eye
mov
emen
ts w
ith h
ead
stati
onar
y ag
ains
t a fe
atur
eles
s sur
face
Gait
and
bala
nce
exer
cise
s•
Excl
udin
g ex
erci
sed
inco
rpor
ating
hea
d m
ovem
ents
Inte
rven
tion:
Adap
tatio
n ex
erci
ses
(×1
and
×2 v
iew
ing
para
digm
s)Ey
e–he
ad e
xerc
ises t
o ta
rget
Gait
and
bala
nce
exer
cise
s
Both
gro
ups:
Hom
e pr
ogra
mm
e•
perf
orm
ed e
xerc
ises 4
–5×
daily
for a
to
tal o
f 20–
30 m
inut
es
• pl
us 2
0 m
inut
es b
alan
ce a
nd g
ait
exer
cise
s
• Dy
nam
ic v
isual
ac
uity
– Pr
edic
tabl
e he
ad
mov
emen
t (s
ubje
ct
mov
es h
ead)
– U
npre
dict
able
he
ad
mov
emen
t (a
sses
sor
mov
es h
ead)
• VA
S fo
r visu
al
blur
ring
Dyna
mic
visu
al a
cuity
cha
nge:
Ther
e w
as n
o ch
ange
in d
ynam
ic vi
sual
acu
ity p
redi
ctab
le
or u
npre
dict
able
in th
e co
ntro
l gro
up. T
here
was
sig
nific
ant i
mpr
ovem
ent (
p <
0.01
) in
dyna
mic
visu
al
acui
ty p
redi
ctab
le in
the
inte
rven
tion
grou
p w
ith 1
2 of
13
subj
ects
retu
rnin
g to
nor
mal
for a
ge. I
nter
venti
on g
roup
al
so h
ad si
gnifi
cant
impr
ovem
ent (
p <
0.01
) in
dyna
mic
vi
sual
acu
ity u
npre
dict
able
O
nly
exer
cise
type
con
trib
uted
sign
ifica
ntly
(p =
0.0
09)
to c
hang
e in
dyn
amic
visu
al a
cuity
pre
dict
able
and
for
50.5
% o
f cha
nge
in d
ynam
ic v
isual
acu
ity u
npre
dict
able
VAS
for v
isual
blu
rrin
g:Th
ere
was
a si
gnifi
cant
redu
ction
in v
isual
blu
rrin
g fo
r co
ntro
l (p
= 0.
02) a
nd in
terv
entio
n gr
oup
(p =
0.0
3)
Sum
mar
yTh
e re
cove
ry o
f gaz
e st
abili
ty d
urin
g pr
edict
able
hea
d m
ovem
ents
and
to a
less
er e
xten
t unp
redi
ctab
le
head
mov
emen
ts, c
an b
e fa
cilita
ted
with
ves
tibul
ar
reha
bilit
ation
exe
rcise
s. Im
prov
emen
t occ
urs i
n <5
wee
ksM
ruze
k et
al.,
19
95
• RC
T•
24 p
atien
ts
sche
dule
d fo
r un
ilate
ral v
estib
ular
ab
latio
n•
Cont
rol g
roup
, (n
= 8
)•
Inte
rven
tion
gr
oup
1 (n
= 8
)•
Inte
rven
tion
gr
oup
2 (n
= 8
)•
Inte
rven
tion:
co
mm
ence
d da
y 1
po
st-h
ospi
tal
disc
harg
e
Cont
rol G
roup
:Ra
nge
of m
otion
pro
gram
me
• Sh
ould
er, e
lbow
, hip
, kne
e an
d an
kle
rang
e of
moti
on e
xerc
ises p
erfo
rmed
in
sitting
pos
ition
• N
o he
ad a
nd n
eck
moti
ons
Soci
al re
info
rcem
ent
• En
cour
agem
ent a
nd p
raise
for
parti
cipa
ting
in e
xerc
ises
• 3–
5 m
inut
e ph
one
calls
, 1–2
tim
es
per w
eek—
rem
inde
d to
do
exer
cise
s,
rein
forc
ed c
ompl
ianc
e an
d en
cour
aged
to
con
tinue
pro
gram
me
• 10
–15
min
ute
mee
tings
with
ph
ysio
ther
apist
dur
ing
follo
w-u
p te
sting
• Dy
nam
ic
post
urog
raph
y–
Sens
ory
Org
anisa
tion
Test
• M
otion
Se
nsiti
vity
Q
uotie
nt•
Dizz
ines
s Ha
ndic
ap
Inve
ntor
y•
Rota
ry c
hair
– As
ymm
etry
in
dex
Sens
ory
orga
nisa
tion
test
:In
terv
entio
n gr
oup
2 pe
rfor
med
sign
ifica
ntly
bett
er
(p =
0.0
13) t
han
the
cont
rol g
roup
on
sens
ory
orga
nisa
tion
test
con
ditio
n tw
o at
five
wee
ks p
ost-
surg
ery.
The
re w
ere
no o
ther
sign
ifica
nt d
iffer
ence
s
Moti
on se
nsiti
vity
quo
tient
:At
7 w
eeks
pos
t-sur
gery
bot
h in
terv
entio
n gr
oups
had
sig
nific
antly
less
(p =
0.0
3) m
otion
sens
itivi
ty th
an th
e co
ntro
l gro
up
Dizz
ines
s han
dica
p in
vent
ory:
At 8
wee
ks p
ost-s
urge
ry, i
nter
venti
on g
roup
1 h
ad
signi
fican
tly le
ss (p
= 0
.05)
phy
sical
disa
bilit
y th
an th
e co
ntro
l gro
up

Page 9 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Review
• As
sess
men
t:
With
in 1
mon
th
pre-
oper
ative
, da
y 5
post
-sur
gery
, th
en 2
, 5 a
nd 7
w
eeks
pos
t-sur
gery
se
ssio
ns—
prog
ress
disc
usse
d,
ques
tions
ans
wer
ed, v
erba
l en
cour
agem
ent o
ffere
d
Subj
ects
wer
e gi
ven
no in
stru
ction
abo
ut
parti
cipa
ting
in a
ny re
gula
r acti
vity
but
m
ay h
ave
rece
ived
gen
eral
inst
ructi
on
from
the
phys
icia
n
Inte
rven
tion
1:Ve
stibu
lar r
ehab
ilita
tion
• Ha
bitu
ation
exe
rcise
s •
Bala
nce
exer
cise
s•
Daily
wal
king
pro
gram
me
Soci
al re
info
rcem
ent
• As
per
con
trol
gro
up
Inte
rven
tion
2:•
Vesti
bula
r reh
abili
tatio
n •
As p
er in
terv
entio
n gr
oup
1
All g
roup
s:Co
mm
ence
d as
hom
e pr
ogra
mm
e on
the
day
after
hos
pita
l disc
harg
eIn
stru
cted
to p
erfo
rm
• 15
-min
ute
sess
ions
, tw
ice
per d
ay•
daily
wal
k (g
roup
s 1 a
nd 2
onl
y)
Asym
met
ry in
dex:
No
signi
fican
t diff
eren
ce b
etw
een
grou
ps. A
sym
met
ry
at se
ven
wee
ks p
ost-s
urge
ry w
as c
lose
to p
re-s
urge
ry
leve
ls
Sum
mar
yPa
tient
s can
effe
ctive
ly c
ompe
nsat
e irr
espe
ctive
of t
he
ther
apy
prog
ram
me
they
par
ticip
ate
in. R
educ
tion
in
moti
on se
nsiti
vity
and
self-
perc
eive
d di
zzin
ess h
andi
cap
for p
atien
ts p
artic
ipati
ng in
ves
tibul
ar re
habi
litati
on
sugg
ests
mor
e ra
pid
and
perh
aps m
ore
com
plet
e re
cove
ry in
thes
e pa
tient
s
Vere
eck
et a
l.,
2008
• RC
T •
57 p
atien
ts fo
r re
secti
on o
f AN
• Co
ntro
l gro
up
<50
year
s (n
= 11
)•
Cont
rol g
roup
>5
0 ye
ars (
n =
11)
• In
terv
entio
n gr
oup
<50
year
s (n
= 16
)•
Inte
rven
tion
grou
p >5
0 ye
ars (
n =
15)
• In
terv
entio
n:
com
men
ced
post
-op
erati
vely
and
Cont
rol:
(gen
eral
inst
ructi
ons)
Pre-
oper
ative
lyIn
form
ation
Post
-sur
gery
Inst
ruct
ed to
wal
k, e
at a
t tab
le, s
tairs
, w
atch
TV,
read
as s
oon
as p
ossib
le
Post
-disc
harg
e fo
llow
-up
Info
rmed
of l
evel
of p
ostu
ral c
ontr
olDi
scus
sed
gene
ral l
evel
of a
ctivi
ty a
nd
frig
hten
ing
mov
emen
ts a
nd si
tuati
ons
Enco
urag
ed to
incr
ease
acti
vity
leve
ls in
clud
ing
wal
king
, cyc
ling,
driv
ing,
spor
tN
o fo
rmal
hom
e pr
ogra
mm
e gi
ven
• St
andi
ng
bala
nce
– Ro
mbe
rg
(floo
r)–
Rom
berg
(fo
am)
– Sh
arpe
ned
Rom
berg
– Si
ngle
lim
b st
ance
• Ti
med
up
and
go te
st•
Tand
em g
ait
• Dy
nam
ic g
ait
inde
x
Patie
nts >
50 y
ears
:Th
e in
terv
entio
n gr
oup
perf
orm
ed si
gnifi
cant
ly b
etter
(p
< 0
.05)
than
con
trol
gro
up o
n al
l tes
ts a
t all
asse
ssm
ents
with
the
exce
ption
of D
ynam
ic G
ait I
ndex
in
the
acut
e re
cove
ry p
erio
d (1
–6 w
eeks
pos
t-sur
gery
) an
d st
andi
ng b
alan
ce a
nd ta
ndem
gai
t in
the
follo
w-u
p pe
riod
(6 a
nd 1
2 m
onth
s pos
t-sur
gery
)At
6 w
eeks
pos
t-sur
gery
, bal
ance
mat
ched
per
surg
ery
mea
sure
s in
the
inte
rven
tion
grou
p. A
t 12
wee
ks p
ost-
surg
ery,
the
inte
rven
tion
grou
p pe
rfor
med
bett
er th
an
pre-
surg
ery
At 1
yea
r pos
t-sur
gery
, the
inte
rven
tion
grou
p sti
ll pe
rfor
med
bett
er th
an p
re-s
urge
ry
(Con
td.)

For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Page 10 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Review
Tabl
e 2
(Con
tinue
d)St
udy
Stud
y de
sign
and
po
pula
tion
Inte
rven
tion
Out
com
e m
easu
res
Sum
mar
y of
resu
lts
• co
ntinu
ed to
12
wee
ks p
ost-s
urge
ry
• As
sess
men
t:
pre-
oper
ative
, ho
spita
l disc
harg
e (1
wee
k po
st-
surg
ery)
, 3, 6
, 9
and1
2 w
eeks
then
6
and
12 m
onth
s po
st-s
urge
ry
Inte
rven
tion:
(c
usto
mize
d ve
stibu
lar r
ehab
ilita
tion)
Pre-
oper
ative
lyIn
form
ation
Post
-ope
rativ
ely
Sam
e as
con
trol
gro
ups p
lus
Basic
exe
rcise
s•
Com
men
ced
day
3–5
post
-sur
gery
• Su
perv
ised
wal
king
with
dec
reas
ing
base
of s
uppo
rt, i
ncor
pora
te h
ead
mov
emen
ts, t
read
mill
wal
king
Post
-disc
harg
e fo
llow
-up
cust
omize
d ho
me
prog
ram
me
• 5
activ
ities
incl
udin
g ga
ze st
abili
ty a
nd
moti
on se
nsiti
vity
, bal
ance
and
wal
king
• Pe
rform
ed 3
× da
ily, t
otal
30
min
/day
Patie
nts <
50 y
ears
: N
o sig
nific
ant e
ffect
of e
xper
imen
tal g
roup
on
test
s
Sum
mar
yFo
r pati
ents
>50
yea
rs e
arly
cus
tom
ized
vesti
bula
r re
habi
litati
on re
sulte
d in
bett
er p
ostu
ral c
ontr
ol th
an
gene
ral i
nstr
uctio
ns o
nly
For p
atien
ts <
50 y
ears
gen
eral
inst
ructi
ons m
ay b
e en
ough
; how
ever
, som
e yo
unge
r pati
ents
may
ben
efit
from
a v
estib
ular
reha
bilit
ation
pro
gram
me

Page 11 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Review
Study limitationsThere were a number of limitations evident from this review of random-ized-controlled trials. In addition to the presence of only a small number of randomized studies, all had small sample sizes. Most of the studies in-vestigated vestibular rehabilitation interventions within the first two weeks post-operatively, with only two14,18 continuing interventions for eight and 12 weeks, respectively. Only one study18 included six- and 12-month follow-up assessments, making it difficult to speculate about the long-term effect of vestibular rehabilitation interventions on the patient group. The heterogeneity in interventions across studies and the outcome measures used did not allow valid meta-analyses. Greater consistency of outcome measures used and standardized time-frames for application of the measures in fu-ture studies will aid the interpreta-tion of pooled results across clinical trials and allow stronger conclusions to be drawn.
Compliance with exercise proto-cols is another important consider-ation that was not adequately reported across the trials. Vestibular rehabilitation interventions include exercises that may induce symptoms of dizziness and related discomfort. Patients may not adhere to treatment protocols to avoid discomfort (or for other reasons). It is likely that some level of adherence to the ves-tibular rehabilitation intervention is a pre-requisite to its effectiveness. Non-compliance with exercises is likely to adversely affect the findings of a study and careful monitoring is warranted. This is perhaps easier among inpatients than community-based patients. It is possible for fu-ture studies to mandate a minimum level of compliance with the inter-vention protocol if the aim is to inves-tigate the direct response to the vestibular rehabilitation intervention. However, if the aim of a trial is to inves-tigate the feasibility and effectiveness
exercises in combination with other vestibular rehabilitation interven-tions such as adaptation exercises, gait and balance training may pro-mote more rapid recovery18.
For patients older than 50 years of age, customized vestibular reha-bilitation incorporating adaptation, habituation, balance and mobility im-proved outcomes18. For most patients younger than 50 years of age, a sim-ple exercise programme may be suf-ficient18, although it may be necessary to screen for patients likely to require more customized or intensive reha-bilitation. The Romberg test with closed eyes performed on the third post-operative day was identified as a potential indicator of such patients17. Interestingly, age was not a predictor of recovery13,16,17 following resection of an acoustic neuroma.
Findings from this review have provided a more focused analysis of the clinical trial evidence for vestibu-lar rehabilitation following resection of an acoustic neuroma than that reported in the 2007 Cochrane re-view of vestibular rehabilitation7. None of the studies of vestibular re-habilitation following resection of an acoustic neuroma included in the Cochrane review were included in a comparative analysis between forms of vestibular rehabilitation. It is possible that the variability in the findings of the Cochrane review is a result of considering vestibular reha-bilitation interventions collectively rather than isolating techniques to determine which approach is the most effective. This is in contrast with this systematic review, which considered the different types of vestibular rehabilitation interven-tions or combinations of interven-tions. A more detailed analysis of the randomized-controlled trials investi-gating vestibular rehabilitation fol-lowing the resection of an acoustic neuroma has provided greater in-sight into the efficacy of various com-ponents of vestibular rehabilitation interventions.
Effect of social reinforcement and attention and instructionThe effect of social reinforcement on post-operative recovery was investi-gated in one study14, which found no statistically significant difference in outcomes between treatment and control groups. However, a trend to-wards reduced emotional scores on the Dizziness Handicap Inventory our weeks post-operatively was evi-dent. The small sample size (n = 24) for this three group trial (8 per group) indicated that a Type 2 error may have occurred.
ConclusionMain findingsThe six investigations included in this systematic review have provided some empirical evidence to support the use of vestibular rehabilitation following resection of an acoustic neuroma. The heterogeneous quality of clinical trial reporting, the inter-ventions evaluated and the outcome measures used helped the authors to draw reserved conclusions on the effectiveness of the vestibular reha-bilitation interventions that were evaluated. Overall, there appears to be evidence for the use of adaptation exercises13,17,18, at least in the acute post-operative period.
Current clinical trial evidence does not support the use of habituation exercises in isolation following resection of an acoustic neuroma. Differences in the findings between the two studies of habituation exercises14,16 may be attributed to the outcome measures used. One study14 used the Motion Sensitivity Quotient19, a measure of motion-induced dizzi-ness, and the Dizziness Handicap Inventory20, a measure of self-perceived disability due to vestibular dysfunction. The inclusion of the Motion Sensitivity Quotient in the other study16 may have yielded a dif-ferent result. A salient finding from this study, though, is that habituation exercises did not produce a change in vestibulo-ocular reflex. Habituation

For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Page 12 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
Review
10. Foley NC, Bhogal SK, Teasell RW, Bureau Y, Speechley MR. Estimates of quality and reliability with the physio-therapy evidence-based database scale to assess the methodology of randomized controlled trials of pharmacological and nonpharmacological interventions. Phys Ther. 2006 Jun;86(6):817–24.11. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of random-ized controlled trials. Phys Ther. 2003 Aug;83(8):713–21.12. Moseley AM, Herbert RD, Sherrington C, Maher CG. Evidence for physiotherapy practice: a survey of the Physiotherapy Evidence Database (PEDro). Aust J Physiother. 2002;48(1):43–9.13. Herdman SJ, Schubert MC, Das VE, Tusa RJ. Recovery of dynamic visual acu-ity in unilateral vestibular hypofunction. Arch Otolaryngol Head Neck Surg. 2003 Aug;129(8):819–24.14. Mruzek M, Barin K, Nichols DS, Burnett CN, Welling DB. Effects of vestib-ular rehabilitation and social reinforce-ment on recovery following ablative vestibular surgery. Laryngoscope. 1995 Jul;105(7 Pt 1):686–92.15. Cakrt O, Chovanec M, Funda T, Kalitová P, Betka J, Zverina E, et al. Exercise with visual feedback improves postural stabil-ity after vestibular schwannoma surgery. Eur Arch Otorhinolaryngol. 2010 Sep; 267(9):1355–60.16. Cohen HS, Kimball KT, Jenkins HA. Factors affecting recovery after acoustic neuroma resection. Acta Otolaryngol. 2002 Dec;122(8):841–50.17. Herdman SJ, Clendaniel RA, Mattox DE, Holliday MJ, Niparko JK. Vestibular adaptation exercises and recovery: acute stage after acoustic neuroma resection. Otolaryngol Head Neck Surg. 1995 Jul; 113(1):77–87.18. Vereeck L, Wuyts FL, Truijen S, De Valck C, Van de Heyning PH. The effect of early customized vestibular rehabilita-tion on balance after acoustic neuroma resection. Clin Rehabil. 2008 Aug;22(8): 698–713.19. Shepard NT, Telian SA. Programmatic vestibular rehabilitation. Otolaryngol Head Neck Surg. 1995 Jan;112(1):173–82.20. Jacobson GP, Newman CW. The devel-opment of the Dizziness Handicap Inventory. Arch Otolaryngol Head Neck Surg. 1990 Apr;116(4):424–7.
outcomes and where the greatest benefit can be achieved.
Abbreviations list CINAHL, Cumulative Index to Nursing and Allied Health Literature; PEDro, Physiotherapy Evidence Database.
AcknowledgementSteven M McPhail was supported by the National Health and Medical Research Council Early Career Award.
References1. Tufarelli D, Meli A, Labini FS, Badaracco C, De Angelis E, Alesii A, et al. Balance im-pairment after acoustic neuroma surgery. Otol Neurotol. 2007 Sep;28(6):814–21.2. Lynn SG, Driscoll CL, Harner SG, Beatty CW, Atkinson EJ. Assessment of dysequi-librium after acoustic neuroma removal. Am J Otol. 1999 Jul;20(4):484–94.3. Kane NM, Kazanas S, Maw AR, Coakham HB, Torrens MJ, Morgan MH, et al. Functional outcome in patients after exci-sion of extracanalicular acoustic neuro-mas using the suboccipital approach. Ann R Coll Surg Engl. 1995 May;77(3): 210–6.4. El-Kashlan HK, Shepard NT, Arts HA, Telian SA. Disability from vestibular symptoms after acoustic neuroma resec-tion. Am J Otol. 1998 Jan;19(1):104–11.5. Hirvonen TP, Aalto H, Pyykkö I. Decreased vestibulo-ocular reflex gain of vestibular schwannoma patients. Auris Nasus Larynx. 2000 Jan;27(1):23–6.6. Choy NL, Johnson N, Treleaven J, Jull G, Panizza B, Brown-Rothwell D. Balance, mobility and gaze stability deficits re-main following surgical removal of ves-tibular schwannoma (acoustic neuroma): an observational study. Aust J Physiother. 2006;52(3):211–6.7. Hillier SL, Hollohan V. Vestibular reha-bilitation for unilateral peripheral vestib-ular dysfunction. Cochrane Database Syst Rev. 2007 Oct;(4):CD005397.8. Herdman S. ‘Vestibular rehabilitation’. Physical therapy diagnosis for vestibular disorders 3rd ed. Philadelphia: FA Davis Company; 2000. pp228–308.9. de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. 2009;55(2): 129–33.
of a vestibular rehabilitation protocol in clinical settings, compliance levels are likely to be relevant to clinical practice. Such a study could report the level of compliance and conduct analyses on an intention-to-treat ba-sis, as well as reporting sub-group analyses for patients who did adhere to the protocol. This would be valu-able for informing clinical practice and for the development of interven-tions to promote optimal adherence to vestibular rehabilitation protocols in clinical settings.
Future researchThere are several key priorities for future research. Randomized-controlled trials with larger sample sizes and more rigorous methodolo-gies are needed to investigate the ef-fects of each element of vestibular rehabilitation, as well as when used in combination with comprehensive vestibular rehabilitation program with patients following resection of an acoustic neuroma. Conducting clinical trials with factorial designs offers a useful approach to make these comparisons. Elements of ves-tibular rehabilitation worthy of in-vestigation on their own or in combination include adaptation ex-ercises, habituation exercises, bal-ance training and gait retraining. Investigation of intervention param-eters such as the timing and duration of interventions as well as the mini-mum and optimal ‘dosage’ require-ment to achieve effectiveness should be considered. The effects of educa-tion and social reinforcement also re-quire further investigation. Finally, the development of a clinical predic-tion rule(s) from empirical data would be useful to aid clinical staff in identifying those patients at risk of adverse outcomes and those who are likely to benefit from vestibular reha-bilitation. This would allow limited healthcare resources for this clinical population to be focused on those patient subgroups at risk of poor

Page 13 of 13
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.Al
l aut
hors
con
trib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, as
wel
l as r
ead
and
appr
oved
the
final
man
uscr
ipt.
All a
utho
rs a
bide
by
the
Asso
ciati
on fo
r Med
ical
Eth
ics (
AME)
eth
ical
rule
s of d
isclo
sure
.
For citation purposes: Passier L, Doherty D, Smith J, McPhail SM. Vestibular rehabilitation following the removal of an acoustic neuroma: a systematic review of randomized trials. Head Neck Oncol. 2012 Sep 9;4(2):59.
Copyright © 2012 OA Publishing London
Review
Appendix 1 Search syntaxesDatabase Search syntaxCochrane Acoustic neuroma or vestibular schwannoma or acoustic schwannoma or acoustic neurilemoma or acoustic
neurinomaPubMed (acoustic neuroma OR vestibular schwannoma OR acoustic neurinoma OR acoustic neurilemoma OR acoustic
neurilemmoma OR acoustic schwannoma) AND (physiotherapy OR physical therapy OR rehabilitation OR adaptation OR habituation OR balance OR exercise OR gaze stability)
Limits: Humans, All Adult: 19+ yearsEmbase (acoustic neuroma.mp. or exp acoustic neurinoma/) or (exp acoustic neurinoma/ or exp neurilemoma/ or
exp vestibular schwannoma/ or exp neuroma/) and ([physiotherapy.mp. or PHYSIOTHERAPY/] or [physical therapy.mp.]) or ([rehabilitation or adaptation or habituation or gaze stability or balance or exercise].mp. [mp=title, abstract, subject headings, heading word, drug trade name, original title, device manufacturer, drug manufacturer])
limit to (human and [adult <18 to 64 years> or aged <65+ years>])CINAHL ([MH Neuroma, Acoustic+] and [acoustic neuroma or acoustic schwannoma or acoustic neurinoma or acoustic
neurilemoma or acoustic neurilemmoma or vestibular schwannoma]) and ([MH Physical Therapy+] or [physical therapy or physiotherapy or rehabilitation or adaptation or habituation or gaze stability or balance or exercise])
Limit: Human; Age Groups: All AdultAUSThealth (‘acoustic neuroma’ or ‘vestibular schwannoma’ or ‘acoustic neurinoma’ or ‘acoustic neurilemoma’ or
‘acoustic neurilemomma’ or ‘acoustic schwannoma’) and (physiotherapy or ‘physical therapy’) or rehabilitation or exercise or ‘gaze stability’ or adaptation or habituation or balance)