Embed Size (px)
Citation preview

Vertical & horizontal strabismus of uncertain cause
OMCFumitaka Nonaka

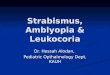
Case 1
• 14yo Female• RE drifting upwards intermittently for some years, no
diplopia• CT: D+N XT with RH• RE poorly reacting to direct light• Other examinations: unremarkable• POH, PMH: nil• CT brain & orbit: normal (not viewed)• TFT: normal


RXT RH
RIR-
RMR-

On Examination
VA-0.50 = 6/8 -0.50 = 6/6
Pupil: R>L
12ΔXT RH16Δ
30ΔXT’ RH’12Δ
Distance
Near
-1-3

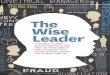
MRI
RMR
RIR LIR
LMR
RMR
RIR LIR
LMR

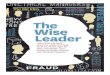
Palsy of the inferior divisionof the third nerve
Superior division
Inferior division
Levator
SR
MR
IR
IO
Sphincter pupillae
Ciliary muscle

Case 2
• 16yo Male• Re: worsening head tilt to right• Noticed LE Amblyopia since 2yo• PMH: Developmental delay• PFH: sister with squint

L Pseudo ptosis
Large LXT, L hypo
Dominant RE can’t depressespecially in R-gaze

On Examination
s gls6/9 6/28
Pupil: ?some asymmetry reaction L>R
25ΔLXT LHypo 25Δ
Distance
RE can’t depressespecially in R-gaze
L Pseudo ptosis

CT

Pre-op Post-op
BSV +
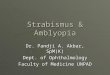
Knapp’s surgical procedure
Treatment Dr Kushner reported the efficacy of “Knapp’s surgical procedure” Simultaneous transposition of
SR toward the insertion of MRLR toward the insertion of IR+ Tenotomy of SO tendon
All 5 patients were free from diplopia in primary position (follow up ranged from 3 to 10 years after surgery)
Surgical Treatment of Paralysis of the Inferior Division of the Oculomotor Nerve. J Kushner, Arch Ophthalmol. 1999;117:485-489

Two cases of congenital inferior division oculomotor palsy were presented.
This is an important diagnosis to make. It has a
very specific & usually successful treatment.