Embed Size (px)
Citation preview

ARTICLE IN PRESS
Applied Radiation and Isotopes 66 (2008) 1930– 1938
Contents lists available at ScienceDirect
Applied Radiation and Isotopes
0969-80
doi:10.1
� Corr
E-m
journal homepage: www.elsevier.com/locate/apradiso
Verification of dose delivery for a prostate sIMRT treatmentusing a SLIC– EPID
Mohammad Mohammadi a,�, Eva Bezak b,c, Paul Reich b,c
a Department of Medical Physics, Faculty of Medicine, Hamadan University of Medical Sciences, Hamadan, Iranb Department of Medical Physics, Royal Adelaide Hospital, Adelaide, SA 5000, Australiac Department of Physics and Mathematical Physics, The University of Adelaide, Adelaide, SA 5000, Australia
a r t i c l e i n f o
Article history:
Received 6 January 2008
Received in revised form
13 March 2008
Accepted 30 April 2008
Keywords:
Dose verification
SLIC–EPID
Segmented IMRT
Transmitted dose
43/$ - see front matter & 2008 Elsevier Ltd. A
016/j.apradiso.2008.04.024
esponding author. Tel.: +98 8118276296 8; fa
ail address: [email protected] (M. Mo
a b s t r a c t
The current work focuses on the verification of transmitted dose maps, measured using a scanning
liquid ionization chamber–electronic portal imaging device (SLIC–EPID) for a typical step-and-shoot
prostate IMRT treatment using an anthropomorphic phantom at anterior–posterior (A–P), and several
non-zero gantry angles. The dose distributions measured using the SLIC–EPID were then compared with
those calculated in the modelled EPID for each segment/subfield and also for the corresponding total
fields using a gamma function algorithm with a distance to agreement and dose difference criteria of
2.54 mm and 3%, respectively.
& 2008 Elsevier Ltd. All rights reserved.
1. Introduction
Although all types of electronic portal imaging devices (EPIDs)including fluoroscopic, scanning liquid ionization chamber (SLIC)and amorphous silicon (a-Si) EPIDs, are primarily used to verifythe patient set up during radiation therapy courses, their use hasbeen gradually extended for dosimetric purposes, includingquality assurance (Kirby and Williams, 1995; Vieira, Dirkx et al.,2002; Yang and Xing, 2004), compensator design (Evans, Hansenet al., 1995; Curtin-Savard and Podgorsak, 1997), pre-treatmentverification (Depuydt, Van Esch et al., 2002; Van Esch, Depuydtet al., 2004) and dose delivery verification (Pasma, Dirkx et al.,1999; Steciw, Warkentin et al., 2005).
As uniform images are acquired by EPIDs for patient set upverification, additional dosimetric calibration is required. Thedosimetric calibration is mainly focused on: long-term, and short-term reproducibility of electronic portal image (EPI) pixel values(Essers, Hoogervorst et al., 1995; Louwe, Tielenburg et al., 2004),the lag of image acquisition time (Essers, Hoogervorst et al., 1995;Curtin-Savard and Podgorsak, 1999; Van Esch, Vanstraelen et al.,2001), the use of extra build-up layer (Chang, Mageras et al.,2000), conversion of EPIDs raw pixel values to dose values (Essers,Hoogervorst et al., 1995; Parsaei and El-Khatib et al., 1998; VanEsch, Vanstraelen et al., 2001), and reconstruction of radiation
ll rights reserved.
x: +98 8118276299.
hammadi).
beam horns. The latter has been reported as being the mostimportant part of a two-dimensional dosimetric calibration andcan be achieved using empirical (Essers, Boellaard et al., 1996;Parsaei and El-Khatib et al., 1998; Chang, Mageras et al., 2001),and mathematical approaches (Boellaard, van Herk et al., 1997;Pasma, Vieira et al., 2002; Steciw, Warkentin et al., 2005).
Two general methods have been developed to verify the dosedelivered to the patient, using portal dose distributions called‘‘transmitted dose maps’’. In the first approach, the transmitteddose maps are back-projected to obtain either exit dose maps i.e.the dose distributions in the exit side of patient where electronicequilibrium is achieved, or mid-plane dose maps. For instance, amethod was introduced to estimate the on-axis exit dose of apatient performing SRI-100 fluoroscopic EPID measurements(Kirby and Williams, 1993). This method has an inherentlimitation of accuracy, especially for intensity modulated beamsbecause of use of an on-axis beam. A kernel-based convolutionmodel was also developed to reconstruct exit dose from thetransmitted dose values measured using the SLIC–EPID. Theaccuracy of this model was reported to be within 2% and 2.5%for homogeneous and inhomogeneous phantoms, respectively(Boellaard, van Herk et al., 1997). In another study, the back-projection of transmitted dose values obtained from EPIs wasperformed through the planning computerized tomography (CT)to yield a primary fluence distribution inside the patient. The dosedistribution was then convolved with dose deposition kernels tocalculate a mid-plane dose map. The results were found to be inagreement with radiographic film and thermo-luminescence

ARTICLE IN PRESS
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–1938 1931
dosimeter (TLD) measurements (within 2%) for a pelvic region ofan anthropomorphic phantom (Hansen, Evans et al., 1996).
Transmitted dose maps, measured using two-dimensionalportal dosimeters, have been compared with the correspondingcalculated dose maps, using treatment planning systems (TPSs).Due to the limitation of TPSs to calculate the transmitted dosebeyond the patient CT data, several methods have been proposedto develop calculated dose maps. A method called ‘‘delta volume’’was introduced (Wong, Slessinger et al., 1990) and the calculateddose maps were compared with radiographic film and TLDmeasurements. Arguing that the ‘‘delta volume’’ method is notwell suited for large air gaps, (i.e. distances between phantom/patient and portal imager), a novel approach was introducedbased on convolution/superposition algorithm. The aim was topredict the transmitted dose distributions through an ‘‘extendedphantom’’ including a phantom, an air gap (up to 22 cm) and amodelled EPID (McNutt, Mackie et al., 1996). The calculated dosemaps were generally found to be in agreement with SLIC–EPIDmeasurements within 4%. For larger air gaps, from 30 to 50 cm, analgorithm was developed to calculate the dose maps for openfields (Pasma, Heijmen et al., 1998; Reich, Bezak et al., 2006) andwedged fields (Pasma, Vieira et al., 2002). A good agreement(approximately 1%) has been reported for regions excluding thepenumbra for open, wedged and smoothly modulated IMRT fields,and a large deviation, greater than 10%, was reported for the use ofthis algorithm in the penumbra regions (Pasma, Dirkx et al., 1999).The transmitted dose maps calculated using a full Monte Carlosimulation technique were also compared with those measuredusing the a-Si EPID (Siebers, Kim et al., 2004). A Monte Carlosimulation using BEAMnrc/DOSXYZnrc code was also developedto calculate dose maps at oblique gantry angles (Chin, Spezi et al.,2003). Furthermore, several new approaches have been recentlydeveloped for three-dimensional dose verification using EPIDs(Renner, Sarfaraz et al., 2003; Ansbacher, 2006; van Elmpt, Nijstenet al., 2006).
Although several studies have been reported to investigateeither conformal radiotherapy (CRT) or IMRT dose verificationusing EPIDs (Chang, Mageras et al., 2000; Fielding, Evans et al.,2002; Vieira, Dirkx et al., 2002; Zeidan, Li et al., 2004), majority ofstudies have been performed for either primary radiation fluenceor homogeneous attenuators in anterior–posterior (A–P) direc-tions only. Only in one case, performed by Kroonwijk et al. (1998),an in-vivo dose verification based on comparison of predicted andmeasured portal dose images for 10 prostate patients for lateraland A–P beams was done (1998). This however, does not readilyapply to CRT and IMRT treatments where multiple gantry anglesother than zero are generally used. These observations motivatedus to investigate the transmitted dose distributions, measuredusing the SLIC–EPID, for a typical step-and-shoot prostate IMRTapplied to an anthropomorphic phantom using A–P direction aswell as all other typically used oblique gantry angles. EPIsacquired for each subfield in five radiation fields were convertedinto the transmitted dose maps using an appropriate calibrationmethod. The results of these measurements were then comparedwith the transmitted dose maps, calculated by the Pinnacle3 TPS,using the gamma function algorithm.
2. Materials and methods
2.1. Materials
All transmitted dose maps were measured using a SLIC–EPID(LC250, PortalVision MK2, Varian Medical System, Palo Alto, CA)incorporated in a Varian 600CD linac, equipped with an 80-leafstandard MLC (Varian Medical Systems, Palo Alto, CA). The linac
produces a standard 6 MV photon beam with a range of repetitionrates from 100 to 600 MU/min. The detector matrix of theSLIC–EPID has a sensitive area of 32.5�32.5 cm2. It contains256�256 liquid ionization chambers with the volume of1.27�1.27�1 mm3. All EPIs were acquired in fast read-out andfull resolution mode as routinely used for image acquisition in ourclinic. In addition, the accuracy of this setting has been reported tobe better than other available options (Chang, Mageras et al.,2003). A commercial Pinnacle3 TPS, version 6-2b (ADAC Inc.PHILIPS Medical System, Milpitas, CA) was also used to calculatethe transmitted dose delivered to the EPID sensitive layer. The TPScalculates the dose using collapsed-cone convolution superposi-tion algorithm (Mackie, Scrimger et al., 1985). An anthropo-morphic Rando phantom, containing real bony anatomy inside asolid water material was used to measure and to calculate thedose transmitted through the phantom. All image processing anddose distribution comparison procedures were performed usingin-house codes written in MATLAB 7 (MathWorks Inc, Natick,MA).
2.2. Methods
EPIs acquired using repetition rate of 300 MU/min, with oneMU corresponding to a calibrated dose delivery of 1 cGy under thereference conditions (SSD ¼ 100 cm, for a 10�10 cm2 field size atthe depth of dmax). Due to the EPI short acquisition time (0.0015 s/two rows) and in order to reduce statistical fluctuations of EPIpixel values, each EPI used in the current study was to determinethe average of three consecutive acquired EPIs with pixel valuestandard deviation of less than 1% on the central part of radiationfield.
2.2.1. SLIC–EPID calibration for dosimetric purposes
For dosimetric purposes, a comprehensive calibration ofSLIC–EPID is required including: evaluation of EPIs reproducibility,the evaluation of EPI pixel values with acquisition time lag, theuse of an extra build-up layer, conversion of EPI pixel values todose, correction of EPID dose values in off-axis regions. These havebeen discussed in depth elsewhere (Mohammadi and Bezak, 2005,2006).
2.2.2. SLIC–EPID response correction for oblique beams
In the current work, a systematic variation in EPI pixel valueswith gantry angle observed for SLIC–EPIDs called ‘‘bulging effect’’(a correction algorithm developed by Van Esch et al. (2001)) wasused to remove this effect from the measured EPIs.
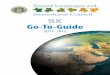
Typical crossplane profiles extracted from EPIs acquired at 01,901, 1801, and 2701 gantry angles are illustrated in Fig. 1(a). Asystematic variation of EPI pixel values was observed for a rangeof gantry positions. The maximum differences in SLIC–EPIDresponse (compared to the response at 01) were found to be atgantry positions 901 and 2701. For these angles, the observedvariation in EPI pixel values corresponds to the measuredtransmitted dose variation in the off-axis regions by 3%.
Typical line profiles of an acquired relative primary fluencemap before and after the correction for the bulging effect for a 901gantry position are shown in Fig. 1(b). In addition, a comparison ofrelative dose difference profiles before and after the correctionwith a corresponding profile measured at 01 is also displayed. Atthe edge of corresponding profiles, the difference was found to bearound 3% compared to the profiles acquired at 01. However, itwas found that while the proposed method corrects all EPIsacquired at all non-zero gantry angles, several inconsistencies inthe penumbra region were observed between line profilescorrected and those measured at 01 gantry position.

ARTICLE IN PRESS
Fig. 1. Crossplane profiles of (a) relative dose for a range of gantry angles and (b) relative dose profiles for gantry angle of 901 before and after the correction, and the
corresponding relative dose difference compared with that acquired at 01 of gantry rotation.
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–19381932
2.2.3. The transmitted dose maps measured using SLIC–EPID
Typical MLC fields defined for prostate sIMRT were applied.The prostate treatment, used in this study, consisted of five fieldsdelivered at gantry angles of 01, 601, 1201, 2401 and 3001. Eachfield consisted of several segments/subfields (around 9–12subfields per field). An anthropomorphic phantom was used forprostate sIMRT delivery and EPI acquisition. EPIs were acquiredfor each delivered subfield and converted to relative-transmitteddose maps (Mohammadi and Bezak, 2006).
2.2.4. The dose map calculated using Pinnacle3 TPS
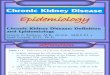
In order to calculate the corresponding transmitted dose maps,measured using a SLIC–EPID, the anthropomorphic phantom wasinitially scanned using a CT simulator (AcQSim CT, Philips MedicalSystem, Cleveland, OH) with a 3 mm slice thickness and a matrixsize of 512�512 pixels. The images were then extended to1024�1024 pixels by adding rows of pixels with pixel valuescorresponding to air CT numbers around the acquired CT image(see Fig. 2(a)). For non-zero gantry angles, in order to extract thecalculated transmitted dose distributions easily through thecalculated dose grid matrix, the original CT images were rotatedin the opposite direction to the gantry rotation (see Fig. 2(b)). TheEPID was modelled as a 4�30�30 cm3 uniform thin slab withdensity of 1.0 g/cm3 positioned perpendicularly to the centralbeam axis, so that the upper edge of modelled slab was placed38.5 cm from the isocentre. The modified images were thentransferred via DICOM to the Pinnacle3 TPS. The CT couch wasremoved by converting the corresponding CT data into air CTnumbers (�1000). A corresponding weighting factor, for 2 Gy dose
per fraction delivered to an isocentre point located inside theanthropomorphic phantom, was assigned to each MLC subfield.All transmitted dose distribution calculations were performedusing the collapsed-cone superposition/convolution dose calcula-tion algorithm. A three-dimensional dose grid consisting of voxelsof 0.175�0.175�0.175 mm3 was defined to calculate the dosedistributions. Due to the discrepancy between the rounded leafend of Varian MLCs and the straight leaf end simulated in theavailable version of Pinnacle3 TPS (Version 6.2b) (Cadman,Bassalow et al., 2002), the dosimetric offset values were foundto be 0.6 mm and manually applied for all MLC positions. Themaximum dose deposited in the modelled EPID was determinedfor each subfield and a two-dimensional transmitted dosedistribution was then extracted at the depth of maximum dosein the modelled EPID layer. Since the quality of radiation beamvaries with the patient thickness, the position of the dosedistribution in the modelled EPID to reach electronic equilibriumshould also be considered. The transmitted dose map matriceswere rescaled to pixel size corresponding to those measured withSLIC–EPID using bilinear interpolation, which was found to be thebest option in MATLAB software for image re-scaling purposes.
2.2.4.1. Evaluation of CT image quality. Due to the digital imagepixilation, the rotation of original CT images around the central pointof the image (in the opposite direction to the gantry rotation) causessome variation of the CT image pixel values. Significant variations inoriginal CT image pixel values could lead to a significant discrepancyin TPSs calculated dose compared to the corresponding measure-ments. In order to investigate this, the CT pixel values before and after

ARTICLE IN PRESS
Fig. 2. Typical extended CT image (a) in A–P direction and (b) at 601 gantry angle position. The position of modelled EPID is shown for the both cases.
Variation of CT pixel values with the rotation of CT image
-1500
-500
500
-25 -15 -5 5 15 25Distance from central point of CT image (cm)
CT
pixe
l val
ues
-400
-300
-200
-100
0
100
200
300
400
PV d
iffer
ence
Original CT Rotated CT Original CT - Rotated CT
Fig. 3. A sample line profile demonstrating the variation of CT image pixel values with the rotation of image for 451 and the corresponding CT number difference.
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–1938 1933
image rotation were compared. Fig. 3 shows the line profiles of theoriginal CT image pixel values and after a 451 rotation. The differencesin the corresponding CT pixel values are also shown on the secondaryy axis. From algorithms available in MATLAB software, the bilinearinterpolation algorithm was found to be the best suited for re-construction of image information during rotation, since the variationbetween the corresponding pixel values was the smallest. The max-imum and average percentage differences in pixel values for a whole2D-CT image before and after rotation by 451 was found to be 11.6%and 0.19%, respectively.
2.2.5. The comparison of measured and calculated transmitted dose
maps
The agreement between measured and calculated transmitteddose maps was assessed for each subfield and for each total field ba-sed on the gamma function algorithm developed by Low et al. (1998)with the DTA and DDmax criteria of 2.54 mm and 3%, respectively.
3. Results
3.1. Evaluation of transmitted dose distributions obtained from EPID
and TPS
The inplane and crossplane profiles of transmitted dosedistributions measured using SLIC–EPID and those calculated using
TPS, as well as the corresponding relative dose difference and thegamma index profiles for all total fields are shown in Fig. 4. Whendisregarding penumbra region of the total field, the gamma valuesnever exceeded 1 i.e. the two dose maps were the same within thespecified criteria for the A–P direction. In contrast, for non-zerogantry positions, several discrepancies were observed between themeasured and calculated crossplane profiles.
The relative two-dimensional transmitted dose distributionsmeasured using a SLIC–EPID and those calculated by a Pinnacle3
TPS and the corresponding gamma maps with cut-off percentagedose of 50% for all accumulated fields are shown in Fig. 5. DTA andDDmax criteria of 2.54 mm and 3% of central axis dose, respectively,were generally used for all cases. Agreement (gamma index lessthan 1) of 90% or more was found for measured and calculatedtransmitted dose profiles in the A–P direction. For fields deliveredat non-zero gantry angles, some differences were observed due tothe presence of the treatment couch edge, causing moreattenuation in the profiles measured by EPID.
The details of agreement between measured and calculatedtransmitted dose distributions for each subfield and total field areshown in Table 1. Although some blurring was observed forsubfields positioned in the off-axis areas, good agreement was stillobserved. Generally, the minimum gamma scores were found tobe related to the peripheral subfields. The maximum, minimumand average gamma scores for all subfields were found to be96.3%, 70.8% and 87.4%, respectively.

ARTICLE IN PRESS
Crossplane profiles obtained from EPID & Pinnacle3 for gantry angle of 0°
-10
30
70
110
-8 -6 -4 -2 0 2 4 6 8Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-1
0
1
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Inplane profiles obtained from EPID & Pinnacle3 for gantry angle of 0°
-10
30
70
110
-10 -8 -6 -4 -2 0 2 4 6 8 10
Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-1
0
1
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Crossplane profiles obtained from EPID & Pinnacle3 for gantry angle of 60°
-20
20
60
100
-8 -6 -4 -2 0 2 4 6 8Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-1
0
1
2
3
4
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Inplane profiles obtained from EPID & Pinnacle3 for gantry angleof 60°
-20
20
60
100
-10 -8 -6 -4 -2 0 2 4 6 8 10
Distance from the Central axis (cm)R
elat
ive
dose
(%)
-1
0
1
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Crossplane profiles obtained from EPID & Pinnacle3for gantry angle of 120°
-10
30
70
110
-8 -6 -4 -2 0 2 4 6 8
Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-1
0
1
2
3
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Inplane profiles obtained from EPID & Pinnacle3 for gantry angle of 120°
-10
30
70
-8 -6 -4 -2 0 2 4 6 8Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-0.5
0
0.5
1
1.5
2
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Crossplane profiles obtained from EPID & Pinnacle3for gantryangle of 240°
-10
30
70
110
-8 -6 -4 -2 0 2 4 6 8Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-0.5
0
0.5
1
1.5
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Inplane profiles obtained from EPID & Pinnacle3 for gantry angle of 240°
-10
30
70
-10 -8 -6 -4 -2 0 2 4 6 8 10
Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-0.5
0
0.5
1
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Crossplane profiles obtained from EPID & Pinnacle3for gantryangle of 300°
-10
30
70
-8 -6 -4 -2 0 2 4 6 8
Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-0.5
0.5
1.5
2.5
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Inplane profiles obtained from EPID & Pinnacle3 for gantry angle of 300°
-10
30
70
-10 -8 -6 -4 -2 0 2 4 6 8 10Distance from the Central axis (cm)
Rel
ativ
e do
se (%
)
-0.5
0.5
1.5
Gam
ma
valu
e
EPID PINNACLE RDD Gamma
Fig. 4. Crossplane and inplane relative transmitted dose profiles measured and calculated using SLIC–EPID and Pinnacle3 TPS and the corresponding gamma and relative
dose difference (RDD) profiles of a prostate field for the A–P direction (a&b-1) and gantry angles of 601 (a&b-2), 1201 (a&b-3), 2401 (a&b-4) and 3001 (a&b-5). The DTA and
DDmax criteria of 2.54 mm and 3%, respectively, have been used.
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–19381934

ARTICLE IN PRESS
Fig. 5. The relative transmitted dose maps (a) measured using a SLIC–EPID, (b) calculated using a Pinnacle3 TPS and (c) the corresponding gamma maps for a prostate IMRT
field for 01, 601, 1201, 2401, and 3001 with cut-off percentage dose of 50%. The DTA and DDmax were selected 2.54 mm and 3% of the dose at CAX.
Table 1The agreement percentages (total gamma scores) between relative transmitted
dose maps measured using a SLIC–EPID and those calculated using a Pinnacle3 TPS.
The DTA and DDmax were 2.54% and 3%, respectively
Agreement percentage between subfields and total field of sIMRT fields
Field Subfield Total field
1 2 3 4 5 6 7 8 9 10 11 12
A–P 83.3 93.8 95.9 93.3 90.3 91.1 95.4 94.9 95.0 93.9 93.4 81.7 96.3
60.01 87.2 91.0 92.5 88.2 87.7 85.8 86.9 86.6 75.0 — — — 74.5
120.01 81.4 70.8 83.5 80.5 81.3 80.2 80.9 85.4 85.6 85.4 — — 80.4
240.01 86.1 92.7 90.5 89.7 89.1 89.1 87.8 89.1 94.9 94.9 87.7 — 82.0
300.01 87.5 94.8 88.6 87.1 87.7 89.1 89.9 89.7 86.3 85.1 — — 87.3
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–1938 1935
4. Discussion
4.1. Transmitted dose measured using a SLIC– EPID
4.1.1. SLIC–EPID calibration for dosimetric purposes
The procedure of SLIC–EPI conversion to the transmitted dosemaps has been comprehensively discussed elsewhere (Moham-madi and Bezak, 2006). The calibration method requires a simpleset-up and processing and can be performed relatively quickly andaccurately compared to empirical approaches reported in theliterature (Parsaei, El-Khatib et al., 1998; Chang, Mageras et al.,2001). It can also be performed in clinics more easily compared tothe use of kernel-based convolution algorithms due to their
dependency on EPID type (Warkentin, Steciw et al., 2003; Steciw,Warkentin et al., 2005) and linac output (beam energy and the useof accessories) (Pasma, Heijmen et al., 1998; Pasma, Vieira et al.,2002). The proposed method can be easily expanded to other EPIDtypes. In addition, EDR2 film calibration is easy to set up andmeasure compared to other techniques e.g. ionization chamberscanning in a water tank. The agreement between transmitteddose maps measured using SLIC–EPID using developed calibrationmethod with other measurements and TPS calculations in thepresence of homogenous attenuators and large inhomogeneitiesfor conventional beams has been reported to be within 1% and2.5%, respectively (Mohammadi and Bezak, 2007).
4.1.2. SLIC–EPID response for oblique beams
For oblique and lateral beam deliveries, rotation of the linacgantry is necessary. Ideally, the radiation fluence incident on theEPID should be invariant with gantry angle if attenuation andscattering conditions are kept constant. In practice, however, theacquired SLIC–EPIs vary significantly with gantry angles. Thevariation of SLIC–EPID response with gantry angle depends onseveral factors. Firstly, it is caused by the variation in response ofthe EPID detector layer as the liquid sandwiching by the cassette isnot completely rigid and the two plates of the ionization chamberflex as the gantry rotates. This causes a non-uniform thickness ofthe liquid film across the EPID matrix. Secondly and to a lesserextent, the variation of linac output with the variation of gantryposition (within 2%) may vary the incident fluence reaching theEPID (Varian-Medical-System, 2000). Thirdly, imperfect mechan-ical rigidity of the support arm may cause vertical, longitudinal

ARTICLE IN PRESS
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–19381936
and lateral shifts of the SLIC–EPID with respect to the isocentre ofup to 1.3 cm. Finally, the variation of EPID position with floor/ceiling at the gantry angles of 01 to 1801 varies the amount ofscattered radiation reaching the EPID from surrounding materials(Chin, Lewis et al., 2004).
4.2. Transmitted dose calculated using Pinnacle3 TPS
4.2.1. The quality of CT images
In the literature, in order to calculate the transmitted dosemaps for non-zero gantry angles, it has been suggested that theEPID should be modelled perpendicular to the central axis of theradiation beam i.e. in an oblique position relative to the patient(original CT image) (McNutt, Mackie et al., 1997). Although thismethod preserves the quality of the CT images, the extraction ofrequired transmitted dose distribution is more complicatedbecause it involves many dose grid slices and the accuracy ofthe region of interest (ROI) extraction decreases due to theundulation of isodose curves which arises from pixilation of thedose grid matrix. In addition, due to the oblique position of theEPID modelled, a larger dose grid matrix is required forcalculation. Because of TPS memory limitation, this leads to largervoxel size in dose grid matrix and consequently to the decrease ofdose resolution in the ROI.
In a new approach proposed in the current study, the patient/phantom positioning during the CT image acquisition, has beenrotated in the opposite direction to the gantry rotation andconsequently the EPID is modelled in a position such that theextraction of ROI is easier and more accurate than explained in theformer method. As Fig. 3 shows, although a difference betweenrotated and un-rotated CT image pixel values can be observed,analysis of data indicates that only in 3 pixels (out of 512 pixels ofa line profile) the PV differences before after rotation were greaterthan 3%. Evaluation of the whole matrices for rotated and un-rotated CT images indicated that less than 0.5% of all pixel valueshave been changed by more than 3%. This shows that the imagedegradation during rotation can be neglected and the rotation ofCT images does not affect the accuracy of dose calculationsignificantly.
4.3. Agreement between planned and measured dose maps
Results show that the calibrated EPID can be used to verifydose delivery for sIMRT. However, the blurring of EPIs observedfor narrow peripheral subfields decreased the agreement between
Crossplane profiles of EPID dos
-10
30
70
110
-8 -6 -4 -2Distance from th
Rel
ativ
e do
se a
nddo
se d
iffer
ence
(%)
No Couch With Couch
Fig. 6. The crossplane profiles of transmitted fluence maps with and without treatment
2.5 mm criteria.
measured and calculated dose maps. Further investigation isrequired to identify the reason EPIs’ blur as well as to findmethods that prevent blurring for radiation fields smaller than3 cm2.
The size of CT images limited the number of TPSs used tocalculate transmitted dose distributions at extended distances,and subsequently a modification/enlargement was required toincrease the dose calculation volume beyond the patient. As aresult of the inclusion of the modelled EPID and the air gapbetween patient and modelled EPID, a large calculation dose gridmatrix was required which may cause several difficulties. Forexample, due to the limitation of the memory of the TPShardware, dose calculation using large dose grid, leads to theincrease of the dose voxel size and consequently to the decrease ofthe resolution of the calculated dose maps. This is one of the mainfactors affecting the accuracy of the dose calculation by any TPS.Other factors affecting the dose prediction accuracy include thesimulation of the exact shape of MLC in TPSs as well as theextraction of transmitted dose in the layer of electronic equili-brium.
As Table 1 indicates, the agreement (total gamma score)between measured and calculated transmitted dose maps for eachtotal sIMRT field is different from those achieved for relevantsubfields. This is most likely the result of the summation ofsubfields (caused by misalignment between measured andcalculated dose maps during summation to create total fieldtransmitted dose map or as a consequence of an uncertainty inselecting the exact normalization point for the both calculatedand measured transmitted dose maps).
The treatment couch presence in the beam path for obliquedose deliveries is one of the main concerns for transmitteddosimetry, due to the exit dose perturbation before reaching tothe dosimeter (Vieira, Kaatee et al., 2003). As described, the CTcouch was removed during dose calculation. In contrast, thetreatment couch was not removed during EPI acquisition. Thecrossplane profiles of two fluence maps measured with andwithout the treatment couch in the radiation beam are shown inFig. 6. This is in agreement with the couch attenuation measuredusing a fluoroscopic EPID (Vieira, Kaatee et al., 2003). Althoughthis effect can be corrected using appropriate correction techni-ques, the presence of different materials such as carbon fibre andaluminium supporting rods and particularly their position inrespect to the EPID position, the evaluation of dose attenuationand consequently it’s reconstruction requires more investigation.In addition, the use of additional corrections decreases theaccuracy and originality of measured data sets. This perturbation
e maps with and without couch
0 2 4 6 8e Central axis (cm)
0
1
2
3
4
5
Gam
ma
valu
e
RDD Gamma
couch, the corresponding relative dose difference and the gamma values with 3%/

ARTICLE IN PRESS
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–1938 1937
in dose distribution not only reduces the applicability ofportal dosimetry, but also further considerations are required forany exit dose or mid-plane dose determination using back-projection techniques (Huyskens, Van Dam et al., 1994; Boellaard,Essers et al., 1998). The use of the same couch as well as the samepatient positioning on the couch during CT scanning and EPIacquisition or removing/correcting for the couch presencethrough software processing in both cases allows to account forthis phenomenon.
Although IMRT is an increasingly popular radiotherapytechnique, the complexity of treatment requires that, moreattention should be paid to the verification of dose delivery. Theagreement between measured and calculated transmitted dosemaps with the gamma function criteria, used in the current workconfirms that SLIC–EPID after an appropriate dosimetric calibra-tion can be used to verify the dose delivery procedure for eithersegmental or total dose assessment. However, any disagreementsbetween a reference and an evaluated two-dimensional trans-mitted dose maps are not easily interpreted in terms of dosedelivery to the patient. Differences may be due to linac outputvariations and/or patient anatomy changes. The average agree-ment between calculated and measured transmitted dose mapswas found to be approximately 95% applying the gamma criteriagenerally used for clinical assessments and in the absence oftreatment couch attenuation. The presence of treatment couch inthe radiation beam path, before reaching to the EPID detectorsraises the disagreement to 15%. In addition, precautions must betaken to calibrate the EPID for dosimetric purposes. The evalua-tion of the agreement between calculated and measured trans-mitted dose maps, used in the current work, can be used todetermine the patient/phantom shift with respect to that definedduring planning procedure. Moreover, the significant change inpatient anatomy in the ROI compared with that acquired duringplanning may also be identified. Further investigation is requiredto extend this dose delivery verification technique for realpatients.
Acknowledgement
This work is supported by the Department of Medical Physics,Royal Adelaide Hospital.
References
Ansbacher, W., 2006. Three-dimensional portal image-based dose reconstructionin a virtual phantom for rapid evaluation of IMRT plans. Med. Phys. 33 (9),3369–3382.
Boellaard, R., van Herk, M., et al., 1997. A convolution model to converttransmission dose images to exit dose distributions. Med. Phys. 24 (2),189–199.
Boellaard, R., Essers, M., et al., 1998. New method to obtain the midplane doseusing in vivo dosimetry. Int. J. Radiat. Oncol. Biol. Phys. 41 (2), 465–474.
Cadman, P., Bassalow, R., et al., 2002. Dosimetric considerations for validation of asequential IMRT process with a commercial treatment planning system. Phys.Med. Biol. 47 (16), 3001–3010.
Chang, J., Mageras, G.S., et al., 2000. Relative profile and dose verification ofintensity-modulated radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 47 (1),231–240.
Chang, J., Mageras, G.S., et al., 2001. An iterative EPID calibration procedure fordosimetric verification that considers the EPID scattering factor. Med. Phys. 28(11), 2247–2257.
Chang, J., Mageras, G.S., et al., 2003. Evaluation of rapid dose map acquisition of ascanning liquid-filled ionization chamber electronic portal imaging device. Int.J. Radiat. Oncol. Biol. Phys. 55 (5), 1432–1445.
Chin, P., Spezi, W.E., et al., 2003. Monte Carlo simulation of portal dosimetry on arectilinear voxel geometry: a variable gantry angle solution. Phys. Med. Biol. 48(16), N231–N238.
Chin, P., Lewis, D., et al., 2004. Correction for dose–response variations in ascanning liquid ion chamber EPID as a function of linear gantry angle. Phys.Med. Biol. 40 (8), N93–N103.
Curtin-Savard, A., Podgorsak, E.B., 1997. An electronic portal imaging device as aphysics tool. Med. Dosimetry 22 (2), 101–105.
Curtin-Savard, A.J., Podgorsak, E.B., 1999. Verification of segmented beam deliveryusing a commercial electronic portal imaging device (EPID). Med. Phys. 26,737–742.
Depuydt, T., Van Esch, A., et al., 2002. A quantitative evaluation of IMRT dosedistribution: refinement and clinical assessment of the gamma evaluation.Radiother. Oncol. 62, 309–319.
Essers, M., Hoogervorst, B.R., et al., 1995. Dosimetric characteristics of a liquid-filled electronic portal imaging device. Int. J. Radiat. Oncol. Biol. Phys. 33 (5),1265–1272.
Essers, M., Boellaard, R., et al., 1996. Transmission dosimetry with a liquid-filled electronic portal imaging device. Int. J. Radiat. Oncol. Biol. Phys. 34,931–941.
Evans, P.M., Hansen, V.N., et al., 1995. Design of compensators forbreast radiotherapy using electronic portal imaging. Radiother. Oncol. 37 (1),43–54.
Fielding, A., Evans, P., et al., 2002. The use of electronic portal imaging toverify patient position during intensity-modulated radiotherapy de-livered by the dynamic MLC technique. Int. J. Radiat. Oncol. Biol. Phys. 54(4), 1225–1234.
Hansen, V.N., Evans, P.M., et al., 1996. The application of transit dosimetry toprecision radiotherapy. Med. Phys. 23 (5), 713–721.
Huyskens, D., Van Dam, J., et al., 1994. Midplane dose determination using in vivodose measurements in combination with portal imaging. Phys. Med. Biol. 39(6), 1089–1101.
Kirby, M.C., Williams, P.C., 1993. Measurement possibilities using an electronicportal imaging device. Radiother. Oncol. 29, 237–243.
Kirby, M.C., Williams, P.C., 1995. The use of an electronic portal imaging device forexit dosimetry and quality control measurements. Int. J. Radiat. Oncol. Biol.Phys. 31 (3), 593–603.
Kroonwijk, M., Pasma, K.L., et al., 1998. In vivo dosimetry for prostate cancerpatients using an electronic portal imaging device (EPID); demonstration ofinternal organ motion. Radiother. Oncol. 49 (2), 125–132.
Louwe, R., Tielenburg, R., et al., 2004. The stability of liquid-filled matrix ionizationchamber electronic portal imaging devices for dosimetry purposes. Med. Phys.31 (4), 819–827.
Low, D.A., Harms, W.B., et al., 1998. A technique for the quantitative evaluation ofdose distribution. Med. Phys. 25 (5), 656–661.
Mackie, T.R., Scrimger, J.W., et al., 1985. A convolution method of calculating dosefor 15 MV X-rays. Med. Phys. 12 (2), 188–196.
McNutt, T.R., Mackie, T.R., et al., 1996. Calculation of portal dose using theconvolution/superposition method. Med. Phys. 12 (4), 527–535.
McNutt, T.R., Mackie, T.R., et al., 1997. Analysis and convergence of the iterativeconvolution/superposition dose reconstruction technique for multiple treat-ment beams and tomotherapy. Med. Phys. 24 (9), 1465–1476.
Mohammadi, M., Bezak, E., 2005. The physical characteristics of a SLIC–EPID fortransmitted dosimetry. Iran. J. Radiat. Res. 2 (4), 175–183.
Mohammadi, M., Bezak, E., 2006. Two-dimensional transmitted dose measure-ments using a scanning liquid lonization chamber EPID. Phys. Med. Biol. 51(11), 2971–2985.
Mohammadi, M., Bezak, E., 2007. The use of extended dose range film fordosimetric calibration of a scanning liquid-filled ionization chamber electronicportal imaging device. J. Appl. Clin. Med. Phys. 8 (1), 69–84.
Parsaei, H., El-Khatib, E., et al., 1998. The use of an electronic portal imaging systemto measure portal dose and portal dose profiles. Med. Phys. 25 (10), 1903–1909.
Pasma, K.L., Heijmen, B.J., et al., 1998. Portal dose image (PDI) prediction fordosimetric treatment verification in radiotherapy. I. An algorithm for openbeams. Med. Phys. 25 (6), 830–840.
Pasma, K.L., Dirkx, M.L., et al., 1999. Dosimetric verification of intensity modulatedbeams produced with dynamic multileaf collimation using an electronic portalimaging device. Med. Phys. 26 (11), 2373–2378.
Pasma, K.L., Vieira, S.C., et al., 2002. Portal dose image prediction for dosimetrictreatment verification in radiotherapy. II. An algorithm for wedged beams.Med. Phys. 29 (6), 925–931.
Reich, P., Bezak, E., et al., 2006. The prediction of transmitted dose distributionsusing a 3D-treatment planning system. Australas. Phys. Eng. Sci. Med. 29 (1),18–29.
Renner, W.D., Sarfaraz, M., et al., 2003. A dose delivery verification method forconventional and intensity-modulated radiation therapy using measured fieldfluence distributions. Med. Phys. 30 (11), 2996–3005.
Siebers, J.V., Kim, J.O., et al., 2004. Monte Carlo computation of dosimetricamorphous silicon electronic portal images. Med. Phys. 31 (7), 2135–2146.
Steciw, S., Warkentin, B., et al., 2005. Three-dimensional IMRT verification with aflat-panel EPID. Med. Phys. 32 (2), 600–612.
van Elmpt, W.J., Nijsten, S.M., et al., 2006. A Monte Carlo-based three-dimensionaldose reconstruction method derived from portal dose images. Med. Phys. 33(7), 2426–2434.
Van Esch, A., Vanstraelen, B., et al., 2001. Pre-treatment dosimetric verification bymeans of a liquid-filled electronic portal imaging device during dynamicdelivery of intensity modulated treatment fields. Radiother. Oncol. 60 (2),181–190.
Van Esch, A., Depuydt, T., et al., 2004. The use of an a-Si-based EPID for routineabsolute dosimetric pre-treatment verification of dynamic IMRT fields.Radiother. Oncol. 71 (2), 223–234.
Varian-Medical-System, 2000. Portal Vision LC250 MKII. Palo Alto CA.

ARTICLE IN PRESS
M. Mohammadi et al. / Applied Radiation and Isotopes 66 (2008) 1930–19381938
Vieira, S.C., Dirkx, M.L., et al., 2002. Fast and accurate leaf verification for dynamicmultileaf collimation using an electronic portal imaging device. Med. Phys. 29(9), 2034–2040.
Vieira, S.C., Kaatee, R.S., et al., 2003. Two-dimensional measurement of photonbeam attenuation by the treatment couch and immobilization devices using anelectronic portal imaging device. Med. Phys. 30 (11), 2981–2987.
Warkentin, B., Steciw, S., et al., 2003. Dosimetric IMRT verification with a flat-panelEPID. Med. Phys. 30 (12), 3143–3155.
Wong, J.W., Slessinger, E.D., et al., 1990. Portal dose images. I: quanti-tative treatment plan verification. Int. J. Radiat. Oncol. Biol. Phys. 18 (6),1455–1463.
Yang, Y., Xing, L., 2004. Quantitative measurement of MLC leaf displacements usingan electronic portal image device. Phys. Med. Biol. 49 (8), 1521–1533.
Zeidan, O.A., Li, J.G., et al., 2004. Verification of step-and-shoot IMRT delivery usinga fast video-based electronic portal imaging device. Med. Phys. 31 (3),463–476.