Embed Size (px)
Citation preview

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 1
If you have not registered for this event, go to the Education Portal to complete your registration. ep.passy-muir.com
o You will also have an opportunity to do this after the meeting ends.
This is an “Audio Broadcast” meeting, which means that the audio signal will be sent out through your computer. A toll telephone number will also be available. Use the “Audio” section of the file menu for audio options.
C ll i t ll b (US) 1 415 655 0001o Call-in toll number (US)+1-415-655-0001o Access code: 665 311 869
The audio for this meeting is one-way, so the presenter will not be able to hear the attendees, nor will the attendees be able to hear each other.
If you have a question for the presenter, please use the Q and A (not the chat box), in the lower right of meeting window
After the webinar ends, you will have an opportunity to fill in your evaluation on the Passy-Muir Education Portal
If you have a technical issue, please call Passy-Muir at 949-833-8255, or email Daniel at [email protected]
Katy Peck, M.A., CCC-SLP, CBIS, CLE, BRS-S
Katy Peck, M.A., CCC-SLP, CBIS, CLE, BRS-S
o Disclosure:• Financial -Received a
ki f f Pspeaking fee from Passy-Muir Inc. for this presentation.
• Nonfinancial -No relevant nonfinancial relationship exists.
Passy-Muir, Inc. has developed and patented a licensed technology trademarked as the
Passy-Muir® Tracheostomy and Ventilator Swallowing and Speaking Valve. This g p gpresentation will focus primarily on the biased-closed position Passy-Muir Valve and will include little to no information on other speaking valves.
16 year old Neuromuscular
10 month old 6 year old Goldenhar
5 month old Unknown Dx
10 month old Expremie
Facial Mass
16 year old Neuromuscular
10 month old 6 year old Goldenhar
5 month old Unknown Dx
10 month old Expremie
Facial Mass

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 2
Medical History
R i t
• Worsening neuromuscular weakness• Unknown diagnosis, central hypotonia• Scoliosis
• Chronic respiratory failure/ @ 10 fRespiratory
Dysphagia
PMV History
• GT removed due to pain associated• Full oral feeds prior to admission• Unable to self feed• Regular-for-age diet
• Trach/vent @ 10 years of age• Admitted for PNA
• “Did not like the feeling”• Refused to use it
DTE MBSS PMV Therapy MBSS Discharge
Frankaspiration,
delayed swallow,and
maximum residue
Clinicals/s of
aspiration, presumed
PNA
PMV Assessment: 55 minutes
PMV and dysphagia therapy to rehearse
compensatory strategies
Safe withPMV inline
Full oral feeds
Mild oral phase dysphagia
Severe pharyngeal phase dysphagia o Maximum residue after swallow
No PMV
o Frank silent aspiration before 1st swallow puree texture and honey thick liquids
o Recommended PMV Assessment
PMV Wear-time (hours)
2
2.5
3
3.5 Diagnostic Therapyo MBSS reviewo Positiono Mode
S ti
0
0.5
1
1.5
2 o Sensory compensations Rehearsed practice
o Mendelsohn Maneuvero Supraglottic swallows
MBSS readiness/timingo ABX course completeo Independent with strategieso PMV tolerance
5/1/13 5/10/13

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 3
Initial MBSS MBSS #2
Puree & Soft Chewable
Bolus formation and
Chilled Honey-Thick: Spoon
Mild residue
Chilled Honey Thick: Med
Cup
Mild residue
PMV in-line
formation and containment
Residue
Retrograde movement
Mild residue
Adequate airway
protection
Mild residue
Adequate airway
protection
Chilled Thin: Spoon
Premature ill
Chilled Thin: Med Cup
Premature ill
Chilled Thin: Single Sips with Straw
Premature ill
PMV in-line
spillage
Adequate airway
protection
spillage
Adequate airway
protection
Mild residue UES- cued supraglottic
spillage
Adequate airway
protection
Oral intake only
AgePrognosisQOLVentilator
DependencyCognition
Controlled volume oral feeds with
supplementation
Enteral feeds
PNASurgeryPain/QOLRespiratory
sequalaeReadmissions
Voice
o Marginal improvement in intensity
Secretion Management
o Reduced endotracheal suction
Cough
o Productive

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 4
16 year old Neuromuscular
10 month old Goldenhar
5 month old Genetic Disorder
10 month old Expremie
6 year old Facial Mass
Medical History
• Chronic respiratory failure • Laryngomalacia
• Cleft palate and lip• Severe HL (microtia and anotia)• Low tone• 3.5 month NICCU course
Respiratory
Dysphagia
PMV History
• Laryngomalacia• OSA- supplemental oxygen (1.5lpm at night)• Trach at 9 months of age
• GT• Reflux• Mouthing objects
• Assessed at 9 months- recommendation to wait 6 months to allow growth of the tracheal lumen
• Primarily nonverbal, audible cry, use of ASL signs • Age appropriate cognitive functioning
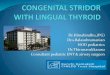
100
120
140
160
180
9 mo. 14 mo. 16 mo.
0
20
40
60
80
Trial 1 (Dx-1)
Trial 2 (Dx-1)
Trial 3 (Dx-2)
Trial 4 (Tx 1)
Trial 5 (Tx 2)
Baseline HR (bpm) Max Trial HR (bpm)
Baseline SpO2 Low Trial SpO2
Duration (min)
Assessment#2
Assessment #1
Therapy Initiated
tom
ical
olog
ica
l
nd F
ear
ehav
ior
Ana
t
Phy
sio
Anx
iety
an
Lear
ned
Be

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 5
tom
ical
olog
ica
l
nd F
ear
ehav
ior
Ana
t
Phy
sio
Anx
iety
an
Lear
ned
Be
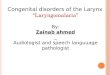
8
10
12
Duration (minutes)
Trial 1
Trial 2
Fear and crying
0
2
4
6
Tri
al 1
Tri
al 2
Tri
al 3
Tri
al 4
Tri
al 5
Tri
al 6
Tri
al 7
Trial 2
Trial 3
Trial 4
Trial 5
Trial 6
Trial 7
Increased HR and
diaphoretic
Increased secretions and
WOB
tom
ical
olog
ica
l
nd F
ear
ehav
ior
Ana
t
Phy
sio
Anx
iety
an
Lear
ned
Be
Gloves Hospital setting Poor PMV tolerance
Settingo Garden, FRC, and
hallway
Medical playo Vibrating frog inside g g
gloveso Cleanup routineo Caregiver/child PMV
placement
PMV toleranceo Lower expectationso Family education
Physiologic Changes?
Behavior?

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 6
tom
ical
olog
ica
l
nd F
ear
ehav
ior
Ana
t
Phy
sio
Anx
iety
an
Lear
ned
Be
Minimal tolerance
6 month therapy hold recommended
Isolated 7 minute trial Refusal
No expectations
Group
Fake PMV and functional
communication
Airway patency
ENT workupo Wait for MORE
tracheal lumen growth
o Downsize trach tube
Learned behaviorAnxiety
Diagnostic therapy to determine causeo Use fake PMV
o Place when in a light sleep
16 year old Neuromuscular
10 month old Goldenhar
5 month old Unknown Dx
10 month old Expremie
6 year old Facial Mass
Medical History
• Retrognathia, microglossia, & hypotonia• NICCU stay for stridor & increased WOB• Genetic and neurology w/u negative
• No significant upper airway obstruction• Epiglottis “somewhat retroflexed”Respiratory
Dysphagia
PMV History
• Enteral feeds (GT)• Receiving feeding/swallowing therapy
without use of PMV
• Epiglottis somewhat retroflexed• Normal VFs and subglottis• Suction 5-7x/day
• ENT from OSH said pt was too young• Patients mother continued to research
and requested assessment• Nonverbal
5 months 10 months
HRI follow
and OT at CHLA
ENT declinedreferral
PMV Dx: 1st sounds
Therapy and
DysphagiaAssessment
MBSS
Early communication & enteral feed
wean

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 7
Oral Motor Swallowing
R d d l
Speech/Voice
Hypotonic
Open mouth posture
Mouthing toys
Reduced oral secretion management
Enteral feeds only- learned caregivers provided tastes
Aphonic- no audible cry
PMV- Effortful vocalizations and cry
Cognition Physiology Tolerance
Excellent
Typical for developmental age
Reddish cheeks: consistent with baseline
Excellent
Cried without voice once removed
Appeared upset
5
6
7
8
Wear-time (hours)
0
1
2
3
4
5
5 months 6 months 7 months 8 months
Wear-time (hours)
Familiaro Faceso Utensilso Tastes
Feeder seato Feeder seat
Sensoryo Preferred coldo Homemade options
Presentationo Distractionso Positive feedback

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 8
Chilled Puree (Thick and
Thin)
Delayed bolus formation and
transfer
Chilled Nectar-Thick
Premature spillage
Chilled ½ Nectar Thick
Mild residue
Chilled Thin Liquid
Increased premature
spillage
PMV in-line
Reduced oral containment and pooling
Mild residue
Adequate airway
protection
Adequate airway
protection
Moderate residue
Adequate airway
protection
Mild to moderate residue
Laryngeal penetration before the swallow
Micro-aspiration before the swallow
Suzanne Abraham (2009)
50 children with trach Age Range: 2 month-
4:9 60
70
80
90
100
24/50 PMV candidateso Wear-time success
achieved• All waking hours• Daily/consistently
o Secretion management • Established within 2
weeks on average0
10
20
30
40
50
PMV candidates
Secretion Management
49%
98%
16 year old Neuromuscular
10 month old Goldenhar
5 month old Genetic Disorder
10 month old Expremie
6 year old Facial Mass
Clinical Findings
• Prematurity: 28 week expremie• Neuro: Grade III IVH (left) and Grade II (right)• Cardiac: VSD and PDA • Adrenal suppression
Respiratory
GI
• Respiratory insufficiency• Chronic lung disease• Supraglottic and arytenoid edema (GERD)• Tracheotomy and mechanical ventilation dependency• Suction every 1-2 hours
• Delayed gastric emptying• GERD• GT and JT
10 months
NonnutritiveStimulation & no sound
play
OT recommended
PMV
PMVAssessment
PMV and dysphagia
therapy
Scanttastes
Early communication
& outpatientreferrals
2025303540
Wear-time Across 10 Sessions
05
101520
Wear-time (minutes)

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 9
PMV Wear-time
Narcotic weano Unpredictable transitions in
neurobehavioral regulation
Ph i l i t
Acute Vs. Outpatient Status
1. Staff availability
2. Frequency and consistency of trials
3. Build confidenceo Physiologic parameters
o Diaphoretic
Variable secretions
Caregiver involvement
Not a candidate for MBSS
4. Initiate speech and swallow therapy
1. Underlying diagnosis
2. Generalized weakness
3. Pharmaceutical intervention(s)
4. Reduced activity
Oral Feeding/Swallowing Sensory responses
o Gago Shaking head
New oral feeder
Baseline Skill Set
o GI concernso Immature oral motor skills
Safety of swallow concernso MBSS candidacy
Caregiver involvemento Passive
stimulation/massageo Scant tastes o Food play and exploration
Hand to mouth
Massage and stretches
Oral exploration
Smell and taste
S ll
Hand exploration
Toys and tubes
Spoon
Massage
Smelle p o a o
Passive Participant => Orofacial massage and intraoral stretches. Peek-a-boo and sound play.
Guided Participation => Facilitate hand to th T til th l d t tmouth. Tactile, thermal, and gustatory
stimulation. Encourage voicing!
Overwhelmed => Monitor stress signs and facial expression
Disinterest or uncertainty => Balance opportunities
16 year old Neuromuscular
10 month old Goldenhar
5 month old Genetic Disorder
10 month old Expremie
6 year old Facial Mass
Medical History
• Large facial mass • Closure of right eye• Disfiguring right side mouth, ear, and
nose
• OSA & hypoventilation• Failure to extubate s/p biopsy
Respiratory
Dysphagia
Communication
• Full oral feeds prior to admission• Enteral feeds (NGT) s/p trach• MBSS before and after trach placement
• Failure to extubate s/p biopsy• Trach placed with ventilation dependency• Mechanical ventilation (<1 week)
• Tracheotomy POD #1• Agitation- unable to communicate• Mandarin and English

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 10
6 years old
MBSS9/24/13
Clinical BedsideAssessment
9/23/13
Clinical Swallow and SLP
Assessment (s/p trach)
10/1/13
PMV, Bedside Assessment and MBSS
10/8/13
Discharge10/14/13
All nutrition by mouth and 80%
intelligible
Speech and Communication
Oral Motor
Ventilation
Pre-Tracheotomy
Sensation
Safety
Recommendations
Pre-tracheostomy
Thin Liquid• Anterior spillage• Premature spillage• Mild Residue• Adequate airway
protection• Esophageal phase
unremarkable
Puree• Labored, delayed oral
transit• Reduced oral
containment, premature spillage
• No residue• Adequate airway
protection
Soft Chew• Timely and labored• Pocketing• Inconsistent pooling• Delayed pharyngeal
swallow• Mild residue
Functional Communication
Trach/Vent Educationo GWN videos
Pre-tracheotomy
o Anatomy/physiology
o Communication vulnerability
o Voice
o Speech
PMV Wear-time (hours)
4
5
6
7 Initial Assessment
MBSS (before tracheotomy)
0
1
2
3
4
MBSS (PMV in place)
MBSS readiness/timingo Wanted to eat
o No alternative mode
o Caregiver support

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 11
Speech and Communication
Oral Motor
Ventilation
After 1st Trach Change
Sensation
Safety
Recommendations
PMV in-line
Puree• Labored, delayed oral
transit• Reduced oral
containment, premature spillage
• No residue• Adequate airway
protection
Thin Liquid• Anterior spillage• Reduced oral
containment/ swallow timing
• Mild Residue• Laryngeal penetration
prior to swallow• Retrograde movement
Soft Chew• Timely and labored• Pocketing• Delayed pharyngeal
swallow• Minimal residue
Talk Muir- Pediatric Issue (Spring 2011). Passy-Muir News, Events and Education,
Passy-Muir, Inc. Pg 1-3.
Reason for tracheotomy Discuss placement Changes in sensation Describe voicing Describe secretion care Define diet progression Socialization
Children with Trachs: Facilitating Speech and Swallowing (December, 2010). Advance Magazine for Speech-Language Pathologists and Audiologists
[Vol. 20, Issue 25, Pg. 5].

OVERCOMING BARRIERS TO SPEAKING VALVE USE
Success Through Teamwork
12/12/13
Katy Peck, M.A., CCC‐SLP, CBIS, CLE, BRS‐SPassy‐Muir Inc. Clinical Consultant 12
Abraham, SS. Clinical and fluoroscopic issues in the management of swallowing disorders in infants and young children with tracheostomies. Perspectives on Swallowing and Swallowing Disorders. 2005;4:19-23.
Abraham, S and Wolf, E. Swallowing Physiology of Toddlers with Long Term Tracheostomies: A Preliminary Study DysphagiaLong-Term Tracheostomies: A Preliminary Study. Dysphagia. 2000;15: 206-212.
Bailey, R. Tracheostomy and Dysphagia: A complex Association. Swallowing and Swallowing Disorders (Dysphagia). 2005;14: 2-7.
Carron JD, Derkay CS, Strope GL, Nosonchuk JE, and Darrow DH. Pediatric Tracheotomies: Changing Indications and Outcomes. Laryngoscope. 2000;110: 1099-1104.
Suiter, D.M. and Easterling, C.S. (2007). Update on current treatment practice patterns for dysphagia. Topics in Geriatric Rehabilitation, 23(3): 197-210.
You will have 5 days from the time this courses ends to complete the evaluation, which is required to receive credit.o Look in your email for a reminder link, or type this into your
Internet browser’s address bar:
• ep.passy-muir.com If you are a late registrant, the meeting code is:
k2727p664o If you are already registered, you do not need to use this code
passy-muir.com/ped_candidacy