Embed Size (px)
Citation preview

J. ELECTROCARDIOLOGY 14 (2), 1981, 201-206
Ventricular Pacing in Atypical Ventricular Tachycardia BY ANDRE KEREN, M.D., DAN TZIVONI, M.D., JOSE M. GOLHMAN, M.D., PROSPER CORCOS, M.D.,
JESAIA BENHORIN, M.D. AND SHLOMO STERN, M.D.
SUMMARY Ventricular pacing was effective in controll ing recurrent bouts o f atypical ventricular
tachycardia (Torsade de Pointes), in four patients. This arrhythmia was induced by quinidine or disopyramide therapy. Isoproterenol, which is the usually recommended therapy, was ineffective in two of the patients and was considered hazardous in two others. We consider ventricular pacing as a safe and reliable method for treatment of AVT, which should be applied if isoproterenol is ineffective or contraindicated.
Atypical ventricular tachycardia (Torsade de Pointes, AVT) is a cardiac emergency which oc- curs most frequently during quinidine therapy, 1-5 but may be induced by other etiologic factors. 6-13 Since the underlying electrophysiological disor- der is a marked and uneven prolongation of ven- t r i c u l a r r epo l a r i za t i on , 3 and the assoc ia ted bradycardia prevailing in these patients fur ther alters the dispersion of repolarization, TM the con- ventional mode of therapy for ventricular tachy- cardia may not only be ineffective but even haz- ardous. 3,~5 Isoproterenol infusion is the currently accepted therapy for AVT 3,5,'6,~7 since it shortens the ventricular repolarization; however this drug is not always effective. ~,ls We report here our ex- perience with ventricular pacing as an effective t rea tment in four patients with AVT in whom isoproterenol was either ineffective or contraindi- cated. Case 1.
A. A., a 65 year old female patient, was hos- pitalized because of acute inferior wall myocar- dial infarction. On the second day of hospitaliza- tion, because of multiple atrial premature beats and periods of atrial tachycardia, disopyramide 150 mgs QID was started, resulting in the disap- pearance of all atrial arrhythmias. Twenty-four hours later a marked prolongation of the QT was noticed (0.64 sec) associated with Mobitz type II second degree atrioventricular block with a v e n -
From the Heiden Department of Cardiology, Bikur Cholim Hospital, and the Hebrew University-Hadassah Medical School Jerusalem, Israel. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. w 1734 solely to indicate this fact. Reprint requests to: Prof, Shlomo Stern, Bikur Cholim Hospi- tal, P.O.B. 492, Jerusalem, 91000, Israel
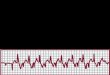
tricular rate of 48/min. Multiple ventricular pre- mature beats started, some of them ini t ia t ing recurrent episodes of AVT (Fig. 1), two of them requiring DC shock. Intravenous lignocaine was ineffective in controlling the AVT. Isoproterenol was contraindicated, because of the acute phase of myocardial infarction and therefore, ventricular pacing at a rate of 100/min was started. This caused immediate disappearance of all ventricu- lar arrhythmias . Pacing was continued with a rate of 80/min for another 36 hours and the elec- trode was removed after disappearance of the at- r ioventricular block and the re turn of the QT interval to normal. The patient left the hospital 14 days later, without recurrence of any rhy thm disturbances. Case 2.
M. M., an 84 year old woman with a long his- tory of hypertension, was hospitalized because of chest pain associated wi th t r ans i en t ST-T changes in the anterior precordial ECG leads. Her blood pressure on admission was 210/110 mg Hg, the pulse was 80/min with multiple VPBs: Due to the persistence of the VPBs even after the dis- appearance of chest pain and ischemic ST-T changes, quinidine was started. Two hours after a single dose of 0.2 gr of quinidine sulfate she lost consciousness in the emergency room. In the ECG, third degree atrioventricular block was re- corded with a junction escape rhythm, and the width of the QRS was 0.08 sec. The ventricular rate was 38/minute, with a marked prolongation of QT interval, to 0.64 sec. Multiple VPBs became more frequent and after about 15 minutes AVT started. Three of the episodes lasted more than 10 seconds and led to loss of consciousness requiring a DC conversion to sinus rhythm. Isoproterenol was contraindicated, because of the excessive hypertension. A pervenous temporary electrode was immediately introduced into the right ventri-
201

202 KEREN ET AL
Fig. 1. An example of an AVT episode which terminated spontaneously. (The two panels are continuous). Second degree AV block is present before and after the AVT.
cle and pac ing was s t a r t e d a t a r a t e of 90 /min which p r e v e n t e d r ecu r rence of all a r r h y t h m i a s (Fig. 2). Pac ing was con t inued a t a r a t e of 75 /min for 48 hour s un t i l the d i s a p p e a r a n c e of the AV block and the r e t u r n of the QT to normal . There - a f t e r the p a t i e n t was t r e a t e d w i th isosorbide di- n i t r a t e and be ta -b lockers and was re leased f rom
hospi ta l seven days l a t e r w i thou t r ecur rence of a r r h y t h m i a s . Case 3.
C. I., a 75 y e a r old m a l e pa t i en t , was hospi ta l - ized because of p n e u m o n i a . He had no prev ious h i s to ry of h e a r t disease, or a n y chronic i l lnesses. The E C G on admiss ion showed s inus r h y t h m a t a
Fig. 2. Complete atrio-ventricular block, with junction escape rhythm on left side of upper panel. Two ineffective pacing spikes follow, during the at tempt to place electrode in the right ventricle. An episode of AVT recurs, termi- nated by uniform ventricular tachycardia (5 beats). The ventricular pacing captures thereafter and prevents recur- rence of AVT. (The two panels are continuous).
J. ELECTROCARDIOLOGY, VOL. 14, NO. 2, 1981

PACING FOR ATYPICAL VENTRICULAR TACHYCARDIA 203
i
Fig. 3. Panel A. A short episode of AVT. Note the marked prolongation of the QT interval and the ventricular premature beats. Panel B. In the same patient atrial pacing at a rate of 105/min prevented recurrence of AVT. Panel C. In the same patient subsequent ventricular pacing at a rate of 78/min prevented recurrence of AVT.
rate of 80/min with RBBB and normal QT inter- val. On the third day of hospitalization, while the patient was on penicillin therapy, atrial fibrilla- tion with a ventricular rate of 130/min developed. Digoxin 0.25 mg was given intravenously and the n e x t d a y q u i n i d i n e 1.2 g r / d a y was added . Twenty-four hours la ter the pa t ien t lost con- sciousness. The ECG revealed sinus rhythm of 54/min, marked prolongation oi ~ QT interval (0.60 sec) VPBs with a long coupling interval, and re- current bouts of AVT.
Lidocaine, given intravenously was ineffective in controlling the arrhythmia, and during its ad- ministrat ion more than 50 episodes of prolonged VT and VF associated with loss of consciousness occurred, requiring the use of DC shock to restore sinus rhythm. More than 100 other episodes ter- minated spontaneously. Adminis t ra t ion of iso- proterenol up to 5/~g/min increased the heart rate to 90-115/min and decreased the number of AVTs so tha t during the next 30 minutes the patient
required only two DC shocks. At this stage tem- porary r ight atrial pacing was started at a rate of 105/min which abolished the ar rhythmia . The isoproterenol infusion was stopped. However, dur- ing episodes of failure to pace, the AVT recurred. Therefore, the electrode was advanced to the right ventricle and pacing was continued with a rate of 70/min for 24 hours. The electrode was removed after an additional 24 hours, when the QT inter- val returned to normal. The patient left the hospi- tal six days later in sinus rhy thm with a normal QT interval, receiving disopyramide t rea tment of 300 mg/day. Case 4.
Z. Z., a 67 year old woman, was admitted to the hospital because of recent onset of atrial fibrilla- tion. She had a history of rheumatic heart disease with moderate mitral stenosis. The patient was treated with quinidine 0.3 g QID for 24 hours and reverted to sinus rhythm only after electric car- dioversion. The next day extreme sinus bradycar-
J. ELECTROCARDIOLOGY, VOL. 14, NO. 2, 1981

204 KEREN ET AL
dia (35/min), QT interval prolongation (0.74 sec) and v e n t r i c u l a r p r e m a t u r e b e a t s appea red . Therefore the quinidine therapy was stopped. Shortly thereaf ter recurrent bouts of AVT oc- curred (Fig. 3). Isoproterenol infusion up to 8 ~g/min was ineffective in preventing the recur- rent AVTs; therefore, r ight atr ial pacing was started, at a rate of 105/min, which abolished all ar rhythmias (Fig. 3). Atrial pacing was replaced by ventricular pacing after 15 minutes, because of possible electrode displacement. During the next two days ventricular pacing was continued at a rate of 73/min (Fig. 3). Pacing was stopped after recovery of sinus rhythm at a rate of 72/min with a normal QT interval. The patient was discharged f rom t h e h o s p i t a l s e v e n d a y s l a t e r w i t h amiodarone treatment.
DISCUSSION The characterist ic ECG features of AVT are
marked prolongation of the QT interval, repeti- t ive bouts of ven t r i cu la r tachycardia , wi th a twist ing QRS axis and polymorphous QRS ap- pearance. The ar rhythmia is usually initiated by a VPB with a long coupling interval. The marked QT prolongation is a result of an uneven prolon- gation of ventricular repolarization, setting the ground for a re-entrant ventricular arrhythmia. 3 AVT appears most frequently during quinidine and other type I ant iarrhythmic drug therapy, ~-s but prenylamine, 5,s psychotropic drugs, 9 hypo- magnesemia, TM hypokalemia, 11 ext reme brady- cardia with or without heart block, 3 increased intracranial pressure 5,~2 and congenital prolon- gation of QT 13 have also been described occasion- ally as precursors.
Conventional ant iarrhythmic therapy, such as lidocaine or procainamide, which have similar ef- fects on ischemic, but dissimilar effects on normal ventricular muscle, s.hould be avoided in AVT, since it may further prolong the QT interval. 3,5 Acceleration of hear t rate is the simplest and fastest way of shortening repolarization; this goal may be achieved by administration of atropine or i sopro te reno l , or by t e m p o r a r y pacing. Iso- proterenol infusion is presently the most common mode of therapy of AVT. 3,~,1~17 However, there are patients who are refractory to this therapy TM and in others, such as those after an acute myocardial infarction or with excessive hypertension, this drug is even contraindicated.
In two of our patients isoproterenol infusion was ineffective in suppressing the AVT while in the other two patients it was regarded as danger-
ous because of recent myocardial infarction or excessive hypertension. Temporary ventr icular pacing in all of our patients, at rates of 90-110/ min, immediately abolished the ventricular ar- rhythmias. Ventricular pacing, by increasing the heart rate, shortens the QT interval and reduces the temporal dispersion of ventricular repolariza- tion. 14,19 By gradual ly decreasing the pacing rate, the minimum rate which prevents the recurrence of AVT can be determined for each individual pa- tient, and pacing can be continued at the lowest rate required. Ventricular pacing has other ad- vantages as it can be performed in patients with recent myocardial infarction, active coronary dis- ease, and hypertension of atrio-ventricular block; several authors have reported good resul ts in selected patients. 5,7,1~ In all our cases pacing could be terminated within 24-48 hours and AVT did not recur in any of them. The electrode was left in place for an additional 24-48 hours and was removed when a significant shortening of the QT interval was observed.
Atrial pacing is another mode of increasing the heart rate which has been reported to be effective in suppressing AVT. 15 We temporarily employed atrial pacing in two of our patients. In one (Case 3), atrial pacing was effective in controlling the AVT, but due to an unstable electrode position, pacing failed intermittently, allowing repeated bouts of AVT. After the electrode was advanced to the right ventricle, stable ventricular pacing was achieved. In the second patient (Case 4), al though atrial pacing was effective, we considered ven- tricular pacing as a safer procedure and, there- fore, after 15 minutes of effective atrial pacing, the electrode was forwarded into the right ventri- cle and pacing was continued from there.
We conclude t ha t the ini t ia l r ecommended mode of therapy at present is isoproterenol infu- sion, but if this drug is ineffective, partially effec- tive or contraindicated, ventricular pacing should be instituted. Pacing can be started at a rate of 120-130/min and soon be reduced to the lowest effective pacing rate.
REFERENCES
1. DESSERTENNE, F: La tachycardia ventriculaire a deux foyers opposes variables. Arch Mal Coeur 59:263, 1966
2. 8ELZER, A AND WRAY, H W: Quinidine syncope. Paroxysmal ventricular fibrillation occurring dur- ing treatment of chronic atrial arrhythmias. Circu- lation 30:17, 1964
3. KRIKLER, D M AND CURRY, P V L: Torsade de
J. ELECTROCARDIOLOGY, VOL. 14, NO. 2, 1981

PACING FOR ATYPICAL VENTRICULAR TACHYCARDIA 205
pointes: an atypical ventricular tachycardia. Br Heart J 38:117, 1976
4. KOSSMANN, C E: Torsade de pointes: an addition to the nosography of ventricular tachycardia. Am J Cardiol 42:1054, 1978
5. SCLAROWSKY, S, STRASBERG, B, LEWIN, R F AND AGMON, J: Polymorphous ventricular tachycardia: clinical features and treatment. Am J Cardiol 44"339, 1979
6. MELTZER, R S, ROBERT, E W, MCMORROW, M AND MARTIN, R P: Atypical ventricular tachycardia as a manifestation of disopyramide toxicity. Am J Car- diol 42:1049, 1978
7. NICHOLSON, W F, MARTIN, W F, GRACEY, F G AND KNOCH, H R: Disopyramide induced ventricular fibrillation. Am J Cardiol 43:1053, 1979
8. BENS, J L, DUBOISSET, M, QUIRET, J C, LESBRE, J P AND BERNASCONI, T: Syncopes par torsades de pointes induites ou facorises par la prenylamine. Arch Mal Coeur 66:1427, 1973
9. SCHOONMAKER, F W, OSTEEN, R T AND GREENFIELD, J C: Thioridazine (Mellaril)-induced ventricular tachycardia controlled with an artificial pace- maker. Ann Intern Med 65:1076, 1966
10. LOEB, H S, PEETRAS, R J, GUNNAR, R M AND TOBIN, JR, J R: Paroxysmal ventricular fibrillation in two patients with hypomagnesemia. Treatment by transvenous pacing. Circulation 37"210, 1968
11. TAMURA, K, TAMURA, T, YOSHIDA, S, INUT, M AND FUKUHARA, N: Transient recurrent ventricular fib- rillation due to hypopotassemia with special note on the U wave. Jap Heart J 8:652, 1967
12. GROSSMAN, M A: Cardiac arrhythmias in acute central nervous system disease. Successful man- agement with stellate ganglion block. Arch Intern Med 136:203, 1976
13. GASCHO, J A AND SCHIEKEN, R: Congenital com- plete heart block and long QT syndrome requiring ventricular pacing for control of refractory ven- tricular tachycardia and fibrillation. J Electrocar- dio 12:331, 1979
14. HAN, F, MILLETT, D, CHIZZONITTI, B AND MOE, G K: Temporal dispersion of recovery of excitability in atrium and ventricle as a function of heart rate. Am Heart J 71:481, 1966
15. BROCHIER, M, MOTTE, G AND FAUCHIER, J P: Tachycardia ventriculair en torsades de pointes. Actualitas Cardio-vasculaires Medico-chirurgi- cales 6:171, 1972
16. LYON, J L, DONOSO, E AND FRIEDBERG, D K: Tem- porary control of ventricular arrhythmias by drug- induced sinus tachycardia . Arch In tern Med 123:436, 1969
17. LINENTHAL, A AND ZOLL, P: Prevention ofventricu- lar tachycardia and fibrillation by intravenous isoproterenol and epinephrine. Circulation 27:5, 1963
18. ANDERSON, J L AND MASON, J W: Successful treat- ment by overdrive pacing of recurrent quinidine syncope due to ventricular tachycardia. Am J of Med 64:715, 1978
19. SOWTON, E, LEATHAM, A AND CARSON, P: The sup- pression of ventricular arrhythmias by artificial pacing of the heart. Lancet 2:!098, 1966
J. ELECTROCARDIOLOGY, VOL. 14, NO. 2, 1981