Embed Size (px)
Citation preview

Ventricular couplets in the young: Prognosis related to underlying substrate
Ventricular couplets may be a risk factor for sudden death in adults, but their prognosis in children is unknown. From 1981 to 1987 104 patients, mean age 13.2 years (0.2 to 37 years), had ventricular couplets on a 24-hour electrocardiogram (ECG) (Holter monitor) and on follow-up with a second Holter (mean, 2.5 years). Of the 104 patients, 22 had a normal heart and 82 had an abnormal heart. Patients with a normal or an abnormal heart did not differ in incidence or severity of symptoms (patients with a normal heart had 17 instances of palpitations and none of syncope; patients with an abnormal heart had 49 instances of palpitations, six of dizziness, and none of syncope). Number of ventricular couplets was higher in patients with a normal heart (33 • 50 /day: mean • 1 SD) than in those with an abnormal heart (17 • 15 /day; p < 0.05). Of the 22 patients with a normal heart, 11 underwent an electrophysiologic study (EPS); none had inducible ventricular tachycardia. After mean follow-up of 29.7 months, all 22 patients with a normal heart were alive without ventricular tachycardia; 6 of 22 were treated for palpitations, with complete suppression of couplets in two. In 11 of 16 untreated patients with a normal heart, ventricular couplets disappeared spontaneously. Of the 82 patients with an abnormal heart, 32 had an EPS: nine (28%) had sustained ventricular tachycardia, 16 (50%) had nonsustained ventricular tachycardia, and seven (22%) had no inducible ventricular tachycardia. ECG criteria and hemodynamic status were of limited value in predicting inducibility of ventricular tachycardia. Two of 82 patients with an abnormal heart had sudden death with documented ventricular tachycardia/fibril lation; 59 of 82 were treated, with success in 55; 23 were not treated, with spontaneous disappearance of ventricular couplets in 10. As a result of this study, we reached the following conclusions. (1) Ventricular couplets appeared benign in patients with a normal heart. (2) In patients with an abnormal heart, inducible ventricular tachycardia was common (78%). (3) Sudden death occurred in 2 of 82 patients with an abnormal heart within less than 3 years of detection of couplets. (4) Thus the prognosis of ventricular couplets in the young may be related to the underlying substrate. (AM HEART J 1990;119 :577 . )
T h o m a s Paul, MD, a Cecile Marchal, MD, and Ar thur Garson, Jr., MD.
Houston, Texas, and Hannover, W. Germany
The presence of ventricular couplets on a 24-hour electrocardiogram (ECG) (Holter monitor) has been shown to be a risk factor for sudden cardiac death in adul t pat ients with coronary ar tery disease. 1, 2 Oc- currence of ventricular couplets in adul t patients with a normal hear t does not imply a poor prognosis with regard to sudden cardiac death, s The signifi-
From the Lillie Frank Abercrombie Section of Cardiology, Department of Pediatrics, Baylor College of Medicine, and Texas Children's Hospital; and aDepartment of Pediatric Cardiology, Children's Hospital, Medizinische Hochschule Hannover. Supported in part by grants HL24916, HL07190, and RR00188 from the National Institutes of Healthl Bethesda, Md.; by a grant from the J.S. Ab- ercrombie Foundation, Houston, Texas; and by Deutsche Forschungsge- meinschaft grant Pa 352/1-1 (Dr. Paul), Bonn-Bad Godesberg, Federal Re- public of Germany. Received for publication Dec. 9, 1988; accepted Nov. 1, 1989. Reprint requests: Arthur Garson, Jr., MD, Pediatric Cardiology, Texas Children's Hospital, 6621 Fannin, Houston, TX 77030. 4 / 1 / 1 8 0 1 6
cance of ventricular couplets in children, adolescents, and young adults has not been systematically inves- tigated. The purpose of the present restrospective s tudy was twofold. First, we tr ied to determine the presentat ion and prognosis of young patients with ventricular couplets who had either a normal or an abnorma l heart, relating couplets to hemodynamics. Second, we wanted to assess the role of electrophys- iologic test ing in identifying young pat ients with ventricular couplets who may be at risk for sudden death.
METHODS
Patient populat ion.The study group consisted of all pa- tients who were seen by the Pediatric Cardiology Section of Texas Children's Hospital between 1981 and 1987 who had (1) documentation of ventricular couplets on Holter monitor, (2) absence of ventricular tachycardia by nonin- vasive evaluation (i.e., standard ECG, Holter monitor, treadmill exercise test), a n d (3) minimal follow-up of 3
577

March 1990
578 Paul, Marchal, and Garson American Heart J . . . . a!
months with a second Holter monitor. Patients older than 18 years were included in the study if they had congenital heart disease.
Noninvasive evaluation. All patients were questioned about symptoms, specifically about episodes of syncope or presyncope. All patients underwent a physical examina- tion, a routine chest x-ray film, and an echocardiographic evaluation including a two-dimensional examination in the appropriate views to assess anatomy and hemodynamics. Those who could cooperate (generally those over 5 years of age) underwent a treadmill exercise test according to a modified Bruce protocol. 4' 5 In this protocol, the patient is encouraged to run to exhaustion.
Electrophysiologic study (EPS). Cardiac catheteriza- tion was performed in the postabsorptive and sedated state, after written informed consent had been obtained from the patient or the patient's parents. All antiarrhyth- mic medication was discontinued at least 5 half-lives before the EPS. Premedication consisted of meperidine (2 mg/kg) and promethazine (1 mg/kg). Sedation throughout the study was maintained with the same drugs.
The protocol for electrophysiologic evaluation in chil- dren has been previously published. 6-w Single and double premature ventricular exstrastimuli were introduced into sinus rhythm after eight beats of ventricular paced rhythm at a cycle length of 500 msec. Ventricular burst pacing was performed for 8 stimuli beginning at a cycle length of 300 msec and decreasing the cycle length in 20 msec steps until 2:1 ventricular capture occurred. 7
Hemodynamic data. Cardiac catheterization and echocardiographic evaluation were performed in 63 pa- tients to assess anatomy and hemodynamics. Cardiac hemodynamic findings were classified as follows: (1) "excellent" = normal hemodynamics; (2) "fair" = abnormal hemodynamics requiring neither medical nor surgical treat- ment; (3) "poor"= hemodynamics that would require eventual operative intervention or, if the condition was in- operable, subpulmonary ventricular pressure of two thirds systemic pressure or end-diastolic pressure greater than 1.5 times normal, or pulmonary artery peak systolic pressure beyond any stenosis of at least two thirds systemic pressure or greater. 11
Medical treatment and follow-up. Treatment was con- sidered successful if there was complete elimination of ventricular couplets and an 85 % reduction in the number of single premature ventricular contractions (PVCs) on Holter recordings. 12,13 For all patients, outpatient follow- up was performed at 3,6, and 12 months and every 6 months thereafter with Holter monitoring.
Statistical analysis. Contingency tables for categorical data were evaluated by Fisher's exact test or by chi square analysis. Numerical data were compared by means of Stu- dent's t test. Statistical significance was indicated if the chance probability for a difference to occur was less than 0.05.
RESULTS Diagnoses. The s tudy group consisted of 104 pa-
t ients in whom ventr icular couplets were detec ted at a mean age of 13.2 years (range 3 months to 37 years).
In 22 of the 104 pat ients an anatomical ly normal hear t was demons t ra ted echocardiographically; 11 had cardiac catheter izat ion. Th e remaining 82 pa- t ients had an abnormal hea r t assessed echocardio- graphically, with cardiac catheter izat ion per formed in 58.
The most common diagnosis was postsurgical re- pair of congenital hear t disease in 49 of the 82 patients: 29 had repair of te t ra logy of Fallot, 13 had an atrial switch procedure for simple t ransposi t ion of the great arteries, and seven had various other types of operat ions performed. Th e mean interval between the surgical procedure and the occurrence of ventric- ular couplets was 8 months (range 0.5 to 57 months) . Unopera ted congenital hea r t disease was present in 11: aortic stenosis/insufficiency in five, ventr icular septal defect with pu lmonary vascular obstruct ive disease in four, and vent r icular inversion with ven- tr icular septal defect and subpulmonic stenosis in two. Card iomyopa thy was found in 10 patients: six had di lated and four had hyper t rophic cardiomyop- athy. Arrhythmogenic r ight ventr icular dysplasia was present in six pa t i en t s . T h e remaining pat ients had mitral valve prolapse (n = three), myocardi t is (n -- two), and left ventr icular f ibroma (n = one).
Demographic and noninvasive data. These d a t a are summarized in Table I. Pa t ien t s with a normal hear t were significantly younger than those with an abnor- mal heart . On Hol ter assessment, pat ients with a normal hear t had a significantly higher number of ventr icular couplets and of single uniform or multi- form PVCs than did pat ients with an abnormal heart . A treadmil l exercise tes t was per formed in 53 of the 104 patients. Ventr icular a r rhy thmia during or im- media te ly af ter the exercise tes t (i.e., PVCs or ven- tricular couplets) was observed less f requent ly in pa- t ients with a normal hea r t than in those with an abnormal heart .
Electrophysiologic study. The 43 patients who un- derwent E P S were in general a representa t ive sample of the 104 s tudy patients, bu t the incidence of symp- toms was higher in pat ients who had EPS: 35 of the 43 pat ients (81%) with E P S had symptoms, in con- t ras t with 37 of the 61 pa t ien ts (61%) without E P S (p < 0.05). Pa t ien ts who did and did not have E PS were not different in age at presentat ion, in the pro- port ion of pat ients with a normal as opposed to an abnormal hear t , in classification of hemodynamic status, in n u m b er of ventr icular couplets or PVCs, in results of the exercise test. Even in the subgroups of pat ients with a normal and an abnormal hear t , no differences were found between those who had E P S and those who did not when these same variables were considered.
Induced ventricular arrhythmias. None of the 11 pa-
Volume 119
Number 3, Part 1 Prognosis of ventricular couplets in the young 5 7 9
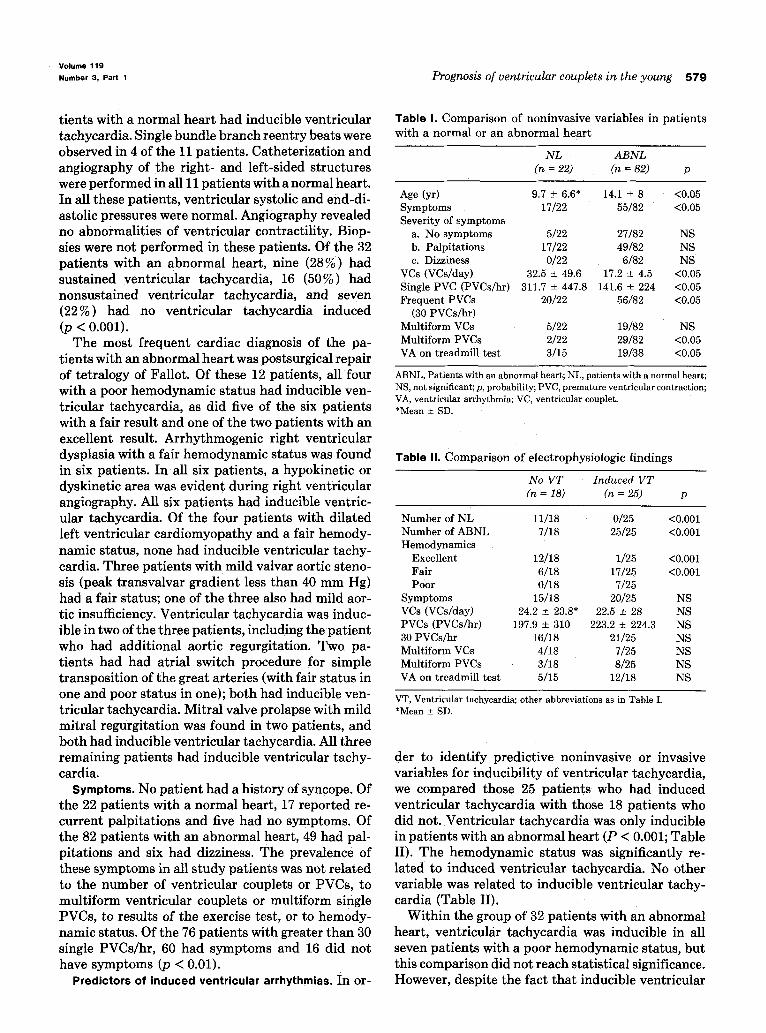
tients with a normal heart had inducible ventricular tachycardia. Single bundle branch reentry beats were observed in 4 of the 11 patients. Catheterization and angiography of the right- and left-sided structures were performed in all 11 patients with a normal heart. In all these patients, ventricular systolic and end-di- astolic pressures were normal. Angiography revealed no abnormalities of ventricular contractility, Biop- sies were not performed in these patients. Of the 32 patients with an abnormal heart, nine (28%) had sustained ventricular tachycardia, 16 (50%) had nonsustained ventricular tachycardia, and seven (22%) had no ventricular tachycardia induced (p < 0.001).
The most frequent cardiac diagnosis of the pa- tients with an abnormal heart was postsurgical repair of tetralogy of Fallot. Of these 12 patients, all four with a poor hemodynamic status had inducible ven- tricular tachycardia, as did five of the six patients with a fair result and one of the two patients with an excellent result. Arrhythmogenic right ventricular dysplasia with a fair hemodynamic status was found in six patients. I n all six patients, a hypokinetic or dyskinetic area was evident during right ventricular angiography. All six patients had inducible ventric- ular tachycardia. Of the four patients with dilated left ventricular cardiomyopathy and a fair hemody- namic status, none had inducible ventricular tachy- cardia. Three patients with mild valvar aortic steno- sis (peak transvalvar gradient less than 40 mm Hg) had a fair status; one of the three also had mild aor- tic insufficiency. Ventricular tachycardia was induc- ible in two of the three patients, including the patient who had additional aortic regurgitation. Two pa- tients had had atrial switch procedure for simple transposition of the great arteries (with fair status in one and poor status in one); both had inducible ven- tricular tachycardia. Mitral valve prolapse with mild mitral regurgitation was found in two patients, and both had inducible ventricular tachycardia. All three remaining patients had inducible ventricular tachy- cardia.
Symptoms. No patient had a history of syncope. Of the 22 patients with a normal heart, 17 reported re- current palpitations and five had no symptoms. Of the 82 patients with an abnormal heart, 49 had pal- pitations and six had dizziness, The prevalence of these symptoms in all study patients was not related to the number of ventricular couplets or PVCs, to multiform ventricular couplets or multiform single PVCs, to results of the exercise test, or to hemody- namic status. Of the 76 patients with greater than 30 single PVCs/hr, 60 had symptoms and 16 did not have symptoms (p < 0.01).
Predictors of induced ventricular arrhythmias. I n o r -
Table I. Comparison of noninvasive variables in patients with a normal or an abnormal heart
NL ABNL =22) ~ = 8 ~ p
Age (yr) 9.7 ___ 6.6* 14.1 -+ 8 <0.05 Symptoms 17/22 55/82 <0.05 Severity of symptoms
a. No symptoms 5/22 27/82 NS b. Palpitations 17/22 49/82 NS c. Dizziness 0/22 6/82 NS
VCs (VCs/day) 32.5 _+ 49.6 17.2 _+ 4.5 <0.05 Single PVC (PVCs/hr) 311.7 _+ 447.8 141.6 +- 224 <0.05 Frequent PVCs 20/22 56/82 <0.05
(30 PVCs/hr) Multiform VCs 5/22 19/82 NS Multiform PVCs 2/22 29/82 <0.05 VA on treadmill test 3/15 19/38 <0.05
ABNL, Patients with an abnormal heart; NL, patients with a normal heart; NS, not significant; p, probability; PVC, premature ventricular contraction; VA, ventricular arrhythmia; VC, ventricular couplet. *Mean + SD.
Table II. Comparison of electrophysiologic findings
No V T Induced V T (n = 18) (n = 25) p
Number of NL 11/18 0/25 <0.001 Number of ABNL 7/18 25/25 <0.001 Hemodynamics
Excellent 12/18 1/25 <0.001 Fair 6/18 17/25 <0.001 Poor 0/18 7/25
Symptoms 15/18 20/25 NS VCs (VCs/day) 24.2 _ 23.8* 22.5 +_28 NS PVCs (PVCs/hr) 197.9 +_ 310 223.2 +_ 224.3 NS 30 PVCs/hr 16/18 21/25 NS Multiform VCs 4/18 7/25 NS Multiform PVCs 3/18 8/25 NS VA on treadmill test 5/15 12/18 NS
VT, Ventricular tachycardia; other abbreviations as in Table I. *Mean _+ SD.
der to identify predictive noninvasive or invasive variables for inducibility of ventricular tachycardia, we compared those 25 patients who had induced ventricular tachycardia with those 18 patients who did not. Ventricular tachycardia was only inducible in patients with an abnormal heart (P < 0.001; Table II). The hemodynamic status was significantly re- lated to induced ventricular tachycardia. No other variable was related to inducible ventricular tachy- cardia (Table II).
Within the group of 32 patients with an abnormal heart, ventricular tachycardia was inducible in all seven patients with a poor hemodynamic status, but this comparison did not reach statistical significance. However, despite the fact that inducible ventricular

March 1990 5 8 0 - - -l~aul, - - - "lV]arctml, a n d G a r s o n American Heart Journal
tachycardia in patients with an abnormal heart was associated with a poor hemodynamic status, it is im- portant to note that of the 25 patients with an abnormal heart who had inducible ventricular tachy- cardia, 17 (68%) had fair hemodynamics, and one of the 25 patients even had an excellent hemodynamic status.
Trea tment and fol low-up
Pat i en t s w i th a normal heart. All 11 patients who had EPS remained untreated. In six patients who did not have EPS, therapy was started for symptomatic palpitations. Initial successful suppression of ven- tricular arrhythmias was achieved in all six patients.
After a mean follow-up of 2.5 years (range 4 months to 6 years), all patients with a normal heart were alive; none of them had developed clinical ventricular tachycardia or syncope. Recurrence of ventricular couplets was observed on Holter monitoring in four of the six patients who received treatment. The remaining two patients continued to have successful suppression of their ventricular ectopy. Of the 16 untreated patients, only five continued to have ven- tricular couplets on a follow-up Holter monitor. In 11 of the 16 patients, ventricular couplets disappeared spontaneously.
Pat i en t s w i th an abnormal heart. Of the 82 pa- tients with an abnormal heart, 23 were not treated including the seven patients who had no inducible ventricular tachycardia during EPS. In the remain- ing 16 patients, no treatment was considered to be justified, as all these patients presented without symptoms and had excellent or fair hemodynamics. Treatment in 59 of the 82 patients with an abnormal heart consisted of surgical correction of congenital heart disease in two and of medical therapy in 57. Of those 59 patients, two (neither of whom had EPS) died. The first patient, 1 year of age, with severe hy- pertrophic cardiomyopathy, died after 3 months of treatment with propranolol and verapamil; these drugs had initially suppressed ventricular ectopy. However, she returned to the hospital with ventric- ular tachycardia that degenerated into ventricular fibrillation. The second patient, 25 years old, had pulmonary hypertension due to a large unoperated ventricular septal defect. She had been treated with mexiletine, which resulted in normalization of her Holter monitor recordings. During a phlebotomy, she had spontaneous ventricular tachycardia that degen- erated into ventricular fibrillation. Both of these cases demonstrate that initial "normalization" of the Holter reading may not be sufficient to predict out: come.
After a mean follow-up of 2.6 years (range 3 months to 7.1 years), ventricular couplets were still present in
I3 of the 23 untreated patients. Of the 57 patients who were treated and who were still alive, only two had late recurrence of ventricular ~ouplets.
DISCUSSION
Ventr icular couplets in patients with a normal heart.
Ventricular couplets are rarely found in adult pa- tients with a normal heart. 1, 3, 14 Prognosis appears benign, but follow-up has been limited. 14 In children with an anatomically normal heart, uniform prema- ture ventricular contractions have been shown to be benign)~, 16 The prognosis of ventricular couplets in young patients with a normal heart has not been in- vestigated, probably due to the low incidence of ven- tricular couplets in infants, children, and young adults with a normal hear t ) 7-19
Of the 104 patients of our study group, 22 had a normal heart. The ventricular stimulation protocol applied to the patients with a normal heart is "specific," as none of these patients developed ven- tricular tachycardia during follow-up without treat- ment. The high specificity of the stimulation protocol may be due to the fact that only double ven- tricular extrastimuli and ventricular burst pacing were used for the ventricular stimulation protocol. Using the same protocol in adult patients, Vandepol et al. 2~ found that ventricular tachycardia was in- duced only rarely in patients without any previously documented clinical ventricular tachycardia. Brugada et el. 21 demonstrated that in adult patients without clinical ventricular tachycardia, the protocol became less specific with more ventricular extra- stimuli. Intepretation of results of ventricular stim- ulation in patients without cIinical ventricular ta- chycardia should be made with caution if an aggres- sive (more than double extrastimuli) ventricular stimulation protocol is to be used. 22
Ventricular couplets appear benign and may even resolve spontaneously in young patients with a nor- mal heart, and they may be comparable with single premature ventricular contractions. Even young pa- tients with clinical ventricular tachycardia and a normal heart rarely develop severe symptoms, 23 and the induction of ventricular tachycardia in a child during EPS may imply that the heart is not normal,24, 25 if there is an underlying substrate for ventricular tachycardia.
Yentricular couplets in patients with an abnormal
heart. In general, children with an abnormal heart who develop ventricular arrhythmias have been dem- onstrated to have a different prognosis from those with a normal heart. 26 Even the presence of single uniform PVCs in patients with an abnormal heart may imply a poor prognosis. 27 In accordance with the

Volume 119
Number 3, Part 1 Prognosis o[ ventricular couplets in the young 581
findings of previous reports, 7, 2s, 29 patients after sur- gical correction of tetralogy of Fallot formed the largest subgroup of patients with an abnormal heart in our study group.
Arrhythmogenic right ventricular dysplasia was found in six patients who had inducible ventricular tachycardia. As exercise-related sudden death is a common finding in these patients, 3~ suppression of ventricular ectopy appears warranted. Since cross- sectional echocardiography may be negative in chil- dren with arrhythmogenic right ventricular dysplasia, 31 cardiac catheterization and EPS should probably be performed in all patients in whom the disease is suspected.
Because of the design of our ventricular stimula- tion protocol, it is unlikely that induction of ventric- ular tachycardia in our patients was a false positive result. 32 Patients with inducible ventricular tachy- cardia were treated. In accordance with the report on specificity of EPS from Byrum e t al . , 33 patients without inducible ventricular tachycardia remained untreated. All of our seven patients without inducible ventricular tachycardia had an uneventful course, but follow-up has only extended to 2.8 years. At the present time, it appears that in those with an abnor- mal heart and couplets, ventricular extrastimulus could be used to make a decision on the need for treatment.
In conclusion, because inducible ventricular tachy- cardia is common in patients with an abnormal heart, ventricular couplets in young patients may be simi- lar to ventricular tachycardia. Due to the major dif- ferences in patients with normal and abnormal hearts, prognosis of ventricular couplets in the young may be related to the underlying substrate.
REFERENCES
1. Bigger JT, Fleiss JL, Kleiger R, Miller JP, Rolnitzky LM. The relationship among ventricular arrhythmias, left ventricular dysfunction, and mortality in 2 years after myocardial infarc- tion. Circulation 1984;69:250-8.
2. Hinkle LE, Carver ST, Stevens M, The frequency of asymp- tomatic disturbances of cardiac rhythm and conduction in middle-aged men. Am J Cardiol 1969;24:629-50.
3. Bethge KP, Bethge D, Meiners G, Lichtelen PR. Incidence and prognostic significance of ventricular arrhythmias in individ- uals without detectable heart disease. Eur Heart J 1983;4:338- 46.
4. Bruce RA. Methods of exercise testing. Stress test, bicycle, treadmill, isometrics. Am J Cardiot 1974;33:715-20.
5. James FW, Kaplan S, Schwartz DC, Chou T; Sandker MJ, Naylor V. Response to exercise in patients after total surgical correction of tetralogy of Fallot. Circulation 1976;54:671-9.
6. Gillette PC, Garson A. Intracardiac electrophysiologic studies: use in determining the site and mechanisms of dysrhythmias. In Gillette PC, Garson A, eds. Pediatric cardiac dysrhythmias. New York: Grune & Stratton, Inc, 1981'.77-120.
7. Garson A, Porter C J, Gillette PC, McNamara DG. Induction
of ventricular tachycardia during electrophysiologic study af- ter repair of tetralogy of Fallot. J Am Coil Cardio11983;1:1493- 502.
8. Garson A. Supraventricular tachycardia. In: Gillette PC, Gar- son A, eds. Pediatric cardiac dysrhythmias. New York: Grune & Stratton, Inc, 1981:177-253.
9. Karpawich PP. First- and second-degree atrioventricular block. In: Gillette PC, Garson A, eds. Pediatric cardiac dysrhythmias. New York: Grune & Stratton, Inc, 1981:361-81.
10. Mehta AV, Wolff GS, Tamer D, Pickoff AS, Casta A, Garcia OL, Helbrand H. Determinants of ventricular refractory peri- ods in children with congenital heart disease: effects of cycle length and age. AM HEART J 1981;102:75-9.
11. Garson A, McNamara DG. Sudden death in a pediatric cardi- ology population, 1958 to 1983: relation to prior arrhythmias. J Am Coil Cardiol 1985;5:134B-7B.
12. Morganroth J, Michelson EL, Horowitz LN, Josephson ME, Pearlman A, Dunkman WB. Limitations of routine long-term electrocardiographic monitoring to assess ventricular ectopic frequency. Circulation 1978;58:408-14.
13. Hordof AJ, Steeg CN, Davies M, Rosen MR. Variability of ventricular ectopic frequency in children with chronic ar- rhythmias [Abstract]. Circulation 1983;68:1028.
14. Kennedy HL, Underhill SJ. Frequent or complex ventricular ectopy in apparently healthy subjects. A clinical study of 25 cases. Am J Cardiol 1976;38:141-8.
15. Jacobsen JR, Garson A, Gillette PC, McNamara DG. Prema- ture ventricular contractions in normal children. J Pediatr 1978;92:36-8.
16. Rozanski JJ, Dimich l, Steinfeld L, Kupersmith J. Maximal exercise stress testing in evaluation of arrhythmias in children: results and reproducibility. Am J Cardiol 1979;43:951-6.
17. Southall DP, Richards J, Mitchell P, Brown DJ, Johnston PGB. Shineborne EA. Study of cardiac rhythm in healthy newborn infants. Br Heart J 1980;43:14-20.
18. Scott O, Williams GJ, Fiddler GI. Results of 24-hour ambula- tory monitoring of electrocardiogram in 131 healthy boys aged 10 to 13 years. Br Heart J 1980;44:304-8.
19. Brodsky M, Wu D, Denes P, Kanakis C, Rosen KM. Arrhyth- mias documented by 24-hour continuous electrocardiographic monitoring in 50 male medical students without apparent heart disease. Am J Cardiol 1977;39:390-5.
20. Vandepol CJ, Farshidi A; Spielman SR, Greenspan AM, Horowitz LN, Josephson ME. Incidence and clinical signifi- cance of induced ventricular tachycardia. Am J Cardiol 1980;45:725-3L
21. Brugada P, Green M, Abdollah H, Wellens HJJ. Significance of ventricular arrhythmias initiated by programmed ventric- ular stimulation: importance of the type of ventricular ar~ rhythmia induced and the number of premature stimuli required. Circulation 1984;69:87-92.
22. Brugada P, Abdollah H, Heddle B, Wellens HJJ. Results of a ventricular stimulation protocol using a maximum of 4 pre- mature stimuli in patients without documented or suspected ventricular arrhythmias. Am J Cardiol 1983;52:1214-18.
23. Bergdaht DM, Stevenson JG, Kawabori I, Guntheroth WG. Prognosis in primary ventricular tachycardia in the pediatric patient. Circulation 1980;62:897-901.
24. Garson A, Gillette PC, Porter CJ. Electrophysiologic induc. tion of ventricular dysrhythmias in 152 children with a normal or abnormal heart [Abstract]. J Am Coll Cardiol 1983;1:614.
25. Deal B J, Miller SM, Scagliotti D, Prechel D, Gallastegui JL, Hariman RJ. Ventricular tachycardia in a young population without overt heart disease. Circulation 1986;73:1111-18.
26. Garson A, Nihill MR, McNamara DG, Cooley DA. Status of the adult and adolescent after repair of tetralogy of Fallot. Circulation 1979;59:1232-40.
27. Garson A. Evaluation and treatment of chronic ventricular dysrhythmias in the youlag. Cardiovasc Rev Rep 1981;2:1164- 96.
28. Garson A, Randall DC, Gillette PC, Smith RT, Moak JP, McVey P, McNamara DG. Prevention of sudden death after

March 1990
5 8 2 Paul, Marchal, and Garson American Heart Journal
repair of tetralogy of Fallot: treatment of ventricUlar arrhyth- mias. J Am Coll Cardiol 1985;6:221-7.
29. Dunnigan :A, Pritzker MR, Benditt DG, Benson DW. Life- threatening ventricular tachycardias in late survivors of sur- gically corrected tetralogy of Fallot. Br Heart J 1984;52:198- 206.
30. Thiene G, Nava A, Corrado D, Rossi L, Pennelli N. Right ven- tricular cardiomyopathy and sudden death in young people. N Engl J Med 1988;318:129-33.
31. Moro E, Pignoni P, Nicolosi GL, Zardo F, Burelli C, Bergara G, Furlanello F, Zanuttini D. Valore e limiti dell' ecocardio- grafia bidimensionale nell' identificazione della "dysplasia ventricolare destra." G Ital Cardiol 1987;17:661-6.
32. Garson A. Chronic arrhythmias after surgery for congenital and acquired heart disease. Curr Opin Cardiol 1986;1:745-57.
33. Byrum CJ, Sondheimer HM, Kavey REW, Blackman MS. Ventricular arrhythmia non-therapy guided by electrophysi- ologic testing. [Abstract]. AM HEART J 1985;110:707.