Embed Size (px)
Citation preview

Ventilation

Intro: why do we breathe?

Key Terms
• Ventilation: Movement of air into and out of the lungs
• Gas exchange: Movement of gases across membranes according to pressure gradients
• Pressure gradients: Determined by the partial pressure of the gas
• Gases: Oxygen necessary for cellular respiration; Carbon dioxide is a volatile acid

Breathing, ventilation and respiration
• Used synonymously– Used to think
respiration occurred in the lung
• Ventilation: movement of air
• Respiration: cellular utilization of O2

• Pulmonary minute ventilation (VE)– The rate of expired
ventilation– Usually expressed
in L/min– VE = VT x f– Expired ventilation
and inspired essentially the same, may differ in transition from rest to exercise
Ventilation
.
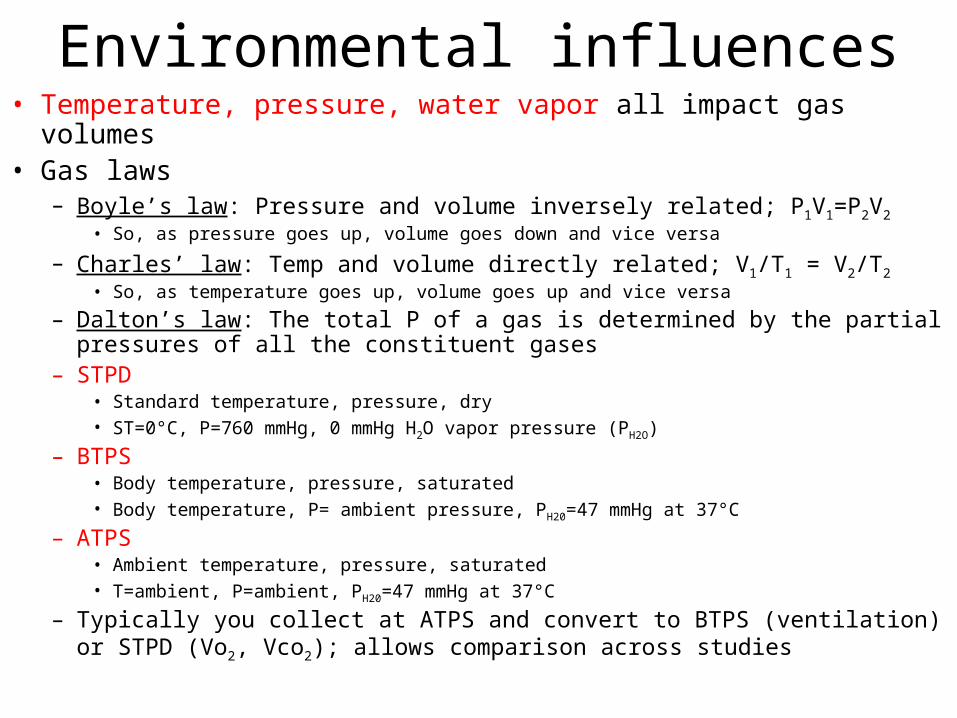
• Temperature, pressure, water vapor all impact gas volumes• Gas laws
– Boyle’s law: Pressure and volume inversely related; P1V1=P2V2
• So, as pressure goes up, volume goes down and vice versa
– Charles’ law: Temp and volume directly related; V1/T1 = V2/T2
• So, as temperature goes up, volume goes up and vice versa
– Dalton’s law: The total P of a gas is determined by the partial pressures of all the constituent gases
– STPD• Standard temperature, pressure, dry• ST=0°C, P=760 mmHg, 0 mmHg H2O vapor pressure (PH2O)
– BTPS• Body temperature, pressure, saturated• Body temperature, P= ambient pressure, PH20=47 mmHg at 37°C
– ATPS• Ambient temperature, pressure, saturated• T=ambient, P=ambient, PH20=47 mmHg at 37°C
– Typically you collect at ATPS and convert to BTPS (ventilation) or STPD (Vo2, Vco2); allows comparison across studies
Environmental influences

Entry of O2 into the blood

Entry of O2 into the blood
• Determined Entirely by pressure gradients
• Partial pressure– Pressure exerted by each gas in a composition
– Atmospheric pressure (PAtm): 760 mmHg
– Partial pressure of O2 (Po2): 159 mmHg (.2094 x 760)
– Rest is nitrogen, some argon and very little CO2
– When air reaches alveoli, Po2 falls, why?• Think of gas laws

Entry of O2 into the blood
1) Water vapor • Gas is fully humidified, so at normal body temp, water vapor
pressure is 47 mmHg
2) Co2 is also higher in the alveoli
• Thus, Po2 of alveoli about 100-105 mmHg
• 760 – 47 = 713 or the pressure of the air in the lung– Dalton’s Law
• 713 x .2094 = 149 (inspired pressure of O2; PiO2)
• PAO2 = PiO2 – (PACO2/RER)– Alveolar gas equation
• PAO2 = 149 – (40/.85) or 149-47 = 102
• RER = respiratory exchange ratio or Vco2/Vo2
– Usually about 0.85 at rest with mixed diet

Entry of O2 into the blood
• Once O2 gets into alveoli it diffuses into the blood– Due to favorable oxygen gradient
(~100 to 40 mmHg)– Most binds with Hb (~97%)– Some dissolved in plasma (3%)
• Oxygen content of blood (CaO2)CaO2=1.34*[Hb]*(%sat of Hb) + 0.003 * PaO2
CaO2 = 1.34 * (15mg/dl)*(.98) + 0.003* (100mmHg)
CaO2 = ~20 ml/dl
[Hb]= hemoglobin concentration
PaO2 = partial pressure of oxygen

Diffusion of gases: Lung

Pulmonary diffusion• Diffusion of gases through tissues (gel)• Major determinants
– Partial pressure difference (major)– Solubility of the gas (minor)
• Gases of lower solubility typically have greater partial pressure gradients
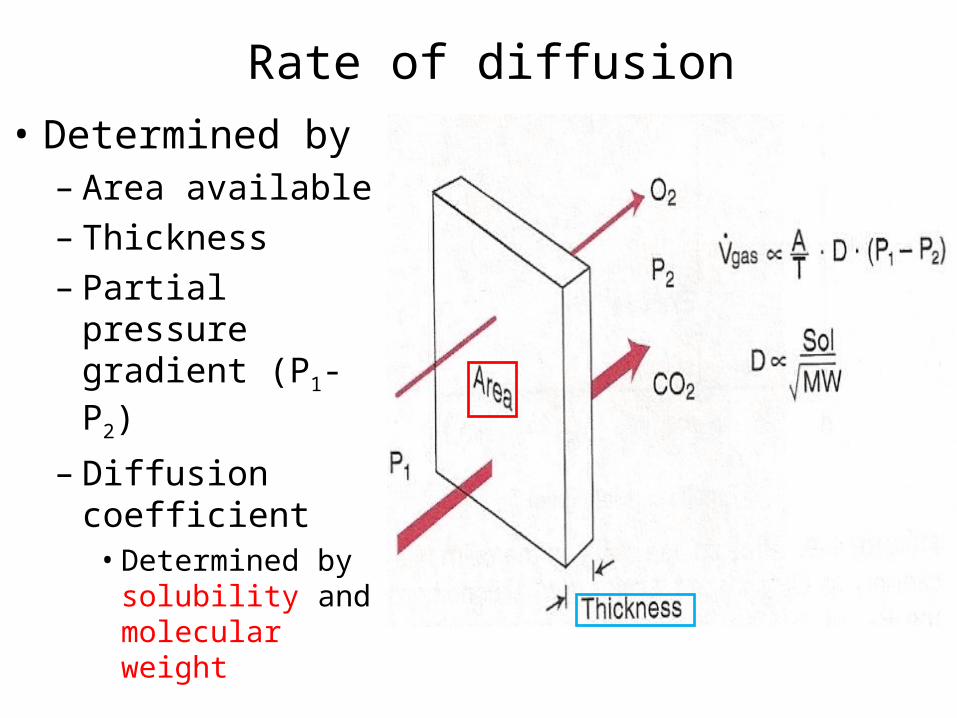
Rate of diffusion
• Determined by– Area available– Thickness– Partial pressure
gradient (P1-P2)
– Diffusion coefficient
• Determined by solubility and molecular weight

Rate of diffusion
• CO2 is slightly larger than O2 (MW; 44 vs 32 g/mol)
• CO2 has a much higher solubility coefficient (0.57 vs 0.024)
• Thus, CO2 has a greater relative diffusion coefficient (~20 x higher)
• Thus, O2 needs a larger pressure gradient to “force” itself across biological membranes

Arterial blood gas homeostasis
• Maintenance of blood gases (PaO2 and PaCO2) very important– Keep driving pressure
for CO2 and O2 high
– Driving pressure is the difference between arterial and venous pressure (PaO2-PvO2)
– Note that gradients increase with exercise

Oxygen transport• Oxygen content• CaO2 = 1.34[Hb]*(%sat) + 0.003 * PaO2
• Cardiac output (Qc) = HR * stroke volume
– Thus, total oxygen transport capacity (or delivery) is Qc*CaO2 or Qo2
• Qo2 is a measure of how much oxygen is circulated around by the heart in one minute– So, if CaO2 = 20 ml/dl and
Qc equals 30 L/min
– Qo2 = 30 * 0.2 or
– Qo2 = 6L/min
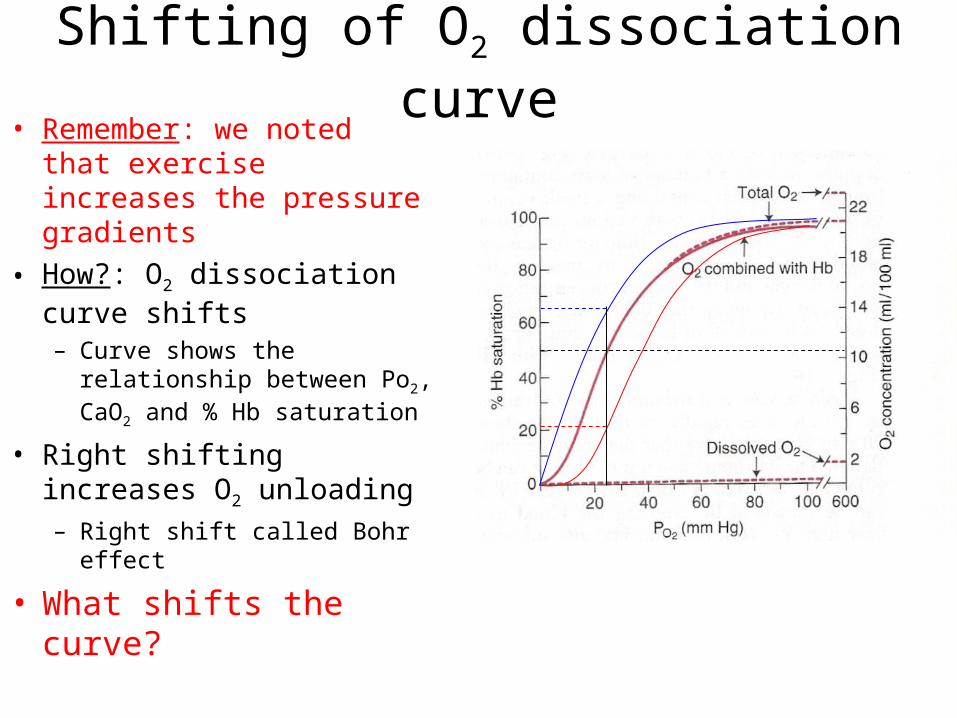
Shifting of O2 dissociation curve• Remember: we noted that
exercise increases the pressure gradients
• How?: O2 dissociation curve shifts– Curve shows the relationship
between Po2, CaO2 and % Hb saturation
• Right shifting increases O2 unloading– Right shift called Bohr effect
• What shifts the curve?

Effects of Co2 and pH on O2 transport
• The shape of the O2 dissociation curve is altered by 4 variables– pH
• < 7.4 = right shift• >7.4 = left shift
– Temperature• >38C = right shift• <38C = left shift
– Co2
• >40 mmHg = right shift• <40 mmHg = left shift
– 2,3 DPG (diphosphoglycerate)
• Altitude increases this

Co2 transport
• Co2 must be transported from tissues to blood and lungs for removal
• Carried in 3 ways– Bound to Hb (carbamino
compounds) (15-20%)– Dissolved in plasma (5-
10%)
– As bicarbonate (HCO3-),
~70%
Co2 transport
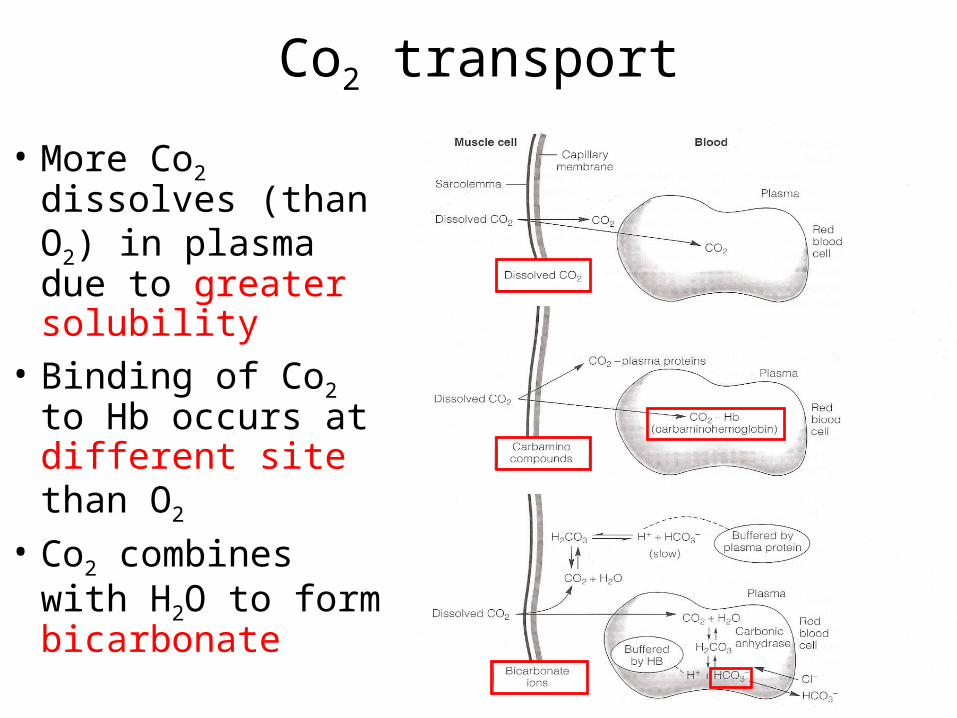
• More Co2 dissolves (than O2) in plasma due to greater solubility
• Binding of Co2 to Hb occurs at different site than O2
• Co2 combines with H2O to form bicarbonate

Co2 content
• Amount of Co2 carried in the blood depends upon Pco2
• Unlike oxygen, the Co2 curve is linear over a much greater range
• Thus, as Co2 production increases– greater driving pressure
(from tissue to blood)– As Co2 is extremely
soluble, this increases Co2 transport (No upper limit)

• When Co2 increases in blood– Shifts O2 curve to right– Facilitates unloading
of O2 at the tissues– Called Bohr effect
• When O2 falls– Shifts Co2 curve up
and right– Facilitates greater Co2
loading– Called Haldane effect
• Thus, at the level of the tissue, high CO2 facilitates unloading of O2 which allows greater amount of CO2 to be carried in blood
• At the lung, high O2 forces CO2 from Hb (and plasma) and it is then exhaled
Effect of O2 on Co2 transport (and vice versa)

Arterial blood gases• Note how
ventilation and PaCo2 inversely mirror each other
• Note also the effect on pH
• Major function of the ventilatory system is to rid the body of Co2 and control pH
• VA = VCo2/PaCo2

Buffering of metabolic acids• pH is a measure if the
acidity of the blood• Several sources of
acid are during exercise– Lactic acid (HLa)– Carbon dioxide
• These cause a fall in pH
– Bicarbonate is a very effective buffer
• A buffer helps to prevent a change in pH pK: Dissociation constant. pH at
which acid (or base) is 50% dissociated (50% acid and 50% base)

Buffering of metabolic acids• Lactic acid produced
– HLa → La- + H+
– H+ + HCO3- → H2CO3 → H2O + CO2 (exhaled)
• Co2 produced
– CO2 + H2O → H2CO3 → HCO3- + H+ (reverses at lung)
• pH– Negative logarithm of the hydrogen concentration
– pH = pk for HCO3-+ log [base/acid)
– pH = 6.1 + log [HCO3-/(pCO2 *0.03)] (Henderson-Hasselbalch eq.)
– pH = 6.1 + log [24 /1.2)– pH = 6.1 + 1.3– pH = 7.4
Control of pH
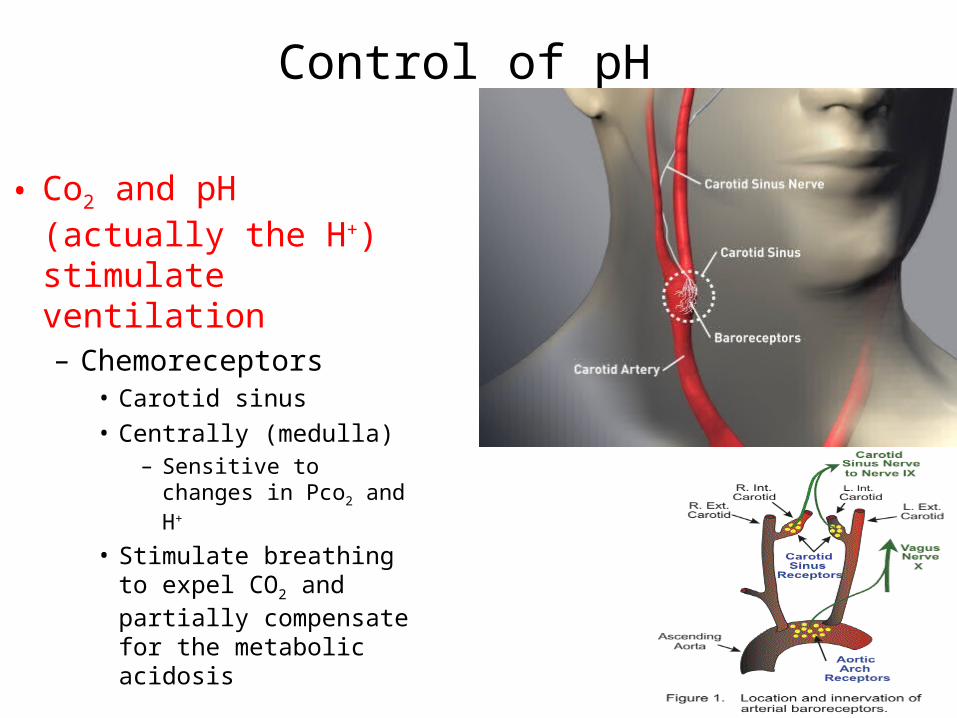
• Co2 and pH (actually the H+) stimulate ventilation– Chemoreceptors
• Carotid sinus• Centrally (medulla)
– Sensitive to changes in Pco2 and H+
• Stimulate breathing to expel CO2 and partially compensate for the metabolic acidosis

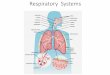
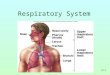
Ventilation• Gross Anatomy
– Pharynx– Trachea– Bronchus– Alveolus

Ventilation• Ventilation
– Moves air into and out of lung
• Two separate areas of lung
– Conducting zone– Respiratory zone
– Conducting zone• Network of tubes whose
function is movement of air
– Trachea and Bronchi
– Respiratory zone• Large, thin area where
gas exchange occurs– Respiratory
bronchioles and alveolar ducts

Ventilatory mechanics
• Diaphragm– Main muscle of ventilation– Only skeletal muscle
necessary for life• Accessory muscles
– Intercostals• External
– Inspiration• Internal
– Expiration
– Sternocleidomastoid, Scalenes
• Inspiration– Abdominal muscles
• Expiration

• Note how much ventilation can increase– Due to large
increases in tidal volume and frequency
– Increases in tidal volume (VT) largely due to accessory muscles
– Increases in frequency (f) due to diaphragm
Ventilatory volumes
Dead space and alveolar ventilation
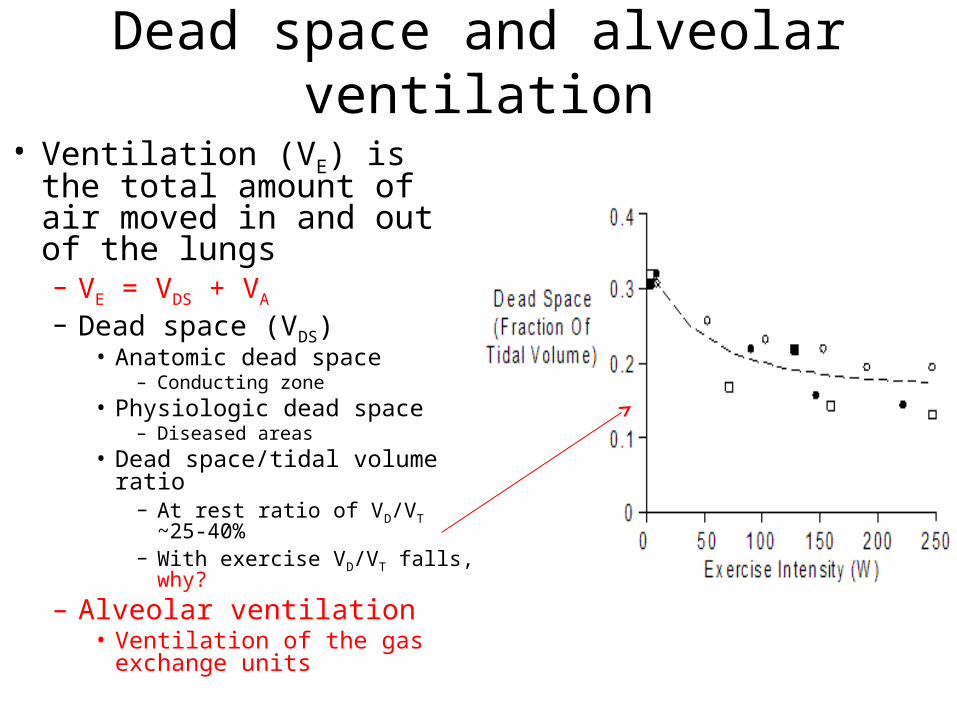
• Ventilation (VE) is the total amount of air moved in and out of the lungs– VE = VDS + VA
– Dead space (VDS)• Anatomic dead space
– Conducting zone• Physiologic dead space
– Diseased areas• Dead space/tidal volume ratio
– At rest ratio of VD/VT ~25-40%
– With exercise VD/VT falls, why?
– Alveolar ventilation• Ventilation of the gas
exchange units

Static lung volumes• Volumes and capacities
– Volume: single measure• Residual volume (RV)
– The amount of air in the lung after a maximal expiration
• Expiratory reserve volume (ERV)– The amount by which you can increase expiration after a normal exhalation
• Inspiratory reserve volume (IRV)– The amount by which you can increase inspiration after a normal inspiration
• Tidal volume (VT)– The volume of a normal breath
• Total lung capacity (TLC)– RV, ERV, VT and IRV
• Vital capacity– ERV, VT and IRV
• Functional residual capacity– RV, ERV
• Where humans breath from
• Inspiratory capacity– VT, IRV


Composition of Alveolar gases
100% oxygen
Air breathing; no water or CO2
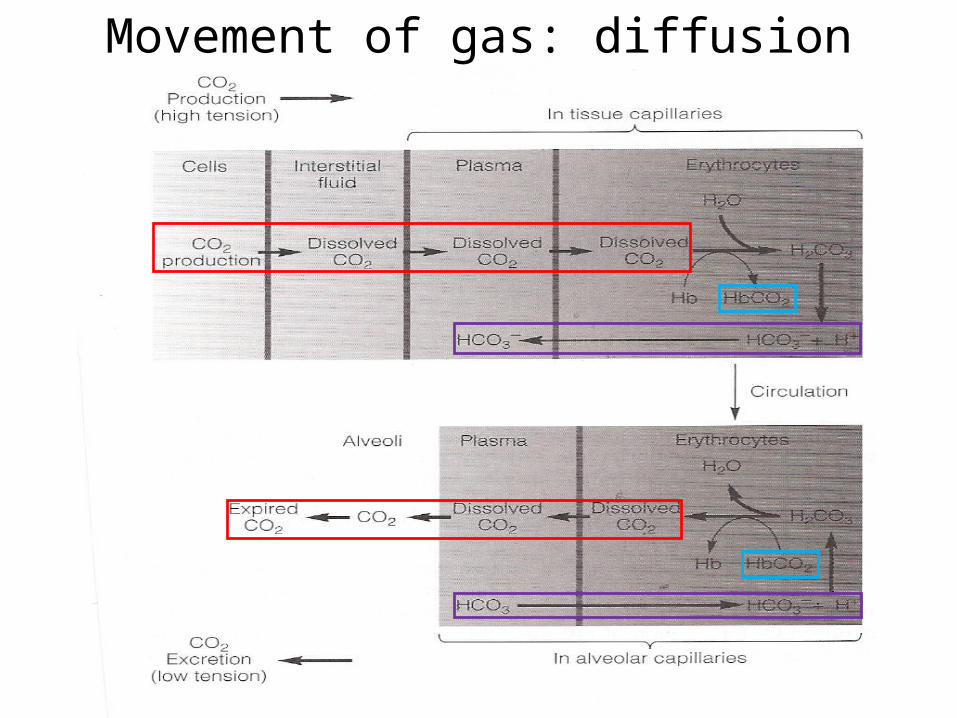
Movement of gas: diffusion

Diffusion• Oxygen
– Breathed into lungs– Diffuses across blood gas
barrier– Binds with hemoglobin
(97%)– Dissolved in plasma (3%)– Circulated to tissues– Diffuses into tissues– Binds with myoglobin
• Keeps oxygen pressure homogeneous within tissues
– Utilized in mitochondria
Mb

Transit time• Capillary blood volume
(Vc)– The blood that is in the
capillaries at one instant in time
• Transit time– the ratio of VC/blood flow
• VC =~70 ml• Qc = 100 ml/s• TT = 0.7 sec• More than adequate for
equilibration of blood gases
• Note that CO2 equillibrates MUCH faster than O2; why?

Control of ventilation
• Respiratory control center– Brainstem
• Medulla• Pons
• Feed forward– Central command
• Feedback– Peripheral and
central chemoreceptors

Central and peripheral control• Feed forward
– Sometimes called “central command”– Co-activation of cardiovascular, ventilatory and
musculoskeletal systems
• Central chemoreceptors– Sensitive to changes in pH
– Caused by Co2 as H+ cannot cross Blood brain barrier
• CO2 + H2O H2CO3 HCO3- + H+
• Peripheral chemoreceptors– Carotid sinus– Muscle metaboreceptors
• Both sensitive to changes in pH, PCO2 and PO2 (particularly at high atltitude)
• Peripheral mechanoreceptors– Sensitive to limb movement

Feed forward 1
1Peripheral3
Peripheral3
2
3 & 4
Central
Peripheral chemoreceptors and mechanoreceptors