Embed Size (px)
Citation preview

Venous Thromboembolism (VE)- Deep Vein Thrombosis
(DVT) and Pulmonary Embolus (PE)
Victoria E. Judd M.D.


Objectives
• Discuss common presentation of Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)
• Describe evidence-based diagnostic and therapeutic strategies for DVT/PE
• Identify when to screen for a hypercoaguable state

Causes of Thromboembolism
• Inherited
• Acquired

Inherited VE
Inherited thrombophilia • Factor V Leiden mutation• Prothrombin gene mutation• Protein S deficiency• Protein C deficiency• Antithrombin (AT) deficiency• Rare disorders • Dysfibrinogenemia

Other Plasma Factors
• In a single, large, population-based case control study performed in the Netherlands, a two to threefold increased risk for a first episode of venous thrombosis was found for elevated levels of a number of plasma components, coagulant factors, and inflammatory chemokines.

Other Plasma Factors
• Plasma factor IX antigen • Plasma factor XI antigen • Thrombin activatable fibrinolysis inhibitor
(TAFI) • Interleukin 8• Fibrinogen• Low levels of tissue factor pathway
inhibitor • Low plasma fibrinolytic activity • Elevated plasma fibronectin levels

Acquired VE
• Malignancy• Presence of a central venous catheter• Surgery, especially orthopedic• Trauma• Pregnancy• Oral contraceptives• Hormone replacement therapy

Categories of risk for venous
thromboembolism in surgical patients Low risk:Minor surgery in patients <40 years of age with no additional risk factors present*
• Risk of calf DVT: 2 percent• Risk of proximal DVT: 0.4 percent• Risk of clinical PE: 0.2 percent• Risk of fatal PE: <0.01 percent

Categories of risk for venous thromboembolism in surgical patients
Moderate risk:Minor surgery in patients with additional risk factor present*, or Surgery in patients aged 40-60 with no additional risk factor
• Risk of calf DVT: 10-20 percent• Risk of proximal DVT: 2-4 percent• Risk of clinical PE: 1-2 percent• Risk of fatal PE: 0.1-0.4 percent

Categories of risk for venous thromboembolism in surgical patients
High risk:Surgery in patients >60, orSurgery in patients aged 40-60 with additional risk factor*
• Risk of calf DVT: 20-40 percent• Risk of proximal DVT: 4-8 percent• Risk of clinical PE: 2-4 percent• Risk of fatal PE: 0.4-1.0 percent

Categories of risk for venous thromboembolism in surgical patients
Highest risk:Surgery in patients >40 with multiple risk factors*, orHip or knee arthroplasty, hip fracture surgery, orMajor trauma, spinal cord injury
• Risk of calf DVT: 40-80 percent• Risk of proximal DVT: 10-20 percent• Risk of clinical PE: 4-10 percent• Risk of fatal PE: 0.2-5 percent

Categories of risk for venous thromboembolism in surgical patients
• * Additional risk factors include one or more of the following: advanced age, cancer, prior venous thromboembolism, obesity, heart failure, paralysis, or presence of a molecular hypercoagulable state (e.g., protein C deficiency, factor V Leiden).
• Data from Geerts, WH, et al. Chest 2004; 126:3385.

Acquired VE
• Oral contraceptive pills that contain third-generation progestins are the most important cause of thrombosis in young women.
• The risk of thrombosis increases within four months of the initiation of therapy and is unaffected by duration of use.
• The risk decreases to previous levels within three months of cessation.
• An increased risk for VTE has also been found in women using contraceptive transdermal patches and ring.

Acquired VE
• Tamoxifen, Bevacizumab, Thalidomide, Lenalidomide
• Immobilization• Congestive failure• Antiphospholipid antibody syndrome• Myeloproliferative disorders • Polycythemia vera • Essential thrombocythemia • Paroxysmal nocturnal hemoglobinuria

Acquired VE
• Inflammatory bowel disease• Nephrotic syndrome• Hyperviscosity • Waldenstrom's macroglobulinemia • Multiple myeloma • Marked leukocytosis in acute leukemia• Sickle cell anemia• HIV/AIDS

Causes of Thromboembolism
• Fifty percent of thrombotic events in patients with inherited thrombophilia are associated with the additional presence of an acquired risk factor (e.g., surgery, prolonged bed rest, pregnancy, oral contraceptives).

Causes of Thromboembolism
• Some patients have more than one form of inherited thrombophilia or more than one form of acquired thrombophilia and appear to be at even greater risk for thrombosis.

Causes of Thromboembolism
• In a population-based study of the incidence of venous thromboembolism (VTE), 56 percent of the patients had three or more of the following six risk factors present at the time of VTE:

Causes of Thromboembolism
• >48 hours of immobility in the preceding month
• Hospital admission• Surgery• Malignancy• Infection in the past three months• Current hospitalization

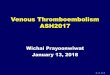
Incidence of pulmonary embolism
according to distance traveled by air

Incidence of pulmonary embolism
according to distance traveled by air • This figure indicates the incidence of
pumonary embolism per million passenger arrivals, arranged according to flight distance in kilometers. Error bars indicate 95 percent confidence limits. To convert kilometers to miles, multiply by 0.62.
• Data from Lapastolle, F, et al. N Engl J Med 2001;
345:779.



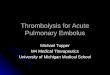
Seasonal variation in venous
thromboembolism

Seasonal variation in venous
thromboembolism • Depicted are the monthly percentage
variations in French hospital admissions for deep vein thrombosis and pulmonary embolism. Hospital admissions for venous thromboembolism were most frequent in the winter and least frequent in the summer.
• Reproduced with permission from: Boulay, F, Berthier, F, Schoukroun, G, et al. Seasonal variations in hospital admission for deep venous thrombosis and pulmonary embolism: analysis of discharge data. BMJ 2001; 323:601. Copyright © 2001, BMJ.

Risks Factors for DVT
• The risk of thrombosis is increased in all forms of major injury.
• In one study of 716 patients admitted to a regional trauma unit, DVT in the lower extremities was found in 58 percent of patients with adequate venographic studies; 18 percent had proximal vein thrombosis.

Risks factors for DVT
Thrombi were detected in: • 54 percent of patients with major head
injuries• 61 percent of patients with pelvic
fracture• 77 percent of patients with tibial
fracture• 80 percent of those with femoral
fracture.

Risk Factors for DVT
• Minor injuries — A large population-based study investigated the VTE risk following a minor injury (i.e., one not requiring surgery, a plaster cast, hospitalization, or extended bed rest at home for at least four days).
• A minor injury occurring in the preceding 3 to 4 weeks was associated with a 3- to 5-fold increase in DVT risk.
• In carriers of factor V Leiden, this risk was increased 50-fold.

Risks Factors for DVT
• Intravenous drug use — Direct trauma, irritation, and infection may be responsible for the high incidence of DVT noted in young drug users who inject these agents directly into their femoral veins.

Risk Factors for DVT
• Pregnancy — Pregnancy is associated with an increased risk of thrombosis that may be due in part to obstruction of venous return by the enlarged uterus, as well as the hypercoagulable state associated with pregnancy.
• Estimates of the age-adjusted incidence of VTE range from 5 to 50 times higher in pregnant versus non-pregnant women.

Pathophysiology
• VIRCHOW'S TRIAD — A major theory delineating the pathogenesis of venous thromboembolism (VTE), often called Virchow's triad, proposes that VTE occurs as a result of:
• Alterations in blood flow (i.e., stasis) • Vascular endothelial injury • Alterations in the constituents of the
blood (i.e., inherited or acquired hypercoagulable state)

Deep Vein Thrombosis (DVT)
• The thrombotic risk associated with the inherited thrombophilias has been assessed in two ways: evaluation of patients with deep vein thrombosis, and evaluation of families with thrombophilia.

DVT
• In a Spanish study of 2132 consecutive unselected patients with venous thromboembolism, for example, 12.9 percent had an anticoagulant protein deficiency (7.3 percent with protein S, 3.2 percent with protein C, and 0.5 percent with antithrombin). An additional 4.1 percent had antiphospholipid antibodies (aPL).

Risks and incidence of a first episode of venous
thrombosis
• Adult subjects only.• Data from the Leiden
Thrombophilia Study.

Condition/risk factor(s) Relative risk
Incidence, percent per year
Normal 1 0.008Hyperhomocysteinemia (MTHFR 677T mutation)
2.5 0.02
Prothrombin gene mutation 2.8 0.02
Oral contraceptives 4 0.03
Factor V Leiden (heterozygous) 7 0.06
Oral contraceptives plus heterozygous factor V Leiden
35 0.29
Factor V Leiden (homozygous) 80 0.5-1.0

DVT
• Similar findings were noted in a series of 277 Dutch outpatients with deep vein thrombosis: 8.3 percent had an isolated deficiency of antithrombin, protein C, protein S, or plasminogen compared to 2.2 percent of controls.
• The incidence of a protein deficiency was only modestly greater in "high risk" patients with recurrent, familial, or juvenile onset deep vein thrombosis (9, 16, and 12 percent respectively).

DVT
• The overall 8 to 13 percent incidence of an isolated anticoagulant protein deficiency in patients with deep vein thrombosis does not include the contribution of factor V Leiden or the prothrombin gene mutation, now considered to be the most common causes of inherited thrombophilia.

DVT
• The Physicians' Health Study and the Leiden Thrombophilia Study found a 12 to 19 percent incidence of heterozygosity for the factor V Leiden mutation in patients with a first DVT (or pulmonary embolism in the Physicians' Health Study) compared to 3 to 6 percent in controls.

DVT
• The incidence reached 26 percent in the Physicians' Health Study in 31 men over the age of 60 with no identifiable precipitating factors.
• The incidence of the prothrombin gene mutation is approximately 6 to 8 percent in patients with deep vein thrombosis compared to 2 to 2.5 percent in controls.

DVT
• The total incidence of an inherited thrombophilia in subjects with a deep vein thrombosis ranges from 24 to 37 percent overall compared to about 10 percent in controls. Another 25 percent of patients appear to have elevated factor VIII levels, although it has not been proven that this is an inherited characteristic.

DVT
• There are a number of questions that arise when a patient is suspected of having deep vein thrombosis (DVT) of the lower extremity.

DVT
• What is the differential diagnosis and what are the possible risk factors for DVT?
• What is the best way to diagnose or exclude DVT?

DVT
• What is the appropriate initial therapy for DVT; when is hospitalization not required?
• What is the recommended long-term treatment for DVT (e.g., agents to use, monitoring the degree of anticoagulation, length of time treatment is needed)?

DVT
• When should one screen for the presence of a hypercoagulable state, not only in the patient, but also in family members?

DVT
INITIAL APPROACH • When approaching the patient with
suspected DVT of the lower extremity, it is important to appreciate that only a minority of patients actually have the disease and will require anticoagulation.

DVT
• This illustrates the importance of using validated algorithms to evaluate patients with suspected DVT, along with objective testing to establish the diagnosis.
• Given the potential risks associated with proximal lower extremity DVT that is not treated (e.g., fatal pulmonary emboli) and the potential risk of anticoagulating a patient who does not have a DVT (e.g., fatal bleeding), accurate diagnosis is essential.

DVT History
• Classic symptoms of DVT include swelling, pain, and discoloration in the involved extremity.
• There is not necessarily a correlation between the location of symptoms and the site of thrombosis.

DVT History
• Symptoms in the calf alone are often the presenting manifestation of significant proximal vein involvement, while some patients with whole leg symptoms are found to have isolated calf vein DVT.

DVT History
• A complete thrombosis history includes the age of onset, location of prior thromboses, and results of objective diagnostic studies documenting thrombotic episodes in the patient, as well as in any family members.
• A positive family history is particularly important, since a well documented history of venous thrombosis in one or more first-degree relatives strongly suggests the presence of a hereditary defect.

DVT History
• Recent potential precipitating conditions
• Underlying conditions: i.e. cancer, collagen-vascular disorders
• Medications

DVT Physical Exam
Special attention should be directed to:• The vascular system• Extremities (e.g., looking for signs of
superficial or deep vein thrombosis)• Chest• Heart• Abdominal organs• Skin (e.g., skin necrosis, livedo
reticularis).


DVT Physical Exam
• There may be pain and tenderness in the thigh along the course of the major veins ("painful deep vein syndrome").
• Tenderness on deep palpation of the calf muscles is suggestive, but not diagnostic.
• Homan's sign is unreliable.

DVT Physical Exam
• A 2005 meta-analysis of diagnostic cohort studies of patients with suspected DVT concluded the following concerning these physical findings:
• Only a difference in calf diameters (likelihood ratio, LR 1.8; 95% CI 1.5-2.2) was of potential value for ruling in DVT.

DVT Physical Exam
• Only absence of calf swelling (LR 0.67; 95% CI 0.58-0.78) and absence of a difference in calf diameters (LR 0.57; 95% CI 0.44-0.72) were of potential value for ruling out DVT
• Individual clinical features are poorly predictive of DVT when not combined in a formal prediction rule (e.g., Wells score, see below).

DVT Physical Exam
Many patients are asymptomatic; however, the history may include the following:
• Edema, principally unilateral, is the most specific symptom. Massive edema with cyanosis and ischemia (phlegmasia cerulea dolens) is rare.
• Leg pain occurs in 50% of patients, but this is entirely nonspecific. Pain can occur on dorsiflexion of the foot (Homans sign).

DVT Physical Exam
Homan’s sign • Discomfort in the calf muscles on forced
dorsiflexion of the foot with the knee straight has been a time-honored sign of DVT. However, this sign is present in less than one third of patients
with confirmed DVT. • The Homan’s sign is found in more than 50% of
patients without DVT and, therefore, is nonspecific.

DVT Physical Exam
-Tenderness occurs in 75% of patients but is also found in 50% of patients without objectively confirmed
DVT. -Clinical signs and symptoms of PE as the primary
manifestation occur in 10-50% of patients with confirmed DVT.
-The pain and tenderness associated with DVT does not usually correlate with the size, location, or extent of
the thrombus. -Warmth or erythema of skin can be present over the area
of thrombosis

DVT Physical Exam
o Superficial thrombophlebitis is characterized by the finding of a palpable, indurated, cordlike,
tender, subcutaneous venous segment.o Forty percent of patients with superficial thrombophlebitis without coexisting varicose
veins and with no other obvious etiology (e.g., intravenous catheters, intravenous drug abuse, soft
tissue injury) have an associated DVT.

DVT Differential Diagnosis
In one study of 160 consecutive patients with suspected DVT who had negative venograms, the following causes of leg pain were identified:
• Muscle strain, tear, or twisting injury to the leg — 40 percent
• Leg swelling in a paralyzed limb — 9 percent

DVT Differential Diagnosis
• Lymphangitis or lymph obstruction — 7 percent
• Venous insufficiency (reflux) — 7 percent
• Baker's cyst — 5 percent • Cellulitis — 3 percent • Knee abnormality — 2 percent • Unknown — 26 percent

DVT Diagnosis
• The clinical assessment of patients with suspected DVT is often difficult because of the interplay between risk factors and the
nonspecific nature of the physical findings.
• Clinicians have observed that a discordance is often present between the clinical
assessment and the results of objective testing.

DVT Diagnosis
• One report of 593 patients with suspected DVT validated a measure of pretest probability in conjunction with an algorithm designed to minimize the use of venography or repeat ultrasonography.
• The measure of pretest probability is referred to as the Wells score or Wells criteria for DVT probability:

DVT Diagnosis
• The Wells clinical prediction guide quantifies the pretest probability of DVT.
• The model enables providers to reliably stratify their patients into high-, moderate-, or low-risk categories.
• Combining this with the results of objective testing greatly simplifies the clinical workup of patients
with suspected DVT. • The Wells clinical prediction guide incorporates risk
factors, clinical signs, and the presence or absence of alternative diagnoses.

DVT Diagnosis
• For example, patients deemed to be at high risk for DVT may have a negative finding on duplex
ultrasonographic study. • In this case, the probability of DVT is still greater
than 20% when the known sensitivity, specificity, and negative likelihood ratio of duplex
ultrasonography are considered. • Having an objective method to determine pretest
probability simplifies clinical management.

Wells Score
• Paralysis, paresis, or recent orthopedic casting of a lower extremity (1 point)
• Recently bedridden for longer than three days or major surgery within the past four weeks (1 point)
• Localized tenderness in the deep vein system (1 point)
• Swelling of an entire leg (1 point)

Wells Score
• Calf swelling 3 cm greater that the other leg, measured 10 cm below the tibial tuberosity (1 point)
• Pitting edema greater in the symptomatic leg (1 point)
• Collateral non-varicose superficial veins (1 point)

Wells Score
• Active cancer or cancer treated within six months (1 point)
• Alternative diagnosis more likely than DVT (e.g., Baker's cyst, cellulitis, muscle damage, post phlebitic syndrome, inguinal lymphadenopathy, external venous compression (-2 points)

Clinical Parameter Score Score
Active cancer (treatment ongoing, or within 6 mo or palliative) +1
Paralysis or recent plaster immobilization of the lower extremities +1
Recently bedridden for >3 d or major surgery <4 wk +1
Localized tenderness along the distribution of the deep venous system +1
Entire leg swelling +1
Calf swelling >3 cm compared with the asymptomatic leg +1
Pitting edema (greater in the symptomatic leg) +1
Previous DVT documented +1
Collateral superficial veins (nonvaricose) +1
Alternative diagnosis (as likely or greater than that of DVT) -2
Total of Above Score
High probability >3
Moderate probability 1 or 2
Low probability <0

Reference for Modified Wells Score
• Adapted from JAMA. 1998 Apr 8;279(14):1094-9.
• Value of assessment of pretest probability of deep-vein thrombosis in clinical
management. Wells PS; Anderson DR; Bormanis J; Guy F; Mitchell M; Gray L; Clement C; Robinson KS; Lewandowski B. Lancet 1997 Dec 20-27;350(9094):1795-8.

DVT Diagnosis
• DVT was documented in 3, 17, and 75 percent of patients with low, moderate, and high pretest probabilities, respectively.
• Serial ultrasonography was required in 28 percent and venography in 6 percent of patients; venous thromboembolism was diagnosed during a three month follow-up period in only 0.6 percent of patients thought not to have a DVT by this algorithm.


DVT D-dimer
• Recent interest has focused on the use of D-dimer in the diagnostic approach to DVT.
• D-dimer fibrin fragments are present in fresh fibrin clot and in fibrin degradation products of cross-linked fibrin.
• Monoclonal antibodies specific for the D-dimer fragment are used to differentiate fibrin-specific clot from non–cross-linked fibrin and from fibrinogen.
• These specific attributes of the D-dimer antibodies account for their high sensitivity for venous
thromboembolism.

DVT D-dimer
• D-dimer level may be elevated in any medical condition where clots form.
• D-dimer level is elevated in trauma, recent surgery, hemorrhage, cancer, and sepsis.
• Many of these conditions are associated with higher risk for DVT.
• The D-dimer assays have low specificity for DVT; therefore, they should only be used to rule out
DVT, not to confirm the diagnosis of DVT.

Medical Conditions Associated With an Elevated D-dimer
Arterial thromboembolic disease • Myocardial infarction • Stroke • Acute limb ischemia • Atrial fibrillation • Intracardiac thrombus

Medical Conditions Associated With an Elevated D-dimer
Venous thromboembolic disease • Deep vein thrombosis • Pulmonary embolism • Disseminated intravascular
coagulation• Preeclampsia and eclampsia
Abnormal fibrinolysis; use of thrombolytic agents

Medical Conditions Associated With an Elevated D-dimer
Systemic inflammatory response syndromeVasoocclusive episode of sickle cell diseaseSevere liver disease (decreased clearance)Malignancy

Medical Conditions Associated With an Elevated D-dimer
Renal disease • Nephrotic syndrome (e.g., renal
vein thrombosis) • Acute renal failure • Chronic renal failure and
underlying cardiovascular disease Normal pregnancyVenous malformations

DVT D-dimer
• D-dimer levels remain elevated in DVT for about 7 days.
• Patients presenting late in the course, after clot organization and adherence have occurred, may have
low levels of D-dimer. • Similarly, patients with isolated calf vein DVT may
have a small clot burden and low levels of D-dimer that are below the analytic cut-off value of the assay.
• This accounts for the reduced sensitivity of the D-dimer assay in the setting of confirmed DVT.

DVT D-dimer
• Many different D-dimer assays are available, with varying sensitivities and specificities.
• The assays are not standardized. • They incorporate different monoclonal antibodies to the D-
dimer fragment. • Results may be reported quantitatively or qualitatively.
• Different units may be used.• Some assay results are reported as fibrinogen equivalent
units (FEU) and others in nanograms per milliliter (ng/mL).
• The results of one assay cannot be extrapolated to another.

DVT D-dimer
• Most studies have confirmed the clinical utility of D-dimer testing, and most clinical
algorithms incorporate their use.
• Providers should know their lab's D-dimer assay

DVT D-dimer
D-dimer results should be used as follows: o A negative D-dimer assay result rules out DVT in
patients with low-to-moderate risk and a Wells DVT score less than 2.
o All patients with a positive D-dimer assay result and all patients with a moderate-to-high risk of
DVT (Wells DVT score >2) require a diagnostic study (duplex ultrasonography).

DVT D-dimer
• A D-dimer level less than 200 to 500 ng/mL by ELISA or a negative SimpliRED assay in conjunction with a low clinical probability of DVT appears to be useful and cost- effective in excluding DVT without the need for an ultrasound examination.

DVT D-dimer
• This has been shown to hold in populations at high risk of having DVT, such as those with malignancy, as well as in populations in which the Wells score and the D-dimer may have reduced specificity, such as in the elderly.

DVT D-dimer
• The pretest probability of DVT is determined from the Wells score and a D-dimer test is performed.

DVT D-dimer
• For those with a "low probability" score and a negative D-dimer, DVT is effectively ruled out.
• If the D-dimer test is positive, ultrasound is performed to rule out DVT.

DVT D-dimer
• For those in whom DVT is likely (i.e., Wells score ≥1) ultrasound is performed in all patients to rule out DVT.
• For the separate group in which the D-dimer test was positive and the initial ultrasound negative, a repeat ultrasound is performed one week later to rule out DVT.

Limitations of the Wells Score
• A meta-analysis of 51 studies has shown that the overall assessment of clinical probability of DVT by use of the Wells score is more useful than any of the individual components comprising the score, with a negative likelihood ratio (0.25, 95% CI 0.21-0.29) similar to that of an empirical assessment.

Limitations of the Wells Score
• Nevertheless, when the population to be assessed contained a large percentage of elderly patients or those with a prior DVT or other comorbidities, as might occur in a primary care setting, the performance of the Wells criteria was reduced.
• Therefore, it seems prudent that the Wells criteria are used to complement rather than displace the clinician's empirical assessment.

Diagnosis of DVT
• In most circumstances, compression ultrasonography is the noninvasive approach of choice for the diagnosis of patients with suspected DVT.
• If unavailable, impedance plethysmography with serial studies is an acceptable alternative.
• One exception noted above is that impedance plethysmography is preferred for possible recurrent DVT since it normalizes more quickly after a previous episode than compression ultrasonography.

Compression Ultrasonography
The diagnosis of venous thrombosis using compression ultrasonography is made by the findings such as:
• Abnormal compressibility of the vein • Abnormal Doppler color flow • The presence of an echogenic band • Abnormal change in diameter during
the Valsalva maneuver

Compression Ultrasonography
• Prospective studies have demonstrated that lack of compressibility of a vein with the ultrasound probe is highly sensitive (>95 percent) and specific (>95 percent) for proximal vein thrombosis.

Compression Ultrasonography
• Color flow imaging, in addition to duplex Doppler ultrasound, is a less demanding study and is also highly accurate for the diagnosis of above the knee DVT.

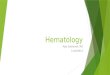
Duplex-Doppler ultrasound image of an acute superficial femoral vein thrombosis
(labeled "V")
Blue color indicates venous blood flow and red indicates arterial blood flow (labeled "A"). Echogenic white speckles are seen in the vein which was non-compressible with the ultrasound probe.

Compression Ultrasonography
• In comparison, the presence of an echogenic band, although sensitive for DVT, has a specificity of only about 50 percent.
• The variation of venous size with the Valsalva maneuver has a low sensitivity and specificity for the presence of DVT and is not performed in many centers.

Compression Ultrasonography
• Serial studies need to be performed when the initial test is negative; approximately 2 percent of patients with an initially negative ultrasound develop a positive study when retested seven days later.
• A single repeat study that is negative five to seven days after an initial negative study predicts a less than 1 percent likelihood of venous thromboembolism over months of follow-up.

Compression Ultrasonography
o Duplex ultrasonography is also helpful to differentiate venous thrombosis from
hematoma, Baker cyst, abscess, and other causes of leg pain and edema.
o Diagnostic accuracy varies depending on local expertise.

MRI
o MRI is the diagnostic test of choice for suspected iliac vein or inferior vena caval thrombosis when CT venography is contraindicated or technically
inadequate. o In the second and third trimester of pregnancy, MRI is more accurate than duplex ultrasonography
because the gravid uterus alters Doppler venous flow characteristics.
o Expense, lack of general availability, and technical issues limit its use.

Screening For A Hypercoaguable State
• A biologic risk factor for venous thrombosis can be identified in over 60 percent of Caucasian patients with idiopathic DVT. In addition, there is often more than one factor at play in a given patient.
• As an example, 50 percent of thrombotic events in patients with inherited thrombophilia are associated with an accompanying acquired risk factor (e.g., surgery, pregnancy, use of oral contraceptives).

Screening For A Hypercoaguable State
• There is currently no consensus regarding whom to test for inherited thrombophilia.
• The likelihood of identifying an inherited thrombophilia is increased several-fold by screening only patients with one or more of the following:

Screening For A Hypercoaguable State
• Initial thrombosis occurring prior to age 50 without an immediately identified risk factor (i.e., idiopathic or unprovoked venous thrombosis)
• A family history of venous thromboembolism

Screening For A Hypercoaguable State
• Recurrent venous thrombosis • Thrombosis occurring in unusual
vascular beds such as portal, hepatic, mesenteric, or cerebral veins
• A history of warfarin-induced skin necrosis, which suggests protein C deficiency

Screening For A Hypercoaguable State
• Patients at increased risk for inherited thrombophilia can be identified.
• There is no clear clinical value to screening for the following reasons:
• Even if a hypercoagulable workup uncovers abnormalities predisposing to VTE, the strongest risk factor for VTE recurrence is the prior VTE event itself, particularly if idiopathic.

Screening For A Hypercoaguable State
• Patients with idiopathic VTE, whether or not they have an identifiable inherited thrombophilia, are at high risk for recurrence (as high as 7 to 8 percent per year in some studies) after warfarin is discontinued, at least for the first few years after the event.
• Thus, the presence or absence of an inherited thrombophilia will usually not change the decision regarding length of warfarin therapy.

Screening For A Hypercoaguable State
• Screening information can be used to identify family members with an inherited thrombophilia, but anticoagulant prophylaxis is rarely recommended in asymptomatic affected family members outside of high risk situations.

Screening For A Hypercoaguable State
Screening test interference — • A number of factors can interfere
with screening tests for thrombophilia.
• Therefore, it is generally best not to undertake testing at the time of presentation with VTE.

Screening For A Hypercoaguable State
Confounding Factors • Acute thrombosis• Heparin therapy• Coumadin therapy

Treatment of DVT
The primary objectives of treatment of DVT are to prevent and/or treat the following complications:
• Prevent further clot extension • Prevention of acute pulmonary
embolism

Treatment of DVT
• Reducing the risk of recurrent thrombosis • Treatment of massive iliofemoral
thrombosis with acute lower limb ischemia and/or venous gangrene (i.e., phlegmasia cerulea dolens)
• Limiting the development of late complications, such as the postphlebitic syndrome, chronic venous insufficiency, and chronic thromboembolic pulmonary hypertension.

Treatment of DVT
• Anticoagulant therapy is indicated for patients with symptomatic proximal DVT, since pulmonary embolism will occur in approximately 50 percent of untreated individuals, most often within days or weeks of the event.

Treatment of DVT
• The use of thrombolytic agents, surgical thrombectomy, or percutaneous mechanical thrombectomy in the treatment of venous thromboembolism must be individualized.
• Patients with hemodynamically unstable PE or massive iliofemoral thrombosis (i.e., phlegmasia cerulea dolens), and who are also at low risk to bleed, are the most appropriate candidates for such treatment.


Treatment of DVT
• Inferior vena caval filter placement is recommended when there is a contraindication to, or a failure of, anticoagulant therapy in an individual with, or at high risk for, proximal vein thrombosis or PE.

Treatment of DVT
• It is also recommended in patients with recurrent thromboembolism despite adequate anticoagulation, for chronic recurrent embolism with pulmonary hypertension, and with the concurrent performance of surgical pulmonary embolectomy or pulmonary thromboendarterectomy.



Treatment of DVT
• Oral anticoagulation with warfarin should prolong the INR to a target of 2.5 (range: 2.0 to 3.0).
• If oral anticoagulants are contraindicated or inconvenient, long-term therapy can be undertaken with either adjusted-dose unfractionated heparin, low molecular weight heparin, or fondaparinux.

Treatment of DVT
• The general medical management of the acute episode of DVT is individualized.
• Once anticoagulation has been started and the patient's symptoms (i.e., pain, swelling) are under control, early ambulation is advised.

Treatment of DVT
• During initial ambulation, and for the first two years following an episode of VTE, use of an elastic compression stocking has been recommended to prevent the postphlebitic syndrome.












PE classification
• Acute vs. chronic
• Massive vs. submassive

PE Classification
• A saddle PE is a PE that lodges at the bifurcation of the main pulmonary artery into the right and left pulmonary arteries.
• Most saddle PE are submassive. • In a retrospective study of 546
consecutive patients with PE, 14 (2.6 percent) had a saddle PE.
• Only two of the patients with saddle PE had hypotension.

PE Epidemiology
• In a study of more than 42 million deaths that occurred over a 20-year duration, almost 600,000 patients (approximately 1.5 percent) were diagnosed with PE.
• PE was the presumed cause of death in approximately 200,000.
• This study certainly underestimates the true incidence and prevalence of PE, since more than half of all PE are probably undiagnosed.

PE Prognosis
• PE is associated with a mortality rate of approximately 30 percent without treatment, primarily due to recurrent embolism.
• However, accurate diagnosis followed by effective anticoagulant therapy decreases the mortality rate to 2 to 8 percent.

PE Prognosis
Poor Prognosis:
• Elevated Brain Natriuretic Peptide (BNP)
• Right Ventricular dysfunction
• Hypotension
• RV thrombus
• Elevated Troponin I

PE Pathophysiology
• Most PE arise from thrombi in the deep venous system of the lower extremities. However, they may also originate in the right heart or the pelvic, renal, or upper extremity veins.

PE Pathophysiology
• Iliofemoral veins are the source of most clinically recognized PE.
• It is estimated that 50 to 80 percent of iliac, femoral, and popliteal vein thrombi (proximal vein thrombi) originate below the popliteal vein (calf vein thrombi) and propagate proximally.
• The remainder arise within the proximal veins.• Fortunately, most calf vein thrombi resolve
spontaneously and only 20 to 30 percent extend into the proximal veins if untreated.

PE Pathophysiology
• After traveling to the lung, large thrombi may lodge at the bifurcation of the main pulmonary artery or the lobar branches and cause hemodynamic compromise.
• Smaller thrombi continue traveling distally and are more likely to produce pleuritic chest pain, presumably by initiating an inflammatory response adjacent to the parietal pleura.

PE Pathophysiology
• Only about 10 percent of emboli cause pulmonary infarction, usually in patients with preexisting cardiopulmonary disease.
• Most pulmonary emboli are multiple, with the lower lobes being involved in the majority of cases.

PE Pathophysiology
• Impaired gas exchange due to PE cannot be explained solely on the basis of mechanical obstruction of the vascular bed and alterations in the ventilation to perfusion ratio.
• Gas exchange abnormalities are also related to the release of inflammatory mediators, resulting in surfactant dysfunction, atelectasis, and functional intrapulmonary shunting.

PE Risk Factors
• PE is a common complication of deep vein thrombosis (DVT), occurring in more than 50 percent of cases with phlebographically confirmed DVT.
• This suggests that factors that promote the development of DVT also increase the risk for PE.

PE Additional Risks Factors in Women
• Obesity (BMI ≥29 kg/m2)• Heavy cigarette smoking (>25
cigarettes per day)• Hypertension

PE Symptoms
• Specific symptoms and signs are not helpful diagnostically because their frequency is similar among patients with and without PE.
• In the Prospective Investigation of Pulmonary Embolism Diagnosis II (PIOPED II), the following frequencies of symptoms and signs were noted among patients with PE who did not have preexisting cardiopulmonary disease:

PE Symptoms
• Dyspnea at rest or with exertion (73 percent). The onset of dyspnea was usually within seconds (46 percent) or minutes (26 percent).
• Pleuritic pain (44 percent)• Cough (34 percent)• >2-pillow orthopnea (28 percent)• Calf or thigh pain (44 percent)• Calf or thigh swelling (41 percent),• Wheezing (21 percent)

PE Signs
The most common signs were • Tachypnea (54 percent)• Tachycardia (24 percent)• Rales (18 percent)• Decreased breath sounds (17 percent)• An accentuated pulmonic component of
the second heart sound (15 percent),• Jugular venous distension (14 percent)

PE DVT Symptoms
• Symptoms or signs of lower extremity deep venous thrombosis (DVT) were common (47 percent).
• They included edema, erythema, tenderness, or a palpable cord in the calf or thigh.

PIOPED II
• Clinical characteristics of patients with acute pulmonary embolism: data from PIOPED II. Stein PD; Beemath A; Matta F; Weg JG; Yusen RD; Hales CA; Hull RD; Leeper KV Jr; Sostman HD; Tapson VF; Buckley JD; Gottschalk A; Goodman LR; Wakefied TW; Woodard PK. Am J Med. 2007 Oct;120(10):871-9.

PE Labs
Routine laboratory findings are nonspecific.
• Leukocytosis• An increased erythrocyte
sedimentation rate (ESR)• Elevated serum LDH or AST (SGOT)• Normal serum bilirubin.

PE Arterial Blood Gases (ABG’s)
• Arterial blood gas (ABG) measurements and pulse oximetry have a limited role in diagnosing PE.
• ABG’s usually reveal hypoxemia, hypocapnia, and respiratory alkalosis.

PE ABG’s
• Patients with room air pulse oximetry readings <95 percent at the time of diagnosis are at increased risk of in-hospital complications, including respiratory failure, cardiogenic shock, and death.

PE Chest X-Ray
• Radiographic abnormalities are common in patients with PE; however, they are not helpful diagnostically because they are similarly common in patients without PE.

PE Ventilation/Perfusion V/Q Scan
• Unfortunately, the combinations of clinical and lung scan probability that was found in most patients had a diagnostic accuracy of only 15 to 86 percent, which is insufficient to either confirm or exclude the diagnosis of PE.
• Additional testing is required in this situation.

PE Venous Ultrasound
• Lower extremity venous ultrasound is sometimes performed during the diagnostic evaluation of PE.
• The rationale is that venous thrombosis detected by ultrasound is treated similar to confirmed PE.

PE Venous Ultrasound
However, there are flaws to this approach:• False positive venous ultrasound studies (3
percent in one report) will result in the anticoagulation of some patients who do not have DVT or PE, thus subjecting them to unnecessary risk.
• Many patients with PE are likely to be missed. • In one report, only 29 percent of patients with
PE (determined by V/Q scan or pulmonary angiogram) had venous thrombosis detected by compression ultrasound.

PE D-dimer Sensitivity
• D-dimer levels are abnormal in approximately 95 percent of all patients with PE when measured by ELISA, quantitative rapid ELISA, or semi-quantitative rapid ELISA.

PE D-dimer Specificity
• D-dimer levels are normal in only 40 to 68 percent of patients without PE, regardless of the assay used.
• This is a consequence of abnormal D-dimer levels being common among hospitalized patients, especially those with malignancy or recent surgery.
• The specificity may decrease further with increasing patient age.

PE Spiral CT
• Due to its widespread availability, spiral (helical) CT scanning with intravenous contrast (i.e., CT pulmonary angiography or CT-PA) is being used increasingly as a diagnostic modality for patients with suspected PE.
• One of the most commonly cited benefits of CT-PA is the ability to detect alternative pulmonary abnormalities that may explain the patient's clinical presentation.

PE Spiral CT
• 83 percent of patients with PE had a positive CT-PA (i.e., sensitivity).
• Conversely, 96 percent of patients without PE had a negative CT-PA (i.e., specificity).
• Addition of venous-phase imaging improved the sensitivity (90 percent), while maintaining a similar specificity (95 percent).

PE Spiral CT
• The likelihood of PE in patients with a positive CT-PA and a high, intermediate, or low clinical probability was 96, 92, and 58 percent, respectively (i.e., positive predictive value).
• The likelihood that PE was absent in patients with a negative CT-PA and a low, intermediate, or high clinical probability was 96, 89, and 60 percent, respectively (i.e., negative predictive value).

PE Echocardiography
• Only 30 to 40 percent of patients with PE have echocardiographic abnormalities suggestive of acute PE.

Case 1
• A 22 year old thin, female student on OCP’s presents to your clinic with painless, right calf swelling
• She has elevated her leg for 2 days due to a right ankle sprain during a soccer game.
• No prior medical history, recent surgery, or weight change.
• She does not smoke and drinks rarely• On exam her right calf is 1.5 cm larger than the
left

Case 1
• She has 2-3 risk factors: (OCP, trauma, +/- immobolization)
• Her Wells score gives her a moderate risk for a DVT.
• A D-dimer test is done.

Case1
• She has a positive quantitative ELISA.
• An imaging study is done.

Case1
• Available imaging and ancillary tests:
– Compression US – first line test, high sens/spec
– Venography – gold standard
– MRI – Lower quality evidence only at present

Case 1
• Compression US negative
• Options include: – Venography or MRI– Serial compression US – single US done at 5-7
days reliably excludes calf-limited DVT– Follow clinically for resolution of symptoms –
riskier, no data supporting safety of this option

Case 1
• The patient elected to be followed clinically. She returned to clinic 3 days later with persistent swelling, but no new symptoms
• She was to return the following week, but instead you are called to the ER 10 days later after she presents with acute onset of dyspnea and pleuritic chest pain.

Case1
• Findings in the ER– Alert white female, mildly anxious– T 101, HR 105, RR 18– R LE edema and redness– Lungs clear to auscultation– ABG – mild respiratory alkalosis– CXR showing mild atelectasis
• D-dimer positive as before, troponin normal

Case 1
• Helical CT – segmental embolus• Therapy
– Enoxaparin 1mg/kg sq every 12 hours for 5 days
– Warfarin started day 1 at 5 mg a day
– CBC on day 3-5 and INR every day if inpatient
– May stop enoxaparin after 5 days if INR > 2.0
– Warfarin continued to keep INR at 2.5 (2.0-3.0 range) for ? 3 months

Case 1
• Anticoagulation same for DVT & PE
• Compression stockings prevent post-phlebitic syndrome
• Thrombolysis - risk/benefit uncertain; clinical outcomes generally not improved
• Vena cava filters - limited evidence and modest benefit