Embed Size (px)
Citation preview

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 167
Venous thromboembolism (VTE) is a major health concern because it increases morbidity and mortality after a surgical procedure. A number of well-defined, evidence-based guidelines are available delineating suitable use of prophylaxis to prevent deep vein thrombosis and pulmonary embolism. Despite the available literature, there are clear gaps between recommendations and clinical practice, affecting the incidence of VTE. Plastic surgeons underuse the sub-stantiated literature and risk stratification tools that are available to decrease the incidence of VTE in the office-based surgical setting because of fear of
bleeding or hematoma complications postoperatively. Venous thromboembolism creates an economic bur-den on both the patient and the healthcare system. The intent of this literature review is to determine existing VTE risk using assessment models available to aid in the implementation of protocols for VTE prevention, specifically for high-risk cosmetic surgical patients in office-based settings.
Keywords: Chemoprophylaxis, deep vein thrombosis, low-molecular-weight heparin, venous thromboembo-lism, plastic surgery.
Venous Thromboembolism Prophylaxis in Plastic Surgery: A Literature Review
Sergio Hernandez, DNP, CRNAJorge Valdes, DNP, CRNAMoises Salama, MD
Venous thromboembolism (VTE) refers to a continuum of disease ranging from deep venous thrombosis (DVT) to pulmonary embolus (PE). According to the Ameri-can College of Chest Physicians (ACCP),
approximately one-third of the 150,000 to 200,000 VTE-related deaths per year in the United States occur follow-ing surgery.1 In 2001, the American Society of Plastic Surgeons (ASPS) estimated 18,000 cases of DVT occur in plastic surgery annually, with an overall incidence of VTE in plastic surgery varying between 0.5% and 2%.2 Although the incidence rate in plastic surgery may seem low, it is postulated these numbers represent only patients who are symptomatic.3 Up to two-thirds of patients with VTE are clinically silent, leading to a substantial delay in diagnosis and treatment.4
Plastic surgery as a specialty stands to benefit from pre-vention of VTE because some authors have suggested that patients undergoing plastic surgery are at higher risk of VTE than typically perceived.5 Despite the data regarding the incidence of VTE and available risk stratification tools for prevention, the use of chemoprophylaxis in high-risk patients remains controversial in the plastic surgery com-munity because of fear of postoperative bleeding or hema-toma complications.3,6,7 Plastic surgeons traditionally rely on early ambulation and pneumatic compression devices to protect against DVT.8 The underutilization of VTE pro-phylaxis in outpatient plastic surgery centers is a public safety concern, predisposing patients to a greater incidence of VTE events. As a result, these patients would benefit from the implementation of a VTE prophylaxis regimen.
Thrombosis can occur at any point during the peri-operative course; therefore, anesthesia providers play a major role in the process of risk stratification for VTE.9 Anesthesia and immobilization cause venous stasis, as do the supine and flexed positions required for surgery.2 The enactment of a successful VTE prophylaxis protocol requires a multidisciplinary effort. It is crucial for sur-geons, anesthesia providers, and ancillary surgical staff to be aware of the risks of VTE and to formulate a treat-ment plan before surgery, which would include choice of chemoprophylaxis medication, timing of initial dose, and duration of treatment.
Venous thromboembolism is a costly complication, affecting the healthcare system economically, creating a financial burden to patients, affecting potential payouts of lawsuit settlements, and increasing liability for plastic surgery centers. Venous thromboembolism continues to be a leading cause of morbidity and mortality in patients during the perioperative process, representing a $500 million burden on the US healthcare system.10 Following an initial VTE event, the rate of recurrence is estimated to be 5% to 14% within 90 days, further increasing health-care expenditures.11 Prophylaxis is more cost-effective than treating an acute event of VTE and risking a poten-tially fatal outcome.12
Little evidence explores risk stratification and the man-agement of patients with thromboembolic disease and associated complications.13 The need for safety measures and opportunities for protocol development in office-based surgery must be evaluated. The VTE prophylaxis recommendations and guidelines can be implemented

168 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
easily, improving patient safety and outcomes. The success of these strategies relies on continuous awareness of preex-isting risk factors, use of available resources, and practice of protocols by all members of the surgical team through the perioperative process. This review will analyze current recommendations for VTE risk assessment and prophy-laxis regimen available to aid in the implementation of protocols for VTE prevention. Specifically, this review will examine recommendations for high-risk cosmetic surgical patients in office-based settings.
MethodsAn electronic search was performed using Cumulative Nursing & Allied Health Literature (CINAHL), PubMed, MEDLINE, and Scopus. Search results were limited to the English language and a publication date within the last 10 years. The following search terms were applied in all in-dividual database searches: venous thromboembolism, deep vein thrombosis, plastic surgery, chemoprophylaxis, and low-molecular weight heparin. Qualitative and quantita-tive studies were used, and duplicate titles were removed. Titles with abstracts not deemed relevant were eliminated. Inclusion criteria consisted of studies of human subjects whose interventions evaluated the efficacy of chemopro-phylaxis in high-risk patients undergoing plastic surgery procedures. Studies not focused on the plastic surgery population were excluded. Study designs involved retro-spective and prospective data consisting of participants undergoing elective cosmetic or reconstructive surgical procedures. Published guidelines and current recommen-dations regarding VTE risk assessment and prophylaxis were also included in this literature review.
The search yielded 66 articles related to the previously mentioned criteria. Of the 66 articles, 13 were found to be relevant and subsequently included for this literature review. Accompanying literature also included data and recommendations from the ACCP and the ASPS.
Review of the LiteratureRudolf Ludwig Karl Virchow in 1859 was the first phy-sician to demonstrate that thrombosis formation was caused by a triad of factors: hypercoagulability of blood, venous stasis, and endothelial damage.2 Perioperative thrombosis and hemostasis management have changed considerably over the past 50 years to include the break-through discovery of heparin and other anticoagulants.14 Since the late 1990s, the medical and surgical literature has experienced a large number of reviews, clinical studies, and meta-analyses of the issues pertaining to VTE in the United States.2 Proximal DVT carries a 90-day risk of PE in 50% of the affected population when un-treated. Symptomatic PE has a 10% mortality rate within the first hour of onset of symptoms.2,7,15 Many VTE-related events are considered potentially preventable.
Effective methods of VTE prevention have been iden-
tified and are updated every 4 years by the ACCP, but VTE as a public health concern and patient safety issue remains largely unrecognized in office-based surgery practices. Patients undergoing plastic surgery were first included in the ACCP recommendations for VTE che-moprophylaxis in 2012 because of the increased volume in plastic surgery.1,9 Of all cosmetic surgery procedures, 71% were performed in physicians’ offices in 2013, ac-cording to the ASPS.16 Debate among healthcare profes-sionals exists regarding the appropriate VTE treatment regimen in high-risk patients presenting for elective plastic surgery in an office-based setting. The exact in-cidence of VTE is unknown because screening and pro-phylactic practices are often lacking in the plastic surgery patient population.2,12
Risk assessment serves as an important tool to identify patients who have a high probability for the development of VTE. The most widely used risk stratification tool is the Caprini model.3 In the Caprini model, preventive measures first include identification of patient-related risk factors such as a previous history of VTE, hormone replacement therapy, obesity, use of oral contraceptives, advanced age, pregnancy, immobility, smoking, cancer, and hypercoagulable blood disorders (Table).17
The type of procedure being performed may also augment patient-related risk factors. Procedural risk factors specific to plastic surgery include large-volume liposuction above 5 L, use of general anesthesia, abdomi-noplasty, and longer procedures or those in combination lasting more than 4 hours (which include mastopexy and abdominoplasty combined).2,5,6,12 A VTE prevention plan should be created in accordance with patient and proce-dural risk factors. Despite the known risks of VTE, fewer than 50% of plastic surgeons are believed to consistently use chemoprophylaxis for high-risk patients.5
• Risk Factors. Independent patient-related factors increasing the risk of VTE not included in the Caprini model are ethnicity and travel. Ethnicity is a contribut-ing factor for hypercoagulable disease. White females, which account for 70% of all cosmetic surgical patients, are most likely to carry the hereditary gene for the hy-percoagulable disorder, factor V Leiden. The gene in this disorder presents as a heterozygous mutation in 3% to 7% of white females, resulting in a sixfold increase in the risk of VTE.2,5,14,16
Another important risk factor to also consider is travel. People are more likely to travel in conjunction with plastic surgical procedures than any other surgical procedure.5 This population may also include patients who travel for breast reconstructive surgery after previ-ous malignancy of the breast. Prolonged air travel carries the greatest risk of DVT or PE compared with other modalities of travel. Traveling compounded with obesity, oral contraception use, and factor V Leiden will increase rate of VTE events even further.2

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 169
Cancer and obesity are considered major risk factors contributing to VTE risk included in the Caprini model. Patients undergoing reconstructive procedures due to breast cancer fall into a high-risk classification for VTE. Breast cancer treatment promotes a twofold to fivefold increase in the risk of VTE because of estrogen receptor modulator medications and malignancy causing a proco-agulant state with abnormal blood flow, blood composi-tion, and vessel walls.5,18 The presence of malignancies, prolonged complex surgical procedures, and postopera-tive immobilization also contribute to the development of VTE.19
Obesity has continuously been recognized as a major risk factor to the development of VTE.2 Because of an increase in the number of bariatric procedures, patients experiencing massive weight loss are more prevalent than ever. With these procedures comes the demand for body contouring procedures, thus prompting plastic surgeons to reconsider their views on VTE prophylaxis.20 Prolonged intraoperative time, increased intra-abdominal pressure with tightening of abdominal fascia, and im-proper postoperative abdominal binder placement have all been postulated as increasing the risk of VTE in plastic surgery, which is the reason why body contouring and abdominoplasty procedures have the highest probability of VTE compared with other procedures in this specialty. Moreover, abdominoplasty and belt lipectomy proce-dures are the most sought-after procedures for massive weight loss patients, and these procedures result in VTE complications ranging from 2% to 9% for symptomatic DVT or PE.2,3,21
• Chemoprophylaxis. Patient-related and procedural-related factors must be weighed against the likelihood of bleeding before chemoprophylaxis can be initiated.5 Timing of administration for chemoprophylaxis contin-ues to be examined. No current consensus in the plastic surgery literature exists regarding the most appropriate time to initiate chemoprophylaxis therapy in high-risk patients. The critical period for thrombosis forma-tion begins at the induction of anesthesia, thus being a concern for the anesthesia provider.2,5,6 Current recom-mendations suggest for pneumatic compression devices to be applied to lower extremities before the induction of anesthesia to prevent venous stasis due to decreases in peripheral vascular resistance secondary to induc-tion.13 Additional anesthesia-related factors contributing to venous stasis and stimulation of coagulation include prolonged operative/anesthetic exposure time, vasodila-tory effects of anesthesia medications, muscle relaxation, and decreases in core body temperature.22
Proper perioperative patient positioning and aggres-sive early postoperative ambulation are mandatory for all patients undergoing surgery, according to the ACCP.5 Not all patients can be fully ambulatory after plastic surgery, requiring additional measures of prophylaxis. Prophylaxis
Table. Risk Assessment Score for Venous Thromboembolism Abbreviations: BMI, body mass index; DVT, deep vein thrombosis; PE, pulmonary embolism.aEach risk factor represents the specified number of points.
Number of points Risk Factorsa
5 • Elective major lower extremity arthroplasty
• Hip, pelvis, or leg fracture (< 1 mo)
• Multiple trauma (< 1 mo)
• Acute spinal cord injury (paralysis, < 1 mo)
• Stroke (< 1 mo)
3 • Age > 75 y
• History of DVT or PE
• Positive factor V Leiden
• Positive for prothrombin 20210A mutation
• Elevated serum homocysteine level
• Positive lupus anticoagulant test
• Elevated levels of anticardiolipin antibodies
• Heparin-induced thrombocytopenia
• Other congenital or acquired thrombophilia
• Family history of thrombosis
2 • Age 60-74 y
• Arthroscopic surgery
• Malignancy (present or previous)
• Major surgery (> 45 min)
• Laparoscopic surgery (> 45 min)
• Prolonged bedrest (> 72 h)
• Immobilizing plaster cast of the leg or foot (< 1 mo)
• Central venous access
1 • Age 41-60 y
• Minor surgery planned
• History of major surgery (< 1 mo)
• History of inflammatory bowel disease
• Obesity (BMI > 25 kg/m2)
• Acute myocardial infarction
• Congestive heart failure (< 1 mo)
• Sepsis (< 1 mo)
• Serious lung disease
• Abnormal pulmonary function
• Varicose veins
• Swollen legs (current)
• Medical patient currently at bedrest
1 (women only)
• Oral contraceptive or hormone replacement therapy
• Unexplained stillborn infant or spontaneous abortion
• Pregnancy or post partum (< 1 mo)
• Premature birth with toxemia or growth-restricted infant

170 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
for the prevention of VTE is broken down into 2 categories: mechanical and pharmacologic. Mechanical prophylaxis refers to devices worn by the patient, which reduces venous stasis, therefore preventing VTE. Chemoprophylaxis refers to anticoagulant medications used systemically to prevent VTE.5 Chemoprophylactic therapy in combination with mechanical modalities con-tinues to be superior to single-modality therapy alone for VTE prevention in patients at highest risk.13 Hesitation to use chemoprophylaxis exists among some plastic sur-geons because of concerns about increased postoperative bleeding; however, this fear is not validated in the plastic surgery literature.2 Plastic surgeons cite lack of evidence as a major driver of the decision to not use chemopro-phylaxis.7
This literature review highlighted issues with pharma-cologic prophylaxis, which include efficacy, safety, and cost-effectiveness. The most effective methods of prophy-laxis are low-dose unfractionated heparin and low-molec-ular-weight heparin (LMWH), reducing the risk of DVT by 68% to 76%.12 Reportedly, LMWH reduced bleeding and the risk of VTE as effectively as heparin, with in-creased bioavailability and longer plasma half-life.22 The evidence is controversial regarding whether either of the 2 medications reduces the risk of bleeding and hematoma.
The decision to provide chemoprophylaxis raises another question, which is when to administer the medi-cation and duration of treatment. Clot formation mostly occurs intraoperatively; therefore, most general, orthope-dic, and bariatric surgeons administer chemoprophylaxis preoperatively.21 Preoperative subcutaneous heparin has been shown to be safe in other surgical groups; however, the large surface areas and dissection involved in abdomi-noplasty, belt lipectomy, and transverse rectus abdominis myocutaneous (TRAM) flap reconstructions have been considered by many plastic surgeons as a relative contra-indication to preoperative chemoprophylaxis. Campbell et al3 retrospectively examined patients undergoing ab-dominoplasty; their results suggested safety and efficacy with preoperative administration and continuation of LMWH for 2 days postoperatively to cover the period of maximum immobility, without any bleeding complica-tions requiring surgical intervention or blood transfusion. Keith and colleagues9 also retrospectively studied preop-erative chemoprophylaxis in patients undergoing breast reconstruction and reported an acceptable rate of postop-erative bleeding complications managed conservatively.
Reish et al21 retrospectively reviewed a single sur-geon’s experience of truncal contouring cases that were at high risk of VTE. The findings of the study showed the combination of preoperative and postoperative che-moprophylaxis with unfractionated heparin did not significantly increase the incidence of bleeding. Seruya et al4 also retrospectively reviewed a single surgeon’s experience; results proved that mechanical prophylaxis
plus subcutaneous heparin (unfractionated or LMWH) postoperatively conferred a statistically significant reduc-tion in the rate of VTE without a significant increase in bleeding vs mechanical prophylaxis alone. Limitations to these studies included a small sample size and a single surgeon’s experience, but they had the advantage of en-abling a strict adherence to a chemoprophylaxis protocol to study efficacy.
Colwell et al8 prospectively analyzed patients undergo-ing abdominal contouring procedures. They noted that the increase in intraoperative thrombin generation was significantly less in patients receiving chemoprophylaxis compared with those who received no prophylaxis (75 vs 997 nM, P = .019). The increase in postoperative throm-bin generation was significantly less in patients receiving chemoprophylaxis compared with those who received no prophylaxis (186 vs 1404 nM, P = .004), with no throm-boembolic events or bleeding complications reported in the immediate postoperative period and in the 6-month follow-up after receiving chemoprophylaxis for 7 days in the treatment group. This study demonstrates a significant intraoperative increase in thrombin generation in patients undergoing body contouring procedures, thus supporting the efficacy of preoperative chemoprophylaxis.
In a prospective, nonrandomized assessment, Kim et al18 compared 2 groups of patients undergoing immedi-ate pedicled TRAM flap breast reconstruction. One group received no chemoprophylaxis, and the other received 7 days of enoxaparin starting 1 hour preoperatively. They found no difference in transfusion rates or hematoma. There was a significant difference in the incidence of asymptomatic PE, 16.7% in the group without chemo-prophylaxis vs 0% in the group receiving preoperative and postoperative chemoprophylaxis. Michaels et al6 also prospectively reviewed a cohort of patients undergoing body contouring procedures after massive weight loss. In a nonrandomized fashion, the control group received mechanical prophylaxis alone, and the experimental group received mechanical prophylaxis plus LMWH 6 hours postoperatively. The experimental group demon-strated no increased risk of transfusion or hematoma after implementing a chemoprophylaxis regimen.
Hatef et al13 showed that enoxaparin administration was associated with a statistically significant decrease (P = .0064) in DVT among patients undergoing circum-ferential abdominoplasty. Data from this retrospective analysis demonstrated that a risk-assessment tool such as the Davison-Caprini risk assessment model should be applied preoperatively to risk-stratify all patients under-going excisional body contouring. The authors examined the relationship between body contouring surgery and enoxaparin administration. They compared enoxaparin treatment timing: 2 hours preoperatively vs intraop-eratively or immediately postoperatively. There was no statistically significant difference in bleeding requiring

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 171
transfusions, intraoperative blood loss, or VTE events. It was noted that patients who received LMWH for 3 days or longer had statistically significant increases in postop-erative bleeding requiring transfusion, but they did not have increased risk of hematoma formation.
Pannuci et al7,15 retrospectively collected and applied a Venous Thromboembolism Prevention Study protocol in a multicenter analysis of various plastic surgery pro-cedures. The goal of this study was to risk-stratify and provide chemoprophylaxis to high-risk plastic surgery patients. The authors noted that postoperative LMWH was protective against 60-day VTE in high-risk patients and did not produce clinically relevant increases in ob-served rates of reoperative hematoma.
Newall et al22 retrospectively studied high-risk pa-tients undergoing liposuction and body contouring pro-cedures and the effect of chemoprophylaxis. The study noted no incidence of VTE following chemoprophylaxis administration 1 hour after surgery without provoking hemorrhage or bleeding complications postoperatively.
Lemaine and colleagues19 studied LMWH chemopro-phylaxis in women who had free-flap autologous breast reconstruction; 5.3% of the study sample had a reopera-tive hematoma. The authors noted that most of the re-operative hematomas were attributed to flap congestion and considered having a low threshold for reoperation considering the nature of the procedure and concerns of flap necrosis. The authors’ findings support the use of chemoprophylaxis and demonstrated that LMWH is a safe and effective method for prevention of VTE.
Implications for Future StudiesGaps exist in the evidence to guide the choice among available anticoagulants, dosing, optimal timing of initia-tion, and duration of therapy for VTE prevention.21 No prospective randomized controlled trials exist on preop-erative chemoprophylaxis for VTE in plastic and recon-structive surgery. However, retrospective reviews present a decrease in the incidence of VTE in patients undergo-ing circumferential abdominoplasty and in patients with massive weight loss following bariatric surgery when postoperative chemoprophylaxis is used.3
The literature demonstrates the need for large mul-ticenter, prospective, randomized studies to examine various thromboembolic therapies and associated com-plications in these patients.13 Additionally, Seruya et al4 suggest that a Doppler analysis of the lower extremities should be included in all future VTE studies of patients preoperatively and on postoperative days 5 and 7 to document the true incidence of VTE and more accurately quantify risk reduction with thromboprophylaxis.4
ConclusionProphylactic modalities to prevent VTE are underutilized by health professionals, particularly in office-based plastic
surgery despite all the data to support thromboprophy-laxis for prevention in high-risk patients. Events of VTE significantly contribute to increased morbidity and mor-tality along with a steady rise in healthcare expenditures. Patient education is paramount and should include in-formation as to their individual risk factors, symptoms of DVT or PE, and an explanation of the risk-to-benefit ratio in using anticoagulants as prophylaxis.2 The Caprini risk assessment tool has proved to be clinically valuable when one assesses patients for VTE and should be included in the patient’s chart in all office-based plastic surgery set-tings. Ethnicity, travel, malignancy, and obesity are some of the patient-related factors contributing to increased risk and must be considered clinically relevant.
Collectively, numerous retrospective studies demon-strate promising results in prevention, and these results can be used to formulate an individualized treatment plan for VTE prophylaxis in high-risk patients undergo-ing plastic surgery. Evidence suggests chemoprophylaxis should be included during the perioperative period and/or postoperatively to cover the period of maximum im-mobility in high-risk patients. Physician attitudes vary re-garding adding chemoprophylaxis as part of multimodal therapy because of concerns of increased surgical blood loss and postoperative hematoma formation, although some literature exists that refutes the notion. Focusing on prophylactic efforts is of utmost value in VTE preven-tion. Multimodal therapy for VTE prophylaxis compared with single-modality therapy or no therapy has shown to be superior in improving patient outcomes.4 This literature review supports the implementation of a VTE screening protocol to assess and recommend prophylaxis for all patients undergoing elective plastic surgery outside a hospital environment. It is paramount to include VTE prophylaxis in office-based plastic surgery settings to increase patient safety, to promote evidence-based prac-tices, and to improve cost-effectiveness through preven-tive measures.
REFERENCES 1. Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in nonor-
thopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 suppl):e227S-e277S.
2. Young VL, Watson ME. The need for venous thromboembolism (VTE) prophylaxis in plastic surgery. Aesthet Surg J. 2006;26(2):157-175.
3. Campbell W, Pierson J, Cohen-Shohet R, Mast BA. Maximizing che-moprophylaxis against venous thromboembolism in abdominoplasty patients with the use of preoperative heparin administration. Ann Plast Surg. 2014;72(6):S94-S96.
4. Seruya M, Venturi ML, Iorio ML, Davison SP. Efficacy and safety of venous thromboembolism prophylaxis in highest risk plastic surgery patients. Plast Reconstr Surg. 2008;122(6):1701-1708.
5. Venturi ML, Davison SP, Caprini JA. Prevention of venous throm-boembolism in the plastic surgery patient: current guidelines and recommendations. Aesthet Surg J. 2009;29(5):421-428.
6. Michaels J, Coon D, Mulvey CL, Rubin JP. Venous thromboembolism prophylaxis in the massive weight loss patient: relative risk of bleed-

172 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
ing. Ann Plast Surg. 2015;74(6):699-702.
7. Pannucci CJ, Wachtman CF, Dreszer G, et al. The effect of postopera-tive enoxaparin on risk for reoperative hematoma. Plast Reconstr Surg. 2012;129(1):160-168.
8. Colwell AS, Reish RG, Kuter DJ, Damjanovic B, Austen WG Jr, Fogerty AE. Abdominal contouring procedures increase activity of the coagulation cascade. Ann Plast Surg. 2012;69(2):129-133.
9. Keith JN, Chong TW, Davar D, Moore AG, Morris A, Gimbel ML. The timing of preoperative prophylactic low-molecular-weight heparin administration in breast reconstruction. Plast Reconstr Surg. 2013;132(2):279-284.
10. Hawkins D. Pharmacoeconomics of thrombosis management. Phar-macotherapy. 2004;24(7 pt 2):95S-99S.
11. Spyropoulos AC, Lin J. Direct medical costs of venous thromboem-bolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm. 2007;13(6):475-486.
12. Miszkiewicz K, Perreault I, Landes G, et al. Venous thromboembolism in plastic surgery: incidence, current practice and recommendations. J Plast Reconstr Aesthet Surg. 2009;62(5):580-588.
13. Hatef DA, Kenkel JM, Nguyen MQ, et al. Thromboembolic risk assessment and the efficacy of enoxaparin prophylaxis in excisional body contouring surgery. Plast Reconstr Surg. 2008;122(1):269-279.
14. Valsami S, Asmis LM. A brief review of 50 years of perioperative throm-bosis and hemostasis management. Semin Hematol. 2013;50(2):79-87.
15. Pannucci CJ, Dreszer G, Wachtman CF, et al. Postoperative enoxa-parin prevents symptomatic venous thromboembolism in high-risk plastic surgery patients. Plast Reconstr Surg. 2011;128(5):1093-1103.
16. American Society of Plastic Surgery. 2013 Plastic surgery statistics report. http://www.plasticsurgery.org/Documents/news-resources/statistics/2013-statistics/plastic-surgery-statistics-full-report-2013.pdf. Published 2013. Accessed September 26, 2014.
17. Caprini JA, Arcelus JI, Reyna JJ. Effective risk stratification of surgical and nonsurgical patients for venous thromboembolic disease. Semin Hematol. 2001;38(2 suppl 5):12-19.
18. Kim EK, Eom JS, Ahn SH, Son BH, Lee TJ. The efficacy of prophylac-
tic low-molecular-weight heparin to prevent pulmonary thromboem-bolism in immediate breast reconstruction using the TRAM flap. Plast Reconstr Surg. 2009;123(1):9-12.
19. Lemaine V, McCarthy C, Kaplan K, et al. Venous thromboembolism following microsurgical breast reconstruction: an objective analysis in 225 consecutive patients using low-molecular-weight heparin pro-phylaxis. Plast Reconstr Surg. 2011;127(4):1399-1406.
20. Colwell AS, Borud LJ. Optimization of patient safety in postbariatric body contouring: a current review. Aesthet Surg J. 2008;28(4):437-442.
21. Reish RG, Damjanovic B, Colwell AS. Deep venous thrombosis pro-phylaxis in body contouring: 105 consecutive patients. Ann Plast Surg. 2012;69(4):412-414.
22. Newall G, Ruiz-Razura A, Mentz HA, Patronella CK, Ibarra FR, Zarak A. A retrospective study on the use of a low-molecular-weight heparin for thromboembolism prophylaxis in large-volume liposuction and body contouring procedures. Aesthetic Plast Surg. 2006;30(1):86-95; discussion 96-97.
AUTHORSSergio Hernandez, DNP, CRNA, was a DNP-anesthesiology candidate at Barry University in the College of Health Sciences DNP Anesthesiology Program, Hollywood, Florida, at the time this research was completed. He is a nurse anesthetist employed by Elite Plastic Surgery, Aventura, Florida. Email: [email protected].
Jorge Valdes, DNP, CRNA, ARNP, is a faculty member at Barry Uni-versity in the College of Health Sciences DNP Anesthesiology Program, Hollywood, Florida. Email: [email protected].
Moises Salama, MD, is chief of Surgery at Elite Plastic Surgery and a staff plastic surgeon at Aventura Hospital and Medical Center, Aventura, Florida. Email: [email protected].
DISCLOSURESThe authors have declared they have no financial relationships with any commercial interest related to the content of this activity. The authors did not discuss off-label use within the article.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 173
Most members of the Jehovah’s Witness community refuse blood transfusions, and there are variations in what alternatives they will accept depending on their personal decisions. To provide culturally competent care, healthcare providers need to be knowledgeable about substitutions for blood administration as well as the risks and benefits of available alternatives so that they can inform their patients. It has been rec-ognized in the literature that preoperative optimiza-tion of hemoglobin levels with alternative treatment modalities through a multidisciplinary approach can improve clinical outcomes in patients who refuse blood
products. The purpose of this article is to illuminate the current beliefs of Jehovah’s Witnesses regarding receiving blood products, discuss ethical and legal considerations for the nurse anesthetist, discuss the risks of blood transfusions, and examine transfusion alternatives. Finally, this article considers a multidis-ciplinary approach to the optimization of preoperative hemoglobin levels.
Keywords: Bloodless surgery, elective surgery, Jeho-vah’s Witnesses, transfusion alternatives.
The Jehovah’s Witness Population: Considerations for Preoperative Optimization of Hemoglobin
Yasmine N. Campbell, DNP, CRNAMelissa D. Machan, DNP, CRNAMarquessa D. Fisher, DNP, CRNA
Jehovah’s Witnesses are a vulnerable patient population that presents unique ethical and legal dilemmas for anesthesia professionals. Comprising approximately 1.2 million of the US population, Jehovah’s Witnesses have reli-
gious beliefs that deter them from receiving blood trans-fusions, which can lead to adverse reactions from the refusal of treatment.1 Surgical procedures that have the potential for large amounts of blood loss for any patient can be challenging for the nurse anesthetist, but when combined with the patient who refuses to receive blood products, the intraoperative fluid hemodynamic manage-ment strategies can become critical. Regardless of the patient’s reasons for declining blood products, healthcare providers should provide culturally competent care and therefore must be knowledgeable about substitutions for blood product administration as well as the risks and ben-efits of such treatments.
Inconsistencies exist in what alternatives a Jehovah’s Witness patient will accept, depending on his or her reli-gious sect. The responsibility of the nurse anesthetist is to ensure that this unique patient population makes informed decisions established on evidence-based transfusion alter-natives, as such treatments relate to their religious prac-tices. Furthermore, failure to optimize hemoglobin (Hgb) status and provide culturally competent patient education on transfusion alternatives before the day of surgery could have financial implications for the institution and may result in cancellation or delay of the surgery.
A multidisciplinary approach to the care of the Jehovah’s Witness population to optimize preoperative Hgb status must be considered when preparing these patients for surgery, and education of the nurse anesthe-tist and patient on transfusion alternatives is important during the preoperative plan of care.
The aim of this article is to illuminate the current beliefs of Jehovah’s Witnesses regarding receiving blood products, discuss ethical and legal considerations for the nurse anesthetist, discuss the risks of blood transfu-sions and examine transfusion alternatives, and, finally, consider a multidisciplinary approach to optimization of preoperative Hgb levels.
Review of the Literature • Jehovah’s Witness Beliefs. Jehovah’s Witness is a Christian religion founded by Charles Taze Russell in Pennsylvania during the 1870s.2 In 1945, the govern-ing body of the Jehovah’s Witnesses, The Watch Tower Society, interpreted the scriptures to proclaim that taking blood into the body would have loss of eternal life and decided that members would be shunned by the congregation and denied the church’s sacraments (“dis-fellowshipped”) for accepting blood.3 Citing the literal translation of the book of Acts (Acts 15:19-20) from The New World Translation of the Holy Scriptures, affiliates of this faith believe the abstinence of whole blood products will bring good health.4
In 2000, The Watch Tower Society revised its policies

174 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
on blood transfusions to include that the acceptance of blood products is to be based on personal decision and conscience.5 Interestingly, if blood is given to a Jehovah’s Witness by force or coercion, or accepted by personal choice, the member can voluntarily disassociate himself or herself from the church and repent to remain in the religion thereafter.3 Under the new doctrine, members of this religion are allowed medical confidentiality from the church, and dissociation is voluntary unless medical concealment is breached. In this instance, the member is “disfellowshipped” by the church.5 Thus, to provide cul-turally competent care to the Jehovah’s Witness patient, it is important for the healthcare provider to interview these patients privately and allow them an opportunity to make informed decisions about their medical care. Once a patient is identified as a Jehovah’s Witness, staff involved in the medical care of the patient should be in-formed and confidentiality regarding medical decisions should be strictly maintained.
• Ethical Issues. The care of the Jehovah’s Witness patient can present various ethical and legal dilemmas for the nurse anesthetist. Adult patients and emancipated minors, under the Patient Self-Determination Act, have the right to decline medical care, even if the result is death.6 The Jehovah’s Witness population is extremely educated about legal rights of refusal, advance directives, and living wills. Additionally, Jehovah’s Witnesses have a standardized advance directive form that they carry at all times and that provides specific instructions regarding their care in the event of an emergency.
It is important for the nurse anesthetist to respect the right to refuse the acceptance of blood products. The refusal of blood products by the Jehovah’s Witness patient is not a refusal of medical treatment, nor should it ever be considered as such.7 Patient care strategies include establishing a rapport as early as possible to ensure the patient is informed about available alterna-tives to the administration of blood products. Second, Jehovah’s Witness patients should be interviewed pri-vately to maintain the integrity of their personal choice to accept or deny blood fractions or allogeneic blood transfusions. Their decisions should remain private and should not be discussed in front of friends or family members. Finally, exclusive perils should be added to the anesthesia consent in relation to the procedure and excessive blood loss. Blood fractions and other accepted treatment modalities by the patient should be clearly indicated in the patient’s medical record and on the an-esthesia preoperative assessment.8
• Transfusion Risks. Although many treatment options for anemia exist, the transfusion of blood prod-ucts remains one of the most commonly used lifesaving treatments. However, receiving blood products is not without inherent risks. Adverse reactions such as infec-tion, transfusion-related acute lung injury (TRALI), fatal
anaphylaxis, blood incompatibility, and immunologic reactions are the most life-threatening reactions of blood transfusions.9,10 Between 2001 and 2006, TRALI was re-sponsible for greater than 50% of the deaths in the United States of patients transfused with allogeneic blood.11 Moreover, blood transfusions are also known to increase hospital length of stay and contribute to poor clinical outcomes postoperatively.9,12
• Erythropoietin and Iron Therapy. Recombinant human erythropoietin (EPO) is an endogenous glyco-protein hormone whose function is to increase the pro-duction of red blood cells and subsequently increase Hgb levels as the result of tissue hypoxia.13,14 Comparatively, intravenous (IV) iron therapy has also been shown to significantly increase Hgb levels in patients with pre-operative iron-deficiency anemia.12,15 Although iron therapy as a primary treatment of preoperative anemia is not recommended, studies have indicated that ad-ministration of EPO, in conjunction with iron therapy preoperatively, can prevent blood transfusions in a wide variety of operations.9,11,14,16,17 In their study, Harwin and colleagues9 found that there was decreased mortality and no morbidity after adequate preoperative optimiza-tion with EPO combined with iron therapy for anemic Jehovah’s Witness patients undergoing total hip replace-ment surgery. Furthermore, other authors reported an increase in Hgb levels after successful treatment of EPO and iron therapy.10,16 Similarly, EPO has been success-fully used for the preoperative optimization of Hgb status in patients who were anemic before cardiac surgery, re-sulting in decreased mortality rates of Jehovah’s Witness patients compared with patients who did not receive EPO preoperatively.11
• Bloodless Surgery. Current literature has indicated that blood transfusions can be avoided by exploring alternative bloodless treatment modalities.11 “Bloodless surgery” is an innovative phenomenon that medical centers are adopting for patients who refuse blood transfusions. Bloodless surgery protocols are essential to minimize risks and to offer patients who decline blood transfusions the same quality of care accessible to pa-tients who do accept blood transfusions.13
Moreover, evidence suggests that mortality rates may be lowered in patients receiving bloodless surgery. Several studies found that the Jehovah’s Witness pa-tients enrolled in a bloodless surgery program had a decreased incidence of in-hospital death, decreased 5-year mortality rates, and shorter lengths of hospital stay compared with non-Jehovah’s Witnesses postopera-tively.1,18,19 Interestingly, the Jehovah’s Witness patients studied had a statistically significant lower occurrence of renal failure, sepsis, and bleeding postoperatively. Furthermore, the authors argue that bloodless surgery is considered a safe practice for patients who do not accept blood.1,18,19 In a similar study, Moskowitz and

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 175
colleagues20 emphasized that restrictive transfusion practices do not adversely affect clinical outcomes and, in fact, can improve clinical outcomes because of blood conservation strategies that minimize complications that are inherent to blood transfusions.
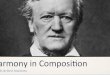
• Guidelines for Jehovah’s Witnesses on Blood Products. Before 1945, Jehovah’s Witnesses were permit-ted to donate and accept blood.21 Current transfusion guidelines by the Watch Tower Society do not allow the acceptance of whole blood or major blood fractions, specifically red blood cells, white blood cells, platelets, and plasma, to be infused despite a life-or-death health situation.21 Jehovah’s Witnesses do not dispute the fact that blood transfusions have saved lives; nevertheless, because of religious beliefs and sanctions, most Jehovah’s Witnesses do not accept blood products.21,22 Conversely, minor fractions of primary components of blood are acceptable for lifesaving measures through personal decision, careful prayer, and consideration.5,21,22 These minor fractions include albumin up to 4% of plasma, immunoglobulins up to 3% of plasma, clotting factors less than 1% of plasma, Hgb 33% of blood cells, hemin less than 2% of red blood cells, and small fraction of white blood cells known as interferons.21 Acceptable fluid replacement for the Jehovah’s Witness includes crystalloid and other colloid hemostatic agents such as desmopressin, recombinant factor VIIa, aprotinin, ε-aminocaproic acid, and tranexamic acid.21,22 Although these are recommendations made by the Watch Tower Society, nurse anesthetists should be aware that every Jehovah’s Witness has different beliefs, and his or her willingness to accept transfusion therapy varies among members (Figure 1).23
• Multidisciplinary Approach. Preoperative consider-ations are enormously challenging when caring for the Jehovah’s Witness patient, especially those patients un-dergoing procedures that carry a risk of large amounts of blood loss. Evidence suggests that clinical outcomes can be improved when there is a multidisciplinary approach
to preoperative care, along with extensive preoperative treatment of anemia in the Jehovah’s Witness patient.24 In a retrospective study, Moraca and colleagues24 found that the use of a multidisciplinary approach that included a screening for transfusion risk and the administration of erythropoiesis-stimulated agents can minimize the risk of morbidity and mortality in Jehovah’s Witness pa-tients undergoing cardiac surgery. Surgery was delayed for approximately 3.7 weeks for preoperative treatment with oral iron and EPO, but the study participants had a mortality rate of only 5%.24 Thus, early referral to facili-ties that provide bloodless procedures and preoperative clinics may provide for optimization of Hgb status pre-operatively in this patient population.
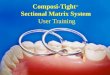
Routine screening for anemia in patients with volun-tary major surgeries can be completed as early as 4 weeks preoperatively to optimize treatment modalities.7,25 The multidisciplinary team should consist of the surgeon, an-esthesia, hematology, and a hospital liaison if available.25 The Jehovah’s Witness patient should have a comprehen-sive bleeding history taken consisting of previous surger-ies, trauma history, and the use of anticoagulant medi-cations.26 Moreover, a thorough history and physical is a necessity. Family history of bleeding complications should be noted because of the risk of possible heredi-tary bleeding disorders such as von Willebrand disease and hemophilia. Medication lists should be reviewed for anticoagulants, including platelet inhibitors, aspirin-containing agents, nonsteroidal anti-inflammatory drugs, and herbal medications, and these should be discontin-ued before surgery if clinically possible.27 In Jehovah’s Witness patients with anemia, symptoms should be assessed, as well as comorbidities and the timing of surgery, and improved hematopoiesis without allogeneic transfusion is necessary in preparation for surgeries with suspected large losses of blood.25 A specialized checklist and algorithm for preassessment of Jehovah’s Witness pa-tients are advantageous tools when preparing for elective surgery (Tables 1 and 2; Figure 2).
Figure 1. Jehovah’s Witnesses’ Position on Allogeneic and Autologous BloodAbbreviations: Blood salvage, blood cell salvage.
Position Allogeneic blood Autologous blood
Refused Whole blood
Red cells White cells Platelets Plasma
Potentially Fractions from Fractions from Fractions from Fractions from acceptable red cells white cells platelets plasma
• Hemin • Albumin • Hemoglobin • Clotting factors • Fibrinogen • Immunoglobins
Witnesses make personal decisions on what they can accept in good conscience. It is important to discuss in advance what products or procedures are acceptable to each patient.
• Preoperative autologous blood collection and stor-age for later reinfusion
• Acute normovolemic hemodilution
• Dialysis• Cardiopulmonary
bypass• Blood salvage

176 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
Implications for PracticeFor the Jehovah’s Witness patient, there are many options available as an alternative to blood transfusions. The use of a multidisciplinary approach, one that is culturally competent and meets specific patient needs, can be es-sential to optimize preoperative Hgb levels before elective surgery. Indeed, the preoperative period is the best time to optimize the Jehovah’s Witness patient and prepare for any known challenges related to blood loss during the procedure; such optimization should begin at least 4 weeks before the day of surgery.7,25 Likewise, the preoper-ative period can be used to develop strategies to minimize blood loss during the procedure, including the use of less invasive surgical techniques, controlled hypotension, or the use of a blood cell salvage system. However, such strategies are beyond the scope of this article.
Despite the evidence suggesting the effectiveness of a multidisciplinary strategy to optimize the Jehovah’s Witness patient preoperatively, there is no evidence in the literature that compares Jehovah’s Witness pa-tients who receive early care with those who do not. Certainly, future research should expand in this area. Equally important is the need to determine whether
facilities located in regions that are heavily populated with Jehovah’s Witnesses have the necessary alternative treatment modalities, such as accepted blood products, to
Table 1. Preoperative Consent for Jehovah’s Witnesses for Transfusion Alternatives
Unacceptable to Jehovah’s Witnesses: Your personal decision whole blood Fractions Choices you need to make
Plasma Albumin up to 4% of plasma ____ I accept albumin Or ____ I refuse albumin
Immunoglobulins up to 3% of plasma ____ I accept immunoglobulins Or ____ I refuse immunoglobulins
Clotting factors less than 1% of plasma ____ I accept blood-derived clotting factors Or ____ I refuse blood-derived clotting factors
Red blood cells Hemoglobin 33% of red blood cells ____ I accept hemoglobin Or ____ I refuse hemoglobin
Hemin less than 2% of red blood cells ____ I accept hemin Or ____ I refuse hemin
White blood cells Interferons: a tiny fraction of white blood cells ____ I accept blood-derived interferons Or ____ I refuse blood-derived interferons
Platelets At present, no fractions from platelets are being isolated for direct medical use
Equipment and procedures Blood cell salvage ____ I accept blood cell salvage Acute normovolemic hemodilution ____ I accept acute normovolemic Cardiopulmonary bypass hemodilution Dialysis ____ I accept cardiopulmonary bypass ____ I accept dialysis
Patient signature________________________________________________________________ Date_______________________
Table 2. Preoperative Checklist for Jehovah’s WitnessesAbbreviation: NSAIDs, nonsteroidal anti-inflammatory drugs.
• Do you have advanced directives? Yes or No
• Do you have a living will? Yes or No
• Is your surgeon aware that you are Jehovah’s Witness? Yes or No
• Do you or your family have a history of bleeding disorders? Yes or No
• Do you bruise easily or have excessive bleeding when you shave or experience frequent nosebleeds? Yes or No
• Do you take blood thinners such as aspirin, anticoagulants, NSAIDs, or herbal medications? Yes or No
• Have you had surgery before? Yes or No
• Have you had bleeding complications with any of your surgeries? Yes or No
• In a life-or-death situation would you accept a blood transfusion? Yes or No

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 177
care for these patients. Preventing patient morbidity and mortality begins with a good plan of care and adequate preparedness for any challenge that may arise. Indeed, by using a multidisciplinary approach for the preoperative care of the Jehovah’s Witness patient, the paradigm shifts the administration of blood products to a more patient-centered approach. Rather than care that is driven by the administration of products, the goal becomes the provi-sion of culturally competent care that adheres to patient beliefs, improves patient outcomes through risk minimi-zation, and reduces costs.7,25
REFERENCES 1. Frank SM, Wick EC, Dezern AE, et al. Risk-adjusted clinical out-
comes in patients enrolled in a bloodless program. Transfusion. 2014;54(10 pt 2): 2668-2677.
2. Knox Z. Writing Witness history: the historiography of the Jehovah’s Witnesses and the Watch Tower Bible and Tract Society of Pennsyl-
vania. J Religious Hist. 2011;35(2):157-180.
3. West JM. Ethical issues in the care of Jehovah’s Witnesses. Curr Opin Anaesthesiol. 2014;27(2):170-176.
4. New World Bible Translation Committee. New World Translation of the Holy Scriptures. Brooklyn, NY: Watchtower Bible and Tract Soci-ety of New York; 2013. www.jw.org/en/publications/bible/. Accessed October 20, 2014.
5. Muramoto O. Bioethical aspects of the recent changes in the policy of refusal of blood by Jehovah’s witnesses. BMJ. 2001;322(7277):37-39.
6. Gaddie K, Montgomery C, Murphy S, et al. Management of blood-less surgery in a trauma setting. Balancing patient wishes with safety. Minn Med. 2013;96(6):49-51.
7. Shander A, Javidroozi M, Perelman S, Puzio T, Lobel G. From bloodless surgery to patient blood management. Mt Sinai J Med. 2012;79(1):56-65.
8. Rogers DM, Crookston KP. The approach to the patient who refuses blood transfusion. Transfusion. 2006;46(9):1471-1477.
9. Harwin SF, Pivec R, Naziri Q, Issa K, Mont MA. Is total hip arthro-plasty a successful and safe procedure in Jehovah’s Witnesses? Mean five-year results. Hip Int. 2014;24(1):69-76.
10. El Azab SR, Vrakking R, Verhage G, Rosseel PM. Safety of cardiac
! Surgical consult and complete history and physical examination inclusive of bleeding risk assessment and evaluation management of anticoagulation and antiplatelet medications
! Surgeon consults anesthesia, hematology, and Hospital Liaison Committee if available as early as 4 weeks before surgery to begin preoperative optimization
! CBC, PT, PTT, and iron in blood samples evaluated ! Surgical consent, advance directives, blood refusal, and signed
statement of acceptable transfusion alternatives completed and faxed to hematology and anesthesia care team
! Multidisciplinary care plan developed by surgical, anesthesia, and hematology teams
Hgb < 13 g/dL in males
Hgb < 12 g/dL in females
No
No further Hgb optimization needed
Yes
Consult hematology
! Consider EPO/iron therapy
! If Hgb < 10g/dL or surgery < 2 weeks away, consider IV iron therapy
! Maintain autonomy and ensure culturally competent care
! Refer patient to Hospital Liaison Committee or local Jehovah’s Witness Hospital Information Services for guidance
Figure 2. Preoperative Care Pathway for Adults Refusing Blood and Jehovah’s Witnesses Requiring Elective SurgeryAbbreviations: CBC, complete blood cell count; EPO, recombinant human erythropoietin; Hgb, hemoglobin; PT, prothrombin time; PTT, partial thromboplastin time.

178 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
surgery without blood transfusion: a retrospective study in Jehovah’s Witness patients. Anaesthesia. 2010;65(4):348-352.
11. Vaislic CD, Dalibon N, Ponzio O, et al. Outcomes in cardiac surgery in 500 consecutive Jehovah’s Witness patients: 21 year experience. J Cardiothorac Surg. 2012;7:95-102.
12. Price E, Artz AS, Barnhart H, et al. A prospective randomized wait list control trial of intravenous iron sucrose in older adults with unex-plained anemia and serum ferritin 20–200 ng/mL. Blood Cells Mol Dis. 2014(4):221-230.
13. Guarino S, Di Matteo F, Sorrenti S, et al. Bloodless surgery in geriatric surgery. Int J Surg. 2014:S82-85.
14. Ferraris VA, Brown JR, Despotis GJ, et al. 2011 update to the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiolo-gists blood conservation clinical practice guidelines. Ann Thorac Surg. 2011;91(3):944-982.
15. Kim YH, Chung HH, Kang SB, Kim SC, Kim YT. Safety and usefulness of intravenous iron sucrose in the management of preoperative ane-mia in patients with menorrhagia: a phase IV, open-label, prospective, randomized study. Acta Haematol. 2009;121(1):37-41.
16. McCartney S, Guinn N, Roberson R, Broomer B, White W, Hill S. Jehovah’s Witnesses and cardiac surgery: a single institution’s experi-ence. Transfusion. 2014;54(10 pt 2):2745-2752.
17. Bacuzzi A, Dionigi G, Piffaretti G, et al. Preoperative methods to improve erythropoiesis. Transplant Proc. 2011;43(1):324-326.
18. Ramanan B, Burns TL, Sugimoto JT, Forse RA. Impact of a blood conservation program on 30-day morbidity and mortality: a cohort study. J Surg Res. 2014;187(1):343-349.
19. Pattakos G, Koch CG, Brizzio ME, et al. Outcome of patients who refuse transfusion after cardiac surgery: a natural experiment with severe blood conservation. Arch Intern Med. 2012;172(15):1154-1160.
20. Moskowitz DM, McCullough JN, Shander A, et al. The impact of blood conservation on outcomes in cardiac surgery: is it safe and effective? Ann Thorac Surg. 2010;90(2):451-458.
21. Grundy P. Jehovah’s Witnesses and blood transfusions. Facts About Jehovah’s Witnesses website. 2014. http://www.jwfacts.com/watch-tower/blood-transfusions.php. Accessed September 20, 2014.
22. Hua M, Munson R, Lucas A, Rovelstad S, Klingensmith M, Kodner IJ. Medical treatment of Jehovah’s witnesses. Surgery. 2008;143(4):463-465.
23. Watchtower Tower Bible and Tract Society of Pennsylvania. Jehovah’s
Witnesses’ position on allogeneic and autologous blood. In: Hospital Information Services for Jehovah’s Witnesses. Pennsylvania, PA: Watch Tower Bible and Tract Society of Pennsylvania; 2012.
24. Moraca RJ, Wanamaker KM, Bailey SH, et al. Strategies and out-comes of cardiac surgery in Jehovah’s Witnesses. J Card Surg. 2011;26(2):135-143.
25. Shander A, Javidroozi M. The approach to patients with bleeding disorders who do not accept blood-derived products. Semin Thromb Hemost. 2013;39(2):182-190.
26. Chee YL, Crawford JC, Watson HG, Greaves M. Guidelines on the assessment of bleeding risk prior to surgery or invasive procedures. British Committee for Standards in Haematology. Br J Haematol. 2008;140(5):496-504.
27. Nuttall GA, Brost BC, Connis RT, et al. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesi-ology. 2006;105(1):198-208. http://search.ebscohost.com.ezproxy.barry.edu/login.aspx?direct=true&db=ccm&AN=2009227342&site=ehost-live Accessed October 17, 2014.
AUTHORSYasmine N. Campbell, DNP, CRNA, is the lead CRNA at University of Miami Hospital, Miami, Florida. Research for this article was conducted while she was a doctoral candidate at Barry University in Hollywood, Florida. Email: [email protected].
Melissa D. Machan, DNP, CRNA, is a full-time nurse anesthetist at Plantation General Hospital, Plantation, Florida, as well as adjunct faculty member at Barry University College of Health Sciences DNP anesthesiol-ogy program in Hollywood, FL. Email: [email protected].
Marquessa D. Fisher, DNP, CRNA, is an assistant professor of clini-cal in the nurse anesthesia program at the University of Miami School of Nursing and Health Sciences in Coral Gables, Florida. Email: [email protected].
DISCLOSURESThe authors have declared they have no financial relationships with any commercial interest related to the content of this activity. The authors did not discuss off-label use within the article.
PARTNERS CARE TOGETHER
A M E R I C A N A S S O C I AT I O N O F N U R S E A N E S T H E T I S T S | A A N A . C O M
AANA is the professional association representing
CRNAs across the nation. We actively form collaborative
relationships with corporate partners to leverage the
important work of each other as we advance patient
safety, practice excellence and the profession.
Partner with the AANA, contact Wendy Stoner, Industry Marketing Manager at [email protected].
AANA CORPORATE PARTNERS

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 181
Stiff-person syndrome (SPS) is a neurologic disorder characterized by painful involuntary episodes of severe muscle rigidity affecting the axial muscles and extremi-ties. Although the etiology of SPS is unknown, it is sus-pected to involve the synthesis of γ-aminobutyric acid (GABA). Symptoms of SPS are precipitated by sudden unexpected movements, noises, and stress. Addition-ally, SPS has been linked with various autoimmune disorders, including diabetes mellitus, thyroid disease, pernicious anemia, and certain cancers. Because of the effect of SPS and SPS medications, inhalational agents and neuromuscular blockers have the potential to cause prolonged hypotonia following anesthesia,
resulting in respiratory failure despite full reversal of neuromuscular blockade. In documented case reports, the outcomes of using general anesthesia with inhala-tional agents and neuromuscular blockers in patients with SPS varied. This case report highlights the anes-thetic management of a 56-year-old woman with diag-nosed SPS undergoing a hemicolectomy for a colon mass using total intravenous anesthesia.
Keywords: Moersch-Woltman syndrome, stiff-man syndrome, stiff-person syndrome, stiff-limb syndrome, total intravenous anesthesia.
Anesthetic Considerations of Stiff-Person Syndrome: A Case Report
Kristi Hylan, DNP, CRNA An-Duyen Nguyen Vu, CRNA Katherine Stammen, MD
Stiff-person syndrome (SPS) is a rare and debilitating neurologic disease that affects the muscles of the extremities and trunk. This syndrome is progressive and described as involuntary activation of the motor unit of
the axial muscles and muscles of the extremities, caus-ing continuous muscle spasms and rigidity.1 The central muscles are affected first, but the disease can progress to affect muscles of the back and extremities,2 particularly the thighs. Clinical presentations range from mild muscle spasms to bone fractures resulting from violent severe muscle spasms.3 The disease occurs more often in women ranging from 20 to 50 years of age.4 No prevalence of SPS exists in any race or ethnic group, and there is no indica-tion in previous studies that it is hereditary.
This syndrome was first documented by neurologists Moersch and Woltman5 in 1956 as stiff-man syndrome after treating 14 cases over a span of 32 years. In 1924, the first reported encounter was a 49-year-old male farmer from Iowa presenting with muscle stiffness and difficultly walking. Before age 34, the patient experi-enced frequent migraines and occasionally cramps in his leg muscles. His condition progressively worsened over 4 years and eventually advanced to his neck, shoulders, upper back, abdominal muscles, lower back, and thighs. His gait was “slow and awkward.” In addition to the ri-gidity, intermittent spasms developed and caused him to fall like “a wooden man.” By 1932, he was unable to walk unassisted.5 In 1958 the first case of SPS in a woman was diagnosed by Dr Richard Asher, and in 1960 Dr David
Bowler published a case report on a 7-year-old child with SPS.6,7 The term stiff-man syndrome was changed to stiff-person syndrome in 1991.8
The incidence of SPS is rare, estimated at approxi-mately 1 in 1 million, and the etiology of SPS is still unknown.4 Stiff-person syndrome is associated with autoimmune disorders based on high titers of glutamate decarboxylase (GAD) antibodies, particularly the 65-kD isoform in the serum and cerebral spinal fluid. GAD is an enzyme responsible for synthesis of γ-aminobutyric acid (GABA) and a decrease of GAD has been found in the brain of patients with SPS. These GAD antibodies have been associated with other neurologic conditions including seizures, cerebellar dysfunction, cortical dys-function, and myelopathy.9 Raju et al10 found that the antibodies decrease GABAA receptor–associated protein, which is responsible for the stability and surface expres-sion of the GABAA receptor. As the primary inhibiting neurotransmitter in the brain and the spinal cord, GABA contributes to motor control and many other cortical functions. Muscle spasms and rigidity result from the lack of inhibition via GABA causing motor neurons to become excitable. Patients with SPS often have other autoimmune diseases, such as diabetes mellitus, thyroid disease, pernicious anemia, and certain cancers, par-ticularly breast and lung cancers.11,12 A notable varia-tion of the disease is called paraneoplastic or stiff-limb syndrome, in which the patient exhibits symptoms in a single limb. Progressive encephalomyelitis with rigidity and myoclonus is another severe form of SPS that rapidly

182 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
affects the central nervous system. In some variants of SPS it is hypothesized the syndrome manifests from the body’s immune response to eliminate cancer cells. Because of the similarities between the tumor antigen and central nervous system (CNS) antigens, high levels of GAD antibodies attack the CNS.12 High levels of GAD antibodies are found in a variety of other neurologic disorders such as cerebellar ataxia, epilepsy, idiopathic limbic encephalitis, and myasthenia gravis.13 However, Newton et al3 mentioned that antibodies to GAD alone do not indicate a definitive diagnosis of SPS. Patients can test GAD negative but still exhibit symptoms of SPS.3
The clinical manifestations of SPS can occur randomly or be triggered by emotional stress and noxious stimuli such as noise and sudden touch. The diagnosis is made in the presence of episodes of muscle spasms and stiff-ness of axial muscles slowly progressing to extremities and deformity of the spinal column (severe lordotic curve).14 Patients often present with a wide stance and an unsteady gait. The gait resembles waddling and has been referred to as tin man like.8 Patients with SPS also have a hunched-over posture and abnormal eye move-ments, experience frequent falls, and are often bedridden. Moersch and Woltman5 described that SPS may be mis-taken for chronic tetanus, but it can also be misdiagnosed as anxiety disorder, multiple sclerosis, Parkinson disease, and somatic disorders.15 Misdiagnosis is common and a correct diagnosis takes an average of 6.2 years from the onset of SPS symptoms.15
Presently no cure for SPS exists, but the primary treat-ment is to enhance GABA receptors by targeting GABAB with baclofen therapy, a GABAergic agonist, and target-ing GABAA with benzodiazepine agents such as diaz-epam.16 Patients requiring higher doses of baclofen may be treated via intrathecal baclofen pumps.3 Spinal cord stimulation may relieve pain associated with spasms. Intravenous (IV) opiates can relieve severe pain epi-sodes and botulinum toxin A injections into the muscles can mitigate severe muscle rigidity.12 Intravenous im-munotherapy such as IV immunoglobulin (IVIG) can modulate the immune response. Corticosteroids and plasmapheresis are also recommended to suppress the antibody response and remove the antibodies respective-ly.4 Furthermore, in a recent case report by Vicente-Valor et al,17 an alternative treatment with cannabis derivatives, tetrahydrocannabinol and cannabidiol oromucosal spray, was successfully used to treat the spasticity symptoms related to SPS.
Case SummaryA 56-year-old African American woman with a diagno-sis of SPS was scheduled for a left hemicolectomy for removal of a colon mass. She presented with a body mass index of 16.9 kg/m2 (height of 1.753 m and weight of 51.71 kg) after a recent weight loss of 15.75 kg. Her SPS
was diagnosed 17 years before her surgery and initially presented with severe abdominal spasms and gagging episodes. At the time of diagnosis, GAD antibodies were elevated to more than 600 U/mL (normal, < 1 U/mL). Her reported activity was limited, as she was wheelchair bound with a severe lordotic curve, but she remained fairly independent. Her symptoms were managed phar-macologically with diazepam, 10 mg 3 times a day; ba-clofen, 20 mg 4 times a day; tizanidine, 2 mg 3 times a day; and IVIG infusions for flare-ups as needed. Her last infusion was 1 month before surgery.
The patient’s medical history also included asthma, osteoporosis, hyperlipidemia, gastroesophageal reflux disease (GERD), uncontrolled type 1 diabetes with hypo-glycemic episodes (last glycated hemoglobin, or HbA1C, was 11.3%), hypothyroidism, pernicious anemia, con-trolled seizures, and rheumatoid arthritis.
An echocardiogram completed 1 month before the scheduled hemicolectomy showed an ejection fraction of 60% to 65% with normal diastolic function, but left ven-tricular hypertrophy was apparent. An electrocardiogram (ECG) showed a prolonged QT interval with a T-wave abnormality in the inferior leads, a new finding from the prior ECG 2 years before the scheduled hemicolectomy. On preoperative interview she denied any recent chest pain, shortness of breath, palpitations, dizziness, new symptoms of spasticity, gagging movements, or abdominal cramping. Specifically, she denied spasticity since a prior admission 5 weeks earlier when she received IVIG. She also conveyed that she commonly has a spastic episode when she discontinues her SPS medications. Before the scheduled hemicolectomy the patient had several episodes of severe hypoglycemia, which required hospitalization and treatment with 50% dextrose, with the last admission being 3 weeks before the scheduled procedure. In the preoperative clinic she was advised to continue her SPS medications, but despite this recommendation she with-held her SPS medications the day of surgery.
The morning of surgery, the patient was asymptomati-cally hypoglycemic with a blood glucose level of 70 mg/dL. Her regimen consisted of metformin at 1 g/d and an insulin glargine injection (Lantus) of 20 U nightly. Her last dose of insulin was the evening before surgery. She was treated with 1.5 ampules of 50% dextrose, which increased her glucose level to 160 mg/dL preoperatively. The patient’s surgical history included cholecystectomy, hernia repair, and multiple colonoscopies managed with inhalational anesthesia and monitored anesthesia care (MAC) techniques that yielded no adverse outcomes. Airway assessment showed Mallampati classification 2, thyromental distance greater than 3 fingerbreadths, mouth opening greater than 3 cm, and limited neck extension.
After preoperative assessment was reviewed and in-formed consent was obtained, the patient was given midazolam, 2 mg IV, before proceeding into the operat-

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 183
ing room. The operating room was quiet and warmed before the patient’s arrival. Standard ASA monitors were applied, and the patient was given 100% oxygen via face mask. Cricoid pressure was applied to the patient throughout induction and intubation given her history of uncontrolled GERD. Induction agents consisted of a ti-tration of fentanyl, 100 μg; lidocaine, 100 mg; and propo-fol, 200 mg, IV. Tracheal intubation with a 7.0-mm oral standard endotracheal tube was easily achieved without the use of a muscle relaxant via a size 3 Macintosh laryn-goscope blade providing a grade 1 view. A 20-gauge arte-rial line was placed in the right radial artery. An 18-gauge peripheral IV was placed to the left forearm. A peripheral nerve stimulator was applied over the ulnar nerve. The patient’s severe lordotic curve was padded along with other pressure points. General anesthesia was maintained with an oxygen and air mixture, propofol infusion was titrated between 120 and 200 μg/kg/min, and a remifent-anil infusion was titrated between 0.1 and 0.25 μg/kg/min to achieve a bispectral index of 40 to 60.
The initial anesthesia plan was to use a paralytic agent throughout the case as needed to facilitate adequate surgical conditions. Vecuronium, 2 mg, was chosen for its intermediate action and predictability. This agent provided adequate muscle relaxation for approximately 20 minutes to achieve a train-of-four (TOF) of 2/4 for a midline incision of the abdominal muscles and surgical exposure. The patient returned to a TOF of 4/4, and after discussion with the surgeon who believed that operative conditions were adequate, the decision was made to forgo additional paralytics. Propofol, administered as a 100-mg bolus in addition to the propofol and remifentanil infu-sions, provided adequate surgical conditions for closure of the abdominal muscles. In addition to 2 L of balanced electrolytes (Normosol-R), 500 mL of 5% dextrose in water was infused at 170 mL/h throughout the case (3 hours), and the blood glucose level was checked every hour to monitor for hypoglycemia. The patient’s glucose levels ranged from 70 to 160 mg/dL throughout the peri-operative period. The total blood loss was 250 mL and urine output was 300 mL. Ondansetron, 4 mg, was given IV before emergence.
Before extubation the patient had a TOF of 4/4 with sustained tetany for 5 seconds showing no fade, a tidal volume of 350 to 400 mL (6-8 mL/kg), and a sustained head lift greater than 3 seconds with eye opening. The patient was not administered neuromuscular block-ade reversal because sustained tetany showed no fade and she did not exhibit signs of muscle weakness. The patient was extubated to 100% oxygen via face mask 10 minutes after the remifentanil and propofol infusions were stopped. Hydromorphone, 6 mg IV, was titrated for pain management, and promethazine (Phenergan), 18.7 mg IV, was titrated for control of nausea.
She was transferred to the surgical intensive care unit
(SICU) on room air for close postoperative monitoring without any complications. Vital signs on SICU admis-sion were blood pressure of 123/72 mm Hg, pulse of 90/min, temperature of 36.6oC, respirations of 18/min; pulse oximetry was 98%, and the glucose level was 150 mg/dL.
Postoperatively the patient was managed by the colorectal surgery service with consultation to both neu-rology and internal medicine. She received morphine, 5 mg IV, as needed for pain and was restarted on her home medication regimen for SPS, including diazepam, 10 mg 3 times a day; baclofen, 20 mg 4 times daily; tiza-nidine, 2 mg 3 times a day; and hyoscyamine, 0.125 mg every 4 hours as needed for cramping. Her antiepileptic regimen also was restarted, which included levetiracetam (Keppra), 500 mg twice a day, and phenytoin, 200 mg twice daily (dosage decreased from 300 mg twice a day as her serum phenytoin level was elevated). She was also continued on a regimen of 5% dextrose with half normal saline with 20 mEq of potassium chloride at 100 mL/h because of concerns for recurrent hypoglycemia and mild hypokalemia.
On postoperative day 2 the patient transitioned from clear liquids to a regular diabetic diet, at which time she moved to the general surgical unit. She did have a decrease in her hemoglobin level to 7.5 g/dL on postoperative day 2, which required transfusion of 1 U of packed red blood cells with adequate response. Internal medicine was con-sulted for diabetes management and recommended that after discharge she be continued on a regimen of insulin glargine, 10 U at bedtime, and metformin, 1 g twice daily. She was able to tolerate a regular diet and did not have any new symptoms of spasticity or rigidity.
She remained stable and was discharged home without any incident on postoperative day 4. The patient was fol-lowed up in the colorectal surgery clinic 3 weeks after the procedure and did not have any complaints at that visit.
Discussion In our case we successfully used propofol and remifent-anil infusions with minimal paralytics, resulting in no hy-potonia at the end of the case. The patient did not report any adverse events with her previous surgery, for which an inhalational agent was used; however, the records were unavailable, and the patient did not know the dates of the surgeries. Since the time of her previous surgeries, it was unclear whether her symptoms had progressed and SPS treatments could have been increased substantially. Although regional anesthesia is an appropriate option, we elected not to use this method because of the patient’s severe spinal deformity, anxiety, failure to take her SPS medications the day of surgery, and the risk of initiating a spasm while placing the epidural/spinal anesthetic.
In a search of the medical literature, only a small number of published case studies were available. The out-comes of using general anesthesia with inhalational agents

184 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
in patients with SPS are varied (Table 1).18-22 Of the 17 cases we reviewed related to SPS, 7 cases used inhalational anesthesia, 2 cases used regional anesthesia combined with MAC, and 2 cases used a sole MAC technique (Table 22,11,23,24). Five case reports we found used a total intra-venous anesthesia (TIVA) technique (Table 3).1,16,18,25,26
• Preoperative Considerations. Preoperatively, patients should continue their immunotherapy, benzodiazepine, and baclofen to optimize the suppression of their SPS
symptoms. Baclofen, if stopped abruptly, can cause withdrawal symptoms and may require oral baclofen. Baclofen withdrawal symptoms mimic alcohol withdrawal and neuroleptic malignant syndrome. The symptoms as-sociated with withdrawal include, but are not limited to, seizures, hallucinations, sweating, confusion, labile heart rate and blood pressure, fever, and increased spasticity.27 Although there is no association with any cardiorespira-tory disorders, it is recommended to perform a pulmonary
Author/patient sex/age, y
SPS medications and dosage
Surgicalprocedure
Drugsadministered
Postoperative outcome
General anesthesia with inhalation agent
Bouw19/F/62 Diazepam, 7.5 mg twice a day; baclofen, 12.5 mg twice a day; prednisone, 20 mg/d
Colon resection Isoflurane, propofol, sufentanil, atracurium, morphine, neostigmine, glycopyrrolate
Prolong intubation 3 hours into the postoperative period
Johnson20/F/46 Diazepam 100 mg/d; intrathe-cal baclofen pumpa
Baclofen pump
Baclofen pump repair 1
Baclofen pump repair 2
Propofol, succinylcholine, desfluraneIsoflurane, nitrous oxide, sufentanil, thiopental, vecuronium, neostigmine, glycopyrrolateMidazolam, halothane, isoflurane, nitrous oxide
Weakness 2 days postoperatively
Muscle weakness and hypotonia present; patient was intubated overnight in ICU
No exacerbation of symptoms present
Obara18/F/40 Not given Thymectomy
Appendectomy
Fentanyl, thiopental, vecuronium, isoflurane, nitrous oxideDiazepam, fentanyl, thiopental, vecuronium, isoflurane, nitrous oxide
No exacerbation of symptoms present
No exacerbation of symptoms present
Qin21/M/58 Diazepam, 5 mg twice a day; baclofen, 10 mg 3 times a day
Thymectomy Midazolam, propofol, remifentanil, rocuronium, isoflurane, nitrous oxide
No exacerbation of symptoms present
Combined general/regional (epidural) anesthesia
Yamamoto22/M/76 Diazepam, 5 mg/d; baclofen, 30 mg/d; clonazepam, 1 mg/d
Thymectomy Sevoflurane, fentanyl, propofol, ropivacaine, 0.25% infusion 24 hours post-operatively
No exacerbation of symptoms present
Table 1. Case Studies of Stiff-Person Syndrome Receiving Either General Anesthesia or Regional Anesthesia Combined With General Anesthesia Abbreviations: ICU, intensive care unit; SPS, stiff-person syndrome.aThe dose was not provided in the case report.(From Ferrandis et al1 and Sidransky, Tran, Kaye24)

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 185
function test to determine if respiratory insufficiencies are present and to aid in determining a postoperative plan for possible respiratory support. Laboratory results, including electrolytes, coagulation panel, and GAD antibody levels, should be checked before surgery. Levels of GAD antibod-ies may indicate the severity of the disease and predict re-sponse to medications and immunotherapy. Coagulation laboratory findings will aid in deciding if spinal or epi-dural anesthesia is an option for the anesthetic plan. It is optimal to schedule IVIG therapy close to the surgery date
to decrease the levels of GAD antibodies, thus decreasing the chance of a spasm occurring.27
• Intraoperative Considerations. The operating room should be warmed and quiet. Any loud noises should be diminished as much as possible because it can elicit a spastic episode.27 In the case studies we reviewed, pa-tients with SPS are not characterized by having difficult airways. As a result of muscle rigidity, patient position-ing can present a challenge from difficulty flexing and extending muscles. The patient’s lordotic curve and other
Method of anesthesia
Author/ patient sex/age, y
SPS medications and dosage
Surgical procedure
Drugs administered
Postoperative outcome
Regional anesthesia (paravertebral block) and MAC
Elkassabany11/M/65 Intrathecal baclofen pumpa
Inguinal hernia Bupivacaine 0.5% Midazolam Fentanyl Propofol
Patient reported improvement of spasticity symptoms during procedure and 1 hour postoperatively
Regional anesthesia (spinal/epidural)
Shanthanna23/F/55 Baclofen, clonazepam, gabapentina
Bilateral amputation of lower extremities
Bupivacaine 0.5% Midazolam Fentanyl
Patient did not experience exacerbation of symptoms; however, anesthesia provider was unable to achieve an appropriate anesthesia level without supplementing with epidural
MAC Sidransky24/M/34 Carisoprodol, 250 mg/d; diazepam, 10 mg twice a day; gabapentin, 600 mg 3 times a day; baclofen, 30 mg/d
Permanent catheter placement
Lidocaine Propofol
No exacerbation of symptoms present
Neubert2/M/55 Not given Left ilioinguinal nerve block
Midazolam Ketamine
No exacerbation of symptoms present
Table 2. Case Studies of Stiff-Person Syndrome Receiving Regional Anesthesia or Monitored Anesthesia CareAbbreviations: MAC, monitored anesthesia care; SPS, stiff-person syndrome.aThe dose was not provided in the case report.(From Ferrandis et al1 and Sidransky, Tran, Kaye24)
Author/patient sex/age, y
SPS medications and dosage
Surgical procedure
Drugs administered Postoperative outcome
Ferrandis1/F/44 Diazepam, 50 mg 3 times daily; tizanidine, 4 mg/d
Double heart-valve replacement
Midazolam, diazepam, fentanyl, etomidate, pancuronium, propofol, remifentanil
Hypotonia was not prolonged; however, pain and stiffness with mild contractions in bilateral upper and lower extremities was present 7 hours postoperatively
Ledowski25/M/74 Clonazepam, quinine, baclofena
ENT Remifentanil, propofol No exacerbation of symptoms present
Toscano16/F/47 Diazepama Incision and drain of breast abscess
Midazolam, fentanyl, propofol, morphine
No exacerbation of symptoms present
Yagan26/M/46 Diazepam, 15 mg/d; baclofen, 30 mg/d; prednisolone, 20 mg/d
Lumbar vertebral compression fracture repair
Midazolam, lidocaine, propofol, remifentanil
No exacerbation of symptoms present
Obara18/F/40 Not given Endoscopic nasal sinus surgery
Propofol, fentanyl, vecuronium,nitrous oxide
No exacerbation of symptoms present
Table 3. Case Studies of Stiff-Person Syndrome Receiving Total Intravenous Anesthesia Abbreviations: ENT, ear, nose, and throat; SPS, stiff-person syndrome.aThe dose was not provided in the case report.(From Ferrandis et al1 and Sidransky, Tran, Kaye24)

186 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
pressure points should be padded. According to the anesthesia recommendations for pa-
tients with SPS made by Shanthanna et al,27 there are no contraindications to any anesthetic agents or procedures and no particular anesthetic technique has been shown to be safer and more effective than another. When weighing the risks and benefits of general anesthesia vs regional anesthesia, the appropriate anesthetic plan should be chosen based on the provider’s comfort level, location and type of surgery, patient preference, and severity of disease. However, it is hypothesized that inhalational agents exert their effect through GABA inhibition,18 and they have been reported to potentiate the hypotonia caused by SPS medications, particularly baclofen.28 In a case unrelated to SPS, a 49-year-old man with a spinal cord injury was scheduled to have a penile implant.28 The patient was prescribed baclofen, 25 mg 3 times a day, for muscle spasms. On induction, the patient was given fentanyl, thiopental, and atracurium. Anesthesia was maintained with isoflurane and nitrous oxide. At the completion of the surgery, the muscle relaxant was re-versed; however, the patient remained intubated because of the presence of muscle hypotonia for 6 hours following the case.28 It was discovered in the postoperative period that the patient was taking the recommended dose of baclofen and additional doses when muscle spasms were not controlled. Inhalation agents should be avoided if possible. In the event that inhalational agents are used in patients with SPS, hypotonia should be monitored closely before extubation.
In the case report by Bouw et al,19 a 62-year-old woman was scheduled for resection of a colon mass. Her SPS symptoms were managed with diazepam, 7.5 mg twice a day; baclofen, 12.5 mg twice a day; and predni-sone, 20 mg daily. On induction, she was given propofol, sufentanil (Sufenta), and atracurium. Her anesthesia was managed with isoflurane, and despite a TOF of 4/4 and full muscle relaxant reversal, the patient remained intubated 3 hours in the postoperative period because of prolonged hypotonia and respiratory failure. It was hypothesized by the authors that the inhalational agent used furthered the hypotonia by potentiating the effect baclofen has on GABAB receptors.
Although the mechanism in unclear, it has also been reported that neuromuscular blockers potentiate the hypotonia caused by SPS medications.20 In the Johnson and Miller20 case report, a 46-year-old woman was scheduled for repair of a baclofen pump. Her surgical history included postoperative weakness 2 days fol-lowing her initial baclofen pump placement. Her SPS symptoms had been managed with diazepam, 100 mg daily, and an intrathecal baclofen pump, in which the dose was not reported. During the follow-up baclofen pump repair surgery, isoflurane and vecuronium were used and resulted in muscle weakness and hypotonia.20 The patient was intubated and admitted to the intensive
care unit (ICU) overnight. When the patient returned to have a baclofen pump repaired 5 months later, inhala-tion anesthesia without muscle relaxants was used. The patient did not exhibit an exacerbation of symptoms or prolonged hypotonia in the postoperative period. Although it has not been shown that muscle relaxants are prolonged in patients with SPS, it has been recom-mended that muscle relaxants should be avoided if pos-sible.20 If muscle relaxants must be used, small doses of short-acting relaxants along with TOF monitoring are recommended.27 Although no relationship has been found between the depth of muscle relaxation and hypo-tonia in patients with SPS, it is recommended for muscle relaxants to be reversed. Currently, there is insufficient information on the use of succinylcholine in adults with diagnosed SPS.11,27
Propofol is the recommended drug for the induction and maintenance phase of anesthesia. In previous studies of propofol, it is shown to be beneficial for managing acute muscle spasms associated with SPS and it can also enhance GABA receptors in GABA-deficient patients.16
In 2 separate studies conducted in rodents, propofol was shown to enhance the GABAA receptor activity by short-ening the phase of the GABAA receptor channel closure and potentiating the GABAA receptor–mediated inhibi-tory postsynaptic currents.10,29
Regional anesthesia is an appropriate option in pa-tients with SPS but can present a challenge to the anes-thesia provider. In the Shanthanna23 case report in which a 55-year-old woman was scheduled for bilateral amputa-tion of the lower extremities, the provider was unable to achieve an appropriate anesthetic level for surgery after a spinal block without supplementing with an epidural. It is noted that the deformity of the spine can cause an unpre-dictable spinal block, and the rigidity of the muscles can make it difficult to position the patient.27 Shanthanna23 mentioned the successful use of regional anesthesia as the safest mode of anesthesia (see Table 2). However, loud noises and emotional stress, such as anxiety can exacerbate spasms. Conscious sedation should be derived in a manner adequate to keep the patient calm before placing the epidural/spinal anesthetic.23 In the case of a 65-year-old man with SPS undergoing a hernia repair, the anesthesia provider performed regional anesthesia using a paravertebral block, supplementing with a MAC technique.11 The patient reported improvement of spas-ticity symptoms during the procedure and 1 hour into the postoperative period.11
• Postoperative Considerations. Postoperatively the patient should be monitored closely for muscle spasms and weakness that could lead to respiratory failure because of drug interactions between baclofen, diazepam, and anesthetic drugs. All SPS medications should be continued in the postoperative period to prevent muscle rigidity from reoccurring. Patients may require supple-mentation with benzodiazepines to alleviate postopera-

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 187
tive symptoms. In the case study by Ferrandis et al,1 a 44-year-old woman scheduled for a double heart valve re-placement was induced with fentanyl, midazolam, etomi-date, and pancuronium. Anesthesia was maintained using TIVA with propofol and remifentanil. Postoperatively she experienced pain in her arms and legs with muscle rigidi-ty in her forearm and lower limbs without spasms. She re-quired a dose of diazepam, 5 mg IV, and morphine, 3 mg IV, in addition to her continuous infusion of midazolam (Versed). Four hours later she exhibited symptoms again and was started on a regimen of diazepam, 50 mg every 8 hours, for pain and stiffness in her legs that eventually subsided. She was discharged from the unit 3 days later without SPS symptoms.1
Conclusion Because of the unique effect that SPS has on GABA and the possible interaction of inhalational agents and muscle relaxants with SPS medications, anesthetic management of a patient with SPS can be challenging for the anesthe-sia provider. In documented case studies TIVA has been used successfully in patients with SPS without causing postoperative hypotonia (see Table 3). The patient’s comfort and safety were achieved without any residual weakness before and following emergence and extuba-tion. There were no undesirable symptoms related to SPS noted, suggesting that in our case the use of minimal paralytics, propofol, and opioids can be an appropriate and safe choice to manage patients with SPS.
REFERENCES 1. Ferrandis R, Belda J, Llau JV, Belda C, Bahamonde JA. Anesthesia for
cardiac surgery on a patient with stiff person syndrome. J Cardiothorac Vasc Anesth. 2005;19(3):370-372.
2. Neubert L, Green P, Green MS. Anesthetic care of stiff person syn-drome in the outpatient setting. J Anesthesiol Clin Sci. 2013;2(1):5.
3. Newton JC, Harned ME, Sloan PA, Salles SS. Trialing of intrathecal baclofen therapy for refractory stiff-person syndrome. Reg Anesth Pain Med. 2013;38(3):248-250.
4. Baizabal-Carvallo JF, Jankovic J. Stiff-person syndrome: insights into a complex autoimmune disorder. J Neurol Neurosurg Psychiatr. 2015;86(8):840-848.
5. Moersch FP, Woltman HW. Progressive fluctuating muscular rigidity and spasm (“stiff-man” syndrome); report of a case and some observa-tions in 13 other cases. Proc Staff Meet Mayo Clin. 1956;31(15):421-427.
6. Asher R. A woman with the stiff-man syndrome. Br Med J. 1958; 1(5065):265-266.
7. Bowler D. The ‘stiff man syndrome’ in a boy. Arch Dis Child. 1960; 35(181):289-292.
8. Ali F, Rowley M, Jayakrishnan B, Teuber S, Gershwin ME, Mackay IR. Stiff-person syndrome (SPS) and anti-GAD-related CNS degenera-tions: protean additions to the autoimmune central neuropathies. J Autoimmun. 2011;37(2):79-87.
9. Geis C, Beck M, Jablonka S, et al. Stiff person syndrome associated anti-amphiphysin antibodies reduce GABA associated [Ca(2+)]i rise in embryonic motoneurons. Neurobiol Dis. 2009; 36(1):191-199.
10. Raju R, Rakocevic G, Chen Z, et al. Autoimmunity to GABAA-recep-tor-associated protein in stiff-person syndrome. Brain. 2006; 129(12): 3270-3276.
11. Elkassabany N, Tetzlaff JE, Argalious M. Anesthetic management of a patient with stiff person syndrome. J Clin Anesth. 2006;18(3):218-20.
12. Kelly PA, Kuberski C. Stiff person syndrome: a case report. Clin J Oncol Nurs. 2014;18(4):465-467.
13. Saiz A, Blanco Y, Sabater L, et al. Spectrum of neurological syndromes associated with glutamic acid decarboxylase antibodies: diagnostic clues for this association. Brain. 2008;131(10):2553-2563.
14. Lorish TR, Thorsteinsson G, Howard FM Jr. Stiff-man syndrome updated. Mayo Clin Proc. 1989;64(6):629-636.
15. Dalakas MC, Fujii M, Li M, McElroy B. The clinical spectrum of anti-GAD antibody-positive patients with stiff-person syndrome. Neurology. 2000;55(10):1531-1535.
16. Toscano F, Vick A, Shay H, Delphin E. Total intravenous anesthesia (TIVA) for stiff-person syndrome. Open J Anesthesiol. 2012;2(4):185-187.
17. Vicente-Valor MI, Garcia-Llopis P, Mejia Andujar L, et al. Cannabis derivatives therapy for a seronegative stiff-person syndrome: a case report. J Clin Pharm Ther. 2013;38(1):71-73.
18. Obara M, Sawamura S, Chinzei M, Komatsu, Hanaoka K. Anaesthetic management of a patient with stiff person syndrome. Anaesthesia. 2002;57(5):511.
19. Bouw J, Leendertse K, Tijssen MA, Dzoljic M. Stiff person syndrome and anesthesia: case report. Anesth Analg. 2003;97(2):486-487.
20. Johnson JO, Miller KA. Anesthetic implications in stiff-person syn-drome. Anesth Analg. 1995;80(3):612-613.
21. Qin X, Wang D-X, Wu X-M. Anesthetic management of a patient with stiff-person syndrome and thymoma: a case report. Chin Med J. 2006;119(11) 963-965.
22. Yamamoto K, Hara K, Horishita T, Sata T. Considerations for general anesthesia combined with epidural anesthesia in a patient with stiff-person syndrome. J Anesth. 2007;21(4):490-492.
23. Shanthanna H. Stiff man syndrome and anaesthetic considerations: successful management using combined spinal epidural anaesthesia. J Anaesthesiol Clin Pharmacol. 2010;26(4):547-548.
24. Sidransky MA, Tran NV, Kaye AD. Anesthesia considerations in stiff person syndrome. Middle East J Anaesthesiol. 2013;22(2):217-221.
25. Ledowski T, Russell P. Anaesthesia for stiff person syndrome: success-ful use of total intravenous anaesthesia. Anesthesia. 2006;61(7):725.
26. Yagan O, Ozyilmaz K, Ozmaden A, Sayin O, Hanci V. Anesthesia in a patient with Stiff Person Syndrome. Rev Brasil Anestesiol. In press.
27. Shanthanna H, Ferrandis R, Goldkamp J. Anesthesia recommendations for patients suffering from stiff man syndrome. Orphan Anesth. 2014; 1-8. https://www.orpha.net/data/patho/Pro/en/Stiff_Man_EN.pdf. Accessed March 21, 2016.
28. Gomar C, Carrero EJ. Delayed arousal after general anesthesia associ-ated with baclofen. Anesthesiology. 1994;81(5):1306-1307.
29. Ying SW, Goldstein PA. Propofol suppresses synaptic responsiveness of somatosensory relay neurons to excitatory input by potentiating GABA(A) receptor chloride channels. Mol Pain. 2005;1(2):1-14.
AUTHORSKristi Hylan, DNP, CRNA, is a staff nurse anesthetist at University Health in Shreveport, Louisiana. She is a graduate of Our Lady of the Lake Col-lege, Baton Rouge, and Louisiana State University Health Sciences Center, New Orleans. Email: [email protected].
An-Duyen Nguyen Vu, CRNA, was a student registered nurse anes-thetist at Texas Wesleyan University in Fort Worth, Texas, at the time this manuscript was submitted. She graduated in December 2015. Email: [email protected].
Katherine Stammen, MD, is a staff anesthesiologist and medical stu-dent clerkship director at LSU Health Sciences Center–Shreveport, Depart-ment of Anesthesia. Email: [email protected].
DISCLOSURESThe authors have declared they have no financial relationships with any commercial interest related to the content of this activity. The authors did not discuss off-label use within the article.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 189
The study purpose was to evaluate preventive use of dorzolamide-timolol ophthalmic solution (Cosopt) during laparoscopic surgery with the patient in steep Trendelenburg (ST) position. Periorbital swelling, venous congestion, and elevated intraocular pres-sure (IOP) may produce low ocular perfusion. Prompt IOP reduction is important because 30- to 40-minute episodes of acute IOP elevations can result in retinal ganglion cell dysfunction. Dorzolamide-timolol oph-thalmic drops reduce IOP and may ameliorate this effect. A double-blind randomized experimental study was conducted to test the effect of dorzolamide-timolol on IOP elevation during laparoscopic surger-ies in ST position. Patients were randomly assigned to receive dorzolamide-timolol treatment or balanced salt solution following anesthesia induction. The IOP levels were measured at baseline and 30-min-
utes intervals throughout surgery. The generalized estimating equations model was used to analyze treatment and time effects and treatment by time interactions. Ninety patients were recruited, with 46 receiving dorzolamide-timolol treatment and 44 receiving balanced salt solution. Statistical analysis revealed significant treatment and time effects and treatment-time interactions on IOP. Patients’ IOP was significantly lower in the treatment group than controls (P < .05 to P < .001). Treatment effects were medium to strong. Prophylactic therapy with dorzol-amide-timolol significantly reduced IOP of surgical patients during ST positioning.
Keywords: Chemosis, intraocular pressure, ischemic optic neuropathy, ocular perfusion pressure, postop-erative visual loss.
Preventive Dorzolamide-Timolol for Rising Intraocular Pressure During Steep Trendelenburg Position Surgery
Bonnie Lee Molloy, PhD, CRNA Xiamei Cong, PhD, RNCharles Watson, MD, FCCM
This study was undertaken following a patient’s blindness due to ischemic optic neuropathy after lengthy laparoscopic prostate surgery in the steep Trendelenburg (ST) position. The anesthesia team became concerned about time-
dependent changes in ocular perfusion, periophthalmic pressure, and intraocular pressure (IOP) during laparo-scopic surgery with ST positioning. Within the confined orbit, ocular perfusion pressure (OPP) is defined as the mean arterial pressure (MAP) minus the IOP, when IOP exceeds jugular venous pressure. Intraocular pressure is the pressure exerted by the fluids (aqueous humor) in the eye and is regulated by the resistance to outflow and orthostatic pressure variations that may obstruct outflow.
Postoperative visual loss (POVL) due to posterior ischemic optic neuropathy is a rare but life-changing event. During laparoscopic abominal surgery, the ST position (> 30-degree head-down tilt of the operating room bed) is required because it enables the surgeon’s visualization of pelvic structures by displacing the bowel cephalad. However, facial engorgement and edema can be substantial in this position. Progressive periorbital edema together with elevated IOP during these proce-dures led to the hypothesis that cerebrovascular and
ophthalmic circulatory autoregulation is impaired during anesthesia administered to the patient in ST position. Increased periorbital swelling and venous congestion could contribute to potential periophthalmic hypoperfu-sion and play a primary role in the increasingly reported phenomenon of ischemic optic neuropathy following lengthy laparoscopic procedures in ST position.
Literature ReviewLee and her colleagues1 hypothesized that hypotensive ischemic optic neuropathy may be caused by a “compart-ment syndrome of the optic nerve” suggesting that “high venous pressure and interstitial tissue edema may com-promise blood flow”. This is possible because the orbit is a relatively confined space, as described by Dunker and colleagues.2 The eye and anterior optic sensing system is in the orbit. The posterior optic nerve passes through the bony optic canal from the orbit to the optic chiasm toward the brain. The authors suggest that swelling in this inelastic space can cause compression and exacerbate ischemia, thus perpetuating a cycle of injury.
Bui et al3 developed a rodent model that showed alterations in ganglion cell-related electroretinogram po-tentials during brief increases in IOP (30-40 minutes at

190 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
> 50 mm Hg). Peak IOP was a principal determinant of functional loss in these studies. Rhee et al4 demonstrated that trabecular meshwork-dysregulated, pressure-depen-dant outflow caused increased periorbital swelling and venous congestion, leading to a low flow state in the eye.
Johnstone and Grant5 studied this phenomenom and concur that with increased IOP, there is dysregulation of the orbital aqueous outflow. They showed that dependent orthostatis increased this effect and resulted in a collapse and occlusion of the lumen of the Schlemm canal. These pressure-responsive aqueous outflow changes caused reflux of blood into the anterior chamber, reversing flow. Increased IOP and impaired orbital outflow can com-press the pial vessels in the posterior segment.1,2 Thus, ocular perfusion is impaired through a progressive series of changes. Regional ischemia and death of optic nerve cells both in the anterior and posterior segments can be explained, potentially resulting in POVL. When patients have prolonged laparoscopic surgery in ST position, the physiologic result is analagous to acute glaucoma.
The purpose of this study was to evaluate preventive use of dorzolamide-timolol (Cosopt) as a measure to limit IOP increase during lower abdominal laparoscopic procedures using ST position. This fixed combination of topical dorzolamide hydrochloride and timolol maleate is widely used by ophthalmologists to control elevated IOP. Dorzolamide hydrochloride is a carbonic anhydrase II inhibitor, and timolol maleate is a topical β-adrenergic receptor blocking agent. Dorzolamide-timolol reduces IOP by decreasing the production of aqueous humor and a direct action on β2-adrenergic receptors in the ciliary processes.6 In a previous study,7 dorzolamide-timolol was administered intraoperatively to 63 of 194 subjects at 3 separate institutions when their IOP reached 40 mm Hg. A nontreatment group did not receive medi-cation because their IOP remained below 35 mm Hg. Interventional dorzolamide-timolol decreased IOP and maintained near-normal pressures while the subjects were in the ST position for 3-hour durations.7
The hypothesis of this current study is that preven-tive treatment with dorzolamide-timolol would maintain near-normal IOP during laparoscopic surgery with ST positioning, while reducing orbital edema and preventing orbital outflow dysregulation.
Materials and Methods• Study Design. A randomized, double-blind, experi-mental design was used to test the effect of preventive use of dorzolamide-timolol vs balanced salt solution (BSS) on maintaining IOP levels during a laparoscopic procedure in ST position. Subjects were randomly as-signed to 2 groups: the dorzolamide-timolol treatment group and the control group (BSS). One drop of topical dorzolamide-timolol (containing 20 mg of dorzolamide and 5 mg of timolol) or BSS was administered topically
to both eyes immediately following induction of anesthe-sia. Patients in both groups received standard anesthesia care throughout the surgery. This included dorzolamide-timolol administration when IOP reached 40 mm Hg during surgery as a standard treatment for all ST-positioned procedures at our institutions. We measured each subject’s IOP at 30-minute intervals throughout the surgery after an anesthetized baseline measurement in the supine position. A final postprocedure measurement in the supine position was obtained after termination of laparoscopy.
• Setting and Samples. All patients planned for pro-longed ST procedures at the medical center were eligible for the study. They were recruited from a population scheduled for robotic-assisted laparoscopic prostate and gynecologic procedures projected to require the ST posi-tion for at least 120 minutes. Full institutional review board approvals were obtained from the regional medical center for the July 2012 to July 2014 timeframe. With no exclusions, informed consent was obtained from each participant before surgery. The sample size estimate was calculated in the Power Analysis and Sample Size (PASS) software package (version 8.0.6, NCSS Statistical Software). Based on our previous findings7 of a medium to strong effect size (d = 0.60) of dorzolamide-timolol intervention compared with the standard care on IOP reduction during ST position, 45 subjects were needed in each group with α = .05 and power .80.• Instruments and Measures. • Demographics. Age, sex, height, weight, body mass index (BMI), and ASA physical status (classes 1-5) were documented, along with surgical procedure, medically indicated tests, fluid maintenance, and vital signs.
• Intraocular Pressure. An applanation tonometer was used for IOP monitoring (Reichert Tono-Pen XL, Reichert Technologies). This applanation tonometer is accepted as the most reliable IOP monitor in both awake and anesthetized patients.8,9 This device was determined to be the most accurate instrument for IOP measurement in a comparison study with other minimally invasive ap-planation devices.10
• Mean Arterial Pressure. The MAP was measured by an arterial catheter or noninvasive blood pressure cuff (NIBP). For direct arterial measurement, MAP was measured after calibrating the transducer at heart level (midaxillary line) when the patients were supine. For measurements in ST position, mean direct arterial pressures were measured with the transducer zeroed to the level of carotid artery. In each case, the MAP was determined as the direct mean carotid level or NIBP de-terminations. The OPP was calculated as the difference between MAP and IOP in all positions.11 • Procedures. • Training. Five anesthesia providers who served as research assistants were credentialed to monitor IOP

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 191
with the patient under anesthesia in ST position during laparoscopic urologic and gynecologic procedures. Credentialed individuals took a video course, and the technique was demonstrated with volunteers. Calibration of the applanation tonometer was performed as outlined in the Reichert Tono-Pen XL manual (black button tapped twice and inverted upside down when “UP” is visualized in the chamber; “GOOD” is visualized when calibrated). This maneuver took place before each pa-tient’s data collection. The principal investigator (BLM) then observed each of the 5 research assistants’ technique and measurements with 10 subjects to determine inter-rater reliability (IRR). The principal investigator’s rating and the calibrated reading displayed in the applanation tonometer’s window were the determinants of the correct measure. Trochim’s12 IRR correlation method was used for 60 observations and established a 98% IRR value.
• Preoperative Procedures. A sterile cover was used on the head of the tonometer for each patient in prepara-tion for IOP monitoring. Four vials of solution were contained in our case; 2 were marked A and B (explained in the section “Tonometry Measurement”), the third was BSS, and the fourth was dorzolamide-timolol. Physiologic anesthesia monitors included a 5-lead electrocardiogram (ECG), NIBP and digital pulse oximetry. Inspired and exhaled gases were monitored by side-stream infrared gas analysis (Dräger/Fabius GS).
• Intraoperative Procedures. Anesthesia protocol was standardized for all patients. Midazolam, 1 to 2 mg, was given in the preoperative holding room. Anesthesia induc-tion consisted of administration of fentanyl (1-2 μg/kg), propofol (2-3 mg/kg), and rocuronium (0.07 mg/kg) or vecuronium (0.01 mg-0.015/kg) to facilitate endotracheal intubation. Additional muscle relaxant use was left to the anesthesia provider’s discretion. Abdominal insufflation pressure was maintained at 14 to 15 mm Hg throughout the procedures. General anesthesia was maintained with a volatile inhalation agent (sevoflurane or desflurane) in 100% oxygen. Supplemental fentanyl was administered as needed. Bispectral index monitoring was used to assess the depth of anesthesia. Minute ventilation was adjusted with volume- or pressure-controlled ventilation to keep end-tidal carbon dioxide in the range of 30 to 39 mm Hg during the intraoperative period. Peak airway pressures were maintained at less than 40 cm H20 and positive end-expiratory pressure ranged from 0 to 5 cm H20.
• Tonometry Measurement. Baseline IOP was deter-mined by applanation tonometry after induction of an-esthesia with the patient in the supine position. A sterile cover was placed on the head of the tonometer, and sterile BSS eyedrops were applied before each measure-ment to prevent dryness. The applanation tonometer was placed above the pupil of each eye, and the black button was pressed once. Following 3 beeps a mean value is dis-played in the window, combining measures of 3 readings.
One drop of either vial A or vial B (dorzolamide-timolol or BSS) was administered in each eye following induction of anesthesia. Vial A or vial B was the only marking on the vials, and anesthesia research assistants were blinded as to which solution was administered. The BSS eyedrops were applied before each reading, and ocular tonometry was repeated every 30 minutes during the surgery while the patient was in ST position. The patient’s eyes were taped to prevent drying between mea-surements. Protective foam was placed over the patient’s face to prevent injury. If the IOP measurement surpassed 40 mm Hg in either group, the surgeon was made aware of the elevated IOP and 1 drop of dorzolamide-timolol was then administered to each eye as a protective measure. If IOP continued to rise in this subset of patients, a time-out occurred and all anesthesia, surgery and operating room personnel were involved in determining the ad-ditional surgical time needed. A reverse ST positioning took place for a 10-minute interval at that time if the surgeon was not nearing completion of the procedure. A return to ST then took place and tonometry monitoring continued, but these participants were removed from the study thereafter because escalating trends of IOP were af-fected by the interventions. There was no variation in the anesthetic treatment.
A protractor at the bedside determined the degree of ST, which ranged from 32 to 40 degrees. Fluid admin-istration was limited to 200 mL/h unless blood loss, he-moconcentration noted by laboratory findings, metabolic acidemia, or hypotension was noted.13 Arterial or venous blood was drawn to assess acid-base status at periodic intervals during the procedures if blood loss or respira-tory status warranted. When the patient was returned to the supine position, a final IOP measurement was obtained before emergence from anesthesia. The MAP was obtained for determination of OPP at the time of IOP reading.
• Statistical Analysis. The IBM SPSS Statistics software version 20 was used for data analysis. Descriptive statis-tics including means, standard deviations, and frequen-cies were used to describe the demographic data and IOP, MAP, and OPP patterns over time. To address the treat-ment effect (dorzolamide-timolol vs control) on repeated measures of outcomes (IOP, MAP, or OPP) throughout the surgery, the generalized estimating equations (GEE) model was used to analyze treatment and time effects and treatment by time interactions. In all GEE models, the baseline values were used as covariates. An a priori level of significance was set at P < .05.
ResultsA total of 90 patients, 42 (47%) men and 48 women (53%), were recruited for the study. Forty-six patients were randomly assigned to the dorzolamide-timolol treat-ment group and 44 patients were assigned to the control

192 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
group. There were no significant differences in demo-graphic characteristics between the 2 groups (Table 1).
• Intraocular Pressure. There was no difference in the baseline IOP levels between the 2 groups. The GEE analysis revealed significant treatment effect (Wald χ2
(1) = 21.85, P < .001) and time effect (Wald χ2
(6) = 284.74, P < .001) and treatment by time interactions (Wald χ2
(6) = 22.81, P < .01). Throughout the surgery, patients’ IOP levels were significantly lower in the dorzolamide-timolol group than in the control group at 60-minute, 90-minute, 120-minute, 150-minute, and 180-minute points (P < .05 to P < .001; Table 2, Figure 1). In the final flat position, no significant differences in IOP were found between the 2 groups. The effect size of the dorzolamide-timolol treatment on IOP reduction compared with the control during the ST position was medium to large (Cohen d = 0.57 to 0.9214).
• Mean Arterial and Ocular Perfusion Pressures. There was a significant time effect on MAP values (Wald χ2
(6) = 47.74, P < .001) throughout the surgery, but there were no treatment effect and interaction of treatment by time on MAP values (Table 3). The OPP values were sig-nificantly affected by the treatment (Wald χ2
(1) = 4.93, P < .05) and time (Wald χ2
(6) = 113.37, P < .001) and the interaction of treatment by time (Wald χ2
(6) = 12.81, P < .05). At 120 and 180 minutes, OPP values were cal-culated to be higher in the treatment group than in the control group (P < .05, respectively), but no differences were found at other data points (Table 4).
DiscussionTo the best of our knowledge, the present double-blind randomized experimental study is the first to examine
prophylactic therapy with Cosopt eyedrops on reduc-ing IOP of patients who undergo laparoscopic surgery in ST position. The results suggest that throughout the surgery, the IOP was significantly lower in the treat-ment group compared with the control group and that treatment effects were medium to strong across different time points. The current findings are consistent with our previous study in which dorzolamide-timolol was used as a perioperative intervention when IOP approached 40 mm Hg and was shown to be beneficial; in the prior study, dorzolamide-timolol reduced the IOP by a mean of 26%, providing a statistically significant decrease at all time points.7 That study was conducted at 3 different institutions, with results and conclusions being the same at all sites and providing a strong basis for conducting the present research. The highest risk population included patients with a BMI greater than 35 kg/m2 and age above 62 years.7 In addition, diabetes, vascular disease, and history of glaucoma were cited as increasing the risk of elevated IOP regardless of surgical position.1,3,6 Patients with glaucoma are asked to take their medications before laparoscopic surgery in ST position and their IOP is rou-tinely monitored at our institution.
Gilbert15 reviewed the literature and concluded that any interruption to blood flow autoregulation can lead to POVL. The IOP must remain within normal ranges to maintain optimum anatomical conditions for refrac-tion and thus vision.16 Harris et al17 studied human autoregulation and found that retinal blood flow in response to increased IOP varied markedly. An IOP of 47 mm Hg, in one subject, reduced flow to one-third of normal, suggesting that human autoregulation may fail if IOP approaches within 40 to 45 mm Hg of the
Table 1. Demographic Characteristics, and Health and Surgical Procedure Statusa
Abbreviations: BMI, body mass index; CO2, carbon dioxide; EBL = estimated blood loss; fluids, fluid maintenance; PIP, peak inspiratory pressure. a Data are shown as mean and standard deviation except for gender, which is number and percentage. There were no significant differences in demographic characteristics between the 2 groups.
Dorzolamide-timolol Characteristic group Control group Total sample
Gender, No. (%) Mean SD Mean SD Mean SD
M 19 (45.23) 23 (54.76) 42 (46.67)
F 27 (56.25) 21 (43.75) 48 (53.33)
Age (y) 56.98 9.52 57.43 10.68 57.20 10.04
BMI 30.85 9.13 29.88 6.72 30.37 8.00
CO2 (L/min) 34.49 3.49 34.74 3.79 34.61 3.62
PIP (cm H2O) 32.42 5.14 32.71 5.10 32.56 5.08
EBL (mL) 145.65 113.09 156.25 80.24 150.58 98.19
Fluids (mL) 2,600.00 678.97 2,381.48 452.38 2,488.68 579.76
ASA class 2.38 0.58 2.30 0.60 2.34 0.59
Hematocrit (%) 39.04 3.92 40.85 4.22 39.94 4.14

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 193
MAP (a critical threshold). The authors suggest that response to an autoregulatory plateau may vary with age, individual anatomy, atherosclerosis, and/or arterial hypotension. Indeed, preexisting pathophysiology, drug therapy, and existing disease entities, such as glaucoma, will disrupt an individual’s response mechanism as seen in the studies by Evans et al.18 In their research, 20 pa-tients with open-angle glaucoma were placed in the ST position, and results were compared with those of 20 healthy subjects in ST position; the results showed that all 20 patients with glaucoma exhibited faulty autoregu-
lation of central retinal artery blood flow measured by Doppler flow imaging. Such variation in patient history may explain why ophthalmic compartment syndrome, unlike intracranial or tissue compartment syndrome, is not uniformly observed at or below a range of OPPs. A compartment syndrome occurs when increased pressure in a closed tissue compartment crosses a critical perfu-sion threshold beyond which blood flow to tissues in the compartment is compromised.
Studies performed by Molloy19 and Awad et al20 noted a marked increase in IOP on ST positioning during
Table 2. Intraocular Pressure (IOP) Measures During SurgeryaIntraocular pressures were measured at baseline supine position (initial, flat), during every 30-minute interval throughout the surgery in steep Trendelenburg (ST) position, and at a final postprocedure in the supine position (final, flat).bTreatment by time interaction effects in the generalized estimating equations model. Boldface indicates statistically significant.
Time point n IOP (mm Hg) P Valueb (patient position)a Group Mean SD
Initial (flat) Control 44 12.00 4.05 > .05
Dorzolamide-timolol 46 12.61 5.32
30 min (ST) Control 44 22.80 5.51 > .05
Dorzolamide-timolol 46 19.83 5.50
60 min (ST) Control 44 27.41 6.47 < .05
Dorzolamide-timolol 46 23.15 5.48
90 min (ST) Control 44 28.30 6.08 < .01
Dorzolamide-timolol 46 22.89 5.14
120 min (ST) Control 43 30.88 7.48 < .001
Dorzolamide-timolol 45 24.11 6.53
150 min (ST) Control 24 31.21 7.76 < .001
dorzolamide-timolol 31 25.00 7.50
180 min (ST) Control 8 35.00 8.80 < .01
Dorzolamide-timolol 16 26.06 8.06
Final (flat) Control 44 18.30 5.48 > .05
Dorzolamide-timolol 46 16.91 6.19
Figure 1. Profile Plot: Preventive Dorzolamide-Timolol (Cosopt) versus Control Group at Surgical Time PointsAbbreviation: IOP, intraocular pressure.

194 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
Table 3. Mean Arterial Blood Pressure (MAP) Measures During SurgeryaMean arterial pressures were measured at baseline supine position (initial, flat), during every 30-minute interval throughout the surgery in steep Trendelenburg (ST) position, and at a final postprocedure in the supine position (final, flat).b Treatment by time interaction effects in the generalized estimating equations model.
Time point n MAP (mm Hg) P Valueb (patient position)a Group Mean SD
Initial (flat) Control 44 89.02 15.10 > .05
Dorzolamide-timolol 46 86.20 14.83
30 min (ST) Control 44 96.05 13.19 > .05
Dorzolamide-timolol 46 93.15 13.29
60 min (ST) Control 44 94.74 10.26 > .05
Dorzolamide-timolol 46 91.70 12.42
90 min (ST) Control 44 89.70 11.55 > .05
Dorzolamide-timolol 46 88.28 11.28
120 min (ST) Control 43 89.45 12.04 > .05
Dorzolamide-timolol 45 87.69 12.00
150 min (ST) Control 25 87.00 10.46 > .05
Dorzolamide-timolol 30 87.53 10.46
180 min (ST) Control 8 83.75 8.70 > .05
Dorzolamide-timolol 16 89.44 11.45
Final (flat) Control 44 85.55 11.62 > .05
Dorzolamide-timolol 46 86.59 11.48
Table 4. Ophthalmic Perfusion Pressure (OPP) Measures During SurgeryaOcular perfusion pressures were measured at baseline supine position (initial, flat), during every 30-minute interval throughout the surgery in steep Trendelenburg (ST) position, and at a final postprocedure in the supine position (final, flat).b Treatment by time interaction effects in the generalized estimating equations (GEE) model. Boldface indicates statistically significant.
Time point n MAP (mm Hg) P Valueb (patient position)a Group Mean SD
Initial (flat) Control 44 77.16 15.51 > .05
Dorzolamide-timolol 46 74.09 14.05
30 min (ST) Control 44 73.89 14.30 > .05
Dorzolamide-timolol 46 73.98 14.13
60 min (ST) Control 44 68.20 12.34 > .05
Dorzolamide-timolol 46 68.63 11.72
90 min (ST) Control 44 61.37 13.22 > .05
Dorzolamide-timolol 46 64.93 12.03
120 min (ST) Control 43 58.69 12.93 < .05
Dorzolamide-timolol 45 64.42 10.70
150 min (ST) Control 25 56.40 3.23 > .05
Dorzolamide-timolol 30 62.20 9.96
180 min (ST) Control 8 49.75 11.35 < .05
Dorzolamide-timolol 16 63.13 9.87
Final (ST) Control 44 66.42 11.31 > .05
Dorzolamide-timolol 46 68.41 11.36

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 195
robotic procedures in higher risk populations. Recent recommendations from the Anesthesia Patient Safety Foundation (APSF) propose that preoperative consent include informing such patients of their risk of visual impairment and that this information be given by both surgical and anesthesia providers. The APSF held a POVL multidisciplinary conference in 2013 with anesthesia, surgery, and ophthalmology researchers and clinicians. A consensus recommendation was to elevate the head of ST position procedures at intervals to relieve venous conges-tion and to stage long prone procedures.21
Because most anesthesia providers rarely measure IOP, a visual observation scale was developed by Molloy/Bridgeport Anesthesia Associates for patients undergoing laparoscopic procedures in ST position. This measure-ment scale correlates ocular signs to IOP levels.22 Eyelid edema warns the practitioner that IOP is rising. In the study by Molloy,22 there was a correlation of eyelid edema with 2.5 times the baseline IOP. Conjunctival edema, known as chemosis, proved a valuable predictor of IOP above 40 mm Hg (area under the curve of the receiver operator curve, 0.79 ± SD 0.718), the critical threshold at which point ophthalmologists suggest in-tervention. Chemosis correlated with IOP 3.4 times the baseline via a logistic regression analysis. In most cases this approaches an IOP of 40 mm Hg since the normal IOP is 10 to 15 mm Hg. Because chemosis has reliably predicted IOP elevation above 35 mm Hg, we recommend treatment whenever chemosis is observed (Figure 2). With the preventive dorzolamide-timolol therapy, visual signs of periorbital edema and chemosis together with IOP decreased.
• Alternative Interventions. Porciatti and Nagaraju23 cited a benefit in reverse Trendelenburg positioning (head-up tilt) and illustrated both a decrease in IOP and an improvement in retinal ganglion cell function with this intervention. Linder et al24 also proposed that eleva-tion of the head above the level of the heart may reverse
the effects of the gravity-induced, orthostatic venous pressure gradient, resulting in a decreased IOP. A trial of flat supine rest stop was investigated by Molloy and Watson25 at the 60-minute point of ST positioning. This intervention requires undocking and redocking the robot for only 7 to 10 minutes during robotic cases, removing instrumentation, then replacing and returning to ST posi-tion. The IOP decreased toward normal when tonometry was measured within 30 minutes of the flat supine inter-vention. By the second hour the mean IOP for the supine intervention group was 18.4 mm Hg, whereas it was 31.6 mm Hg in the control group. The findings support the contention that a flat supine interval minimizes the impact on IOP and OPP of lengthy laparoscopic surgery in ST position. The beneficial effect was demonstrable after an additional 2 hours’ return to the ST position. Johnstone and Grant5 also found that outflow improved on inversion. They showed that the orthostatic pressure change unloaded the trabecular meshwork drainage system and reopened the lumen of the Schlemm canal.
Surgeons may be resistant to modifying position once surgery is under way. Therefore, preventive measures that directly limit escalating IOP without disruption of surgery should be considered.
• Practice Implications. Both preventive and interven-tional dorzolamide-timolol may be employed to control IOP during laparoscopic procedures involving ST posi-tion. Shamesh et al26 identified the benefits of a second daily dose. Subsequent dosing lowers IOP 25.9%. As a result, we employ preventive dorzolamide-timolol in the high-risk population (diabetes, vascular disease, glau-coma history, high BMI, and age above 62 years). Also, when patients present with a history of glaucoma or high IOP, their scheduled therapy is administered before they enter the operating room, as a preventive measure. A subsequent dorzolamide-timolol intervention should be considered if IOP levels approach 40 mm Hg or if chemo-sis is observed.
Pinkney and colleagues27 reviewed the relationship of patient positioning and IOP across all surgical specialties. They concluded that the rise in IOP was time dependent and, consequently, that patients were very likely to be at risk of POVL events as the duration of surgery in-creased. Both prone and ST position cases were included. Cases of POVL reported to the American Society of Anesthesiologists registry occurred after a mean surgi-cal time of 5.5 hours.1 We recommend a time-out at the 4-hour surgical time point to discuss projected surgical completion. A supine intervention is introduced at that time if ST or prone position is needed for an additional hour or more.
ConclusionDorzolamide-timolol (Cosopt) drops significantly reduce elevated IOP and periorbital edema of patients who
Figure 2. Chemosis Effects After 2.5 hours of Steep Trendelenburg PositionaaChemosis correlated to 3.4 times baseline intraocular pressure (> 35-40 mm Hg).

196 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
undergo lengthy laparoscopic robotic surgery in the ST position. Preventive and interventive treatment at any time during the ST procedure arrested the trend in esca-lating IOP. Practitioners should monitor signs of perior-bital edema if not IOP, and an institutional protocol may help limit the potential for ischemic optic neuropathy and POVL when procedures in prolonged ST or prone position are indicated. Preventive dorzolamide-timolol may provide practitioners with an alternative to frequent repositioning during these prolonged surgical procedures.
REFERENCES 1. Lee LA, Roth S, Posner KL, et al. The American Society of Anesthesi-
ologists Postoperative Visual Loss Registry: analysis of 93 spine cases with postoperative visual loss. Anesthesiology. 2006;105(4):652-659.
2. Dunker S, Hsu HY, Sebag J, Sadun AA. Perioperative risk factors for pos-terior ischemic optic neuropathy. J Am Coll Surg. 2002;194(6):705-710.
3. Bui BV, Edmunds B, Cioffi GA, Fortune B. The gradient of retinal functional changes during acute intraocular pressure elevation. Invest Ophthalmol Vis Sci. 2005;46(1):202-213.
4. Rhee DJ, Alvarado JA, Calkins DJ, Gupta N. The brain the drain. Eye Net. 2011 Nov/Dec;36-41.
5. Johnstone MA, Grant WG. Pressure-dependent changes in structures of the aqueous outflow system of human and monkey eyes. Am J Ophthalmol. 1973;75(3):365-383.
6. Yeh J, Kravitz D, Francis B. Rational use of the fixed combination of dorzolamide-timolol in the management of raised intraocular pres-sure and glaucoma. Clin Ophthalmol. 2008;2(2):389-399.
7. Molloy BL, Cong X. Perioperative dorzolamide-timolol intervention for rising intraocular pressure during steep Trendelenburg position surgery. AANA J. 2014;82(3):203-211.
8. Riva CE, Hero M, Titze P, Petrig B. Autoregulation of human optic nerve head blood flow in response to acute changes in ocular perfusion pressure. Graefes Arch Clin Exp Ophthalmol. 1997;235(10):618-626.
9. Baskaran M, Raman K, Ramani KK, Roy J, Vijaya L, Badrinath SS. Intraocular pressure changes and ocular biometry during Sirsa-sana (headstand posture) in yoga practitioners. Ophthalmology. 2006;113(8):1327-1332.
10. Lasseck J, Jehle T, Feltgen N, Lagrèze WA. Comparison of intraocular tonometry using three different non-invasive tonometers in children. Graefes Arch Clin Exp Ophthalmol. 2008;246(10):1463-1466.
11. Hayreh SS. Ischemic optic neuropathy. Prog Retin Eye Res. 2009;28(1): 34-62.
12. Trochim WMK, Donnelly JP. Nonprobability sampling. The Research Methods Knowledge Base website. http://www.socialresearchmethods.net/kb/sampnon.php. Updated October 20, 2006. Accessed March 26, 2014.
13. Baig MN, Lubow M, Immesoete P, Bergese SD, Hamdy EA, Mendel E. Vision loss after spine surgery: review of the literature and recom-mendations. Neurosurg Focus. 2007;23(5):E15.
14. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: Lawrence Earlbaum Associates; 1988.
15. Gilbert ME. Postoperative visual loss: a review of the current litera-ture. Neuroophthalmology. 2008;32(4):194-199.
16. Murgatroyd H, Bembridge J. Intraocular pressure. Br J Anaesth. 2008;8(3):100-103.
17. Harris A, Ciulla TA, Chung HS, Martin B. Regulation of retinal and optic nerve blood flow. Arch Ophthalmol. 1998;116(11):1491-1495.
18. Evans D, Harris A, Garrett M, Chung HS, Kagemann L. Glaucoma
patients demonstrate faulty autoregulation of ocular blood flow dur-ing posture change. Br J Ophthalmol. 1999;83(7):809-813.
19. Molloy BL. Implications for postoperative visual loss: steep Tren-delenburg position and effects on intraocular pressure. AANA J. 2011;79(2):115-121.
20. Awad H, Santilli S, Ohr M, et al. The effects of steep Trendelenburg positioning on intraocular pressure during robotic radical prostatec-tomy. Anesth Analg. 2009;109(2):473-478.
21. Cooper J, Caplan R, Gaba D. APSF workshop engages audience in communication skills and drills. APSF Newslett. 2013:27(3):45-72.
22. Molloy BL. A preventive intervention for rising intraocular pressure: the development of the Molloy/Bridgeport Anesthesia Associates observation scale. AANA J. 2012;80(3):213-222.
23. Porciatti V, Nagaraju M. Head-up tilt lowers IOP and improves RGC dysfunction in glaucomatous DBA/2J mice. Exp Eye Res. 2010; 90(3):452-460.
24. Linder BJ, Trick GL, Wolf ML. Altering body position affects intra-ocular pressure and visual function. Invest Ophthalmol Vis Sci. 1988; 29(10):1492-1497.
25. Molloy BL, Watson C. A comparative assessment of intraocular pres-sure in prolonged steep Trendelenburg vs. supine position interven-tion. J Anesth Clin Sci. 2012;1-9. http://www.hoajonline.com/journals/jacs/content/pdf/9.pdf. Accessed March 21, 2016.
26. Shamesh G, Moisseiev E, Lazar M, Kurtz S. Intraocular pressure reduction of fixed combination timolol maleate 0.5% and dorzol-amide 2% (Cosopt) administered three times a day. Clin Ophthalmol. 2012;6:283-287.
27. Pinkney TD, King AJ, Walter C, Wilson TR, Maxwell-Armstrong C, Acheson AG. Raised intraocular pressure (IOP) and perioperative visual loss in laparoscopic colorectal surgery: a catastrophe waiting to happen? A systematic review of evidence from other surgical speciali-ties. Tech Coloproctol. 2012;16(5):331-335.
AUTHORSBonnie Lee Molloy, PhD, CRNA, is a Certified Registered Nurse Anes-thetist employed by and affiliated with Bridgeport Anesthesia Associates, Bridgeport Hospital/Yale New Haven Health System, Bridgeport, Con-necticut. Email: [email protected].
Xiamei Cong, PhD, RN, is employed by the University of Connecticut School of Nursing, Storrs, Connecticut. Email: [email protected] .
Charles Watson, MD, FCCM, is past chairman, Anesthesia Department, Bridgeport Hospital, and employed by Bridgeport Anesthesia Associates, Bridgeport, Connecticut. Email: [email protected].
DISCLOSURESThe authors have declared they have no financial relationships with any commercial interest related to the content of this activity. The authors did not discuss off-label use within the article.
ACKNOWLEDGMENTSThe authors thank the AANA Foundation, Park Ridge, Illinois, for financial and collaborative support. They also thank these mentors and advisors: Anthony Peluso, MD, Anesthesia Department, Bridgeport Anes-thesia Associates, Bridgeport, Connecticut, advisor; Anthony Musto, MD, chairman of ophthalmology, Bridgeport Hospital Bridgeport, Connecticut; Bruce Shields, MD, past chairman, Department of Ophthalmology, Yale New Haven Health System, New Haven, Connecticut; research assistants Esra Anson, CRNA; Keisha Johnson, CRNA; Kathryn Sapiente, CRNA, and Theresa Donnelly, CRNA; and surgical associates Scott Thornton, MD, colorectal surgeon, Bridgeport Hospital, Daniel Silasi, MD, robotic gyne-cologic surgeon, Yale New Haven Health System; and medical illustrator Victoria Skomal Wilchinsky.

198 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
Pseudocholinesterase abnormalities are a genetic cause of aberrant metabolism of the depolarizing muscle relaxant succinylcholine. This article examines a case where succinylcholine was chosen to facili-tate intubation due to its ultra short duration and the request of the surgeon to monitor motor evoked poten-tials. Following succinylcholine administration the neu-
rophysiologist was unable to obtain motor evoked potentials. This case study highlights the intraoperative and postoperative management of an elderly patient with an unknown pseudocholinesterase deficiency.
Keywords: Anesthesia, dibucaine number, motor evoked potentials, pseudocholinesterase deficiency.
Unknown Pseudocholinesterase Deficiency in a Patient Undergoing TIVA with Planned Motor Evoked Potential Monitoring: A Case Report
Candace Binkley, MSN, CRNA
Cholinesterase is a broad term used to describe a family of enzymes that hydrolyze choline esters. Two subtypes of cholinesterase exist: acetylcholinesterase and pseudocholinester-ase (PChE). Some individuals demonstrate
genetic variations in PChE that can cause prolonged apnea and paralysis when exposed to the depolarizing muscle relaxant succinylcholine due to aberrant metabo-lism of the drug. Sixty-five inherited variants have been identified that may cause slight to marked post-succi-nylcholine paralysis.1 Monitoring intraoperative motor evoked potentials requires the absence of paralysis. This frequently leads the anesthesia provider to select suc-cinylcholine to facilitate intubation due to its ultra short duration. In the presence of an unknown pseudocholin-esterase deficiency, the duration of paralysis after succi-nylcholine administration may be significantly increased, resulting in the inability to monitor evoked potentials. This case report is an addition to the available literature describing the impact an unknown pseudocholinesterase deficiency can have on the anesthetic plan.
Case SummaryAn 81-year-old man (182 cm, 88 kg) presented to the surgical suite for C3-C6 anterior discectomy and fusion. The patient had a past medical history significant for hy-pertension, sleep apnea, chronic obstructive pulmonary disorder (COPD), and lung cancer status post chemo and radiation. Past surgical history included an appen-dectomy, cholecystectomy, surgically repaired abdominal aortic aneurysm (AAA), and left upper lobectomy. The preoperative evaluation completed by the anesthesi-ologist indicated that the patient complained of fear due to the inability to move during a previous anesthetic. During the interview with the student registered nurse anesthetist, the patient could not recall what surgery this
had occurred but stated it was not experienced during his last procedure. The patient had no allergies and was unaware of any surgical or anesthetic complications among his closest blood relatives. The student registered nurse anesthetist’s subjective preoperative airway assess-ment did not indicate a potential difficult airway. The patient’s electronic record from the previous aneurysm repair revealed an uncomplicated intubation facilitated by succinylcholine. When reviewing the record for the lobectomy it was noted that rocuronium had been given to assist with intubation.
The patient was transported into the OR. Standard anesthesia monitors were applied and preoxygenation occurred with 10 L per minute of oxygen. General an-esthesia was induced at 0754 with lidocaine, 100 mg; propofol, 150 mg; and fentanyl, 250 μg. Intubation was facilitated with 100 mg, succinylcholine.
In this case the surgeon requested that nervous system function be monitored utilizing motor evoked potentials (MEPs). When MEP monitoring is indicated, anesthesia providers typically avoid nondepolarizing neuromuscu-lar blockers and volatile anesthetics due to profound de-pression of motor evoked response amplitude.2 For this reason succinylcholine was chosen to assist with tracheal intubation and total intravenous anesthesia was planned. The anesthetist intubated the patient without difficulty and endotracheal tube placement was confirmed by the presence of end-tidal carbon dioxide (ETCO2), chest rise, and bilateral breath sounds. Total intravenous anesthesia (TIVA) was initiated utilizing a propofol drip started at100 μg/kg/min and a remifentanil drip started at 0.25 μg/kg/min. These infusions were titrated based on hemo-dynamic parameters and surgical stimulation to maintain an adequate plane of anesthesia.
The patient was prepped and an arterial line was placed for hemodynamic monitoring. Incision was made at 0856.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 199
The neurophysiologist attempted to establish the patient’s baseline MEPs. At 0901 the neurophysiologist made the surgeon, CRNA, and student registered nurse anesthetist aware that motor evoked potentials were unable to be elicited. After confirming with the anesthesia team that succinylcholine had been administered the neurophysi-ologist began to troubleshoot the monitoring equipment.
The student registered nurse anesthetist checked a train of four (TOF) response using the nerve stimulator to evaluate the patient’s recovery from neuromuscular blockade. The lack of response led to a presumptive di-agnosis of pseudocholinesterase deficiency. The battery and electrodes of the nerve stimulator were checked and confirmed to be in working order. The surgeon and anes-thesiologist were made aware of the lack of response. The surgeon stated the case could be safely continued without the motor evoked potentials and requested that MEPs periodically be followed to detect the return of muscle responsiveness.
Early in the case the patient experienced hypotension and a phenylephrine infusion was initiated and titrated to maintain a mean arterial pressure of 70 or greater. Otherwise, the case remained uneventful. Approximately 3 hours into the case, at 1202, the neurophysiologist notified the team that the MEPs had returned to the pa-tients’ presurgery baseline. The student registered nurse anesthetist rechecked the TOF response and noted 4 strong equal twitches. MEPs were then monitored con-tinuously throughout the remainder of the surgery.
The case was completed at 13:04. Five hours and 10 minutes had elapsed since the succinylcholine had been administered. After discussion among the anesthesia team, propofol and remifentanil were discontinued in an-ticipation of emergence. Approximately 20 minutes later, despite measurable MEPs and a complete return of the TOF, the patient remained weak. The patient was able to blink eyes in response to questions but could not lift arms, legs, or head off the bed. When asked to take a maximal inhalation, tidal volume was noted to be less than 100 mL. The cause of the prolonged paralysis was explained to the patient to decrease anxiety. Fentanyl, 100 μg and a propofol drip at 50 μg/kg/min were initiated for patient comfort and sedation. The patient was taken to the post anesthesia care unit (PACU) intubated. The anesthesiolo-gist continued the care of the patient in PACU. According to the extubation note written by the anesthesiologist, the patient was weaned to a t-piece and the endotracheal tube was removed at 14:46. This was approximately 7 hours after the succinylcholine administration. The patient was taken from the PACU to the intensive care unit for con-tinued airway monitoring and subsequently discharged to a rehabilitation facility 5 days later.
DiscussionProlongation of succinylcholine can be caused by either
a decreased quantity or quality of pseudocholinesterase. Diminished quantities may be seen in the presence of malignancies, pregnancy, liver disease, collagen vascu-lar disease, malnutrition, and hypothyroidism.3 In this case, the dibucaine inhibition test was drawn and sent for analysis to determine if the patient had an atypical variant of PChE. The normal result of the dibucaine inhibition test is 80. This means that 80% of the PChE activity was inhibited by the local anesthetic dibucaine. These individuals are labeled homozygous normal and would be briefly paralyzed by succinylcholine. Those with a dibucaine number of 20 would be homozygous atypical and can be expected to have a marked response to succinylcholine with paralysis typically exceeding 1 hour. A dibucaine inhibition test result of 60 would be defined as heterozygous and generally only produce a slight prolongation of succinylcholine. Postoperatively, it was noted that the patient’s dibucaine inhibition test result was 27. This indicates an atypical PChE variant with the genetic label of homozygote atypical.1,2 The inci-dence of a patient homozygous for pseudocholinesterase mutations is one in 2,500 patients.4
Studies have shown that patients with pseudocholin-esterase deficiency have a normal response to remifent-anil, leading the author to believe it is unlikely that the remifentanil contributed to the prolonged recovery of the patient.5 Remifentanil is a synthetic opioid with swift onset and short duration. It allows predictable titration of anesthesia with rapid recovery of consciousness and respiration independent of the duration of infusion. The context-sensitive half-life is 3-4 minutes. Remifentanil is metabolized by nonspecific esterases in tissues and blood and is not mediated by pseudocholinesterase.6
An indication that this patient may have had a pseu-docholinesterase deficiency came from the preoperative interview when the patient stated that he was unable to move during a prior anesthetic. Past surgical records for the aortic aneurysm repair did include the administra-tion of succinylcholine followed by rocuronium. TOF response had not been charted between the two, however 6 hours later a four-twitch response to TOF was docu-mented prior to reversal. The patient was taken to PACU intubated and the reason indicated on the anesthesia dis-charge summary was pulmonary edema. The lobectomy had occurred after the AAA repair and succinylcholine had not been administered. This explains why the patient had indicated he could not recall having an anesthetic complication with his most recent surgery.
The author acknowledges that a baseline TOF should have been elicited prior to the administration of suc-cinylcholine. An early discovery could have alerted the surgeon to the inability to elicit intraoperative MEPs prior to skin incision. Multiple case reports describe the importance of monitoring neuromuscular blockade when administering succinylcholine.3,4,7,8

200 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
When faced with a patient experiencing a prolonged duration of paralysis, in addition to safety, a primary goal is comfort of the patient. The patient was found to be awake and able to blink eyes in response to questioning. The patient was reassured, sedated, and ventilated until it was decided by the anesthesiologist that the patient satisfactorily met the extubation criteria. The patient was educated regarding his atypical enzyme and given a letter regarding his pseudocholinesterase deficiency for future anesthesia experiences.
ConclusionIn summary, this was a unique case of unanticipated prolonged paralysis observed in an elderly patient during a surgery where motor evoked potentials were being monitored. The inability to elicit a TOF response led the student registered nurse anesthetist to an early presump-tive diagnosis of pseudocholinesterase deficiency. In this patient population education regarding the cause of the paralysis is important to decrease anxiety and avoid the future use of depolarizing muscle relaxants by other healthcare providers.
REFERENCES 1. Soliday FK, Conley YP, Henker R. Pseudocholinesterase deficiency:
a comprehensive review of genetic, acquired, and drug influences. AANA J. 2010;78(4):313-20.
2. Haghighi SS, Madsen R, Green KD, Oro JJ, Kracke GR. Suppression of motor evoked potentials by inhalation anesthetics. J Neurosurg Anesthesiol.1990;2(2):73-78.
3. Maiorana A, Roach RB Jr. Heterozygous pseudocholinesterase defi-ciency: a case report and review of the literature. J Oral Maxillofac Surg. 2003;61(7): 845-847.
4. Cassel J, Staehr-Rye AK, Nielsen CV, Gätke MR. Use of neuromuscular monitoring to detect prolonged effect of succinylcholine or mivacu-rium: three case reports. Acta Anaesthesiol Scand. 2014;58(8):1040-043.
5. Manullang J, Egan TD. Remifentanil’s effect is not prolonged in a patient with pseudocholinesterase deficiency. Anesth Analg. 1999;89(2): 229-230.
6. Michelsen LG, Hug CC, Jr. The pharmacokinetics of remifentanil. J Clin Anesth. 1996;8(8):679-682.
7. Ramirez JG, Sprung J, Keegan MT, Hall BA, Bourke DL. Neostigmine-induced prolonged neuromuscular blockade in a patient with atypical pseudocholinesterase. J Clin Anesth. 2005;17(3):221-224.
8. Branch A, Rafacz J, Boudreaux L. Prolonged neuromuscular block in a 74-year-old patient. AANA J. 2011;79(4):317-21.
AUTHORCandace Binkley, MSN, CRNA, was a senior student registered nurse anes-thetist at Bloomsburg University, Geisinger school of nurse anesthesia, in Danville, Pennsylvania at the time this article was written. She currently is practicing as a CRNA in Virginia and Pennsylvania. Email: [email protected].
DISCLOSURESThe author has declared no financial relationships with any commercial interest related to the content of this activity. The author did not discuss off-label use within the article.
ACKNOWLEDGMENTThe author thanks the Geisinger Bloomsburg Nurse Anesthesia Program Director, Brenda Wands, PhD, CRNA, for her dedication to her students and encouragement to publish.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 201
AANA Journal CourseUpdate for Nurse Anesthetists
Tranexamic Acid in Anesthetic Management of Surgical Procedures
Jessica Mayeux, MSN, CRNA Kathy Alwon, MSN, CRNAShawn Collins, DNP, PhD, CRNAIan Hewer, MSN, MA, CRNA
ObjectivesAt the completion of this course, the reader should be able to:
1. Describe the physiologic process in which tran-examic acid inhibits fibrinolysis.
2. Identify contraindications to the administration of tranexamic acid.
3. Describe administration guidelines of tranexamic acid.
4. Identify surgeries in which tranexamic acid could provide benefit to the patient.
5 Discuss adverse effects associated with administra-tion of tranexamic acid.
IntroductionHigher perioperative blood loss is associated with surgi-cal procedures such as cardiac, orthopedic, and trauma procedures. One of the most common treatments of massive blood loss is blood transfusion, but there are many complications and risks associated with this practice. With advancements in surgical techniques,
autologous blood donations, cell scavenge, and antifi-brinolytic drugs, healthcare providers have been able to decrease the number of blood transfusions and thus the associated complications. Decreasing perioperative bleeding through the prophylactic use of antifibrinolytic agents, such as aprotinin, tranexamic acid (TXA), and ε-aminocaproic acid (EACA), has become increasingly popular. This journal course will examine the properties of TXA and use of this medication in the operating room.
Historical BackgroundPresently, the only labeled indications for TXA by the US Food and Drug Administration (FDA) are for short-term use in patients with hemophilia undergoing tooth extractions and to treat menorrhagia.1 However, since the 1960s, TXA commonly has been prescribed off-label to minimize blood loss for various high blood loss surger-ies such as cardiac and orthopedic surgical procedures. Recently, TXA also has been used in trauma surgery to decrease blood loss.2 Despite the success of TXA as an an-tifibrinolytic—and its widespread use in countries such
2
Blood loss during surgical procedures poses a grave risk to the patient, but transfusion is costly and associ-ated with adverse outcomes. Antifibrinolytics, how-ever, offer an economical and effective means of decreasing blood loss associated with surgical proce-dures. Tranexamic acid (TXA) is an antifibrinolytic that blocks lysine-binding sites of fibrinogen and fibrin, pre-venting the breakdown of existing clots. This journal course reviews extensive research demonstrating that antifibrinolytics such as TXA decrease blood loss and in some studies reduce allogeneic transfusion require-ments. In addition, this journal course addresses con-
cerns that use of antifibrinolytics increases embolic events, reviews research that demonstrates TXA does not increase the incidence of vascular occlusive events, and describes methods of TXA use in cardiac and orthopedic surgical procedures, neurosurgery, and obstetrics. The Certified Registered Nurse Anesthetist should consider the possibility, on a case-by-case basis, of using TXA in surgical procedures to reduce blood loss with minimal adverse effects.
Keywords: Antifibrinolytic, coagulant, surgery, surgi-cal blood loss, tranexamic acid.
AANA Journal Course No. 36: AANA Journal course will consist of 6 successive articles, each with an objective for the reader and sources for additional reading. This educational activity is being presented with the understanding that any conflict of interest on behalf of the planners and presenters has been reported by the author(s). Also, there is no mention of off-label use for drugs or products. Please visit AANALearn.com for the corresponding exam questions for this article.

202 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
as the United Kingdom and Japan—it was not as popular in the United States until the early 2000s, when apro-tinin, an antifibrinolytic, was removed from the market.
In 2008, TXA was proposed to be included in the World Health Organization (WHO) Model List of Essential Medicines for reducing perioperative blood loss in adults undergoing cardiac surgical procedures requiring cardiopulmonary bypass (CPB); in 2011, that proposal was approved. The Model List of Essential Medicines helps countries plan for effective healthcare delivery by identifying the potential impact and impor-tance of medications. Following inclusion of TXA in the Model List of Essential Medicines for cardiac procedures, in 2013 it was included for use in adult trauma patients with ongoing substantial hemorrhage, or at risk of severe hemorrhage within 8 hours of injury.3
Use of Tranexamic Acid to Decrease Alloge-neic Blood RequirementsProviding universal access to safe blood products is a major objective of global health agencies, such as the WHO. However, considering the limited supply and cost of blood products and the risk of adverse outcomes asso-ciated with blood transfusion, interventions such as TXA administration that could reduce transfusion require-ments are highly desirable. A systematic literature review suggests that administration of blood products is associ-
ated with increased morbidity and mortality, and urges reevaluation of transfusion practices among healthcare providers.4
Allogeneic blood transfusion is a multibillion-dollar industry with increasing costs and decreasing supply.5 In 2009 alone, the costs the American Red Cross incurred to provide whole blood and its components were estimated to be $2.217 billion.5 The most recent estimated cost of 1 U of red blood cells is $210.74, and the charge to the patient receiving the transfusion is $343.63.6 In compari-son, 1 g of TXA supplied in a 10-mL vial is estimated to cost between $45 and $55.7 There is growing evidence to support the use of drugs such as TXA in the reduction of perioperative blood loss; this could reduce the frequency of blood transfusion requirements, ultimately allowing for improved allocation of resources and decreased costs to patients.5
Coagulation and FibrinolysisHemostasis is the complex process of maintaining vas-cular integrity, limiting blood loss, and keeping blood in a fluid state. It is a delicate balance between vascular, platelet, and plasma factors that create a fibrin clot and the regulatory mechanisms of the fibrinolytic system that dissolve a fibrin clot.8 Hemostasis begins with the forma-tion of a platelet plug, followed by the creation of a fibrin network that binds to and strengthens the platelet plug.8
Figure 1. Coagulation Cascade and FibrinolysisAbbreviations: Ca++, calcium ion; tPA, tissue plasminogen activator; uPA, urokinase.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 203
The coagulation cascade and fibrinolytic system are ac-tivated simultaneously in normal circumstances, which allows repair of the vascular injury while preventing thrombosis and ischemia.8 Figure 1 depicts the different components of hemostasis: platelet-mediated hemostasis, plasma-mediated hemostasis, and fibrinolysis.
Just as important as forming a blood clot through coagulation is the process of removing the blood clot by fibrinolysis. The coordinated events of coagulation and fibrinolysis must occur together to allow appropriate blood flow without blood loss.9 The fibrinolytic system consists of plasminogen, which becomes converted into plasmin using plasminogen activators: tissue plasminogen activator (tPA) and urokinase.9 In the initial stages of co-agulation, plasminogen becomes trapped in the clot while waiting to be activated into plasmin.8 Plasminogen acti-vators tPA and urokinase are released slowly by the sur-rounding damaged endothelial cells.9 Within a few days of the clot being formed and the blood vessel stabilized, tPA reaches plasminogen and converts it into plasmin.9
Once activated, lysine-binding sites on plasmin are responsible for binding with fibrin, cell surface recep-tors, and other proteins that help mediate fibrinolysis, such as α2-antiplasmin.9 One of the primary regulatory proteins of the fibrinolytic system, α2-antiplasmin is re-sponsible for inactivating tPA and urokinase.9 Plasmin proteolyzes fibrin into soluble fibrin degradation prod-ucts and d-dimer, which are then removed by the circula-tory system.10 Figure 2 presents a schematic diagram of fibrinolysis.
Inhibition of fibrinolysis can occur at 2 points, by either inhibiting binding of the plasminogen activators or preventing the binding of plasmin to the fibrin mesh by
blocking the lysine-binding sites.11 Tranexamic acid acts to prevent fibrinolysis by blocking the lysine-binding sites in a similar mechanism to α2-antiplasmin.
Pharmacology of Tranexamic AcidTranexamic acid is a synthetic antifibrinolytic amino acid that competitively blocks the lysine-binding sites of both plasminogen and plasmin, therefore inhibiting each enzyme’s action. Plasmin usually assists with dissolving blood clots, but when TXA saturates the lysine-binding sites of plasminogen and plasmin, plasminogen can still be converted to plasmin, but plasmin can no longer bind to fibrin. Without the presence of plasmin, there is no degradation of fibrin, and thus bleeding is reduced.
Potency comparisons have varied significantly accord-ing to tests used, but TXA has approximately 8 times the antifibrinolytic activity of EACA.2 Tranexamic acid is minimally protein bound and cleared by the kidneys. In patients with normal renal function, TXA’s half-life is 2 to 3 hours.12 Lower dosing strategies should be con-sidered for patients with kidney disease because of TXA being cleared by the kidneys. Impaired renal function does not constitute a contraindication, but to avoid ac-cumulation, it should be given over longer intervals and adjusted to patient weight. The most recent suggestions regarding renal dosing have been given by Nuttall et al (Table 1).13
Side effects and adverse reactions of TXA are rare and appear limited; mild side effects include nausea, vomit-ing, and diarrhea. Absolute contraindications include active intravascular clotting disorders (Table 2).12 Use of TXA in conjunction with other procoagulant drugs could also increase the likelihood of thrombotic complications. The most recent 2011 Cochrane Review on antifibrino-lytics indicated that TXA does not increase or decrease the risk of thrombotic events such as myocardial infarc-tion, stroke, or renal dysfunction (Table 3).20 The low incidence of these adverse events and lack of evidence showing a positive correlation or association with TXA administration compared with placebo suggest its safety for use in the perioperative period.
In addition to undesirable procoagulant effects, a potential adverse effect of TXA is retinal change. In an animal model, doses approximately 7 times greater than the maximum dose for humans were associated with retinal changes.21 For diagnosis of TXA toxicity using an ophthalmic examination, it would require a patient to have functioning color vision before surgery. Therefore, patients with acquired defective color vision (color blind-ness) should not receive TXA. Despite no human testing having been done, it is still recommended to screen pa-tients for acquired defective color vision.12
Although TXA has a low incidence of side effects, its safety has recently been challenged. The large retrospec-tive study of Sharma et al22 associated a cumulative high
Figure 2. Schematic Diagram of Molecular Interactions During Fibrinolysisa aFibrinolytic system consists of plasminogen, which is converted into plasmin by tissue plasminogen activator. Once plasmin is activated, it binds to fibrin via the lysine-binding sites (represented as legs of the animal). Free circulating plasmin glycoproteins become inactivated by α2-antiplasmin. (From Collen and Lijnen.11 Reprinted with permission from Lippincott Williams & Wilkins.)

204 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
dose of TXA (80 mg/kg) with an increased incidence of postoperative seizures in cardiac surgical patients. Controversy remains regarding this association because of the selection bias that confounds retrospective studies. Researchers theorize that seizures due to TXA may be secondary to neuronal γ-aminobutyric acid (GABA) inhi-bition or the crossing of TXA into cerebrospinal fluid.23
There are only a few reported studies on the pharma-cokinetics of intravenous TXA; therefore, determining the minimum effective dose that inhibits fibrinolytic activity has been challenging. Furthermore, those studies have investigated TXA plasma concentrations in healthy volunteers, and have not proven relevancy in more hemo-dynamically fragile older patient populations.24 Dosing schedules thus far have been empirical and hypothesized, and dosages cited in studies may vary over a 10-fold
range (loading dose, 10-150 mg/kg).20 The discrepancy of dosing and efficacy among studies has created confu-sion about the optimal duration of TXA treatment and techniques to maintain therapeutic TXA concentrations.20 Comparatively, there is a higher ratio of cardiac studies concerning the dosing of TXA vs TXA dosing in ortho-pedic or trauma surgeries. Without definitive guidelines, anesthesia providers must proceed with caution when choosing a dosing regimen for their patient. A summary of dosing strategies for specific procedures can be seen in Table 1.
Use in Cardiac SurgeryClose to 1.25 million adults worldwide undergo cardiac surgery each year.25 Surgical blood loss and the need for blood transfusions pose serious complications for many
Procedure (unlabeled use) Dosing regimena Reference
Elective cesarean delivery 10 min before incision: 1 g over 5 min Gungorduk, 201314
Vaginal delivery At delivery of anterior aspect of shoulder: 1g over 5 min Gungorduk, 201314
Hip fracture surgery 15 mg/kg; repeat dose 3 h later Zufferey, 201015
Cardiac surgery 30 mg/kg over 30 min, followed by 16 mg/kg/h until sternal closure; add 2 mg/kg to CPB circuit
Fergusson, 200816
Cardiac surgery 10 mg/kg over 20 min, followed by 2 mg/kg/h continued for 2 h after transfer to ICU; add 50 mg for a 2.5-L CPB circuit
Nuttall, 200813
Spinal surgery 10 mg/kg, followed by 1 mg/kg/h until wound closure Wong, 200817
Total hip arthroplasty 15 min before skin incision: 10-15 mg/kg (or 1 g) over 5-10 min; followed by either of the following: 1. 10 mg/kg (or 1 g), 3 h after surgery 2. 1 mg/kg/h for 10 h
Oremus, 201418
Total knee arthroplasty First dose (10 mg/kg) immediately before tourniquet was deflated; repeat dose 3 h later
Camarasa, 200619
Trauma 1 g over 10 min, followed by 1g over 8 h; begin treatment within 8 h of injury CRASH-2 Trial Collaborators, 20102
Renal dosing, cardiac surgery
Same loading dose. Reduce maintenance infusion based on serum creatinine level as follows:
Nuttall, 200813
1.6-3.3 mg/dL 1.5 mg/kg/h (25% reduction)
3.3-6.6 mg/dL 1 mg/kg/h (50% reduction)
> 6.6 mg/dL 0.5 mg/kg/h (75% reduction)
Table 1. Recommended Dosing Strategies for Tranexamic AcidAbbreviations: CPB, cardiopulmonary bypass; ICU, intensive care unit.aTranexamic acid should be administered intravenously immediately before skin incision unless specified otherwise. Tranexamic acid may be mixed with any crystalloid solution, and loading doses of varying amounts diluted in 50 to 250 mL administered over 5 to 30 minutes. With rapid administration, one may see orthostatic reaction; therefore, the recommended maximum rate of injection should be 100 mg/min.
Table 2. Contraindications to Tranexamic Acid12
Abbreviation: TXA, tranexamic acid.(From Pharmacia and Upjohn Co. Cyklokapron—tranexamic acid injectable, solution. May 2013.)
Absolute contraindication Relative contraindication
Acquired defective color vision History of vascular occlusive events
Hypersensitivity to TXA Concomitantly with another procoagulant
Active intravascular clotting Concomitantly with hormonal contraception
Subarachnoid hemorrhage

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 205
cardiac surgical patients and have shown a strong asso-ciation with in-hospital mortality.26 These risks have led to the use of antifibrinolytics such as TXA in the cardiac surgical patient to minimize blood loss. Although its use in cardiac surgery remains off-label, TXA shows promise in decreasing complications associated with blood loss.
Over the last 20 years, several meta-analyses have as-sessed the efficacy and safety of TXA using endpoints such as blood loss, frequency of blood transfusions, occurrence of adverse events, in-hospital mortality rate, and reopera-tion due to rebleeding. Unfortunately, the measurement of these endpoints has differed substantially among studies, making it difficult for researchers to decipher statistically significant results. To make analysis even harder, some studies have grouped the lysine analogs TXA and EACA together when comparing them with aprotinin, instead of assessing each independently. Overall, meta-analyses of randomized clinical trials agree that TXA is effective at reducing the need for blood transfusions when compared with no antifibrinolytic treatment.27-29
Currently, there is no consensus regarding optimal TXA dosing in cardiac surgery. In 2008, the WHO rec-ommended a TXA dose of 10 to 30 mg/kg intravenously followed by an infusion of 1 to 16 mg/kg/h and 1 to 2 mg/kg added to the cardiopulmonary circuit (pump prime).25 Some researchers have implied that CPB may influence TXA’s elimination kinetics and subsequently blood concentrations of TXA, but no specific research has been conducted regarding CPB kinetics of TXA. Butterworth et al23 did find CPB-related elimination effects with EACA, so it is common practice to supple-ment the circuit with additional TXA because EACA and TXA have similar kinetic properties.
Indications for use of TXA vary among professional guidelines. For example, in 2006 the American Society of Anesthesiologists published guidelines concerning an-tifibrinolytic therapy, stating that antifibrinolytics should
not be administered routinely and use should be deter-mined on an individual basis.30 However, the Society of Thoracic Surgeons and the Society of Cardiovascular Anesthesiologists published their joint guidelines in 2007, which recommended the use of TXA for blood con-servation in cardiac surgery since TXA limits total blood loss and reduces the number of patients who require blood transfusion after cardiac procedures.31
In a 2011 Cochrane Review, when TXA was compared with no treatment in cardiac surgical patients, there was no significant difference in mortality rate. The authors also determined that there is no conclusive evidence of increased risk of thrombosis associated with TXA. This review looked at 34 studies published on the use of TXA in 3,006 cardiac surgical patients. The TXA loading or bolus dose ranged from 2.5 to 100 mg/kg, and the maintenance dose of TXA ranged from 0.25 to 4.0 mg/kg/h delivered over 1 to 12 hours. Comparison of the literature was difficult because data collected vary among studies, including the volume of blood transfused and the amount of blood loss, whether it be intraoperative, postoperative, or recorded as combined. Other variables making comparison challenging are hospitals’ variation in transfusion protocols and providers’ blood transfusion thresholds; perioperative aspirin use, autotransfusion procedures, and types of CPB technology and practice. In the context of cardiac surgery, postoperative bleeding was shown, on average, to be reduced 273 mL across 22 of the trials. Tranexamic acid did not significantly reduce the risk of reoperation for bleeding, exposure to blood transfusions; nor did it reduce length of hospital stay. The authors concluded that the decrease in postoperative bleeding and limited side effects of TXA offset possible fear or belief that TXA may increase the risk of vascu-lar occlusion events. The findings from the Cochrane Review confirmed and strengthened previous research on the use of TXA in cardiac surgery.
Use in Orthopedic SurgeryOrthopedic surgery can be associated with substantial intraoperative and postoperative blood loss and may require blood transfusion to replace blood loss. Although the pneumatic tourniquet is one strategy commonly used to address blood loss intraoperatively, recent meta-analyses have found that the use of a tourniquet does not decrease total blood loss or the transfusion rate in the perioperative period, and there are several adverse com-plications associated with its use, including increased risk of thromboembolic events.32,33
However, TXA does effectively reduce postoperative blood loss. A Cochrane Review20 compares TXA with placebo in orthopedic surgery, including total knee and total hip arthroplasties. It finds that the use of TXA in orthopedic surgery reduced intraoperative blood loss by 116 mL per patient, and postoperative blood loss by 229
Table 3. Adverse Events Associated With Tranexamic Acid Administrationa During the Perioperative Period20
Abbreviations: CI, confidence interval; RR, risk ratio.aData were extrapolated from 65 trials (4,482 patients) that compared tranexamic acid (TXA) with a control in a variety of surgical procedures. Results showed no difference in the rate of events between TXA and placebo.
Effect of tranexamic acid
Adverse event RR 95% CI
Death 0.60 0.33 to 1.10
Myocardial infarction 0.79 0.41 to 1.52
Stroke 1.23 0.49 to 3.07
Deep venous thrombosis 0.71 0.35 to 1.43
Renal failure 0.89 0.33 to 2.37
Pulmonary embolism 0.67 0.23 to 1.99

206 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
mL per patient. Overall, the review concludes that the use of TXA in orthopedic surgery significantly reduces the total amount of blood lost during the perioperative period. This conclusion is based on the results of 20 trials that compared TXA with placebo in orthopedic surgery, including 1,201 patients, of which 605 received TXA and 596 received a placebo.
Many meta-analyses and studies have been conducted attempting to discern the best practice for administer-ing TXA in orthopedic surgery; however, the best drug dosage, dosing regimen, or method of delivery of TXA for total knee or total hip arthroplasty has yet to be definitively determined. Studies either choose to give an upfront bolus of medication before inflation of tourniquet or skin incision, with no medication to follow, another bolus to follow, or a continuous infusion to follow. In a subgroup analysis of the meta-analysis by Huang et al,34 it was determined that regardless of the dosing scheme or amount delivered, there continued to be a positive effect and reduction of blood loss from TXA administration. A systematic review of the literature by Alshryda et al35 concluded that not only did TXA reduce blood loss, but it also reduced blood transfusion requirements during total knee arthroplasties. A meta-analysis evaluating the use of TXA for total hip arthroplasty also determined that TXA reduces intraoperative blood loss by a mean of 104 mL and reduces allogeneic blood transfusions.36 These meta-analyses support continued investigation and improved heterogeneity in further studies to obtain clear data on proper TXA administration.
A major concern with the use of TXA in orthopedic procedures is the risk of thrombosis. Administration of TXA has been slow to become popular in orthopedic populations because of this perceived risk. In their sys-tematic review of the literature , Huang et al34 observed no increase in thromboembolic events in patients who received TXA compared with placebo. Other meta-anal-yses, performed by Alshryda et al35 and Sukeik et al,36
confirmed that there was no increased risk of adverse events or complications among study groups when TXA was used for total knee or total hip arthroplasty.
Although there remains controversy over optimal timing, dosage and method of administration of TXA in orthopedic surgery, there is overwhelming evidence to suggest that providing TXA in these procedures reduces blood loss in total knee and total hip arthroplasty. A survey of the literature reveals that TXA does not in-crease likelihood of adverse effects, such as deep-vein thrombosis or pulmonary embolism as previously be-lieved. Continued research is necessary to fully deter-mine best practice for TXA administration in orthopedic procedures.
Use in NeurosurgeryIn spine surgery, higher blood loss occurs because of sur-
gical techniques using spinal instrumentation since bony surfaces are not conducive to traditional hemostatic ma-neuvers used during soft-tissue surgery.17 Other potential causes of blood loss during spinal surgery include surgery duration and the number of vertebral levels decom-pressed.17 Formation of an epidural hematoma in close proximity to the spinal canal can lead to severe neurologic damage due to spinal cord or cauda equina compression.37
A meta-analysis38 published in 2013 suggests TXA significantly decreases blood loss and frequency of blood transfusion, without increasing the risk of deep-vein thrombosis in spine surgery. However, a limitation of the publication is the small number of studies that were included in the meta-analysis. In 2008, Wong et al17 as-sessed the efficacy of TXA in adults undergoing elective spinal reconstructive surgery and found that calculated perioperative blood loss was significantly less in the TXA group vs the placebo group.17 The incidence of transfu-sion of blood products or the hospital length of stay did not differ significantly between the 2 groups.17
Topical use of TXA in lumbar spine fixation surgery has the potential to reduce postoperative blood loss. Krohn et al39 compared 30 patients who received either TXA in irrigation solution during wound closure (n = 16) or saline irrigation solution alone (n = 14). The TXA group had significantly reduced postoperative blood loss compared with the placebo group.39
Substantial perioperative blood loss is associated with surgical correction of scoliosis in the pediatric population and often requires administration of blood products.40 Sethna et al40 studied efficacy of TXA in children and adolescents undergoing elective spinal fusion, evaluat-ing whether TXA administration would decrease blood loss or transfusion requirements. The TXA group had a statistically significant reduction in blood loss, by 41%, compared with the placebo.40
Further research comparing dosing regimens, (eg, single bolus vs bolus and continuous infusion) is im-portant to determine a safe and effective treatment for patients undergoing neurosurgery. At this time, there is a discrepancy between study dosing strategies, as well as insufficient numbers of studied patients to be able to de-termine best practice. Although current evidence strong-ly suggests TXA reduces blood loss in neurosurgery, additional research is necessary to establish best practice.
Use in Trauma SurgeryTrauma is the sixth leading cause of death worldwide, with hemorrhaging as the secondary cause.41 Trauma patients experience many coagulopathies, including hy-perfibrinolysis leading to hemorrhage, and it is believed that trauma and surgery have similar hemostatic responses after severe vascular injury. Tranexamic acid may oppose hyperfibrinolysis and reduce mortality due to bleeding in trauma patients.42 Recently, TXA has been incorporated

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 207
into several resuscitation and massive transfusion proto-cols across the United States.
The Clinical Randomization of an Antifibrinolytic in Significant Haemorrhage-2 (CRASH-2) study was the first to assess the effects of TXA administration in trauma patients with or at risk of major hemorrhaging. This study specifically looked at the influence of TXA on death rate, vascular occlusive events, and frequency of blood transfusions in more than10,000 patients random-ly assigned to receive TXA. Both all-cause mortality and risk of death due to bleeding were significantly reduced with TXA administration. Vascular occlusive events and blood product administration did not vary significantly between placebo and TXA groups. The absence of an increased risk of thrombotic events with TXA adminis-tration reemphasizes its safety profile. The power of the study may be reduced because diagnosis of traumatic hemorrhage is difficult and the study included patients in the trial who may not have been actually hemorrhaging.2 As of now, no other studies have been published compar-ing TXA with placebo in trauma patients.
Early administration of TXA is crucial to decrease blood loss. Therefore, the CRASH-2 study dosed TXA as a bolus of 1 g over 10 minutes and then an infusion of 1 g over 8 hours. The study investigators also believed that stopping TXA administration within 8 hours would decrease the risk of death due to thrombotic events and coagulopathies associated with trauma in the later hours after injury. In the event of an emergency, it may be dif-ficult to determine a patient’s weight, so fixed dosing was the best solution.2
Use in Obstetric and Gynecologic ProceduresThe use of TXA in obstetric-gynecologic procedures is controversial; however, multiple studies are under in-vestigation to determine the safety and efficacy of TXA in the obstetric population. In 2013, global accounts of maternal mortality included 289,000 women who died from complications during pregnancy or childbirth, 99% of which occurred in developing countries.43 Because severe bleeding accounts for 27% of all maternal deaths worldwide,43 the use of TXA could prove beneficial in reducing blood loss and saving lives.
Tranexamic acid crosses the placenta, producing cord blood concentrations similar to maternal plasma concentrations.44 The FDA has categorized TXA as a Category B drug, because there have been no adequate, well-controlled studies in pregnant women; however, the administration of TXA in animal reproduction studies have failed to demonstrate risk to the fetus.12 Tranexamic acid is present in mothers’ breast milk at low concentrations, approximately 1% of the maternal serum concentration.44
The WHO recommends the use of TXA for postpar-tum hemorrhage in the event that the administration
of oxytocin and second-line treatment options are in-effective, or if the bleeding is also due to trauma.45 A Cochrane Review published in 2010, concludes, from the results of 2 randomized control trials, that there was decreased postpartum blood loss after vaginal and cesar-ean births when TXA was used.46 However, the reviewers recommend that further investigations are necessary to illustrate the safety and efficacy of TXA in preventing postpartum hemorrhage.46
The use of TXA has been studied for populations undergoing elective cesarean delivery or vaginal de-livery.14,47 Each study demonstrated decreased mean estimated blood loss in the TXA group compared with the placebo group. There was no significant difference between the 2 study groups for requiring blood trans-fusion or hospital length of stay for those undergoing cesarean delivery or having vaginal delivery. However, significantly more women in the placebo group required additional uterotonic agents and had lower hemoglobin and hematocrit levels the day after delivery in the study assessing use of TXA for vaginal delivery.14
A large, international, randomized, double-blind study, World Maternal Antifibrinolytic Trial (WOMAN), is currently under way to determine the efficacy of TXA compared with a placebo in 15,000 women with postpar-tum hemorrhage.48 It aims to determine the effect of early administration of TXA following vaginal or cesarean delivery assessing mortality, hysterectomy, surgical inter-vention, and blood transfusion.48 Studies to date have not been powered sufficiently to demonstrate risk of adverse vascular events related to TXA administration, but the WOMAN Trial will have sufficient power to determine the risk of TXA.48 Recruitment is ongoing, with hospitals from Africa, Asia, Latin America, and Europe currently collaborating.
ConclusionCurrently, TXA is being used in a wide range of surgical procedures without increased risk of thrombosis or other adverse effects.20 The results of several large clinical trials and many small trials support its use to decrease bleeding and reduce mortality and have a proven safe pharmaceutical profile.20 It is yet to be determined if the increased use of antifibrinolytic agents actually reduces the rate of blood transfusions, but TXA has been shown to reduce the degree of blood loss perioperatively. This inexpensive and safe drug is increasingly being used since aprotinin went off the market and because it is more potent than EACA. Further research is needed to differentiate possible alternate mechanisms of action of TXA, procedure-specific dosing regimens, and even use of TXA in traumatic brain injuries, including hemor-rhage. In addition, future research should involve larger trials that definitively prove the effectiveness of TXA because existing smaller trials may be biased.

208 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
REFERENCES 1. Napolitano LM, Cohen MJ, Cotton BA, Schreiber MA, Moore EE.
Tranexamic acid in trauma: how should we use it? J Trauma Acute Care Surg. 2013;74(6):1575-1586.
2. CRASH-2 Trial Collaborators, Shakur H, Roberts I, Bautista R, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet. 2010;376 (9734):23-32.
3. Roberts I, Kawahara T, 18th Expert Committee on the Selection and Use of Essential Medicines, World Health Organization. Proposal for the inclusion of tranexamic acid (anti-fibrinolytic–lysine analogue) in the WHO model list of essential medicines. http://www.who.int/selec-tion_medicines/committees/expert/18/applications/TRANEXAMIC_ACID_10_2.pdf?ua=1. Published June 2010. Updated link accessed March 23, 2016.
4. Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008; 36(9):2667-2674.
5. Leahy MF, Mukhtar SA. From blood transfusion to patient blood management: a new paradigm for patient care and cost assessment of blood transfusion practice. J Intern Med. 2012;42(3):332-338.
6. Toner RW, Pizzi L, Leas B, Ballas SK, Quigley A, Goldfarb NI. Costs to hospitals of acquiring and processing blood in the US: a survey of hospital-based blood banks and transfusion services. Appl Health Econ Health Policy. 2014;9(1):29-37.
7. Reed H. The role of tranexamic acid in EMS & preoperative trauma management. JEMS. March 27, 2013, issue 4. http://www.jems.com/articles/print/volume-38/issue-4/patient-care/role-tranexamic-acid-ems-preoperative-tr.html. Accessed March 28, 2016.
8. Guyton AC, Hall JE. Hemostasis and blood coagulation. In: Textbook of Medical Physiology. 12th ed. Philadelphia, PA: Saunders Elsevier; 2011:451-461.
9. Cesarman-Maus G, Hajjar KA. Molecular mechanisms of fibrinolysis. Br J Haematol. 2005;129(3):307-321.
10. Moake JL. Overview of hemostasis [online]. Merck Manual Online. http://www.merckmanuals.com/professional/hematology_and_oncol-ogy/hemostasis/overview_of_hemostasis.html. Accessed September 14, 2014.
11. Collen D, Lijnen HR. Basic and clinical aspects of fibrinolysis and thrombolysis. Blood. 1991;78(12):3114-3124.
12. Cyklokapron-tranexamic acid injectable, solution [package insert]. Kalamazoo, MI: Pharmacia & Upjohn Co; May 2013.
13. Nuttall GA, Gutierrez MC, Dewey JD, et al. A preliminary study of a new tranexamic acid dosing schedule for cardiac surgery. J Cardiothorac Vasc Anesth. 2008;22(2):230-235.
14. Gungorduk K, Asiciog lu O, Yildirim G, Ark C, Tekirdag AI, Besi-moglu B. Can intravenous injection of tranexamic acid be used in routine practice with active management of the third stage of labor in vaginal delivery? A randomized controlled study. Am J Perinatol. 2013;30(5):407-413.
15. Zufferey PJ, Miquet M, Quenet S, et al, for the investigators of the tranexamic acid in hip-fracture surgery (THIF) study. Tranexamic acid in hip fracture surgery: a randomized controlled trial. Br J Anaesth. 2010;104(1):23-30.
16. Fergusson DA, Hébert PC, Mazer CD, et al, BART Investigators. A com-parison of aprotinin and lysine analogues in high-risk cardiac surgery [published correction appears in N Engl J Med. 2010;363(13):1290]. N Engl J Med. 2008;358(22):2319-2331.
17. Wong J, El Beheiry H, Rampersaud YR, et al. Tranexamic acid reduces perioperative blood loss in adult patients having spinal fusion surgery. Anesth Analg. 2008;107(5):1479-1486.
18. Oremus K, Sostaric S, Trkulja V, Haspl M. Influence of tranexamic acid on postoperative autologous blood retransfusion in primary total hip and knee arthroplasty: a randomized controlled trial. Transfusion. 2014;54(1):31-41.
19. Camarasa MA, Ollé G, Serra-Prat M, et al. Efficacy of aminocaproic,
tranexamic acids in the control of bleeding during total knee replace-ment: a randomized clinical trial. Br J Anaesth. 2006;96(5):576-582.
20. Henry DA, Carless PA, Moxey AJ, et al. Anti-fibrinolytic use for mini-mising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev. 2011(3): CD001886 .
21. Ekvarn S. Summary and evaluation of toxicological data. Stockholm, Sweden: Data on file, KabiVitrum AB; 1983.
22. Sharma V, Fan J, Jerath A, et al. Pharmacokinetics of tranexamic acid in patients undergoing cardiac surgery with use of cardiopulmonary bypass. Anaesthesia. 2012;67(11):1242-1250.
23. Dowd NP, Karski JM, Cheng DC, et al. Pharmacokinetics of tranexamic acid during cardiopulmonary bypass. Anesthesiology. 2002;97(2):390-399.
24. Benoni G, Bjorkman S, Fredin H. Application of pharmacokinetic data from healthy volunteers for the predication of plasma con-centrations of tranexamic acid in surgical patients. Clin Drug Invest. 1995;10(5):280-287.
25. Carless P, 17th Expert Committee on the Selection and Use of Essential Medicines, World Health Organization. Proposal for the inclusion of tranexamic acid (anti-fibrinolytic -lysine analogue) in the WHO Model List of Essential Medicines [draft report]. http://www.who.int/selection_medicines/committees/expert/17/application/TRANEXAMIC_ACID.pdf. Published November 25, 2008. Accessed September 12, 2014.
26. Karkouti K, Wijeysundera DN, Yau TM, et al. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion. 2004;44(10):1453-1462.
27. Laupacis A, Fergusson D. Drugs to minimize perioperative blood loss in cardiac surgery: meta-analyses using perioperative blood transfu-sion as the outcome. The International Study of Peri-operative Trans-fusion (ISPOT) Investigators. Anesth Analg. 1997;85(6):1258-1267.
28. Fremes SE, Wong BI, Lee E, et al. Metaanalysis of prophylactic drug treatment in the prevention of postoperative bleeding. Ann Cardiotho-rac Surg. 1994;58(6):1580-1588.
29. Henry D, Carless P, Fergusson D, Laupacis A. The safety of aprotinin and lysine-derived antifibrinolytic drugs in cardiac surgery: a meta-analysis. CMAJ. 2009;180(2):183-193.
30. American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Practice guidelines for perioperative blood transfusion and adjuvant therapies: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Blood Transfusion and Adjuvant Therapies. Anesthesiol-ogy. 2006;105(1):198-208.
31. Society of Thoracic Surgeons Blood Conservation Guideline Task Force and Society of Cardiovascular Anesthesiologists Special Task Force on Blood Transfusion. Perioperative blood transfusion and blood conservation in cardiac surgery: the Society of Thoracic Sur-geons and The Society of Cardiovascular Anesthesiologists clinical practice guideline. Ann Thorac Surg. 2007;83(5 suppl):S27-S86.
32. Smith TO, Hing CB. Is a tourniquet beneficial in total knee replacement surgery? A meta-analysis and systematic review. Knee. 2010;17(2):141-147.
33. Zhang W, Li N, Chen S, Tan Y, Al-Aidaros M, Chen L. The effects of a tourniquet used in total knee arthroplasty: a meta-analysis. J Orthop Surg Res. 2014;9(1):13.
34. Huang F, Wu D, Ma G, Yin Z, Wang Q. The use of tranexamic acid to reduce blood loss and transfusion in major orthopedic surgery: a meta-analysis. J Surg Res. 2014;186(1):318-327.
35. Alshryda S, Sarda P, Sukeik M, Nargol A, Blenkinsopp J, Mason JM. Tranexamic acid in total knee replacement: a systematic review and meta-analysis. J Bone Joint Surg Br. 2011;93(12):1577-1585.
36. Sukeik M, Alshryda S, Haddad FS, Mason JM. Systematic review and meta-analysis of the use of tranexamic acid in total hip replacement. J Bone Joint Surg Br. 2011;93(1):39-46.
37. Tsutsumimoto T, Shimogata M, Ohta H, Yui M, Yoda I, Misawa H. Tranexamic acid reduces perioperative blood loss in cervical lamino-plasty. Spine. 2011;36(23):1913-1918.
38. Yuan C, Zhang H, He S. Efficacy and safety of using antifibrinolytic

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 209
agents in spine surgery: a meta-analysis. PLoS One. 2013;8(11): e82063.
39. Krohn CD, Sørensen R, Lange JE, Riise R, Bjørnsen S, Brosstad F. Tranexamic acid given into the wound reduces postoperative blood loss by half in major orthopaedic surgery. Eur J Surg Suppl. 2003;588:57-61.
40. Sethna NF, Zurakowski D, Brustowicz RM, Bacsik J, Sullivan LJ, Shapiro F. Tranexamic acid reduces intraoperative blood loss in pediatric patients undergoing scoliosis surgery. Anesthesiology. 2005;102(4):727-732.
41. Søreide K. Epidemiology of major trauma. Br J Surg. 2009;96(7): 697-698.
42. Lawson JH, Murphy MP. Challenges for providing effective hemosta-sis in surgery and trauma. Semin Hematol. 2004;41(1 suppl 1):55-64.
43. WHO, UNICEF, UNFPA, The World Bank, United Nations Popula-tion Division. Trends in maternal mortality: 1990-2013. Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division [online]. http://www.who.int/reproductivehe-alth/publications/monitoring/maternal-mortality-2013/en/. Published May 2014. Accessed September 4, 2014.
44. McCormack PL. Tranexamic acid: a review of its use in the treatment of hyperfibrinolysis. Drugs. 2012;72(5):585-617.
45. WHO Guidelines for the Management of Postpartum Haemorrhage and Retained Placenta. Geneva, Switzerland: World Health Organization; 2009. http://apps.who.int/iris/bitstream/10665/44171/1/9789241598514_eng.pdf. Accessed March 28, 2016.
46. Novikova N, Hofmeyr GJ. Tranexamic acid for preventing postpar-tum haemorrhage. Cochrane Database Syst Rev. 2010;(7): CD007872.
47. Gungorduk K, Yildirim G, Asiciog lu O, Gungorduk O, Sudolmus S, Ark C. Efficacy of intravenous tranexamic acid in reducing blood loss after elective cesarean section: a prospective, randomized, double-blind, placebo-controlled study. Am J Perinatol. 2011;28(3):233-239.
48. Shakur H, Elbourne D, Gülmezoglu M, et al. The WOMAN Trial (World Maternal Antifibrinolytic Trial): tranexamic acid for the treatment of postpartum haemorrhage: an international randomized, double blind placebo controlled trial. Trials. 2010;11:40-53.
AUTHORSJessica Mayeux, MSN, CRNA, is employed by Mission Health System, Asheville, North Carolina. At the time this article was written she was a student at Western Carolina University, Asheville, North Carolina.
Kathy Alwon, MSN, CRNA, is employed by Harborview Medical Center, Seattle, Washington. At the time this article was written she was a student at Western Carolina University, Asheville, North Carolina.
Shawn Collins, PhD, DNP, CRNA, is the director of the Nurse Anes-thesia Program at Western Carolina University, Asheville, North Carolina. Email: [email protected].
Ian Hewer, MSN, MA, CRNA, is the assistant director of the Nurse Anes-thesia Program at Western Carolina University, Asheville, North Carolina.
DISCLOSURESThe authors have declared they have no financial relationships with any commercial interest related to the content of this activity. The authors did discuss off-label use within the article.

210 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
June 1, 2016-December 31, 2017, Texas; Dannemiller, Inc. - Provider-Directed Independent Study - 36 CEC. “AnesthesiaFile: Notebook Vol. 33.” Barbra Thompson, 5711 Northwest Parkway, San Antonio, TX 78249; (210) 641-8311; fax (210) 641-8329; email, [email protected]; www.dannemiller.com.
June 1, 2016-December 31, 2017, Texas; Dannemiller, Inc. - Provider-Directed Independent Study - 36 CEC. “Anesthesiology Online Vol. 16.” Barbra Thompson, 5711 Northwest Parkway, San Antonio, TX 78249; (210) 641-8311; fax (210) 641-8329; email, [email protected]; www.dannemiller.com.
June 1, 2016-December 31, 2017, Texas; Dannemiller, Inc. - Provider-Directed Independent Study - 24 CEC. “Painstracts Volume 16.” Barbra Thompson, 5711 Northwest Parkway, San Antonio, TX 78249; (210) 641-8311; fax (210) 641-8329; email, [email protected]; www.dannemiller.com.
June 1, 2016-May 31, 2018, Florida; Frank Moya Continuing Education Programs - Provider-Directed Independent Study - 26 CEC. “Current Reviews for Nurse Anesthetists, Volume 39.” Frank Moya, MD, 1828 SE First Avenue, Ft. Lauderdale, FL 33316; (954) 763-8003; fax (800) 425-1995; email, [email protected]; www.currentreviews.com.
June 1, 2016-December 31, 2018, Michigan; Institute For Post Graduate Education - 40 CEC. “CE Anywhere - Self Directed Independent Study.” Bernard Kuzava, CRNA, PO Box 28, Hastings, MI 49058; (877) 692-0430; fax (269) 948-2507; email, [email protected]; www.ipge.com.
June 1, 2016-April 10, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-New Technological Modalities in Anesthesia.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-April 12, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-Inhalational Anesthetics.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-April 17, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-Everything You Wanted to Know About Hormones But Were Afraid to Ask.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-April 19, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-Ultrasound Physics.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-April 24, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-The Wondrous Story of Anesthesia: Where Nurses Led and Where They Followed.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-May 1, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-Parenteral Anesthetics.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-May 3, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-The History of Supervision.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-May 8, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn- Potential Pee: A Journey Through the Nephron.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-May 10, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-Neonatal Anesthesia.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-May 15, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-Ultrasound Scanning Basics.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 1, 2016-May 15, 2019, Illinois; American Association of Nurse Anesthetists - 2 CEC. “CPC Module 1 - Airway Management Techniques.” (847) 939-3530; email, [email protected]; www.AANALearn.com.
CALENDAR OF EVENTSAdvertisers who list their prior-approved CE programs in the Calendar of Events enjoy wider exposure for their approved pro-grams because the $125 per listing fee includes a duplicate listing on the AANA website as well as a link directly to the online Calendar of Events in the bi-monthly Anesthesia E-ssential (the AANA’s electronic newsletter). Additionally, the web address provided in the advertisement will be hyperlinked directly to the
websites allowing viewers access to company and program infor-mation for more exposure and target-directed traffic.
Go to http://www.aana.com/cecalendarofevents for specific deadline dates. The fee can be paid along with the CE Application submission.
For additional information, contact Ann Carlson, Continuing Education Department, at (847) 655-1190.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 211
June 1, 2016-May 17, 2019, Illinois; American Association of Nurse Anesthetists - 1 CEC. “AANA Learn-Jan Stewart Lecture: Empowering Calm Through Engaged Resilience.” American Association of Nurse Anesthetists, Park Ridge, IL. (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 13, 2016-June 12, 2018, Illinois; American Association of Nurse Anesthetists - 2.5 CEC. “CPC Module 2 - Applied Clinical Pharmacology.” (847) 939-3530; email, [email protected]; www.AANALearn.com.
June 24-25, 2016, Illinois; American Association of Nurse Anesthetists - 15.75 CEC. “Business of Anesthesia Conference.” Sofitel Chicago Water Tower, Chicago, IL. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
June 24-26, 2016, Alabama; Lower Alabama Continuing Education Seminars, Inc. - 20 CEC. “2016 LACES Summer Seminar.” Perdido Beach Resort, Orange Beach, AL. Laura Lesley, MS, 5571 Carrington Lake Pkwy, Trussville, AL 35173; (205) 937-4139; email, [email protected]; www.Lacesinc.com.
July 11-14, 2016, Massachusetts; Northwest Seminars - 20 CEC. “Topics in Emergency Medicine: Emphasis on Pediatrics.” Sea Crest Beach Hotel, North Falmouth (Cape Cod), MA. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; email, [email protected]; www.northwestseminars.com.
July 11-15, 2016, Hawaii; Northwest Seminars - 20 CEC. “Current Topics in Emergency Medicine.” The Royal Hawaiian, Honolulu, HI. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.northwestseminars.com.
July 11-15, 2016, Montana; Northwest Anesthesia Seminars - 20 CEC. “Current Anesthesia Practice.” The Lodge at Whitefish Lake, Glacier National Park, Whitefish, MT. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
July 11-16, 2016, British Columbia, Canada; Northwest Seminars - 20 CEC. “Topics in Emergency Medicine.” Holland America - ms Noordam, Vancouver, British Columbia, Canada. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; email, [email protected]; www.northwestseminars.com.
July 11, 2016-July 10, 2019, Illinois; American Association of Nurse Anesthetists - 9 CEC. “CPC Module 3 - Human Physiology and Pathophysiology.” (847) 939-3530; email, [email protected]; www.AANALearn.com.
July 14-17, 2016, Missouri; Northwest Anesthesia Seminars - 20 CEC. “Current Topics in Anesthesia.” Hilton Branson Convention Center Hotel, Branson, MO. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
July 15-17, 2016, Connecticut; Core Concepts Anesthesia Review - 24 CEC. “Core Concepts Anesthesia Review/Refresher Course.” The Omni Hotel at Yale, New Haven, CT. Marianne S. Cosgrove, CRNA, DNAP, APRN, 64 Signal Hill Road, Madison, CT 06443; (203) 567-0272; email, [email protected]; www.ccanesthesiareview.com.
July 18-21, 2016, California; Northwest Seminars - 20 CEC. “Topics in Emergency Medicine.” Disney’s Grand Californian Hotel & Spa, Anaheim, CA. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; email, [email protected]; www.northwestseminars.com.
July 18-22, 2016, Oregon; Northwest Anesthesia Seminars - 20 CEC. “Current Topics in Anesthesia.” Sunriver Resort, Sunriver, OR. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
July 25-28, 2016, Florida; Northwest Anesthesia Seminars - 20 CEC. “Current Topics in Anesthesia.” Opal Sands Resort, Clearwater Beach, FL. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
July 25-30, 2016, Alaska; Northwest Anesthesia Seminars - 20 CEC. “Clinical Concerns in Anesthesia.” Celebrity Infinity Alaska Hubbard Glacier Cruise sailing from Vancouver, BC, Canada. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
July 29-31, 2016, Washington DC; EverWonk, Inc. - 20 CEC. “Topics in Anesthesia Practice.” Mayflower Hotel, Washington, DC. Kendall Pease, 3337 Crescent Oaks Blvd., Tarpon Springs, FL 34688; (619) 892-2467; email, [email protected]; www.everwonk.com.
August 1-4, 2016, Hawaii; Dannemiller - 24 CEC. “Hawaii Anesthesiology Update 2016.” Sheraton Kaui Resort, Poipu Beach, Koloa, HI. Barbra Thompson, 5711 Northwest Parkway, San Antonio, TX 78249; (210) 641-8311; fax (201) 641-8329; email, [email protected]; www.dannemiller.com.
August 1-5, 2016, Canada; Northwest Anesthesia Seminars - 20 CEC. “Clinical Topics in Anesthesia.” The Rimrock Resort Hotel, Banff, Alberta, Canada. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
August 7-18, 2016, Amsterdam; Northwest Anesthesia Seminars - 20 CEC. “Topics in Anesthesia.” 14 Day British Isles Cruise, aboard Celebrity Silhouette, sailing from Amsterdam, The Netherlands. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
August 9-12, 2016, California; Northwest Anesthesia Seminars - 24 CEC. “Relevant Topics in Anesthesia.” Hotel Solamar, San Diego, CA. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
August 15-18, 2016, North Carolina; Northwest Anesthesia Seminars - 20 CEC. “Topics in Anesthesia.” The Omni Grove Park Inn Resort, Asheville, NC. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
August 15, 2016-August 14, 2018, Illinois; American Association of Nurse Anesthetists - 3.5 CEC. “CPC Module 4 - Anesthesia Technology.” (847) 939-3530; email, [email protected]; www.AANALearn.com.
August 16-19, 2016, Pennsylvania; Northwest Anesthesia Seminars - 20 CEC. “Topics in Anesthesia.” The Hershey Lodge, Hershey, PA. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
August 21-26, 2016, Washington; Northwest Anesthesia Seminars - 20 CEC. “Clinical Concerns in Anesthesia.” 7-Night Alaska Explorer Cruise via Glacier Bay aboard ms Westerdam sailing from Seattle, WA. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.

212 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
August 21-27, 2016, Tennessee; Healthy Visions - American School of Clinical Hypnosis, International - 40 CEC. “Hypnosis Certification.” Healthy Visions, Clinton, TN. Ron Eslinger, CRNA, 351 Market Street, Clinton, TN 37716; (865) 269-4616 or toll free (866) 312-3159; email, [email protected]; www.hypnosiscertification.com.
August 22-26, 2016, Montana; Northwest Seminars - 20 CEC. “Current Topics in Emergency Medicine.” The Lodge at Whitefish Lake, Whitefish, MT. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.northwestseminars.com.
August 30, 2016, Florida; Gulfcoast Ultrasound Institute - 7.25 CEC. “Ultrasound-Guided Regional Anesthesia.” Gulfcoast Ultrasound Institute, St. Pete Beach, FL. Lori Green, 4615 Gulf Blvd Ste 205, St. Pete Beach, FL 33706; (727) 363-4500; email, [email protected]; www.gcus.com.
September 4, 2016, Nevada; Northwest Anesthesia Seminars - 8 CEC. “Business Concepts in Healthcare: A Practical Approach for Healthcare Providers.” The Cosmopolitan, Las Vegas, NV. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
September 5-8, 2016, Nevada; Northwest Anesthesia Seminars - 20 CEC. “Topics in Anesthesia.” The Cosmopolitan, Las Vegas, NV. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
September 9, 2016, Washington, DC; American Association of Nurse Anesthetists - 7 CEC. “Airway on Demand Workshop.” Washington Marriott Wardman Park, Washington, DC; (847) 655-8797; email, [email protected]; www.aana.com/meetings.
September 9, 2016, Washington, DC; American Association of Nurse Anesthetists - 6 CEC. “Fundamentals in Perioperative Transesophageal Echocardiogram Workshop.” Washington Marriott Wardman Park, Washington, DC; (847) 655-8797; email, [email protected]; www.aana.com/meetings.
September 9, 2016, Washington, DC; American Association of Nurse Anesthetists - 7 CEC. “Neuraxial Regional Anesthesia-Epidural Workshop.” Washington Marriott Wardman Park, Washington, DC; (847) 655-8797; email, [email protected]; www.aana.com/meetings.
September 10, 2016, Florida; Twin Oaks Anesthesia - 8 CEC. “Twin Oaks Anesthesia 2016 Cardiac Conference.” Renaissance Tampa International Plaza Hotel, Tampa, FL. Jonathan Kline, 26714 Winged Elm Drive, Wesley Chapel, FL 33544; (813) 857-5559; email, [email protected]; www.twinoaksanesthesia.com.
September 10-13, 2016, Washington, DC; American Association of Nurse Anesthetists - 25 CEC. “AANA Nurse Anesthesia Annual Congress.” Washington Marriott Wardman Park, Washington, DC; (847) 655-8797; email, [email protected]; www.aana.com/meetings.
September 12-16, 2016 California; Northwest Anesthesia Seminars - 20 CEC. “Clinical Anesthesia Update.” Tenaya Lodge, Fish Camp, CA. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
September 16-18, 2016, Alabama; Lower Alabama Continuing Education Seminars, Inc. - 20 CEC. “2016 LACES Fall Seminar.” Perdido Beach Resort, Orange Beach, AL. Laura Lesley, MS, 5571 Carrington Lake Pkwy, Trussville, AL 35173; (205) 937-4139; email, [email protected]; www.Lacesinc.com.
September 17-18, 2016, Virginia; Nurse Anesthesiology Faculty Associates - 15 CEC. “2016 Anesthesia Crisis Resource Management Course.” Virginia Commonwealth University, Richmond, VA. Michael Fallacaro, PO Box 980226, Richmond, VA 23298; (804) 828-6734; email, [email protected]; http://www.nafa-va.org/.
September 17-30, 2016, Greece; Spiekermann Travel - 20 CEC. “Current Issues in CRNA Practice.” Greece. Michael Rieker, DNP, CRNA, Nurse Anesthesia Program, Medical Center Boulevard, Winston-Salem, NC 27157; (800) 645-3233; fax (586) 775-9556; email, [email protected]; http://www.mideasttrvl.com/.
September 19-23, 2016, Wyoming; Northwest Anesthesia Seminars - 20 CEC. “Anesthesia Update: Emphasis on Trauma.” Hotel Terra, Teton Village, WY. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
September 19-29, 2016, Amersterdam; Northwest Anesthesia Seminars - 20 CEC. “Current Topics in Anesthesia.” 12-Night Iberian Adventure Cruise (Holland America/ms Koningsdam), Amsterdam, The Netherlands. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
September 22-25, 2016, South Carolina; Northwest Anesthesia Seminars - 20 CEC. “Relevant Topics in Anesthesia.” Westin Hilton Head Island Resort and Spa, Hilton Head Island, SC. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
September 24-25, 2016, Illinois; American Association of Nurse Anesthetists - 12 CEC. “Upper and Lower Extremity Nerve Block Workshop.” AANA Foundation Learning Center, Park Ridge, IL. 222 S. Prospect, Park Ridge, IL 60068; (847) 655-8797; email, [email protected]; www.aana.com/meetings.
September 26-29, 2016, Arizona; Northwest Seminars - 20 CEC. “Topics in Emergency Medicine.” Hilton Sedona Resort at Bell Rock, Sedona, AZ. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.northwestseminars.com.
September 26-29, 2016, California; Med City Anesthesia Seminars - 20 CEC. “A Taste of Anesthesia in Wine Country.” The Lodge at Sonoma Renaissance Resort & Spa, Sonoma, CA. Karissa Goodrich, CRNA, PO Box 711, St. Charles, MN 55972; (800) 558-0217; email, [email protected]; www.medcityanesthesiaseminars.com.
September 26-29, 2016, Rhode Island; Northwest Anesthesia Seminars - 20 CEC. “Current Topics in Anesthesia.” Hyatt Regency Newport Hotel & Spa, Newport, RI. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
September 30-October 2, 2016, Florida; EverWonk, Inc. - 20 CEC. “Topic in Anesthesia Practice.” Sanibel Harbour Resort & Spa, Fort Myers, FL. Kendall Pease, 3337 Crescent Oaks Blvd., Tarpon Springs, FL 34688; (619) 892-2467; email, [email protected]; www.everwonk.com.
September 30-October 2, 2016, Massachusetts; Airway Management Education Center - 18.5 CEC. “The Difficult Airway Course: Anesthesia.” Hyatt Regency Boston, Boston, MA. Registration Office, 333 South State Street, Suite V-324, Lake Oswego, OR 97034; (866) 924-7929; fax (404) 795-0711; email, [email protected]; www.theairwaysite.com.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 213
October 1-15, 2016, Israel and Jordan; Spiekermann Travel - 20 CEC. “Current Issues in CRNA Practice.” Israel and Jordan. Michael Rieker, DNP, CRNA, Nurse Anesthesia Program, Medical Center Boulevard, Winston-Salem, NC 27157; (800) 645-3233; fax (586) 775-9556; email, [email protected]; http://www.mideasttrvl.com/.
October 3-6, 2016, Bahamas; Northwest Anesthesia Seminars - 20 CEC. “Current Anesthesia Topics.” Atlantis Resort, Paradise Island, Bahamas. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
October 3-6, 2016, Florida; Northwest Anesthesia Seminars - 20 CEC. “Anesthesia Update.” Ritz Carlton Amelia Island, Fernandina Beach, FL. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
October 3-6, 2016, Maine; Encore Symposiums - 21 CEC. “Autumn in Bar Harbor & Acadia National Park 2016 Anesthesia Encore Symposiums.” The Harborside Hotel, Spa & Marina Resort, Bar Harbor, ME. Nancy LaBrie, RN, 1907 Loch Lomond Court, Winston-Salem, NC 27106; (336) 768-9095; fax (336) 768-9055; email, [email protected]; www.escrnas.com.
October 4-12, 2016, Spain; Northwest Anesthesia Seminars - 20 CEC. “Clinical Concerns in Anesthesia.” Celebrity Equinox, sailing from Barcelona, Spain. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
October 6-9, 2016, Tennessee; Northwest Anesthesia Seminars - 20 CEC. “Anesthesia Spectrum.” The Park Vista, a Doubletree Hotel, Gatlinburg, TN. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
October 7-9, 2016, New Mexico; Institute For Post Graduate Education - 15 CEC. “The Annual Balloon Fiesta Anesthesia Meeting.” Sheraton Albuquerque Uptown Hotel, Albuquerque, NM. Bernard Kuzava, CRNA, PO Box 28, Hastings, MI 49058; (877) 692-0430; fax (269) 948-2507; email, [email protected]; www.ipge.com.
October 7-9, 2016, Oregon; Oregon Association of Nurse Anesthetists - 17 CEC. “2016 ORANA Annual Conference.” Marriott Portland Downtown Waterfront, Portland, OR. Evelyn Bloomhart, PO Box 4444, Salem, OR 97302; (503) 874-1105; email, [email protected]; www.oregon-crna.org.
October 15-18, 2016, Florida; Valley Anesthesia - 20 CEC. “CE for the CRNA.” Naples Grande Beach Resort, Naples, FL. Scott Schaus, 2583 Alpine Dr., Woodbury, MN 55125; (651) 395-0777; fax (651) 846-5034, email, [email protected]; www.valleyanesthesia.com.
October 17-20, 2016, Rhode Island; Encore Symposiums - 21 CEC. “Newport Mansions Fall Foliage Experience 2016 Anesthesia Encore Symposiums.” Hotel Viking, Newport, RI. Nancy LaBrie, RN, 1907 Loch Lomond Court, Winston-Salem, NC 27106; (336) 768-9095; fax (336) 768-9055; email, [email protected]; www.escrnas.com.
October 17-21, 2016, Colorado; Northwest Anesthesia Seminars - 20 CEC. “Clinical Anesthesia Update.” Gateway Canyons Resort, Gateway, CO. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
October 21-23, 2016, Kansas; Core Concepts Anesthesia Review - 24 CEC. “Core Concepts Anesthesia Review/Refresher Course.” University of Kansas at KUMC, Kansas City, KS. Marianne S. Cosgrove, CRNA, DNAP, APRN, 64 Signal Hill Road, Madison, CT 06443; (203) 567-0272; email, [email protected], www.ccanesthesiareview.com.
October 29-30, 2016, Illinois; American Association of Nurse Anesthetists. “Jack Neary Advanced Pain Management Workshop Part II.” Orthopedic Learning Center, Rosemont, IL. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
October 30-November 4, 2016, Hawaii; Northwest Anesthesia Seminars - 20 CEC. “Anesthesia Topics.” Hyatt Regency Maui, Lahaina, HI. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
November 2, 2016, Illinois; American Association of Nurse Anesthetists - 8 CEC. “Essentials of Obstetric Analgesia/Anesthesia Workshop.” AANA Foundation Learning Center, Park Ridge, IL. 222 S. Prospect, Park Ridge, IL 60068; (847) 655-8797; email, [email protected]; www.aana.com/meetings.
November 3-5, 2016, Illinois; American Association of Nurse Anesthetists - 21 CEC. “Spinal and Epidural Workshop.” AANA Foundation Learning Center, Park Ridge, IL. 222 S. Prospect, Park Ridge, IL 60068; (847) 655-8797; email, [email protected]; www.aana.com/meetings.
November 3-6, 2016, Florida; Northwest Anesthesia Seminars - 20 CEC. “Keys in Anesthesia.” Westin Resort & Marina, Key West, FL. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
November 4-6, 2016, Nevada; Airway Management Education Center - 18.5 CEC. “The Difficult Airway Course: Anesthesia.” Bally’s Resort Las Vegas, Las Vegas, NV. Registration Office, 333 South State Street, Suite V-324, Lake Oswego, OR 97034; (866) 924-7929; fax (404) 795-0711; email, [email protected]; www.theairwaysite.com.
November 4-6, 2016, Tennessee; Focus Nurse Anesthesia Review - 15 CEC. “The Basics and Beyond Session 1: Focus in Music City.” Sheraton Nashville Downtown Hotel, Nashville, TN. Lindsay Studt, 5031 Timber Lake Trail, Clarkston, MI 48346; (248) 618-3481; email, [email protected]; www.focusnar.com.
November 5-6, 2016, Florida; Northwest Anesthesia Seminars - 14 CEC. “Ophthalmic Regional Block Hands-On Workshop.” The Hyatt Grand Cypress, Orlando, FL. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
November 5-20, 2016, India; Spiekermann Travel - 20 CEC. “Current Issues in CRNA Practice.” India. Michael Rieker, DNP, CRNA, Nurse Anesthesia Program, Medical Center Boulevard, Winston-Salem, NC 27157; (800) 645-3233; fax (586) 775-9556; email, [email protected]; http://www.mideasttrvl.com/.
November 6, 2016, Arizona; Encore Symposiums - 8 CEC. “Sedona Ultrasound Workshop 2016 by Encore Symposiums.” Hilton Sedona Resort at Bell Rock, Sedona, AZ. Nancy LaBrie, RN, 1907 Loch Lomond Court, Winston-Salem, NC 27106; (336) 768-9095; fax (336) 768-9055; email, [email protected]; www.escrnas.com.

214 AANA Journal June 2016 Vol. 84, No. 3 www.aana.com/aanajournalonline
November 6-9, 2016, South Carolina; Wake Forest School of Medicine - 19 CEC. “22nd Annual Advances in Physiology & Pharmacology in Anesthesia and Critical Care.” The Westin Hilton Head Island Resort & Spa, Hilton Head Island, SC. Pam Martin, Medical Center Blvd., Winston-Salem, NC 27157; (336) 716-2712; Fax (336) 716-8190; email, [email protected]; www.Wakehealth.edu/anes-cme-annual-meeting.
November 7-10, 2016, Arizona; Encore Symposiums - 21 CEC. “Sedona Red Rock & Grand Canyon Adventure 2016 Anesthesia Encore Symposiums.” Hilton Sedona Resort at Bell Rock, Sedona, AZ. Nancy LaBrie, RN, 1907 Loch Lomond Court, Winston-Salem, NC 27106; (336) 768-9095; fax (336) 768-9055; email, [email protected]; www.escrnas.com.
November 7-10, 2016, Florida; Institute For Post Graduate Education - 20 CEC. “Discussions in Clinical Anesthesia.” Westin Key West Resort & Spa, Key West, FL. Bernard Kuzava, CRNA, PO Box 28, Hastings, MI 49058; (877) 692-0430; fax (269) 948-2507; email, [email protected]; www.ipge.com.
November 7-10, 2016, Virginia; Nurse Anesthesiology Faculty Associates - 22 CEC. “40th Annual Anesthesia Conference.” Williamsburg Lodge, Williamsburg, VA. Michael Fallacaro, PO Box 980226, Richmond, VA 23298; (804) 828-6734; email, [email protected]; www.nafa-va.org.
November 11-13, 2016, California; University of California, Davis Health System - 20.75 CEC. “27th Annual UC Davis Anesthesiology Update.” Monterey Plaza Hotel, Monterey, CA. Beng Salud, 4150 V Street, PSSB Suite 1200, Sacramento, CA 95817; (916) 734-1574; fax (916) 734-2975; email, bsalud@ ucdavis.edu; www.ucdmc.ucdavis.edu/anesthesiology/.
November 11-13, 2016, Florida; Frank Moya Continuing Education Programs - 20 CEC. “45th Annual Refresher Course for Nurse Anesthetists.” Hilton Orlando Walt Disney World Resort, Lake Buena Vista, FL. Frank Moya, MD, 1828 SE First Ave, Ft. Lauderdale, FL 33316; (954) 763-8811; fax (954) 762-9111; email, [email protected]; www.currentreviews.com.
November 11-13, 2016, Illinois; American Association of Nurse Anesthetists. “2016 Fall Leadership Academy.” Westin O’Hare Hotel, Rosemont, IL. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
November 14, 2016, Nevada; Northwest Anesthesia Seminars - 8 CEC. “Business Concepts in Healthcare: A Practical Approach for Healthcare Providers.” The Cosmopolitan, Las Vegas, NV. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
November 14-18, 2016, Costa Rica; Southwest Anesthesia and Medical Seminars - 20 CEC. “Medical Spanish for Health Professionals.” Playa Flamingo, Guanacaste, Costa Rica. Richard M. Saucier,CRNA, MBA, 4466 North Saddle View Drive, Tucson, AZ 85750; (614) 582-3393; email, [email protected]; www.swamseminars.com.
November 28-December 1, 2016, Florida; Nurse Anesthesiology Faculty Associates - 22 CEC. “35th Annual Anesthesia Meeting.” Disney’s Yacht and Beach Club Resort, Lake Buena Vista, FL. Michael Fallacaro, PO Box 980226, Richmond, VA 23298; (804) 828-6734; email, [email protected]; www.nafa-va.org.
November 29-December 2, 2016 California; Northwest Anesthesia Seminars - 20 CEC. “Topics in Anesthesia.” Napa Valley Marriott Hotel and Spa, Napa, CA. Anna Hilliard, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
November 29-December 2, 2016 Georgia; Northwest Anesthesia Seminars - 24 CEC. “Current Topics in Anesthesia.” Hyatt Regency Savannah, Savannah, GA. Anna Hilliard, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
December 5-8, 2016, Bahamas; International Seminars, LLC - 20 CEC. “Nurse Anesthesia Update.” Atlantis, Paradise Island, Bahamas. Barbara McNulty, 1828 SE First Avenue, Ft. Lauderdale, FL 33316; (954) 763-2233; fax (954) 762-9111; email, [email protected]; www.nurseanesthetist.com.
December 5-9, 2016, Christiansted, St. Croix, US Virgin Islands; Northwest Anesthesia Seminars - 20 CEC. “Applied Pharmacology Update.” The Buccaneer, Christiansted, St. Croix, US Virgin Islands. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
December 13-16, 2016, Florida; Northwest Anesthesia Seminars - 20 CEC. “Current Topics in Anesthesia.” Eden Roc Miami Beach, Miami Beach, FL. NWAS, PO Box 2797, Pasco, WA 99302; (800) 222-6927; (509) 547-7065; fax (509) 547-1265; email, [email protected]; www.nwas.com.
January 9-11, 2017, California; C & H Educational Systems - 20 CEC. “The California Wine Country Anesthesia Update.” The Fairmont Sonoma Mission Inn and Spa, Sonoma, CA. Catherine Wagner, CRNA, MS, 130 Mackinaw Dr, Twin Lakes, CO 81251; (719) 486-3558; email, [email protected]; www.homestead.com/chedusys/index.html.
January 16-20, 2017, Aruba; Frank Moya Continuing Education Programs - 20 CEC. “Caribbean Seminar in Anesthesiology.” Aruba Marriott Resort & Stellaris Casino, Palm Beach, Aruba. Frank Moya, MD, 1828 SE First Ave, Ft. Lauderdale, FL 33316; (954) 763-8811; fax (954) 762-9111; email, [email protected]; www.currentreviews.com.
February 4-10, 2017, Colorado; University of Florida - 25 CEC. “Concepts in Anesthesiology.” Steamboat Grand Hotel, Steamboat Springs, CO. Medical Seminars LLC, 2451 Cumberland Parkway, Suite 3366, Atlanta, GA 30339; (800) 871-0326; fax (770) 847-8655; email, [email protected]; www.conceptsinanesthesiology.com.
February 24-26, 2017, Florida; American Association of Nurse Anesthetists. “Assembly of School Faculty.” Westin Beach Resort, Fort Lauderdale, FL. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
April 7-11, 2017, Washington, DC; American Association of Nurse Anesthetists. “Mid-Year Assembly 2017.” Renaissance Washington DC Downtown Hotel, Washington, DC. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
September 8-12, 2017, Washington; American Association of Nurse Anesthetists. “Nurse Anesthesia Annual Congress.” Washington State Convention Center, Seattle, WA. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
February 16-18, 2018, Arizona; American Association of Nurse Anesthetists. “Assembly of School Faculty.” The Scottsdale Resort, Scottsdale, AZ. (847) 655-8797; email, [email protected]; www.aana.com/meetings.

www.aana.com/aanajournalonline AANA Journal June 2016 Vol. 84, No. 3 215
April 20-24, 2018, Washington, DC; American Association of Nurse Anesthetists. “Mid-Year Assembly 2018.” Grand Hyatt, Washington, DC. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
September 21-25, 2018, Massachusetts; American Association of Nurse Anesthetists. “Nurse Anesthesia Annual Congress.” Hynes Convention Center, Boston, MA. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
April 5-9, 2019, Washington, DC; American Association of Nurse Anesthetists. “Mid-Year Assembly 2019.” Grand Hyatt, Washington, DC. (847) 655-8797; email, [email protected]; www.aana.com/meetings.
August 9-13, 2019, Illinois; American Association of Nurse Anesthetists. “Nurse Anesthesia Annual Congress.” Hyatt Regency Chicago Hotel, Chicago, IL. (847) 655-8797; email, [email protected]; www.aana.com/meetings.