Embed Size (px)
Citation preview

Copyright © 1093790 (OPIC 28/02/2012)
INTERNATIONAL CLINICAL PRACTICE GUIDELINES (CPG)
under the auspices of the International Society of Thrombosis and Hemostasis (ISTH)
VENOUS THROMBOEMBOLISM
AND CANCER
2 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Copyright © 1093790 (OPIC 28/02/2012)
These international guidelines were developed by the International Society of Thrombosis and
Haemostasis (ISTH) following an initiative from the “Groupe Francophone Thrombose et
Cancer” (GFTC) with the methodological support of the French National Cancer Institute
(INCa).
Financial support was provided by the Groupe Francophone Thrombose et Cancer
(www.thrombose-cancer.com), the Paris 7 Institut Universitaire d’Hématologie (IUH St Louis
Hospital), the International Society of Thrombosis and Haemostasis (ISTH) 2007 Presidential
Fund, the Société Médicale des Amis de Desgenettes du Service de Santé des Armées and the
French National Cancer Institute (INCa).

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Co p y r ig h t © 1 0 9 3 7 9 0 ( O P I C 2 8 / 0 2 / 2 0 1 2 ) | 3
Table of contents
1. INTRODUCTION ......................................................................................................................... 7
1.1. Epidemiology ............................................................................................................................. 7
1.2. Risk factors for DVT and PE in cancer patients ............................................................................. 7
1.3. Risk factors for catheter-related thrombosis in cancer patients .................................................. 10
1.4. Context ................................................................................................................................... 13
1.5. Expectations ............................................................................................................................ 13
1.6. Aims ........................................................................................................................................ 15 1.6.1. Clinical questions ............................................................................................................... 15 1.6.2. Targeted users ................................................................................................................... 17
1.7. Project management ................................................................................................................ 17 1.7.1. Sponsors ............................................................................................................................ 17 1.7.2. Funding ............................................................................................................................. 18 1.7.3. Working group ................................................................................................................... 18 1.7.4. Methodological support of INCa ......................................................................................... 19 1.7.5. Planning ............................................................................................................................ 20
2. METHODS ............................................................................................................................... 21
2.1. Literature search ..................................................................................................................... 21
2.2. Article selection ....................................................................................................................... 22
2.3. Critical appraisal and data extraction (see appendix 4 page 129) ................................................ 26
2.4. Conclusions and levels of evidence ........................................................................................... 26
2.5. Recommendations ................................................................................................................... 27 2.5.1. Economic considerations .................................................................................................... 27 2.5.2. General considerations: ..................................................................................................... 28
2.6. Peer-review process ................................................................................................................. 28
1. CHAPTER 1. INITIAL TREATMENT OF ESTABLISHED VTE .............................................................. 29
1.1. Bibliographic strategy results ................................................................................................... 29
1.2. Data extraction ........................................................................................................................ 30
1.3. Data analysis ........................................................................................................................... 45
1.4. Discussion ............................................................................................................................... 47
1.5. Recommendations – Initial treatment (first 5 to 10 days) of established VTE .............................. 48
2. CHAPTER 2. EARLY MAINTENANCE (10 DAYS TO 3 MONTHS) AND LONG-TERM TREATMENT
(BEYOND 3 MONTHS) OF ESTABLISHED VTE ............................................................................... 49
2.1. Bibliographic strategy results ................................................................................................... 49
2.2. Data extraction ........................................................................................................................ 50
2.3. Data analysis ........................................................................................................................... 55
2.4. Discussion ............................................................................................................................... 56
2.5. Recommendations – early maintenance treatment (10 days to 3 months) and long-term treatment (beyond 3 months) of established VTE ...................................................................................... 57
3. CHAPTER 3. TREATMENT OF RECURRENCE OF VTE IN CANCER PATIENTS UNDER ANTICOAGULATION59
3.1. Bibliographic strategy results ................................................................................................... 59
3.2. Data extraction ........................................................................................................................ 60
3.3. Data analysis ........................................................................................................................... 61
3.4. Discussion ............................................................................................................................... 62
3.5. Recommendations – recurrent VTE in cancer patients ............................................................... 62
4 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Copyright © 1093790 (OPIC 28/02/2012)
4. CHAPTER 4. PROPHYLAXIS OF VTE IN SURGICAL CANCER PATIENTS ............................................ 63
4.1. Bibliographic strategy results ................................................................................................... 63
4.2. Data extraction ........................................................................................................................ 64
4.3. Data analysis ........................................................................................................................... 72
4.4. Discussion ............................................................................................................................... 74
4.5. Recommendations – prophylaxis of VTE in surgical cancer patients ............................................ 76
5. CHAPTER 5. PROPHYLAXIS OF VTE IN MEDICAL CANCER PATIENTS .............................................. 78
5.1. Bibliographic strategy results ................................................................................................... 78
5.2. Data extraction ........................................................................................................................ 79
5.3. Data analysis ........................................................................................................................... 86
5.4. Discussion ............................................................................................................................... 87
5.5. Recommendations – prophylaxis of VTE in medical cancer patients ............................................ 89
6. CHAPTER 6. TREATMENT OF ESTABLISHED CATHETER-RELATED THROMBOSIS ............................. 91
6.1. Data extraction ........................................................................................................................ 92
6.2. Data analysis ........................................................................................................................... 94
6.3. Discussion ............................................................................................................................... 95
6.4. Recommendations: treatment of established catheter-related thrombosis ................................. 96
7. CHAPTER 7. PROPHYLAXIS OF CATHETER-RELATED THROMBOSIS ............................................... 97
7.1. Bibliographic strategy results ................................................................................................... 97
7.2. Data extraction ........................................................................................................................ 98
7.3. Data analysis ......................................................................................................................... 108
7.4. Discussion ............................................................................................................................. 109
8. CHAPTER 8. SPECIAL CASES .................................................................................................... 112
8.1. Bibliographic strategy results ................................................................................................. 112
8.2. Data extraction ...................................................................................................................... 113
8.3. Data analysis ......................................................................................................................... 117
8.4. Discussion ............................................................................................................................. 117
8.5. Recommendations: special cases ............................................................................................ 119
9. APPENDIX 1. WORKING GROUP AND COORDINATION .............................................................. 121
10. APPENDIX 2. BIBLIOGRAPHY SEARCH ...................................................................................... 122
11. APPENDIX 3. EBM WEBSITES SEARCH ...................................................................................... 128
12. APPENDIX 4. CRITICAL APPRAISAL GRIDS ................................................................................ 129
13. APPENDIX 5. METHODOLOGY OF GUIDELINES ELABORATION ................................................... 133
14. APPENDIX 6. METHODOLOGICAL TOOLS.................................................................................. 135
15. REFERENCES .......................................................................................................................... 139

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Co p y r ig h t © 1 0 9 3 7 9 0 ( O P I C 2 8 / 0 2 / 2 0 1 2 ) | 5
Abbreviations ACCP American College of Chest Physicians
ALL Acute Lymphocytic Leukemia
aPTT Actived Partial Thromboplastine Time
aRR Absolute Risk Reduction
ASA Acetylsalicylique Acid (Aspirin)
ASCO American Society of Clinical Oncology
ASH American Society of Hematology
ATIII AntiThrombin III
BMT Bone Marrow Transplant
CCTR Cochrane Controlled Trials Register
CI Confidence Interval
CP Continuous Perfusion
CPG Clinical Practice Guideline
CRT Catheter-Related Thrombosis
CT Chemotherapy
CS Compression Stockings
CVAD Central Venous Access Device
CVC Central Venous Catheter
D or d Day
DIC Disseminated Intravascular Coagulation
Doppler US Doppler UltraSonography
DVT Deep-Vein Thrombosis
ECD External Compression device
ESA Erythropoietin-Stimulating Agent
F Female
F II Factor II
F V L Factor V Leyden
FUT Fibrinogen Uptake Test
GCS Graduated Compression Stockings
H Hour
HR Hazard Ratio
HTA Health Technology Assessment
ICD Intermittent Compression Device
ICH IntraCranial Hemorrhage
IJV Internal Jugular Vena
INCa Institut National du Cancer
IMiD Thalidomide and lenalidomide
INR International Normalized Ratio
IPC Intermittent Pneumatic Compression
ISTH International Society of Thrombosis and Haemostasis
IV Intra Venous
IVC Inferior Vena Cava
IVCF Inferior Vena Cava Filter
Kc Cancer
KPS Karnofsky performance status
L4 or L3 Fourth or third lumbar vertebra
LMWH Low-Molecular-Weight Heparin

6 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Copyright © 1093790 (OPIC 28/02/2012)
M Male
mg milligram
MRI Magnetic Resonnace Imaging
MTHFR MethyleneTetraHydroFolate Reductase
NNT Number Needed to Treat
NS Not statistically Significant
OA Oral Anticoagulant
OR Odds Ratio
OS Overall Survival
PAR Population Attributable Risk
PBSC Peripheral Blood Stem Cell
PE Pulmonary Embolism
PICC Peripheral Indwelling Central Catheter
po per os
PT Prothrombin Time
PTT Partial Thromboplastin Time
RA Right Atrium
RCT Randomized Controlled Trial
RR Relative Risk
RRR Relative Risk Reduction
SCD Sequential Compression Device
SVC Superior Vena Cava
T4 or T3 Fourth or third thoracic vertebra
UFH Unfractionated Heparin
UMCG University Medical Center Groningen
VCF Vena Cava Filter
VKA Vitamin K Antagonists
VTE Venous ThromboEmbolism
W or w Week
WAR Warfarin
Yrs Years
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Co p y r ig h t © 1 0 9 3 7 9 0 ( O P I C 2 8 / 0 2 / 2 0 1 2 ) | 7
1. Introduction
1.1. Epidemiology
Cancer is an independent and major risk factor for venous thromboembolism (VTE)
[LEVITAN1999] [HEIT2000]. Venous thromboembolism (VTE) is defined as deep-vein
thrombosis (DVT), including catheter-related thrombosis (CRT), and pulmonary embolism (PE).
VTE occurs in 4 to 20% of cancer patients. In hospitalized patients included in the National
Hospital Discharge Survey (USA), the rate of VTE was 2% in patients with cancer and 1% among
patients without cancer [STEIN2006].
Although the association between cancer and thrombosis has been known since Trousseau's
first report [TROUSSEAU1865], cancer care providers now have increased awareness of the
impact of thrombotic complications in patients with cancer. Several factors have contributed
to this heightened awareness.
Firstly, cancer-associated VTE is increasingly prevalent. In an analysis of more than 1 million
hospitalized patients with cancer, the rate of VTE increased by 28% from 1995 to 2003
(p <0.0001) [KHORANA2007]. In an exhaustive review of the literature, the frequency of
symptomatic catheter-related thrombosis was 5%, a figure subsequently confirmed in
prospective clinical trials [VERSO2003] [DEBOURDEAU2009].
Secondly, the consequences of VTE are better understood. Thrombosis is the second-leading
cause of death in patients with cancer [KHORANA2007A]. Furthermore, VTE is an independent
prognosis factor of worsened mortality in cancer patients. Cancer patients with VTE have a
shorter global survival than cancer patients with similar tumoral stage and anti-cancer
treatments but without VTE. Among 1 211 944 patients with cancer, global survival was 6% in
patients with VTE compared to 58% in subjects without VTE [LEVITAN1999]. In a study of
235 149 cancer patients included in the California Cancer Registry, adjusting for age, race and
stage, diagnosis of VT, was a significant predictor of decreased survival during the first year for
all cancer types (hazard ratios, 1.6-4.2; p<0.01) [CHEW2006]. In addition, patients with cancer
who suffer from VTE have an increased risk of recurrent VTE, bleeding complications,
morbidity, and utilization of health care resources [PRANDONI2002] [ELTING2000]. In this last
study, 525 of the 529 patients with venous thromboembolic events were hospitalized for initial
anticoagulation therapy, for a mean of 11 days. The mean cost of hospitalization was
20 065 US $ [ELTING2000].
1.2. Risk factors for DVT and PE in cancer patients
The high incidence of VTE in cancer patients is due to the presence of various simultaneous
risk factors: the underlying neoplasm (histological type, stage and site), type of surgery,
hospitalization, presence of a central venous catheter, and use of chemotherapy and/or
erythropoiesis stimulating agents (ESA) [BOHLIUS2006] [BENNETT2008] [MAREC-
BERARD2009]. Cancer-associated VTE is a multifactorial illness. A recently developed risk score
can identify cancer patients treated with chemotherapy who are at high risk for VTE by utilizing
a combination of easily available clinical and laboratory variables (Table 1) [KHORANA2008].
The risk score for VTE was derived from a development cohort of 2701 patients and then

8 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Copyright © 1093790 (OPIC 28/02/2012)
validated in an independent cohort of 1365 patients from a prospective registry. The stage-
adjusted multivariate model identified five predictive variables. Observed rates of VTE in the
development and validation cohorts were 0.8% and 0.3% in the low-risk category, 1.8% and 2%
in the intermediate-risk category and 7.1% and 6.7% in the high-risk category, respectively.
This model has now been externally validated by the Vienna CATS study in 819 cancer patients
[AY2010]. The 6-month cumulative probabilities of developing VTE in this study population
were 1.5% (score of 0), 3.8% (score of 1), 9.4% (score of 2) and 17.7% (score ≥3). Several other
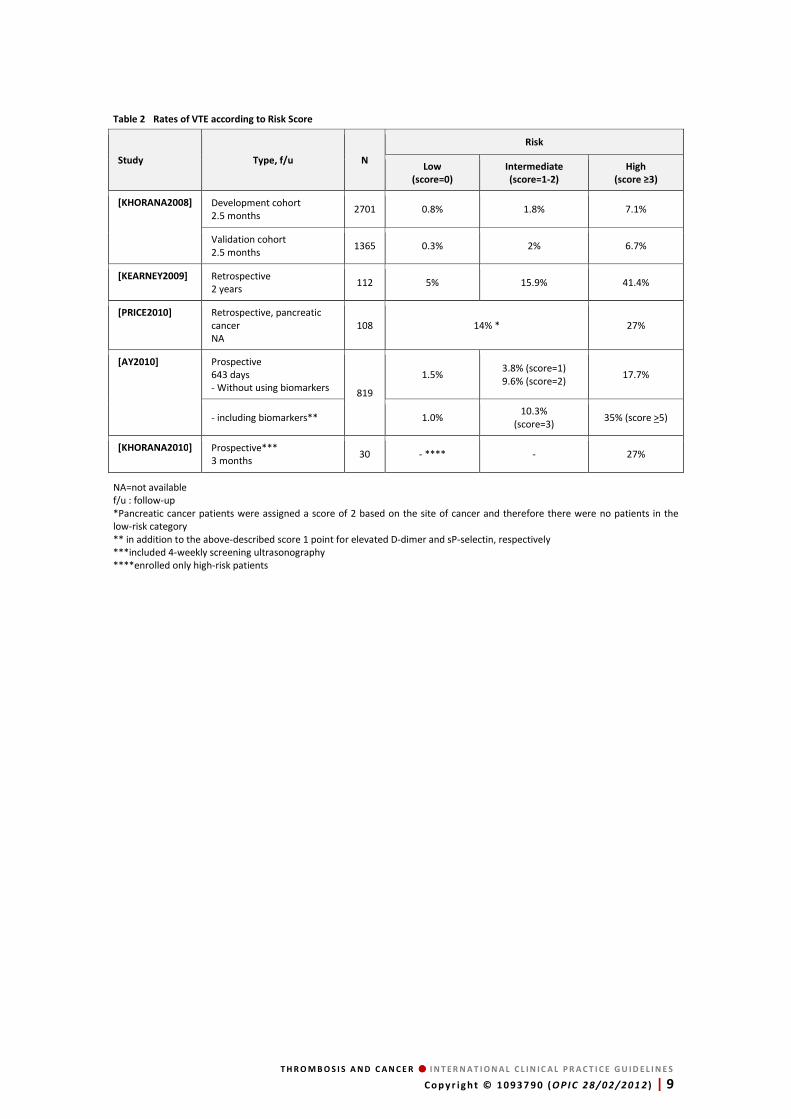
retrospective and prospective studies have further validated this risk score, although rates vary
between studies because of differences in patient selection and follow-up periods (Table 2). In
addition, the Vienna group has described an expansion of this original risk score with the
inclusion of two additional biomarkers: D-dimer and soluble P-selectin (sP-selectin). This
further improved the prediction, specifically the positive predictive value. Patients with a score
of 5 or higher had a risk/cumulative probability of 35% to develop thrombosis within 6 months
after diagnosis of cancer. However, biomarker tests need to be available. This issue has already
been widely achieved with the D-dimer test, but still has to be further confirmed for the
sP-selectin.
Table 1 Predictive model for cancer-associated/chemotherapy-associated VTE ([KHORHANA2008])
Patient Characteristics Risk score
Site of cancer Very high risk (stomach, pancreas) High risk (lung, lymphoma, gynecologic sites, bladder, testis)
2 1
Prechemotherapy platelet count ≥350 000/mm3 1
Hemoglobin level ≤10g/dL or use of red cell growth factors 1
Prechemotherapy leukocyte count ≥11 000/mm3 1
Body mass index ≥35 kg/m2 1
No risk factor 0
Risk score TOTAL
Low 0
Intermediate 1-2
High ≥3
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Co p y r ig h t © 1 0 9 3 7 9 0 ( O P I C 2 8 / 0 2 / 2 0 1 2 ) | 9
Table 2 Rates of VTE according to Risk Score
NA=not available f/u : follow-up *Pancreatic cancer patients were assigned a score of 2 based on the site of cancer and therefore there were no patients in the low-risk category ** in addition to the above-described score 1 point for elevated D-dimer and sP-selectin, respectively ***included 4-weekly screening ultrasonography ****enrolled only high-risk patients
Study Type, f/u N
Risk
Low
(score=0)
Intermediate
(score=1-2)
High
(score ≥3)
[KHORANA2008] Development cohort 2.5 months
2701 0.8% 1.8% 7.1%
Validation cohort 2.5 months
1365 0.3% 2% 6.7%
[KEARNEY2009] Retrospective 2 years
112 5% 15.9% 41.4%
[PRICE2010] Retrospective, pancreatic cancer NA
108 14% * 27%
[AY2010] Prospective 643 days - Without using biomarkers
819
1.5% 3.8% (score=1) 9.6% (score=2)
17.7%
- including biomarkers** 1.0% 10.3%
(score=3) 35% (score >5)
[KHORANA2010] Prospective*** 3 months
30 - **** - 27%

10 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Copyright © 1093790 (OPIC 28/02/2012)
1.3. Risk factors for catheter-related thrombosis in cancer patients
Several risk factors for CRT have been identified in cancer patients.
Risk factors that are related to patient’ characteristics and to catheter insertion modalities
were studied in these guidelines because of their clinical consequences. Conversely, different
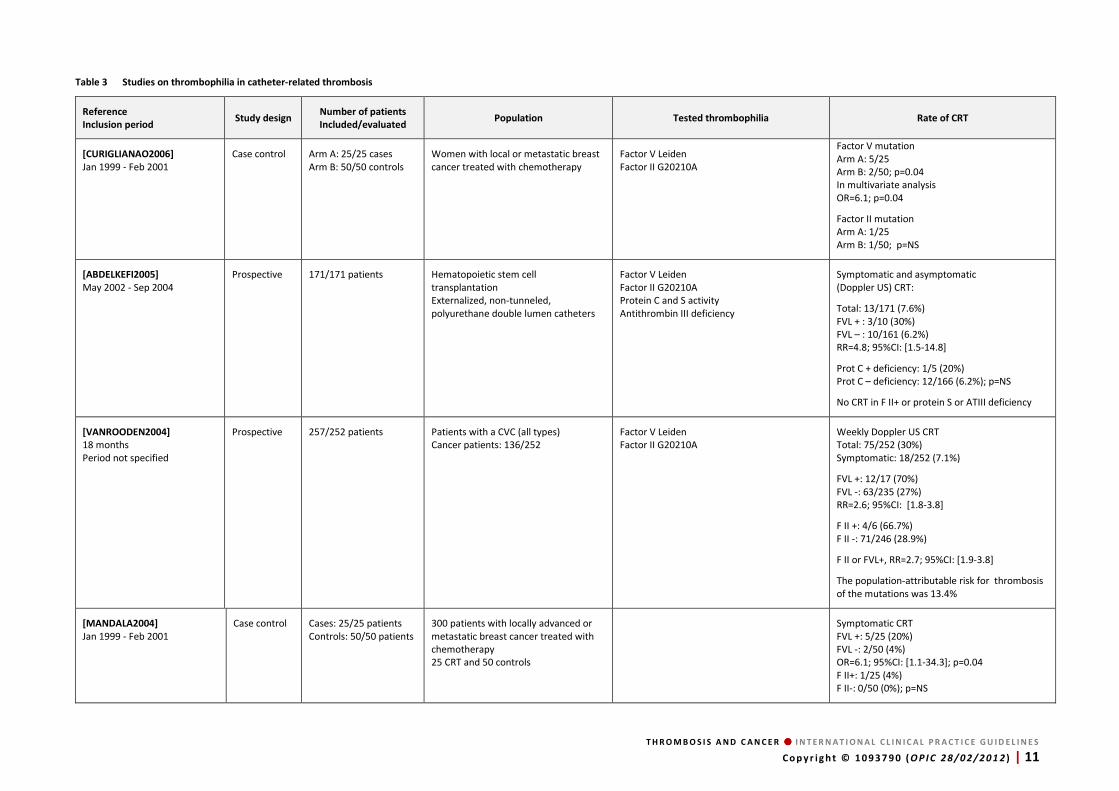
types of thrombophilia are associated with CRT in cancer patients without any clinical
implications (see Table 3).
The most common thrombophilias shown to be risk factors for CRT in cancer patients are
those involving factor II mutation (G20210A prothrombin mutation) and factor V mutation
(Q 506 mutation factor V Leiden), in most cases as heterozygous mutations. The estimated
attributable risk of CRT conferred by the presence of factor V and factor II mutations was
about 13.1% and 4.5% respectively in the meta-analysis by Dentali et al. [DENTALI2007], but
their clinical consequences cannot be assessed in the absence of dedicated studies. Similarly,
few studies have analysed the respective incidence and role of protein S and protein C
deficiency.
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S Co p y r ig h t © 1 0 9 3 7 9 0 ( O P I C 2 8 / 0 2 / 2 0 1 2 ) | 11
Table 3 Studies on thrombophilia in catheter-related thrombosis
Reference
Inclusion period Study design
Number of patients
Included/evaluated Population Tested thrombophilia Rate of CRT
[CURIGLIANAO2006]
Jan 1999 - Feb 2001 Case control Arm A: 25/25 cases
Arm B: 50/50 controls Women with local or metastatic breast cancer treated with chemotherapy
Factor V Leiden Factor II G20210A
Factor V mutation Arm A: 5/25 Arm B: 2/50; p=0.04 In multivariate analysis OR=6.1; p=0.04
Factor II mutation Arm A: 1/25 Arm B: 1/50; p=NS
[ABDELKEFI2005]
May 2002 - Sep 2004 Prospective 171/171 patients Hematopoietic stem cell
transplantation Externalized, non-tunneled, polyurethane double lumen catheters
Factor V Leiden Factor II G20210A Protein C and S activity Antithrombin III deficiency
Symptomatic and asymptomatic (Doppler US) CRT:
Total: 13/171 (7.6%) FVL + : 3/10 (30%) FVL – : 10/161 (6.2%) RR=4.8; 95%CI: [1.5-14.8]
Prot C + deficiency: 1/5 (20%) Prot C – deficiency: 12/166 (6.2%); p=NS
No CRT in F II+ or protein S or ATIII deficiency
[VANROODEN2004]
18 months Period not specified
Prospective 257/252 patients Patients with a CVC (all types) Cancer patients: 136/252
Factor V Leiden Factor II G20210A
Weekly Doppler US CRT Total: 75/252 (30%) Symptomatic: 18/252 (7.1%)
FVL +: 12/17 (70%) FVL -: 63/235 (27%) RR=2.6; 95%CI: [1.8-3.8]
F II +: 4/6 (66.7%) F II -: 71/246 (28.9%)
F II or FVL+, RR=2.7; 95%CI: [1.9-3.8]
The population-attributable risk for thrombosis of the mutations was 13.4%
[MANDALA2004]
Jan 1999 - Feb 2001 Case control Cases: 25/25 patients
Controls: 50/50 patients 300 patients with locally advanced or metastatic breast cancer treated with chemotherapy 25 CRT and 50 controls
Symptomatic CRT FVL +: 5/25 (20%) FVL -: 2/50 (4%) OR=6.1; 95%CI: [1.1-34.3]; p=0.04 F II+: 1/25 (4%) F II-: 0/50 (0%); p=NS

12 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 3 Studies on thrombophilia in catheter-related thrombosis (continued)
Reference
Inclusion period Study design
Number of patients
Included/evaluated Population Tested thrombophilia Rate of CRT
[JANSEN2005]
Jul 1996 - Apr 2002 Case control Cases: 30/30 patients
Controls: 30/30 patients 235 patients undergoing allogeneic bone marrow transplantation
Factor V Leiden
Symptomatic CRT FVL+: 5/30 (17%) FVL -: 0/30; p <0.02
[FIJNHEER2002]
Jan 1999 - Dec 2000 Prospective 299/277 patients Patients aged 18 years or older who had
undergone allogenic bone marrow transplantation Tunneled Hickman catheters
Factor V Leiden
Symptomatic CRT FVL+: 7/13 (54%) FVL-: 26/264 (9.8%) RR=7.7; 95%CI: [3.3 -17.9]
The population-attributable risk for thrombosis of the mutations was 17.3%
[RUUD2002]
Not specified Prospective 41/41 patients 41 consecutive patients, aged
10 months -15 years with leukemia, lymphoma or malignant brain tumor
Factor V Leiden Factor II G20210A
Asymptomatic CRT DopplerUS inclusion + M3 and M5 Total: 18/41 (44%) No mutation for F V and F II
[WERMES1999]
Not specified Prospective 137/137 patients Pediatric patients with solid tumors or
leukemia/lymphoma Factor V Leiden Factor II G20210A Protein C and S activity Homozygous MTHFR ATIII deficiency
Symptomatic CRT FVL+: 1/11 (9.1%) FV -: 9/126 (7.1%)
F II+: 1/4 (25%) F II-: 3/133(2.5%); p=NS
Protein S deficiency+: 1/1 Protein S deficiency-: 0/136; p=NS
[RATCLIFFE1999]
Not specified Prospective 84/84 patients Adult patients with solid or
hematological malignancies treated with chemotherapy
Factor V Leiden Factor VIII levels Anticardiolipin antibodies
Symptomatic CRT FVL+: 1/10 (10%) FVL–: 2/74 (2.7%) OR=4; 95%CI: [0.33-48]
[DENTALI2007]
1994 - Mar 2007 Meta-analysis 10 studies
[ABDELKEFI2005], [MANDALA2004], [VANROODEN2004], [MITCHELL2003], [FIJNHEER2002], [RUUD2002], [KNOFLER1999], [RATCLIFFE1999], [WERMES1999], [SIFONTES1997]
OR were calculated using a fixed-effect model (Mantel-Haenszel method) and comparing these findings with results obtained using a random-effects model (Der Simionan and Laird method). Statistical heterogeneity was evaluated using the Chi-Square statistic. The proportion of CVC-related thrombosis in the population that could be attributed to the mutation was calculated as follows: PAR = 100 x [Prevalence (OR – 1) / Prevalence (OR – 1) + 1].
Factor V Leiden 211 cases and 860 controls G20210A prothrombin mutation 140 cases and 502 controls
Factor V mutation OR=4.6; 95%CI: [2.6-8.1] The estimated attributable risk of CRT conferred by the mutation is 13.1% in this pooled cohort.
G20210A prothrombin mutation OR=4.9; 95%CI: [1.7-14.3] The estimated attributable risk of CRT conferred by the mutation is 4.5% in this pooled cohort.
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 13 Copyright © 1093790 (OPIC 28/02/2012)
1.4. Context
Venous thromboembolism (VTE) is a major therapeutic issue in cancer patients. VTE is an
independent prognostic factor and a leading cause of death [KOHRANA2007A].
In this population,
• for the treatment of DVT and PE: Low-Molecular-Weight Heparins (LMWH) have been shown to be superior to vitamin K antagonists (VKA) |MEYER2002] [LEE2003] [HULL2006];
• for the prophylaxis of VTE in surgical patients: use of LMWH has been validated ([AKL2008D] [AKL2008E];
• for the prophylaxis of VTE in medical cancer patients: many clinical trials have been published or are about to be published, which will further inform our practice.
Therefore, the prevention and the treatment of VTE in cancer patients represent a major
therapeutic challenge since:
• implementation of specific prophylactic regimens in onco-hematology has recently become an area of interest;
• the management of established VTE in cancer patients has changed over the last ten years, given the results of comparisons between classical anticoagulation protocols using LMWH and early VKA therapy and the long-term use of LMWH for 3 to 6 months. Because cancer patients often present with a variety of risk factors and co-morbidities, specific oncology guidelines on the subject were established using various methodological approaches.
These national guidelines for the treatment of VTE in cancer patients were successively
published by:
• the Italian Association of Medical Oncology (AIOM) [MANDALA2006],
• the American Society of Clinical Oncology (ASCO) [LYMAN2007],
• the French “Institut National du Cancer” (INCa) [FARGE2008] [DEBOURDEAU2009],
• the American College of Chest Physicians (ACCP) [GEERST2008] [KEARON2008],
• the National Comprehensive Cancer Network (NCCN) [NCCN2011].
Meanwhile, the European Society of Medical Oncology (ESMO) has published its own
recommendations [MANDALA2009] [MANDALA2011].
Despite the paucity of evidence-based data in hematology patients, recommendations were
also issued for the treatment of VTE in multiple myeloma patients [PALUMBO2008].
1.5. Expectations
Despite some methodological variations and although few guidelines covered all the questions
to be assessed [KHORANA2007] [FARGE2010], the final recommendations were similar.
However, worldwide, there is still large heterogeneity in the clinical knowledge and
implementation of these recommendations. In addition, many clinicians are reluctant to
modify their practice or still have doubt on the tolerability and acceptance of long-term daily
subcutaneous treatment [DEBOURDEAU2008] when applying standard therapeutic
recommendations. A subset of cancer patients with either life-threatening thrombotic disease,
advanced cancer disease, renal insufficiency or thrombocytopenia may require alternative

14 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
therapeutic options, since specific precautions must be taken into consideration in the decision
to anticoagulate.
In addition, underuse of VTE prophylaxis still represents a major clinical challenge in the
general population, and use of adequate prophylaxis in the surgical or medical setting is even
less frequent in the cancer subgroup than in other patients [COHEN2008]. Tolerance and cost
effectiveness of long-term use of LMWH may account for large heterogeneity in daily clinical
practice and the implementation of specific recommendations for cancer patients is still low in
daily clinical practice. VTE in cancer patients requires a multidisciplinary approach, but
downstream of guidelines publication, the potential organizational barriers to applying these
recommendations have not been discussed.
In a previous paper, the authors of the present guidelines called for a sustained research effort
to investigate the clinical issues identified here to reduce the burden of VTE and its
consequences in cancer patients. They highlighted the need for an homogenization of
guidelines by an international consensus working group followed by educational and active
implementation strategies [KHORANA2009]. The aims of these international clinical practice
guidelines (CPG) are:
• to pool the data of existing guidelines to reach consensus,
• to take into account the difficulties in order to make each CPG easier to use and implement at each national level,
• to study clinical questions that are unanswered.
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 15 Copyright © 1093790 (OPIC 28/02/2012)
1.6. Aims
1.6.1. Clinical questions
These CPG concern venous thrombosis management in cancer patients: treatment and
prophylaxis of deep venous thrombosis, pulmonary embolism and catheter-related
thrombosis.
Based on the context and the expectations, described above, the working group selected the
following clinical questions because they remain unanswered and/or needed to be
internationally homogenized:
Q1. Initial treatment (0 up to 10 days) of established VTE (specific cases excluded)
1. UFH followed by VKA
2. LMWH followed by VKA
3. LMWH vs. UFH
4. Fondaparinux
5. Thrombolytics
6. Vena cava filters
Q2. Early maintenance treatment (10 days to 3 months) and long-term treatment (beyond
3 months) of established VTE (specific cases excluded)
1. Early maintenance and long-term use of LMWH
2. Idraparinux
3. Duration of the treatment
Q3. Treatment of VTE recurrence (specific cases excluded)
1. VKA or LMWH
2. Vena cava filter
Q4. Prophylaxis of VTE in surgical cancer patients (specific cases excluded)
1. LMWH or UFH vs. placebo or no treatment
2. LMWH vs. UFH
3. Comparison of drugs
4. Dose of LMWH
5. Duration of prophylaxis and extended treatment
6. Use of external compression devices

16 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Q5. Prophylaxis in medical cancer patients (specific cases excluded)
1. Hospitalized patients
2. Children with Acute Lymphoblastic Leukemia (ALL) treated with L-asparaginase
3. Patients treated with chemotherapy
4. Patients treated with thalidomide or lenalidomide
Q6. Treatment of established Catheter-Related Thrombosis (CRT)
1. LMWH+VKA
2. Withdrawal of CVC
3. Thrombolytics
Q7. Prophylaxis of CRT
1. VKA
2. UFH
3. LMWH
4. Thrombolytics
5. Type of CVC and insertion modalities
Q8. Specific cases: all these specific cases which were not studied in the above clinical
questions
1. Initial treatment (0-10 days), early maintenance treatment (10 days to 3 months) and
long-term treatment of established VTE in patients with brain tumors
2. Prophylaxis of VTE in cancer patients with neurosurgery
3. Treatment and prophylaxis of VTE in cancer patients with renal failure
4. Treatment and prophylaxis of VTE in patients with thrombocytopenia
5. Treatment and prophylaxis of VTE in pregnant women with cancer
The focus of these guidelines is the treatment and prophylaxis of DVT, PE and CRT. The
following questions were not addressed either because they were beyond the scope of the
guidelines or because of the lack of data:
• Role of anticoagulation treatment on tumor response
• Treatment adherence
• Effect of anticoagulation on patient survival
• Search for underlying cancer in the case of new onset of idiopathic VTE
• Economic evaluation is too heterogeneous to be assessed as a specific question. Indeed, the recommended drugs are not available in each country. Furthermore, the price of drugs varies substantially in each country. The present CPG recommendations were elaborated using medical data and could not be based on cost of anticoagulation approaches. In some specific cases, where strong evidence is lacking, the price could have been taken into account to elaborate a recommendation that was cheaper than another one.
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 17 Copyright © 1093790 (OPIC 28/02/2012)
1.6.2. Targeted users
The professionals for whom the guidelines are intended are:
1. Health care providers
• oncologists
• hematologists
• surgeon-oncologists
• gynecologist-oncologists
• surgeons
• vascular disease specialists
• internal medicine specialists
• palliative medicine specialists
• gynecologists
• geriatricians
• radiation oncologists
• neurologists
• general practitioners
• pharmacists
• nurses
2. Stakeholders
• hospital directors
• public health institutions
• health networks
• medical societies
3. Although these recommendations were not specifically established for patients’ use,
members from patients’ associations were included in the reading group. They reviewed these
guidelines and patients’ preferences, opinions, expectations and needs were taken into
account.
1.7. Project management
1.7.1. Sponsors
These international guidelines were elaborated by the International Society of Thrombosis and
Haemostasis (ISTH), following an initiative from the Groupe Francophone Thrombose et Cancer
(GFTC) with the collaboration of the Academic Medical Centre (AMC) and the University
Medical Center Groningen (UMCG) Netherlands, and the methodological support of the French
Institute of Cancer (INCa).
18 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
1.7.2. Funding
Financial support was given by the Groupe Francophone Thrombose et Cancer
(www.thrombose-cancer.com), the Paris 7 Institut Universitaire d’Hématologie (IUH Saint
Louis Hospital), The International Society on Thrombosis and Haemostasis (ISTH) 2007
Presidential Fund, and the French Institute of Cancer (INCa).
The authors acknowledge the role of the ISTH, the IUH, the INCa and the GFTC for their
financial support.
1.7.3. Working group
A multidisciplinary working group from different countries was set up to develop these
international guidelines according to INCa methodology.
The working group consisted of:
• 24 experts from the following specialities :
� Oncology, Hematology, Palliative medicine
� Internal medicine, Vascular disease
� Biology, Epidemiology
• Others:
� 2 nurses: from Europe and USA;
� 2 patient representatives
� 2 methodologists
� 2 coordinators
Three major working subgroups were constituted throughout the process:
1- VTE treatment in the general population and for specific patient groups
2- VTE prophylaxis:
2.1. Surgical patients
2.2. Medical patients
3- Catheter-related thrombosis: prophylaxis/treatment
Coordinators and methodologists were particularly assigned to each specific group, but could
of course cover every single subject.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 19 Copyright © 1093790 (OPIC 28/02/2012)
Role of the working group members in the project
Coordinators Methodologists Experts Nurses Patients
Selection of clinical questions to adress x x x
Bibliographic search x x x
Article selection x x
Validation of literature selection x x x x
Critical appraisal of the literature x x
Extraction of data in evidence tables x
Validation of the first draft x x x x x
Conclusions and recommendations writing
x x x x x
Validation of the final draft x x x x x
Website X
Project planning x x
1.7.4. Methodological support of INCa
This support aimed:
• to advise on project management and the CPG method;
• to perform a professional literature search on EBM websites and in the Medline® database;
• to review intermediate drafts and advise on the presentation of the data;
• to set up a collaborative website for the working group dedicated to the project.

20 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
1.7.5. Planning
The planning of the project was the following:
STEPS Date
Project planning 03 Nov 2009 - 28 Nov 2009
First draft of clinical questions to be validated by the working group 05 Jan 2010 - 31 Jan 2010
First literature search and selection 01 Feb 2010 - 15 Mar 2010
Agreement on the topics of the recommendations 01 Apr 2010 - 15 May 2010
Constitution of the working group 03 Nov 2009 - 31 Jul 2010
First meeting - Paris
• Choice of clinical questions to be studied
• Choice of the methodology to be used
• Choice of gradation system for the CPG
• Allocating tasks to the members of the working group
28 Oct 2010
First draft validation by the working group via the dedicated website 15 Apr 2011 - 15 May 2011
Second meeting - Paris
• Validation of the literature levels of evidence made for each clinical question 19 May 2011
Elaboration of recommendations 20 May 2011 - 20 Jul 2011
Third meeting - ISTH meeting in Kyoto
• Elaboration of the recommendations July 2011
First draft writing 01 Sep 2011 - 15 Nov 2011
Fourth meeting
• Validation of recommendations after external review process 20 Apr 2012
Update
These guidelines will be updated every 4 years.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 21 Copyright © 1093790 (OPIC 28/02/2012)
2. Methods This clinical practice guideline methodology is based on Clinical Practice Guidelines (CPG)
method with the following steps:
• literature exhaustive review and selection;
• critical appraisal;
• data extraction;
• conclusions and recommendations writing;
• peer-review process.
The different steps of the methodology are shown in appendix 5 page 133. This method is fully
detailed below and in appendix 6 page 135.
2.1. Literature search
A literature search for all studies published between January 1996 and January 2011 was
performed using the Medline® database and the following subject headings: cancer, venous
thromboembolism, and anticoagulant drugs. A prospective follow-up of the literature was
continued up to June 2011. Members of the working group also added other references: those
not found by the bibliographic search. In addition, when available, data previously extracted by
the working group members from former guidelines or meta-analyses [LYMAN20007]
[FARGE2008] [NOBLE2008] [GEERST2008] [DEBOURDEAU2009] were added into the analysis,
even if the original paper had been published before 1996. National guidelines and several
sites of Evidence-Based Medicine were also consulted (see list of URL link visited in appendix 3
page 128).
The literature search was limited to publications in English or in French.
Meta-analyses, systematic reviews, randomized clinical trials, or non-randomized prospective
or retrospective studies in the absence of randomized clinical trials, were included in the
analysis. Editorials, letters to the editor, case reports, publications without an abstract, press
releases and animal studies were excluded. Abstracts were included only if a full paper was
accepted in a peer-reviewed medical journal.
In the absence of specific studies on patients with cancer, we also analyzed studies performed
in the general population of VTE patients, which also included patients with cancer. In this
case, results were extrapolated to cancer patients and methodological biases were taken into
account.
The terms used in the literature search for the treatment of VTE were: treatment,
anticoagulation, low-molecular-weight heparin, unfractionated heparin, and therefore
included new oral anticoagulants,
The bibliographic search strategy is shown in appendix 2 on page 122.

22 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
2.2. Article selection Q1. Initial treatment (0 up to 10 days) of established VTE
Inclusion criteria Exclusion criteria
Population Patients with:
• cancer (solid tumors),
• acute leukemia,
• multiple myeloma,
• lymphoma. Confirmed VTE (deep-vein thrombosis and pulmonary embolism) Patients treated by all cancer associated therapies:
• chemotherapy,
• growth factors,
• hormonal therapy,
• targeted therapy (anti-angiogenics, monoclonal antibodies),
• surgery,
• radiotherapy. Initial treatment of VTE corresponds to the first 10 days of anticoagulation.
Patients with a tumor thrombus, or a history of cancer in remission for more than five years Patients with no VTE (prophylaxis) Catheter-related thrombosis Superficial-vein thrombosis
Intervention UFH VKA LMWH Fondaparinux Thrombolytics Vena cava filters External compression devices
Drugs or devices that are not marketed
Outcomes Rates of VTE (de novo VTE or VTE extension) Major and minor bleeding Thrombocytopenia Death
Catheter-related thrombosis Superficial-vein thrombosis
Major bleeding was defined as [SCHULMAN2005] [SCHULMAN2010]:
• fatal bleeding,
• bleeding into a critical organ (brain, intra-abdominal bleeding, gastrointestinal tract)
• associated with a decrease in hemoglobin level of more than 2 g/dL
• leading to the transfusion of two or more units of blood.
Minor bleeding was defined as all other bleeds.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 23 Copyright © 1093790 (OPIC 28/02/2012)
Q2. Early maintenance (10 days to 3 months) and long-term treatment (beyond 3 months) of established VTE
Inclusion criteria Exclusion criteria
Population Patients with:
• cancer (solid tumors),
• acute leukemia,
• myeloma,
• lymphoma. Confirmed VTE (deep-vein thrombosis and pulmonary embolism) Patients treated by all cancer-associated therapies:
• chemotherapy,
• growth factors,
• hormonal therapy,
• targeted therapy (anti-angiogenics, monoclonal antibodies)
• surgery,
• radiotherapy.
Patients with tumor thrombus, or a history of cancer in remission for more than five years Patients with no VTE (prophylaxis) Catheter-related thrombosis Superficial-vein thrombosis
Intervention VKA LMWH : long-term use of Idraparinux
Drugs or devices that are not marketed
Outcomes Rates of VTE:
• de novo VTE
• VTE extension Major and minor bleeding Thrombocytopenia Death
Catheter-related thrombosis Superficial-vein thrombosis
Q3. Recurrent VTE treatment
Inclusion criteria Exclusion criteria
Population Patients with:
• cancer (solid tumor),
• acute leukemia,
• multiple myeloma,
• lymphoma. Confirmed VTE (deep-vein thrombosis and pulmonary embolism) Patients treated by all cancer-associated therapies:
• chemotherapy,
• growth factors,
• hormonal therapy,
• targeted therapy (anti-angiogenics, monoclonal antibodies),
• surgery,
• radiotherapy.
Patients with a tumor thrombus, or a history of cancer in remission for more than five years Patients with no VTE (prophylaxis) Catheter-related thrombosis Superficial-vein thrombosis
Intervention VKA Vena cava filters
Drugs or devices that are not marketed
Outcomes Rate of VTE:
• de novo VTE
• VTE extension Major and minor bleeding Thrombocytopenia Death
Catheter-related thrombosis Superficial-vein thrombosis
24 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
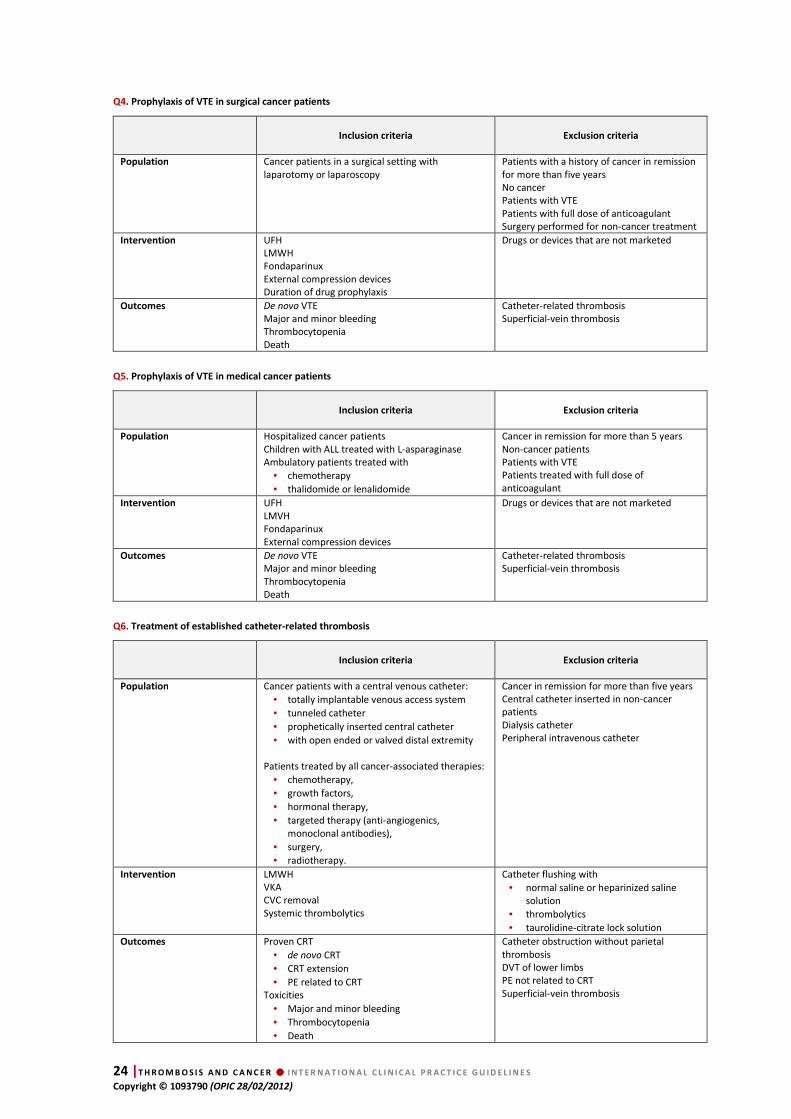
Q4. Prophylaxis of VTE in surgical cancer patients
Inclusion criteria Exclusion criteria
Population Cancer patients in a surgical setting with laparotomy or laparoscopy
Patients with a history of cancer in remission for more than five years No cancer Patients with VTE Patients with full dose of anticoagulant Surgery performed for non-cancer treatment
Intervention UFH LMWH Fondaparinux External compression devices Duration of drug prophylaxis
Drugs or devices that are not marketed
Outcomes De novo VTE Major and minor bleeding Thrombocytopenia Death
Catheter-related thrombosis Superficial-vein thrombosis
Q5. Prophylaxis of VTE in medical cancer patients
Inclusion criteria Exclusion criteria
Population Hospitalized cancer patients Children with ALL treated with L-asparaginase Ambulatory patients treated with
• chemotherapy
• thalidomide or lenalidomide
Cancer in remission for more than 5 years Non-cancer patients Patients with VTE Patients treated with full dose of anticoagulant
Intervention UFH LMVH Fondaparinux External compression devices
Drugs or devices that are not marketed
Outcomes De novo VTE Major and minor bleeding Thrombocytopenia Death
Catheter-related thrombosis Superficial-vein thrombosis
Q6. Treatment of established catheter-related thrombosis
Inclusion criteria Exclusion criteria
Population Cancer patients with a central venous catheter:
• totally implantable venous access system
• tunneled catheter
• prophetically inserted central catheter
• with open ended or valved distal extremity Patients treated by all cancer-associated therapies:
• chemotherapy,
• growth factors,
• hormonal therapy,
• targeted therapy (anti-angiogenics, monoclonal antibodies),
• surgery,
• radiotherapy.
Cancer in remission for more than five years Central catheter inserted in non-cancer patients Dialysis catheter Peripheral intravenous catheter
Intervention LMWH VKA CVC removal Systemic thrombolytics
Catheter flushing with
• normal saline or heparinized saline solution
• thrombolytics
• taurolidine-citrate lock solution
Outcomes Proven CRT
• de novo CRT
• CRT extension
• PE related to CRT Toxicities
• Major and minor bleeding
• Thrombocytopenia
• Death
Catheter obstruction without parietal thrombosis DVT of lower limbs PE not related to CRT Superficial-vein thrombosis
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 25 Copyright © 1093790 (OPIC 28/02/2012)
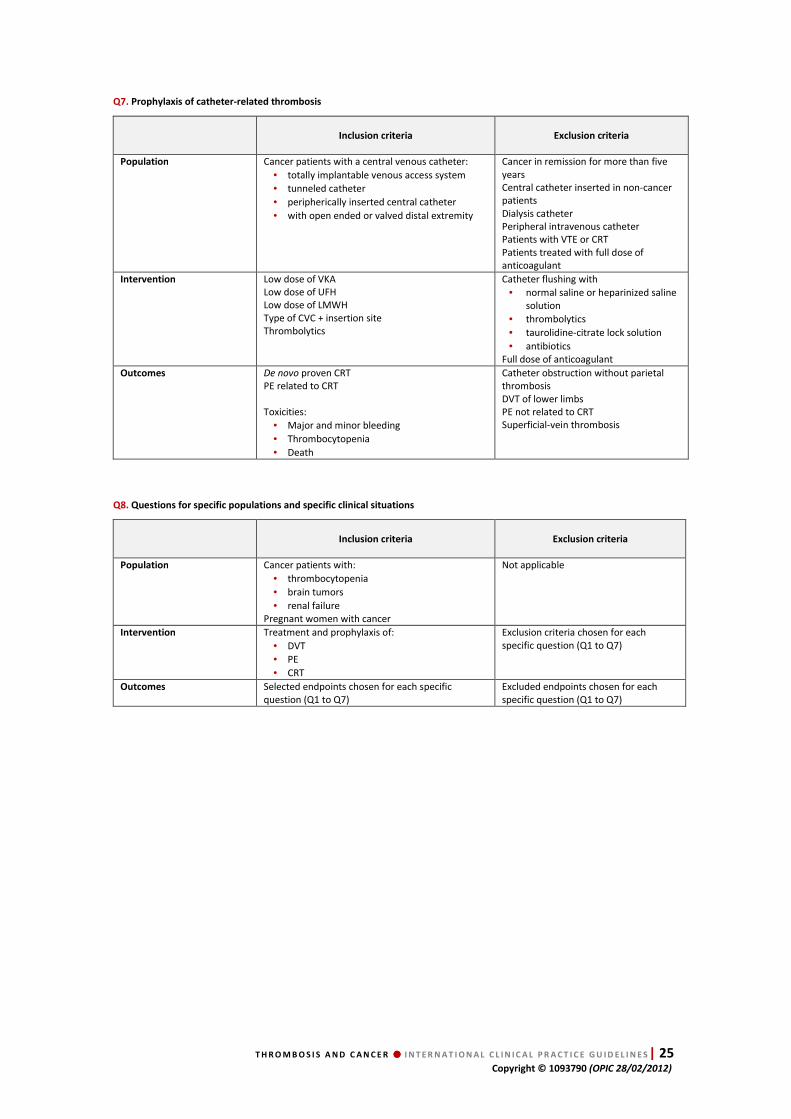
Q7. Prophylaxis of catheter-related thrombosis
Inclusion criteria Exclusion criteria
Population Cancer patients with a central venous catheter:
• totally implantable venous access system
• tunneled catheter
• peripherically inserted central catheter
• with open ended or valved distal extremity
Cancer in remission for more than five years Central catheter inserted in non-cancer patients Dialysis catheter Peripheral intravenous catheter Patients with VTE or CRT Patients treated with full dose of anticoagulant
Intervention Low dose of VKA Low dose of UFH Low dose of LMWH Type of CVC + insertion site Thrombolytics
Catheter flushing with
• normal saline or heparinized saline solution
• thrombolytics
• taurolidine-citrate lock solution
• antibiotics Full dose of anticoagulant
Outcomes De novo proven CRT PE related to CRT Toxicities:
• Major and minor bleeding
• Thrombocytopenia
• Death
Catheter obstruction without parietal thrombosis DVT of lower limbs PE not related to CRT Superficial-vein thrombosis
Q8. Questions for specific populations and specific clinical situations
Inclusion criteria Exclusion criteria
Population Cancer patients with:
• thrombocytopenia
• brain tumors
• renal failure Pregnant women with cancer
Not applicable
Intervention Treatment and prophylaxis of:
• DVT
• PE
• CRT
Exclusion criteria chosen for each specific question (Q1 to Q7)
Outcomes Selected endpoints chosen for each specific question (Q1 to Q7)
Excluded endpoints chosen for each specific question (Q1 to Q7)
26 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
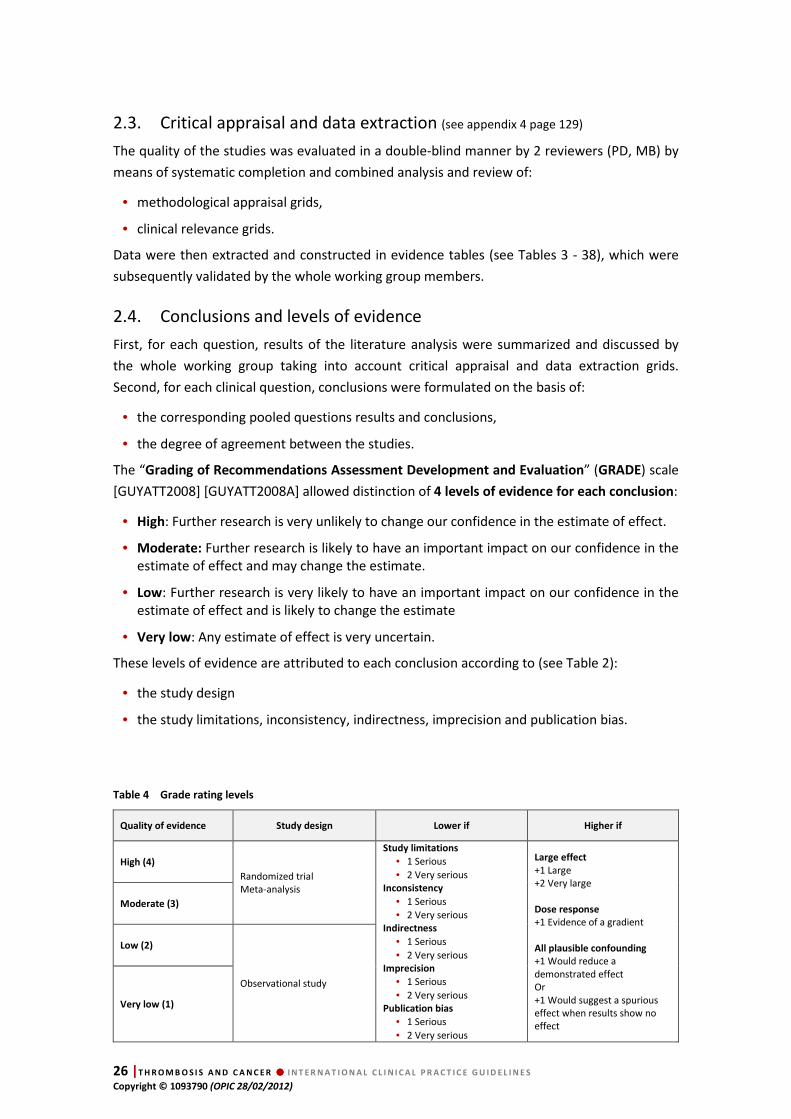
2.3. Critical appraisal and data extraction (see appendix 4 page 129)
The quality of the studies was evaluated in a double-blind manner by 2 reviewers (PD, MB) by
means of systematic completion and combined analysis and review of:
• methodological appraisal grids,
• clinical relevance grids.
Data were then extracted and constructed in evidence tables (see Tables 3 - 38), which were
subsequently validated by the whole working group members.
2.4. Conclusions and levels of evidence
First, for each question, results of the literature analysis were summarized and discussed by
the whole working group taking into account critical appraisal and data extraction grids.
Second, for each clinical question, conclusions were formulated on the basis of:
• the corresponding pooled questions results and conclusions,
• the degree of agreement between the studies.
The “Grading of Recommendations Assessment Development and Evaluation” (GRADE) scale
[GUYATT2008] [GUYATT2008A] allowed distinction of 4 levels of evidence for each conclusion:
• High: Further research is very unlikely to change our confidence in the estimate of effect.
• Moderate: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
• Low: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate
• Very low: Any estimate of effect is very uncertain.
These levels of evidence are attributed to each conclusion according to (see Table 2):
• the study design
• the study limitations, inconsistency, indirectness, imprecision and publication bias.
Table 4 Grade rating levels
Quality of evidence Study design Lower if Higher if
High (4)
Randomized trial Meta-analysis
Study limitations
• 1 Serious
• 2 Very serious Inconsistency
• 1 Serious
• 2 Very serious Indirectness
• 1 Serious
• 2 Very serious Imprecision
• 1 Serious
• 2 Very serious Publication bias
• 1 Serious
• 2 Very serious
Large effect
+1 Large +2 Very large Dose response
+1 Evidence of a gradient All plausible confounding
+1 Would reduce a demonstrated effect Or +1 Would suggest a spurious effect when results show no effect
Moderate (3)
Low (2)
Observational study
Very low (1)
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 27 Copyright © 1093790 (OPIC 28/02/2012)
2.5. Recommendations
Following the conclusions for each clinical question, recommendations were established taking
into account the following parameters:
• Conclusion level of evidence (high, moderate, low, very low): the higher the quality of the evidence, the higher the likelihood that a strong recommendation is warranted;
• Balance between desirable and undesirable effects: the larger the difference between the desirable and undesirable effects, the higher the likelihood that a strong recommendation is warranted. The smaller the net benefit and the lower certainty for that benefit, the more likely that a weak recommendation is warranted;
• Values and preferences: the more values and preferences vary, or the greater the uncertainty in values and preferences, the higher the likelihood that a weak recommendation is warranted;
• Costs (resource allocation): the higher the costs of an intervention (i.e., the greater the resources consumed), the lower the likelihood that a strong recommendation is warranted.
GRADE scale [GUYATT2008] [GUYATT2008 A] allows distinction of 2 levels for each
recommendation, corresponding to “the degree of confidence that the desirable effects of
adherence to a recommendation outweighs the undesirable effects.”
• Strong: the panel is confident that the desirable effects of adherence to a recommendation outweigh the undesirable effects.
• Weak: the panel concludes that the desirable effects of adherence to a recommendation probably outweigh the undesirable effects, but is not confident.
For previously selected questions without any clear scientific evidence or any data available
after an extensive search and analysis of the literature, the working group decided to add a
third level of recommendation, defined as “Best Clinical Practices”. Elaboration of the Best
Clinical Practices recommendation had to be based on the consensus of the international
working group experts after discussion, taking into account the professional experience and all
experts’ opinion.
2.5.1. Economic considerations
The following economic and general considerations were taken into account to elaborate the
recommendations.
• The price of a drug varies different countries and in different regions of the world.
• In the case of a strong recommendation, the benefit to the patient outweighs health economics considerations.
• In the case of a weak recommendation, health economics aspects were considered.
• Costs of anticoagulants are negligible compared with the cost of cancer treatment.

28 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
2.5.2. General considerations:
For each patient and before applying a recommendation, the working group advocates a
careful evaluation of:
• Contraindications to anticoagulation,
• Creatinine clearance,
• Risk of hepatic dysfunction ,
• Bleeding risk,
• Benefit-risk ratio of each treatment,
• Patient preferences.
2.6. Peer-review process
These guidelines were peer-reviewed in February 2012 by 43 independent experts in different
medical specialties involved in VTE management (internal medicine = 5, vascular medicine =
13, hematology = 10, oncology = 7, anticoagulation clinical nurse specialist = 2, pharmacist = 1;
pneumology = 1, anesthesiology = 1, palliative medicine = 1), working in public and private
institutions.
Reviewers were sollicited among "International Scientific Societies", "National experts",
"International patients’ associations", etc.
A grid was proposed allowing partial and general appreciation of the document via
a quantitative (quotation) and a qualitative evaluation (comments). All the comments were
examined and discussed by the members of the working group and were then integrated
in the final version of the document in April 2012. The members who took part in this
peer-review process are named in the document as reviewers (see appendix 1, page 121).
Any discrepancies in opinion between reviewers and members of the working group were
resolved by consensus during the last meeting.
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 29 Copyright © 1093790 (OPIC 28/02/2012)
1. Chapter 1.
Initial treatment of established VTE
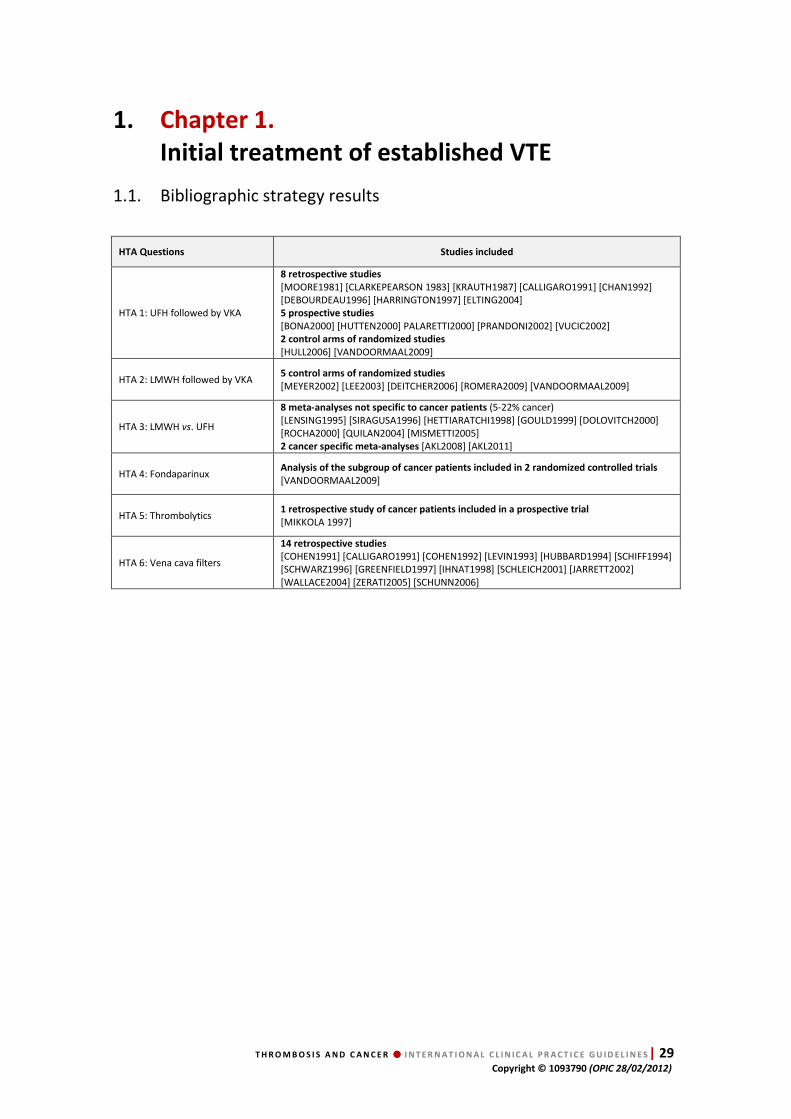
1.1. Bibliographic strategy results
HTA Questions Studies included
HTA 1: UFH followed by VKA
8 retrospective studies
[MOORE1981] [CLARKEPEARSON 1983] [KRAUTH1987] [CALLIGARO1991] [CHAN1992] [DEBOURDEAU1996] [HARRINGTON1997] [ELTING2004] 5 prospective studies
[BONA2000] [HUTTEN2000] PALARETTI2000] [PRANDONI2002] [VUCIC2002] 2 control arms of randomized studies
[HULL2006] [VANDOORMAAL2009]
HTA 2: LMWH followed by VKA 5 control arms of randomized studies
[MEYER2002] [LEE2003] [DEITCHER2006] [ROMERA2009] [VANDOORMAAL2009]
HTA 3: LMWH vs. UFH
8 meta-analyses not specific to cancer patients (5-22% cancer) [LENSING1995] [SIRAGUSA1996] [HETTIARATCHI1998] [GOULD1999] [DOLOVITCH2000] [ROCHA2000] [QUILAN2004] [MISMETTI2005] 2 cancer specific meta-analyses [AKL2008] [AKL2011]
HTA 4: Fondaparinux Analysis of the subgroup of cancer patients included in 2 randomized controlled trials
[VANDOORMAAL2009]
HTA 5: Thrombolytics 1 retrospective study of cancer patients included in a prospective trial
[MIKKOLA 1997]
HTA 6: Vena cava filters
14 retrospective studies
[COHEN1991] [CALLIGARO1991] [COHEN1992] [LEVIN1993] [HUBBARD1994] [SCHIFF1994] [SCHWARZ1996] [GREENFIELD1997] [IHNAT1998] [SCHLEICH2001] [JARRETT2002] [WALLACE2004] [ZERATI2005] [SCHUNN2006]
30 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
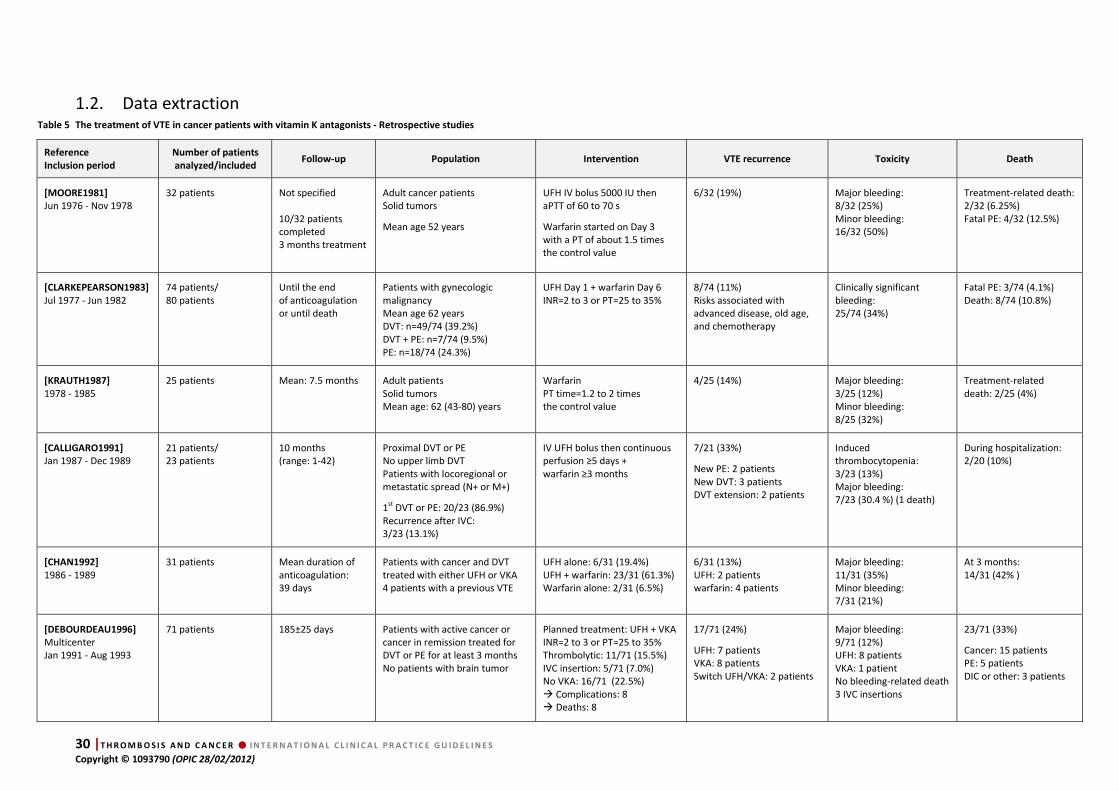
1.2. Data extraction Table 5 The treatment of VTE in cancer patients with vitamin K antagonists - Retrospective studies
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity Death
[MOORE1981]
Jun 1976 - Nov 1978 32 patients Not specified
10/32 patients completed 3 months treatment
Adult cancer patients Solid tumors
Mean age 52 years
UFH IV bolus 5000 IU then aPTT of 60 to 70 s
Warfarin started on Day 3 with a PT of about 1.5 times the control value
6/32 (19%) Major bleeding: 8/32 (25%) Minor bleeding: 16/32 (50%)
Treatment-related death: 2/32 (6.25%) Fatal PE: 4/32 (12.5%)
[CLARKEPEARSON1983]
Jul 1977 - Jun 1982 74 patients/ 80 patients
Until the end of anticoagulation or until death
Patients with gynecologic malignancy Mean age 62 years DVT: n=49/74 (39.2%) DVT + PE: n=7/74 (9.5%) PE: n=18/74 (24.3%)
UFH Day 1 + warfarin Day 6 INR=2 to 3 or PT=25 to 35%
8/74 (11%) Risks associated with advanced disease, old age, and chemotherapy
Clinically significant bleeding: 25/74 (34%)
Fatal PE: 3/74 (4.1%) Death: 8/74 (10.8%)
[KRAUTH1987]
1978 - 1985 25 patients Mean: 7.5 months Adult patients
Solid tumors Mean age: 62 (43-80) years
Warfarin PT time=1.2 to 2 times the control value
4/25 (14%) Major bleeding: 3/25 (12%) Minor bleeding: 8/25 (32%)
Treatment-related death: 2/25 (4%)
[CALLIGARO1991]
Jan 1987 - Dec 1989 21 patients/ 23 patients
10 months (range: 1-42)
Proximal DVT or PE No upper limb DVT Patients with locoregional or metastatic spread (N+ or M+)
1st DVT or PE: 20/23 (86.9%) Recurrence after IVC: 3/23 (13.1%)
IV UFH bolus then continuous perfusion ≥5 days + warfarin ≥3 months
7/21 (33%)
New PE: 2 patients New DVT: 3 patients DVT extension: 2 patients
Induced thrombocytopenia: 3/23 (13%) Major bleeding: 7/23 (30.4 %) (1 death)
During hospitalization: 2/20 (10%)
[CHAN1992]
1986 - 1989 31 patients
Mean duration of anticoagulation: 39 days
Patients with cancer and DVT treated with either UFH or VKA 4 patients with a previous VTE
UFH alone: 6/31 (19.4%) UFH + warfarin: 23/31 (61.3%) Warfarin alone: 2/31 (6.5%)
6/31 (13%) UFH: 2 patients warfarin: 4 patients
Major bleeding: 11/31 (35%) Minor bleeding: 7/31 (21%)
At 3 months: 14/31 (42% )
[DEBOURDEAU1996]
Multicenter Jan 1991 - Aug 1993
71 patients 185±25 days Patients with active cancer or cancer in remission treated for DVT or PE for at least 3 months No patients with brain tumor
Planned treatment: UFH + VKA INR=2 to 3 or PT=25 to 35% Thrombolytic: 11/71 (15.5%) IVC insertion: 5/71 (7.0%) No VKA: 16/71 (22.5%) � Complications: 8 � Deaths: 8
17/71 (24%)
UFH: 7 patients VKA: 8 patients Switch UFH/VKA: 2 patients
Major bleeding: 9/71 (12%) UFH: 8 patients VKA: 1 patient No bleeding-related death 3 IVC insertions
23/71 (33%)
Cancer: 15 patients PE: 5 patients DIC or other: 3 patients
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 31 Copyright © 1093790 (OPIC 28/02/2012)
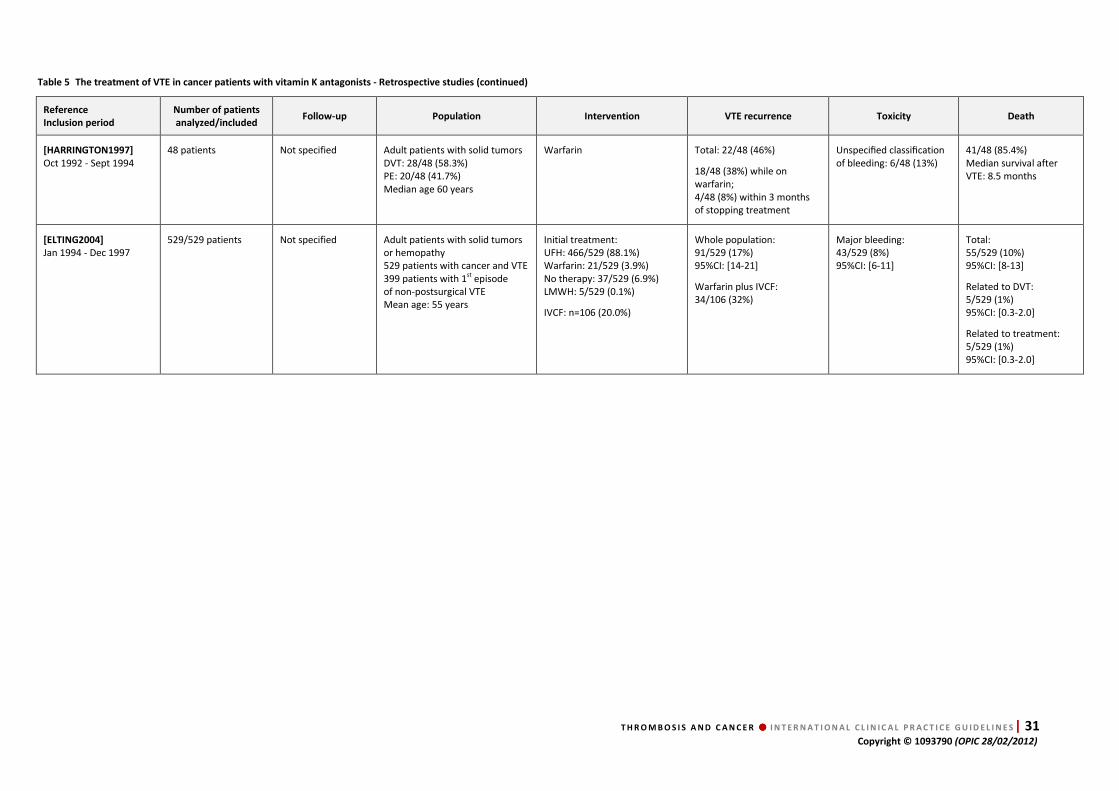
Table 5 The treatment of VTE in cancer patients with vitamin K antagonists - Retrospective studies (continued)
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity Death
[HARRINGTON1997]
Oct 1992 - Sept 1994 48 patients Not specified Adult patients with solid tumors
DVT: 28/48 (58.3%) PE: 20/48 (41.7%) Median age 60 years
Warfarin Total: 22/48 (46%)
18/48 (38%) while on warfarin; 4/48 (8%) within 3 months of stopping treatment
Unspecified classification of bleeding: 6/48 (13%)
41/48 (85.4%) Median survival after VTE: 8.5 months
[ELTING2004]
Jan 1994 - Dec 1997 529/529 patients Not specified Adult patients with solid tumors
or hemopathy 529 patients with cancer and VTE 399 patients with 1st episode of non-postsurgical VTE Mean age: 55 years
Initial treatment: UFH: 466/529 (88.1%) Warfarin: 21/529 (3.9%) No therapy: 37/529 (6.9%) LMWH: 5/529 (0.1%)
IVCF: n=106 (20.0%)
Whole population: 91/529 (17%) 95%CI: [14-21]
Warfarin plus IVCF: 34/106 (32%)
Major bleeding: 43/529 (8%) 95%CI: [6-11]
Total: 55/529 (10%) 95%CI: [8-13]
Related to DVT: 5/529 (1%) 95%CI: [0.3-2.0]
Related to treatment: 5/529 (1%) 95%CI: [0.3-2.0]
32 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
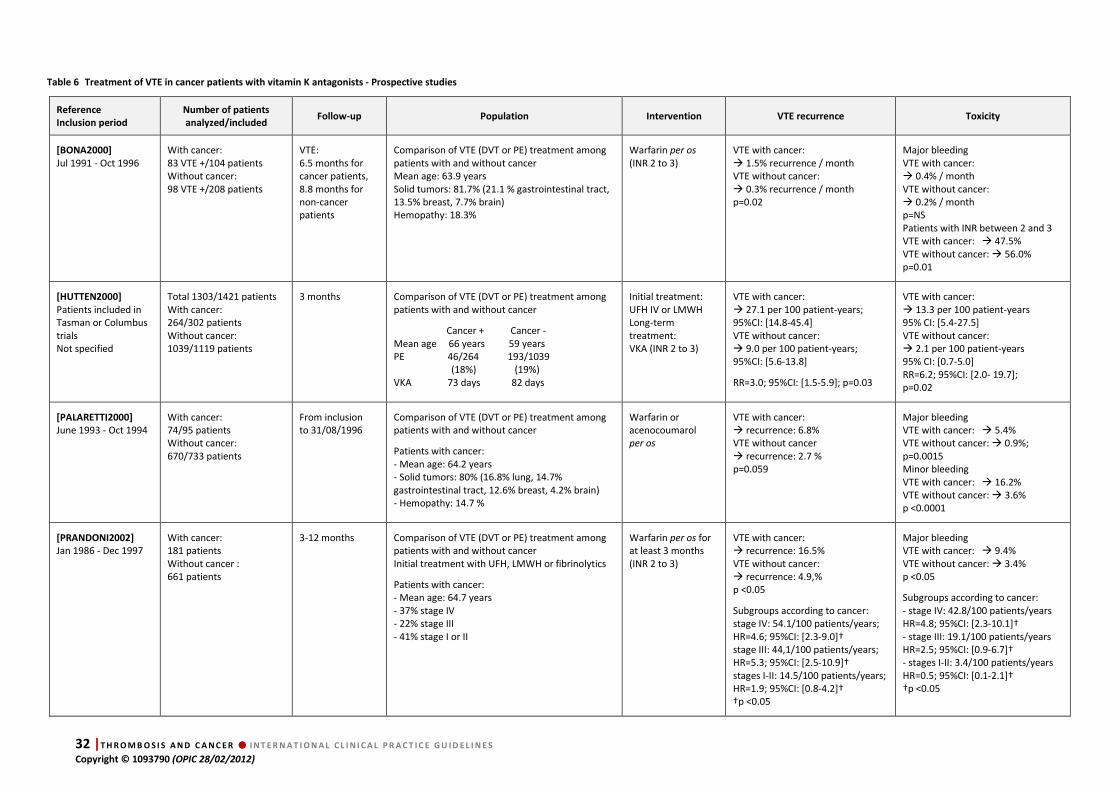
Table 6 Treatment of VTE in cancer patients with vitamin K antagonists - Prospective studies
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity
[BONA2000]
Jul 1991 - Oct 1996 With cancer: 83 VTE +/104 patients Without cancer: 98 VTE +/208 patients
VTE: 6.5 months for cancer patients, 8.8 months for non-cancer patients
Comparison of VTE (DVT or PE) treatment among patients with and without cancer Mean age: 63.9 years Solid tumors: 81.7% (21.1 % gastrointestinal tract, 13.5% breast, 7.7% brain) Hemopathy: 18.3%
Warfarin per os (INR 2 to 3)
VTE with cancer: � 1.5% recurrence / month VTE without cancer: � 0.3% recurrence / month p=0.02
Major bleeding VTE with cancer: � 0.4% / month VTE without cancer: � 0.2% / month p=NS Patients with INR between 2 and 3 VTE with cancer: � 47.5% VTE without cancer: � 56.0% p=0.01
[HUTTEN2000]
Patients included in Tasman or Columbus trials Not specified
Total 1303/1421 patients With cancer: 264/302 patients Without cancer: 1039/1119 patients
3 months Comparison of VTE (DVT or PE) treatment among patients with and without cancer
Cancer + Cancer - Mean age 66 years 59 years PE 46/264 193/1039 (18%) (19%) VKA 73 days 82 days
Initial treatment: UFH IV or LMWH Long-term treatment: VKA (INR 2 to 3)
VTE with cancer: � 27.1 per 100 patient-years; 95%CI: [14.8-45.4] VTE without cancer: � 9.0 per 100 patient-years; 95%CI: [5.6-13.8]
RR=3.0; 95%CI: [1.5-5.9]; p=0.03
VTE with cancer: � 13.3 per 100 patient-years 95% CI: [5.4-27.5] VTE without cancer: � 2.1 per 100 patient-years 95% CI: [0.7-5.0] RR=6.2; 95%CI: [2.0- 19.7]; p=0.02
[PALARETTI2000]
June 1993 - Oct 1994 With cancer: 74/95 patients Without cancer: 670/733 patients
From inclusion to 31/08/1996
Comparison of VTE (DVT or PE) treatment among patients with and without cancer
Patients with cancer: - Mean age: 64.2 years - Solid tumors: 80% (16.8% lung, 14.7% gastrointestinal tract, 12.6% breast, 4.2% brain) - Hemopathy: 14.7 %
Warfarin or acenocoumarol per os
VTE with cancer: � recurrence: 6.8% VTE without cancer � recurrence: 2.7 % p=0.059
Major bleeding VTE with cancer: � 5.4% VTE without cancer: � 0.9%; p=0.0015 Minor bleeding VTE with cancer: � 16.2% VTE without cancer: � 3.6% p <0.0001
[PRANDONI2002]
Jan 1986 - Dec 1997 With cancer: 181 patients Without cancer : 661 patients
3-12 months Comparison of VTE (DVT or PE) treatment among patients with and without cancer Initial treatment with UFH, LMWH or fibrinolytics
Patients with cancer: - Mean age: 64.7 years - 37% stage IV - 22% stage III - 41% stage I or II
Warfarin per os for at least 3 months (INR 2 to 3)
VTE with cancer: � recurrence: 16.5% VTE without cancer: � recurrence: 4.9,% p <0.05
Subgroups according to cancer: stage IV: 54.1/100 patients/years; HR=4.6; 95%CI: [2.3-9.0]† stage III: 44,1/100 patients/years; HR=5.3; 95%CI: [2.5-10.9]† stages I-II: 14.5/100 patients/years; HR=1.9; 95%CI: [0.8-4.2]† †p <0.05
Major bleeding VTE with cancer: � 9.4% VTE without cancer: � 3.4% p <0.05
Subgroups according to cancer: - stage IV: 42.8/100 patients/years HR=4.8; 95%CI: [2.3-10.1]† - stage III: 19.1/100 patients/years HR=2.5; 95%CI: [0.9-6.7]† - stages I-II: 3.4/100 patients/years HR=0.5; 95%CI: [0.1-2.1]† †p <0.05
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 33 Copyright © 1093790 (OPIC 28/02/2012)
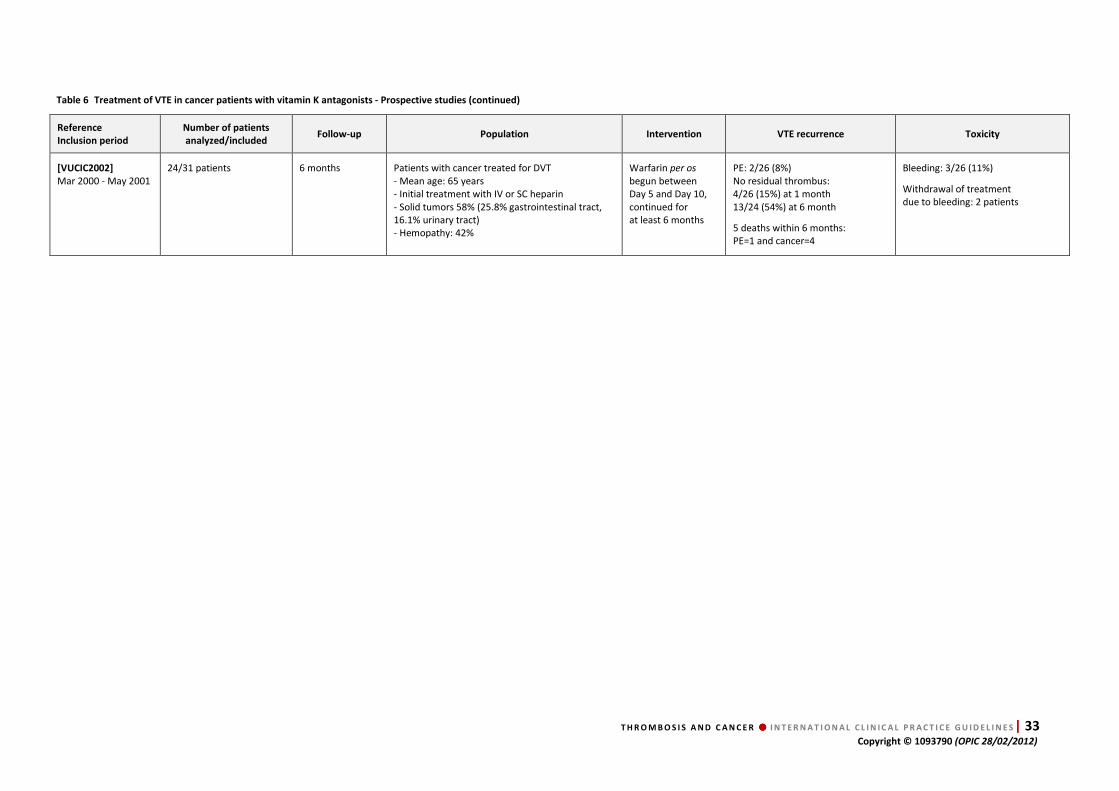
Table 6 Treatment of VTE in cancer patients with vitamin K antagonists - Prospective studies (continued)
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity
[VUCIC2002]
Mar 2000 - May 2001 24/31 patients 6 months Patients with cancer treated for DVT
- Mean age: 65 years - Initial treatment with IV or SC heparin - Solid tumors 58% (25.8% gastrointestinal tract, 16.1% urinary tract) - Hemopathy: 42%
Warfarin per os begun between Day 5 and Day 10, continued for at least 6 months
PE: 2/26 (8%) No residual thrombus: 4/26 (15%) at 1 month 13/24 (54%) at 6 month
5 deaths within 6 months: PE=1 and cancer=4
Bleeding: 3/26 (11%)
Withdrawal of treatment due to bleeding: 2 patients
34 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
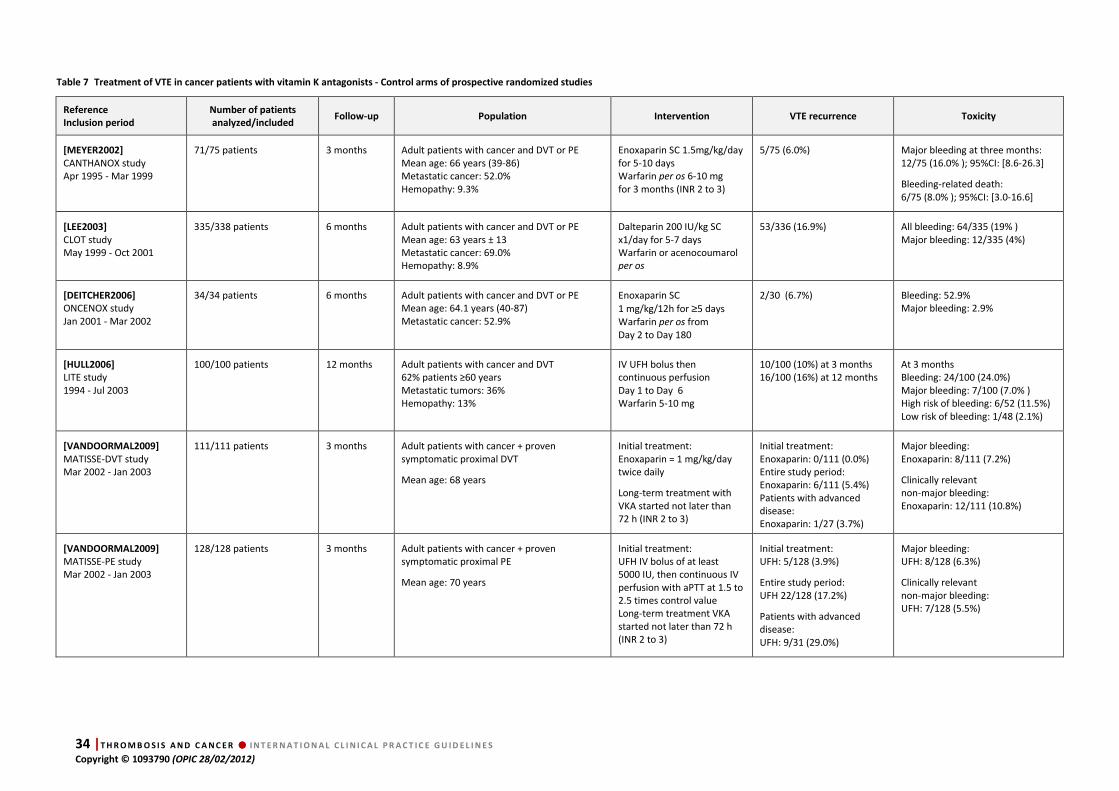
Table 7 Treatment of VTE in cancer patients with vitamin K antagonists - Control arms of prospective randomized studies
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity
[MEYER2002]
CANTHANOX study Apr 1995 - Mar 1999
71/75 patients 3 months Adult patients with cancer and DVT or PE Mean age: 66 years (39-86) Metastatic cancer: 52.0% Hemopathy: 9.3%
Enoxaparin SC 1.5mg/kg/day for 5-10 days Warfarin per os 6-10 mg for 3 months (INR 2 to 3)
5/75 (6.0%) Major bleeding at three months: 12/75 (16.0% ); 95%CI: [8.6-26.3]
Bleeding-related death: 6/75 (8.0% ); 95%CI: [3.0-16.6]
[LEE2003]
CLOT study May 1999 - Oct 2001
335/338 patients 6 months Adult patients with cancer and DVT or PE Mean age: 63 years ± 13 Metastatic cancer: 69.0% Hemopathy: 8.9%
Dalteparin 200 IU/kg SC x1/day for 5-7 days Warfarin or acenocoumarol per os
53/336 (16.9%)
All bleeding: 64/335 (19% ) Major bleeding: 12/335 (4%)
[DEITCHER2006]
ONCENOX study Jan 2001 - Mar 2002
34/34 patients 6 months Adult patients with cancer and DVT or PE Mean age: 64.1 years (40-87) Metastatic cancer: 52.9%
Enoxaparin SC
1 mg/kg/12h for ≥5 days Warfarin per os from Day 2 to Day 180
2/30 (6.7%) Bleeding: 52.9% Major bleeding: 2.9%
[HULL2006]
LITE study 1994 - Jul 2003
100/100 patients 12 months Adult patients with cancer and DVT 62% patients ≥60 years Metastatic tumors: 36% Hemopathy: 13%
IV UFH bolus then continuous perfusion Day 1 to Day 6 Warfarin 5-10 mg
10/100 (10%) at 3 months 16/100 (16%) at 12 months
At 3 months Bleeding: 24/100 (24.0%) Major bleeding: 7/100 (7.0% ) High risk of bleeding: 6/52 (11.5%) Low risk of bleeding: 1/48 (2.1%)
[VANDOORMAL2009]
MATISSE-DVT study Mar 2002 - Jan 2003
111/111 patients 3 months Adult patients with cancer + proven symptomatic proximal DVT
Mean age: 68 years
Initial treatment: Enoxaparin = 1 mg/kg/day twice daily
Long-term treatment with VKA started not later than 72 h (INR 2 to 3)
Initial treatment: Enoxaparin: 0/111 (0.0%) Entire study period: Enoxaparin: 6/111 (5.4%) Patients with advanced disease: Enoxaparin: 1/27 (3.7%)
Major bleeding: Enoxaparin: 8/111 (7.2%)
Clinically relevant non-major bleeding: Enoxaparin: 12/111 (10.8%)
[VANDOORMAL2009]
MATISSE-PE study Mar 2002 - Jan 2003
128/128 patients 3 months Adult patients with cancer + proven symptomatic proximal PE
Mean age: 70 years
Initial treatment: UFH IV bolus of at least 5000 IU, then continuous IV perfusion with aPTT at 1.5 to 2.5 times control value Long-term treatment VKA started not later than 72 h (INR 2 to 3)
Initial treatment: UFH: 5/128 (3.9%)
Entire study period: UFH 22/128 (17.2%)
Patients with advanced disease: UFH: 9/31 (29.0%)
Major bleeding: UFH: 8/128 (6.3%)
Clinically relevant non-major bleeding: UFH: 7/128 (5.5%)

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 35 Copyright © 1093790 (OPIC 28/02/2012)
Table 7 Treatment of VTE in cancer patients with vitamin K antagonists - Control arms of prospective randomized studies (continued)
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity
[ROMERA2009]
Jan 2002 - Jan 2005
70/70 patients 12 months Patients with cancer and proven DVT treated with either long-term use of tinzaparin alone or acenocoumarol + tinzaparin
Tinzaparin 175 IU/kg/day then acenocoumarol 3 mg (INR 2 to 3) for 6 months
VTE recurrence at 6 months Arm B: 3/34 (9.1%)
VTE recurrence at 12 months Arm B: 7/34 (20.6%)
No data for major bleeding in cancer patients
[VANDOORMAAL2010]
VANGOGH-DVT study May 2003 - Nov 2004
Month 3: 138/201 patients Month6: 130/201 patients
92 days Patients with active cancer and confirmed DVT and no sign of PE Mean age: 67 years Men: 52%
LMWH or UFH then VKA for 3 or 6 months of treatment according to the physician's judgment ; 92% of patients were treated for 6 months
VTE recurrence at 3 months VKA: 10/138 (7.2%)
VTE recurrence at 6 months VKA: 10/130 (7.7%)
All clinically relevant bleedings Month 3: VKA: 18/138 (13.0%) Month 6: VKA: 18/130 (16.2%)
Major bleeding Month 3: VKA: 2/138 (1.4%) Month 6: VKA: 5/130 (3.8%)
36 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
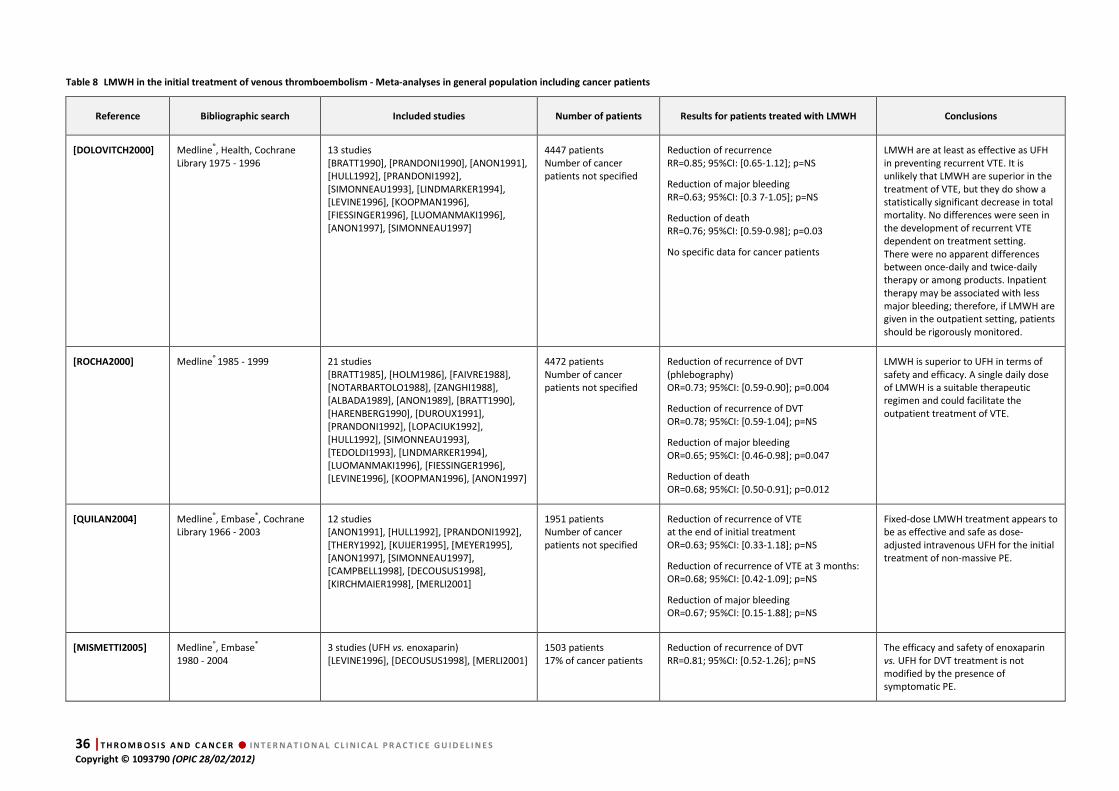
Table 8 LMWH in the initial treatment of venous thromboembolism - Meta-analyses in general population including cancer patients
Reference Bibliographic search Included studies Number of patients Results for patients treated with LMWH Conclusions
[DOLOVITCH2000] Medline®, Health, Cochrane Library 1975 - 1996
13 studies [BRATT1990], [PRANDONI1990], [ANON1991], [HULL1992], [PRANDONI1992], [SIMONNEAU1993], [LINDMARKER1994], [LEVINE1996], [KOOPMAN1996], [FIESSINGER1996], [LUOMANMAKI1996], [ANON1997], [SIMONNEAU1997]
4447 patients Number of cancer patients not specified
Reduction of recurrence RR=0.85; 95%CI: [0.65-1.12]; p=NS
Reduction of major bleeding RR=0.63; 95%CI: [0.3 7-1.05]; p=NS
Reduction of death RR=0.76; 95%CI: [0.59-0.98]; p=0.03
No specific data for cancer patients
LMWH are at least as effective as UFH in preventing recurrent VTE. It is unlikely that LMWH are superior in the treatment of VTE, but they do show a statistically significant decrease in total mortality. No differences were seen in the development of recurrent VTE dependent on treatment setting. There were no apparent differences between once-daily and twice-daily therapy or among products. Inpatient therapy may be associated with less major bleeding; therefore, if LMWH are given in the outpatient setting, patients should be rigorously monitored.
[ROCHA2000] Medline® 1985 - 1999 21 studies [BRATT1985], [HOLM1986], [FAIVRE1988], [NOTARBARTOLO1988], [ZANGHI1988], [ALBADA1989], [ANON1989], [BRATT1990], [HARENBERG1990], [DUROUX1991], [PRANDONI1992], [LOPACIUK1992], [HULL1992], [SIMONNEAU1993], [TEDOLDI1993], [LINDMARKER1994], [LUOMANMAKI1996], [FIESSINGER1996], [LEVINE1996], [KOOPMAN1996], [ANON1997]
4472 patients Number of cancer patients not specified
Reduction of recurrence of DVT (phlebography) OR=0.73; 95%CI: [0.59-0.90]; p=0.004
Reduction of recurrence of DVT OR=0.78; 95%CI: [0.59-1.04]; p=NS
Reduction of major bleeding OR=0.65; 95%CI: [0.46-0.98]; p=0.047
Reduction of death OR=0.68; 95%CI: [0.50-0.91]; p=0.012
LMWH is superior to UFH in terms of safety and efficacy. A single daily dose of LMWH is a suitable therapeutic regimen and could facilitate the outpatient treatment of VTE.
[QUILAN2004] Medline®, Embase®, Cochrane Library 1966 - 2003
12 studies [ANON1991], [HULL1992], [PRANDONI1992], [THERY1992], [KUIJER1995], [MEYER1995], [ANON1997], [SIMONNEAU1997], [CAMPBELL1998], [DECOUSUS1998], [KIRCHMAIER1998], [MERLI2001]
1951 patients Number of cancer patients not specified
Reduction of recurrence of VTE at the end of initial treatment OR=0.63; 95%CI: [0.33-1.18]; p=NS
Reduction of recurrence of VTE at 3 months: OR=0.68; 95%CI: [0.42-1.09]; p=NS
Reduction of major bleeding OR=0.67; 95%CI: [0.15-1.88]; p=NS
Fixed-dose LMWH treatment appears to be as effective and safe as dose-adjusted intravenous UFH for the initial treatment of non-massive PE.
[MISMETTI2005] Medline®, Embase® 1980 - 2004
3 studies (UFH vs. enoxaparin) [LEVINE1996], [DECOUSUS1998], [MERLI2001]
1503 patients 17% of cancer patients
Reduction of recurrence of DVT RR=0.81; 95%CI: [0.52-1.26]; p=NS
The efficacy and safety of enoxaparin vs. UFH for DVT treatment is not modified by the presence of symptomatic PE.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 37 Copyright © 1093790 (OPIC 28/02/2012)
Table 8 LMWH in the initial treatment of venous thromboembolism - Meta-analyses in general population including cancer patients (continued)
Reference Bibliographic search Included studies Number of patients Results for patients treated with LMWH Conclusions
[LENSING1995] Medline®, current contents 1984 - 1994
10 studies [BRATT1985], [HOLM1986], [FAIVRE1987], [BRATT1990], [DUROUX1991], [PRANDONI1992], [LOPACIUK1992], [HULL1992], [SIMONNEAU1993], [LINDMARKER1994]
1512 patients 12% of cancer patients
Reduction of VTE recurrence (DVT or PE) 53%; 95%CI: [18-73]; p <0.01
Reduction of major bleeding 68%; 95%CI: [31-85]; p <0.05
Reduction of death 64%; 95%CI: [24-83]; p <0.01
LMWH administered subcutaneously in fixed doses adjusted for body weight and without laboratory monitoring are more effective and safer than adjusted-dose standard heparin.
[SIRAGUSA1996] Medline®, Embase® 1980 - 1994
13 studies [BRATT1985], [HOLM1986], [FAIVRE1988], [ALBADA1989], [BRATT1990], [HANDELAND1990], [DUROUX1991], [THERY1992], [LOPACIUK1992], [HULL1992], [PRANDONI1992], [LINDMARKER1993], [SIMONNEAU1993]
1723 patients 9% of cancer patients
At day 15 reduction of VTE recurrence RR=0.24; 95%CI: [0.06-0.80]; p=0.02
At day 90 reduction of VTE recurrence RR=0.39; 95%CI: [0.30-0.80]; p=0.006
Reduction of major bleeding RR=0.42; 95%CI: [0.20-0.90]; p=0.01
Reduction of death Global population: RR=0.51; 95%CI: [0.20-0.90]; p=0.01 Patients with cancer: RR=0.33; 95%CI: [0.10-0.80]; p=0.01
LMWH are likely to be more effective than UFH in preventing recurrent VTE, to produce less major bleeding, and to be associated with a lower mortality rate, particularly in the subgroup of patients with cancer.
[HETTIARATCHI1998] Medline®, Embase®, current contents Search period not specified
13 studies [KOOPMAN1996], [LEVINE1996], [HULL1992], [ANON1997], [SIMONNEAU1997], [FAIVRE1988], [DUROUX1991], [PRANDONI1992], [LOPACIUK1992], [SIMONNEAU1993], [DECOUSUS1998], [LINDMARKER1994] [FIESSINGER1996]
4019 patients 6% to 23% of cancer patients depending on the studies
Reduction of VTE recurrence at 3 months OR=0.77; 95%CI: [0.56-1.04]; p=NS
Reduction of major bleeding OR=0.60; 95%CI: [0.38-0.95]; p <0.05
Reduction of death OR=0.72; 95%CI: [0.55-0.96]; p <0.05 Published results do not differ with the rate of cancer patients included in the studies (p >0.2)
The risk of recurrence of VTE, major bleeding and mortality was lower with LMWH compared with UFH. The proportion of cancer patients in these studies had a statistically significant effect on the incidence of recurrent VTE and mortality, but no influence on the estimated treatment effects of LMWH. LMWH is effective and safe in the initial treatment of VTE.
[GOULD1999] Medline® + individual search (non-indexed journals, abstracts, proceedings, etc.), Jan 1985 - Sept 1997
11 studies [DUROUX1991], [HULL1992], [PRANDONI1992], [LOPACIUK1992], [SIMONNEAU1993], [LINDMARKER1994], [LEVINE1996], [KOOPMAN1996], [FIESSINGER1996], [LUOMANMAKI1996], [ANON1997]
3674 patients 5% to 22% of cancer patients depending on the studies
Reduction of VTE recurrence RR=0.85; 95%CI: [0.63-1.14]; p=NS
Reduction of major bleeding RR=0.57; 95%CI: [0.33-0.99]; p <0.05
Reduction of death Global population: OR=0.71; 95%CI: [0.53-0.94]; p <0,05 Patients with cancer: OR=0.57; 95%CI: [0.31-1.03]; p=NS
LMWH treatment reduces mortality rates after acute deep VTE. These drugs appear to be as safe as UFH with respect to major bleeding complications and to be as effective in preventing VTE recurrences.
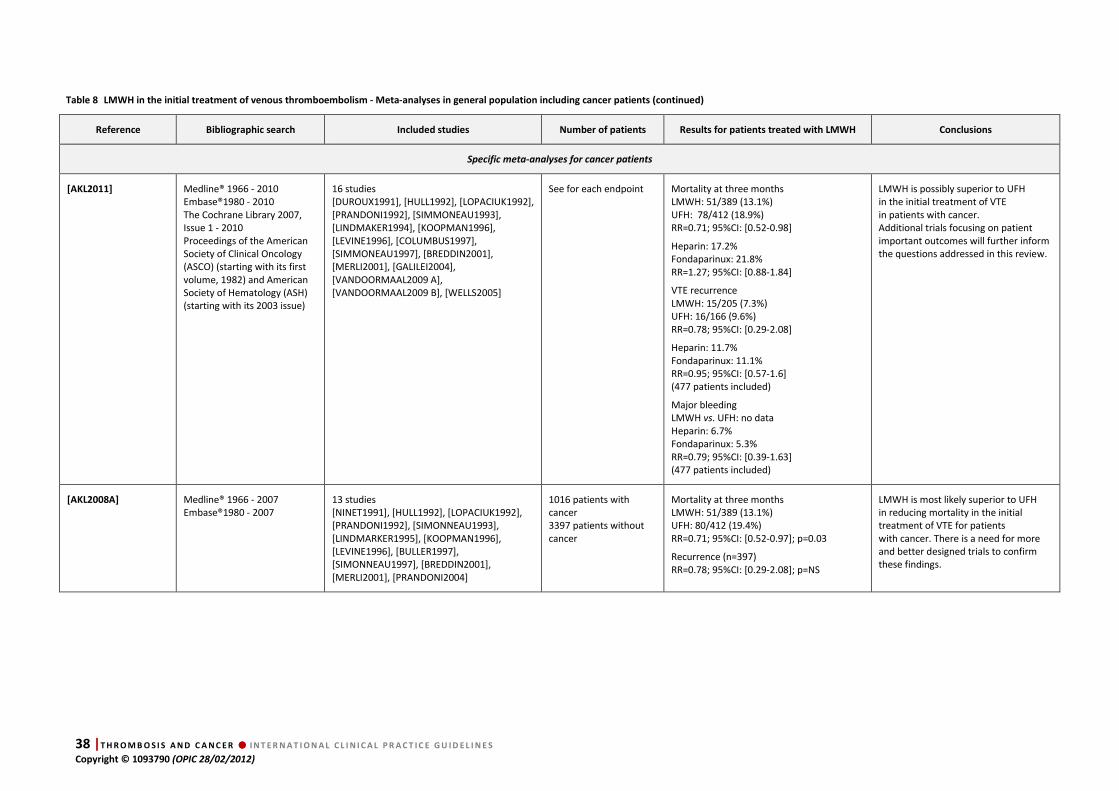
38 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 8 LMWH in the initial treatment of venous thromboembolism - Meta-analyses in general population including cancer patients (continued)
Reference Bibliographic search Included studies Number of patients Results for patients treated with LMWH Conclusions
Specific meta-analyses for cancer patients
[AKL2011] Medline® 1966 - 2010 Embase®1980 - 2010 The Cochrane Library 2007, Issue 1 - 2010 Proceedings of the American Society of Clinical Oncology (ASCO) (starting with its first volume, 1982) and American Society of Hematology (ASH) (starting with its 2003 issue)
16 studies [DUROUX1991], [HULL1992], [LOPACIUK1992], [PRANDONI1992], [SIMMONEAU1993], [LINDMAKER1994], [KOOPMAN1996], [LEVINE1996], [COLUMBUS1997], [SIMMONEAU1997], [BREDDIN2001], [MERLI2001], [GALILEI2004], [VANDOORMAAL2009 A], [VANDOORMAAL2009 B], [WELLS2005]
See for each endpoint Mortality at three months LMWH: 51/389 (13.1%) UFH: 78/412 (18.9%) RR=0.71; 95%CI: [0.52-0.98]
Heparin: 17.2% Fondaparinux: 21.8% RR=1.27; 95%CI: [0.88-1.84]
VTE recurrence LMWH: 15/205 (7.3%) UFH: 16/166 (9.6%) RR=0.78; 95%CI: [0.29-2.08]
Heparin: 11.7% Fondaparinux: 11.1% RR=0.95; 95%CI: [0.57-1.6] (477 patients included)
Major bleeding LMWH vs. UFH: no data Heparin: 6.7% Fondaparinux: 5.3% RR=0.79; 95%CI: [0.39-1.63] (477 patients included)
LMWH is possibly superior to UFH in the initial treatment of VTE in patients with cancer. Additional trials focusing on patient important outcomes will further inform the questions addressed in this review.
[AKL2008A] Medline® 1966 - 2007 Embase®1980 - 2007
13 studies [NINET1991], [HULL1992], [LOPACIUK1992], [PRANDONI1992], [SIMONNEAU1993], [LINDMARKER1995], [KOOPMAN1996], [LEVINE1996], [BULLER1997], [SIMONNEAU1997], [BREDDIN2001], [MERLI2001], [PRANDONI2004]
1016 patients with cancer 3397 patients without cancer
Mortality at three months LMWH: 51/389 (13.1%) UFH: 80/412 (19.4%) RR=0.71; 95%CI: [0.52-0.97]; p=0.03
Recurrence (n=397) RR=0.78; 95%CI: [0.29-2.08]; p=NS
LMWH is most likely superior to UFH in reducing mortality in the initial treatment of VTE for patients with cancer. There is a need for more and better designed trials to confirm these findings.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 39 Copyright © 1093790 (OPIC 28/02/2012)
Table 9 Thrombolytic therapy
References
Design
Inclusion period Number of patients Follow-up Population Intervention VTE recurrence Toxicity Survival
[MIKKOLA1997]
Retrospective study of cancer patients included in 5 randomized trials 1985 - 1994
57 patients 14 days Cancer patients with PE Thrombolytic treatment with recombinant t-PA or urokinase followed by IV UFH (adjusted dosages for an aPTT between 60 and 90 seconds)
Within the first 14 days: 3/57 (6%)
Major bleeding (within the first 72 h): 12%
During hospitalization: 5/57 (9%)

40 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 10 Vena cava filters
References
Design
Inclusion period
Number of patients
included/evaluated Included population Intervention Follow-up Recurrence Toxicity Survival
[COHEN1991]
Monocenter retrospective study 1986 - 1989
29 patients Cancer patients treated for DVT or PE
Anticoagulant: n=11 - Mean age: 60 years (range 41-76); - Metastatic: 8/11 - Lung: 18%; gastrointestinal tract: 18%
Filter (n=18): - Mean age: 62 years (range 47-74); - - - Metastatic: 18//18 - Lung: 23%; gastrointestinal tract: 30%
Arm A : Vena cava filter insertion (Greenfield filter)
Arm B : anticoagulation (IV UFH 10-15 IU/kg for 7-10 days, then warfarin)
7 months Arm A: 0% (0/18) Arm B: 9% (1/11)
Bleeding Arm A: 0% (0/18) Arm B: 27% (3/11)
Treatment related mortality Arm A: 0% (0/18) Arm B: 18 % (2/11) p=NS
[CALLIGARO1991]
Retrospective cohort Jan 1987 - Dec 1989
IVCF: 10/10 patients Anticoagulant: 23/21 patients
Proximal DVT or PE No upper limb DVT
Patients with locoregional or metastatic spread (N+ or M+)
Arm A: IV UFH bolus, then continuous perfusion for ≥5 days + warfarin for ≥3 months
Arm B: IVCF
10 months (1-42)
DVT Arm A: 7/21 (33%) Arm B: 3/10 (30%)
Arm A: Induced thrombocytopenia 3/23 (13%) Major bleeding 7/23 (30.4%) (1 death) Arm B: 1 guide wire-induced arrhythmia
During hospitalization Arm A: 10% (2/20) Arm B: 10% (1/10)
[COHEN1992]
Monocenter retrospective study 1985 - 1990
41 patients Cancer patients treated for DVT or PE
Metastatic: 56% Lung: 19%; gastrointestinal tract: 24%; urinary tract: 19%
Vena cava filter insertion 6.4 months PE: 2.4 % (1/41) IVCF-related complications: 4.8% (2/41)
1 death due to PE recurrence
[LEVIN1993]
Multicenter retrospective study 1977 - 1991
49/42 patients Patients with brain tumor or brain metastasis and proven DVT or PE
IVCF insertion: n=42 Warfarin: n=5 Inferior vena cava interruption: n=1 No treatment: n=1
Unspecified IVCF PE: 11.9% (5/42) DVT: 21.4% (9/42)
IVCF-related insertion complications: 3/42 (7%) Inferior vena cava or filter thrombosis: 11/42 (26.2%)
Anticoagulant treatment: no major bleeding
Unspecified
[HUBBARD1994]
Monocenter retrospective study Aug 1984 - Mar 1989
31 patients Patients with metastatic cancer and poor performans status mean age: 58 years (range 18-77) 32% PE; 26% inferior vena cava thrombosis Gastrointestinal tract: 54.8%; Prostate: 9.7%
IV UFH, then vena cava filter insertion (Bird's nest inferior vena cava filter)
31.8 patient-years
PE: 0% Filter thrombosis: 19% (6/31)
Bleeding: 0%
Lower limb edema: 26% (8/31)
No further treatment with UFH or VKA
Unspecified
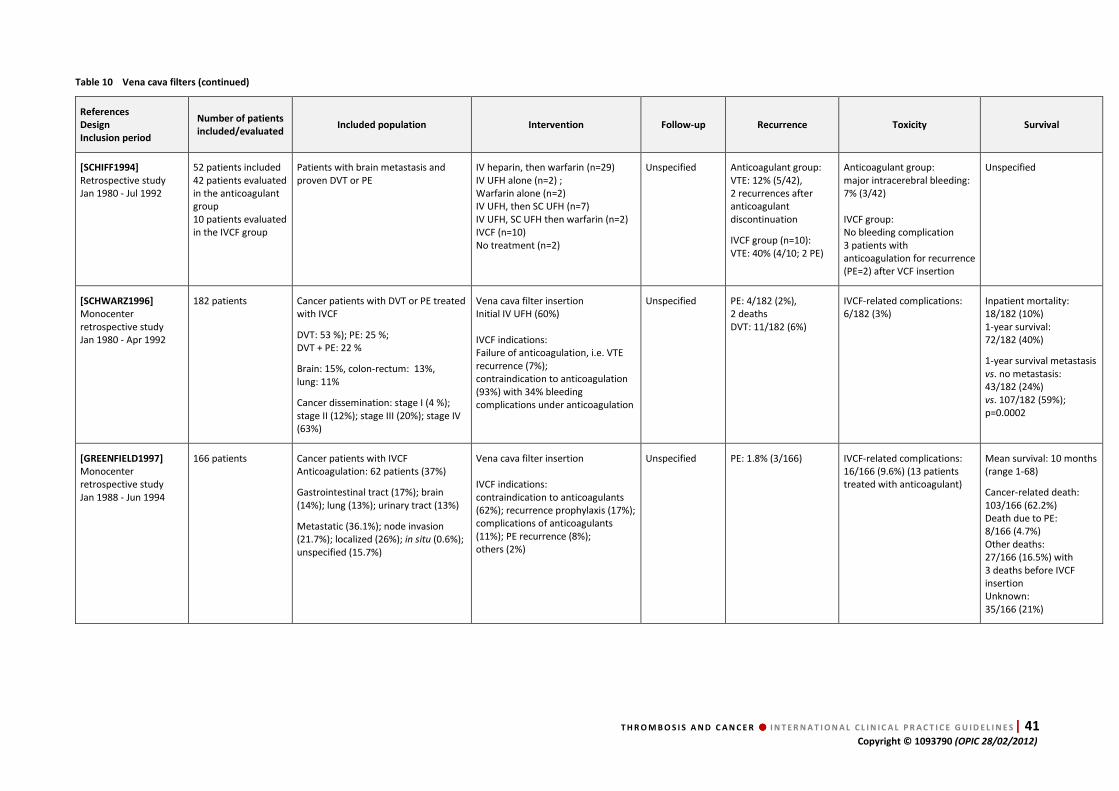
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 41 Copyright © 1093790 (OPIC 28/02/2012)
Table 10 Vena cava filters (continued)
References
Design
Inclusion period
Number of patients
included/evaluated Included population Intervention Follow-up Recurrence Toxicity Survival
[SCHIFF1994]
Retrospective study Jan 1980 - Jul 1992
52 patients included 42 patients evaluated in the anticoagulant group 10 patients evaluated in the IVCF group
Patients with brain metastasis and proven DVT or PE
IV heparin, then warfarin (n=29) IV UFH alone (n=2) ; Warfarin alone (n=2) IV UFH, then SC UFH (n=7) IV UFH, SC UFH then warfarin (n=2) IVCF (n=10) No treatment (n=2)
Unspecified Anticoagulant group: VTE: 12% (5/42), 2 recurrences after anticoagulant discontinuation
IVCF group (n=10): VTE: 40% (4/10; 2 PE)
Anticoagulant group: major intracerebral bleeding: 7% (3/42) IVCF group: No bleeding complication 3 patients with anticoagulation for recurrence (PE=2) after VCF insertion
Unspecified
[SCHWARZ1996]
Monocenter retrospective study Jan 1980 - Apr 1992
182 patients Cancer patients with DVT or PE treated with IVCF
DVT: 53 %); PE: 25 %; DVT + PE: 22 %
Brain: 15%, colon-rectum: 13%, lung: 11%
Cancer dissemination: stage I (4 %); stage II (12%); stage III (20%); stage IV (63%)
Vena cava filter insertion Initial IV UFH (60%) IVCF indications: Failure of anticoagulation, i.e. VTE recurrence (7%); contraindication to anticoagulation (93%) with 34% bleeding complications under anticoagulation
Unspecified PE: 4/182 (2%), 2 deaths DVT: 11/182 (6%)
IVCF-related complications: 6/182 (3%)
Inpatient mortality: 18/182 (10%) 1-year survival: 72/182 (40%)
1-year survival metastasis vs. no metastasis: 43/182 (24%) vs. 107/182 (59%); p=0.0002
[GREENFIELD1997]
Monocenter retrospective study Jan 1988 - Jun 1994
166 patients Cancer patients with IVCF Anticoagulation: 62 patients (37%)
Gastrointestinal tract (17%); brain (14%); lung (13%); urinary tract (13%)
Metastatic (36.1%); node invasion (21.7%); localized (26%); in situ (0.6%); unspecified (15.7%)
Vena cava filter insertion IVCF indications: contraindication to anticoagulants (62%); recurrence prophylaxis (17%); complications of anticoagulants (11%); PE recurrence (8%); others (2%)
Unspecified PE: 1.8% (3/166) IVCF-related complications: 16/166 (9.6%) (13 patients treated with anticoagulant)
Mean survival: 10 months (range 1-68)
Cancer-related death: 103/166 (62.2%) Death due to PE: 8/166 (4.7%) Other deaths: 27/166 (16.5%) with 3 deaths before IVCF insertion Unknown: 35/166 (21%)
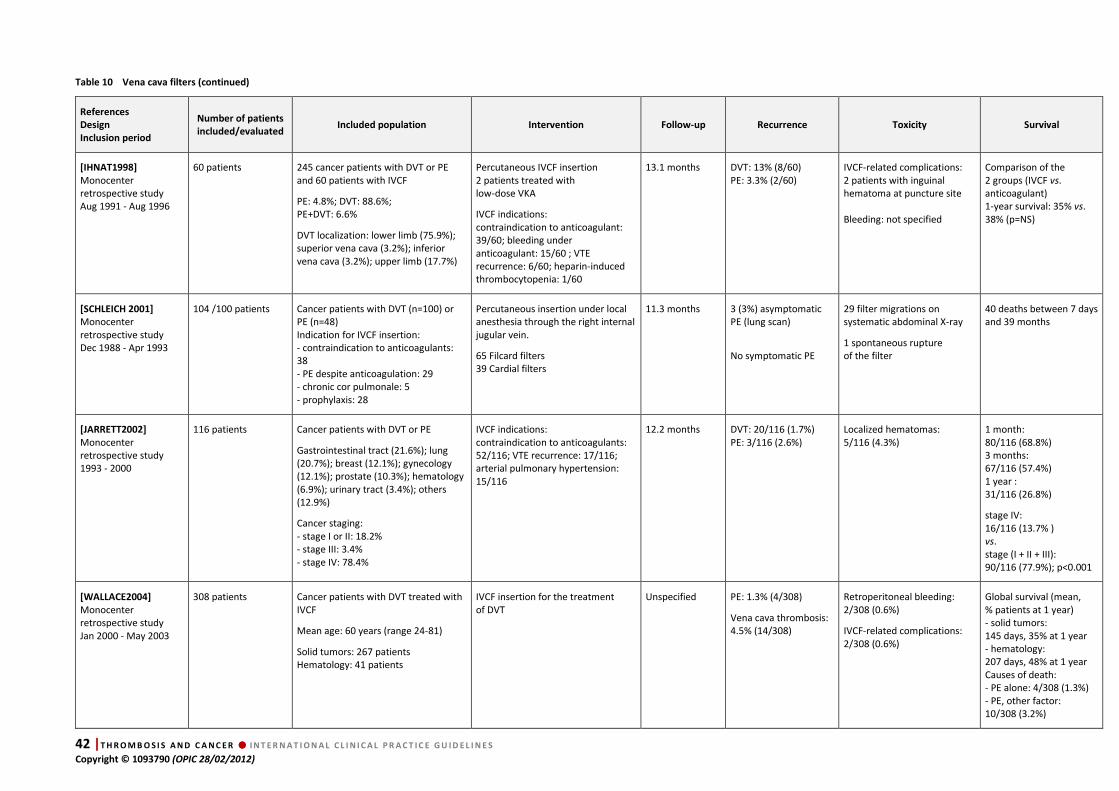
42 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 10 Vena cava filters (continued)
References
Design
Inclusion period
Number of patients
included/evaluated Included population Intervention Follow-up Recurrence Toxicity Survival
[IHNAT1998]
Monocenter retrospective study Aug 1991 - Aug 1996
60 patients
245 cancer patients with DVT or PE and 60 patients with IVCF
PE: 4.8%; DVT: 88.6%; PE+DVT: 6.6%
DVT localization: lower limb (75.9%); superior vena cava (3.2%); inferior vena cava (3.2%); upper limb (17.7%)
Percutaneous IVCF insertion 2 patients treated with low-dose VKA
IVCF indications: contraindication to anticoagulant: 39/60; bleeding under anticoagulant: 15/60 ; VTE recurrence: 6/60; heparin-induced thrombocytopenia: 1/60
13.1 months DVT: 13% (8/60) PE: 3.3% (2/60)
IVCF-related complications: 2 patients with inguinal hematoma at puncture site Bleeding: not specified
Comparison of the 2 groups (IVCF vs. anticoagulant) 1-year survival: 35% vs. 38% (p=NS)
[SCHLEICH 2001]
Monocenter retrospective study Dec 1988 - Apr 1993
104 /100 patients Cancer patients with DVT (n=100) or PE (n=48) Indication for IVCF insertion: - contraindication to anticoagulants: 38 - PE despite anticoagulation: 29 - chronic cor pulmonale: 5 - prophylaxis: 28
Percutaneous insertion under local anesthesia through the right internal jugular vein.
65 Filcard filters 39 Cardial filters
11.3 months 3 (3%) asymptomatic PE (lung scan)
No symptomatic PE
29 filter migrations on systematic abdominal X-ray
1 spontaneous rupture of the filter
40 deaths between 7 days and 39 months
[JARRETT2002]
Monocenter retrospective study 1993 - 2000
116 patients Cancer patients with DVT or PE
Gastrointestinal tract (21.6%); lung (20.7%); breast (12.1%); gynecology (12.1%); prostate (10.3%); hematology (6.9%); urinary tract (3.4%); others (12.9%)
Cancer staging: - stage I or II: 18.2% - stage III: 3.4% - stage IV: 78.4%
IVCF indications: contraindication to anticoagulants: 52/116; VTE recurrence: 17/116; arterial pulmonary hypertension: 15/116
12.2 months DVT: 20/116 (1.7%) PE: 3/116 (2.6%)
Localized hematomas: 5/116 (4.3%)
1 month: 80/116 (68.8%) 3 months: 67/116 (57.4%) 1 year : 31/116 (26.8%)
stage IV: 16/116 (13.7% ) vs. stage (I + II + III): 90/116 (77.9%); p<0.001
[WALLACE2004]
Monocenter retrospective study Jan 2000 - May 2003
308 patients Cancer patients with DVT treated with IVCF
Mean age: 60 years (range 24-81)
Solid tumors: 267 patients Hematology: 41 patients
IVCF insertion for the treatment of DVT
Unspecified PE: 1.3% (4/308)
Vena cava thrombosis: 4.5% (14/308)
Retroperitoneal bleeding: 2/308 (0.6%)
IVCF-related complications: 2/308 (0.6%)
Global survival (mean, % patients at 1 year) - solid tumors: 145 days, 35% at 1 year - hematology: 207 days, 48% at 1 year Causes of death: - PE alone: 4/308 (1.3%) - PE, other factor: 10/308 (3.2%)

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 43 Copyright © 1093790 (OPIC 28/02/2012)
Table 10 Vena cava filters (continued)
References
Design
Inclusion period
Number of patients
included/evaluated Included population Intervention Follow-up Recurrence Toxicity Survival
[ZERATI2005]
Monocenter retrospective study Jan 1998 - Jan 2004
50 patients Cancer patients with VTE treated with IVCF
ICVF insertion
IVCF indications : Contraindication to anticoagulants: 40/50 (80%); PE despite anticoagulation: 6/50 (12%); PE with severe respiratory insufficiency 4/50 (8%)
5 years PE: 4/50 (2%) Inferior vena cava thrombosis: 8/50 (4% )
IVCF thrombosis: 4/50 (2%)
5-year survival: 60% (no VTE-related death) median survival: 496 days
[SCHUNN2006]
Monocenter retrospective study Feb 1998 - Apr 2003
Global analysis: n=55 patients
Case-control study: n=16 patients
3 patients lost to follow-up (2 cases + 1 control = censored data)
Metastatic or locally advanced cancers with DVT or PE
DVT alone: 42/55 (76%) PE alone: 6/55 (11%) DVT+PE: 7/55 (13%)
IVCF insertion (55 patients) anticoagulant + IVCF: 22/55 (60%) IVCF alone: 33/55 (40%)
IVCF indications: high bleeding risk: 10/55 (18.2%); brain metastasis 21/55 (38.2%); thrombocytopenia 7/55 (12.7%); bleeding 8/55 (14.5%); anticoagulation failure: 2/55 (3.7%); perioperative: 7/55 (12.7%)
LMWH low dose: 2 patients LMWH high dose: 2 patients VKA low dose: 5 patients VKA full dose: 2 patients UFH: 2 patients No anticoagulation: 2 patients
Mean: 248.3± 48.5 days
Median: 136 days
IVCF: 18.2% (10/55)
Control: 18.7% (3/16)
IVCF complications: 7.2% (4/55)
Death at 1 month Filter: 43.7% (7/16) Control: 25% (4/16)
1-year survival: Filter: 19.0% Control: 12.5%
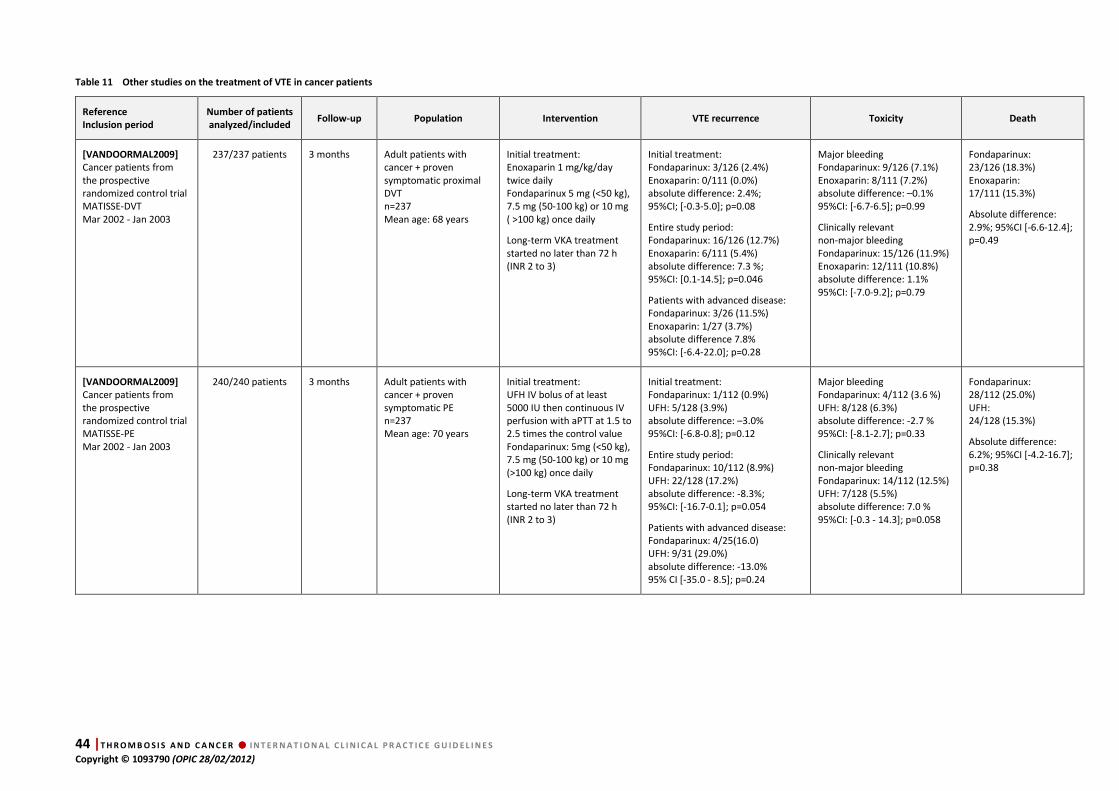
44 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 11 Other studies on the treatment of VTE in cancer patients
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity Death
[VANDOORMAL2009]
Cancer patients from the prospective randomized control trial MATISSE-DVT Mar 2002 - Jan 2003
237/237 patients 3 months Adult patients with cancer + proven symptomatic proximal DVT n=237 Mean age: 68 years
Initial treatment: Enoxaparin 1 mg/kg/day twice daily Fondaparinux 5 mg (<50 kg), 7.5 mg (50-100 kg) or 10 mg ( >100 kg) once daily
Long-term VKA treatment started no later than 72 h (INR 2 to 3)
Initial treatment: Fondaparinux: 3/126 (2.4%) Enoxaparin: 0/111 (0.0%) absolute difference: 2.4%; 95%CI; [-0.3-5.0]; p=0.08
Entire study period: Fondaparinux: 16/126 (12.7%) Enoxaparin: 6/111 (5.4%) absolute difference: 7.3 %; 95%CI: [0.1-14.5]; p=0.046
Patients with advanced disease: Fondaparinux: 3/26 (11.5%) Enoxaparin: 1/27 (3.7%) absolute difference 7.8% 95%CI: [-6.4-22.0]; p=0.28
Major bleeding Fondaparinux: 9/126 (7.1%) Enoxaparin: 8/111 (7.2%) absolute difference: –0.1% 95%CI: [-6.7-6.5]; p=0.99
Clinically relevant non-major bleeding Fondaparinux: 15/126 (11.9%) Enoxaparin: 12/111 (10.8%) absolute difference: 1.1% 95%CI: [-7.0-9.2]; p=0.79
Fondaparinux: 23/126 (18.3%) Enoxaparin: 17/111 (15.3%)
Absolute difference: 2.9%; 95%CI [-6.6-12.4]; p=0.49
[VANDOORMAL2009]
Cancer patients from the prospective randomized control trial MATISSE-PE Mar 2002 - Jan 2003
240/240 patients 3 months Adult patients with cancer + proven symptomatic PE n=237 Mean age: 70 years
Initial treatment: UFH IV bolus of at least 5000 IU then continuous IV perfusion with aPTT at 1.5 to 2.5 times the control value Fondaparinux: 5mg (<50 kg), 7.5 mg (50-100 kg) or 10 mg (>100 kg) once daily
Long-term VKA treatment started no later than 72 h (INR 2 to 3)
Initial treatment: Fondaparinux: 1/112 (0.9%) UFH: 5/128 (3.9%) absolute difference: –3.0% 95%CI: [-6.8-0.8]; p=0.12
Entire study period: Fondaparinux: 10/112 (8.9%) UFH: 22/128 (17.2%) absolute difference: -8.3%; 95%CI: [-16.7-0.1]; p=0.054
Patients with advanced disease: Fondaparinux: 4/25(16.0) UFH: 9/31 (29.0%) absolute difference: -13.0% 95% CI [-35.0 - 8.5]; p=0.24
Major bleeding Fondaparinux: 4/112 (3.6 %) UFH: 8/128 (6.3%) absolute difference: -2.7 % 95%CI: [-8.1-2.7]; p=0.33
Clinically relevant non-major bleeding Fondaparinux: 14/112 (12.5%) UFH: 7/128 (5.5%) absolute difference: 7.0 % 95%CI: [-0.3 - 14.3]; p=0.058
Fondaparinux: 28/112 (25.0%) UFH: 24/128 (15.3%)
Absolute difference: 6.2%; 95%CI [-4.2-16.7]; p=0.38

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 45 Copyright © 1093790 (OPIC 28/02/2012)
1.3. Data analysis
Q 1: UFH followed by VKA
Studies
8 retrospective studies
[MOORE1981] [CLARKEPEARSON1983] [KRAUTHE1987] [CALLIGARO1991] [CHAN1992] [DEBOURDEAU1996] [HARRINGTON1997] [ELTING2004] 5 prospective studies
[BONA2000] [HUTTEN2000] PALARETTI 2000] [PRANDONI2002] [VUCIC2002] 2 control arms of randomized studies
[HULL2006] [VANDOORMAAL2009]
Agreement Yes
Quality of evidence Moderate (retrospective + large effect)
Results
Retrospective studies: high complication rate with 25-30 % relapse and 15-30 % major bleeding
Control arm of randomized studies (UFH + VKA): 7-10 % relapses and 4-7 % major bleeding at 6 months under treatment
Conclusion
Treatment of VTE in cancer patients with UFH followed by VKA is associated with a high rate of
relapse and bleeding.
Q 2: LMWH followed by VKA
Studies 5 control arms of randomized studies
[MEYER2002] [LEE2003] [DEITCHER2006] [ROMERA2009] [VANDOORMAAL2009]
Agreement Yes
Quality of evidence High (randomized + consistency)
Results
In the “cancer” population: at six months high rate of relapse (2-16.9 %) and major bleeding (2.7-16 %) in patients with cancer vs. patients without cancer In the control arm of prospective studies (LMWH + VKA): 6-16.9 % relapses and 2.9-16 % major bleeding at 6 months
Conclusion
Treatment of VTE in cancer patients with LMWH followed by VKA is associated with a high rate
of relapse and bleeding.
Using indirect comparison, the rate of major bleeding and relapse of VTE in cancer patients
treated with LMWH and VKA:
• appears lower than the rate with UFH + VKA,
• is increased in “cancer patients” compared to “non-cancer patients”.
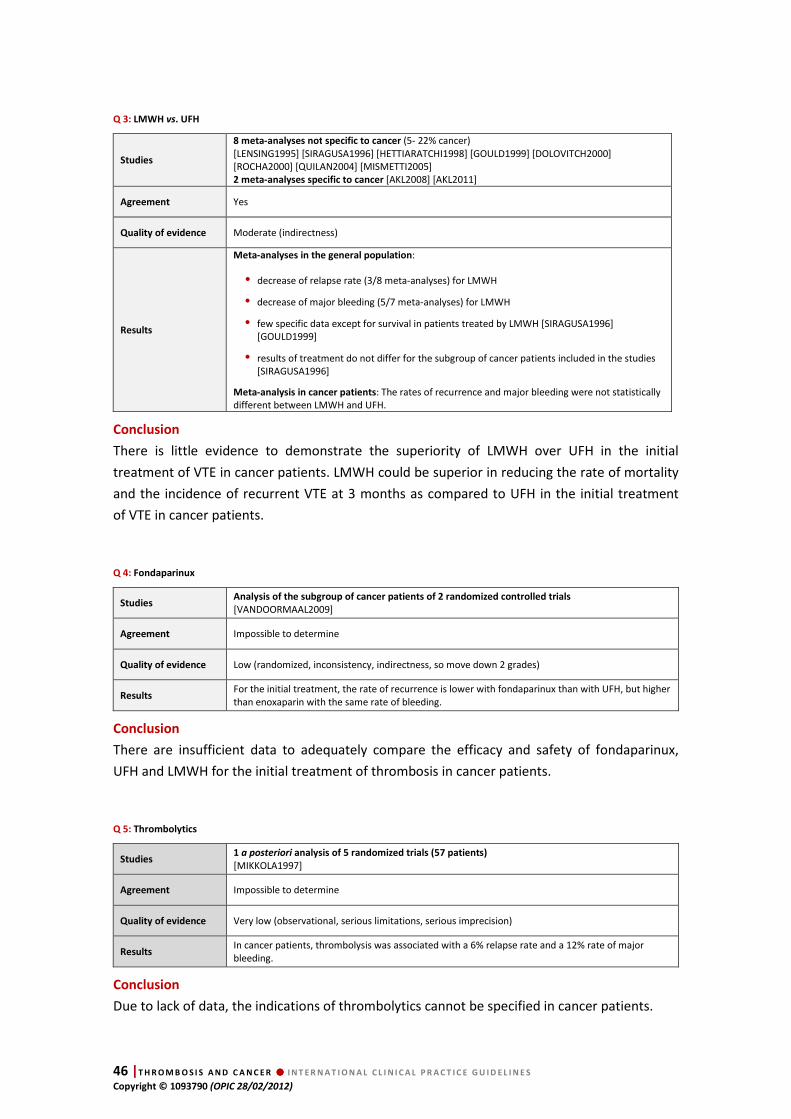
46 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Q 3: LMWH vs. UFH
Studies
8 meta-analyses not specific to cancer (5- 22% cancer) [LENSING1995] [SIRAGUSA1996] [HETTIARATCHI1998] [GOULD1999] [DOLOVITCH2000] [ROCHA2000] [QUILAN2004] [MISMETTI2005] 2 meta-analyses specific to cancer [AKL2008] [AKL2011]
Agreement Yes
Quality of evidence Moderate (indirectness)
Results
Meta-analyses in the general population:
• decrease of relapse rate (3/8 meta-analyses) for LMWH
• decrease of major bleeding (5/7 meta-analyses) for LMWH
• few specific data except for survival in patients treated by LMWH [SIRAGUSA1996] [GOULD1999]
• results of treatment do not differ for the subgroup of cancer patients included in the studies [SIRAGUSA1996]
Meta-analysis in cancer patients: The rates of recurrence and major bleeding were not statistically different between LMWH and UFH.
Conclusion
There is little evidence to demonstrate the superiority of LMWH over UFH in the initial
treatment of VTE in cancer patients. LMWH could be superior in reducing the rate of mortality
and the incidence of recurrent VTE at 3 months as compared to UFH in the initial treatment
of VTE in cancer patients.
Q 4: Fondaparinux
Studies Analysis of the subgroup of cancer patients of 2 randomized controlled trials
[VANDOORMAAL2009]
Agreement Impossible to determine
Quality of evidence Low (randomized, inconsistency, indirectness, so move down 2 grades)
Results For the initial treatment, the rate of recurrence is lower with fondaparinux than with UFH, but higher than enoxaparin with the same rate of bleeding.
Conclusion
There are insufficient data to adequately compare the efficacy and safety of fondaparinux,
UFH and LMWH for the initial treatment of thrombosis in cancer patients.
Q 5: Thrombolytics
Studies 1 a posteriori analysis of 5 randomized trials (57 patients)
[MIKKOLA1997]
Agreement Impossible to determine
Quality of evidence Very low (observational, serious limitations, serious imprecision)
Results In cancer patients, thrombolysis was associated with a 6% relapse rate and a 12% rate of major bleeding.
Conclusion
Due to lack of data, the indications of thrombolytics cannot be specified in cancer patients.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 47 Copyright © 1093790 (OPIC 28/02/2012)
Q 6: Vena cava filters
Studies
14 retrospective studies
[COHEN1991] [CALLIGARO1991] [COHEN1992] [LEVIN1993] [HUBBARD1994] [SCHIFF1994] [SCHWARZ1996] [GREENFIELD1997] [IHNAT1998] [SCHLEICH2001] [JARRETT2002] [WALLACE2004] [ZERATI2005] [SCHUNN2006]
Agreement Impossible to determine heterogeneity
Quality of evidence Very low (observational, serious limitations, serious imprecision)
Results The efficacy of vena cava filters is not proven in cancer patients.
Conclusion
Since vena cava filters were inserted in cancer patients included in the studies for different
reasons, evidence is lacking to recommend their use in the case of VTE recurrence. Cancer is
neither a specific indication nor a special contraindication to vena cava filter placement.
1.4. Discussion
Initial treatment is defined as the first ten days of anticoagulation. There is little evidence to
demonstrate the superiority of LMWH over UFH in the initial treatment of VTE in cancer
patients. In this setting, LMWH could be superior in reducing the rate of mortality and the
incidence of recurrent VTE at 3 months as compared to UFH. Overall, in the general
population, the results favor the use of short-term LMWH vs. UFH. Given that no RCTs have
evaluated the optimal initial therapy in cancer patients, but that no study reported a
difference between cancer and non-cancer patients, the experts considered that this
conclusion may be applied to the cancer population, although the meta-analyses did not show
any substantial differences in the subgroup of patients with cancer.
The balance between desirable and undesirable effects favors the use of LMWH (lower risk
of heparin-induced thrombocytopenia) which are more convenient to use (once or twice a day
vs. continuous perfusion or three times a day).
Analysis of cancer patients included in the studies performed in the general population shows
that UFH and fondaparinux can be used during the first ten days of treatment.
Although the data were insufficient to conclude on the indications of thrombolytic drugs
in cancer patients with VTE, they suggest that the use of fibrinolytics is possible in these
patients and that cancer in general is not a contraindication to thrombolytic therapy, with
the exception of patients with brain metastases or with a high bleeding risk because of the
unfavorable balance between desirable and undesirable effects.
Studies on vena cava filters are not specific for patients with cancer. Since cancer patients have
a high risk of recurrent VTE and bleeding, the benefit of these devices should be further
analyzed. Furthermore, because the quality of the evidence is very low and the balance
between desirable and undesirable effects cannot be determined, the experts consider that
temporary or retrievable (optional) vena cava filters may prove to be particularly valuable in
cancer patients, especially when anticoagulation is contraindicated. However, further studies
are necessary.
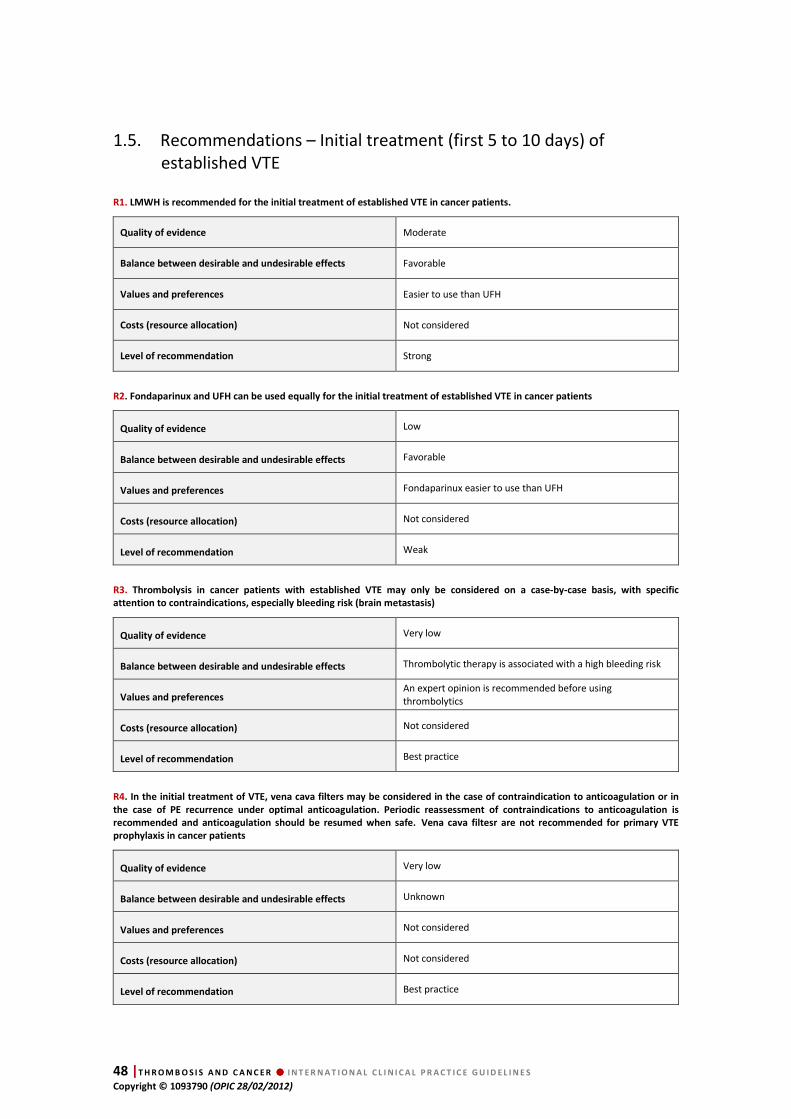
48 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
1.5. Recommendations – Initial treatment (first 5 to 10 days) of established VTE
R1. LMWH is recommended for the initial treatment of established VTE in cancer patients.
Quality of evidence Moderate
Balance between desirable and undesirable effects Favorable
Values and preferences Easier to use than UFH
Costs (resource allocation) Not considered
Level of recommendation Strong
R2. Fondaparinux and UFH can be used equally for the initial treatment of established VTE in cancer patients
Quality of evidence Low
Balance between desirable and undesirable effects Favorable
Values and preferences Fondaparinux easier to use than UFH
Costs (resource allocation) Not considered
Level of recommendation Weak
R3. Thrombolysis in cancer patients with established VTE may only be considered on a case-by-case basis, with specific
attention to contraindications, especially bleeding risk (brain metastasis)
Quality of evidence Very low
Balance between desirable and undesirable effects Thrombolytic therapy is associated with a high bleeding risk
Values and preferences An expert opinion is recommended before using thrombolytics
Costs (resource allocation) Not considered
Level of recommendation Best practice
R4. In the initial treatment of VTE, vena cava filters may be considered in the case of contraindication to anticoagulation or in
the case of PE recurrence under optimal anticoagulation. Periodic reassessment of contraindications to anticoagulation is
recommended and anticoagulation should be resumed when safe. Vena cava filtesr are not recommended for primary VTE
prophylaxis in cancer patients
Quality of evidence Very low
Balance between desirable and undesirable effects Unknown
Values and preferences Not considered
Costs (resource allocation) Not considered
Level of recommendation Best practice
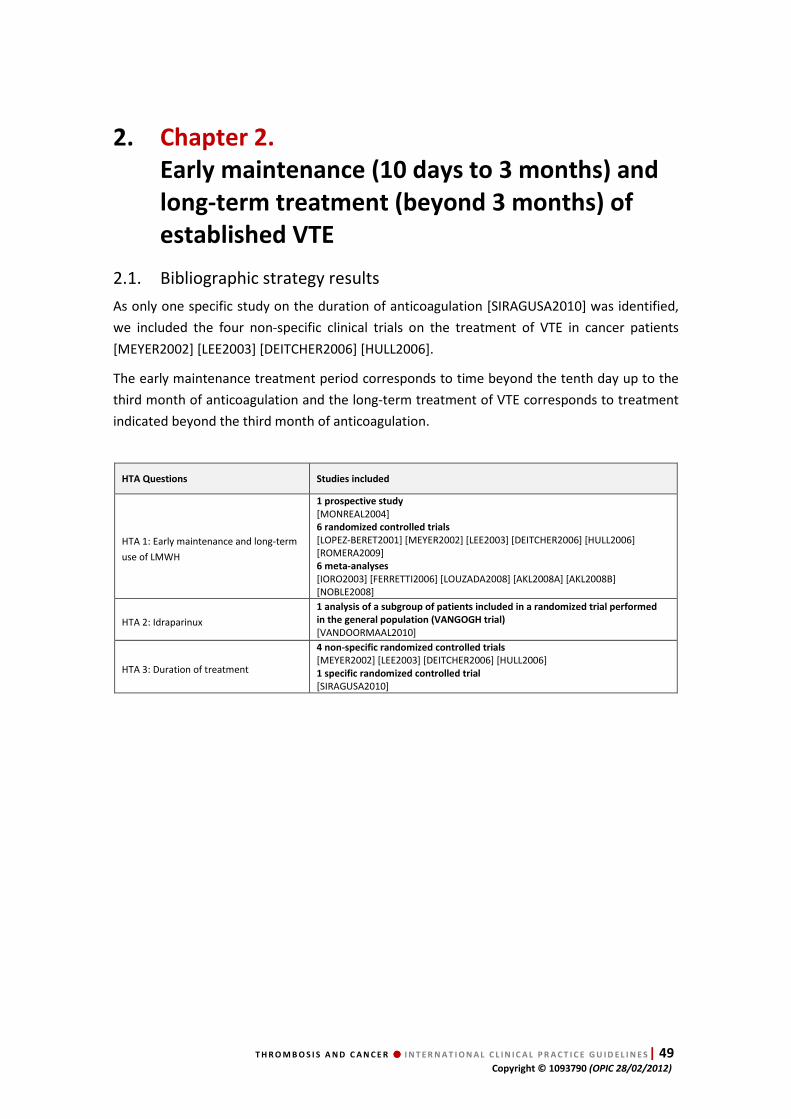
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 49 Copyright © 1093790 (OPIC 28/02/2012)
2. Chapter 2.
Early maintenance (10 days to 3 months) and
long-term treatment (beyond 3 months) of
established VTE
2.1. Bibliographic strategy results
As only one specific study on the duration of anticoagulation [SIRAGUSA2010] was identified,
we included the four non-specific clinical trials on the treatment of VTE in cancer patients
[MEYER2002] [LEE2003] [DEITCHER2006] [HULL2006].
The early maintenance treatment period corresponds to time beyond the tenth day up to the
third month of anticoagulation and the long-term treatment of VTE corresponds to treatment
indicated beyond the third month of anticoagulation.
HTA Questions Studies included
HTA 1: Early maintenance and long-term
use of LMWH
1 prospective study
[MONREAL2004] 6 randomized controlled trials
[LOPEZ-BERET2001] [MEYER2002] [LEE2003] [DEITCHER2006] [HULL2006] [ROMERA2009] 6 meta-analyses
[IORO2003] [FERRETTI2006] [LOUZADA2008] [AKL2008A] [AKL2008B] [NOBLE2008]
HTA 2: Idraparinux
1 analysis of a subgroup of patients included in a randomized trial performed
in the general population (VANGOGH trial)
[VANDOORMAAL2010]
HTA 3: Duration of treatment
4 non-specific randomized controlled trials
[MEYER2002] [LEE2003] [DEITCHER2006] [HULL2006] 1 specific randomized controlled trial
[SIRAGUSA2010]
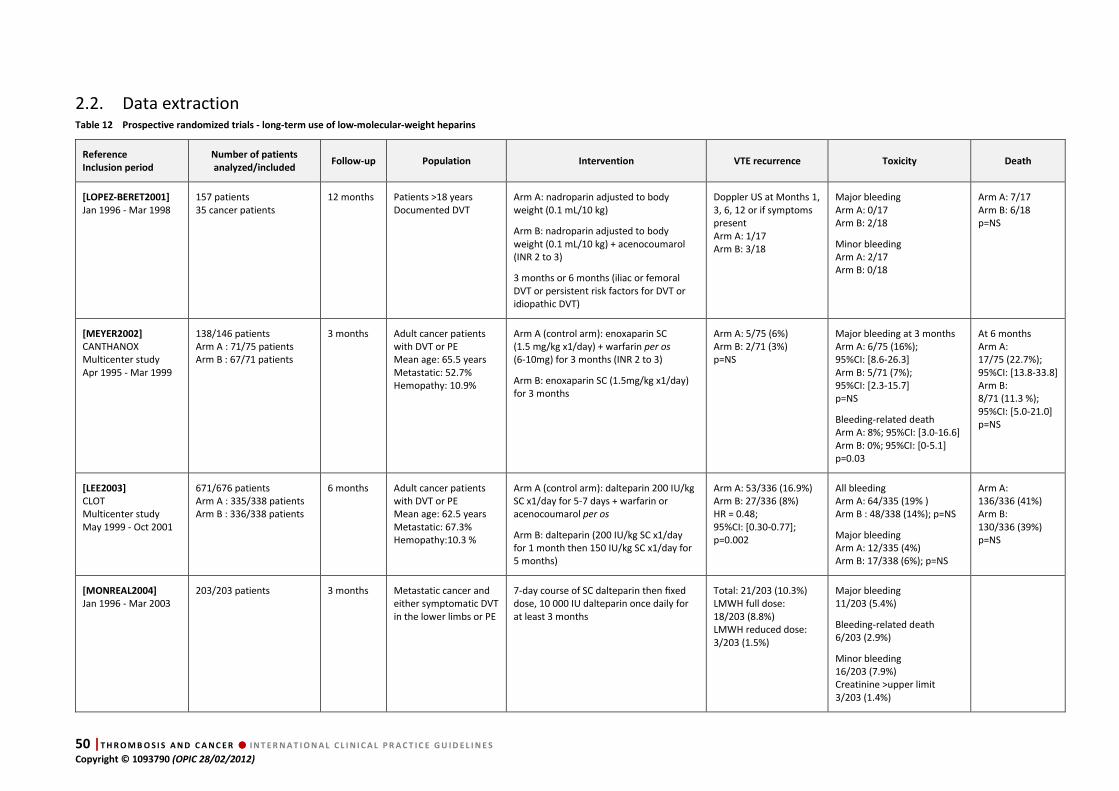
50 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
2.2. Data extraction Table 12 Prospective randomized trials - long-term use of low-molecular-weight heparins
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity Death
[LOPEZ-BERET2001]
Jan 1996 - Mar 1998
157 patients 35 cancer patients
12 months Patients >18 years Documented DVT
Arm A: nadroparin adjusted to body weight (0.1 mL/10 kg)
Arm B: nadroparin adjusted to body weight (0.1 mL/10 kg) + acenocoumarol (INR 2 to 3)
3 months or 6 months (iliac or femoral DVT or persistent risk factors for DVT or idiopathic DVT)
Doppler US at Months 1, 3, 6, 12 or if symptoms present Arm A: 1/17 Arm B: 3/18
Major bleeding Arm A: 0/17 Arm B: 2/18
Minor bleeding Arm A: 2/17 Arm B: 0/18
Arm A: 7/17 Arm B: 6/18 p=NS
[MEYER2002]
CANTHANOX Multicenter study Apr 1995 - Mar 1999
138/146 patients Arm A : 71/75 patients Arm B : 67/71 patients
3 months Adult cancer patients with DVT or PE Mean age: 65.5 years Metastatic: 52.7% Hemopathy: 10.9%
Arm A (control arm): enoxaparin SC (1.5 mg/kg x1/day) + warfarin per os (6-10mg) for 3 months (INR 2 to 3)
Arm B: enoxaparin SC (1.5mg/kg x1/day) for 3 months
Arm A: 5/75 (6%) Arm B: 2/71 (3%) p=NS
Major bleeding at 3 months Arm A: 6/75 (16%); 95%CI: [8.6-26.3] Arm B: 5/71 (7%); 95%CI: [2.3-15.7] p=NS
Bleeding-related death Arm A: 8%; 95%CI: [3.0-16.6] Arm B: 0%; 95%CI: [0-5.1] p=0.03
At 6 months Arm A: 17/75 (22.7%); 95%CI: [13.8-33.8] Arm B: 8/71 (11.3 %); 95%CI: [5.0-21.0] p=NS
[LEE2003]
CLOT Multicenter study May 1999 - Oct 2001
671/676 patients Arm A : 335/338 patients Arm B : 336/338 patients
6 months Adult cancer patients with DVT or PE Mean age: 62.5 years Metastatic: 67.3% Hemopathy:10.3 %
Arm A (control arm): dalteparin 200 IU/kg SC x1/day for 5-7 days + warfarin or acenocoumarol per os
Arm B: dalteparin (200 IU/kg SC x1/day for 1 month then 150 IU/kg SC x1/day for 5 months)
Arm A: 53/336 (16.9%) Arm B: 27/336 (8%) HR = 0.48; 95%CI: [0.30-0.77]; p=0.002
All bleeding Arm A: 64/335 (19% ) Arm B : 48/338 (14%); p=NS
Major bleeding Arm A: 12/335 (4%) Arm B: 17/338 (6%); p=NS
Arm A: 136/336 (41%) Arm B: 130/336 (39%) p=NS
[MONREAL2004]
Jan 1996 - Mar 2003 203/203 patients 3 months Metastatic cancer and
either symptomatic DVT in the lower limbs or PE
7-day course of SC dalteparin then fixed dose, 10 000 IU dalteparin once daily for at least 3 months
Total: 21/203 (10.3%) LMWH full dose: 18/203 (8.8%) LMWH reduced dose: 3/203 (1.5%)
Major bleeding 11/203 (5.4%)
Bleeding-related death 6/203 (2.9%)
Minor bleeding 16/203 (7.9%) Creatinine >upper limit 3/203 (1.4%)
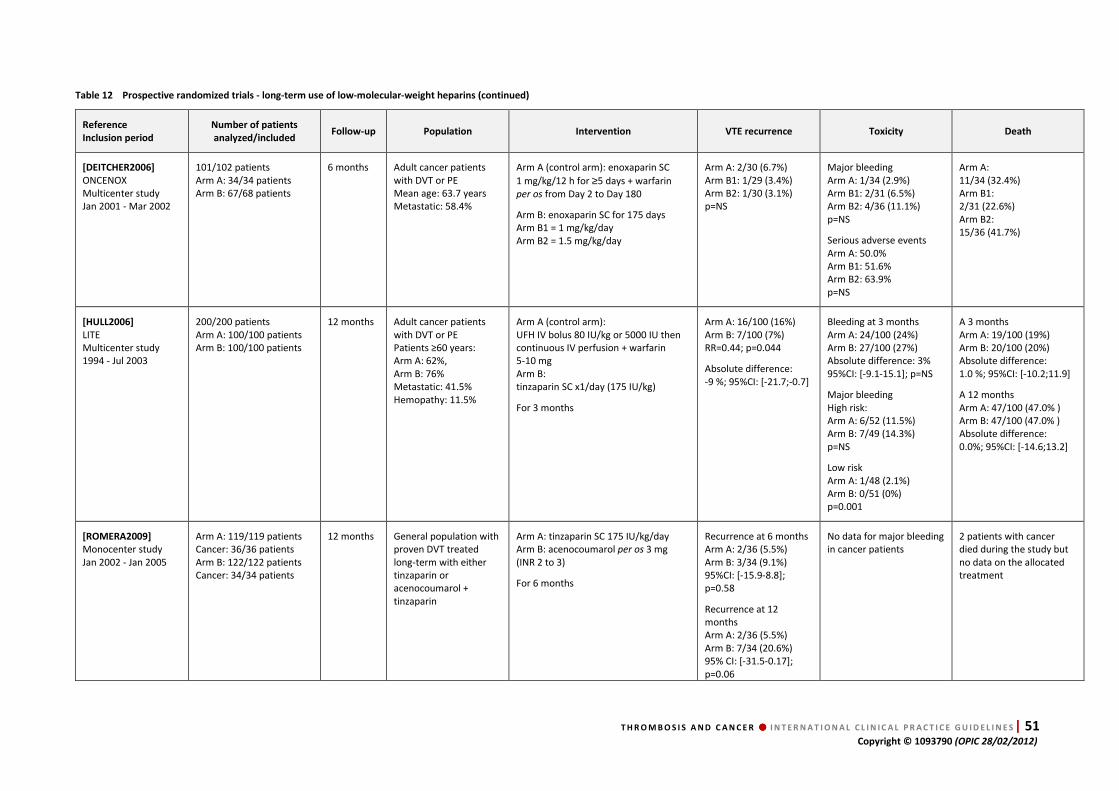
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 51 Copyright © 1093790 (OPIC 28/02/2012)
Table 12 Prospective randomized trials - long-term use of low-molecular-weight heparins (continued)
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity Death
[DEITCHER2006]
ONCENOX Multicenter study Jan 2001 - Mar 2002
101/102 patients Arm A: 34/34 patients Arm B: 67/68 patients
6 months Adult cancer patients with DVT or PE Mean age: 63.7 years Metastatic: 58.4%
Arm A (control arm): enoxaparin SC
1 mg/kg/12 h for ≥5 days + warfarin per os from Day 2 to Day 180
Arm B: enoxaparin SC for 175 days Arm B1 = 1 mg/kg/day Arm B2 = 1.5 mg/kg/day
Arm A: 2/30 (6.7%) Arm B1: 1/29 (3.4%) Arm B2: 1/30 (3.1%) p=NS
Major bleeding Arm A: 1/34 (2.9%) Arm B1: 2/31 (6.5%) Arm B2: 4/36 (11.1%) p=NS
Serious adverse events Arm A: 50.0% Arm B1: 51.6% Arm B2: 63.9% p=NS
Arm A: 11/34 (32.4%) Arm B1: 2/31 (22.6%) Arm B2: 15/36 (41.7%)
[HULL2006]
LITE Multicenter study 1994 - Jul 2003
200/200 patients Arm A: 100/100 patients Arm B: 100/100 patients
12 months Adult cancer patients with DVT or PE Patients ≥60 years: Arm A: 62%, Arm B: 76% Metastatic: 41.5% Hemopathy: 11.5%
Arm A (control arm): UFH IV bolus 80 IU/kg or 5000 IU then continuous IV perfusion + warfarin 5-10 mg Arm B: tinzaparin SC x1/day (175 IU/kg)
For 3 months
Arm A: 16/100 (16%) Arm B: 7/100 (7%) RR=0.44; p=0.044
Absolute difference: -9 %; 95%CI: [-21.7;-0.7]
Bleeding at 3 months Arm A: 24/100 (24%) Arm B: 27/100 (27%) Absolute difference: 3% 95%CI: [-9.1-15.1]; p=NS
Major bleeding High risk: Arm A: 6/52 (11.5%) Arm B: 7/49 (14.3%) p=NS
Low risk Arm A: 1/48 (2.1%) Arm B: 0/51 (0%) p=0.001
A 3 months Arm A: 19/100 (19%) Arm B: 20/100 (20%) Absolute difference: 1.0 %; 95%CI: [-10.2;11.9]
A 12 months Arm A: 47/100 (47.0% ) Arm B: 47/100 (47.0% ) Absolute difference: 0.0%; 95%CI: [-14.6;13.2]
[ROMERA2009]
Monocenter study Jan 2002 - Jan 2005
Arm A: 119/119 patients Cancer: 36/36 patients Arm B: 122/122 patients Cancer: 34/34 patients
12 months General population with proven DVT treated long-term with either tinzaparin or acenocoumarol + tinzaparin
Arm A: tinzaparin SC 175 IU/kg/day Arm B: acenocoumarol per os 3 mg (INR 2 to 3)
For 6 months
Recurrence at 6 months Arm A: 2/36 (5.5%) Arm B: 3/34 (9.1%) 95%CI: [-15.9-8.8]; p=0.58
Recurrence at 12 months Arm A: 2/36 (5.5%) Arm B: 7/34 (20.6%) 95% CI: [-31.5-0.17]; p=0.06
No data for major bleeding in cancer patients
2 patients with cancer died during the study but no data on the allocated treatment
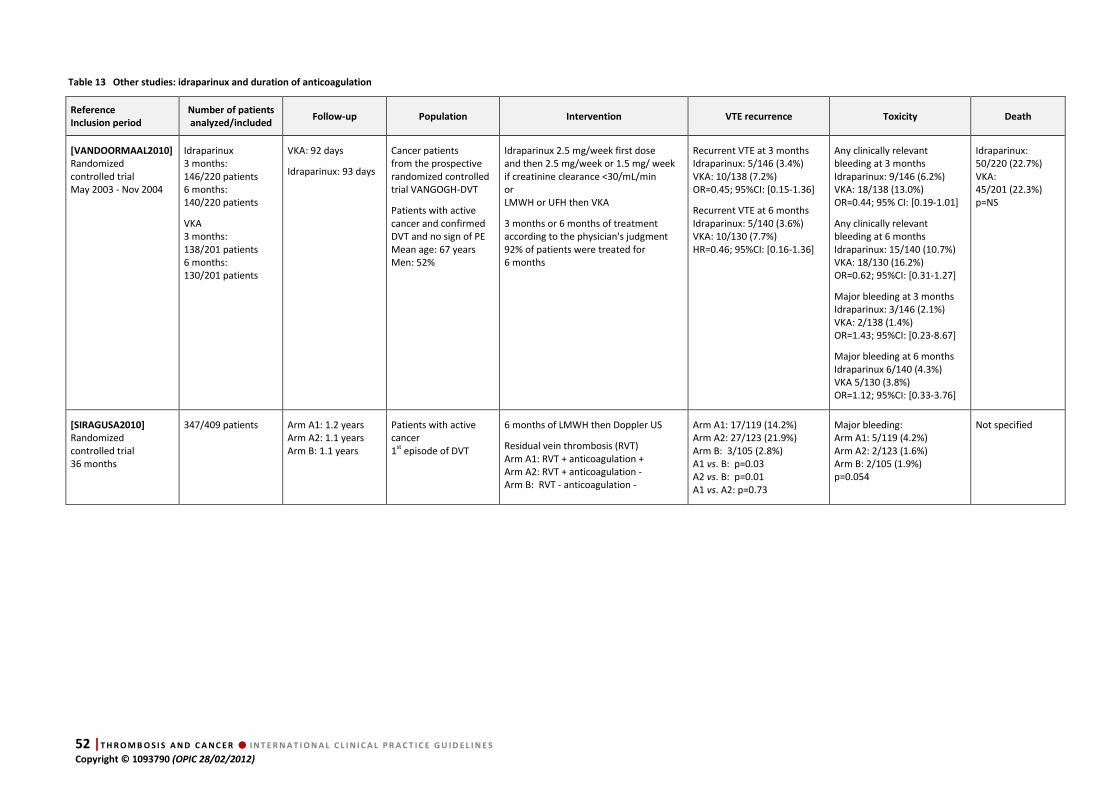
52 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 13 Other studies: idraparinux and duration of anticoagulation
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE recurrence Toxicity Death
[VANDOORMAAL2010]
Randomized controlled trial May 2003 - Nov 2004
Idraparinux 3 months: 146/220 patients 6 months: 140/220 patients
VKA 3 months: 138/201 patients 6 months: 130/201 patients
VKA: 92 days
Idraparinux: 93 days
Cancer patients from the prospective randomized controlled trial VANGOGH-DVT
Patients with active cancer and confirmed DVT and no sign of PE Mean age: 67 years Men: 52%
Idraparinux 2.5 mg/week first dose and then 2.5 mg/week or 1.5 mg/ week if creatinine clearance <30/mL/min or LMWH or UFH then VKA
3 months or 6 months of treatment according to the physician's judgment 92% of patients were treated for 6 months
Recurrent VTE at 3 months Idraparinux: 5/146 (3.4%) VKA: 10/138 (7.2%) OR=0.45; 95%CI: [0.15-1.36]
Recurrent VTE at 6 months Idraparinux: 5/140 (3.6%) VKA: 10/130 (7.7%) HR=0.46; 95%CI: [0.16-1.36]
Any clinically relevant bleeding at 3 months Idraparinux: 9/146 (6.2%) VKA: 18/138 (13.0%) OR=0.44; 95% CI: [0.19-1.01]
Any clinically relevant bleeding at 6 months Idraparinux: 15/140 (10.7%) VKA: 18/130 (16.2%) OR=0.62; 95%CI: [0.31-1.27]
Major bleeding at 3 months Idraparinux: 3/146 (2.1%) VKA: 2/138 (1.4%) OR=1.43; 95%CI: [0.23-8.67]
Major bleeding at 6 months Idraparinux 6/140 (4.3%) VKA 5/130 (3.8%) OR=1.12; 95%CI: [0.33-3.76]
Idraparinux: 50/220 (22.7%) VKA: 45/201 (22.3%) p=NS
[SIRAGUSA2010]
Randomized controlled trial 36 months
347/409 patients Arm A1: 1.2 years Arm A2: 1.1 years Arm B: 1.1 years
Patients with active cancer 1st episode of DVT
6 months of LMWH then Doppler US
Residual vein thrombosis (RVT) Arm A1: RVT + anticoagulation + Arm A2: RVT + anticoagulation - Arm B: RVT - anticoagulation -
Arm A1: 17/119 (14.2%) Arm A2: 27/123 (21.9%) Arm B: 3/105 (2.8%) A1 vs. B: p=0.03 A2 vs. B: p=0.01 A1 vs. A2: p=0.73
Major bleeding: Arm A1: 5/119 (4.2%) Arm A2: 2/123 (1.6%) Arm B: 2/105 (1.9%) p=0.054
Not specified

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 53 Copyright © 1093790 (OPIC 28/02/2012)
Table 14 Meta-analyses
References [FERRETI2006] [IORO2003] [LOUZADA2008]
Bibliographic search Medline® ; CCTR ; ASCO abstract database, ASH abstract database, from 1966 to 2006
Medline®, Embase® up to 2003 Medline® (1950 to January 2008), Embase® (1980 to 2008 week 6), the Cochrane Register of Controlled Trials (1st quarter 2008) and Medline® in-process and other non-indexed citations (Feb 12, 2008)
Included studies 11 studies [PINI1994, [DAS1996], [GONZALEZ-FAJARDO1999] [LOPACIUK1999], [VEIGA2000], [LOPEZ-BERET2001], [MEYER2002, [HULL2002, [KAKKAR2003], [LEE2003], [DEITCHER2003]
Studies with cancer patients: [MEYER2002], [HULL2002], [LEE2003], [DEITCHER2003]
7 studies [PINI1994], [DAS1996], [GONZALEZ-FAJARDO1999], [LOPACIUK1999], [VEIGA2000], [LOPEZ-BERET2001], [HULL2002]
No specific study in patients with cancer
5 studies in cancer patients (LÓPEZ-BERET2001], (MEYER2002], [LEE2003], [DEITCHER2003], [HULL 2006]
Primary endpoint VTE recurrence VTE recurrence rate at 3 months VTE recurrence
Secondary endpoint None Bleeding and death at 3 months Bleeding and death
Statistical tests Inverse variance and Mantel-Haenszel method Mantel-Haenszel method Intention-to-treat analysis Relative Risk (RR): primary measurement Heterogeneity: Cochrane Q/Chi-Square tests.
Results Recurrence in the subgroup of cancer patients (n=1115) RR=0.525; 95%IC: [0.359-0.769]; p=0.001
No results for cancer patients Results for the general population for primary endpoint
VTE recurrence VKA: 44/672 (6.5%); LMWH: 31/688 (4.5%); p=NS
Bleeding VKA: 14/685 (2%); LMWH: 6/694 (0.9%); p=NS
Cancer-related death VKA: 24/451 (5.3%); LMWH: 27/457 (5.9%); p=NS
VTE recurrence VKA: 73/565 (12.9%); LMWH: 40/593 (6.7%) RR=0.53; 95%CI: [0.36-0.76]; p=0.0007
Bleeding VKA: 42/685 (7.7%); LMWH: 37/593 (6.4%) RR=0.98; 95%CI: [0.49-1.93]; p=0.45
All-cause mortality VKA: 184/513 (35.8%); LMWH: 172/509 (33.8%) RR=0.94; 95%CI: [0.80-1.11]; p=0.47
Authors’ conclusions There is a significant reduction of the risk of recurrent symptomatic VTE in favor of LMWH over VKA during treatment. Patients treated with long-term LMWH do not seem to experience recurrent VTE events more frequently compared to those treated with VKA after cessation of therapy. The significant difference favoring LMWH over VKA among all patients receiving treatment is mostly derived from studies enrolling cancer patients
A 3-month course of LMWH is as effective and safe as a corresponding period of oral anticoagulant (OA) treatment, and may therefore be considered as a valuable alternative option for patients in whom OA treatment appears to be contraindicated or problematic.
Long-term use of LMWH after the first week or initial treatment is superior to VKAs for secondary prevention of VTE in adult patients with cancer.
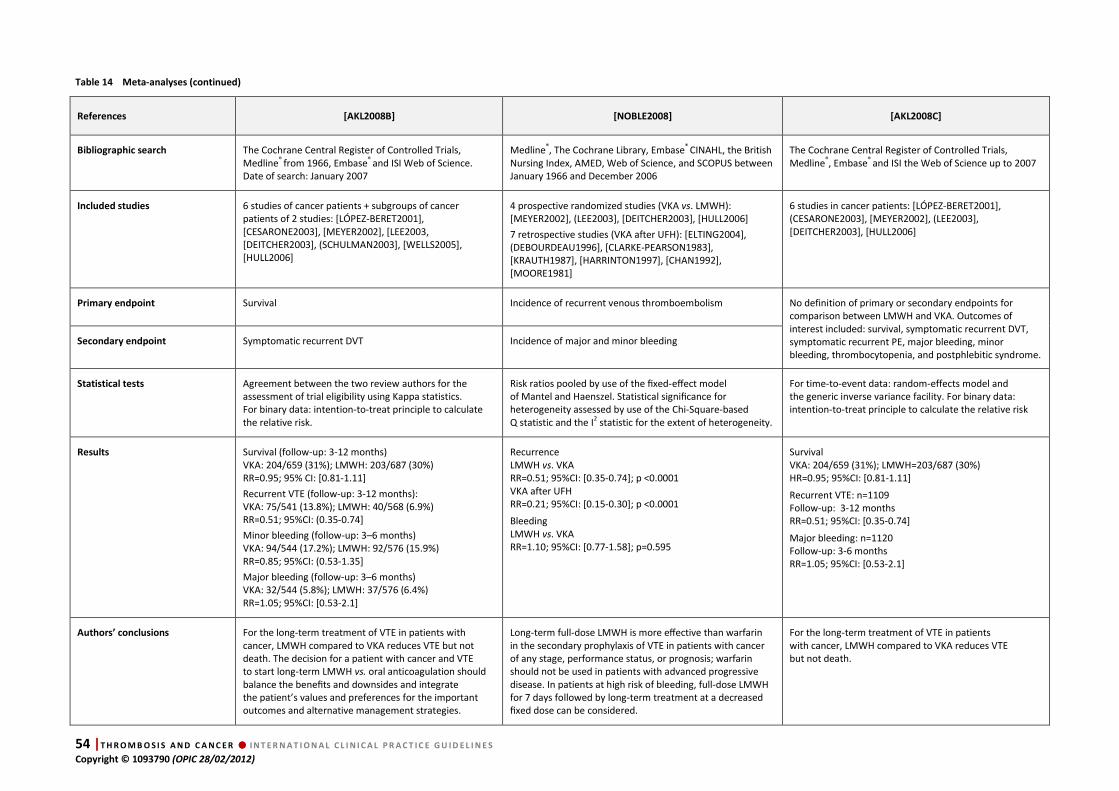
54 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 14 Meta-analyses (continued)
References [AKL2008B] [NOBLE2008] [AKL2008C]
Bibliographic search The Cochrane Central Register of Controlled Trials, Medline® from 1966, Embase® and ISI Web of Science. Date of search: January 2007
Medline®, The Cochrane Library, Embase® CINAHL, the British Nursing Index, AMED, Web of Science, and SCOPUS between January 1966 and December 2006
The Cochrane Central Register of Controlled Trials, Medline®, Embase® and ISI the Web of Science up to 2007
Included studies 6 studies of cancer patients + subgroups of cancer patients of 2 studies: [LÓPEZ-BERET2001], [CESARONE2003], [MEYER2002], [LEE2003, [DEITCHER2003], (SCHULMAN2003], [WELLS2005], [HULL2006]
4 prospective randomized studies (VKA vs. LMWH): [MEYER2002], (LEE2003], [DEITCHER2003], [HULL2006]
7 retrospective studies (VKA after UFH): [ELTING2004], (DEBOURDEAU1996], [CLARKE-PEARSON1983], [KRAUTH1987], [HARRINTON1997], [CHAN1992], [MOORE1981]
6 studies in cancer patients: [LÓPEZ-BERET2001], (CESARONE2003], [MEYER2002], (LEE2003], [DEITCHER2003], [HULL2006]
Primary endpoint Survival Incidence of recurrent venous thromboembolism No definition of primary or secondary endpoints for comparison between LMWH and VKA. Outcomes of interest included: survival, symptomatic recurrent DVT, symptomatic recurrent PE, major bleeding, minor bleeding, thrombocytopenia, and postphlebitic syndrome.
Secondary endpoint
Symptomatic recurrent DVT Incidence of major and minor bleeding
Statistical tests Agreement between the two review authors for the assessment of trial eligibility using Kappa statistics. For binary data: intention-to-treat principle to calculate the relative risk.
Risk ratios pooled by use of the fixed-effect model of Mantel and Haenszel. Statistical significance for heterogeneity assessed by use of the Chi-Square-based Q statistic and the I2 statistic for the extent of heterogeneity.
For time-to-event data: random-effects model and the generic inverse variance facility. For binary data: intention-to-treat principle to calculate the relative risk
Results Survival (follow-up: 3-12 months) VKA: 204/659 (31%); LMWH: 203/687 (30%) RR=0.95; 95% CI: [0.81-1.11]
Recurrent VTE (follow-up: 3-12 months): VKA: 75/541 (13.8%); LMWH: 40/568 (6.9%) RR=0.51; 95%CI: (0.35-0.74]
Minor bleeding (follow-up: 3–6 months) VKA: 94/544 (17.2%); LMWH: 92/576 (15.9%) RR=0.85; 95%CI: (0.53-1.35]
Major bleeding (follow-up: 3–6 months) VKA: 32/544 (5.8%); LMWH: 37/576 (6.4%) RR=1.05; 95%CI: [0.53-2.1]
Recurrence LMWH vs. VKA RR=0.51; 95%CI: [0.35-0.74]; p <0.0001 VKA after UFH RR=0.21; 95%CI: [0.15-0.30]; p <0.0001
Bleeding LMWH vs. VKA RR=1.10; 95%CI: [0.77-1.58]; p=0.595
Survival VKA: 204/659 (31%); LMWH=203/687 (30%) HR=0.95; 95%CI: [0.81-1.11]
Recurrent VTE: n=1109 Follow-up: 3-12 months RR=0.51; 95%CI: [0.35-0.74]
Major bleeding: n=1120 Follow-up: 3-6 months RR=1.05; 95%CI: [0.53-2.1]
Authors’ conclusions For the long-term treatment of VTE in patients with cancer, LMWH compared to VKA reduces VTE but not death. The decision for a patient with cancer and VTE to start long-term LMWH vs. oral anticoagulation should balance the benefits and downsides and integrate the patient’s values and preferences for the important outcomes and alternative management strategies.
Long-term full-dose LMWH is more effective than warfarin in the secondary prophylaxis of VTE in patients with cancer of any stage, performance status, or prognosis; warfarin should not be used in patients with advanced progressive disease. In patients at high risk of bleeding, full-dose LMWH for 7 days followed by long-term treatment at a decreased fixed dose can be considered.
For the long-term treatment of VTE in patients with cancer, LMWH compared to VKA reduces VTE but not death.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 55 Copyright © 1093790 (OPIC 28/02/2012)
2.3. Data analysis Early maintenance treatment (10 days to 3 months) and long-term treatment by use of LMWH
Studies
1 prospective study
[MONREAL2004] 6 randomized controlled trials
[LOPEZ-BERET2001] [MEYER2002] [LEE2003] [DEITCHER2006] [HULL2006] [ROMERA 2009] 6 meta-analyses
[IORO2003] [FERRETTI2006] [LOUZADA2008] [AKL2008A] [AKL2008B] [NOBLE2008]
Agreement Yes, except studies with low number of patients [DEITCHER 2006] [ROMERA2009] Coherent data for cancer patients (3/5 good-quality trials and meta-analyses)
Quality of evidence High (randomized, meta-analysis, consistency)
Results
Early maintenance treatment (10 days to 3 months) and long-term treatment by LMWH alone (beyond 3 months) vs. heparins (UFH/LMWH) with early VKA in cancer patients with VTE decreases the recurrence rate by 50% with no increase in bleeding risk or any effect on the mortality rate.
Conclusion
LMWH at therapeutic dose for 3 to 6 months is superior to VKA in the treatment of VTE
in cancer patients.
Long-term use of idraparinux
Studies 1 randomized trial non-specific to cancer patients
[VANDOORMAAL 2010]
Agreement Not applicable
Quality of evidence Low (randomized, inconsistency, indirectness, idraparinux not available, so move down 2 grades)
Results
For early maintenance treatment (10 days to 3 months) and long-term treatment (beyond 3 months) of VTE in cancer patients, idraparinux is as effective as VKA with the same rate of bleeding.
Conclusion
There are not enough data to evaluate the efficacy of idraparinux, which has now been
withdrawn form the market.
Duration of anticoagulation
Studies
4 randomized controlled trials not specifically designed to evaluate the duration
of anticoagulation [MEYER2002] [LEE2003] [DEITCHER2006] [HULL2006] 1 specific randomized controlled trial
[SIRAGUSA2010]
Agreement Impossible to determine because of only one specific study
Quality of evidence Low (a randomized trial but serious indirectness; 4 non-specific studies)
Results
Early maintenance treatment (10 days to 3 months) and long-term treatment by LMWH alone (beyond 3 months) are validated in cancer patients.
There is no study comparing 3 vs. 6 months of LMWH, but two specific positive studies used a 6-month regimen. It is important to distinguish between the duration of anticoagulation and the duration of LMWH treatment.
In patients with DVT, after 6 months of anticoagulation, the use of:
• Doppler US is not reliable and remains debated at this stage
• Use of D-dimer assay to determine the need for further anticoagulation is not well documented

56 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Conclusion
Among studies conducted in a cancer patient population, two used LMWH for six months
[LEE2003, DEITCHER2006], the two others for three months [MEYER2002, HULL2006].
No specific study assessed the optimal duration of anticoagulation in cancer patients.
The use of D-dimer assay and the presence of residual thrombosis on Doppler US cannot
be recommended to determine the duration of anticoagulation.
2.4. Discussion
The benefit of long-term use of LMWH over VKA is well documented with 3 positive
randomized trials. These results consistently showed that in cancer patients with VTE,
compared with short-term heparin followed by VKA, early maintenance treatment (10 days to
3 months) and long-term treatment by LMWH (3 to 6 months) significantly reduced the risk of
VTE recurrence by approximately 50% without increasing the bleeding risk; this treatment had
no effect on mortality. In all the selected trials, the safety in terms of bleeding risk, in patients
receiving long-term LMWH, was at least as good as in patients with cancer treated with short-
term heparin followed by VKA. Several meta-analysis focused on the treatment of VTE
in cancer patients confirmed the importance of the pivotal trials.
Whenever possible, it is better to prescribe the same LMWH at the same dosage and the same
duration as those noted in the studies. When these LMWH are not available on the market,
it is best to treat patients with another LMWH than with VKA. The following table indicates the
different drugs used in these studies.
Drug Dosage and duration Study
Dalteparin 200 IU/kg/day for 1 month 150 IU/kg/day for 5 months
CLOT [LEE2003]
Tinzaparin 175 IU/kg/day for 3 months LITE [HULL2006]
Enoxaparin 1.5 mg/kg/day for 3 months CANTHANOX [MEYER2002]
Idraparinux 2.5 mg/week first dose, then 2.5 mg/week or 1.5 mg/week if creatinine clearance <30 mL/min For 3 or 6 months
VANGOGH subgroup [VANDOORMAAL2010]
For early maintenance treatment and long-term treatment periods, there is only one study
comparing idraparinux and VKA, which corresponds to the analysis of cancer patients included
in the VANGOGH trial. Therefore, the data for cancer patients are drawn from a subgroup
analysis and should be interpreted with caution. Thus it is not possible to exactly evaluate
the efficacy of idraparinux, which is no longer available. In the VANGOGH trial, idraparinux was
not biotinylated and no antidote is available for this drug in the event of major bleeding.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 57 Copyright © 1093790 (OPIC 28/02/2012)
Cancer DACUS is the only study evaluating an individual marker for assessing the duration of
anticoagulation in an active cancer population [SIRAGUSA2010]. The absence of residual
venous thrombosis (RVT) of the lower limbs could be of help to identify patients at low risk for
recurrent VTE, who could safely stop LMWH after 6 months [SIRAGUSA2010].
However, no clinical trial has compared 3 months of LMWH vs. 6 months or more in cancer
patients. The value of RVT is not well documented in either the general population or in cancer
patients and the screening of RVT is not useful in patients without confirmed DVT of the lower
limbs [DOUKETIS2010]. Therefore, in patients with DVT, after 6 months of anticoagulation,
the use of Doppler US is not reliable and remains debated at this stage, especially in cancer
patients who are at high risk of recurrence. Similarly, the value of D-dimer assay has been
tested in the general population, but is not documented to be of help to determine the need
for further anticoagulation in cancer patients. For all these reasons, the duration of LMWH
recommended by the working group is at least three months. It is important to distinguish
between the duration of LMWH treatment and the duration of anticoagulation, since many
patients, especially those with active cancer or those treated with chemotherapy or
anti-angiogenic therapy, are still at high risk of VTE after six months of anticoagulant therapy.
2.5. Recommendations – early maintenance treatment (10 days to 3 months) and long-term treatment (beyond 3 months) of established VTE
R1. LMWH are preferred over VKA for the early maintenance treatment (ten days to third month) and long-term
treatment (beyond 3 months) of VTE in cancer patients
Quality of evidence High
Balance between desirable and undesirable effects Favorable
Values and preferences Daily subcutaneous injection, no variability, no uncertainty
Costs (resource allocation) Not considered
Level of recommendation Strong
R2. Idraparinux is not recommended for the early maintenance treatment (10 days to 3 months) and long-term treatment
(beyond 3 months) of VTE in cancer patients. Idraparinux is currently not available on the market.
Quality of evidence Low
Balance between desirable and undesirable effects Uncertain
Values and preferences Easier to use
Costs (resource allocation) Not considered
Level of recommendation Weak

58 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
R3. LMWH should be used for a minimum of three months to treat established VTE in cancer patients. However, in this setting
the largest study treated patients for six months.
Quality of evidence High
Balance between desirable and undesirable effects Favorable
Values and preferences Daily injection, no variability, no uncertainty
Costs (resource allocation) Not considered
Level of recommendation Strong
R4. After 3 to 6 months, termination or continuation of anticoagulation (LMWH or VKA) should be based on individual
evaluation of the benefit-risk ratio, tolerability, patients’ preference and cancer activity
Quality of evidence Not applicable (no data)
Balance between desirable and undesirable effects Depending on the benefit-risk ratio
Values and preferences Daily injection, no variability, no uncertainty
Costs (resource allocation) Not considered
Level of recommendation Best practice

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 59 Copyright © 1093790 (OPIC 28/02/2012)
3. Chapter 3.
Treatment of recurrence of VTE in cancer
patients under anticoagulation
3.1. Bibliographic strategy results
The results of the bibliographic search for vena cava filters (VCF) are also shown in a previous
chapter. In these studies, the main indications of insertion of vena cava filter (IVCF) were
recurrence of VTE and contraindication to anticoagulation. In some cases, VCF were inserted
as a primary treatment of VTE.
HTA Questions Studies included
HTA 1: Recurrence in patients
treated with LMWH or VKA
1 specific retrospective study
[CARRIER2009]
HTA 2: Vena cava filters
14 retrospective studies
[COHEN1991] [CALLIGARO1991] [COHEN1992] [LEVIN1993] [HUBBARD1994] [SCHIFF1994] [SCHWARZ1996] [GREENFIELD1997] [IHNAT1998] [SCHLEICH2001] [JARRETT2002] [WALLACE2004] [ZERATI2005] [SCHUNN2006]
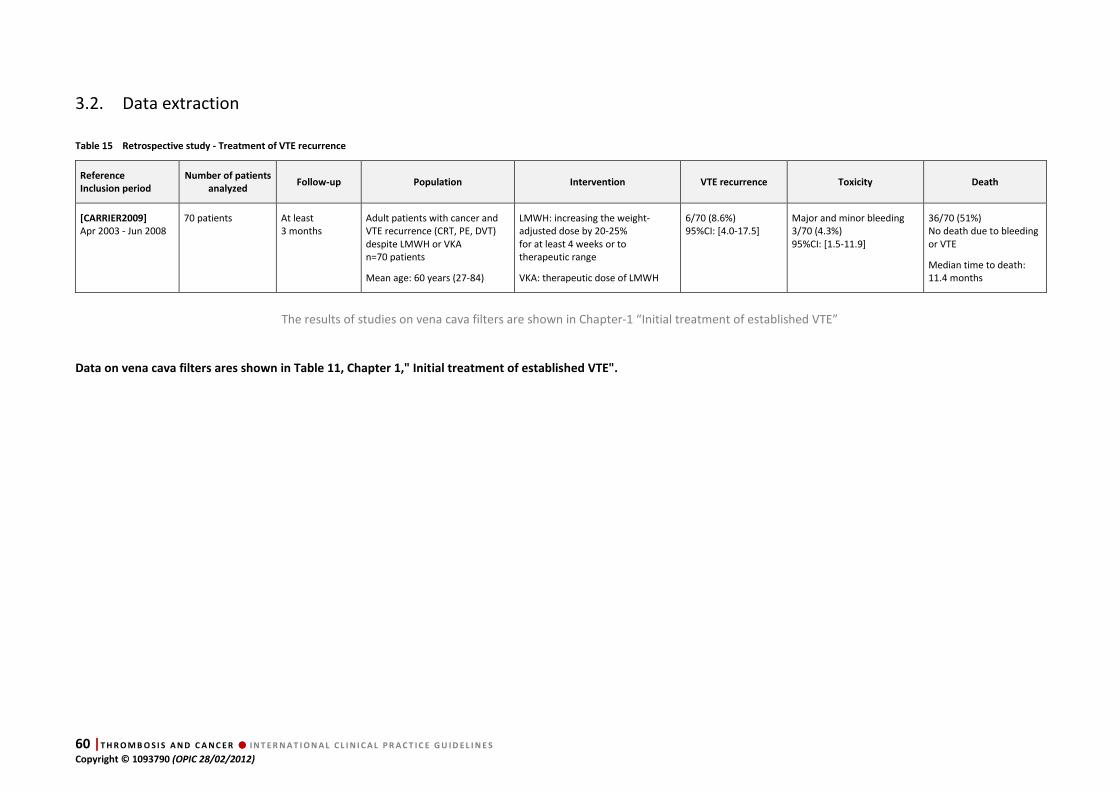
60 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
3.2. Data extraction
Table 15 Retrospective study - Treatment of VTE recurrence
Reference
Inclusion period
Number of patients
analyzed Follow-up Population Intervention VTE recurrence Toxicity Death
[CARRIER2009]
Apr 2003 - Jun 2008 70 patients At least
3 months
Adult patients with cancer and VTE recurrence (CRT, PE, DVT) despite LMWH or VKA n=70 patients
Mean age: 60 years (27-84)
LMWH: increasing the weight-adjusted dose by 20-25% for at least 4 weeks or to therapeutic range
VKA: therapeutic dose of LMWH
6/70 (8.6%) 95%CI: [4.0-17.5]
Major and minor bleeding 3/70 (4.3%) 95%CI: [1.5-11.9]
36/70 (51%) No death due to bleeding or VTE
Median time to death: 11.4 months
The results of studies on vena cava filters are shown in Chapter-1 “Initial treatment of established VTE”
Data on vena cava filters ares shown in Table 11, Chapter 1," Initial treatment of established VTE".
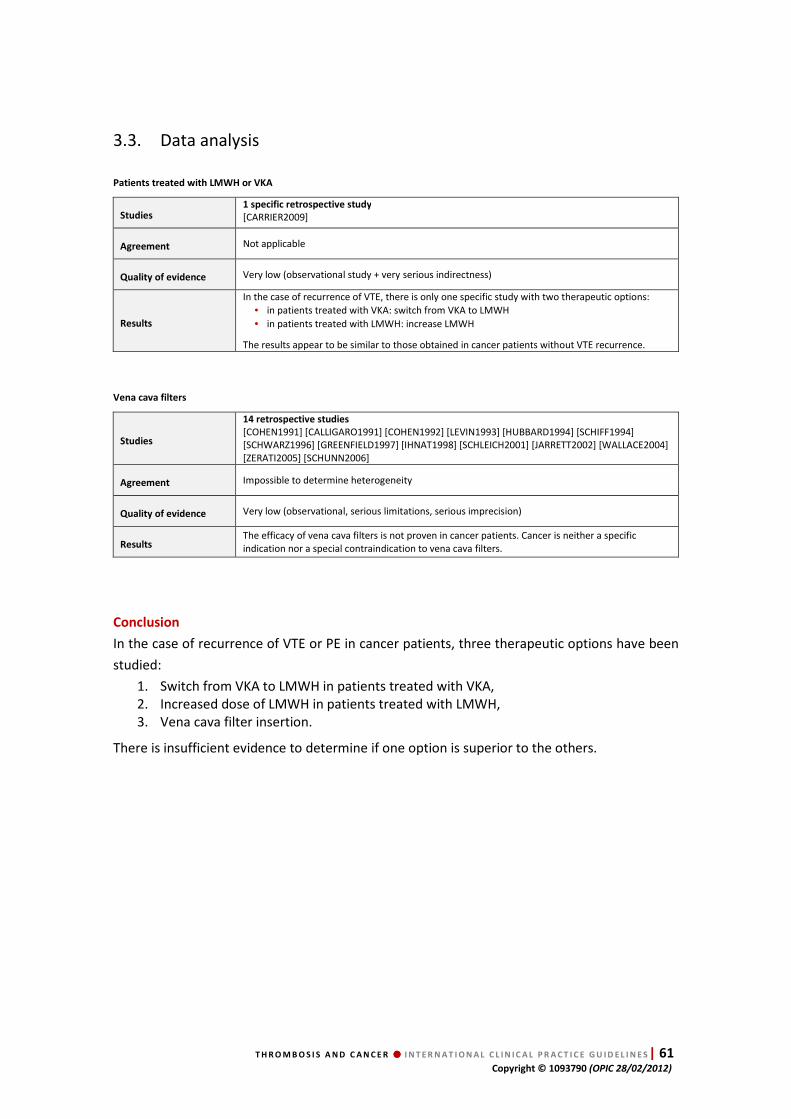
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 61 Copyright © 1093790 (OPIC 28/02/2012)
3.3. Data analysis
Patients treated with LMWH or VKA
Studies 1 specific retrospective study
[CARRIER2009]
Agreement Not applicable
Quality of evidence Very low (observational study + very serious indirectness)
Results
In the case of recurrence of VTE, there is only one specific study with two therapeutic options:
• in patients treated with VKA: switch from VKA to LMWH
• in patients treated with LMWH: increase LMWH
The results appear to be similar to those obtained in cancer patients without VTE recurrence.
Vena cava filters
Studies
14 retrospective studies
[COHEN1991] [CALLIGARO1991] [COHEN1992] [LEVIN1993] [HUBBARD1994] [SCHIFF1994] [SCHWARZ1996] [GREENFIELD1997] [IHNAT1998] [SCHLEICH2001] [JARRETT2002] [WALLACE2004] [ZERATI2005] [SCHUNN2006]
Agreement Impossible to determine heterogeneity
Quality of evidence Very low (observational, serious limitations, serious imprecision)
Results The efficacy of vena cava filters is not proven in cancer patients. Cancer is neither a specific indication nor a special contraindication to vena cava filters.
Conclusion
In the case of recurrence of VTE or PE in cancer patients, three therapeutic options have been
studied:
1. Switch from VKA to LMWH in patients treated with VKA, 2. Increased dose of LMWH in patients treated with LMWH, 3. Vena cava filter insertion.
There is insufficient evidence to determine if one option is superior to the others.
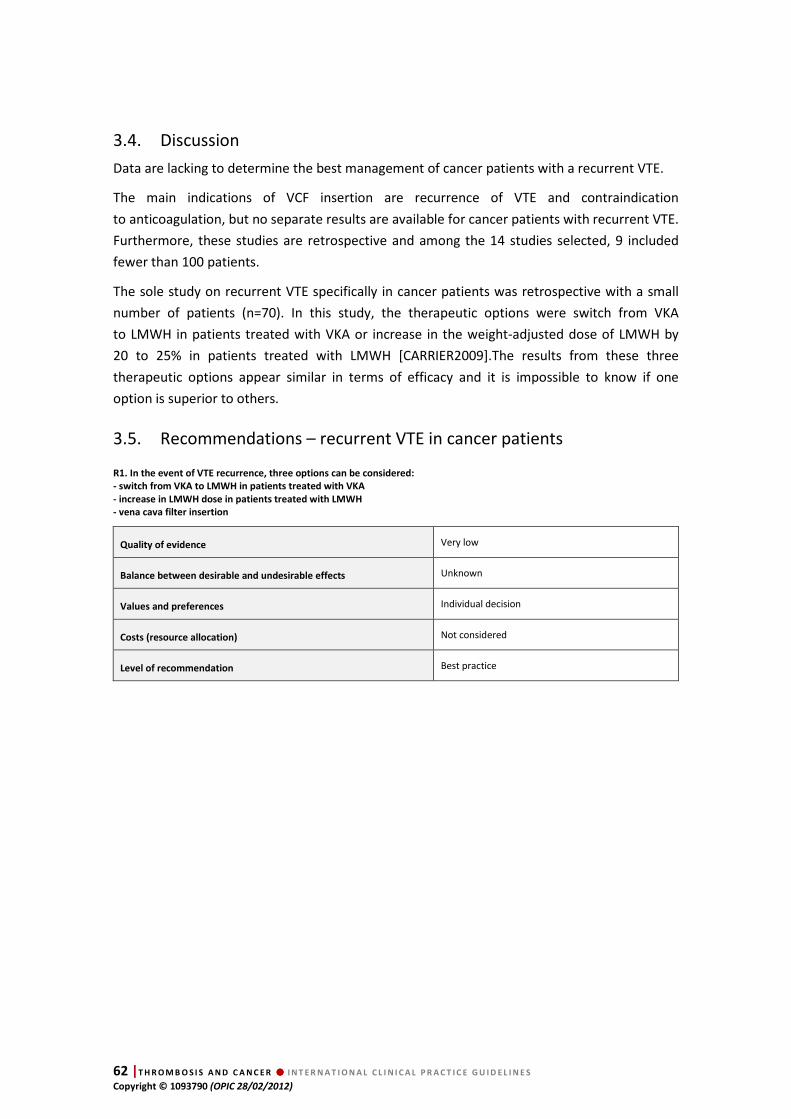
62 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
3.4. Discussion
Data are lacking to determine the best management of cancer patients with a recurrent VTE.
The main indications of VCF insertion are recurrence of VTE and contraindication
to anticoagulation, but no separate results are available for cancer patients with recurrent VTE.
Furthermore, these studies are retrospective and among the 14 studies selected, 9 included
fewer than 100 patients.
The sole study on recurrent VTE specifically in cancer patients was retrospective with a small
number of patients (n=70). In this study, the therapeutic options were switch from VKA
to LMWH in patients treated with VKA or increase in the weight-adjusted dose of LMWH by
20 to 25% in patients treated with LMWH [CARRIER2009].The results from these three
therapeutic options appear similar in terms of efficacy and it is impossible to know if one
option is superior to others.
3.5. Recommendations – recurrent VTE in cancer patients
R1. In the event of VTE recurrence, three options can be considered:
- switch from VKA to LMWH in patients treated with VKA
- increase in LMWH dose in patients treated with LMWH
- vena cava filter insertion
Quality of evidence Very low
Balance between desirable and undesirable effects Unknown
Values and preferences Individual decision
Costs (resource allocation) Not considered
Level of recommendation Best practice
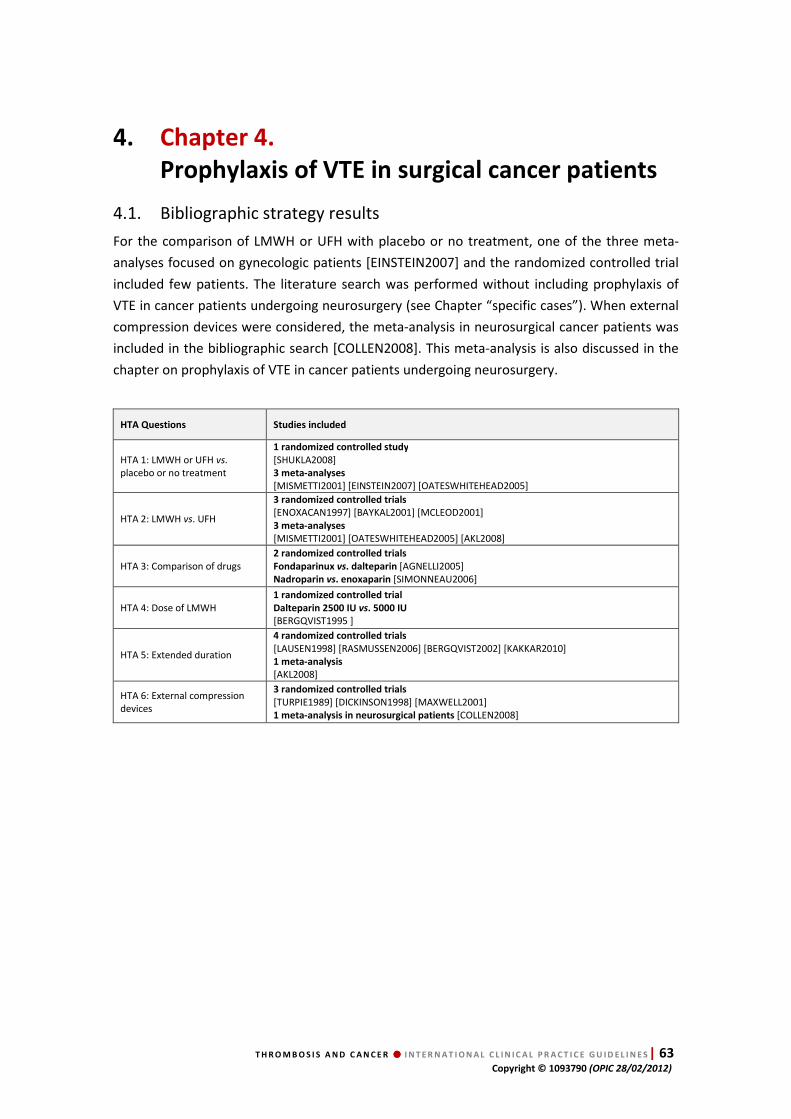
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 63 Copyright © 1093790 (OPIC 28/02/2012)
4. Chapter 4.
Prophylaxis of VTE in surgical cancer patients
4.1. Bibliographic strategy results
For the comparison of LMWH or UFH with placebo or no treatment, one of the three meta-
analyses focused on gynecologic patients [EINSTEIN2007] and the randomized controlled trial
included few patients. The literature search was performed without including prophylaxis of
VTE in cancer patients undergoing neurosurgery (see Chapter “specific cases”). When external
compression devices were considered, the meta-analysis in neurosurgical cancer patients was
included in the bibliographic search [COLLEN2008]. This meta-analysis is also discussed in the
chapter on prophylaxis of VTE in cancer patients undergoing neurosurgery.
HTA Questions Studies included
HTA 1: LMWH or UFH vs. placebo or no treatment
1 randomized controlled study
[SHUKLA2008] 3 meta-analyses
[MISMETTI2001] [EINSTEIN2007] [OATESWHITEHEAD2005]
HTA 2: LMWH vs. UFH
3 randomized controlled trials
[ENOXACAN1997] [BAYKAL2001] [MCLEOD2001] 3 meta-analyses
[MISMETTI2001] [OATESWHITEHEAD2005] [AKL2008]
HTA 3: Comparison of drugs 2 randomized controlled trials
Fondaparinux vs. dalteparin [AGNELLI2005] Nadroparin vs. enoxaparin [SIMONNEAU2006]
HTA 4: Dose of LMWH 1 randomized controlled trial
Dalteparin 2500 IU vs. 5000 IU
[BERGQVIST1995 ]
HTA 5: Extended duration
4 randomized controlled trials
[LAUSEN1998] [RASMUSSEN2006] [BERGQVIST2002] [KAKKAR2010] 1 meta-analysis
[AKL2008]
HTA 6: External compression devices
3 randomized controlled trials
[TURPIE1989] [DICKINSON1998] [MAXWELL2001] 1 meta-analysis in neurosurgical patients [COLLEN2008]

64 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
4.2. Data extraction
Table 16 Randomized controlled trials - LMWH or UFH vs. placebo or no treatment and LMWH vs. UFH
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[ENOXACAN1997]
Double-blind study Apr 1993 - Feb 1995
Bleeding 1115/1116 patients
VTE: 631/631 patients
Three months
Patients >40 years. Elective open surgery for abdominal or pelvic cancer (gastrointestinal, urological, gynecological) Surgery >45 min
Arm A: UFH 5000 IU x 3/day Arm B: Enoxaparin 40 mg x1/day + placebo x2/day For 10±2 days
Beginning of treatment: H-2
Asymptomatic DVT detected by phlebography at Day 10±2 + symptomatic proven DVT or PE Arm A: 58/319 (18.2%) Arm B: 46/312 (14.7%) p=NS
Major bleeding Arm A: 16/560 (2.9%) Arm B: 23/550 (4.1%); p=NS
Minor bleeding Arm A: 80/560 (14.3%) Arm B: 81/550 (14.6%); p=NS
Transfusion requirement Arm A: 242/560 (43.2%) Arm B: 284/550 (51.2%); p=NS
Day 10±2 Arm A: 7/560 (12.5%) Arm B: 4/550 (7.3%)
At 3 months Arm A: 27/560 (4.9%) Arm B: 22/550 (4%)
[BAYKAL2001]
Double-blind study 1998 - 1999
102/102 patients Arm A: 9.7 days Arm B: 9.4 days
Patients undergoing pelvic and para-aortic node dissection for gynecologic cancer
Arm A: Enoxaparin 2500 IU/day Arm B: UFH 5000 IU 3/day
Beginning of treatment: H-2
Clinically significant events Arm A: 0/47 Arm B: 0/55 p not specified
Wound hematoma + hemorrhage Arm A: 0/47; Arm B: 0/55; p=NS
Intraoperative blood loss Arm A: 915 mL; Arm B: 798 mL; p=NS
Blood transfusion Arm A: 1.43 units; Arm B: 1.2 units; p=NS
Decrease in hematocrit Arm A: 10.3 g/L; Arm B: 7.6 g/L; p=NS
Not specified
[MCLEOD2001]
Double-blind study Not specified
Efficacy 936/1349 patients
Safety 1296/1349 patients
10 days Adult patients undergoing colorectal resection or rectal dissection Surgery under general anesthesia and lasting >1 h Cancer patients: n=475/1349
Arm A: UFH 5000 IU 3/day Arm B: Enoxaparin 40 mg + 2 SC injections of placebo
Treatment for up to 10 days
Beginning of treatment: H-2
All VTE (DVT + PE): Day-9 bilateral venography or earlier if symptoms + if suspected PE perfusion/ventilation lung scintigraphy and if non-conclusive Doppler US, venography or angiography
VTE all patients Arm A: 44/468 (9.4%); Arm B: 44/468 (9.4%) 95%CI of the difference: [0±3.7%] VTE cancer patients Arm A: 39/234 (16.9%); Arm B: 33/241 (13.9%); p=NS
No data for cancer patients
All bleeding events Arm A: 42/643 (6.5%); Arm B: 68/653 (10.4%); p=0.02
Major bleeding events Arm A: 10/643 (1.5%) Arm B: 18/653 (2.7%); p=NS
Minor bleeding events Arm A: 32/643 (5.0%) Arm B: 52/653 (8.0%); p=0.03
Not specified
[SHUKLA2008)
Controlled trial Mar 2002 - Jan 2004
99/99 patients 6 days Colorectal surgery for cancer under general anesthesia Lithotomy position Age >30 years No DVT on preoperative Doppler US
Arm A: Dalteparin 2500 IU SC for 6±1 days Arm B: No prophylaxis
Beginning of treatment: H-2
Symptomatic DVT or PE and asymptomatic DVT on duplex ultrasonography at Day 6 Arm A: 0/51 Arm B: 0/48
Blood loss: Arm A: 506 mL Arm B: 445 mL; p=NS
No reintervention for bleeding
No death
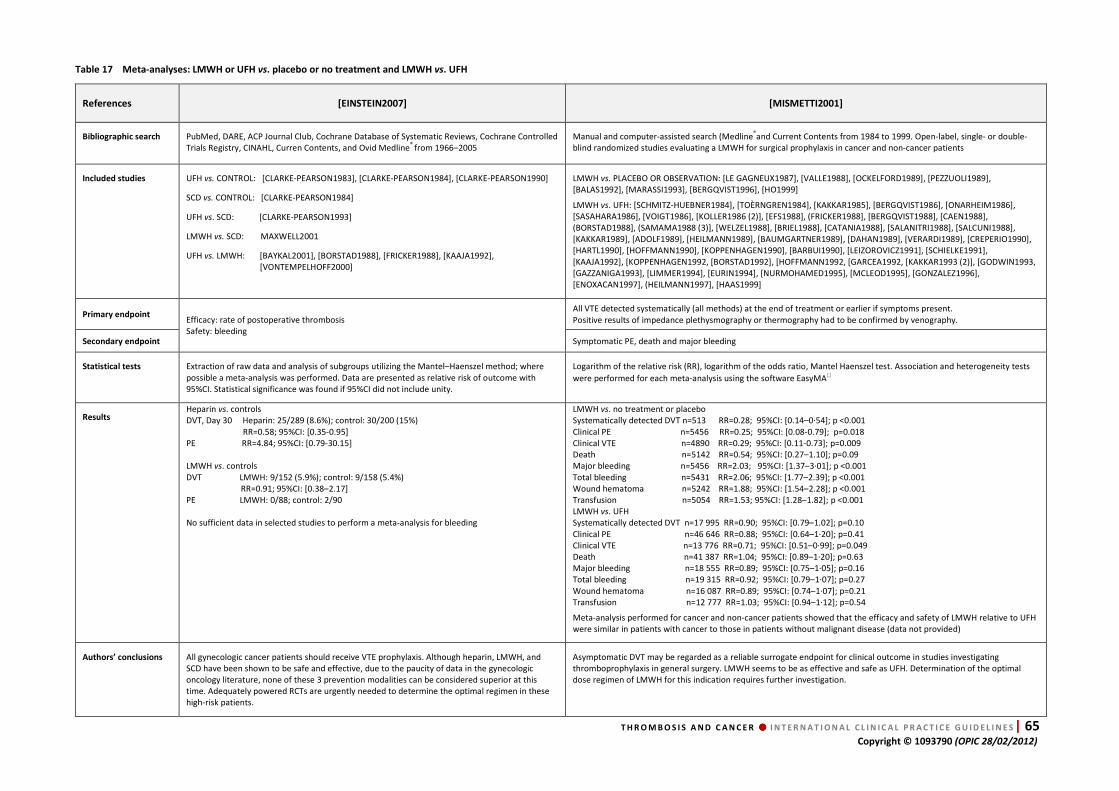
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 65 Copyright © 1093790 (OPIC 28/02/2012)
Table 17 Meta-analyses: LMWH or UFH vs. placebo or no treatment and LMWH vs. UFH
References [EINSTEIN2007] [MISMETTI2001]
Bibliographic search PubMed, DARE, ACP Journal Club, Cochrane Database of Systematic Reviews, Cochrane Controlled Trials Registry, CINAHL, Curren Contents, and Ovid Medline® from 1966–2005
Manual and computer-assisted search (Medline®and Current Contents from 1984 to 1999. Open-label, single- or double-blind randomized studies evaluating a LMWH for surgical prophylaxis in cancer and non-cancer patients
Included studies UFH vs. CONTROL: [CLARKE-PEARSON1983], [CLARKE-PEARSON1984], [CLARKE-PEARSON1990]
SCD vs. CONTROL: [CLARKE-PEARSON1984]
UFH vs. SCD: [CLARKE-PEARSON1993]
LMWH vs. SCD: MAXWELL2001
UFH vs. LMWH: [BAYKAL2001], [BORSTAD1988], [FRICKER1988], [KAAJA1992], [VONTEMPELHOFF2000]
LMWH vs. PLACEBO OR OBSERVATION: [LE GAGNEUX1987], [VALLE1988], [OCKELFORD1989], [PEZZUOLI1989], [BALAS1992], [MARASSI1993], [BERGQVIST1996], [HO1999]
LMWH vs. UFH: [SCHMITZ-HUEBNER1984], [TOÈRNGREN1984], [KAKKAR1985], [BERGQVIST1986], [ONARHEIM1986], [SASAHARA1986], [VOIGT1986], [KOLLER1986 (2)], [EFS1988], (FRICKER1988], [BERGQVIST1988], [CAEN1988], (BORSTAD1988], (SAMAMA1988 (3)], [WELZEL1988], [BRIEL1988], [CATANIA1988], [SALANITRI1988], [SALCUNI1988], [KAKKAR1989], [ADOLF1989], [HEILMANN1989], [BAUMGARTNER1989], [DAHAN1989], [VERARDI1989], [CREPERIO1990], [HARTL1990], [HOFFMANN1990], [KOPPENHAGEN1990], [BARBUI1990], [LEIZOROVICZ1991], [SCHIELKE1991], [KAAJA1992], [KOPPENHAGEN1992, [BORSTAD1992], [HOFFMANN1992, [GARCEA1992, [KAKKAR1993 (2)], [GODWIN1993, [GAZZANIGA1993], [LIMMER1994], [EURIN1994], [NURMOHAMED1995], [MCLEOD1995], [GONZALEZ1996], [ENOXACAN1997], (HEILMANN1997], [HAAS1999]
Primary endpoint Efficacy: rate of postoperative thrombosis Safety: bleeding
All VTE detected systematically (all methods) at the end of treatment or earlier if symptoms present. Positive results of impedance plethysmography or thermography had to be confirmed by venography.
Secondary endpoint Symptomatic PE, death and major bleeding
Statistical tests Extraction of raw data and analysis of subgroups utilizing the Mantel–Haenszel method; where possible a meta-analysis was performed. Data are presented as relative risk of outcome with 95%CI. Statistical significance was found if 95%CI did not include unity.
Logarithm of the relative risk (RR), logarithm of the odds ratio, Mantel Haenszel test. Association and heterogeneity tests
were performed for each meta-analysis using the software EasyMA
Results Heparin vs. controls DVT, Day 30 Heparin: 25/289 (8.6%); control: 30/200 (15%) RR=0.58; 95%CI: [0.35-0.95] PE RR=4.84; 95%CI: [0.79-30.15] LMWH vs. controls DVT LMWH: 9/152 (5.9%); control: 9/158 (5.4%) RR=0.91; 95%CI: [0.38–2.17] PE LMWH: 0/88; control: 2/90 No sufficient data in selected studies to perform a meta-analysis for bleeding
LMWH vs. no treatment or placebo Systematically detected DVT n=513 RR=0.28; 95%CI: [0.14–0·54]; p <0.001 Clinical PE n=5456 RR=0.25; 95%CI: [0.08-0.79]; p=0.018 Clinical VTE n=4890 RR=0.29; 95%CI: [0.11-0.73]; p=0.009 Death n=5142 RR=0.54; 95%CI: [0.27–1.10]; p=0.09 Major bleeding n=5456 RR=2.03; 95%CI: [1.37–3·01]; p <0.001 Total bleeding n=5431 RR=2.06; 95%CI: [1.77–2.39]; p <0.001 Wound hematoma n=5242 RR=1.88; 95%CI: [1.54–2.28]; p <0.001 Transfusion n=5054 RR=1.53; 95%CI: [1.28–1.82]; p <0.001 LMWH vs. UFH Systematically detected DVT n=17 995 RR=0.90; 95%CI: [0.79–1.02]; p=0.10 Clinical PE n=46 646 RR=0.88; 95%CI: [0.64–1·20]; p=0.41 Clinical VTE n=13 776 RR=0.71; 95%CI: [0.51–0·99]; p=0.049 Death n=41 387 RR=1.04; 95%CI: [0.89–1·20]; p=0.63 Major bleeding n=18 555 RR=0.89; 95%CI: [0.75–1·05]; p=0.16 Total bleeding n=19 315 RR=0.92; 95%CI: [0.79–1·07]; p=0.27 Wound hematoma n=16 087 RR=0.89; 95%CI: [0.74–1·07]; p=0.21 Transfusion n=12 777 RR=1.03; 95%CI: [0.94–1·12]; p=0.54
Meta-analysis performed for cancer and non-cancer patients showed that the efficacy and safety of LMWH relative to UFH were similar in patients with cancer to those in patients without malignant disease (data not provided)
Authors’ conclusions All gynecologic cancer patients should receive VTE prophylaxis. Although heparin, LMWH, and SCD have been shown to be safe and effective, due to the paucity of data in the gynecologic oncology literature, none of these 3 prevention modalities can be considered superior at this time. Adequately powered RCTs are urgently needed to determine the optimal regimen in these high-risk patients.
Asymptomatic DVT may be regarded as a reliable surrogate endpoint for clinical outcome in studies investigating thromboprophylaxis in general surgery. LMWH seems to be as effective and safe as UFH. Determination of the optimal dose regimen of LMWH for this indication requires further investigation.

66 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 17 Meta-analyses: LMWH or UFH vs. placebo or no treatment and LMWH vs. UFH (continued)
References [OATESWHITEHEAD2005] [AKL2008D]
Bibliographic search Randomized controlled trials comparing treatments for the prevention of postoperative VTE after major gynecological surgery
Medline®
- 1966 to April 2003, Embase® - 1980 to April 2003, CINAHL - 1982 to April 200
Medline®
from 1966, Embase® from 1980, ISI Web of Science, and CENTRAL (The Cochrane Central Register of Controlled
Trials), abstracts from ASCO and ASH congress in January 2007
Included studies [BAYKAL2001], [CLARKE-PEARSON1983], [CLARKE-PEARSON1990], [HEILMANN1989], [HEILMANN1998], [STEINER1989], [TABERNER1978], [VONTEMPELHOFF1997]
No study evaluating VKA or aspirin prophylaxis
[ONARHEIM1986], (FRICKER1998], (EFS1988], [BERGQVIST1990], [DAHAN1990], [GALLUS1993], [GODWIN1993], [ENOXACAN1997], [VON TEMPELHOFF1997], [HEILMANN1998], [VONTEMPELHOFF2000], [BAYKAL2001], [BONCINELLI2001], [MCLEOD2001],
Primary endpoint Incidence of identified DVT by either venography, 125I-fibrinogen-uptake test, or Doppler US. Incidence of PE identified by either ventilation perfusion lung scan, pulmonary angiogram, or post-mortem examination
Efficacy: VTE Safety: death, thrombocytopenia and bleeding
Secondary endpoint Death resulting from confirmed thromboembolism identified by either ventilation perfusion lung scan, pulmonary angiogram, or post-mortem examination
Statistical tests For dichotomous data, calculation of odds ratio with 95%CI, combination of OR for meta-analysis with the Peto-modified Mantel-Haenszel method. Calculation of summary statistics with a fixed-effect and random-effects model. Analysis of the heterogeneity of studies by inspecting the scatter data points and the overlap in the confidence intervals and by checking the results of the Chi-Square test.
For categorical variables, calculation of the pooled relative risk (RR). For continuous variables calculation of the standardized mean difference (SMD). Measure of the homogeneity across trial results using the I2 test. Results pooled using random effects
Results PE, all patients Heparin: 5/289 (1.7%); placebo: 1/200 (0.5%); OR=2.13; 95%CI: [0.42-10.91] LMWH: 8/204 (3.8%); UFH: 5/225 (2.2%); OR=1.82; 95%CI: [0.57-5.80]
PE, cancer patients LMWH: 7/139 (5.0%); UFH: 4/157 (2.5%); OR=2.03; 95%CI: [0.56-7.28]
DVT, cancer patients Heparin: 17/292 (5.8%); placebo: 32/204 (15.6%); OR=0.30; 95%CI: [0.10-0.90] LMWH: 15/289 (5.2%); UFH: 15/307 (4.8%); OR=1.10; 95%CI: [0.25-4.83]
Too many endpoints for bleeding complications (wound hematoma, postoperative blood loss, blood transfusion, injection site hematoma, total transfusion, major bleeding) with too few data for each one to provide results.
Meta-analyses of UFH and LMWH showed no statistical difference in any comparison. No study compared aspirin alone to placebo, heparin or warfarin. There was a statistically significant increase in injection-site hematomas associated with heparin compared to placebo (OR=0.30; 95%CI: [0.10-0.89].
DVT (symptomatic + asymptomatic any search strategy) LMWH vs. UFH x2/day - LMWH: 41/1222 (3.3%); UFH: 65/961 (6.7%); RR=0.66; 95%CI: [0.44-0.99] LMWH vs. UFH x3/day - LMWH: 44/971 (4.5%); UFH: 53/980 (5.4%); RR=0.78; 95%CI: [0.53-1.15] LMWH vs. UFH global - LMWH: 85/2193 (3.9%); UFH: 118/1941 (6.0%); RR=0.72; 95%CI: [0.55-0.94]
Death LMWH: 67/1480 (4.6%); UFH: 79/1528 (5.1%); RR=0.88; 95%CI: [0.65-1.19]
Minor bleeding 3 studies; RR=0.88; 95%CI: [0.47-1.66]
Major bleeding 6 studies; RR=0.95; 95%CI: [0.51-1.77]
Thrombocytopenia 3 studies; RR=1.18; 95%CI: [0.49-2.81] (no case of HIT)
Authors’ conclusions The meta-analysis of heparin vs. placebo found a statistically significant decrease in the number of DVT in both the all women group (including those with and without malignancy) (OR=0.30; 95%CI: [0.12-0.76]) and the subgroup of only women with malignancy (OR=0.30; 95%CI: [0.10-0.89]). There was no significant difference in the incidence of PE. Oral warfarin reduced DVT compared to placebo in all women (OR=0.22; 95%CI: [0.06-0.86]) and in women with malignancy (OR=0.18; 95%CI: [0.04-.87]).
There was no difference in mortality rate between patients with cancer receiving perioperative thromboprophylaxis with LMWH vs. UFH. Further trials are needed to evaluate the benefits and the harms of different heparin thromboprophylaxis strategies in this cancer population.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 67 Copyright © 1093790 (OPIC 28/02/2012)
Table 18 Randomized controlled trials - Comparison of drugs and dose of LMWH
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[BERGQVIST1995]
Double-blind study Mar 1988 - Nov 1991
Intent to treat 1303/1375 patients
Correct prophylaxis 1154/1375 patients
Not specified Patients >40 years undergoing major elective abdominal surgery (>30 min) 70% of patients undergoing surgery for cancer
Arm A: Dalteparin 2500 IU/day Arm B: Dalteparin 5000 IU/day
Treatment for 8 days
Beginning of treatment: evening before surgery
DVT diagnosed with I-labeled fibrinogen uptake performed daily for 7 days or until discharge or VTE occurrence
Intent to treat Arm A: 14,9% Arm B: 8.5% 95%CI of the difference: [2.1-8.9]; p<0.001
Correct prophylaxis Arm A: 15.1% Arm B: 8.8% 95%CI of the difference: [2.1-9.4]; p=0.001
Bleeding complications (major and minor bleeding, wound hematoma, surgical bleeding) Arm A: 3.6% Arm B: 4.6% 95%CI of the difference: [-2.8-1.4]; p >0.05
Cancer and non-cancer patients Arm A: 12% Arm B: 15%
[AGNELLI2005]
Double-blind study Oct 2001 - Oct 2002
Total population Safety 2858/2927 patients Efficacy 2048/2927 patients
Cancer patients Efficacy 1408/1941 patients Safety 1841/1941 patients
30 days Abdominal surgery >45 min under general anesthesia Patients >60 years or >40 years + one additional risk factor (cancer)
Arm A: Fondaparinux 2.5 mg/day Arm B: Dalteparin 5000 IU/day
Treatment for 5-9 days
Beginning of treatment: Fondaparinux: H+6 Dalteparin H-2
Symptomatic and asymptomatic VTE (bilateral ascending contrast venography at Day 5 to Day 10 + DVT and PE confirmed by objective tests)
Arm A: 33/696 (4.7%) Arm B: 55/712 (7.7%) Relative risk reduction: 38.6%; 95%CI: [6.7-59·6]
Major bleeding Arm A: 32/954 (3.4%) Arm B: 25/987 (2.5%)
Total population on Day 32 Arm A: 40/1433 (2.8%) Arm B: 55/1425 (3.9%)
[SIMONNEAU2006]
Double-blind study Sep 1994 - Feb 1999
Efficacy 950/1296 patients
Safety 1271/1296 patients
60 days Elective resection of colorectal adenocarcinoma under general anesthesia No contraindication for anticoagulant therapy
Arm A: 2850 anti-FXa IU of nadroparin + placebo enoxaparin Arm B: 4000 anti-FXa IU of enoxaparin + placebo nadroparin
Treatment for 7-11 days
Beginning of treatment: H-4 to H-2
Primary efficacy outcome: DVT detected by bilateral venography or documented
Symptomatic DVT or PE up to Day 12 All VTE at Day 12 (primary endpoint) Arm A: 74/464 (15.9%) Arm B: 61/486 (12.6%) RR=1.27; 95%CI: [0.93–1.74]
Symptomatic VTE at D12 Arm A: 1/464 (0.2%) Arm B: 9/486 (1.4%) RR=0.12; 95%CI: [0.01-0.92]
Symptomatic VTE at Day 60 Arm A: 4/464 (0.6%) Arm B: 13/486 (2.1%) p=NS
Major bleeding Arm A: 47/643 (7.3%) Arm B: 72/628 (11.5%) RR=0.64; 95%CI: [0.45-0.91]; p=0.012
Severe thrombocytopenia Arm A: 9/643 (1.4%) Arm B: 8/628 (1.3%) p=NS
Death from any cause on Day 60 Arm A: 23/653 (3.5%) Arm B: 23/635 (3.6%)

68 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 19 Randomized controlled trials - Duration of prophylaxis
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[LAUSEN1998]
Controlled trial Nov 1991 - May 1993
Arm A: 58/87 patients Arm B: 60/89 patients
28 days Major elective abdominal or non-cardiac thoracic operations Duration >1 hour Patients >18 years No contraindication to LMWH No use of other anticoagulants
Cancer patients: Arm A: 39/58; Arm B: 42/60
Tinzaparin 3500 IU/day for 7 days + high-length graded CS then:
Arm A: tinzaparin 3500 IU/day for 3 weeks Arm B: observation
Beginning of treatment: H-2
Bilateral venography on Day 28 or earlier if symptoms present. If suspected PE, perfusion/ventilation lung scintigraphy.
Arm A: 3/58 (5.2%); 95%CI: [1-14] Arm B: 6/60 (10%); 95%CI: [4%-21] p=NS
Reoperation: 12/118
No differences between groups for anastomotic leaks, wound dehiscence, wound infections, abscesses, or pneumonia No data for each group
Not specified
[BERGQVIST2002]
Double-blind study Oct 1998 - Jun 2000
Bleeding complications 501/501 patients
Recurrent VTE 332/332 patients
3 months Patients >40 years. Elective open surgery for cancer (gastrointestinal other than the esophagus, genitourinary tract, or female reproductive organs Surgery >45 min
Enoxaparin 40 mg/day Placebo Arm A: Enoxaparin for 6-10 days + placebo for 19-21 days Arm B: Enoxaparin for 25-31 days
Beginning of treatment: H-14 to H-10
Phlebography between Days 25 and 31 Arm A: 20/167 (12%) Arm B: 8/165 (4,8%); p=0.02
At 3 months Arm A: 23/167 (13.8%) Arm B: 9/165 (5.5%); p=0.01
Double-blind phase Minor bleeding Arm A: 9/248 (3.6%) Arm B: 12/253 (4.7%); p=NS Major bleeding Arm A: 0/248 Arm B: 1/253(0.4%); p=NS
At 3 months Minor bleeding Arm A: 9/248 (3.6%) Arm B: 12/253 (4.7%); p=NS Major bleeding Arm A: 1/248 (0.4%) Arm B: 3/253 (1.2%)
Double-blind phase No death At 3 months Arm A: 6/248 (3.6%) Arm B: 3/253 (1.8%)
[RASMUSSEN2006]
Controlled trial Jan 1997 - Jun 2003
Arm A: 165/205 patients Arm B: 178/222 patients
28 days Patients >18 years Open abdominal surgical intervention Surgery >1 hour
Cancer patients Arm A: 123/205 (60%); Arm B: 124/222 (56%)
Dalteparin 5000 IU + GCS for 7 days
After day 7 Arm A: dalteparin 5000 IU for 21 days Arm B: observation
Beginning of treatment: the evening of surgery and H-2
Asymptomatic DVT detected by venography (Day 28), symptomatic DVT or PE verified by objective means or by autopsy Arm A: 12/165 (7.3%) Arm B: 29/178 (16.3%) Risk Reduction: 55%; 95%CI: [15-76]; p=0.012
DVT Arm A: 12/165 (7.3%) Arm B: 26/178 (14.9%) Risk Reduction: 51%; 95%CI: [6-74]; p=0.027
Major bleeding Arm A: 1/205 Arm B: 4/222
Arm A: 22/205 Arm B: 17/222
[KAKKAR2010]
Double-blind study Jul 2005 - Feb 2008
Efficacy patients 488/625
Safety patients 625/625
22 days Patients aged 40 years or older Open, curative or palliative surgery for a malignant disease of the gastrointestinal (excluding esophagus) tract, genitourinary tract or female reproductive organs Duration of surgery >30 min
Cancer patients Arm A: 39/58; Arm B: 40/60
Bemiparin 3500 IU (0.2 mL) for 8±2 days then:
Arm A: bemiparin 3500 IU (0.2 mL) for 20 days Arm B: placebo (0.9% sodium chloride, 0.2 mL) for 20 days Beginning of treatment: H+6
Bilateral venography on Day 18-22 Endpoint: phlebographic and symptomatic DVT, PE and death at the end of double-blind phase
Arm A: 25/248 (10.1%) Arm B: 32/240 (13.3%) RR=24.4; 95%CI: [23.7-53.8]; p=0.26
Only DVT Arm A: 19/248 (7.7%) Arm B: 29/240 (12.1%) RR = 36.6; 95%CI: [10.0-63.4]; p=0.10
During double-blind period
Major bleeding (primary safety endpoint) 2/315 (0.6%) vs. 1/310 (0.3%); p=NS
Minor bleeding 1/315 (0.3) vs. 1/310 (0.3%); p=NS
All-cause death Arm A: 8/248 (3.2%) Arm B: 6/240 (2.5%) RR= -29.0%; 95%CI: [-266.4-54.6]; p=0.63

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 69 Copyright © 1093790 (OPIC 28/02/2012)
Table 20 Extended prophylaxis meta-analysis
References [AKL2008E]
Bibliographic search Medline® from 1966, Embase® from 1980, ISI the Web of Science, and The Cochrane Central Register of Controlled Trials in January 2007
Included studies [JORGENSEN2002], [BERGQVIST2002], [RASMUSSEN2006]
Primary endpoint Efficacy: VTE
Secondary endpoint Safety: death and bleeding
Statistical tests Not specified in the paper and in the appendix
Results DVT screening venography (198 patients, 1 study) RR=0.21; 95%CI: [0.05-0.94] - low evidence
Major bleeding (501 patients, 1 study) RR=2.94; 95%CI: [0.12-71.85] - low evidence
Minor bleeding (501 patients, 1 study) RR=1.31; 95%CI: [0.56-3.05] - moderate evidence
Mortality (501 patients, 1 study) RR=0.49; 95%CI: [0.12-1.94] - low evidence
Authors’ conclusions There is limited and low-quality evidence that extended duration LMWH for perioperative thromboprophylaxis reduces DVT in patients with cancer undergoing major abdominal or pelvic surgery. More and better quality evidence is needed to justify extended regimens.

70 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 21 Randomized controlled trials: external compression device with intermittent compression device (ICD)
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[TURPIE1989]
Not specified 173/239 patients 3 months Patients >16 years undergoing
surgery for a brain tumor, spinal cord tumor, head injury, spinal cord injury or subarachnoid hemorrhage
Cancer patients Arm A: 38/80 Arm B: 39/78 Arm C: 40/81
Arm A: GCS for 14 days Arm B: GCS for 14 days+IPC for 7 days Arm C: control
125I-labeled fibrinogen scanning x1/day until discharge + impedance plethysmography on Days 3, 5, 7, 9, 11, 14 with double-blind interpretation of results
Arm A: 7/80 (8.8%) Arm B: 7/79 (9%) Arm C: 16/81 (19.8%) p=0.023 A vs. C p=0.027 B vs. C p=0.028 A + B vs. C
Compliance with treatment Arm A: 77/80 (96%) Arm B: 69/79 (87%)
Arm A: 10/80 (12.5%) Arm B: 4/79 (50.6%) Arm C: 4/81 (49.4%)
[DICKINSON1998]
Jan 1990 - Dec 1992 66/66 patients 1 month Patients 18 years of age or older
with an intracranial neoplasm and undergoing craniotomy
Arm A: SCD alone Arm B: enoxaparin 30 mg/day Arm C: SCD+enoxaparin 30 mg/day Duration: up to discharge
Beginning of treatment: during anesthesia
Venous duplex ultrasonographic examinations at Day 1-3, Day 5-7, Day 10-14, Month 1 Arm A: 3/22 (13.6%) Arm B: 1/21 (4.7%) Arm C: 2/23 (8.7%) p=NS
Major bleeding Arm A: 0/22 (0%) Arm B: 2/21 (9.5%) Arm C: 3/23 (13.1%) Difference between enoxaparin groups and SCD group p=0.024
Intracranial bleeding LMWH: 4/44 (9.1%) SCD: 0/22 (0%); p=0.29
Arm A: 1/22 (4.5%) Arm B: 1/21 (4.8%) Arm C: 0/23 (0%)
[MAXWELL2001]
Not specified 211/231 patients Hospitalization Patients >40 years
Major abdominal or pelvic surgery for a known or suspected gynecologic malignancy
Arm A: external pneumatic compression sleeves, beginning at induction of anesthesia, for 5 days, then temporarily removed when the patient is ambulatory Arm B: dalteparin 2500 IU postoperatively and then 12 h after, then 5000 IU/day for 5 days or until discharge
Beginning of treatment: H-2
Doppler US at Day 3 to 5 Arm A: 1/106 (1%) Arm B: 2/106 (2%) p=NS
Blood loss Arm A: m=350 mL, >2000 mL: n=3 Arm B: m=350 mL, >2000 mL: n=4
Transfusions in operating room Arm A: 22/106 (20.7%) Arm B: 20/105 (19%)
Postoperative transfusions Arm A: 12/106 (11.3%) Arm B: 13/105 (12.4%)
Not specified

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 71 Copyright © 1093790 (OPIC 28/02/2012)
Table 22 Meta-analysis of studies in neurosurgical cancer patients: external compression device
References [COLLEN2008]
Bibliographic search
Published literature (from 1960 through August 2007) Medline® ; PubMed; Cochrane RCT; Embase®; Biosis; PASCAL; Sci Search; IPA; and Computer Retrieval of Information on Scientific Projects
Included studies
Patients included in randomized trials or prospective cohort studies evaluating pharmacologic VTE prophylaxis (with UFH or LMWH) or in randomized trials or prospective cohort studies evaluating mechanical VTE prophylaxis (with ICD or CS) [AGNELLI1998], [BARNETT1977], [BOSTROM1986], [BUCCI1989], [BYNKE1987], [CERRATO1978], [CONSTANTINI2001], [DICKINSON1998], [EPSTEIN2005], [EPSTEIN2006], [FRIM1992], [GERLACH2003], [GOLDHABER2002], [GRUBER1984], [KURTOGLU2004], [MACDONALD1999], [MACDONALD2003], [NORWOOD2002], [NURMOHAMED1996], [PAOLETTI1989], [PRESTAR1992], [ROKITO1996], [SKILLMAN1978], [SMITH1994], [TURPIE1989], [VOTH1992], [WAUTRECHT 1996], [WEN198], [WOOD1997]
Primary endpoint Objective assessment of DVT
Secondary endpoint Major and minor bleeding, death
Statistical tests
RRs were pooled using the Der Simonian and Laird random-effects method. Calculation of the overall rate of events. Calculation of the variance for each outcome using the binomial method Heterogeneity was assessed visually by Galbraith plots, as well as Q statistics (Chi-Square test) and the I2 statistic.
Results
ICD vs. CS: 3 studies DVT RR=0.81; 95%CI: [0.32-1.78] PE RR=0.49; 95%CI: [0.08-2.80] ICD vs. placebo: 2 studies DVT RR=0.41; 95%CI: [0.21-0.78] PE RR=0.37; 95%CI: [0.03-4.06] LMWH vs. CS: 2 studies DVT RR=0.60; 95%CI: [0.44-0.81] PE RR=0.29; 95%CI: [0.05-1.85] LMWH vs. ICD: 2 studies DVT RR=0.79; 95%CI: [0.30-2.12] PE RR=1.62; 95%CI: [0.35-7.46] LMWH vs. UFH: 4 studies DVT RR=1.46; 95%CI: [0.61-3.51] PE RR=0.43; 95%CI: [0.08-2.41] UFH vs. placebo: 3 studies DVT RR=0.50; 95%CI: [0.11-2.38] PE RR=0.96; 95%CI: [0.10-9.06]
LMWH vs. non-pharmacologic management: 4 studies Minor bleeding RR=2.06; 95%CI: [1.07-3.96] Major bleeding RR=0.95; 95%CI: [0.18-5.09] ICH RR=1.97; 95%CI: [0.64-6.09] Death RR=0.96; 95%CI: [0.47-1.96]
UFH vs. non-pharmacologic management: 3 studies Minor bleeding RR=1.00; 95%CI: [0.48-2.11] Major bleeding RR=0.85; 95%CI: [0.12-5.99] ICH RR=2.11 95%CI: [0.39-11.31] Death RR=0.97; 95%CI: [0.13-7.37]
LMWH vs. UFH: 4 studies Minor bleeding RR=1.28; 95%CI: [0.64-2.59] Major bleeding RR=1.00; 95%CI: [0.18-5.74] ICH RR=1.78; 95%CI: [0.37-8.50] Death RR=0.72; 95%CI: [0.11-4.42]
Authors’ conclusions In a mixed neurosurgical population, LMWH and ECD are both effective in the prevention of VTE. Sensitivity analyses suggested that isolated high-risk groups, such as patients undergoing craniotomy for a brain neoplasm, may benefit from a combination of prophylactic methods, suggesting the need for a more individualized approach to these patients.
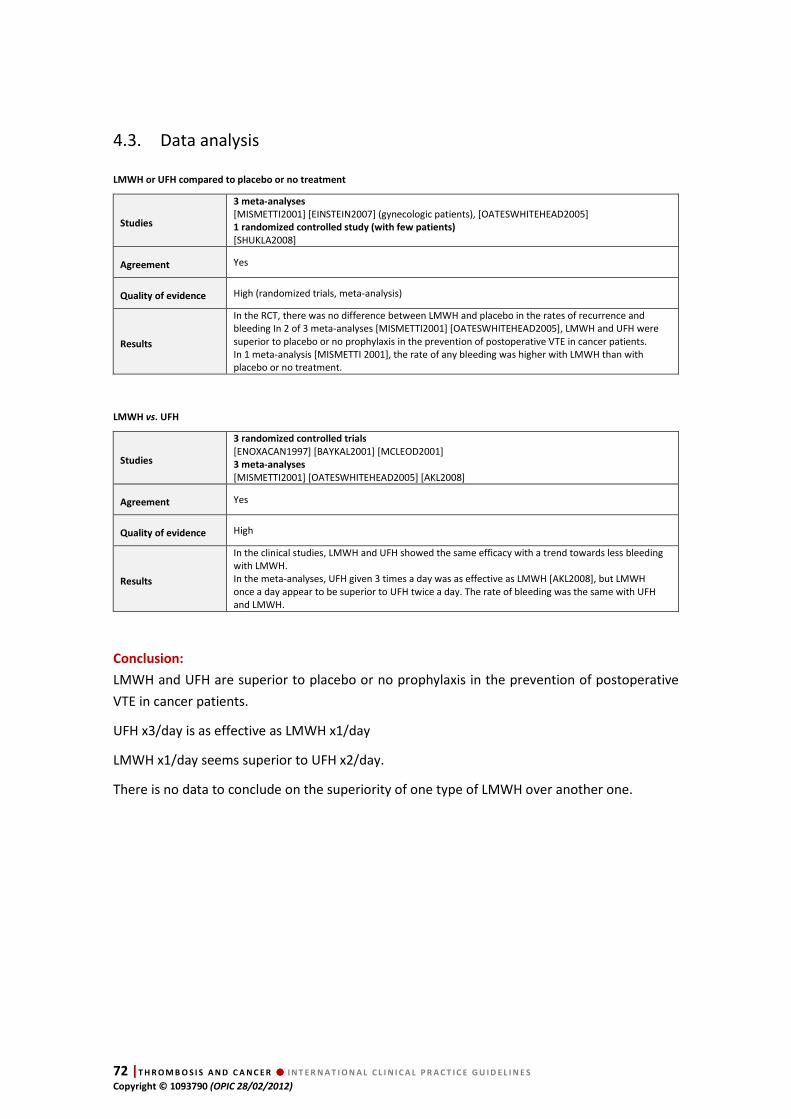
72 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
4.3. Data analysis LMWH or UFH compared to placebo or no treatment
Studies
3 meta-analyses
[MISMETTI2001] [EINSTEIN2007] (gynecologic patients), [OATESWHITEHEAD2005] 1 randomized controlled study (with few patients)
[SHUKLA2008]
Agreement Yes
Quality of evidence High (randomized trials, meta-analysis)
Results
In the RCT, there was no difference between LMWH and placebo in the rates of recurrence and bleeding In 2 of 3 meta-analyses [MISMETTI2001] [OATESWHITEHEAD2005], LMWH and UFH were superior to placebo or no prophylaxis in the prevention of postoperative VTE in cancer patients. In 1 meta-analysis [MISMETTI 2001], the rate of any bleeding was higher with LMWH than with placebo or no treatment.
LMWH vs. UFH
Studies
3 randomized controlled trials
[ENOXACAN1997] [BAYKAL2001] [MCLEOD2001] 3 meta-analyses
[MISMETTI2001] [OATESWHITEHEAD2005] [AKL2008]
Agreement Yes
Quality of evidence High
Results
In the clinical studies, LMWH and UFH showed the same efficacy with a trend towards less bleeding with LMWH. In the meta-analyses, UFH given 3 times a day was as effective as LMWH [AKL2008], but LMWH once a day appear to be superior to UFH twice a day. The rate of bleeding was the same with UFH and LMWH.
Conclusion:
LMWH and UFH are superior to placebo or no prophylaxis in the prevention of postoperative
VTE in cancer patients.
UFH x3/day is as effective as LMWH x1/day
LMWH x1/day seems superior to UFH x2/day.
There is no data to conclude on the superiority of one type of LMWH over another one.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 73 Copyright © 1093790 (OPIC 28/02/2012)
Comparison of drugs
Studies
2 randomized controlled trials
Fondaparinux vs. dalteparin [AGNELLI2005] Nadroparin vs. enoxaparin [SIMONNEAU2006]
Agreement Not applicable
Quality of evidence Low (randomized, indirectness for one study, imprecision because of a non-inferiority study with a secondary endpoint)
Results
Nadroparin (2850 IU) is at least as effective as enoxaparin (4000 IU) with less major bleeding In one study including two-thirds of cancer patients, fondaparinux compared to dalteparin is associated with less VTE recurrence and with a trend towards an increase in bleeding.
Conclusion
There is insufficient evidence to conclude on the superiority of fondaparinux over dalteparin
(1 study with two-thirds of cancer patients) or on the superiority of nadroparin over
enoxaparin (1 study showing the same rate of venous thromboembolic events but with a
difference in the rate of bleeding events).
Dose of LMWH
Studies
1 randomized controlled trial
Dalteparin 2500 IU vs. 5000 IU
[BERGQVIST1995 ]
Agreement Not applicable
Quality of evidence High (one randomized study but with a large effect size)
Results For prophylaxis a high dose of LMWH is superior to a low dose
Conclusion
One study with a large effect size showed that a high dosage of LMWH is superior to a low
dosage of LMWH in the prevention of VTE in surgical cancer patients.
Extended duration of prophylaxis
Studies
4 prospective randomized studies
[LAUSEN1998] [RASMUSSEN2006] [BERGQVIST2002] [KAKKAR2010] 1 meta-analysis
[AKL2008]
Agreement No: 2 negative studies (but one was stopped before the calculated number of patients was achieved), 2 positive studies
Quality of evidence Moderate (randomized trials, inconsistency, one study with limitations)
Results There is little evidence for better efficacy of extended prophylaxis, but a trend towards a higher risk of bleeding was reported in one study [BERGQVIST2002] .
Conclusion
Four weeks of LMWH reduced the rate of postoperative VTE after major laparotomy surgery in
cancer patients. The superiority of extended duration of LMWH (4 weeks) cannot be
generalized to all cancer patients undergoing major abdominal surgery for cancer, but may be
considered in selected patients without a high risk of bleeding.

74 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
External compression devices
Studies
3 randomized studies
[TURPIE1989] [DICKINSON1998] [MAXWELL2001] 1 meta-analysis in neurosurgical patients [COLLEN2008]
Agreement Not applicable (different external compression devices were used)
Quality of evidence
Low (randomized but serious study limitations due to the differences in study design, study population and the external compression device used, inconsistency and imprecisions, so move down two grades)
Results
To prevent VTE in major abdominal or pelvic surgery for gynecologic malignancies, ECD and LMWH appeared equivalent For prophylaxis after surgery for brain tumors:
• GCS + IPC had the same efficacy as GCS alone, and both were superior to no prophylaxis.
• In neurosurgical patients, LMWH were superior to ECD despite an increase of minor bleeding but with no increase in intracranial bleeding or in major bleeding.
Conclusion
External compression devices (ECD) are superior to no prophylaxis but inferior to LMWH.
There are insufficient data to conclude on the superiority of one type of ECD or one ECD
regimen over others.
4.4. Discussion
Cancer patients undergoing surgery have an increased risk of VTE as compared to those
without cancer. Therefore, VTE prophylaxis after surgery is warranted in cancer patients. The
risk is increased depending on the type of surgery. In general, it is commonly acknowledged
that surgeries with a high risk of VTE are laparotomy, laparoscopy, thoracotomy and brain
surgery lasting more than 30 minutes. Breast cancer surgery is considered to be associated
with a lower risk of VTE, even in the case of breast reconstruction [PANUCCI2009].
Several methods of prophylaxis have been investigated in cancer patients undergoing surgery:
low-molecular-weight heparins (LMWH), unfractionnated heparin (UFH) and external
compression devices (ECD). Three meta-analyses have shown that LMWH and UFH are both
superior to placebo or no prophylaxis in the prevention of VTE in cancer patients
[MISMETTI2001] [EINSTEIN2007] [OATESWHITEHEAD2005]. For VTE prophylaxis, both LMWH
and UFH have overall the same efficacy. However, LMWH once daily seem to be superior to
UFH twice daily. UFH three times daily is as effective as LMWH once daily. The use of LWMH
and UFH as VTE prophylaxis in cancer patients is acceptable with respect to bleeding risk. In
several studies in cancer patients undergoing major abdominal or pelvic surgery, the
occurrence of bleeding did not differ significantly, in terms of major and minor bleeding,
between LMWH and UFH [ENOXACAN1997] [BAYCAL2001] [MISMETTI2001]. The latter meta-
analysis did not only concern abdominal surgery [MISMETTI2001]. Of note, significantly more
bleeding events with LMWH vs. UFH were reported in one study [MCLEOD 2001].
Prophylaxis is started 12 to 2 hours before surgery and should be continued up to 7-10 days
after surgery. However, the optimal duration of VTE prophylaxis in cancer patients after
surgery remained to be determined. In patients undergoing major abdominal or pelvic surgery,
extended prophylaxis reduced the incidence of VTE in certain studies [BERQVIST2002]
[RASMUSSEN2006], but this finding was not confirmed in other studies [LAUSEN1998]
[KAKKAR2010]. Therefore, an extended duration (>4 weeks) of prophylaxis should be
considered in patients undergoing major abdominal surgery, especially those with a low
bleeding risk and a high risk of VTE recurrence.
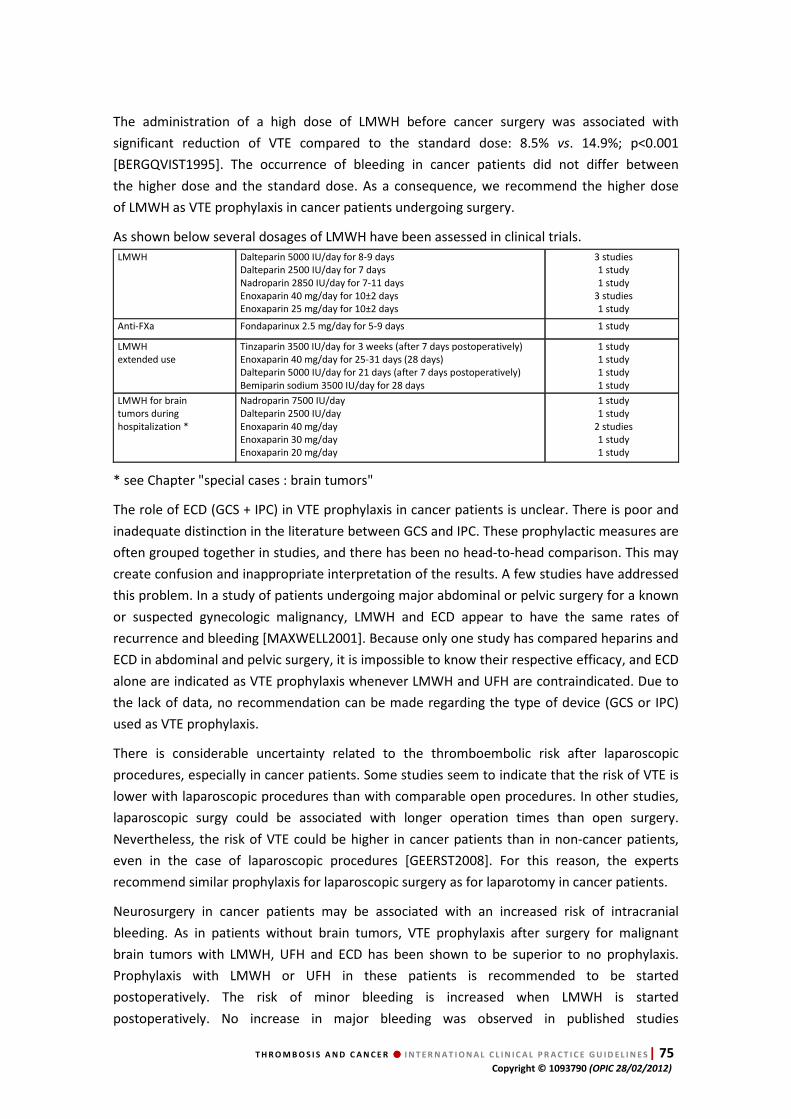
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 75 Copyright © 1093790 (OPIC 28/02/2012)
The administration of a high dose of LMWH before cancer surgery was associated with
significant reduction of VTE compared to the standard dose: 8.5% vs. 14.9%; p<0.001
[BERGQVIST1995]. The occurrence of bleeding in cancer patients did not differ between
the higher dose and the standard dose. As a consequence, we recommend the higher dose
of LMWH as VTE prophylaxis in cancer patients undergoing surgery.
As shown below several dosages of LMWH have been assessed in clinical trials.
LMWH Dalteparin 5000 IU/day for 8-9 days Dalteparin 2500 IU/day for 7 days Nadroparin 2850 IU/day for 7-11 days Enoxaparin 40 mg/day for 10±2 days Enoxaparin 25 mg/day for 10±2 days
3 studies 1 study 1 study
3 studies 1 study
Anti-FXa Fondaparinux 2.5 mg/day for 5-9 days 1 study
LMWH extended use
Tinzaparin 3500 IU/day for 3 weeks (after 7 days postoperatively) Enoxaparin 40 mg/day for 25-31 days (28 days) Dalteparin 5000 IU/day for 21 days (after 7 days postoperatively) Bemiparin sodium 3500 IU/day for 28 days
1 study 1 study 1 study 1 study
LMWH for brain tumors during hospitalization *
Nadroparin 7500 IU/day Dalteparin 2500 IU/day Enoxaparin 40 mg/day Enoxaparin 30 mg/day Enoxaparin 20 mg/day
1 study 1 study
2 studies 1 study 1 study
* see Chapter "special cases : brain tumors"
The role of ECD (GCS + IPC) in VTE prophylaxis in cancer patients is unclear. There is poor and
inadequate distinction in the literature between GCS and IPC. These prophylactic measures are
often grouped together in studies, and there has been no head-to-head comparison. This may
create confusion and inappropriate interpretation of the results. A few studies have addressed
this problem. In a study of patients undergoing major abdominal or pelvic surgery for a known
or suspected gynecologic malignancy, LMWH and ECD appear to have the same rates of
recurrence and bleeding [MAXWELL2001]. Because only one study has compared heparins and
ECD in abdominal and pelvic surgery, it is impossible to know their respective efficacy, and ECD
alone are indicated as VTE prophylaxis whenever LMWH and UFH are contraindicated. Due to
the lack of data, no recommendation can be made regarding the type of device (GCS or IPC)
used as VTE prophylaxis.
There is considerable uncertainty related to the thromboembolic risk after laparoscopic
procedures, especially in cancer patients. Some studies seem to indicate that the risk of VTE is
lower with laparoscopic procedures than with comparable open procedures. In other studies,
laparoscopic surgy could be associated with longer operation times than open surgery.
Nevertheless, the risk of VTE could be higher in cancer patients than in non-cancer patients,
even in the case of laparoscopic procedures [GEERST2008]. For this reason, the experts
recommend similar prophylaxis for laparoscopic surgery as for laparotomy in cancer patients.
Neurosurgery in cancer patients may be associated with an increased risk of intracranial
bleeding. As in patients without brain tumors, VTE prophylaxis after surgery for malignant
brain tumors with LMWH, UFH and ECD has been shown to be superior to no prophylaxis.
Prophylaxis with LMWH or UFH in these patients is recommended to be started
postoperatively. The risk of minor bleeding is increased when LMWH is started
postoperatively. No increase in major bleeding was observed in published studies

76 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
[DICKINSON1998]. There were five cases of bleeding complications (four cases of intracerebral
bleeding and one epidural hematoma) among the enoxaparin-treated patients, with no such
complications for the SCD-treated group, this difference being not statistically significant
[DICKINSON1998].
4.5. Recommendations – prophylaxis of VTE in surgical cancer patients R1. Use of LMWH once a day or low dose of UFH x3/day is recommended to prevent postoperative VTE in cancer patients.
Pharmacological prophylaxis should be started 12 to 2 hours preoperatively and continued for at least 7 to 10 days. There are
no data allowing conclusion on the superiority of one type of LMWH over another
Quality of evidence High
Balance between desirable and undesirable effects Overwhelming evidence of benefit
Values and preferences LMWH once a day is more convenient
Costs (resource allocation) Not considered
Level of recommendation Strong
R2. There is no evidence to support fondaparinux as an alternative to LMWH for the prophylaxis of postoperative VTE in cancer
patients
Quality of evidence Low
Balance between desirable and undesirable effects Undetermined
Values and preferences Similar
Costs (resource allocation) Not considered
Level of recommendation Weak
R3. Use of the highest prophylactic dose of LMWH to prevent postoperative VTE in cancer patients is recommended
Quality of evidence High
Balance between desirable and undesirable effects Favorable
Values and preferences Equal
Costs (resource allocation) Not considered
Level of recommendation Strong
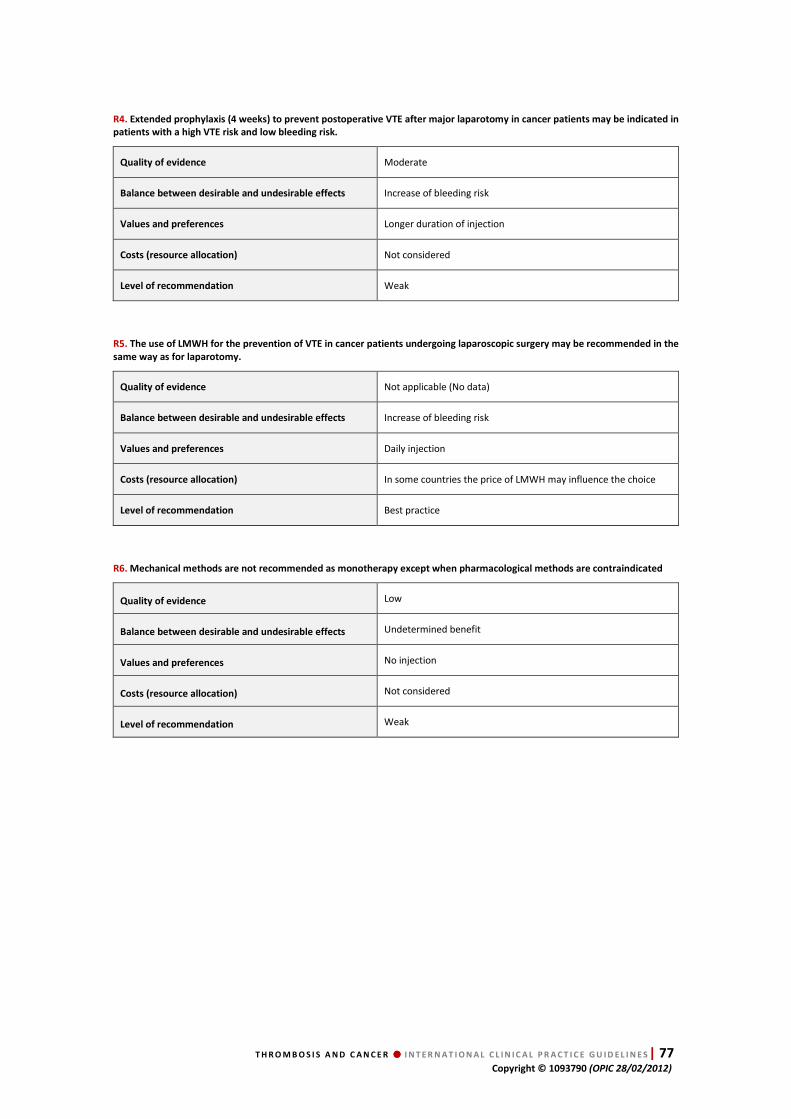
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 77 Copyright © 1093790 (OPIC 28/02/2012)
R4. Extended prophylaxis (4 weeks) to prevent postoperative VTE after major laparotomy in cancer patients may be indicated in
patients with a high VTE risk and low bleeding risk.
Quality of evidence Moderate
Balance between desirable and undesirable effects Increase of bleeding risk
Values and preferences Longer duration of injection
Costs (resource allocation) Not considered
Level of recommendation Weak
R5. The use of LMWH for the prevention of VTE in cancer patients undergoing laparoscopic surgery may be recommended in the
same way as for laparotomy.
Quality of evidence Not applicable (No data)
Balance between desirable and undesirable effects Increase of bleeding risk
Values and preferences Daily injection
Costs (resource allocation) In some countries the price of LMWH may influence the choice
Level of recommendation Best practice
R6. Mechanical methods are not recommended as monotherapy except when pharmacological methods are contraindicated
Quality of evidence Low
Balance between desirable and undesirable effects Undetermined benefit
Values and preferences No injection
Costs (resource allocation) Not considered
Level of recommendation Weak

78 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
5. Chapter 5.
Prophylaxis of VTE in medical cancer patients
5.1. Bibliographic strategy results
For the prophylaxis of VTE in hospitalized medical cancer patients, no specific studies were
found. For this reason, the main studies comparing LMWH and UFH in the general population
were analyzed for this question. Thus, the clinical trials included [BERGMANN1996]
[HARENBERG1996] [LECHLER1996] [KLEBER2003] in the ACCP guidelines, which previously
addressed this question, were selected [GEERTS2008]. The percentage of cancer patients in
these studies varied from 5% to 15%.
For children with acute lymphocytic leukemia (ALL) treated with L-asparaginase, we found two
small studies [MEISTER2008] [MITCHELL2003].
For the studies that were only available in abstract form, the main author was contacted to
make sure that the paper had been accepted by a peer-reviewed medical journal (in this case
methodological limits were taken in account).
HTA Questions Studies included
HTA 1: Hospitalized patients
4 prospective randomized studies
[BERGMANN1996] [HARENBERG1996] [LECHLER1996] [KLEBER2003] 4 randomized double-blind studies
[DAHAN1986] [SAMAMA1999] [LEIZOROVICZ2004] [COHEN2006]
HTA 2: Children with ALL treated with L-asparaginase
1 prospective non-randomized study [MEISTER2008] 1 randomized study [MITCHELL2003]
HTA 3: Ambulatory patients treated with chemotherapy
2 prospective randomized studies [RIESS2009] [MARAVEYAS2011] 3 randomized double-blind trials [HASS2005] [AGNELLI2009] [PERRY2010] 1 analysis of pooled data [VERSO2010]
HTA 3: Patients treated with thalidomide or lenalidomide
2 retrospective studies [ZANGARI2004] [IKHLAQUE2006] 1 prospective randomized study [PALUMBO2011 ] 2 meta-analyses [ELACCAOUI 2007] [HICKS2008]
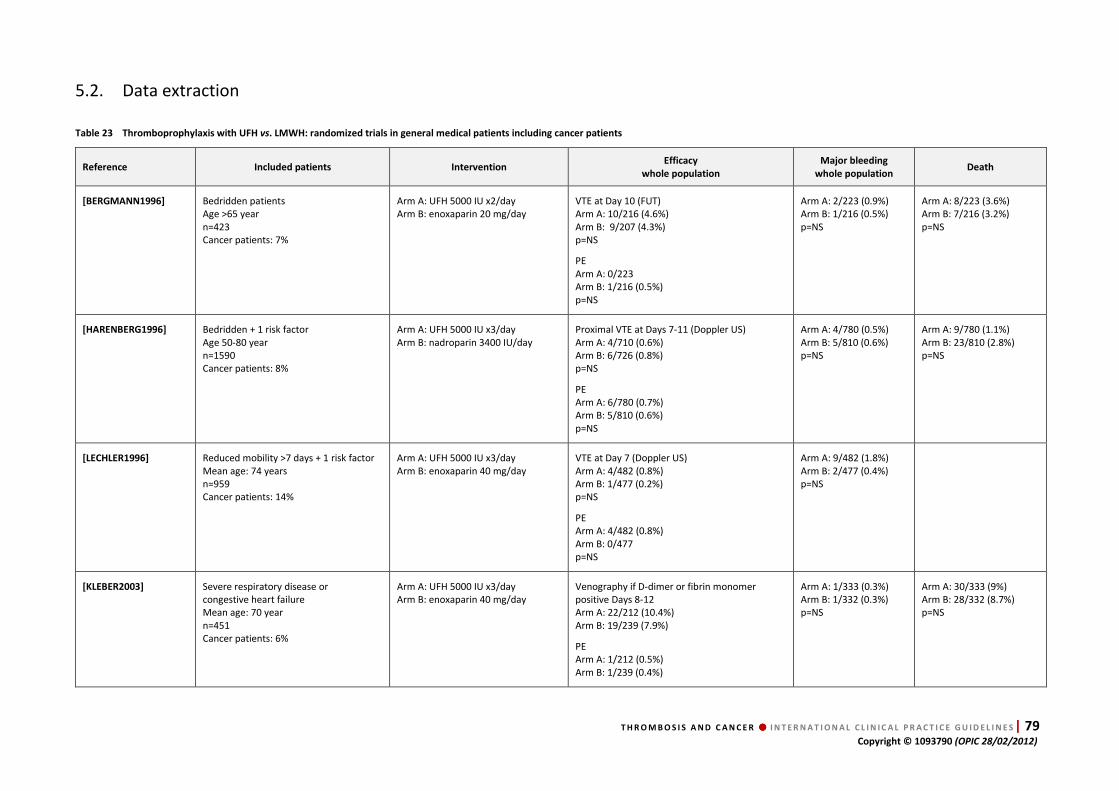
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 79 Copyright © 1093790 (OPIC 28/02/2012)
5.2. Data extraction
Table 23 Thromboprophylaxis with UFH vs. LMWH: randomized trials in general medical patients including cancer patients
Reference Included patients Intervention Efficacy
whole population
Major bleeding
whole population Death
[BERGMANN1996] Bedridden patients Age >65 year n=423 Cancer patients: 7%
Arm A: UFH 5000 IU x2/day Arm B: enoxaparin 20 mg/day
VTE at Day 10 (FUT) Arm A: 10/216 (4.6%) Arm B: 9/207 (4.3%) p=NS
PE Arm A: 0/223 Arm B: 1/216 (0.5%) p=NS
Arm A: 2/223 (0.9%) Arm B: 1/216 (0.5%) p=NS
Arm A: 8/223 (3.6%) Arm B: 7/216 (3.2%) p=NS
[HARENBERG1996] Bedridden + 1 risk factor Age 50-80 year n=1590 Cancer patients: 8%
Arm A: UFH 5000 IU x3/day Arm B: nadroparin 3400 IU/day
Proximal VTE at Days 7-11 (Doppler US) Arm A: 4/710 (0.6%) Arm B: 6/726 (0.8%) p=NS
PE Arm A: 6/780 (0.7%) Arm B: 5/810 (0.6%) p=NS
Arm A: 4/780 (0.5%) Arm B: 5/810 (0.6%) p=NS
Arm A: 9/780 (1.1%) Arm B: 23/810 (2.8%) p=NS
[LECHLER1996] Reduced mobility >7 days + 1 risk factor Mean age: 74 years n=959 Cancer patients: 14%
Arm A: UFH 5000 IU x3/day Arm B: enoxaparin 40 mg/day
VTE at Day 7 (Doppler US) Arm A: 4/482 (0.8%) Arm B: 1/477 (0.2%) p=NS
PE Arm A: 4/482 (0.8%) Arm B: 0/477 p=NS
Arm A: 9/482 (1.8%) Arm B: 2/477 (0.4%) p=NS
[KLEBER2003] Severe respiratory disease or congestive heart failure Mean age: 70 year n=451 Cancer patients: 6%
Arm A: UFH 5000 IU x3/day Arm B: enoxaparin 40 mg/day
Venography if D-dimer or fibrin monomer positive Days 8-12 Arm A: 22/212 (10.4%) Arm B: 19/239 (7.9%)
PE Arm A: 1/212 (0.5%) Arm B: 1/239 (0.4%)
Arm A: 1/333 (0.3%) Arm B: 1/332 (0.3%) p=NS
Arm A: 30/333 (9%) Arm B: 28/332 (8.7%) p=NS

80 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 24 Thromboprophylaxis with LMWH or fondaparinux: randomized double-blind trials in general medical patients including cancer patients
Reference Included patients Intervention Efficacy
whole population
Major bleeding
whole population Death
[DAHAN1986]* Age >65 years Mean age: 80 years n=263 Cancer patients: 13%
Arm A: placebo Arm B: enoxaparin 60 mg/day
VTE at Day 10 (FUT) Arm A: 12/131 (9.1%) Arm B: 4/132 (3.0%) p <0.05
PE Arm A: 3/135 (2.2%) Arm B: 0/135
Arm A: 3/135 (2.2%) Arm B: 1/135 (0.7%) p=NS
Arm A: 6/135 (4.4%) Arm B: 1/135 (0.7%) p=NS
[SAMAMA1999] Age >40 years + 1 risk factor Mean age: 73 years n=1102 Cancer patients: 14%
Arm A: placebo Arm B: enoxaparin 20 mg/day Arm C: enoxaparin 40 mg/day
VTE at Day 14 (Venography or Doppler US)
Arm A: 43/288 (14.9%) Arm B: 43/287 (15.0%) Arm C: 16/291 (5.5%) A vs. B: p=NS A vs. C and B vs. C: p <0.05
Arm A: 7/362 (1.9%) Arm B: 4/351 (1.1%) Arm C: 12/360 (3.3%) p=NS
Arm A: 50/362 (13.8%) Arm B: 51/351 (14.5%) Arm C: 41/360 (11.4%) p=NS
[LEIZOROVICZ2004] Age >40 years + acutely ill medical patients Mean age: 69 years n=3706 Cancer patients: 5%
Arm A: placebo Arm B: dalteparin 5000 IU/day
VTE at Day 21 (Doppler US) Arm A: 73/1473 (5.0%) Arm B: 42/1518 (2.8%) p <0.05
PE: Arm A: 4/1740 (0.2%) Arm B: 5/1759 (0.2%)
Arm A: 0/1850 (0%) Arm B: 8/1856 (0.4%) p=NS
Arm A: 7/1831 (0.4%) Arm B: 8/1846 ((0.4%) p=NS
[COHEN2006] Age >60 years + acutely ill medical patients Mean age: 75 years n=849 Cancer patients: 15%
Arm A: placebo Arm B: fondaparinux 2.5 mg/day
VTE at Day 15 (Venography) Arm A: 34/323 (10.5%) Arm B: 18/321 (5.6%) p <0.05
PE: Arm A: 5/414 (1.2%) Arm B : 0/425
Arm A: 1/414 (0.2%) Arm B: 1/425 (0.2%) p=NS
Arm A: 25/414 (6.0%) Arm B: 14/425 (3.3%) p=NS
*Included in the ACCP guidelines
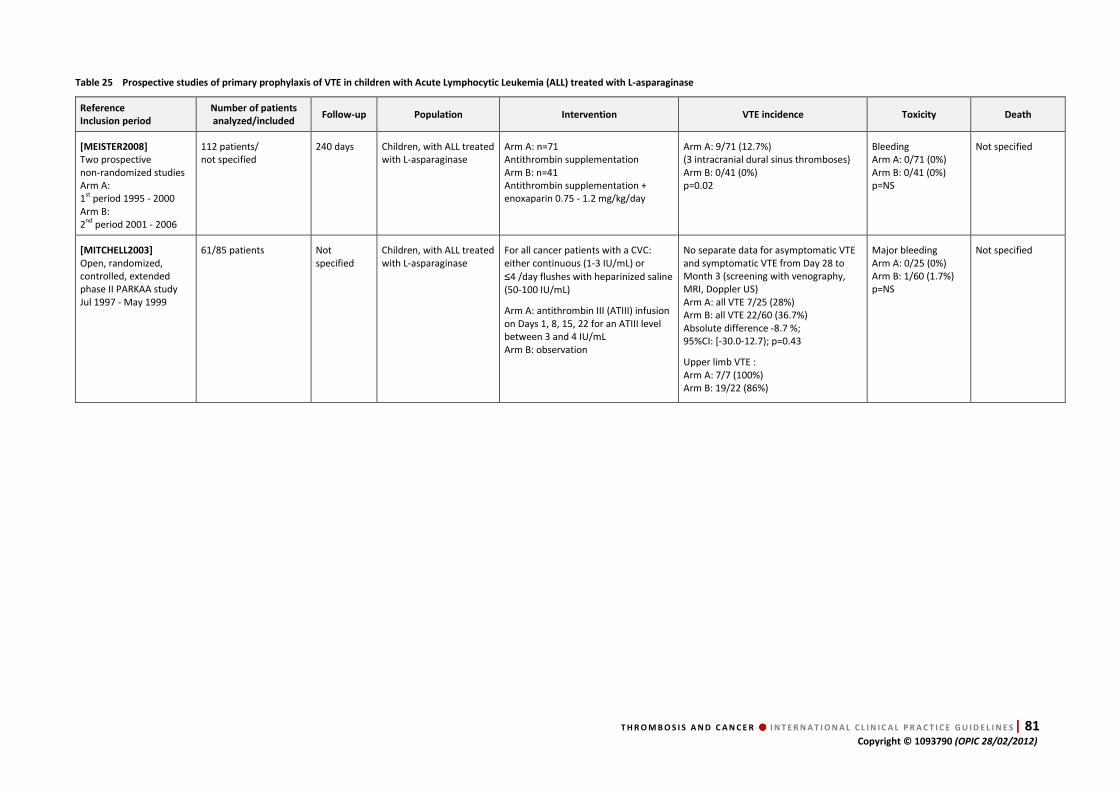
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 81 Copyright © 1093790 (OPIC 28/02/2012)
Table 25 Prospective studies of primary prophylaxis of VTE in children with Acute Lymphocytic Leukemia (ALL) treated with L-asparaginase
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[MEISTER2008]
Two prospective non-randomized studies Arm A: 1st period 1995 - 2000 Arm B: 2nd period 2001 - 2006
112 patients/ not specified
240 days Children, with ALL treated with L-asparaginase
Arm A: n=71 Antithrombin supplementation Arm B: n=41 Antithrombin supplementation + enoxaparin 0.75 - 1.2 mg/kg/day
Arm A: 9/71 (12.7%) (3 intracranial dural sinus thromboses) Arm B: 0/41 (0%) p=0.02
Bleeding Arm A: 0/71 (0%) Arm B: 0/41 (0%) p=NS
Not specified
[MITCHELL2003]
Open, randomized, controlled, extended phase II PARKAA study Jul 1997 - May 1999
61/85 patients Not specified
Children, with ALL treated with L-asparaginase
For all cancer patients with a CVC: either continuous (1-3 IU/mL) or
≤4 /day flushes with heparinized saline (50-100 IU/mL)
Arm A: antithrombin III (ATIII) infusion on Days 1, 8, 15, 22 for an ATIII level between 3 and 4 IU/mL Arm B: observation
No separate data for asymptomatic VTE and symptomatic VTE from Day 28 to Month 3 (screening with venography, MRI, Doppler US) Arm A: all VTE 7/25 (28%) Arm B: all VTE 22/60 (36.7%) Absolute difference -8.7 %; 95%CI: [-30.0-12.7); p=0.43
Upper limb VTE : Arm A: 7/7 (100%) Arm B: 19/22 (86%)
Major bleeding Arm A: 0/25 (0%) Arm B: 1/60 (1.7%) p=NS
Not specified
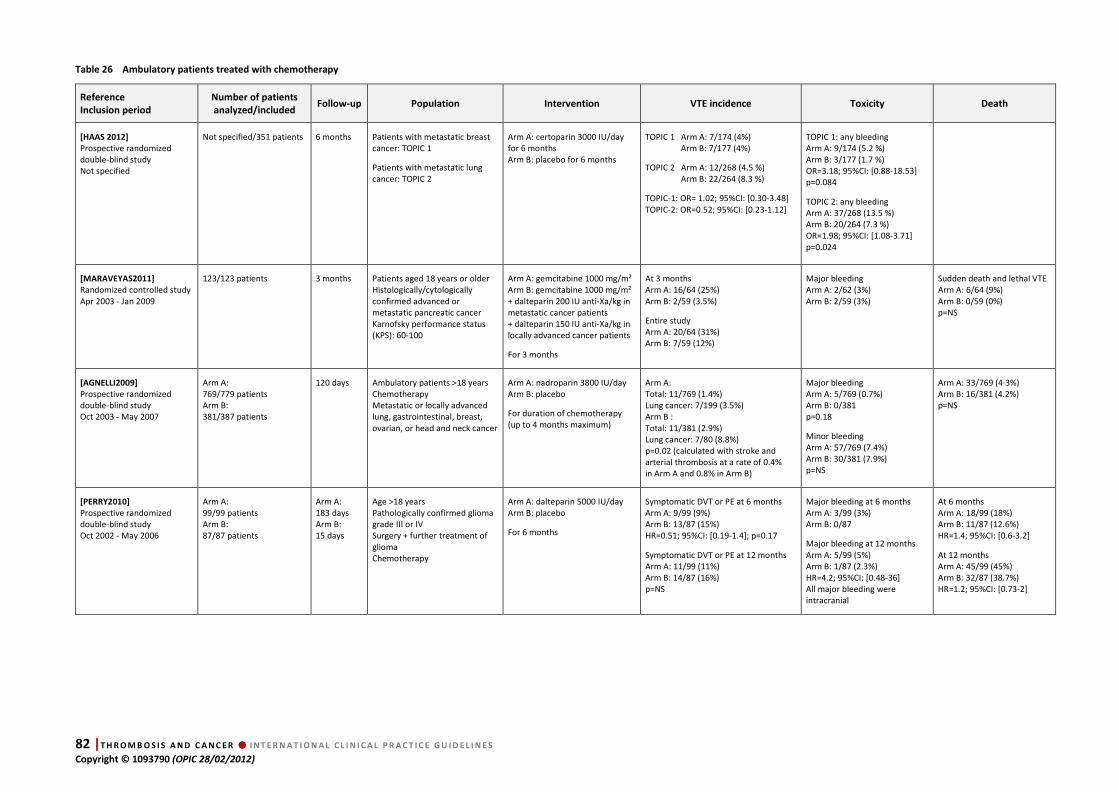
82 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 26 Ambulatory patients treated with chemotherapy
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[HAAS 2012]
Prospective randomized double-blind study Not specified
Not specified/351 patients 6 months Patients with metastatic breast cancer: TOPIC 1
Patients with metastatic lung cancer: TOPIC 2
Arm A: certoparin 3000 IU/day for 6 months Arm B: placebo for 6 months
TOPIC 1 Arm A: 7/174 (4%) Arm B: 7/177 (4%)
TOPIC 2 Arm A: 12/268 (4.5 %) Arm B: 22/264 (8.3 %)
TOPIC-1: OR= 1.02; 95%CI: [0.30-3.48] TOPIC-2: OR=0.52; 95%CI: [0.23-1.12]
TOPIC 1: any bleeding Arm A: 9/174 (5.2 %) Arm B: 3/177 (1.7 %) OR=3.18; 95%CI: [0.88-18.53] p=0.084
TOPIC 2: any bleeding Arm A: 37/268 (13.5 %) Arm B: 20/264 (7.3 %) OR=1.98; 95%CI: [1.08-3.71] p=0.024
[MARAVEYAS2011]
Randomized controlled study Apr 2003 - Jan 2009
123/123 patients 3 months Patients aged 18 years or older Histologically/cytologically confirmed advanced or metastatic pancreatic cancer Karnofsky performance status (KPS): 60-100
Arm A: gemcitabine 1000 mg/m² Arm B: gemcitabine 1000 mg/m² + dalteparin 200 IU anti-Xa/kg in metastatic cancer patients + dalteparin 150 IU anti-Xa/kg in locally advanced cancer patients
For 3 months
At 3 months Arm A: 16/64 (25%) Arm B: 2/59 (3.5%)
Entire study Arm A: 20/64 (31%) Arm B: 7/59 (12%)
Major bleeding Arm A: 2/62 (3%) Arm B: 2/59 (3%)
Sudden death and lethal VTE Arm A: 6/64 (9%) Arm B: 0/59 (0%) p=NS
[AGNELLI2009]
Prospective randomized double-blind study Oct 2003 - May 2007
Arm A: 769/779 patients Arm B: 381/387 patients
120 days Ambulatory patients >18 years Chemotherapy Metastatic or locally advanced lung, gastrointestinal, breast, ovarian, or head and neck cancer
Arm A: nadroparin 3800 IU/day Arm B: placebo
For duration of chemotherapy (up to 4 months maximum)
Arm A: Total: 11/769 (1.4%) Lung cancer: 7/199 (3.5%) Arm B : Total: 11/381 (2.9%) Lung cancer: 7/80 (8.8%) p=0.02 (calculated with stroke and arterial thrombosis at a rate of 0.4% in Arm A and 0.8% in Arm B)
Major bleeding Arm A: 5/769 (0.7%) Arm B: 0/381 p=0.18
Minor bleeding Arm A: 57/769 (7.4%) Arm B: 30/381 (7.9%) p=NS
Arm A: 33/769 (4·3%) Arm B: 16/381 (4.2%) p=NS
[PERRY2010]
Prospective randomized double-blind study Oct 2002 - May 2006
Arm A: 99/99 patients Arm B: 87/87 patients
Arm A: 183 days Arm B: 15 days
Age >18 years Pathologically confirmed glioma grade III or IV Surgery + further treatment of glioma Chemotherapy
Arm A: dalteparin 5000 IU/day Arm B: placebo
For 6 months
Symptomatic DVT or PE at 6 months Arm A: 9/99 (9%) Arm B: 13/87 (15%) HR=0.51; 95%CI: [0.19-1.4]; p=0.17
Symptomatic DVT or PE at 12 months Arm A: 11/99 (11%) Arm B: 14/87 (16%) p=NS
Major bleeding at 6 months Arm A: 3/99 (3%) Arm B: 0/87
Major bleeding at 12 months Arm A: 5/99 (5%) Arm B: 1/87 (2.3%) HR=4.2; 95%CI: [0.48-36] All major bleeding were intracranial
At 6 months Arm A: 18/99 (18%) Arm B: 11/87 (12.6%) HR=1.4; 95%CI: [0.6-3.2]
At 12 months Arm A: 45/99 (45%) Arm B: 32/87 (38.7%) HR=1.2; 95%CI: [0.73-2]
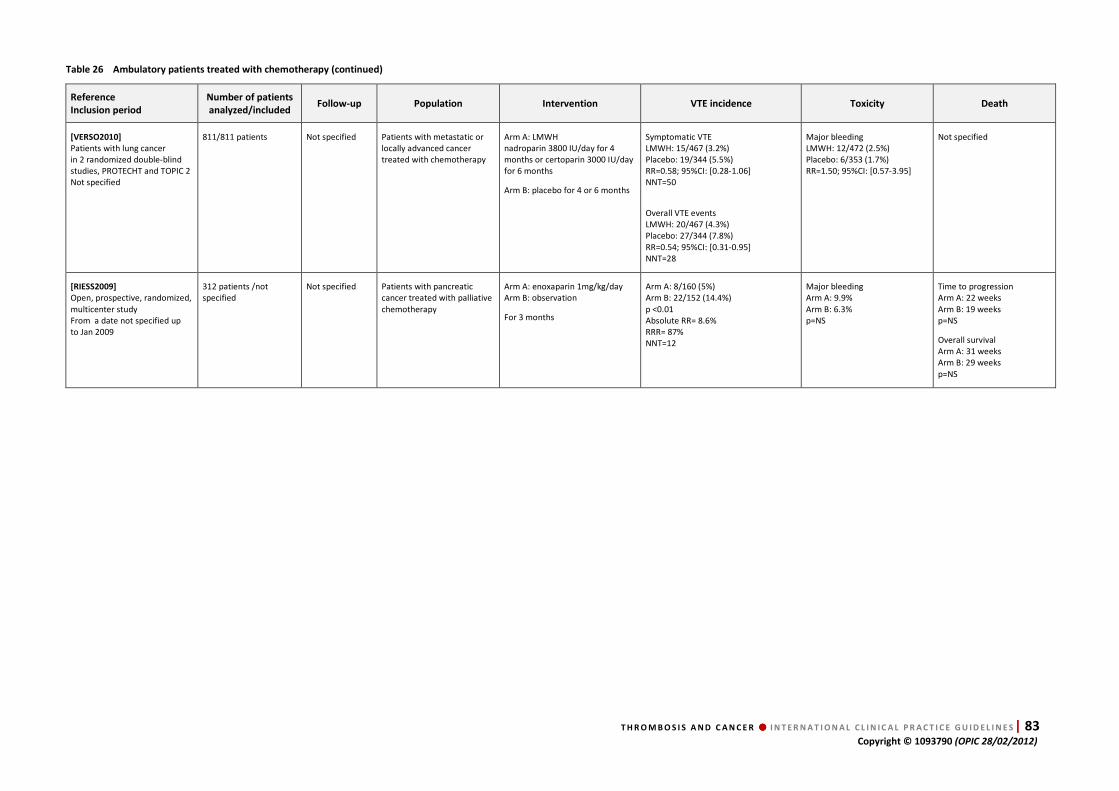
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 83 Copyright © 1093790 (OPIC 28/02/2012)
Table 26 Ambulatory patients treated with chemotherapy (continued)
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[VERSO2010]
Patients with lung cancer in 2 randomized double-blind studies, PROTECHT and TOPIC 2 Not specified
811/811 patients Not specified Patients with metastatic or locally advanced cancer treated with chemotherapy
Arm A: LMWH nadroparin 3800 IU/day for 4 months or certoparin 3000 IU/day for 6 months
Arm B: placebo for 4 or 6 months
Symptomatic VTE LMWH: 15/467 (3.2%) Placebo: 19/344 (5.5%) RR=0.58; 95%CI: [0.28-1.06] NNT=50
Overall VTE events LMWH: 20/467 (4.3%) Placebo: 27/344 (7.8%) RR=0.54; 95%CI: [0.31-0.95] NNT=28
Major bleeding LMWH: 12/472 (2.5%) Placebo: 6/353 (1.7%) RR=1.50; 95%CI: [0.57-3.95]
Not specified
[RIESS2009]
Open, prospective, randomized, multicenter study From a date not specified up to Jan 2009
312 patients /not specified
Not specified Patients with pancreatic cancer treated with palliative chemotherapy
Arm A: enoxaparin 1mg/kg/day Arm B: observation
For 3 months
Arm A: 8/160 (5%) Arm B: 22/152 (14.4%) p <0.01 Absolute RR= 8.6% RRR= 87% NNT=12
Major bleeding Arm A: 9.9% Arm B: 6.3% p=NS
Time to progression Arm A: 22 weeks Arm B: 19 weeks p=NS
Overall survival Arm A: 31 weeks Arm B: 29 weeks p=NS
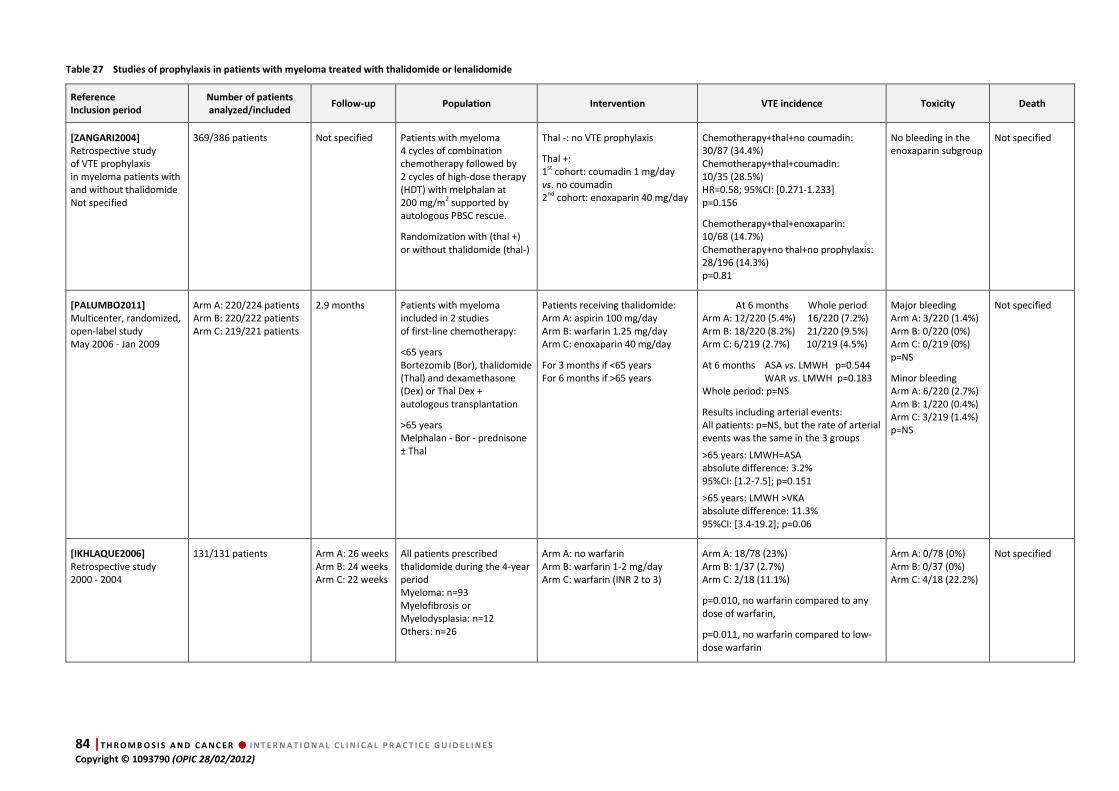
84 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 27 Studies of prophylaxis in patients with myeloma treated with thalidomide or lenalidomide
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[ZANGARI2004]
Retrospective study of VTE prophylaxis in myeloma patients with and without thalidomide Not specified
369/386 patients Not specified Patients with myeloma 4 cycles of combination chemotherapy followed by 2 cycles of high-dose therapy (HDT) with melphalan at 200 mg/m2 supported by autologous PBSC rescue.
Randomization with (thal +) or without thalidomide (thal-)
Thal -: no VTE prophylaxis
Thal +: 1st cohort: coumadin 1 mg/day vs. no coumadin 2nd cohort: enoxaparin 40 mg/day
Chemotherapy+thal+no coumadin: 30/87 (34.4%) Chemotherapy+thal+coumadin: 10/35 (28.5%) HR=0.58; 95%CI: [0.271-1.233] p=0.156
Chemotherapy+thal+enoxaparin: 10/68 (14.7%) Chemotherapy+no thal+no prophylaxis: 28/196 (14.3%) p=0.81
No bleeding in the enoxaparin subgroup
Not specified
[PALUMBO2011]
Multicenter, randomized, open-label study May 2006 - Jan 2009
Arm A: 220/224 patients Arm B: 220/222 patients Arm C: 219/221 patients
2.9 months Patients with myeloma included in 2 studies of first-line chemotherapy:
<65 years Bortezomib (Bor), thalidomide (Thal) and dexamethasone (Dex) or Thal Dex + autologous transplantation
>65 years Melphalan - Bor - prednisone ± Thal
Patients receiving thalidomide: Arm A: aspirin 100 mg/day Arm B: warfarin 1.25 mg/day Arm C: enoxaparin 40 mg/day
For 3 months if <65 years For 6 months if >65 years
At 6 months Whole period Arm A: 12/220 (5.4%) 16/220 (7.2%) Arm B: 18/220 (8.2%) 21/220 (9.5%) Arm C: 6/219 (2.7%) 10/219 (4.5%)
At 6 months ASA vs. LMWH p=0.544 WAR vs. LMWH p=0.183 Whole period: p=NS
Results including arterial events: All patients: p=NS, but the rate of arterial events was the same in the 3 groups
>65 years: LMWH=ASA absolute difference: 3.2% 95%CI: [1.2-7.5]; p=0.151
>65 years: LMWH >VKA absolute difference: 11.3% 95%CI: [3.4-19.2]; p=0.06
Major bleeding Arm A: 3/220 (1.4%) Arm B: 0/220 (0%) Arm C: 0/219 (0%) p=NS
Minor bleeding Arm A: 6/220 (2.7%) Arm B: 1/220 (0.4%) Arm C: 3/219 (1.4%) p=NS
Not specified
[IKHLAQUE2006]
Retrospective study 2000 - 2004
131/131 patients Arm A: 26 weeks Arm B: 24 weeks Arm C: 22 weeks
All patients prescribed thalidomide during the 4-year period Myeloma: n=93 Myelofibrosis or Myelodysplasia: n=12 Others: n=26
Arm A: no warfarin Arm B: warfarin 1-2 mg/day Arm C: warfarin (INR 2 to 3)
Arm A: 18/78 (23%) Arm B: 1/37 (2.7%) Arm C: 2/18 (11.1%)
p=0.010, no warfarin compared to any dose of warfarin,
p=0.011, no warfarin compared to low-dose warfarin
Arm A: 0/78 (0%) Arm B: 0/37 (0%) Arm C: 4/18 (22.2%)
Not specified
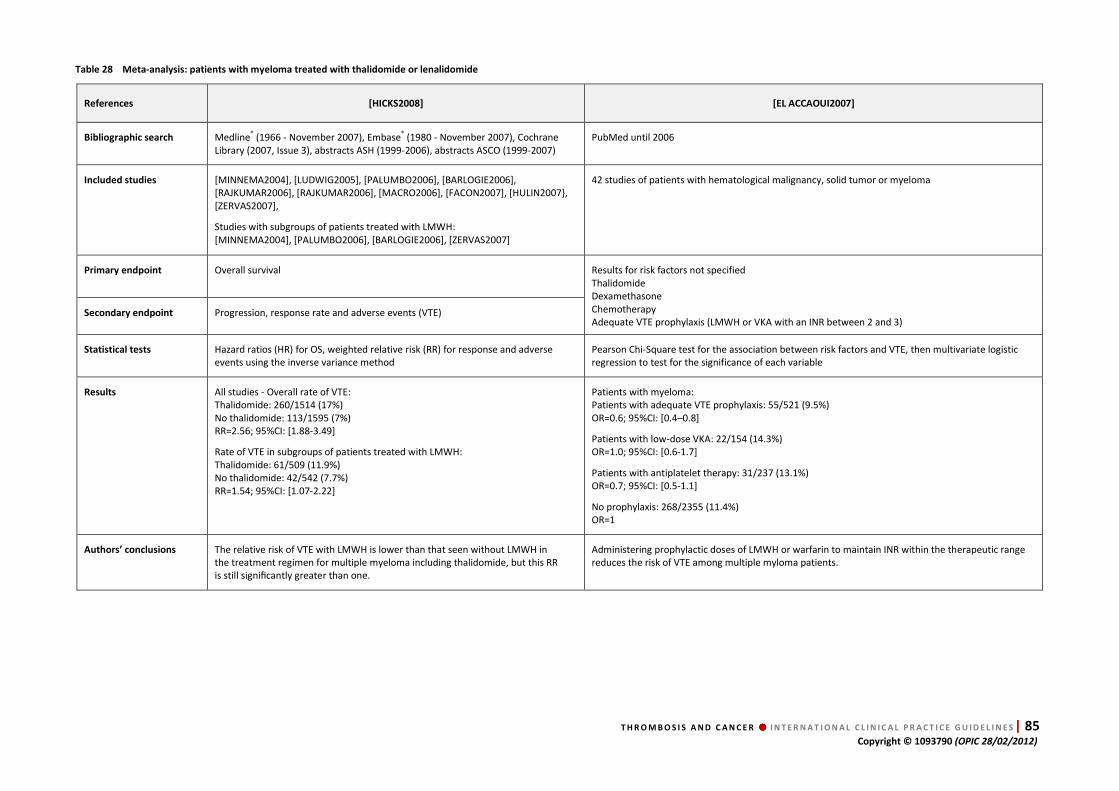
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 85 Copyright © 1093790 (OPIC 28/02/2012)
Table 28 Meta-analysis: patients with myeloma treated with thalidomide or lenalidomide
References [HICKS2008] [EL ACCAOUI2007]
Bibliographic search Medline® (1966 - November 2007), Embase® (1980 - November 2007), Cochrane Library (2007, Issue 3), abstracts ASH (1999-2006), abstracts ASCO (1999-2007)
PubMed until 2006
Included studies [MINNEMA2004], [LUDWIG2005], [PALUMBO2006], [BARLOGIE2006], [RAJKUMAR2006], [RAJKUMAR2006], [MACRO2006], [FACON2007], [HULIN2007}, [ZERVAS2007],
Studies with subgroups of patients treated with LMWH: [MINNEMA2004], [PALUMBO2006], [BARLOGIE2006], [ZERVAS2007]
42 studies of patients with hematological malignancy, solid tumor or myeloma
Primary endpoint Overall survival
Results for risk factors not specified Thalidomide Dexamethasone Chemotherapy Adequate VTE prophylaxis (LMWH or VKA with an INR between 2 and 3)
Secondary endpoint Progression, response rate and adverse events (VTE)
Statistical tests Hazard ratios (HR) for OS, weighted relative risk (RR) for response and adverse events using the inverse variance method
Pearson Chi-Square test for the association between risk factors and VTE, then multivariate logistic regression to test for the significance of each variable
Results All studies - Overall rate of VTE: Thalidomide: 260/1514 (17%) No thalidomide: 113/1595 (7%) RR=2.56; 95%CI: [1.88-3.49]
Rate of VTE in subgroups of patients treated with LMWH: Thalidomide: 61/509 (11.9%) No thalidomide: 42/542 (7.7%) RR=1.54; 95%CI: [1.07-2.22]
Patients with myeloma: Patients with adequate VTE prophylaxis: 55/521 (9.5%) OR=0.6; 95%CI: [0.4–0.8]
Patients with low-dose VKA: 22/154 (14.3%) OR=1.0; 95%CI: [0.6-1.7]
Patients with antiplatelet therapy: 31/237 (13.1%) OR=0.7; 95%CI: [0.5-1.1]
No prophylaxis: 268/2355 (11.4%) OR=1
Authors’ conclusions The relative risk of VTE with LMWH is lower than that seen without LMWH in the treatment regimen for multiple myeloma including thalidomide, but this RR is still significantly greater than one.
Administering prophylactic doses of LMWH or warfarin to maintain INR within the therapeutic range reduces the risk of VTE among multiple myloma patients.

86 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
5.3. Data analysis
Hospitalized cancer patients
Studies
4 prospective randomized studies
[BERGMANN1996] [HARENBERG1996] [LECHLER1996] [KLEBER2003] 4 randomized double-blind studies
[DAHAN1986] [SAMAMA1999] [LEIZOROVICZ2004] [COHEN2006]
Agreement Yes
Quality of evidence Moderate (randomized studies but indirectness)
Results
For primary prophylaxis of VTE in hospitalized medical cancer patients:
• LMWH and UFH have a similar efficacy and safety
• LMWH and fondaparinux are superior to placebo with a non-significant trend towards increased bleeding (except for enoxaparin 20 or 40 mg and fondaparinux)
• the rate of cancer patients included in these studies varies from 5 to 15%
• no study reports a difference of efficacy between cancer and non-cancer patients
Conclusions
Primary prophylaxis with UFH, LMWH and fondaparinux has been shown to be effective
in studies including hospitalized cancer patients with reduced mobility.
Children with ALL treated with L-Asparaginase
Studies
1 prospective non-randomized study
[MEISTER2008] 1 randomized study
[MITCHELL2003]
Agreement No: only two studies with few patients and different designs (ATIII + LMWH vs. ATIII, ATIII vs. observation)
Quality of evidence Very low (observational, study limitations, inconsistency, imprecision)
Results In children with ALL, the rate of symptomatic VTE is around 5%.
Conclusions
It seems difficult to draw any conclusions about the efficacy of antithrombin III (ATIII) and
the combination of LMWH with ATIII.
Ambulatory patients treated with chemotherapy
Studies
2 prospective randomized studies
[RIESS2009] [MARAVEYAS2011 ] 3 randomized double-blind trials
[HASS2005] [AGNELLI2009] [PERRY2010] 1 analysis of pooled data
[VERSO2010]
Agreement No, results depend on the type of cancer
Quality of evidence Moderate (randomized, but serious inconsistency)
Results
Primary prophylaxis with LMWH in patients treated with chemotherapy:
• increases non-significantly intracranial bleeding in patients with a brain tumor
• decreases the rate of VTE without an excess of bleeding in patients with locally advanced or metastatic pancreatic (at subtherapeutic dosages) or locally advanced or metastatic lung cancers
• has no effect on VTE in patients with metastatic breast cancer

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 87 Copyright © 1093790 (OPIC 28/02/2012)
Conclusions In cancer patients treated with chemotherapy, prophylaxis with LMWH:
• could have a benefit in patients with locally advanced or metastatic pancreatic (at subtherapeutic dosages) or locally advanced or metastatic lung cancers,
• has no effect on VTE in patients with metastatic breast cancer,
• might be dangerous for patients with a brain tumor,
• may increase the bleeding risk in the presence of thrombocytopenia.
Patients treated with thalidomide or lenalidomide
Studies
2 retrospective studies
[ZANGARI2004] [IKHLAQUE2006] 1 prospective randomized study [PALUMBO2011 ] 2 meta-analyses
[ELACCAOUI 2007] [HICKS2008]
Agreement Yes
Quality of evidence Low (1 randomized study with serious limitations and imprecision; meta-analyses did not take into account this study)
Results
Prophylactic doses of LMWH or aspirin (100 mg/day) or warfarin to maintain INR within the therapeutic range reduce the risk of thromboembolic events among multiple myeloma patients treated with lenalidomide or thalidomide with no increase in bleeding risk
Conclusions
The rate of VTE in patients treated with IMiDs (thalidomide, lenalidomide) combined with
steroids and/or chemotherapy (doxorubicine) is very high. VTE prophylaxis in patients treated
with thalidomide or lenalidomide produces similar results irrespective of whether LMWH,
therapeutic VKA (INR 2-3), low-dose VKA or low-dose aspirin (100 mg/day) is used. In the
absence of a placebo group the efficacy of these regimens remains elusive.
5.4. Discussion
As there was no clear definition in the literature enabling distinction between inpatients and
outpatients, we chose to use the term medical patients to denote both hospitalized and
ambulatory patients. In the absence of specific studies, the results of primary VTE prophylaxis
in hospitalized patients can be applied to cancer patients with reduced mobility. None of the
included studies concerning prophylaxis in medical patients reported differences between
non-cancer and cancer patients (5% to 15 % of the population). In this setting, the efficacy of
both LMWH and fondaparinux is superior to that of placebo; UFH and LMWH have been shown
to have the same efficacy.
The risk of VTE during hospitalization and after discharge is higher in medical cancer patients
than in non-cancer patients, so the risk reduction in this population could be particularly
important [KHORANA2008]. For this reason, in selected high-risk patients, continued
prophylaxis after hospital discharge may be considered (best practice in view of the lack of
specific data).
Only two non-randomized studies, including small numbers of patients and differing in design,
were performed in children with ALL treated with L-asparaginase [MITCHELL2003]
[MEISTER2008]. One study tested the value of adding LMWH to ATIII substitution

88 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
[MEISTER2008] and the other compared the prescription of ATIII to no treatment
[MITCHELL2003]. There is no consensus supporting any particular prophylactic regimen in
children and adults with ALL treated with L-asparaginase to prevent VTE and the experts of the
Working group reported a wide divergence in practices in this case. So recommendations can
only be based on local policy and individual patient characteristics.
The trials of primary prophylaxis of VTE in medical patients have included ambulatory cancer
patients treated with chemotherapy and have used LMWH. The prevention of VTE with LMWH
in medical cancer patients treated with chemotherapy could be restricted to a subgroup in
which the rate of VTE is much higher than the bleeding risk. In the case of locally advanced or
metastatic pancreatic cancer the risk of VTE is so high that the benefit of the LMWH used in a
subtherapeutic regimen in two studies [RIESS2009] [MARAVEYAS2011] outweighed the
bleeding risk. For locally advanced and metastatic pulmonary cancer, the benefit-risk ratio was
lower in the studies included in this guideline [HAAS2012] [AGNELLI2009] [VERSO2010] and
the recommandation is weak. The benefit of such prophylaxis could be restricted to non-small
cell carcinoma (NSCC), because one study included only NSCC [HAAS2012] and the second
probably included only a small number of patients with small cell carcinoma (SCC) which is far
less frequent than NSCC [AGNELLI2009]. Analysis of clinical trials shows that primary
prophylaxis with LMWH might be dangerous for patients with a brain tumor [PERRY2009],
because of an excess of intracranial bleeding, but it can decrease the rate of VTE without
excess of bleeding in locally advanced or metastatic pancretic or lung cancers [RIESS2009]
[MARAVEYAS2011] [AGNELLI2009] [VERSO2010] . The experts think there is a need for further
studies before recommending routine prophylaxis with LMWH in cancer patients receiving
chemotherapy.
The risk of VTE associated with first-line treatment of multiple myeloma patients with
thalidomide and lenalidomide (IMiDs) is very high, especially when these drugs are combined
with high doses of dexamethasone or with chemotherapy (doxorubicin). Multiple myeloma is a
common disease and IMiDs are the gold standard for the treatment of patients not eligible for
autologous haemopoietic stem-cell transplantation, but only one randomized study has been
performed. In this study, patients with multiple myeloma treated with thalidomide-based
regimens, aspirin and low-dose warfarin (1.25 mg/day) showed similar efficacy in reducing
serious thromboembolic events, acute cardiovascular events, and sudden deaths compared
with LMWH, except in elderly patients in whom warfarin showed less efficacy than LMWH
[PALUMBO2001]. The two meta-analyses indicate that administering prophylactic doses of
LMWH or warfarin to maintain a therapeutic INR reduces the risk of thromboembolic events
[ELACCAOUI2007] [HICKS2008]. As no study with a placebo or observation group has been
performed to date, the efficacy of such regimen remains unclear. Furthermore, as the rate of
non-multiple myeloma patients treated either with thalidomide or lenalidomide is very low in
the studies selected, these recommendations can only apply to patients with multiple
myeloma treated with IMiDs.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 89 Copyright © 1093790 (OPIC 28/02/2012)
5.5. Recommendations – prophylaxis of VTE in medical cancer patients R1. We recommend prophylaxis with LMWH, UFH or fondaparinux in hospitalized medical patients with cancer and reduced
mobility.
Quality of evidence Moderate
Balance between desirable and undesirable effects Favorable
Values and preferences Subcutaneous injections
Costs (resource allocation) In some countries price differences between LMWH, UFH or fondaparinux may influence the choice
Level of recommendation Strong
R2. For children with ALL treated with L-asparaginase, depending on local policy and individual patient characteristics (platelet
count, kidney function, fibrinogen and antithrombin III levels, etc.), prophylaxis may be considered in some patients. The same
therapeutic option can be considered for adults
Quality of evidence Very low
Balance between desirable and undesirable effects Depends on individual patient characteristics
Values and preferences Subcutaneous injections
Costs (resource allocation) Not considered
Level of recommendation Best practice
R3. In patients receiving chemotherapy, prophylaxis cannot be recommended routinely
Quality of evidence Moderate
Balance between desirable and undesirable effects Uncertain for all types of cancer
Values and preferences Subcutaneous injections
Costs (resource allocation) Not considered
Level of recommendation Strong
R4. Primary pharmacological prophylaxis of VTE may be indicated in patient with locally advanced or metastatic pancreatic
cancer treated with chemotherapy and having a low bleeding risk.
Quality of evidence Moderate
Balance between desirable and undesirable effects Favorable
Values and preferences Subcutaneous injections
Costs (resource allocation) Not considered
Level of recommendation Strong
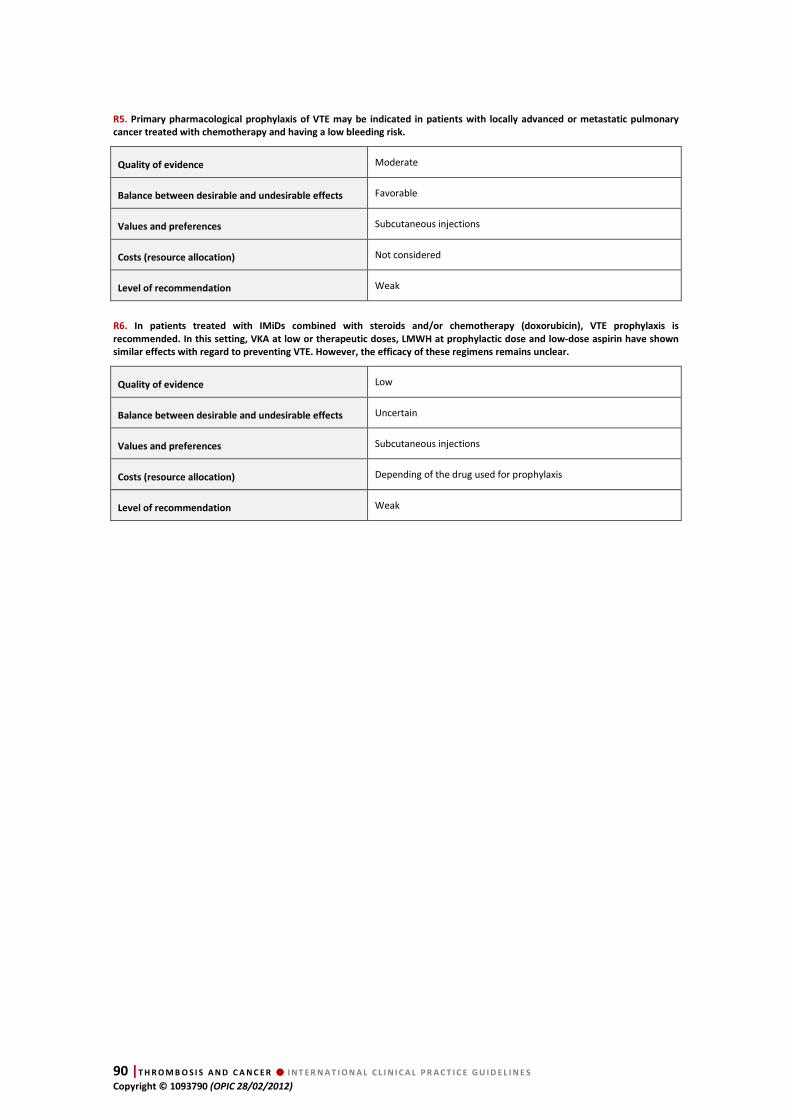
90 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
R5. Primary pharmacological prophylaxis of VTE may be indicated in patients with locally advanced or metastatic pulmonary
cancer treated with chemotherapy and having a low bleeding risk.
Quality of evidence Moderate
Balance between desirable and undesirable effects Favorable
Values and preferences Subcutaneous injections
Costs (resource allocation) Not considered
Level of recommendation Weak
R6. In patients treated with IMiDs combined with steroids and/or chemotherapy (doxorubicin), VTE prophylaxis is
recommended. In this setting, VKA at low or therapeutic doses, LMWH at prophylactic dose and low-dose aspirin have shown
similar effects with regard to preventing VTE. However, the efficacy of these regimens remains unclear.
Quality of evidence Low
Balance between desirable and undesirable effects Uncertain
Values and preferences Subcutaneous injections
Costs (resource allocation) Depending of the drug used for prophylaxis
Level of recommendation Weak
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 91 Copyright © 1093790 (OPIC 28/02/2012)
6. Chapter 6.
Treatment of established catheter-related
thrombosis The literature search retrieved no prospective randomized study.
HTA Questions Studies included
HTA 1: Treatment of CVC Thrombosis: LMWH +
VKA
2 prospective non-randomized studies
[SAVAGE1999] [KOVACS2007] 1 retrospective study
[TRAN2010]
HTA 2: Treatment of CVC Thrombosis: CVC
removal
1 retrospective study
[FRANK2000]
HTA 3: Treatment of CVC thrombosis:
thrombolytic therapy
2 retrospective studies
[PUCHEU1996][SCHINDLER1999]
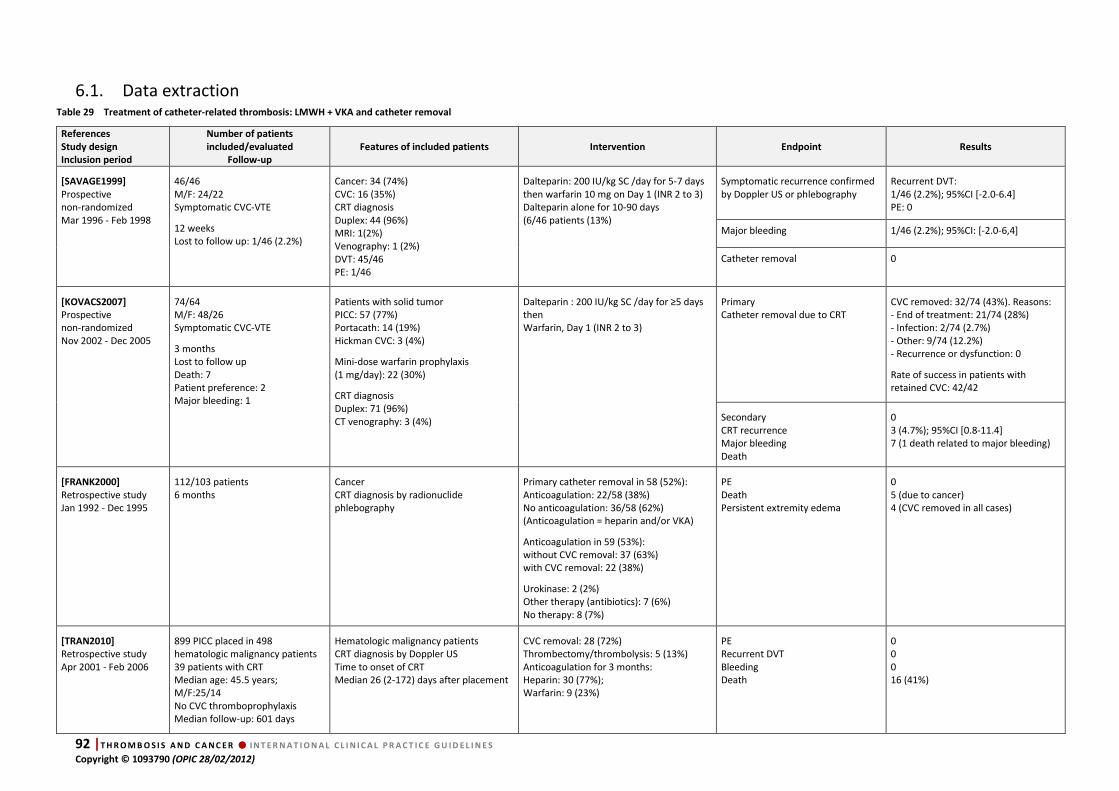
92 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
6.1. Data extraction Table 29 Treatment of catheter-related thrombosis: LMWH + VKA and catheter removal
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Endpoint Results
[SAVAGE1999]
Prospective non-randomized Mar 1996 - Feb 1998
46/46 M/F: 24/22 Symptomatic CVC-VTE
12 weeks Lost to follow up: 1/46 (2.2%)
Cancer: 34 (74%) CVC: 16 (35%) CRT diagnosis Duplex: 44 (96%) MRI: 1(2%) Venography: 1 (2%) DVT: 45/46 PE: 1/46
Dalteparin: 200 IU/kg SC /day for 5-7 days then warfarin 10 mg on Day 1 (INR 2 to 3) Dalteparin alone for 10-90 days (6/46 patients (13%)
Symptomatic recurrence confirmed by Doppler US or phlebography
Recurrent DVT: 1/46 (2.2%); 95%CI [-2.0-6.4] PE: 0
Major bleeding 1/46 (2.2%); 95%CI: [-2.0-6,4]
Catheter removal 0
[KOVACS2007]
Prospective non-randomized Nov 2002 - Dec 2005
74/64 M/F: 48/26 Symptomatic CVC-VTE
3 months Lost to follow up Death: 7 Patient preference: 2 Major bleeding: 1
Patients with solid tumor PICC: 57 (77%) Portacath: 14 (19%) Hickman CVC: 3 (4%)
Mini-dose warfarin prophylaxis (1 mg/day): 22 (30%)
CRT diagnosis Duplex: 71 (96%) CT venography: 3 (4%)
Dalteparin : 200 IU/kg SC /day for ≥5 days then Warfarin, Day 1 (INR 2 to 3)
Primary Catheter removal due to CRT
CVC removed: 32/74 (43%). Reasons: - End of treatment: 21/74 (28%) - Infection: 2/74 (2.7%) - Other: 9/74 (12.2%) - Recurrence or dysfunction: 0
Rate of success in patients with retained CVC: 42/42
Secondary CRT recurrence Major bleeding Death
0 3 (4.7%); 95%CI [0.8-11.4] 7 (1 death related to major bleeding)
[FRANK2000]
Retrospective study Jan 1992 - Dec 1995
112/103 patients 6 months
Cancer CRT diagnosis by radionuclide phlebography
Primary catheter removal in 58 (52%): Anticoagulation: 22/58 (38%) No anticoagulation: 36/58 (62%) (Anticoagulation = heparin and/or VKA)
Anticoagulation in 59 (53%): without CVC removal: 37 (63%) with CVC removal: 22 (38%)
Urokinase: 2 (2%) Other therapy (antibiotics): 7 (6%) No therapy: 8 (7%)
PE Death Persistent extremity edema
0 5 (due to cancer) 4 (CVC removed in all cases)
[TRAN2010]
Retrospective study Apr 2001 - Feb 2006
899 PICC placed in 498 hematologic malignancy patients 39 patients with CRT Median age: 45.5 years; M/F:25/14 No CVC thromboprophylaxis Median follow-up: 601 days
Hematologic malignancy patients CRT diagnosis by Doppler US Time to onset of CRT Median 26 (2-172) days after placement
CVC removal: 28 (72%) Thrombectomy/thrombolysis: 5 (13%) Anticoagulation for 3 months: Heparin: 30 (77%); Warfarin: 9 (23%)
PE Recurrent DVT Bleeding Death
0 0 0 16 (41%)
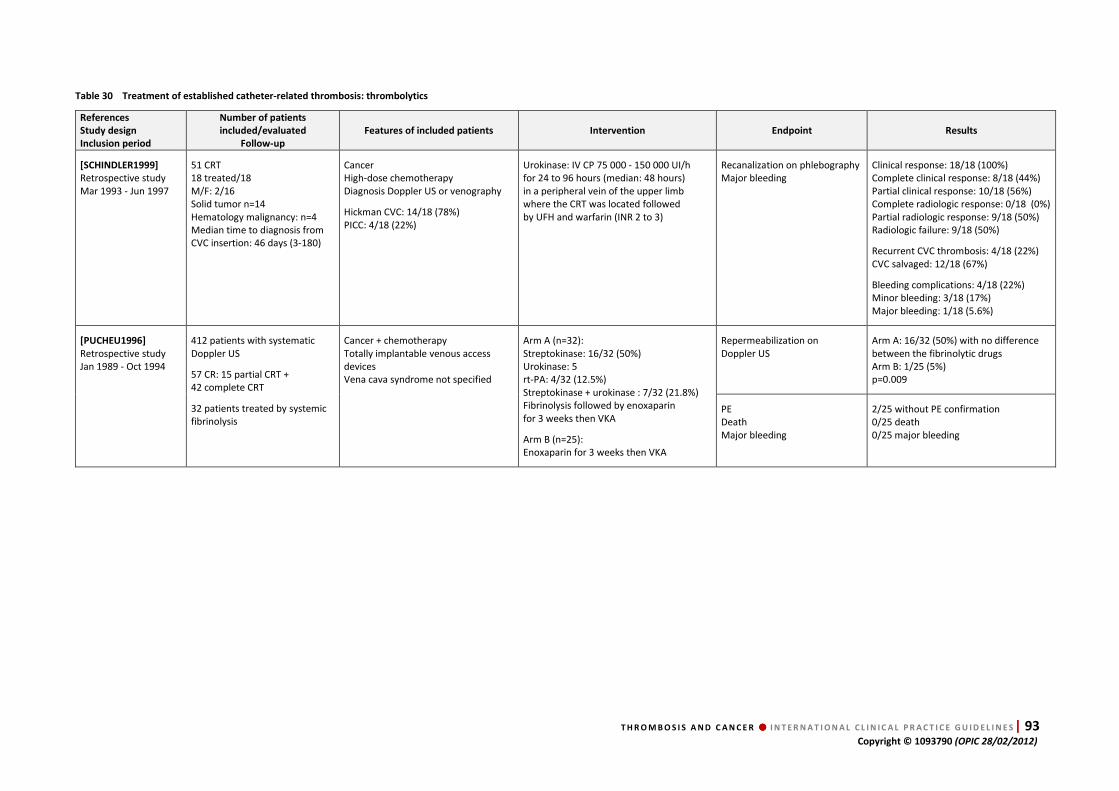
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 93 Copyright © 1093790 (OPIC 28/02/2012)
Table 30 Treatment of established catheter-related thrombosis: thrombolytics
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Endpoint Results
[SCHINDLER1999]
Retrospective study Mar 1993 - Jun 1997
51 CRT 18 treated/18 M/F: 2/16 Solid tumor n=14 Hematology malignancy: n=4 Median time to diagnosis from CVC insertion: 46 days (3-180)
Cancer High-dose chemotherapy Diagnosis Doppler US or venography
Hickman CVC: 14/18 (78%) PICC: 4/18 (22%)
Urokinase: IV CP 75 000 - 150 000 UI/h for 24 to 96 hours (median: 48 hours) in a peripheral vein of the upper limb where the CRT was located followed by UFH and warfarin (INR 2 to 3)
Recanalization on phlebography Major bleeding
Clinical response: 18/18 (100%) Complete clinical response: 8/18 (44%) Partial clinical response: 10/18 (56%) Complete radiologic response: 0/18 (0%) Partial radiologic response: 9/18 (50%) Radiologic failure: 9/18 (50%)
Recurrent CVC thrombosis: 4/18 (22%) CVC salvaged: 12/18 (67%)
Bleeding complications: 4/18 (22%) Minor bleeding: 3/18 (17%) Major bleeding: 1/18 (5.6%)
[PUCHEU1996]
Retrospective study Jan 1989 - Oct 1994
412 patients with systematic Doppler US
57 CR: 15 partial CRT + 42 complete CRT
32 patients treated by systemic fibrinolysis
Cancer + chemotherapy Totally implantable venous access devices Vena cava syndrome not specified
Arm A (n=32): Streptokinase: 16/32 (50%) Urokinase: 5 rt-PA: 4/32 (12.5%) Streptokinase + urokinase : 7/32 (21.8%) Fibrinolysis followed by enoxaparin for 3 weeks then VKA
Arm B (n=25): Enoxaparin for 3 weeks then VKA
Repermeabilization on Doppler US
Arm A: 16/32 (50%) with no difference between the fibrinolytic drugs Arm B: 1/25 (5%) p=0.009
PE Death Major bleeding
2/25 without PE confirmation 0/25 death 0/25 major bleeding

94 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
6.2. Data analysis
LMWH + VKA
Studies
2 prospective non-randomized studies
[SAVAGE1999] [KOVACS2007] 1 retrospective study
[TRAN2010]
Agreement Not applicable, poor quality (39, 46 and 64 patients)
Quality of evidence Very low (observational studies, serious limitations, serious imprecision)
Results There are insufficient data to determine the efficacy and tolerance of LMWH + VKA for treating CVC-VTE.
Catheter removal
Studies 1 retrospective study
[FRANK2000]
Agreement Not applicable
Quality of evidence Very low (observational study, serious limitations)
Results
There are insufficient data to conclude on the efficacy and tolerance of CVC withdrawal for treating CVC-VTE. There are no data on the optimal timing between withdrawal and the initiation of anticoagulant therapy.
Thrombolytics
Studies 2 retrospective studies
[PUCHEU1996][SCHINDLER1999]
Agreement Yes
Quality of evidence Very low (observational studies, serious limitations, very serious imprecision)
Results
There are insufficient data to determine the efficacy and tolerance of systemic or localized thrombolytic therapy for treatment of CVC-VTE. Nonetheless thrombolysis can be used even with intensive chemotherapy.
Conclusions
There is no evidence in cancer patients with catheter-related thrombosis to support:
• The withdrawal of a non-infected, functioning, well-positioned CVC
• The use of LMWH + VKA or long-term LMWH
• Thrombolytic therapy via the catheter or systemic thrombolysis.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 95 Copyright © 1093790 (OPIC 28/02/2012)
6.3. Discussion
Central venous catheters/access devices (CVC or CVAD) are an essential part of therapy for
cancer patients, facilitating blood sampling, drug and intravenous fluid/nutrition delivery and
blood product administration. One of the unavoidable complications associated with this
convenience is CVC-associated VTE. In one prospective study of 444 consecutive cancer
patients, 19 patients (4.3%) suffered a symptomatic CVC-related DVT at a median of 30 (range
6-162) days post-catheter placement, corresponding to an incidence of 0.3 per 1000 catheter-
days (95%CI: [0.2-0.5]) [LEE2006]. A prospective study of 2144 patients with peripherally
inserted central venous catheters (PICC) found a similar rate of thrombosis (3%) [EVANS2010].
Consequently, treatment of CVC associated thrombosis is a routine part of contemporary
oncology practice. Our systematic review of studies evaluating the treatment of CVC-
associated thrombosis found 2 non-randomized prospective studies of anticoagulation
[SAVAGE1999] [KOVACS2007], 1 retrospective study of CVC removal [FRANK2000],
2 retrospective studies of localized or systemic thrombolysis [PUCHEU1996] [SCHINDLER1999]
and 1 retrospective study with a variable treatment approach (thrombolysis, CVC removal and
anticoagulation) [TRAN2010]. Although both the studies on anticoagulation and the two
studies on thrombolysis found evidence of a favorable treatment response, the level of
evidence was very poor. Current recommendations are therefore based upon expert opinion
and treatment choice is left to the discretion of the treating physician.
The experts do not recommend catheter removal if all the following conditions are met: (i) the
distal catheter tip is in the right position (at the junction between the superior vena cava and
the right atrium), (ii) the catheter is functional (good blood reflux), (iii) the catheter is
mandatory or vital for the patient, and (iv) there is no fever or any sign or symptom of infected
thrombophlebitis. In contrast, catheter removal is warranted if there is a prime risk factor for
thrombosis (catheter too short, misplaced, etc. ). There are no reliable data on the optimal
duration of anticoagulant treatment after catheter removal.
The basis for this recommendation is several-fold:
1. CVC-associated VTE represents a triggered episode of VTE associated with the CVC and the
coagulopathy associated with the underlying cancer and its treatment.
2. The risk for recurrence is high, as long as the CVC remains in place, therefore treatment
should continue until the CVC is removed.
3. Most cancer patients will need another form of central venous access after CVC removal.
Placement of another CVC will likely place them at high risk for recurrent CVC-VTE.
4. It is likely that underlying activation of coagulation associated with this triggered event will
abate in a time course similar to that of other triggered VTE (i.e. surgery, trauma); therefore at
least 3 months of anticoagulation should be sufficient.
5. Once the CVC has been removed and at least 3 months of anticoagulation have been
completed, patients with CVC-VTE should be at low risk for recurrent VTE, as their thrombotic
event required the presence of a CVC as a local trigger.
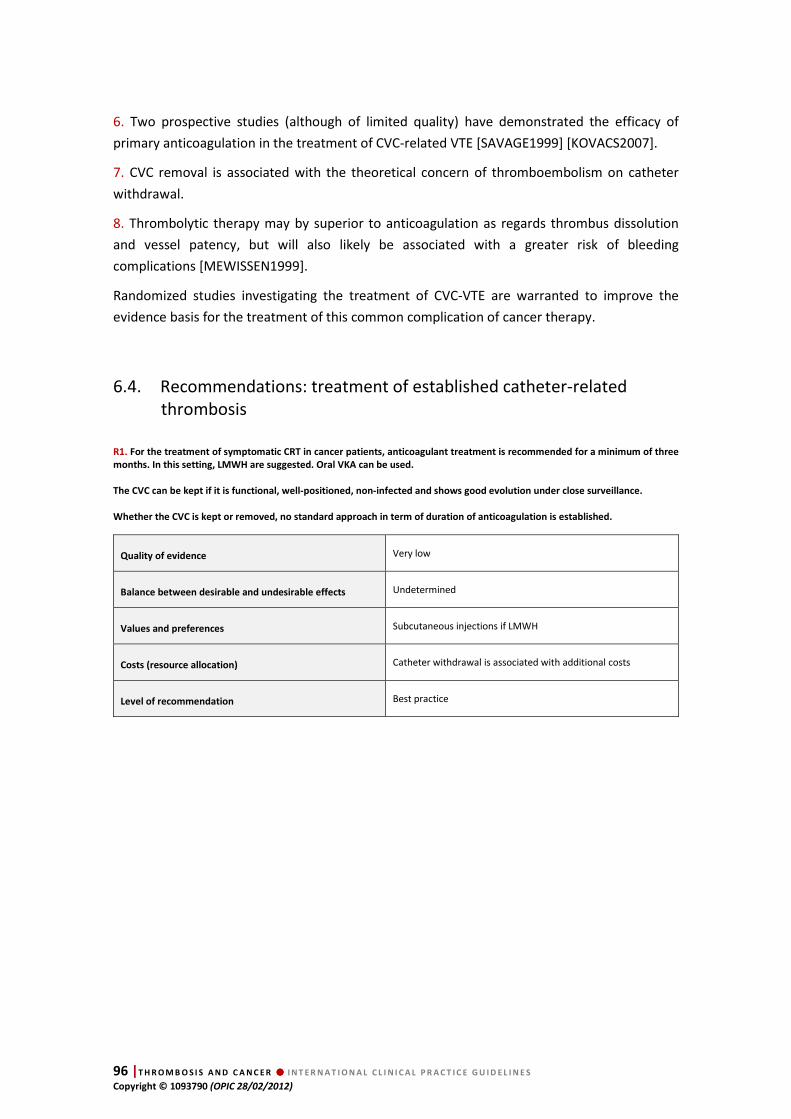
96 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
6. Two prospective studies (although of limited quality) have demonstrated the efficacy of
primary anticoagulation in the treatment of CVC-related VTE [SAVAGE1999] [KOVACS2007].
7. CVC removal is associated with the theoretical concern of thromboembolism on catheter
withdrawal.
8. Thrombolytic therapy may by superior to anticoagulation as regards thrombus dissolution
and vessel patency, but will also likely be associated with a greater risk of bleeding
complications [MEWISSEN1999].
Randomized studies investigating the treatment of CVC-VTE are warranted to improve the
evidence basis for the treatment of this common complication of cancer therapy.
6.4. Recommendations: treatment of established catheter-related thrombosis
R1. For the treatment of symptomatic CRT in cancer patients, anticoagulant treatment is recommended for a minimum of three
months. In this setting, LMWH are suggested. Oral VKA can be used.
The CVC can be kept if it is functional, well-positioned, non-infected and shows good evolution under close surveillance.
Whether the CVC is kept or removed, no standard approach in term of duration of anticoagulation is established.
Quality of evidence Very low
Balance between desirable and undesirable effects Undetermined
Values and preferences Subcutaneous injections if LMWH
Costs (resource allocation) Catheter withdrawal is associated with additional costs
Level of recommendation Best practice
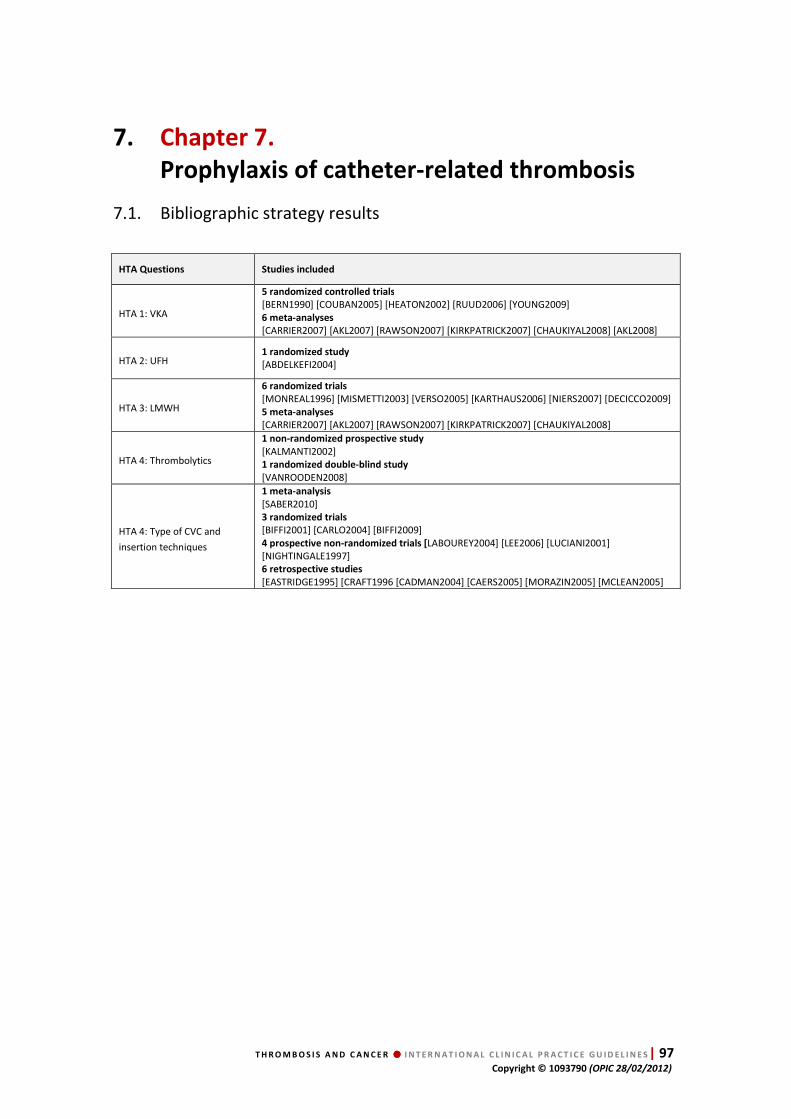
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 97 Copyright © 1093790 (OPIC 28/02/2012)
7. Chapter 7.
Prophylaxis of catheter-related thrombosis
7.1. Bibliographic strategy results
HTA Questions Studies included
HTA 1: VKA
5 randomized controlled trials
[BERN1990] [COUBAN2005] [HEATON2002] [RUUD2006] [YOUNG2009] 6 meta-analyses
[CARRIER2007] [AKL2007] [RAWSON2007] [KIRKPATRICK2007] [CHAUKIYAL2008] [AKL2008]
HTA 2: UFH 1 randomized study
[ABDELKEFI2004]
HTA 3: LMWH
6 randomized trials
[MONREAL1996] [MISMETTI2003] [VERSO2005] [KARTHAUS2006] [NIERS2007] [DECICCO2009] 5 meta-analyses
[CARRIER2007] [AKL2007] [RAWSON2007] [KIRKPATRICK2007] [CHAUKIYAL2008]
HTA 4: Thrombolytics
1 non-randomized prospective study
[KALMANTI2002] 1 randomized double-blind study
[VANROODEN2008]
HTA 4: Type of CVC and
insertion techniques
1 meta-analysis
[SABER2010] 3 randomized trials
[BIFFI2001] [CARLO2004] [BIFFI2009] 4 prospective non-randomized trials [LABOUREY2004] [LEE2006] [LUCIANI2001] [NIGHTINGALE1997] 6 retrospective studies
[EASTRIDGE1995] [CRAFT1996 [CADMAN2004] [CAERS2005] [MORAZIN2005] [MCLEAN2005]

98 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
7.2. Data extraction Table 31 Randomized studies: VKA in the prevention of catheter-related thrombosis (CRT)
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Catheter flushing Endpoint Arm A Arm B p value
95%CI
[BERN1990]
Randomized controlled trial Not specified
121/82 patients
90 days
Solid tumors Lymphomas CVC ("port-a-cath", subclavian) Chemotherapy Inclusion 3 days before catheter insertion
Arm A (n=42): Warfarin 1 mg/day (3 days before CVC insertion and until Day 90 after insertion) PT measured weekly for 1 month, then at least monthly. If PT ≥15 seconds, then warfarin stopped, Vitamin K given and warfarin resumed when PT normal Arm B (n=40): no warfarin (no placebo)
UFH up to 500 IU / week
Rate of CRT Phlebography at Day 90 orif symptoms occurred
4/42 (9.5% ) (4 symptomatic)
All CRT: 15/40 (37.5% ) Symptomatic CRT: 13/40 (32.5%)
p <0.001
[COUBAN2005]
Randomized controlled trial Mar 1999 - Jul 2002
255/255 patients
Median: 25 (1-184) weeks
Solid tumors: 20% Most tumors: hematological malignancies
Arm A (n=130): Warfarin 1 mg/day (72h after catheter insertion), median duration: 8 weeks Arm B (n=125): Placebo, median duration: 9 weeks
Not specified Rate of symptomatic CRT 6/130 (4.6%) 5/125 (4.0%) HR=1.20 95% CI: [0.37-3.94]
Death 22/130 (17%) 21/125 (17%) p=0.98
Major bleeding 0/130 (0%) 3 /125 (2%) p=0.07 95% CI: [-5.1-0.3]
[RUUD2006]
Randomized controlled trial Jan 2002 - Oct 2003
73/62 patients
6 months
Children with cancer
Catheter inserted in the jugular vein
Arm A (n=29): Warfarin 0.1 mg/kg started on the day of catheter insertion (1.3 < INR < 1.9) Arm B (n=33): no warfarin
Frequency of INR in target range: 64%
Not specified Asymptomatic CRT Doppler US performed at Months 1, 3, 6
Arm A: 14/29 (48%) (intent-to-treat analysis: 15/31; 48%) Arm B: 12/33 (36%) (intent-to-treat analysis: 17/42; 40%) p=0.44 (intent-to-treat analysis of the 73 patients: p=0.63)
Major bleeding Arm A: 2 events Arm B: 0 events (p not specified)
Symptomatic events (CRT / PE)
Arm A: 1 patient / 0 patient Arm B: 1 patient / 0 patient (p not specified)
[HEATON2002]
Randomized controlled trial Not specified
102 CVC placed in 88 patients 88 first CVC in the 88 patients studied
90 days
Hematological malignancies Subclavian catheter Hickman + Groshong®
Arm A (45/51): Warfarin 1 mg/day started on the day of catheter insertion Arm B (43/51): No anticoagulation
Hickman: UFH 50 mg x2/day
Groshong®: NaCl
Number of patients with CRT confirmed by phlebography
Thrombosis: 8/45 (17.8%) Vein Thrombosis: 2/45 (4.4%) Intra luminal catheter thrombus: 6/45 (13.3%)
Thrombosis: 5/43 (11.6%) Vein thrombosis: 1/43 (2.3%) Intraluminal catheter thrombus: 4/43 (9.3%)
p=0.42

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 99 Copyright © 1093790 (OPIC 28/02/2012)
Table 31 Randomized studies: VKA in the prevention of catheter-related thrombosis (CRT) - (continued)
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Catheter flushing Endpoint Arm A Arm B p value
95%CI
[YOUNG2009]
Randomized controlled trial Not specified
1590/1570 patients
Not specified
Solid or hematological tumors Age >16 years
High frequency of colorectal tumor (52%)
CVC Chemotherapy
A: warfarin 1 mg/day B: warfarin (INR 1.5 to 2) C: control (no warfarin)
812 assigned to uncertain warfarin benefit randomized to A or B or C 778 assigned to certain warfarin benefit randomized to A or B
Analysis 1 Warfarin (408 patients: 322 in A + 84 in B) vs. no warfarin (404 patients)
Analysis 2 Fixed dose A: 471 patients vs. adjusted dose B: 473 patients
Not specified Symptomatic CRT radiologicaly confirmed
Any dose of warfarin: 24/404 (5.9%)
No warfarin: 24/408 (5.9%)
OR=0,99 95%CI: [0.57-1.72] p=0,98
Fixed dose of warfarin: 34/471 (7.2%)
Adjusted dose of warfarin: 13/473 (2.7%)
OR=0.38 95%CI: [0.20-0.71] p=0.002
Major bleeding Any dose of warfarin: 7/408 (1.7%)
No warfarin: 1/404 (0.25%)
OR=6.93 95%CI: [0.86-56.00] p=0.07
Fixed dose of warfarin: 7/471 (1.5%)
Adjusted dose of warfarin: 16/473 (3.4%)
OR=2,28 95%CI: [0.95-5.48] p=0.04

100 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 32 Randomized studies: heparins in the prevention of catheter-related thrombosis (CRT)
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Catheter flushing Endpoint Arm A Arm B p value
95%CI
[ABDELKEFI2004]
Randomized controlled trial May 2002 - Sep 2003
108/108 patients
128 CVC patients/128
17 months
Adults <60 years Children >4 years Bone marrow transplant
Arm A (patients: 55, CVC: 65): UFH (continuous IV perfusion 100 IU/kg/day), maximum: 10 000 IU/day) Arm B (patients: 53, CVC: 63): saline 50 mL/day
Catheter obstruction urokinase (2500 IU in 9.5 mL)
Symptomatic CRT+ asymptomatic CRT (Doppler US at catheter removal)
1/65 (1.5%) 8/63 (12.6%) p=0.03
Major bleeding 2/65 (3%) 3/63 (4.7%) RR=0.95 95%CI: [0.06-14.6] p >0.05
[KARTHAUS2006]
Randomized double-blind study Aug 1999 - Jun 2001
439/425 patients
16 weeks
Cancer Chemotherapy CVC inserted 5 to 7 days before randomization A/B: 2/1 Solid tumors: 271/125 Hematological tumors: 23/20
Arm A (294 included / 285 treated): dalteparin 5000 IU SC x1/day for 16 weeks
Arm B (145 included / 140 treated) : placebo SC x1/day for 16 weeks
UFH 500 IU
Symptomatic CRT 11/285 (3.7%) 5/140 (3.4%) RR=1.08; 95%CI: [0.37-3.19] p=0.88
Asymptomatic CRT (phlebography or Doppler US for patients under 35 years)
11/285 (3.7%) 6/140 (4.1%) OR=0.81 95%CI: [0.29-2.29] p >0.05
Major bleeding Major and minor bleeding
1/285 (0.35%) 50/285 (17.5%)
1/140 (0.7%) 21/140 (15.0%)
RR=1.20 95%CI: [0.69-2.10] p=NS
[MISMETTI2003]
Randomized controlled trial May 1998 - Mar 2000
59 /45 patients
6 months
Adults Solid tumors CVC
Arm A (29 included / 21 evaluated): nadroparin SC 2850 IU x1/day, started 2h before catheter insertion
Arm B (30 included / 24 evaluated) : warfarin 1 mg/day, started 3 days before catheter insertion
for 90±5 days or up to symptomatic CRT
Saline (10 mL) and heparinized saline (500 IU, 5 mL)
Asymptomatic and symptomatic CRT (venography) at 90 days
6/21 (28.6 %) 4/24 (16.7%) p=0.48
All VTE events at 6 months
8/22 (36.4%) 4/24 (16.7% ) p=0.13
Major bleeding 1 patient 0 patient p not specified
[MONREAL1996]
Prospective open study Mar 1993 - Mar 1995
32/29 patients
90 days
Solid tumors CVC (Port-a-cath) platelet count >100 G/L no previous DVT
Arm A (n=16): dalteparin 2500 IU x1/day, started 2h before catheter insertion Arm B (n=13): no treatment
For 90 days or up to symptomatic CRTconfirmed by phlebography
Heparinized saline (10 mL, once a week)
Asymptomatic CRT (venography)
1/16 (6.2%) 8/13 (61.5%) RR=6.75 95%CI: [1.05-43.58] p=0.002
Major bleeding 1 patient 0 patient p not specified
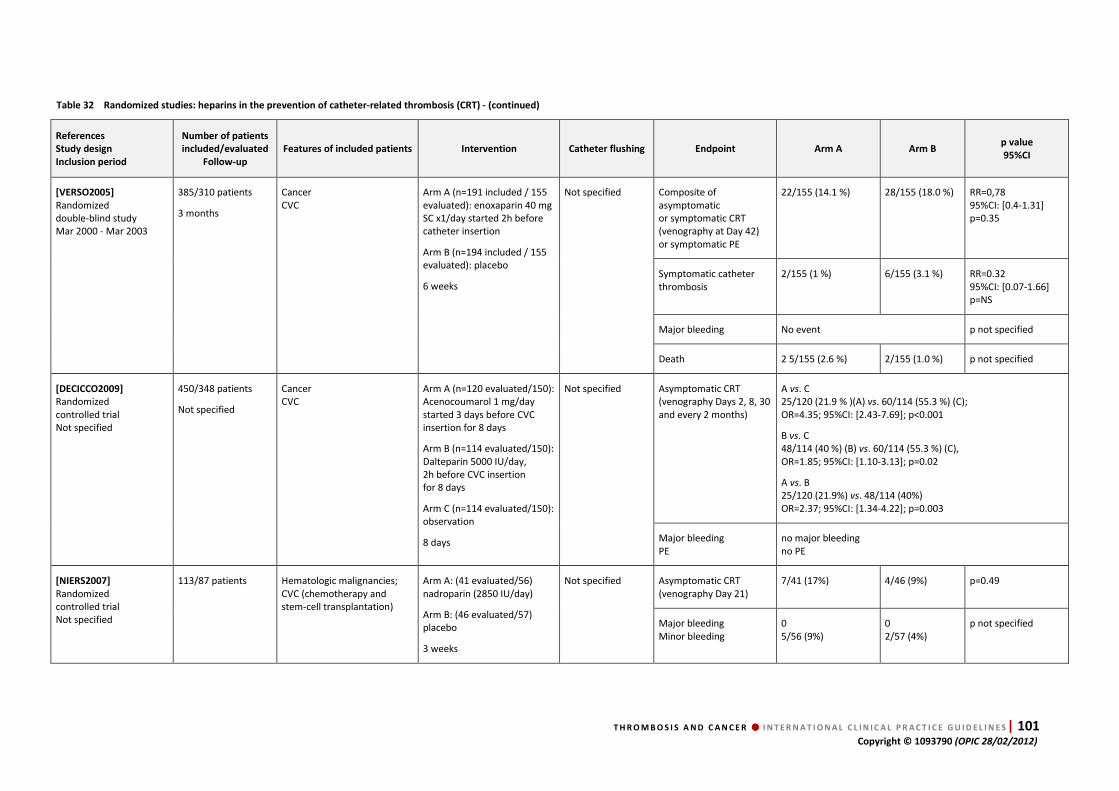
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 101 Copyright © 1093790 (OPIC 28/02/2012)
Table 32 Randomized studies: heparins in the prevention of catheter-related thrombosis (CRT) - (continued)
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Catheter flushing Endpoint Arm A Arm B p value
95%CI
[VERSO2005]
Randomized double-blind study Mar 2000 - Mar 2003
385/310 patients
3 months
Cancer CVC
Arm A (n=191 included / 155 evaluated): enoxaparin 40 mg SC x1/day started 2h before catheter insertion
Arm B (n=194 included / 155 evaluated): placebo
6 weeks
Not specified Composite of asymptomatic or symptomatic CRT (venography at Day 42) or symptomatic PE
22/155 (14.1 %) 28/155 (18.0 %) RR=0,78 95%CI: [0.4-1.31] p=0.35
Symptomatic catheter thrombosis
2/155 (1 %) 6/155 (3.1 %) RR=0.32 95%CI: [0.07-1.66] p=NS
Major bleeding No event p not specified
Death 2 5/155 (2.6 %) 2/155 (1.0 %) p not specified
[DECICCO2009]
Randomized controlled trial Not specified
450/348 patients
Not specified
Cancer CVC
Arm A (n=120 evaluated/150): Acenocoumarol 1 mg/day started 3 days before CVC insertion for 8 days
Arm B (n=114 evaluated/150): Dalteparin 5000 IU/day, 2h before CVC insertion for 8 days
Arm C (n=114 evaluated/150): observation
8 days
Not specified Asymptomatic CRT (venography Days 2, 8, 30 and every 2 months)
A vs. C 25/120 (21.9 % )(A) vs. 60/114 (55.3 %) (C); OR=4.35; 95%CI: [2.43-7.69]; p<0.001
B vs. C 48/114 (40 %) (B) vs. 60/114 (55.3 %) (C), OR=1.85; 95%CI: [1.10-3.13]; p=0.02
A vs. B 25/120 (21.9%) vs. 48/114 (40%) OR=2.37; 95%CI: [1.34-4.22]; p=0.003
Major bleeding PE
no major bleeding no PE
[NIERS2007]
Randomized controlled trial Not specified
113/87 patients Hematologic malignancies; CVC (chemotherapy and stem-cell transplantation)
Arm A: (41 evaluated/56) nadroparin (2850 IU/day)
Arm B: (46 evaluated/57) placebo
3 weeks
Not specified Asymptomatic CRT (venography Day 21)
7/41 (17%) 4/46 (9%) p=0.49
Major bleeding Minor bleeding
0 5/56 (9%)
0 2/57 (4%)
p not specified

102 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 33 Meta-analysis: anticoagulation (VKA, UFH, and LMWH) in the prevention of catheter-related thrombosis (CRT)
References
Bibliographic search
Number of studies analyzed
Period of study selection
Number of patients
Treatment Thrombosis Bleeding Other outcomes
[CARRIER2007] Medline® (1950 - 2007) Embase® (1980 - 2007) CCTR (first semester 2007)
7 studies; 1950 - 2007
2131 patients
VKA (warfarin 1 mg) or LMWH
Symptomatic CRT (defined as upper extremity DVT or CVC occlusion)
VKA vs. control: RR=0.82; 95%CI: [0.46-1.47]
LMWH vs. control: RR=0.473; 95%CI: [0.120-1.560]
VKA or LMWH vs. control: RR=0.71; 95%CI: [0.42-1.20]
Major Bleeding
VKA vs. control: 0 vs. 3 (2%) RR=0.14; 95%CI: [0.001-2.63]
LMWH vs. control: RR=0.49; 95%CI: [0.03-7.83]
Minor Bleeding
VKA vs. control: RR=0.93; 95%CI: [0.31-2.77]
LMWH vs. Control: RR=1.32; 95%CI: [0.87-2.02]
Mortality
VKA vs. control RR=0.95; 95%CI: [0.62-1.46]
LMWH vs. control RR=1.51; 95%CI: [0.49-4.70]
[RAWSON2007] Medline® (1966 - 2007) Embase® (1988 - 2007) Cancerlit (1975 - 2007) Cinahl (1982 - 2007) ASCO abstracts (1999 - 2007) ASH abstracts (2001 - 2007)
4 studies 1966 - 2007
1236 patients
Warfarin 1 mg or INR >1.5
Symptomatic or asymptomatic CRT
VKA vs. control: 40/625 (6.4%) vs. 46/611 (7.5%) Risk difference: 5.0% ; 95%CI: [-9.0%-5.0%]; p=0.56
[KIRKPATRICK2007] Medline® (1964 - 2006) Embase® (2002 - 2005) ASCO, abstracts (1999 - 2006) ISTH, abstracts (2001 - 2005)
15 studies (10 studies on only cancer patients)
1714 patients
VKA (fixed low dose) or LMWH
CRT (symptomatic or asymptomatic)
VKA vs. control: 30/162 (18.5%) vs. 78/154 (50.6%) RR=0.37; 95%CI: [0.26-0.52]; p <0.001
LMWH vs. control: 93/617 (15.1%) vs. 113/447 (25.3%) RR=0.72; 95%CI: [0.57-0.90]; p=0.045
LMWH vs. VKA: 46/114 (40.4%) vs. 26/120 (21.7%) RR=1.88; 95%CI: [1.28-2.75]
CRT (symptomatic)
VKA vs. control: 12/217 (5.5%) vs. 19/208 (9.1%) RR=0.60; 95%CI: [0.30-1.20]
LMWH vs. control: 12/500 (2.4%) vs. 11/352 (3.1%) RR=0.69; 95%CI: [0.30-1.59]
Major bleeding
VKA vs. control: 0/175 (0%) vs. 3/168 (1.8%) RR=0.24; 95%CI: [0.03-2.13]
LMWH vs. control: 1/529 (0.2%) vs. 1/368 (0.3%) RR=0.66; 95%CI: [0.12-3.68]
All-cause mortality
VKA vs. control RR=0.95; 95%CI: [0.62-1.46]
LMWH vs. control: RR=1.57; 95%CI: [0.54-4.58]
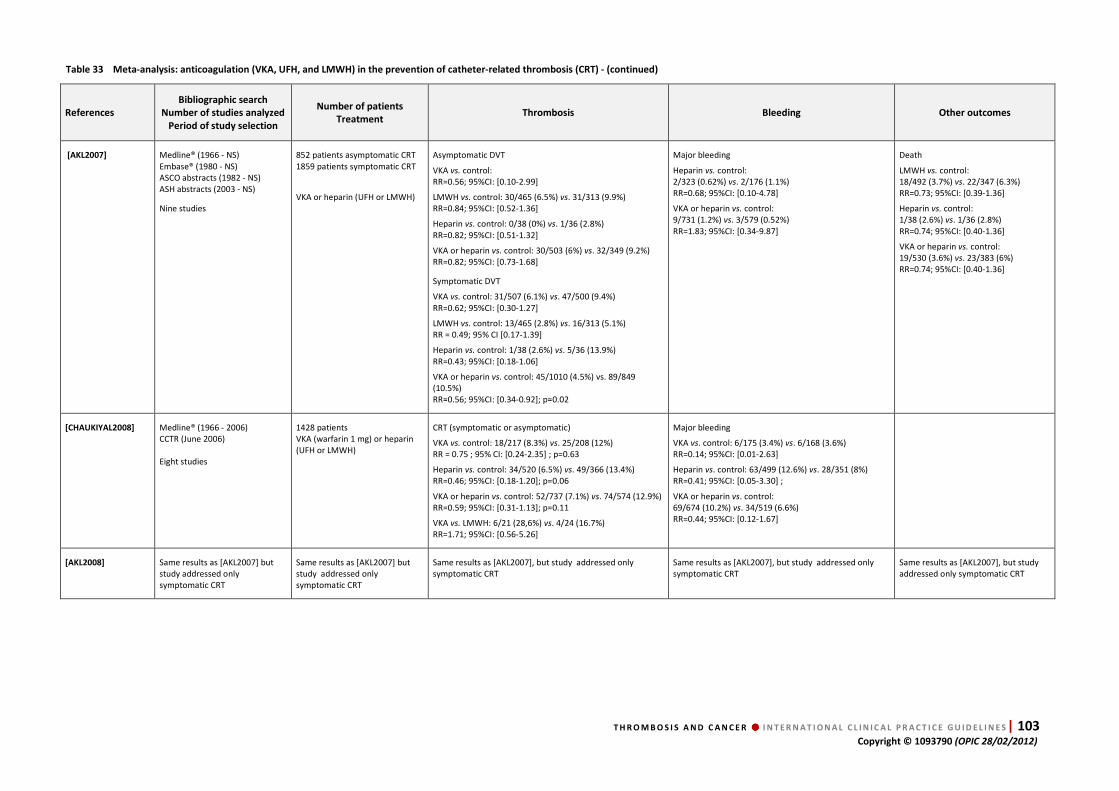
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 103 Copyright © 1093790 (OPIC 28/02/2012)
Table 33 Meta-analysis: anticoagulation (VKA, UFH, and LMWH) in the prevention of catheter-related thrombosis (CRT) - (continued)
References
Bibliographic search
Number of studies analyzed
Period of study selection
Number of patients
Treatment Thrombosis Bleeding Other outcomes
[AKL2007] Medline® (1966 - NS) Embase® (1980 - NS) ASCO abstracts (1982 - NS) ASH abstracts (2003 - NS)
Nine studies
852 patients asymptomatic CRT 1859 patients symptomatic CRT
VKA or heparin (UFH or LMWH)
Asymptomatic DVT
VKA vs. control: RR=0.56; 95%CI: [0.10-2.99]
LMWH vs. control: 30/465 (6.5%) vs. 31/313 (9.9%) RR=0.84; 95%CI: [0.52-1.36]
Heparin vs. control: 0/38 (0%) vs. 1/36 (2.8%) RR=0.82; 95%CI: [0.51-1.32]
VKA or heparin vs. control: 30/503 (6%) vs. 32/349 (9.2%) RR=0.82; 95%CI: [0.73-1.68]
Symptomatic DVT
VKA vs. control: 31/507 (6.1%) vs. 47/500 (9.4%) RR=0.62; 95%CI: [0.30-1.27]
LMWH vs. control: 13/465 (2.8%) vs. 16/313 (5.1%) RR = 0.49; 95% CI [0.17-1.39]
Heparin vs. control: 1/38 (2.6%) vs. 5/36 (13.9%) RR=0.43; 95%CI: [0.18-1.06]
VKA or heparin vs. control: 45/1010 (4.5%) vs. 89/849 (10.5%) RR=0.56; 95%CI: [0.34-0.92]; p=0.02
Major bleeding
Heparin vs. control: 2/323 (0.62%) vs. 2/176 (1.1%) RR=0.68; 95%CI: [0.10-4.78]
VKA or heparin vs. control: 9/731 (1.2%) vs. 3/579 (0.52%) RR=1.83; 95%CI: [0.34-9.87]
Death
LMWH vs. control: 18/492 (3.7%) vs. 22/347 (6.3%) RR=0.73; 95%CI: [0.39-1.36]
Heparin vs. control: 1/38 (2.6%) vs. 1/36 (2.8%) RR=0.74; 95%CI: [0.40-1.36]
VKA or heparin vs. control: 19/530 (3.6%) vs. 23/383 (6%) RR=0.74; 95%CI: [0.40-1.36]
[CHAUKIYAL2008] Medline® (1966 - 2006) CCTR (June 2006) Eight studies
1428 patients VKA (warfarin 1 mg) or heparin (UFH or LMWH)
CRT (symptomatic or asymptomatic)
VKA vs. control: 18/217 (8.3%) vs. 25/208 (12%) RR = 0.75 ; 95% CI: [0.24-2.35] ; p=0.63
Heparin vs. control: 34/520 (6.5%) vs. 49/366 (13.4%) RR=0.46; 95%CI: [0.18-1.20]; p=0.06
VKA or heparin vs. control: 52/737 (7.1%) vs. 74/574 (12.9%) RR=0.59; 95%CI: [0.31-1.13]; p=0.11
VKA vs. LMWH: 6/21 (28,6%) vs. 4/24 (16.7%) RR=1.71; 95%CI: [0.56-5.26]
Major bleeding
VKA vs. control: 6/175 (3.4%) vs. 6/168 (3.6%) RR=0.14; 95%CI: [0.01-2.63]
Heparin vs. control: 63/499 (12.6%) vs. 28/351 (8%) RR=0.41; 95%CI: [0.05-3.30] ;
VKA or heparin vs. control: 69/674 (10.2%) vs. 34/519 (6.6%) RR=0.44; 95%CI: [0.12-1.67]
[AKL2008] Same results as [AKL2007] but study addressed only symptomatic CRT
Same results as [AKL2007] but study addressed only symptomatic CRT
Same results as [AKL2007], but study addressed only symptomatic CRT
Same results as [AKL2007], but study addressed only symptomatic CRT
Same results as [AKL2007], but study addressed only symptomatic CRT
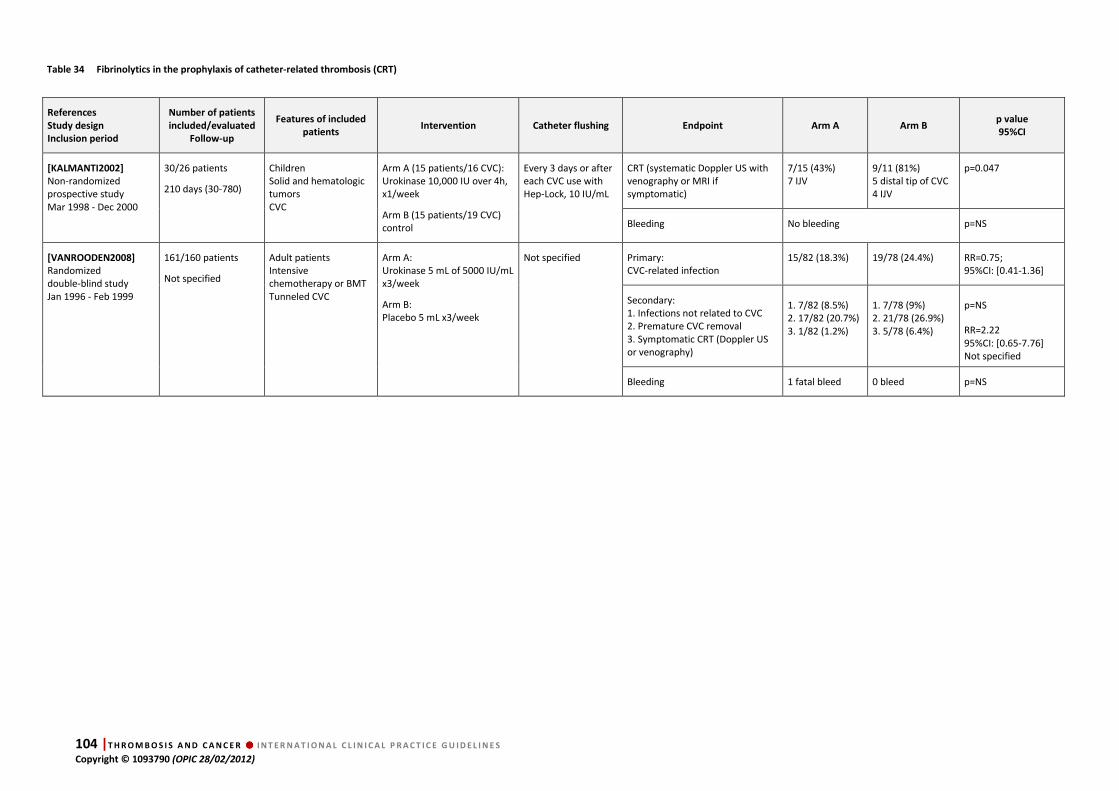
104 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 34 Fibrinolytics in the prophylaxis of catheter-related thrombosis (CRT)
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included
patients Intervention Catheter flushing Endpoint Arm A Arm B
p value
95%CI
[KALMANTI2002]
Non-randomized prospective study Mar 1998 - Dec 2000
30/26 patients
210 days (30-780)
Children Solid and hematologic tumors CVC
Arm A (15 patients/16 CVC): Urokinase 10,000 IU over 4h, x1/week
Arm B (15 patients/19 CVC) control
Every 3 days or after each CVC use with Hep-Lock, 10 IU/mL
CRT (systematic Doppler US with venography or MRI if symptomatic)
7/15 (43%) 7 IJV
9/11 (81%) 5 distal tip of CVC 4 IJV
p=0.047
Bleeding No bleeding p=NS
[VANROODEN2008]
Randomized double-blind study Jan 1996 - Feb 1999
161/160 patients
Not specified
Adult patients Intensive chemotherapy or BMT Tunneled CVC
Arm A: Urokinase 5 mL of 5000 IU/mL x3/week
Arm B: Placebo 5 mL x3/week
Not specified Primary: CVC-related infection
15/82 (18.3%) 19/78 (24.4%) RR=0.75; 95%CI: [0.41-1.36]
Secondary: 1. Infections not related to CVC 2. Premature CVC removal 3. Symptomatic CRT (Doppler US or venography)
1. 7/82 (8.5%) 2. 17/82 (20.7%) 3. 1/82 (1.2%)
1. 7/78 (9%) 2. 21/78 (26.9%) 3. 5/78 (6.4%)
p=NS
RR=2.22 95%CI: [0.65-7.76] Not specified
Bleeding 1 fatal bleed 0 bleed p=NS

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 105 Copyright © 1093790 (OPIC 28/02/2012)
Table 35 Influence of type, position and method of insertion of catheter in the primary prevention of CVC-associated thrombosis: non-randomized prospective trials and retrospective studies
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Endpoint Results
[NIGHTINGALE1997]
Non-randomized prospective study 1993 -1994
949/832 patients
Not specified
Gastrointestinal cancer Tunneled CVC in: - right subclavian vein (727) - left subclavian vein (81) - right femoral vein (2) - jugular vein (1)
Warfarin (1 mg/day) Flushing: heparinized saline
1. Thrombotic complications leading to CVC removal
2. Predictive factor for CVC removal (multivariate analysis)
1. 4.7% (38/817); p=NS If distal CVC tip in SVC: 3.5% (20/569) If distal CVC tip in right atrium: 2.5%, (4/160),
2. CVC in SVC: HR=2.57; 95%CI: [1.29-5.11]
[LUCIANI2001]
Non-randomized prospective study 1995 - 1998
145 patientsts/not specified 113 CVC/not specified
>3 years
Oropharyngeal tract cancer Totally implantable CVC
Flushing: saline (10 mL), then heparinized saline (5 mL at 50 UI/mL)
Asymptomatic or symptomatic CVC-associated DVT (Doppler US)
11.7% (17/145), 76% asymptomatic
1. Distal CVC tip location SVC or junction SVC-right atrium: 6% (5/87) Above junction SVC-right atrium: 46% (12/26); p <0.001
2. Left-sided CVC: 65% (11/17) Right-sided CVC: 35% (6/17), p=NS
[LABOUREY2004]
Non-randomized prospective study One year but not specified
246 patients/not specified 249 CVC/not specified
332 days (1-725)
Solid tumors CVC not specified
Flushing: 3-5 mL heparinized saline (100 UI/mL) after insertion Occlusion: urokinase (5000 to 10000 units)
Catheter occlusion
Catheter-related thrombosis
1. Catheter occlusion: CVC >T4: 4/5 (80%) vs. CVC <T4: 9/244 (3.6%); p <0.001
2. CRT as mediastinal and/or cervical mass: >6 cm: 5/12 (41%) vs. <6 cm: 6/237 (2.5%); p <0.001
[LEE2006]
Non-randomized prospective study 2002 - 2003
444 patients/not specified 555 CVC/not specified CVC removal + 4 weeks or up to 52 weeks after CVC insertion
Solid tumors (66%) Hematologic malignancies (34%) All types of CVC in the upper limb vasculature
Flushing: - Implanted ports: heparinized saline (100 U/mL), - Other CVC: saline
Predictive factors for symptomatic CVC-associated DVT (Doppler US, venography, contrast-computed tomography, or MRI) by multivariate analysis
1. >1 insertion attempts: OR=5.5; 95%CI: [1.2-24.6]; p=0.03 2. Previous CVC insertion: OR=3.8;95%CI: [1.4-10.4]; p=0.01 3. CVC blockage: OR=14.7; 95%CI: [5.5-40]; p <0.001
[EASTRIDGE1995]
Non-randomized retrospective study 1989 - 1992
274 patients/not specified 332 CVC/not specified
Not specified
Solid tumors (51%) Hematologic malignancies (49%) Tunneled CVC (65%) Implantable CVC (35%)
Flushing: heparinized saline (3 mL/day at 100 UI/mL)
Predictive factors for symptomatic CVC-associated DVT (venography or clinical follow-up)
1. Position of CVC tip and CRT: >T3 CRT: 78% vs. <T3 CRT: 37%; p<0.05 2. Triple-lumen CVC CRT: 21% (10/48) vs. Double-lumen CVC CRT: 7% (11/160); p<0.05 3. Implantable CVC CRT: 6% (7/113) vs. Tunneled CVC CRT; 10% (21/209); p=NS
[CRAFT1996]
Non-randomized retrospective study Not specified
122/120 patients 153/150 CVC 55 days (1-650)
Solid tumors (48%) Hematologic malignancies (41%) Tunneled CVC (Hickman®)
Flushing: heparinized saline CVC-associated DVT
Predictive factors for symptomatic CVC-associated DVT (venography)
8% (12/150)
1. Position of CVC tip: - Junction SVC-right atrium or lower third of SVC CRT: 6/73 (8.2%) - Upper third of SVC CRT 3/40 (7.5%); RR=0.9; 95%CI: [0.2-3.4]; p=NS 2. Side of CVC: Right-sided: CRT 4/92 (5%) vs. Left-sided: CRT 4/21 (19%) RR=4.4; 95%CI: [1.2-16]; p=0.04

106 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 35 Influence of type, position and method of insertion of catheter in the primary prevention of CVC-associated thrombosis: non-randomized prospective trials and retrospective studies (continued)
References
Study design
Inclusion period
Number of patients
included/evaluated
Follow-up
Features of included patients Intervention Endpoint Results
[CADMAN2004]
Randomly sampled retrospective study 1996 - 2001
334 patients/not specified 448 CVC/not specified
72 (1-720) days
Solid tumors (69%) Hematologic malignancies (31%) Tunneled CVC
Not specified CVC-associated DVT
Predictive factors for symptomatic CVC-associated DVT (venography, Doppler US)
9% (30/334) 1. Position of CVC tip: - Right atrium: 0% - Lower third of SVC: 2.6% - Middle third of SVC: 5.3% - Upper third of SVC: 41.7%; p <0.005 2. Side of CVC placement: - Right-sided: 6.8% - Left-sided: 25.6%; p <0.001
[CAERS2005]
Non-randomized Retrospective study 1993 - 1998
437 patients/not specified 448 CVC/not specified
Solid tumors (84%) Hematologic malignancies (13%)
Flushing: saline (10 mL), then heparinized saline (5 mL at 100 UI/mL)
Predictive factors for symptomatic CVC-associated DVT (venography, Doppler US) (multivariate analysis)
8.5% (37/437) CVC tip vs. right atrium or inferior vena cava: Brachiocephalic vein: OR=64.7; 95%CI: [7.6-553.8] Cranial part of the SVC: OR=17.4; 95%CI: [2.0-148.8]
[MORAZIN2005]
Non-randomized prospective study 1995 - 1999
5447 CVC/not specified
Up to CVC removal
Solid tumors (50% breast cancer) Tunneled CVC (silicone)
Not specified CVC-associated DVT Predictive factors for symptomatic CVC-associated DVT (venography, Doppler US, contrast computed tomography) (multivariate analysis)
2.5% (135/5447)
1. Left subclavian vein + jugular vein vs. right subclavian vein: RR=2.6; 95% CI not provided; p <0.001 2. Femoral vein vs. right subclavian vein: RR=6.5; p <0.001 3. Placement duration >25 min vs. ≤25 min: RR=1.52; p=0.02
[MCLEAN2005]
Retrospective analysis of 2 phase III studies Jun 1992 - Nov 1999
374/362 patients 362/308 CVC
Children + ALL Internal CVC: 245 External CVC: 63
Chemotherapy induction for ALL Not specified for CVC
Predictive factors for CRT, CVC removal and CVC infection (multivariate analysis)
External vs. internal CVC: 1. Infection: OR=3.1; 95%CI: [1.3-7.5]; p=0.01 2. Thrombosis: OR=3.9; 95%CI: [1.5-10.3]; p=0.006 3. Removal: OR=5.6; 95%CI: [2.7-11.6]; p=0.001
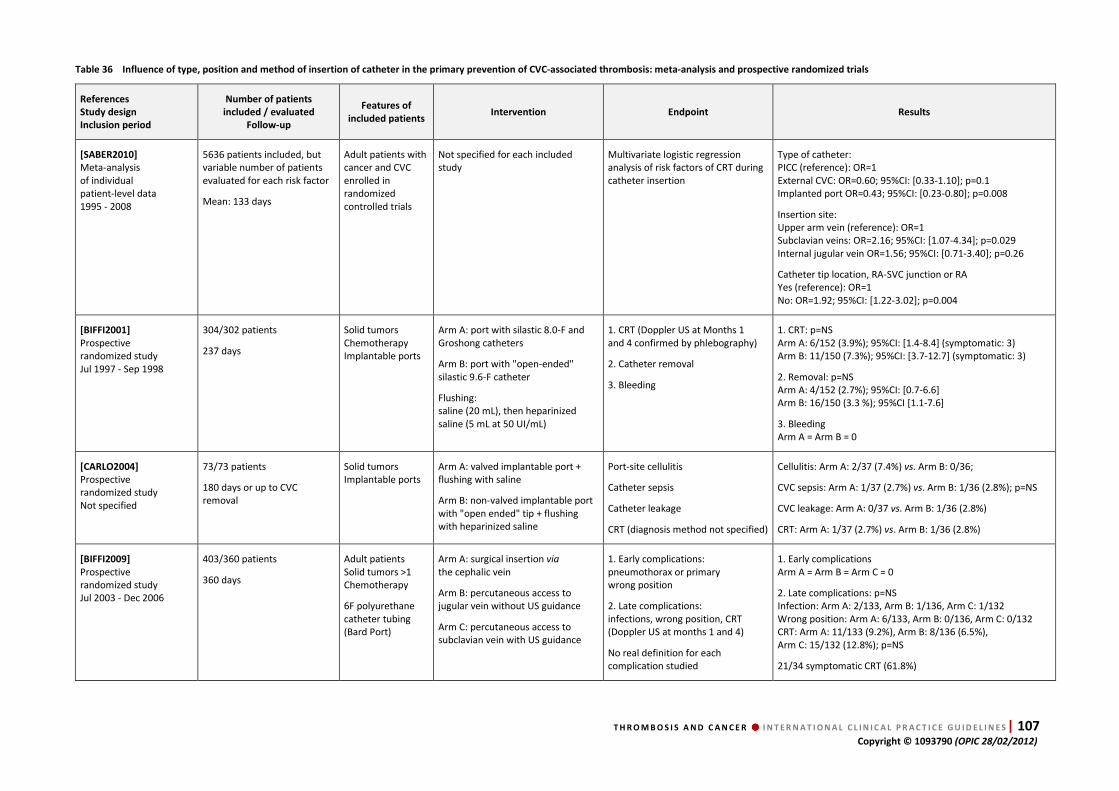
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 107 Copyright © 1093790 (OPIC 28/02/2012)
Table 36 Influence of type, position and method of insertion of catheter in the primary prevention of CVC-associated thrombosis: meta-analysis and prospective randomized trials
References
Study design
Inclusion period
Number of patients
included / evaluated
Follow-up
Features of
included patients Intervention Endpoint Results
[SABER2010]
Meta-analysis of individual patient-level data 1995 - 2008
5636 patients included, but variable number of patients evaluated for each risk factor
Mean: 133 days
Adult patients with cancer and CVC enrolled in randomized controlled trials
Not specified for each included study
Multivariate logistic regression analysis of risk factors of CRT during catheter insertion
Type of catheter: PICC (reference): OR=1 External CVC: OR=0.60; 95%CI: [0.33-1.10]; p=0.1 Implanted port OR=0.43; 95%CI: [0.23-0.80]; p=0.008
Insertion site: Upper arm vein (reference): OR=1 Subclavian veins: OR=2.16; 95%CI: [1.07-4.34]; p=0.029 Internal jugular vein OR=1.56; 95%CI: [0.71-3.40]; p=0.26
Catheter tip location, RA-SVC junction or RA Yes (reference): OR=1 No: OR=1.92; 95%CI: [1.22-3.02]; p=0.004
[BIFFI2001]
Prospective randomized study Jul 1997 - Sep 1998
304/302 patients
237 days
Solid tumors Chemotherapy Implantable ports
Arm A: port with silastic 8.0-F and Groshong catheters
Arm B: port with "open-ended" silastic 9.6-F catheter
Flushing: saline (20 mL), then heparinized saline (5 mL at 50 UI/mL)
1. CRT (Doppler US at Months 1 and 4 confirmed by phlebography)
2. Catheter removal
3. Bleeding
1. CRT: p=NS Arm A: 6/152 (3.9%); 95%CI: [1.4-8.4] (symptomatic: 3) Arm B: 11/150 (7.3%); 95%CI: [3.7-12.7] (symptomatic: 3)
2. Removal: p=NS Arm A: 4/152 (2.7%); 95%CI: [0.7-6.6] Arm B: 16/150 (3.3 %); 95%CI [1.1-7.6]
3. Bleeding Arm A = Arm B = 0
[CARLO2004]
Prospective randomized study Not specified
73/73 patients
180 days or up to CVC removal
Solid tumors Implantable ports
Arm A: valved implantable port + flushing with saline
Arm B: non-valved implantable port with "open ended" tip + flushing with heparinized saline
Port-site cellulitis
Catheter sepsis
Catheter leakage
CRT (diagnosis method not specified)
Cellulitis: Arm A: 2/37 (7.4%) vs. Arm B: 0/36;
CVC sepsis: Arm A: 1/37 (2.7%) vs. Arm B: 1/36 (2.8%); p=NS
CVC leakage: Arm A: 0/37 vs. Arm B: 1/36 (2.8%)
CRT: Arm A: 1/37 (2.7%) vs. Arm B: 1/36 (2.8%)
[BIFFI2009]
Prospective randomized study Jul 2003 - Dec 2006
403/360 patients
360 days
Adult patients Solid tumors >1 Chemotherapy
6F polyurethane catheter tubing (Bard Port)
Arm A: surgical insertion via the cephalic vein
Arm B: percutaneous access to jugular vein without US guidance
Arm C: percutaneous access to subclavian vein with US guidance
1. Early complications: pneumothorax or primary wrong position
2. Late complications: infections, wrong position, CRT (Doppler US at months 1 and 4)
No real definition for each complication studied
1. Early complications Arm A = Arm B = Arm C = 0
2. Late complications: p=NS Infection: Arm A: 2/133, Arm B: 1/136, Arm C: 1/132 Wrong position: Arm A: 6/133, Arm B: 0/136, Arm C: 0/132 CRT: Arm A: 11/133 (9.2%), Arm B: 8/136 (6.5%), Arm C: 15/132 (12.8%); p=NS
21/34 symptomatic CRT (61.8%)
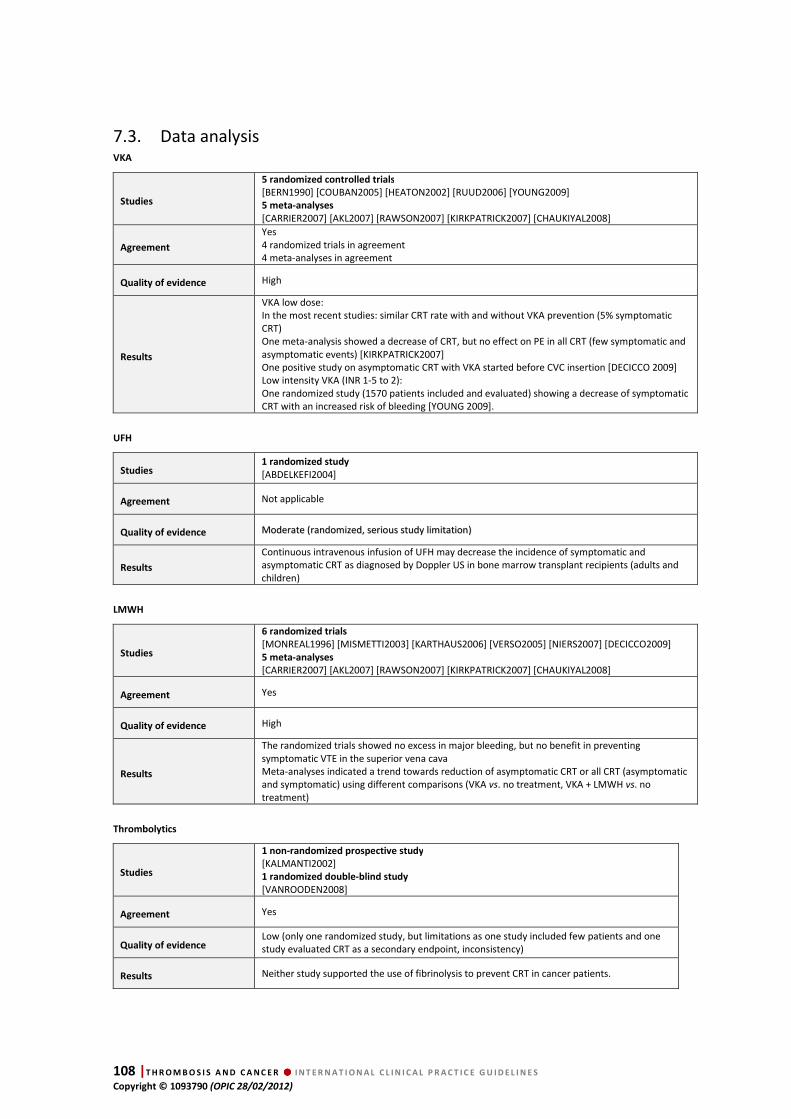
108 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
7.3. Data analysis VKA
Studies
5 randomized controlled trials
[BERN1990] [COUBAN2005] [HEATON2002] [RUUD2006] [YOUNG2009] 5 meta-analyses
[CARRIER2007] [AKL2007] [RAWSON2007] [KIRKPATRICK2007] [CHAUKIYAL2008]
Agreement
Yes 4 randomized trials in agreement 4 meta-analyses in agreement
Quality of evidence High
Results
VKA low dose: In the most recent studies: similar CRT rate with and without VKA prevention (5% symptomatic CRT) One meta-analysis showed a decrease of CRT, but no effect on PE in all CRT (few symptomatic and asymptomatic events) [KIRKPATRICK2007] One positive study on asymptomatic CRT with VKA started before CVC insertion [DECICCO 2009] Low intensity VKA (INR 1-5 to 2): One randomized study (1570 patients included and evaluated) showing a decrease of symptomatic CRT with an increased risk of bleeding [YOUNG 2009].
UFH
Studies 1 randomized study
[ABDELKEFI2004]
Agreement Not applicable
Quality of evidence MMooddeerraattee ((rraannddoommiizzeedd,, sseerriioouuss ssttuuddyy lliimmiittaattiioonn))
Results
Continuous intravenous infusion of UFH may decrease the incidence of symptomatic and asymptomatic CRT as diagnosed by Doppler US in bone marrow transplant recipients (adults and children)
LMWH
Studies
6 randomized trials
[MONREAL1996] [MISMETTI2003] [KARTHAUS2006] [VERSO2005] [NIERS2007] [DECICCO2009] 5 meta-analyses
[CARRIER2007] [AKL2007] [RAWSON2007] [KIRKPATRICK2007] [CHAUKIYAL2008]
Agreement Yes
Quality of evidence High
Results
The randomized trials showed no excess in major bleeding, but no benefit in preventing symptomatic VTE in the superior vena cava Meta-analyses indicated a trend towards reduction of asymptomatic CRT or all CRT (asymptomatic and symptomatic) using different comparisons (VKA vs. no treatment, VKA + LMWH vs. no treatment)
Thrombolytics
Studies
1 non-randomized prospective study
[KALMANTI2002] 1 randomized double-blind study
[VANROODEN2008]
Agreement Yes
Quality of evidence Low (only one randomized study, but limitations as one study included few patients and one study evaluated CRT as a secondary endpoint, inconsistency)
Results Neither study supported the use of fibrinolysis to prevent CRT in cancer patients.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 109 Copyright © 1093790 (OPIC 28/02/2012)
Conclusions
For the prevention of CRT, when compared to no prophylaxis, there is no evidence to support:
• the routine use of low dose of VKA (warfarin 1 mg )
• the routine use of VKA to maintain an INR between 1.5 and 2
• the use of continuous IV UFH or fibrinolytics
• the routine use of LMWH
Type of CVC and insertion techniques
Studies
1 meta-analysis
[SABER2010] 3 randomized trials
[BIFFI2001] [CARLO2004] [BIFFI2009] 4 prospective non-randomized trials [LABOUREY2004] [LEE2006] [LUCIANI2001] [NIGHTINGALE1997] 6 retrospective studies
[EASTRIDGE1995] [CRAFT1996] [CADMAN2004] [CAERS2005] [MORAZIN2005] [MCLEAN2005]
Agreement Yes
Quality of evidence High (meta-analysis + consistency)
Results
Independent risk factors for CRT include: - Catheter tip location: SVC-RA junction or RA - Insertion site: jugular vein better than subclavian, right side better than left side - Type of catheter: valved tips = open-ended tips, implanted ports better than external catheter - Past medical history of CVC - Doppler US guidance: no data
Conclusion
The catheter should be located:
• at the SVC-RA junction
• in the jugular vein rather than the subclavian vein
Implanted ports are better than a SC catheter
There is no evidence to support the use of Doppler US guidance to prevent CRT.
7.4. Discussion
Central venous catheter thrombosis is an important cause of morbidity in cancer patients
[LEE2007; AKL2008A]. Consequently, many investigators have attempted to identify an
effective CVC-DVT prophylaxis regimen. An open, randomized study by Bern and colleagues
suggested that low-dose warfarin (1 mg daily) could significantly reduce the incidence of
CVC-DVT in cancer patients (37.5% vs. 9.5%) [BERN1999]. However, several subsequent RCTs
failed to demonstrate any protective effect with fixed low-dose warfarin [HEATON2002]
[COUBAN2005] [RUUD2006] [YOUNG2009]. In the WARP study, a large multicenter open-label
study comparing no warfarin, fixed dose warfarin (1 mg daily) and adjusted-dose warfarin
(INR 1.5 to 2.0), Young and colleagues demonstrated that adjusted-dose warfarin was
associated with a significant reduction in CRT (13/473, 2.7% vs. 34/471, 7.2%; OR=0.38; 95%CI:
[0.20-0.71]; p=0.002), but also with a trend towards more major bleeding events (16/473, 3.4%

110 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
vs. 7/471, 1.5%; p=0.04) when compared with fixed-dose VKA [YOUNG2009]. Randomized,
controlled trials of LMWH showed a similar findings. A small, open RCT conducted by Monreal
et al. demonstrated that dalteparin 2500 IU once daily significantly reduced CVC-DVT
compared with no treatment (1/16, 6.2% vs. 8/13, 61.5%; p=0.002) [MONREAL1996].
However, subsequent larger RCTs employing prophylactic regimens of dalteparin, nadroparin
and enoxaparin were unable to demonstrate reductions in CVC-DVT [VERSO2005]
[KARTHAUS2006] [NIERS2007] [DECICCO2009]. A small, open-label trial of continuous infusion
UFH (100 IU/kg/day) performed in adult and pediatric bone marrow transplant patients noted
a significant reduction in CVC-DVT (1/65 1.5% vs. 8/63 12.6%; p=0.03) [ABDELKEFI2004].
However, this regimen has not been replicated perhaps because it is rather cumbersome and
labor-intensive to administer.
Two studies tested thrombolytic agents in the prevention of CVC-DVT [KALMANTI2002]
[VANROODEN2008]. In a small study in 30 pediatric oncology patients, Kalmanti et al found
that 10000 units of urokinase administered once weekly reduced the rate of CVC thrombosis
from 81% (9/11) to 43% (7/15) [KALMANTI2002]. No bleeding was noted. In contrast, Van
Rooden et al found no difference in symptomatic CRT, catheter-related and non-catheter-
associated infections and premature catheter removal with 5000 units of urokinase
administered three times weekly compared with placebo [VANROODEN2008].
Six meta-analyses of anticoagulant CVC thromboprophylaxis have been performed
[CARRIER2007] [RAWSON2007] [KIRKPATRICK2007] [AKL2007] [CHAUKIYAL2008] [AKL2008].
Carrier et al. and Kirkpatrick et al. did not note any reduction in symptomatic CVC-associated
DVT, while Akl et al. found a 44% relative risk reduction in symptomatic CVC-DVT episodes
when the results of all anticoagulant modalities were combined [AKL2007]. Kirkpatrick et al.
reported that VKA and LMWH were associated with a 63% and 28% relative risk reduction,
respectively, in all CVC-DVT (asymptomatic plus symptomatic) [KIRKPATRICK2007], whereas
Chaukiyal et al. did not, likely due to differences in study inclusion criteria [CHAUKIYAL2008].
No study demonstrated the superiority of any anti-thrombotic regimen (e.g., VKA vs. LMWH).
No differences in major bleeding or mortality between control patients and patients receiving
anticoagulants were noted.
Retrospective and prospective observational studies, as well as randomized controlled trials
[BIFFI2001] [CARLO2004] and one meta-analysis [SABER2011], suggest that catheter insertion
site (left>right, femoral>subclavian>jugular) and catheter tip location (SVC>RA) can influence
the risk of CVC-DVT. A history of a previous CVC and more than one insertion attempt were
found to be risk factors for CVC-DVT in one study [LEE2006]. Implanted ports may have a lower
risk than PICC catheters or external CVC [MCLEAN2005]. In contrast, ultrasound-guided
placement has not been shown to decrease CVC-DVT [BIFFI2009].
In summary, the existing literature does not support the use of thromboprophylaxis for CVC in
cancer patients. The results of the WARP trial [YOUNG2009] suggest that more intensive
anticoagulant regimens such as dose-adjusted warfarin may be promising, but more research
is warranted to identify convenient, effective and safe regimens for CVC thromboprophylaxis.
Catheter location can influence the risk of CVC-DVT, so low-risk locations should be
preferentially utilized.
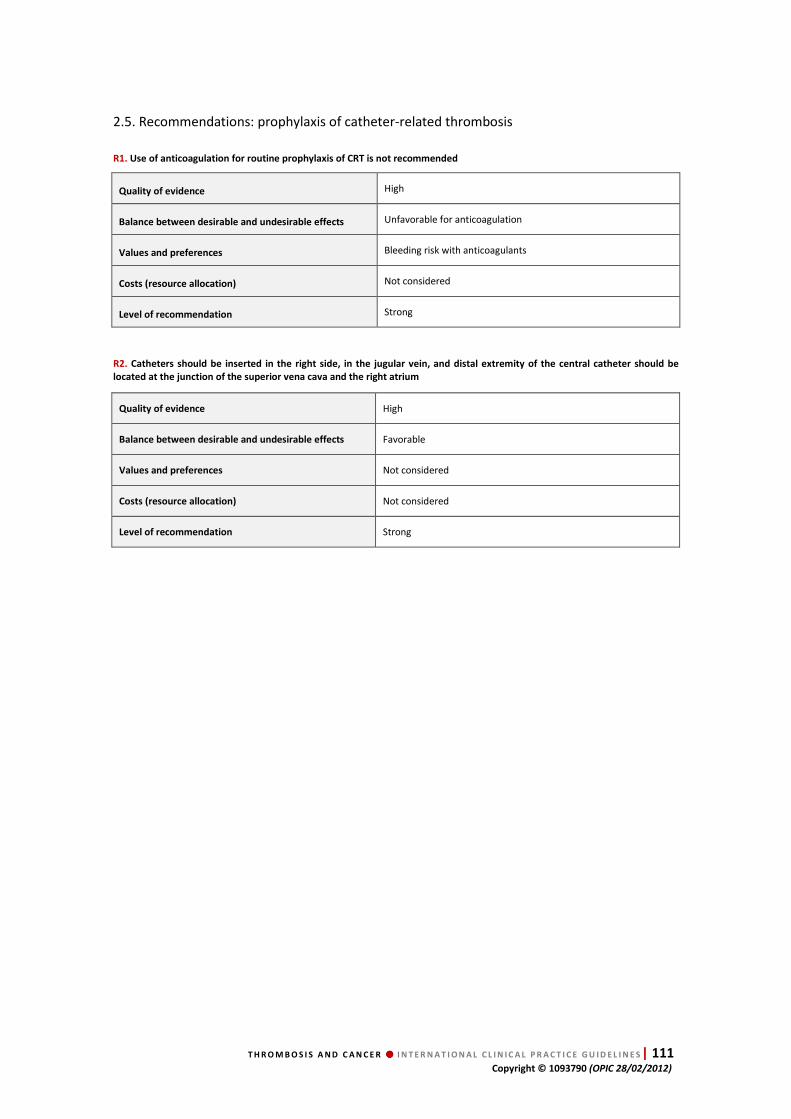
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 111 Copyright © 1093790 (OPIC 28/02/2012)
2.5. Recommendations: prophylaxis of catheter-related thrombosis
R1. Use of anticoagulation for routine prophylaxis of CRT is not recommended
Quality of evidence High
Balance between desirable and undesirable effects Unfavorable for anticoagulation
Values and preferences Bleeding risk with anticoagulants
Costs (resource allocation) Not considered
Level of recommendation Strong
R2. Catheters should be inserted in the right side, in the jugular vein, and distal extremity of the central catheter should be
located at the junction of the superior vena cava and the right atrium
Quality of evidence High
Balance between desirable and undesirable effects Favorable
Values and preferences Not considered
Costs (resource allocation) Not considered
Level of recommendation Strong
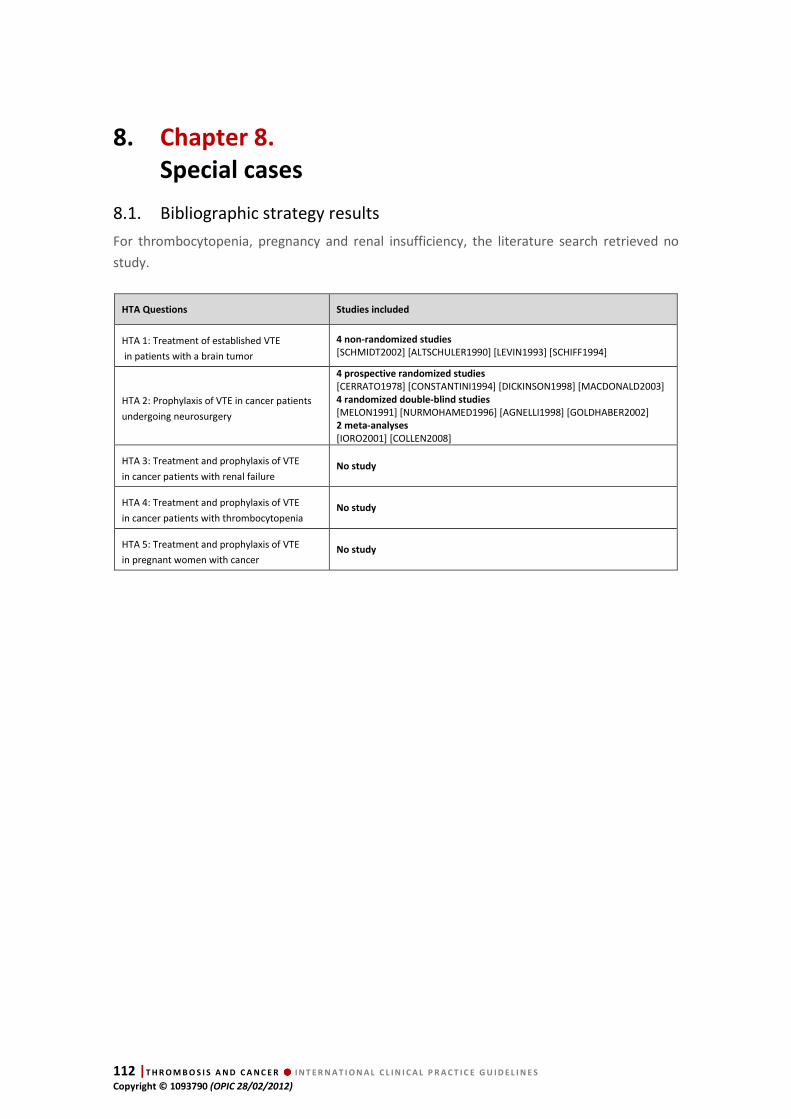
112 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
8. Chapter 8.
Special cases
8.1. Bibliographic strategy results
For thrombocytopenia, pregnancy and renal insufficiency, the literature search retrieved no
study.
HTA Questions Studies included
HTA 1: Treatment of established VTE
in patients with a brain tumor
4 non-randomized studies
[SCHMIDT2002] [ALTSCHULER1990] [LEVIN1993] [SCHIFF1994]
HTA 2: Prophylaxis of VTE in cancer patients
undergoing neurosurgery
4 prospective randomized studies
[CERRATO1978] [CONSTANTINI1994] [DICKINSON1998] [MACDONALD2003] 4 randomized double-blind studies
[MELON1991] [NURMOHAMED1996] [AGNELLI1998] [GOLDHABER2002] 2 meta-analyses
[IORO2001] [COLLEN2008]
HTA 3: Treatment and prophylaxis of VTE
in cancer patients with renal failure No study
HTA 4: Treatment and prophylaxis of VTE
in cancer patients with thrombocytopenia No study
HTA 5: Treatment and prophylaxis of VTE
in pregnant women with cancer No study

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 113 Copyright © 1093790 (OPIC 28/02/2012)
8.2. Data extraction
Table 37 Treatment of established VTE in patients with a brain tumor
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity
[SCHMIDT2002]
Prospective study Oct 1998 - Jan 2001
11/11 patients unspecified Patients with a histologically confirmed malignant brain tumor and proven DVT (Doppler US or venography) No surgery within the 48 hours before anticoagulation 9 glioblastomas, 1 anaplastic oligoastrocytoma et 1 anaplastic astrocytoma
Tinzaparin 175 IU/kg/day for 10 days then 100 IU/kg/day for 3 months Compression stockings for 3 months
No recurrence of VTE No major bleeding No HIT
[ALTSCHULER1990]
Retrospective study 1986 - not specified
23 patients unspecified Patients with astrocytoma or glioblastoma (proven by surgical biopsy) and DVT or PE DVT: 15 patients DVT + PE: 8 patients
Continuous IV heparin, then warfarin for 3 months
PE recurrence: 1 patient (bleeding � withdrawal of warfarin� recurrence � IVCF insertion)
Major bleeding : 4 patientss (gastrointestinal tract)
Treatment discontinuation: 8 patients: - 4 patients: gastrointestinal tract bleeding - 3 patients: no DVT on control - 1 patient: best supportive care
[LEVIN1993]
Retrospective multicenter study 1977 - 1991
42/49 patients unspecified Patients with a brain tumor or brain metastasis and proven DVT or PE
IVCF insertion (n=42) Warfarin (n=5) Inferior vena cava interruption (n=1) No treatment (n=1)
IVCF PE: 11.9 % (5/42) DVT: 21.4 % (9/42)
IVCF insertion-related complications: 3/42 Inferior vena cava or filter thrombosis: 11/42 (26.2%)
Anticoagulant treatment: no major bleeding
[SCHIFF1994]
Retrospective study Jan 1980 - Jul 1992
52 patients included 42 patients evaluated in the anticoagulant group 10 patients evaluated in the IVCF group
unspecified Patients with a brain metastasis and proven DVT or PE
IV heparin then warfarin (n=29) IV UFH alone (n=2) Warfarin alone (n=2) IV UFH then SC UFH (n=7) IV UFH, SC UFH then warfarin (n=2) IVCF (n=10) No treatment (n=2)
Anticoagulant group: 12% (5/42), 2 recurrences after anticoagulant discontinuation
IVCF (n=10) VTE: 40% (4/10) (2 PE)
Anticoagulant group: Major intracerebral bleeding: 7% (3/42) IVCF group: No bleeding complication 3 patients received anticoagulant therapy for thromboembolic events (2 PE) after IVCF insertion

114 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 38 VTE prophylaxis in cancer patients undergoing neurosurgery
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[CERRATO1978]
Randomized controlled study Not specified
Arm A: 50/50 patients Arm B: 50/50 patients
7 days Patients over 40 years of age Elective intracranial neurosurgery No suspicion of DVT on 125I-labeled fibrinogen test Arm A: 50 patients; cancer = 17 Arm B: 50 patients; cancer = 20
Arm A: control Arm B: UFH 5000 IU x3/day for 7 days with an heparin plasma level less than 0.18 units/mL
DVT on 125I-labeled fibrinogen test every day up to Day 7 after surgery
Arm A: 17/50 (34%) Arm B: 3/50 (6%); p <0.05
Postoperative hematoma Arm A: 1/50 (2%) Arm B: 1/50 (2%); p=NS
Postoperative transfusion Arm A: 25/50 (50%) Arm B: 28/50 56%); p=NS
Postoperative hemoglobin levels Arm A: -0.6±1.2 Arm B: -0.7±1.3; p=NS
Not specified
[MELON 1991]
Randomized double-blind study Not specified
Arm A: 64/67 patients Arm B: 58/63 patients
10 days Adult patients Weight between 45 and 90 kg Intracranial surgery (number of patients with cancer not specified) No intracranial bleeding on postoperative CT scan
Arm A: enoxaparin 20 mg/day Arm B: placebo
Phlebography on Day 10 or earlier if symptoms
DVT Arm A: 10/64 (15.6%) Arm B: 14/58 (24%); p=NS
No bleeding Not specified
[CONSTANTINI1994]
Randomized controlled study Not specified
103/103 patients 7 days Patients over 40 years of age Elective intracranial neurosurgery for brain tumor No preexisting changes in coagulation or severe systemic disease, no medication that influenced coagulation Meningioma: 63%; malignant tumor: 37%
Arm A: 1 mL 0.9% NaCl with 5000 IU heparin Arm B: placebo (0.9% NaCl alone)
x2/day from H-2 to Day 7 (maximum 14 doses)
Beginning of treatment: H-2
DVT Arm A: 2/55 (3.6%) Arm B: 2/48 (4.2%)
Gastrointestinal bleeding Arm A: 2/55 ((3.6%) Arm B: 1/48 (2.1%); p=NS
Cerebral hematoma requiring surgery Arm A: 1/55 (1.8%) Arm B: 1/48 (2.1%); p=NS
Postoperative transfusion Arm A: 7/55 (12.7%) Arm B: 7/48 (14.6%); p=NS
Day 7
Arm A: 0/55 (0%) Arm B: 1/48 (2.1%) p=NS
[NURMOHAMED1996]
Randomized double-blind study Not specified
Cancer patients Arm A: 196/241 patients Arm B: 210/241 patients
56 days Total population (n=241): patients over 18 years undergoing craniotomy or spinal surgery for a tumor or injury
Graduated compression stockings Arm A: nadroparin 7500 IU/day starting 18-24 h postoperatively Arm B: placebo
For 10 days or until discharge
Beginning of treatment: H-2
DVT (symptomatic and asymptomatic using Doppler US on Days 6, 8 and 10 post-surgery or venography on Day 10 post-surgery or at discharge Arm A: 31/166 (18.7%) Arm B: 47/179 (26.3%); p=0.047
All events at Day 56: Arm A: 33/241 (20.9%) Arm B: 51/244 (26.3%); p=0.018
Major bleeding Arm A: 6/241 (2.5%) Arm B: 2/244 (0.8%); p=0.087
Minor bleeding Arm A: 4/241 (1.7%) Arm B: 1/244 (0.4%); p=NS
All bleeding Arm A: 10/241 (4.1%) Arm B: 3/244 (1.2%); p=0.047
Day 56
Arm A: 22/241 (9.1%) Arm B: 10/244 (4.1%) p=0.026

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 115 Copyright © 1093790 (OPIC 28/02/2012)
Table 38 VTE prophylaxis in cancer patients undergoing neurosurgery (continued)
Reference
Inclusion period
Number of patients
analyzed/included Follow-up Population Intervention VTE incidence Toxicity Death
[AGNELLI1998]
Randomized double-blind studiy Not specified
Arm A: 130/153 patients
Arm B: 130/154 patients
60 days Patients >18 years, body weight between 40 and 120 kg undergoing elective cranial or spinal surgery. Meningioma: n=124 Glioma: n=85 Sheath tumors: n=25 Metastasis: n=20 Other tumors: n=45 No tumors: n=8
Thigh-length compression stockings for all patients Arm A: enoxaparin 40 mg/day Arm B: placebo 1/day
Beginning of treatment: within 24 h after surgery
Phlebography at day 8±1 and symptomatic confirmed DVT or PE Arm A: 22/130 (17%) Arm B: 43/130 (33%) RR=0.51; 95%CI: [0.33-0.80] p=0.004
Major and minor bleeding Arm A: 18/153 (12%) Arm B: 11/154 (7%) p=0.18
Day 60
Arm A: 6/153 (5%) Arm B: 5/154 (4%) p=NS
[DICKINSON1998]
Prospective randomized study Jan 1990 - Dec 1992
66/66 patients 1 month Patients 18 years of age or older with intracranial neoplasm and craniotomy
Arm A: SCD alone Arm B: enoxaparin 30 mg/day Arm C: SCD+enoxaparin 30 mg/day
Duration: up to discharge
Beginning of treatment: during anesthesia
Venous duplex ultrasonographic examinations at Day 1-3, Day 5-7, Day 10-14, Month 1 Arm A: 3/22 (13.6%) Arm B: 1/21 (4.7%) Arm C: 2/23 (8.7%) p=NS
Major bleeding Arm A: 0/22 Arm B: 2/21 (9.5%) Arm C: 3/23 (13.1%) Difference between enoxaparin groups and SCD group: p=0.024
Arm A: 1/22 (4.5%) Arm B: 1/21 (4.7%) Arm C: 0/23 (0%) p=NS
[GOLDHABER2002]
Randomized double-blind studiy Jun 1996 - Sep 2001
150/150 patients 30 days Patients undergoing craniotomy with suspected primary or metastatic brain tumor
All patients: intermittent pneumatic compression devices + GCS
Arm A: enoxaparin 40 mg morning + placebo evening Arm B: UFH 5000 IU morning and evening
Beginning of treatment: within 24 h after surgery
Duplex venous ultrasonography examination the day of discharge Arm A: 9/75 (12%) Arm B: 5/75 (6.7%) p=0.401
Major bleeding Arm A: 2/75 (2.7%) Arm B: 1/75 (1.3%) p=NS
No death during 30 days of follow-up.
[MACDONALD2003]
Prospective randomized study Sept 1998 - Dec 1999
97/100 patients 1 month Patients >18 years Craniotomy Cancer patients Arm A: 28/49 (47%) Arm B: 35/61 (69%)
SCD for all patients
Arm A: heparin 5000 IU SC x2/day Arm B: dalteparin 2500 IU x1/day
Duration: 7 days
Beginning of treatment: during surgery
Duplex ultrasound scanning of lower limbs Day 7 + symptomatic DVT and PE confirmed by ventilation-perfusion scan ,CT scan or angiography at one month
DVT Arm A: 0/49 (0%) Arm B: 2/51 (4%) (asymptomatic: n=1) No PE
Intracranial bleeding Arm A: 1/49 (2%) Arm B: 2/51 (4%) p=NS
Transfusion Arm A: 4/49 (8%) Arm B: 5/51 (8%) p=NS
Arm A: 1/49 (2%) Arm B: 0/51 (0%) p=NS
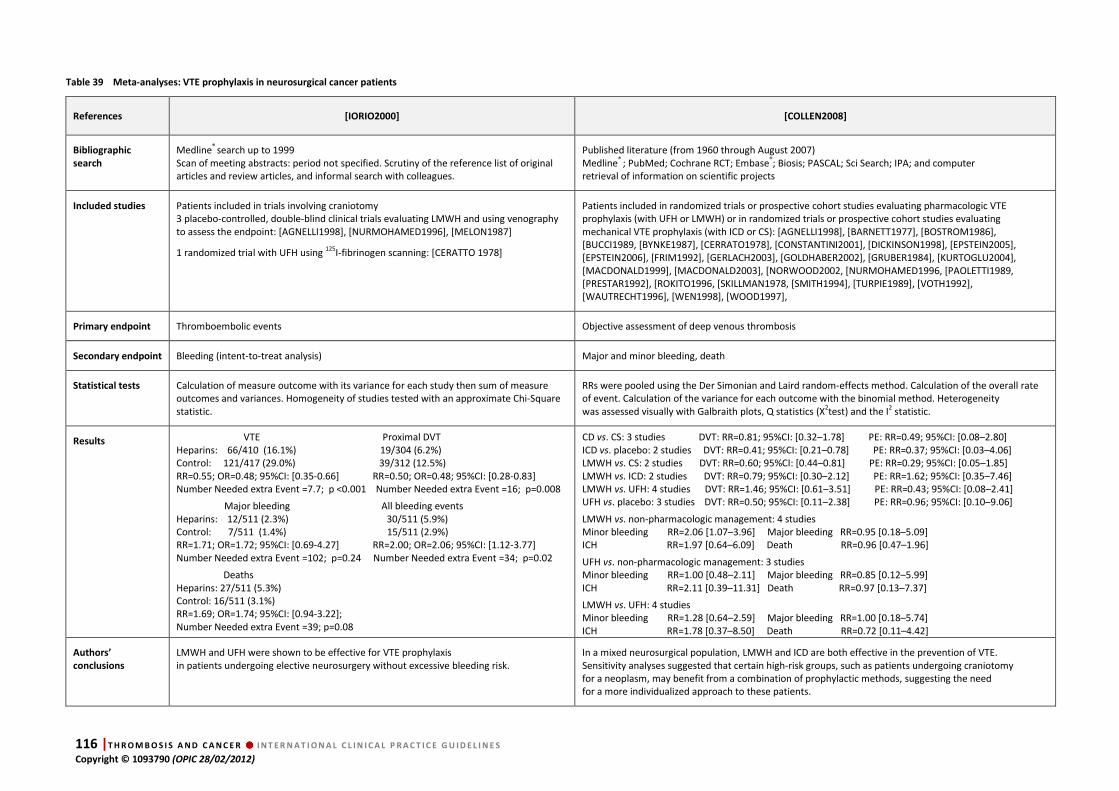
116 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Table 39 Meta-analyses: VTE prophylaxis in neurosurgical cancer patients
References [IORIO2000] [COLLEN2008]
Bibliographic
search
Medline® search up to 1999 Scan of meeting abstracts: period not specified. Scrutiny of the reference list of original articles and review articles, and informal search with colleagues.
Published literature (from 1960 through August 2007) Medline® ; PubMed; Cochrane RCT; Embase®; Biosis; PASCAL; Sci Search; IPA; and computer retrieval of information on scientific projects
Included studies Patients included in trials involving craniotomy 3 placebo-controlled, double-blind clinical trials evaluating LMWH and using venography to assess the endpoint: [AGNELLI1998], [NURMOHAMED1996], [MELON1987]
1 randomized trial with UFH using 125I-fibrinogen scanning: [CERATTO 1978]
Patients included in randomized trials or prospective cohort studies evaluating pharmacologic VTE prophylaxis (with UFH or LMWH) or in randomized trials or prospective cohort studies evaluating mechanical VTE prophylaxis (with ICD or CS): [AGNELLI1998], [BARNETT1977], [BOSTROM1986], [BUCCI1989, [BYNKE1987], [CERRATO1978], [CONSTANTINI2001], [DICKINSON1998], [EPSTEIN2005], [EPSTEIN2006], [FRIM1992], [GERLACH2003], [GOLDHABER2002], [GRUBER1984], [KURTOGLU2004], [MACDONALD1999], [MACDONALD2003], [NORWOOD2002, [NURMOHAMED1996, [PAOLETTI1989, [PRESTAR1992], [ROKITO1996, [SKILLMAN1978, [SMITH1994], [TURPIE1989], [VOTH1992], [WAUTRECHT1996], [WEN1998], [WOOD1997],
Primary endpoint Thromboembolic events Objective assessment of deep venous thrombosis
Secondary endpoint Bleeding (intent-to-treat analysis) Major and minor bleeding, death
Statistical tests Calculation of measure outcome with its variance for each study then sum of measure outcomes and variances. Homogeneity of studies tested with an approximate Chi-Square statistic.
RRs were pooled using the Der Simonian and Laird random-effects method. Calculation of the overall rate of event. Calculation of the variance for each outcome with the binomial method. Heterogeneity was assessed visually with Galbraith plots, Q statistics (X2test) and the I2 statistic.
Results VTE Proximal DVT Heparins: 66/410 (16.1%) 19/304 (6.2%) Control: 121/417 (29.0%) 39/312 (12.5%) RR=0.55; OR=0.48; 95%CI: [0.35-0.66] RR=0.50; OR=0.48; 95%CI: [0.28-0.83] Number Needed extra Event =7.7; p <0.001 Number Needed extra Event =16; p=0.008
Major bleeding All bleeding events Heparins: 12/511 (2.3%) 30/511 (5.9%) Control: 7/511 (1.4%) 15/511 (2.9%) RR=1.71; OR=1.72; 95%CI: [0.69-4.27] RR=2.00; OR=2.06; 95%CI: [1.12-3.77] Number Needed extra Event =102; p=0.24 Number Needed extra Event =34; p=0.02
Deaths Heparins: 27/511 (5.3%) Control: 16/511 (3.1%) RR=1.69; OR=1.74; 95%CI: [0.94-3.22]; Number Needed extra Event =39; p=0.08
CD vs. CS: 3 studies DVT: RR=0.81; 95%CI: [0.32–1.78] PE: RR=0.49; 95%CI: [0.08–2.80] ICD vs. placebo: 2 studies DVT: RR=0.41; 95%CI: [0.21–0.78] PE: RR=0.37; 95%CI: [0.03–4.06] LMWH vs. CS: 2 studies DVT: RR=0.60; 95%CI: [0.44–0.81] PE: RR=0.29; 95%CI: [0.05–1.85] LMWH vs. ICD: 2 studies DVT: RR=0.79; 95%CI: [0.30–2.12] PE: RR=1.62; 95%CI: [0.35–7.46] LMWH vs. UFH: 4 studies DVT: RR=1.46; 95%CI: [0.61–3.51] PE: RR=0.43; 95%CI: [0.08–2.41] UFH vs. placebo: 3 studies DVT: RR=0.50; 95%CI: [0.11–2.38] PE: RR=0.96; 95%CI: [0.10–9.06]
LMWH vs. non-pharmacologic management: 4 studies Minor bleeding RR=2.06 [1.07–3.96] Major bleeding RR=0.95 [0.18–5.09] ICH RR=1.97 [0.64–6.09] Death RR=0.96 [0.47–1.96]
UFH vs. non-pharmacologic management: 3 studies Minor bleeding RR=1.00 [0.48–2.11] Major bleeding RR=0.85 [0.12–5.99] ICH RR=2.11 [0.39–11.31] Death RR=0.97 [0.13–7.37]
LMWH vs. UFH: 4 studies Minor bleeding RR=1.28 [0.64–2.59] Major bleeding RR=1.00 [0.18–5.74] ICH RR=1.78 [0.37–8.50] Death RR=0.72 [0.11–4.42]
Authors’
conclusions
LMWH and UFH were shown to be effective for VTE prophylaxis in patients undergoing elective neurosurgery without excessive bleeding risk.
In a mixed neurosurgical population, LMWH and ICD are both effective in the prevention of VTE. Sensitivity analyses suggested that certain high-risk groups, such as patients undergoing craniotomy for a neoplasm, may benefit from a combination of prophylactic methods, suggesting the need for a more individualized approach to these patients.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 117 Copyright © 1093790 (OPIC 28/02/2012)
8.3. Data analysis Treatment of established VTE in patients with a brain tumor
Studies 4 non-randomized studies
[SCHMIDT2002] [ALTSCHULER1990] [LEVIN1993] [SCHIFF1994]
Agreement Yes
Quality of evidence LLooww ((oobbsseerrvvaattiioonnaall bbuutt ccoonnssiisstteenntt))
Results
In patients with brain tumors, treatment of VTE with use of anticoagulation yield the same rate of VTE recurrence (0 to 12%) and bleeding (intracerebral bleeding: 0 to 7%) as in other cancer patients without brain tumors.
Conclusion
The results of anticoagulation for established VTE are the same in patients with and without
brain tumors.
Prophylaxis of VTE in cancer patients undergoing neurosurgery: heparins
Studies
4 prospective randomized studies
[CERRATO1978] [CONSTANTINI1994] [DICKINSON1998] [MACDONALD2003] 4 randomized double-blind studies
[MELON1991] [NURMOHAMED1996] [AGNELLI1998] [GOLDHABER2002] 2 meta-analyses
[IORIO2000] [COLLEN2008]
Agreement Yes
Quality of evidence HHiigghh
Results
For VTE prophylaxis after surgery for brain or spinal tumors in cancer patients: - LMWH and UFH (5000 IU SC/12 h) are associated with the same rates of VTE and bleeding and lead to a 50% reduction in the risk of VTE without an excess of major bleeding but with a two-fold higher rate of minor bleeding. - GCS + IPC have the same efficacy as GCS alone - the reduction of VTE with ECD is about 60% when compared to no prophylaxis, - LMWH are superior to ECD with a reduction of VTE from 20 to 40%, and an increase of minor bleeding (relative risk: 2), with no increase in intracranial bleeding or major bleeding [COLLEN2008].
Conclusion
LMWH and UFH have a similar efficacy and safety (in terms of major bleeding and intracranial
bleeding) and are superior to no treatment. In this setting, pharmacological prophylaxis should
be started postoperatively.
After surgery for brain or spinal tumors, adding LMWH to an intermittent compression device
increases the risk of minor bleeding but not the risk of major or intracranial bleeding.
8.4. Discussion
The treatment of VTE in patients with brain tumors varied among the selected studies: UFH +
VKA, tinzaparin alone and vena cava filter insertion. Depending on the therapeutic options, the
rate of recurrence and bleeding varied from 0 to 12% and from 0% to 17%, respectively
(intracerebral bleeding 0-7%). These figures appear to be quite similar to those noted in
retrospective studies performed with the same drugs in patients with cancer other than brain
tumors. In a small prospective non-randomized study assessing tinzaparin, no VTE recurrence
and no bleeding were detected [SCHMIDT2002]. So the presence of a brain tumor is not a

118 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
contraindication to a full anticoagulation provided that there is no other associated bleeding
risk. In this setting, the experts prefer to prescribe LMWH that has been shown to be superior
to VKA in patients with cancer other than brain tumors.
The studies available concerning the prophylaxis of VTE included in the majority of cases
cancer patients undergoing elective intracranial neurosurgery, but also patients undergoing
spinal surgery for tumors. In contrast to studies performed in surgical patients with no brain or
spinal tumor, timing of prophylaxis varied but it seems reasonable to start anticoagulation
after surgery. The duration of VTE prevention was limited to the hospitalization period and no
study has been conducted with extended prophylaxis. LMWH and UFH have similar efficacy
and safety (in terms of major bleeding and intracranial bleeding) and are superior to no
treatment. LMWH are more efficacious than external compression devices and are associated
with an increase in minor bleeding but not in major and intracranial bleeding; external
compression devices can be prescribed alone in patients with a contraindication to
pharmacological prophylaxis.
Severe renal failure has been defined as a creatinine clearance below 30 mL/min. In this case
LMWH and fondaparinux are contraindicated. No data have been published on the
management of anticoagulation in cancer patients with renal insufficiency. For the treatment
of VTE, the working group suggests using UFH followed by early VKA (possible from Day 1) or
LMWH adjusted on the basis of anti-Xa level according to each LMWH for the treatment of
established VTE. Such monitoring of anticoagulation could be helpful, since non-therapeutic
anti-Xa levels are common among medical patients treated with LMWH, especially cancer
patients [SALIBA2011]. The pharmacological prophylaxis of VTE in such patients may be
considered on a case-by-case basis, knowing that UFH is not contraindicated.
The bleeding risk is correlated with platelet count and is significantly higher when below
50 G/L. In most studies, anticoagulation was withheld from patients with a platelet count of
less than 50 G/L and resumed at the scheduled dose when the count was 100 G/L or higher.
For the treatment of VTE, the risk of recurrence is higher than the bleeding risk and the
working group chose the cut-off point of 50 G/L for treatment with a full-dose anticoagulant.
Between 30 and 50 G/L, the decision must be based on a case-by-case analysis with a careful
evaluation of the benefit-risk ratio. For prophylaxis, the risk of VTE is lower than the bleeding
risk and the experts decided to select the cut-off point of 80 G/L.
During pregnancy VKA are contraindicated. So standard treatment of established VTE with
long-term LMWH and standard prophylaxis with LMWH or UFH should be implemented (best
practice because the judgment is based on experts’ opinion in view of the lack of data).

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 119 Copyright © 1093790 (OPIC 28/02/2012)
8.5. Recommendations: special cases R1. A brain tumor per se is not a contraindication to anticoagulation for established VTE
Quality of evidence Low
Balance between desirable and undesirable effects High bleeding risk to be assessed individually
Values and preferences Based on individual clinical assessment
Costs (resource allocation) Not considered
Level of recommendation Weak
R2. For the treatment of established VTE in cancer patients with brain tumors we prefer LMWH
Quality of evidence Very low
Balance between desirable and undesirable effects High bleeding risk to be assessed individually
Values and preferences This opinion reflects the views of the panel group
Costs (resource allocation) Not considered
Level of recommendation Best practice
R3. We recommend the use of LMWH or UFH commenced postoperatively for the prevention VTE in cancer patients undergoing
neurosurgery
Quality of evidence High
Balance between desirable and undesirable effects Favorable
Values and preferences Subcutaneous injection
Costs (resource allocation) In some countries price difference between LMWH and UFH may influence the choice
Level of recommendation Strong
R4. In the presence of severe renal failure (creatinine clearance <30 mL/min) we suggest using UFH followed by early VKA
(possible from Day 1) or LMWH adjusted to anti-Xa level for the treatment of established VTE
Quality of evidence Not applicable (no data)
Balance between desirable and undesirable effects Unknown
Values and preferences Not considered
Costs (resource allocation) Not considered
Level of recommendation Best practice
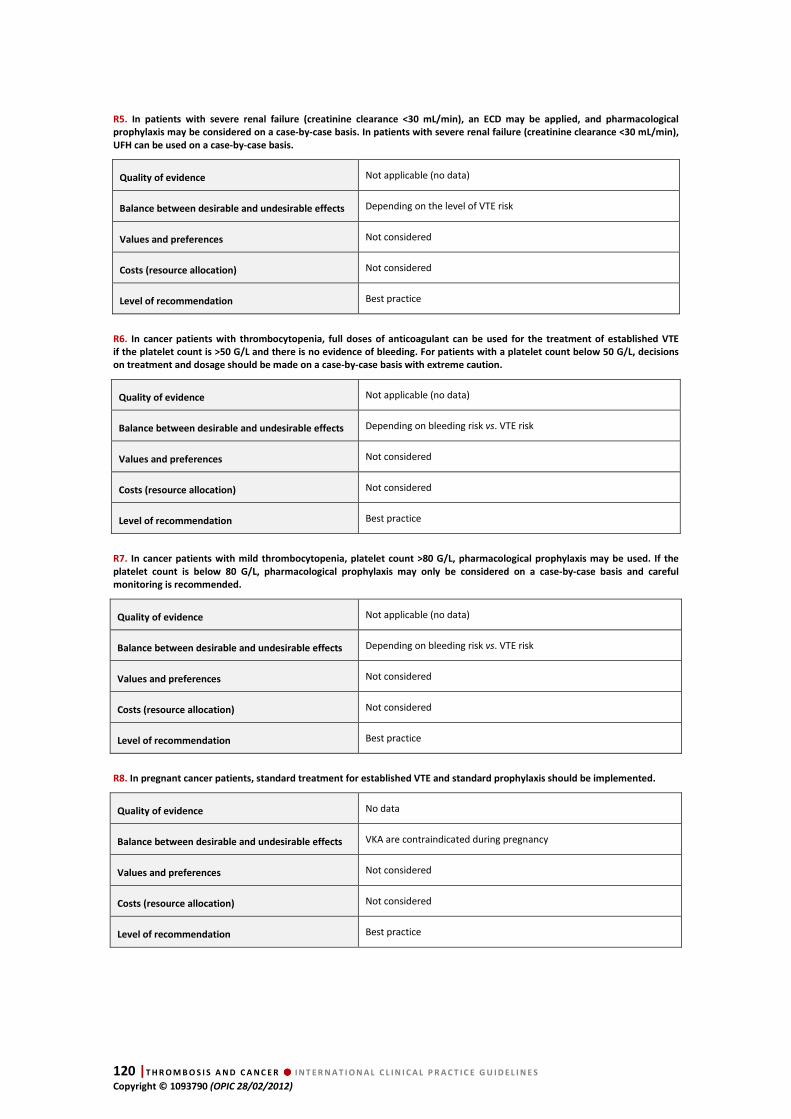
120 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
R5. In patients with severe renal failure (creatinine clearance <30 mL/min), an ECD may be applied, and pharmacological
prophylaxis may be considered on a case-by-case basis. In patients with severe renal failure (creatinine clearance <30 mL/min),
UFH can be used on a case-by-case basis.
Quality of evidence Not applicable (no data)
Balance between desirable and undesirable effects Depending on the level of VTE risk
Values and preferences Not considered
Costs (resource allocation) Not considered
Level of recommendation Best practice
R6. In cancer patients with thrombocytopenia, full doses of anticoagulant can be used for the treatment of established VTE
if the platelet count is >50 G/L and there is no evidence of bleeding. For patients with a platelet count below 50 G/L, decisions
on treatment and dosage should be made on a case-by-case basis with extreme caution.
Quality of evidence Not applicable (no data)
Balance between desirable and undesirable effects Depending on bleeding risk vs. VTE risk
Values and preferences Not considered
Costs (resource allocation) Not considered
Level of recommendation Best practice
R7. In cancer patients with mild thrombocytopenia, platelet count >80 G/L, pharmacological prophylaxis may be used. If the
platelet count is below 80 G/L, pharmacological prophylaxis may only be considered on a case-by-case basis and careful
monitoring is recommended.
Quality of evidence Not applicable (no data)
Balance between desirable and undesirable effects Depending on bleeding risk vs. VTE risk
Values and preferences Not considered
Costs (resource allocation) Not considered
Level of recommendation Best practice
R8. In pregnant cancer patients, standard treatment for established VTE and standard prophylaxis should be implemented.
Quality of evidence No data
Balance between desirable and undesirable effects VKA are contraindicated during pregnancy
Values and preferences Not considered
Costs (resource allocation) Not considered
Level of recommendation Best practice

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 121 Copyright © 1093790 (OPIC 28/02/2012)
9. Appendix 1. Working group and coordination Working group
Coordinators
FARGE Dominique, BÜLLER Harry
Methodologists
DEBOURDEAU Philippe, BECKERS Marielle
Experts
Oncology Hematology: BECKERS Marielle, BRILHANTE, Dialina, DEBOURDEAU Philippe, HAIM Nissim, KHORANA Alok, LECUMBERRI
Ramon, MANDALA Mario, MARTY Michel, QARI Mohamed, STREIFF Mickael, SYRIGOS Konstantinos.
Vascular disease Internal medicine: BAUERSACHS Ruppert, BOUNAMEAUX Henri, BRENNER Benjamin, BÜLLER Harry, FARGE
Dominique, KAKKAR Ajay, MONRÉAL Manuel, NOBLE Simon, PRANDONI Paolo.
Biology, Epidemiology, Others: GEROTZAFIAS Grigoris, Mousa Shaker, PABINGER Ingrid, PRINS Martin
Nurses
BALIN Caroline
Patients’ representatives
None
REVIEWERS
ALHEJJI Ibrahim, ALIKHAN Raza, ANDRE Thierry, ANDRES Emmanuel, BARRELIER Marie Thérèse, BLAIS Normand,
BRAGUER Diane, CARTER Kim, CROFT Andrea, DIMAKAKOS Evangelos, DUCHOSAI Michel, ELIAS Antoine, ELLIS Martin,
ESPIE Marc, GEORGOULIAS Vassili, GIRARD Philippe, GONZALEZ-BILLALABEITIA Enrique, HAMULYAK Karly, HOFFMAN
Ron, HULL Russel, JOHNSON Miriam, KAMPHUISEN Pieter Willem, KLEIJMAN Ankie, KRUIP Marieke, LAROCHE Jean
Pierre, LE HELLO Claire, LEE Agnes, LONG Anne, MAZZOLAI DUCHOSAL Lucia, OTTEN Hans-Martin, PARASKEVI Kotsis,
PEREZ-SEGURA Pedro, PERNOD Gilles, RHODES Sue, RIGHINI Marc, SEVESTRE Marie Antoinette, STRICKER Hans, TAZI
Zoubida, TEIXEIRA Luis Manuel, TRUJILLO SANTOS Antonio Javier, VILLIERS Stéphane.
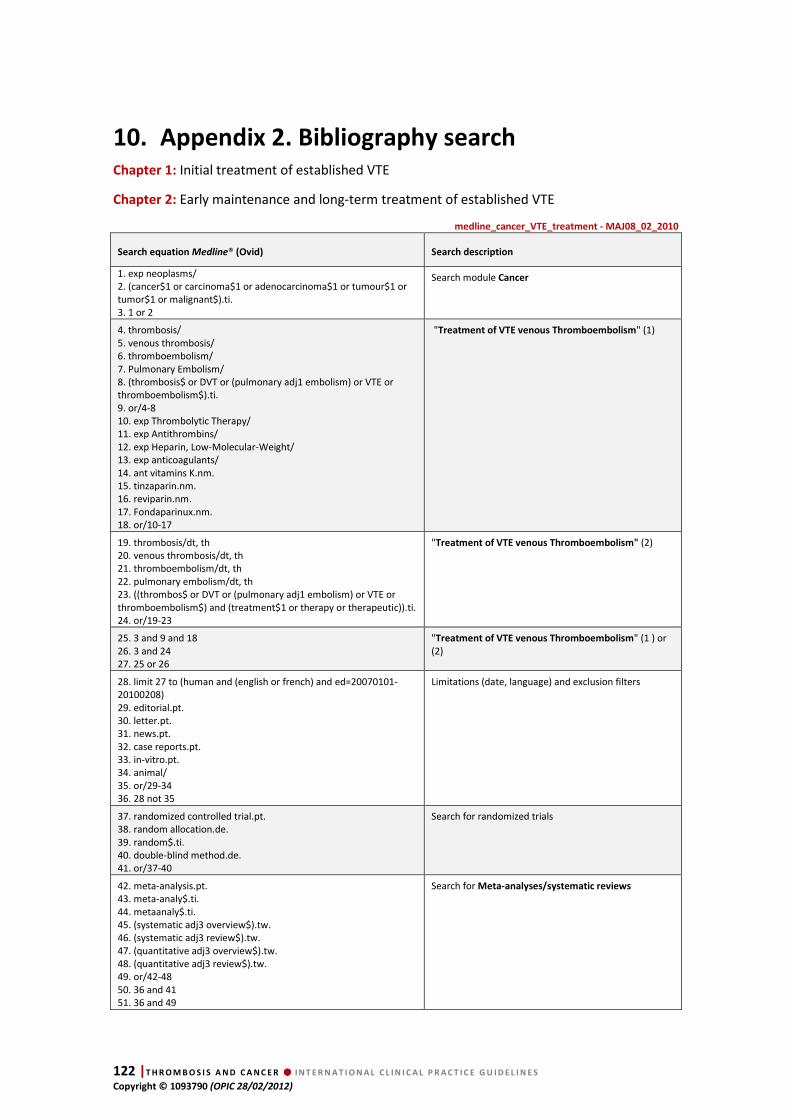
122 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
10. Appendix 2. Bibliography search Chapter 1: Initial treatment of established VTE
Chapter 2: Early maintenance and long-term treatment of established VTE
medline_cancer_VTE_treatment - MAJ08_02_2010
Search equation Medline® (Ovid) Search description
1. exp neoplasms/ 2. (cancer$1 or carcinoma$1 or adenocarcinoma$1 or tumour$1 or tumor$1 or malignant$).ti. 3. 1 or 2
Search module Cancer
4. thrombosis/ 5. venous thrombosis/ 6. thromboembolism/ 7. Pulmonary Embolism/ 8. (thrombosis$ or DVT or (pulmonary adj1 embolism) or VTE or thromboembolism$).ti. 9. or/4-8 10. exp Thrombolytic Therapy/ 11. exp Antithrombins/ 12. exp Heparin, Low-Molecular-Weight/ 13. exp anticoagulants/ 14. ant vitamins K.nm. 15. tinzaparin.nm. 16. reviparin.nm. 17. Fondaparinux.nm. 18. or/10-17
"Treatment of VTE venous Thromboembolism" (1)
19. thrombosis/dt, th 20. venous thrombosis/dt, th 21. thromboembolism/dt, th 22. pulmonary embolism/dt, th 23. ((thrombos$ or DVT or (pulmonary adj1 embolism) or VTE or thromboembolism$) and (treatment$1 or therapy or therapeutic)).ti. 24. or/19-23
"Treatment of VTE venous Thromboembolism" (2)
25. 3 and 9 and 18 26. 3 and 24 27. 25 or 26
"Treatment of VTE venous Thromboembolism" (1 ) or (2)
28. limit 27 to (human and (english or french) and ed=20070101-20100208) 29. editorial.pt. 30. letter.pt. 31. news.pt. 32. case reports.pt. 33. in-vitro.pt. 34. animal/ 35. or/29-34 36. 28 not 35
Limitations (date, language) and exclusion filters
37. randomized controlled trial.pt. 38. random allocation.de. 39. random$.ti. 40. double-blind method.de. 41. or/37-40
Search for randomized trials
42. meta-analysis.pt. 43. meta-analy$.ti. 44. metaanaly$.ti. 45. (systematic adj3 overview$).tw. 46. (systematic adj3 review$).tw. 47. (quantitative adj3 overview$).tw. 48. (quantitative adj3 review$).tw. 49. or/42-48 50. 36 and 41 51. 36 and 49
Search for Meta-analyses/systematic reviews
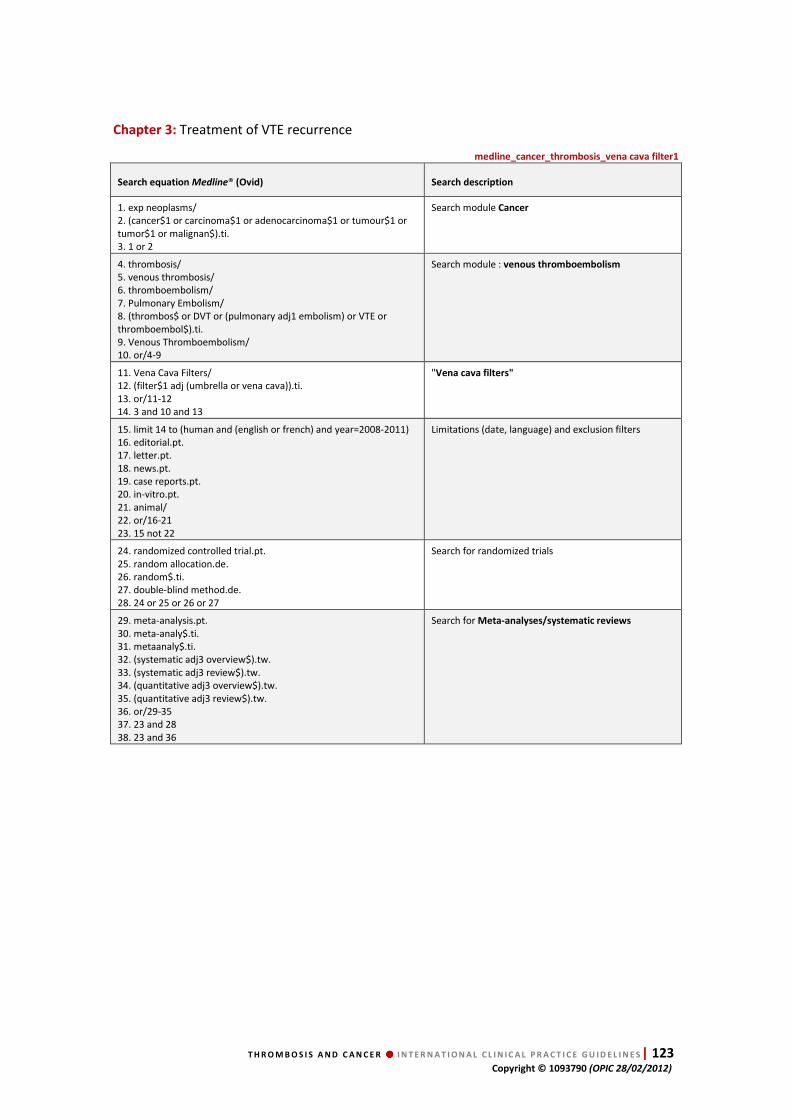
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 123 Copyright © 1093790 (OPIC 28/02/2012)
Chapter 3: Treatment of VTE recurrence
medline_cancer_thrombosis_vena cava filter1
Search equation Medline® (Ovid) Search description
1. exp neoplasms/ 2. (cancer$1 or carcinoma$1 or adenocarcinoma$1 or tumour$1 or tumor$1 or malignan$).ti. 3. 1 or 2
Search module Cancer
4. thrombosis/ 5. venous thrombosis/ 6. thromboembolism/ 7. Pulmonary Embolism/ 8. (thrombos$ or DVT or (pulmonary adj1 embolism) or VTE or thromboembol$).ti. 9. Venous Thromboembolism/ 10. or/4-9
Search module : venous thromboembolism
11. Vena Cava Filters/ 12. (filter$1 adj (umbrella or vena cava)).ti. 13. or/11-12 14. 3 and 10 and 13
"Vena cava filters"
15. limit 14 to (human and (english or french) and year=2008-2011) 16. editorial.pt. 17. letter.pt. 18. news.pt. 19. case reports.pt. 20. in-vitro.pt. 21. animal/ 22. or/16-21 23. 15 not 22
Limitations (date, language) and exclusion filters
24. randomized controlled trial.pt. 25. random allocation.de. 26. random$.ti. 27. double-blind method.de. 28. 24 or 25 or 26 or 27
Search for randomized trials
29. meta-analysis.pt. 30. meta-analy$.ti. 31. metaanaly$.ti. 32. (systematic adj3 overview$).tw. 33. (systematic adj3 review$).tw. 34. (quantitative adj3 overview$).tw. 35. (quantitative adj3 review$).tw. 36. or/29-35 37. 23 and 28 38. 23 and 36
Search for Meta-analyses/systematic reviews

124 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
medline_cancer_thrombosis_vena cava filter2
Search equation Medline® (Ovid) Search description
1. thrombosis/ 2. venous thrombosis/ 3. thromboembolism/ 4. Pulmonary Embolism/ 5. (thrombos$ or DVT or (pulmonary adj1 embolism) or VTE or thromboembol$).ti. 6. Venous Thromboembolism/ 7. or/1-6
Search module: venous thromboembolism
8. Vena Cava Filters/ 9. (filter$1 adj (umbrella or vena cava)).ti. 10. or/8-9 11. 7 and 10
"Vena cava filters"
12. limit 11 to (human and (english or french) and year=1995-2011) 13. editorial.pt. 14. letter.pt. 15. news.pt. 16. case reports.pt. 17. in-vitro.pt. 18. animal/ 19. or/13-18 20. 12 not 19
Limitations (date, language) and exclusion filters
21. meta-analysis.pt. 22. meta-analy$.ti. 23. metaanaly$.ti. 24. (systematic adj3 overview$).tw. 25. (systematic adj3 review$).tw. 26. (quantitative adj3 overview$).tw. 27. (quantitative adj3 review$).tw. 28. or/21-27 29. 20 and 28
Search for Meta-analyses/systematic reviews

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 125 Copyright © 1093790 (OPIC 28/02/2012)
Chapter 4 : Prophylaxis of VTE in surgical cancer patients
Chapter 5 : Prophylaxis of VTE in medical cancer patients
medline_cancer_VTE_prophylaxis
Search equation Medline® (Ovid) Search description
1. exp neoplasms/ 2. (cancer$1 or carcinoma$1 or adenocarcinoma$1 or tumour$1 or tumor$1 or malignan$).ti. 3. 1 or 2
Search module Cancer
4. thrombosis/ 5. venous thrombosis/ 6. thromboembolism/ 7. Pulmonary Embolism/ 8. (thrombos$ or DVT or (pulmonary adj1 embolism) or VTE or thromboembol$).ti. 9. or/4-8
Search module Venous Thromboembolism
10. thrombosis/pc 11. venous thrombosis/pc [Prevention & Control] 12. thromboembolism/pc [Prevention & Control] 13. Pulmonary Embolism/pc [Prevention & Control] 14. 10 or 11 or 12 or 13 15. ((thrombos$ or DVT or VTE or thromboembol$ or (pulmonary adj1 embolism)) adj4 (recurrence or recurrent or second$) adj2 (risk$ or prevent$ or prophylaxy or prophylaxi$)).ti,ab. 16. (risk$ or prevent$ or prophylaxy or prophylaxi$).ti,ab. 17. ((thrombos$ or DVT or VTE or thromboembol$ or (pulmonary adj1 embolism)) adj4 (recurrence or recurrent or second$)).ti,ab. 18. 3 and 9 and 16 19. 3 and 15 20. 3 and 14 and 17 21. 18 or 19 or 20
"Venous thromboembolism prophylaxis"
22. editorial.pt. 23. letter.pt. 24. news.pt. 25. case reports.pt. 26. in vitro.pt. 27. animal/ 28. or/22-27 29. 21 not 28 30. limit 29 to (human and (english or french) and year=2000-2010)
Limitations (date, language) and exclusion filters
31. randomized controlled trial.pt. 32. random allocation.de. 33. random$.ti. 34. double-blind method.de. 35. 31 or 32 or 33 or 34
Search for Randomized trials
36. meta-analysis.pt. 37. meta-analy$.ti. 38. metaanaly$.ti. 39. (systematic adj3 overview$).tw. 40. (systematic adj3 review$).tw. 41. (quantitative adj3 overview$).tw. 42. (quantitative adj3 review$).tw. 43. or/36-42
Search for Meta-analyses/systematic reviews
44. clinical trials, phase iii/ 45. clinical trial, phase iii.pt. 46. (phase III or phase 3).ti. 47. 44 or 45 or 46
Search for Phase III Randomized trials
48. exp "cohort studies"/ 49. prospective stud$.ti. 50. prospective studies/ 51. 48 or 49 or 50 52. 30 and 35 53. 30 and 43 54. 30 and 47 55. 30 and 51
Search for Prospective studies

126 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Chapter 6 : Treatment of established catheter-related thrombosis (CRT)
Chapter 7 : Prophylaxis of CRT
medline_cancer_thrombosis and catheter - MAJ 2010
Search equation Medline® (Ovid) Search description
1. exp neoplasms/ 2. (cancer$1 or carcinoma$1 or adenocarcinoma$1 or tumour$1 or tumor$1 or malignan$).ti. 3. 1 or 2
Search module Cancer
4. thrombosis/ 5. venous thrombosis/ 6. thromboembolism/ 7. Pulmonary Embolism/ 8. (thrombos$ or DVT or (pulmonary adj1 embolism) or VTE or thromboembol$).ti. 9. or/4-8
Search module Venous Thromboembolism
10. Catheterization/ 11. Catheterization, Central Venous/ 12. (Catheterization$ or CCV or (central adj1 venous) or catheter$).ti. 13. or/10-12 14. 3 and 9 and 13
Search module Catheter
15. limit 14 to (human and (english or french) and ed=20070101-20100128) 16. editorial.pt. 17. letter.pt. 18. news.pt. 19. case reports.pt. 20. in-vitro.pt. 21. animal/ 22. or/16-21 23. 15 not 22
Limitations (date, language) and exclusion filters
24. randomized controlled trial.pt. 25. random allocation.de. 26. random$.ti. 27. double-blind method.de. 28. 24 or 25 or 26 or 27
Search for Randomized trials
29. meta-analysis.pt. 30. meta-analy$.ti. 31. metaanaly$.ti. 32. (systematic adj3 overview$).tw. 33. (systematic adj3 review$).tw. 34. (quantitative adj3 overview$).tw. 35. (quantitative adj3 review$).tw. 36. or/29-35 37. 23 and 28 38. 23 and 36
Search for Meta-analyses/systematic reviews
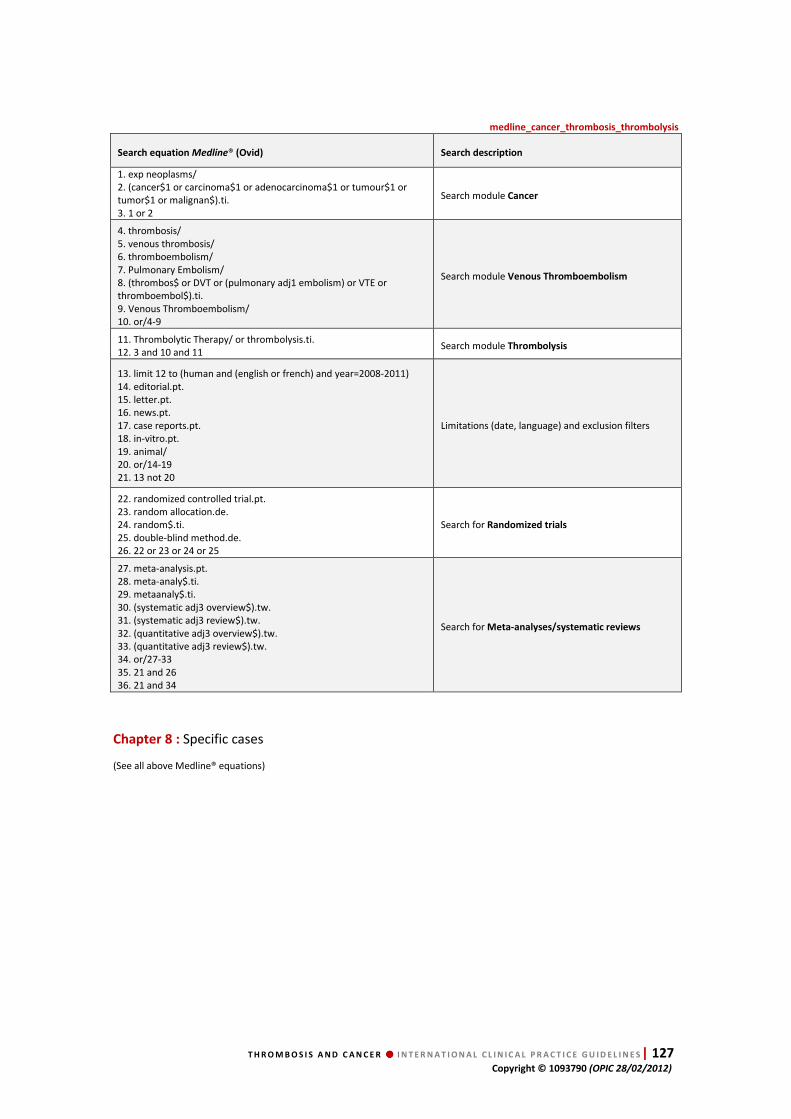
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 127 Copyright © 1093790 (OPIC 28/02/2012)
medline_cancer_thrombosis_thrombolysis
Search equation Medline® (Ovid) Search description
1. exp neoplasms/ 2. (cancer$1 or carcinoma$1 or adenocarcinoma$1 or tumour$1 or tumor$1 or malignan$).ti. 3. 1 or 2
Search module Cancer
4. thrombosis/ 5. venous thrombosis/ 6. thromboembolism/ 7. Pulmonary Embolism/ 8. (thrombos$ or DVT or (pulmonary adj1 embolism) or VTE or thromboembol$).ti. 9. Venous Thromboembolism/ 10. or/4-9
Search module Venous Thromboembolism
11. Thrombolytic Therapy/ or thrombolysis.ti. 12. 3 and 10 and 11
Search module Thrombolysis
13. limit 12 to (human and (english or french) and year=2008-2011) 14. editorial.pt. 15. letter.pt. 16. news.pt. 17. case reports.pt. 18. in-vitro.pt. 19. animal/ 20. or/14-19 21. 13 not 20
Limitations (date, language) and exclusion filters
22. randomized controlled trial.pt. 23. random allocation.de. 24. random$.ti. 25. double-blind method.de. 26. 22 or 23 or 24 or 25
Search for Randomized trials
27. meta-analysis.pt. 28. meta-analy$.ti. 29. metaanaly$.ti. 30. (systematic adj3 overview$).tw. 31. (systematic adj3 review$).tw. 32. (quantitative adj3 overview$).tw. 33. (quantitative adj3 review$).tw. 34. or/27-33 35. 21 and 26 36. 21 and 34
Search for Meta-analyses/systematic reviews
Chapter 8 : Specific cases
(See all above Medline® equations)
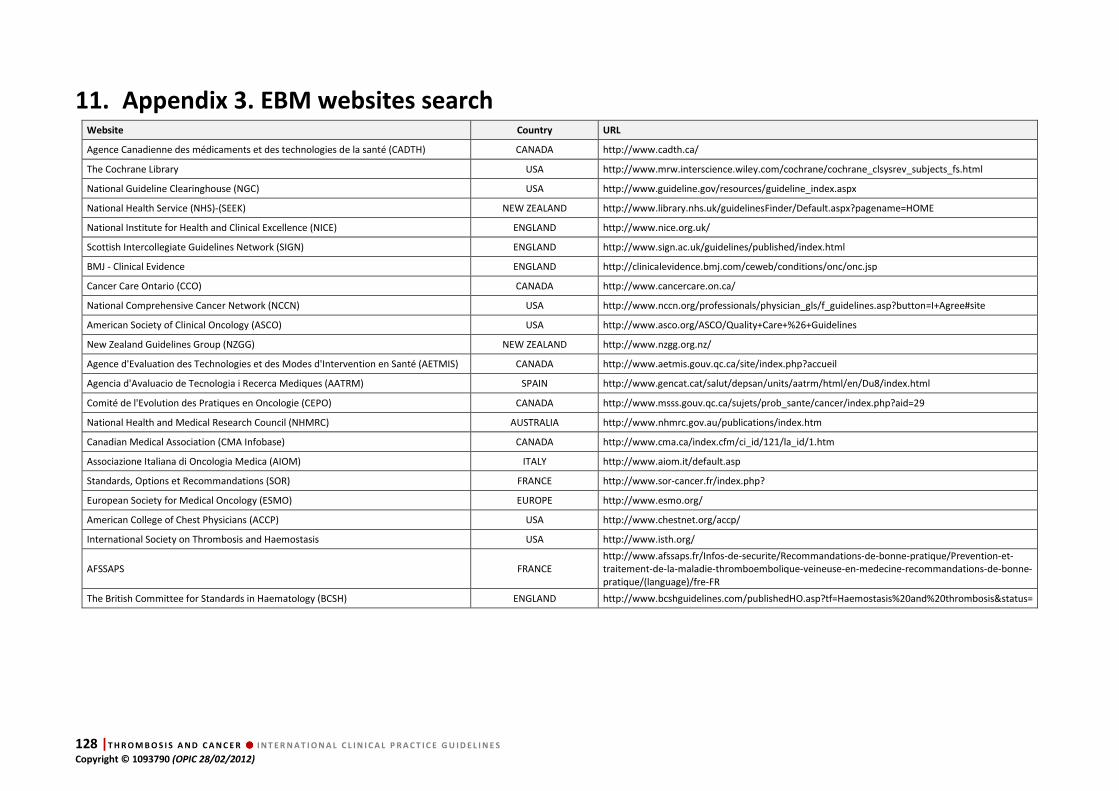
128 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
11. Appendix 3. EBM websites search Website Country URL
Agence Canadienne des médicaments et des technologies de la santé (CADTH) CANADA http://www.cadth.ca/
The Cochrane Library USA http://www.mrw.interscience.wiley.com/cochrane/cochrane_clsysrev_subjects_fs.html
National Guideline Clearinghouse (NGC) USA http://www.guideline.gov/resources/guideline_index.aspx
National Health Service (NHS)-(SEEK) NEW ZEALAND http://www.library.nhs.uk/guidelinesFinder/Default.aspx?pagename=HOME
National Institute for Health and Clinical Excellence (NICE) ENGLAND http://www.nice.org.uk/
Scottish Intercollegiate Guidelines Network (SIGN) ENGLAND http://www.sign.ac.uk/guidelines/published/index.html
BMJ - Clinical Evidence ENGLAND http://clinicalevidence.bmj.com/ceweb/conditions/onc/onc.jsp
Cancer Care Ontario (CCO) CANADA http://www.cancercare.on.ca/
National Comprehensive Cancer Network (NCCN) USA http://www.nccn.org/professionals/physician_gls/f_guidelines.asp?button=I+Agree#site
American Society of Clinical Oncology (ASCO) USA http://www.asco.org/ASCO/Quality+Care+%26+Guidelines
New Zealand Guidelines Group (NZGG) NEW ZEALAND http://www.nzgg.org.nz/
Agence d'Evaluation des Technologies et des Modes d'Intervention en Santé (AETMIS) CANADA http://www.aetmis.gouv.qc.ca/site/index.php?accueil
Agencia d'Avaluacio de Tecnologia i Recerca Mediques (AATRM) SPAIN http://www.gencat.cat/salut/depsan/units/aatrm/html/en/Du8/index.html
Comité de l'Evolution des Pratiques en Oncologie (CEPO) CANADA http://www.msss.gouv.qc.ca/sujets/prob_sante/cancer/index.php?aid=29
National Health and Medical Research Council (NHMRC) AUSTRALIA http://www.nhmrc.gov.au/publications/index.htm
Canadian Medical Association (CMA Infobase) CANADA http://www.cma.ca/index.cfm/ci_id/121/la_id/1.htm
Associazione Italiana di Oncologia Medica (AIOM) ITALY http://www.aiom.it/default.asp
Standards, Options et Recommandations (SOR) FRANCE http://www.sor-cancer.fr/index.php?
European Society for Medical Oncology (ESMO) EUROPE http://www.esmo.org/
American College of Chest Physicians (ACCP) USA http://www.chestnet.org/accp/
International Society on Thrombosis and Haemostasis USA http://www.isth.org/
AFSSAPS FRANCE http://www.afssaps.fr/Infos-de-securite/Recommandations-de-bonne-pratique/Prevention-et-traitement-de-la-maladie-thromboembolique-veineuse-en-medecine-recommandations-de-bonne-pratique/(language)/fre-FR
The British Committee for Standards in Haematology (BCSH) ENGLAND http://www.bcshguidelines.com/publishedHO.asp?tf=Haemostasis%20and%20thrombosis&status=

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 129 Copyright © 1093790 (OPIC 28/02/2012)
12. Appendix 4. Critical appraisal grids
References
De
sig
n
En
dp
oin
t d
efi
nit
ion
De
scri
pti
on
of
ran
do
miz
ati
on
Sa
mp
le s
ize
calc
ula
tio
n
De
scri
pti
on
of
sta
tist
ica
l p
lan
De
scri
pti
on
of
en
dp
oin
t m
eth
od
of
me
asu
rem
en
t
Do
cum
en
tati
on
of
lost
to
foll
ow
-up
Inte
nt-
to-t
rea
t
an
aly
sis
To
xic
ity
: d
ata
an
d g
rad
ing
Co
nfl
ict
of
in
tere
st
Comments
MOORE1981 RS Yes No No No Yes No No Yes – Yes No
CLARKE-PEARSON 1983 RS Yes No No Yes No Yes No Yes – No No
KRAUTHE1987 RS Yes No No No Yes No No Yes -Yes No
ALTSCHULER1990 RS Yes No No No No No No Yes No
CALLIGARO1991 RS Yes No No No No No No Yes - No No
CHAN1992 RS Yes No No No Yes No No Yes –Yes No
LEVIN1993 RS Yes No No No No No No No No
SCHIFF1994 RS Yes No No No No No No Yes No
DEBOURDEAU1996 RS Yes No No No Yes No No Yes - No No
HARRINGTON1997 RS Yes No No No No No No Yes – No No
BONA2000 PNRS No No No No Yes No No Yes - Yes Yes Study focusing on bleeding risk with VKA in cancer patients
ELTING2004 RS Yes No No Yes Yes Yes No Yes - Yes Yes
HUTTEN2000 PNRS Yes Yes No Yes No Yes No Yes - Yes No Cancer patients included in 2 RCT (Tasman, Colombus)
PALARETTI2000 PNRS Yes No No Yes Yes No No Yes - Yes No Comparison of VKA in cancer and non-cancer patients
PRANDONI2002 PNRS Yes No No Yes Yes Yes No Yes - Yes No
VUCIC2002 PNRS Yes No No Yes Yes Yes No Yes - Yes No
MONREAL2004 PNRS Yes No No Yes Yes Yes No Yes - Yes No
SCHMIDT2002 PNRS Yes No No No No No No No No
MEYER2002 RCT Yes Yes Yes Yes Yes Yes Yes Yes - Yes No Fewer patients included than calculated
LEE2003 RCT Yes Yes Yes Yes Yes Yes Yes Yes - Yes No
DEITCHER2006 RCT Yes No No Yes Yes Yes Yes Yes - Yes No Pilot feasibility study testing different doses of enoxaparin
HULL2006 RCT Yes Yes No Yes Yes Yes No Yes - Yes No
VANDOORMAL2009 RCT Yes Yes Yes Yes Yes No Yes Yes - Yes No
ROMERA2009 RCT Yes No Yes Yes Yes Yes No Yes - Yes No
CARRIER2009 RS Yes No No Yes Yes No No No - No Yes
SIRAGUSA2010 RCT Yes No No No No Yes No Yes - Yes No Only as an abstract
VANDOORMAL2010 RCT Yes Yes Yes Yes Yes Yes Yes Yes - Yes No
Treatment of VTE and PE (with brain tumors)
RS = Randomized Study, PNRS = Prospective Non-Randomized Study, RCT = Randomized Controlled Trial, RDBT = Randomized Double-Blind Trial

130 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
References
De
sig
n
En
dp
oin
t d
efi
nit
ion
De
scri
pti
on
of
ran
do
miz
ati
on
Sa
mp
le s
ize
calc
ula
tio
n
De
scri
pti
on
of
sta
tist
ica
l p
lan
De
scri
pti
on
of
en
dp
oin
t m
eth
od
of
me
asu
rem
en
t
Do
cum
en
tati
on
of
lost
to
fo
llo
w-u
p
Inte
nt-
to-t
rea
t
an
aly
sis
To
xic
ity
:
da
ta -
gra
din
g
Co
nfl
ict
of
inte
rest
Comments
CERRATO1978 RCT Yes No No No No Yes No Yes – Yes No
TURPIE1989 RCT Yes No Yes Yes Yes No Yes Yes – Yes No
MELON1991 RCT Yes No Yes No Yes Yes No Yes – Yes No Only an abstract, no full paper for this study
ENOXACAN1997 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes No
CONSTANTINI1994 RCT Yes Yes No Yes Yes Yes No Yes – Yes No Primary endpoint was safety no data about DVT diagnosis
NURMOHAMED1996 RCT Yes No No Yes Yes Yes No Yes – Yes No The study population consisted out of patients with both malign and benign conditions. No separate results are reported
DICKINSON1998 RCT Yes No No Yes Yes Yes Yes Yes – Yes No
LAUSEN1998 RCT Yes Yes Yes Yes Yes Yes No Yes – Yes Yes The number of included patients was lower than expected and calculated at the beginning of the study
AGNELLI1998 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes No
BAYKAL2001 RDBT Yes No No Yes Yes No No Yes – Yes No
MCLEOD2001 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes No The data for cancer patients are extracted from a subgroup for efficacy; the data are provided for the whole group for safety
MAXWELL2001 RCT Yes Yes Yes Yes Yes Yes Yes Yes – Yes No
BERGQVIST2002 RDBT Yes No Yes Yes Yes Yes No Yes – Yes No
GOLDHABER2002 RDBT Yes No Yes Yes Yes Yes Yes Yes – Yes No
MACDONALD2003 RCT Yes No Yes Yes Yes No No Yes – Yes No
AGNELLI2005 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes No
SIMONNEAU2006 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes Yes Patients treated with dalteparin experienced fewer symptomatic VTE and fewer epsiode of major bleeding, but it was not the primary endpoint
RASMUSSEN2006 RCT Yes Yes Yes Yes Yes Yes Yes Yes – Yes Yes
SHUKLA2008 RCT Yes Yes Yes Yes Yes No No Yes – Yes No The planned number of patients to be included was 189, but only 99 patients were included in this study
KAKKAR2010 RDBT Yes Yes Yes Yes Yes Yes Yes Yes – Yes Yes
Prophylaxis in surgical patients
RS = Randomized Study, PNRS = Prospective Non-Randomized Study, RCT = Randomized Controlled Trial, RDBT = Randomized Double-Blind Trial

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 131 Copyright © 1093790 (OPIC 28/02/2012)
References
De
sig
n
En
dp
oin
t d
efi
nit
ion
De
scri
pti
on
of
ran
do
miz
ati
on
Sa
mp
le s
ize
calc
ula
tio
n
De
scri
pti
on
of
sta
tist
ica
l p
lan
De
scri
pti
on
of
en
dp
oin
t m
eth
od
of
me
asu
rem
en
t
Do
cum
en
tati
on
of
lost
to
fo
llo
w-u
p
Inte
nt-
to-t
rea
t
an
aly
sis
To
xic
ity
:
da
ta -
gra
din
g
Co
nfl
ict
of
inte
rest
Comments
DAHAN1986 RDBT Yes Yes No Yes Yes Yes No Yes - Yes No
BERGMANN1996 RDBT Yes Yes Yes Yes Yes Yes Yes Yes – Yes No
HARENBERG1996 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes No
LECHLER1996 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes No
SAMAMA1999 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes No
MITCHELL2003 RCT Yes Yes Yes Yes Yes Yes No Yes – Yes Yes
KLEBER2003 RCT Yes Yes Yes Yes Yes Yes No Yes – Yes No
LEIZOROVICZ2004 RDBT Yes Yes Yes Yes Yes Yes Yes Yes – Yes Yes
ZANGARI2004 RS Yes No No Yes No Yes No Yes – Yes No
HASS2005 RDBT Yes Yes No No Yes No No Yes – Yes No Study interrupted prematurely, only available as an abstract
COHEN2006 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes Yes
IKHLAQUE2006 RS Yes No No No No No No No –No No
MEISTER2008 PNRS Yes No No No Yes No No Yes – Yes No
MARAVEYAS2009 RCT Yes Yes No No No No No No – No Yes Only an abstract is available
RIESS2009 RCT Yes No No No No No No Yes – Yes No Only an abstract is available
AGNELLI2009 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes Yes
PERRY2010 RDBT Yes Yes Yes Yes Yes Yes No Yes – Yes Yes
VERSO2010 RDBT Yes Yes No Yes Yes Yes No Yes – Yes Yes
PALUMBO2011 RCT Yes Yes Yes Yes Yes Yes No Yes – Yes Yes
Prophylaxis in medical patients
RS = Randomized Study, PNRS = Prospective Non-Randomized Study, RCT = Randomized Controlled Trial, RDBT = Randomized Double-Blind Trial
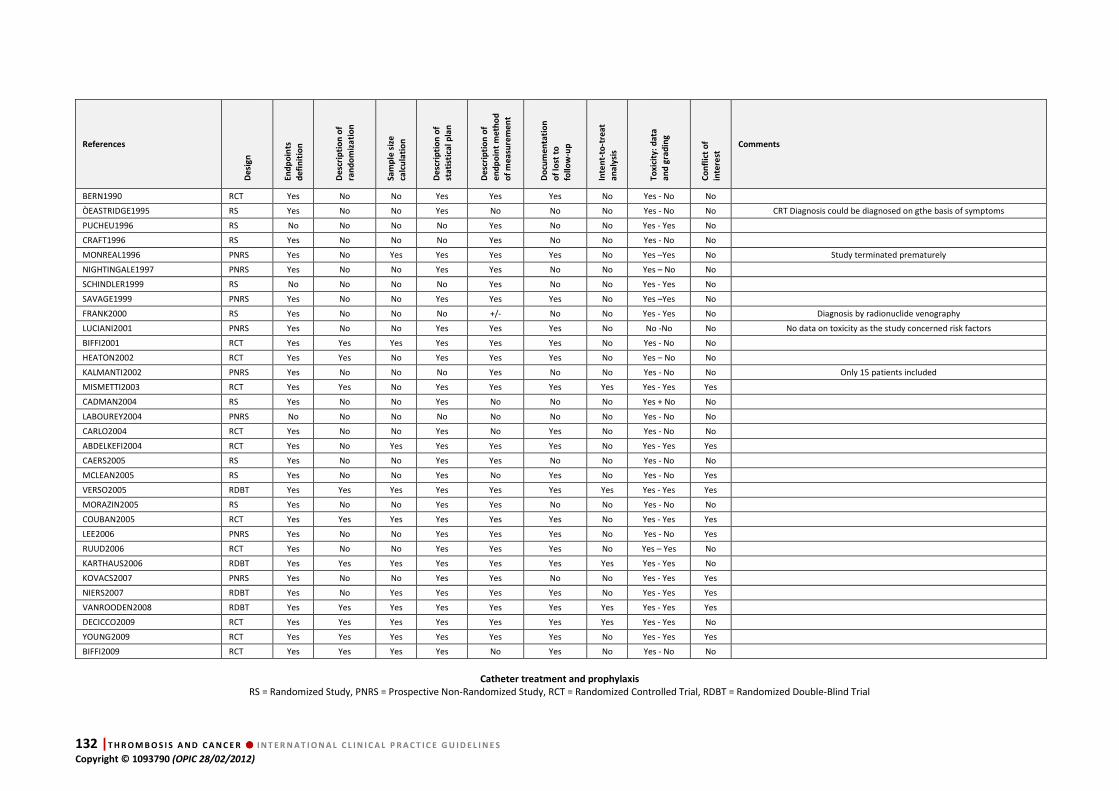
132 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
References
De
sig
n
En
dp
oin
ts
de
fin
itio
n
De
scri
pti
on
of
ran
do
miz
ati
on
Sa
mp
le s
ize
calc
ula
tio
n
De
scri
pti
on
of
sta
tist
ica
l p
lan
De
scri
pti
on
of
en
dp
oin
t m
eth
od
of
me
asu
rem
en
t
Do
cum
en
tati
on
of
lost
to
foll
ow
-up
Inte
nt-
to-t
rea
t
an
aly
sis
To
xic
ity
: d
ata
an
d g
rad
ing
Co
nfl
ict
of
inte
rest
Comments
BERN1990 RCT Yes No No Yes Yes Yes No Yes - No No
ÒEASTRIDGE1995 RS Yes No No Yes No No No Yes - No No CRT Diagnosis could be diagnosed on gthe basis of symptoms
PUCHEU1996 RS No No No No Yes No No Yes - Yes No
CRAFT1996 RS Yes No No No Yes No No Yes - No No
MONREAL1996 PNRS Yes No Yes Yes Yes Yes No Yes –Yes No Study terminated prematurely
NIGHTINGALE1997 PNRS Yes No No Yes Yes No No Yes – No No
SCHINDLER1999 RS No No No No Yes No No Yes - Yes No
SAVAGE1999 PNRS Yes No No Yes Yes Yes No Yes –Yes No
FRANK2000 RS Yes No No No +/- No No Yes - Yes No Diagnosis by radionuclide venography
LUCIANI2001 PNRS Yes No No Yes Yes Yes No No -No No No data on toxicity as the study concerned risk factors
BIFFI2001 RCT Yes Yes Yes Yes Yes Yes No Yes - No No
HEATON2002 RCT Yes Yes No Yes Yes Yes No Yes – No No
KALMANTI2002 PNRS Yes No No No Yes No No Yes - No No Only 15 patients included
MISMETTI2003 RCT Yes Yes No Yes Yes Yes Yes Yes - Yes Yes
CADMAN2004 RS Yes No No Yes No No No Yes + No No
LABOUREY2004 PNRS No No No No No No No Yes - No No
CARLO2004 RCT Yes No No Yes No Yes No Yes - No No
ABDELKEFI2004 RCT Yes No Yes Yes Yes Yes No Yes - Yes Yes
CAERS2005 RS Yes No No Yes Yes No No Yes - No No
MCLEAN2005 RS Yes No No Yes No Yes No Yes - No Yes
VERSO2005 RDBT Yes Yes Yes Yes Yes Yes Yes Yes - Yes Yes
MORAZIN2005 RS Yes No No Yes Yes No No Yes - No No
COUBAN2005 RCT Yes Yes Yes Yes Yes Yes No Yes - Yes Yes
LEE2006 PNRS Yes No No Yes Yes Yes No Yes - No Yes
RUUD2006 RCT Yes No No Yes Yes Yes No Yes – Yes No
KARTHAUS2006 RDBT Yes Yes Yes Yes Yes Yes Yes Yes - Yes No
KOVACS2007 PNRS Yes No No Yes Yes No No Yes - Yes Yes
NIERS2007 RDBT Yes No Yes Yes Yes Yes No Yes - Yes Yes
VANROODEN2008 RDBT Yes Yes Yes Yes Yes Yes Yes Yes - Yes Yes
DECICCO2009 RCT Yes Yes Yes Yes Yes Yes Yes Yes - Yes No
YOUNG2009 RCT Yes Yes Yes Yes Yes Yes No Yes - Yes Yes
BIFFI2009 RCT Yes Yes Yes Yes No Yes No Yes - No No
Catheter treatment and prophylaxis
RS = Randomized Study, PNRS = Prospective Non-Randomized Study, RCT = Randomized Controlled Trial, RDBT = Randomized Double-Blind Trial

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 133 Copyright © 1093790 (OPIC 28/02/2012)
13. Appendix 5. Methodology of guidelines
elaboration
DEFINED HEALTH QUESTIONS
SEARCH AND SCREEN GUIDELINES
ASSESS EXISTING GUIDELINES
1 EXTRACTION OF DATA FROM
EXISTING GUIDELINES
2 LITERATURE SEARCH
FOR MISSING POINTS +
QUESTIONS PREVIOUSLY STUDIED QUESTIONS NOT STUDIED
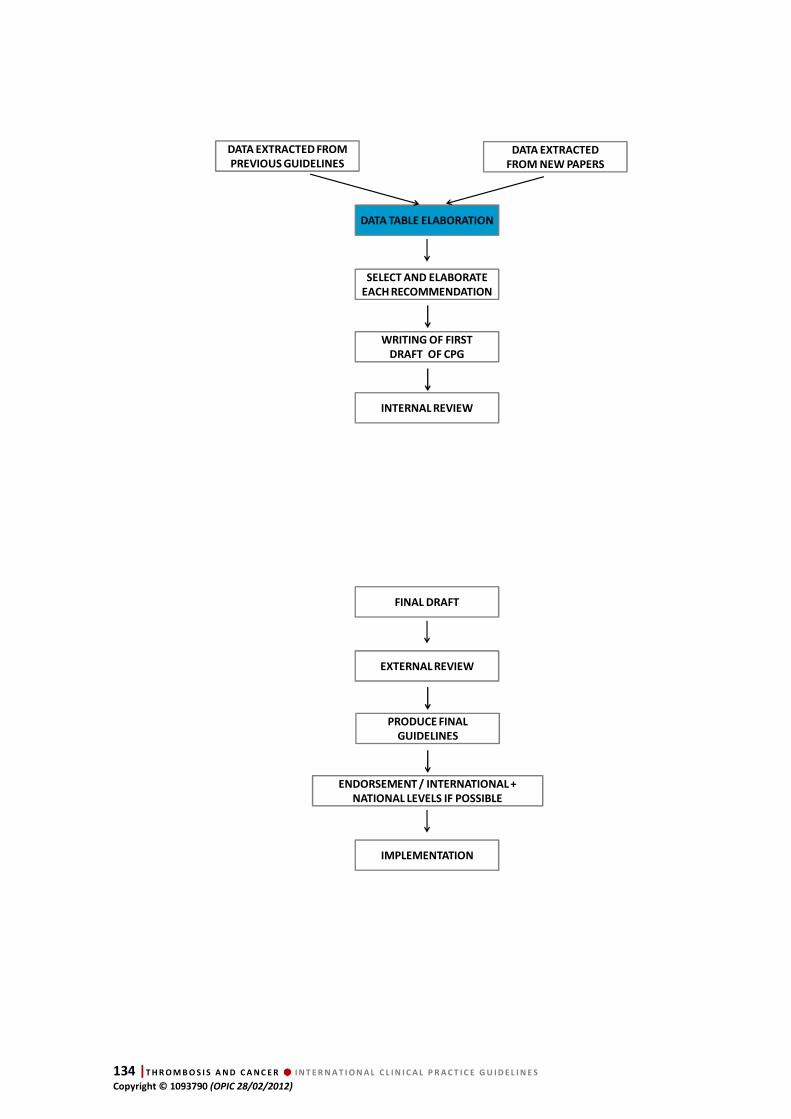
134 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
DATA TABLE ELABORATION
SELECT AND ELABORATE
EACH RECOMMENDATION
WRITING OF FIRST
DRAFT OF CPG
INTERNAL REVIEW
DATA EXTRACTED FROM
PREVIOUS GUIDELINES
DATA EXTRACTED
FROM NEW PAPERS
FINAL DRAFT
EXTERNAL REVIEW
PRODUCE FINAL
GUIDELINES
ENDORSEMENT / INTERNATIONAL +
NATIONAL LEVELS IF POSSIBLE
IMPLEMENTATION

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 135 Copyright © 1093790 (OPIC 28/02/2012)
14. Appendix 6. Methodological tools
Grids for methodological appraisal OF meta-analyses
EXPERT NAME
BIBLIOGAPHIC REFERENCE Author, year of publication
1. An a priori hypothesis was made before beginning the study Yes / No
Unspecified
2. Objectives (main and secondary) are well defined Yes / No
Unspecified
3. Primary and secondary endpoints are well defined
Yes / No
Unspecified
Irrelevant
4. Bibliographic search is clear and well done Yes / No
Unspecified
5. Inclusion and exclusion criteria are well defined Yes / No
Unspecified
6. The methods of selection and analysis of the quality of the studies are
described.
Yes / No
Unspecified
Irrelevant
7. The main criteria used to assess the comparability of groups are relevant. Yes / No
Unspecified
8. A meta–analysis is performed Yes / No
Unspecified
9. In the case of a meta-analysis, was this performed on individual data? Yes / No
Unspecified
10. In the case of a meta-analysis, was this an intent-to-treat analysis? Yes / No
Unspecified
11. Results of the bibliographic search are described Yes / No
Unspecified
12. The risk of publication bias was considered Yes / No
Unspecified
13. Included studies are described Yes / No
Unspecified
14. Quality of studies is described Yes / No
Unspecified
15. The result (s) is (are) not drawn from an analysis of subgroups. Yes / No
Unspecified
16. The homogeneity of the results was checked by a test of heterogeneity Yes / No
Unspecified
17. The biases and methodological limitations of the meta-analysis are discussed Yes / No
Unspecified
18. Conclusions are consistent with the results Yes / No
19. The authors discussed the results of other studies on the same issue Yes / No
20. Authors' conflicts of interest are documented Yes / No
Comments Free text
Clinical query
VTE treatment
VTE prophylaxis
CRT treatment
CRT prophylaxis
Final decision To be included
Not to be included
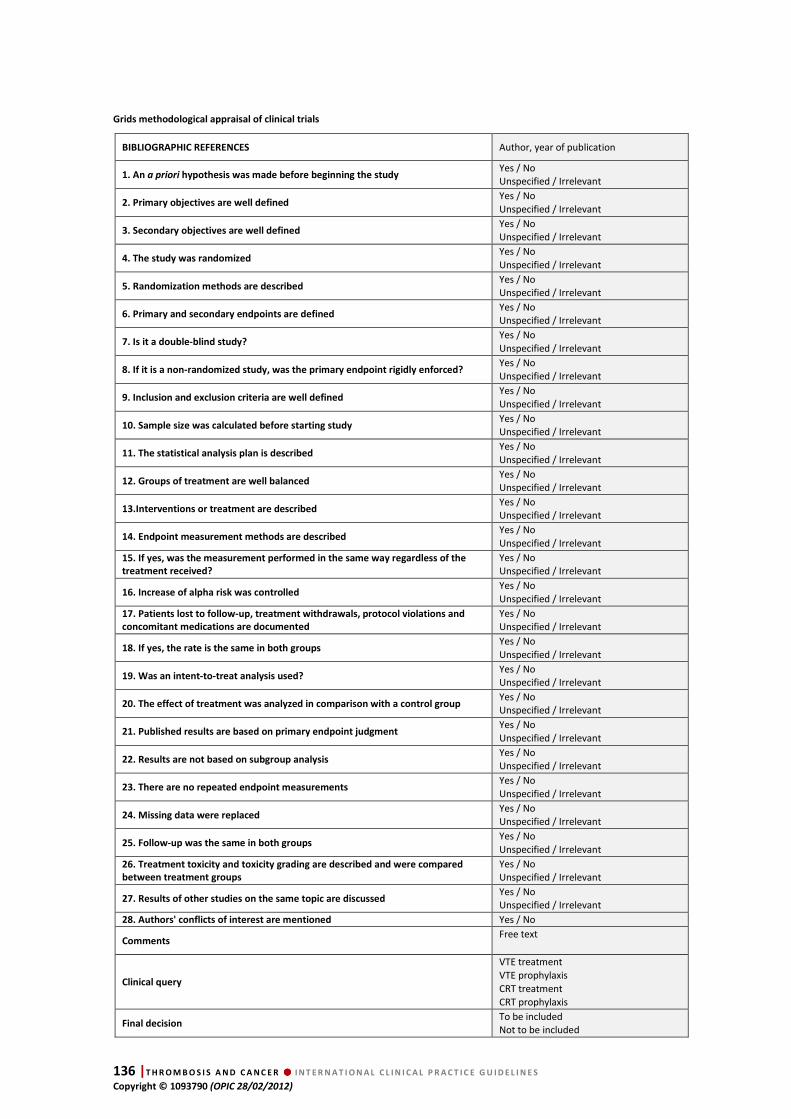
136 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Grids methodological appraisal of clinical trials
BIBLIOGRAPHIC REFERENCES Author, year of publication
1. An a priori hypothesis was made before beginning the study Yes / No Unspecified / Irrelevant
2. Primary objectives are well defined Yes / No
Unspecified / Irrelevant
3. Secondary objectives are well defined Yes / No Unspecified / Irrelevant
4. The study was randomized Yes / No
Unspecified / Irrelevant
5. Randomization methods are described Yes / No Unspecified / Irrelevant
6. Primary and secondary endpoints are defined Yes / No Unspecified / Irrelevant
7. Is it a double-blind study? Yes / No
Unspecified / Irrelevant
8. If it is a non-randomized study, was the primary endpoint rigidly enforced? Yes / No Unspecified / Irrelevant
9. Inclusion and exclusion criteria are well defined Yes / No
Unspecified / Irrelevant
10. Sample size was calculated before starting study Yes / No Unspecified / Irrelevant
11. The statistical analysis plan is described Yes / No
Unspecified / Irrelevant
12. Groups of treatment are well balanced Yes / No Unspecified / Irrelevant
13.Interventions or treatment are described Yes / No Unspecified / Irrelevant
14. Endpoint measurement methods are described Yes / No
Unspecified / Irrelevant
15. If yes, was the measurement performed in the same way regardless of the
treatment received?
Yes / No Unspecified / Irrelevant
16. Increase of alpha risk was controlled Yes / No
Unspecified / Irrelevant
17. Patients lost to follow-up, treatment withdrawals, protocol violations and
concomitant medications are documented
Yes / No Unspecified / Irrelevant
18. If yes, the rate is the same in both groups Yes / No
Unspecified / Irrelevant
19. Was an intent-to-treat analysis used? Yes / No Unspecified / Irrelevant
20. The effect of treatment was analyzed in comparison with a control group Yes / No Unspecified / Irrelevant
21. Published results are based on primary endpoint judgment Yes / No
Unspecified / Irrelevant
22. Results are not based on subgroup analysis Yes / No Unspecified / Irrelevant
23. There are no repeated endpoint measurements Yes / No
Unspecified / Irrelevant
24. Missing data were replaced Yes / No Unspecified / Irrelevant
25. Follow-up was the same in both groups Yes / No
Unspecified / Irrelevant
26. Treatment toxicity and toxicity grading are described and were compared
between treatment groups
Yes / No Unspecified / Irrelevant
27. Results of other studies on the same topic are discussed Yes / No Unspecified / Irrelevant
28. Authors' conflicts of interest are mentioned Yes / No
Comments Free text
Clinical query
VTE treatment
VTE prophylaxis
CRT treatment
CRT prophylaxis
Final decision To be included Not to be included
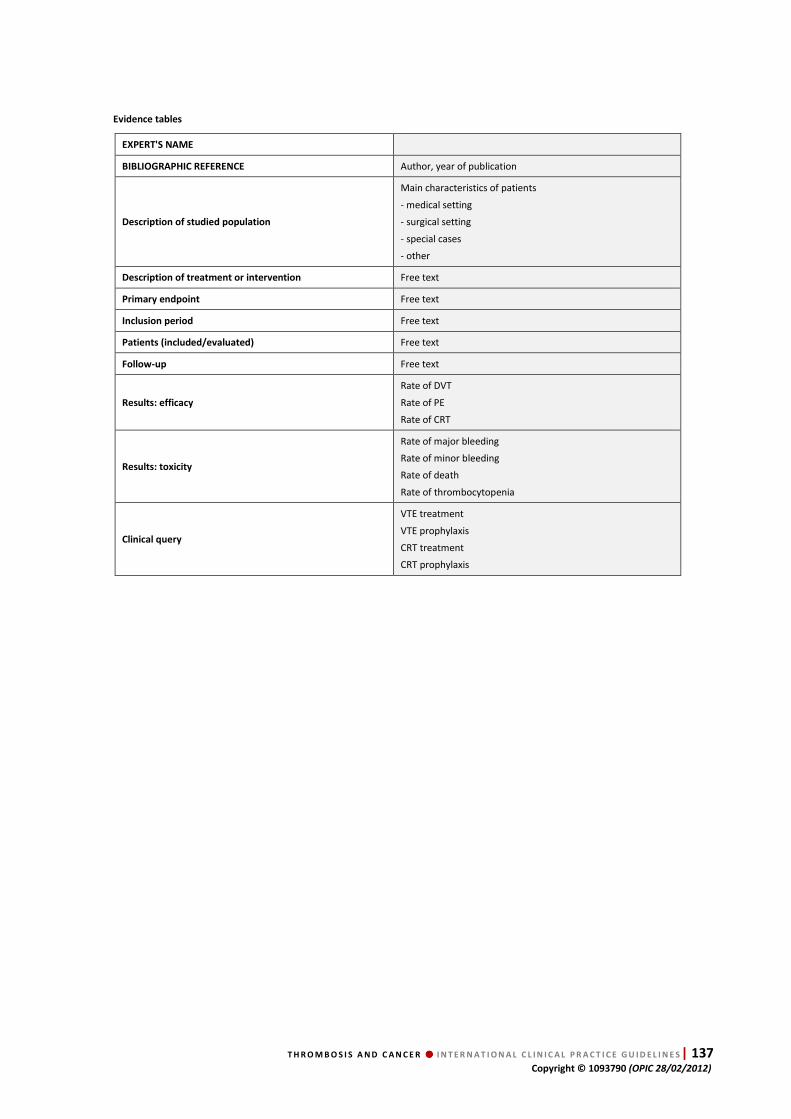
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 137 Copyright © 1093790 (OPIC 28/02/2012)
Evidence tables
EXPERT'S NAME
BIBLIOGRAPHIC REFERENCE Author, year of publication
Description of studied population
Main characteristics of patients
- medical setting
- surgical setting
- special cases
- other
Description of treatment or intervention Free text
Primary endpoint Free text
Inclusion period Free text
Patients (included/evaluated) Free text
Follow-up Free text
Results: efficacy
Rate of DVT
Rate of PE
Rate of CRT
Results: toxicity
Rate of major bleeding
Rate of minor bleeding
Rate of death
Rate of thrombocytopenia
Clinical query
VTE treatment
VTE prophylaxis
CRT treatment
CRT prophylaxis

138 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
Grids for clinical relevance
EXPERT'S NAME
BIBLIOGAPHIC REFERENCE Author, year of publication
1. The definition of the pathology is consistent with
recognized diagnostic criteria
Yes / No
Unspecified
Irrelevant
2. Follow-up was adapted to the evolution of the disease
Yes / No
Unspecified
Irrelevant
3. Patients are representative of those seen in medical
practice
Yes / No
Unspecified
Irrelevant
4. Care settings are similar to those of everyday practice
Yes / No
Unspecified
Irrelevant
5. Endpoints are relevant, reliable and objective
Yes / No
Unspecified
Irrelevant
6. Endpoint evaluation methods are rigorous
Yes / No
Unspecified
Irrelevant
7. The main criteria used to assess the comparability of
groups are relevant
Yes / No
Unspecified
Irrelevant
8. The treatments studied are still used today
Yes / No
Unspecified
Irrelevant
9. The treatments were administered optimally
Yes / No
Unspecified
Irrelevant
10.The effect of the new treatment is compared to the gold
standard treatment or a validated comparator
Yes / No
Unspecified
Irrelevant
11. The results of the study are clinically relevant or could
have a clinical impact
Yes
No
12. Main side effects are reported
Yes / No
Unspecified
Irrelevant
13. The benefit-risk ratio is acceptable Yes
No
Comments Free text
Clinical query
VTE treatment
VTE prophylaxis
CRT treatment
CRT prophylaxis
Final decision To be included
Not to be included
T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 139 Copyright © 1093790 (OPIC 28/02/2012)
15. References
ABDELKEFI2004: Abdelkefi A, Ben OT, Kammoun L et al. Prevention of central venous line-related thrombosis by continuous infusion of low-dose unfractionated heparin, in patients with haemato-oncological disease. Thromb
Haemost 2004;92:654-61.
ABDELKEFI2005: Abdelkefi A, Ben Romdhane N, Kriaa A etal. Prevalence of inherited prothrombotic abnormalities and central venous catheter-related thrombosis in haematopoietic stem cell transplant recipients. Bone Marrow Transplant 2005;36:885-9.
AGNELLI2005: Agnelli G, Bergqvist D, Cohen A et al. on behalf of the PEGASUS investigators. Randomized clinical trial of postoperative fondaparinux versus perioperative dalteparin for prevention of venous thromboembolism in high-risk abdominal surgery. Br J Surg 2005;92:1212-20.
AGNELLI2009: Agnelli G, Gussoni G, Bianchini C et al. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: a randomised, placebo-controlled, double-blind study. Lancet Oncology 2009;10:943-9.
AKL2007: Akl EA, Karmath G, Yosuico V et al. Anticoagulation for thrombosis prophylaxis in cancer patients with central venous catheters. Cochrane
Database Syst Rev 2007;(3):CD006468.
AKL2008A: Akl EA, Rohilla S, Barba M et al. Anticoagulation for the initial treatment of venous thromboembolism in patients with cancer: a systematic review. Cancer 2008;113:1685-94.
AKL2008B: Akl EA, Barba M, Rohilla S et al. Anticoagulation for the long term treatment of venous thromboembolism in patients with cancer. Cochrane
Database Syst Rev 2008;(2):CD006650.
AKL2008C: Akl EA, Barba M, Rohilla S, Terrenato I, Sperati F, Muti P, Schunemann HJ. Low-molecular-weight heparins are superior to vitamin K antagonists for the long term treatment of venous thromboembolism in patients with cancer: a Cochrane systematic review. J Exp Clin Cancer Res 2008;27:21.
AK2008D: Akl EA, Terrenato I, Barba M et al. Low-molecular-weight heparin vs unfractionated heparin for perioperative thromboprophylaxis in patients with cancer: a systematic review and meta-analysis. Arch
Intern Med 2008;168:1261-9
AKL2008E: Akl EA, Terrenato I, Barba M et al. Extended perioperative thromboprophylaxis in patients with cancer. Thromb Haemost 2008;100:1176-80.
AKL2011: Akl EA, Vasireddi SR, Gunukula S et al. Anticoagulation for the initial treatment of venous thromboembolism in patients with cancer (Review). Cochrane Database Syst Rev 2011;(6):CD006649.
AY2010: Ay C, Dunkler D, Marosi C et al. Prediction of venous thromboembolism in cancer patients. Blood
2010;116:5377-82.
BAYKAL2001: Baykal C, Al A, Demirtaş E et al. Comparison of enoxaparin and standard heparin in gynaecologic oncologic surgery: a randomised prospective double-blind clinical study. Eur J Gynaecol
Oncol 2001;22:127-30.
BENNETT2008: Bennett C, Silver S, Djulbegovic B et al. Venous thromboembolism and mortality associated with recombinant erythropoietin and darbepoetin administration for the treatment of cancer-associated anemia. JAMA 2008;299:914-24.
BERGQVIST1995: Bergqvist D, Burkmark U, Flordal P et al. Low molecular weight heparin started befoe surgery as prophylaxis against deep vein thrombosis: 2500 vs 5000 XaI units in 2070 patients. Br J Surg 1995;82:496-
501.
BERGQVIST2002A: Bergqvist D, Agnelli G, Cohen A et al, ENOXACAN II, I. Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med 2002;346:975-80.
BOHLIUS2006: Bohlius J, Wilson J, Seidenfeld J et al. Recombinant human erythropoietins and cancer patients: updated meta-analysis of 57 studies including 9353 patients. J Natl Cancer Inst. 2006;98:708-14.
BONA2000: Bona RD, Hickey AD, Wallace DM. Warfarin is safe as secondary prophylaxis in patients with cancer and a previous episode of venous thrombosis. Am J Clin
Oncol 2000;23:71-3.
BERGMANN1996: Bergmann JF, Neuhart E. A multicenter randomized double- blind study of enoxaparin compared with unfractionated heparin in the prevention of venous thromboembolic disease in elderly in-patients bedridden for an acute medical illness. Thromb Haemost 1996;76:529-34.
BERN1990: Bern M, Lokich J, Wallach S et al. Very low doses of warfarin can prevent thrombosis in central venous catheters. A randomized prospective trial. Ann
Intern Med 1990;112:423-8.
BIFFI2001: Biffi R, De Braud F, Orsi F et al. A randomized, prospective trial of central venous ports connected to standard open-ended or Groshong catheters in adult oncology patients. Cancer 2001;92:1204-12.
BIFFI2009: Biffi R, Orsi F, Pozzi S et al. Best choice of central venous insertion site for the prevention of catheter-related complications in adult patients who need cancer therapy: a randomized trial. Ann Oncol
2009;20:935-40.
CADMAN2004: Cadman A, Lawrance JA, Fitzsimmons L et al. To clot or not to clot? That is the question in central venous catheters. Clin Radiol 2004;59:349-55.
140 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
CAERS2005: Caers J, Fontaine C, Vinh-Hung V et al. Catheter tip position as a risk factor for thrombosis associated with the use of subcutaneous infusion ports. Support Care Cancer 2005;13:325-31.
CALLIGARO1991: Calligaro K, Bergen W, Haut M et al. Thromboembolic complications in patients with advanced cancer: anticoagulation versus Greenfield filter placement. Ann Vasc Surg 1991;5:186-9.
CARLO2004: Carlo JT, Lamont JP, McCarty TM et al. A prospective randomized trial demonstrating valved implantable ports have fewer complications and lower overall cost than nonvalved implantable ports. Am J Surg
2004;188:722-27.
CARRIER2007: Carrier M, Tay J, Fergusson D, Wells PS. Thromboprophylaxis for catheter-related thrombosis in patients with cancer: a systematic review of the randomized, controlled trials. J Thromb Haemost
2007;5:2552-54.
CARRIER2009: Carrier M, Le G, Cho R et al. Dose escalation of low molecular weight heparin to manage recurrent venous thromboembolic events despite systemic anticoagulation in cancer patients. J Thromb
Haemost 2009;7:760-5.
CERRATO1978: Cerrato D, Ariano C, Fiacchino F. Deep vein thrombosis and low-dose heparin prophylaxis in neurosurgical patients. J Neurosurg 1978;49:378-81.
CHAN1992: Chan A, Woodruff RK. Complications and failure of anticoagulation therapy in the treatment of venous thromboembolism in patients with disseminated malignancy. Aust N Z J Med 1992;22:119-22.
CHAUKIAL2008: Chaukiyal P, Nautiyal A, Radhakrishnan S et al. Thromboprophylaxis in cancer patients with central venous catheters. A systematic review and meta-analysis.Thromb Haemost 2008;99:38-43.
CHEW2006: Chew HK, Wun T, Harvey D, et al. Incidence of venous thromboembolism and its effect on survival among patients with common cancers. Arch Intern Med
2006;166:458-64.
CLARKEPEARSON1983: Clarke-Pearson D, Coleman R, Synan I et al. Anticoagulation therapy for VTE in patients with gynaecologic malignancy. Am J Obstet Gynecol
1983;147:369-75.
COHEN1991: Cohen J, Tenenbaum N, Citron M. Greenfield filter as primary therapy for deep venous thrombosis and/or pulmonary embolism in patients with cancer. Surgery 1991;109:12-5.
COHEN1992: Cohen J, Grella L, Citron M. Greenfield filter instead of heparin as primary treatment for deep venous thrombosis or pulmonary embolism in patients with cancer. Cancer 1992;70:1993-6.
COHEN2006: Cohen AT, Davidson B, Gallus A et al. Efficacy and safety of fondaparinux for the prevention of venous thromboembolism in older acute medical patients: randomised placebo controlled trial. BMJ
2006;332:325-9.
COEHN2008: Cohen AT, Tapson VF, Bergmann JF, Goldhaber SZ, Kakkar AK, Deslandes B, Huang W, Zayaruzny M, Emery L, Anderson FA Jr; ENDORSE Investigators. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet.
2008;371:387-94.
COLLEN2OO8: Collen J, Jackson J, Shorr A et al. Prevention of venous thromboembolism in neurosurgery : a metaanalysis. Chest 2008;134;237-49.
CONSTANTINI2001: Constantini S, Kanner A, Friedman A et al. Safety of perioperative minidose heparin in patients undergoing brain tumor surgery: a prospective, randomized, double-blind study. J Neurosurg.
2001;94:918-21.
COUBAN2005: Couban S, Goodyear M, Burnell M et al. Randomized placebo-controlled study of low-dose warfarin for the prevention of central venous catheter-associated thrombosis in patients with cancer. J Clin
Oncol 2005;23:4063-9.
CRAFT1996: Craft PS, May J, Dorigo A et al. Hickman catheters: left-sided insertion, male gender, and obesity are associated with an increased risk of complications. Aust N Z J Med 1996;26:33-39.
CURIGLIANO2006: Curigliano G, Mandalà M, Sbanotto A et al. Factor v Leiden mutation in patients with breast cancer with a central venous catheter: risk of deep vein thrombosis. Support Cancer Ther 2006;3:98-102.
DAHAN1986: Dahan R, Houlbert D, Caulin C, et al. Prevention of deep vein thrombosis in elderly medical in-patients by a low molecular weight heparin: a randomized double-blind trial. Haemostasis
1986;16:159-64.
DEBOURDEAU1996: Debourdeau P, Meyer G, Sayeg H et al. Traitement anticoagulant classique de la maladie thromboembolique veineuse chez les patients cancéreux. A propos d'une série rétrospective de 71 patients. Rev Med Int 1996;17:207-12.
DEBOURDEAU2008: Debourdeau P, Elalamy I, De Raigniac A, Meria P, Gornet JM, Amah Y, Korte Y, Marty M, Farge-Bancel D. Long term use of daily sub-cutaneous low-molecular-weight heparin in cancer patients: why hesitate any longer? Support Care Cancer. 2008
Dec;16:1333-41
DEBOURDEAU2009: Debourdeau P, Kassab-Chahmi D, Le Gal G et al. 2008 SOR guidelines for the prevention and treatment of thrombosis associated with central venous catheters in patients with cancer: report from the working group. Ann Oncol 2009;20:1459-71.
DECICCO2009: De Cicco M, Matovic M, Balestreri L et al. Early and short-term acenocumarine or dalteparin for the prevention of central vein catheter-related thrombosis in cancer patients: a randomized controlled study based on serial venographies. Ann Oncol
2009;20:1936-42.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 141 Copyright © 1093790 (OPIC 28/02/2012)
DEITCHER2006: Deitcher SR, Kessler CM, Merli G, et al. Secondary prevention of venous thromboembolic events in patients with active cancer: enoxaparin alone versus initial enoxaparin followed by warfarin for a 180-day period. Clin Appl Thromb Hemost 2006;12: 389-96.
DENTALI2008: Dentali F, Gianni M, Agnelli G, Ageno W. Association between inherited thrombophilic abnormalities and central venous catheter thrombosis in patients with cancer: a meta-analysis. J Thromb Haemost
2008;6:70-5.
DICKINSON1998: Dickinson L, Miller L, Patel C, Gupta S. Enoxaparin Increases the incidence of postoperative intracranial hemorrhage when initiated preoperatively for deep venous thrombosis prophylaxis in patients with brain tumors. Neurosurgery. 1998;43:1074-81.
DOLOVICH2000: Dolovich L, Ginsberg J, Douketis J et al. A meta-analysis comparing low-molecular-weight heparins with unfractionated heparin in the treatment of venous thromboembolism: examining some unanswered questions regarding location of treatment, product type, and dosing frequency. Arch Intern Med 2000;160:181-8.
DOUKETIS2010 Douketis J, Tosetto A, Marcucci M, et al. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med.
2010;153:523-31.
EASTRIDGE1995: Eastridge BJ, Lefor AT. Complications of indwelling venous access devices in cancer patients. J Clin Oncol 1995;13:233-38.
EINSTEIN2007: Einstein MH, Pritts EA, Hartenbach EM. Venous thromboembolism prevention in gynecologic cancer surgery: a systematic review. Gynecol Oncol
2007;105:813-9.
ELACCAOUI2007: El Accaoui RN, Shamseddeen WA, Taher AT. Thalidomide and thrombosis. Thromb Haemost
2007;97:1031-6.
ELTING2004: Elting LS, Escalante CP, Cooksley C, et al. Outcomes and cost of deep venous thrombosis among patients with cancer. Arch Intern Med. 2004;164:1653-
61.
ENOXACAN1997: ENOXACAN Study Group. Efficacy and safety of enoxaparin versus unfractionated heparin for prevention of deep vein thrombosis in elective cancer surgery: a double-blind randomized multicentre trial with venographic assessment. Br J Surg 1997;84,1099-
103.
EVANS 2010: Evans RS, Sharp JH, Linford LH, Lloyd JF, Tripp JS, Jones JP, Woller SC, Stevens SM, Elliott CG, Weaver LK. Risk of symptomatic DVT associated with peripherally inserted central catheters. Chest. 2010 Oct;138(4):803-10.
FARGE 2008: Farge D, Bosquet L, Kassab-Chahmi D et al. 2008 French national guidelines for the treatment of venous thromboembolism in patients with cancer: Report from the working group. Crit Rev Oncol Hematol
2010;73:31-46.
FARGE2010: Farge D, Durant C, Villers S, e al. Lessons from French national guidelines on the treatment of venous thrombosis and central venous catheter thrombosis in cancer patients. Thrombosis Research 2010; 125(suppl 2):S110-119.
FERRETTI2006: Ferretti G, Bria E, Giannarelli D et al. Is recurrent venous thromboembolism after therapy reduced by low-molecular-weight heparin compared with oral anticoagulants? Chest 2006;130:1808-16.
FIJNHEER2002: Fijnheer R, Paijmans B, Verdonck L et al. Factor V Leiden in central venous catheter-associated thrombosis. Br J Haematol. 2002;118:267-70.
FRANK2000: Frank D, Meuse J, Hirsch D et al. The treatment and outcome of cancer patients with thromboses on central venous catheters. J Thromb
Thrombolysis 2000;10:271-5.
GEERST2008: Geerts W, Bergqvist D, Pineo G et al. American College of Chest Physicians. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133(6 Suppl):381S-453S.
GOULD1999: Gould M, Dembitzer A, Doyle R et al. Low-molecular-weight heparins compared with unfractionated heparin for treatment of acute deep venous thrombosis. A meta-analysis of randomized, controlled trials. Ann Intern Med 1999;130:800-9.
GREENFIELD1997: Greenfield L, Proctor M, Saluja A. Clinical results of Greenfield filter use in patients with cancer. Cardiovasc Surg 1997;5:145-9.
GUYATT2008: Guyatt G, Oxman A, Kunz R et al. Rating quality of evidence of and strength of recommandations. BMJ 2008;336:1049-51.
GUYATT2008A: Guyatt G, Oxman A, Kunz R et al. for the GRADE. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ
2008;336;924-6
HARENBERG1996: Harenberg J, Roebruck P, Heene DL et al. Subcutaneous low-molecular-weight heparin versus standard heparin and the prevention of thromboembolism in medical inpatients. Haemostasis
1996;26:127-39.
HAAS2012: Haas SK, Freund M, Heigener D, Heilmann L, Kemkes-Matthes B, von Tempelhoff GF, Melzer N, Kakkar AK; TOPIC Investigators. Low-molecular-weight heparin versus placebo for the prevention of venous thromboembolism in metastatic breast cancer or stage III/IV lung cancer. Clin Appl Thromb Hemost.
2012;18:159-65.
HARRINGTON1997: Harrington K, Bateman A, Syrigos K, et al. Cancer-related thromboembolic disease in patients with solid tumours: a retrospective analysis. Ann Oncol
1997:8:669-73.
HEATON2002A: Heaton D, Han D, Inder A. Minidose (1 mg) warfarin as prophylaxis for central vein catheter thrombosis. Intern Med J 2002;32:84-8.

142 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
HEIT2000: Heit J, Silverstein M, Mohr D et al. Risk factors for deep vein thrombosis and pulmonary embolism: a population-based case-control study. Arch Intern Med
2000;160:809-15.
HETTIARACHCHI1998: Hettiarachchi R, Prins M, Lensing A, et al. Low molecular weight heparin versus unfractionated heparin in the initial treatment of venous thromboembolism. Curr Opin Pulm Med 1998;4:220-5.
HICKS2008: Hicks L, Haynes A, Reece D, et al. Hematology Disease Site Group of the Cancer Care Ontario Program in Evidence-based Care. A meta-analysis and systematic review of thalidomide for patients with previously untreated multiple myeloma. Cancer Treat Rev. 2008;34:442-52.
HUBBARD1994: Hubbard K, Roehm J, Abbruzzese JL. The Bird's Nest Filter. An alternative to long-term oral anticoagulation in patients with advanced malignancies. Am J Clin Oncol 1994;17:115-7.
HULL2006: Hull R, Pineo G, Brant R, et al. Long-term low-molecular-weight heparin versus usual care in proximal-vein thrombosis patients with cancer. Am J Med 2006;119:1062-72.
HUTTEN2000: Hutten B, Prins M, Gent M, et al. Incidence of recurrent thromboembolic and bleeding complications among patients with venous thromboembolism in relation to both malignancy and achieved international normalized ratio: a retrospective analysis. J Clin Oncol 2000;18:3078-83.
IHNAT1998: Ihnat D, Mills J, Hughes J, et al. Treatment of patients with venous thromboembolism and malignant disease: should vena cava filter placement be routine? J Vasc Surg 1998;28:800-7.
IKHLAQUE2006: Ikhlaque N, Seshadri V, Kathula S, et al. Efficacy of prophylactic warfarin for prevention of thalidomide-related deep venous thrombosis. Am J
Hematol 2006;81:420-2.
IORIO2000: Iorio A, Agnelli G. Low-molecular-weight and unfractionated heparin for prevention of venous thromboembolism in neurosurgery: a meta-analysis. Arch Intern Med. 2000;160:2327-32.
IORIO2003: Iorio A, Guercini F, Pini M. Low-molecular-weight heparin for the long-term treatment of symptomatic venous thromboembolism: meta-analysis of the randomized comparisons with oral anticoagulants. J Thromb Haemost2003;1:1906-13.
JANSEN2005: Jansen F, van der Straaten H, Roest M, et al. Elevated levels of D-dimer and fragment 1+2 upon central venous catheter insertion and factor V Leiden predict subclavian vein thrombosis. Haematologica.
2005;90:499-504.
JARRETT2002: Jarrett BP, Dougherty MJ, Calligaro KD. Inferior vena cava filters in malignant disease. J Vasc
Surg 2002;36:704-7.
KALMANTI2002: Kalmanti M, Germanakis J, Stiakaki E, et al. Prophylaxis with urokinase in pediatric oncology patients with central venous catheters. Pediatr Hematol
Oncol 2002;19:173-9.
KAKKAR2010: Kakkar V, Balibrea J, Martínez-González J, et al. for the CANBESURE Study Group. Extended prophylaxis with bemiparin for the prevention of venous thromboembolism after abdominal or pelvic surgery for cancer: the CANBESURE randomized study. J Thromb
Haemost 2010;8:1223-9.
KARTHAUS2006: Karthaus M, Kretzschmar A, Kroning H, et al. Dalteparin for prevention of catheter-related complications in cancer patients with central venous catheters: final results of a double-blind, placebo-controlled phase III trial. Ann Oncol 2006;17:289-96.
KEARNEY2009: Kearney J, Rossi S, Glinert K, et al. Venous thromboembolism (VTE) and survival in a cancer chemotherapy outpatient clinic: a retrospective chart validation of a VTE prediction model. Blood
2009;114:2503.
KEARON 2008: Kearon C, Kahn S, Agnelli G, et al. Antithrombotic therapy for venous thromboembolic disease: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest
2008;133(6 Suppl):454S-545S.
KHORANA2003: Khorana A. Malignancy, thrombosis and Trousseau: The case for an eponym. J Thromb Haemost
2003;1:2463-5.
KHORANA2007: Khorana A, Francis C, Culakova E, et al. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer 2007 15;110:2339-46.
KHORANA2007A: Khorana A, Francis C, Culakova E, et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb
Haemost. 2007;5:632-4.
KHORANA2008: Khorana A, Kuderer N, Culakova E, et al. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood
2008;111:4902-7.
KHORANA2009: Khorana A, Streiff M, Farge D, et al. Venous thromboembolism prophylaxis and treatment in cancer: a consensus statement of major guidelines panels and call to action. J Clin Oncol 2009;27:4919-26.
KHORANA2010: Khorana A, Herman K, Rubens D, et al. A Predictive risk score for cancer-associated thrombosis: role of screening in a prospective study. Blood 2010;116:
3173.
KIRPATRICK2007: Kirkpatrick A, Rathbun S, Whitsett T, et al. Prevention of central venous catheter-associated thrombosis: a meta-analysis. Am J Med 2007;120:901-13.
KLEBER2003: Kleber FX, Witt C, Vogel G, et al. Randomized comparison of enoxaparin with unfractionated heparin for the prevention of venous thromboembolism in medical patients with heart failure or severe respiratory disease. Am Heart J 2003;145:614-
21.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 143 Copyright © 1093790 (OPIC 28/02/2012)
KOVACS2006: Kovacs M, Kahn S, Rodger M, et al. A pilot study of central venous catheter survival in cancer patients using low-molecular-weight heparin (dalteparin) and warfarin without catheter removal for the treatment of upper extremity deep vein thrombosis (The Catheter Study). J Thromb Haemost 2007; 5:1650-3.
KRAUTH1987: Krauth D, Holden A, Knapic N, et al. Safety and efficacy of long-term oral anticoagulation in cancer patients. Cancer 1987;59:983-5.
LABOUREY2004: Labourey JL, Lacroix P, Genet D, et al. Thrombotic complications of implanted central venous access devices: prospective evaluation. Bull Cancer
2004;91:431-6.
LAUSEN1998: Lausen I, Jensen R, Jorgensen L, et al. Incidence and prevention of deep venous thrombosis occurring late after general surgery: randomised controlled study of prolonged thromboprophylaxis. Eur J
Surg 1998;164:657-63.
LECHLER1996: Lechler E, Schramm W, Flosbach CW, et al. The venous thrombotic risk in non-surgical patients: epidemiological data and efficacy/safety profile of a low-molecular-weight heparin (enoxaparin). Haemostasis
1996; 26(suppl 2):49-56.
LEE2003: Lee A, Levine M, Baker R, et al. Low-molecular-weight heparin versus a coumarin for the prevention of recurrent venous thromboembolism in patients with cancer. N Engl J Med 2003;349:146-53.
LEE2006: Lee A, Levine M, Butler G, et al. Incidence, risk factors, and outcomes of catheter-related thrombosis in adult patients with cancer. J Clin Oncol 2006;24:1404-8.
LEVIN1993: Levin J, Schiff D, Loeffler J, et al. Complications of therapy for venous thromboembolic disease in patients with brain tumors. Neurology
1993;43:1111-4.
LEVITAN1999: Levitan N, Dowlati A, Remick SC, et al. Rates of initial and recurrent thromboembolic disease among patients with malignancy versus those without malignancy. Risk analysis using Medicare claims data. Medicine (Baltimore) 1999;78:285-91.
LEIZOROVICZ2004: Leizorovicz A, Cohen A, Turpie A, et al. Randomized, placebo-controlled trial of dalteparin for the prevention of venous thromboembolism in acutely ill medical patients.Circulation 2004;110:874-9.
LENSING1995: Lnsing A, Prins M, Davidson B, et al. Treatment of deep venous thrombosis with low-molecular-weight heparins. A meta-analysis. Arch Intern
Med 1995;155:601-7.
LOPEZ-BERET2001: López-Beret P, Orgaz A, Fontcuberta J, et al. Low molecular weight heparin versus oral anticoagulants in the long-term treatment of deep venous thrombosis. J Vasc Surg 2001;33:77-90.
LOUZADA2009: Louzada M, Majeed H, Wells P. Efficacy of low- molecular-weight-heparin versus vitamin K antagonists for long term treatment of cancer-associated venous thromboembolism in adults: a systematic review of randomized controlled trials. Thromb Res
2009;123:837-44.
LUCIANI2001: Luciani A, Clement O, Halimi P, et al. Catheter-related upper extremity deep venous thrombosis in cancer patients: a prospective study based on Doppler US. Radiology 2001;220: 655–60.
LYMAN2007: Lyman G, Khorana A, Falanga A, et al. American Society of Clinical Oncology guideline: recommendations for venous thromboembolism prophylaxis and treatment in patients with cancer. J Clin
Oncol 2007;25:5490-505.
MANDALA2004: Mandalà M, Curigliano G, Bucciarelli P, et al. Factor V Leiden and G20210A prothrombin mutation and the risk of subclavian vein thrombosis in patients with breast cancer and a central venous catheter. Ann Oncol 2004;15:590-3.
MANDALA2006: Mandala M, Falanga A, Piccioli A, et al. Venous thromboembolism and cancer: guidelines of the Italian Association of Medical Oncology (AIOM). Crit Rev
Oncol Hematol 2006;59:194-204.
MANDALA2009: Mandala M, Falanga A, Roila F On behalf of the ESMO Guidelines Working Group. Management of venous thromboembolism in cancer patients: ESMO Clinical Recommendations. Ann Oncol 2009;20(S4):iv82-
iv84.
MANDALA2011: Mandalà M, Falanga A, Roila F; ESMO Guidelines Working Group. Management of venous thromboembolism (VTE) in cancer patients: ESMO Clinical Practice Guidelines. Ann Oncol 2011;22 Suppl 6:vi85-92.
MARAVEYAS2011: Maraveyas A, Waters J, Roy R, et al. Gemcitabine versus gemcitabine plus dalteparin thromboprophylaxis in pancreatic cancer. Eur J Cancer. 2011 Nov 17 [Epub ahead of print].
MAREC-BERARD2009: Marec-Berard P, Chastagner P, Kassab-Chahmi D, Casadevall N, Marchal C, Misset JL, Ray-Coquard I. 2007 Standards, Options, and Recommendations: use of erythropoiesis-stimulating agents (ESA: epoetin alfa, epoetin beta, and darbepoetin) for the management of anemia in children with cancer. Pediatr Blood Cancer. 2009;53(1):7-12.
MAXWELL2001: Maxwell G, Synan I, Dodge R, et al. Pneumatic compression versus low molecular weight heparin in gynecologic oncology surgery: a randomized trial. Obst Gynecol 2001;98:989-95.
MCLEAN2005: Mc Lean T, Fisher C, Snively B, et al. Central venous lines in children with lesser risk acute lymphoblastic leukemia: optimal type and timing of placement. J Clin Oncol 2005;23:3024-9.

144 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
MCLEOD2001: Mc Leod R, Geerts W, Sniderman K, et al. Canadian colorectal surgery DVT prophylaxis trial investigators. Subcutaneous heparin versus low-molecular-weight Heparin as thromboprophylaxis in patients undergoing colorectal surgery. Ann Surg
2001;233:438-44.
MEISTER2008: Meister B, Kropshofer G, Klein-Franke A, et al. Comparison of low-molecular-weight heparin and antithrombin versus antithrombin alone for the prevention of symptomatic venous thromboembolism in children with acute lymphoblastic leukemia. Pediatr Blood Cancer 2008;50:298-303.
MEWISSEN1999: Mewissen MW, Seabrook GR, Meissner MH, Cynamon J, Labropoulos N, Haughton SH. Catheter-directed thrombolysis for lower extremity deep venous thrombosis: report of a national multicenter registry. Radiology. 1999;211:39-49.
MEYER2002: Meyer G, Marjanovic Z, Valcke J, et al. Comparison of low-molecular weight heparin and warfarin for the secondary prevention of venous thromboembolism in patients with cancer: a randomized controlled study. Arch Intern Med 2002;162:1729-35.
MIKKOLA1997: Mikkola K, Patel S, Parker J, et al. Attenuation over 24 hours of the efficacy of thrombolysis of pulmonary embolism among patients with cancer. Am
Heart J 1997;134:603-7.
MITCHELL2003: Mitchell L, Andrew M, Hanna K, et al. Trend to efficacy and safety using antithrombin concentrate in prevention of thrombosis in children receiving l-asparaginase for acute lymphoblastic leukemia. Thromb Haemost 2003;90:235-44.
MISMETTI2001: Mismetti P, Laporte S, Darmon JY, et al. Meta-analysis of low molecular weight heparin in the prevention of venous thromboembolism in general surgery. Br J Surg 2001;88:913-30.
MISMETTI2003: Mismetti P, Mille D, Laporte S, et al. Low-molecular-weight heparin (nadroparin) and very low doses of warfarin in the prevention of upper extremity thrombosis in cancer patients with indwelling long-term central venous catheters: a pilot randomized trial. Haematologica 2003;88:67-73.
MISMETTI2005: Mismetti P, Quenet S, Levine M, et al. Enoxaparin in the treatment of deep vein thrombosis with or without pulmonary embolism: an individual patient data meta-analysis. Chest 2005;128:2203-10.
MONREAL1996: Monreal M, Alastrue A, Rull M, et al. Upper extremity deep venous thrombosis in cancer patients with venous access devices—prophylaxis with a low molecular weight heparin (Fragmin). Thromb Haemost 1996;75:251-3.
MONREAL2004: Monreal M, Zacharski L, Jimenez J, et al. Fixed dose low-molecular-weight heparin for secondary prevention of venous thromboembolism in patients with disseminated cancer: a prospective cohort study. J Thromb Haemost 2004;2:1311-5.
MOORE1981: Moore FD, Osteen R, Karp D, et al. Anticoagulants, venous thromboembolism and the cancer patient. Arch Surg 1981;116:405-7.
MORAZIN2005: Morazin F, Kriegel I, Asselain B, et al. Thrombose symptomatique sur cathéter veineux central de longue durée en oncologie: un score de risque prédictif? Rev Med Intern 2005;26:273-9.
NCCN 20111: Venous thromboembolic disease NCCN guidelines V2.2009. 2009. http://www.nccn.org/professionals/physician_gls/PDF/vte.pdf Accessed on 08.08.2011.
NIERS2007: Niers T, Di N, Klerk C, et al. Prevention of catheter-related venous thrombosis with nadroparin in patients receiving chemotherapy for hematologic malignancies: a randomized, placebo-controlled study. J Thromb Haemost 2007;5:1878-82.
NIGHTINGALE1997: Nightingale C, Norman A, Cunningham D, et al. A prospective analysis of 949 long-term central venous access catheters for ambulatory chemotherapy in patients with gastrointestinal malignancy. Eur J Cancer 1997;33:398-403.
NOBLE2008: Noble S, Shelley M, Coles B, et al (Thrombosis Taskgroup); on behalf of Association for Palliative Medicine for Great Britain and Ireland. Management of venous thromboembolism in patients with advanced cancer: a systematic review and meta-analysis. Lancet Oncol 2008;9:577-84
NURMOHAMED1996: Nurmohamed M, van Riel A, Henkens C, et al. Low molecular weight heparin and compression stockings in the prevention of venous thromboembolism in neurosurgery. Thromb Haemost
1996;75:233-8.
OATESWHITEHEAD2003: Oates-Whitehead R, D'Angelo A, Mol B. Anticoagulant and aspirin prophylaxis for preventing thromboembolism after major gynaecological surgery. Cochrane Database Syst Rev 2003;(4):CD003679.
PALARETI2000: Palareti G, Legnani C, Lee A, et al. A comparison of the safety and efficacy of oral anticoagulation for the treatment of venous thromboembolic disease in patients with or without malignancy. Thromb Haemost 2000;84:805-10.
PALUMBO2008: Palumbo A, Rajkumar S, Dimopoulos M, et al on behalf of the International Myeloma Working Group. Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia
2008;22:414-23.
PALUMBO2011: Palumbo A, Cavo M, Bringhen S, et al. Aspirin, warfarin, or enoxaparin thromboprophylaxis in patients with multiple myeloma treated with thalidomide: a phase III, open-label, randomized trial. J Clin Oncol 2011;10;29:986-93.
PANUCCI2009: Pannucci CJ, Chang EY, Wilkins EG. Venous thromboembolic disease in autogenous breast reconstruction. Ann Plast Surg.2009;63:34-8.
PERRY2009: Perry S, Bohlin C, Reardon D, et al. Tinzaparin prophylaxis against venous thromboembolic complications in brain tumor patients. J Neurooncol
2009;95:129-34.

T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S| 145 Copyright © 1093790 (OPIC 28/02/2012)
PRANDONI2002: Prandoni P, Lensing AW, Piccioli A, et al. Recurrent venous thromboembolism and bleeding complications during anticoagulant treatment in patients with cancer and venous thrombosis. Blood
2002;100:3484–8.
PRICE2010: Price L, Nguyen M, Picozzi V, et al. Portal vein thrombosis in pancreatic cancer: natural history, risk factors and implications for patient management. 2010
Gastrointestinal Cancer Symposium Program and
Proceedings. 2010;Abstract 143.
PUCHEU1996: Pucheu A, Dierhas M, Leduc B, et al. Fibrinolyse des thromboses veineuses profondes sur dispositifs de perfusion implantables. A propos d'une série consécutive de 57 thromboses et de 32 fibrinolyses. Bull Cancer 1996;83:293-9.
QUINLAN2004: Quinlan D, McQuillan A, Eikelboom JW. Low-molecular-weight heparin compared with intravenous unfractionated heparin for treatment of pulmonary embolism: a meta-analysis of randomized, controlled trials. Ann Intern Med 2004;140:175-83.
RASMUSSEN2006: Rasmussen M, Jorgensen L, Wille-Jörgensen P, et al on the behalf of the FAME investigators. Prolonged prophylaxis with dalteparin to prevent late thromboembolic complications in patients undergoing major abdominal surgery: a multicenter randomized open-label study. J Thromb Haemost
2006;4:2384-90.
RATCLIFFE1999: Ratcliffe M, Broadfoot C, Davidson M, et al. Thrombosis, markers of thrombotic risk, indwelling central venous catheters and antithrombotic prophylaxis using low-dose warfarin in subjects with malignant disease. Clin Lab Haematol 1999;21:353-7.
RAWSON2007: Rawson K, Newburn-Cook C. The use of low-dose warfarin as prophylaxis for central venous catheter thrombosis in patients with cancer: a meta-analysis. Oncol Nurs Forum 2007;34:1037-43.
RIESS2009: Riess H, Pelzer U, Deutschinoff G, et al. PROSPECT-CONKO 004: a prospective, randomized trial of simultaneous pancreatic cancer treatment with enoxaparin and chemotherapy). ASCO 2009, abstract
LBA4506.
ROCHA2000: Rocha E, Martinez-Gonzalez M, Montes R, et al. Do the low molecular weight heparins improve efficacy and safety of the treatment of deep venous thrombosis? A meta-analysis. Haematologica
2000;85:935-42.
ROMERA2009: Romera A, Cairols M, Vila-Coll R, et al. A randomised open-label trial comparing long-term sub-cutaneous low-molecular-weight heparin compared with oral-anticoagulant therapy in the treatment of deep venous thrombosis. Eur J Vasc Endovasc Surg
2009;37:349-56.
RUUD2002: Ruud E, Holmstrøm H, Natvig S, et al. Prevalence of thrombophilia and central venous catheter-associated neck vein thrombosis in 41 children with cancer: a prospective study. Med Pediatr Oncol
2002;38:405-10.
RUUD2006: Ruud E, Holmstrom H, De Lange C, et al. Low-dose warfarin for the prevention of central line-associated thromboses in children with malignancies--a randomized, controlled study. Acta Paediatr
2006;95:1053-9.
SABER2011 Saber W, Moua T, Williams E, et al. Risk factors of catheter-related thrombosis (CRT) in cancer patients: a patient-level data (IPD) meta-analysis of clinical trials and prospective studies. J Thromb Haemost 2011;9:312-9.
SALIBA2011: Saliba W, Nitzan O, Rock W, et al. Non-therapeutic anti-FXa levels are common among medical ward patients treated with enoxaparin. Ann Hematol
2011;90:1345-51.
SAMAMA1999: Samama MM, Cohen AT, Darmon JY, et al. A comparison of enoxaparin with placebo for the prevention of venous thromboembolism in acutely ill medical patients. N Engl J Med 1999;341:793-800.
SAVAGE1999: Savage KJ, Wells PS, Schulz V, et al. Outpatient use of low molecular weight heparin (Dalteparin) for the treatment of deep vein thrombosis of the upper extremity. Thromb Haemost 1999;82:1008-
10.
SCHIFF1994: Schiff D, De Angelis LM. Therapy of venous thromboembolism in patients with brain metastases. Cancer1994;73:493-8.
SCHINDLER1999: Schindler J, Bona R, Chen H, et al. Regional thrombolysis with urokinase for central venous catheter-related thrombosis in patients undergoing high-dose chemotherapy with autologous blood stem cell rescue. Clin Appl Thromb Hemostas 1999;5:25-9.
SCHLEICH2001: Schleich J, Morla O, Laurent M, et al. Long-term follow-up of percutaneous vena cava filters: a prospective study in 100 consecutive patients. Eur J Vasc
Endovas Surg 2001;21:450-7.
SCHULMAN2005: Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb
Haemost 2005;3:692-4.
SCHULMAN2010: Schulman S, Angerås U, Bergqvist D, et al Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in surgical patients. J Thromb Haemost 2010;8:202-4.
SCHUNN2006: Schunn C, Schunn G, Hobbs G, et al. Inferior vena cava filter placement in late-stage cancer. Vasc Endovasc Surg 2006;40:287-94.
SCHWARZ1996: Schwarz R, Marrero A, Conlon K et al. Inferior vena cava filters in cancer patients: indications and outcome. J Clin Oncol 1996;14:652-7.

146 |T H R O M B O S I S A N D C A N C E R ���� I N T E R N A T I O N A L C L I N I C A L P R A C T I C E G U I D E L I N E S
Copyright © 1093790 (OPIC 28/02/2012)
SHUKLA2008: Shukla P, Siddachari R, Ahire S, et. Postoperative deep vein thrombosis in patients with colorectal cancer. Ind J Gastroenterol 2008;27:71-3.
SIMONNEAU2006: Simonneau G, Laporte S, Mismetti P, et al. A randomized study comparing the efficacy and safety of nadroparin 2850 IU. J Thromb Haemost
2006;4:1693-700.
SIRAGUSA1996: Siragusa S, Cosmi B, Piovella F, et al. Low-molecular-weight heparins and unfractionated heparin in the treatment of patients with acute venous thromboembolism: results of a meta-analysis. Am J Med
1996;100:269-77.
SIRAGUSA2010: Siragusa S, Malato A, Mascheroni D, et al. The optimal duration of anticoagulant therapy In patients with cancer-related deep vein thrombosis: the advantage of using residual vein thrombosis (the Cancer-DACUS Study). Blood 2010;116:190.
STEIN2006: Stein P, Beemath A, Meyers F, et al. Incidence of venous thromboembolism in patients hospitalized with cancer. Am J Med. 2006;119:60-8.
TRAN 2010: Tran H, Arellano M, Chamsuddin A, Flowers C, Heffner LT, Langston A, Lechowicz MJ, Tindol A, Waller E, Winton EF, Khoury HJ. Deep venous thromboses in patients with hematological malignancies after peripherally inserted central venous catheters. Leuk Lymphoma. 2010;51:1473-7
TROUSSEAU 1865: Trousseau A. Plegmasia alba dolens. Lectures on clinical medicine, delivered at the Hotel-Dieu, Paris. 1865;5:281-332.
TURPIE1989: Turpie A, Hirsch J, Gent M, et al. Prevention of deep vein thrombosis in potential neurosurgical patients; a randomized trial comparing graduated compression stockings plus intermittent pneumatic compression with control. Arch Med Intern
1989;149:679-681.
VANDOORMAAL2009: van Doormaal F, Raskob G, Davidson B, et al. Treatment of venous thromboembolism in patients with cancer: subgroup analysis of the Matisse clinical trials. Thromb Haemost
2009;101:762-9.
VANDOORMAAL2010: van Doormaal F, Cohen A, Davidson B, et al. Idraparinux versus standard therapy in the treatment of deep venous thrombosis in cancer patients: A subgroup analysis of the VANGOGH-DVT trial. Thromb Haemost 2010;104:86-91.
VANROODEN2004 : Van Rooden C, Rosendaal F, Meinders A, et al. The contribution of factor V Leiden and prothrombin G20210A mutation to the risk of
central venous catheter-related thrombosis. Haematologica 2004;89:201-6.
VANROODEN2008: van Rooden C, Schippers E, Guiot H, et al. Prevention of coagulase-negative staphylococcal central venous catheter-related infection using urokinase rinses: a randomized double-blind controlled trial in patients with hematologic malignancies. J Clin Oncol
2008;26:428-33.
VERSO2003: Verso M, Agnelli G. Venous thromboembolism associated with long-term use of central venous catheters in cancer patients. J Clin Oncol
2003;21:3665-75.
VERSO2005: Verso M, Agnelli G, Bertoglio S, et al. Enoxaparin for the prevention of venous thromboembolism associated with central vein catheter: a double-blind, placebo-controlled, randomized study in cancer patients. J Clin Oncol 2005;23:4057-62.
VERSO2010: Verso M, Gussoni G, Agnelli G. Prevention of venous thromboembolism in patients with advanced lung cancer receiving chemotherapy: a combined analysis of the PROTECHT and TOPIC-2 studies. J Thromb
Haemost 2010 Jul;8:1649-51.
VUCIC2002: Vucic N, Ostojic R, Svircic T. Treatment of deep vein thrombosis with oral anticoagulants in patients with malignancy: prospective cohort study. Croat Med J 2002;43:296-300.
WALLACE2004: Wallace M, Jean J, Gupta S, et al. Use of inferior vena caval filters and survival in patients with malignancy. Cancer 2004;101:1902-7.
WERMES1999: Wermes C, von Depka Prondzinski M, Lichtinghagen R, et al. Clinical relevance of genetic risk factors for thrombosis in paediatric oncology patients with central venous catheters. Eur J Pediatr 1999;158
Suppl 3:S143-6.
YOUNG2009: Young A, Billingham L, Begum G, et al WARP Collaborative Group. Warfarin thromboprophylaxis in cancer patients with central venous catheters (WARP): an open-label randomised trial. Lancet 2009;373:567-74.
ZANGARI2004: Zangari M, Barlogie B, Anaissie E, et al. Deep vein thrombosis in patients with multiple myeloma treated with thalidomide and chemotherapy: effects of prophylactic and therapeutic anticoagulation. Br J
Haematol 2004;126:715-21.
ZERATI2005: Zerati A, Wolosker N, Yazbek G, et al. Vena cava filters in cancer patients: experience with 50 patients. Clinics (Sao Paulo, Brazil) 2005;60:361-6.