Embed Size (px)
Citation preview

7/8/2011
1
VENOUS DOPPLER SONOGRAPHY OF THE EXTREMITIES
The 35th Annual Vanderbilt Diagnostic Sonography Symposium
July 23-24, 2011E. JAMES ANDREWS, JR., M.D., FACR, FACC
DEPARTMENT OF RADIOLOGY AND RADIOLOGICAL SCIENCESVANDERBILT UNIVERSITY MEDICAL CENTER
DISCLOSURESTATEMENT
There are no financial relationships to disclose
As you can see, I have nothing elseto disclose.
“Longevity is a vascular question.”g y
Sir William Osler
MORTALITY FROM PULMONARY EMBOLUS AND OTHER CONSEQUENCES OF DVT
200,000 DEATHS PER YEAR FROM DVT AND IT’S CONSEQUENCESCONSEQUENCES
ANNUAL COMBINED INCIDENCE OF PE & DVT IN US: 70/100,000
American Public Health Association report 2004
SCOPE OF THE PROBLEM
UP TO 20 MILLION CASES OF DVT/YR
MANY ARE ASYMPTOMATIC
MAJORITY ARE INFRAPOPLITEAL
20-30% WILL PROPOGATE, RESULTING IN INCREASED RISK OF PE
30% MORTALITY IF UNTREATED
UP TO 50% WITH DVT HAVE SILENT PE
90% OF PE COME FROM LOWER EXT
7/8/2011
2
NUMBERS
26,279 Ultrasound studies were performed at Vanderbilt during a 12 month period in 2010-2011.
4,274 were venous sonograms of the extremities to evaluate for DVT.
DVT studies account for approximately 16% of all ultrasound exams at Vanderbilt.
The average is about 12 cases per day.
1. Discuss risk factors and compare various diagnostic tests for the diagnosis of DVT
OBJECTIVES
diagnosis of DVT.
2. Present sonographic technique for evaluation of the extremities for deep venous thrombosis (DVT).
3. Develop an algorithm for diagnostic testing for DVT including D-dimer.
DEEP VENOUS THROMBOSIS
CLINICAL DIAGNOSIS IS DIFFICULTRISK FACTORS ARE IMPORTANT PATHOPHYSIOLOGY – ANATOMY TECHNIQUE – PROTOCOLSACUTE VS. CHRONIC DVTUPPER EXTREMITY DVTA FEW INTERESTING CASE EXAMPLESD-DIMER AND ALGORITHM
DIAGNOSTIC TESTS FOR DVT
SonographyContrast venography (90% sensitive)Nuclear medicine MRI (MRV) - abdomen and pelvis Impedance pletysmographyCT PET ?D-DIMER
COMPARISON OF DIAGNOSTIC TESTS
Sonography – 97% sensitive for DVT
MRI (MRV) – 96% sensitive for DVT( )
CT – 97% sensitive for DVT
D-Dimer – 99% sensitive for DVT
48% specific
DVT - CLINICAL DIAGNOSIS
Clinical signs present in only 50%
Acute unilateral leg swelling
Calf asymmetry of more than 2 cmCalf asymmetry of more than 2 cm
Risk factors are important
Clinical evaluation is not reliable
Criado et al; Surgery 1997
Meyer et al; Ann Vasc Surg 1995
Anderson; J Vasc Tech 1989
7/8/2011
3
PULMONARY EMBOLUS
3rd most common form of CV disease
At autopsy, 64% have sub-clinical PE
Only approximately 30/100 cases diagnosed
CT FROM ER IN A PATIENT WITH SHORTNESS OF BREATH
THE PROBLEM CONTINUES
40-70% OF PATIENTS WITH DVT WILL DEVELOP POST PLEBOTIC SYNDROME
1 Pain1. Pain
2. Chronic swelling
3. Soft tissue ulceration
4. Valve injury with incompetence
5. Venous hypertension
RISK FACTORS – THE BIG 3
AGE OLDER THAN 75 YEARS
PREVIOUS HISTORY OF DVT
CANCER
Arch Intern Med.164:963-968,2004
7/8/2011
4
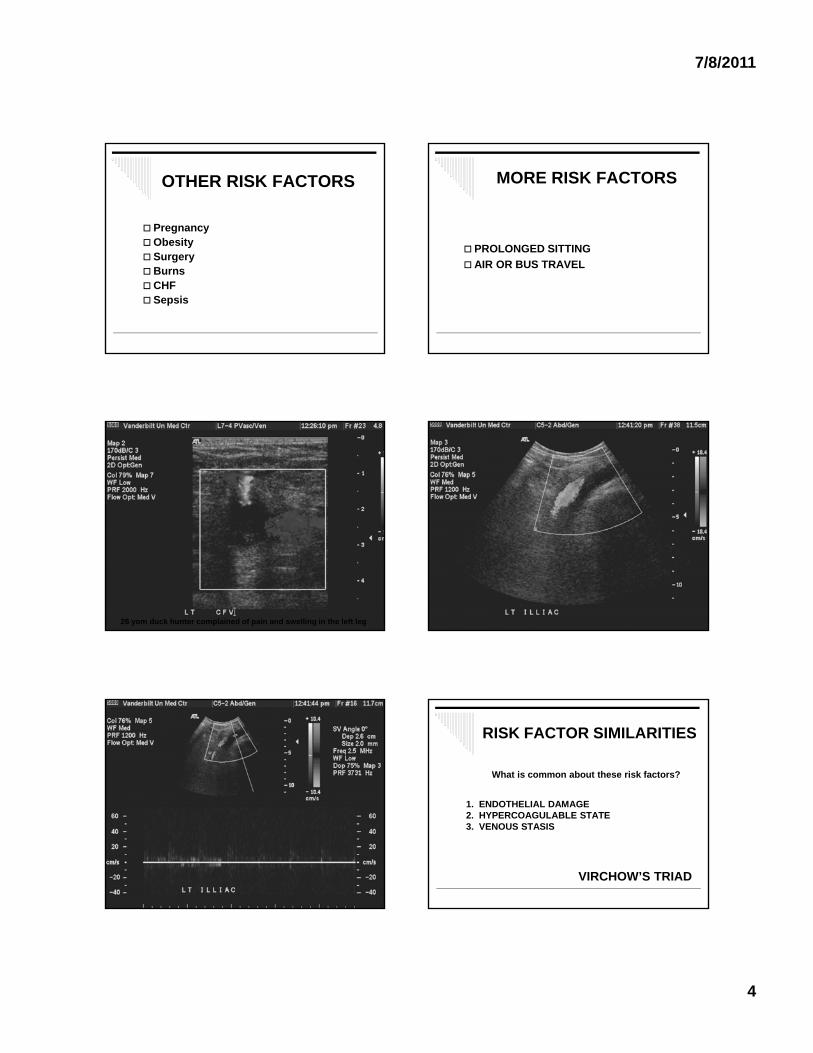
OTHER RISK FACTORS
PregnancyObesity SurgeryBurnsCHF Sepsis
MORE RISK FACTORS
PROLONGED SITTING PROLONGED SITTING
AIR OR BUS TRAVEL
26 yom duck hunter complained of pain and swelling in the left leg
RISK FACTOR SIMILARITIES
1 ENDOTHELIAL DAMAGE
What is common about these risk factors?
1. ENDOTHELIAL DAMAGE2. HYPERCOAGULABLE STATE3. VENOUS STASIS
VIRCHOW’S TRIAD
7/8/2011
5
COAGULATION ACTIVATED BY AIR TRAVEL ?
71 volunteers exposed to three conditions: 1. 8 hour plane flight; 2. 8 hours of immobilization in a cinema; 3. 8hours of immobilization in a cinema; 3. 8 hours of normal activity.
Thrombin-antithrombin (TAT) levels higher after plane flight.
D-Dimer values rose after plane flight
Rosendaal, F.; The Lancet; March 11, 2006
CT AFTER A LONG PLANE RIDE
ORIGINALLY DIAGNOSED AS PNEUMONIA
PATHOPHYSIOLOGY OF LOWER EXTREMITY DVT
Usually begins in the calf veins
Typically behind valve leaflets
40% l 40% resolve
40% organize
20% propagate
Acute/partially occlusive tend to embolize
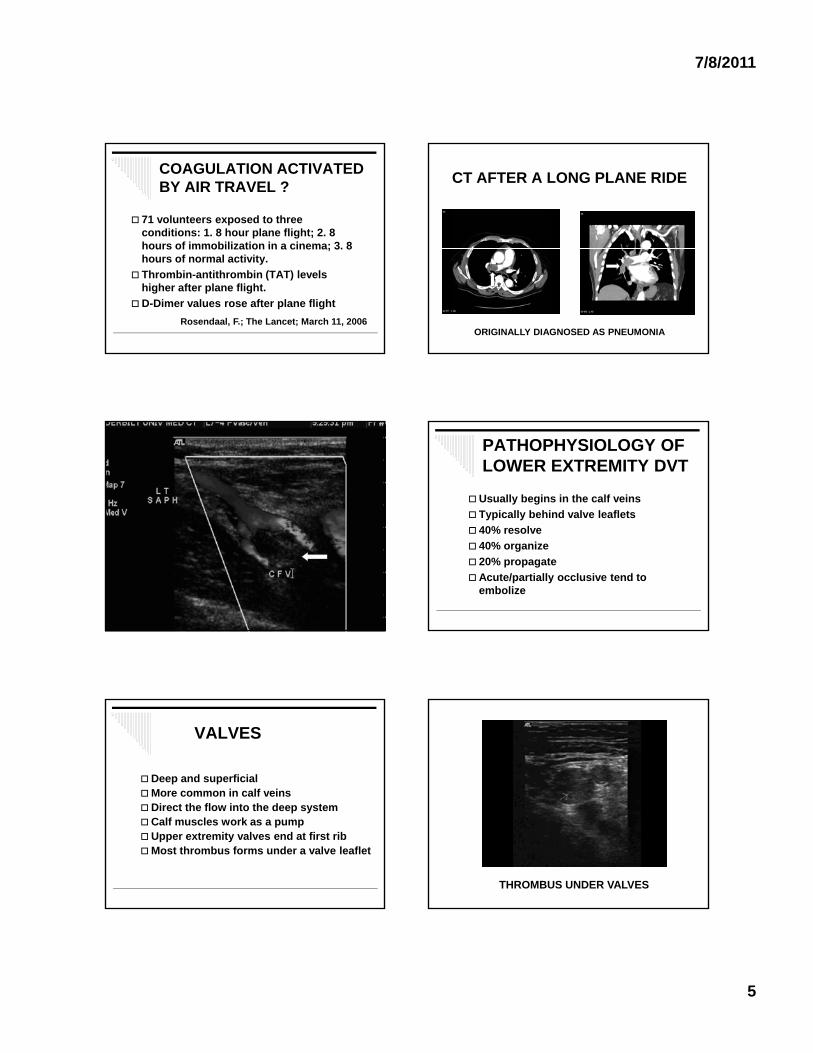
VALVES
Deep and superficialMore common in calf veins
Di t th fl i t th d tDirect the flow into the deep systemCalf muscles work as a pumpUpper extremity valves end at first ribMost thrombus forms under a valve leaflet
THROMBUS UNDER VALVES
7/8/2011
6
THROMBUS UNDER VALVE
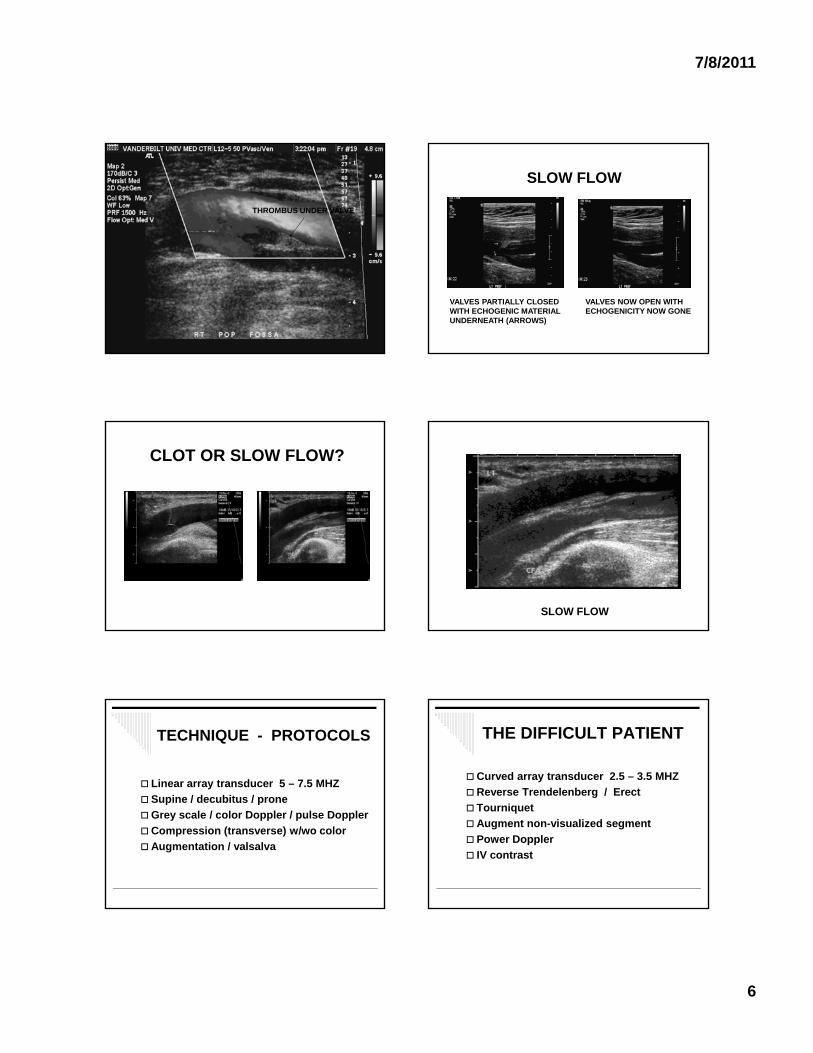
SLOW FLOW
VALVES PARTIALLY CLOSED WITH ECHOGENIC MATERIAL UNDERNEATH (ARROWS)
VALVES NOW OPEN WITHECHOGENICITY NOW GONE
CLOT OR SLOW FLOW?
SLOW FLOW
TECHNIQUE - PROTOCOLS
Linear array transducer 5 – 7.5 MHZ
Supine / decubitus / pronep p
Grey scale / color Doppler / pulse Doppler
Compression (transverse) w/wo color
Augmentation / valsalva
THE DIFFICULT PATIENT
Curved array transducer 2.5 – 3.5 MHZ
Reverse Trendelenberg / Erect
T i t Tourniquet
Augment non-visualized segment
Power Doppler
IV contrast
7/8/2011
7
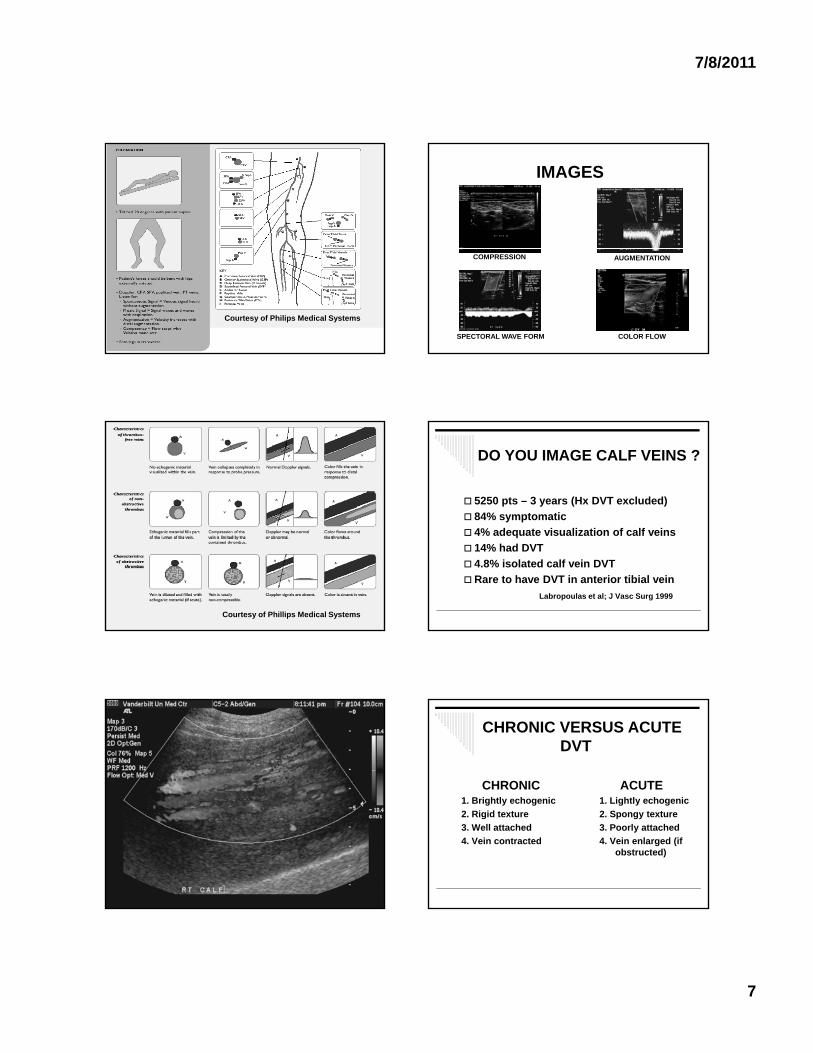
Courtesy of Philips Medical Systems
IMAGES
COMPRESSION AUGMENTATION
SPECTORAL WAVE FORM COLOR FLOW
Courtesy of Phillips Medical Systems
DO YOU IMAGE CALF VEINS ?
5250 pts – 3 years (Hx DVT excluded)
84% symptomatic
4% adequate visualization of calf veins
14% had DVT
4.8% isolated calf vein DVT
Rare to have DVT in anterior tibial vein
Labropoulas et al; J Vasc Surg 1999
CHRONIC VERSUS ACUTE DVT
CHRONIC1. Brightly echogenic
ACUTE1. Lightly echogenicg y g
2. Rigid texture
3. Well attached
4. Vein contracted
g y g
2. Spongy texture
3. Poorly attached
4. Vein enlarged (if obstructed)
7/8/2011
8
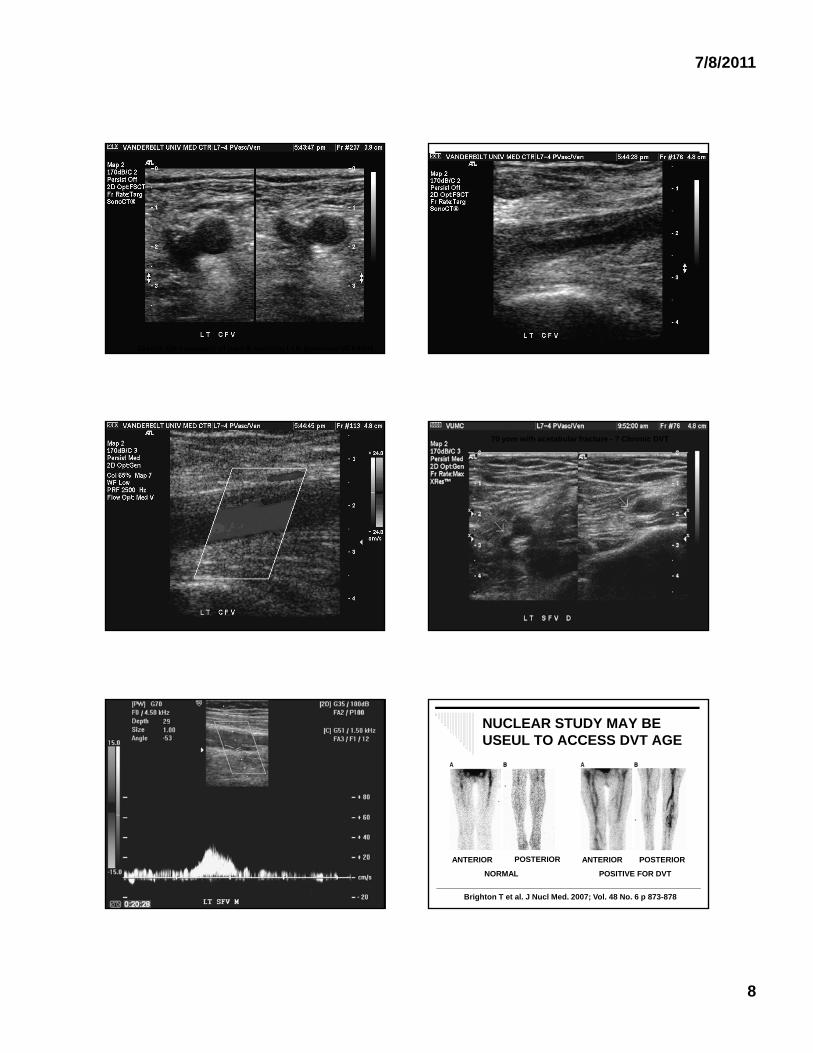
33yom, ER complaint of pain & swelling LLE (previous VCFilter)
70 yom with acetabular fracture - ? Chronic DVT
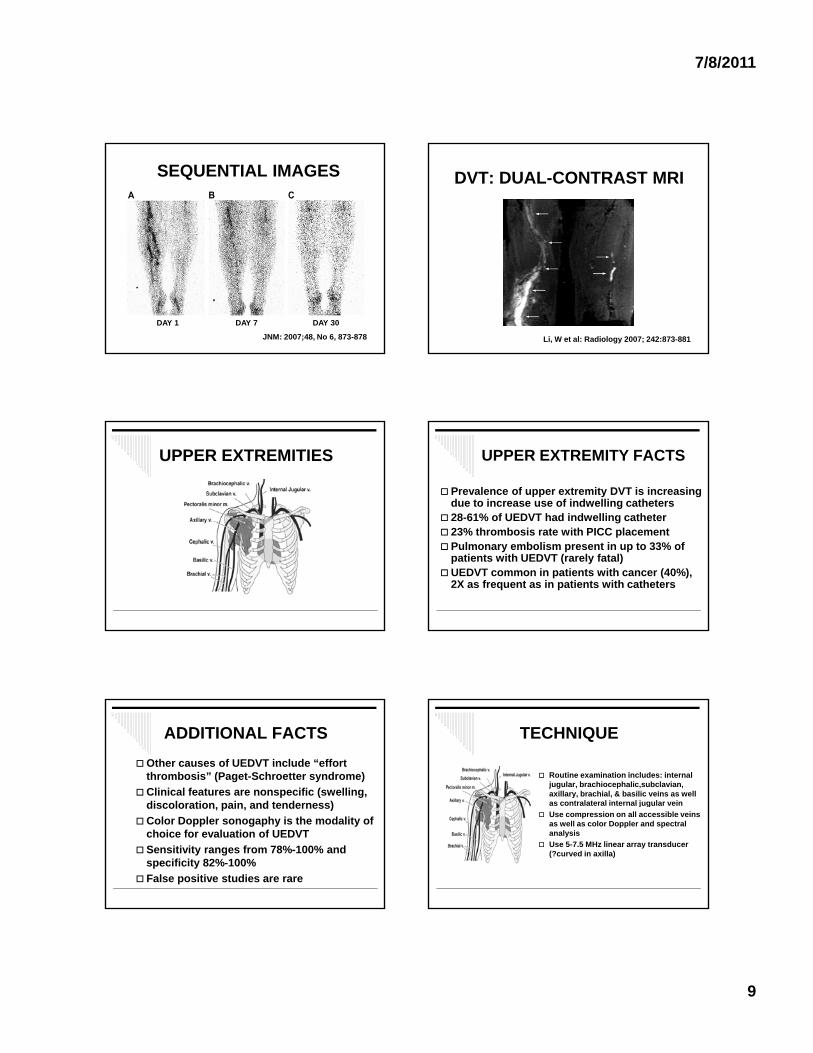
NUCLEAR STUDY MAY BE USEUL TO ACCESS DVT AGE
ANTERIOR POSTERIOR
NORMAL
ANTERIOR POSTERIOR
POSITIVE FOR DVT
Brighton T et al. J Nucl Med. 2007; Vol. 48 No. 6 p 873-878
7/8/2011
9
SEQUENTIAL IMAGES
DAY 1 DAY 7 DAY 30
JNM: 2007;48, No 6, 873-878
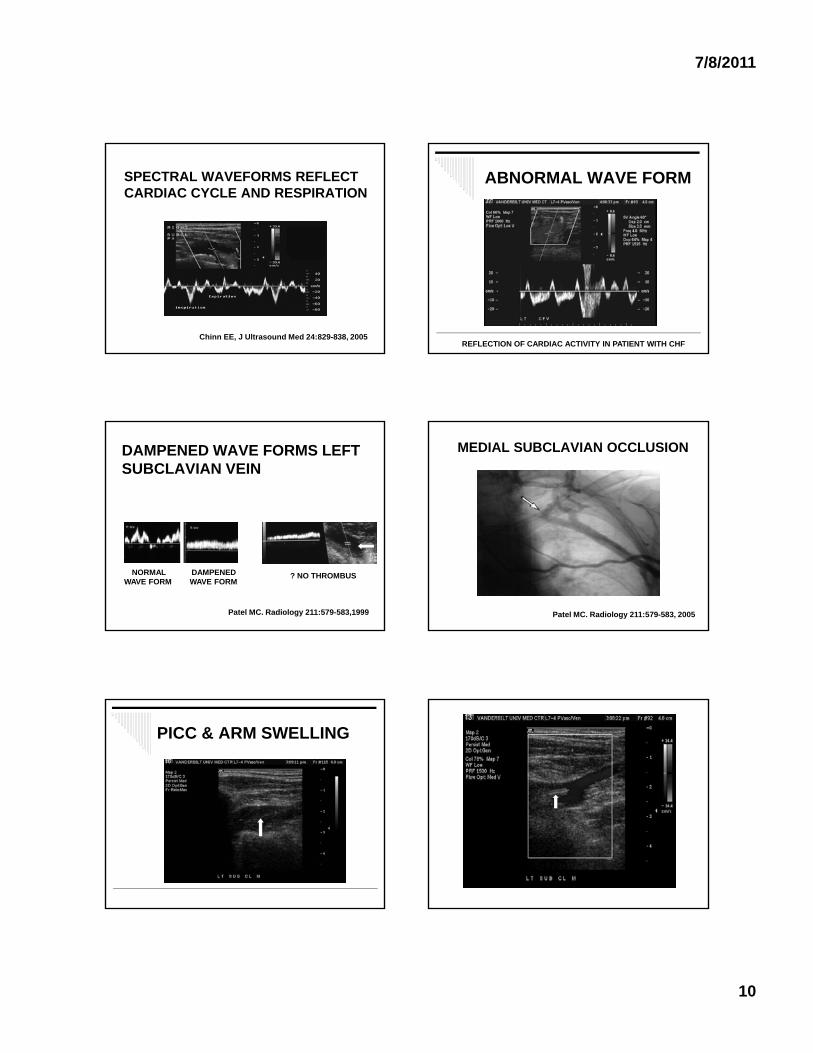
DVT: DUAL-CONTRAST MRI
Li, W et al: Radiology 2007; 242:873-881
UPPER EXTREMITIES UPPER EXTREMITY FACTS
Prevalence of upper extremity DVT is increasing due to increase use of indwelling catheters
28-61% of UEDVT had indwelling catheter 23% thrombosis rate with PICC placement Pulmonary embolism present in up to 33% of
patients with UEDVT (rarely fatal)UEDVT common in patients with cancer (40%),
2X as frequent as in patients with catheters
ADDITIONAL FACTS
Other causes of UEDVT include “effort thrombosis” (Paget-Schroetter syndrome)
Clinical features are nonspecific (swelling, discoloration pain and tenderness)discoloration, pain, and tenderness)
Color Doppler sonogaphy is the modality of choice for evaluation of UEDVT
Sensitivity ranges from 78%-100% and specificity 82%-100%
False positive studies are rare
TECHNIQUE
Routine examination includes: internal jugular, brachiocephalic,subclavian, axillary, brachial, & basilic veins as well as contralateral internal jugular veinas contralateral internal jugular vein
Use compression on all accessible veins as well as color Doppler and spectral analysis
Use 5-7.5 MHz linear array transducer (?curved in axilla)
7/8/2011
10
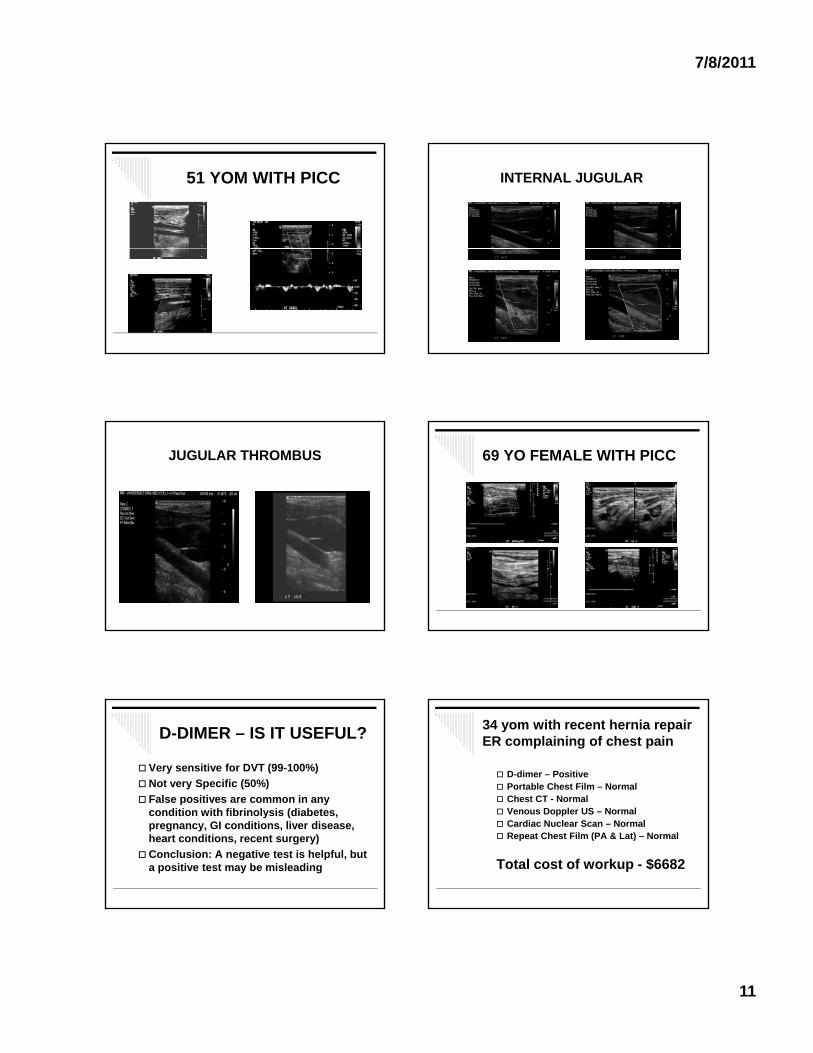
SPECTRAL WAVEFORMS REFLECT CARDIAC CYCLE AND RESPIRATION
Chinn EE, J Ultrasound Med 24:829-838, 2005
ABNORMAL WAVE FORM
REFLECTION OF CARDIAC ACTIVITY IN PATIENT WITH CHF
DAMPENED WAVE FORMS LEFT SUBCLAVIAN VEIN
DAMPENED WAVE FORM
NORMALWAVE FORM
? NO THROMBUS
Patel MC. Radiology 211:579-583,1999
MEDIAL SUBCLAVIAN OCCLUSION
Patel MC. Radiology 211:579-583, 2005
PICC & ARM SWELLING
7/8/2011
11
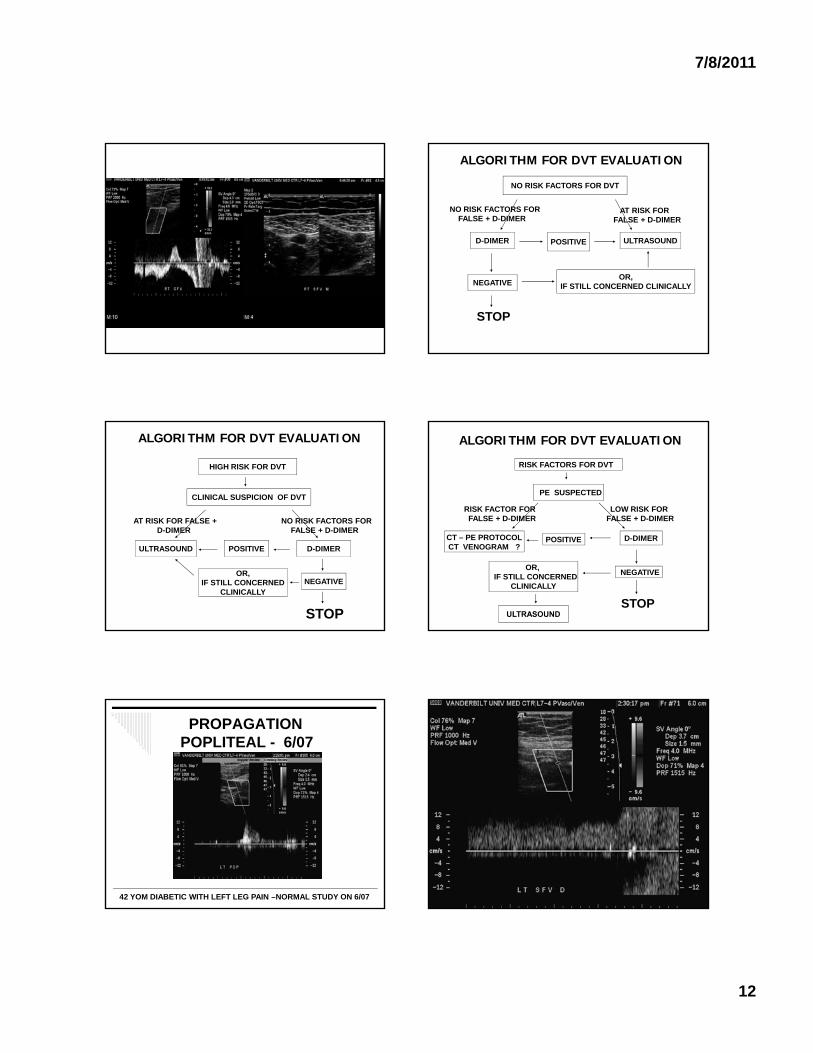
51 YOM WITH PICC INTERNAL JUGULAR
JUGULAR THROMBUS 69 YO FEMALE WITH PICC
D-DIMER – IS IT USEFUL?
Very sensitive for DVT (99-100%)
Not very Specific (50%)
False positives are common in any p ycondition with fibrinolysis (diabetes, pregnancy, GI conditions, liver disease, heart conditions, recent surgery)
Conclusion: A negative test is helpful, but a positive test may be misleading
34 yom with recent hernia repairER complaining of chest pain
D-dimer – Positive Portable Chest Film – Normal Chest CT - Normal Venous Doppler US – Normal Cardiac Nuclear Scan – Normal Repeat Chest Film (PA & Lat) – Normal
Total cost of workup - $6682
7/8/2011
12
ALGORITHM FOR DVT EVALUATION
NO RISK FACTORS FOR DVT
NO RISK FACTORS FORFALSE + D-DIMER
D-DIMER
AT RISK FOR FALSE + D-DIMER
ULTRASOUNDPOSITIVE
NEGATIVE
STOP
OR,IF STILL CONCERNED CLINICALLY
ALGORITHM FOR DVT EVALUATION
HIGH RISK FOR DVT
CLINICAL SUSPICION OF DVT
AT RISK FOR FALSE + NO RISK FACTORS FORD-DIMER
ULTRASOUND
FALSE + D-DIMER
D-DIMERPOSITIVE
NEGATIVEOR,
IF STILL CONCERNEDCLINICALLY
STOP
ALGORITHM FOR DVT EVALUATION
RISK FACTORS FOR DVT
RISK FACTOR FOR FALSE + D-DIMER
PE SUSPECTED
LOW RISK FOR FALSE + D-DIMER
CT – PE PROTOCOLCT VENOGRAM ?
POSITIVE
NEGATIVEOR,
IF STILL CONCERNEDCLINICALLY
D-DIMER
STOP
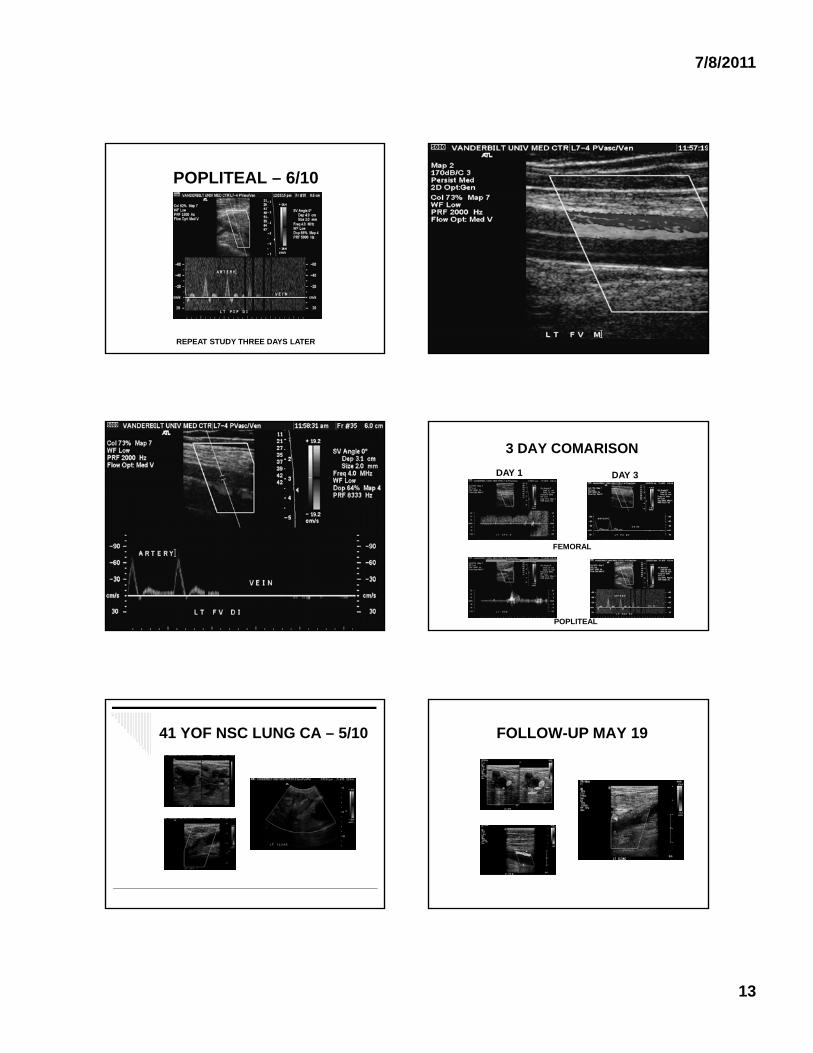
PROPAGATION POPLITEAL - 6/07
42 YOM DIABETIC WITH LEFT LEG PAIN –NORMAL STUDY ON 6/07
7/8/2011
13
POPLITEAL – 6/10
REPEAT STUDY THREE DAYS LATER
3 DAY COMARISON
DAY 1 DAY 3
FEMORAL
POPLITEAL
41 YOF NSC LUNG CA – 5/10 FOLLOW-UP MAY 19
7/8/2011
14
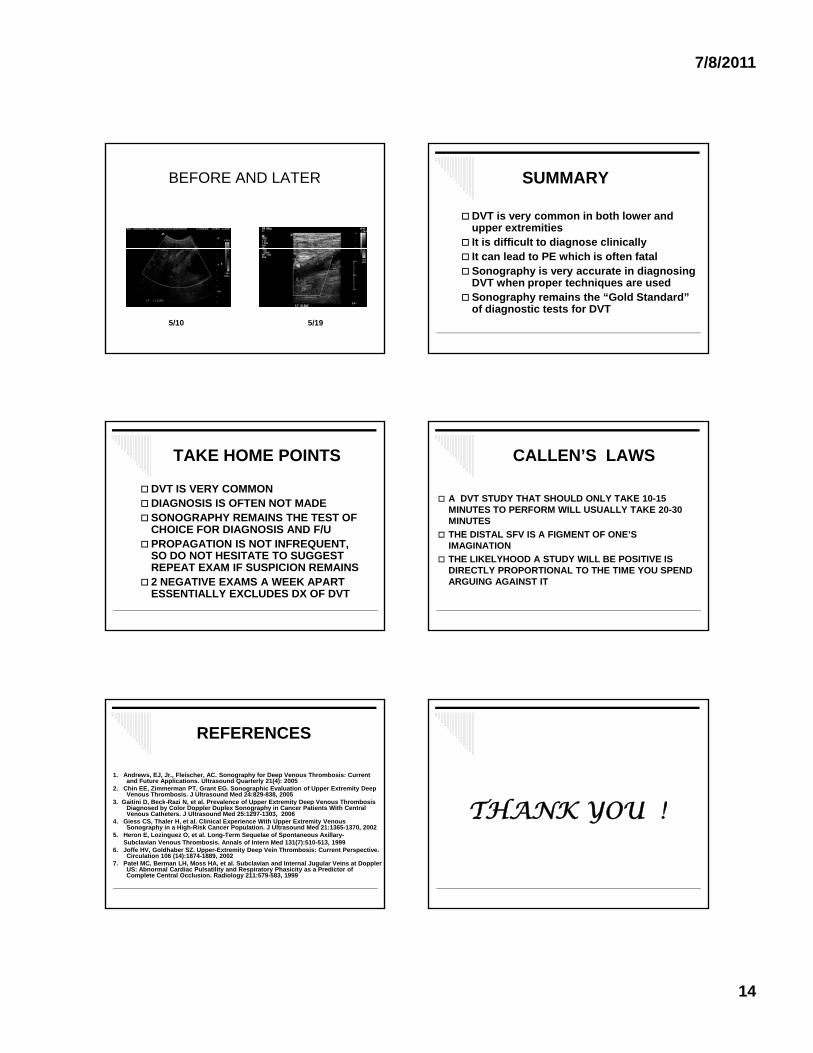
BEFORE AND LATER
5/10 5/19
SUMMARY
DVT is very common in both lower and upper extremities
It is difficult to diagnose clinically It can lead to PE which is often fatal Sonography is very accurate in diagnosing
DVT when proper techniques are used Sonography remains the “Gold Standard”
of diagnostic tests for DVT
TAKE HOME POINTS
DVT IS VERY COMMON DIAGNOSIS IS OFTEN NOT MADE SONOGRAPHY REMAINS THE TEST OF
CHOICE FOR DIAGNOSIS AND F/UCHOICE FOR DIAGNOSIS AND F/U PROPAGATION IS NOT INFREQUENT,
SO DO NOT HESITATE TO SUGGEST REPEAT EXAM IF SUSPICION REMAINS
2 NEGATIVE EXAMS A WEEK APART ESSENTIALLY EXCLUDES DX OF DVT
CALLEN’S LAWS
A DVT STUDY THAT SHOULD ONLY TAKE 10-15 MINUTES TO PERFORM WILL USUALLY TAKE 20-30 MINUTES
THE DISTAL SFV IS A FIGMENT OF ONE’S IMAGINATION
THE LIKELYHOOD A STUDY WILL BE POSITIVE IS DIRECTLY PROPORTIONAL TO THE TIME YOU SPEND ARGUING AGAINST IT
REFERENCES
1. Andrews, EJ, Jr., Fleischer, AC. Sonography for Deep Venous Thrombosis: Current and Future Applications. Ultrasound Quarterly 21(4): 2005
2. Chin EE, Zimmerman PT, Grant EG. Sonographic Evaluation of Upper Extremity Deep Venous Thrombosis. J Ultrasound Med 24:829-838, 2005
3. Gaitini D, Beck-Razi N, et al. Prevalence of Upper Extremity Deep Venous Thrombosis3. Gaitini D, Beck Razi N, et al. Prevalence of Upper Extremity Deep Venous Thrombosis Diagnosed by Color Doppler Duplex Sonography in Cancer Patients With Central Venous Catheters. J Ultrasound Med 25:1297-1303, 2006
4. Giess CS, Thaler H, et al. Clinical Experience With Upper Extremity Venous Sonography in a High-Risk Cancer Population. J Ultrasound Med 21:1365-1370, 2002
5. Heron E, Lozinguez O, et al. Long-Term Sequelae of Spontaneous Axillary-Subclavian Venous Thrombosis. Annals of Intern Med 131(7):510-513, 1999
6. Joffe HV, Goldhaber SZ. Upper-Extremity Deep Vein Thrombosis: Current Perspective. Circulation 106 (14):1874-1889, 2002
7. Patel MC, Berman LH, Moss HA, et al. Subclavian and Internal Jugular Veins at Doppler US: Abnormal Cardiac Pulsatility and Respiratory Phasicity as a Predictor of Complete Central Occlusion. Radiology 211:579-583, 1999
THANK YOU !THANK YOU !