Embed Size (px)
Citation preview

VENOUS AIR EMBOLISMVENOUS AIR EMBOLISM
BYBY
DRDR. . EILIA MELIKAEILIA MELIKA
ANESTHESIOLOGISTANESTHESIOLOGIST
TAYMA GENERAL HOSPITALTAYMA GENERAL HOSPITAL

TYPES OF VAETYPES OF VAE Gas embolism(air,CO2,N2O)Gas embolism(air,CO2,N2O)
a)a) CO2,N2O embolism CO2,N2O embolism → insufflation procedures(laparoscopy→ insufflation procedures(laparoscopy, , hysteroscopy , hysteroscopy , arthroscopy)arthroscopy)
b)b) air embolismair embolism→ → head & neck , orthopedic , chest surgeries + intravascular head & neck , orthopedic , chest surgeries + intravascular cannulas + epidural injectioncannulas + epidural injection
• Fat embolism Fat embolism →→orthopedic surgeryorthopedic surgery• Venous thrombo embolism Venous thrombo embolism → surgical manipulation in the pelvis→ surgical manipulation in the pelvis• Tumor embolismTumor embolism• Amniotic fluid embolismAmniotic fluid embolism

Brief notes on venous air embolismBrief notes on venous air embolism
Pathophysiology.Pathophysiology.
Volume of entrained airVolume of entrained air
Rate of accumulation.Rate of accumulation.
Position of the patientPosition of the patient
Height of the vein above the right heartHeight of the vein above the right heart

Critical volume of airCritical volume of air
200-300 ml or 3-5 ml/kg200-300 ml or 3-5 ml/kg
The closer the vein of entrainment to the The closer the vein of entrainment to the right heart the lower the critical volumeright heart the lower the critical volume

How big a hole ?How big a hole ?
A pressure decrease of 5 cm. H2O across A pressure decrease of 5 cm. H2O across a 14G cannula(1.8 internal diameter) can a 14G cannula(1.8 internal diameter) can entrain 100ml of air/second.entrain 100ml of air/second.

Clinical presentation in Clinical presentation in anesthetized patientsanesthetized patients
TachyarrythmiasTachyarrythmias
Cardiovascular collapseCardiovascular collapse

High risk proceduresHigh risk procedures
Sitting position craniotomySitting position craniotomy Posterior fossa/neck surgery.Posterior fossa/neck surgery. Laparoscopic proceduresLaparoscopic procedures Total hip arthroplasty.Total hip arthroplasty. Cesarean sectionCesarean section Central venous accessCentral venous access

DetectionDetection
Trans-oesophageal echocardiography can Trans-oesophageal echocardiography can detect 0.02ml/kgdetect 0.02ml/kg
Pre-cordial Doppler can detect Pre-cordial Doppler can detect 0.05ml/kg.Confirm position with “Bubble” test.0.05ml/kg.Confirm position with “Bubble” test.
End-tidal nitrogen-0.04% is significantly faster End-tidal nitrogen-0.04% is significantly faster than E-tidal C02 by 30-90 secondsthan E-tidal C02 by 30-90 seconds
End-tidal C02; decrease by 2mm Hg significant?End-tidal C02; decrease by 2mm Hg significant? VigilanceVigilance

Management Management It is better to prevent VAE than to treat itIt is better to prevent VAE than to treat it
A.A. Prevention:Prevention: Aim is to keep small +ve pressure in the Aim is to keep small +ve pressure in the
veins at the operative site by;veins at the operative site by;
1)1) Proper positioning e.g park bench versus Proper positioning e.g park bench versus sitting position for post.F. cran.sitting position for post.F. cran.
2)2) High index of suspicion wherever there is High index of suspicion wherever there is a negative gradient between surgical a negative gradient between surgical field and heart.field and heart.
3)3) Reverse Trendelenberg 5deg. In c.sReverse Trendelenberg 5deg. In c.s

Prevention (contin.)Prevention (contin.)
Avoid N2O as possible as you canAvoid N2O as possible as you can Expansion of the intravascular volumeExpansion of the intravascular volume Controlled ventilation with Controlled ventilation with peep peep
(controversial)(controversial)

Treatment Treatment When VAE is detected or suspected intra When VAE is detected or suspected intra
operativelyoperatively
1.1. Measures to prevent further air entryMeasures to prevent further air entry
2.2. Measures to ↑venous pressure at the Measures to ↑venous pressure at the operative siteoperative site
3.3. Measures to avoid expansion of air bubblesMeasures to avoid expansion of air bubbles
4.4. Aspiration of air bubblesAspiration of air bubbles
5.5. Circulatory supportCirculatory support
6.6. Finally rt. thoracotomyFinally rt. thoracotomy

TreatmentTreatment
Prevent further air entrainmentPrevent further air entrainment 100% oxygen100% oxygen Trendelenberg position/Durant positionTrendelenberg position/Durant position CPR/ inotropes.CPR/ inotropes. Aspiration of air.Aspiration of air.
-Swan Ganz Catheter 6-16%-Swan Ganz Catheter 6-16%
- Multi-orifice Cooke catheter 30-60%- Multi-orifice Cooke catheter 30-60%

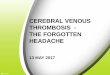
Chest radiograph after central venous cannulation showing a round opacity of homogenous density but without airbronchogram in the right lower lung field.
Ku S et al. Thorax 2007;62:372-372
©2007 by BMJ Publishing Group Ltd and British Thoracic Society

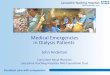
(A) Contrast-enhanced chest CT scan showing air bubble trapped around the central venous catheter in the superior vena cava (arrow).
(B) Bilateral pleural-based, wedge-shaped ,mass-like consolidations with central necrosis in both lower lobes
Ku S et al. Thorax 2007;62:372-372
©2007 by BMJ Publishing Group Ltd and British Thoracic Society

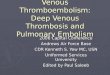
Transoesophageal echocardiogram (bubble study), patent foramen ovale.
Eichhorn V et al. Br. J. Anaesth. 2009;102:717-718
© The Author [2009]. Published by Oxford University Press on behalf of The Board of Directors of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: [email protected]