Embed Size (px)
Citation preview

Archives of Medical Research 42 (2011) 405e411
ORIGINAL ARTICLE
VEGF-C as a Decision-making Biomarker for Selected Patients with InvasiveBladder Cancer Who Underwent Bladder-preserving Radical Surgery
Zhuo Li, Fan Qi, Lin Qi, Huihui Zhang, Minfeng Chen, Long Wang, and Xiongbing Zu
Department of Urology, Xiangya Hospital, Central South University, Changsha city, Hunan province, China
Received for publication March 3, 2011; accepted July 18, 2011 (ARCMED-D-11-00112).
Address reprint re
Xiangya Hospital, Ce
Phone: 86-731-84327
163.com
0188-4409/$ - see frodoi: 10.1016/j.arcm
Background and Aims. We proved the feasibility of radical transurethral resection inselected patients with muscle-invasive bladder cancer with a minimum follow-up ofO5 years. A follow-up schedule was developed based on progression and recurrenceduring this period.
Methods. The study included 93 patients with invasive bladder cancer treated by radicaltransurethral resection. Student t test was used for continuous variables to establishclinical progression predictive factors. VEGF-C protein expressions were tested byimmunohistochemistry postsurgery.
Results. The overall survival and disease-specific survival rates for all 93 patients were59.1% and 65.2%, respectively. The clinical stage of the tumor influenced overall survival( p 5 0.024) and disease-specific survival ( p 5 0.047). A significantly higher overallsurvival and disease-specific survival rate for patients with low levels of VEGF-C was69.6% and 75.0%, respectively, than for those with high levels of VEGF-C (45.9 and54.1%, respectively, p !0.05).The presence of bladder Tis reduced the survival rate(41.2 vs. 65.3%) and disease-specific survival (45.4 vs. 72.1%). Sensitivity, specificityand accuracy of VEGF-C in the evaluation of disease progression were 76.7, 77.8,77.4%, respectively.
Conclusions. Patients with T2 stage, low level of VEGF-C and absence of bladder Tiswere associated with high overall survival and disease-specific survival rate. VEGF-Clevel can evaluate disease progression and assist in choosing the appropriate treat-ment. � 2011 IMSS. Published by Elsevier Inc.
Key Words: Bladder transitional cell carcinoma, Radical transurethral resection, Vascular
endothelial growth factor C, Lymphatic metast asis.Introduction
Radical cystectomy for muscle-invasive transitional cellcarcinoma of the bladder is the recommended treatmentoption according to the European Association of UrologyGuidelines and other evidence-based literature reports (1).However, in several clinical studies radical transurethralresection (TUR) has been shown to control the disease,particularly in patients with lower clinical disease stages(T2-3) (2e4). In selected patients, TUR can achieve
quests to: Dr. Xiongbing Zu, Department of Urology,
ntral South University, Changsha 410008, China;
242; FAX: 86-731-84327242; E-mail: whzuxb@
nt matter. Copyright � 2011 IMSS. Published by Elseviered.2011.07.006
5-year survival rates comparable to those rates achievedwith radical cystectomy (5e6). Herr (7) also reported thatTUR may be sufficient as monotherapy in some selectedpatients from a 10-year outcome.
The question remains how to select patients with muscle-invasive cancer for bladder preservation? Imaging, cystos-copy and biopsy have been relied on for decision making.But we still do not know the malignant potential of tumorcells in patients. There is no established biomarker; hence,several molecular markers are under investigation forpatients with muscle-invasive bladder cancer.
It is well known that vascular endothelial growth factor(VEGF) is essential in vasculogenesis and angiogenesis.VEGF-C, a member of the VEGF family, induces lym-phatic endothelial proliferation and vessel enlargement
Inc.

406 Li et al./ Archives of Medical Research 42 (2011) 405e411
and facilitates nodal metastasis (8). Overexpression ofVEGF-C in tumors has been shown to be closely relatedto the presence of lymphatic invasion and lymph nodemetastasis (9). Our previous study also demonstrated thatVEGF-C expression is associated with tumor size, patho-logical T stage, pathological grade, lymphatic-venousinvolvement and pelvic lymph node metastasis of bladdercancer (10). Therefore, VEGF-C expression may be usedto evaluate the malignant potential of tumor cells and helpus in decision-making for patients with muscle-invasivebladder cancer for bladder preservation.
We analyzed the outcome of a prospective series of93 patients with muscle-invasive bladder cancer undergoingradical TUR with a minimum follow-up of O5 years. Wealso evaluated the relationship between expressions ofVEGF-C and survival rate and present our experience inthis selected population. We report on factors that maypredict treatment response and risk of relapse.
Materials and Methods
Patients and Samples
The study included 112 patients and was performed from1998e2006 to evaluate the feasibility of radical TUR forthe treatment of selected patients with muscle-invasivebladder cancer. All patients were informed that the standardtreatment is radical cystectomy and that the efficacy ofbladder preservation therapy is currently under investiga-tion. Patients chose the treatment to preserve their ownbladder function. Inclusion criteria for this study werehistological confirmation of muscular infiltration. Whenthe muscularis propria was macroscopically completelycleaned of tumor, three or more biopsies were takenin the areas of the depth and periphery of the tumor bed.Biopsies always included the muscular layer and, in mostcases, perivesical fat. Among patients who underwentcomplete TUR, those with negative biopsies of the musclelayer of the tumor bed were included in an observation groupand those with positive biopsies were enrolled in a radicaltreatment group. Exclusion criteria were as follows: patientswith macroscopically residual tumor after TUR or withhydronephrosis and those with lymph node involvement orwith distant metastases or pathological examinationconfirmed on T4 were also excluded from the trial. However,patients with Tis bladder tumor and multifocal tumors wereincluded in the study.
Finally, 93 patients were chosen for the study and19 patients were excluded for positive biopsies or T4. Themedian (range) age of the patients at the time of treatmentwas 67 years (39e88 years). Histological cell types of thetumors were assigned according to the WHO classification:42 as grade II and 51 as grade III. Staging was reviewedbased on the UICC-TNM staging system: 65 tumors werestage T2 and 28 were T3.
Immunohistochemical Staining for VEGF-C
After surgery, each specimen was fixed in 10% formal-dehyde solution for histopathological examination. Forimmunohistochemical staining for VEGF-C protein,sections of formalin-fixed paraffin-embedded tissues werecut with a microtome and dried overnight at 37�C ona silanized slide. Samples were deparaffinized in xyleneat room temperature for 80 min and washed with a gradedethanol/water mixture and then with distilled water. Thesamples for VEGF-C antigen were soaked in citrate buffer(10 mM citrate), microwaved for 10 min and then treatedwith 3% H2O2 in PBS at room temperature for 20 min. Theprotocol for the LSAB2 kit with peroxidase (Dako,Copenhagen, Denmark) was followed for each sampleexcept for the incubation condition for the first antibody.Goat anti-human VEGF-C (200 mg/mL, Santa CruzBiotechnology, Santa Cruz, CA) was used at a dilutionof 1:50 as the first antibody with incubation at 4�C over-night. Addition of the first antibody, goat anti-humanVEGF-C, was omitted in the protocols for negativecontrols of VEGF-C.
Under low-power microscopy field, each slide was eval-uated randomly in 10 different areas containing tumor cellsby two independent investigators unaware of the clinico-pathological data (11); $100 tumor cells were examinedper field. Two scoring systems, staining intensity andpercentage of stained cells were included. Staining intensitywas scored on a semiquantitative 4-point scale as follows:0, equivalent to the negative control; 1, weak cytoplasmicstain slightly darker than the negative control; 2, moderatestain, defined as an intensity of score 1e3; 3, intense stain,equivalent to or darker than the positive control. Thepercentage of stained cells was also scored on a semiquan-titative 4-point scale as follows: 0, !10%; 1, 10e25%; 2,25e50%; 3, O50%. Then, combining the score of stainingintensity and percentage of stained cells, a score of 0e1was I, 2 was II, 3e4 was III and 5e6 was IV.
Follow-up Schedule
Patients in this trial followed a strict surveillance program.They were first evaluated at 3 months after TUR. After-ward, these patients were evaluated every 3 months for2 years, then every 6 months for 3 more years and annuallythereafter. At each evaluation, cystoscopy, urinary cytology,random bladder mucosa biopsies and computerized tomog-raphy or magnetic resonance imaging and chest x-ray weredone. Blood analyses were also performed for symptomaticpatients. Recurrence was defined as superficial bladdertumor or upper urinary tract or prostatic involvementlimited to the mucosa after radical transurethral resection.Progression was considered when invasive bladder tumoror lymph node metastasis or stromal prostatic involvementwas observed, when bladder carcinoma in situ requiredcystectomy or when metastases developed.

407VEGF-C in Muscle-invasive Bladder Cancer
Treatment after Surgery
Pirarubicin (THP) was scheduled for patients after TURat a dose of 30 mg as the intravesical treatment. Patientsreceived the treatment 24 h after surgery and every 1 weekfor 4e8 weeks and every 1 month for the next 6e12months. Patients with bladder Tis were treated with intra-vesical bacillus Calmette-Guerin (BCG) and those withrecurrence of high-risk non-muscle-invasive bladder tumorswere treated with reTUR. Patients with local progressionwere treated with radical cystectomy or radio/chemo-therapy according to performance status and patient deci-sion, whereas those with distant metastasis or with poorperformance status received systemic radio/chemotherapyor palliative approaches.
Statistical Analysis
Overall and disease-specific survival intervals were calcu-lated from the day of the first TUR to the time of death orthe last follow-up examination, and death or disease-related death as an event. These rates were calculated usingthe Kaplan-Meier method. Two-tailed c2 test was used todetermine statistical significance between proportions andStudent t test was used for continuous variables. The levelof significance was 0.05 in all statistical testing. Severalfactors were tested for predictive and prognostic impact onprogression and survival including age, gender, presence ofbladder Tis, number, size, grade and T category. Statisticalanalysis was performed using SPSS for Windows v.13.0.
Results
Patient Characteristics and Follow-up
Table 1 shows patient characteristics in this series. Witha minimum follow-up of O5 years and a mean of44.3 months (range 4e96 months), 38 patients (40.9%)
Table 1. Patient characteristics
Number of patients 93
Mean age, years (range) 67 (39e88)
Mean size, cm (range) 3.8 (1e12)
Number by gender (%)
Male 82 (88.2)
Female 11 (11.8)
No. grade (%)
2 42 (45.2)
3 51 (54.8)
Clinical tumor classification (%)
T2 65 (69.9)
T3 28 (30.1)
Number Ca in situ (%) 20 (21.5)
Number tumors (%)
Solitary 81 (87.1)
Multiple 12 (12.9)
never had disease relapse, 25 patients (26.9%) had diseaserecurrence and 30 patients (32.3%) had disease progression(Table 2). Of the patients with disease recurrence, 23 weretreated with reTUR once, two patients were treated withreTUR twice. All had bladder preservation and had noevidence of tumor recurrence after reTUR until the endof the study.
Of the patients with disease progression, 13 weretreated with radical cystectomy, 10 patients receivedradio/chemotherapy because they refused or were not suit-able for radical cystectomy and seven patients receivedonly palliative therapy because of poor performance status.Of these 30 patients, 18 (60.0%) died as a result of thetumor, including two (15.4%), nine (90%), seven (100%)after radical cystectomy, radio/chemotherapy, or palliativetherapy, respectively.
VEGF-C Levels in Patients
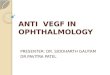
All samples were classified into two groups according tothe score of VEGF-C levels: VEGF-C (I, II) were lowexpression group and VEGF-C (I, II) were high expressiongroup. The frequency of detectable VEGF-C in diseaseprogression was markedly higher than that in disease recur-rence or no recurrence of bladder tissue ( p !0.05). Therewere 23 patients with VEGF-C (III, IV) and diseaseprogression, 14 patients with VEGF-C (III, IV) and diseaserecurrence or no recurrence, 49 patients with VEGF-C(I, II) and disease recurrence or no recurrence, seven patientswith VEGF-C (I, II) and disease progression. (Table 3).Sensitivity, specificity and accuracy of VEGF-C in the eval-uation of disease progression were 76.7%, 77.8%, and77.4%, respectively. In the progression group, therewere fivepatients with lymph node metastasis, and they were allVEGF-C IV.
Predictive Factors for Survival
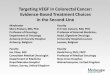
The actuarial overall survival and disease-specific survivalrates for all 93 patients and for some clinically importantsubgroups are shown in Table 4. In the univariate analysis,the clinical stage of the tumor (Figure 1) significantly influ-enced overall survival ( p 5 0.024) and disease-specificsurvival ( p 5 0.047). We also found a significantly higher
Table 2. Follow-up of entire series
No. of patients (%)
No recurrence 38 (40.9)
Recurrence
Superficial bladder cancer (T1, Tis) 24 (25.8)
Upper urinary tract or prostate involvement
limited to the mucosa
1 (1.1)
Progression
T O2, M0 25 (26.9)
Lymph node metastasis 5 (5.4)
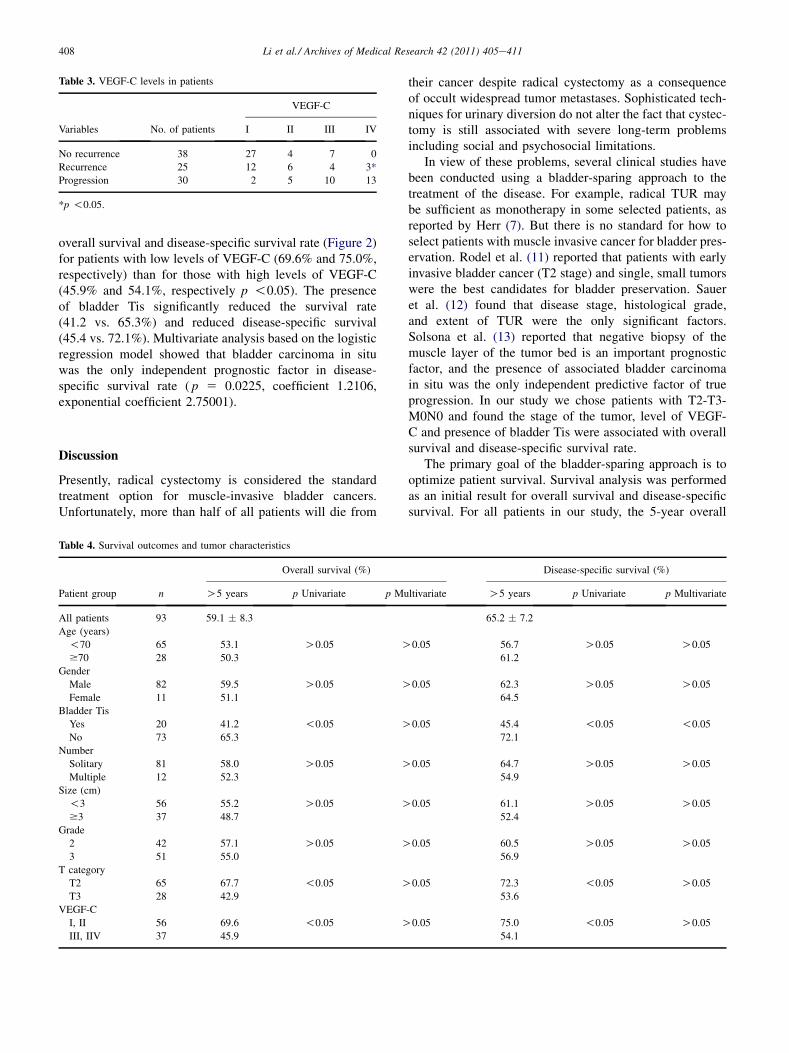
Table 3. VEGF-C levels in patients
Variables No. of patients
VEGF-C
I II III IV
No recurrence 38 27 4 7 0
Recurrence 25 12 6 4 3*
Progression 30 2 5 10 13
*p !0.05.
408 Li et al./ Archives of Medical Research 42 (2011) 405e411
overall survival and disease-specific survival rate (Figure 2)for patients with low levels of VEGF-C (69.6% and 75.0%,respectively) than for those with high levels of VEGF-C(45.9% and 54.1%, respectively p !0.05). The presenceof bladder Tis significantly reduced the survival rate(41.2 vs. 65.3%) and reduced disease-specific survival(45.4 vs. 72.1%). Multivariate analysis based on the logisticregression model showed that bladder carcinoma in situwas the only independent prognostic factor in disease-specific survival rate ( p 5 0.0225, coefficient 1.2106,exponential coefficient 2.75001).
Discussion
Presently, radical cystectomy is considered the standardtreatment option for muscle-invasive bladder cancers.Unfortunately, more than half of all patients will die from
Table 4. Survival outcomes and tumor characteristics
Patient group n
Overall survival (%)
O5 years p Univariate p Mu
All patients 93 59.1 � 8.3
Age (years)
!70 65 53.1 O0.05 O$70 28 50.3
Gender
Male 82 59.5 O0.05 OFemale 11 51.1
Bladder Tis
Yes 20 41.2 !0.05 ONo 73 65.3
Number
Solitary 81 58.0 O0.05 OMultiple 12 52.3
Size (cm)
!3 56 55.2 O0.05 O$3 37 48.7
Grade
2 42 57.1 O0.05 O3 51 55.0
T category
T2 65 67.7 !0.05 OT3 28 42.9
VEGF-C
I, II 56 69.6 !0.05 OIII, IIV 37 45.9
their cancer despite radical cystectomy as a consequenceof occult widespread tumor metastases. Sophisticated tech-niques for urinary diversion do not alter the fact that cystec-tomy is still associated with severe long-term problemsincluding social and psychosocial limitations.
In view of these problems, several clinical studies havebeen conducted using a bladder-sparing approach to thetreatment of the disease. For example, radical TUR maybe sufficient as monotherapy in some selected patients, asreported by Herr (7). But there is no standard for how toselect patients with muscle invasive cancer for bladder pres-ervation. Rodel et al. (11) reported that patients with earlyinvasive bladder cancer (T2 stage) and single, small tumorswere the best candidates for bladder preservation. Saueret al. (12) found that disease stage, histological grade,and extent of TUR were the only significant factors.Solsona et al. (13) reported that negative biopsy of themuscle layer of the tumor bed is an important prognosticfactor, and the presence of associated bladder carcinomain situ was the only independent predictive factor of trueprogression. In our study we chose patients with T2-T3-M0N0 and found the stage of the tumor, level of VEGF-C and presence of bladder Tis were associated with overallsurvival and disease-specific survival rate.
The primary goal of the bladder-sparing approach is tooptimize patient survival. Survival analysis was performedas an initial result for overall survival and disease-specificsurvival. For all patients in our study, the 5-year overall
Disease-specific survival (%)
ltivariate O5 years p Univariate p Multivariate
65.2 � 7.2
0.05 56.7 O0.05 O0.05
61.2
0.05 62.3 O0.05 O0.05
64.5
0.05 45.4 !0.05 !0.05
72.1
0.05 64.7 O0.05 O0.05
54.9
0.05 61.1 O0.05 O0.05
52.4
0.05 60.5 O0.05 O0.05
56.9
0.05 72.3 !0.05 O0.05
53.6
0.05 75.0 !0.05 O0.05
54.1
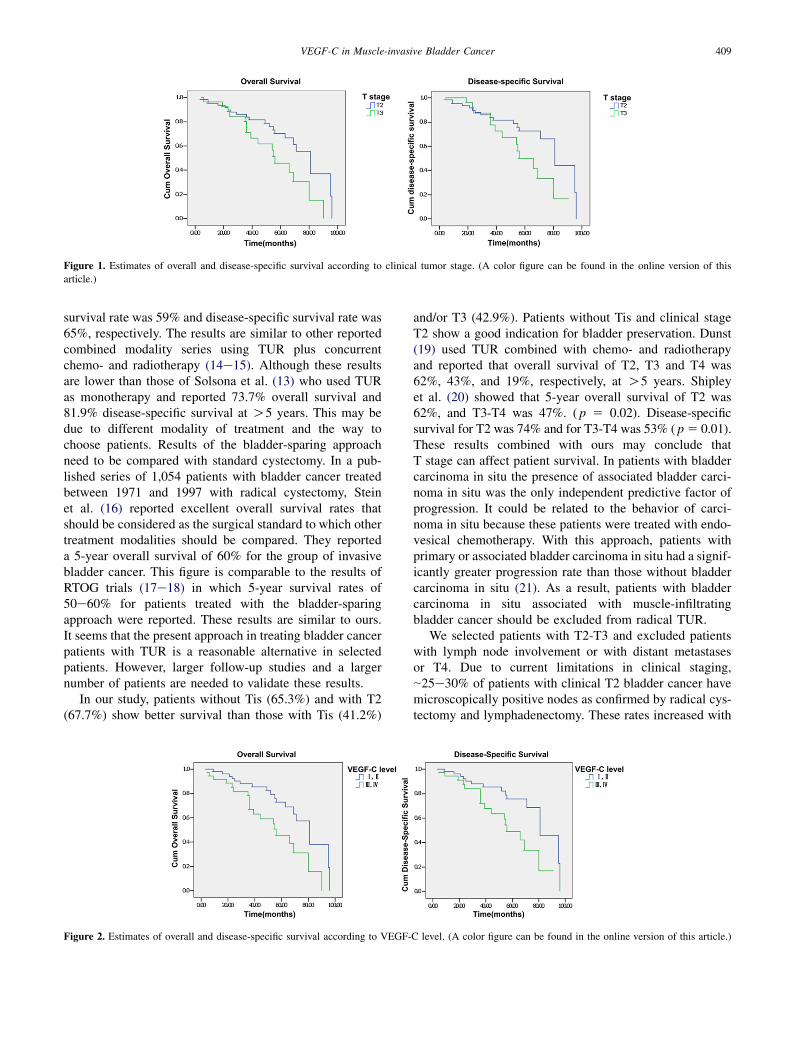
Figure 1. Estimates of overall and disease-specific survival according to clinical tumor stage. (A color figure can be found in the online version of this
article.)
409VEGF-C in Muscle-invasive Bladder Cancer
survival rate was 59% and disease-specific survival rate was65%, respectively. The results are similar to other reportedcombined modality series using TUR plus concurrentchemo- and radiotherapy (14e15). Although these resultsare lower than those of Solsona et al. (13) who used TURas monotherapy and reported 73.7% overall survival and81.9% disease-specific survival at O5 years. This may bedue to different modality of treatment and the way tochoose patients. Results of the bladder-sparing approachneed to be compared with standard cystectomy. In a pub-lished series of 1,054 patients with bladder cancer treatedbetween 1971 and 1997 with radical cystectomy, Steinet al. (16) reported excellent overall survival rates thatshould be considered as the surgical standard to which othertreatment modalities should be compared. They reporteda 5-year overall survival of 60% for the group of invasivebladder cancer. This figure is comparable to the results ofRTOG trials (17e18) in which 5-year survival rates of50e60% for patients treated with the bladder-sparingapproach were reported. These results are similar to ours.It seems that the present approach in treating bladder cancerpatients with TUR is a reasonable alternative in selectedpatients. However, larger follow-up studies and a largernumber of patients are needed to validate these results.
In our study, patients without Tis (65.3%) and with T2(67.7%) show better survival than those with Tis (41.2%)
Figure 2. Estimates of overall and disease-specific survival according to VEGF-
and/or T3 (42.9%). Patients without Tis and clinical stageT2 show a good indication for bladder preservation. Dunst(19) used TUR combined with chemo- and radiotherapyand reported that overall survival of T2, T3 and T4 was62%, 43%, and 19%, respectively, at O5 years. Shipleyet al. (20) showed that 5-year overall survival of T2 was62%, and T3-T4 was 47%. ( p 5 0.02). Disease-specificsurvival for T2 was 74% and for T3-T4 was 53% ( p5 0.01).These results combined with ours may conclude thatT stage can affect patient survival. In patients with bladdercarcinoma in situ the presence of associated bladder carci-noma in situ was the only independent predictive factor ofprogression. It could be related to the behavior of carci-noma in situ because these patients were treated with endo-vesical chemotherapy. With this approach, patients withprimary or associated bladder carcinoma in situ had a signif-icantly greater progression rate than those without bladdercarcinoma in situ (21). As a result, patients with bladdercarcinoma in situ associated with muscle-infiltratingbladder cancer should be excluded from radical TUR.
We selected patients with T2-T3 and excluded patientswith lymph node involvement or with distant metastasesor T4. Due to current limitations in clinical staging,|25e30% of patients with clinical T2 bladder cancer havemicroscopically positive nodes as confirmed by radical cys-tectomy and lymphadenectomy. These rates increased with
C level. (A color figure can be found in the online version of this article.)

410 Li et al./ Archives of Medical Research 42 (2011) 405e411
higher T stage. This observation has been confirmed bymany studies. Vieweg et al. (22) reported on a contemporarycystectomy series in which nodal metastases were seen in9% of patients (12/121) with T2 tumors vs. 37% (119/321)with T3 cancers. TUR does not provide the opportunity forpathological staging of lymph nodes. Computerized tomog-raphy lacks sensitivity and specificity for pelvic lymph nodemetastasis. Death due to bladder cancer is invariably due tometastatic disease and understaging of the primary tumor.Failure to accurately stage pelvic lymph nodes will inevi-tably result in progression and metastases. We encourageinvestigation of molecular markers to further stratify patientsinto high- and low-risk groups for local recurrence andprogression with systemic metastatic disease.
Several studies have correlated elevated VEGF levelexpression with disease recurrence or progression, oftenas an independent predictor by multivariate analysis (23).Since 1996, VEGF-C has been described as a relativelyspecific growth factor for the lymphatic vascular system.The present data are compatible with reports of a positivecorrelation between VEGF-C expression and lymphaticinvasion in patients with breast cancer, gastric cancer andcervical cancer (24e27). These findings indicate thatVEGF-C expression is implicated in lymphatic invasionand lymph node metastasis. In our previous study, we foundthat the frequency of detectable VEGF-C expression ofbladder tumor was significantly higher than in normalbladder tissue. These findings are consistent with otherreports showing high VEGF-C expression in tumor tissuesin contrast to the low levels in normal tissues (28,29). Wealso found that VEGF-C expression was associated withtumor size, tumor grade, tumor stage, lymph node involve-ment and lymph node metastasis ( p !0.01). Logisticregression analysis showed that the high VEGF-C expres-sion was the exclusive independent factor influencingpelvic lymph node metastasis in bladder tumors.
In our present study, as to evaluating disease progressionof bladder tumor using VEGF-C, there were 30 cases ofprogression for bladder tumor, and this was due to highVEGF-C expression in 23 cases. In 56 cases there waslow VEGF-C expression; seven of these cases showedprogression for bladder tumor. Sensitivity, specificity andaccuracy of VEGF-C in the evaluation of disease progres-sion were 76.7%, 77.8%, and 77.4%, respectively. Therewere five patients with lymph node metastasis, and theywere all identified with VEGF-C IV. We also found a signif-icantly higher overall survival and disease-specific survivalrate for patients with low levels of VEGF-C (69.6% and75.0%, respectively) than for those with high levels ofVEGF-C (45.9% and 54.1%, respectively, p 5 0.013).The present study indicates that patients with highVEGF-C expression have poorer prognoses than those withno or low VEGF-C expression. VEGF-C expression, whichis strongly correlated with pelvic lymph node metastasis,may affect prognosis. We may conclude that VEGF-C
could be a potential clinical application as a marker forevaluating disease progression of muscle-invasive bladdercancer. Moreover, it may aid us in decision-making inregard to bladder preservation.
As a biomarker, VEGF-C can be detected before andafter surgery. Comparing with T-stage, VEGF-C can bemore quantitative. In our study we divided the level ofVEGF-C into four grades, as a score of 0e1 was I, 2 wasII, 3e4 was III and 5e6 was IV. The prognosis becomespoorer with higher grades. In fact, it can be more quantita-tive as the study continues. Testing method of VEGF-C isvery simple and will enrich the predictive tools of bladdercarcinoma prognosis.
In conclusion, our results show that patients with T2tumor stage, low level of VEGF-C and absence of bladderTis were associated with high overall survival and disease-specific survival rate. VEGF-C level as a marker can eval-uate disease progression of muscle-invasive bladder cancerand aid in the selection of the appropriate treatment.
AcknowledgmentThis research was supported by National Natural ScienceFoundation of China (No. 30700832).
Conflict of Interest
None declared.
References1. Stenzl A, Cowan NC, De Santis M, et al. Treatment of muscle-invasive
and metastatic bladder cancer: update of the EAU guidelines. Eur Urol
2011;59:1009e1018.
2. Barnee RW, Dick AL, Hadley HL, et al. Survival following transure-
thral resection of bladder carcinoma. Cancer Res 1997;37:2895e2897.
3. Henry K, Miller J, Mori M, et al. Comparison of transurethral resection to
radical therapies for stage B bladder tumors. J Urol 1988;140:964e967.
4. O’Flynn JD, Smith JD, Hanson JS, et al. Transurethral resection for
the assessment and treatment of vesical neoplasms: a review of
840 consecutive cases. Eur Urol 1975;1:38e40.
5. Herr HW. Conservative management of muscle-infiltrating bladder
cancer: prospective experience. J Urol 1987;138:1162e1163.6. Solsona E, Iborra I, Collado A, et al. Feasibility of radical transure-
thral resection as monotherapy for selected patients with muscle
invasive bladder cancer. J Urol 2010;184:475e481.
7. Herr HW. Transurethral resection of muscle-invasive bladder cancer:
10-year outcome. J Clin Oncol 2001;19:89e93.
8. Kukk E, Lymboussaki A, Taira S, et al. VEGF-C receptor binding and
pattern of expression with VEGFR-3 suggests a role in lymphatic
vascular development. Development 1996;122:3829e3837.9. Ueda M, Terai Y, Yamashita Y, et al. Correlation between vascular
endothelial growth factor-C expression and invasion phenotype in
cervical carcinomas. Int J Cancer 2002;98:335e343.10. Zu XB, Tang ZY, Li Y, et al. Vascular endothelial growth factor-C
(VEGF-C) expression in bladder transitional cell cancer and its rela-
tionship to lymph node metastasis. BJU Int 2006;98:1090e1093.
11. Rodel C, Grabenbauer GG, Kuhn R, et al. Combined-modality treat-
ment and selective organ preservation in invasive bladder cancer:
long-term results. J Clin Oncol 2002;20:3061e3071.

411VEGF-C in Muscle-invasive Bladder Cancer
12. Sauer R, Birkenhake S, Kuhn R, et al. Efficacy of radio-chemotherapy
with platin derivatives compared to radiotherapy alone in organ-
sparing treatment of bladder cancer. Int J Radiat Oncol Biol Phys
1998;40:121e127.
13. Solsona E, Iborra I, Ricos JV, et al. Feasibility of transurethral resec-
tion for muscle-infiltrating carcinoma of the bladder: long-term
follow-up of a prospective study. J Urol 1998;159:95e99.
14. Tester W, Porter A, Heaney J, et al. Neoadjuvant combined modality
therapy with possible organ preservation for invasive bladder cancer.
J Clin Oncol 1996;14:119e126.
15. Housset M, Maulard C, Chretien YC, et al. Combined radiation and
chemotherapy for invasive transitional cell carcinoma of the bladder:
a prospective study. J Clin Oncol 1993;11:2150e2157.16. Stein JP, Lieskovsky G, Cote R, et al. Radical cystectomy in the treat-
ment of invasive bladder cancer: long-term results in 1,054 patients.
J Clin Oncol 2001;19:666e675.
17. Shipley WU, Kaufman DS, Tester WJ, et al. Overview of bladder
cancer trials in the Radiation Therapy Oncology Group. Cancer
2003;97:2115e2119.
18. Shipley WU, Winter KA, Kaufman DS, et al. Phase III trial of neoad-
juvant chemotherapy in patients with invasive bladder cancer treated
with selective bladder preservation by combined radiation therapy
and chemotherapy: initial results of Radiation Therapy Oncology
Group 89e03. J Clin Oncol 1998;16:3576e3583.19. Dunst J, Diestelhomt A, Kohn R, et al. Organ-sparing treatment in
muscle-invasive bladder cancer. Strahlenther Onkol 2005;181:
632e637.
20. Shipley WU, Kaufman DS, Zehr E, et al. Selective bladder preserva-
tion by combined modal protocol treatment: long-term outcomes of
190 patients with invasive bladder cancer. Urology 2002;60:62e67.
21. Solsona E, Iborra I, Rids JV, et al. Carcinoma in situ associated with
superficial bladder tumor. Eur Urol 1991;19:93e96.22. Vieweg J, Gschwend J, Herr HW, et al. The impact of pelvic lympha-
denectomy and radical cystectomy on outcome in lymph node positive
bladder cancer. J Urol 1999;161:72e76.
23. Williams SG, Buscarini M, Stein JP, et al. Molecular markers for
diagnosis, staging and prognosis of bladder cancer. Oncology 2001;
15:1461e1484.
24. Koyama Y, Kaneko K, Akazawa K, et al. Vascular endothelial growth
factor-C and vascular endothelial growth factor-d messenger RNA
expression in breast cancer: association with lymph node metastasis.
Clin Breast Cancer 2003;4:354e360.
25. Onogawa S, Kitadai Y, Tanaka S, et al. Expression of VEGF-C and
VEGF-D at the invasive edge correlates with lymph node metastasis
and prognosis of patients with colorectal carcinoma. Cancer Sci
2004;95:32e39.
26. Ishikawa M, Kitayama J, Kazama S, et al. Expression of vascular
endothelial growth factor C and D (VEGF-C and -D) is an important
risk factor for lymphatic metastasis in undifferentiated early gastric
carcinoma. Jpn J Clin Oncol 2003;33:21e27.
27. Fujimoto J, Toyoki H, Sato E, et al. Clinical implication of expression
of vascular endothelial growth factor-C in metastatic lymph nodes of
uterine cervical cancers. Br J Cancer 2004;91:466e469.
28. Hung CJ, Ginzinger DG, Zarnegar R, et al. Expression of vascular
endothelial growth factor-C in benign and malignant thyroid tumors.
J Clin Endocrinol Metab 2003;88:3694e3699.
29. Arinaga M, Noguchi T, Takeno S, et al. Clinical significance of
vascular endothelial growth factor C and vascular endothelial growth
factor receptor 3 in patients with nonsmall cell lung carcinoma.
Cancer 2003;97:457e464.